
Submitted:
07 February 2024
Posted:
08 February 2024
You are already at the latest version
Abstract
Background. On the subject of couple relationships, the literature pays attention to clinical, socio-anthropological profiles and psychological issues related to the capacity to love, empathy, satisfaction and happiness; however, there is a lack of a psychometric tool that can address the issue of couple stability in a structured and organized manner from an emotional-affective perspective. Objectives. To develop and adjust a psychometric tool that can be efficient and effective in solving the analysis of a coefficient of couple relational stability. Materials and Methods. Clinical interview, based on narrative-anamnestic and documentary evidence, and battery of psychometric tests. Results. In CGa, those who scored more than 20% differential at PLS-Q1 were 58/118 (69%), while in CGb they were 118/118 (100%). In therapy, in the CGa, the resolved cases were 58/58 (100%), while in the CGb, the resolved cases were 110/118 (93%). At the clinical interview, it was found that the 8/118 (7%) "resistant" patients had, according to the PICI-3 model, a diagnosis of borderline personality disorder (5/8, 63%), histrionic-narcissistic (2/8, 25%), and bipolar (1/8, 12%), and thus by their nature not very prone to therapeutic adherence. Conclusions. Perrotta Love Stability Questionnaire (PLS-Q1) is a psychometric tool that offers therapists the opportunity to explore the topic of couple relationship stability, helping them to better focus on patients' vulnerable emotional positions to construct the most appropriate and targeted clinical intervention
Keywords:
Love
; Love stability
; Couple stability
; Perrotta Love Stability Questionnaire
1. Introduction and background
Vocabulary in hand [1], “Love” is a masculine noun defined as "a feeling of lively affection toward a person that manifests itself as a desire to procure his or her good and to seek his or her company". It is precisely this elusive definition that leaves the door open to interpretation. For centuries, poets and philosophers have been extolling love, basically defining it as a "feeling", and declining it in its many forms: as an alchemical magic, as a bond that has a socio-emotional basis, as a meeting of subjective chemistry. The truth is that, to date, we know very little about this "mystery", especially concerning its biochemical nature. [2,3,4] But love may not be only a matter of biochemistry, finding other elements at play that have a strong socio-anthropological, cultural, moral, spiritual, and carnal-reproductive impact.
To define love, cognitive psychologist Robert Sternberg, one of the leading scholars of the construct of intelligence (the triarchical theory: analytic-creative-practical) and emotionality, made a construct that sought to explain the components of love [5,6,7], through the combination of 3 elements: a) passion, which characterizes physical attraction and falling in love; b) intimacy, which defines the stage of mutual emotional attachment and bonding; and c) dedication, which is proper to the rational stage in which each person commits to living with the beloved and decides not to consider other options. From these 3 components of love can arise, according to the author, 7 possible "love" combinations: a) Sympathy: involves only the dimension of intimacy. There is the union between the people but without passion or the characteristics of commitment; b) Infatuation: involves only the dimension of passion, i.e. there is an idealization of the other than a and real knowledge; c) Empty Love: only commitment-decision. That is, the two people are together only because of a rationally made decision that may include economic reasons, values, children, etc.; d) Romantic Love: includes intimacy and passion. It is the love of the great stories of literature, cinema and youth. An immature love but rich in pathos; e) Love-Friendship: includes the dimension of decision-commitment and that of intimacy, but lacks the passion component. These are those relationships in which the couple works, but the passion is gradually blurred; f) Fatuous Love: includes the dimensions of passion and decision-commitment. In these relationships, commitment is dictated only by passion and the desire for possession. These are the classic passionate stories, which run the risk of breaking at the first hitch; g) Perfect Love: is the love that includes all 3 dimensions. A type of love that is complete and difficult to achieve and maintain, but which is not impossible to find.
There is more emphasis in the literature on the topic of love, relationships and possible clinical and psychopathological correlates, while the topic of relationship bonding takes on the connotations of a sociological or anthropological investigation, as in a recent Chinese study [8] that focused on love feeling in general in various relational contexts. To explore the basic elements of love, the "grounded theory" was used to analyze the open-ended responses of 468 people on their feeling of being loved in family, romantic, and friendship relationships, and the results indicated that the feeling of love is an interpersonal process in which one receives a positive response from the other and experiences an authentic bond with the other in a manner consistent across conditions and time (i.e., in a sense of stability). The results of this study suggested an integrated theoretical conceptualization of love as a feeling and shared resource among relationships, which provided important insights into the conceptualization of love.
Based on these findings and the importance of the concept of "couple stability", which is absent in the literature when placed concerning the use of a specific psychometric instrument, it was decided to proceed with the development of a questionnaire aimed at the topic under consideration, taking into account that the literature offers psychometric instruments only on the relationship satisfaction profile (Relationship Assessment Scale, RAS) [9] or on the more general capacity to love (Capacity to Love Inventory, CTL-I) [10,11]
2. Objectives
The main objective of the research, based on the results of the literature and this study, is to identify the exact formula for determining couple relationship stability between two individuals under sentimental bonding, about the participants in the selected population sample and to try to answer the following profiles: 1) ontological, i.e., whether the reality under consideration exists objectively (and thus whether it is possible to determine a couple relationship stability coefficient to compare); 2) epistemological, i.e., whether the reality under consideration is knowable (and whether it is possible to identify the scaling of couple relationship stability to be compared); 3) methodological, i.e., whether the reality under consideration is measurable (and whether it is possible to identify the degree of couple relational stability to be compared using a numerical system); 4) axiological, i.e., whether the reality under consideration is worth studying (and thus whether the coefficient of couple relational stability is functional for determining the critical elements that if modified would lead to an improvement in the framework of couple relational stability).
3. Materials and methods
3.1. Materials
I searched in Pubmed until January 2024, for reviews, meta-analyses, clinical trials and randomized controlled trials, using the keywords “love”, “stability love”, “stability relationship” and “questionnaire” or “test”, content on the abstract and title, have been selected 7 useful results. Simple reviews, opinion contributions or systematic reviews were included because there are no published clinical trials. No limit was placed on the year of publication. [Figure 1]
Perrotta's PHEM-2 model [12,13], while sharing the global view of Sternberg's triarchic construct, departs from it because it examines not only the emotional-cognitive component but also and above all the human bond that depends on interpretative dynamics that do not only concern the subjective emotional plane but also all those dynamics that interfere on it, effectively creating a confusion about the elements at play. The triarchic construct is undoubtedly the summary schema of the love relationship profile, but it does not sufficiently explain the emotional profile without contamination. For this reason, the PHEM-2 was structured taking into account primarily the structural-emotional plane (emotions, feelings and their reactions) and then the functional-emotional plane (consequences, styles and functioning) that would also take into consideration the relational profile, on the one hand keeping the two planes of study well separated but uniting them to proceed to the unified interpretation, using the construct of emotional trajectories (226 in total) according to the specific adaptive mode (distress and pleasure). According to this approach (PHEM-2), therefore, Love is well distinguished from other emotional positions such as passion, friendship, and sympathy, and is described as an adaptive consequence (and not a feeling) that originates from pleasure and through the emotion of joy and the feeling of infatuation (if no oppositely polarizing distressing factors, e.g., fear or frustration, intervene). [Figure 2]
Also according to the PHEM-2 approach, it is not Love that is the cause of pain and suffering, for the following 3 reasons: 1) The "Love", and all its evolutionary path, derives from the positive adaptive mode of pleasure, and therefore can never give rise to negative elements (which instead always originate from distress); 2) To be able to "Love", one must be "available" (understood as a style of behavior oriented toward openness and confrontation, accepting one's limitations and working on them to improve them, questioning oneself) and "sensitive" (understood as global functioning oriented toward knowledge of oneself and others' emotional plan). These characteristics cannot be imitated or simulated, let alone acquired over time, as they pertain to one's structural sphere of personality; if anything, one's functioning can be oriented over time, but with constant effort in this regard. All psychopathologies, however, stem from distress and orient the subject to be neurotic, dramatic or psychotic, thus the exact opposite of the positive modes that lead one to be helpful and sensitive; 3) The pain is an adaptive consequence that always results from anguish, the opposite of pleasure from which the emotional postures connected with Love are derived. Therefore, it is evident that when we suffer "out of Love" we are not suffering from the bond we feel (assuming it derives from pleasure) but from negative emotional positions. In essence, it is never Love that makes us suffer but one of these possible causes: a) the person with whom we are having the relationship, is not suitable for us or does not share the same positive emotional positions as we do, and therefore triggers distressing processes in us that lead to fear, anger or frustration; b) our perception about the emotional bond creates "illusion of love" (and thus fixation) and makes us believe that we feel emotional positions arising from pleasure when in fact they arise from anguish (fear, anger, and frustration); c) our perceptual state is conditioned by one or more elements that interfere with the functional processing of our feelings (e.g. psychopathologies, beliefs, cognitive distortions, etc.). On these assumptions, the development of the PLS-Q1 [Attachment 1] satisfies the need to understand what elements are critical to determine in detail the coefficient of couple relational stability.
"Perrotta Love Stadial Model" (PLSM) recognizes 5 stages (or developmental level), with each specifically describing positive and negative emotional stances. [Table 1]
3.2. Methods
The methods used are three: 1) Clinical interview, based on narrative-anamnestic and documentary evidence and the basis of the Perrotta Human Emotions Model (PHEM) [12,13] concerning their emotional and perceptual-reactive experience; 2) Administration of the battery of psychometric tests published in international scientific journals by the author of this work: a) Perrotta Integrative Clinical Interviews (PICI-3TA) [14], to investigate dysfunctional personality traits; b) Perrotta Individual Sexual Matrix Questionnaire (PSM-Q) [15], to investigate individual sexual matrix; c) Perrotta Love Stability Questionnaire (PLS-Q1), to investigate the stability coefficient of one's love relationship.
The phases of the research were divided as follows: 1) selection of the population sample, according to the parameters indicated in the following paragraph; 2) clinical interview, with each population group; 3) administration of the psychometric tests; 4) data processing following administration and comparison of data obtained; 5) psychotherapy cycle of 4 sessions of couples therapy; 6) administration of the PLS-Q1; 7) data processing following administration and comparison of data obtained.
4. Setting and participants
Inclusion criteria for the first clinical group (CGa) are: 1) age between 21 years and 80 years; 2) sexual gender (male/female) defined; 3) heterosexual orientation; 4) healthy and robust physical constitution, in the absence of striking pathophysiological symptoms; 5) declaration of a stable and lasting romantic relationship, for at least 24 continuous months and in the absence of relationship criticalities capable of interrupting the union relationship; and 6) absence of psychopathological diagnosis or known neurological and neurodegenerative disorders at the time of study participation. Exclusion criteria for the clinical group (CG) are: 1) age less than 21 years and over 80 years; 2) undefined sexual gender (transsexual and non-binary); 3) orientation other than heterosexuality; 4) presence of striking pathophysiological symptoms; 5) declaration of a stable and lasting romantic relationship, less than 24 continuous months or in the presence of current relational crisis; 6) presence of psychopathological diagnoses or known neurological and neurodegenerative disorders at the time of study participation, of at least one of the two partners.
Inclusion criteria for the second clinical group (CGb) are: 1) age between 21 years and 80 years; 2) sexual gender (male/female) defined; 3) heterosexual orientation; 4) healthy and robust physical constitution, in the absence of striking pathophysiological symptoms; 5) declaration of a stable and lasting romantic relationship, for at least 24 continuous months and in the absence of relationship criticalities capable of interrupting the union relationship; and 6) presence of psychopathological diagnoses or known neurological and neurodegenerative disorders at the time of study participation, of at least one of the two partners. Exclusion criteria for the clinical group (CGb) are: 1) age less than 21 years and over 80 years; 2) undefined sexual gender (transsexual and non-binary); 3) orientation other than heterosexuality; 4) presence of striking pathophysiological symptoms; 5) declaration of stable and lasting romantic relationship, less than 24 continuous months or in the presence of current relational crisis; 6) absence of psychopathological diagnoses or known neurological and neurodegenerative disorders at the time of study participation.
The selected setting, taking into account the protracted pandemic period (already in progress since the beginning of the present research), is the online platform via Skype and Video call WhatsApp, both for the clinical interview and for the administration. The present research work was carried out from March 2019 to January 2024. All participants were guaranteed anonymity and the ethical requirements of the Declaration of Helsinki were met. Since the research is not financed by anyone, it is free of conflicts of interest.
The selected first population clinical sample (CGa), which meets the requirements, is 118 couples of participants (236 in total), divided into 6 subgroups [Table 2]:
The selected second population clinical sample (CGb), which meets the requirements, is 118 couples of participants (236 in total), divided into 6 subgroups [Table 3]:
The total population sample is 236 couples, with a total of 472 participants (M: 47.6 years).
5. Results
After the selection of the chosen population sample (first phase), we proceeded with the clinical interviews (second phase), from which the first significant data emerged:
- The total population sample (472 participants) is divided into 236 couples, male/female in monoaffective relationships, further divided into 6 equally distributed subgroups to facilitate statistical analysis.
- Subjects with psychopathological disorders confirmed by certified clinical diagnosis underwent PICI-3 to confirm the diagnosis, and accounted for 40% (189/472) of the total sample (all grouped in CGb), thus at least 1 member per couple (118/118, 100%) or both partners (71/118, 60%).
- Using, during the interview, the strategic language and the PHEM-2 [12,13], the entirety of the population sample selected in the second clinical group (CGb) exhibits a full distress orientation, facilitating feelings such as guilt, shame, anger, frustration, fear, and disappointment, in the presence of unresolved past (childhood) and current (interpersonal and work) stressogenic events.
The third and fourth phases of the research focused on the administration of the battery of questionnaires, to the two study groups, from which the following results emerged for the “clinical group”:
- Administration of the PICI-3. Regarding the analysis of dysfunctional traits (PICI-3TA), the questionnaire confirmed the absence of psychopathology in the first clinical group (CGa), while in the second clinical group (CGb), the correlation emerged that the more marked the psychopathological presence, the greater the gap between the two coefficients of couple stability.
- Administration of the PSM-Q. The PSM questionnaires demonstrated that almost 2/3 of the participants (303/472, 64%) show a dysfunctional tendency towards sexual behaviour and a marked tendency to chronicle feelings of shame in avoidance behaviour or hyposexuality / hypersexuality. Furthermore, 89% (419/472) of the sample of the population interviewed reported having suffered significant or serious psychological or physical abuse at a young age, intra-parental relational imbalances, or in any case a sexual upbringing that was not open and lacking in free communication.
- Administration of the PLS-Q1. Using the PLS-Q1, it was found that the population sample with a divergent “coefficient of couple stability” (Total ERS) between the partners for at least 20% (normal tolerance cut-off: 0-20%) was 200/236 (84.7%) of the total, correlating directly with the temporal duration of the relationship (the longer the relationship duration, the greater the gap between the coefficients of couple stability) and inversely with the fulfillment of relationship promises, such as fidelity or dedication (the greater the gap between the coefficients of couple stability, the lower the score in the emotional position of stages 3, 4 and 5 of the model).
The fifth phase of the research focused on the administration of the couple psychotherapy cycle (a strategic approach) [16,17,18,19], amounting to 4 sessions, weekly lasting 30 minutes each, to rework the data obtained from PLS-Q1 and reinforce any deficiencies. L’approccio strategico è stato preferito ad altri approcci psicoterapeutici in quanto coniuga in sé tecniche, strategie e manovre anche di natura cognitivo-comportamentale [20,21], costruttivista [22,23], umanistica [24,25] e psicodinamica [26,27], ed è la forma che meglio si adatta al campione di popolazione selezionato.
PICI-Model has been the basis of study for the classification of psychopathologies, taking into account that it is based on the classification of the Diagnostic and Statistical Manual of Mental Disorders (DSM-V-TR) [28] and the Psychodynamic Diagnostic Manual (PDM-2). [29] The first 2 sessions focused on the use of strategic language and classical psychotherapeutic intervention, while the last 2 sessions introduced the outcomes of PLS-Q1. Completed the pathway of the entire population sample with divergence greater than 20% (200/200 couples, 100%). [Table 4 and Table 5]
The sixth and seventh phases of the research focused on the re-administration of the PLS-Q1, to check any progress achieved in psychotherapy, confirmed in the second part of the psychotherapy cycle (in the part where the PLS-Q1 data were introduced) due to the use of this psychometric instrument a better focus on couple emotional issues (192/200, 96%) and an absolute resolution of therapy goals even in terms of continuation of the romantic experience or its conclusion (200/200, 100%). [Table 6]
6. Discussions and limits
The present study showed that by using the PLS-Q1, it is possible to improve the focus on the couple's emotional problems and to optimize the resolution of therapeutic goals even in terms of the continuation of the romantic experience or its termination, fostering a more humanistic and clinical approach through the use of this new psychometric instrument.
In the first clinical group (CGa), the one that groups the subjects in the absence of the obvious psychopathological state, those who obtained the PLS-Q1 (Total ERS) score a differential score higher than 20% were 58/118 (69%) in the absence of sentimental-relational crisis, thus more than 2/3 of the sample of the reference population; this figure is rather alarming, as it suggests that they remain in an affective-emotional relationship despite the strong criticalities on the relational level that affect the subjective profile by inducing the subjects also to favor extramarital situations or at any rate different from dialogue and confrontation (through occasional flirtations without consummation of sexual intercourse, cheating, omission, use of chat tools to divert attention from the frustrating relational relationship, pornography and dysregulating sexual behaviors), as revealed by the PSM-Q data that brings out these tendencies in 50/58 subjects (86.2%).
In the second clinical group (CGb), the one that groups subject in the presence of overt psychopathological status or at least 5/9 traits at PICI-3, those who obtained the PLS-Q1 (Total ERS) score a differential score higher than 20% were 118/118 (100%) in the absence of sentimental-relational crisis, thus the totality of the sample of the reference population; this figure is even more alarming than the previous one, as it suggests that these people remain in affective-sentimental relationships despite the strong criticality on the relational level and that these relationships serve as a pathological activator of their dysfunctional psychic state, as also emerges from the PSM-Q data, which compared with the previous group also brings out a total tendency to more or less marked sexual dysfunctional behaviors (118/118, 100%).
Then analyzing the data about the age group shows that in the first clinical group (CGa), the age most representative of relational criticality is the 41-70 age group, with a tendency to decrease with advanced age (an element emphasized during the clinical restitution interviews and justified by the subjects with behaviors of "partial acceptance" concerning the divergences between partners); in the second clinical group (CGb), the age most representative of relational criticality has a greater extent and also covers the younger age groups (21-40 years), demonstrating that the dysfunctional tendency is the representation of the subjective personological picture (an element emphasized during the clinical restitution interviews and justified by the subjects with behaviors of "resignation" concerning the divergences between partners, and for this reason, in this case, dysfunctional sexual behaviors find more space).
The use of the PLS-Q1 is recommended in clinical settings, as its technical support helps the therapist to more effectively centralise the therapy and intervention on the couple. This assertion is confirmed by the data obtained after the administration of a cycle of 4 psychotherapeutic sessions with a strategic approach and the re-administration of the PLS-Q1 to check for changes, both in an ameliorative and a pejorative sense. The data confirmed the marked improvement in the health intervention between the outcome of the first two sessions (without the use of the data obtained from the questionnaire) and the outcome of the second two sessions (with the use of the data obtained from the questionnaire), with a patient satisfaction index of more than 7/10 using a scaling technique. It was also shown that in the first clinical group (CGa), the cases that were resolved (bringing a concrete benefit of at least 50% improvement over the previous emotional position) were 58/58 (100%), while in the second clinical group (CGb), the cases that were resolved (bringing a concrete benefit of at least 50% improvement over the previous emotional position) were 110/118 (93%). At the clinical interview, it was found that the 8/118 (7%) "resistant" patients had, according to the PICI-3 model, a diagnosis of borderline personality disorder (5/8, 63%), hystrio-narcissistic (2/8, 25%), and bipolar (1/8, 12%), and therefore by their nature not very prone to therapeutic adherence.
The present study has both structural and functional limitations that do not, in the writer's opinion, invalidate the quality of the results obtained, but should be taken into consideration for future research to avoid analytical bias. Structurally, the study design calls for the use of three psychometric instruments, such as the PICI-3, PSM-Q and PLS-Q1, but only the first is a validated, efficient and effective psychometric instrument, while the second instrument is a questionnaire that investigates the individual sexual matrix (and thus returns a useful overview for the therapist to better frame the patient) but is not validated, and the same discourse should be applied to the third questionnaire that investigates couple relational stability; in particular, the third questionnaire was designed for this study to fill the gap in the literature about the existence of other instruments that, however, investigated other indices, such as satisfaction and capacity to love. Therefore, it was felt that it could not be validated in the absence of a questionnaire capable of guaranteeing the correct comparisons; however, in psychotherapeutic sessions, as shown in this study, the PLS-Q1 demonstrated all its efficiency and effectiveness as a tool to foster a better emotional approach to relationship problems, focusing in detail on possibly critical emotional positions. Functionally, the study recruited 472 subjects in stable love relationships for at least 2 years, thus 236 actual couples, heterosexual, m/f defined, dividing them first into 2 clinical groups (each of 118 couples) and then into subgroups characterized by age group. Recruitment followed the criteria of inclusion and exclusion, assuming for certain that the declaration of the existence of the love relationship was indeed free from crises capable of compromising the subjective intention to continue; this assumption was necessary to arrive at the study, but this could mask a selection bias, which was, however, excluded by the therapist during the clinical interviews. In the future, therefore, we will try to investigate the selected emotional positions even more thoroughly, introducing new ones and trying to further the validation process of the present questionnaire.
7. Conclusions
In conclusion, Perrotta Love Stability Questionnaire (PLS-Q1) is the psychometric instrument that offers the therapist an opportunity to explore the issue of a couple's relational stability through the analysis of ten emotional positions that characterize the typical stable affective-sentimental relationship. In 30 items, with a dichotomous yes/no response, it helps to better focus the respective vulnerable positions, effectively guaranteeing a more appropriate targeted clinical intervention, and in a strategic key, for the specific couple in crisis or available to deepen their inner knowledge, even in the presence of overt psychopathologies and regardless of the psychotherapeutic approach used.
Funding
This work received no external funding.
Ethics statement
All participants were assured of compliance with the ethical requirements of the Charter of Human Rights, the Declaration of Helsinki in its most up-to-date version, the Oviedo Convention, the guidelines of the National Bioethics Committee, the standards of "Good Clinical Practice" (GCP) in the most recent version, the national and international codes of ethics of reference, as well as the fundamental principles of state law and international laws according to the updated guidelines on observation studies and clinical trial studies.
Informed Consent Statement
Subjects who gave regular informed consent agreements were recruited; moreover, these subjects requested and obtained from GP, as the sole examiner and project manager, not to meet the other study collaborators, thus remaining completely anonymous.
Data Availability Statement
The subjects who participated in the study requested and obtained that GP be the sole examiner during the therapeutic sessions and that all other authors be aware of the participant's data in an exclusively anonymous form.
Acknowledgements
The author who contributed to the work is 1. The author has read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
Perrotta Love Stability Questionnaire (PLS-Q1). Perrotta Love Stadial Theory (PLST). Perrotta Love Stadial Model (PLSM). Perrotta Integrative Clinical Interview 3 (PICI-3). Perrotta Human Emotions Model 2 (PHEM-2).
References
- Treccani. Love. Source: treccani.it/vocabolario/amore/. Accessed in 16.11.23.
- de Boer A, van Buel EM, Ter Horst GJ. Love is more than just a kiss: a neurobiological perspective on love and affection. Neuroscience, 2012; 201:114-24. [CrossRef]
- Bartels A, Zeki S. The neural correlates of maternal and romantic love. Neuroimage, 2004; 21(3):1155-66. [CrossRef]
- Zeki, S. The neurobiology of love. FEBS Lett, 2007; 581(14):2575-9. [CrossRef]
- Sternberg, RJ. A triangular theory of love. Psychological Review, 1986; 93(2):119-135.
- Sternberg, RJ. The Triangle of Love. Intimacy, Passion, Commitment. Basic Books, 1988.
- Sternberg, RJ. Cognitive Psychology. 6th Ed. Pearson Ed., 2018.
- Xia M, Chen Y, Dunne S. What makes people feel loved? An exploratory study on core elements of love across family, romantic, and friend relationships. Fam Process, 2023; e12873. [CrossRef]
- Hendrick SS, Dicke A, Hendrick C. The Relationship Assessment Scale. Journal of Social and Personal Relationships, 1998; 15(1): 137–142.
- Kapusta ND, Jankowski KS, Wolf V, et al. Measuring the Capacity to Love: Development of the CTL-Inventory. Front Psychol, 2018; 9:1115. [CrossRef]
- Margherita G, Gargiulo A, Troisi G, et al. Italian Validation of the Capacity to Love Inventory: Preliminary Results. Front. Psychol., 2018; 9:1434. [CrossRef]
- Perrotta G, Basiletti V, Eleuteri S. The “Human Emotions” and the new “Perrotta Human Emotions Model” (PHEM-2): Structural and functional updates to the first model. Open J Trauma, 2023; 7(1):022-034. Open J Trauma. [CrossRef]
- Perrotta, G. Ergo Sum. I ed. rev. LK ed., 2024.
- Perrotta, G. Perrotta Integrative Clinical Interviews 3 (PICI-3): Development, regulation, updation, and validation of the psychometric instrument for the identification of functional and dysfunctional personality traits and diagnosis of psychopathological disorders, for children (8-10 years), preadolescents (11-13 years), adolescents (14-18 years), adults (19-69 years), and elders (70-90 years). Ibrain, 2024; 14-55. [CrossRef]
- Perrotta, G. “Perrotta Individual Sexual Matrix Questionnaire” (PSM-Q): Technical updates and clinical research. Int J Sex Reprod Health Care, 2021; 4(1):062-066. [CrossRef]
- Perrotta G (2020) The strategic clinical model in psychotherapy: theoretical and practical profiles. J Addi Adol Beh, 2020; 3(1). [CrossRef]
- Perrotta, G. Accepting "change" in psychotherapy: from consciousness to awareness. J Addiction Research and Adolescent Behaviour, 2020; 3(1). [CrossRef]
- Perrotta G (2021) Strategic psychotherapy and the "decagonal model" in clinical practice. Ann Psychiatry Treatm, 5(1): 028-035. [CrossRef]
- Espugnatore G, Fabiano G, Gentili S, et al. La psicoterapia strategica nella pratica clinica. Primiceri Ed., 2023.
- Poerio V, Merenda MT. La psicoterapia cognitivo comportamentale nella pratica clinica. F&L Pub., 2006.
- Ruggiero GM, Sassaroli S. Il colloquio in psicoterapia cognitiva. Tecnica e pratica clinica. Raffaello Cortina Ed., 2013.
- Rezzonico GFA, De Marco I. Lavorare con le emozioni nell’approccio costruttivista. Bollati Boringhieri Ed., 2012.
- Armanino D, Furlani FAP. Identità, personalità e dissociazione. Franco Angeli Ed., 2023.
- Rogers, CR. Un modo di essere. Giunti Ed., 2002.
- Rogers, CR. Potere personale. Astrolabio Ed., 1990.
- Rogers, CR. Terapia centrata sul paziente. Giunti Ed., 2012.
- Gabbard. Psichiatria psicodinamica. Raffaello Cortina Ed., 2019.
- Vasta FN, Gullo S, Girelli R. Psicoterapia psicodinamica di gruppo e ricerca empiricia. Alpes Ed., 2019.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR®). APA, 2022.
- Lingiardi V, McWilliams N. Manuale Diagnostico Psicodinamico. Cortina Ed., 2018.
Figure 1.
PRISMA flow diagram template. Matthew J Page et al. BMJ 2021; 372:bmj.n71.
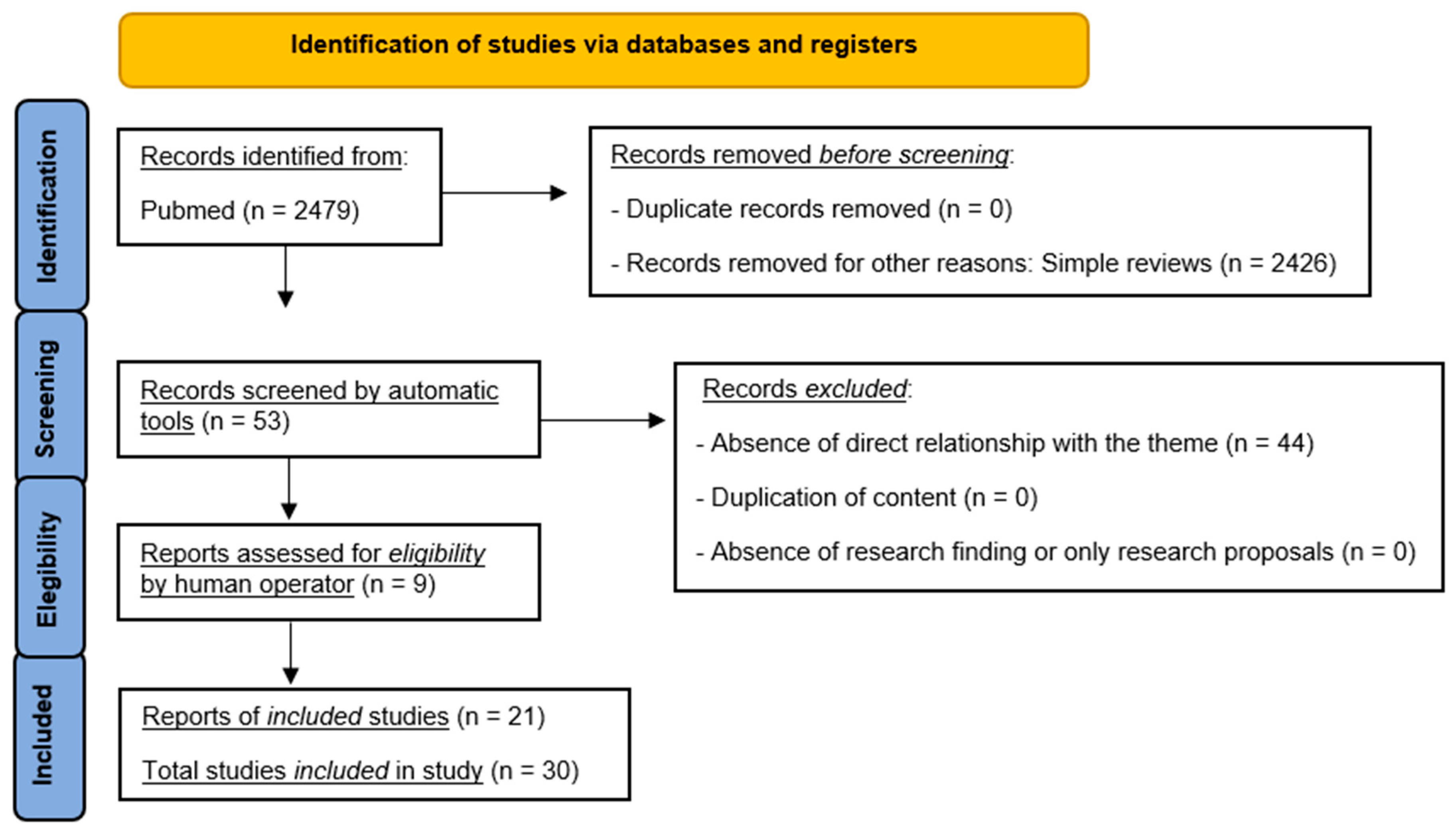
Figure 2.
Perrotta Love Stadial Theory (PLST).
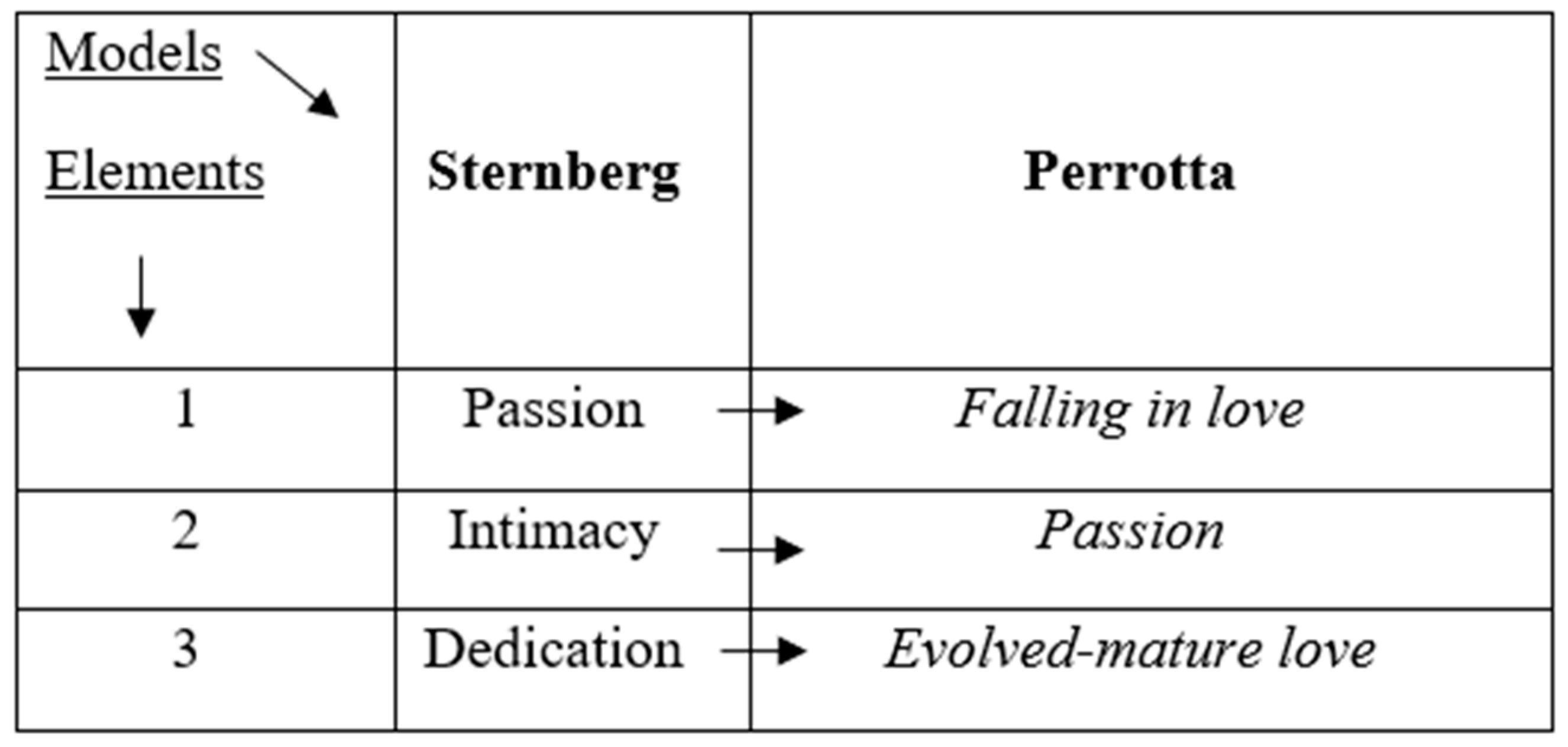

Table 1.
Perrotta Love Stadial Model (PLSM).
|
Level |
Description |
|---|---|
|
A perceives attraction to B. The pleasure resulting from this interest generates admiration for one or more of B's subjective elements and thus triggers in A a first emotional bond. This position may be definitive as the "primordial stage" because it indicates the basis for the potential establishment of love-based bonding. Attraction (AT) is the result of the product between Fascination (FA) and the sum of Satisfaction (SO) and Expectation (AS), and the result is divided by 2: AT = [(SO+AS)*FA]: 2 "Satisfaction" (SO) means the perceptual state of fulfillment of a superficial pleasure, desire or drive. "Expectation" (AS) means the perfect match between what is sought/desired and what is found there. "Fascination" (FA) means the perceptual state of arousal relative to a specific physical or mental feature that can create a link of pleasure. If B reciprocates, “infatuation” is generated in A (1), if he does not reciprocate or the needs are different “disapproval” is generated (2), and if it feeds into both but fades quickly “disinterest” is generated (3). |
|
A, reinforced by B in his previous stage (attraction) feels "infatuation" for B. This stage can last up to 6 months (oxytocin effect) from the conscious moment of feeling attraction. This position can be definitive as the "before-love stage" because it indicates a reinforcement of the basis of the potential establishment of love-based bonding. Infatuation (INF) is the result of the product between the formula of Attraction (AT) and the sum of Passion (PA) and Sharing (CO), and the result divided by 9: INF = [AT*(PA+CO)]: 9 "Passion" (PA) means the intensity of attraction that generates desire, originates from pleasure and consists of perceiving the state of well-being about the enjoyment and exaltation of the experience. "Sharing" (CO) means the perfect match between what one would like to experience/know and what one is experiencing/knowing, finding in the relationship the pleasure of sharing experiences. If B reciprocates in A it generates "falling in love" (1), if it does not reciprocate or the needs are different it generates "fixation" (2); if it feeds into both but fades quickly it generates "disappointment" (3). |
|
A, reinforced by B in his previous stage (infatuation), experiences falling in love with B. This position can be definitive as the "primary love stage" because it indicates a bond that is becoming more and more love-driven. Infatuation (INN) is the result of the product between the formula of Infatuation (INF) and the sum of Esteem (ST) and Sincerity (SI), and the result divided by 6: INN = [INF*(ST+SI)]: 6 "Esteem" (ST) refers to the emotional bond that makes one perceive the other as qualitatively valuable and deserving of attention. "Sincerity" (SI) means the emotional bond that is established as a result of showing that there is consistency between the things they say and the things that happen, there is in essence exact correspondence of truth If B reciprocates in A, evolutionary love is generated (1); if it does not reciprocate or the needs are different, the illusion of love is generated (2); if it feeds into both but fades, loneliness is generated (3). This stage can last up to 18 months from the conscious moment of infatuation. Falling in love is distinguished from infatuation because the purpose of bonding is precisely the lasting extension of the established relationship. |
|
A, reinforced by B in his previous stage (falling in love), experiences an evolved love for B, aimed at stability. This position can be definitive as a "secondary love stage" because it indicates an intense bond of love but is still fragile and meant to be nurtured continuously in a healthy way. Evolutionary love (AE) is the result of the product between the formula of In Love (INN) and the sum of Trust (FI) and Loyalty (LE), and the result divided by 6: AE = [INN*(FI+LE)]: 6 "Trust" (FI) means the emotional bond that is established as a result of demonstrating that there is consistency between the things they say and the things they accomplish. "Loyalty" (LE) means the emotional bond that is established as a result of demonstrating that the person is reliable, efficient, and effective for the partner and by the emotional relationship between them. If B reciprocates in A, mature love is generated (1); if it does not reciprocate or the needs are different, hatred is generated (2); if it is nurtured in both but fades, emptiness is generated (3). This stage can last several decades before evolving (if reinforced and nurtured properly) into mature love. This stage is characterized by a relationship marked by shared couple principles, honesty, sincerity, loyalty, trust and fidelity. |
|
A, strengthened by B in his pre-ceding stage (evolutionary love), feels a mature love for B, which now thrives on stability and complicity. This position can be definitive as "tertiary or circumferential love stage or love need," because it indicates a now stable and lasting love bond. A and B can only reciprocate what they feel because the very nature of this stage is a biological need to belong. Mature love (AM) is the result of the product between the formula of Evolved Love (AE) and Dedication (DE), and the result is divided by 6: AM = [AE*DE]: 6 "Dedication" (DE) means the healthy time spent, in quality and quantity, that is devoted to the relationship. This stage is present in relationships that have lasted for decades, have always been nurtured healthily, and have found their dimension in the coexistence and sharing of their worlds. This stage, as with evolutionary love, is characterized by a relationship marked by shared couple principles, honesty, sincerity, loyalty, trust and fidelity, but also by the need to belong and be there for each other, until a death event marks the conclusion of this love story. |
Table 2.
Population sample (numerousness) - CGa.
| Age | Male | Female | Total |
|---|---|---|---|
| 21-30 | 8 | 8 | 16 |
| 31-40 | 16 | 16 | 32 |
| 41-50 | 30 | 30 | 60 |
| 51-60 | 32 | 32 | 64 |
| 61-70 | 26 | 26 | 52 |
| 71-80 | 6 | 6 | 12 |
| Total | 118 (50%) | 118 (50%) | 236 (100%) |
Table 3.
Population sample (numerousness) - CGb.
| Age | Male | Female | Total |
|---|---|---|---|
| 21-30 | 8 | 8 | 16 |
| 31-40 | 16 | 16 | 32 |
| 41-50 | 30 | 30 | 60 |
| 51-60 | 32 | 32 | 64 |
| 61-70 | 26 | 26 | 52 |
| 71-80 | 6 | 6 | 12 |
| Total | 118 (50%) | 118 (50%) | 236 (100%) |
Table 4.
S.P.S.S., T-test for tests and CGa/CGb differential (descriptive).
|
Test |
CGa |
CGb |
Δ CGa/CGb |
M±DS |
P |
|---|---|---|---|---|---|
|
PICI-3TA |
0% |
100% |
+ 100% |
CGa = 122.6±16.1 |
< 0.001 |
| CGb = 145.0±23.4 | |||||
|
PSM-Q |
33% |
97% |
+ 64% |
CGa = 20.5±5.3 |
< 0.001 |
| CGb = 29.9±8.8 | |||||
|
PLS-Q1 |
69% |
100% |
+ 31% |
CGa = 21.5±4.9 |
< 0.001 |
| CGb = 26.2±4.7 |
Table 5.
S.P.S.S., T-test for tests and groups.
|
Test |
Groups |
CGa (n/%) |
CGb (n/%) |
P |
|---|---|---|---|---|
|
PICI-3TA |
1 (21-30 y) | 0 (0%) | 16 (6.8%) | < 0.001 |
| 2 (31-40 y) | 0 (0%) | 32 (13.6%) | < 0.001 | |
| 3 (41-50 y) | 0 (0%) | 60 (25.4%) | < 0.001 | |
| 4 (51-60 y) | 0 (0%) | 64 (27.1%) | < 0.001 | |
| 5 (61-70 y) | 0 (0%) | 52 (22%) | < 0.001 | |
| 6 (71-80 y) | 0 (0%) | 12 (5.1%) | < 0.001 | |
|
PSM-Q |
1 (21-30 y) | 2 (1%) | 47 (20%) | < 0.001 |
| 2 (31-40 y) | 4 (2%) | 54 (22.9%) | < 0.001 | |
| 3 (41-50 y) | 3 (1.5%) | 49 (20.8%) | < 0.001 | |
| 4 (51-60 y) | 3 (1.5%) | 57 (24.1%) | < 0.001 | |
| 5 (61-70 y) | 1 (0.5%) | 17 (7.2%) | < 0.001 | |
| 6 (71-80 y) | 1 (0.5%) | 5 (2.1%) | < 0.001 | |
|
PLS-Q1 |
1 (21-30 y) | 5 (4.2%) | 21 (17.8%) | < 0.001 |
| 2 (31-40 y) | 5 (4.2%) | 25 (21.2%) | < 0.001 | |
| 3 (41-50 y) | 18 (15.3%) | 36 (30.5%) | < 0.001 | |
| 4 (51-60 y) | 15 (12.6%) | 32 (27.1%) | < 0.001 | |
| 5 (61-70 y) | 10 (8.4%) | 20 (16.9%) | < 0.001 | |
| 6 (71-80 y) | 5 (4.2%) | 8 (6.8%) | < 0.001 |
Table 6.
S.P.S.S., T-test for tests and CGa/CGb differential (after strategic psychotherapy).
|
Test |
Groups |
CGa (n/before) |
CGa (n/after) |
Δ before/after |
P |
|---|---|---|---|---|---|
|
PLS-Q1 |
1 (21-30 y) | 5 | 0 | - 5 | < 0.001 |
| 2 (31-40 y) | 5 | 0 | - 5 | < 0.001 | |
| 3 (41-50 y) | 18 | 0 | - 18 | < 0.001 | |
| 4 (51-60 y) | 15 | 0 | - 15 | < 0.001 | |
| 5 (61-70 y) | 10 | 0 | - 10 | < 0.001 | |
| 6 (71-80 y) | 5 | 0 | - 5 | < 0.001 | |
|
Test |
Groups |
CGb (n/before) |
CGb (n/after) |
Δ before/after |
P |
|
PLS-Q1 |
1 (21-30 y) | 21 | 0 | - 21 | < 0.001 |
| 2 (31-40 y) | 25 | 1 | - 24 | < 0.001 | |
| 3 (41-50 y) | 36 | 2 | - 34 | < 0.001 | |
| 4 (51-60 y) | 32 | 2 | - 30 | < 0.001 | |
| 5 (61-70 y) | 20 | 2 | - 18 | < 0.001 | |
| 6 (71-80 y) | 8 | 1 | - 7 | < 0.001 |
|
Attachment 1. Perrotta Love Stability Questionnaire, first edition (PLS-Q1).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||

© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



