
Submitted:
07 February 2024
Posted:
08 February 2024
You are already at the latest version
Abstract
Oncology has emerged as a crucial field of study and treatment in the domain of medicine. Computed tomography has gained widespread adoption as a radiological modality for the identification and characterisation of pathologies, particularly in oncology, enabling precise identification of affected organs and tissues. However, achieving accurate liver segmentation in computed tomography scans remains a challenge due to the presence of artefacts and the varying densities of soft tissues and adjacent organs. This paper compares artificial intelligence algorithms and traditional medical image processing techniques to assist radiologists in liver segmentation on computed tomography scans, and evaluates their accuracy and efficiency. It is noteworthy that although studies have been conducted on liver segmentation in computed tomography scans, they often lack an intuitive and visual component that allows healthcare professionals to manipulate and observe the results obtained, thereby limiting interaction with the outcomes. From the literature review, challenges such as under-segmentation, over-segmentation, and poor boundary detection, as well as the selection of methods to improve the accuracy and efficiency of liver segmentation in computed tomography scanners, are highlighted as needs to be addressed. The importance of future research in understanding the essential features for the study, generating more datasets, improving segmentation efficiency, and developing lightweight artificial intelligence frameworks for liver segmentation is outlined.
Keywords:
Artificial intelligence
; computed tomography
; hepatic pathologies
; liver segmentation
1. Introduction
As one of the most important organs in the digestive system, the liver performs critical functions such as breaking down nutrients, producing bile and eliminating toxic substances. However, liver-related diseases, particularly oncological diseases, pose health risks, and liver cancer is a leading cause of cancer-related mortality worldwide [1,2]. Computed tomography (CT) has become an integral part of the diagnosis, treatment planning and monitoring the progress of oncological diseases [3,4], providing detailed cross-sectional images for accurate visualisation of internal structures, including liver tumours [5,6].
With the advancement of technology and artificial intelligence (AI) in medicine, there is a growing need to optimise the identification of oncological diseases [7]. Medical image segmentation is emerging as a fundamental step in the pipeline [8,9,10,11]. Liver segmentation in CT scans has emerged as a critical area, requiring accurate identification and delimitation of the liver region for treatment planning and progress monitoring, as well as for early detection of liver lesions and metastases to other organs [12,13,14]. However, accurate liver segmentation on CT scans is challenging due to factors such as artefacts, varying soft tissue densities, and the complexity of adjacent organ proximity [15,16].
The aim of this paper is to provide an overview of the state of the art in the application of AI, as well as traditional methods and techniques for liver segmentation in CT scans, to enable an understanding of which factors most influence the performance of the models and methods used by the selected studies and lead them to perform differently for the same objective.
Some of the aspects that will be compared include datasets considerations, algorithm used, robustness, performance, and evaluation. Specifically, we aim to answer the following research questions (RQ):
- RQ1—What are the challenges and limitations associated with accurate liver segmentation in CT scans?
- RQ2 — How does the choice of the method impact the accuracy and efficiency of liver segmentation in CT scans?
- RQ3 — What are the evaluation metrics commonly used to assess the performance of AI models and traditional methods for liver segmentation in CT scans?
A systematic review of the literature was conducted to address these research questions. Google Scholar was used for document retrieval, and the most representative documents from each year were selected. It is worth noting that only few studies were found that provided an intuitive and visual approach for healthcare professionals to manipulate and interpret the segmentation results.
This paper reviews studies on liver segmentation from CT scans, organised according to the methods used. The papers selection methodology is detailed in Section 2, followed by a categorisation of AI models and medical image processing methods in Section 3. Section 4 summarises the main findings, while Section 5 provides a discussion of the results of the methods used. The paper concludes in Section 6 with the conclusions and the directions for future work.
2. Methodology
This section outlines the approach taken in conducting the literature review, which involved synthesising existing knowledge, critically assessing methodologies, and analysing results to compare the performance of each AI model and traditional methods for liver segmentation in CT scans.
2.1. Data Sources
Google Scholar (https://scholar.google.com/) has developed over the years and has become a robust database for scientific literature [17]. It was therefore chosen as the research tool for the present study.
2.2. Search Queries
A search performed on January 30, 2024, with the query “intitle:Liver + intitle:segmentation + (intitle:CT OR + intitle:tomography)” returned approximately 980 results in just 0.04 seconds.
2.3. Inclusion Criteria
The most relevant papers from each year have been included in the this historical overview. In the context of Google Scholar, relevance refers to the degree to which the search results match the criteria or context of the query. The sorting algorithm takes into account several factors to determine the order of the results, including the presence of search terms and citation counts. In addition, the review papers were all included in the current state of the art, which amounted to a further five documents.
2.4. Exclusion Criteria
Papers that did not meet the criteria defined in Section 2.3 were not included. Papers written in languages other than English, Portuguese and Spanish were also excluded. As a final exclusion criterion, papers were excluded if the full document was not publicly available.
2.5. Characterisation of Selected Papers
The earliest paper dates from 1990, and thus, potentially total of 35 papers could be selected (the most relevant per year between the years 1990 and 2024). A distribution of the total number of papers retrieved per year is given in Figure 1. As can be seen, some years do not have any papers, and thus a total of 30 documents were finally included in the historical review. It is also clear that interest in the topic has increased over the years.
A Word Cloud constructed from the titles of the selected papers is shown on the left side of Figure 2. On the right side is a pie chart showing the number of journals, conference proceedings and reports.
Figure 3 provides the chosen papers by category of image segmentation techniques, according to the categories presented by Sakshi and Kukreja (2023).
3. Literature Review
Based on the selected papers, this literature review provides a historical overview of different methods and approaches for liver segmentation in medical imaging (Section 3.1). It covers neuronal network-based segmentation, region-based segmentation, edge-based segmentation, threshold segmentation, semantic segmentation, and cluster-based segmentation techniques. The review includes a comparison of the results and discusses the potential applications and strengths of each method. Section 3.2 compares this review with other existing summaries of the state of the art.
3.1. Historical Overview
As mentioned in Section 2, one paper per year between the years 1990 and 2024 was selected, summing to a total of 35 documents. For five years the search retrieved no results (see Figure 1) resulting in 30 documents. Unfortunately, the full text of two works was not available. The remaining 28 documents are briefly described below.
The oldest work found to tackle liver segmentation is the one of Bae et al. (1993) [19] present a similar sequential image-by-image segmentation technique using a reference image, where the liver occupies a significant portion of the abdomen cross-section. Image processing techniques, including grey-level thresholding, Gaussian smoothing, and connectivity tracking, are employed to extract the liver boundaries. The resulting boundaries are then smoothed using mathematical morphology techniques and B-splines. The study focuses on a living-donor liver transplant program, and the computer-determined boundaries are compared with those drawn by a radiologist, showing agreement within 10% of the calculated areas.
Gao et al. (1996) [20] focus on facilitating 3D visualisation for surgical planning. The method employs global histogram analysis, morphologic operations, and a parametrically deformable contour model to delineate the liver boundary. Ten cases were used to validate the approach and promising results were found with minimal operator intervention required.
Soler et al. (1997) [21] propose an automatic method for segmenting the portal vein, with the primary objective of achieving accurate segmentation with detailed branching and topological information, facilitating the localisation of liver tumours concerning Couinaud’s anatomical segmentation. The approach involves the initial detection of liver contours using 3D deformable models, followed by limiting the CT images to a liver mask containing hepatic tissue, vascular trees, and potential tumours. Classification of anatomical structures is performed using Gaussian curves fitted to the intensity histogram. The vascular trees and tumours are segmented through a hysteresis thresholding technique based on a distance map, considering the Gaussian parameters. An isotropic image is obtained through shape-based interpolation, and the portal vein is reconstructed using skeletonization, eliminating short branches and correcting errors. Results demonstrate that the algorithm automatically extracts the first three main bifurcations of the portal vein, comparable to manual segmentations.
Yoo et al. (2000) [22] focus on the use of pixel ratios. By analysing the grey value range of a normal liver in CT images, a binary image is generated and then processed into four mesh images based on hole ratios to eliminate noise. A template representing the general outline of the liver is generated from the union image of these mesh images and subtracted from the binary image to accurately represent the organ boundary. The pixel ratio, which takes into account the distribution of organ pixels, was used to discriminate between the organ and noise, especially in cases where organs have similar grey value ranges. The proposed method reduced processing time compared to existing methods and was validated against manual segmentation by medical experts.
Pan and Dawant (2001) [23] introduce a level-set approach, which addresses the challenge of defining appropriate speed functions for contour propagation. A speed function is proposed to stop the propagation of the contour at organ boundaries with weak edges by incorporating accumulative speed based on the path of the contour, enhancing the robustness of segmentation in noisy images. The method also leverages a-priori anatomical information to improve accuracy. Tested on five CT datasets, including cases with abnormal livers, the method demonstrates good agreement with manual delineations.
Saitoh et al. (2002) [24] present an automated method for segmenting the liver region from the third phase of abdominal CT scans. The approach involves the extraction of blood vessels using a threshold, followed by morphological dilation to define an approximate liver region useful for removal of adjacent organs. The final liver region is then extracted using a threshold. The method is thus based on mathematical morphology and thresholding techniques, using the unique characteristics of blood vessels to functionally identify the liver region. The experiments performed on eight CT datasets show a good agreement between the automatically and manually detected liver regions.
Masumoto et al. (2003) [25] use multislice CT images. The method uses two time-varying images acquired during the contrast medium circulation phase, highlighting the liver region through CT value changes. The proposed scheme involves generating a liver likelihood image by analysing CT value changes and subsequently extracting the liver region while considering the geometric characteristics of blood vessels and tumours. The evaluation, based on Receiver Operating Characteristic (ROC) analyses, demonstrates the superiority of the proposed method over other approaches, especially when using information from both phases.
The scheme proposed by Lim et al. (2004) [26] uses a ROI approach to optimise computational efficiency. Morphological filters, incorporating a priori knowledge of liver location and intensity, detect the initial boundary. The algorithm then generates a gradient image using the weighted initial boundary and employs an immersion-based watershed algorithm for segmentation. Post-processing includes region merging based on statistical information to refine the segmentation.
Liu et al. (2005) [27] present a Gradient Vector Flow (GVF) snake-based method for the semiautomatic segmentation of liver volumes in contrast-enhanced CT images. The algorithm follows a stepwise approach, starting with the computation of an initial edge map using the Canny edge detector and the estimation of a liver template. The edge map is then modified to suppress edges within the liver using the liver template, and a concavity removal algorithm is applied to refine the liver boundary. The GVF field is computed based on the modified edge map, and the initial liver contour is determined by considering the candidate initial contour and the computed GVF field. The final liver contour is obtained by deforming the initial contour using the snake. The method is evaluated on 20 contrast-enhanced volumetric liver images, and the results are compared with a radiologist’s manual delineation. The median difference ratio between the computer-generated results and manual results is 5.3%, with a range of 2.9% to 7.6%.
A three-stage approach is used by Lim et al. (2006) [28]. The first stage involves image simplification as preprocessing, where a ROI is identified and thresholds are determined using multilevel thresholding. The second stage detects a search range using multiscale morphological filtering, region-labelling, and partition clustering. The third stage uses a contour-based segmentation approach with a labelling-based search algorithm to refine the initial liver boundary. The effectiveness of the algorithm is demonstrated through experimental results on contrast-enhanced abdominal CT images, with an average segmentation accuracy of 96%. Volume measurement is performed based on the segmented liver regions, with an average error rate of 3%.
Beichel et al. (2007) [29] introduce a two-step process. First, an initial segmentation is generated using graph cuts, overcoming challenges such as the high variability in liver shape and grey-value appearance. Second, an interactive refinement step is introduced, allowing users to correct segmentation errors in a 3D environment. The refinement is facilitated by a hybrid desktop/virtual reality (VR) user interface. This approach is demonstrated on ten contrast-enhanced liver CT scans, demonstrating robustness to variations in patient data. The results also indicate improved segmentation quality with low interaction times.
The authors Massoptier and Casciaro (2008) [30] present a fully automated method that uses a statistical model-based approach to distinguish liver tissue from other abdominal organs. An active contour technique using gradient vector flow is used for smoother segmentation of the liver surface segmentation. Automatic classification is performed to isolate hepatic lesions from liver parenchyma. The method is evaluated on 21 datasets and demonstrates robust and efficient liver and lesion segmentations close to the ground truth, with an average processing time of 11.4 seconds per 512x512-pixel slice. Volume overlap for liver surface segmentation is 94.2%, and accuracy is 3.7 mm. Tumour detection achieved a sensitivity and specificity of 82.6% and 87.5%, respectively.
Heimann et al. (2009) [31] focus on the comparison and evaluation of different methods. The image data, acquired from different CT scanners, consisted of contrast-dye-enhanced scans showing pathological conditions like tumours and cysts. Radiology experts manually delineated the liver contours in transversal slices to create reference segmentations. A total of 40 images were divided into training and test sets for algorithm evaluation. Evaluation measures included volumetric overlap, relative volume difference, and surface distances. Fully automated and interactive segmentation methods were employed, with the former showing discernible performance differences. The best performing automated approaches used statistical shape models. Interactive methods achieved higher scores with more user interaction. A combined approach using majority voting from the best performing methods outperformed individual automated and interactive results.
A three-step procedure is outlined by Akram et al. (2010) [32]. Firstly, a pre-processing step involves converting the image to greyscale and applying a 3x3 median filter to reduce noise. The second step focuses on liver segmentation, with a global threshold and morphological operations to obtain the final segmented liver region. Finally, post-processing steps include adaptive histogram equalisation, Gaussian smoothing, and grey-level transformations to enhance the segmented liver region. Experimental tests on 100 CT images demonstrate the accuracy of the proposed method by comparing automated segmentation results with manually segmented images by hepatologists and oncologists.
The approach of Oliveira et al. (2011) [33] involves a sequence of four steps. First, the liver is segmented using level sets with parameters optimised by a genetic algorithm (GA). A Gaussian fit is employed to define the speed image for level set propagation. Secondly, vessels and nodules are segmented using a Gaussian mixture model, focusing on adipose nodules. A region-growing method with information from the Gaussian model is applied. Thirdly, vessels are classified into portal vein or hepatic vein using a vein tracking method. Finally, a geometric approach based on the identified veins is used to segment the liver into different Couinaud regions. The liver segmentation is based on the assumption that the liver parenchyma homogeneity and veins being mainly inside the liver. The parameters are estimated using a GA, and fitness evaluation involves comparing the segmentation with a reference using five disparity metrics. The proposed method shows good performance, ranking among the top methods in the MICCAI-SLiver07 conference evaluation.
The method developed by Linguraru et al. (2012) [34] uses a robust parameterisation of 3-D surfaces for point-to-point correspondence overcoming challenges such as inconsistent contrast enhancement and imaging artefacts. A shape descriptor that is invariant, invariant under rotation and scale is used to compare local shape features of organs. An initial liver segmentation is refined using a shape-driven geodesic active contour, and hepatic tumours are detected and segmented using graph cuts and support vector machines (SVMs). The technique is evaluated on a dataset of 101 CT scans and shows improvements in liver segmentation accuracy, particularly in cases with large tumours and segmentation errors. Furthermore, the method identifies liver tumours with a low rate of false positives.
Li et al. (2013) [35] discuss a method that makes use of fuzzy clustering and level set techniques. The fuzzy c-Mean (FCM) clustering algorithm is employed, which assigns pixels to different categories based on fuzzy memberships, considering both grey level intensity and spatial information. The FCM algorithm is iteratively optimised by minimising a cost function, allowing for the fuzziness of the resulting partition. To overcome the limitations of standard FCM, a spatial FCM algorithm is introduced that incorporates spatial information into fuzzy membership functions. The paper also introduces the level set method, a continuous deformable model for segmentation. A distance regularised level set evolution (DRLSE) is proposed to address reinitialisation issues and improve efficiency. The proposed method is evaluated using accuracy, sensitivity, and specificity metrics and demonstrates high performance in liver segmentation, especially in cases with unclear boundaries.
Platero et al. (2014) [36] integrate a multi-atlas segmentation approach with graph cuts. The method includes several steps: (1) obtain an initial solution using low-level operations to define the ROI around the liver; (2) construct a fast probabilistic atlas for the ROI and compute a coarse binary segmentation using segmentation-affine registration; (3) rank the atlases based on segmentation similarity and propagating selected atlases to the target image; (4) improve segmentation accuracy through label fusion, minimising a discrete energy function; (5) evaluate the approach using a public liver segmentation database. The experimental results show high accuracy, competitive with human expert segmentation.
Artificial Bee Colony (ABC) optimisation is used by Mostafa et al. (2015) [37]. Their algorithm use ABC to cluster different intensity values in abdominal CT images, followed by mathematical morphological operations to manipulate and separate the clusters. The process eliminates small and thin regions, such as flesh regions or organ edges. The extracted regions form an initial estimate of the liver area, which is further enhanced using a region-growing technique. The proposed approach demonstrates a segmentation accuracy of 93.73% on a test dataset of 38 CT images, taken in the pre-contrast phase.
A 3D Deeply Supervised Network (DSN) is introduced by Dou et al. (2016) [38]. The proposed architecture consists of 11 layers, including 6 convolutional layers, 2 max-pooling layers, 2 deconvolution layers, and 1 softmax layer. The network is designed in a 3D format to effectively capture spatial information. The 3D DSN employs deep supervision via additional deconvolutional layers to counteract vanishing gradients, thus improving the training process. The learning objective is to minimise per-voxel-wise binary classification errors, with deep supervision injected at specific layers. The MICCAI-SLiver07 dataset is used for evaluation, demonstrating that the 3D DSN has a faster convergence and lower errors when compared to traditional 3D Convolutional Neuronal Networks (CNNs).
Christ et al. (2017) [14] propose a Cascaded Fully CNN (CFCN) on CT slices that sequentially segments the liver and lesions. First, various preprocessing steps, including Hounsfield unit windowing and contrast enhancement are applied. Then, the cascaded approach involving two U-Net architectures is used for liver and lesion segmentation. Finally, 3D conditional random fields (CRF) are used to refine the segmentation results. Generalisation and scalability to different modalities and real-life datasets, including a diffusion-weighted Magnetic Resonance Imaging (MRI) dataset and a large multi-centre CT dataset, are shown.
Hiraman (2018) [39] presents a slice alignment method that addresses the challenges through optimal threshold selection, skeletonization, and Enhanced Correlation Coefficient (ECC) alignment. Next, a CNN-based liver region of interest detection method is proposed to classify 2D slices for focused processing.
The study presented by Wang et al. (2019) [40] investigates the application of a Generalised CNN for automated liver segmentation and biometry using cross-sectional data from abdominal CT and MRI scans. The retrospective study included a sample of 563 abdominal scans from 530 adults, covering different imaging modalities. The CNN was initially trained on 300 unenhanced multiecho 2D SPGR MRI sets and then subjected to transfer learning for generalisation across different imaging methods. The accuracy of the CNN was evaluated using internal and external validation datasets. The study also investigates the impact of training data size on segmentation accuracy and explores the feasibility of using automated liver segmentation for volumetry and hepatic PDFF quantification.
Almotairi et al. (2020) [41] explore the application of the SegNet architecture. The proposed modified SegNet model uses the VGG-16 network as an encoder. Tests were performed on a standard dataset for liver CT scans (3D-IRCADb01 [42]) and achieved tumour accuracy of up to 99.9% in the training phase and 86% for tumour identification.
Ayalew et al. (2021) [43] present a modified U-Net architecture and introduce a new class balancing method. To address the class imbalance between liver and tumour, a weighting factor is applied and slices without tumour are removed during data preparation. The U-Net based network architecture includes batch normalisation, dropout layers, and filter size reduction. Training involves tuning hyperparameters, such as learning rate and batch size. The datasets used are derived from the 3D-IRCADb01 [42] and LiTS [44] databases and the results achieve Dice Similarity Coefficient (DSC) of 0.96 and 0.74, respectively. The algorithm also introduces a novel approach for direct tumour segmentation from abdominal CT scan images, with comparable performance to existing two-step methods.
The study of Scicluna (2022) [45] is motivated by challenges such as the Combined Healthy Abdominal Organ Segmentation (CHAOS) Challenge [46], which focuses on healthy abdominal organs. The study focuses on replicating the v16pUNet1.1C model, which demonstrated superior performance in Task 2 of the CHAOS Challenge. Results from the v16pUNet1.1C model are presented and compared with variations in the loss function and scaling transformation. The application of a 3D largest-connected-component filter is discussed, showing improvements in mean scores.
A deep semantic segmentation CNN is used by Ezzat et al. (2023) [47]. A three-stage architecture is proposed, including pre-processing with data augmentation, deep CNN training, and testing. The CNN-based semantic segmentation model is shown to be robust, achieving a test accuracy of 98.8%. The approach does not require user input, making it accessible to non-experts.
Shao et al. (2024) [48] present the Attention Connect Network (AC-Net) for liver tumour segmentation in CT and MRI images. The AC-Net consists of two main modules: the Axial Attention Module (AAM) and the Vision Transformer Module (VTM). The AAM uses an axial attention mechanism to merge features of matching dimensions, maximising the use of spatial features extracted by a CNN. The VTM processes high-level semantic features extracted by the CNN using a methodology similar to Vision Transformers (ViT) [49]. The network achieves a DSC of 0.90, a Jaccard Coefficient (JC) of 0.82, a recall of 0.92, a precision of 0.89, a Hausdorff Distance (HD) of 11.96, and an Average Symmetric Surface Distance (ASD) of 4.59.
3.2. Other Review Papers
The search described in Section 2 retrieved six literature review documents. For one of the works, however, the full document was not available. The remaining five are briefly presented next.
A comparative analysis of various available techniques, focusing on their advantages and disadvantages, is given in [50]. Recognising the challenges posed by the variable shape of the liver and the weak edges in adjacent organ regions, the survey covers approaches such as Threshold, Model, Level Set, Region, Active Contour, and Clustering. The paper also divides its investigation into sections, covering both image pre-processing and segmentation techniques, providing an overview of the current landscape in liver segmentation from CT images.
The study [51] provides a survey of 3D image segmentation methods, focusing on selected binarization and segmentation techniques suitable for processing volume images. For thresholding methods, both global and local techniques are considered, and challenges such as hysteresis in dealing with voxel value distributions are addressed. The region growing section explores voxel-based procedures, including growing by grey value and adaptive region growing. In addition, deformable surfaces and level set methods are discussed, before other segmentation concepts such as fuzzy connectedness and watershed algorithms are introduced. The concluding remarks underline the complexity of image segmentation, emphasising the absence of a universal solution and the need to carefully evaluate and select methods based on specific tasks and dataset characteristics. The challenges posed by 3D data, including the data volume and issues of interactivity and visualisation, are also acknowledged.
The study [52] reviews and proposes a literature survey on methods for segmenting liver images, distinguishing between semi-automatic and fully automated techniques. The challenges of liver image segmentation, such as low contrast, blurred edges, and the complexity of liver morphology, are discussed. Different approaches are reviewed, including neuronal network based methods, support vector machine based methods, clustering based methods and hybrid methods. It is concluded that, despite progress, liver image segmentation remains a challenging task, and the paper encourages further development of hybrid approaches for more accurate segmentation.
Various segmentation methods, including statistical shape models, probabilistic atlas-based approaches, geometric deformable models, and machine learning-based methods, are reviewed in [53]. The review includes information on avaliable databases and challenges in liver tumour segmentation, highlighting the scarcity of public datasets and the need for improved segmentation methods. Liver blood vessel segmentation and computer-assisted diagnosis (CAD) systems are also reviewed. The conclusion highlights the importance of the segmentation, particularly in pathological cases, and the need for improved CAD systems with accurate segmentation for comprehensive analysis of liver treatment.
The survey paper [54] provides a comparative analysis of various available techniques, focusing on their advantages and disadvantages. Grey level-based techniques, such as region growing and active contour methods, are highlighted as effective for liver segmentation. The survey acknowledges the challenges of detecting early-phase liver lesions and emphasises the need for a combination of methods to achieve seamless segmentation, with region growing and active contour methods considered more efficient than other segmentation techniques.
This survey differs from the other documents in this section in a number of ways. Firstly, the most recent of the review papers found dates from 2022. One of the contributions of this work is to present a more up-to-date view of the works published since then. In addition, none of the other works presents a historical perspective on the subject, starting from 1990, as is the case with the present review.
4. Findings
A summary of the papers reviewed in Section 3.1 is given in Table 1. The columns of the table contain the following information: identification of each study (column Authors); publication year (column Year); general category or approach used in the segmentation method as defined in [18] (column Segmentation Category); the specific segmentation technique or algorithm (column Method); whether the method is fully-automatic or semi-automatic (column Autom. Level for Automation Level); whether the segmentation is performed in 2D or 3D (column Dim. for Dimensionality); the dataset or database used for evaluation (column Database); and the key results of the best segmentation method in each paper (column Results).
It is clear from this table that prior to 2016 there was no predominant category. Region-based Segmentation, Edge-based Segmentation, Threshold Segmentation, Semantic Segmentation, Cluster-based Segmentation and even combinations of several methods were tried. However, since 2016, Neuronal network-based techniques have dominated the field. Remembering the huge impact that AlexNet [55] had in winning the ImageNet Large Scale Visual Recognition Challenge (ILSVRC) in 2012 [56], it is clear that Liver Segmentation in CT scans took a few years to catch up with the state of the art research. This is probably due to the arrival of U-Net [57], which was proposed in 2015, and is specifically designed for biomedical image segmentation.
In terms of automation, both fully automated and semi-automated techniques have been explored. While it is nice to have fully-automatic, accurate and fast techniques, the final decision should always belong to the specialist. Thus, we advocate fully automatic methods for contour initialisation, together with the development of intuitive tools that allow specialists to modify the fully-automatically generated contour if they feel the need to do so.
Both slice-based (2D) and volume-based (3D) methods have been developed. As an anatomical structure, we believe that liver segmentation methods should be inherently three-dimensional. This would have two main advantages. On the one hand, fully 3D methods would make use of more contextual information and thus potentially provide better segmentations. On the other hand, the development of fully three-dimensional techniques would avoid the need of the slice-based methods to aggregate all of the segmentations into a coherent volume. This aggregation could not only lead to errors and anatomically incorrect structures, but would also increase computational time.
Data availability is a major concern, as most methods use private datasets. This inhibits reproducibility of the results. In addition, researchers who do not have access to hospitals or other facilities with CT scanners, cannot develop new techniques for this particular problem. We advocate making the data available, while respecting all the ethical that are important when dealing with medical data and properly anonymising any sensitive information. Some notable exceptions to publicly available datasets are listed in Section 5.1.
5. Discussion
As seen in the previous section, significant advances in liver segmentation techniques have been presented, with particular impact due to the adoption of AI methods, more specifically neuronal network techniques. In this section, we provide some considerations on publicly available databases (Section 5.1), the impact of the widespread adoption of neuronal networks since 2017 (Section 5.2), a comparison between 2D and 3D implementations (Section 5.3), and Section 5.4 present answers to the research questions posed in the introductory section.
5.1. Public Datasets Analysis
The most common public datasets used in studies of liver segmentation on CT scans include 3D-IRCADb01, LiTS17 and MICCAI-SLiver07. According to the dataset’s comparison provided by Al-Saeed et al. [58] (shown in Table 2), it is possible to identify several key differences that may have implications for data processing and analysis, as different formats and significant differences in resolution between datasets may require different approaches to processing and interpretation.
5.2. Impact of the Adoption of Neuronal Network-based Methods
The growth of neuronal network-based approaches has led to remarkable progress in liver segmentation, particularly with respect to CT scans. These models have led to a new era of accuracy and efficiency, significantly outperforming traditional methods [55,57]. This improved accuracy has become critical in the field of medical imaging, where the correct interpretation of CT scans can directly affect the diagnosis and treatment plans of patients. Furthermore, the efficiency of these neuronal network models translates into faster processing times, allowing for more agile decision making in clinical settings.
Another positive aspect of neuronal networks in liver segmentation is their ability to cope with the complexity of liver anatomy. Neuronal networks, with their systematic and complex pattern recognition capabilities, are able to navigate these anatomical variations. As a result, they are better able to deal with the variety of appearances that liver tissue can have on CT scans. This ability to handle complex datasets ensures that neuronal networks can provide consistent and accurate segmentation in a wide range of cases.
5.3. Comparison between 2D and 3D Methods for Liver Segmentation
-
Importance of Choosing between 2D and 3D Methods
- –
- In medical imaging, and in particular liver segmentation, the choice between slice-based 2D and volume-based 3D segmentation methods is crucial. This decision is highly dependent on the anatomical structure of the liver. Given the complex, three-dimensional nature of the liver, 3D segmentation techniques often prove to be the most appropriate choice [21] [39]. These methods are inherently designed to understand and process the volumetric characteristics of the liver, which is a critical consideration for accurate segmentation results.
-
2D Segmentation Limitations
- –
- Although 2D slice-based segmentation is widely used, it has limitations, particularly when it comes to dealing with complex organs such as the liver. The main challenge with 2D methods is their inability to fully capture all the regions of the liver. They involve working with individual slices, which can provide a fragmented understanding of the organ structure, but this fragmentation can lead to inconsistencies and errors when these individual slices are aggregated to form a complete image [40].
-
3D Segmentation Advantages
- –
- In order to overcome the limitations of 2D segmentation, 3D segmentation has the ability to use more contextual information. Unlike 2D methods, which visualise the liver in individual slices, 3D techniques consider the organ in its integrity, as they have the ability to ensure anatomical correctness by processing the liver as a single, continuous volume, avoiding errors that can arise from the aggregation of 2D slices [14] [38]. In 2D segmentation, inconsistencies can occur when individual slices are combined, leading to inaccuracies in the representation of liver anatomy. The holistic view provided by the 3D segmentation, results in more accurate segmentation, as it takes into account the spatial relationships and continuity between the different sections of the liver. The inclusion of this additional contextual information can potentially lead to segmentation results, especially in complex cases where the shape and size of the liver can vary considerably.
5.4. Exploring Research Questions
Following the specific analysis of the studies presented and their main findings, the questions raised in Section 1 are answered as follows.
-
RQ1—What are the challenges and limitations associated with accurate liver segmentation in CT scans?
- –
- Challenges and limitations associated with accurate liver segmentation in CT images include under-segmentation, over-segmentation, low contrast, poor boundary detection and background segmentation due to noise. In addition, liver segmentation in CT scans is further challenged by the presence of artefacts, such as partial volumes, noise, and low sharpness and contrast between organs, making it difficult to identify the boundaries between different tissues.
-
RQ2 — How does the choice of the method impact the accuracy and efficiency of liver segmentation in CT scans?
- –
- The choice of the method has a significant impact on the accuracy and efficiency of liver segmentation in CT scans. Traditional techniques such as image processing and region-growing approaches have shown varying degrees of sensitivity and specificity, with some challenges in dealing with large injuries. In contrast, newer methods such as FCN, DBN-DNN, and techniques like ResU-Net and SegNet showed higher accuracy, with some reaching up the highest accuracy levels. Notably, advances in methods have also led to significant improvements in processing times, with strategies such as using GPU over CPU leading to significant time reductions, indicating a trend towards more efficient and accurate liver segmentation techniques.
-
RQ3 — What are the evaluation metrics commonly used to assess the performance of AI models and traditional methods for liver segmentation in CT scans?
- –
- Some of the key metrics used to measure the outcome of segmentation techniques include Dice Similarity Coefficient (DSC), accuracy, precision, sensitivity, specificity, and segmentation speed. There is not much consistency in the metrics presented by the various studies except for DSC.
6. Conclusions and Future Work
The evolution of liver segmentation techniques throughout history reflects the broad impact of AI technologies across a wide range of disciplines. The transition to fully automated segmentation methods has been an important breakthrough in the process, although the indispensable involvement of medical experts continues to play a key role in ensuring the accuracy and clinical relevance of these techniques. The emerging prevalence of 3D segmentation methods, which follow the structure of the liver, promises more accurate and anatomically consistent results.
However, there are a number of challenges that need to be addressed in order to advance the field. The lack of public datasets is one of the main barriers to the advancement of liver segmentation technologies. Research has mainly been conducted on private datasets, often restricted to specific medical centres, which limits wider participation in research and makes it difficult to replicate.
In terms of future developments, the outlook for the evolution of liver segmentation is unfolding in several core areas that promise to have a significant impact on research and application in this field. The increasing availability of public datasets is key to fostering innovation, enabling the contribution of researchers from diverse backgrounds and promoting a dynamic research environment. In addition, the definition of specific standardised evaluation metrics is crucial to allow meaningful comparisons between segmentation methods and to guide the development towards more efficient, accurate and user-friendly solutions, such as contour and region-based metrics, performance metrics and user intervention metrics.
The further application of 3D segmentation techniques may be a good investment, as they can provide more anatomically accurate and consistent anatomical results, overcoming the limitations of 2D segmentations. Furthermore, the effective integration of medical expertise in segmentation automation is indeed essential, with the aim of developing interfaces that allow specialists to interact with automated segmentation results, ensuring that liver segmentation tools are both technically advanced and clinically relevant and feasible. Collaboration between cutting-edge technology and human expertise is a good approach, combining the efficiency of automation with the refined understanding of healthcare professionals, whose oversight remains critical to maintain the accuracy and reliability of the final results.
Author Contributions
Conceptualisation, J.B.; Methodology, S.B.N. and J.B.; Software, S.B.N.; Validation, S.B.N., I.D. and J.B.; Formal analysis, S.B.N., I.D. and J.B.; Investigation, S.B.N.; Resources, S.B.N.; Data curation, S.B.N.; Writing—original draft preparation, S.B.N.; Writing—review and editing, S.B.N., I.D. and J.B.; Supervision, J.B. and I.D.; Project administration, J.B. and I.D.; Funding acquisition, I.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Francque, S. The Liver and the Cardiovascular System: Two of a Kind? Journal of the American Heart Association 2021, 10, e020286. [Google Scholar] [CrossRef]
- Trefts, E.; Gannon, M.; Wasserman, D.H. The liver. Current Biology 2017, 27, R1147–R1151. [Google Scholar] [CrossRef]
- Mendes, B.; Domingues, I.; Silva, A.; Santos, J. Prostate Cancer Aggressiveness Prediction Using CT Images. Life 2021, 11, 1164. [Google Scholar] [CrossRef]
- Pereira, G.; Domingues, I.; Martins, P.; Abreu, P.H.; Duarte, H.; Santos, J. Registration of CT with PET: A Comparison of Intensity-Based Approaches. In International Workshop on Combinatorial Image Analysis (IWCIA); Springer, 2018; pp. 134–149. [Google Scholar] [CrossRef]
- Zhang, H.; Luo, K.; Deng, R.; Li, S.; Duan, S. Deep Learning-Based CT Imaging for the Diagnosis of Liver Tumor. Computational Intelligence and Neuroscience 2022, 2022, 1–7. [Google Scholar] [CrossRef]
- Vernuccio, F.; Cannella, R.; Bartolotta, T.V.; Galia, M.; Tang, A.; Brancatelli, G. Advances in liver US, CT, and MRI: moving toward the future. European Radiology Experimental 2021, 5, 52. [Google Scholar] [CrossRef]
- Domingues, I.; Cardoso, J.S. Using Bayesian surprise to detect calcifications in mammogram images. 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, 2014, pp. 1091–1094. [CrossRef]
- Mendes, B.; Domingues, I.; Santos, J. Multi-class Semantic Segmentation for Prostate Cancer Radiotherapy Treatment Optimization. International Conference on Mathematical Analysis and Applications in Science and Engineering (ICMA2SC), 2022.
- Bechar, M.E.A.; Settouti, N.; Domingues, I. Deep Learning vs. Super Pixel Classification for Breast Masses Segmentation. In Deep Learning for Biomedical Applications; CRC Press, 2021; pp. 121–156. [Google Scholar]
- Oliveira, A.C.; Domingues, I.; Duarte, H.; Santos, J.; Abreu, P.H. Going Back to Basics on Volumetric Segmentation of the Lungs in CT: A Fully Image Processing Based Technique. In Iberian Conference on Pattern Recognition and Image Analysis (IbPRIA); Springer, 2019; Vol. 11868 LNCS, pp. 322–334. [Google Scholar]
- Carbone, I.; Martins, P.; Teixeira, A.; Silva, A. A Vocal Tract Segmentation and Analysis over a European Portuguese MRI Database. Revista do Departamento de Electrónica e Telecomunicações, Universidade de Aveiro 2008, 4, 1050–1053. [Google Scholar]
- Zhou, L.Q.; Wang, J.Y.; Yu, S.Y.; Wu, G.G.; Wei, Q.; Deng, Y.B.; Wu, X.L.; Cui, X.W.; Dietrich, C.F. Artificial intelligence in medical imaging of the liver. World Journal of Gastroenterology 2019, 25, 672–682. [Google Scholar] [CrossRef] [PubMed]
- Chlebus, G.; Schenk, A.; Moltz, J.H.; van Ginneken, B.; Hahn, H.K.; Meine, H. Automatic liver tumor segmentation in CT with fully convolutional neural networks and object-based postprocessing. Scientific Reports 2018, 8, 15497. [Google Scholar] [CrossRef] [PubMed]
- Christ, P.F.; Ettlinger, F.; Grün, F.; Elshaera, M.E.A.; Lipkova, J.; Schlecht, S.; Ahmaddy, F.; Tatavarty, S.; Bickel, M.; Bilic, P.; Rempfler, M.; Hofmann, F.; Anastasi, M.D.; Ahmadi, S.A.; Kaissis, G.; Holch, J.; Sommer, W.; Braren, R.; Heinemann, V.; Menze, B. Automatic Liver and Tumor Segmentation of CT and MRI Volumes using Cascaded Fully Convolutional Neural Networks. arXiv 1702.05970 2017, [1702.05970].
- Ansari, M.Y.; Abdalla, A.; Ansari, M.Y.; Ansari, M.I.; Malluhi, B.; Mohanty, S.; Mishra, S.; Singh, S.S.; Abinahed, J.; Al-Ansari, A.; Balakrishnan, S.; Dakua, S.P. Practical utility of liver segmentation methods in clinical surgeries and interventions. BMC Medical Imaging 2022, 22, 97. [Google Scholar] [CrossRef]
- Le, D.C.; Chinnasarn, K.; Chansangrat, J.; Keeratibharat, N.; Horkaew, P. Semi-automatic liver segmentation based on probabilistic models and anatomical constraints. Scientific Reports 2021, 11, 6106. [Google Scholar] [CrossRef] [PubMed]
- Halevi, G.; Moed, H.; Bar-Ilan, J. Suitability of Google Scholar as a source of scientific information and as a source of data for scientific evaluation—Review of the Literature. Journal of Informetrics 2017, 11, 823–834. [Google Scholar] [CrossRef]
- Sakshi.; Kukreja, V. Image Segmentation Techniques: Statistical, Comprehensive, Semi-Automated Analysis and an Application Perspective Analysis of Mathematical Expressions. Archives of Computational Methods in Engineering 2023, 30, 457–495. [CrossRef]
- Bae, K.T.; Giger, M.L.; Chen, C.T.; Kahn Jr, C.E. Automatic segmentation of liver structure in CT images. Medical physics 1993, 20, 71–78. [Google Scholar] [CrossRef]
- Gao, L.; Heath, D.G.; Kuszyk, B.S.; Fishman, E.K. Automatic liver segmentation technique for three-dimensional visualization of CT data. Radiology 1996, 201, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Soler, L.; Malandain, G.; Montagnat, J.; Delingette, H.; Ayache, N.; Clément, J.M.; Roy, C.; Russier, Y.; Tassetti, V.; Marescaux, J. Automatic Segmentation of Portal Vein in CT-Scans of the Liver. World Congress on Medical Physics and Biomedical Engineering (MPBE), 1997, p. 788.
- Yoo, S.W.; Cho, J.S.; Noh, S.M.; Shin, K.S.; Park, J.W. Advanced Liver Segmentation by Using Pixel Ratio in Abdominal CT Image. IEEK Conference. The Institute of Electronics and Information Engineers, 2000, pp. 39–42.
- Pan, S.; Dawant, B.M. Automatic 3D segmentation of the liver from abdominal CT images: a level-set approach. Medical Imaging: Image Processing. SPIE, 2001, Vol. 4322, pp. 128–138. [CrossRef]
- Saitoh, T.; Tamura, Y.; Kaneko, T. Automatic segmentation of liver region through blood vessels on multi-phase CT. International Conference on Pattern Recognition. IEEE, 2002, Vol. 1, pp. 735–738. [CrossRef]
- Masumoto, J.; Hori, M.; Sato, Y.; Murakami, T.; Johkoh, T.; Nakamura, H.; Tamura, S. Automated liver segmentation using multislice CT images. Systems and Computers in Japan 2003, 34, 71–82. [Google Scholar] [CrossRef]
- Lim, S.J.; Jeong, Y.Y.; Lee, C.W.; Ho, Y.S. Automatic segmentation of the liver in CT images using the watershed algorithm based on morphological filtering. Medical Imaging: Image Processing. SPIE, 2004, Vol. 5370, pp. 1658–1666. [CrossRef]
- Liu, F.; Zhao, B.; Kijewski, P.K.; Wang, L.; Schwartz, L.H. Liver segmentation for CT images using GVF snake. Medical physics 2005, 32, 3699–3706. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.J.; Jeong, Y.Y.; Ho, Y.S. Automatic liver segmentation for volume measurement in CT Images. Journal of Visual Communication and Image Representation 2006, 17, 860–875. [Google Scholar] [CrossRef]
- Beichel, R.; Bauer, C.; Bornik, A.; Sorantin, E.; Bischof, H. Liver segmentation in CT data: A segmentation refinement approach. 3D Segmentation in The Clinic: A Grand Challenge, 2007, pp. 235–245.
- Massoptier, L.; Casciaro, S. A new fully automatic and robust algorithm for fast segmentation of liver tissue and tumors from CT scans. European radiology 2008, 18, 1658–1665. [Google Scholar] [CrossRef]
- Heimann, T.; Van Ginneken, B.; Styner, M.A.; Arzhaeva, Y.; Aurich, V.; Bauer, C.; Beck, A.; Becker, C.; Beichel, R.; Bekes, G.; others. Comparison and evaluation of methods for liver segmentation from CT datasets. IEEE transactions on medical imaging 2009, 28, 1251–1265. [CrossRef]
- Akram, M.U.; Khanum, A.; Iqbal, K. An automated system for liver CT enhancement and segmentation. ICGST Journal of Graphics, Vision and Image Processing (ICGST-GVIP) 2010, 10, 17–22. [Google Scholar]
- Oliveira, D.A.; Feitosa, R.Q.; Correia, M.M. Segmentation of liver, its vessels and lesions from CT images for surgical planning. Biomedical engineering online 2011, 10, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Linguraru, M.G.; Richbourg, W.J.; Jianfei Liu.; Watt, J.M.; Pamulapati, V.; Shijun Wang.; Summers, R.M. Tumor Burden Analysis on Computed Tomography by Automated Liver and Tumor Segmentation. IEEE Transactions on Medical Imaging 2012, 31, 1965–1976. [CrossRef]
- Li, X.; Luo, S.; Li, J. Liver Segmentation from CT Image Using Fuzzy Clustering and Level Set. Journal of Signal and Information Processing 2013, 04, 36–42. [Google Scholar] [CrossRef]
- Platero, C.; Tobar, M.C.; others. A multiatlas segmentation using graph cuts with applications to liver segmentation in CT scans. Computational and mathematical methods in medicine 2014, 2014. [CrossRef]
- Mostafa, A.; Fouad, A.; Abd Elfattah, M.; Hassanien, A.E.; Hefny, H.; Zhu, S.Y.; Schaefer, G. CT liver segmentation using artificial bee colony optimisation. Procedia Computer Science 2015, 60, 1622–1630. [Google Scholar] [CrossRef]
- Dou, Q.; Chen, H.; Jin, Y.; Yu, L.; Qin, J.; Heng, P.A. 3D deeply supervised network for automatic liver segmentation from CT volumes. 19th International Conference on Medical Image Computing and Computer-Assisted Intervention (MICCAI). Springer, 2016, pp. 149–157. [CrossRef]
- Hiraman, A. Liver segmentation using 3D CT scans. PhD thesis, University of Kwazulu-Natal, 2018.
- Wang, K.; Mamidipalli, A.; Retson, T.; Bahrami, N.; Hasenstab, K.; Blansit, K.; Bass, E.; Delgado, T.; Cunha, G.; Middleton, M.S.; others. Automated CT and MRI liver segmentation and biometry using a generalized convolutional neural network. Radiology: Artificial Intelligence 2019, 1, 180022. [CrossRef]
- Almotairi, S.; Kareem, G.; Aouf, M.; Almutairi, B.; Salem, M.A.M. Liver tumor segmentation in CT scans using modified SegNet. Sensors 2020, 20, 1516. [Google Scholar] [CrossRef]
- Soler, L.; Hostettler, A.; Agnus, V.; Charnoz, A.; Fasquel, J.; Moreau, J.; Osswald, A.; Bouhadjar, M.; Marescaux, J. 3D Image Reconstruction for Comparison of Algorithm Database: A Patient Specific Anatomical and Medical Image Database. Tech. rep, IRCAD, Strasbourg, France, 2010.
- Ayalew, Y.A.; Fante, K.A.; Mohammed, M.A. Modified U-Net for liver cancer segmentation from computed tomography images with a new class balancing method. BMC Biomedical Engineering 2021, 3, 4. [Google Scholar] [CrossRef]
- LiTS Challenge Dataset. https://competitions.codalab.org/competitions/17094. Accessed: Nov. 27, 2023.
- Scicluna, D. Automatic segmentation of healthy liver in abdominal computed tomography scans. Master’s thesis, University of Malta, 2022.
- Kavur, A.E.; Gezer, N.S.; Barış, M.; Aslan, S.; Conze, P.H.; Groza, V.; Pham, D.D.; Chatterjee, S.; Ernst, P.; Özkan, S.; Baydar, B.; Lachinov, D.; Han, S.; Pauli, J.; Isensee, F.; Perkonigg, M.; Sathish, R.; Rajan, R.; Sheet, D.; Dovletov, G.; Speck, O.; Nürnberger, A.; Maier-Hein, K.H.; Bozdağı Akar, G.; Ünal, G.; Dicle, O.; Selver, M.A. CHAOS Challenge - combined (CT-MR) healthy abdominal organ segmentation. Medical Image Analysis 2021, 69, 101950. [Google Scholar] [CrossRef] [PubMed]
- Ezzat, K.A.; Omran, L.N.; El Seddawy, A.I.B. Automatic liver segmentation in computed tomography scans using deep semantic segmentation. Bulletin of Electrical Engineering and Informatics 2023, 12, 250–256. [Google Scholar] [CrossRef]
- Shao, J.; Luan, S.; Ding, Y.; Xue, X.; Zhu, B.; Wei, W. Attention Connect Network for Liver Tumor Segmentation from CT and MRI Images. Technology in Cancer Research & Treatment 2024, 23, 15330338231219366. [Google Scholar] [CrossRef]
- Maurício, J.; Domingues, I.; Bernardino, J. Comparing Vision Transformers and Convolutional Neural Networks for Image Classification: A Literature Review. Applied Sciences 2023, 13. [Google Scholar] [CrossRef]
- Priyadarsini, S.; Selvathi, D. Survey on segmentation of liver from CT images. IEEE international conference on advanced communication control and computing technologies (ICACCCT), 2012, pp. 234–238. [CrossRef]
- Mharib, A.M.; Ramli, A.R.; Mashohor, S.; Mahmood, R.B. Survey on liver CT image segmentation methods. Artificial Intelligence Review 2012, 37, 83–95. [Google Scholar] [CrossRef]
- Khan, F. Automated segmentation of CT liver images: a review. Journal of Communications Technology, Electronics and Computer Science 2018, 19, 5–9. [Google Scholar]
- Moghbel, M.; Mashohor, S.; Mahmud, R.; Saripan, M.I.B. Review of liver segmentation and computer assisted detection/diagnosis methods in computed tomography. Artificial Intelligence Review 2018, 50, 497–537. [Google Scholar] [CrossRef]
- Vanmore, S.V.; Chougule, S.R. Survey on automatic liver segmentation techniques from abdominal CT images. International Conference on Intelligent Computing and Control Systems (ICCS). IEEE, 2019, pp. 1030–1035. [CrossRef]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Advances in neural information processing systems 2012, 25. [Google Scholar] [CrossRef]
- Russakovsky, O.; Deng, J.; Su, H.; Krause, J.; Satheesh, S.; Ma, S.; Huang, Z.; Karpathy, A.; Khosla, A.; Bernstein, M.; Berg, A.C.; Fei-Fei, L. ImageNet Large Scale Visual Recognition Challenge. International Journal of Computer Vision (IJCV) 2015, 115, 211–252. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. CoRR 2015, abs/1505.04597, [1505.04597].
- Al-Saeed, Y.; Gab-Allah, W.; Elmogy, M. Hepatic tumors diagnosis system based on fuzzy c-means using computed tomography images. Research Square Preprint 2022. [Google Scholar] [CrossRef]
- MICCAI-Sliver07. https://sliver07.grand-challenge.org/. Accessed: Nov. 27, 2023.
Figure 1.
Distribution of the retrieved papers over the years
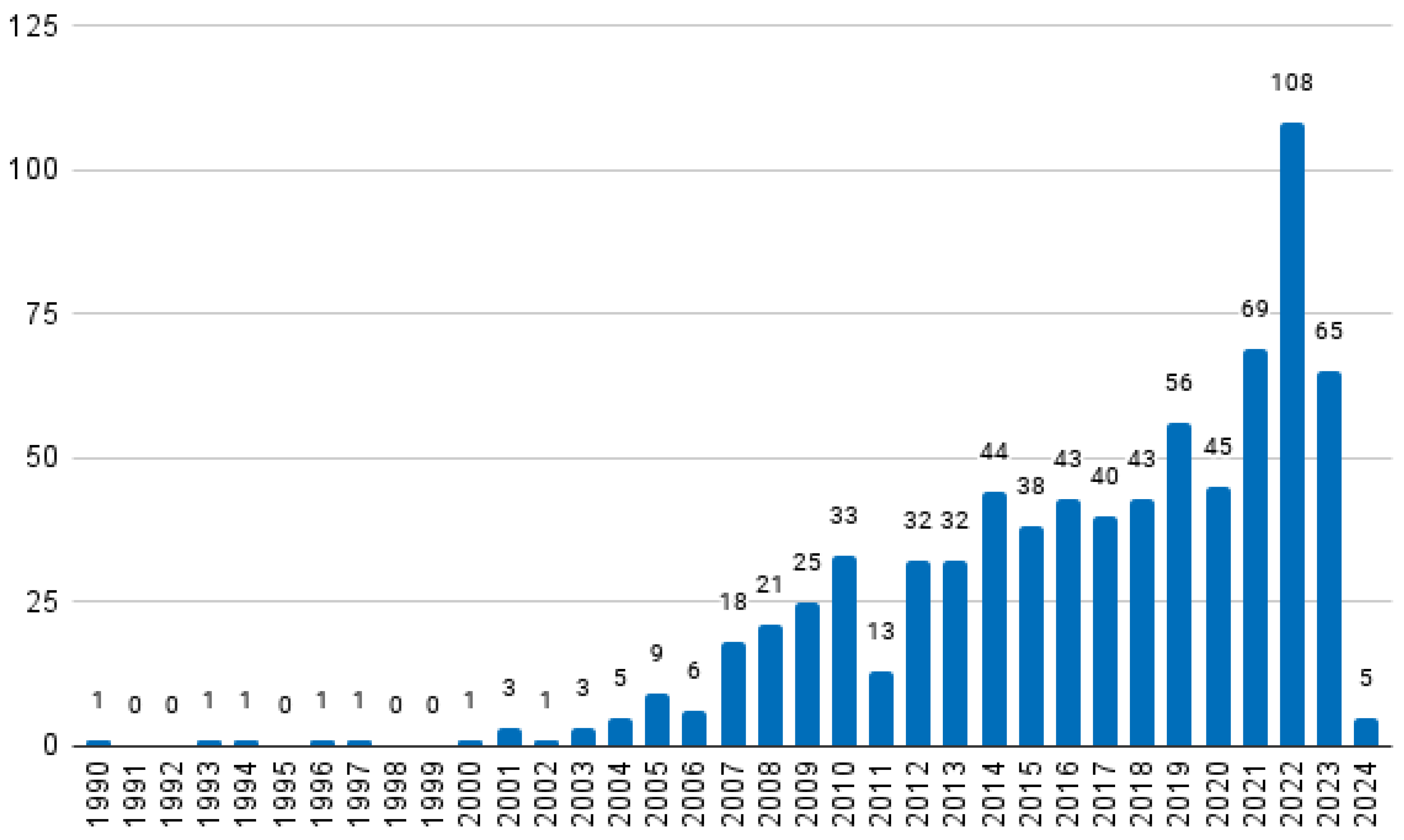
Figure 2.
Characterisation of the selected papers
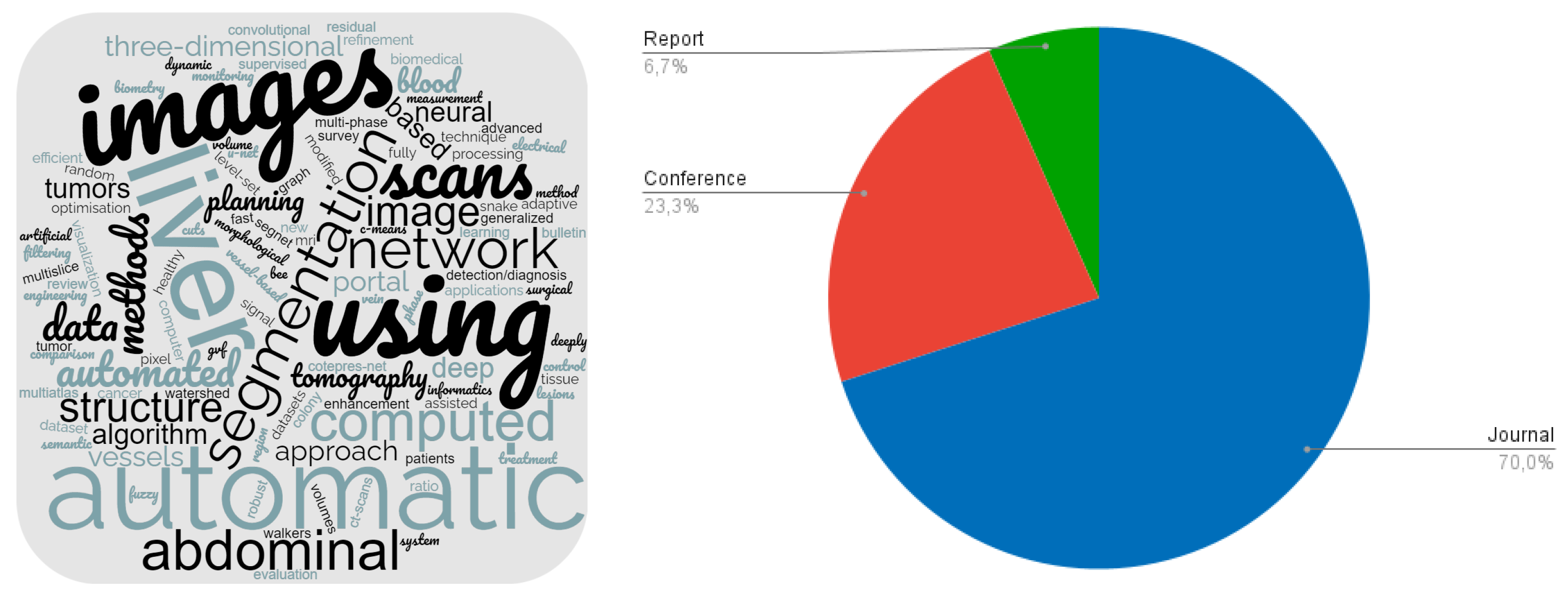
Figure 3.
Selected papers distribution according to the categories of image segmentation techniques
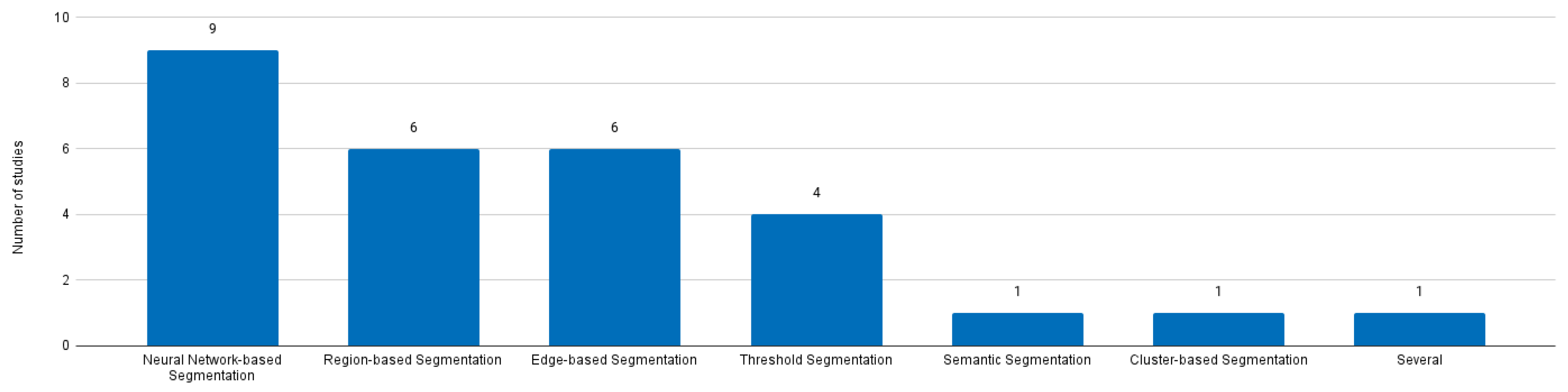

Table 1.
Summary of reviewed documents.
| Authors | Year | Segmentation Category | Method | Autom. Level | Dim. | Database | Results |
| Bae et al. | 1993 | Threshold | Gray-level Thresholding | Semi | 2D | Private | 0.985 DSC with mean percent error within 10%. |
| Gao et al. | 1996 | Edge | Parametrically deformable contour model | Fully | 3D | Private | 13.2% of the results required user modifications. |
| Soler et al. | 1997 | Region | Deformable models | Fully | 3D | Private | Claimed to be comparable to manual segmentations. |
| Yoo et al. | 2000 | Threshold | Threshold | Fully | 2D | Private | 3.41% error. |
| Pan and Dawant | 2001 | Edge | Level sets | Fully | Both | Private | [0.874,0.963] average similarities. |
| Saitoh et al. | 2002 | Threshold | Threshold | Fully | 3D | Private | ∼20 minutes computation time. |
| Masumoto et al. | 2003 | Region | Differences between time-phase images | Fully | 3D | Private | 67% Volume ratio average; 32% in the worst cases. |
| Lim et al. | 2004 | Region | Watershed | Fully | 2D | Private | Only qualitative. |
| Liu et al. | 2005 | Edge | GVF snake | Semi | 2D | Private | 5.3% median value of the difference ratios. |
| Lim et al. | 2006 | Semantic | Labeling-based search | Fully | 2D | Private | 96% average correctness; 3% average error rate. |
| Beichel et al. | 2007 | Region | Graph cuts | Semi | 3D | Private | 5.2% average overlap error. |
| Massoptier and Casciaro | 2008 | Edge | Active contour | Fully | 3D | Private | 94.2% mean DSC. |
| Heimann et al. | 2009 | Several | Majority Voting | Both | Both | Private | 5% Overlap error; -0.7 Volume difference; 0.8 Average Distance; 1.7 RMS distance; 19.1 Max Distance. |
| Akram et al. | 2010 | Threshold | Global Threshold | Fully | 3D | Private | 0.96 Average accuracy; 0.0017 std; 96% Accurately Segmented; 4% Poorly Segmented. |
| Oliveira et al. | 2011 | Edge | Level sets | Semi | 2D | SLiver07 | 82.05 overall score. |
| Linguraru et al. | 2012 | Region | Graph cuts | Fully | 3D | Private; SLiver07 | 2.2 VOE. |
| Li et al. | 2013 | Edge | Fuzzy clust. and level set | Fully | 2D | Private | 0.9986 average accuracy; 0.9989 average specificity. |
| Platero et al. | 2014 | Region | Graph cuts | Semi | 3D | SLiver07 | 76.3 maximum score; 0.973 DSC. |
| Mostafa et al. | 2015 | Cluster | ABC optimization | Fully | 2D | Private | 93.73% accuracy; 84.82% average SI. |
| Dou et al. | 2016 | NN | 3D DSN | Fully | 3D | SLiver07 | 5.42% VOE; 0.79mm ASD. |
| Christ et al. | 2017 | NN | CFCN | Fully | 2D | 3Dircadb | 94.3% mean DSC. |
| Hiraman | 2018 | NN | CNN | Fully | 2D | SLiver07 | 12.07% average VOE; -1.96% RVD; 2.25mm ASD; 2.60mm RMSD; 43.01mm MSSD. |
| Wang et al. | 2019 | NN | CNN | Fully | 3D | Private | 0.94 ± 0.06 DSC. |
| Almotairi et al. | 2020 | NN | SegNet | Fully | 3D | 3D-IRCADb01 | 94.57% overall accuracy. |
| Ayalew et al. | 2021 | NN | U-Net | Fully | 2D | 3D-IRCADb01; LiTS | 0.9612 DSC. |
| Scicluna | 2022 | NN | UNet; VGG16UNetC | Fully | 2D | CHAOS | 85.84 mean score; 97.85 DSC; 80.33 RAVD; 94.80 ASD; 70.38 MSSD. |
| Ezzat et al. | 2023 | NN | CNN | Fully | 2D | Private | 98.80% accuracy. |
| Shao et al. | 2024 | NN | AC-Net | Fully | 3D | LiTS; Private | 0.90 DSC; 0.82 JC; 0.92 recall; 0.89 precision; 11.96 HD; 4.59 ASD. |
ABC: Artificial Bee Colony AC-Net: Attention Connect Network ASD: Average Symmetric Surface Distance CFCN: Cascaded fully CNN CNN: Convolutional Neuronal Network DSC: Dice Similarity Coefficient DSN: Deeply Supervised Network GVF: Gradient Vector Flow HD: Hausdorff Distance JC: Jaccard Coefficient MSSD: Maximum Symmetric Surface Distance NN: Neuronal Network r: Correlation Coefficient RAVD: Relative Absolute Volume Difference RMS: Root Mean Square RMSD: Root Mean Square Symmetric Surface Distance RVD: Relative Volume Difference SI: Similarity Index std: standard deviation VOE: Volumetric Overlap Error
Table 2.
Characteristics of each dataset used by the main studies analysed (based in [58]).
Table 2.
Characteristics of each dataset used by the main studies analysed (based in [58]).
| Dataset | Date | Format | Number of subjects | Slices per subject | Resolution |
| MICCAI-SLiver07 [59] | 2007 | RAW | 30 | 74 to 260 | 512x512 |
| 3D-IRCADb01 [42] | 2010 | DICOM | 20 | 74 to 260 | 512x512 |
| LiTS17 [44] | 2017 | RAW | 200 | 42 to 1024 | Variable |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



