
Submitted:
07 February 2024
Posted:
08 February 2024
You are already at the latest version
Abstract
Annually, more than 1.5 million preventable new hepatitis B (HBV) infections continue to occur, with an estimated global burden of 296 million individuals living with chronic hepatitis B infection. This substantial health challenge results in over 820,000 annual deaths attributed to complications such as liver cirrhosis and hepatocellular carcinoma (HCC). HBV vaccination remains the cornerstone of public health policy to prevent chronic hepatitis B and its related complications. It serves as a crucial element in the global effort to eliminate HBV, as established by the World Health Organization (WHO), with an ambitious 90% vaccination target by 2030. However, reports on global birth dose coverage reveal substantial variability, with an overall coverage rate of only 46%. This comprehensive review thoroughly examines global trends in HBV vaccination coverage, investigating the profound impact of vaccination on HBV prevalence and its consequences across diverse populations, including both high-risk and general demographics. Additionally, the review addresses the formidable challenges and facilitating factors essential for achieving WHO's HBV vaccination coverage objectives and elimination strategies in the coming decade and beyond.
Keywords:
Hepatitis B
; liver disease
; WHO
; vaccination
; elimination
; barriers
1. Introduction
1.1. Overview of hepatitis B and its global impact
Decades of progress in the fight against Hepatitis B (HBV) have produced effective screening tools, preventive vaccines, and antiviral medications, significantly enhancing patient outcomes [1]. Despite these advancements, HBV remains a critical global public health threat, causing both acute and chronic liver diseases, contributing substantially to the worldwide disease burden and mortality [2]. HBV Complications rank as the seventh-highest cause of global mortality, according to the Centers for Disease Control and Prevention [3].
Without intervention, individuals with chronic Hepatitis B (CHB) face a lifetime risk of developing cirrhosis, liver failure, or hepatocellular carcinoma (HCC) ranging from 15-40% [4,5,6]. Correspondingly, HBV attributes to an estimated 29% of cirrhosis-related deaths worldwide [7]. Recent statistics indicate that approximately 50-80% of HCC cases globally result from HBV infection, making it the sixth most common cancer worldwide and the fourth leading cause of cancer-related death [8]. Moreover, about 90% of infants born to mothers testing positive for Hepatitis B surface antigens (HBsAg) or e antigens (HBeAg) will develop chronic infection, posing a significant global public health challenge [9,10].
In 2019, the World Health Organization (WHO) estimated alarmingly high global CHB infection prevalence, affecting around 296 million individuals worldwide [11]. That same year witnessed roughly 1.5 million new HBV infections, with HBV being responsible for an estimated 820,000 deaths, primarily attributed to complications like cirrhosis and HCC [11]. A 2022 modeling study by the Polaris Observatory group estimated the global CHB prevalence at 3.2%, equivalent to 257.5 million cases (Figure 1) [12].
Notably, only approximately 14% of chronically infected individuals are diagnosed, and only around 8% of those eligible for treatment receive it (Figure 2) [12].
This disparity is pronounced, with the majority of diagnosed and treated individuals concentrated in developed regions. In contrast, sub-Saharan Africa and certain parts of Asia bear a disproportionate burden, encountering elevated prevalence rates and challenges related to limited access to vaccination, diagnostics, and treatment [3,5]. Additionally, the prevalence of CHB and new infections tends to be higher in lower-income or underdeveloped countries [13,14].
In 2022, the prevalence of HBV infection among children aged ≤5 years was estimated at 0.7%, corresponding to 5.6 million children (Figure 3) [12]. Notably, Nigeria, Indonesia, India, China, Angola, and Niger collectively accounted for 56.5% of all infections among this age group.
Despite the global decline in CHB infection prevalence, particularly among children under five due to infant vaccination programs, there are concerning disparities. While the WHO Western Pacific region (WPR) has a higher number of CHB carriers compared to the WHO Africa region, the most significant percentage of children under five with HBV resides in Africa, with an estimated prevalence of 2.5% [15,16]. This persistent prevalence among African children under 5 indicates missed opportunities to control mother-to-child transmission (MTCT) of HBV [16,17]. While 85% of infants received the three-dose HBV vaccination before one year of age, only 46% received a timely birth dose, and 14% received hepatitis B immunoglobulin (HBIG) as part of the complete regimen. Additionally, only 3% of mothers with a high HBV viral load received antiviral treatment to reduce the risk of MTCT [12].
HBV transmission occurs through various routes, primarily via perinatal transmission, unsafe medical procedures, and unprotected sexual contact [18]. The chronicity of the infection varies geographically, with a significant proportion of infected individuals progressing to CHB, a long-term condition carrying substantial morbidity and mortality risks [19]. Despite advancements in vaccination-based prevention, barriers persist in achieving universal coverage and ensuring access to diagnosis and treatment, especially in resource-limited settings [20]. A comprehensive understanding of HBV’s epidemiology, transmission dynamics, and impact on affected populations is crucial for formulating effective control and elimination strategies.
Efforts toward HBV control and elimination encompass a multifaceted approach, integrating vaccination programs, enhanced diagnostics, and affordable therapies. The WHO emphasizes the importance of vaccination as a cornerstone for prevention, aiming to expand coverage to reduce new infections [21]. However, achieving elimination targets demands not only robust vaccination programs but also improved access to diagnostics and antiviral therapies coupled with strengthened health systems [22].
1.2. Significance of achieving HBV elimination by 2030
Eliminating HBV by 2030 represents a critical global health milestone, aiming to significantly reduce the burden of this viral infection and its complications. In 2014, the Global Health Assembly assigned the WHO the task of supporting member states in developing comprehensive strategies for preventing, diagnosing, and treating viral hepatitis [15]. Subsequently, in May 2016, the WHO established ambitious yet achievable targets to eliminate viral hepatitis as a public health threat by 2030 (Table 1) [15,23]. This goal relies on two key factors: service coverage and impact leading to elimination. Service coverage focuses on prevention and treatment, encompassing four key preventive strategies:
- Infant vaccination: Administering the three-dose HBV vaccine to infants.
- Preventing mother-to-child transmission (MTCT): Using either the HBV birth dose vaccine or alternative approaches.
- Ensuring blood and injection safety: Implementing protocols to minimize transmission through unsafe medical practices.
- Harm reduction: Implementing strategies to reduce transmission among high-risk groups like intravenous drug users.
This global strategy aims for 90% of patients with HBV to be aware of their infection and 80% of eligible individuals to receive antiviral treatment by 2030 [23,24,25]. This would result in a 90% reduction in the incidence of new infections and a 65% reduction in mortality. Achieving this necessitates comprehensive global efforts in prevention, diagnosis, treatment, and vaccination programs [24,26]. Aligned with the Global Health Sector Strategy (GHSS), new guidelines for the processes and standards for validating the elimination of viral hepatitis as a public health problem were provided by the WHO in 2021. According to those guidelines, the WHO suggests using absolute impact targets to validate elimination at the national level instead of the relative reduction targets initially defined in the 2016 GHSS. The leading impact indicators and targets for measuring the elimination of HBV new infection are ≤ 0.1% HBsAg prevalence in those aged five years or under.
Reducing new HBV infections is paramount, necessitating multifaceted strategies like expanding vaccination coverage, especially in high-risk regions, and implementing effective prevention programs addressing various transmission routes [24]. Two seemingly achievable goals are implementing the three-dose infant vaccine regimen and preventing MTCT [27]. While most countries have incorporated HBV vaccination into their national immunization programs, scaling up harm reduction practices among high-risk populations remains a crucial but challenging aspect of combating HBV transmission [24].
Reducing mortality rates from HBV-related complications significantly contributes to elimination [28]. Deaths from chronic HBV infections, including liver cirrhosis and HCC, remain alarmingly high [19]. However, increased access to diagnostics, timely antiviral therapies, and improved healthcare infrastructure can significantly mitigate these adverse outcomes [19,22]. It is estimated that the implementation of the WHO 2023 elimination strategy would prevent 7.1 million deaths between 2015 and 2030.
Efforts toward HBV elimination offer not only health benefits but also substantial economic advantages. Numerous studies suggest that successful elimination could save healthcare systems billions annually by reducing disease management and complication costs [20]. However, achieving the 2030 elimination goal requires a critical reassessment of strategies and a renewed global effort [19,27]. Highlight the potential need to adjust elimination targets for practicality in regions grappling with high burdens of chronic HBV infection [12]. Therefore, achieving global elimination by 2030 necessitates a two-pronged approach: rigorous and continuous evaluation of progress toward existing goals and the concurrent development of new, practically aligned strategies [21].
Despite being an ambitious task, the global elimination of HBV by 2030 requires considerable work in the coming decade. The review article aims to evaluate the pivotal role of HBV vaccination as a primary tool in realizing the ambitious goal set by the WHO to eliminate HBV by 2030. It focuses on analyzing the impact, effectiveness, and challenges associated with widespread HBV vaccination programs. The article likely discusses the vaccine’s ability to reduce transmission rates, prevent new infections, and contribute significantly to the WHO’s objective of lowering HBV-related morbidity and mortality. Additionally, it may explore strategies to enhance vaccine coverage, address barriers to immunization, and propose comprehensive approaches to harness the vaccine’s potential in achieving global HBV elimination targets set for 2030.
2. Methodology
The review employed comprehensive search strategies across multiple databases (PubMed, Scopus, Web of Science, ScienceDirect, and Embase) using keywords like “Hepatitis B infection,” “Hepatitis B vaccine,” “Hepatitis B elimination,” and “WHO 2030 targets” to gather relevant literature. Studies, articles, and reports focusing on HBV vaccination, global elimination efforts, WHO’s 2030 targets, vaccination barriers, and strategies for eradication were likely included. Papers not directly related to HBV vaccination, studies outside the scope of the WHO’s 2030 targets, or those lacking relevance to global elimination strategies might have been excluded. Relevant data, including vaccination efficacy, barriers to immunization, global progress toward elimination, and strategies for achieving WHO targets, were extracted and synthesized from selected articles. The gathered data was critically analyzed to identify trends, challenges, successes, and gaps in HBV vaccination programs and their role in meeting WHO’s 2030 targets for HBV elimination. Findings from the selected studies were integrated to create a cohesive narrative, emphasizing the role of the HBV vaccine as a pivotal tool in achieving global elimination goals by 2030.
3. Hepatitis B Vaccines: Evolution and Effectiveness
Combating HBV infection involves three main strategies: treating chronic infections, eliminating transmission routes, and immunizing vulnerable populations [30]. Vaccination, arguably the most effective method, forms the cornerstone of the WHO’s strategy to eliminate and ultimately eradicate HBV. Throughout the last three decades, HBV prevention and even treatment through HBV vaccination have been the subject of extensive research work. This section delves into HBV vaccine development, safety, adoption, and economic impact over the past three decades.
3.1. From Plasma to Recombinant: A Paradigm Shift
The first commercially available vaccine, launched in 1982, relied on extracting antigenic elements from the plasma of asymptomatic chronic HBV carriers [31,32]. Extracting the antigenic hepatitis B surface antigen (HBsAg) from the plasma of asymptomatic carriers formed the manufacturing process. This process involved ultracentrifugation and chemical decontamination, including formalin treatment to eliminate blood-borne pathogens [33]. The recommended three-dose schedule over six months proved highly effective and safe, establishing the benchmark for subsequent vaccines [31].
However, limitations existed. First, a theoretical but unproven risk of blood-borne infections like HIV raised public concerns, impacting vaccine acceptance [34]. Second, relying on chronic carriers as a source of HBsAg became unsustainable due to the vaccine’s success in reducing infection rates. These factors spurred the development of recombinant HBV vaccines [31]. In 1986, DNA recombination technology in yeast allowed the synthesis of an HBsAg-like protein, leading to the FDA-approved recombinant vaccine [35]. Similar in efficacy and safety to its predecessor, it too required a three-dose, six-month schedule. These vaccines could provide long-term protection for over 30 years [32].
The latest advancement arrived in 2018 with HEPLISAV-B®, specifically designed for adults ≥18 years. This “combo” vaccine incorporates recombinant HBsAg with an adjuvant that amplifies the immune response, enabling a potent two-dose regimen compared to the three doses required by earlier versions. Studies consistently demonstrate its superiority, achieving an impressive 96.6% response rate after just one month, compared to only 24.0% for the conventional vaccine [36].
3.2. Efficacy and Safety of HBV Vaccination
The HBV vaccine’s effectiveness can be measured in two ways: its ability to induce protective antibodies (anti-HBs) and its success in preventing MTCT. Recombinant and combo vaccines show efficacy and safety comparable to the conventional version [35,36,37,38]. Across diverse vaccination schedules, they consistently achieve seroprotection levels exceeding 95% in healthy individuals.
Global adoption of HBV vaccination has yielded remarkable results, with the worldwide prevalence in children under five plummeting from 4.7% in the early 1990s to 1.3% by 2015 [31]. However, studies indicate a decline in seroprotection among older adults (>40 years), highlighting the need for further research and tailored approaches for this population [39].
All HBV vaccines have undergone rigorous safety assessments, with over a billion doses administered since 1982, demonstrating an excellent safety profile [33,40,41,42]. Adverse events are typically mild and transient, such as injection-site reactions. Severe reactions are exceedingly rare, and studies have debunked unsubstantiated claims linking HBV vaccination to conditions like multiple sclerosis [43,44]. HBV vaccination is demonstrably safe for pregnant and lactating women, low birth weight infants, and even HIV-positive individuals, further expanding its reach and impact. Notably, the only contraindication is a known hypersensitivity to any vaccine component or a history of severe reactions.
3.3. Concerns with HBV vaccination
3.3.1. Durability of the immune response
The duration of immunity following HBV vaccination is not definitively determined. However, in individuals, including both adults and children, who complete the initial vaccination series, attaining an anti-HB level of 10 mIU/mL or higher within two to three months after the final dose indicates a strong immune response effective against both acute and chronic HBV infections [45]. Studies show that this primary protection lasts for decades in most immunocompetent individuals [46]. Even when anti-HBs levels dip below 10 mIU/mL, protection has been documented for up to 30 years [47]. Follow-up studies reveal a natural decline in anti-HBs concentration over time, with a steeper drop in the first year and a slower decline later [48,49]. This pattern holds true regardless of the initial peak antibody level. Other factors like age, weight, sex, and smoking history at vaccination can also influence the vaccine’s durability (measured by anti-HBs levels above 10 mIU/mL) in immunocompetent individuals [50,51]. However, the effectiveness of HBV vaccination is not only linked to the induction of anti-HB antibodies but also involves the activation of memory B and T cells [47,52]. So, even if anti-HBs levels decrease, that doesn’t necessarily mean you’re unprotected. Immunological memory of the HBsAg antigen can persist even when antibodies are no longer detectable [53,54,55,56]. In light of current scientific evidence, various advisory groups do not advocate for routine booster doses of the HBV vaccine in fully vaccinated, healthy, and immunocompetent individuals. This is because the majority of previously fully vaccinated individuals with anti-HBs antibody concentrations of 10 mIU/mL or less exhibit an anamnestic response when given when exposed to HBV or given a booster dose, indicating sustained protection by memory B and T cells [56,57,58,59,60,61]. However, there are exceptions where a booster dose might be recommended, such as for immunocompromised individuals or healthcare workers who are at higher risk of exposure [53,56,58,59,62,63].
3.3.2. Vaccine escape mutants
HBV vaccines and HBIG have effectively prevented infection before and after exposure [64,65]. However, the emergence of vaccine escape mutants poses challenges to the efficacy of these preventive measures. Studies highlight that mutations in the S gene of HBV, particularly in the α-determinant, can be selected under the immune pressure exerted by vaccination, especially when HBIG is administered [65]. The most common escape mutant, G145R, involves a glycine-to-arginine change at amino acid position 145 [64]. Despite concerns, it’s crucial to note that the baseline prevalence of these mutants varies geographically. In Taiwan, for example, the prevalence of α-mutants was 7.8% in HBsAg carrier children, remaining around 20% during the initial 15 years of the universal mass vaccination program [66]. Contrarily, over the last decade, there has been no substantial increase in vaccine escape HBV mutants among Taiwanese carrier children, with no evidence of widespread virus spread [67]. This lack of escalation is attributed to the weakened nature of the mutant virus [67]. Similar findings in Italy suggest that these mutants may not pose a significant threat to ongoing control efforts [68]. Furthermore, studies reveal that current HBV vaccines can protect against infection with these mutant viruses, supporting the continued use of existing vaccines [69]. While these findings shed light on the challenges posed by vaccine escape mutants, the overall effectiveness of HBV vaccination remains significant in preventing HBV infection. In addition, current HBV vaccines demonstrate efficacy in protecting chimpanzees from infection with these mutant viruses, supporting the continued use of the existing vaccines [70,71].
3.3.3. Impact of HBV genotypic variability
HBV exhibits significant genotypic variability, categorized into ten distinct genotypes (A-J) possessing unique genetic characteristics [69,70]. This diversity manifests in geographically specific distributions, with certain genotypes dominating particular regions. For instance, genotype D is prevalent in Asia, while genotype B holds sway in Europe and North America [73]. This heterogeneity presents a challenge to vaccine efficacy, as current vaccines target a specific region of the viral surface antigen (HBsAg) – the “α-determinant” [39]. The challenge lies in the potential for reduced vaccine effectiveness against non-targeted genotypes, hindering the achievement of universal protection.
Furthermore, the varying prevalence of HBV genotypes across regions can impact the overall efficacy of vaccination programs. Studies suggest that vaccines based on the A2 genotype may not offer complete protection against infection with non-A2 genotypes [74,75]. This underscores the intricate interplay between genotypic diversity and the potential for occult HBV infections, where the virus persists despite vaccination efforts [75,76,77]. Despite these challenges, large-scale studies reassure us that currently available HBV vaccines remain highly effective against all genotypes, demonstrating a 94–98% protective rate against CHB infection for at least 20 years [73,78]. Moreover, the successful implementation of vaccination programs has led to a substantial decrease in the HBV carrier rate and HBV-related morbidity [63].
3.3.4. Vaccine non-responders
Individuals who develop an anti-HBs titer below 10 mIU/mL after complete vaccination are classified as “vaccine non-responders.” This blunted immune response, often attributed to impaired T cell activation or recognition of the HBsAg antigen, presents a significant challenge [79]. Globally, an estimated 10% of vaccine recipients fall into this category, highlighting the need for effective identification and management strategies [80]. Key risk factors include older age at primary immunization, obesity, smoking, comorbidities (diabetes mellitus, chronic kidney disease, chronic liver disease), HIV infection, and immune suppression [79,80,81,82,83,84,85,86,87,88]. Identifying these risk groups is crucial for planning follow-up screenings for anti-HBs levels and administering booster doses if needed.
In studies of individuals over 60, only 45.7% developed anti-HBs antibodies [89]. Participants over 59 years old showed a 60% antibody titer greater than 10 mIU/mL at seven months post-vaccination [90].
For patients with chronic kidney disease, seroconversion rates after three doses were 87.5%, 66.6%, and 35.7% for mild, moderate, and severe cases, respectively. Rates significantly improved after a fourth dose [91]. Patients with low glomerular filtration rates, higher creatinine, diabetes, and old age are less likely to seroconvert [92].
Patients with chronic liver diseases, especially hepatitis C infection, demonstrated a diminished response, with only 55% achieving seroconversion [93]. Genotype 1 patients exhibited a poorer response. The immune response correlated inversely with advanced liver disease measured by the MELD score [94]
In HIV patients, the seroconversion rate ranges from 18% to 72%, depending on immune status. Those not receiving Highly Active Antiretroviral Therapy (HAART) exhibit response rates between 30% and 50%, while individuals on HAART experience an increased response ranging from 60% to 70% [95,96,97]. This response correlates directly with the CD-4 count and inversely with the viral load.
Blunted response to HBV vaccination can be augmented by interventions like additional booster doses, increased vaccine dose, intradermal route, or combo vaccine [83,98,99,100]. One intervention, doubling the standard vaccine dose in cirrhosis patients, showed marginal success [101].
The intradermal route’s success relies on Langerhans cells and macrophages’ efficient antigen presentation, showing response rates of 69%-100% [102]. A total antigen dose of 70-80 μg divided over 7-8 sessions or 5 μg weekly proved more effective than the standard 40 μg intramuscular protocol [98].
Vaccine advancements, like third-generation recombinant vaccines and adjuvanted vaccines, aim to improve responses, especially for immunocompromised and elderly populations [39,99,103]. Emerging vaccines present potential simplified schedules as alternatives to the traditional 0, 1, and 6-month regimen [39].
3.4. Vaccine for healthcare workers
Healthcare workers (HCWs) constitute a crucial target group for HBV vaccination, not only due to their susceptibility to infection but also because they may serve as potential sources of infection during exposure-related procedures. Globally, there exists a significant disparity in HCW immunization against HBV. Only 18% of HCWs in Africa reported HB vaccination, contrasting with 77% in Australia and New Zealand [104]. A recent report highlights that almost half of HCWs in India remain unvaccinated. Conversely, Egypt boasts a higher adherence to immune prophylaxis, with nearly 82% of HCWs receiving the vaccination [22]. This discrepancy might be partially explained by Egypt’s inclusion of HBV vaccination among its compulsory immunizations since 1992. However, the long-term retention of the protective effect in HCWs needs to be evident. A study revealed that 30% of previously immunized HCWs lost the protective Anti-HBs titer (< 10 IU) [105]. In light of these findings, making HBV vaccination and regular anti-HBs checks mandatory for HCWs is imperative.
3.5. Cost-effectiveness of HBV vaccination
Ideally, all individuals at intermediate or high risk of acquiring HBV infection should receive vaccination. Implementing such a strategy requires economic studies to validate cost-effectiveness. A recent study conducted in the USA demonstrated that administering the HBV vaccine was more cost-effective than the test and vaccination strategy in selected high-risk groups. These groups included foreign-born Asians, Africans, incarcerated individuals, refugees, IV drug abusers, and men who have sex with men (MSM). The study compared the incremental cost-effectiveness ratios (ICERs) of vaccination versus the screening and treating strategy. The findings indicated that vaccination had ICERs of $6000 per quality-adjusted life-year gain, whereas the screen and treat strategy had a higher cost of $21,000 [106].
The universal vaccination of infants has been extensively studied. Generally, vaccination proves cost-effective in areas with intermediate or high HBV endemicity, but it could be more effective in low-endemicity areas. Cost-effectiveness has been reported in Iran [107], China [108], and Vietnam [109] as opposed to the UK [110].
3.6. Recent advances in HBV vaccination
3.6.1. AI applications
Initiating the HBV transmission control circle begins with delivering timely vaccination; however, identifying individuals at risk of suboptimal immune response to the HBV vaccine is equally vital. One research group explored implementing machine learning to detect individuals at risk of vaccine failure and deliver a precision booster dose for those at high risk [111]. This pilot project requires validation in further studies.
3.6.2. Therapeutic HBV vaccine
Chronic HBV infection commonly encounters T-cell failure [112]. The evolving approach to treating HBV depends on enhancing host cytotoxic T-cell activity targeting HBV-infected hepatocytes [113]. The ongoing quest is to discover the ideal antigen that can successfully recruit T-cells with low toxicity to healthy liver cells. In a recent clinical trial, the GS-4774 vaccine, a complex antigen composed of HBs, HBc, and a partial HBV X protein, stimulated the immune system but failed to provoke sufficient virus-specific CD4+ T-cells or B-cells to reduce circulating HBs levels [114]. In another study, an AI-powered model predicted the immunogenicity of 30 possible therapeutic vaccine legends. The model identified four epitopes with suitable profiles, exhibiting both immunogenicity and safety [115]. The hype surrounding AI in scientific studies suggests its potential to fill many gaps in the field of HBV prevention.
3.7. The effectiveness of the HBV vaccine in different populations
The HBV vaccine demonstrates substantial efficacy across diverse populations, particularly in high-risk groups. In pre-exposure scenarios, the vaccine plays a pivotal role in imparting immunity against HBV infection, especially for high-risk individuals such as healthcare workers and those in close contact with infected persons. Timely vaccination post-exposure significantly diminishes the risk of HBV transmission, providing a crucial protective layer against infection following potential exposure. Due to challenges in engaging and accessing populations at risk of HBV infection [116], a more practical and cost-effective approach emerged—universal vaccination of newborns [117,118,119]. Consequently, the WHO endorsed and implemented the integration of the HBV vaccine into the Expanded Program on Immunization (EPI) [112,113].
Mass or universal vaccination campaigns, especially in regions with high prevalence, exhibit profound impacts, markedly reducing chronic HBsAg carriage rates and consequently lowering the burden of acute and chronic HBV-related diseases. This widespread immunization effort significantly decreases the incidence of HCC, a severe consequence of CHB infection, by suppressing the virus’s prevalence in the population and mitigating potential long-term complications.
3.7.1. Vaccination for High-risk populations
3.7.1.1. Pre-exposure high-risk groups
The HBV vaccine proves highly effective in safeguarding various high-risk population segments against HBV. For instance, it significantly benefits healthcare providers, fostering protective antibodies and long-term immunity [122], especially in high-risk groups like renal hemodialysis unit staff [123,124].
3.7.1.2. Patients with End-stage Kidney diseases
Studies reveal that while HBV vaccination is recommended for End-stage Kidney Disease (ESKD) patients on hemodialysis, this population often exhibits a lower immune response, with only approximately 50-60% achieving adequacy [125,126]. As chronic kidney disease (CKD) progresses, vaccine efficacy tends to decline [126]. The lower immunogenicity of the HBV vaccine in this high-risk population is attributed to various factors, including malnutrition, impaired immune function due to CKD, uremia-related immune dysfunction, and altered immune responses [127]. Response diminishes in patients with serum creatinine levels ≥4 mg/dL compared to those with lower levels (86% vs. 37%) [128,129]. Diminished responsiveness is associated with a glomerular filtration rate below 10 mL/min, age over 60, and diabetes mellitus [128,130,131,132]. Improved antibody responses occur among patients undergoing efficient hemodialysis [7,132,133]. Notably, coexisting hepatitis C virus infection may reduce vaccine effectiveness in patients undergoing maintenance hemodialysis [132,134].
The standard vaccination regimen often involves multiple doses (typically four) of the HBV vaccine before initiating hemodialysis [135]. However, achieving a robust immune response remains a challenge despite this regimen. Researchers have explored different approaches to enhance the vaccine response in this population, such as using higher vaccine doses, adjuvants, or alternative vaccination strategies [136,137]. Further research is needed to determine the most effective approach [131,138].
3.7.1.3. Post-Renal Transplant Patients
The immune response to the HBV vaccine is reduced post-renal transplant, with studies indicating decreased seroconversion rates and only 17-36% achieving protective antibody levels [139]. The vaccine’s efficacy diminishes as CKD progresses, posing challenges to attaining adequate immunity before renal transplant [140]. Immunosuppressive medications post-transplantation can further compromise vaccine effectiveness, influencing the patient’s ability to mount an adequate immune response [141]. Various strategies, such as alternative dosing regimens and routes of administration (e.g., intradermal), show promise in improving response rates [142]. Administering HBV vaccination as early as feasible, preferably pre-renal transplantation, is crucial for ESKD patients due to the age-related correlation with immune response [143] and the significantly heightened immunogenicity when given pre-transplant [144].
3.7.1.4. Men having sex with Men (MSM)
Studies show that HBV vaccination remains highly effective in preventing HBV infection among MSM despite potential variations in immune response [145,146,147,148]. Randomized trials demonstrate an effectiveness of 80–88% in providing protection among MSM [147,148,149]. However, vaccine coverage remains a concern, lacking comprehensive data [150]. A systematic review suggests a possible association between HBV vaccination among MSM and socio-demographic characteristics, behavioral patterns, and social-cognitive factors [150].
3.7.1.5. HIV patients
HBV vaccination efficacy is diminished in HIV patients, leading to a reduced immune response [151,152,153,154]. Higher CD4 counts of ≥500/mm3 and lower HIV viral loads of ≤1000 copies/mL correlate with a more effective humoral response to HBV vaccination among HIV patients [155]. The immune response might improve among patients with acquired immune deficiency syndrome (AIDS) undergoing highly active antiretroviral therapy (HAART) [151,152,153,154,155,156]. However, efficacy declines in HIV patients with older age, particularly after 40 years, obesity, stress, and smoking [157]. Strategies such as using double doses or booster shots have been shown to improve the immune response, enhancing the effectiveness of the HBV vaccine in HIV patients [151]. The recombinant HBV vaccine shows safety, efficacy, and cost-effectiveness in HIV-infected individuals [158] and should be offered to all patients regardless of their CD4 counts or viral loads.
3.7.1.6. Patients with Chronic Liver Disease
HBV vaccination is generally safe in patients with chronic liver disease, displaying immunogenicity rates, although reduced (35%) compared to the general population (95%) [159,160,161]. Studies emphasize the importance of assessing individual responses, revealing varied seroconversion rates ranging from 16% to 79% in clinical practice [159]. The severity of liver disease significantly influences the response to HBV vaccination, with rates differing between Child A (75.9%) and Child B (24.1%), highlighting the need for tailored approaches based on disease stage [159,162]. Older age, diabetes mellitus, and cirrhosis are associated with reduced responses to the HBV vaccine [162,163]. Additionally, the underlying etiology plays a role; for example, patients with hepatitis C and alcohol-related chronic liver disease exhibit a low response to the hepatitis B vaccine [163,164,165]. Patients with chronic liver disease face an increased risk of encountering severe complications due to acute viral hepatitis A or B. This highlights the critical significance of vaccination for both hepatitis A and B in this patient population [166].
3.7.1.7. Post-Liver Transplant patients
In liver transplant recipients, studies assessing post-liver transplant vaccination effectiveness vary significantly due to heterogeneity in recipient and donor types (cadaveric or living), vaccine type, adjuvant usage, vaccination protocol, response definition, and simultaneous HBIG or Lamivudine use [167]. Several studies highlight the challenge of achieving adequate immunity against HBV with a response rate as low as less than 30% [167,168]. Vaccination is notably more effective in patients transplanted due to HBV-related acute liver failure than CHB infection-related indications [167]. Immunoprophylaxis strategies, including HBIG and potent antiviral therapy (e.g., Entecavir, tenofovir), are often employed post-transplantation to prevent HBV recurrence [153,154]. Combining HBIG with antiviral medication proves more effective in preventing recurrence than HBIG alone [170]. However, this regimen’s critical weakness lies in its high cost and the risk of escape mutations related to HBIG. Therefore, the HB vaccine is being explored as a lower-cost substitute at many transplant centers, with varying reported effects [171,172]. Despite challenges, post-liver transplant HBV vaccination may offer added immunity and is considered an active immunoprophylaxis strategy [172]. Some patients who receive the HBV vaccine develop sufficiently high hepatitis B surface antibody (HBsAb) titers to stop lifelong HBIG administration [171]. However, the efficacy might vary based on the regimen [172,173]. Studies analyzing different immunization schedules before and after transplantation stress the importance of optimized vaccination protocols in these patients [173]. Recent reports highlight a limitation in the effectiveness of repeated vaccine doses to sustain adequate anti-HBs levels, primarily due to the emergence of escape mutations. This phenomenon poses a risk of diminished efficacy and increases the potential for recurrence of HBV infection recurrence if used alone as a prophylaxis strategy [171]. Consequently, the strategy of post-liver transplant vaccination is not accepted as a reliable approach for preventing HBV recurrence in patients with chronic infection, necessitating the continuation of antiviral prophylaxis [167,168,174].
3.7.1.8. Mother-to-Child Transmission (MTCT) setting
MTCT, also known as perinatal or vertical transmission of HBV, represents one of the primary routes of worldwide HBV spread (>85%), particularly prevalent in regions like Southeast Asia and China with high prevalence rates. WHO estimated that in 2015, 65 million women of childbearing age were chronically infected and at risk of transmitting HBV to their offspring [175], and 90% of infants infected with HBV at birth are at risk of chronicity [180,181]. MTCT correlates with an increased risk of subsequent chronic liver disease and HCC [178]. Preventing MTCT is a crucial strategy to meet WHO 2030 goals and eradicate HBV [179]. Fortunately, the safe and effective HBV vaccine has revolutionized MTCT prevention, significantly reducing transmission rates. Numerous studies demonstrate the remarkable efficacy of the HBV vaccine in preventing MTCT [179,180,181,182,183].
Early studies reported significantly reduced MTCT rates with prompt vaccination of newborns, achieving an MTCT reduction of 70-90% in HBeAg-positive mothers [177,181,182,183,184,185]. These findings support using vaccines in regions where pregnant women are not subjected to screening for HBsAg and HBeAg [186]. Subsequent research highlighted the synergistic effect of combining birth dose vaccination with HBIG given within the first 24 hours after birth, bridging the gap between HBV exposure and active anti-HBs production induced by the HBV vaccine. This strategy yields even lower MTCT rates, reducing them by more than 90% and approaching 98% in some cases [180]. Timely administration of dual immune-prophylaxis (HBV vaccine and HBG) within 24 hours of delivery is crucial, as delays have been linked to heightened infection risks among infants born to HBsAg-positive mothers.
Research indicates that maternal HBeAg positivity significantly impacts MTCT risk. In HBeAg-negative mothers, HBV vaccination alone can achieve impressive protection, with some studies reporting 0% MTCT [184]. However, adding HBIG to the vaccination schedule offers additional protection for HBeAg-positive mothers, further reducing MTCT rates [183,187]. Even with HBV vaccination, approximately 3% of newborns from mothers who are carriers of HBsAg but negative for HBeAg may persistently contract the infection [119], indicating that defining infectivity by HBeAg in HBsAg carriers is not perfect [188].
HBV viral load emerges as a critical predictor in assessing MTCT risk, surpassing the significance of HBeAg status. Studies consistently demonstrate a significant correlation between high maternal viral load and increased MTCT risk, even in HBeAg-positive cases [189,190]. Recent studies suggest that higher maternal HBsAg levels are associated with an increased risk of perinatal transmission [190,191,192]. HBIG and vaccine failures occur almost exclusively in HBeAg-positive women with high HBV DNA levels (>200,000 IU/ml) and/or HBsAg levels above 4–4.5 log10 IU/ml [189,190,191,192]. Recognizing the paramount importance of early intervention, prophylactic measures during the third trimester have been recommended [193]. However, the decision to initiate NA prophylaxis is contingent upon the HBV viral load and HBsAg level, with a consensus emerging around the threshold of 200,000 IU/mL and above 4–4.5 log10 IU/ml, respectively [189,190,191,192,194].
3.7.2. HBV mass vaccination
After introducing the HBV vaccine, challenges arose when directing efforts toward high-risk populations like sex workers, homosexuals, or intravenous drug abusers [195]. Conversely, deeming universal vaccination for HBV in all newborns more feasible and cost-effective became apparent [196]. WHO champions comprehensive HBV vaccine programs for newborns as a cornerstone in the global effort to prevent MTCT of HBV [197]. WHO initiated universal vaccination in 1991 to prevent HBV transmission during the perinatal period and early childhood, as these stages carry a higher risk of developing chronic infections [198]. This initiative emphasizes universal vaccination strategies to ensure maximum coverage and effectiveness. As of 2022, the WHO reported the nationwide introduction of the HBV vaccination program for infants in 190 Member States, showcasing widespread adoption [199]. The primary strategy involves providing the HBV vaccine to all newborns, regardless of maternal HBsAg or HBeAg status. Screening pregnant women for HBsAg, with the addition of HBIG to newborns born to HBsAg-positive mothers, aims to enhance protection against MTCT, irrespective of the mother’s HBeAg status. Numerous studies substantiate the effectiveness of these mass vaccination programs, demonstrating a significant impact on reducing HBV infection incidence, especially in regions with a high disease burden [200,201]. Moreover, the overall success of these programs is underscored by integration into national immunization schedules, leading to increased coverage and sustained protection against HBV. Taiwan’s response to the substantial burden of CHB infection is characterized by a pioneering national vaccination program initiated in 1984. This marked a pivotal moment in Taiwan’s public health landscape and a strategic intervention to mitigate the widespread prevalence of CHB infection. By successfully incorporating HBV vaccination into routine immunization schedules, the program achieved remarkable progress in lowering the prevalence of CHB infection, HCC, and mortality of fulminant hepatitis in vaccinated birth cohorts [201,202]. Different long-term cohort studies conducted in Taiwan have demonstrated the enduring effectiveness of this vaccination initiative over decades, with a decrease of more than 90% in chronic liver disease and HCC mortality and more than 80% in HCC incidence [9,10,11,12,13]. Taiwan’s experience serves as a model for other nations, showcasing the impact of a well-structured and enduring national vaccination program in mitigating the burden of chronic HBV infection.
Another study from Iran further supports Taiwan’s vaccination strategy on the effectiveness of the national HBV vaccination program 25 years after its introduction [206]. The study included over 100,000 individuals born before and after the program’s introduction. The results showed that the vaccination program was highly effective in preventing HBV infection, with a vaccine effectiveness of over 95%. Additionally, the study found that the program was cost-effective, with the benefits far exceeding the costs, making it a major public health success story that significantly improved the health of the Iranian population. From 1992 to 2015, HBV control through vaccination in the Southeast Asia Region made significant progress, preventing approximately 16 million CHB infections and 2.6 million related deaths during the same period [207].
Moreover, a study from China revealed that the vaccination strategy implemented over 20 years (1992-2012) was cost-effective and led to a significant decline in the incidence of HBV infection among children and adolescents [28]. The incidence among children aged 1-4 years decreased from 9.7% in 1992 to 0.3% in 2012, while the incidence among adolescents aged 15-19 dropped from 11.9% in 1992 to 1.1% in 2012.
Globally, four distinct strategies for universal HBV vaccination in newborns are outlined in Table 2. [69,208].
The most straightforward approach involves administering the vaccine to all newborns without considering maternal HBV status. This strategy eliminates the need for screening pregnant women and bypasses the use of HBIG in newborns, resulting in the lowest associated costs. However, it is crucial to note that the efficacy of this strategy may be compromised, as indicated by various studies [180,204,209,210]. Conversely, the most comprehensive yet cost-intensive strategy is universally administering the HBV vaccine to newborns. This approach involves screening pregnant women and administering HBIG to newborns if the mother tests positive for HBsAg, irrespective of the HBeAg status. The choice of vaccination strategy is at the discretion of each country, guided by considerations such as epidemiological factors, disease burden, public health system readiness, and economic constraints. It is imperative to emphasize that any selected approach for implementing HBV vaccination plays a pivotal role in controlling the prevalence of HBV within a given country. The decision-making process should be meticulous, considering various factors to tailor the strategy to the specific needs of each nation.
3.7.2.1. Effect on chronic HBV infection
HBV vaccination programs globally have caused a dramatic decrease in chronic HBV carrier rates, especially among younger generations. For instance, the HBsAg positivity rate in Taiwan plummeted from 19.7% in 1986 to 0.6% in 2015 [78]. The impact of HBV vaccination on the worldwide prevalence and incidence of CHB infection has been substantial. The implementation of routine infant vaccination in over 180 countries has notably reduced global HBV transmission and diminished chronic HBV prevalence [211]. By 2019, the coverage of three doses of the HBV vaccine reached 85% globally, marking a significant increase from approximately 30% in 2000, highlighting the successful implementation of vaccination programs [63].
The global effectiveness of the HBV vaccine is apparent in the substantial reduction in CHB prevalence and incidence, supported by comprehensive vaccination programs and documented success in diverse populations [28,119,188,200,201,202,203,204,205,206,208]. In regions with lower endemicity, the prevalence of the HBsAg carrier post-vaccination may effectively decrease to zero [69]. This phenomenon signifies a promising trajectory toward the elimination and ultimate eradication of HBV within the population [69]. Furthermore, the research emphasizes the highly effective nature of current vaccines, providing a protection rate of 94-98% against chronic HBV infection for at least 20 years [69]. The decline in reported acute HBV infections by approximately 90% since the introduction of HepB vaccination recommendations further underscores the vaccine’s impact, reducing the rate from 9.6 cases per 100,000 [212]. Additionally, recent findings indicate that HBV vaccination positively influences the survival of patients with chronic liver disease, further emphasizing the vaccine’s broader health benefits [39,159,161]
3.7.2.2. Effect on diseases related to acute HBV infection
Research consistently demonstrates the HBV vaccine’s effectiveness in reducing diseases related to acute hepatitis B infection [213,214,215,216,217]. Studies reveal a significant decline in the incidence of symptomatic acute hepatitis B and fulminant hepatitis in vaccinated individuals as opposed to those who have not received vaccination [213,215,216,217]. The vaccine effectively reduces the risk of severe liver-related complications linked to acute infection, such as liver failure or chronic hepatitis [214]. Additionally, it substantially decreases the likelihood of hospitalizations and mortality related to acute hepatitis B [213]. In Italy, where universal HBV vaccination was initiated in 1991, there was a notable decrease in CHB infection and the incidence of acute hepatitis B and acute hepatitis D [215,216]. However, it was observed that interrupting HBV infection through household contacts of chronic HBsAg carriers, injection drug use, and iatrogenic procedures was still necessary to eradicate residual HBV infection in the country. This evidence underscores the vaccine’s crucial role in preventing the severe health consequences of acute hepatitis B, highlighting its importance in public health initiatives aimed at reducing the burden of hepatitis-related illnesses.
3.7.2.3. Effect on Diseases related to chronic HBV infection
Extensive research consistently supports the effectiveness of the HBV vaccine in reducing HBV-associated membranous nephropathy (HBV-MN). Several studies conducted in different populations indicate that vaccination significantly decreases the incidence of HBV-MN following nationwide HBV vaccination [218,219,220]. Additionally, the vaccine substantially reduces the risk of CHB-related mortality by over 90% over 30 years [202].
3.7.2.4. Effect on Hepatocellular carcinoma (HCC):
HCC stands as the most prevalent primary liver cancer, representing a leading cause of global cancer-related deaths. CHB infection remains a significant risk factor for HCC, contributing to approximately 50-80% of cases worldwide [8]. In areas with intermediate to high HBV endemicity, HCC predominantly affects individuals in middle age and older; however, occasional cases are observed in children, usually linked to chronic HBV infection acquired through maternal transmission [221].
The development of a safe and effective HBV vaccine has provided a potent tool for preventing HBV infection and its associated complications, including HCC. Vaccination programs globally have resulted in a substantial reduction in chronic HBV carrier rates, particularly among younger generations [69]. For example, in Taiwan, the HBsAg positivity rate dropped from 19.7% in 1986 to 0.6% in 2015 [222]. As fewer individuals contract chronic HBV infection, the long-term expectation is a decline in the prevalence of HCC cases. This trend is already evident in certain regions, with younger populations exhibiting significantly lower HCC rates compared to their older, unvaccinated counterparts [69].
Numerous studies have illustrated the remarkable effectiveness of HBV vaccination in reducing both the incidence and prevalence of HCC. In Taiwan, the introduction of universal neonatal HBV vaccination in 1984 resulted in a significant decline in HCC incidence among younger age groups, achieving an 80% decrease after 30 years [223]. Similar positive trends were observed in Shanghai, with a 49.2% reduction in HCC incidence in males and 51.9% in females 30 years after the initiation of their vaccination program [223]. Globally, studies conducted across various regions and countries consistently report substantial reductions in HCC incidence among cohorts born after the implementation of vaccination programs [224,225,226,227].
4. Global Impact of HBV Vaccination Programs: Successes and Challenges
The HBV vaccine is the keystone intervention in combating the worldwide burden of HBV infection. As of the close of 2022, the WHO reported that an impressive 190 nations (97%) integrated birth doses into their EPI schedules for comprehensive coverage [199]. Infant completion rates for the 3-dose HBV vaccine regimen surged remarkably from 1% in 1990 to 84% in 2022 [199]. Furthermore, 113 Member States implemented nationwide single-dose HBV vaccine administration to newborns within the initial 24 hours of life.
The HBV vaccine boasts a remarkable track record, demonstrating a near 95% reduction in CHB infection [198]. Global HBV prevalence significantly dropped from over 10% in the 1980s to around 2.9% in 2020, resulting in millions of lives saved and the prevention of chronic liver disease and HCC cases [224].
The vaccine’s impact transcends individual protection, safeguarding entire communities and future generations from the devastating consequences of HBV infection. This herd immunity effect is evident in countries with high-coverage infant vaccination programs, observing a noteworthy decline in transmission among both vaccinated and unvaccinated groups [228].
Recent large studies analyzing the positive impact of universal HBV vaccination reveal a global decline in HBV prevalence, especially in children under five [17,229], considering prophylaxis programs, notably infant vaccination. Mainland China, with the highest overall HBV prevalence, ranking 16th in HBV infections among ≤ 5-year-old children, attributes its success to timely birth dose coverage of 90% or greater [17].
This remarkable progress can be attributed to several key factors. Foremost, the WHO established global goals to attain HBV elimination by 2030, underscoring the importance of timely birth doses to prevent MTCT and early horizontal transmission of the virus, the most prevalent cause of HBV transmission worldwide [11,12,15,25,224]. Increased awareness among healthcare providers and communities about the benefits of timely birth doses has contributed to higher acceptance and implementation [230]. Moreover, the significant reduction in vaccine cost (below $1 per dose), crucial financial and logistical support provided by GAVI since 2001, and the substantial rise in pentavalent vaccine coverage in GAVI-supported countries all played a significant role [231]. Despite overall progress, regional disparities persist. While the Western Pacific (90%), Americas (89%), and Southeast Asia (87%) regions exceed the global average, Europe (81%), the Eastern Mediterranean (80%), and Africa (75%) lag behind [199].
The WPR, with early adoption of birth-dose vaccination, stands as a testament to the program’s efficacy. Notably, the region’s HBsAg positivity rate dropped from 8.3% to a mere 0.93% between 2002 and 2015 [39]. Furthermore, HBV vaccination effectively protects healthcare workers from occupational infection and subsequent chronic disease [51,62,104,105].
Early adopters like Taiwan, Bulgaria, Malaysia, The Gambia, Italy, Spain, and the United States exemplify success through universal HBV immunization. Taiwan, in particular, witnessed a dramatic decline in HBV transmission, disease burden, and HBsAg positivity since its mass neonatal vaccination program in 1984 [10,78,119,188,201,202,205]. The annual HCC incidence among children aged 6-14 significantly decreased, solidifying the vaccine’s potential as a successful cancer-preventative measure [222].
The global adoption of HBV vaccination and enhanced coverage have yielded remarkable results in reducing the HBV burden and preventing HCC. Ongoing efforts to achieve universal coverage, particularly in regions with lower implementation rates, offer substantial potential for further alleviating the public health impact of this critical viral infection.
Despite undeniable successes, meeting the 2030 WHO targets for HBV vaccination necessitates addressing substantial challenges associated with vaccine utilization. Numerous barriers impacting the effective expansion of HBV vaccine uptake have been identified [232,233,234,235,236], presenting diverse characteristics across countries and affecting different target groups. These barriers vary based on healthcare systems, caregiver awareness, cultural beliefs, and accessibility to vaccination services. These barriers can be categorized into different groups, including System Issues”, “User Issues”, “Service Provider Issues” and “Socio-Culture Factors” [235]. Key barriers include limited availability and accessibility to health-facility-based immunization, lack of caregiver awareness, inadequate communication by healthcare workers, negative relationships with beneficiaries, high vaccine costs in the private sector, and challenges related to the time and place of vaccination [235]. Emphasizing the contextual nature of these barriers is crucial, recognizing that different countries are at varying stages of implementing HBV vaccination [235].
Understanding the intricate challenges is essential to achieving widespread HBV vaccination aligned with the WHO framework. A comprehensive strategy involves addressing issues of affordability, enhancing healthcare infrastructure, eliminating sociocultural obstacles, prioritizing HBV within public health frameworks, and fostering effective communication and collaboration. These measures constitute fundamental building blocks for a future where the impact of HBV is significantly reduced, realizing the full potential of this life-saving vaccine.
5. Progress Towards Achieving WHO Targets for 2030 HBV Elimination: 2016-2023
5.1. Impact of HBV vaccination
Since its introduction in 1982, the HBV vaccine has revolutionized the battle against this insidious pathogen. As the WHO sets ambitious targets for HBV elimination by 2030, the vaccine emerges as a cornerstone intervention with a profound impact on reducing the disease burden [15]. From 2015 to 2020, global coverage of the third dose of the HBV vaccine increased from 82% to 85%, while the administration of the birth dose increased from 38% to 43% [237]. Infant vaccination programs, particularly in high-endemic regions like Taiwan, showcase a notable decline in HBsAg positivity from 9.8% in 1984 to 0.6% in 2004, primarily driven by neonatal immunization [119,188,202,204].
The influence of the HBV vaccine extends beyond preventing chronic infection. Reducing carrier rates subsequently lowers the incidence of HBV-related complications, including HCC, a major cause of mortality [238]. Mathematical modeling estimates reveal that global HBV vaccination programs averted 210 million new HBV infections and 1.2 million HCC deaths between 2000 and 2015, translating to millions of lives saved and significantly reducing healthcare costs associated with HBV-related complications [175,239].
5.2. The Feasibility of HBV Elimination by 2030
HBV elimination, per the epidemiological definition, means a reduction to zero of HBV incidence in defined geographical areas due to deliberate efforts. Presently, HBV elimination aligns with the 2016 WHO targets for viral HBV infections, focusing on controlling viral hepatitis by reducing its incidence, morbidity, and mortality to locally acceptable levels rather than absolute elimination [16,249]. The global initiative for HBV elimination by 2030, outlined by WHO, encompasses three primary objectives: establishing a world free from viral transmission of HBV, ensuring individuals with viral hepatitis access safe, affordable, and effective care, and eliminating viral hepatitis as a major public health threat by 2030 (with a note that complete elimination may not be achieved). Additionally, the aim is to substantially decrease the incidence of chronic viral hepatitis and the associated morbidity and mortality [11,16].
The feasibility of global HBV elimination is rooted in the virus’s characteristics, reliable diagnostic assays, and cost-effective measures. These measures involve implementing universal HBV immunization, antiviral treatment for highly viremic mothers in the third trimester to prevent MTCT, HBV screening in blood donors, adopting safe injection practices, implementing stringent infection-control programs to reduce HBV infections, and providing antiviral treatments for patients with HBV infection [240]. Despite the ambitious task of achieving global HBV elimination by 2030, substantial work is imperative in the coming few years.
The available evidence suggests that the ambitious goal of achieving global HBV elimination by 2030 faces significant challenges. Despite the existence of tools to reach these goals since 2015, they remain insufficient or absent in various countries and regions, including high-income nations. Globally, HBV diagnosis rates are alarmingly low, averaging only 8% [250,251]. While certain areas make strides in prophylaxis and prevalence targets for HBV infection, studies emphasize that all regions must significantly increase rates of diagnosis and access to treatment to meet the global targets [12,19,251].
Unfortunately, given the staggering number of individuals chronically infected with viral hepatitis (257 million) and its devastating global burden (almost 900,000 annual deaths) [175] and coupled with the current efforts to combat the disease, achieving these targets in the next remaining years appears unlikely, particularly in resource-limited settings. WHO has advocated for multiple key interventions to achieve these targets, yet implementation remains lacking in most locations [175]. For instance, attaining a 90% HBV immunization coverage, including HBV birth-dose vaccine coverage, proves challenging in regions like Africa, with current HBV birth-dose vaccine coverage estimated at 11% or even lower in resource-constrained areas [245]. Similarly, increasing antiviral treatment provision to 80% by 2030 seems extremely challenging, especially in low- and middle-income countries (LMICs), where less than 5% of individuals infected with HBV or HCV are currently tested and enrolled in care and treatment programs [175]. In many LMICs, affordable access to viral hepatitis testing and treatment is nearly impossible, posing a significant barrier to scaling up screen-and-treat interventions [242]. High-income countries face their challenges, with millions remaining undiagnosed and infected individuals often belonging to vulnerable populations (undocumented migrants, injection drug users, homeless individuals) who are challenging to reach and enroll in care. In various locations, including LMICs, where the population is aging and untested, there is a potential for an increase in mortality due to viral hepatitis in 2030 compared to 2015. Lastly, tracking progress on WHO elimination targets necessitates not only the development of national hepatitis plans by countries but also establishing surveillance systems to measure the incidence and burden of liver disease, currently either nonexistent or of poor quality in most LMICs [175].
While recognizing commendable initiatives by the WHO in collaboration with different stakeholders to initiate the elimination of viral hepatitis, an urgent need arises for developing and implementing realistic strategies tailored to diverse environments and specific populations. This imperative involves a heightened mobilization of civil society, health policymakers, and funders, as the current commitment to the fight against viral hepatitis remains notably inadequate. In comparison to other infectious diseases such as HIV and malaria, viral hepatitis faces substantial underfunding for both research and elimination efforts.
The WHO implores all countries and regions to invest in eliminating hepatitis by incorporating costing, budgeting, and financing elimination services within their universal health coverage plans. Achieving this objective necessitates not only effective treatment but also comprehensive policies addressing the prevention of new infections, financial structures, political will, stakeholder engagement, and integration within the healthcare system. The fusion of prevention and treatment to combat viral hepatitis is a feasible approach, albeit requiring substantial investments in healthcare system strengthening and the complete continuum of viral hepatitis services. This investment is expected to yield direct, indirect, and cross-sectoral economic benefits by saving lives and alleviating the cost burden of the disease on individuals, their families, and the state [246].
The estimated cost of implementing key interventions in low- and middle-income countries (LMICs) between 2016 and 2021 amounts to US$11.9 billion, with the principal cost drivers being testing and treatment for hepatitis B and C [24]. Economic analyses in various regions highlight the cost-effectiveness of population-based approaches to testing and treating, emphasizing the need for a strategic investment of $6 billion annually to avert 4.5 million premature deaths by 2030 and more than 26 million deaths beyond that target date. However, if medicines remain inaccessible and patent-protected in 13 LMICs, the cost would escalate to $118 billion [247].
For instance, to align with the WHO’s goal of eliminating viral hepatitis, global diagnosis coverage should surge from 9–20% in 2015 to 90% in 2030. Additionally, treatment coverage must advance from 7–8% in 2015 to 80% in 2030 [241]. In clinical practice, treatment coverage hinges on diagnosis followed by linkage to care, requiring countries to intensify national plan efforts. Nevertheless, critical gaps persist in current policies.
In a 2017 survey encompassing all 194 Member States, approximately 70% (135 countries/regions) formulated national plans for WHO elimination goals. However, fewer than 50% secured funding, and even in funded cases, the allocated amounts fell short of covering the entire plan [237]. High-income countries confront ‘diagnostic burnout,’ treating easily accessible patients while leaving marginalized populations, such as homeless individuals, prisoners, people who inject drugs, and a significant portion of the general population, undiagnosed. Consequently, only 11 high-income countries are currently on track to eliminate viral hepatitis by 2030 [248].
This lack of progress signifies a policy failure. In 2019, as part of the Lancet Gastroenterology & Hepatology Commission, major policy deficiencies were highlighted in 66 studied countries [242]. These deficiencies encompassed a lack of available national epidemiological data and publicly funded screening programs for viral hepatitis. Across countries, there was a diverse spectrum of policy responses, with some having all recommended policies in place. In contrast, others ranked poorly, often with only a single policy, such as mandatory screening of blood products [249]. Moreover, many countries lacked estimates of the potential economic impact of viral hepatitis on their populations [249].
5.3. Effect of COVID-19 on the 2030 elimination plan
The COVID-19 pandemic has had profound effects on global initiatives to eliminate hepatitis B and C by 2030. A multinational European Association for the Study of the Liver (EASL) survey reveals a significant impact, resonating across diverse regions [250]. Numerous elimination programs have experienced slowdowns or complete halts due to the pandemic, resulting in a potential one-year delay in hepatitis diagnosis and treatment. This delay could lead to an alarming increase in liver cancers and deaths attributed to HCV, with projections estimating 44,800 additional liver cancers and 72,300 deaths globally by 2030 [251].
The WHO’s elimination target of viral hepatitis worldwide by 2030 was severely affected by the divergence of attention and resources towards COVID-19. The necessary focus on the pandemic has led to doubts about achieving the previously commendable goal [251]. To combat this setback, a collective reassessment and revision of global and national goals and action plans are imperative within the hepatitis community.
The economic downturn associated with the pandemic has posed challenges for committing new funds and jeopardized previously allocated resources for viral hepatitis elimination [252]. The long-term impact of COVID-19 on global healthcare systems underscores the need for strategic utilization of resources invested in mitigating the pandemic’s effects. These funds could contribute to the reinforcement of surveillance and healthcare systems, ultimately enhancing viral hepatitis services [253].
5.4. Key areas of progress towards the 2030 elimination goals:
Significant strides have been made since 2015 towards achieving the World Health Organization’s (WHO) ambitious 2030 elimination goals for hepatitis. The WHO has been instrumental in providing crucial tools for the development of national strategies, test-and-treat guidelines for hepatitis B and C, cost-effectiveness quantitative analysis (WHO CHOICE), a global hepatitis reporting system, and consolidated strategic information guidelines [259,260,261].
A 2019 study revealed that 62% of Member States had formulated national hepatitis plans, with 27% in the draft stage by 2017. Of these plans, 58% included domestic funding [237]. Forty-five countries/regions have contributed data to the new global reporting system for hepatitis.
Regarding HBV infection, there has been notable progress in immunization coverage. By the end of 2018, the HBV infant vaccine had been introduced in 189 countries/regions, achieving global coverage of three vaccine doses estimated at 84% [245].
Historically, the WHO WPR had the world’s highest prevalence of chronic HBV infection. Various countries in this region, including Papua New Guinea, the Philippines, Vietnam, Lao People’s Democratic Republic, and China, had prevalence rates exceeding 5%. In 2017, the WPR successfully reduced the prevalence of chronic HBV infection to 0.93% in 5-year-old children, meeting the WHO target [257]. GAVI’s expanded support for HBV vaccine birth-dose coverage has been crucial, potentially averting 0.3–1.2 million perinatal infection-related deaths and 1.2–1.5 million cases from 2021–2025.
Despite this progress, estimates indicate insufficient HBV birth-dose vaccine coverage globally, particularly in Africa, where only 11% of newborns receive the recommended dose within 24 hours [245]. Civil society bodies like the World Hepatitis Alliance continue to play a pivotal role in engaging donors and stakeholders, ensuring an evidence-based approach to the response.
Examining Taiwan as a case study reveals substantial advancements toward the 2030 elimination goals. These include preventing vertical HBV transmission through immunization and antiviral treatment for highly viremic mothers, ensuring widespread access to potent, safe, and affordable HBV treatments, and initiating changes in reimbursement policies for HBV therapy. Taiwan’s proactive approach, including universal HBV vaccination since 1986, significantly reduces HBsAg carriage rates and expands treatment indications. The country aims to reach the WHO goals by 2025, five years ahead of the 2030 deadline [202].
Developed over a decade ago, the latest generation of nucleoside analogues for HBV has demonstrated enduring safety and effectiveness in preventing CHB-related liver complications, such as cirrhosis and HCC [258]. The introduction of generic medications has not only decreased treatment costs but has also expanded treatment accessibility in numerous countries. Additionally, a crucial stride towards enhancing global vaccine coverage involves the creation of polyvalent vaccine formulations encompassing the HBV vaccine for infants and children.
Advancements in HBV therapeutics have been witnessed recently, with industry investments paving the way for new drugs targeting various steps in the HBV life cycle and immune responses. Although no new therapeutics have reached phase III trials, the development of combination therapies holds promise for a functional cure, suppressing HBV replication after a finite course of treatment [259].
The emergence of viral hepatitis patient associations, non-governmental groups, and national hepatitis programs in many countries/regions signifies growing public and political awareness, contributing to the global effort to eliminate hepatitis [20]
5.5. Strategies for Achieving HBV Elimination by 2030
The development of an effective HBV vaccine has substantially contributed to controlling the spread and progression of HBV-related diseases. However, projections indicate that the persistence of HBsAg prevalence requires intervention. Post-2050, numerous countries are expected to make strides toward established goals. Specifically, only three countries are projected to achieve a 90% reduction in HBV incidence, with none reaching a 65% reduction in mortality compared to 2015, and no country is expected to meet all current HBV elimination targets [260].
While notable progress has been made, meeting the WHO’s ambitious goals for HBV elimination by 2030 necessitates continual monitoring and addressing persisting barriers hindering effective prevention, diagnosis, and treatment interventions. Critical examination of these barriers aims to identify practical solutions, paving the way for a more holistic and equitable approach towards WHO targets.
Each country and community must develop practical and sustainable strategies tailored to their unique circumstances. The primary focus for the next seven years should be on prevention through universal birth-dose vaccination for all newborns globally. Additionally, health education, tailored to different high-risk populations, is crucial in increasing awareness of HBV infection risk factors, consequences of chronic liver disease, and the benefits of screening and effective treatment regimens.
Another critical aspect involves increasing public awareness of HBV infections through mass screening programs and linking patients to point-of-care facilities [261]. The imperative task of addressing undiagnosed individuals, known as the “missing millions,” involves combating the barriers of awareness, limited healthcare access, and diagnostic challenges on a global scale. Initiatives like the World Hepatitis Alliance’s “Find the Missing Millions” campaign are pivotal in heightening awareness and improving diagnostic endeavors worldwide [261,262].
To ensure the success of elimination strategies, we must make concerted efforts to eradicate the stigma associated with HBV. Due to public misconceptions regarding HBV transmission, individuals with CHB infection often face unjust bias attributed to perceived ‘bad behaviors,’ leading to discrimination based on the fear of casual transmission [267].
The adoption of Micro-elimination strategies targets individual population segments for quicker and more efficient treatment and prevention interventions [264]. These programs may address districts with high prevalence, identify pockets of high prevalence within districts, take measures to prevent transmission, address risk factors, and identify target groups to treat infection and prevent transmission. For example, these programs may focus on antenatal screening, infant vaccination, catch-up vaccination, vaccination of persons who inject drugs, prisoners, decompensated cirrhosis, veterans, or patients with hemophilia, and homosexuals. Creating a lifetime Markov model demonstrates that strategies to vaccinate, prevent, or treat CHB in high-risk populations significantly reduce cirrhosis, decompensation, liver cancer, and chronic hepatitis death compared to no intervention [106]. Micro-elimination strategies are tailored with realistic and well-defined targets and goals. These are pragmatic, with a shorter time to achievement, and costs can be predicted. Micro-elimination projects may generate a template in a small, geographically defined population that may then be used to model services for larger intervention programs. Successful micro-elimination efforts encourage further public health strategies. Micro-elimination of HBV appears cost-effective and positively impacts long-term outcomes with screening and treatment or vaccination strategy compared with no intervention [264].
In the context of HBV, imperative initiatives involve implementing programs for the timely administration of HBV vaccines at birth in Africa and other highly endemic regions [245]. Given that a significant number of HBV-infected individuals reside in resource-poor areas, urgent actions are required to enhance access to diagnosis, treatment, and cure. Considering that HBV is a primary contributor to HCC, it is essential to establish screening programs for HCC in individuals infected with HBV [265].
The path to HBV elimination demands sustained commitment, improved coordination among diverse HBV prevention programs, and heightened efforts to diagnose and treat eligible individuals. Given the substantial occurrence of MTCT, comprehensive testing for HBV in pregnant women is crucial. If infection is detected, administering HBIG to newborns promptly is vital to prevent transmission. Addressing challenges in HBIG administration in Low- and Middle-Income Countries (LMICs), where MTCT is prevalent, underscores the need for HBV diagnosis and treatment strategies in eligible women of child-bearing age to mitigate MTCT. In general, broad-scale diagnosis and treatment of HBV-infected individuals are imperative for achieving HBV elimination [12,19,254].
A pivotal objective for the upcoming decade is the discovery of agents that functionally cure HBV, moving beyond mere suppression.
Countries with limited resources require international investments in viral hepatitis programs encompassing prevention and treatment strategies. Additionally, enhancing blood safety and harm reduction programs, particularly among people who inject drugs, is vital to curtail HBV transmission. Reducing drug costs, including introducing generic agents, can elevate treatment coverage for HBV infections. Crucially, the development of curative regimens for HBV will significantly expedite the achievement of elimination goals [266].
Regular monitoring and evaluation are indispensable for assessing the efficacy of implemented solutions and making necessary adjustments. By addressing these challenges comprehensively, we can expedite progress toward the 2030 goal of eliminating HBV ultimately saving millions of lives.
6. The Road Ahead: Sustaining Progress Beyond 2030
Achieving continual advancement in the quest for HBV elimination beyond 2030 necessitates the establishment of robust healthcare systems, the implementation of ongoing surveillance, and the initiation of accessible vaccination initiatives. The integration of these measures into primary healthcare, coupled with the fostering of community engagement, serves to fortify prevention efforts [20]. The long-term sustainability of this progress hinges on the proactive management of HBV, with a particular emphasis on the pivotal role played by the HBV vaccine. Continuous research endeavors are imperative to enhance diagnostics, develop cost-effective treatments, and pursue a functional cure. The prospect of HBV elimination is significantly enhanced if a ‘cure,’ even in a functional form, can be realized through a finite course of safe and affordable oral medications, as opposed to the current protracted treatments [267]. Ongoing innovations in drug development technology are anticipated to expedite progress toward discovering a sterilizing cure for HBV, working in tandem with vaccination programs to facilitate global HBV eradication.
Innovations in vaccine technology, including multi-antigen or therapeutic vaccines, hold promise for prevention and treatment. Developing Next-Generation HBV Vaccines with improved attributes, such as thermostability, broader coverage, and longer-lasting immunity, can enhance accessibility and overall effectiveness. Encouraging innovations in hepatitis vaccine delivery methods is paramount for eradicating hepatitis beyond 2030.
Advancements in rapid diagnostic tests, point-of-care technologies, and novel antiviral therapies are poised to streamline early diagnosis, simplify treatment procedures, and enhance patient outcomes. The integration of digital tools for data collection and program management optimizes resource allocation and tailors interventions, thereby improving program efficacy. Addressing social determinants of health, reducing health disparities, and fostering global collaboration is indispensable for ensuring long-term success [268].
Despite the efficacy of the currently available antiviral therapy in suppressing HBV, patients with advanced hepatic fibrosis or cirrhosis remain susceptible to liver cancer. The clinical importance of monitoring these patients with novel biomarkers for risk stratification cannot be overstated. Future research directions include the development of chemopreventive agents to mitigate hepatocarcinogenesis post-viral control or cure. While a reduction in advanced liver diseases related to HBV infection is anticipated post-2030, the emergence of other liver diseases, such as metabolic liver disease, alcoholic liver disease, or drug-induced liver injury, is a possibility [269]. Emphasizing health education on risk factors and promoting a healthy lifestyle becomes paramount in the coming decades.
Furthermore, to ensure sustained progress beyond 2030, diligent monitoring and evaluation initiatives are indispensable for pinpointing and enhancing specific actions, thereby securing the retention of achievements. A global deficiency persists in addressing viral hepatitis, with it remaining low on the policy agenda for most governments worldwide. Sub-Saharan Africa encounters challenges, treating only a limited number of individuals and conducting minimal testing, exacerbated by insufficient technical assistance from the WHO and amplified human resource limitations, especially amidst and after the COVID-19 pandemic [20]. Country-level barriers, from procurement to deployment and restrictive regulations, impede progress. Even upon achieving the 2030 target, substantial ongoing work is envisaged, as not all countries may eliminate viral hepatitis by then, and reaching WHO targets does not guarantee universal diagnosis and treatment. The primary focus should be removing viral hepatitis from the major public health threats list by 2030 while upholding continuous attention to the issue.
7. Conclusions
Worldwide, approximately 257 million individuals have been affected by HBV infection, presenting a substantial global public health threat, with complications ranking as the seventh-leading cause of mortality. Despite the formidable nature of the task, the ambitious objective to eliminate HBV by 2030 necessitates significant efforts. Ongoing global initiatives face feasibility challenges influenced by diverse factors, posing specific challenges in various regions or populations. The implementation of HBV vaccination emerges as a cost-effective and pivotal intervention, contributing to an impressive 95% reduction in CHB infection. The global prevalence of HBV has seen a substantial decrease from over 10% in the 1980s to 2.9% in 2020, resulting in the preservation of millions of lives and the prevention of chronic liver disease and liver cancer cases. While the global adoption of HBV vaccination is considered successful, addressing existing challenges is crucial for achieving WHO’s ambitious elimination targets, with a focus on realizing the vaccine’s full potential. Integral components of the program encompass prevention strategies, perinatal and neonatal vaccination, post-vaccination monitoring, catch-up vaccination, and carrier registration. Enhancing the program’s effectiveness involves a continuum of care, integration with local healthcare services, and the implementation of simplified guidelines for diagnosis and treatment. Sustaining progress demands a long-term commitment to sustainability and continuous innovation, with an emphasis on the establishment of national policies, micro-elimination strategies, and surveillance to monitor progress and assess the program’s impact on incidence, mortality, and services.
Author Contributions
Conceptualization, S.A.B. writing—original draft preparation, S.A.B.; writing—review and editing, S.A.B. and A.W.; visualization, S.A.B., and A.W.; supervision, S.A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This paper received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- S. Locarnini, A. Hatzakis, D. S. Chen, and A. Lok, ‘Strategies to control hepatitis B: Public policy, epidemiology, vaccine and drugs’, J Hepatol, vol. 62, no. 1 Suppl, pp. S76–S86, 2015. [CrossRef]
- C. W. Spearman et al., ‘Hepatitis B in sub-Saharan Africa: strategies to achieve the 2030 elimination targets’, Lancet Gastroenterol Hepatol, vol. 2, no. 12, p. 900, Dec. 2017. [CrossRef]
- J. D. Stanaway et al., ‘The global burden of viral hepatitis from 1990 to 2013: findings from the Global Burden of Disease Study 2013′, Lancet, vol. 388, no. 10049, pp. 1081–1088, Sep. 2016. [CrossRef]
- J. H. Kao, P. J. Chen, and D. S. Chen, ‘Recent Advances in the Research of Hepatitis B Virus-Related Hepatocellular Carcinoma: Epidemiologic and Molecular Biological Aspects’, Adv Cancer Res, vol. 108, no. C, pp. 21–72, Jan. 2010. [CrossRef]
- G. Fattovich, T. Stroffolini, I. Zagni, and F. Donato, ‘Hepatocellular carcinoma in cirrhosis: Incidence and risk factors’, Gastroenterology, vol. 127, no. 5, pp. S35–S50, Nov. 2004. [CrossRef]
- A. S. F. Lok, ‘Chronic hepatitis B’, N Engl J Med, vol. 346, no. 22, pp. 1682–1683, May 2002. [CrossRef]
- S. Ibrahim, S. El Din, and I. Bazzal, ‘Antibody level after hepatitis-B vaccination in hemodialysis patients: impact of dialysis adequacy, chronic inflammation, local endemicity and nutritional status.’, J Natl Med Assoc, vol. 98, no. 12, p. 1953, Dec. 2006, Accessed: Dec. 29, 2023. [Online]. Available: /pmc/articles/PMC2569692/?report=abstract.
- A. P. Venook, C. Papandreou, J. Furuse, and L. Ladrón de Guevara, ‘The incidence and epidemiology of hepatocellular carcinoma: a global and regional perspective’, Oncologist, vol. 15 Suppl 4, no. S4, pp. 5–13, Nov. 2010. [CrossRef]
- C. E. Stevens et al., ‘Perinatal Hepatitis B Virus Transmission in the United States: Prevention by Passive-Active Immunization’, JAMA, vol. 253, no. 12, pp. 1740–1745, Mar. 1985. [CrossRef]
- C. E. Stevens, R. P. Beasley, J. Tsui, and W.-C. Lee, ‘Vertical transmission of hepatitis B antigen in Taiwan’, N Engl J Med, vol. 292, no. 15, pp. 771–774, Apr. 1975. [CrossRef]
- WHO, ‘Global Health Sector Strategies on HIV, Viral Hepatitis and the sexually transmitted infections’, World Health Organization, vol. ector stra, no. June 2021, pp. 2022–2030, 2021, Accessed: Dec. 16, 2023. [Online]. Available: https://www.who.int/publications/i/item/9789240027077.
- D. Razavi-Shearer et al., ‘Global prevalence, cascade of care, and prophylaxis coverage of hepatitis B in 2022: a modelling study’, Lancet Gastroenterol Hepatol, vol. 8, no. 10, pp. 879–907, Oct. 2023. [CrossRef]
- A. Jaquet, G. Muula, D. K. Ekouevi, and G. Wandeler, ‘Elimination of Viral Hepatitis in Low and Middle-Income Countries: Epidemiological Research Gaps’, Current Epidemiology Reports 2021 8:3, vol. 8, no. 3, pp. 89–96, Jul. 2021. [CrossRef]
- Y. Ding, X. Sun, Y. Xu, L. Yang, Y. Zhang, and Q. Shen, ‘Association Between Income and Hepatitis B Seroprevalence: A Systematic Review and Meta-analysis’, Hepatitis Monthly 2020 20:10, vol. 20, no. 10, p. 104675, Oct. 2020. [CrossRef]
- ‘Global health sector strategy on viral hepatitis 2016-2021. Towards ending viral hepatitis’. Accessed: Jan. 16, 2024. [Online]. Available: https://www.who.int/publications/i/item/WHO-HIV-2016.06.
- T. Solomon-Rakiep, J. Olivier, and E. Amponsah-Dacosta, ‘Weak Adoption and Performance of Hepatitis B Birth-Dose Vaccination Programs in Africa: Time to Consider Systems Complexity?-A Scoping Review’, Trop Med Infect Dis, vol. 8, no. 10, Oct. 2023. [CrossRef]
- D. Razavi-Shearer et al., ‘Global prevalence, cascade of care, and prophylaxis coverage of hepatitis B in 2022: a modelling study’, Lancet Gastroenterol Hepatol, vol. 8, no. 10, pp. 879–907, Oct. 2023. [CrossRef]
- J. Howell et al., ‘Pathway to global elimination of hepatitis B: HBV cure is just the first step’, Hepatology, vol. 78, no. 3, p. 976, Sep. 2023. [CrossRef]
- K. McCulloch, N. Romero, J. MacLachlan, N. Allard, and B. Cowie, ‘Modeling Progress Toward Elimination of Hepatitis B in Australia’, Hepatology, vol. 71, no. 4, pp. 1170–1181, Apr. 2020. [CrossRef]
- A. L. Cox et al., ‘Progress towards elimination goals for viral hepatitis’, Nature Reviews Gastroenterology & Hepatology 2020 17:9, vol. 17, no. 9, pp. 533–542, Jul. 2020. [CrossRef]
- Y. Waheed, M. Siddiq, Z. Jamil, and M. H. Najmi, ‘Hepatitis elimination by 2030: Progress and challenges’, World J Gastroenterol, vol. 24, no. 44, p. 4959, Nov. 2018. [CrossRef]
- A. Elsharkawy, R. Samir, M. Abdallah, M. Hassany, and M. El-Kassas, ‘The implications of the COVID-19 pandemic on hepatitis B and C elimination programs in Egypt: current situation and future perspective’, Egyptian Liver Journal, vol. 13, no. 1, pp. 1–10, Dec. 2023. [CrossRef]
- ‘Global Viral Hepatitis: Millions of People are Affected | CDC’. Accessed: Dec. 23, 2023. [Online]. Available: https://www.cdc.gov/hepatitis/global/index.htm.
- S. Chen, W. Mao, L. Guo, J. Zhang, and S. Tang, ‘Combating hepatitis B and C by 2030: achievements, gaps, and options for actions in China’, BMJ Glob Health, vol. 5, no. 6, p. 2306, Jun. 2020. [CrossRef]
- F. Cui et al., ‘Global reporting of progress towards elimination of hepatitis B and hepatitis C’, Lancet Gastroenterol Hepatol, vol. 8, no. 4, pp. 332–342, Apr. 2023. [CrossRef]
- Geneva: World Health Organization, ‘Global health sector stategies on, respectively, HIV, viral hepatitis and sexual transmitted infections for the period 2022-2030′, Braz Dent J., vol. 33, no. 1, pp. 1–12, 2022.
- S. M. F. Akbar, M. Al-Mahtab, S. Khan, O. Yoshida, and Y. Hiasa, ‘Elimination of Hepatitis by 2030: Present Realities and Future Projections’, Infectious Diseases and Immunity, vol. 2, no. 1, pp. 3–8, Jan. 2022. [CrossRef]
- Z. Luo, L. Li, and B. Ruan, ‘Impact of the implementation of a vaccination strategy on hepatitis B virus infections in China over a 20-year period’, International Journal of Infectious Diseases, vol. 16, no. 2, pp. e82–e88, Feb. 2012. [CrossRef]
- A. S. Chitnis and R. J. Wong, ‘Review of Updated Hepatitis B Vaccine Recommendations and Potential Challenges With Implementation’, Gastroenterol Hepatol (N Y), vol. 18, no. 8, p. 447, Aug. 2022, Accessed: Dec. 16, 2023. [Online]. Available: /pmc/articles/PMC9666805/.
- J. H. Kao and D. S. Chen, ‘Global control of hepatitis B virus infection’, Lancet Infect Dis, vol. 2, no. 7, pp. 395–403, Jul. 2002. [CrossRef]
- H. Zhao, X. Zhou, and Y. H. Zhou, ‘Hepatitis B vaccine development and implementation’, Hum Vaccin Immunother, vol. 16, no. 7, pp. 1533–1544, Jul. 2020. [CrossRef]
- P. Van Damme, ‘Long-term Protection After Hepatitis B Vaccine’, J Infect Dis, vol. 214, no. 1, pp. 1–3, Jul. 2016. [CrossRef]
- M. R. Hilleman, W. J. McAleer, E. B. Buynak, and A. A. McLean, ‘The preparation and safety of hepatitis B vaccine’, vol. 7, pp. 3–8. [CrossRef]
- D. P. Francis et al., ‘The Safety of the Hepatitis B Vaccine: Inactivation of the AIDS Virus During Routine Vaccine Manufacture’, JAMA, vol. 256, no. 7, pp. 869–872, Aug. 1986. [CrossRef]
- S. CE et al., ‘Yeast-recombinant hepatitis B vaccine. Efficacy with hepatitis B immune globulin in prevention of perinatal hepatitis B virus transmission’, JAMA, vol. 257, no. 19, pp. 2612–2616, May 1987. [CrossRef]
- A. M. Krieg, ‘CpG Motifs in Bacterial DNA and Their Immune Effects’, vol. 20, no. 1, pp. 709–760. [CrossRef]
- M. Davidson and S. Krugman, ‘IMMUNOGENICITY OF RECOMBINANT YEAST HEPATITIS B VACCINE’, vol. 325, no. 8420, pp. 108–109. [CrossRef]
- W. Jilg, M. Schmidt, G. Zoulek, B. Lorbeer, B. Wilske, and F. Deinhardt, ‘CLINICAL EVALUATION OF A RECOMBINANT HEPATITIS B VACCINE’, vol. 324, no. 8413, pp. 1174–1175. [CrossRef]
- J. Pattyn, G. Hendrickx, A. Vorsters, and P. Van Damme, ‘Hepatitis B Vaccines’, J Infect Dis, vol. 224, no. Suppl 4, p. S343, Oct. 2021. [CrossRef]
- J. M. Janssen, W. L. Heyward, J. T. Martin, and R. S. Janssen, ‘Immunogenicity and safety of an investigational hepatitis B vaccine with a Toll-like receptor 9 agonist adjuvant (HBsAg-1018) compared with a licensed hepatitis B vaccine in patients with chronic kidney disease and type 2 diabetes mellitus’, vol. 33, no. 7, pp. 833–837. [CrossRef]
- R. S. Janssen et al., ‘Immunogenicity and safety of an investigational hepatitis B vaccine with a toll-like receptor 9 agonist adjuvant (HBsAg-1018) compared with a licensed hepatitis B vaccine in patients with chronic kidney disease’, vol. 31, no. 46, pp. 5306–5313. [CrossRef]
- B. P. Sablan et al., ‘Demonstration of safety and enhanced seroprotection against hepatitis B with investigational HBsAg-1018 ISS vaccine compared to a licensed hepatitis B vaccine’, vol. 30, no. 16, pp. 2689–2696. [CrossRef]
- C. Hristian et al., ‘Vaccinations and the Risk of Relapse in Multiple Sclerosis’. vol. 344, no. 5, pp. 319–326, Feb. 2001. [CrossRef]
- M. A. Hernán, S. S. Jick, M. J. Olek, and H. Jick, ‘Recombinant hepatitis B vaccine and the risk of multiple sclerosis: A prospective study’, Neurology, vol. 63, no. 5, pp. 838–842, Sep. 2004. [CrossRef]
- A. D. Jack, A. J. Hall, N. Maine, M. Mendy, and H. C. Whittle, ‘What level of hepatitis B antibody is protective?’, J Infect Dis, vol. 179, no. 2, pp. 489–492, 1999. [CrossRef]
- J. Poorolajal, M. Mahmoodi, R. Majdzadeh, S. Nasseri-Moghaddam, A. Haghdoost, and A. Fotouhi, ‘Long-term protection provided by hepatitis B vaccine and need for booster dose: A meta-analysis’, vol. 28, no. 3, pp. 623–631. [CrossRef]
- ‘Hepatitis B vaccines: WHO position paper – July 2017′. Accessed: Jan. 19, 2024. [Online]. Available: https://www.who.int/publications/i/item/WER9227.
- W. Jilg, M. Schmidt, and F. Deinhardt, ‘Persistence of specific antibodies after hepatitis B vaccination’, J Hepatol, vol. 6, no. 2, pp. 201–207, 1988. [CrossRef]
- W. Jilg, M. Schmidt, F. Deinhardt, and R. Zachoval, ‘Hepatitis B vaccination: how long does protection last?’, Lancet, vol. 2, no. 8400, p. 458, Aug. 1984. [CrossRef]
- T. Bauer and W. Jilg, ‘Hepatitis B surface antigen-specific T and B cell memory in individuals who had lost protective antibodies after hepatitis B vaccination’, vol. 24, no. 5, pp. 572–577. [CrossRef]
- N. Gara et al., ‘Durability of antibody response against hepatitis B virus in healthcare workers vaccinated as adults’, vol. 60, no. 4, pp. 505–513. [CrossRef]
- L. C. Meireles, R. T. Marinho, and P. Van Damme, ‘Three decades of hepatitis B control with vaccination’, World J Hepatol, vol. 7, no. 18, pp. 2127–2132, 2015. [CrossRef]
- D. J. West and G. B. Calandra, ‘Vaccine induced immunologic memory for hepatitis B surface antigen: Implications for policy on booster vaccination’, Vaccine, vol. 14, no. 11, pp. 1019–1027, 1996. [CrossRef]
- L. I. M. Huang, B. L. Chiang, C. Y. Lee, P. I. Lee, W. K. Chi, and M. H. Chang, ‘Long-term response to hepatitis B vaccination and response to booster in children born to mothers with hepatitis B e antigen’, Hepatology, vol. 29, no. 3, pp. 954–959, 1999. [CrossRef]
- B. J. McMahon et al., ‘Antibody levels and protection after hepatitis B vaccination: results of a 15-year follow-up’, Ann Intern Med, vol. 142, no. 5, pp. 333–341, Mar. 2005. [CrossRef]
- S. Plotkin, E. Leuridan, and P. Van Damme, ‘Hepatitis B and the need for a booster dose’, Clin Infect Dis, vol. 53, no. 1, pp. 68–75, Jul. 2011. [CrossRef]
- D. J. West and G. B. Calandra, ‘Vaccine induced immunologic memory for hepatitis B surface antigen: Implications for policy on booster vaccination’, Vaccine, vol. 14, no. 11, pp. 1019–1027, 1996. [CrossRef]
- J. E. Banatvala and P. Van Damme, ‘Hepatitis B vaccine -- do we need boosters?’, J Viral Hepat, vol. 10, no. 1, pp. 1–6, Jan. 2003. [CrossRef]
- A. J. Hall, ‘Boosters for hepatitis B vaccination? Need for an evidence-based policy’, Hepatology, vol. 51, no. 5, pp. 1485–1486, May 2010. [CrossRef]
- J. C. Ma et al., ‘Long-term protection at 20-31 years after primary vaccination with plasma-derived hepatitis B vaccine in a Chinese rural community’, Hum Vaccin Immunother, vol. 16, no. 1, pp. 16–20, Jan. 2020. [CrossRef]
- C. F. Jan et al., ‘Determination of immune memory to hepatitis B vaccination through early booster response in college students’, Hepatology, vol. 51, no. 5, pp. 1547–1554, May 2010. [CrossRef]
- T. Yoshida and I. Saito, ‘Hepatitis B booster vaccination for healthcare workers’, Lancet, vol. 355, no. 9213, p. 1464, Apr. 2000. [CrossRef]
- J. Banatvala, P. Van Damme, and J. Van Hattum, ‘Boosters for hepatitis B’, Lancet, vol. 356, no. 9226, pp. 337–338, 2000. [CrossRef]
- M. A. Purdy, ‘Hepatitis B virus S gene escape mutants’, Asian J Transfus Sci, vol. 1, no. 2, p. 62, 2007. [CrossRef]
- W. F. Carman et al., ‘Vaccine-induced escape mutant of hepatitis B virus’, Lancet, vol. 336, no. 8711, pp. 325–329, Aug. 1990. [CrossRef]
- H. Y. Hsu, M. H. Chang, Y. H. Ni, and H. L. Chen, ‘Survey of hepatitis B surface variant infection in children 15 years after a nationwide vaccination programme in Taiwan’, Gut, vol. 53, no. 10, pp. 1499–1503, Oct. 2004. [CrossRef]
- T. Kalinina, A. Iwanski, H. Will, and M. Sterneck, ‘Deficiency in Virion Secretion and Decreased Stability of the Hepatitis B Virus Immune Escape Mutant G145R’, Hepatology, vol. 38, no. 5, pp. 1274–1281, 2003. [CrossRef]
- .A. Mele et al., ‘Effectiveness of hepatitis B vaccination in babies born to hepatitis B surface antigen-positive mothers in Italy’, J Infect Dis, vol. 184, no. 7, pp. 905–908, Oct. 2001. [CrossRef]
- D. S. Chen, ‘Hepatitis B vaccination: The key towards elimination and eradication of hepatitis B’, J Hepatol, vol. 50, no. 4, pp. 805–816, Apr. 2009. [CrossRef]
- N. Ogata et al., ‘Licensed recombinant hepatitis B vaccines protect chimpanzees against infection with the prototype surface gene mutant of hepatitis B virus’, Hepatology, vol. 30, no. 3, pp. 779–786, 1999. [CrossRef]
- S. F. Wieland, ‘The Chimpanzee Model for Hepatitis B Virus Infection’, Cold Spring Harb Perspect Med, vol. 5, no. 6, pp. 1–19, Jun. 2015. [CrossRef]
- A. Kuo and R. Gish, ‘Chronic Hepatitis B Infection’, Clin Liver Dis, vol. 16, no. 2, pp. 347–369, May 2012. [CrossRef]
- T. Inoue and Y. Tanaka, ‘Cross-Protection of Hepatitis B Vaccination among Different Genotypes’, Vaccines 2020, Vol. 8, Page 456, vol. 8, no. 3, p. 456, Aug. 2020. [CrossRef]
- S. L. Stramer et al., ‘Nucleic Acid Testing to Detect HBV Infection in Blood Donors’, New England Journal of Medicine, vol. 364, no. 3, pp. 236–247, Jan. 2011. [CrossRef]
- T. Li, Y. Fu, J.-P. Allain, and C. Li, ‘Chronic and occult hepatitis B virus infections in the vaccinated Chinese population’, Ann Blood, vol. 2, no. 3, pp. 4–4, Apr. 2017. [CrossRef]
- H. L. Zhu, X. Li, J. Li, and Z. H. Zhang, ‘Genetic variation of occult hepatitis B virus infection’, World J Gastroenterol, vol. 22, no. 13, p. 3531, Apr. 2016. [CrossRef]
- S. C. Mu, Y. M. Lin, G. M. Jow, and B. F. Chen, ‘Occult hepatitis B virus infection in hepatitis B vaccinated children in Taiwan’, J Hepatol, vol. 50, no. 2, pp. 264–272, Feb. 2009. [CrossRef]
- Y. H. Ni et al., ‘Two Decades of Universal Hepatitis B Vaccination in Taiwan: Impact and Implication for Future Strategies’, Gastroenterology, vol. 132, no. 4, pp. 1287–1293, Apr. 2007. [CrossRef]
- S. Yang et al., ‘Factors influencing immunologic response to hepatitis B vaccine in adults’, vol. 6, p. 27251. [CrossRef]
- ‘Hepatitis B Foundation: Vaccine Non-Responders’. Accessed: Jan. 20, 2024. [Online]. Available: https://www.hepb.org/prevention-and-diagnosis/vaccination/vaccine-non-responders/.
- G. Corrao et al., ‘Immune response to anti-HBV vaccination: Study of conditioning factors’, vol. 4, no. 4, pp. 492–496. [CrossRef]
- D. N. Fisman, D. Agrawal, and K. Leder, ‘The Effect of Age on Immunologic Response to Recombinant Hepatitis B Vaccine: A Meta-analysis’, vol. 35, no. 11, pp. 1368–1375. [CrossRef]
- O. Launay, ‘Safety and Immunogenicity of 4 Intramuscular Double Doses and 4 Intradermal Low Doses vs Standard Hepatitis B Vaccine Regimen in Adults With HIV-1′, vol. 305, no. 14, p. 1432. [CrossRef]
- Th. F. Senden, ‘Response to intradermal hepatitis B vaccination: differences between males and females?’, vol. 8, no. 6, pp. 612–613. [CrossRef]
- F. E. Shaw et al., ‘Effect of anatomic injection site, age and smoking on the immune response to hepatitis B vaccination’, vol. 7, no. 5, pp. 425–430. [CrossRef]
- E. M. Tedaldi et al., ‘Hepatitis A and B Vaccination Practices for Ambulatory Patients Infected with HIV’, vol. 38, no. 10, pp. 1478–1484. [CrossRef]
- H. Van Loveren et al., ‘Vaccine-induced antibody responses as parameters of the influence of endogenous and environmental factors’, vol. 109, no. 8, pp. 757–764. [CrossRef]
- WINTER, E. FOLLETT, J. MCINTYRE, J. STEWART, and I. SYMINGTON, ‘Influence of smoking on immunological responses to hepatitis B vaccine’, vol. 12, no. 9, pp. 771–772. [CrossRef]
- F. Denis et al., ‘Hepatitis-B vaccination in the elderly’, J Infect Dis, vol. 149, no. 6, p. 1019, 1984. [CrossRef]
- S. de Rave, R. A. Heijtink, M. Bakker-Bendik, J. Boot, and S. W. Schalm, ‘Immunogenicity of standard and low dose vaccination using yeast-derived recombinant hepatitis B surface antigen in elderly volunteers’, Vaccine, vol. 12, no. 6, pp. 532–534, 1994. [CrossRef]
- C. A. M. McNulty, J. K. Bowen, and A. J. Williams, ‘Hepatitis B vaccination in predialysis chronic renal failure patients a comparison of two vaccination schedules’, Vaccine, vol. 23, no. 32, pp. 4142–4147, Jul. 2005. [CrossRef]
- G. DaRoza et al., ‘Stage of Chronic Kidney Disease Predicts Seroconversion after Hepatitis B Immunization: Earlier is Better’, American Journal of Kidney Diseases, vol. 42, no. 6, pp. 1184–1192, 2003. [CrossRef]
- A. A. De Mattos, E. B. Gomes, C. V. Tovo, C. O. P. Alexandre, and J. O. D. R. Remião, ‘Hepatitis B vaccine efficacy in patients with chronic liver disease by hepatitis C virus’, Arq Gastroenterol, vol. 41, no. 3, pp. 180–184, 2004. [CrossRef]
- I. Gutierrez Domingo et al., ‘Response to vaccination against hepatitis B virus with a schedule of four 40-μg doses in cirrhotic patients evaluated for liver transplantation: factors associated with a response’, Transplant Proc, vol. 44, no. 6, pp. 1499–1501, Jul. 2012. [CrossRef]
- E. T. Overton, S. Sungkanuparph, W. G. Powderly, W. Seyfried, R. K. Groger, and J. A. Aberg, ‘Undetectable plasma HIV RNA load predicts success after hepatitis B vaccination in HIV-infected persons’, Clin Infect Dis, vol. 41, no. 7, pp. 1045–1048, Oct. 2005. [CrossRef]
- L. G. Rubin et al., ‘2013 IDSA clinical practice guideline for vaccination of the immunocompromised host’, Clinical Infectious Diseases, vol. 58, no. 3, pp. 309–318, Feb. 2014. [CrossRef]
- M. Cruciani et al., ‘Serologic response to hepatitis B vaccine with high dose and increasing number of injections in HIV infected adult patients’, Vaccine, vol. 27, no. 1, pp. 17–22, Jan. 2009. [CrossRef]
- F. Fabrizi, V. Dixit, P. Messa, and P. Martin, ‘Hepatitis B virus vaccine in chronic kidney disease: Improved immunogenicity by adjuvants? A meta-analysis of randomized trials’, vol. 30, no. 13, pp. 2295–2300. [CrossRef]
- S. Walayat, Z. Ahmed, D. Martin, S. Puli, M. Cashman, and S. Dhillon, ‘Recent advances in vaccination of non-responders to standard dose hepatitis B virus vaccine’, vol. 7, no. 24, pp. 2503–2509. [CrossRef]
- T. Vesikari et al., ‘Immunogenicity and Safety of a 3-Antigen Hepatitis B Vaccine vs a Single-Antigen Hepatitis B Vaccine: A Phase 3 Randomized Clinical Trial’, vol. 4, no. 10, pp. e2128652–e2128652. [CrossRef]
- Aggeletopoulou, P. Davoulou, C. Konstantakis, K. Thomopoulos, and C. Triantos, ‘Response to hepatitis B vaccination in patients with liver cirrhosis’, vol. 27, no. 6. [CrossRef]
- M. Filippelli et al., ‘Hepatitis B vaccine by intradermal route in non responder patients: An update’, World Journal of Gastroenterology : WJG, vol. 20, no. 30, p. 10383, Aug. 2014. [CrossRef]
- F. Mahmood et al., ‘HBV Vaccines: Advances and Development’, Vaccines (Basel), vol. 11, no. 12, Dec. 2023. [CrossRef]
- A. Prüss-Üstün, E. Rapiti, and Y. Hutin, ‘Estimation of the global burden of disease attributable to contaminated sharps injuries among health-care workers’, vol. 48, no. 6, pp. 482–490. [CrossRef]
- V. Batra, A. Goswami, S. Dadhich, D. Kothari, and N. Bhargava, ‘Hepatitis B immunization in healthcare workers’, Annals of Gastroenterology : Quarterly Publication of the Hellenic Society of Gastroenterology, vol. 28, no. 2, p. 276, 2015, Accessed: Dec. 16, 2023. [Online]. Available: /pmc/articles/PMC4367220/.
- H. S. Chahal, M. G. Peters, A. M. Harris, D. McCabe, P. Volberding, and J. G. Kahn, ‘Cost-effectiveness of Hepatitis B Virus Infection Screening and Treatment or Vaccination in 6 High-risk Populations in the United States’, Open Forum Infect Dis, vol. 6, no. 1, Jan. 2019. [CrossRef]
- A. M. Mokhtari, M. Barouni, M. Moghadami, J. Hassanzadeh, R. S. Dewey, and A. Mirahmadizadeh, ‘Evaluating the cost-effectiveness of universal hepatitis B virus vaccination in Iran: a Markov model analysis’, vol. 17, no. 6, pp. 1825–1833. [CrossRef]
- S. Q. Lu, S. M. McGhee, X. Xie, J. Cheng, and R. Fielding, ‘Economic evaluation of universal newborn hepatitis B vaccination in China’, vol. 31, no. 14, pp. 1864–1869. [CrossRef]
- G. Woo et al., ‘Health state utilities and quality of life in patients with hepatitis B’, vol. 26, no. 7, pp. 445–451. [CrossRef]
- M. R. Siddiqui, N. Gay, W. J. Edmunds, and M. Ramsay, ‘Economic evaluation of infant and adolescent hepatitis B vaccination in the UK’, vol. 29, no. 3, pp. 466–475. [CrossRef]
- S. Vijayalakshmi and A. Upadhyay, ‘Disease Prediction Using Machine Learning for Healthcare’, pp. 181–202. [CrossRef]
- M. K. Maini and L. J. Pallett, ‘Defective T-cell immunity in hepatitis B virus infection: why therapeutic vaccination needs a helping hand’, vol. 3, no. 3, pp. 192–202. [CrossRef]
- A. R. Burton et al., ‘Circulating and intrahepatic antiviral B cells are defective in hepatitis B’, vol. 128, no. 10, pp. 4588–4603. [CrossRef]
- J.-H. Horng et al., ‘HBV X protein-based therapeutic vaccine accelerates viral antigen clearance by mobilizing monocyte infiltration into the liver in HBV carrier mice’, vol. 27, no. 1, p. 70. [CrossRef]
- J. Zheng et al., ‘In Silico Analysis of Epitope-Based Vaccine Candidates against Hepatitis B Virus Polymerase Protein’, vol. 9, no. 5, p. 112. [CrossRef]
- M. J. Alter et al., ‘The Changing Epidemiology of Hepatitis B in the United States: Need for Alternative Vaccination Strategies’, JAMA, vol. 263, no. 9, pp. 1218–1222, Mar. 1990. [CrossRef]
- J. A. Arevalo and A. E. Washington, ‘Cost-effectiveness of Prenatal Screening and Immunization for Hepatitis B Virus’, JAMA, vol. 259, no. 3, pp. 365–369, Jan. 1988. [CrossRef]
- P. Van Damme, A. Meheus, and M. Kane, ‘Integration of hepatitis B vaccination into national immunisation programmes. Viral Hepatitis Prevention Board’, BMJ, vol. 314, no. 7086, p. 1033, Apr. 1997. [CrossRef]
- D. S. Chen et al., ‘A Mass Vaccination Program in Taiwan Against Hepatitis B Virus Infection in Infants of Hepatitis B Surface Antigen—Carrier Mothers’, JAMA, vol. 257, no. 19, pp. 2597–2603, May 1987. [CrossRef]
- T. A. Ruff et al., ‘Lombok Hepatitis B Model Immunization Project: toward universal infant hepatitis B immunization in Indonesia’, J Infect Dis, vol. 171, no. 2, pp. 290–296, 1995. [CrossRef]
- M. Fortuin et al., ‘Efficacy of hepatitis B vaccine in the Gambian expanded programme on immunisation’, The Lancet, vol. 341, no. 8853, pp. 1129–1132, May 1993. [CrossRef]
- S. K. Acharya, ‘Does the level of hepatitis B virus vaccination in health-care workers need improvement?’, J Gastroenterol Hepatol, vol. 23, no. 11, pp. 1628–31, Nov. 2008. [CrossRef]
- J. Crosnier et al., ‘RANDOMISED PLACEBO-CONTROLLED TRIAL OF HEPATITIS B SURFACE ANTIGEN VACCINE IN FRENCH HAEMODIALYSIS UNITS: II, HAEMODIALYSIS PATIENTS’, The Lancet, vol. 317, no. 8224, pp. 797–800, Apr. 1981. [CrossRef]
- W. Szmuness et al., ‘Hepatitis B Vaccine in Medical Staff of Hemodialysis Units: Efficacy and Subtype Cross-Protection’, New England Journal of Medicine, vol. 307, no. 24, pp. 1481–1486, Dec. 1982. [CrossRef]
- C. E. Stevens, H. J. Alter, P. E. Taylor, E. A. Zang, E. J. Harley, and W. Szmuness, ‘Hepatitis B Vaccine in Patients Receiving Hemodialysis: Immunogenicity and Efficacy’, New England Journal of Medicine, vol. 311, no. 8, pp. 496–501, Aug. 1984. [CrossRef]
- B. M. Ma, D. Y. H. Yap, T. P. S. Yip, I. F. N. Hung, S. C. W. Tang, and T. M. Chan, ‘Vaccination in patients with chronic kidney disease—Review of current recommendations and recent advances’, Nephrology, vol. 26, no. 1, pp. 5–11, Jan. 2021. [CrossRef]
- F. Fabrizi, R. Cerutti, V. Dixit, and E. Ridruejo, ‘Hepatitis B virus vaccine and chronic kidney disease. The advances’, Nefrologia, vol. 41, no. 2, pp. 115–122, Mar. 2021. [CrossRef]
- G. M. Faser et al., ‘Increasing serum creatinine and age reduce the response to hepatitis B vaccine in renal failure patients’, J Hepatol, vol. 21, no. 3, pp. 450–454, 1994. [CrossRef]
- A. E. Grzegorzewska, ‘Hepatitis B Vaccination in Chronic Kidney Disease: Review of Evidence in Non-Dialyzed Patients’, Hepat Mon, vol. 12, no. 11, p. 7359, Nov. 2012. [CrossRef]
- G. DaRoza et al., ‘Stage of Chronic Kidney Disease Predicts Seroconversion after Hepatitis B Immunization: Earlier is Better’, American Journal of Kidney Diseases, vol. 42, no. 6, pp. 1184–1192, Dec. 2003. [CrossRef]
- K. Y. Ong, H. Y. Wong, and G. Y. Khee, ‘What is the hepatitis B vaccination regimen in chronic kidney disease?’, Cleve Clin J Med, vol. 85, no. 1, pp. 32–34, Jan. 2018. [CrossRef]
- S. Udomkarnjananun et al., ‘Hepatitis B virus vaccine immune response and mortality in dialysis patients: a meta-analysis’, J Nephrol, vol. 33, no. 2, pp. 343–354, Apr. 2020. [CrossRef]
- V. Kovacic, M. Sain, and V. Vukman, ‘Efficient haemodialysis improves the response to hepatitis B virus vaccination’, Intervirology, vol. 45, no. 3, pp. 172–176, Jan. 2002. [CrossRef]
- A. Asan et al., ‘Factors affecting responsiveness to hepatitis B immunization in dialysis patients’, Int Urol Nephrol, vol. 49, no. 10, pp. 1845–1850, Oct. 2017. [CrossRef]
- M. A. Ayub, M. R. Bacci, F. L. A. Fonseca, and E. Z. Chehter, ‘Hemodialysis and hepatitis B vaccination: a challenge to physicians’, Int J Gen Med, vol. 7, pp. 109–114, Feb. 2014. [CrossRef]
- E. Benhamou et al., ‘Hepatitis B vaccine: Randomized trial of immunogenicity in hemodialysis patients’, Clin Nephrol, vol. 21, no. 3, pp. 143–147, Jan. 1984.
- K. Bel’eed, M. Wright, D. Eadington, M. Farr, and L. Sellars, ‘Vaccination against hepatitis B infection in patients with end stage renal disease’, Postgrad Med J, vol. 78, no. 923, pp. 538–540, Sep. 2002. [CrossRef]
- M. H. Somi and B. Hajipour, ‘Improving Hepatitis B Vaccine Efficacy in End-Stage Renal Diseases Patients and Role of Adjuvants’, ISRN Gastroenterol, vol. 2012, pp. 1–9, Sep. 2012. [CrossRef]
- P. Friedrich, A. Sattler, K. Müller, M. Nienen, P. Reinke, and N. Babel, ‘Comparing Humoral and Cellular Immune Response Against HBV Vaccine in Kidney Transplant Patients’, American Journal of Transplantation, vol. 15, no. 12, pp. 3157–3165, Dec. 2015. [CrossRef]
- B. M. Ma, D. Y. H. Yap, T. P. S. Yip, I. F. N. Hung, S. C. W. Tang, and T. M. Chan, ‘Vaccination in patients with chronic kidney disease—Review of current recommendations and recent advances’, Nephrology, vol. 26, no. 1, pp. 5–11, Jan. 2021. [CrossRef]
- S. Marinaki, K. Kolovou, S. Sakellariou, J. N. Boletis, and I. K. Delladetsima, ‘Hepatitis B in renal transplant patients’, World J Hepatol, vol. 9, no. 25, p. 1054, Sep. 2017. [CrossRef]
- T. Eleftheriadis, G. Pissas, G. Antoniadi, V. Liakopoulos, and I. Stefanidis, ‘Factors affecting effectiveness of vaccination against hepatitis B virus in hemodialysis patients’, World Journal of Gastroenterology : WJG, vol. 20, no. 34, p. 12018, Sep. 2014. [CrossRef]
- A. F. Lefebure, G. A. Verpooten, M. M. Couttenye, and M. E. De Broe, ‘Immunogenicity of a recombinant DNA hepatitis B vaccine in renal transplant patients’, Vaccine, vol. 11, no. 4, pp. 397–399, Jan. 1993. [CrossRef]
- F. Fabrizi, P. Martin, V. Dixit, S. Bunnapradist, and G. Dulai, ‘Meta-analysis: The effect of age on immunological response to hepatitis B vaccine in end-stage renal disease’, Aliment Pharmacol Ther, vol. 20, no. 10, pp. 1053–1062, Nov. 2004. [CrossRef]
- C. Goilav and P. Piot, ‘Vaccination against hepatitis B in homosexual men: A review’, Am J Med, vol. 87, no. 3, pp. S21–S25, Sep. 1989. [CrossRef]
- W. Szmuness et al., ‘Hepatitis B Vaccine: Demonstration of Efficacy in a Controlled Clinical Trial in a High-Risk Population in the United States’, New England Journal of Medicine, vol. 303, no. 15, pp. 833–841, Oct. 1980. [CrossRef]
- N. Odaka et al., ‘Comparative Immunogenicity of Plasma and Recombinant Hepatitis B Virus Vaccines in Homosexual Men’, JAMA: The Journal of the American Medical Association, vol. 260, no. 24, pp. 3635–3637, Dec. 1988. [CrossRef]
- D. P. Francis et al., ‘The prevention of hepatitis B with vaccine. Report of the centers for disease control multi-center efficacy trial among homosexual men’, Ann Intern Med, vol. 97, no. 3, pp. 362–366, Jan. 1982. [CrossRef]
- D. P. Francis et al., ‘The prevention of hepatitis B with vaccine. Report of the centers for disease control multi-center efficacy trial among homosexual men’, Ann Intern Med, vol. 97, no. 3, pp. 362–366, Jan. 1982. [CrossRef]
- R. Vet, J. B. F. de Wit, and E. Das, ‘Factors associated with hepatitis B vaccination among men who have sex with men: a systematic review of published research’. vol. 28, no. 6, pp. 534–542, Oct. 2015. [CrossRef]
- H. Haban et al., ‘Assessment of the HBV vaccine response in a group of HIV-infected children in Morocco’, BMC Public Health, vol. 17, no. 1, pp. 1–6, Sep. 2017. [CrossRef]
- F. X. Catherine and L. Piroth, ‘Hepatitis B virus vaccination in HIV-infected people: A review’, Hum Vaccin Immunother, vol. 13, no. 6, p. 1304, Jun. 2017. [CrossRef]
- F. Pippi et al., ‘Serological response to hepatitis B virus vaccine in HIV-infected children in Tanzania’, HIV Med, vol. 9, no. 7, pp. 519–525, Jan. 2008. [CrossRef]
- G. Zuin et al., ‘Impaired response to hepatitis B vaccine in HIV infected children’, Vaccine, vol. 10, no. 12, pp. 857–860, Jan. 1992. [CrossRef]
- J. C. Laurence, ‘Hepatitis A and B immunizations of individuals infected with human immunodeficiency virus’, Am J Med, vol. 118, no. 10, pp. 75–83, Oct. 2005. [CrossRef]
- L. Paitoonpong and C. Suankratay, ‘Immunological response to hepatitis B vaccination in patients with AIDS and virological response to highly active antiretroviral therapy’, Scand J Infect Dis, vol. 40, no. 1, pp. 54–58, Jan. 2008. [CrossRef]
- A. F. Rech-Medeiros, P. dos S. Marcon, C. do V. Tovo, and A. A. de Mattos, ‘Evaluation of response to hepatitis B virus vaccine in adults with human immunodeficiency virus’, Ann Hepatol, vol. 18, no. 5, pp. 725–729, Sep. 2019. [CrossRef]
- A. M. Mohareb and A. Y. Kim, ‘Hepatitis B Vaccination in People Living With HIV—If at First You Don’t Succeed, Try Again’, JAMA Netw Open, vol. 4, no. 8, pp. e2121281–e2121281, Aug. 2021. [CrossRef]
- Y. Kim, J. Loucks, and M. Shah, ‘Efficacy of Hepatitis B Vaccine in Adults with Chronic Liver Disease’. vol. 36, no. 4, pp. 839–844, Feb. 2022. [CrossRef]
- D. A. Roni, R. M. Pathapati, A. S. Kumar, L. Nihal, K. Sridhar, and S. Tumkur Rajashekar, ‘Safety and efficacy of hepatitis B vaccination in cirrhosis of liver’, Adv Virol, vol. 2013, 2013. [CrossRef]
- G. Reiss and E. B. Keeffe, ‘Hepatitis vaccination in patients with chronic liver disease’, Aliment Pharmacol Ther, vol. 19, no. 7, pp. 715–727, Apr. 2004. [CrossRef]
- D. Horta et al., ‘Efficacy of Hepatitis B Virus Vaccines HBVaxpro40© and Fendrix© in Patients with Chronic Liver Disease in Clinical Practice’, Vaccines 2022, Vol. 10, Page 1323, vol. 10, no. 8, p. 1323, Aug. 2022. [CrossRef]
- A. A. Hassnine et al., ‘Clinical study on the efficacy of hepatitis B vaccination in hepatitis C virus related chronic liver diseases in Egypt’, Virus Res, vol. 323, p. 198953, Jan. 2023. [CrossRef]
- C. Mendenhall et al., ‘Hepatitis B vaccination - Response of alcoholic with and without liver injury’, Dig Dis Sci, vol. 33, no. 3, pp. 263–269, Mar. 1988. [CrossRef]
- F. Degos et al., ‘Hepatitis B vaccination in chronic alcoholics’, J Hepatol, vol. 2, no. 3, pp. 402–409, Jan. 1986. [CrossRef]
- G. Reiss and E. B. Keeffe, ‘Hepatitis vaccination in patients with chronic liver disease’, Aliment Pharmacol Ther, vol. 19, no. 7, pp. 715–727, Apr. 2004. [CrossRef]
- I. Fernández, J. M. Pascasio, and J. Colmenero, ‘Prophylaxis and treatment in liver transplantation. VII Consensus Document of the Spanish Society of Liver Transplantation’, Gastroenterología y Hepatología (English Edition), vol. 43, no. 3, pp. 169–177, Mar. 2020. [CrossRef]
- A. Takaki, T. Yasunaka, and T. Yagi, ‘Molecular Mechanisms to Control Post-Transplantation Hepatitis B Recurrence’, International Journal of Molecular Sciences 2015, Vol. 16, Pages 17494-17513, vol. 16, no. 8, pp. 17494–17513, Jul. 2015. [CrossRef]
- M. Nasir and G. Y. Wu, ‘Prevention of HBV Recurrence after Liver Transplant: A Review’, J Clin Transl Hepatol, vol. 8, no. 2, p. 150, Jun. 2020. [CrossRef]
- M. Jiménez-Pérez, R. González-Grande, J. Mostazo Torres, C. González Arjona, and F. J. Rando-Muñoz, ‘Management of hepatitis B virus infection after liver transplantation’, World J Gastroenterol, vol. 21, no. 42, p. 12083, Nov. 2015. [CrossRef]
- M. Ishigami et al., ‘Frequent incidence of escape mutants after successful hepatitis B vaccine response and stopping of nucleos(t)ide analogues in liver transplant recipients’, Liver Transplantation, vol. 20, no. 10, pp. 1211–1220, Oct. 2014. [CrossRef]
- H. S. Jo, J. F. Khan, J. H. Han, Y. D. Yu, and D. S. Kim, ‘Efficacy and Safety of Hepatitis B Virus Vaccination Following Hepatitis B Immunoglobulin Withdrawal After Liver Transplantation’, Transplant Proc, vol. 53, no. 10, pp. 3016–3021, Dec. 2021. [CrossRef]
- I. C. Rodrigues, R. C. M. A. De Da Silva, H. C. C. De Felício, and R. F. Da Silva, ‘NEW IMMUNIZATION SCHEDULE EFFECTIVENESS AGAINST HEPATITIS B IN LIVER TRANSPLANTATION PATIENTS’, Arq Gastroenterol, vol. 56, no. 4, pp. 440–446, Nov. 2019. [CrossRef]
- S. Saab, P. yu Chen, C. E. Saab, and M. J. Tong, ‘The Management of Hepatitis B in Liver Transplant Recipients’, Clin Liver Dis, vol. 20, no. 4, pp. 721–736, Nov. 2016. [CrossRef]
- ‘Global hepatitis report, 2017′. Accessed: Jan. 17, 2024. [Online]. Available: https://www.who.int/publications/i/item/9789241565455.
- D. Razavi-Shearer and H. Razavi, ‘Global prevalence of hepatitis B virus infection and prevention of mother-to-child transmission – Authors’ reply’, vol. 3, no. 9, p. 599. [CrossRef]
- S. Shan and J. Jia, ‘Prevention of Mother-to-Child Transmission of Hepatitis B Virus in the Western Pacific Region’, Clin Liver Dis (Hoboken), vol. 18, no. 1, p. 18, Jul. 2021. [CrossRef]
- M. -H Chang, D. -S Chen, H. -C Hsu, H. -Y Hsu, and C. -Y Lee, ‘Maternal transmission of hepatitis B virus in childhood hepatocellular carcinoma’, Cancer, vol. 64, no. 11, pp. 2377–2380, Dec. 1989. [CrossRef]
- C. E. Stevens et al., ‘Eradicating hepatitis B virus: The critical role of preventing perinatal transmission’, Biologicals, vol. 50, pp. 3–19, Nov. 2017. [CrossRef]
- A. Assateerawatt, V. S. Tanphaichitr, V. Suvatte, and S. Yodthong, ‘Immunogenicity and efficacy of a recombinant DNA hepatitis B vaccine, GenHevac B Pasteur in high risk neonates, school children and healthy adults’, Asian Pac J Allergy Immunol, vol. 11, no. 1, pp. 85–91, Jan. 1993.
- Y. Poovorawan, S. Sanpavat, W. Pongpunlert, S. Chumdermpadetsuk, P. Sentrakul, and A. Safary, ‘Protective Efficacy of a Recombinant DNA Hepatitis B Vaccine in Neonates of HBe Antigen—Positive Mothers’, JAMA, vol. 261, no. 22, pp. 3278–3281, Jun. 1989. [CrossRef]
- A. Milne, D. J. West, D. Van Chinh, C. D. Moyes, and G. Poerschke, ‘Field evaluation of the efficacy and immunogenicity of recombinant hepatitis B vaccine without HBIG in newborn Vietnamese infants’, J Med Virol, vol. 67, no. 3, pp. 327–333, Jan. 2002. [CrossRef]
- C. X. T. Tan et al., ‘Serologic Responses after Hepatitis B Vaccination in Preterm Infants Born to Hepatitis B Surface Antigen-Positive Mothers: Singapore Experience’, Pediatric Infectious Disease Journal, vol. 36, no. 8, pp. e208–e210, Aug. 2017. [CrossRef]
- W. Zhang et al., ‘Efficacy of the hepatitis B vaccine alone in the prevention of hepatitis B perinatal transmission in infants born to hepatitis B e antigen-negative carrier mothers’, J Virus Erad, vol. 8, no. 2, p. 100076, Jun. 2022. [CrossRef]
- A. Assateerawatt, V. S. Tanphaichitr, V. Suvatte, and S. Yodthong, ‘Immunogenicity and efficacy of a recombinant DNA hepatitis B vaccine, GenHevac B Pasteur in high risk neonates, school children and healthy adults’, Asian Pac J Allergy Immunol, vol. 11, no. 1, pp. 85–91, Jan. 1993.
- Y. Poovorawan et al., ‘Impact of hepatitis B immunisation as part of the EPI’, Vaccine, vol. 19, no. 7–8, pp. 943–949, Nov. 2000. [CrossRef]
- C. E. Stevens, P. T. Toy, P. E. Taylor, T. Lee, and H. Y. Yip, ‘Prospects for Control of Hepatitis B Virus Infection: Implications of Childhood Vaccination and Long-term Protection’, Pediatrics, vol. 90, no. 1, pp. 170–173, Jul. 1992. [CrossRef]
- H. M. Hsu et al., ‘Efficacy of a Mass Hepatitis B Vaccination Program in Taiwan: Studies on 3464 Infants of Hepatitis B Surface Antigen—Carrier Mothers’, JAMA, vol. 260, no. 15, pp. 2231–2235, Oct. 1988. [CrossRef]
- R. D. Burk, L. Y. Hwang, G. Y. F. Ho, D. A. Shafritz, and R. P. Beasley, ‘Outcome of perinatal hepatitis b virus exposure is dependent on maternal virus load’, Journal of Infectious Diseases, vol. 170, no. 6, pp. 1418–1423, Dec. 1994. [CrossRef]
- M. Belopolskaya, V. Avrutin, S. Firsov, and A. Yakovlev, ‘HBsAg level and hepatitis B viral load correlation with focus on pregnancy’, Annals of Gastroenterology : Quarterly Publication of the Hellenic Society of Gastroenterology, vol. 28, no. 3, p. 379, 2015, Accessed: Jan. 11, 2024. [Online]. Available: /pmc/articles/PMC4480176/.
- W. H. Wen et al., ‘Quantitative maternal hepatitis B surface antigen predicts maternally transmitted hepatitis B virus infection’, Hepatology, vol. 64, no. 5, pp. 1451–1461, Nov. 2016. [CrossRef]
- K. X. Sun et al., ‘A predictive value of quantitative HBsAg for serum HBV DNA level among HBeAg-positive pregnant women’, Vaccine, vol. 30, no. 36, pp. 5335–5340, Aug. 2012. [CrossRef]
- P. Lampertico et al., ‘EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection’, J Hepatol, vol. 67, no. 2, pp. 370–398, Aug. 2017. [CrossRef]
- C. Q. Pan et al., ‘Tenofovir to Prevent Hepatitis B Transmission in Mothers with High Viral Load’, N Engl J Med, vol. 374, no. 24, pp. 2324–2334, Jun. 2016. [CrossRef]
- M. J. Alter et al., ‘The Changing Epidemiology of Hepatitis B in the United States: Need for Alternative Vaccination Strategies’, JAMA, vol. 263, no. 9, pp. 1218–1222, Mar. 1990. [CrossRef]
- P. Van Damme, A. Meheus, and M. Kane, ‘Integration of hepatitis B vaccination into national immunisation programmes’, BMJ, vol. 314, no. 7086, p. 1033, Apr. 1997. [CrossRef]
- ‘Hepatitis B is preventable with safe and effective vaccines’. Accessed: Jan. 12, 2024. [Online]. Available: https://www.who.int/southeastasia/activities/hepatitis-b-is-preventable-with-safe-and-effective-vaccines.
- M. H. Chang and D. S. Chen, ‘Prevention of Hepatitis B’, Cold Spring Harb Perspect Med, vol. 5, no. 3, 2015. [CrossRef]
- ‘Immunization coverage’. Accessed: Jan. 16, 2024. [Online]. Available: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage.
- Z. Liu et al., ‘Impact of the national hepatitis B immunization program in China: a modeling study’, Infect Dis Poverty, vol. 11, no. 1, pp. 1–10, Dec. 2022. [CrossRef]
- S. Wait and D. S. Chen, ‘Towards the eradication of hepatitis B in Taiwan’, Kaohsiung J Med Sci, vol. 28, no. 1, pp. 1–9, Jan. 2012. [CrossRef]
- C. J. Chiang, Y. W. Yang, S. L. You, M. S. Lai, and C. J. Chen, ‘Thirty-Year Outcomes of the National Hepatitis B Immunization Program in Taiwan’, JAMA, vol. 310, no. 9, pp. 974–976, Sep. 2013. [CrossRef]
- Y. H. Ni, M. H. Chang, J. F. Wu, H. Y. Hsu, H. L. Chen, and D. S. Chen, ‘Minimization of hepatitis B infection by a 25-year universal vaccination program’, J Hepatol, vol. 57, no. 4, pp. 730–735, Oct. 2012. [CrossRef]
- H. M. Hsu, C. F. Lu, S. C. Lee, S. R. Lin, and D. S. Chen, ‘Seroepidemiologic survey for hepatitis B virus infection in Taiwan: The effect of hepatitis B mass immunization’, Journal of Infectious Diseases, vol. 179, no. 2, pp. 367–370, Jan. 1999. [CrossRef]
- H. M. Hsu, C. F. Lu, S. C. Lee, S. R. Lin, and D. S. Chen, ‘Seroepidemiologic survey for hepatitis B virus infection in Taiwan: The effect of hepatitis B mass immunization’, Journal of Infectious Diseases, vol. 179, no. 2, pp. 367–370, Jan. 1999. [CrossRef]
- M. Moghadami, N. Dadashpour, A. M. Mokhtari, M. Ebrahimi, and A. Mirahmadizadeh, ‘The effectiveness of the national hepatitis B vaccination program 25 years after its introduction in Iran: a historical cohort study’, Braz J Infect Dis, vol. 23, no. 6, pp. 419–426, Nov. 2019. [CrossRef]
- L. Childs, S. Roesel, and R. A. Tohme, ‘Status and progress of hepatitis B control through vaccination in the South-East Asia Region, 1992–2015′, Vaccine, vol. 36, no. 1, p. 6, Jan. 2018. [CrossRef]
- M. H. Chang, ‘Hepatitis B virus infection’, Semin Fetal Neonatal Med, vol. 12, no. 3, pp. 160–167, Jun. 2007. [CrossRef]
- S. Lolekha, B. Warachit, A. Hirunyachote, P. Bowonkiratikachorn, D. J. West, and G. Poerschke, ‘Protective efficacy of hepatitis B vaccine without HBIG in infants of HBeAg-positive carrier mothers in Thailand’, Vaccine, vol. 20, no. 31, pp. 3739–3743, Nov. 2002. [CrossRef]
- C. X. T. Tan et al., ‘Serologic Responses after Hepatitis B Vaccination in Preterm Infants Born to Hepatitis B Surface Antigen-Positive Mothers: Singapore Experience’, Pediatric Infectious Disease Journal, vol. 36, no. 8, pp. e208–e210, Aug. 2017. [CrossRef]
- N. P. Nelson, P. J. Easterbrook, and B. J. McMahon, ‘Epidemiology of Hepatitis B Virus Infection and Impact of Vaccination on Disease’, Clin Liver Dis, vol. 20, no. 4, p. 607, Nov. 2016. [CrossRef]
- ‘Pinkbook: Hepatitis B | CDC’. Accessed: Jan. 13, 2024. [Online]. Available: https://www.cdc.gov/vaccines/pubs/pinkbook/hepb.html.
- J. H. Kao, H. M. Hsu, W. Y. Shau, M. H. Chang, and D. S. Chen, ‘Universal hepatitis B vaccination and the decreased mortality from fulminant hepatitis in infants in Taiwan’, J Pediatr, vol. 139, no. 3, pp. 349–352, Sep. 2001. [CrossRef]
- H. L. Chen et al., ‘Pediatric fulminant hepatic failure in endemic areas of hepatitis B infection: 15 years after universal hepatitis B vaccination’, Hepatology, vol. 39, no. 1, pp. 58–63, Jan. 2004. [CrossRef]
- A. Mele et al., ‘Acute hepatitis B 14 years after the implementation of universal vaccination in Italy: Areas of improvement and emerging challenges’, Clinical Infectious Diseases, vol. 46, no. 6, pp. 868–875, Mar. 2008. [CrossRef]
- A. Mele et al., ‘Acute hepatitis delta virus infection in Italy: incidence and risk factors after the introduction of the universal anti-hepatitis B vaccination campaign.’, Clin Infect Dis, vol. 44, no. 3, pp. e17–e24, Feb. 2007. [CrossRef]
- K. T. Goh, ‘Prevention and control of hepatitis B virus infection in Singapore.’, Ann Acad Med Singap, vol. 26, no. 5, pp. 671–681, Sep. 1997, Accessed: Jan. 14, 2024. [Online]. Available: https://europepmc.org/article/med/9494677.
- R. Bhimma, H. M. Coovadia, M. Adhikari, and C. A. Connolly, ‘The impact of the hepatitis B virus vaccine on the incidence of hepatitis B virus-associated membranous nephropathy’, Arch Pediatr Adolesc Med, vol. 157, no. 10, pp. 1025–1030, Oct. 2003. [CrossRef]
- H. Xu, L. Sun, L. J. Zhou, L. J. Fang, F. Y. Sheng, and Y. Q. Guo, ‘The effect of hepatitis B vaccination on the incidence of childhood HBV-associated nephritis’, Pediatric Nephrology, vol. 18, no. 12, pp. 1216–1219, Dec. 2003. [CrossRef]
- M. T. Liao, M. H. Chang, F. G. Lin, I. J. Tsai, Y. W. Chang, and Y. K. Tsau, ‘Universal Hepatitis B Vaccination Reduces Childhood Hepatitis B Virus–Associated Membranous Nephropathy’, Pediatrics, vol. 128, no. 3, pp. e600–e604, Sep. 2011. [CrossRef]
- M. -H Chang, D. -S Chen, H. -C Hsu, H. -Y Hsu, and C. -Y Lee, ‘Maternal transmission of hepatitis B virus in childhood hepatocellular carcinoma’, Cancer, vol. 64, no. 11, pp. 2377–2380, Dec. 1989. [CrossRef]
- M.-H. Chang et al., ‘Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. Taiwan Childhood Hepatoma Study Group’, N Engl J Med, vol. 336, no. 26, pp. 1855–1859, Jun. 1997. [CrossRef]
- S. Yu et al., ‘Accelerating Decreases in the Incidences of Hepatocellular Carcinoma at a Younger Age in Shanghai Are Associated With Hepatitis B Virus Vaccination’, Front Oncol, vol. 12, p. 855945, Apr. 2022. [CrossRef]
- J. E. Flores, A. J. Thompson, M. Ryan, and J. Howell, ‘The Global Impact of Hepatitis B Vaccination on Hepatocellular Carcinoma’, Vaccines (Basel), vol. 10, no. 5, May 2022. [CrossRef]
- T. A. Madani, ‘Trend in incidence of hepatitis B virus infection during a decade of universal childhood hepatitis B vaccination in Saudi Arabia’, Trans R Soc Trop Med Hyg, vol. 101, no. 3, pp. 278–283, Mar. 2007. [CrossRef]
- R. cheng Li et al., ‘Efficacy of hepatitis B vaccination on hepatitis B prevention and on hepatocellular carcinoma’, Zhonghua Liu Xing Bing Xue Za Zhi, vol. 25, no. 5, pp. 385–387, May 2004.
- M. S. Lee et al., ‘Hepatitis B vaccination and reduced risk of primary liver cancer among male adults: A cohort study in Korea’, Int J Epidemiol, vol. 27, no. 2, pp. 316–319, Apr. 1998. [CrossRef]
- L. C. Meireles, R. T. Marinho, and P. Van Damme, ‘Three decades of hepatitis B control with vaccination’, World J Hepatol, vol. 7, no. 18, p. 2127, Aug. 2015. [CrossRef]
- B. S. Sheena et al., ‘Global, regional, and national burden of hepatitis B, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019′, Lancet Gastroenterol Hepatol, vol. 7, no. 9, pp. 796–829, Sep. 2022. [CrossRef]
- A. Schweitzer, M. K. Akmatov, and G. Krause, ‘Hepatitis B vaccination timing: results from demographic health surveys in 47 countries’, Bull World Health Organ, vol. 95, no. 3, p. 199, Mar. 2017. [CrossRef]
- ‘Vaccine Introduction and Coverage in Gavi-Supported Countries 2015-2018: Implications for Gavi 5.0 | Center For Global Development’. Accessed: Jan. 25, 2024. [Online]. Available: https://www.cgdev.org/publication/vaccine-introduction-and-coverage-gavi-supported-countries-2015-2018-implications-gavi.
- J. BIGHAM, ‘Implementing and Understanding Barriers to the Updated Hepatitis B Vaccination Recommendations and Guidance’, Fam Pract Manag, vol. 30, no. 5, pp. 29–32, Sep. 2023, Accessed: Jan. 30, 2024. [Online]. Available: http://localhost:4503/content/brand/aafp/pubs/fpm/issues/2023/0900/hepatitis-b-vaccination-barriers.html.
- P. B. Machmud, A. Führer, C. Gottschick, and R. Mikolajczyk, ‘Barriers to and Facilitators of Hepatitis B Vaccination among the Adult Population in Indonesia: A Mixed Methods Study’, Vaccines (Basel), vol. 11, no. 2, p. 398, Feb. 2023. [CrossRef]
- C. Freeland et al., ‘Barriers and facilitators to hepatitis B birth dose vaccination: Perspectives from healthcare providers and pregnant women accessing antenatal care in Nigeria’, PLOS Global Public Health, vol. 3, no. 6, p. e0001332, Jun. 2023. [CrossRef]
- P. Mohanty, P. Jena, and L. Patnaik, ‘Vaccination against Hepatitis B: A Scoping Review’, Asian Pac J Cancer Prev, vol. 21, no. 12, pp. 3453–3459, Dec. 2020. [CrossRef]
- A. S. Ali, N. A. Hussein, E. O. H. Elmi, A. M. Ismail, and M. M. Abdi, ‘Hepatitis B vaccination coverage and associated factors among medical students: a cross-sectional study in Bosaso, Somalia, 2021′, BMC Public Health, vol. 23, no. 1, pp. 1–8, Dec. 2023. [CrossRef]
- S. Smith et al., ‘Global progress on the elimination of viral hepatitis as a major public health threat: An analysis of WHO Member State responses 2017′, JHEP Rep, vol. 1, no. 2, pp. 81–89, Aug. 2019. [CrossRef]
- A. Vogel, T. Meyer, G. Sapisochin, R. Salem, and A. Saborowski, ‘Hepatocellular carcinoma’, The Lancet, vol. 400, no. 10360, pp. 1345–1362, Oct. 2022. [CrossRef]
- ‘Hepatitis B’. Accessed: Jan. 16, 2024. [Online]. Available: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b.
- ‘The Global Hepatitis Health Sector Strategy – Global Targets’, 2017, Accessed: Jan. 29, 2024. [Online]. Available: https://www.ncbi.nlm.nih.gov/books/NBK442270/.
- D. L. Thomas, ‘Global Elimination of Chronic Hepatitis’, N Engl J Med, vol. 380, no. 21, pp. 2041–2050, May 2019. [CrossRef]
- G. S. Cooke et al., ‘Accelerating the elimination of viral hepatitis: a Lancet Gastroenterology & Hepatology Commission’, Lancet Gastroenterol Hepatol, vol. 4, no. 2, pp. 135–184, Feb. 2019. [CrossRef]
- J. Liu, W. Liang, W. Jing, and M. Liu, ‘Countdown to 2030: eliminating hepatitis B disease, China’, Bull World Health Organ, vol. 97, no. 3, pp. 230–238, Mar. 2019. [CrossRef]
- D. Razavi-Shearer et al., ‘Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study’, Lancet Gastroenterol Hepatol, vol. 3, no. 6, pp. 383–403, Jun. 2018. [CrossRef]
- S. Nayagam, Y. Shimakawa, and M. Lemoine, ‘Mother-to-child transmission of hepatitis B: What more needs to be done to eliminate it around the world?’, J Viral Hepat, vol. 27, no. 4, pp. 342–349, Apr. 2020. [CrossRef]
- S. E. Schröeder et al., ‘Innovative strategies for the elimination of viral hepatitis at a national level: A country case series’, Liver Int, vol. 39, no. 10, pp. 1818–1836, Oct. 2019. [CrossRef]
- D. Tordrup et al., ‘Additional resource needs for viral hepatitis elimination through universal health coverage: projections in 67 low-income and middle-income countries, 2016-30′, Lancet Glob Health, vol. 7, no. 9, pp. e1180–e1188, Sep. 2019. [CrossRef]
- H. Razavi, Y. Sanchez Gonzalez, C. Yuen, and M. Cornberg, ‘Global timing of hepatitis C virus elimination in high-income countries’, Liver Int, vol. 40, no. 3, pp. 522–529, Mar. 2020. [CrossRef]
- A. Palayew, H. Razavi, S. J. Hutchinson, G. S. Cooke, and J. V. Lazarus, ‘Do the most heavily burdened countries have the right policies to eliminate viral hepatitis B and C?’, Lancet Gastroenterol Hepatol, vol. 5, no. 10, pp. 948–953, Oct. 2020. [CrossRef]
- L. A. Kondili et al., ‘Impact of the COVID-19 pandemic on hepatitis B and C elimination: An EASL survey’, JHEP Reports, vol. 4, no. 9, p. 100531, Sep. 2022. [CrossRef]
- S. Blach et al., ‘Impact of COVID-19 on global HCV elimination efforts’, J Hepatol, vol. 74, no. 1, p. 31, Jan. 2021. [CrossRef]
- L. Sowah and C. Chiou, ‘Impact of Coronavirus Disease 2019 Pandemic on Viral Hepatitis Elimination: What Is the Price?’, AIDS Res Hum Retroviruses, vol. 37, no. 8, p. 585, Aug. 2021. [CrossRef]
- J. Laury, L. Hiebert, and J. W. Ward, ‘Impact of COVID-19 Response on Hepatitis Prevention Care and Treatment: Results From Global Survey of Providers and Program Managers’, Clin Liver Dis (Hoboken), vol. 17, no. 1, pp. 41–46, Jan. 2021. [CrossRef]
- M. Y. Bertram and T. T. T. Edejer, ‘Introduction to the Special Issue on “The World Health Organization Choosing Interventions That Are Cost-Effective (WHO-CHOICE) Update”’, Int J Health Policy Manag, vol. 10, no. 11, pp. 670–672, Nov. 2021. [CrossRef]
- ‘Consolidated strategic information guidelines for viral hepatitis planning and tracking progress towards elimination: guidelines’. Accessed: Feb. 03, 2024. [Online]. Available: https://www.who.int/publications/i/item/9789241515191.
- ‘New cost-effectiveness updates from WHO-CHOICE’. Accessed: Feb. 03, 2024. [Online]. Available: https://www.who.int/news-room/feature-stories/detail/new-cost-effectiveness-updates-from-who-choice.
- ‘Hepatitis WPRO’. Accessed: Feb. 03, 2024. [Online]. Available: https://www.who.int/westernpacific/health-topics/hepatitis#tab=tab_1.
- S. W. Lee et al., ‘Comparison of tenofovir and entecavir on the risk of hepatocellular carcinoma and mortality in treatment-naïve patients with chronic hepatitis B in Korea: a large-scale, propensity score analysis’, Gut, vol. 69, no. 7, pp. 1301–1308, Jul. 2020. [CrossRef]
- M. Cornberg et al., ‘Guidance for design and endpoints of clinical trials in chronic hepatitis B - Report from the 2019 EASL-AASLD HBV Treatment Endpoints Conference’, Hepatology, vol. 71, no. 3, pp. 1070–1092, Mar. 2019. [CrossRef]
- ‘Polaris Observatory – CDA Foundation’. Accessed: Feb. 02, 2024. [Online]. Available: https://cdafound.org/polaris/.
- ‘The Hepatitis Prevention, Control, and Elimination Program in Mongolia - Элэг бүтэн Мoнгoл үндэсний хѳтѳлбѳр (National program) | Coalition for Global Hepatitis Elimination’. Accessed: Feb. 03, 2024. [Online]. Available: https://www.globalhep.org/about/partner-programs/hepatitis-prevention-control-and-elimination-program-mongolia-eleg-buten.
- ‘Find the Missing Millions - World Hepatitis Alliance’. Accessed: Feb. 04, 2024. [Online]. Available: https://www.worldhepatitisalliance.org/find-the-missing-millions/.
- R. Rajbhandari and R. T. Chung, ‘Screening for hepatitis B virus infection: a public health imperative’, Ann Intern Med, vol. 161, no. 1, pp. 76–77, Jul. 2014. [CrossRef]
- Z. Abbas and M. Abbas, ‘Challenges in Formulation and Implementation of Hepatitis B Elimination Programs’, Cureus, vol. 13, no. 4, Apr. 2021. [CrossRef]
- M. Lemoine et al., ‘Acceptability and feasibility of a screen-and-treat programme for hepatitis B virus infection in The Gambia: the Prevention of Liver Fibrosis and Cancer in Africa (PROLIFICA) study’, Lancet Glob Health, vol. 4, no. 8, pp. e559–e567, Aug. 2016. [CrossRef]
- C. L. Lin and J. H. Kao, ‘Review article: novel therapies for hepatitis B virus cure – advances and perspectives’, Aliment Pharmacol Ther, vol. 44, no. 3, pp. 213–222, Aug. 2016. [CrossRef]
- G. C. Fanning, F. Zoulim, J. Hou, and A. Bertoletti, ‘Therapeutic strategies for hepatitis B virus infection: towards a cure’, Nat Rev Drug Discov, vol. 18, no. 11, pp. 827–844, Nov. 2019. [CrossRef]
- J. Howell et al., ‘A global investment framework for the elimination of hepatitis B’, J Hepatol, vol. 74, no. 3, pp. 535–549, Mar. 2021. [CrossRef]
- D. S. Chen, ‘Fighting against viral hepatitis: Lessons from Taiwan’, Hepatology, vol. 54, no. 2, pp. 381–392, Aug. 2011. [CrossRef]
Figure 1.
2022 HBV prevalence in all countries (all ages) [12]. HBV — hepatitis B virus.
Figure 1.
2022 HBV prevalence in all countries (all ages) [12]. HBV — hepatitis B virus.
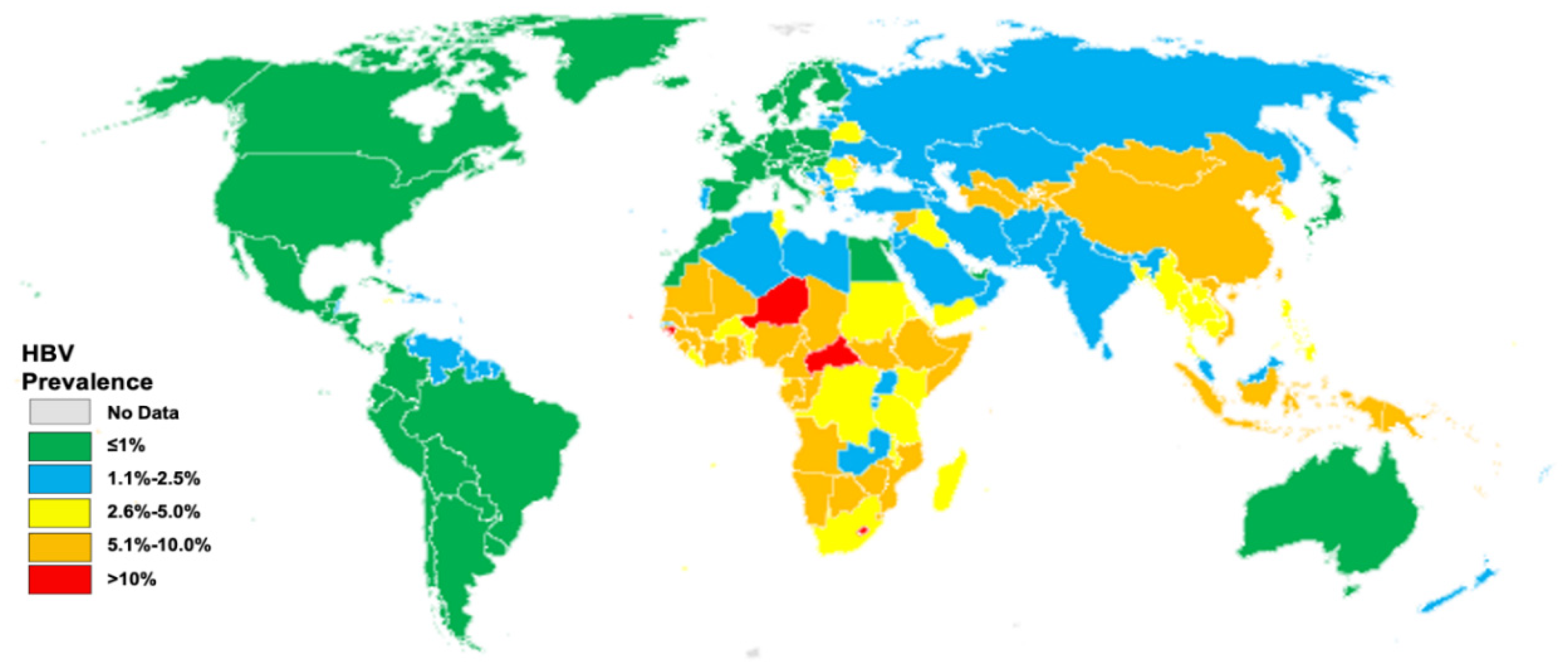
Figure 2.
Global and Regional HBV Cascade of Care, 2022 [12]. AFRO – World Health Organization Africa Regional Office; EMRO – World Health Organization Eastern Mediterranean Regional Office; EURO – World Health Organization Europe Regional Office; HBV — hepatitis B virus; PAHO – Pan-American Health Organization; SEARO – World Health Organization South East Asia Regional Office; WPRO – World Health Organization WPRal Office.
Figure 2.
Global and Regional HBV Cascade of Care, 2022 [12]. AFRO – World Health Organization Africa Regional Office; EMRO – World Health Organization Eastern Mediterranean Regional Office; EURO – World Health Organization Europe Regional Office; HBV — hepatitis B virus; PAHO – Pan-American Health Organization; SEARO – World Health Organization South East Asia Regional Office; WPRO – World Health Organization WPRal Office.
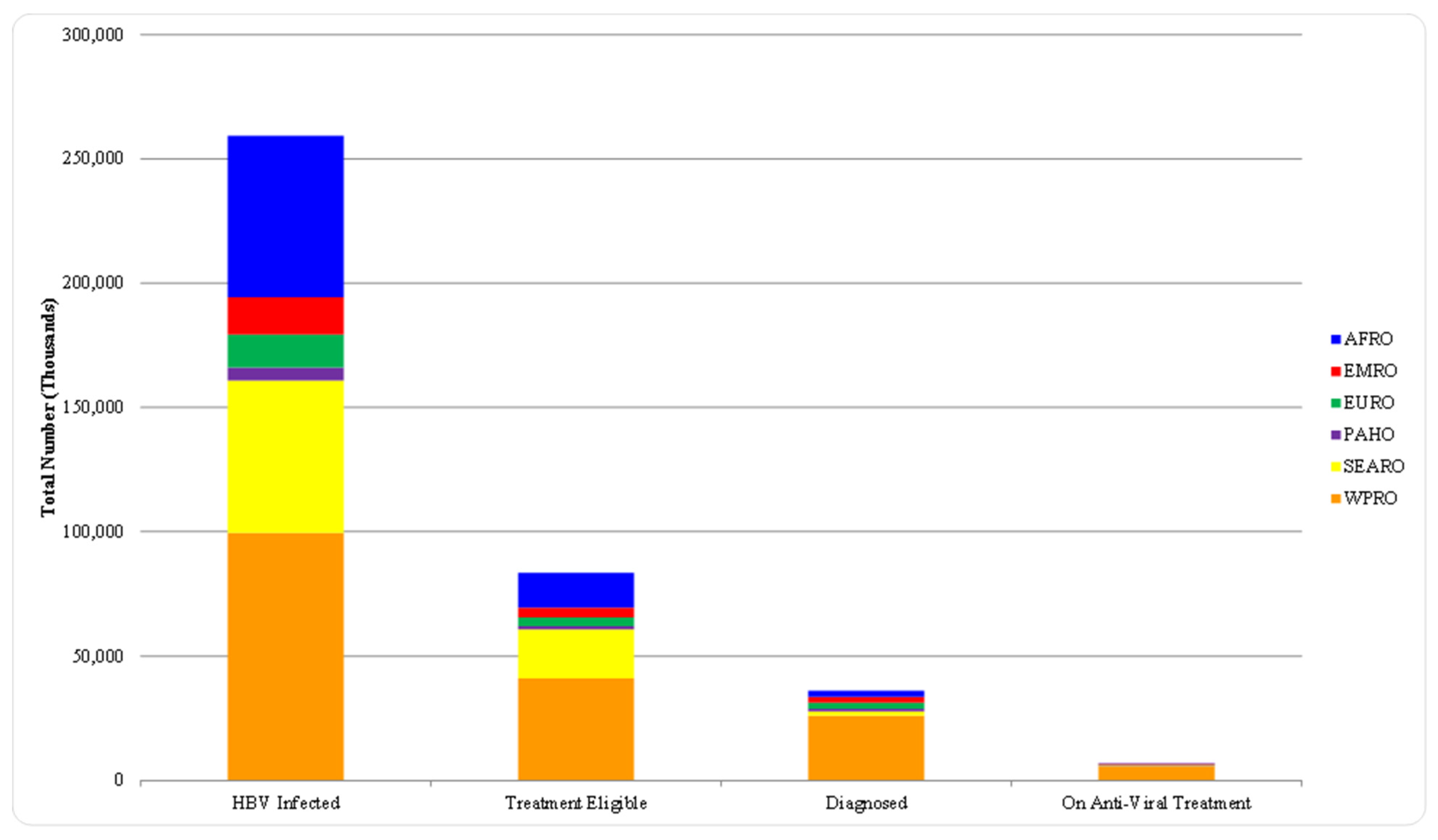
Figure 3.
2022 HBV prevalence in all countries (five-year-old children) [12]. HBV — hepatitis B virus.
Figure 3.
2022 HBV prevalence in all countries (five-year-old children) [12]. HBV — hepatitis B virus.
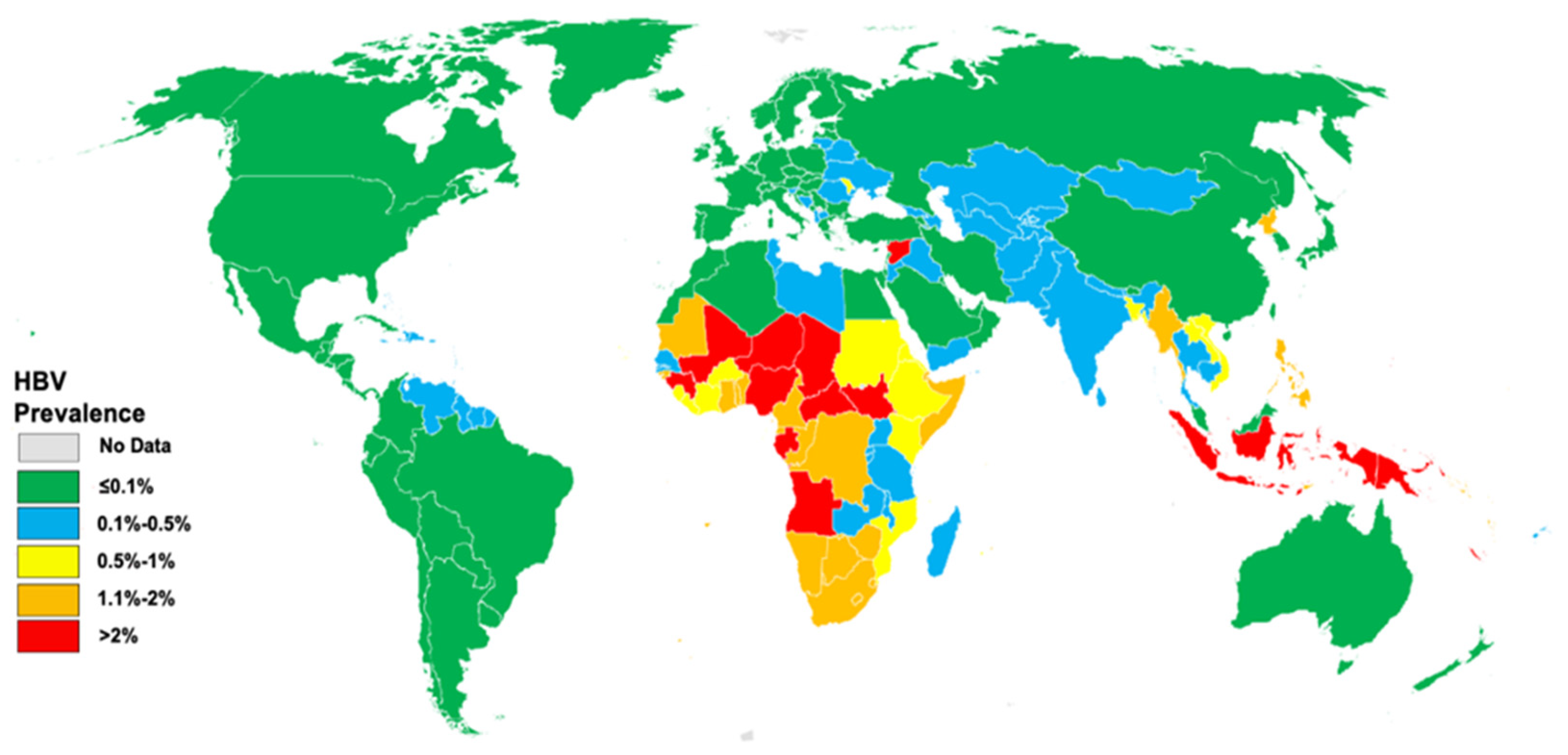

Table 1.
WHO 2020 and 2030 targets eliminating chronic viral hepatitis B and C infection.
| TARGET AREA | BASELINE 2015 | 2020 TARGETS | 2030 TARGETS |
|---|---|---|---|
| Impact targets | |||
| Incidence: New cases of CHB and CHC infections | Between 6 and 10 million infections are reduced to 0.9 million infections by 2030 (95% decline in HBV infections, 80% decline in HCV infections) | 30% reduction (equivalent to 1% prevalence of HBsAg among children) | 90% reduction (equivalent to 0.1% prevalence of HBsAg among children) |
| Mortality: HBV and HCV deaths | 1.4 million deaths reduced to less than 500 000 by 2030 (65% for both HBV and HCV) | 10% reduction | 65% reduction |
| Service coverage targets | |||
| HBV vaccination: childhood vaccine coverage (third dose coverage) | 82% in infants | 90% | 90% |
| Prevention of HBV MTCT: HBV birth-dose vaccination coverage or other approach to prevent MTCT | 38% | 50% | 90% |
| Blood safety | 39 countries do not routinely test all blood donations for transfusion transmissible infections 89% of donations are screened in a quality-assured manner | All countries have hemovigilance systems in place to identify and quantify viral hepatitis transfusion transmission rates | Reduce rates of transmission by 99% compared with 2020. |
| Safe injections: percentage of injections administered with safety-engineered devices in and out of health facilities | 5% | 50% | 90% |
| Harm reduction: number of sterile needles and syringes provided per person who injects drugs per year | 20 | 200 | 300 |
| HBV and HCV diagnosis | <5% of chronic hepatitis infections diagnosed | 50% | 90% |
| HBV and HCV treatment | <1% receiving treatment | 5 million people receiving HBV treatment, 3 million people received HCV treatment | 80% of eligible persons with CHB infection treated 80% of eligible persons with CHC infection treated |
The abbreviation: HBsAg: hepatitis B virus surface antigen, HBV: Hepatitis B virus, HCV: hepatitis C virus, CHB: chronic hepatitis B, CHC: chronic hepatitis C,.
Table 2.
Four Strategies to Universal Hepatitis B Vaccination in Infants.
| Maternal screening | Infants receive | Efficacy | Cost | Example | |
| Vaccine | HBIG | ||||
| Yes (HBsAg and then HBeAg) | Yes | HBeAg-positive mothers’ infants only | Higher | Higher | Taiwan |
| Yes (HBsAg only) | Yes | All HBsAg-positive mothers’ infants | Highest | Highest | US |
| Yes (HBeAg only) | Yes | HBeAg-positive mothers’ infants only (2 doses) | High | Highest | Japan |
| No | Yes | No | Modest | Low | Thailand |
Abbreviations: HBsAg: hepatitis B surface antigen, HBeAg: hepatitis B e antigen, HBIG: hepatitis B immune globulin.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



