Submitted:
09 February 2024
Posted:
12 February 2024
You are already at the latest version
Abstract
Some studies investigated the relationship between frequency domain analysis of heart rate variability and the cognitive performance at the Stroop task. We propose a combined assessment also of trunk mobility in 72 healthy women to investigate the relationship between cognitive, cardiac and motor variables based on a principal component analysis. We also assessed the change on this result after an intervention of two months aiming at improving the perception-action link. At baseline, the PCA correctly identified 3 components: one related to cardiac variables, one to trunk motion and one to the performance of Stroop task. After the intervention, only two components were found with trunk symmetry and range of motion, accuracy and time to complete the Stroop task and low frequency heart rate variability aggregated in a single component by PCA. It suggested that this protocol was effective in investigating the embodied cognition and we defined this approach as “embodimetrics”.
Keywords:
embodiment
; heart rate variability
; stroop task
; motor control
1. Introduction
Any comprehensive model of wellness should account for a complex mix of cognitive, affective, behavioral, and physiological factors that contribute to individual differences in health and disease [1]. These individual differences related to blood and pulse pressures are often related to autonomic balance and may influence the cognitive performance [1]. In fact, there are some scientific evidences that highlighted the relationship between vagally mediated heart-rate variability (HRV) and good performance in cognitive tasks that require the use of mental functions [1,2]. HRV is a widely used measure because of its convenience and noninvasive features, and because associated to an activation of the SNS, with a decrease of its high frequency components (and a relevant increase of low frequency ones) when the sympathetic nervous system (SFS) is activated [3,4].
The heart rate variability was also found associated to the performance at the Stroop task [5] that is a task frequently used to represent the ability to manage interfering information at cognitive level [6]. In the Stroop task the subject is asked to verbally read a word, that is the name of a colour, that could be written in the same colour semantically represented by that word (congruent condition) or in another colour (incongruent condition). It is a widely used cognitive test assessing the ability to regulate thoughts and actions in accordance with internally maintained behavioral goals, by the activation of a cognitive control [7].
In the last decades, there has been an increasing diffusion of wearable devices allowing to measure cardiac functions, electrodermal activity, skin temperature and electromyographic activity and also kinematic parameters of trunk movements thanks to embedded inertial sensors [8,9]. More recently, researchers tried to use these wearable devices to investigate the complex relationships between cardiac functions, cognitive aspects and control of movements [10]. In fact, the control of movements requires the management of sensorial feedback together with an internal body representation and often with superior cognitive processes. For example, it has been observed that the higher is the speed at which subjects walk, the higher is the coupling with cardiac rhythm and also with cognitive performances [10].
According to the idea of a comprehensive model, the relationship between physiological factors related to the autonomic system and cognitive performance should also take into account motor and behavioral aspects. But despite this growing body of literature, there were not protocols for testing if in the coupling between HRV and Stroop task performance also the motor control can play a role. Conversely, there are many direct and indirect pathways linking the frontal cortex to autonomic motor circuits responsible for both the sympatho-excitatory and parasympatho-inhibitory effects on the heart [1]. On the other hand, a wide range of inhibitory processes across cognitive, motor, and affective tasks are related to the same brain region: the right prefrontal cortex [1]. It may explain the reason for which the motor awareness can be reduced in presence of a cognitive load [11].
Most of the studies investigate the unidirectional effects of cognitive load on heart rate variability [5,12] but not how the heart rate variability, and also the motor behavior, may affect the cognitive performance. To study the complex system including cognitive, motor and cardiac functions is fundamental to identify the basic components transversally involved in the three systems.
The aim of this study is to propose a simple protocol to identify the principal components of this complex bidirectional system integrating heart, motor control and cognitive functions. According to the literature this protocol is based on the analysis of HRV and its relationship to the results of Stroop task, adding the analysis of trunk rotations, performed using a wearable inertial unit containing a triaxial accelerometer, a triaxial gyroscope and a magnetometer for the measure of the range of motion [8,9]. From a bioengineering point of view a device including inertial sensors for analyzing trunk movements and electrodes recording the cardiac signal for computing the heart rate variability has been proposed. Then, we tested if this sensorized protocol can be sensitive to assess the changes induced by a specific intervention focused on putting attention to the perception-action link that is at the basis of the embodied cognition [13]. Because some previous studies showed gender differences both in trunk accelerations [14] and in the performance at the Stroop task [15], in this first study about this topic, we focused our analysis only on women. Then, because recently a new frontier of data analysis was based on the use of artificial neural network [16], also in the analysis of heart rate variability [17,18], we used an ANN to verify the relationship between principal components and the cognitive outcome.
2. Materials and Methods
2.1. Participants
A sample of 72 healthy women was enrolled in this study (mean age: 49.4±7.7) without any orthopedic, neurological or psychological disease. Signed informed consent was obtained from all participants involved in the study.
2.2. Protocol
Participants were assessed twice. They sit on a comfortable table dressing a sensorized trunk band (Beyond Inertial, Motustech, Rome, Italy) as shown in Figure 1. The device embedded an inertial measurement unit (with a triaxial accelerometer, a triaxial gyroscope and a magnetometer) and electrodes for the assessment of heart signal. The assessment protocol implied the measure of the heart rate variability at baseline for 5 minutes. Then the subject was asked to perform a trunk rotation with the arm flexed on the trunk on the left and on the right side.
The device enabled the measurement of intervals between successive R waves (RR). From these data, Heart Rate Variability (HRV) was assessed by examining the temporal variations within these intervals. HRV analysis was conducted in both the time and frequency domains. In the frequency domain, the analysis involved the decomposition of the signal into distinct frequency components. The designated frequency bands included high-frequency (HRV-HF: 0.15 – 0.4 Hz), low frequency (HRV-LF: 0.04 – 0.15 Hz), and very low frequency (HRV-VLF: 0.01-0.04 Hz). The percentage of the signal in each one of the above frequency domains was analyzed according to the literature reporting that HF is mediated by the vagus nerve of the parasympathetic nervous system (PNS), whereas LF mainly reflects the activity of sympathetic nervous system (SNS) and their balance reflects the balance between these two systems [19]. The inertial measurement unit (IMU) was employed for the quantification of accelerations, angular velocities, and magnetic field orientation within a given system. The acquisition of these measurements served as a precursor for subsequent analyses. Leveraging a sensor fusion algorithm, the IMU facilitates the estimation of the sensor’s orientation within the inertial reference system [20]. The determination of rotation angles corresponding to left and right rotations was feasible through this algorithmic integration. We computed the trunk range of motion (ROM) as the sum of left and right rotation reported in the absolute values, and the symmetry index (SI) as the ratio between the lower and the higher angle multiplied for 100, so to obtain a value of 100% for two equal (symmetric) rotations of the trunk in both the direction [21]. Then, the participants were asked to perform a classical version of the Stroop Task with 15 words and the time to complete the task (TCT) was recorded together with the number of performed errors (ne). Starting from this two parameters we computed the percentage accuracy (ACC) of the subject as (15- ne)/15*100 and the normalized time to complete the Stroop task (NTCT) combining time and ne as follows: TTC*15/(15- ne). After the first assessment subjects were re-assessed after an intervention in which they received a pamphlet with a protocol to follow for 2 months, requiring them to walk outdoor at least for 20 minutes per day breathing through the nose and to improve their perception and body control by moving their barefoot on a soft small ball in upright posture maintained with the knee slightly flexed for 5 minutes per day, alternatively using both feet putting attention to the perception-action link during these actions. All subjects reported the adherence to the protocol.
2.3. Statistical Analysis
Data have been reported in terms of means and standard deviations. Pearson’s coefficient (R) was used to assess the correlation between variables, the relevant regression equations have been reported as y=a*x+b. The main analysis of this study to identify the basic components among the three assessments (cardiac: variables: HRV-VLF, HRV-LF, HRV-HF; motor variables: ROM and SI, and cognitive variables: ACC, NTCT) was a Principal Component Analysis (PCA) performed on the variables assessed at baseline and after the intervention to identify how the data could be aggregated. The number of the components was not previously set, but it was based on a parallel analysis based on the parallel analysis on the scree-plot. The rotational algorithm used was the varimax method. Paired t-tests were used to compare the measured variables before and after the intervention. The percentage changes between after and before intervention were computed as the difference between the post and pre score, divided by the pre-intervention score and multiplied by 100. The effects of changes in HRV and the embodied motor behavior on the change in cognitive performance were evaluated by ARIANNA, that is an ARtificial Intelligent Assistant for Neural Network Analysis, used to predict the modification in cognitive performance at Stroop test after intervention. ARIANNA is ARIANNA is a multilayer perceptron, formed by the input layer, two hidden layers with 5 nodes each one [16]. The architecture of the ARIANNA was that of a feed-forward neural network (FFNN), with data moving in only one direction, from the input nodes through the two hidden layers to the output nodes. The activation function for all the units in the hidden layers and for the output layer was a hyperbolic tangent. The chosen computational procedure was based on online training. The input layers were: trunk ROM, trunk Simmetry Index, HRV-VLF, HRV-LF and HRV-HF, whereas two output were predicted: Stroop Accuracy and Stroop NTCT.
The alpha level of statistically significance was set at 5% for rejecting the null hypothesis for all the performed analyses. The software Jamovi 2.3.21 and IBM SPSS Statistics (version 23) was used for all the above analyses.
3. Results
3.1. Baseline a Post Intervention Parameters
Table 1 shows the parameters measured at baseline and post the intervention. First of all, it is possible to note that HRV-LF did not significantly changed, whereas the change in HRV-HF is significant and mainly related to a change in HRV-VLF, despite the change of this last parameter was not enough for rejecting the null hypothesis. To deeply investigate this aspect, we have analyzed the HF with respect to LF, as reported in Figure 1. Pre-intervention the equation of the regression was: HRV-HF= -0.64*HRV-LF+62, with a Pearson correlation coefficient of R=-0.43 (p<0.001). After intervention, this relationship was still statistically significant, but less strong R=-0.32 (p=0.006), with the regression equation that was: HRV-HF= -0.43*HRV-LF+51.
The cognitive performance improved both in terms of Accuracy and normalized time to complete the task. From a motor point of view, the trunk ROM significantly improved of about 17 degrees, whereas the Symmetry Index did not vary.
3.2. Principal Component Analyses
The Baseline PCA correctly identified three main domains (Table 2): the first component at which mainly contributed Stroop task variables (ACC, NTCT), the second component with the three frequency domains of HRV, and the third component with trunk kinematic variables (ROM and SI). Despite this clear subdivision, the HRV-LF resulted a trasversal parameter, contributing to all the three components.
The protocol and the following PCA were able to assess the changes after the intervention, with a re-arrangement of the parameters. As shown in Table 3, only two components have been identified, one for cognitive and motor control, and another one related to cardiac parameters (HRV-HF and HRV-VLF). The HRV-LF was associated to cognitive and motor control, according to the aim of the intervention of aligning these three systems.
3.3. Artificial Neural Network Analysis
Figure 2 shows the architecture of the artificial neural network ARIANNA. The computed importance assigned to each one of the input layer is reported in Table 4. The change in the Stroop performance was mainly predicted by the changes in HRV-LF (21.4%) and those in trunk movement parameters: ΔROM (23.3%) and ΔSI (19.6%). The accuracy of the ANN in performing the prediction was high as shown in Figure 3 for both the outputs.
4. Discussion
A sensorized quantitative assessment of heart rate variability has often been put in relationship to cognitive performances, in particular with that at the Stroop task (in athletes [22], people with post traumatic stress syndrome [23], and in healthy subjects managing the daily stress [24]) and to motor control (also in terms of range of motion and interoceptive accuracy [25]), but a protocol considering these three domains together was still lacking. For this reason, the first aim of this study was to define a simple protocol to identify the components aggregating heart rate variability, trunk motion variability and the cognition parameters obtained with the Stroop task.
The protocol proposed in our study used a sensorized band worn at trunk level and measuring the temporal distance between R waves and the trunk left and right rotations using an embedded inertial device. This protocol involved a PCA that correctly identified three components related to the above domains: cardio, cognition, motion. As confirmatory analysis we used an approach based on the assessment of weights in the prediction of changes in cognitive performance using an artificial neural network, already used in literature [16].
According to the previous literature [26], the HRV-LF was found associated not only to cardiac parameters but also to cognitive ones [5] and, as we suggested, also to kinematic parameters. In healthy subjects, to perform a symmetric wide rotation not only depends on the kinematic functions but also to the perception of the trunk mid-line [21], to the afferent feedback and to the perception-action link [13].
The second aim was to verify if and how it was possible to measure the alteration of these relationships after a specific intervention focused on the embodiment of sensations and cognition. After this intervention, only two components were identified, one related to high and very low frequencies of heart rate variability, and another one putting together HRV-LF, the parameters related to the Stroop task performance and those related to the execution of symmetric wide trunk rotations.
This result is not surprising. After many years in which cognition and motor control were separately investigated, with a sharp distinction between mind and body, many authors started to criticize this view. Damasio talked about Descartes’ error of dividing mind and body [27], Clark claimed at the need of putting brain, body and world together again in neuroscience [28], and Berthoz defined the brain’s sense of movement [29].
More recently, the 4E theory of cognition proposed that the body is a constituent of the mind, and cognition is strictly related to physiological parameters and performed motor actions [30]. The theory of embodied cognition and, furtherly, the “4E” approach suggested that the cognition does not occur solely in the brain, but is also embodied, embedded, enacted, or extended by way of body structures, functions and processes [30].
According to these recent theories, a recent research reported that the cognitive performance of executive function tasks that evoke attentional control partially depend on the responsiveness of autonomic control parameters that could be assessed by heart rate variability [31].
The results of our PCA were furtherly confirmed by those of the analysis conducted using artificial neural network to assess the weight of the changes in HRV and trunk movements on the changes in the Stroop Task performance. We have used an artificial intelligence tool already used in some different studies [16,32,33]. The input associated to a higher relative importance were the changes in trunk range of motion, trunk movement symmetry and those in HRV-LF. These results confirmed those found by PCA, and were able to provide a high predictability of the observed outcome (as shown in Figure 3) Furthermore, artificial neural network is an emerging approach for identify more complex relationship among variables, especially when those are not simply linear as in this case. For these purposes, the artificial neural network analyses seemed particularly adapted for investigating the parameters extracted by inertial magnetic unit such as that used in this study, as previously done in clinical contexts [32].
De Bartolo and colleagues claimed the need of evaluation methods for a quantitative assessment of cardiac, cognitive and motor interactions that could be helpful in physiological research, sport training of athletes and, more specifically, for rehabilitation purposes [10]. In fact, neurorehabilitation may benefit of an integrated approach not aiming at the separate recovery of specific single functions, but curing and caring the patient as a whole person [34]. Even more, the investigation of this connection and of the brain’s sense of movement are particularly interesting in developmental age [35] when the trunk mental representation could be altered affecting the symmetry of posture and movements [36].
The use of a multimodal assessment based on principal component analysis on heart rate variability and brain data is not new [37,38], but in this study we proposed a combined approach to quantify the level of overlapping of cognitive, motor and cardiac functions. We could define this approach as “embodimetrics” because focused on the assessment of embodiment, as well as psychometrics is the discipline concerning the quantitative measurement of psychological aspects [39].
The results of this study should be read at the light of its limits: only female gender was involved in this study, the adherence to the intervention was verbally reported by participants but not quantitatively assessed, the environment was not taken into account despite it was seen it may act as a selective tuning between different strategies in cognition and motor coupling [40]. Further researchers on this topic should be conducted on the male gender and including other tests assessing cognitive functions. Finally, as previously reported the artificial neural network analysis, despite provide good results in term of accuracy, often lacks of a high reliability [33].
In conclusion, our study using the combined assessment of HRV and trunk mobility identified the level of connection with the cognitive aspects measured by Stroop task, providing a useful approach for measuring how much strong the relationship between cognitive functions, autonomic cardiac functions and body movements is. Then, according to the emerging literature about the embodied cognition [13] and the theory of 4E [30] we have suggested the definition of a new term for defining the field of research within psychometrics concerning the techniques and properties of objective measurements, assessments and analyses related to the latent construct of the embodied cognition and with all the aspect related to the 4E theory: Embodimetrics.
Author Contributions
Conceptualization, A.C.; data acquisition: A.C.; K.S.; M.D.D.; N.G.; methodology, M.D.; software and validation, M.D.; data analysis, M.I.; writing—original draft preparation, M.I.; review and editing, A.C.; K.S.; M.D.D.; N.G.; M.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Santa Lucia Foundation and the Italian Ministry of Health, name of grant: “NEURO-METAVERSE: Application in Neurorehabilitation and Neuroscience of Metaverse Technologies as Virtual Reality and Artificial Intelligence”.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, approved by the Institutional Review Board of Santa Lucia Foundation (CE/PROG.814).
Data Availability Statement
Data are available on motivated requests to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Thayer, J.F.; Hansen, A.L.; Saus-Rose, E.; Johnsen, B.H. Heart rate variability, prefrontal neural function, and cognitive performance: The neurovisceral integration perspective on self-regulation, adaptation, and health. Ann. Behav. Med. 2009, 37, 141–153. [Google Scholar] [CrossRef]
- Thayer, J.F.; Sternberg, E. Beyond heart rate variability: Vagal regulation of allostatic systems. Ann. New York Acad. Sci. 2006, 1088, 361–372. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Gedeon, T. Objective measures, sensors and computational techniques for stress recognition and classification: A survey. Comput. Methods Programs Biomed. 2012, 108, 1287–1301. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Liu, B.; Xie, L.; Yu, X.; Li, M.; Zhang, J. Cerebral and neural regulation of cardiovascular activity during mental stress. Biomed. Eng. Online 2016, 15, S2. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.L.; Liao, S.C.; Gau, S.S. Association between Stroop tasks and heart rate variability features in patients with somatic symptom disorder. J. Psychiatr. Res. 2021, 136, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Lansbergen, M.M.; Kenemans, J.L.; van Engeland, H. Stroop interference and attention-deficit/hyperactivity disorder: A review and meta-analysis. Neuropsychology 2007, 21, 251–262. [Google Scholar] [CrossRef]
- Braver, T.S. The variable nature of cognitive control: A dual mechanisms framework. Trends Cogn. Sci. 2012, 16, 106–113. [Google Scholar] [CrossRef]
- Iosa, M.; Picerno, P.; Paolucci, S.; Morone, G. Wearable inertial sensors for human movement analysis. Expert. Rev. Med. Devices. 2016, 13, 641–59. [Google Scholar] [CrossRef]
- Picerno, P.; Iosa, M.; D’Souza, C.; Benedetti, M.G.; Paolucci, S.; Morone, G. Wearable inertial sensors for human movement analysis: A five-year update. Expert. Rev. Med. Devices 2021, 18 (Suppl. S1), 79–94. [Google Scholar] [CrossRef]
- De Bartolo, D.; De Giorgi, C.; Compagnucci, L.; Betti, V.; Antonucci, G.; Morone, G.; Paolucci, S.; Iosa, M. Effects of cognitive workload on heart and locomotor rhythms coupling. Neurosci Lett. 2021, 762, 136140. [Google Scholar] [CrossRef]
- Kannape, O.A.; Barré, A.; Aminian, K.; Blanke, O. Cognitive loading affects motor awareness and movement kinematics but not locomotor trajectories during goal-directed walking in a virtual reality environment. PLoS ONE 2014, 9, e85560. [Google Scholar] [CrossRef] [PubMed]
- Fuller, D.; Colwell, E.; Low, J.; Orychock, K.; Tobin, M.A.; Simango, B.; Buote, R.; Van Heerden, D.; Luan, H.; Cullen, K.; et al. Reliability and validity of commercially available wearable devices for measuring steps, energy expenditure, and heart rate: Systematic review. JMIR mHealth uHealth 2020, 8, e18694. [Google Scholar] [CrossRef] [PubMed]
- Bridgeman, B.; Tseng, P. Embodied cognition and the perception-action link. Phys. Life Rev. 2011, 8, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Mazzà, C.; Iosa, M.; Picerno, P.; Cappozzo, A. Gender differences in the control of the upper body accelerations during level walking. Gait Posture 2009, 29, 300–303. [Google Scholar] [CrossRef] [PubMed]
- Mekarski, J.E.; Cutmore, T.R.; Suboski, W. Gender differences during processing of the Stroop task. Percept. Mot. Skills. 1996, 83, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Ciancarelli, I.; Morone, G.; Tozzi Ciancarelli, M.G.; Paolucci, S.; Tonin, P.; Cerasa, A.; Iosa, M. Identification of Determinants of Biofeedback Treatment’s Efficacy in Treating Migraine and Oxidative Stress by ARIANNA (ARtificial Intelligent Assistant for Neural Network Analysis). Healthcare 2022, 10, 941. [Google Scholar] [CrossRef] [PubMed]
- Tjolleng, A.; Jung, K.; Hong, W.; Lee, W.; Lee, B.; You, H.; Son, J.; Park, S. Classification of a Driver’s cognitive workload levels using artificial neural network on ECG signals. Appl. Ergon. 2017, 59 Pt A, 326–332. [Google Scholar] [CrossRef]
- Yasumoto, Y.; Yagi, S.; Yana, K.; Nozawa, M.; Ono, T. State classification of heart rate variability by an artificial neural network in frequency domain. In Proceedings of the 2010 Annual International Conference of the IEEE Engineering in Medicine and Biology, Buenos Aires, Argentina, 31 August–4 September 2010; pp. 1401–1404. [Google Scholar]
- Appelhans, B.M.; Luecken, L.J. Heart rate variability as an index of regulated emotional responding, Rev. Gen. Psychol. 2006, 10, 229–240. [Google Scholar] [CrossRef]
- Mahony, R.; Hamel, T.; Pflimlin, J.M. Nonlinear Complementary Filters on the Special Orthogonal Group. IEEE Trans. Autom. Control. 2008, 53, 1203–1218. [Google Scholar] [CrossRef]
- De Bartolo, D.; D’amico, I.; Iosa, M.; Aloise, F.; Morone, G.; Marinozzi, F.; Bini, F.; Paolucci, S.; Spadini, E. Validation of SuPerSense, a Sensorized Surface for the Evaluation of Posture Perception in Supine Position. Sensors 2022, 23, 424. [Google Scholar] [CrossRef]
- Chakraborty, S.; Suryavanshi, C.A.; Nayak, K.R. Cognitive function and heart rate variability in open and closed skill sports. Ann. Med. 2023, 55, 2267588. [Google Scholar] [CrossRef] [PubMed]
- Pyne, J.M.; Constans, J.I.; Wiederhold, B.K.; Jegley, S.; Rabalais, A.; Hu, B.; Weber, M.C.; Hinkson, K.D. Jr, Wiederhold, M.D. Predicting Post-Traumatic Stress Disorder Treatment Response Using Heart Rate Variability to Virtual Reality Environment and Modified Stroop Task: An Exploratory Study. Cyberpsychol Behav. Soc. Netw. 2023, 26, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Yu, J.; Kang, S.; Lee, H.; Dong, S.Y. Effect of Daily Stress on Heart-Rate Variability during Stroop Color Word Task. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2020, 2020, 5976–5979. [Google Scholar]
- Edwards, D.J.; Young, H.; Cutis, A.; Johnston, R. The Immediate Effect of Therapeutic Touch and Deep Touch Pressure on Range of Motion, Interoceptive Accuracy and Heart Rate Variability: A Randomized Controlled Trial With Moderation Analysis. Front. Integr. Neurosci. 2018, 12, 41. [Google Scholar] [CrossRef]
- Mathewson, K.J.; Jetha, M.K.; Drmic, I.E.; Bryson, S.E.; Goldberg, J.O.; Hall, G.B.; Santesso, D.L.; Segalowitz, S.J.; Schmidt, L.A. Autonomic predictors of Stroop performance in young and middle-aged adults. Int. J. Psychophysiol. 2010, 76, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Damasio, A.R. Descartes’ Error: Emotion, Reason and the Human Brain; G. P. Putnam’s Sons: New York, NY, USA, 1994. [Google Scholar]
- Clark, A. Being There: Putting Brain, Body, and World Together Again; MIT Press: Cambridge, MA, USA, 1997. [Google Scholar]
- Berthoz, A. Le Sens du Mouvement; Editions Odile Jacob: Paris, France, 1997. [Google Scholar]
- Carney, J. Thinking avant la lettre: A Review of 4E Cognition. Evol. Stud. Imaginative Cult. 2020, 4, 77–90. [Google Scholar] [CrossRef] [PubMed]
- Mathewson, K.J.; Jetha, M.K.; Drmic, I.E.; Bryson, S.E.; Goldberg, J.O.; Hall, G.B.; Santesso, D.L.; Segalowitz, S.J.; Schmidt, L.A. Autonomic predictors of Stroop performance in young and middle-aged adults. Int. J. Psychophysiol. 2010, 76, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Iosa, M.; Capodaglio, E.; Pelà, S.; Persechino, B.; Morone, G.; Antonucci, G.; Paolucci, S.; Panigazzi, M. Artificial Neural Network Analyzing Wearable Device Gait Data for Identifying Patients With Stroke Unable to Return to Work. Front. Neurol. 2021, 12, 650542. [Google Scholar] [CrossRef]
- Iosa, M.; Benedetti, M.G.; Antonucci, G.; Paolucci, S.; Morone, G. Artificial Neural Network Detects Hip Muscle Forces as Determinant for Harmonic Walking in People after Stroke. Sensors 2022, 22, 1374. [Google Scholar] [CrossRef]
- Iosa, M.; Paolucci, S.; Morone, G. The Future of Neurorehabilitation: Putting the Brain and Body Together Again. Brain Sci. 2023, 13, 1617. [Google Scholar] [CrossRef]
- Iosa, M.; Zoccolillo, L.; Montesi, M.; Morelli, D.; Paolucci, S.; Fusco, A. The brain’s sense of walking: A study on the intertwine between locomotor imagery and internal locomotor models in healthy adults, typically developing children and children with cerebral palsy. Front. Hum. Neurosci. 2014, 8, 859. [Google Scholar] [CrossRef] [PubMed]
- Di Vita, A.; Cinelli, M.C.; Raimo, S.; Boccia, M.; Buratin, S.; Gentili, P.; Inzitari, M.T.; Iona, T.; Iosa, M.; Morelli, D.; et al. Body Representations in Children with Cerebral Palsy. Brain Sci. 2020, 10, 490. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Padial, E.; Mercado, F. In exogenous attention, time is the clue: Brain and heart interactions to survive threatening stimuli. PLoS ONE 2021, 16, e0243117. [Google Scholar] [CrossRef] [PubMed]
- Grässler, B.; Herold, F.; Dordevic, M.; Gujar, T.A.; Darius, S.; Böckelmann, I.; Müller, N.G.; Hökelmann, A. Multimodal measurement approach to identify individuals with mild cognitive impairment: Study protocol for a cross-sectional trial. BMJ Open 2021, 11, e046879. [Google Scholar] [CrossRef] [PubMed]
- Wijsen, L.D.; Borsboom, D.; Alexandrova, A. Values in Psychometrics. Perspect. Psychol. Sci. 2022, 17, 788–804. [Google Scholar] [CrossRef] [PubMed]
- Iosa, M.; Fusco, A.; Morone, G.; Paolucci, S. Walking there: Environmental influence on walking-distance estimation. Behav. Brain Res. 2012, 226, 124–132. [Google Scholar] [CrossRef]
Figure 1.
Percentages of Heart Rate Variability (HRV) in low frequencies (LF, x-axis) and high frequencies (HF, y-axis), pre (black dots) and post (grey dots) intervention, with the relevant regression lines.
Figure 1.
Percentages of Heart Rate Variability (HRV) in low frequencies (LF, x-axis) and high frequencies (HF, y-axis), pre (black dots) and post (grey dots) intervention, with the relevant regression lines.
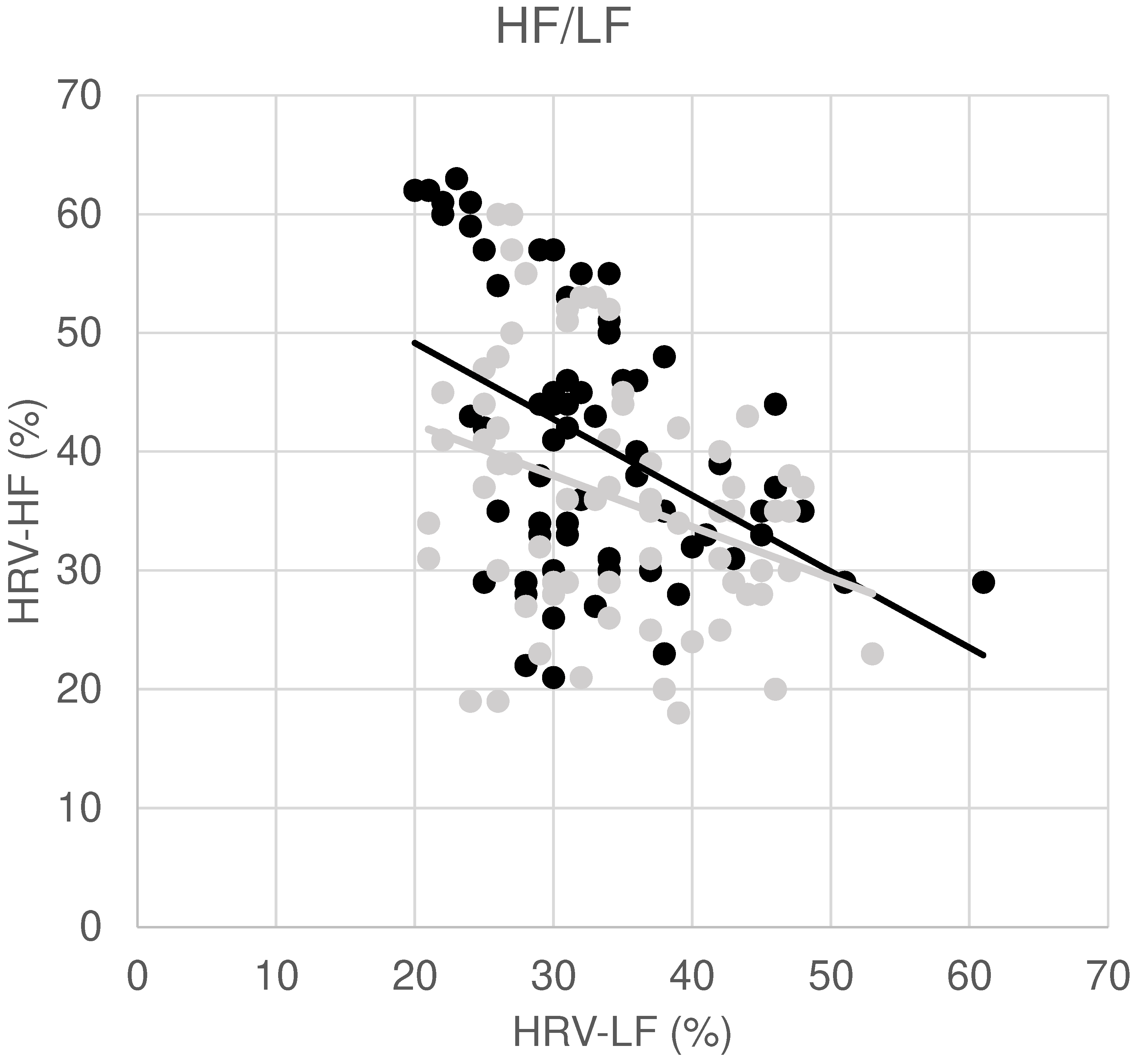
Figure 2.
Architecture of ARIANNA (Artificial Intelligence Assistance for Neural Network Analysis). Δ: change in the parameters post vs. pre, HRV: Heart Rate Variabilit, VLF: very low frequency, LF: low frequency, HF: high frequency, ROM: Range of motion of the trunk, SI: Simmetry Index, NTCT: Normalized time to complete the Stroop task.
Figure 2.
Architecture of ARIANNA (Artificial Intelligence Assistance for Neural Network Analysis). Δ: change in the parameters post vs. pre, HRV: Heart Rate Variabilit, VLF: very low frequency, LF: low frequency, HF: high frequency, ROM: Range of motion of the trunk, SI: Simmetry Index, NTCT: Normalized time to complete the Stroop task.
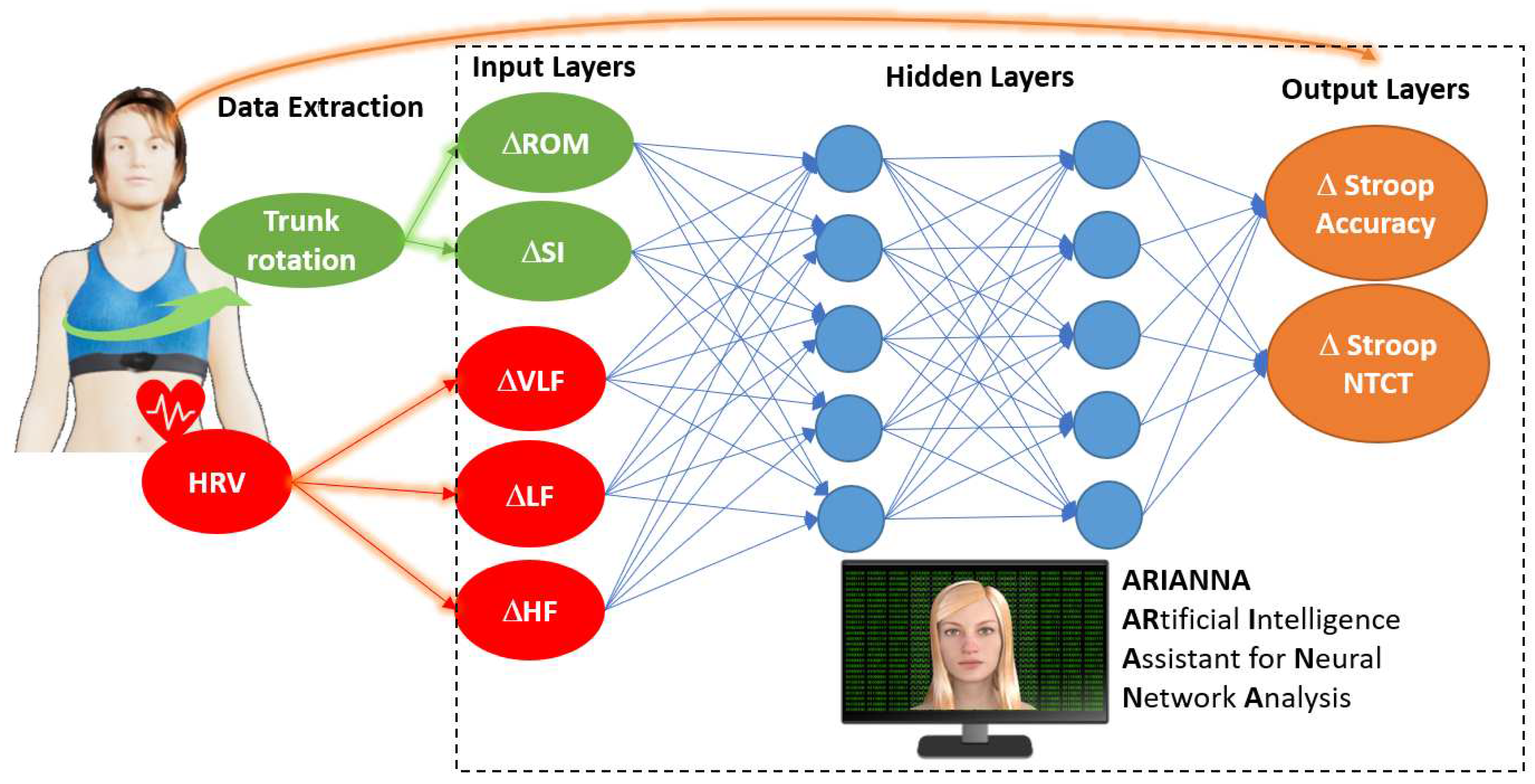
Figure 3.
Predictions of the change in the performance (Δ) at the Stroop Task on the basis of the parameters reported in Table 4. NTCT: Normalized time to complete the task.
Figure 3.
Predictions of the change in the performance (Δ) at the Stroop Task on the basis of the parameters reported in Table 4. NTCT: Normalized time to complete the task.
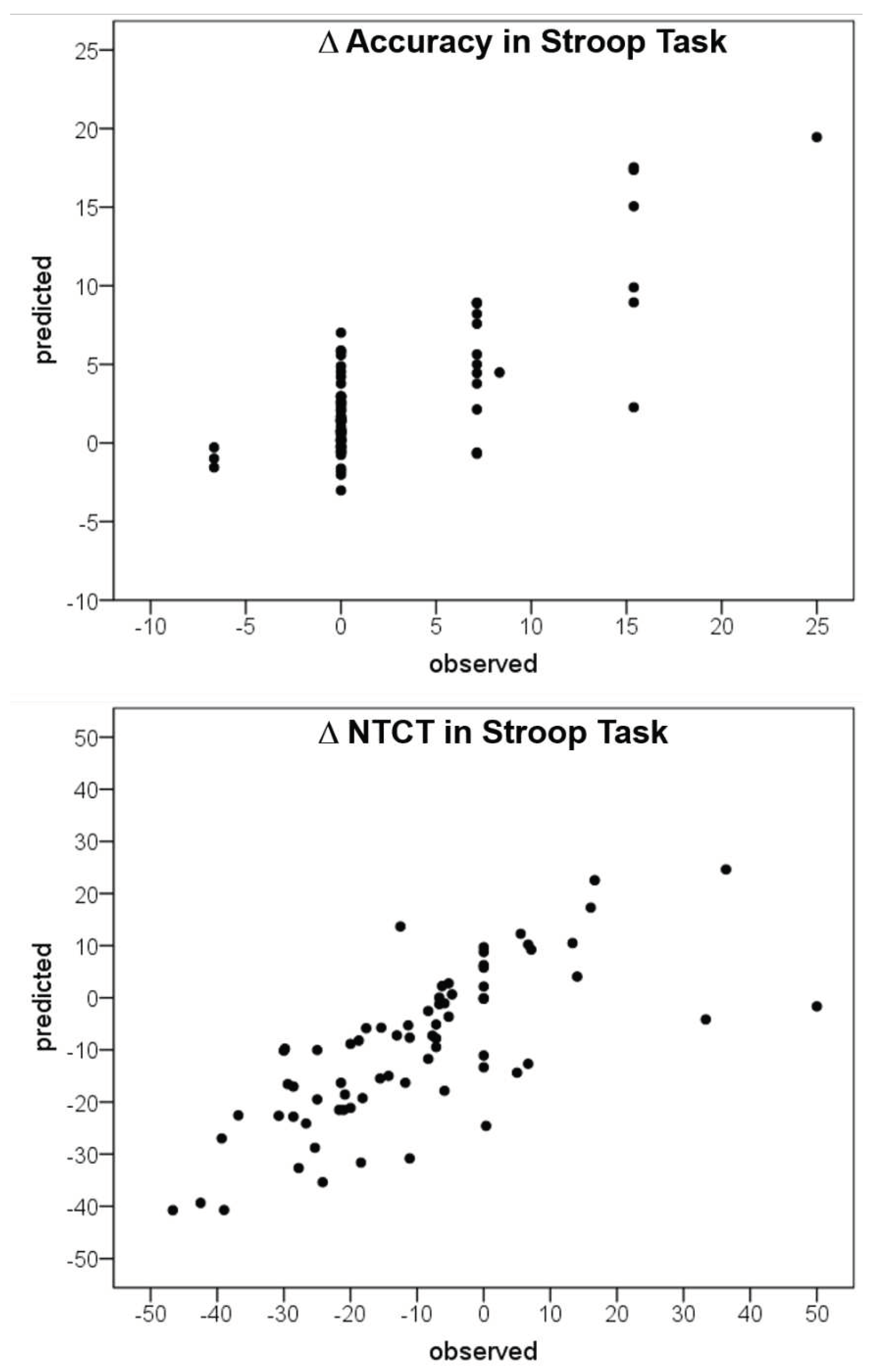

Table 1.
Mean ± standard deviation of the measured variables pre- and post- intervention with the p-value obtained by Wilcoxon rank test (in bold if p<0.05). HRV: heart rate variability, VLF: very low frequency, LF: low frequency, HF: high frequency, ACC: Stroop task accuracy, NTCT: normalized time to complete the Stroop task, ROM: range of motion, SI: symmetry index.
Table 1.
Mean ± standard deviation of the measured variables pre- and post- intervention with the p-value obtained by Wilcoxon rank test (in bold if p<0.05). HRV: heart rate variability, VLF: very low frequency, LF: low frequency, HF: high frequency, ACC: Stroop task accuracy, NTCT: normalized time to complete the Stroop task, ROM: range of motion, SI: symmetry index.
| Variable | Pre | Post | p-value |
|---|---|---|---|
| HRV-VLF (%) | 26.3±10.2 | 29.2±10.7 | 0.096 |
| HRV-LF (%) | 33.1±7.5 | 34.2±7.9 | 0.522 |
| HRV-HF (%) | 40.8±11.1 | 36.2±10.5 | 0.002 |
| HF/LF | 1.3±0.6 | 1.0±0.5 | 0.001 |
| Stroop task NTCT (s) | 18.8±5.2 | 16.4±3.9 | <0.001 |
| Stroop task ACC | 96.6±5.2 | 98.9±2.7 | <0.001 |
| Trunk ROM (deg) | 110.0±21.5 | 127.0±28.0 | <0.001 |
| Trunk SI (%) | 87.4±9.1 | 87.9±10.0 | 0.743 |
Table 2.
Weights of the variables assessed at baseline (pre-intervention) on the components obtained with a principal component analysis (in bold if their absolute value is >0.25).
Table 2.
Weights of the variables assessed at baseline (pre-intervention) on the components obtained with a principal component analysis (in bold if their absolute value is >0.25).
| Variable | Component 1 | Component 2 | Component 3 |
|---|---|---|---|
| HRV-VLF | -0.20 | 0.84 | -0.19 |
| HRV-LF | 0.34 | 0.36 | 0.43 |
| HRV-HF | -0.03 | -0.99 | -0.06 |
| Stroop task NTCT | 0.87 | -0.11 | -0.07 |
| Stroop task ACC | -0.83 | 0.04 | -0.02 |
| Trunk ROM | 0.12 | -0.09 | 0.72 |
| Trunk SI | -0.13 | -0.02 | 0.77 |
Table 3.
Weights of the variables assessed post-intervention on the components obtained with a principal component analysis (in bold if their absolute value is >0.25).
Table 3.
Weights of the variables assessed post-intervention on the components obtained with a principal component analysis (in bold if their absolute value is >0.25).
| Variable | Component 1 | Component 2 |
|---|---|---|
| HRV-VLF | -0.24 | 0.92 |
| HRV-LF | 0.62 | -0.01 |
| HRV-HF | -0.19 | -0.94 |
| Stroop task NTCT | 0.80 | 0.03 |
| Stroop task ACC | -0.53 | 0.05 |
| Trunk ROM | -0.27 | 0.14 |
| Trunk SI | 0.35 | 0.04 |
Table 4.
Results of Artificial Neural Network Analysis in predicting the Stroop Task normalized time to complete the task and accuracy. Δ: change in the parameters post vs. pre, HRV: Heart Rate Variabilit, VLF: very low frequency, LF: low frequency, HF: high frequency, ROM: Range of motion of the trunk, SI: Simmetry Index, NTCT: Normalized time to complete the Stroop task.
Table 4.
Results of Artificial Neural Network Analysis in predicting the Stroop Task normalized time to complete the task and accuracy. Δ: change in the parameters post vs. pre, HRV: Heart Rate Variabilit, VLF: very low frequency, LF: low frequency, HF: high frequency, ROM: Range of motion of the trunk, SI: Simmetry Index, NTCT: Normalized time to complete the Stroop task.
| Input layer parameters | Importance of the input layer in the output prediction | ||
|---|---|---|---|
| Raw Weight | Relative | Normalized | |
| ΔHRV-VLF | 0.191 | 19.1% | 81.9% |
| ΔHRV-LF | 0.214 | 21.4% | 91.8% |
| ΔHRV-HF | 0.166 | 16.6% | 71.4% |
| ΔTrunk ROM | 0.233 | 23.3% | 100% |
| ΔTrunk SI | 0.196 | 19.6% | 84.4% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



