
Submitted:
08 February 2024
Posted:
08 February 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Various vaccines have been developed in response to the SARS-CoV-2 pandemic, and the safety of vaccines has become an important issue. COVID-19 vaccines-related central nervous system inflammatory demyelinating diseases (CNS IDDs) have been reported recently. We present one case of AstraZeneca vaccine-related myelin oligodendrocyte glycoprotein (MOG) antibody-associated disease and literature review another 78 patients published from January 2020 to October 2022. Patients were divided into three vaccine groups (viral vector, mRNA and inactivated vaccines) for further analyses. Among 79 patients with COVID-19 vaccines-related CNS IDDs, 49 (62%) cases received viral vector vaccines, 20 (25.3%) received mRNA vaccines and 10 (12.7%) received inactivated vaccines. Twenty-seven cases (34.2%) were confirmed with autoantibodies, including 15 patients (19%) with anti-MOG, 11 (13.9%) with anti-aquaporin 4 (AQP4), and one (1.3%) with both antibodies. Significantly, more males developed CNS IDDs post viral vector vaccines compared to mRNA and inactivated vaccines. Patients receiving mRNA vaccines were older than other groups. Furthermore, mRNA and inactivated vaccines correlated more with anti-AQP4 antibodies, while viral vector vaccines showed higher MOG positivity. The research suggests potential associations between COVID-19 vaccines-related CNS IDDs and gender, age, and autoantibodies, contingent on vaccine types. Protein sequence analysis implies similarities between the S protein and AQP4/MOG. Further studies may elucidate the mechanisms of CNS IDDs, aiding vaccine selection for specific groups.
Keywords:
Acute disseminated encephalomyelitis
; Central nervous system inflammatory demyelinating diseases
; COVID-19 vaccines
; Myelin oligodendrocyte glycoprotein antibody-associated disease
; Neuromyelitis optica spectrum disorders
; Transverse myelitis
1. Introduction
Diseases of myelin sheaths in the central nervous system (CNS) can be divided into two categories including genetic dysmyelinating diseases with abnormal myelin formation and acquired inflammatory demyelinating diseases, so called central nervous system inflammatory demyelinating diseases (CNS IDDs). CNS IDDs include multiple sclerosis (MS), neuromyelitis optica spectrum disorders (NMOSD), myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD), acute disseminated encephalomyelitis (ADEM), optic neuritis (ON) and transverse myelitis (TM) [1].
Among CNS IDDs, MS is the most common one disorder. The worldwide incidence rate of MS is 2.1 per 100,000 person-year, and the prevalence is estimated 35.9 per 100,000 people [2]. MS has been considered as a T cells and B cells-mediated disease, while NMOSD and MOGAD are both related to autoantibodies, which target aquaporin 4 (AQP4) and myelin oligodendrocyte glycoprotein (MOG), respectively. The incidence and prevalence of NMOSD is about 0.28–0.73 per 100,000 person-years and 0.52–10 per 100,000 people, respectively [3]. The epidemiological data of NMOSD ranged widely might be due to different study designs, regions, and ethnicity. NMOSD is more common in East Asian, African and Latin American than other Western populations, and the prevalence is 2.3 to 7.6 times higher in women than in men [4]. Previous studies in Europe estimated that the incidence of MOGAD is around 0.16–0.34 per 100,000 person-years, and the prevalence is 2 per 100,000 people [5,6]. The median age of onset is from early to mid-thirties with a slight predominance in females (57–68%) [7,8,9]. The clinical manifestations of MOGAD are diverse and can include one or a combination of the following diseases, such as ON, TM and ADEM [10]. ON was the most common symptom (54–68.5%), followed by TM (27–30%), and ADEM or ADEM-like presentation (18–25%) [7,9,11]. The initial presentations of MOGAD in children and adults were also different, that ADEM was the most common in children and ON was primarily found in adults [8].
ADEM is characterized by monophasic multifocal neurologic symptoms, and its diagnosis requires exclusion of MS, NMOSD, MOGAD or other demyelinating diseases [12]. ADEM is primarily regarded as a post-infectious disease, whereas vaccines related ADEM is a rare condition. It has been published that < 5% of ADEM cases were related to vaccination for diseases such as rabies, measles, mumps, smallpox, or Japanese B encephalitis [13]. However, a recent study in the United States reported that there were no statistically significant increased risks of ADEM after vaccination for 5–28 days, except for tetanus, reduced diphtheria, and acellular pertussis (Tdap) [14]. Another study further demonstrated that there was no association between ADEM and various types of vaccines, including Tdap [15]. The controversial relationship between vaccination and ADEM remains ambiguous, and large-scale epidemiologic data and clinical studies are required to confirm their association.
During the outbreak of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic, vaccines are currently one of the most effective ways to prevent infection. The mechanisms of COVID-19 vaccines include viral vectors (AstraZeneca, Janssen, Sputnik V, CanSino), mRNA (Pfizer-BioNTech and Moderna), inactivated vaccines (Sinovac, Sinopharm, Covaxin), and protein subunit vaccines (Medigen). Various side effects of COVID-19 vaccines have been widely reported recently. Although the distinct mechanism has not yet been elucidated, some adverse events may be related to specific groups of vaccines. For example, vaccines-induced immune thrombotic thrombocytopenia (VITT) and Guillain–Barre syndrome are generally considered to be related to the viral vector COVID-19 vaccines [16,17,18,19]. An elevated risk of myocarditis was observed in a population of young men who received mRNA COVID-19 vaccines [20]. CNS IDDs, such as TM, NMOSD, ADEM or ON, have been reported after receiving AstraZeneca [21,22,23,24,25,26,27,28], Janssen [29], Sputnik V [30], Pfizer-BioNTech [31,32,33,34,35], Moderna [36,37,38,39,40], Sinovac [41,42], Sinopharm [43,44] and an unknown inactivated vaccine [45].
We speculate that the COVID-19 vaccines may induced CNS IDDs in a small subset of populations. Additionally, different types of COVID-19 vaccines may lead to different clinical manifestations, laboratory or imaging characteristics of CNS IDDs. We now present a patient who developed MOGAD following COVID-19 vaccination and recruit relevant cases from the update literature in details for comparison and analysis.
2. Materials and Methods
2.1. Case presentation
Our report describes a 50-year-old man who has chronic hepatitis B virus (HBV) hepatitis and with no other comorbidities. After the first dose with COVID-19 vaccine (AZD1222, AstraZeneca), the patient experienced mild headache and general weakness that persisted for 2 days and then spontaneously subsided. On the 13th day following vaccination, he experienced acute onset of headache which was exacerbated upon waking up in the morning. In addition, fever, bilateral lower limb numbness, low back pain, confusion, slow response, unsteady gait, constipation, and urine retention requiring insertion of a Foley catheter developed over the following 4 days. Neurologic examination revealed Glasgow coma scale E4V5M6, but with episodic lethargy and obtunded. Impaired proprioception over the bilateral lower limbs causing ataxic gait and a dermatome level with a pin-prick sensation decreased below the T4 level were found. Motor function and deep tendon reflexes were normal, and the Babinski reflex was bilateral plantar flexion. Autonomic dysfunction led to constipation and urine retention. Cervical and thoracic spinal MRI revealed T2-hyperintensity in the spinal cord at the T3 to T4 level without contrast enhancement, resembling focal myelitis (Figure 1a and 1c, 19th day post-vaccination). Brain MRI revealed symmetric, poorly demarcated hyperintensities involving the brainstem, bilateral pulvinar thalami, putamen, centrum semiovale, and subcortical white matter on FLAIR and T2WI without gadolinium enhancement (Figure 2, 20th day post-vaccination). Blood tests revealed leukocytosis (11,000 cells/uL) with neutrophil predominance (85%) and elevated CRP (48.49 mg/L). Urinalysis for intoxication was negative. CSF analysis showed lymphocytic predominant pleocytosis (175 cells/µL, 99% lymphocytes), elevated total protein (78.1 mg/dL), and low CSF/serum glucose ratio (0.47).
He was administered empiric antibiotics (ceftriaxone and vancomycin) and antiviral (acyclovir) treatment initially which were discontinued because bacterial culture and viral examination of CSF and blood were negative results. Other pathogens, including COVID-19 (nasopharyngeal swab for SARS-CoV-2-RT-PCR), Japanese encephalitis virus, herpes simplex virus (HSV), cytomegalovirus (CMV), Epstein-Barr virus (EBV), varicella zoster virus (VZV), human immunodeficiency virus (HIV), cryptococcus, tuberculosis, syphilis, hepatitis C, and mycoplasma, were all negative. Further tests for vitamin B12 deficiency, vasculitis, connective tissue diseases, and tumor markers were unremarkable findings. Anti-AQP4 antibodies and oligoclonal bands were not found, but anti-MOG antibodies were detected in serum by cell-based assay (CBA) (Figure 3).
Pulse therapy with methylprednisolone (1 g per day for 5 consecutive days) was administered, followed by oral prednisolone (1 mg/kg/day) with gradual tapering. His consciousness and response became clear, and proprioception and pin-prick sensation gradually improved since the 2nd day after pulse therapy. The patient was discharged with total recovery of proprioception, pin-prick sensory level receding to T10 level, and improvement in constipation. The Foley catheter was successfully removed on the 38th day post-vaccination. Spinal MRI 5 months after vaccination revealed total resolution of T3 to T4 myelitis (Figure 1b,d). All neurological deficits have fully recovered. Anti-MOG antibodies in serum remained positive after 7 months of follow-up.
2.2. Literature review
To analyze the clinical presentations and MRI findings of patients with CNS IDDs after COVID-19 vaccination, a literature review of studies published in English was conducted using PubMed, EMBASE, Google Scholar, Ovid, and SCOPUS. Published articles and preprint of cases between January 2020 and October 2022 were included to obtain sufficient data, particularly brain and spinal MR imaging. The Medical Subject Heading (MeSH) terms “acute disseminated encephalomyelitis (ADEM),” “myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD)”, “neuromyelitis optica spectrum disorders (NMOSD)”, “optic neuritis” and “myelitis” with “COVID-19 vaccines” were used to retrieve all accessible articles. We aimed to identify cases with first onset of CNS IDDs related to COVID-19 vaccination. Those diagnosed with relapses of MS and NMOSD, SARS-CoV-2 infection, and CNS infection were excluded. We recorded the clinical features, past history, laboratory findings, brain/spinal MR imaging, treatment, and outcomes of our index patient in addition to previously reported cases of CNS IDDs after receiving COVID-19 vaccines. The lesions on brain MRI were classified as cortical, deep gray matters, white matters (periventricular, subcortical, periaqueductal), brainstem, and with or without gadolinium enhancement. The lesions on spinal MRI were divided into long cord (≥3 segments) or short cord (<3 segments), and with or without gadolinium enhancement.
2.3. Statistical analysis
SPSS 26.0 (IBM Corp., Armonk, NY, USA) was used for statistical analyses. Categorical variables were compared using Pearson’s chi-square test or Fisher’s exact test. One-way analysis of variance (ANOVA) was used to compare unpaired groups. An independent samples t-test was applied for continuous variables. The level of significance was set at P < 0.05. All tests were two-tailed.
3. Results
In total, there were 79 cases (including our index case of MOGAD) diagnosed with CNS IDDs after COVID-19 vaccination. Among them, the proportion of female (54.4%) was higher than that of males (45.6%), with average ages of 46.2 and 48.5 (p=0.524), respectively (Table 1). The majority of patients developed symptoms after the first dose (77.2%) or second dose (21.5%) of the COVID-19 vaccination, while one patient (1.3%) developed CNS IDDs after the third dose. The mean time of onset from vaccination to clinical symptoms was approximately 12.2 days (range 1-42 days). Twenty-four patients (30.4%) presented with ADEM or ADEM-like, 21 cases (26.6%) with myelitis, 17 (21.5%) with ADEM with myelitis, 13 (16.5%) with NMOSD, and four (5.1%) with ON. A total of 27 patients (34.2%) had autoantibodies, including 15 patients (19%) with anti-MOG antibodies, 11 patients (13.9%) with anti-AQP4 antibodies, and one patient (1.3%) with both anti-MOG and anti-AQP4 antibodies. In the CSF examination of the 79 cases, the average WBC was 63.5 cells/µL with lymphocyte predominant, and the average total protein was 69.5 mg/dL. Additionally, oligoclonal bands were positive in 13 cases (16.5%).
COVID-19 vaccines with different mechanisms of action may lead to different manifestations of CNS IDDs. We categorize the vaccines into three major groups, including viral vector (49 cases, 62%), mRNA (20 cases, 25.3%) and inactivated vaccines (10 cases, 12.7%), to analyze their clinical presentations and laboratory examinations of CNS IDDs (Table 2). Compared to viral vector vaccines, CNS IDDs were more commonly observed in female patients receiving mRNA or inactivated vaccines (p = 0.027). The mean age of onset of patients received mRNA vaccines was much older than those receiving viral vector or inactivated vaccines (p = 0.002). The vast majority of patients in the viral vector vaccine group developed CNS IDDs after the first dose. Approximately two-thirds of the mRNA vaccine group experienced CNS IDDs after the first dose, and one-third after the second dose. In the inactivated vaccine group, there was one patient developed CNS IDDs after the third dose. The time interval between vaccination and clinical presentations of CNS IDDs in patients receiving mRNA vaccines appears to be shorter than the other two groups, although it is not statistically significant. There was no significant difference in the clinical presentations of CNS IDDs among these three groups. Patients receiving mRNA or inactivated vaccines were more commonly found to have anti-AQP4 antibodies, while those receiving viral vector vaccines were frequently associated with anti-MOG antibodies (p = 0.044). On the other hand, a higher rate of CSF pleocytosis with lymphocyte predominant was observed in patients administered viral vector and mRNA vaccines (p = 0.004). Spinal cord lesions with gadolinium enhancement were most commonly found in patients who received mRNA vaccines (p = 0.015). There was no significant difference in the distribution of brain lesions or LETM (>= 3 contiguous vertebral segments) between the three groups. In past history, hypertension and diabetes were the most common, with 6 patients each (Table 1). The next most common diseases were hyperlipidemia and autoimmune diseases, with 4 patients each. Nevertheless, there was no statistically significant correlation between past history and the occurrence of CNS IDDs due to receiving different groups of vaccines (data not presented in Table 2).
The majority of patients (86%) received the first-line immunotherapy, including steroid pulse therapy, plasmapheresis/plasma exchange, or IVIG. Ten patients (13%) underwent additional second-line immunotherapy, such as cyclophosphamide or Rituximab. Except for the three mortality cases (3.8%), the rest of the patients had either totally recovered (20 patients) or shown improvement (27 patients).
Discussion
During the global SARS-CoV-2 pandemic, universal vaccination is a key factor in preventing infection and avoiding critical illness. The overall safety and tolerability of COVID-19 vaccines has been shown to be generally acceptable in patients with underlying CNS IDDs, but there were still some patients (16.7%) reported worsening of their symptoms after vaccination during the first week, with rapid resolution within 3 days [46]. The cases we reviewed in our study resulted from exposure to COVID-19 vaccines and they did not have a past history of CNS IDDs. The decision whether to receive the 2nd or booster shots of COVID-19 vaccines, or to shift to another kind of vaccine, are important clinical issues.
According to statistics from the Centers for Disease Control in Taiwan, as of April 2023, the COVID-19 vaccine coverage rate was 94% for the first dose, 89% for the second dose, and 76.7% for additional doses. Most people received mRNA or viral vector vaccines, including Moderna (42.7%), Pfizer-BioNTech (29.2%), AstraZeneca (22.5%), Medigen (4.5%, a type of protein subunit vaccine produced in Taiwan), and Novavax (0.9%). Various adverse effects were reported. Six ADEM (not included our index case), two NMOSD, 13 ON, and four myelitis cases were suspected to be related to COVID-19 vaccination been reported on Taiwan CDC website, but they had not been formally published [47]. Thrombosis with thrombocytopenia syndrome (TTS, also known as VITT) was suspected in 74 cases (86% of them received AstraZeneca, 8% received Moderna, 4% received Pfizer and 1% received Medigen) [47]. In Taiwan, the first case of VITT after the AstraZeneca vaccination was diagnosed in May 2021 at Chang Gung Memorial Hospital, a tertiary medical center. The patient presented with severe headaches, thrombocytopenia, and abdominal pain without neurological deficit. Brain CT revealed lacunar infarction in the right centrum semiovale. His platelet count normalized after treatment with high-dose IVIG (2 g/kg for two consecutive days) and he was discharged without further thrombotic or hemorrhagic events [48].
The pathophysiology of vaccines-induced CNS IDDs remains unclear. Many studies have suggested the molecular mimicry theory. For example, amino acid similarities between small HBV surface antigen (SHBsAg, the ingredient of HBV non-infectious viral subunit vaccine) and MOG have been analyzed, displaying 66–100% homology in several sequences [49]. This finding suggests the possibility of immunological cross-reactivity. H1N1 and HPV vaccines have been identified with suspicious overlapping targets, which may result in certain autoimmune diseases [50]. Although there is no evidence of molecular mimicry regarding COVID-19 vaccines to date, the positive findings of anti-MOG antibodies and anti-AQP4 antibodies after receiving COVID-19 vaccines imply the possible similar amino acid sequences of MOG, AQP4, and spike (S) protein of SARS-CoV-2 virus or other unidentified immunological mechanisms. Through protein sequence analysis, it is possible that the S protein shares similar protein sequences with AQP4 and MOG (Figure 4). Once the definite pathological mechanisms have been elucidated, CNS IDDs induced by COVID-19 vaccines may be avoided by the development of safer vaccines. These results have limitations because of a short follow-up period and a small number of patients. A larger database is required for further investigation into the relationship between demographics and vaccine types. The occurrence of CNS IDDs may be reduced by employing more precise indications for each kind of COVID-19 vaccines.
The rare complication of CNS IDDs after vaccination should not restrain the use of vaccines during the COVID-19 pandemic. For those who develop vaccines-related neuroimmunological adverse effects, further treatment strategies should be considered. Although the short-term outcomes were primarily ideal among the patients listed in our review following appropriate treatment, the possibility of long-term sequelae or recurrence of CNS IDDs still exists. To our knowledge, NMOSD and MOGAD patients have a higher risk of relapse if persistent seropositivity, and prolonged immunotherapy should be considered to prevent relapse [10,51]. Therefore, patients initially positive for autoantibodies are recommended for regular follow up MRI and antibody testing. Attention is also required for seronegative cases because of the possibility of seroconversion or the existence of other yet undefined autoantibodies.
5. Conclusions
We observed that there were more male patients with CNS IDDs in the viral vector vaccine group and they were often accompanied with anti-MOG antibodies. Patients receiving mRNA vaccines were older and more commonly positive for anti-AQP4 antibodies. The current consensus is that the rare occurrence of CNS IDDs is not a contraindication to vaccination. More extensive studies with larger cohorts are necessary to elucidate the pathological mechanisms of vaccines-related CNS IDDs and can provide physicians to select safer and more appropriate vaccines for each individual group to reduce the risk of adverse effects.
Author Contributions
All authors contributed to the study conception and design. Data collection and analysis were performed by Mei-Yun Cheng, Hsuan-Chen Ho, Jung-Lung Hsu, and Ming-Feng Liao. Protein sequence analysis was undertaken by Yi Wang and Lin-Yi Chen. The first draft of the manuscript was written by Mei-Yun Cheng and Hsuan-Chen Ho. Long-Sun Ro supervised the editing of the writing. All authors critically reviewed the manuscript and approved the final version for submission.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (No: 202200651B0) of Chang Gung Memorial Hospital for studies involving humans.
Informed Consent Statement
Patient consent was waived due to retrospective medical chart reviews.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author.
Acknowledgments
The cell-based immunofluorescence assay was performed and photographed by Yang-Hsuan at Chang-Gung Memorial Hospital in Linkou, Taiwan.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hegen, H.; Reindl, M. Recent developments in MOG-IgG associated neurological disorders. Ther Adv Neurol Disord 2020, 13, 1756286420945135. [Google Scholar] [CrossRef] [PubMed]
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; La Rocca, N.; Uitdehaag, B.; van der Mei, I.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult Scler 2020, 26, 1816–1821. [Google Scholar] [CrossRef] [PubMed]
- Jarius, S.; Aktas, O.; Ayzenberg, I.; Bellmann-Strobl, J.; Berthele, A.; Giglhuber, K.; Häußler, V.; Havla, J.; Hellwig, K.; Hümmert, M.W.; et al. Update on the diagnosis and treatment of neuromyelits optica spectrum disorders (NMOSD) - revised recommendations of the Neuromyelitis Optica Study Group (NEMOS). Part I: Diagnosis and differential diagnosis. J Neurol 2023. [Google Scholar] [CrossRef] [PubMed]
- Papp, V.; Magyari, M.; Aktas, O.; Berger, T.; Broadley, S.A.; Cabre, P.; Jacob, A.; Kira, J.I.; Leite, M.I.; Marignier, R.; et al. Worldwide Incidence and Prevalence of Neuromyelitis Optica: A Systematic Review. Neurology 2021, 96, 59–77. [Google Scholar] [CrossRef] [PubMed]
- de Mol, C.L.; Wong, Y.; van Pelt, E.D.; Wokke, B.; Siepman, T.; Neuteboom, R.F.; Hamann, D.; Hintzen, R.Q. The clinical spectrum and incidence of anti-MOG-associated acquired demyelinating syndromes in children and adults. Mult Scler 2020, 26, 806–814. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, K.; Hamilton-Shield, A.; Woodhall, M.; Messina, S.; Mariano, R.; Waters, P.; Ramdas, S.; Leite, M.I.; Palace, J. Prevalence and incidence of neuromyelitis optica spectrum disorder, aquaporin-4 antibody-positive NMOSD and MOG antibody-positive disease in Oxfordshire, UK. J Neurol Neurosurg Psychiatry 2020, 91, 1126–1128. [Google Scholar] [CrossRef]
- Wynford-Thomas, R.; Jacob, A.; Tomassini, V. Neurological update: MOG antibody disease. J Neurol 2019, 266, 1280–1286. [Google Scholar] [CrossRef]
- Ramanathan, S.; Mohammad, S.; Tantsis, E.; Nguyen, T.K.; Merheb, V.; Fung, V.S.C.; White, O.B.; Broadley, S.; Lechner-Scott, J.; Vucic, S.; et al. Clinical course, therapeutic responses and outcomes in relapsing MOG antibody-associated demyelination. J Neurol Neurosurg Psychiatry 2018, 89, 127–137. [Google Scholar] [CrossRef]
- Jurynczyk, M.; Messina, S.; Woodhall, M.R.; Raza, N.; Everett, R.; Roca-Fernandez, A.; Tackley, G.; Hamid, S.; Sheard, A.; Reynolds, G.; et al. Clinical presentation and prognosis in MOG-antibody disease: a UK study. Brain 2017, 140, 3128–3138. [Google Scholar] [CrossRef]
- López-Chiriboga, A.S.; Majed, M.; Fryer, J.; Dubey, D.; McKeon, A.; Flanagan, E.P.; Jitprapaikulsan, J.; Kothapalli, N.; Tillema, J.M.; Chen, J.; et al. Association of MOG-IgG Serostatus With Relapse After Acute Disseminated Encephalomyelitis and Proposed Diagnostic Criteria for MOG-IgG-Associated Disorders. JAMA Neurol 2018, 75, 1355–1363. [Google Scholar] [CrossRef] [PubMed]
- Cobo-Calvo, A.; Ruiz, A.; Maillart, E.; Audoin, B.; Zephir, H.; Bourre, B.; Ciron, J.; Collongues, N.; Brassat, D.; Cotton, F.; et al. Clinical spectrum and prognostic value of CNS MOG autoimmunity in adults: The MOGADOR study. Neurology 2018, 90, e1858–e1869. [Google Scholar] [CrossRef]
- Pohl, D.; Alper, G.; Van Haren, K.; Kornberg, A.J.; Lucchinetti, C.F.; Tenembaum, S.; Belman, A.L. Acute disseminated encephalomyelitis: Updates on an inflammatory CNS syndrome. Neurology 2016, 87, S38–45. [Google Scholar] [CrossRef]
- Bennetto, L.; Scolding, N. Inflammatory/post-infectious encephalomyelitis. J Neurol Neurosurg Psychiatry 2004, 75 Suppl 1, i22–28. [Google Scholar] [CrossRef]
- Baxter, R.; Lewis, E.; Goddard, K.; Fireman, B.; Bakshi, N.; DeStefano, F.; Gee, J.; Tseng, H.F.; Naleway, A.L.; Klein, N.P. Acute Demyelinating Events Following Vaccines: A Case-Centered Analysis. Clin Infect Dis 2016, 63, 1456–1462. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Ma, F.; Xu, Y.; Chu, X.; Zhang, J. Vaccines and the risk of acute disseminated encephalomyelitis. Vaccine 2018, 36, 3733–3739. [Google Scholar] [CrossRef] [PubMed]
- Woo, E.J.; Mba-Jonas, A.; Dimova, R.B.; Alimchandani, M.; Zinderman, C.E.; Nair, N. Association of Receipt of the Ad26.COV2.S COVID-19 Vaccine With Presumptive Guillain-Barré Syndrome, February-July 2021. Jama 2021, 326, 1606–1613. [Google Scholar] [CrossRef] [PubMed]
- MacNeil, J.R.; Su, J.R.; Broder, K.R.; Guh, A.Y.; Gargano, J.W.; Wallace, M.; Hadler, S.C.; Scobie, H.M.; Blain, A.E.; Moulia, D.; et al. Updated Recommendations from the Advisory Committee on Immunization Practices for Use of the Janssen (Johnson & Johnson) COVID-19 Vaccine After Reports of Thrombosis with Thrombocytopenia Syndrome Among Vaccine Recipients - United States, April 2021. MMWR Morb Mortal Wkly Rep 2021, 70, 651–656. [Google Scholar] [CrossRef] [PubMed]
- Pottegård, A.; Lund, L.C.; Karlstad, Ø.; Dahl, J.; Andersen, M.; Hallas, J.; Lidegaard, Ø.; Tapia, G.; Gulseth, H.L.; Ruiz, P.L.; et al. Arterial events, venous thromboembolism, thrombocytopenia, and bleeding after vaccination with Oxford-AstraZeneca ChAdOx1-S in Denmark and Norway: population based cohort study. Bmj 2021, 373, n1114. [Google Scholar] [CrossRef] [PubMed]
- Su, S.C.; Lyu, R.K.; Chang, C.W.; Tseng, W.J. The First Guillain-Barr? Syndrome After SARS-CoV-2 Vaccination in Taiwan. Acta Neurol Taiwan 2022, 31(1), 46–51. [Google Scholar]
- Gargano, J.W.; Wallace, M.; Hadler, S.C.; Langley, G.; Su, J.R.; Oster, M.E.; Broder, K.R.; Gee, J.; Weintraub, E.; Shimabukuro, T.; et al. Use of mRNA COVID-19 Vaccine After Reports of Myocarditis Among Vaccine Recipients: Update from the Advisory Committee on Immunization Practices - United States, June 2021. MMWR Morb Mortal Wkly Rep 2021, 70, 977–982. [Google Scholar] [CrossRef]
- Rinaldi, V.; Bellucci, G.; Romano, A.; Bozzao, A.; Salvetti, M. ADEM after ChAdOx1 nCoV-19 vaccine: A case report. Mult Scler 2021, 13524585211040222. [Google Scholar] [CrossRef]
- Permezel, F.; Borojevic, B.; Lau, S.; de Boer, H.H. Acute disseminated encephalomyelitis (ADEM) following recent Oxford/AstraZeneca COVID-19 vaccination. Forensic Sci Med Pathol 2021, 1–6. [Google Scholar] [CrossRef]
- Pagenkopf, C.; Südmeyer, M. A case of longitudinally extensive transverse myelitis following vaccination against Covid-19. J Neuroimmunol 2021, 358, 577606. [Google Scholar] [CrossRef]
- Tan, W.Y.; Yusof Khan, A.H.K.; Mohd Yaakob, M.N.; Abdul Rashid, A.M.; Loh, W.C.; Baharin, J.; Ibrahim, A.; Ismail, M.R.; Inche Mat, L.N.; Wan Sulaiman, W.A.; et al. Longitudinal extensive transverse myelitis following ChAdOx1 nCOV-19 vaccine: a case report. BMC Neurol 2021, 21, 395. [Google Scholar] [CrossRef] [PubMed]
- Notghi, A.A.; Atley, J.; Silva, M. Lessons of the month 1: Longitudinal extensive transverse myelitis following AstraZeneca COVID-19 vaccination. Clin Med (Lond) 2021, 21, e535–e538. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, Y.T.; Tsai, M.J.; Chen, Y.H.; Hsu, C.F. Acute Transverse Myelitis after COVID-19 Vaccination. Medicina (Kaunas) 2021, 57. [Google Scholar] [CrossRef]
- Vegezzi, E.; Ravaglia, S.; Buongarzone, G.; Bini, P.; Diamanti, L.; Gastaldi, M.; Prunetti, P.; Rognone, E.; Marchioni, E. Acute myelitis and ChAdOx1 nCoV-19 vaccine: Casual or causal association? J Neuroimmunol 2021, 359, 577686. [Google Scholar] [CrossRef] [PubMed]
- Singh Malhotra, H.; Gupta, P.; Prabhu, V.; Garg, R.K.; Dandu, H.; Agarwal, V. COVID-19 vaccination-associated myelitis. Qjm 2021. [Google Scholar] [CrossRef] [PubMed]
- Tahir, N.; Koorapati, G.; Prasad, S.; Jeelani, H.M.; Sherchan, R.; Shrestha, J.; Shayuk, M. SARS-CoV-2 Vaccination-Induced Transverse Myelitis. Cureus 2021, 13, e16624. [Google Scholar] [CrossRef]
- Badrawi, N.; Kumar, N.; Albastaki, U. Post COVID-19 vaccination neuromyelitis optica spectrum disorder: Case report & MRI findings. Radiol Case Rep 2021, 16, 3864–3867. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, M.; Ogaki, K.; Nakamura, R.; Kado, E.; Nakajima, S.; Kurita, N.; Watanabe, M.; Yamashiro, K.; Hattori, N.; Urabe, T. An 88-year-old woman with acute disseminated encephalomyelitis following messenger ribonucleic acid-based COVID-19 vaccination. eNeurologicalSci 2021, 25, 100381. [Google Scholar] [CrossRef]
- Vogrig, A.; Janes, F.; Gigli, G.L.; Curcio, F.; Negro, I.D.; D’Agostini, S.; Fabris, M.; Valente, M. Acute disseminated encephalomyelitis after SARS-CoV-2 vaccination. Clin Neurol Neurosurg 2021, 208, 106839. [Google Scholar] [CrossRef]
- Khayat-Khoei, M.; Bhattacharyya, S.; Katz, J.; Harrison, D.; Tauhid, S.; Bruso, P.; Houtchens, M.K.; Edwards, K.R.; Bakshi, R. COVID-19 mRNA vaccination leading to CNS inflammation: a case series. J Neurol 2021, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Alshararni, A. Acute Transverse Myelitis Associated with COVID-19 vaccine: A Case Report. International Journal of Research in Pharmaceutical Sciences 2021, Vol. 12, no. 3, 5. [Google Scholar] [CrossRef]
- McLean, P.; Trefts, L. Transverse myelitis 48 hours after the administration of an mRNA COVID 19 vaccine. Neuroimmunology Reports 2021, 1, 100019. [Google Scholar] [CrossRef]
- Kania, K.; Ambrosius, W.; Tokarz Kupczyk, E.; Kozubski, W. Acute disseminated encephalomyelitis in a patient vaccinated against SARS-CoV-2. Ann Clin Transl Neurol 2021, 8, 2000–2003. [Google Scholar] [CrossRef]
- Fujikawa, P.; Shah, F.A.; Braford, M.; Patel, K.; Madey, J. Neuromyelitis Optica in a Healthy Female After Severe Acute Respiratory Syndrome Coronavirus 2 mRNA-1273 Vaccine. Cureus 2021, 13, e17961. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.J.; Tseng, H.P.; Lin, C.L.; Shiu, J.S.; Lee, M.H.; Liu, C.H. Acute Transverse Myelitis Following COVID-19 Vaccination. Vaccines (Basel) 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Khan, E.; Shrestha, A.K.; Colantonio, M.A.; Liberio, R.N.; Sriwastava, S. Acute transverse myelitis following SARS-CoV-2 vaccination: a case report and review of literature. J Neurol 2021, 1–12. [Google Scholar] [CrossRef]
- Fitzsimmons, W.; Nance, C.S. Sudden Onset of Myelitis after COVID-19 Vaccination: An Under-Recognized Severe Rare Adverse Event. 2021.
- Ozgen Kenangil, G.; Ari, B.C.; Guler, C.; Demir, M.K. Acute disseminated encephalomyelitis-like presentation after an inactivated coronavirus vaccine. Acta Neurol Belg 2021, 121, 1089–1091. [Google Scholar] [CrossRef]
- Erdem, N.; Demirci, S.; Özel, T.; Mamadova, K.; Karaali, K.; Çelik, H.T.; Uslu, F.I.; Özkaynak, S.S. Acute transverse myelitis after inactivated COVID-19 vaccine. Ideggyogy Sz 2021, 74, 273–276. [Google Scholar] [CrossRef]
- Cao, L.; Ren, L. Acute disseminated encephalomyelitis after severe acute respiratory syndrome coronavirus 2 vaccination: a case report. Acta Neurol Belg 2021, 1–3. [Google Scholar] [CrossRef]
- Sepahvand, M.; Yazdi, N.; Rohani, M.; Emamikhah, M. Cervical longitudinally extensive myelitis after vaccination with inactivated virus-based COVID-19 vaccine. Radiol Case Rep 2022, 17, 303–305. [Google Scholar] [CrossRef]
- Chen, S.; Fan, X.R.; He, S.; Zhang, J.W.; Li, S.J. Watch out for neuromyelitis optica spectrum disorder after inactivated virus vaccination for COVID-19. Neurol Sci 2021, 42, 3537–3539. [Google Scholar] [CrossRef]
- Lotan, I.; Romanow, G.; Levy, M. Patient-reported safety and tolerability of the COVID-19 vaccines in persons with rare neuroimmunological diseases. Mult Scler Relat Disord 2021, 55, 103189. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Food and Drug Administration. The report of adverse effects after COVID-19 vaccines in Taiwan. Available online: https://www.fda.gov.tw/tc/includes/GetFile.ashx?id=f637814781667990040&type=2&cid=39989 (accessed on.
- Huang, C.T.; Hsu, S.Y.; Wang, C.H.; Tseng, W.J.; Yang, C.Y.; Ng, C.J.; Warkentin, T.E.; Cheng, M.H. Double high-dose immunoglobulin for ChAdOx1 nCov-19 vaccine-induced immune thrombotic thrombocytopenia. Thromb Res 2021, 206, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Bogdanos, D.P.; Smith, H.; Ma, Y.; Baum, H.; Mieli-Vergani, G.; Vergani, D. A study of molecular mimicry and immunological cross-reactivity between hepatitis B surface antigen and myelin mimics. Clin Dev Immunol 2005, 12, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Segal, Y.; Shoenfeld, Y. Vaccine-induced autoimmunity: the role of molecular mimicry and immune crossreaction. Cell Mol Immunol 2018, 15, 586–594. [Google Scholar] [CrossRef] [PubMed]
- Weinshenker, B.G.; Wingerchuk, D.M.; Vukusic, S.; Linbo, L.; Pittock, S.J.; Lucchinetti, C.F.; Lennon, V.A. Neuromyelitis optica IgG predicts relapse after longitudinally extensive transverse myelitis. Ann Neurol 2006, 59, 566–569. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, D.G.; Cañete, L.A.Q.; Dos Santos, G.A.C.; de Oliveira, R.V.; Brandão, C.O.; da Cruz, L.C.H., Jr. Neurological symptoms and neuroimaging alterations related with COVID-19 vaccine: Cause or coincidence? Clin Imaging 2021, 80, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, Y.; Ohyama, A.; Kubota, T.; Ikeda, K.; Kaneko, K.; Takai, Y.; Warita, H.; Takahashi, T.; Misu, T.; Aoki, M. MOG Antibody-Associated Disorders Following SARS-CoV-2 Vaccination: A Case Report and Literature Review. Front Neurol 2022, 13, 845755. [Google Scholar] [CrossRef]
- Dams, L.; Kraemer, M.; Becker, J. MOG-antibody-associated longitudinal extensive myelitis after ChAdOx1 nCoV-19 vaccination. Mult Scler 2022, 28, 1159–1162. [Google Scholar] [CrossRef] [PubMed]
- Mumoli, L.; Vescio, V.; Pirritano, D.; Russo, E.; Bosco, D. ADEM anti-MOG antibody-positive after SARS-CoV2 vaccination. Neurol Sci 2022, 43, 763–766. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, V.; Bansal, P.; Arora, S.; Kapila, S.; Bedi, G.S. Myelin Oligodendrocyte Glycoprotein Antibody Disease After COVID-19 Vaccination - Causal or Incidental? Cureus 2022, 14, e27024. [Google Scholar] [CrossRef]
- Garg, R.K.; Malhotra, H.S.; Kumar, N.; Pandey, S.; Patil, M.R.; Uniyal, R.; Rizvi, I. Tumefactive Demyelinating Brain Lesion Developing after Administration of Adenovector-Based COVID-19 Vaccine: A Case Report. Neurol India 2022, 70, 409–411. [Google Scholar] [CrossRef]
- Ballout, A.A.; Babaie, A.; Kolesnik, M.; Li, J.Y.; Hameed, N.; Waldman, G.; Chaudhry, F.; Saba, S.; Harel, A.; Najjar, S. A Single-Health System Case Series of New-Onset CNS Inflammatory Disorders Temporally Associated With mRNA-Based SARS-CoV-2 Vaccines. Front Neurol 2022, 13, 796882. [Google Scholar] [CrossRef] [PubMed]
- Dr. Md, R.; Tasnim, J.; Dr. Md. Biplob, H.; Dr. Beauty, S.; Dr. Subash Kanti, D.; Dr. Md, S. Post Covid19 Vaccination Acute Disseminated Encephalomyelitis: A Case Report in Bangladesh. International Journal Of Medical Science And Clinical Research Studies 2021, 1, 31–36. [CrossRef]
- Nagaratnam, S.A.; Ferdi, A.C.; Leaney, J.; Lee, R.L.K.; Hwang, Y.T.; Heard, R. Acute disseminated encephalomyelitis with bilateral optic neuritis following ChAdOx1 COVID-19 vaccination. BMC Neurol 2022, 22, 54. [Google Scholar] [CrossRef]
- Yazdanpanah, F.; Iranpour, P.; Haseli, S.; Poursadeghfard, M.; Yarmahmoodi, F. Acute disseminated encephalomyelitis (ADEM) after SARS- CoV-2 vaccination: A case report. Radiol Case Rep 2022, 17, 1789–1793. [Google Scholar] [CrossRef]
- Doi, K.; Ohara, Y.; Ouchi, T.; Sasaki, R.; Maki, F.; Mizuno, J. Cervical Transverse Myelitis Following COVID-19 Vaccination. NMC Case Rep J 2022, 9, 145–149. [Google Scholar] [CrossRef]
- Ahmad, H.R.; Timmermans, V.M.; Dakakni, T. Acute Disseminated Encephalomyelitis After SARS-CoV-2 Vaccination. Am J Case Rep 2022, 23, e936574. [Google Scholar] [CrossRef] [PubMed]
- Maramattom, B.V.; Lotlikar, R.S.; Sukumaran, S. Central nervous system adverse events after ChAdOx1 vaccination. Neurol Sci 2022, 43, 3503–3507. [Google Scholar] [CrossRef] [PubMed]
- Al-Quliti, K.; Qureshi, A.; Quadri, M.; Abdulhameed, B.; Alanazi, A.; Alhujeily, R. Acute Demyelinating Encephalomyelitis Post-COVID-19 Vaccination: A Case Report and Literature Review. Diseases 2022, 10. [Google Scholar] [CrossRef] [PubMed]
- Mousa, H.; Patel, T.H.; Meadows, I.; Ozdemir, B. Acute Disseminated Encephalomyelitis (ADEM) After Consecutive Exposures to Mycoplasma and COVID Vaccine: A Case Report. Cureus 2022, 14, e26258. [Google Scholar] [CrossRef] [PubMed]
- Motahharynia, A.; Naghavi, S.; Shaygannejad, V.; Adibi, I. Fulminant neuromyelitis optica spectrum disorder (NMOSD) following COVID-19 vaccination: A need for reconsideration? Mult Scler Relat Disord 2022, 66, 104035. [Google Scholar] [CrossRef]
- Anamnart, C.; Tisavipat, N.; Owattanapanich, W.; Apiwattanakul, M.; Savangned, P.; Prayoonwiwat, N.; Siritho, S.; Rattanathamsakul, N.; Jitprapaikulsan, J. Newly diagnosed neuromyelitis optica spectrum disorders following vaccination: Case report and systematic review. Mult Scler Relat Disord 2022, 58, 103414. [Google Scholar] [CrossRef] [PubMed]
- Kuntz, S.; Saab, G.; Schneider, R. Antibody-Positive Neuromyelitis Optica Spectrum Disorder After Second COVID-19 Vaccination: a Case Report. SN Compr Clin Med 2022, 4, 130. [Google Scholar] [CrossRef]
- Caliskan, I.; Bulus, E.; Afsar, N.; Altintas, A. A Case With New-Onset Neuromyelitis Optica Spectrum Disorder Following COVID-19 mRNA BNT162b2 Vaccination. Neurologist 2022, 27, 147–150. [Google Scholar] [CrossRef]
- Netravathi, M.; Dhamija, K.; Gupta, M.; Tamborska, A.; Nalini, A.; Holla, V.V.; Nitish, L.K.; Menon, D.; Pal, P.K.; Seena, V.; et al. COVID-19 vaccine associated demyelination & its association with MOG antibody. Mult Scler Relat Disord 2022, 60, 103739. [Google Scholar] [CrossRef]
Figure 1.
Spinal MRI: On the 6th day after onset, an intramedullary spotty lesion with T2-hyperintensity at T3 to T4 was showed (red arrows. a: sagittal view. c: axial view). Five months later, the lesion over T3 to T4 was totally resolved on T2 FLAIR images (red arrows. b: sagittal view. d: axial view).
Figure 1.
Spinal MRI: On the 6th day after onset, an intramedullary spotty lesion with T2-hyperintensity at T3 to T4 was showed (red arrows. a: sagittal view. c: axial view). Five months later, the lesion over T3 to T4 was totally resolved on T2 FLAIR images (red arrows. b: sagittal view. d: axial view).
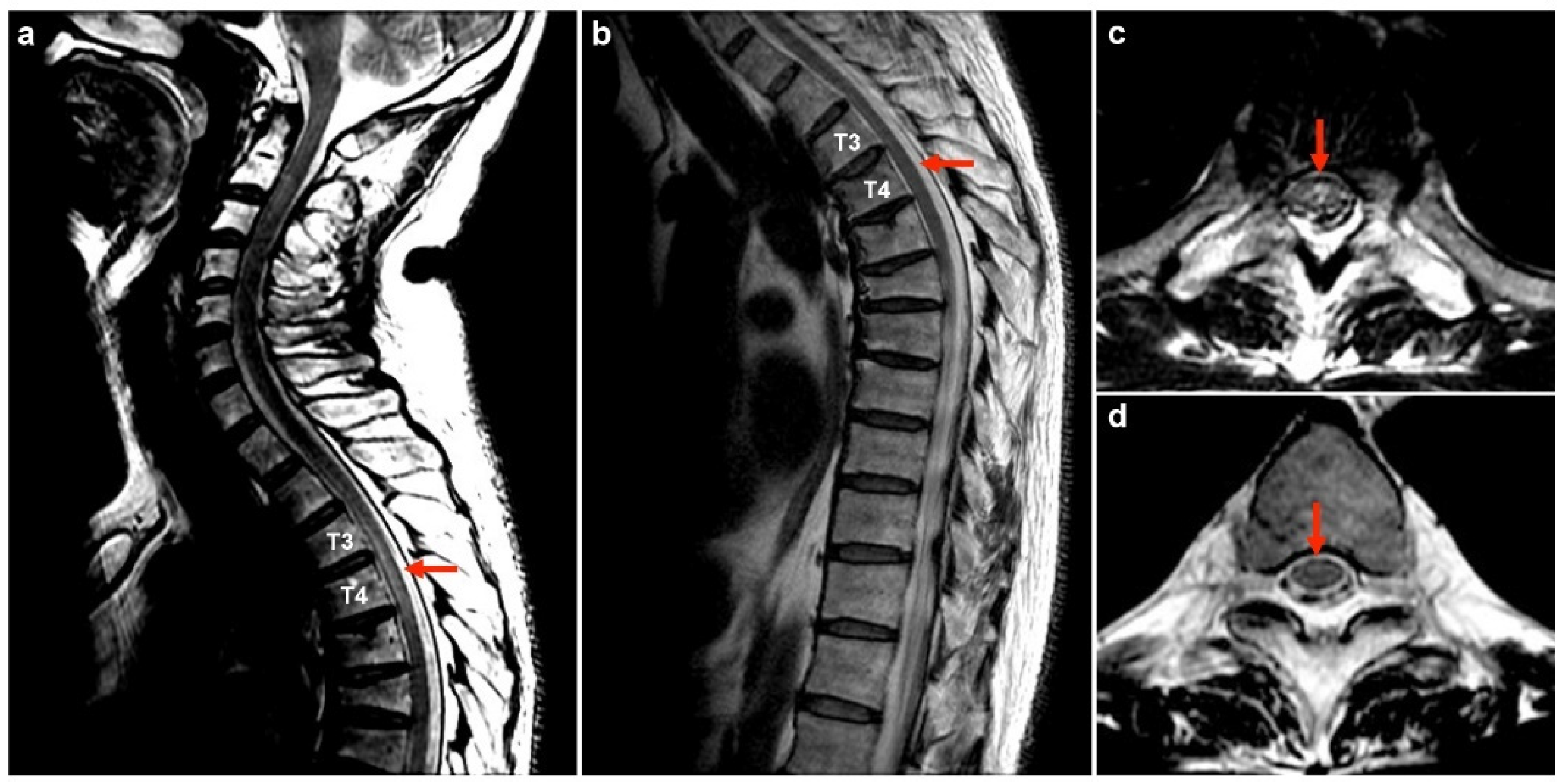
Figure 2.
Brain MRI: Bilateral poorly demarcated T2 FLAIR hyperintensities at brainstem (a, b, c), pulvinar thalami (d), putamen (d), centrum semiovale (e) and subcortical white matters (f) were marked by red arrows in the image.
Figure 2.
Brain MRI: Bilateral poorly demarcated T2 FLAIR hyperintensities at brainstem (a, b, c), pulvinar thalami (d), putamen (d), centrum semiovale (e) and subcortical white matters (f) were marked by red arrows in the image.
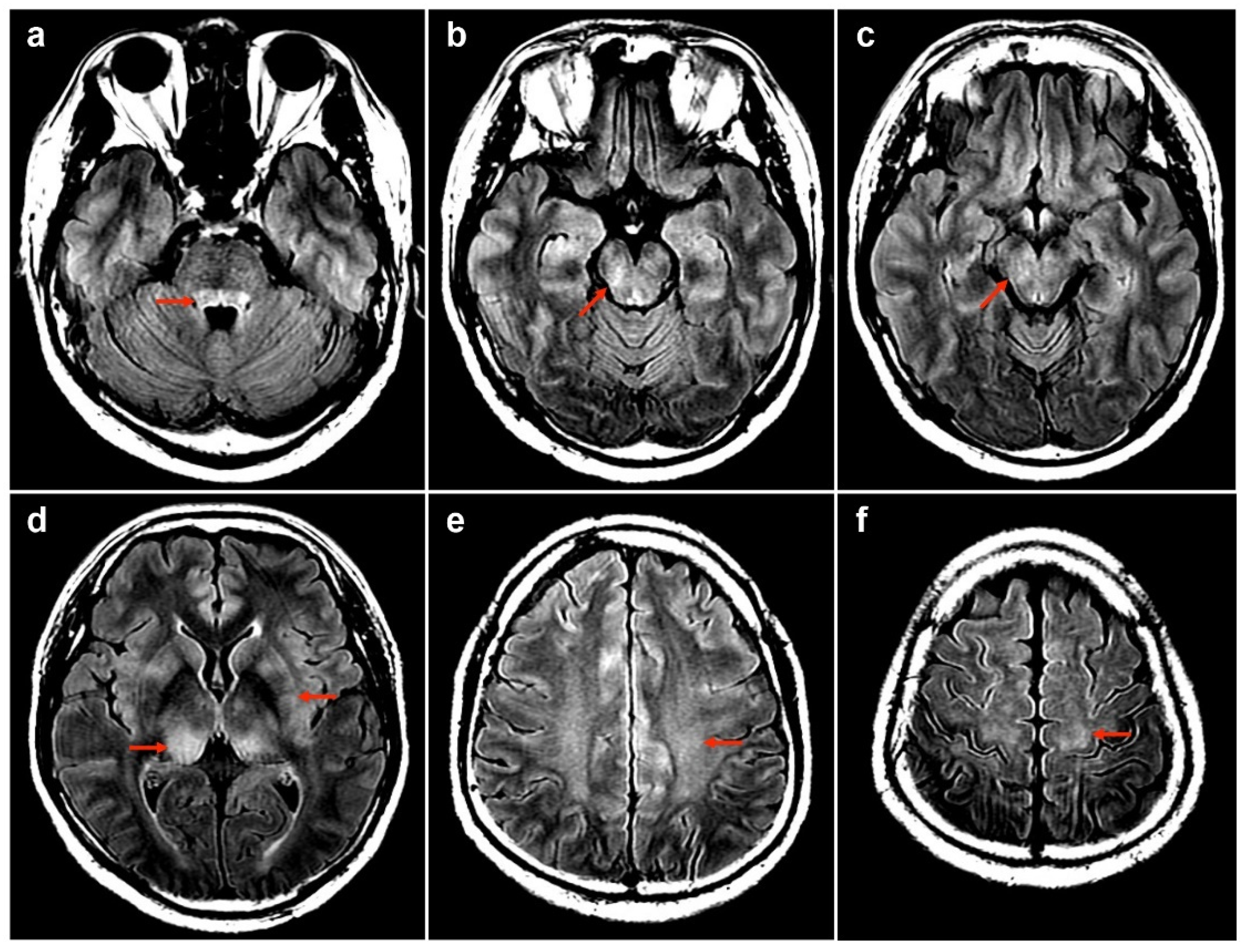
Figure 3.
Cell-based immunofluorescence assay (Euroimmun Lübeck, Germany): Indirect immunofluorescence test was used on HEK-293 cells transfected with plasmids containing MOG. After applying diluted (1:10) patient’s serum, a positive fluorescent reactivity was indicated over cell membrane and cytoplasm in transfected HEK-293 cells.
Figure 3.
Cell-based immunofluorescence assay (Euroimmun Lübeck, Germany): Indirect immunofluorescence test was used on HEK-293 cells transfected with plasmids containing MOG. After applying diluted (1:10) patient’s serum, a positive fluorescent reactivity was indicated over cell membrane and cytoplasm in transfected HEK-293 cells.
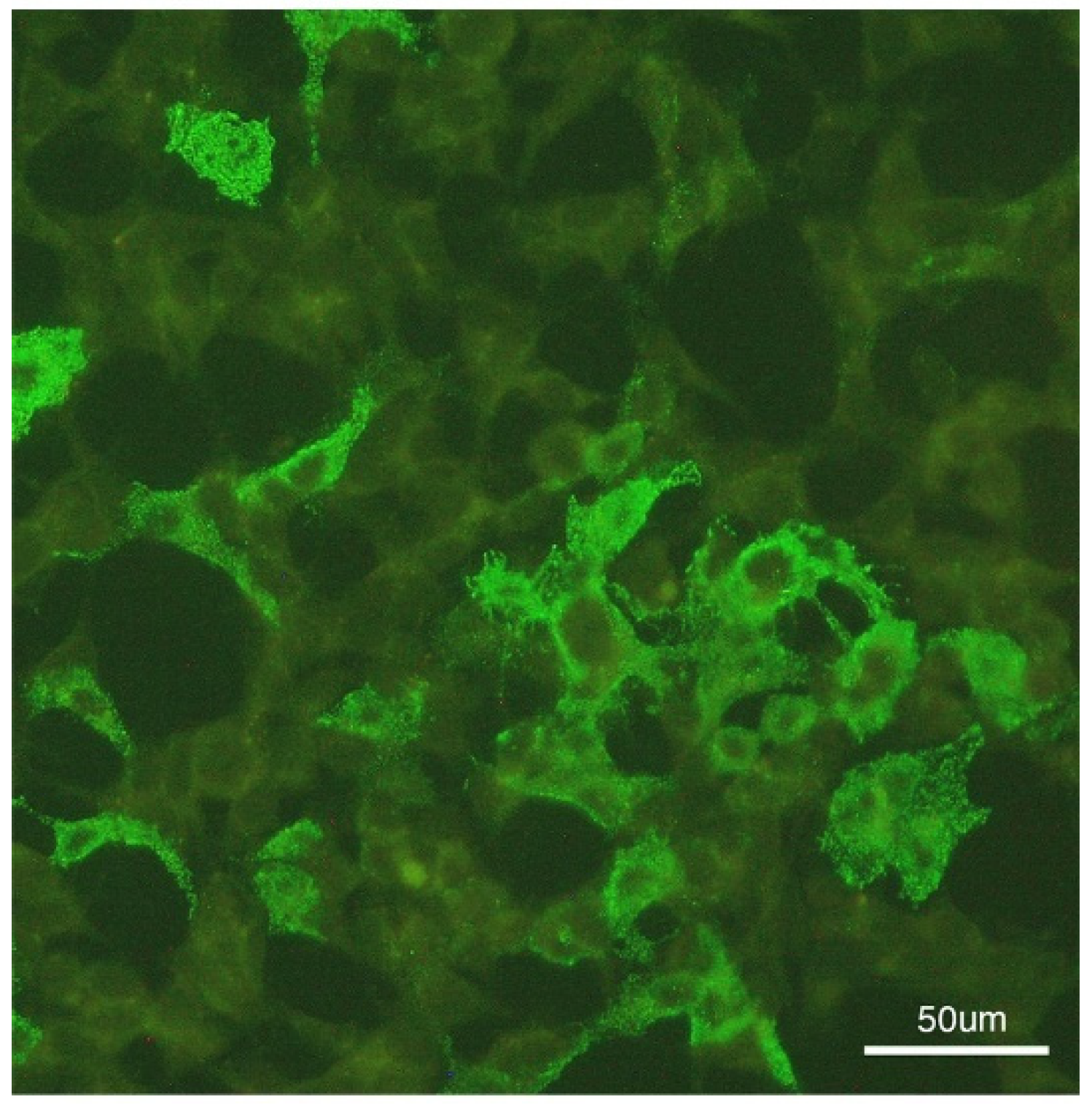
Figure 4.
S-Covid 19 refers to the spike protein of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), retrieved from the Protein Data Bank (PDB) under the accession number 6X29. Aquaporin 4 (AQP4) has a well-documented 3D structure with established structural domains, sourced from the PDB with the accession number 3GD8 (a). Notably, the extracellular loop of the AQP4 transmembrane protein could function as an antigen or be recognized by antibodies. The 3D structure of MOG is unknown (b). The Expasy SIM protein sequence alignment tool was utilized for analysis (https://web.expasy.org/sim/). Additionally, we employed PyMOL for protein structural analysis. The red-highlighted structure represents regions of high similarity between the two proteins.
Figure 4.
S-Covid 19 refers to the spike protein of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), retrieved from the Protein Data Bank (PDB) under the accession number 6X29. Aquaporin 4 (AQP4) has a well-documented 3D structure with established structural domains, sourced from the PDB with the accession number 3GD8 (a). Notably, the extracellular loop of the AQP4 transmembrane protein could function as an antigen or be recognized by antibodies. The 3D structure of MOG is unknown (b). The Expasy SIM protein sequence alignment tool was utilized for analysis (https://web.expasy.org/sim/). Additionally, we employed PyMOL for protein structural analysis. The red-highlighted structure represents regions of high similarity between the two proteins.
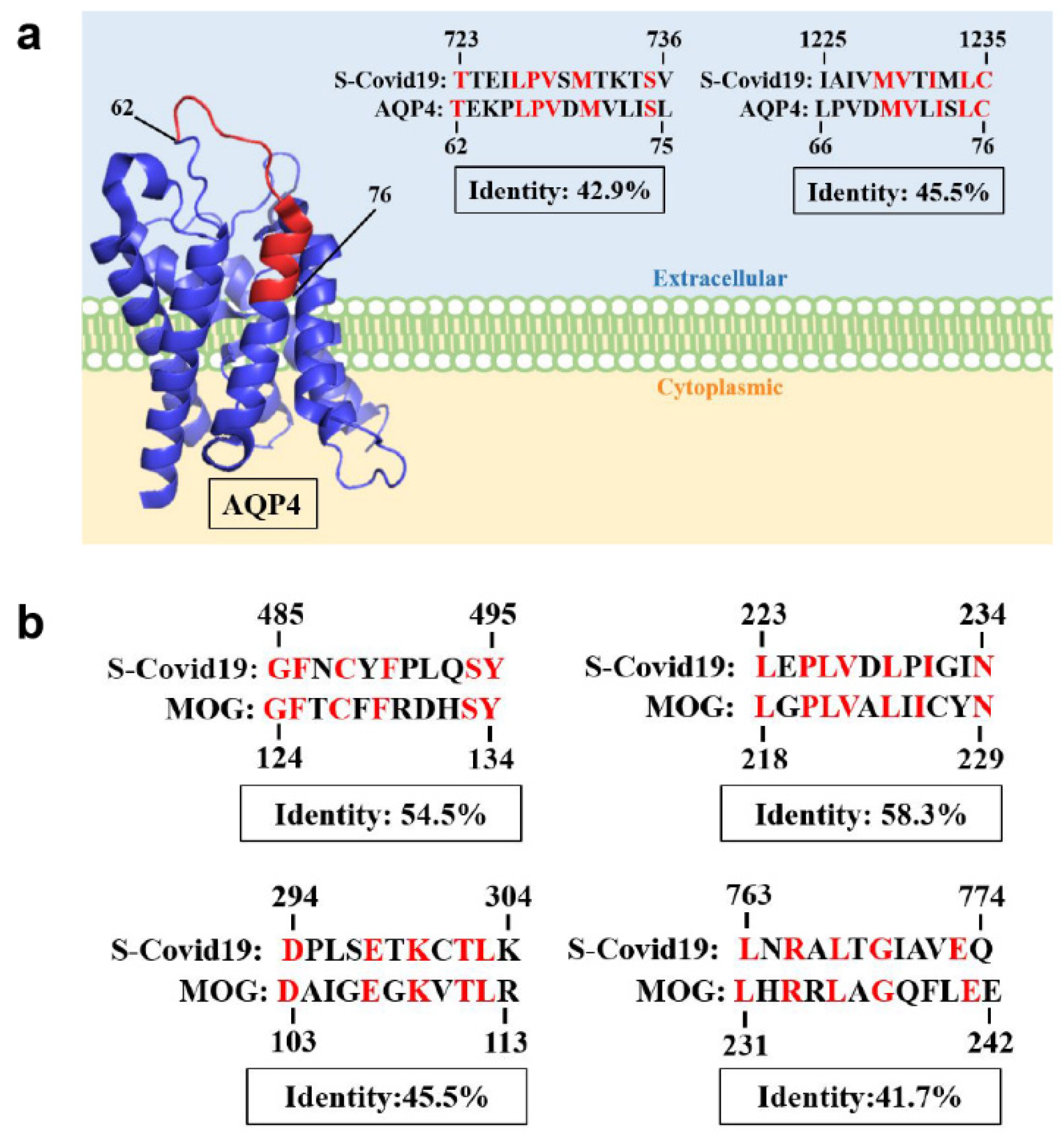

Table 1.
Demographic, clinical features, and laboratory data of 79 patients with CNS IDDs after COVID-19 vaccines.
Table 1.
Demographic, clinical features, and laboratory data of 79 patients with CNS IDDs after COVID-19 vaccines.
| No | Age/sex/PH | Vaccine/ interval (D) |
Dx | Serum | CSF | MRI | Tx | Outcome | Ref | ||||||||
| AQP4 | MOG | OCB | WBC | Lym(%) | Neut(%) | TP | Glu ratio | OCB | Brain | Spine(myelitis) | |||||||
| 1 | 50M/HBV carrier | 1st AZ/13 | MOGAD | - | + | - | 175 | 99 | 0 | 78.1 | 0.47 | NA | Bil thalami, pu, subcortical WM, brainstem | T3-T4 | PT | R | Index case |
| 2 | 45M | 1st AZ/12 | ADEM+ SSM | - | - | NA | 44 | P | NA | N | NA | + | Pons, R MCP, R thalamus; C+ | Cervical, thoracic and conus medullaris;C+ | PT | R | [21] |
| 3 | 63M/DM, HL, IHD, Af | 1st AZ/12 | ADEM | - | - | NA | 2 | NA | NA | 69 | N | + | Bil WM, bil CC, L thalamus, IC, L midbrain, lower pons, R MCP | N | PT + PP | E(D20) | [22] |
| 4 | 45M/atopic dermatitis | 1st AZ/8 | LETM | - | - | NA | 481 | NA | 67 | 140 | 0.43 | - | N | C3-T2 | PT | I | [23] |
| 5 | 25F | 1st AZ/12 | LETM | - | - | NA | NA | NA | NA | 54.6 | 0.55 | - | N | T3-T5, T7-T8, T11-L1 ;C+ in T7-T8 | PT | I | [24] |
| 6 | 58M/DM, pulmonary sarcoidosis | 1st AZ/7 | LETM | - | - | + | 11 | 100 | 0 | 162 | 0.54 | + | NA | C1-T10; C+ in T3-T4, T9-T10 | PT + PE | I | [25] |
| 7 | 41M/DM | 1st AZ/14 | LETM | - | NA | NA | 11 | 100 | 0 | 44.3 | NA | NA | N | T1-T6; C+ | PT | R | [26] |
| 8 | 44F | 1st AZ/4 | SSM | - | - | NA | ↑ | P | NA | 76.7 | NA | - | N | T7-T8, T10-T11; C+ in T7-T8 | PT | R | [27] |
| 9 | 36M | 1st AZ/8 | SSM | - | - | NA | NA | NA | NA | 54 | NA | NA | N | C6-C7; C+ | PT | R | [28] |
| 10 | 44F | 1st Janssen/10 | LETM | - | NA | NA | 227 | 96 | 0 | 43 | N | - | N | C2 to upper thoracic | PT + PE | R | [29] |
| 11 | 34M | 2nd Sputnik V/21 | NMOSD | + | - | NA | ↑ | P | NA | ↑ | NA | - | Lateral, 3rd and 4th ventricles, thalamus, CC, optic chiasma | N | PP | I | [30] |
| 12 | 88F/DM, AD | 2nd Pfizer/29 | ADEM | NA | NA | NA | NA | NA | NA | NA | NA | - | Bil MCPs | NA | PT | R | [31] |
| 13 | 56F/Post-infectious rhombencephalitis | 1st Pfizer/14 | ADEM-like | - | - | - | N | NA | NA | N | N | - | L cerebellar peduncle and L centrum semiovale | NA | Oral steroid | R | [32] |
| 14 | 64M | 1st Pfizer/18 | NMOSD | + | NA | NA | N | NA | NA | N | N | - | CC, L frontal and parietal WM; C- | Cervical to the conus; C+ | PT + PE + RTX | I | [33] |
| 15 | 38M | 1st Pfizer/2 | SSM | NA | NA | NA | NA | NA | NA | 62.1 | N | NA | NA | T11-T12; C+ | NA | NA | [34] |
| 16 | 69F/cervical ca, HL, hypothyroidism | 1st Pfizer/2 | LETM | - | - | + | N | NA | NA | N | N | + | N | C3-C4 to T2-T3 | PT | I | [35] |
| 17 | 19F/atopic dermatitis, depression | 1st Moderna/14 | ADEM+ LETM |
- | - | - | 294 | 91 | 1 | 64.8 | NA | - | Bil hemispheres, pons, medulla, cerebellum; C+ | Medulla to T11; C+ | PT + PE | R | [36] |
| 18 | 46F/c | 1st Moderna/2 | NMOSD | - | NA | NA | NA | NA | NA | NA | NA | NA | N | C6-T2 | PT | R | [37] |
| 19 | 76F/HTN, vit B12 deficiency | 1st Moderna/2 | LETM | - | NA | NA | 15 | NA | 73 | 57.2 | NA | - | N | C2-C5; C+ in C3 | PT | I | [38] |
| 20 | 67F/CAD, CKD, neuropathy | 1st Moderna/1 | LETM | - | - | + | 2 | NA | NA | 56 | 0.61 | + | Nonspecific WM | C1-C3; C+ | PT + PP | I | [39] |
| 21 | 63M | 2nd Moderna/1 | SSM | - | - | NA | 3 | NA | NA | 37 | N | NA | Nonspecific bil corona radiata | Conus medullaris; C+ | IVIG + PT | I | [40] |
| 22 | 46F/Hashimoto’s thyroiditis | 2nd Sinovac/30 | ADEM-like | - | - | NA | 0 | 0 | 0 | 45 | NA | - | L thalamus, bil corona radiata, L diencephalon, R parietal cortex | NA | PT | R | [41] |
| 23 | 78F/DM, HTN, breast ca | 2nd Sinovac/21 | LETM | - | - | NA | 2 | NA | NA | 56 | 0.69 | - | N | C1-T3 | PT | I | [42] |
| 24 | 24F | 1st Sinopharm/14 | ADEM | - | - | - | 51 | NA | NA | NA | NA | - | Bil temporal | NA | IVIG | I | [43] |
| 25 | 71M/DM, HTN, IHD | 1st Sinopharm/5 | LETM | - | - | NA | 0 | 0 | 0 | N | N | - | N | Cervico-medullary junction to C3 | PT | I | [44] |
| 26 | 50F | 1st inactivated/3 | NMOSD | + | - | NA | 31 | NA | NA | N | N | - | Area postrema , bil hypothalamus | N | PT | I | [45] |
| 27 | 65M | 1st AZ/8 | LETM | - | - | NA | N | NA | NA | 70 | NA | - | NA | C4-C6 | PT | R | [52] |
| 28 | 68F/HTN, pancreatic ca | 2nd Moderna/14 | MOGAD | - | + | NA | 0 | 0 | 0 | 32 | NA | + | R lateral pons, trigeminal nerve, MCP | NA | PT | I | [53] |
| 29 | 59M | 1st AZ/14 | MOGAD | - | + | NA | 110 | NA | NA | 625 | N | + | N | T7-L1 | PT + PE | I | [54] |
| 30 | 45M/allergic asthma | 1st AZ/7 | MOGAD | - | + | NA | 43 | NA | NA | 40.6 | N | - | Bil subcortical and gray-white matter | T10-conus | PT | I | [55] |
| 31 | 26M | 1st AZ/20 | MOGAD | - | + | NA | 184 | NA | NA | 88 | NA | - | Bil MCPs, pons | C3-C6 | PT | I | [56] |
| 32 | 56F/HTN | 1st AZ/2 | ADEM-like | NA | NA | NA | NA | NA | NA | NA | NA | NA | L parietal WM, body of CC | NA | Oral steroid | I | [57] |
| 33 | 81M | 1st Moderna/13 | ADEM | NA | - | NA | 69 | 83% | NA | 52 | N | NA | R dorsal medulla, L pons, midbrain, thalami | NA | PT + IVIG + PP | E(D26) | [58] |
| 34 | 63F/HL, hypothyroidism | 1st Pfizer/7 | NMOSD | + | - | NA | 33 | 91% | NA | 57 | NA | - | L thalamus | T6-T12 | PT + PP | R | |
| 35 | 54F/ITP | 2nd Moderna/3 | NMOSD | + | - | NA | 26 | 86% | NA | 71 | NA | - | N | T2-T9 | PT | I | |
| 36 | 55M | 1st mRNA/21 | ADEM | NA | NA | NA | 200 | 95% | NA | 75 | N | NA | Bil WM | NA | PT | R | [59] |
| 37 | 36F | 1st AZ/14 | ADEM | - | - | + | 59 | NA | NA | 40 | N | + | Subcortical WM, PIC, pons and L MCP | N | PT | R | [60] |
| 38 | 37M | 1st Sinopharm/30 | ADEM | NA | NA | NA | 2 | NA | NA | 56 | 0.61 | - | L cerebral peduncle, bil pons, medulla | N | PT | R | [61] |
| 39 | 27F/Rectovaginal fistula | 2nd Pfizer/4 | LETM | - | - | NA | 7 | NA | NA | 43 | N | - | N | C5-C7 | PT | I | [62] |
| 40 | 61F/HTN, anxiety | 1st Pfizer/5 | ADEM | NA | - | NA | N | NA | NA | 61 | N | - | Deep WM, brainstem, cerebellum | N | PT + IVIG | I | [63] |
| 41 | 64M | 1st AZ/10 | ADEM | - | - | NA | 25 | P | NA | NA | N | NA | Bil mesial temporal, hippocampus, MCPs | NA | PT + PP + RTX | R | [64] |
| 42 | 64M | 2nd AZ/20 | ADEM+ SSM | - | - | NA | N | NA | NA | N | N | NA | Bil perirolandic cortex, corona radiata | T8-T9 dorsal | PT + IVIG + RTX | I | |
| 43 | 46M | 1st AZ/5 | ADEM + LETM | - | - | NA | 63 | NA | NA | 52 | N | NA | Bil MCP, pontine tegmentum, R paramedian medulla, L thalamocapsular | LETM | PT + PE | I | |
| 44 | 42F | 1st AZ/5 | ADEM-like | - | - | NA | N | NA | NA | N | N | NA | R temporal | NA | Oral steroid | R | |
| 45 | 56F | 1st AZ/10 | ADEM-like | NA | NA | NA | 1 | 16% | 20% | ↑ | N | NA | Subcortical WM, basal ganglia | NA | PT | R | [65] |
| 46 | 44F/HL, hypothyroidism, renal stone, anxiety | 1st mRNA/6 | ADEM+ LETM |
- | NA | NA | 105 | NA | NA | 98 | N | - | Multifocal PV lesions; C+ in L frontal WM | C3-C4 to thoracic with sparing C5-C6; C+ in T7-T8 | PT + PP | I | [66] |
| 47 | 70F | 3rd Sinovac/7 | NMOSD | + | NA | NA | N | N | N | N | N | - | NA | C1-C7 and T1-T3 | PT + PE + CP | E(M2) | [67] |
| 48 | 26F | 1st Sinovac/10 | NMOSD | + | NA | NA | N | N | N | N | N | - | N | C4-C5 | PT + PE + RTX | I | [68] |
| 49 | 46F | 1st AZ/10 | NMOSD | + | NA | NA | N | N | N | N | N | - | R lateral medulla, PV | C2-C3 | PT +AZT | I | |
| 50 | 80M | 2nd Pfizer/2 | NMOSD | + | + | NA | 39 | 93% | NA | N | N | - | N | T3-T10 | PT + PE + MMF | I | [69] |
| 51 | 43F | 2nd Pfizer/1 | NMOSD | + | - | NA | 6 | NA | NA | 40.1 | N | + | R ON, R periatrium, L crus cerebri | C1 to mid-thoracic | PT + PE + RTX | R | [70] |
| 52 | 29F | 1st AZ/11 | MOGAD | NA | + | NA | 0 | NA | NA | 18 | N | - | Long intraorbital segment of R ON | NA | PT + PP | NA | [71] |
| 53 | 26F | 1st Covaxin/11 | LETM | - | - | NA | 207 | NA | P | 95.8 | N | NA | NA | C2-L1 | PT + PP | NA | |
| 54 | 54F | 1st AZ/14 | ADEM-like | - | - | NA | 8 | P | NA | 77 | N | NA | CC, PV, subcortical WM, infratentorial | NA | PT + PP | NA | |
| 55 | 44M | 1st AZ/7 | MOGAD | NA | + | NA | 130 | P | NA | 38 | N | NA | NA | Cervical and dorsal cord, conus | PT + PP | NA | |
| 56 | 50F | 1st AZ/28 | SSM | - | - | NA | 2 | P | NA | 28 | N | NA | NA | C6 | PT | NA | |
| 57 | 39M | 1st AZ/14 | MOGAD | NA | + | NA | NA | NA | NA | NA | NA | NA | Long intraorbital segment of R ON | NA | PT | NA | |
| 58 | 54M | 1st AZ/14 | MOGAD | NA | + | NA | NA | NA | NA | NA | NA | NA | R pons | N | PT | NA | |
| 59 | 34M | 1st AZ/1 | ON | - | - | NA | 2 | P | NA | 26 | N | NA | R ON | NA | PT | NA | |
| 60 | 35M | 1st AZ/9 | MOGAD | NA | + | NA | 58 | P | NA | 47.4 | N | NA | Midbrain, pons, L MCP, PICs, thalamus, bil centrum semiovale | Cervical to conus | PT | NA | |
| 61 | 20F | 1st AZ/3 | ADEM-like | - | - | NA | NA | NA | NA | NA | NA | NA | Pericallosal, callososeptal, PV, fronto-parietal | NA | PT | NA | |
| 62 | 31M | 1st AZ/14 | LETM | - | - | NA | 370 | NA | P | 174 | N | NA | NA | Cervico-dorsal long segment | PT + PP + RTX | NA | |
| 63 | 20F | 1st Covaxin/1 | ADEM+ SSM |
- | - | NA | 8 | P | NA | 24.9 | N | - | Juxtacortical | C5 | PT + PP | NA | |
| 64 | 45F | 1st AZ/21 | MOGAD | NA | + | NA | 2 | P | NA | 52.3 | N | + | Bil ON | N | PT + PP | NA | |
| 65 | 33F | 1st AZ/14 | MOGAD | NA | + | NA | 105 | P | NA | 28.12 | N | NA | Bil fronto-parietal | NA | PT | NA | |
| 66 | 53F | 2nd AZ/1 | ADEM+ LETM |
- | - | NA | 6 | P | NA | 54.2 | N | NA | Bil subcortical, PV WM, insular, cerebellum, brainstem | C5-C7 and T6-T7 | PT | NA | |
| 67 | 38M | 2nd AZ/6 | ADEM-like | - | - | NA | 6 | NA | NA | 67.8 | N | NA | L MCP, R corona radiata | NA | PT | NA | |
| 68 | 30M | 1st AZ/14 | ADEM+ ON | - | - | NA | 4 | 50 | NA | 26.8 | N | + | Bil subcortical lesions, bil ON | NA | PT + PP + RTX | NA | |
| 69 | 30F | 1st AZ/15 | ADEM+ SSM |
- | - | NA | 4 | NA | NA | 36 | N | + | CC | C3 | PT + PP + MMF | NA | |
| 70 | 36M | 2nd AZ/32 | MOGAD | NA | + | NA | 720 | 80 | NA | 144.4 | N | NA | Bil trigeminal n, pons | Obex to conus | PT + PP | NA | |
| 71 | 27F | 1st AZ/8 | ADEM-like | - | - | NA | Clear | NA | NA | 27.7 | N | NA | Bil PV WM | N | PT | NA | |
| 72 | 60M | 2nd AZ/14 | ADEM | - | - | NA | 9 | 90 | NA | 68.3 | N | - | R pons, midbrain, temporal, parietal, CC | NA | PT + MMF | NA | |
| 73 | 23F | 2nd AZ/7 | ADEM+ LETM |
- | - | NA | NA | NA | NA | NA | NA | - | R frontal horn and bil lateral ventricles | C2-C5 and T4 myelitis | PT | NA | |
| 74 | 40M | 1st AZ/10 | MOGAD | NA | + | NA | 8 | 100 | 0 | 32 | N | + | Pons, bil thalami and R frontal cortex | C4-T3 | PT + MMF | NA | |
| 75 | 45M | 1st AZ/10 | MOGAD | - | + | NA | 44 | 44 | NA | 90.9 | N | NA | Brainstem, supratentorial | Cervicodorsal cord | PT + PP | NA | |
| 76 | 34F | 2nd AZ/36 | NMOSD | + | - | NA | 1 | NA | NA | 15.3 | N | - | Dorsal aspect of medulla | NA | PT + PP + RTX | NA | |
| 77 | 31M | 1st AZ/42 | ADEM+ LETM |
- | - | NA | 32 | 100 | 0 | 49.2 | N | NA | Cervico-medullary junction, R frontal subcortical | C2-C5 | PT + PP + MMF | NA | |
| 78 | 52F | 1st AZ/35 | ADEM-like | - | - | NA | 2 | NA | NA | 40.5 | N | NA | L frontal, insular, midbrain | NA | PT + PP + RTX | NA | |
| 79 | 65F | 1st AZ/42 | NMOSD | + | - | NA | 17 | NA | NA | 49 | N | NA | Frontal subcortical WM | T2-T11 | PT + PP + MMF | NA | |
| Abbreviations: Af: atrial fibrillation. AD: Alzheimer’s disease. AZT: azathioprine. C+: with contrast enhancement. CC: corpus callosum. CKD: chronic kidney disease. CP: cyclophosphamide. DM: diabetes mellitus. E: expired. HBV: hepatitis B virus. HL: hyperlipidemia. HTN: hypertension. I: improvement. IC: internal capsule. IHD: ischemic heart disease. ITP: immune thrombocytopenic purpura. MCP: middle cerebellar peduncle. MMF: Mycophenolate mofetil. N: normal. NA: not available. ON: optic neuritis. P: predominant. PIC: posterior limb of internal capsule. PP: plasmapheresis. PT: steroid pulse therapy. PU: putamen. PV: periventricular. R: complete recovery. RTX: rituximab. WM: white matter. a Oxford-AstraZeneca, marketed as Covishield. A kind of viral vector (chimpanzee adenovirus) vaccine. b Johnson & Johnson’s Janssen, a kind of viral vector (human adenovirus) vaccine. c A kind of viral vector (human adenovirus) vaccine. d Pfizer-BioNTech, marketed as Comirnaty. A kind of messenger RNA vaccine. e A kind of messenger RNA vaccine. f Marketed as CoronaVac. A kind of inactivated vaccine. g Also known as BBIBP-CorV. A kind of inactivated vaccine. h Clinical and MRI features are compatible with ADEM, but without presentation of encephalopathy | |||||||||||||||||
Table 2.
Differences between three major vaccine groups.
| Vaccine types | ||||
| Viral vector (n=49) | mRNA (n=20) | Inactivated(n=10) | P value | |
| Sex, n (%) | 0.027* | |||
| Male | 28 (57) | 6 (30) | 2 (20) | |
| Female | 21 (43) | 14 (70) | 8 (80) | |
| Mean age of onset (S.D.) | 44.3 (12.2) | 58.1 (17.9) | 44.8 (21.8) | 0.002* |
| Doses (1st/2nd/3rd) | 41/8/0 | 13/7/0 | 7/2/1 | 0.042* |
| Post-vaccination onset time (days) | 13.6 | 8.1 | 13.6 | 0.086 |
| Clinical presentations, n (%) | 0.200 | |||
| ADEM | 15 (31) | 6 (30) | 3 (30) | |
| ADEM with myelitis | 14 (29) | 2 (10) | 1 (10) | |
| Pure myelitis | 12 (24) | 6 (30) | 3 (30) | |
| ON | 4 (8) | 0 (0) | 0 (0) | |
| NMOSD | 4 (8) | 6 (30) | 3 (30) | |
| Serum Autoantibodies , n | 0.044* | |||
| Negative | 31 | 14 | 7 | |
| MOG | 14 | 1 | 0 | |
| AQP4 | 4 | 4 | 3 | |
| MOG+AQP4 | 0 | 1 | 0 | |
| CSF, n | ||||
| WBC count | 74.2 | 57.1 | 30.1 | 0.605 |
| Lym predominant (yes/no) | 23/3 | 6/2 | 1/4 | 0.004* |
| Elevated total protein (yes/no)@ | 24/19 | 10/8 | 4/5 | 0.817 |
| CSF/serum glu ratio (<0.6/>0.6) | 4/33 | 0/13 | 0/8 | 0.295 |
| Oligoclonal bands (+/-) | 9/13 | 4/11 | 0/9 | 0.071 |
| Brain MRI lesions, n | ||||
| Cortex (+/-) | 7/33 | 1/16 | 2/5 | 0.329 |
| Deep grey matters (+/-) | 8/32 | 2/15 | 2/5 | 0.598 |
| Subcortical white matters (+/-) | 18/22 | 5/12 | 2/5 | 0.454 |
| Periventricular white matters (+/-) | 16/24 | 6/11 | 1/6 | 0.424 |
| Periaqueductal white matters (+/-) | 3/37 | 0/17 | 0/7 | 0.389 |
| Brainstem (+/-) | 20/20 | 7/10 | 2/5 | 0.532 |
| Gadolinium enhanced (+/-) | 1/9 | 2/9 | 0/5 | 0.562 |
| Spine MRI, n | ||||
| Segments of cord lesions (≥ 3/< 3) | 20/8 | 12/2 | 4/2 | 0.143 |
| Gadolinium enhanced (+/-) | 6/6 | 7/1 | 0/4 | 0.015* |
| Treatment, n | 0.754 | |||
| 1st line immunotherapy | 43 | 17 | 8 | |
| 1st and 2nd line immunotherapy | 6 | 2 | 2 | |
| Outcome, n | 0.762 | |||
| Recovery | 11 | 7 | 2 | |
| Improved | 11 | 11 | 5 | |
| Expired | 1 | 1 | 1 | |
|
*Pearson chi-squared test, p<0.05 # Independent t test, p<0.05 @ Elevated total protein defined as total protein > 45 mg/dL | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



