Submitted:
12 February 2024
Posted:
12 February 2024
You are already at the latest version
Abstract
Cadmium (Cd) is a metal with no nutritional or physiological value, but is found in most people because it is a contaminant in nearly all food types. The intestinal absorption rate determines the body burden of Cd because humans lack a physiologic mechanism for excretion of the metal. Most acquired Cd accumulates in the kidneys, in which the Cd content increases through age 50 but falls thereafter. The decline from maximal kidney content is probably due to release of Cd from injured tubular cells into urine and replacement of destroyed nephrons by scar tissue. Chronic kidney disease is diagnosed when the estimated glomerular filtration rate (eGFR) falls below 60 mL/min/1.73 m2, or when albuminuria is present. Albuminuria is defined as an albumin-to-creatinine ratio ≥ 30 mg/g creatinine in women or ≥ 20 mg/g creatinine in men that persists for at least 3 months. Generally, Cd-induced reductions in eGFR are not reversible, and Cd nephropathy may progress to end-stage kidney disease. There is no evidence that elimination of current environmental exposure can reverse Cd nephropathy, and no theoretical reason to believe that such a reversal is possible. This review provides an update of knowledge concerning CKD in population environmentally exposed to Cd. Special attention is devoted to mechanisms of Cd-induced albuminuria concurrently with eGFR reductions, and the difficult challenge of exposure guidelines sufficient to eliminate the risk of Cd-induced CKD is addressed.
Keywords:
albuminuria
; β2-microglobulin
; cadmium
; chronic kidney disease
; GFR
; proteinuria
; receptor-mediated endocytosis
1. Introduction
Cadmium (Cd) is a metal pollutant, found in most food types; as such, dietary exposure to the metal is inevitable for most people [1]. Significant sources of Cd in human diet include rice, potatoes, wheat, and leafy salad vegetables [1,2,3,4,5]. Current evidence indicates that the intestinal absorption of Cd and its transport pathways to kidneys and other targets follow closely those for essential metals, notably iron, zinc, and calcium [1,6]. Genetic linkage studies are consistent with the roles of zinc and iron transporters and proteins of iron homeostasis as determinants of blood and urinary Cd levels [7,8,9], while body iron stores and nutritional status of zinc were found to be inversely related to the body burden of Cd in a meta-analysis [10].
There is also evidence that Cd complexed with phytochelatin (PC) and the metal binding protein metallothionein (MT), denoted respectively as CdPC and CdMT, can be assimilated intact through transcytosis and receptor-mediated endocytosis (RME) [11,12,13]. The CdMT of dietary origin may be targeted to the distal nephrons, especially when proximal tubules are injured [6,14,15].
Other non-workplace exposure sources of Cd are polluted air, passive and active cigarette smoking [16,17,18]. Indeed, Cd was found to be the constituent of a cigarette smoke that contributed the most to chronic ailments associated with smoking [19]. This result reflects a typical feature of a toxicant, like Cd, which persists throughout the lifespan of cells due to a lack of excretory mechanism. Studies in humans and rats showed that Cd was excreted in urine, only when kidney tubular cell died, due to the toxic Cd accumulation [20,21].
In humans, the overall elimination rate of Cd is an extremely slow; only 0.001-0.005% of the body burden is excreted in urine each day [22,23]. The estimated half-life of Cd in the human body varied between 7.4 and 30 years [24,25,26]. In comparison, other cigarette smoke constituent, such as nicotine, can be eliminated completely in less than 3 hours through hepatic xenobiotic metabolism and urinary excretion [27,28,29].
The present review aims to provide an update of knowledge on adverse health outcomes of exposure to environmental Cd, focusing on chronic kidney disease (CKD), which is a progressive disease with high morbidity and mortality, affecting 8-16% of the world’s population [30,31,32]. Special emphasis is given to the mechanisms by which Cd causes albuminuria concurrently with a reduction of glomerular filtration rate (GFR). Understanding the pathophysiologic mechanisms underlying Cd-induced albuminuria is of potential significance, given that the global rising incidence of CKD and the escalating treatment costs necessitate screening for an early warning sign of CKD [33]. In addition, this review highlights the implications of Cd-induced GFR reduction for health risk assessment, and benchmark dose calculation of the body burden of Cd that may carry a negligible health risk. Current exposure guidelines are outdated and do not afford a sufficient health protection.
2. Environmental Cadmium and the Increased Prevalence of Chronic Kidney Disease
CKD is diagnosed when the estimated glomerular filtration rate (eGFR) falls below 60 mL/min/1.73 m2, termed low eGFR, or there is albuminuria that persists for at least 3 months [30,31]. Albuminuria is designated, when the excretion of albumin (Ealb), measured as albumin-to-creatinine ratio (ACR), rises to levels above 20 and 30 mg/g creatinine in men and women, respectively [30,31]. A higher ACR cutoff value is necessary to define albuminuria in women to adjust for gender differences in muscle mass, which is a principal determinant of creatinine excretion (Ecr). This practice simply reflects the fact that women have universally lower muscle mass, and thus lower Ecr, compared to men.
For the same reason as ACR, normalization of Cd excretion to Ecr yields typically higher ECd/Ecr values in women, compared to men of similar age. The ramification of normalization of excretion rate of Cd to Ecr is further discussed in Section 2.4.
2.1. Findings from Systematic Reviews and Meta-Analyses
Doccioli et al. (2024) conducted a systematic review and meta-analysis to evaluate the strength of an association between CKD and Cd exposure [34]. They reported that Cd exposure was associated with increased risk of CKD, only when assessed by eGFR, and the association was more evident for blood than for urinary Cd or dietary exposure [35].
In a previous systematic review and meta-analysis, Jalili et al. (2021) reported that an association of eGFR and urinary Cd was insignificant, but the risk of proteinuria rose 35%, when the top category of Cd dose metrics was compared with the bottom Cd exposure category [35]. In another meta-analysis, Byber et al. (2016) concluded that Cd exposure was not associated with progressive eGFR reductions [36].
Nearly all studies used ACR to define albuminuria, while using ECd/Ecr as an indicator exposure to Cd. However, the Ecr-adjustment, introduces variance to datasets and creates a high degree of statistical uncertainty [37]. In effect, associations of ECd/Ecr with eGFR and Ealb/Ecr (ACR) deemed to be statistically insignificant.
2.2. Exposure Levels of Concern
Dose-responses studies showing Cd exposure levels associated with low eGFR, albuminuria and proteinuria can be found in Table 1.
A study from Thailand (n = 1189) reported 6.2-fold and 10.6-fold increases in risk of low eGFR as urinary Cd excretion levels rose from ≤ 0.37 to 0.38–2.49 and ≥ 2.5 µg/g creatinine, respectively [38]. In a study from China, there was a 2.98-fold increase in risk of elevated albumin excretion, as urinary Cd levels rose from ≤ 0.32 to > 1.72 µg/g creatinine [42]. In a study from Spain, 1.58-fold and 4.54-fold increases in risk of albuminuria were associated with urinary Cd levels > 0.27 and > 0.54 µg/g creatinine, respectively [43].
An association of CKD with Cd exposure was observed in U.S. population studies, known as National Health and Nutrition Examination Surveys (NHANES) [44,45,46,47]. Specifically, increased risk of CKD among U.S. citizens, enrolled in NHANES 1999−2016 was linked to blood Cd levels ≥ 0.6 µg/L and urinary Cd levels ≥ 1 µg/g creatinine.
The median for ECd/Ecr in women enrolled in NHANES 1988–1994 was 0.77 μg/g creatinine, higher than that of men (0.58 μg/g creatinine) [48]. A study from Taiwan, including 977 men and 1470 women (mean age 55), reported a mean urinary Cd concentration was higher in women than men (0.9 vs. 0.7 µg/L) [49]. A study from Swen observed higher blood Cd in women than men of a similar age [50]. In a population-based study of Chinese subjects, aged 2.8 to 86.8 years (n = 1235), urinary Cd levels increased with age, peaking at 50 and 60 years in non-smoking women and men, respectively [51].
Of concern, eGFR decline due to Cd nephropathy has increasingly been observed in both children and adult populations. Lower eGFR values were found to be associated with higher Cd excretion rates in studies from Guatemala [52] and Myanmar [53]. In a prospective cohort study of Bangladeshi preschool children, an inverse relationship between ECd and kidney volume was seen in children at 5 years of age. This was in addition to a decrease in eGFR [54]. ECd was inversely associated with eGFR, especially in girls. In another prospective cohort study, the reported mean for Cd intake among Mexican children was 4.4 µg/d at the baseline and rose to 8.1 µg/d after nine years, when such Cd intake levels showed a marginally inverse association with eGFR [55].
As data in Table 1 indicate, ECd/Ecr values ≥ 0.27-0.32 µg/g creatinine may be sufficient dose levels caused an increase albuminuria excretion and eGFR decline. Thus, eGFR loss and an increased albumin excretion appeared to occur long before ECd/Ecr reached 5.24 μg/g creatinine level at which Eβ2M/Ecr rose to ≥ 300 μg/g creatinine. In theory, for a toxicant with multiple targets, its toxicity threshold level should be based on the most sensitive endpoint [56]. Thus, CKD may serve as a suitable adverse effect, based on which protective exposure guidelines should be formulated (Section 4).
In summary, studies from various countries report disparate levels of urinary and blood Cd, but they are broadly consistent in that they find that urinary Cd levels associated with low eGFR and albuminuria did not exceed 5.24 µg/g creatinine, which was suggested to be the nephrotoxicity threshold level of Cd. This Cd toxicity threshold level was obtained from a risk assessment model that used β2M excretion as a toxic endpoint, detailed in Section 4.
2.3. Methods of Normalization of Cadmium Excretion Rate
For many years, the custom has been to normalize ECd to the excretion rate of creatinine, Ecr. If Vu is the rate of urine flow, ECd and Ecr equal [Cd]uVu and [cr]uVu, respectively, and ECd/Ecr simplifies to [Cd]u/[cr]u. Since these two variables, [cr]u and [Cd]u, are not connected biologically, the ratio does not normalize [Cd]u to a factor that affects ECd. The sole virtue of [Cd]u/[cr]u, as opposed to [Cd]u alone, is that it adjusts [Cd]u for Vu. However, this adjustment introduces a different and arguably comparable source of imprecision, because Ecr is proportional to muscle mass, which varies by a multiple within some populations [57].
ECd/Ccr is determined by calculation using an equation [Cd]u[cr]p/[cr]u, which is algebraically simplified from [Cd]uVu/[cr]uVu/[cr]p, where p = plasma and u = urine; ECd = urinary excretion rate of Cd; Vu = urine flow rate; cr = creatinine [58]. ECd/Ccr is expressed as µg/ L of filtrate.
The GFR is the product of nephron number and mean single nephron GFR, while creatinine clearance (Ccr) approximates the GFR [30,59,60,61]. Because Ccr varies directly with nephron mass, ECd/Ccr depicts the burden of Cd per surviving nephron. Because most or all excreted Cd emanates from injured or dying tubular cells [62]. ECd/Ccr quantifies the severity of the injury due to Cd accumulation at the present time, not the risk of injury in the future.
Timed urine collections are not required. Variation of [cr]u with muscle mass does not affect ECd/Ccr, because [cr]u and [cr]p are uniformly related at any Ccr. At a given tubular cell Cd content, the effect of a reduced nephron number to lower ECd is offset in the calculation by a rise in [cr]p as Ccr falls, and excretion of Cd per intact nephron is accurately depicted [1,62,63,64].
2.5. Demonstrable Dose-Response Relationships
To demonstrate the utility of Ccr-normalization in dose-effect relationship evaluation, data on measurement of Cd exposure and its effects in those resided in an Cd-contaminated area of Thailand [63], are recapitulated in Table 2.
Among 215 study subjects, 33 (15.3%), 131 (61%), and 51 (23.7%) had eGFR > 90, 61–90, and ≤ 60 mL/min/1.73 m2, respectively (Table 2). Relative to the high-eGFR group, the excretion of creatinine tended to rise in the moderate- and the low-eGFR groups. The urinary Cd concentrations (µg/L) and ECd/Ecr in three eGFR groups showed no variation, thereby suggesting a non-association of eGFR decline and Cd exposure, measured as ECd/Ecr. These results in errors were reported in two meta-analyses [35,36].
In comparison, an inverse dose response relationship was observed between with eGFR ECd/Ccr; the mean ECd/Ccr was highest, middle, and lowest in the low-, moderate-, and high-eGFR groups. Those in the low-eGFR group excreted β2M, α1M, albumin, total protein, and Cd at the highest rates. Thus, accurate quantification of Cd nephropathy can only be realized, when excretion rates of β2M, α1M, albumin, total protein, and Cd itself are normalized to Ccr, which is not superfluous, but it eliminates conceptual flaw in the adjustment of excretion rate to creatinine excretion as noted above.
In summary, Ccr normalization is not affected by muscle mass while it corrects for differences in urine dilution and surviving and functioning nephrons. The utility of Ccr-normalized data in mechanistic dissection of albuminuria in Cd nephropathy, and health risk calculation are indicated also in Table 3 and Table 4.
No dose-effect relationships were observed between ECd/Ecr and the prevalence odds of albuminuria and β2-microglobulinuria. There was a 3.5-fold increase in risk of low eGFR in those with Cd excretion rates of 5−9.99 µg/g creatinine, but not the most serverly affected group, compared with Cd excretion rate < 2 µg/g creatinine. In comparison, a clear dose-response relationships were observed for all three adverse outcomes (Table 4). Thus, in subjects with Cd nephropathy, normalization of excretion rates to Ccr demonstrated dose-effect relationships that were not evident with normalization to Ecr.
Based on Ccr-normalized data, all three adverse outcomes of Cd exposure, increases in albumin and β2M excretion rates, and a reduction in eGFR, appeared to occur simultaneously. Among the three outcomes, eGFR was affected the most, while albumin and β2M were similarly affected. Of note, the eGFR effect of Cd was obscured completely, when ECd was normalized to Ecr (Table 2 vs. Table 3). For Ccr-normalized data, respective prevalence odds ratios for low eGFR rose 5.7-fold, 10.3-fold, and 18.1-fold in those with (ECd/Ccr) ×100 values of 2−4.99, 5−9.99 and ≥ 10 µg/L of filtrate, compared with (ECd/Ccr) ×100 values below 2 µg/L of filtrate.
Clearly, Ecr normalization of the excretion rate of Cd has dramatically underestimated the severity of Cd nephropathy. As tubular cells and nephrons are lost, an amount of Cd excreted is expected to be reduced. However, the effect of a reduced nephron number to lower ECd is offset in the Ccr normalization by a rise in [cr]p as Ccr falls. Consequently, excretion of Cd per intact nephron is accurately depicted. These scenarios can be found in Table 2 and Table 4, thereby enabling a crucial dose-effect analysis and toxic risk calculation to be undertaken with a high degree of certainty (Section 4).
3. Impacts of Cadmium on Tubular Protein Reabsorption
Blood perfuses the kidneys at the rate of 1 L per minute, and all renal blood flow is directed through afferent arterioles into glomeruli [66]. In normal physiologic conditions, 20 % of plasma entering the glomerulus is filtered into Bowman’s space. At least 90% of the circulating protein is ultrafilterable, and 99.9% of the filtered load is reabsorbed [67,68,69]. An approximate 40–50 g of protein can be retrieved each day in the proximal tubule of the kidneys, which is divided into segments S1, S2, and S3 [70,71,72,73,74,75,76]. Reabsorption of protein via receptor mediated endocytosis (RME) involving megalin and cubilin occurs mostly in S1, whereas fluid phase endocytosis (FPE) occurs in all three segments [77,78].
Impaired tubular reabsorption of proteins is a known sign of Cd intoxication, which is reflected by an increased excretion of the low-molecular weight proteins, namely retinol binding protein, α1M, and β2M, reviewed in Satarug and Phelps, 2021 [79]. Given that Cd intoxication is known to impair reabsorption of β2M, it was hypothesized that Cd may interfere with reabsorption of albumin as well (Figure 1).
In normal kidney health, filtered β2M is reabsorbed and degraded mostly in S1 and to a lesser extent in S2 [80]. β2M is a constituent of FcRn, which mediates transcytosis of reabsorbed albumin [81,82,83]. There is little evidence for transcytosis of β2M. Albumin reabsorption occurs in S1, S2, and S3 [76,84] and FPE is believed to initiate most transcytosis of albumin [70].
In the circulation, most of Cd (90%) are bound to hemoglobin in red blood cells [85,86,87,88]. The remainder Cd (10%) is found in plasma, associated with albumin, histidine, and other non-protein thiols, including glutathione, cysteinylglycine, homocysteine, and γ-glutamylcysteine [89,90,91,92]. The total plasma concentrations of albumin thiols and non-protein thiols were 0.6 mM and 12−20 µM, respectively [93]. As a principal carrier of plasma Cd, reabsorption albumin complexed with Cd may provide Cd an entry route to PTCs. In an in vitro experiment, cell injury was observed in the rat proximal tubule WKPT-0293 Cl.2 cells, exposed to albumin and β2M complexed with Cd, but the injury was not evident, when cells were exposed to albumin or β2M alone [96].
Because binding of Cd alters the conformational structure of albumin [94,95], Cd-bound albumin probably undergo RME by the megalin-cubilin system and subsequent lysosomal degradation. Cd released during this process may then disrupt megalin homeostasis.
3.1. Cadmium-Induced Albuminuria
Albumin is a globular protein with a molecular weight of 66 kDa, which is synthesized in the liver and secreted into the circulation at a rate of 10–15 g per day [74,75]. Catabolism in muscle, the liver, and the kidney proximal tubular epithelial cells balance synthesis, and homeostasis is continued. Normal plasma concentration of albumin is between 3.5 g/dL and 5 g/dL, and the average half-life in plasma is 19 days [74,75]. Albumin is not normally filtered by glomeruli, due to its large molecular weight and its negative charge. However, by means of transcytosis through endothelial cells and podocyte foot processes, albumin reaches tubular lumen at a rate of 1–10 g per day [97,98].
In an experimental study, Cd was found to disable the cubilin/megalin RME, leading to albuminuria [99]. In addition, Cd diminished expression of megalin and ClC5 channels [100]. Cd may also increase glomerular permeability to albumin, as shown in other studies, where a non-cytotoxic concentration of Cd (1 µM) increased the permeability of human renal glomerular endothelial cells in monolayers and caused the redistribution of the adherens junction proteins vascular endothelial-cadherin and β-catenin [101,102].
In any mechanistic dissection, a clear dose–response relationship must be first established and a population exposed to a wide range of Cd doses is required to meet this requirement. The Mae Sot District in western Thailand appeared to be ideal because it was an area where environmental Cd pollution was endemic [103,104,105]. This geographic area provided a well-circumscribed population of people with the same level of exposure that would enable one to discern the health impact of dietary Cd exposure [106,107,108]. More than 40% of residents aged ≥ 40 years were at risk of Cd-induced toxic injury, and Cd-induced tubular dysfunction [108]. Furthermore, the level of Cd exposure among the Mae Sot residents appeared to be moderate enough to be likely experienced by many populations.
In a logistic regression analysis of data from the Mae Sot residents (Table 4), the risk of albuminuria rose 2.1-7.9% for every one-year increase in age; it also rose 2-fold, and 1.9-fold in smokers and those with hypertension. In comparison, the risk of β2-microglobulinuria was not affected by age, smoking, or hypertension. However, β2-microglobulinnura and albuminuria both were related to the excretion of Cd in a dose-dependent manner. Adjustment for age reduced variance, and tightened the correlations of albumin excretion, β2M excretion and Cd excretion. Consequently, the slope of albumin excretion vs. β2M excretion regressions approached unity. Apparently, these data indicated that Cd affected a single mechanism, leading to reduction of reabsorption of both albumin and β2M. Proposed mechanism of Cd-induced albuminuria is depicted in Figure 2.
In S1, β2M is reabsorbed by RME, involving the apical protein megalin. β2M is then degraded in lysosomes. Albumin is reabsorbed by RME in S1, and FPE in S1, S2 and S3, and mostly returned to the circulation by transcytosis. A small fraction of albumin, reabsorbed through RME, undergoes lysosomal degradation. Cd does not disrupt transcytosis of albumin, but it impairs a single mechanism for RME and degradation of both β2M and albumin. As inferred from the literature reports, it is proposed that Cd disrupts particularly the function of megalin, thereby decreasing reabsorption rates of both proteins [64].
3.2. Fractional Reductions in the Reabsorption of Albumin and β2M
Fractional reductions in reabsorption of albumin and β2M were estimated to assess the functional consequences of renal Cd accumulation on protein reabsorption [64].
In the least affected subjects (eGFR > 90 mL/min/1.73 m2), mean Ealb/Ccr was 8.57 ×10−2 mg/L of filtrate, and mean Eβ2M/Ccr was 5.97 µg/L of filtrate. In the most affected subjects (eGFR < 60 mL/min/1.73 m2), corresponding values of Ealb/Ccr and Eβ2M/Ccr were 70.27 ×10−2 mg/L of filtrate and 411 µg/L of filtrate, respectively. In the latter group, mean eGFR was 46.6 mL/min, or 67.1 L/d/1.73 m2.
Fractional excretion of albumin (FEalb; excretion rate/filtration rate of albumin) can be estimated as (Ealb/Ccr)(eGFR)/(GSCalb)([alb]p])(eGFR), or (0.7027 mg/L of filtrate)(67.1 L/d)/(10-2)(40,000 mg/L)(67.1 L/d) = 0.0018, or 0.18%, if a glomerular sieving coefficient for albumin (GSCalb) of 10−2 and plasma albumin concentration ([alb]p) of 40 gm/L are assumed. This means that mean fractional tubular reabsorption of albumin (FTRalb) was 99.8% even though a rise in absolute albumin excretion was discernible as eGFR fell. If GSCalb is assumed to have been 10−4 instead of 10−2, FEalb was 18%, and FTRalb was 82%.
If GSCβ2M of 1 and [β2M]p of 2.0 mg/L (2000 µg/L) are assumed, mean FEβ2M was (Eβ2M/Ccr)(eGFR)/(GSCβ2M)([β2M]p)(eGFR), or (411 µg/L of filtrate)(67.1L/d)/(1)(2,000 µg/L of plasma)(67.1 L/d) = 0.2055, or 21%. This means that FTRβ2M was 79%.
It is noteworthy that although the reductions are likely to have resulted from the same altered mechanism, fractional reductions in reabsorption of albumin and β2M differed greatly if GSCalb of 10−2 is assumed and were similar if GSCalb of 10−4 is assumed.
3.3. Overall Effects of Cadmium Burden on Tubular Function
To assess the overall impact of Cd on tubular protein reabsorption function, the amounts of albumin and β2M that were reabsorbed through RME, and subjected to catabolism in lysosomes were estimated, assuming glomerular sieving coefficients for albumin (GSCalb) and β2M (GSCβ2M) to be 0.01 and 1, respectively (Table 5).
3.4. Implication of Albumin Reabsorption for Delivery of Cadmium to Proximal Tubules
The evolving concept that proximal tubules reabsorb dozens of grams of albumin per day (Table 5) raises important theoretical possibilities concerning access of Cd to tubular cells. Red blood cells (RBCs) carry at least 90% of circulating Cd [85,86]. In a lysate of rabbit RBCs, the metal associated primarily with hemoglobin and glutathione [87]; in lysates of RBCs from mice pretreated with subcutaneous Cd for six months, the metal was bound to hemoglobin and to a smaller species, probably MT [86,88]. Multiple investigative techniques have shown that Cd binds to specific sites on the globin chains of hemoglobin, represented in Figure 1 [109,110].
The normal mean lifespan of RBCs (and therefore of hemoglobin) is 120 days, but changes in RBC membranes induced by Cd may alter the shape of cells, induce premature hemolysis in the reticuloendothelial system (RES), and thereby shorten cellular lifespan [111,112,113]. When senescent RBCs are destroyed in the RES, heme porphyrin groups are metabolized to bilirubin, which is taken up by circulating albumin [114,115]. Presumably, Cd is simultaneously released from globin chains as they are broken down to their constituent amino acids, and since albumin is so abundant in plasma, it is speculated that it is the principal scavenger of Cd from the RES. Cd-albumin complexes are continuously presented to hepatocytes and proximal tubular cells at high rates of blood flow, and both cell types store Cd that acquired as CdMT [79,116,117]. The internalization of Cd from albumin complexes has been shown [118].
Because binding of Cd binds alters the conformational structure of albumin [119,120], filtered Cd-albumin complexes probably undergo RME by the megalin-cubilin system and subsequent lysosomal degradation. Cd released during this process may then disrupt megalin homeostasis. If the above proposal is correct, then most Cd assimilated from exogenous sources is destined to interact with albumin eventually even if it is bound to hemoglobin initially.
3.5. Summary on the Impact of Cadmium on Protien Reabsorptuve Function
Accumulation of Cd in kidneys reduced receptor-mediated endocytosis of albumin and β2M. Estimated fractional reductions in reabsorptions of albumin and β2M were similar (18 vs 21%), assuming the glomerular sieving coefficients for albumin and β2M to be 10−4 and 0.01, respectively. These impacts of Cd were quantifiable because of the clear dose-effect relationships of Ealb/Ccr, Eβ2M/Ccr, eGFR and the nephron burden of Cd, indicated by ECd/Ccr. In contrast, Ealb/Ecr (ACR), Eβ2M/Ecr and ECd/Ecr were unrelated, thereby precluding dose-response analysis and nullifying the quantification of Cd effects.
4. CKD and the Health Risk Assessment of Environmental Cadmium
In this section human kidney accumulation of Cd and the excretion of Cd by this organ are addressed together with the estimation of the kidney burden of Cd that may carry discernable health risk using eGFR decline as a representative toxic endpoint and benchmark dose method to calculate benchmark dose limit (BMDL) value of Cd.
To derive exposure guidance values, the BMDL has increasingly been used as a replacement of no-observed-adverse effect level (NOAEL) to reflect the point of departure (POD) from population norm [56,121,122]. BMD method corrects some of the shortcomings of the NOAEL [56,123,124,125]
4.1 Measurement of Kidney Burden of Cadmium
Cd accumulation in human kidneys can be found in reports of analysis of post mortem and biopsied samples (Table 6).
It is noteworthy that Australian study measured lung Cd content, which was used to assess contribution of inhalational exposure, where females were found to have higher hepatic and renal cortical Cd levels than males of after adjustment for age and inhalational exposure. Renal cortical Cd content increases progressively to age 50 years and declines sharply thereafter. Peak kidney Cd content was 25.9 µg/g [126].
Hepatic Cd content increased gradually with age without interruption, and it was higher in women than in men. It is speculated that iron depletion due to menstrual losses promoted intestinal Cd absorption in women during the premenopausal years, and we speculate that nephron loss and interstitial scarring due to aging and Cd toxicity caused the observed decline in cortical Cd content after age 50 [132,133].
4.4. Cadmium Excretion and Glomerular Filtration Rate
A paradox is evident in reported relationships of GFR to environmental Cd exposure. Some investigators found that ECd rose with GFR when exposure was low [134,135,136]. On the other hand, many investigators associated tubular dysfunction with low environmental exposure [137,138,139,140], and at least two groups found that GFR fell from normal values as ECd rose minimally [141,142,143].
To reconcile these observations, we speculate that Cd nephropathy begins with a transitory phase in which cell injury is releasing Cd to filtrate but has not yet led to cell death; during that phase, the number of nephrons determines ECd. As Cd begins to destroy cells, ECd increases further even though nephrons drop out and GFR begins to decline. Lending support to this speculation is a recent study in which that eGFR rose with ECd at low kidney burden (ECd/Ccr) < 0.01 µg/L filtrate, and this parameter (eGFR) showed an inverse association with ECd as ECd/Ccr levels > 0.01 µg/L filtrate.
A large body of work shows that GFR fell as a consequence of intense occupational or environmental exposure to Cd. Nephron loss was most extreme in polluted regions of Japan [144], but it was also documented in other Asian countries and in Europe. Progression of CKD often continued after cessation of exogenous exposure [145,146,147].
Reductions in GFR due to Cd nephropathy are sometimes attributed to glomerular injury. Although this inference may be at least partially correct, it is not necessary. Sufficient tubular injury disables glomerular filtration and ultimately leads to nephron atrophy, glomerulosclerosis, and interstitial inflammation and fibrosis [148].
Cd that eludes MT complexation promotes synthesis of ROS that inflict injury. That injury induces autophagy, apoptosis, and necrosis of tubular cells, and it undermines adhesion of cells to one another. Cellular injury also leads to the release of proteins and CdMT into filtrate; compromises reabsorption of filtered proteins and substances co-transported with sodium; and ultimately reduces GFR through destruction of nephrons.
4.3. An Acceptable Kidney Burden of Cadmium?
The kidney burden of Cd that was unlikely to reduce eGFR more than 5% has been determined, for the first time [149] using data from 1189 Thai subjects (493 males and 696 females) mean age of 43.2 years (Figure 3).
The overall percentages of smokers, subjects with hypertension and low eGFR in this group of subjects were 33.6%, 29.4% and 6.2%, respectively. In a conventional dose-response evaluation, low eGFR was associated with higher ECd/Ccr, older age and higher BMI, but not with gender, smoking, or hypertension.
In benchmark dose estimation (Figure 3), the BMDL value of ECd/Ccr × 100 producing a 5% reduction in eGFR was 1.13 µg/L of filtrate in both men and women. These BMDL values can be translatable to Cd excretion rate between 0.01 and 0.02 µg/g creatinine. Because the basic (fundamental) mechanism of Cd toxicity should be the same, the BMDL value for any effect of Cd. In comparison, however, a previous risk analysis conducted on Mae Sot residents, the BMDL values of ECd/Ecr for the β2M endpoint were 6.9 and 8.1 μg/g creatinine in men and women, respectively [108].
Another conventional dose–response analysis of data from 482 non-occupationally exposed persons with a 1250-fold difference in Cd burden and a 667-fold difference in levels of blood Cd, environmental exposure to Cd was confirmed to be closely associated with a declining GFR and albuminuria [150]. When a declining GFR is considered along with albuminuria, the NOAEL equivalent of Cd excretion ranged is 0.01–0.02 µg/g creatinine. Now is the time to acknowledge there is no safe level of Cd exposure.
4.4. Past and Present Health Threat of Environemnatl Cadmium
An outbreak of human cases with severe Cd poisoning, referred to as “itai-itai” disease [151,152], has brought into focus health threat from consumption of rice heavily contaminated with Cd. To safeguard against excessive dietary exposure, a tolerable intake level of Cd, a reference dose (RfD), toxicological reference value, and permissible levels of Cd in foods were determined [121,131,153,154].
Cd is now detectable in virtually all food types, and is becoming a toxic metal pollutant of global public health significance because lifelong Cd exposure has now been identified as one of the contributing factors to the rising prevalence of CKD, diabetes type 2 and many types of cancer worldwide [155,156]. New health guidance values are needed and this Section is aimed to address the practice of health risk estimation of non-occupational exposure situations.
In theory, for a toxicant that affects many organs and tissue, a threshold level of its toxicity and exposure guidelines should be based on the most sensitive endpoint with consideration given to susceptible subpopulations [56]. For any risk assessment practice, the critical elements are accurate measurements of both exposure and adverse effects. The impact of these key elements has revealed by systematic reviews and meta-analyses reporting discrepancies [34,35,36] (Section 2.2 and Section 2.3).
4.4.1. The WHO Exposure Guidelines and the Nephrotoxicity Threshold Level
The Joint FAO/WHO Expert Committee on Food Additives and Contaminants (JECFA) suggested a tolerable monthly intake (TMI) of Cd to be 25 μg per kg body weight per month, equivalent to 0.83 μg per kg body weight per day (58 µg/day for a 70 kg person), and ECd/Ecr of 5.24 μg/g creatinine was adopted as a nephrotoxicity threshold value [153]. Both figures were based on a risk assessment model based solely on Eβ2M/Ecr ≥ 300 μg/g creatinine, as a toxic endpoint or an effect of health concern. Consequently, an increased β2M excretion became the most frequently reported adverse effect of oral Cd exposure.
A rice Cd content of 0.27 mg/kg was associated with kidney and bone damage like those found in itai-itai disease patients [157]. This rice Cd content is below the Codex standard for rice of 0.4 mg/kg [154]. Also, a lifetime Cd intake ≥ 1 g, which is half of the JECFA exposure guideline [253], yielded a 49% increase in mortality from kidney failure, especially among women [158]. These findings cast considerable doubt on the Codex maximally permissible Cd level in rice of 0.4 mg/kg, and the lifetime tolerable Cd intake of 2 g, as suggested by JECFA [153].
Studies from China suggested an upper limit of permissible level of Cd in rice to be 0.2 mg/kg, one half of the Codex standard [159,160,161]. All these estimations relied on ECd/Ecr of 5.24 μg/g creatinine to indicate a toxic Cd accumulation level. Of note, prevalence odds for low eGFR and albuminuria rose at ECd/Ecr values ≥ 0.27-0.32 µg/g creatinine (Table 1). Thus, these indicators of Cd toxicity occurred long before ECd/Ecr reached 5.24 μg/g creatinine level, at which Eβ2M/Ecr rises to ≥ 300 μg/g creatinine. Furthermore, the likelihood of eGFR to fall below 60 mL/min/1.73 m2 rose 4.7-fold, 6.2-fold and 10.5-fold in those who had Eβ2M/Ecr values of 100–299, 300–999, and ≥ 1000 μg/g creatinine, respectively [162]. Because eGFR values ≤ 60 mL/min/1.73 m2 are indicative of destruction and loss of nephrons [162]. A rise of Eβ2M/Ecr ≥ 300 μg/g creatinine is a manifestation of severe toxicity of Cd; as such its use in health risk estimation is inappropriate. Reasons for a rise of β2M excretion in those with low eGFR can be found below.
4.4.2. β2-Microglobulinuria as an Indicator of Toxicity?
The protein β2M with a molecular weight of 11.8 kDa is a component of class I major histocompatibility complexes, found on the surface of most nucleated cells [83]. The plasma β2M concentration is relatively constant, but it may rise in patients with chronic inflammatory conditions or hematologic malignancies [163].
By β2M is eliminated exclusively by the kidneys. A modest fraction of the amount removed is taken up from peritubular capillaries [164], but most elimination results from glomerular filtration, proximal tubular reabsorption, and intracellular degradation. When the GFR is normal, the equilibrium between plasma influx and renal processing establishes a plasma concentration between 1.2 and 2.7 mg/L [163]. As GFR falls, the filtrate is presented to proximal tubules at a rate that is absolutely reduced but normal or increased per surviving nephron. Plasma β2M concentration rise secondarily, and equilibrium between the influx and the degradation of the protein is maintained [164,165,166,167,168,169].
In Cd research, it has been customary to declare that proximal tubular toxicity is present at Eβ2M/Ecr > 300 µg/g creatinine [153]. At an arbitrary Eβ2M of 300 µg/d, Ecr of 1 g/d, GFR of 144 L/d (100 mL/min), and filterable [β2M]p of 2.0 mg/L, fractional excretion of β2M (FEβ2M) is 0.1% and fractional reabsorption (FRβ2M) is 99.9%. Doubling of Eβ2M to 600 µg/g creatinine, a clearly elevated value, entails an increase in FEβ2M from 0.1% to 0.2% and a reduction in FRβ2M to 99.8%. Miniscule Cd-induced reductions in FRβ2M, therefore, lead to substantial increments in Eβ2M [170].
The sensitivity of Eβ2M to slight reductions of FRβ2M should not be interpreted as evidence that the underlying cellular injury is trivial. Values of ECd at which Eβ2M exceeds 300 µg/g creatinine are at least 10 times higher than in normal populations [171,172]. If ECd itself is a marker of toxicity, then the customary cutoff value of Eβ2M is not a sensitive metric for detecting tubular injury. For pathophysiologic insight, Eβ2M is most logically related to the normal maximal reabsorptive capacity for the protein—i.e., the tubular maximum (Tmβ2M)—if such a Tm exists. Hall could not demonstrate one in dogs with an infusion of human β2M [164], but in rats, Gauthier documented a Tmβ2MG when [β2M]p was approximately four times the norm [67].
In theory, if a Tmβ2M existed in humans, a decline in GFR might expose it. In this circumstance, surviving nephrons would be presented with a higher concentration of β2M in less total filtrate volume, and a normal rate of presentation to a reduced nephron mass could exceed a putative Tmβ2M. Multiple investigators have argued that this scenario occurs, but it is often possible that the disease lowering GFR has also lowered Tmβ2M [166,169]. In patients with hepatorenal syndrome, in which the perfusion of normal kidneys is severely limited, a Tmβ2M was not demonstrable despite extreme reductions in GFR and elevations in [β2M]p [168]. Similarly, in children with glomerular disease exclusively, on biopsy, FEβ2M did not correlate with GFR [169].
If some humans can reabsorb all filtered β2M despite a low GFR and high [β2M]p, then nephron loss is insufficient to explain excessive Eβ2M in patients with Cd nephropathy. It appears that Cd imposes a Tmβ2M or reduces one that already exists, and increased Eβ2M indicates reduced β2M reabsorption per nephron at any GFR [173]. Once Cd has established a Tmβ2M, we expect Eβ2M to rise substantially as GFR falls. Multiple investigators have documented this phenomenon [162,174,175], but none have quantified the individual contributions of GFR and Tmβ2M to excessive Eβ2M.
5. Conclusions
As the result of cadmium accumulation in renal proximal tubular cells, the fractional reabsorption rates for albumin and β2-microglobulin are reduced simultaneously, leading to an increased excretion of both proteins. It appears that cadmium adversely affects a single phenomenon involved in reabsorption of both albumin and β2-mcroglobulin. The affected phenomenon is probably receptor-mediated endocytosis involving megalin.
The conventional method for adjusting the excretion rates of cadmium and albumin to the excretion of creatinine incorporates a conceptual flaw that can be eliminated if the rates are normalized to creatinine clearance. The NOAEL equivalent of Cd accumulation levels corresponding to a discernable GFR reduction are is extremely low. Now is the time to acknowledge there is no safe level of Cd exposure.
At present, no treatments exist for mitigation of Cd nephropathy or effective chelation therapy for removal of Cd from tubular cells. Commonsense therapeutic measures include cessation of environmental exposure.
Funding
This work was supported with resources from the Centre for Kidney Disease Research, Translational Research Institute, and the Department of Kidney and Transplant Services, Princess Alexandra Hospital.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The author thanks Aleksandar Cirovic for his assistance with drawing figures. The author gratefully acknowledges overseas travel grants and partial research project funds through the Thailand Reverse Brain Drain Project, the Commission of Higher Education, Ministry of Education, and the National Science and Technology Development Agency (NSTDA), Ministry of Sciences and Technology.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Satarug, S.; Vesey, D.A.; Gobe, G.C.; Phelps, K.R. Estimation of health risks associated with dietary cadmium exposure. Arch. Toxicol. 2023, 97, 329–358. [Google Scholar] [CrossRef]
- Fechner, C.; Hackethal, C.; Höpfner, T.; Dietrich, J.; Bloch, D.; Lindtner, O.; Sarvan, I. Results of the BfR MEAL Study: In Germany, mercury is mostly contained in fish and seafood while cadmium, lead, and nickel are present in a broad spectrum of foods. Food Chem. X 2022, 14, 100326. [Google Scholar] [CrossRef]
- Xiao, G.; Liu, Y.; Dong, K.F.; Lu, J. Regional characteristics of cadmium intake in adult residents from the 4th and 5th Chinese Total Diet Study. Environ. Sci. Pollut. Res. 2020, 27, 3850–3857. [Google Scholar] [CrossRef]
- Kim, H.; Lee, J.; Woo, H.D.; Kim, D.W.; Choi, I.J.; Kim, Y.-I.; Kim, J. Association between dietary cadmium intake and early gastric cancer risk in a Korean population: A case–control study. Eur. J. Nutr. 2019, 58, 3255–3266. [Google Scholar] [CrossRef]
- Watanabe, T.; Kataoka, Y.; Hayashi, K.; Matsuda, R.; Uneyama, C. Dietary Exposure of the Japanese General Population to Elements: Total Diet Study 2013–2018. Food Saf. 2022, 10, 83–101. [Google Scholar] [CrossRef] [PubMed]
- Thévenod, F.; Herbrechter, R.; Schlabs, C.; Pethe, A.; Lee, W.K.; Wolff, N.A.; Roussa, E. Role of the SLC22A17/lipocalin-2 receptor in renal endocytosis of proteins/metalloproteins: A focus on iron- and cadmium-binding proteins. Am. J. Physiol. Renal. Physiol. 2023, 325, F564–F577. [Google Scholar] [CrossRef]
- Rentschler, G.; Kippler, M.; Axmon, A.; Raqib, R.; Skerfving, S.; Vahter, M.; Broberg, K. Cadmium concentrations in human blood and urine are associated with polymorphisms in zinc transporter genes. Metallomics 2014, 6, 885–891. [Google Scholar] [CrossRef] [PubMed]
- Rentschler, G.; Kippler, M.; Axmon, A.; Raqib, R.; Ekström, E.-C.; Skerfving, S.; Vahter, M.; Broberg, K. Polymorphisms in Iron Homeostasis Genes and Urinary Cadmium Concentrations among Nonsmoking Women in Argentina and Bangladesh. Environ. Health Perspect. 2013, 121, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Ng, E.; Lind, P.M.; Lindgren, C.; Ingelsson, E.; Mahajan, A.; Morris, A.; Lind, L. Genome-wide association study of toxic metals and trace elements reveals novel associations. Hum. Mol. Genet. 2015, 24, 4739–4745. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Li, C.; Zhao, D.; Huang, L. Associations of micronutrients exposure with cadmium body burden among population: A systematic review. Ecotoxicol. Environ. Saf. 2023, 256, 114878. [Google Scholar] [CrossRef]
- Fujita, Y.; el Belbasi, H.I.; Min, K.S.; Onosaka, S.; Okada, Y.; Matsumoto, Y.; Mutoh, N.; Tanaka, K. Fate of cadmium bound to phytochelatin in rats. Res. Commun. Chem. Pathol. Pharmacol. 1993, 82, 357–365. [Google Scholar]
- Langelueddecke, C.; Roussa, E.; Fenton, R.A.; Thévenod, F. Expression and function of the lipocalin-2 (24p3/NGAL) receptor in rodent and human intestinal epithelia. PLoS ONE 2013, 8, e71586. [Google Scholar] [CrossRef] [PubMed]
- Langelueddecke, C.; Lee, W.K.; Thévenod, F. Differential transcytosis and toxicity of the hNGAL receptor ligands cadmi-um-metallothionein and cadmium-phytochelatin in colon-like Caco-2 cells: Implications for in vivo cadmium toxicity. Toxicol. Lett. 2014, 226, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Langelueddecke, C.; Roussa, E.; Fenton, R.A.; Wolff, N.A.; Lee, W.-K.; Thevenod, F. Lipocalin-2 (24p3/Neutrophil Gelatinase-associated Lipocalin (NGAL)) receptor is expressed in distal nephron and mediates protein endocytosis. J. Biol. Chem. 2012, 287, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Zavala-Guevara, I.P.; Ortega-Romero, M.S.; Narváez-Morales, J.; Jacobo-Estrada, T.L.; Lee, W.-K.; Arreola-Mendoza, L.; Thévenod, F.; Barbier, O.C. Increased Endocytosis of Cadmium-Metallothionein through the 24p3 Receptor in an In Vivo Model with Reduced Proximal Tubular Activity. Int. J. Mol. Sci. 2021, 22, 7262. [Google Scholar] [CrossRef] [PubMed]
- Pappas, R.S.; Fresquez, M.R.; Watson, C.H. Cigarette Smoke Cadmium Breakthrough From Traditional Filters: Implications for Exposure. J. Anal. Toxicol. 2015, 39, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Repić, A.; Bulat, P.; Antonijević, B.; Antunović, M.; Džudović, J.; Buha, A.; Bulat, Z. The influence of smoking habits on cadmium and lead blood levels in the Serbian adult people. Environ. Sci. Pollut. Res. 2020, 27, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Świetlik, R.; Trojanowska, M. Chemical fractionation in environmental studies of potentially toxic particulate-bound elements in urban air: A critical review. Toxics 2022, 10, 124. [Google Scholar] [CrossRef]
- Kim, J.; Song, H.; Lee, J.; Kim, Y.J.; Chung, H.S.; Yu, J.M.; Jang, G.; Park, R.; Chung, W.; Oh, C.-M.; et al. Smoking and passive smoking increases mortality through mediation effect of cadmium exposure in the United States. Sci. Rep. 2023, 13, 3878. [Google Scholar] [CrossRef]
- Nakajima, M.; Kobayashi, E.; Suwazono, Y.; Uetani, M.; Oishi, M.; Inaba, T.; Kido, T.; Zahir A Shaikh, Z.A.; Nogawa, K. Excretion of urinary cadmium, copper, and zinc in cadmium-exposed and nonexposed subjects, with special reference to urinary excretion of beta2-microglobulin and metallothionein. Biol. Trace Elem. Res, 2005; 18, 17–31. [Google Scholar] [CrossRef]
- Aoyagi, T.; Hayakawa, K.; Miyaji, K.; Ishikawa, H.; Hata, M. Cadmium nephrotoxicity and evacuation from the body in a rat modeled subchronic intoxication. Int. J. Urol. 2003, 10, 332–338. [Google Scholar] [CrossRef]
- Elinder, C.G.; Lind, B.; Kjellstorm, T.; Linnman, L.; Friberg, L. Cadmium in kidney cortex, liver and pancreas from Swedish autopsies: Estimation of biological half time in kidney cortex, considering calorie intake and smoking habits. Arch. Environ. Health 1976, 31, 292–301. [Google Scholar] [CrossRef]
- Elinder, C.-G.; Kjellstöm, T.; Lind, B.; Molander, M.-L.; Silander, T. Cadmium concentrations in human liver, blood, and bile: Comparison with a metabolic model. Environ. Res. 1978, 17, 236–241. [Google Scholar] [CrossRef]
- Jarup, L.; Rogenfelt, A.; Elinder, C.; Nogawa, K.; Kjellstrom, T. Biological half-time of cadmium in the blood of workers after cessation of exposure. Scand. J. Work. Environ. Health 1983, 9, 327–331. [Google Scholar] [CrossRef]
- Suwazono, Y.; Kido, T.; Nakagawa, H.; Nishijo, M.; Honda, R.; Kobayashi, E.; Dochi, M.; Nogawa, K. Biological half-life of cadmium in the urine of inhabitants after cessation of cadmium exposure. Biomarkers 2009, 14, 77–81. [Google Scholar] [CrossRef]
- Ishizaki, M.; Suwazono, Y.; Kido, T.; Nishijo, M.; Honda, R.; Kobayashi, E.; Nogawa, K.; Nakagawa, H. Estimation of biological half-life of urinary cadmium in inhabitants after cessation of environmental cadmium pollution using a mixed linear model. Food Addit. Contam. Part A 2015, 32, 1273–1276. [Google Scholar] [CrossRef]
- Satarug, S.; Nishijo, M.; Ujjin, P.; Vanavanitkun, Y.; Baker, J.R.; Moore, M.R. Evidence for Concurrent Effects of Exposure to Environmental Cadmium and Lead on Hepatic CYP2A6 Phenotype and Renal Function Biomarkers in Nonsmokers. Environ. Health Perspect. 2004, 112, 1512–1518. [Google Scholar] [CrossRef]
- Satarug, S.; Tassaneeyakul, W.; Na-Bangchang, K.; Cashman, J.R.; Moore, M.R. Genetic and Environmental Influences on Therapeutic and Toxicity Outcomes: Studies with CYP2A6. Curr. Clin. Pharmacol. 2006, 1, 291–309. [Google Scholar] [CrossRef]
- Apinan, R.; Tassaneeyakul, W.; Mahavorasirikul, W.; Satarug, S.; Kajanawart, S.; Vannaprasaht, S.; Ruenweerayut, R.; Na-Bangchang, K. The influence of CYP2A6 polymorphisms and cadmium on nicotine metabolism in Thai population. Environ. Toxicol. Pharmacol. 2009, 28, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Becker, C.; Inker, L.A. Glomerular filtration rate and albuminuria for detection and staging of acute and chronic kidney disease in adults: A systematic review. JAMA 2015, 313, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Murton, M.; Goff-Leggett, D.; Bobrowska, A.; Sanchez, J.J.G.; James, G.; Wittbrodt, E.; Nolan, S.; Sörstadius, E.; Pecoits-Filho, R.; Tuttle, K. Burden of Chronic Kidney Disease by KDIGO Categories of Glomerular Filtration Rate and Albuminuria: A Systematic Review. Adv. Ther. 2021, 38, 180–200. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Jafar, T.H.; Nitsch, D.; Neuen, B.L.; Perkovic, V. Chronic kidney disease. Lancet 2021, 398, 786–802. [Google Scholar] [CrossRef]
- George, C.; Mogueo, A.; Okpechi, I.; Echouffo-Tcheugui, J.B.; Kengne, A.P. Chronic kidney disease in low-income to middle-income countries: The case for increased screening. BMJ Glob. Health 2017, 2, e000256. [Google Scholar] [CrossRef] [PubMed]
- Doccioli, C.; Sera, F.; Francavilla, A.; Cupisti, A.; Biggeri, A. Association of cadmium environmental exposure with chronic kidney disease: A systematic review and meta-analysis. Sci. Total. Environ. 2024, 906, 167165. [Google Scholar] [CrossRef]
- Jalili, C.; Kazemi, M.; Cheng, H.; Mohammadi, H.; Babaei, A.; Taheri, E.; Moradi, S. Associations between exposure to heavy metals and the risk of chronic kidney disease: A systematic review and meta-analysis. Crit. Rev. Toxicol. 2021, 51, 165–182. [Google Scholar] [CrossRef] [PubMed]
- Byber, K.; Lison, D.; Verougstraete, V.; Dressel, H.; Hotz, P. Cadmium or cadmium compounds and chronic kidney disease in workers and the general population: A systematic review. Crit. Rev. Toxicol. 2016, 46, 191–240. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Gobe, G.C.; Yimthiang, S.; Đorđević, A.B. Health Risk in a Geographic Area of Thailand with Endemic Cadmium Contamination: Focus on Albuminuria. Toxics 2023, 11, 68. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Đorđević, A.B.; Yimthiang, S.; Vesey, D.A.; Gobe, G.C. The NOAEL Equivalent of Environmental Cadmium Exposure Associated with GFR Reduction and Chronic Kidney Disease. Toxics 2022, 10, 614. [Google Scholar] [CrossRef]
- Myong, J.-P.; Kim, H.-R.; Baker, D.; Choi, B. Blood cadmium and moderate-to-severe glomerular dysfunction in Korean adults: Analysis of KNHANES 2005–2008 data. Int. Arch. Occup. Environ. Health 2012, 85, 885–893. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.; Chung, J.H.; Kim, S.J.; Koh, E.S.; Yoon, H.E.; Park, C.W.; Chang, Y.S.; Shin, S.J. Blood lead and cadmium levels and renal function in Korean adults. Clin. Exp. Nephrol. 2014, 18, 726–734. [Google Scholar] [CrossRef]
- Tsai, H.-J.; Hung, C.-H.; Wang, C.-W.; Tu, H.-P.; Li, C.-H.; Tsai, C.-C.; Lin, W.-Y.; Chen, S.-C.; Kuo, C.-H. Associations among Heavy Metals and Proteinuria and Chronic Kidney Disease. Diagnostics 2021, 11, 282. [Google Scholar] [CrossRef]
- Feng, X.; Zhou, R.; Jiang, Q.; Wang, Y.; Yu, C. Analysis of cadmium accumulation in community adults and its correlation with low-grade albuminuria. Sci. Total. Environ. 2022, 834, 155210. [Google Scholar] [CrossRef] [PubMed]
- Grau-Perez, M.; Pichler, G.; Galan-Chilet, I.; Briongos-Figuero, L.S.; Rentero-Garrido, P.; Lopez-Izquierdo, R.; Navas-Acien, A.; Weaver, V.; García-Barrera, T.; Gomez-Ariza, J.L.; et al. Urine cadmium levels and albuminuria in a general population from Spain: A gene-environment interaction analysis. Environ. Int. 2017, 106, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Navas-Acien, A.; Tellez-Plaza, M.; Guallar, E.; Muntner, P.; Silbergeld, E.; Jaar, B.; Weaver, V. Blood Cadmium and Lead and Chronic Kidney Disease in US Adults: A Joint Analysis. Am. J. Epidemiol. 2009, 170, 1156–1164. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, P.M.; Costanzi, S.; Naticchia, A.; Sturniolo, A.; Gambaro, G. Low level exposure to cadmium increases the risk of chronic kidney disease: Analysis of the NHANES 1999-2006. BMC Public Health 2010, 10, 304. [Google Scholar] [CrossRef]
- Madrigal, J.M.; Ricardo, A.C.; Persky, V.; Turyk, M. Associations between blood cadmium concentration and kidney function in the U.S. population: Impact of sex, diabetes and hypertension. Environ. Res. 2018, 169, 180–188. [Google Scholar] [CrossRef]
- Zhu, X.-J.; Wang, J.-J.; Mao, J.-H.; Shu, Q.; Du, L.-Z. Relationships of Cadmium, Lead, and Mercury Levels With Albuminuria in US Adults: Results From the National Health and Nutrition Examination Survey Database, 2009–2012. Am. J. Epidemiol. 2019, 188, 1281–1287. [Google Scholar] [CrossRef]
- Lin, Y.-S.; Caffrey, J.L.; Lin, J.-W.; Bayliss, D.; Faramawi, M.F.; Bateson, T.F.; Sonawane, B. Increased Risk of Cancer Mortality Associated with Cadmium Exposures in Older Americans with Low Zinc Intake. J. Toxicol. Environ. Health Part A 2012, 76, 1–15. [Google Scholar] [CrossRef]
- Huang, C.-H.; Wang, C.-W.; Chen, H.-C.; Tu, H.-P.; Chen, S.-C.; Hung, C.-H.; Kuo, C.-H. Gender Difference in the Associations among Heavy Metals with Red Blood Cell Hemogram. Int. J. Environ. Res. Public Health 2021, 19, 189. [Google Scholar] [CrossRef]
- Olsén, L.; Lind, P.M.; Lind, L. Gender differences for associations between circulating levels of metals and coronary risk in the elderly. Int. J. Hyg. Environ. Health 2012, 215, 411–417. [Google Scholar] [CrossRef]
- Sun, H.; Wang, D.; Zhou, Z.; Ding, Z.; Chen, X.; Xu, Y.; Huang, L.; Tang, D. Association of cadmium in urine and blood with age in a general population with low environmental exposure. Chemosphere 2016, 156, 392–397. [Google Scholar] [CrossRef] [PubMed]
- Butler-Dawson, J.; James, K.A.; Krisher, L.; Jaramillo, D.; Dally, M.; Neumann, N.; Pilloni, D.; Cruz, A.; Asensio, C.; Johnson, R.J.; et al. Environmental metal exposures and kidney function of Guatemalan sugarcane workers. J. Expo. Sci. Environ. Epidemiol. 2022, 32, 461–471. [Google Scholar] [CrossRef]
- Win-Thu, M.; Myint-Thein, O.; Win-Shwe, T.-T.; Mar, O. Environmental cadmium exposure induces kidney tubular and glomerular dysfunction in the Myanmar adults. J. Toxicol. Sci. 2021, 46, 319–328. [Google Scholar] [CrossRef]
- Skröder, H.; Hawkesworth, S.; Kippler, M.; El Arifeen, S.; Wagatsuma, Y.; Moore, S.E.; Vahter, M. Kidney function and blood pressure in preschool-aged children exposed to cadmium and arsenic - potential alleviation by selenium. Environ. Res. 2015, 140, 205–213. [Google Scholar] [CrossRef]
- Rodríguez-López, E.; Tamayo-Ortiz, M.; Ariza, A.C.; Ortiz-Panozo, E.; Deierlein, A.L.; Pantic, I.; Tolentino, M.C.; Estrada-Gutiérrez, G.; Parra-Hernández, S.; Espejel-Núñez, A.; et al. Early-Life Dietary Cadmium Exposure and Kidney Function in 9-Year-Old Children from the PROGRESS Cohort. Toxics 2020, 8, 83. [Google Scholar] [CrossRef]
- Moffett, D.B.; Mumtaz, M.M.; Sullivan, D.W., Jr.; Whittaker, M.H. Chapter 13, General Considerations of Dose-Effect and Dose-Response Relationships. In Handbook on the Toxicology of Metals, 5th ed.; Volume I: General, Considerations; Nordberg, G., Costa, M., Eds.; Academic Press: Cambridge, MA, USA, 2022; pp. 299–317. [Google Scholar]
- Heymsfield, S.B.; Arteaga, C.; McManus, C.; Smith, J.; Moffitt, S. Measurement of muscle mass in humans: validity of the 24-hour urinary creatinine method. Am. J. Clin. Nutr. 1983, 37, 478–494. [Google Scholar] [CrossRef] [PubMed]
- Phelps, K.R.; Gosmanova, E.O. A generic method for analysis of plasma concentrations. Clin. Nephrol. 2020, 94, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Denic, A.; Elsherbiny, H.; Rule, A.D. In-vivo techniques for determining nephron number. Curr. Opin. Nephrol. Hypertens. 2019, 28, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Soveri, I.; Berg, U.B.; Björk, J.; Elinder, C.G.; Grubb, A.; Mejare, I.; Sterner, G.; Bäck, S.E.; SBU GFR Review Group. Measuring GFR: A Systematic Review. Am. J. Kidney Dis. 2014, 64, 411–424. [Google Scholar] [CrossRef] [PubMed]
- White, C.A.; Allen, C.M.; Akbari, A.; Collier, C.P.; Holland, D.C.; Day, A.G.; Knoll, G.A. Comparison of the new and traditional CKD-EPI GFR estimation equations with urinary inulin clearance: A study of equation performance. Clin. Chim. Acta 2019, 488, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Ruangyuttikarn, W.; Nishijo, M.; Gobe, G.C.; Phelps, K.R. The Source and Pathophysiologic Significance of Excreted Cadmium. Toxics 2019, 7, 55. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Gobe, G.C. Cadmium-Induced Proteinuria: Mechanistic Insights from Dose–Effect Analyses. Int. J. Mol. Sci. 2023, 24, 1893. [Google Scholar] [CrossRef]
- Satarug, S.; Vesey, D.A.; Gobe, G.C.; Phelps, K.R. The pathogenesis of albuminuria in cadmium nephropathy. Curr. Res. Toxicol. 2024, 6, 100140. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., III; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Navar, L.G.; Maddox, D.A.; Munger, K.A. In: Brenner and Rector’s the kidney, 11th edn. Elsevier, Philadelphia, USA; 2020. Chapter 3, the renal circulations and glomerular filtration, pp 80-114.
- Gauthier, C.; Nguyen-Simonnet, H.; Vincent, C.; Revillard, J.-P.; Pellet, M.V. Renal tubular absorption of β2-microglobulin. Kidney Int. 1984, 26, 170–175. [Google Scholar] [CrossRef]
- Norden, A.G.; Lapsley, M.; Lee, P.J.; Pusey, C.D.; Scheinman, S.J.; Tam, F.W.; Thakker, R.V.; Unwin, R.J.; Wrong, O. Glomerular protein sieving and implications for renal failure in Fanconi syndrome. Kidney Int. 2001, 60, 1885–1892. [Google Scholar] [CrossRef]
- Nielsen, R.; Christensen, E.I.; Birn, H. Megalin and cubilin in proximal tubule protein reabsorption: from experimental models to human disease. Kidney Int. 2016, 89, 58–67. [Google Scholar] [CrossRef]
- Molitoris, B.A.; Sandoval, R.M.; Yadav, S.P.S.; Wagner, M.C. Albumin uptake and processing by the proximal tubule: Physiological, pathological, and therapeutic implications. Physiol. Rev. 2022, 102, 1625–1667. [Google Scholar] [CrossRef] [PubMed]
- Eshbach, M.L.; Weisz, O.A. Receptor-Mediated Endocytosis in the Proximal Tubule. Annu. Rev. Physiol. 2017, 79, 425–448. [Google Scholar] [CrossRef]
- Bökenkamp, A. Proteinuria-take a closer look! Pediatr. Nephrol. 2020, 35, 533–541. [Google Scholar] [CrossRef]
- Comper, W.D.; Vuchkova, J.; McCarthy, K.J. New insights into proteinuria/albuminuria. Front. Physiol. 2022, 13, 991756. [Google Scholar] [CrossRef]
- Gburek, J.; Konopska, B.; Gołąb, K. Renal Handling of Albumin—From Early Findings to Current Concepts. Int. J. Mol. Sci. 2021, 22, 5809. [Google Scholar] [CrossRef] [PubMed]
- Benzing, T.; Salant, D. Insights into Glomerular Filtration and Albuminuria. New Engl. J. Med. 2021, 384, 1437–1446. [Google Scholar] [CrossRef] [PubMed]
- Clapp, W.L.; Park, C.H.; Madsen, K.M.; Tisher, C.C. Axial heterogeneity in the handling of albumin by the rabbit proximal tubule. Lab. Invest. 1988, 58, 549–558. [Google Scholar] [PubMed]
- Schuh, C.D.; Polesel, M.; Platonova, E.; Haenni, D.; Gassama, A.; Tokonami, N.; Ghazi, S.; Bugarski, M.; Devuyst, O.; Ziegler, U.; et al. Combined Structural and Functional Imaging of the Kidney Reveals Major Axial Differences in Proximal Tubule Endocytosis. J. Am. Soc. Nephrol. 2018, 29, 2696–2712. [Google Scholar] [CrossRef] [PubMed]
- Wagner, M.C.; Sandoval, R.M.; Yadav, S.P.S.; Campos, S.B.; Rhodes, G.J.; Phillips, C.L.; Molitoris, B.A. Lrpap1 (RAP) Inhibits Proximal Tubule Clathrin Mediated and Clathrin Independent Endocytosis, Ameliorating Renal Aminoglycoside Nephrotoxicity. Kidney360 2023, 4, 591–605. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Phelps, K.R. Chapter 14, Cadmium exposure and toxicity. In Metal Toxicology; Bagchi, M., Bagchi, D., Eds.; CRC Press: Boca Raton, FL, USA, 2021. [Google Scholar]
- Polesel, M.; Kaminska, M.; Haenni, D.; Bugarski, M.; Schuh, C.; Jankovic, N.; Kaech, A.; Mateos, J.M.; Berquez, M.; Hall, A.M. Spatiotemporal organisation of protein processing in the kidney. Nat. Commun. 2022, 13, 5732. [Google Scholar] [CrossRef]
- Sarav, M.; Wang, Y.; Hack, B.K.; Chang, A.; Jensen, M.; Bao, L.; Quigg, R.J. Renal FcRn Reclaims Albumin but Facilitates Elimination of IgG. J. Am. Soc. Nephrol. 2009, 20, 1941–1952. [Google Scholar] [CrossRef]
- Tenten, V.; Menzel, S.; Kunter, U.; Sicking, E.-M.; van Roeyen, C.R.C.; Sanden, S.K.; Kaldenbach, M.; Boor, P.; Fuss, A.; Uhlig, S.; et al. Albumin is recycled from the primary urine by tubular transcytosis. J. Am. Soc. Nephrol. 2013, 24, 1966–1980. [Google Scholar] [CrossRef]
- Argyropoulos, C.P.; Chen, S.S.; Ng, Y.-H.; Roumelioti, M.-E.; Shaffi, K.; Singh, P.P.; Tzamaloukas, A.H. Rediscovering Beta-2 Microglobulin As a Biomarker across the Spectrum of Kidney Diseases. Front. Med. 2017, 4, 73. [Google Scholar] [CrossRef]
- Tojo, A.; Endou, H.; Nolin, A.C.; Mulhern, R.M.; Panchenko, M.V.; Pisarek-Horowitz, A.; Wang, Z.; Shirihai, O.; Borkan, S.C.; Havasi, A.; et al. Intrarenal handling of proteins in rats using fractional micropuncture technique. Am. J. Physiol. Physiol. 1992, 263, F601–F606. [Google Scholar] [CrossRef]
- Carlson, L.A.; Friberg, L. The Distribution of Cadmium in Blood After Repeated Exposure. Scand. J. Clin. Lab. Investig. 1957, 9, 67–70. [Google Scholar] [CrossRef]
- Nordberg, G.F.; Piscator, M.; Nordberg, M. On the Distribution of Cadmium in Blood. Acta Pharmacol. et Toxicol. 1971, 30, 289–295. [Google Scholar] [CrossRef]
- Gibson, M.A.; Sarpong-Kumankomah, S.; Nehzati, S.; George, G.N.; Gailer, J. Remarkable differences in the biochemical fate of Cd2+, Hg2+, CH3Hg+ and thimerosal in red blood cell lysate. Metallomics 2017, 9, 1060–1072. [Google Scholar] [CrossRef]
- Nordberg, M.; Nordberg, G.F. Metallothionein and Cadmium Toxicology—Historical Review and Commentary. Biomolecules 2022, 12, 360. [Google Scholar] [CrossRef]
- Scott, B.J.; Bradwell, A.R. Identification of the serum binding proteins for iron, zinc, cadmium, nickel, and calcium. Clin. Chem. 1983, 29, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Horn, N.M.; Thomas, A.L. Interactions between the histidine stimulation of cadmium and zinc influx into human erythrocytes. J. Physiol. 1996, 496, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Morris, T.T.; Keir, J.L.; Boshart, S.J.; Lobanov, V.P.; Ruhland, A.M.; Bahl, N.; Gailer, J. Mobilization of Cd from human serum albumin by small molecular weight thiols. J. Chromatogr. B 2014, 958, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Sagmeister, P.; Gibson, M.A.; McDade, K.H.; Gailer, J. Physiologically relevant plasma d,l-homocysteine concentrations mo-bilize Cd from human serum albumin. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2016, 1027, 181–186. [Google Scholar] [CrossRef]
- Turell, L.; Radi, R.; Alvarez, B. The thiol pool in human plasma: The central contribution of albumin to redox processes. Free. Radic. Biol. Med. 2013, 65, 244–253. [Google Scholar] [CrossRef]
- Shen, X.-C.; Liou, X.-Y.; Ye, L.-P.; Liang, H.; Wang, Z.-Y. Spectroscopic studies on the interaction between human hemoglobin and CdS quantum dots. J. Colloid Interface Sci. 2007, 311, 400–406. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, M.; Jiang, L.; Song, L. New insight into molecular interaction of heavy metal pollutant—cadmium(II) with human serum albumin. Environ. Sci. Pollut. Res. 2014, 21, 6994–7005. [Google Scholar] [CrossRef]
- Fels, J.; Scharner, B.; Zarbock, R.; Guevara, I.P.Z.; Lee, W.-K.; Barbier, O.C.; Thévenod, F. Cadmium Complexed with β2-Microglubulin, Albumin and Lipocalin-2 rather than Metallothionein Cause Megalin:Cubilin Dependent Toxicity of the Renal Proximal Tubule. Int. J. Mol. Sci. 2019, 20, 2379. [Google Scholar] [CrossRef]
- Edwards, A.; Long, K.R.; Baty, C.J.; Shipman, K.E.; Weisz, O.A. Modelling normal and nephrotic axial uptake of albumin and other filtered proteins along the proximal tubule. J. Physiol. 2022, 600, 1933–1952. [Google Scholar] [CrossRef]
- Castrop, H.; Schießl, I.M. Novel routes of albumin passage across the glomerular filtration barrier. Acta Physiol. 2016, 219, 546–555. [Google Scholar] [CrossRef] [PubMed]
- Santoyo-Sánchez, M.P.; Pedraza-Chaverri, J.; Molina-Jijón, E.; Arreola-Mendoza, L.; Rodríguez-Muñoz, R.; Barbier, O.C. Impaired endocytosis in proximal tubule from subchronic exposure to cadmium involves angiotensin II type 1 and cubilin receptors. BMC Nephrol. 2013, 14, 211. [Google Scholar] [CrossRef] [PubMed]
- Gena, P.; Calamita, G.; Guggino, W.B. Cadmium Impairs Albumin Reabsorption by Down-regulating Megalin and ClC5 Channels in Renal Proximal Tubule Cells. Environ. Health Perspect. 2010, 118, 1551–1556. [Google Scholar] [CrossRef]
- Li, L.; Dong, F.; Xu, D.; Du, L.; Yan, S.; Hu, H.; Lobe, C.G.; Yi, F.; Kapron, C.M.; Liu, J. Short-term, low-dose cadmium exposure induces hyperpermeability in human renal glomerular endothelial cells. J. Appl. Toxicol. 2016, 36, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Jiang, L.; Tao, T.; Su, W.; Guo, Y.; Yu, H.; Qin, J. Assessment of cadmium-induced nephrotoxicity using a kidney-on-a-chip device. Toxicol. Res. 2017, 6, 372–380. [Google Scholar] [CrossRef]
- Simmons, R.W.; Noble, A.D.; Pongsakul, P.; Sukreeyapongse, O.; Chinabut, N. Cadmium-hazard mapping using a general linear regression model (Irr-Cad) for rapid risk assessment. Environ. Geochem. Health 2009, 31, 71–79. [Google Scholar] [CrossRef]
- Simmons, R.; Pongsakul, P.; Saiyasitpanich, D.; Klinphoklap, S. Elevated Levels of Cadmium and Zinc in Paddy Soils and Elevated Levels of Cadmium in Rice Grain Downstream of a Zinc Mineralized Area in Thailand: Implications for Public Health. Environ. Geochem. Health 2005, 27, 501–511. [Google Scholar] [CrossRef]
- Suwatvitayakorn, P.; Ko, M.-S.; Kim, K.-W.; Chanpiwat, P. Human health risk assessment of cadmium exposure through rice consumption in cadmium-contaminated areas of the Mae Tao sub-district, Tak, Thailand. Environ. Geochem. Health 2020, 42, 2331–2344. [Google Scholar] [CrossRef]
- Satarug, S.; Swaddiwudhipong, W.; Ruangyuttikarn, W.; Nishijo, M.; Ruiz, P. Modeling Cadmium Exposures in Low- and High-Exposure Areas in Thailand. Environ. Health Perspect. 2013, 121, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Swaddiwudhipong, W.; Nguntra, P.; Kaewnate, Y.; Mahasakpan, P.; Limpatanachote, P.; Aunjai, T.; Jeekeeree, W.; Punta, B.; Funkhiew, T.; Phopueng, I. Human health effects from cadmium exposure: Comparison between persons living in cadmium-contaminated and non-contaminated areas in northwestern Thailand. Southeast Asian J. Trop. Med. Publ. Health 2015, 46, 133–142. [Google Scholar]
- Nishijo, M.; Suwazono, Y.; Ruangyuttikarn, W.; Nambunmee, K.; Swaddiwudhipong, W.; Nogawa, K.; Nakagawa, H. Risk assessment for Thai population: benchmark dose of urinary and blood cadmium levels for renal effects by hybrid approach of inhabitants living in polluted and non-polluted areas in Thailand. BMC Public Health 2014, 14, 702–702. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.-C.; Liou, X.-Y.; Ye, L.-P.; Liang, H.; Wang, Z.-Y. Spectroscopic studies on the interaction between human hemoglobin and CdS quantum dots. J. Colloid Interface Sci. 2007, 311, 400–406. [Google Scholar] [CrossRef]
- Guo, D.; Liu, R. Spectroscopic investigation of the effects of aqueous-phase prepared CdTe quantum dots on protein hemoglobin at the molecular level. J. Biochem. Mol. Toxicol. 2017, 31, 21953. [Google Scholar] [CrossRef] [PubMed]
- Sopjani, M.; Föller, M.; Dreischer, P.; Lang, F. Stimulation of Eryptosis by Cadmium Ions. Cell. Physiol. Biochem. 2008, 22, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Lang, F.; Bissinger, R.; Abed, M.; Artunc, F. Eryptosis - the Neglected Cause of Anemia in End Stage Renal Disease. Kidney Blood Press. Res. 2017, 42, 749–760. [Google Scholar] [CrossRef] [PubMed]
- Horiguchi, H.; Oguma, E.; Kayama, F. Cadmium Induces Anemia through Interdependent Progress of Hemolysis, Body Iron Accumulation, and Insufficient Erythropoietin Production in Rats. Toxicol. Sci. 2011, 122, 198–210. [Google Scholar] [CrossRef]
- Gray, R.; Stroupe, S. Kinetics and mechanism of bilirubin binding to human serum albumin. J. Biol. Chem. 1978, 253, 4370–4377. [Google Scholar] [CrossRef]
- Petersen, C.E.; Ha, C.-E.; Harohalli, K.; Feix, J.B.; Bhagavan, N.V. A Dynamic Model for Bilirubin Binding to Human Serum Albumin. J. Biol. Chem. 2000, 275, 20985–20995. [Google Scholar] [CrossRef]
- Torra, M.; To-Figueras, J.; Brunet, M.; Rodamilans, M.; Corbella, J. Total and methionein-bound cadmium in the liver and the kidney of a population in Barcelona (Spain). Bull. Environ. Contam. Toxicol. 1994, 53, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, M.; Ohta, H.; Yamaguchi, Y.; Seki, Y.; Sagi, M.; Yamazaki, K.; Sumi, Y. Age-dependent changes in metallothionein levels in liver and kidney of the Japanese. Biol. Trace Element Res. 1998, 63, 167–175. [Google Scholar] [CrossRef] [PubMed]
- DelRaso, N.J.; Foy, B.D.; Gearhart, J.M.; Frazier, J.M. Cadmium uptake kinetics in rat hepatocytes: correction for albumin binding. Toxicol. Sci. 2003, 72, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Guo, H.; Liu, Y.; Zhang, Q. Structural changes of human serum albumin induced by calcium acetate. J. Biochem. Mol. Toxicol. 2014, 28, 281–287. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, M.; Jiang, L.; Song, L. New insight into molecular interaction of heavy metal pollutant—cadmium(II) with human serum albumin. Environ. Sci. Pollut. Res. 2014, 21, 6994–7005. [Google Scholar] [CrossRef]
- Wong, C.; Roberts, S.M.; Saab, I.N. Review of regulatory reference values and background levels for heavy metals in the human diet. Regul. Toxicol. Pharmacol. 2022, 130, 105122. [Google Scholar] [CrossRef] [PubMed]
- Hardy, A.; Benford, D.; Halldorsson, T.; Jeger, M.J.; Knutsen, K.H.; More, S.; Mortensen, A.; Naegeli, H.; Noteborn, H.; et al.; EFSA Scientific Committee Update: use of the benchmark dose approach in risk assessment. EFSA J. 2017, 15, e04658. [Google Scholar] [CrossRef] [PubMed]
- Slob, W.; Moerbeek, M.; Rauniomaa, E.; Piersma, A.H. A Statistical Evaluation of Toxicity Study Designs for the Estimation of the Benchmark Dose in Continuous Endpoints. Toxicol. Sci. 2005, 84, 167–185. [Google Scholar] [CrossRef]
- Slob, W.; Setzer, R.W. Shape and steepness of toxicological dose–response relationships of continuous endpoints. Crit. Rev. Toxicol. 2014, 44, 270–297. [Google Scholar] [CrossRef]
- Zhu, Y.; Wang, T.; Jelsovsky, J.Z. Bootstrap Estimation of Benchmark Doses and Confidence Limits with Clustered Quantal Data. Risk Anal. 2007, 27, 447–465. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Baker, J.R.; Reilly, P.E.B.; Moore, M.R.; Williams, D.J. Cadmium Levels in the Lung, Liver, Kidney Cortex, and Urine Samples from Australians without Occupational Exposure to Metals. Arch. Environ. Health Int. J. 2002, 57, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Lyon, T.D.B.; Aughey, E.; Scott, R.; Fell, G.S. Cadmium concentrations in human kidney in the UK: 1978-1993. J. Environ. Monit. 1999, 1, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, J.L.; Samuel, O.; Dewailly, E.; Gingras, S.; Lefebvre, M.A. Levels of cadmium in kidney and liver tissues among a Canadian population (province of Quebec). J. Toxicol. Environ. Health, 1999, 56, 145–163. [Google Scholar] [CrossRef]
- Johansen, P.; Mulvad, G.; Pedersen, H.S.; Hansen, J.C.; Riget, F. Accumulation of cadmium in livers and kidneys in Greenlanders. Sci. Total. Environ. 2006, 372, 58–63. [Google Scholar] [CrossRef]
- Barregard, L.; Fabricius-Lagging, E.; Lundh, T.; Mölne, J.; Wallin, M.; Olausson, M.; Modigh, C.; Sallsten, G. Cadmium, mercury, and lead in kidney cortex of living kidney donors: Impact of different exposure sources, Environ. Res. 2010, 110, 47–54. [Google Scholar] [CrossRef]
- Schaefer, H.R.; Flannery, B.M.; Crosby, L.M.; Pouillot, R.; Farakos, S.M.S.; Van Doren, J.M.; Dennis, S.; Fitzpatrick, S.; Middleton, K. Reassessment of the cadmium toxicological reference value for use in human health assessments of foods. Regul. Toxicol. Pharmacol. 2023, 144, 105487. [Google Scholar] [CrossRef]
- Fleming, R.E.; Bacon, B.R. Orchestration of Iron Homeostasis. N. Engl. J. Med. 2005, 352, 1741–1744. [Google Scholar] [CrossRef]
- Camaschella, C. Iron-deficiency anemia. N. Engl. J. Med. 2015, 373, 485–486. [Google Scholar] [CrossRef] [PubMed]
- Weaver, V.M.; Kim, N.-S.; Jaar, B.G.; Schwartz, B.S.; Parsons, P.J.; Steuerwald, A.J.; Todd, A.C.; Simon, D.; Lee, B.-K. Associations of low-level urine cadmium with kidney function in lead workers. Occup. Environ. Med. 2011, 68, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Jin, R.; Zhu, X.; Shrubsole, M.J.; Yu, C.; Xia, Z.; Dai, Q. Associations of renal function with urinary excretion of metals: Evidence from NHANES 2003–2012. Environ. Int. 2018, 121, 1355–1362. [Google Scholar] [CrossRef]
- Buser, M.C.; Ingber, S.Z.; Raines, N.; Fowler, D.A.; Scinicariello, F. Urinary and blood cadmium and lead and kidney function: NHANES 2007–2012. Int. J. Hyg. Environ. Health 2016, 219, 261–267. [Google Scholar] [CrossRef]
- Roels, H.; Bernard, A.M.; Cardenas, A.; Buchet, J.P.; Lauwerys, R.R.; Hotter, G.; Ramis, I.; Mutti, A.; Franchini, I.; Bundschuh, I. Markers of early renal changes induced by industrial pollutants. III. Application to workers exposed to cadmium. Occup. Environ. Med. 1993, 50, 37–48. [Google Scholar] [CrossRef]
- Bernard, A.; Thielemans, N.; Roels, H.; Lauwerys, R. Association between NAG-B and cadmium in urine with no evidence of a threshold. Occup. Environ. Med. 1995, 52, 177–180. [Google Scholar] [CrossRef]
- Järup, L.; Hellström, L.; Alfvén, T.; Carlsson, M.D.; Grubb, A.; Persson, B.; Pettersson, C.; Spång, G.; Schütz, A.; Elinder, C.-G. Low level exposure to cadmium and early kidney damage: the OSCAR study. Occup. Environ. Med. 2000, 57, 668–672. [Google Scholar] [CrossRef]
- Wallin, M.; Sallsten, G.; Lundh, T.; Barregard, L. Low-level cadmium exposure and effects on kidney function. Occup. Environ. Med. 2014, 71, 848–854. [Google Scholar] [CrossRef]
- Åkesson, A.; Lundh, T.; Vahter, M.; Bjellerup, P.; Lidfeldt, J.; Nerbrand, C.; Samsioe, G.; Strömberg, U.; Skerfving, S. Tubular and Glomerular Kidney Effects in Swedish Women with Low Environmental Cadmium Exposure. Environ. Health Perspect. 2005, 113, 1627–1631. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Ruangyuttikarn, W.; Nishijo, M.; Ruiz, P. Urinary Cadmium Threshold to Prevent Kidney Disease Development. Toxics 2018, 6, 26. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Boonprasert, K.; Gobe, G.C.; Ruenweerayut, R.; Johnson, D.W.; Na-Bangchang, K.; Vesey, D.A. Chronic exposure to cadmium is associated with a marked reduction in glomerular filtration rate. Clin. Kidney J. 2018, 12, 468–475. [Google Scholar] [CrossRef]
- Saito, H.; Shioji, R.; Hurukawa, Y.; Nagai, K.; Arikawa, T. Cadmium-induced proximal tubular dysfunction in a cadmium-polluted area. Contrib. Nephrol. 1977, 6, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Roels, H.A.; Lauwerys, R.R.; Buchet, J.P.; Bernard, A.M.; Vos, A.; Oversteyns, M. Health significance of cadmium induced renal dysfunction: A five year follow up. Occup. Environ. Med. 1989, 46, 755–764. [Google Scholar] [CrossRef]
- Jarup, L.; Persson, B.; Elinder, C.G. Decreased glomerular filtration rate in solderers exposed to cadmium. Occup. Environ. Med. 1995, 52, 818–822. [Google Scholar] [CrossRef]
- Swaddiwudhipong, W.; Limpatanachote, P.; Mahasakpan, P.; Krintratun, S.; Punta, B.; Funkhiew, T. Progress in cadmium-related health effects in persons with high environmental exposure in northwestern Thailand: A five-year follow-up. Environ. Res. 2012, 112, 194–198. [Google Scholar] [CrossRef]
- Schnaper, H.W. The Tubulointerstitial Pathophysiology of Progressive Kidney Disease. Adv. Chronic Kidney Dis. 2017, 24, 107–116. [Google Scholar] [CrossRef]
- Satarug, S.; Đorđević, A.B.; Yimthiang, S.; Vesey, D.A.; Gobe, G.C. The NOAEL Equivalent of Environmental Cadmium Exposure Associated with GFR Reduction and Chronic Kidney Disease. Toxics 2022, 10, 614. [Google Scholar] [CrossRef] [PubMed]
- Satarug, S.; Vesey, D.A.; Khamphaya, T.; Pouyfung, P.; Gobe, G.C.; Yimthiang, S. Estimation of the Cadmium Nephrotoxicity Threshold from Loss of Glomerular Filtration Rate and Albuminuria. Toxics 2023, 11, 755. [Google Scholar] [CrossRef] [PubMed]
- Aoshima, K. Epidemiology of renal tubular dysfunction in the inhabitants of a cadmium-polluted area in the Jinzu River basin in Toyama prefecture. Tohoku J. Exp. Med. 1987, 152, 151–172. [Google Scholar] [CrossRef] [PubMed]
- Horiguchi, H.; Aoshima, K.; Oguma, E.; Sasaki, S.; Miyamoto, K.; Hosoi, Y.; Katoh, T.; Kayama, F. Latest status of cadmium accumulation and its effects on kidneys, bone, and erythropoiesis in inhabitants of the formerly cadmium-polluted Jinzu River Basin in Toyama, Japan, after restoration of rice paddies. Int. Arch. Occup. Environ. Health 2010, 83, 953–970. [Google Scholar] [CrossRef] [PubMed]
- JECFA. In Proceedings of the Joint FAO/WHO Expert Committee on Food Additives and Contaminants, Seventy-Third Meeting, Geneva, Switzerland, 8–17 June 2010. In Summary and Conclusions; JECFA/73/SC; Food and Agriculture Organization of the United Nations/World Health Organization: Geneva, Switzerland. 2011. Available online: https://apps.who.int/iris/handle/10665/44521 (accessed on 12 February 2024).
- [Codex Alimentarius, CODEX STAN 193–1995, General Standard for Contaminants and Toxins in Food and Feed. Available online: http://www.fao.org/fileadmin/user_upload/livestockgov/documents/1_CXS_193e.pdf (accessed on 12 February 2024).
- Satarug, S. Is environmental cadmium exposure causally related to diabetes and obesity? Cells 2024, 13, 83. [Google Scholar] [CrossRef] [PubMed]
- Cirovic, A.; Satarug, S. Toxicity Tolerance in the Carcinogenesis of Environmental Cadmium. Int. J. Mol. Sci. 2024, 25, 1851. [Google Scholar] [CrossRef]
- Nogawa, K.; Sakurai, M.; Ishizaki, M.; Kido, T.; Nakagawa, H.; Suwazono, Y. Threshold limit values of the cadmium concentration in rice in the development of itai-itai disease using benchmark dose analysis. J. Appl. Toxicol. 2017, 37, 962–966. [Google Scholar] [CrossRef]
- Nishijo, M.; Nogawa, K.; Suwazono, Y.; Kido, T.; Sakurai, M.; Nakagawa, H. Lifetime Cadmium Exposure and Mortality for Renal Diseases in Residents of the Cadmium-Polluted Kakehashi River Basin in Japan. Toxics 2020, 8, 81. [Google Scholar] [CrossRef]
- Liu, P.; Zhang, Y.; Su, J.; Bai, Z.; Li, T.; Wu, Y. Maximum cadmium limits establishment strategy based on the dietary exposure estimation: An example from Chinese populations and subgroups. Environ. Sci. Pollut. Res. 2018, 25, 18762–18771. [Google Scholar] [CrossRef]
- Wei, J.; Cen, K. Assessment of human health risk based on characteristics of potential toxic elements (PTEs) contents in foods sold in Beijing, China. Sci. Total. Environ. 2020, 703, 134747. [Google Scholar] [CrossRef]
- Cheng, Y.; Ma, J.; Li, S.; Tang, Q.; Shi, W.; Liang, Y.; Shi, G.; Qian, F. Dietary cadmium health risk assessment for the Chinese population. Environ. Sci. Pollut. Res. 2023, 30, 82421–82436. [Google Scholar] [CrossRef]
- Satarug, S.; Vesey, D.A.; Nishijo, M.; Ruangyuttikarn, W.; Gobe, G.C. The inverse association of glomerular function and urinary β2-MG excretion and its implications for cadmium health risk assessment. Environ. Res. 2019, 173, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Schardijn, G.H.C.; Statius van Eps, L.W. β2-microglobulin: Its significance in the evaluation of renal function. Kidney Int. 1987, 32, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Hall, P.W., III; Chung-Park, M.; Vacca, C.V.; London, M.; Crowley, A.Q. The renal handling of beta2-microglobulin in the dog. Kidney Int. 1982, 22, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Wibell, L.; Evrin, P.-E.; Berggård, I. Serum β2-Microglobulin in Renal Disease. Nephron 1973, 10, 320–331. [Google Scholar] [CrossRef] [PubMed]
- Wibell, L.B. Studies on β2-microglobulin in patients and normal subjects. Acta Clin. Belg. 1976, 31, 14–26. [Google Scholar]
- Wibell, L. The serum level and urinary excretion of β2-microglobulin in health and renal disease. Pathol. Biol. (Paris) 1978, 26, 295–301. [Google Scholar] [PubMed]
- Hall, P.W., III; Ricanati, E.S. Renal handling of β2-microglobulin in renal disorders with special reference to hepatorenal syndrome. Nephron 1981, 27, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Portman, R.J.; Kissane, J.M.; Robson, A.M. Use of β2 microglobulin to diagnose tubulo-interstitial renal lesions in children. Kidney Int. 1986, 30, 91–98. [Google Scholar] [CrossRef]
- Bernard, A. Renal dysfunction induced by cadmium: biomarkers of critical effects. BioMetals 2004, 17, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Nogawa, K.; Kobayashi, E.; Honda, R. A study of the relationship between cadmium concentrations in urine and renal effects of cadmium. Environ. Health Perspect. 1979, 28, 161–168. [Google Scholar] [CrossRef]
- Ikeda, M.; Ezaki, T.; Moriguchi, J.; Fukui, Y.; Ukai, H.; Okamoto, S.; Sakurai, H. The threshold cadmium level that causes a substantial increase in β2-microglobulin in urine of general populations. Tohoku J. Exp. Med. 2005, 205, 247–261. [Google Scholar] [CrossRef]
- Peterson, P.A.; Evrin, P.-E.; Berggard, I. Differentiation of glomerular, tubular, and normal proteinuria: Determinations of urinary excretion of β2-microglobulin, albumin, and total protein. J. Clin. Investig. 1969, 48, 1189–1198. [Google Scholar] [CrossRef]
- Jarup, L.; Persson, B.; Elinder, C.G. Decreased glomerular filtration rate in solderers exposed to cadmium. Occup. Environ. Med. 1995, 52, 818–822. [Google Scholar] [CrossRef]
- Elinder, C.G.; Edling, C.; Lindberg, E.; Kagedal, B.; Vesterberg, O. Assessment of renal function in workers previously exposed to cadmium. Occup. Environ. Med. 1985, 42, 754–760. [Google Scholar] [CrossRef]
Figure 1.
Tubular reabsorption of β2-microglobulin (β2M) and albumin. β2M is reabsorbed by receptor-mediated endocytosis (RME), and is catabolized (C) in lysosomes. Only a small fraction of albumin is reabsorbed through RME. Most albumin is returned to the circulation by transcytosis. Cd intoxication increases excretion of both β2M and albumin. As a carrier of Cd, reabsorption albumin may provide a delivery route for Cd to PTCs.
Figure 1.
Tubular reabsorption of β2-microglobulin (β2M) and albumin. β2M is reabsorbed by receptor-mediated endocytosis (RME), and is catabolized (C) in lysosomes. Only a small fraction of albumin is reabsorbed through RME. Most albumin is returned to the circulation by transcytosis. Cd intoxication increases excretion of both β2M and albumin. As a carrier of Cd, reabsorption albumin may provide a delivery route for Cd to PTCs.
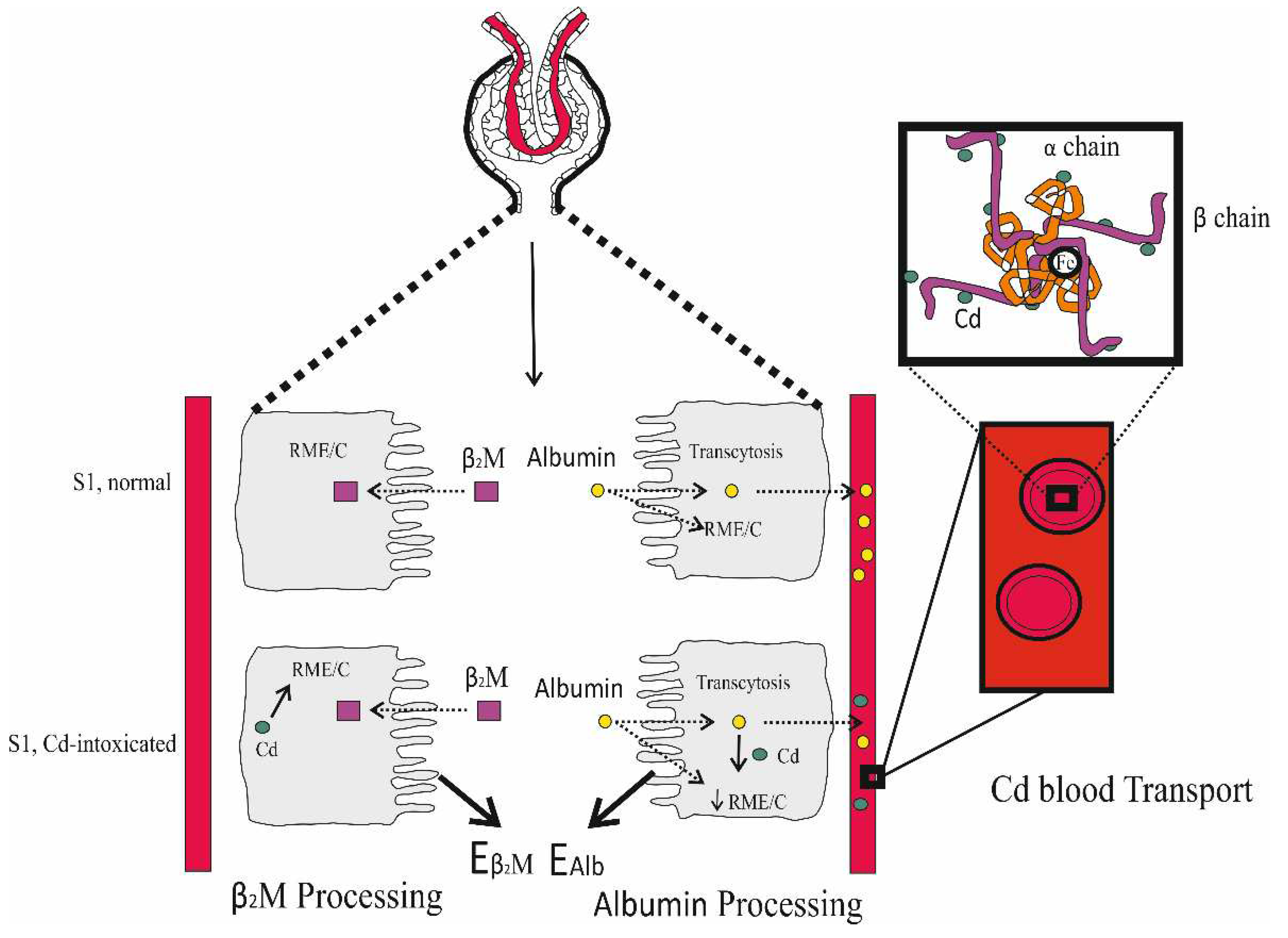
Figure 2.
Proposed pathogenesis of reduced proximal tubular reabsorption of albumin and β2-microglobulin in Cd nephropathy. In S1, all β2M is reabsorbed through receptor-mediated endocytosis (RME) and is catabolized (C) in lysosomes. Albumin is reabsorbed through RME in S1 and transcytosis in S1, S2 and S3. A small fraction of reabsorbed albumin is subjected to lysosomal catabolism, while most are returned to the blood stream by transcytosis. Cd impairs RME function, which compromises reabsorption and increases excretion of both albumin and β2M.
Figure 2.
Proposed pathogenesis of reduced proximal tubular reabsorption of albumin and β2-microglobulin in Cd nephropathy. In S1, all β2M is reabsorbed through receptor-mediated endocytosis (RME) and is catabolized (C) in lysosomes. Albumin is reabsorbed through RME in S1 and transcytosis in S1, S2 and S3. A small fraction of reabsorbed albumin is subjected to lysosomal catabolism, while most are returned to the blood stream by transcytosis. Cd impairs RME function, which compromises reabsorption and increases excretion of both albumin and β2M.
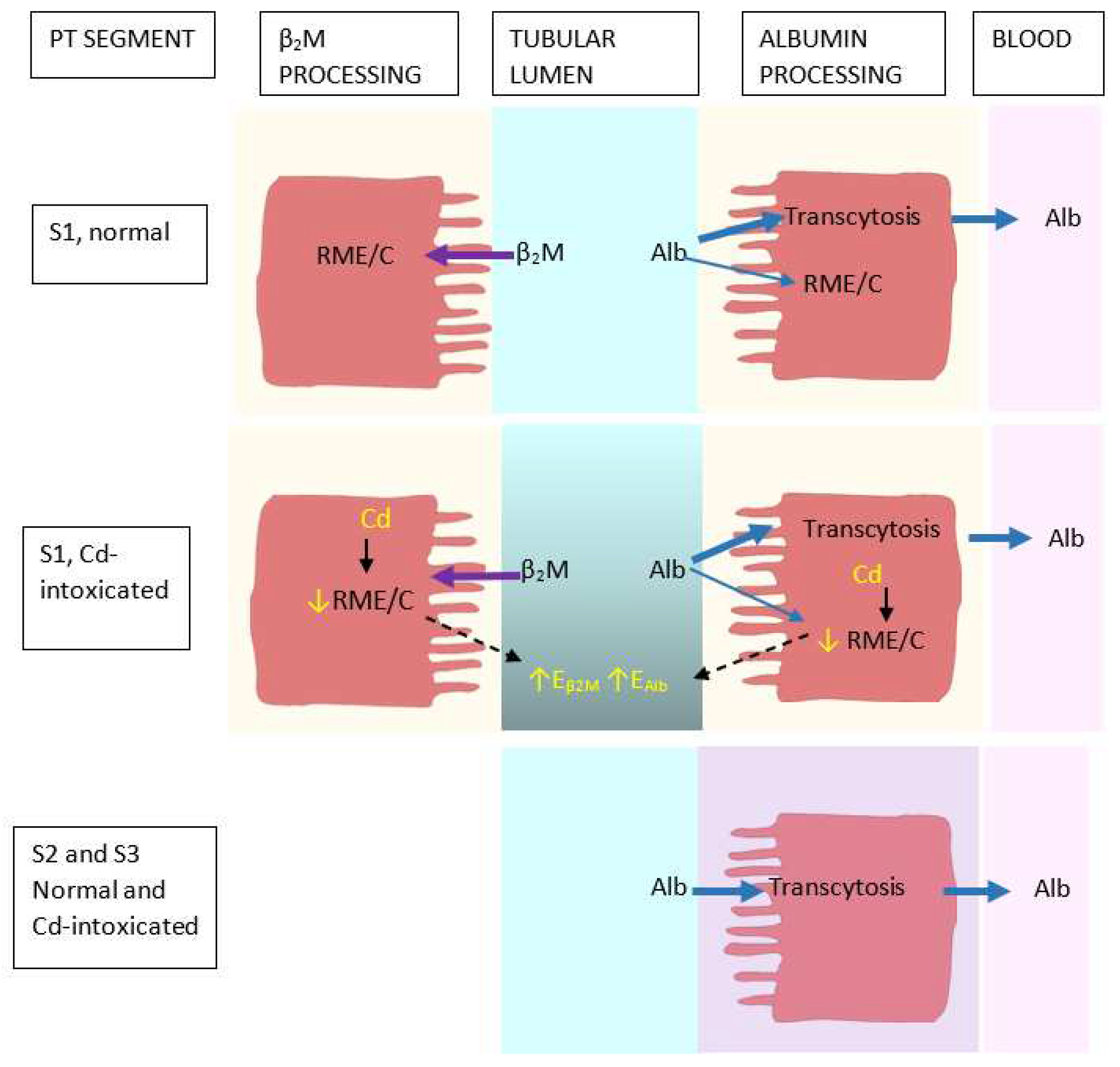
Figure 3.
Determination of the burden of Cd producing 5% reduction in eGFR. ECd/Ccr and eGFR data were fitted to (a) an inverse exponential model; (b) a natural logarithmic model; (c) an exponential model; and (d) Hill model. Bootstrap curves for model averaging of ECd/Ccr BMD estimates for all subjects (e). BMDL/BMDU values of ECd/Ccr producing 5% reduction in eGFR (f). Data are from Satarug et al. 2022 [149].
Figure 3.
Determination of the burden of Cd producing 5% reduction in eGFR. ECd/Ccr and eGFR data were fitted to (a) an inverse exponential model; (b) a natural logarithmic model; (c) an exponential model; and (d) Hill model. Bootstrap curves for model averaging of ECd/Ccr BMD estimates for all subjects (e). BMDL/BMDU values of ECd/Ccr producing 5% reduction in eGFR (f). Data are from Satarug et al. 2022 [149].
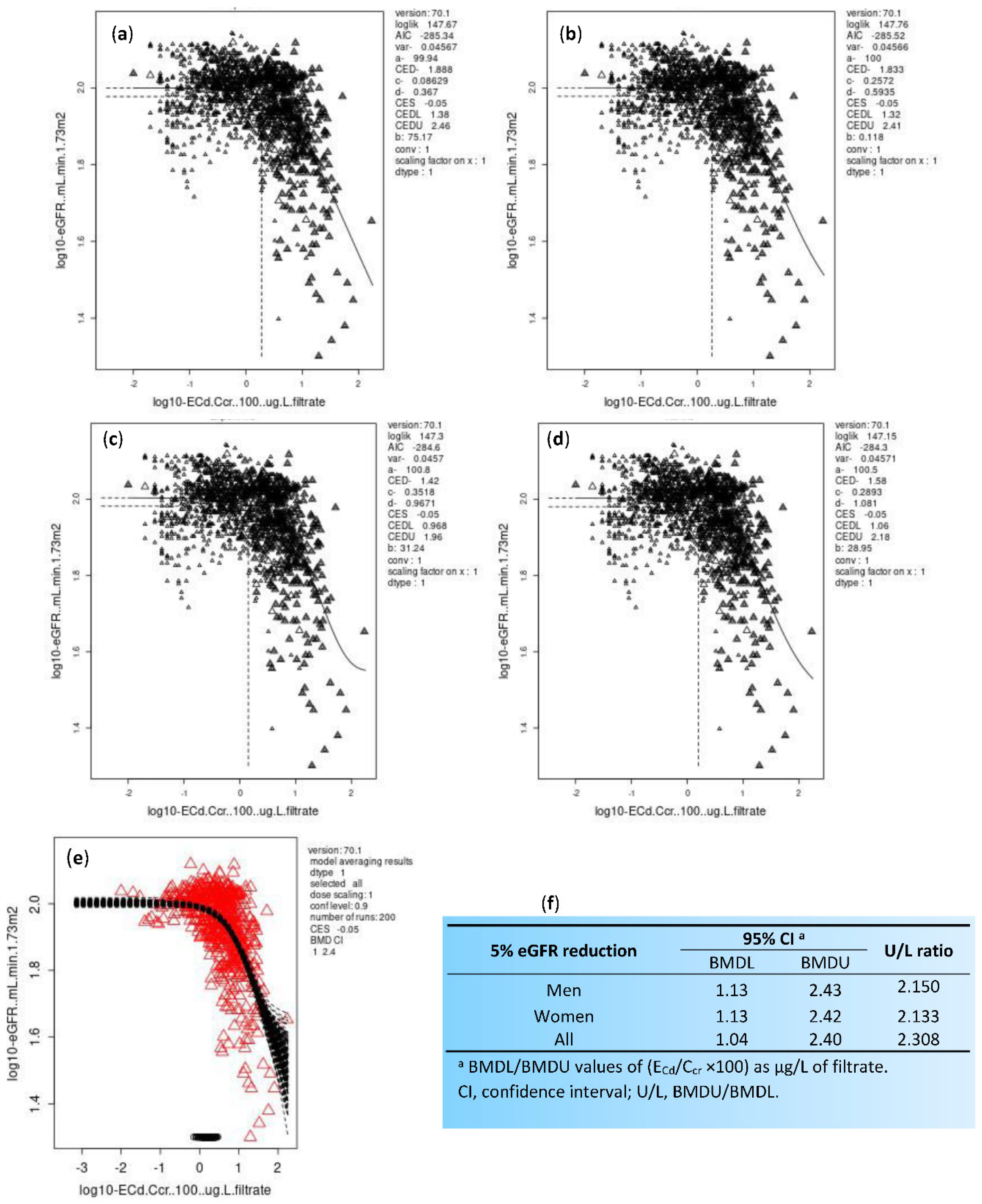

Table 1.
Associations of enhanced risk of CKD with blood and urinary cadmium.
| Study Location | Cadmium Exposure Metrics and Effects Observed | Reference |
|---|---|---|
| Thailand, n 1189 16−87 years mean age 43.2 years |
Risk of low eGFRa increased 6.2-fold and 10.6-fold, comparing urinary Cd levels 0.38–2.49 and ≥ 2.5 µg/g creatinine with ≤ 0.37 µg/g creatinine, respectively. | Satarug et al. 2022 [38]. |
| Korea, n 2992 20–65 years |
Increased risk of low eGFR (OR 1.97) in women was associate with blood Cd levels > 1.74 μg/L. | Myong et al. 2012 [39] |
| Korea, n 2005 ≥ 20 years |
Increased risk of low eGFR (OR 1.93) was associated with blood Cd in the top quartile (mean, 2.08 μg/L). | Chung et al. 2014 [40] |
| Taiwan, n 2447 mean age 55.1 years |
Increased risk of proteinuria was associated with urinary Cd (OR 2.67) and copper (OR 1.94). Mean urinary Cd in subjects with proteinuria (1.1 μg/L) was 27.3% higher than those without proteinuria. | Tsai et al. 2021 [41] |
| China n 683 (64.7% women) mean age 57.4 years |
Risk of elevated albumin excretion increased 2.98-fold, comparing urinary Cd levels ≤ 0.32 with > 1.72 µg/g creatinine. | Feng et al. 2022 [42] |
| Spain, n 1397 age 18–85 years |
Increased risks of albuminuriab by1.58-fold and 4.54-fold were associated with urinary Cd levels > 0.27 and > 0.54 µg/g creatinine, respectively | Grau-Perez et al. 2017 [43] |
| United States NHANES 1999 − 2006 n 14,778, ≥ 20 years |
Blood Cd levels ≥ 0.6 μg/L were associated with low eGFR (OR 1.32), albuminuria (OR 1.92) and low eGFR plus albuminuria (OR 2.91) | Navas-Acien et al. 2009 [44] |
| United States NHANES 1999 − 2006 n 5426, ≥ 20 years |
Blood Cd levels > 1 µg/L plus urinary Cd levels > 1 µg/g creatinine was associated with albuminuria (OR 1.63). Blood Cd levels > 1 µg/L were associated with low eGFR (OR 1.48) and albuminuria (OR 1.41). |
Ferraro et al. 2010 [45] |
| United States NHANES 2007 − 2012 n 12,577, ≥ 20 years |
Blood Cd levels > 0.61 μg/L were associated with low eGFR (OR 1.80) and albuminuria (OR 1.60). eGFR reduction due to Cd was more pronounced in the diabetics, hypertensive, or both |
Madrigal et al. 2019 [46] |
| United States NHANES 2009 − 2012 n 2926, ≥ 20 years |
Urinary Cd levels > 0.220 μg/L were associated with elevated albumin excretion, compared with urinary Cd levels < 0.126 μg/L. Blood Cd levels > 0.349 μg/L were associated with elevated albumin excretion, compared with blood Cd levels < 0.243 μg/L |
Zhu et al. 2019 [47] |
n, sample size; OR, odds ratio; aLow eGFR was defined as estimated glomerular filtration rate ≥ 60 mL/min/1.73 m2. bAlbuminuria was defined as urinary albumin-to-creatinine ratio ≥ 20 and 30 mg/g creatinine in men and women, respectively. NHANES, National Health and Nutrition Examination Survey.
Table 2.
Comparing excretion rates of various proteins and cadmium in residents of an area of Thailand with endemic cadmium contamination.
Table 2.
Comparing excretion rates of various proteins and cadmium in residents of an area of Thailand with endemic cadmium contamination.
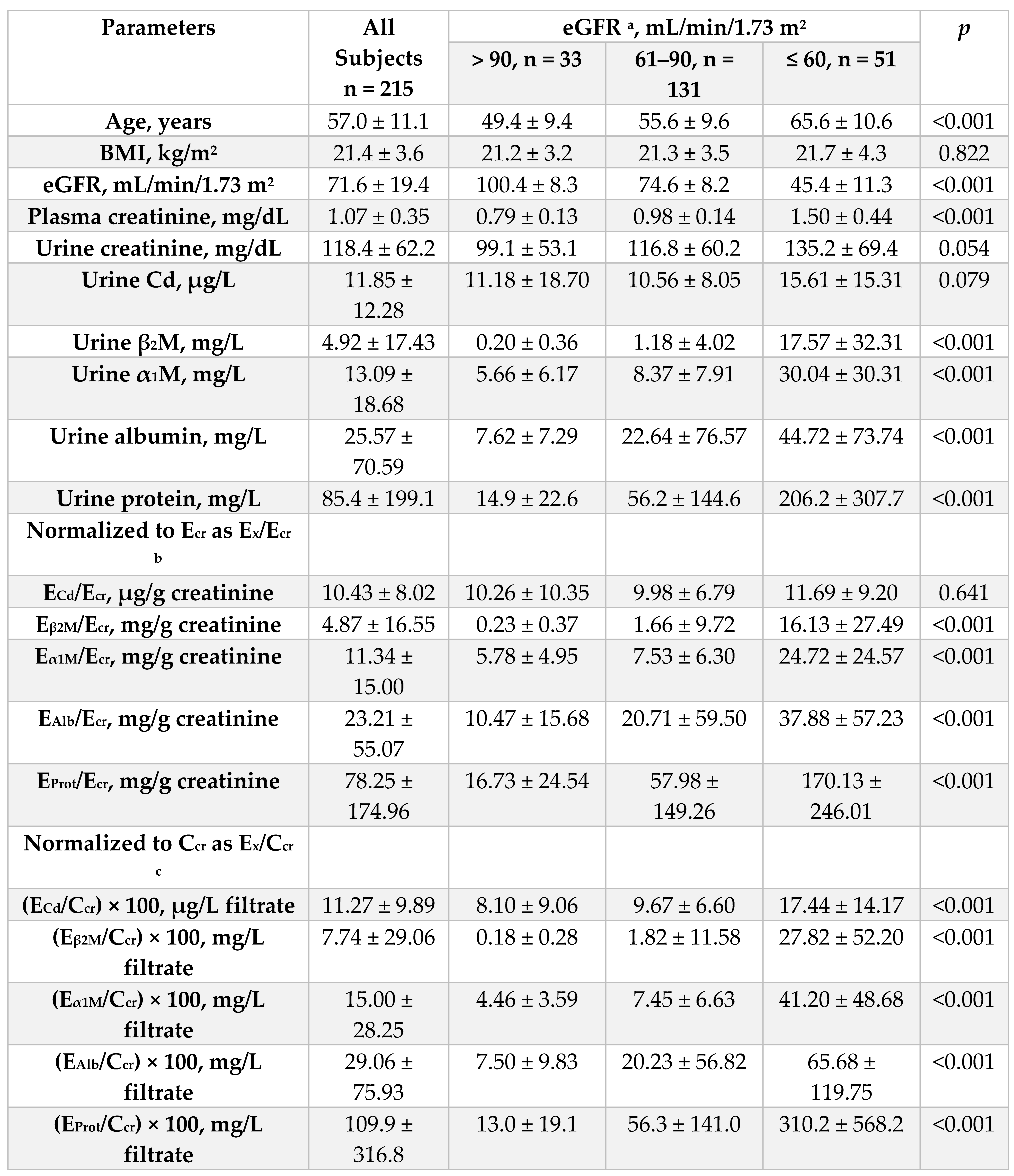 |
n, number of subjects; eGFR, estimated glomerular filtration rate; Ex, excretion of x; cr, creatinine; Ccr, creatinine clearance; Prot, protein; Cd, cadmium; a eGFR was determined by equations of the Chronic Kidney Disease Epidemiology Collaboration [65]. b Ex/Ecr = [x]u/[cr]u; c Ex/Ccr = [x]u[cr]p/[cr]u, where x = Prot or Cd. Data for all continuous variables are arithmetic means ± standard deviation (SD). For all tests, p ≤ 0.05 identifies statistical significance, determined by Kruskal–Wallis test for mean differences across three eGFR ranges. Data are from Satarug et al. 2023 [63].
Table 3.
Dose-response assessment using Ecr-normalized data.
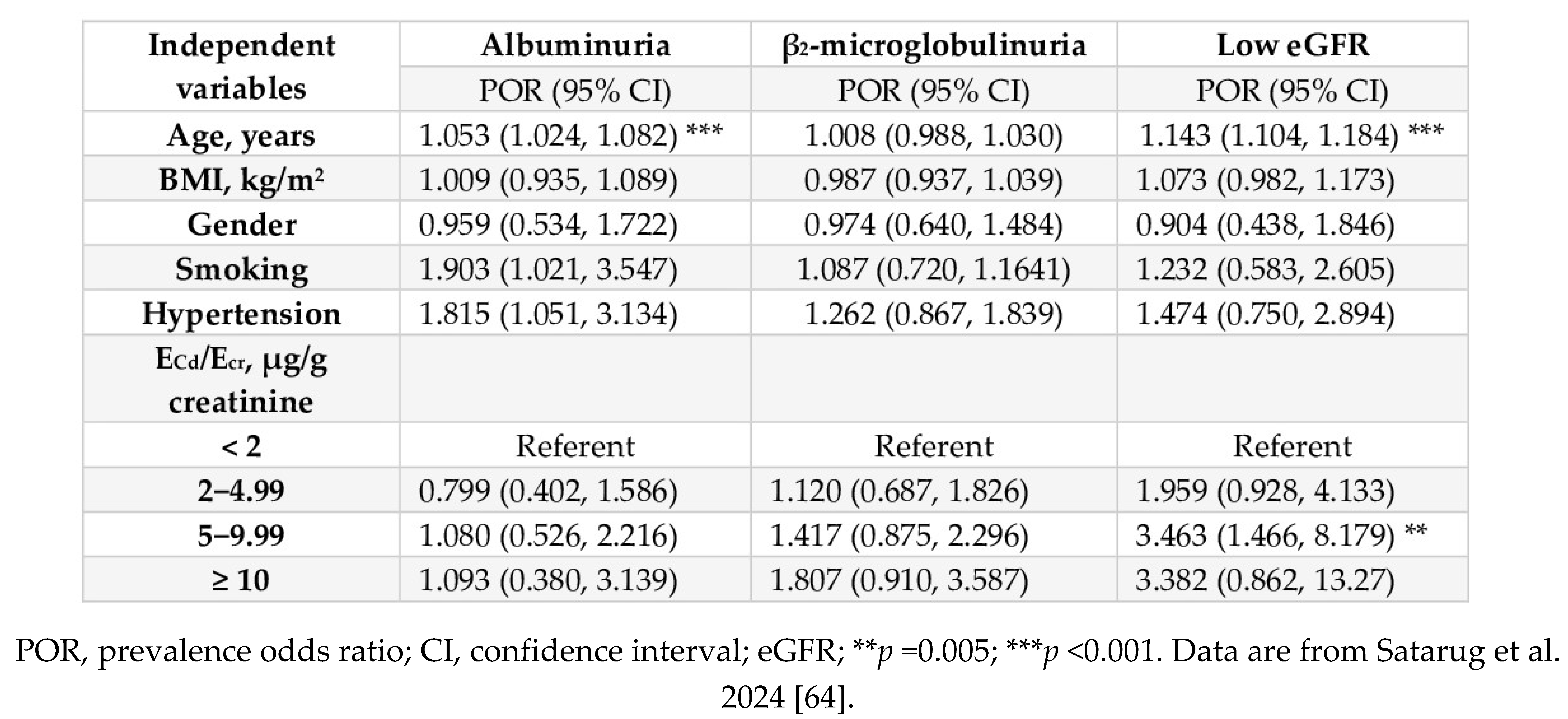 |
Table 4.
Dose-response assessment using Ccr-normalized data.
 |
Table 5.
Representative rates of filtration, excretion, catabolism, and transcytosis in normal and Cd-intoxicated proximal tubular cells.
Table 5.
Representative rates of filtration, excretion, catabolism, and transcytosis in normal and Cd-intoxicated proximal tubular cells.
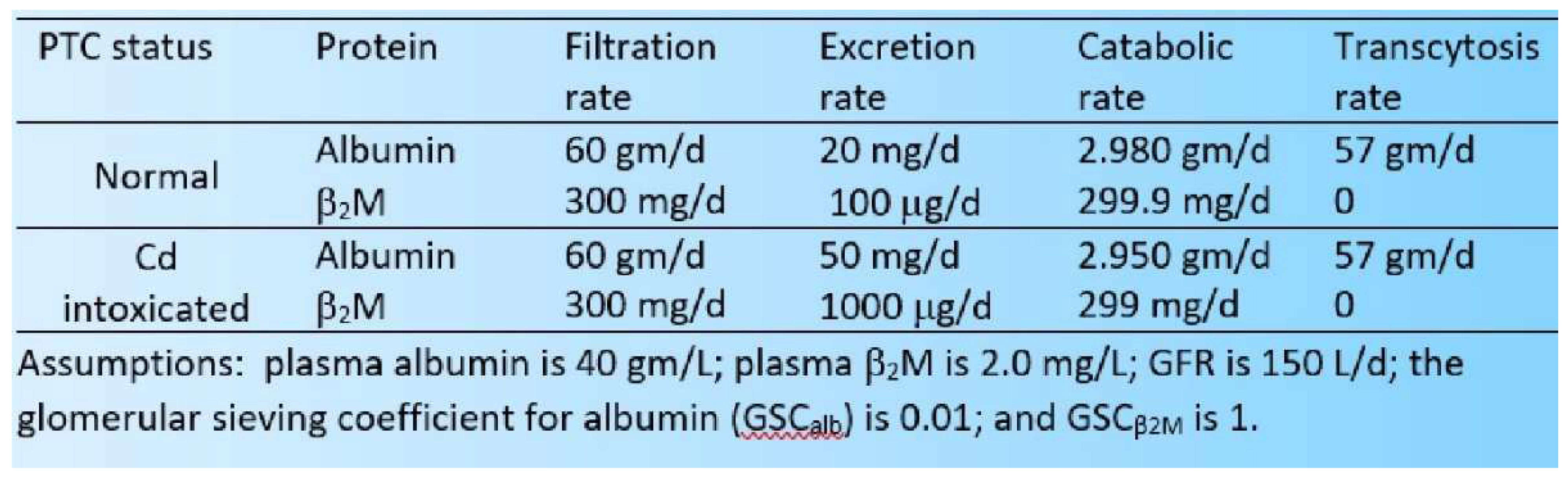 |
Table 6.
Cadmium accumulation in human kidneys.
| Country of Origin | Cadmium content, µg/g wet tissue weight | Reference |
|---|---|---|
| Australia, Autopsy, n 61, 2–89 years |
The percentage of kidney Cd content ≥ 50 µg/g was 3.3%.a Mean lung, liver and kidney Cd were 0.13, 0.95, and 15.45 µg/g, respectively. Mean kidney Cd was 16 times higher than liver. Peak hepatic and renal Cd levels were 1.5 and 25.9 µg/g. |
Satarug et al. [126] |
| United Kingdom, Autopsy, n 2700, nationwide (1978−1993) |
The percentage of kidney Cd content ≥ 50 µg/g was 3.9%. Mean kidney Cd content was 19 µg/g. Peak renal Cd level was 23 µg/g. |
Lyon et al. [127] |
| Canada (Quebec) Autopsy, n 314 |
Respective mean liver (kidney) Cd in smokers, ex-smokers and non-smokers were 2.5 (34.5), 1.4 (20.3) and 0.7(7.0) µg/g. Mean liver Cd in female smokers was higher than male smokers (3.6 vs. 2.2 µg/g). Peak hepatic and renal Cd levels were 2.2 and 44.2 µg/g. |
Benedetti et al. [128] |
| Greenland [101] Autopsy, n 95, 19−89 years |
Mean (range) liver Cd content was 5.3 (0.3−24.3) μg/g. Mean (range) kidney Cd content was 43.8 (6.7−126) μg/g. Peak hepatic and renal Cd levels were 1.97 and 22.3 μg/g. |
Johansen et al. [129] |
| Sweden Kidney transplant donors, n 109, 24−70 years, median age 51. |
Median kidney Cd was 12.9 μg/g. In non-smokers, renal Cd accumulation rate was 3.9 μg/g in every 10-year increase in age. An additional 3.7 μg/g accumulation rate in every 10-year smoking. In women who had serum ferritin levels ≤ 20 µg/L (depleted iron stores), renal Cd accumulation rate was 4.5 μg/g in every 10-year increase in age. |
Barregard et al. [130] |
a Kidney Cd content of 50 µg/g was used as a toxicological reference value [131].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



