
Submitted:
12 February 2024
Posted:
14 February 2024
You are already at the latest version
Abstract
Contrast-Induced Acute Kidney Injury (CI-AKI) remains a frequent iatrogenic condition since radiological procedures using intra-vascular iodinated contrast media (CM) are being widely administered for diagnostic and therapeutic purposes. Despite the improvement of the medical healthcare system worldwide, CI-AKI is still associated with direct short-term and indirect long-term outcomes including increased morbidity and mortality, specially, in patients under-lying pre-existing renal function impairment, cardiovascular disease or diabetes that could rap-idly progress into Chronic Kidney Disease. Although the RIFLE (Risk, Injury, Failure, Loss, End-Stage Kidney Disease), AKIN (Acute Kidney Injury Network) and KDIGO (Kidney Disease Improving Global Outcomes) clinical criteria and recommendation guidelines are based on tra-ditional “gold standard” biomarkers known as serum creatinine, glomerular filtration rate and urinary output, new reliable serum and urinary biomarkers are still needed for an effective uni-fied diagnostic strategy for AKI. Starting from previous and recent publications on the benefits and limitations of validated biomarkers responding to kidney injury, glomerular filtration and inflammation among others, this review unravels the role of new emerging biomarkers used alone or in combination, as reliable tools for early diagnosis and prognosis of CI-AKI, taking into account patients and procedures-risk factors towards a new clinical perspective.
Keywords:
Contrast-Induced Acute Kidney Injury
; Biomarkers
; Contrast Media
; Nephrotoxicity
1. Introduction
Iodinated contrast drugs are widely used in diagnostics and surgical procedures. However, it is well established that contrast media (CM) exposure causes iatrogenic renal function impairment, which incidence is highly increasing, especially, in subjects with preexisting cardiovascular, diabetes or renal disease. Therefore, CM-associated kidney dysfunction variates from slight serum creatinine (SCr) increase to severe Acute Kidney Injury (AKI) [1,2,3]. AKI secondary to CM injection has historically been called contrast-induced nephropathy (CIN) or contrast-induced AKI (CI-AKI). Worryingly, the enormous burden of CM used in contemporary clinical practice explains why CI-AKI is one of the top leading forms of hospital-acquired renal disease, being in fact, the third most common cause of AKI [4]. To date, CI-AKI is defined as a rise in SCr of 0.5 mg/dL (or higher) or 25% (or higher) from baseline, occurring within the 2-3 days after the intravascular injection of iodinated radiographic CM, that cannot be attributed to other direct sources [1,2,5,6,7,8,9,10]. Additionally, AKIN (Acute Kidney Injury Network) and KDIGO (Kidney Disease Improving Global Outcomes) guidelines suggested a rise in SCr≥0.3 mg/dL with oliguria after hospitalization as a new standard to follow [6,11,12]. Since SCr is less accurate, it is better to define CI-AKI as a decrease in SCr clearance or estimated Glomerular Filtration Rate (eGFR) by 30-60 mL/min [1,7,8,9]. In some cases, CI-AKI may cause a more severe renal function impairment with progressive oliguria, requiring dialysis, which is associated with high mortality [1,7,10].
The overall incidence of CI-AKI is low, however, this rate increases critically in high-risk populations, where mortality is also higher [1,2,3,6,7,8,9,13]. Consequently, it is necessary to early identify those high-risk patients to avoid post-procedure renal function impairment, to guide precise therapeutic management, and hence, to improve patient outcomes. Besides, there is an extremely narrow window for intervention, increasing the risk of fatality.
For all these reasons, the identification and selection of specific urinary and/or serum biomarkers for early diagnosis of renal cell damage rather than functional impairment due to their high sensitivity and specificity, may overcome the limitations of SCr and urinary output (UO) as “gold standard” normalizing markers of CM-associated renal failure.
2. Pathophysiology of CI-AKI
Renal hemodynamic changes and nephrotoxic effects occur immediately after intravascular administration of iodinated contrast drugs and could last many hours to days. These unwanted side effects could be aggravated by intrinsic CM properties like osmolality and viscosity, but also due to concentration and volume administration. Generally, CM produces a rapid non-physiological vasodilatation followed by a long vasoconstriction, resulting in a prompt decrease in renal flow. This process results in a vicious cycle of medullary ischemia which causes, in turn, reactive oxygen species (ROS) generation and consequently, vascular endothelial and tubular injury [1,7]. Direct effects of kidney injury from exposure to CM are due to tubular epithelium toxicity substantiated by disruption of cell integrity, leading to loss of function, apoptosis, and eventually, necrosis. CM also increases blood viscosity, decreases microcirculation, and decreases urine flow rate, which increases the time that CM remains in the body and could produce microvascular thrombosis. All of this leads to an abrupt decrease in GFR, therefore, in kidney function [1,8,10] (Figure 1). Notwithstanding the above, the diagnosis of CI-AKI in clinical practice could be catastrophically delayed, as it is radically based on the identification of a late elevation of SCr and/or a decrease in eGFR. Consequently, this delay in diagnosis which places patients at high risk of progressive kidney damage, highlights the critical need to identify other blood and/or urine sensitive and specific biomarkers of incipient tubular injury, leading to rapid prognosis and diagnosis of CI-AKI development.
3. Traditional “Gold Standard” Markers
Traditionally, the RIFLE (Risk, Injury, Failure, Loss, End-Stage Kidney Disease), AKIN and KDIGO guidelines recommend the use of classic markers for AKI diagnosis and management. However, increased levels of these markers suggest functional changes, not kidney damage [14]. Despite this, the reliability of these markers is questioned and still controversial due to their lack of specificity and sensitivity, and high variability [15]. Worryingly, when these parameters are measurable in serum or urine, at least, 50% of the renal function may be lost [16]. Taken together, these reasons compel us to consider these obsolete markers as “data normalizers” for new accurate biomarkers of kidney injury.
3.1. Serum creatinine (SCr)
The diagnosis of CI-AKI is commonly based on an absolute (≥0.5 mg/dL) or relative (≥25%) increase in SCr within 48-72 hours after intravascular CM administration [5]. Consequently, changes in SCr are used to estimate acute changes in renal function and SCr monitoring, remains the cornerstone for CIN diagnosis. Unfortunately, this confirms that SCr is the most widely used and accepted biomarker by nephrologists and the scientific community. However, SCr is not an adequate marker of renal function, mainly because there is no correlation between SCr and actual kidney function under nonstationary conditions. Thus, SCr becomes a retrospective, late, insensitive and misleading measure of kidney damage [16].
3.2. Glomerular filtration rate (GFR)
Commonly, renal function is defined as the filtration capacity of the kidney, which could be expressed as GFR. However, GFR does not cover all kidney function which also involves glomerular permeability, tubular function, and several specific functions, such as vitamin D metabolism and erythropoietin production [17]. In addition, GFR could be estimated (eGFR) based on the empirical Cockcroft-Gault, MDRD (Modification of Diet of Renal Disease) or CKD-EPI (Chronic Kidney Disease Epidemiology Collaboration) formulas [18,19], which involve SCr levels as a common variable. Currently, patients with CI-AKI are diagnosed with an eGFR of 30-60 mL/min [7]. However, the latter issue is of particular importance, as changes in SCr lag behind changes in GFR, leading to the possibility of progression of AKI stage despite actual improvement in renal function, a shortcoming that could be overcome with the availability of real-time assessment of GFR [20]. For this reason, the aforementioned concerns about SCr may also apply to the determination of GFR, as the interpretation of changes using one parameter alone is difficult. However, two recent clinical trials established the primary endpoint of drug efficacy by Iohexol plasma clearance-based GFR and by serum cystatin-based (eGFRecys), respectively [21,22].
3.3. Urinary Output (UO)
Nephrologists recognized UO as the most sensitive system for determining CI-AKI. Due to some limitations, it is not regularly used in the clinical setting, as it requires regular urine collection and catheterization of the patient. Surprisingly, in a retrospective study, UO captured >40% AKI results than SCr [23].
4. Novel Biomarkers: The necessity for a precise CI-AKI diagnosis
In recent decades, the identification of new biomarkers of AKI has been the subject of interest by scientists worldwide. However, the predictive, diagnostic and prognostic ability of biomarkers in the context of iodinated contrast administration, has been less studied. In recent years, many additional potential biomarkers have been newly described for the early detection of tubular dysfunction/lesion associated with CM administration, to reliably measure CI-AKI, and thus prevent patient outcomes. Some of them are well characterized and categorized and could be divided into different groups in response to different physiological conditions: some involved in glomerular filtration, others related to the inflammatory response and tubular cell injury or with a not well-defined relationship with the disease and new emergent biomarkers under study. Figure 2 schematically represents the traditional and novel biomarkers described for CI-AKI.
4.1. Glomerular filtration biomarkers
4.1.1. Cystatin C (CysC)
CysC is a small molecule freely filtered by the glomerulus, and subsequently reabsorbed and metabolized by the proximal tubule [24]. Compared with SCr, serum CysC concentration (sCysC) is less dependent on age, gender, muscle mass and nutrition and therefore, more reliably predicts deterioration of renal function, becoming a sensitive marker of kidney injury. An increase in sCysC levels reflects a decrease in GFR and therefore, there is an inherent delay between renal injury and a detectable increase in its levels [25]. Thus, sCysC increases more rapidly than SCr when GFR decreases [14,15]. CysC is usually undetectable in the urine of patients with normal renal function; however, tubular injury could result in measurable urinary levels, suggesting urinary CysC as a potential biomarker for AKI [25,26].
Regarding CI-AKI, the study of CKD patients undergoing coronary (CA) or peripheral angiography demonstrated that increased sCyC is a reliable marker to rule out CI-AKI and an independent predictor of death and dialysis [14,27,28]. Complementary studies in patients undergoing coronary angiography and/or therapeutic percutaneous coronary intervention (PCI) showed that sCysC is incremented 24 hours after CM application, and this correlated with CI-AKI and was associated with a higher incidence of adverse events at one year [8,29,30,31,32,33]. Finally, a recent publication stated that sCysC at 24 hours was the best biomarker for CIN diagnosis, while baseline levels of other common biomarkers were the best predictors of prognosis [34].
4.1.2. α1-Microglobulin (α1-m)
α1-m is a member of the lipocalin family of proteins that is synthesized in the liver, freely filtered by glomeruli and reabsorbed by the renal proximal tubular cells, where it is catabolized. The α1-m form is stable and, under normal conditions, appears very poorly filtered in the final excreted urine [35]. Therefore, urine levels above the reference values could indicate proximal tubular damage, resulting α1-m as a preferred biomarker. Terzi et al. showed that α1-m can early predict the development of sepsis-associated AKI (SA-AKI) in critically ill patients by ensuring proximal tubular dysfunction [35]. Furthermore, a recent study concluded that α1-m is a suitable biomarker for early-stage kidney injury detection after cardiac surgery [36].
4.1.3. β2-Microglobulin (β2-m)
β2-m is a little protein, expressed on the cell surface of every nucleated cell and which is filtrated by the glomerulus and almost all β2-m proteins have undergone reabsorption and catabolism by the proximal tubular cells [15]. Increased levels of β2-m excretion in urine have been described as an early sign of tubular dysfunction due to many causes, such as exposure to nephrotoxic substances, cardiac surgery and renal transplantation, preceding by 4-5 days the rise in serum creatinine levels. However, the disadvantage of β2-m as a biomarker is its instability in the urine and fast degradation in room temperature and urine with pH <6.0 [37]. Recent publications suggest that β2-m could be a suitable biomarker for predicting prognosis in CI-AKI [34,38].
4.1.4. Microalbuminuria
The term microalbuminuria indicates urinary albumin at a concentration that is below the threshold for albumin detection by conventional measurement protocols and its value ranges between 30-300 mg/L [15]. It is suggested to be an important marker of glomerular structure and function alterations and it was designated as a biomarker to investigate the attenuation of CI-AKI by N-acetylcysteine [39]. In addition, a recent clinical study shows that increased preprocedural urinary microalbumin is associated with a high risk of renal deterioration after CA [40].
4.1.5. Proteinuria
Increased urinary protein excretion (proteinuria) is the result of alterations in the glomerular filtration barrier, generally associated with specific podocyte damage. Therefore, total urinary protein has been highlighted as a diagnostic marker and as a predictive factor for progressive loss of renal function in clinical and non-clinical settings [41,42,43]. Specifically, in CI-AKI it has been demonstrated that protenuria is an important risk factor and an independent indicator of 1-year mortality in patients with cerebrovascular disease [44].
4.2. Inflammatory biomarkers
4.2.1. Monocyte Chemoattractant Protein 1 (MCP-1)
MCP-1 is a potent chemotactic factor for monocytes and macrophages involved in ischemic and toxic AKI. However, its potential use as a biomarker has been less well studied. Several studies have shown that urinary MCP-1 expression (uMCP-1) is increased in both murine models and in patients with kidney injury [45]. Additionally, recent studies have shown that uMCP-1 in combination with other markers (e.g., epidermal growth factor –EGF-, kidney injury molecule-1 -KIM-1-, neutrophil gelatinase-associated lipocalin –NGAL-) appears to represent a potent diagnostic and prognostic biomarker of tubulointerstitial injury and repair [16,45,46,47]. Therefore, MCP-1 alone or in combination with other molecules, could be considered a useful biomarker in AKI, which could also be extrapolated to CI-AKI.
4.2.2. Interleukin 18 (IL-18)
IL-18 is a pro-inflammatory cytokine released by proximal tubular epithelial cells in response to injury. After kidney injury, IL-18 is massively secreted into the urine and increases in the first 6 to 12 hours before a significant decline in renal function and remains elevated for up to 48 hours [25]. Human studies demonstrated that urinary IL-18 (uIL-18) levels were significantly higher in patients with AKI than in those without AKI at 24 and 48 hours before SCr increased [43,48,49]. Surprisingly, a similar study in elderly patients undergoing gadolinium-enhanced magnetic resonance imaging (MRI) displayed an increase in uIL-18 after CM administration for 24 hours, compared to a delayed increase in SCr levels [50]. However, several clinical performed to evaluate new diagnostic biomarkers of CI-AKI following CA or PCI, indicated that no statistically significant differences in uIL-18 were observed in patients with CI-AKI compared to patients without CI-AKI; neither were significant changes observed between uIL-18 before and after the intervention [51,52].
4.3. Kidney damage biomarkers
4.3.1. Neutrophil Gelatinase-Associated Lipocalin (NGAL)
NGAL is a protein of the lipocalin family that covalently binds to neutrophil gelatinase and is dramatically upregulated in the kidneys after ischemic or toxic damage [53,54]. NGAL has been shown to decrease apoptosis and increase tubular cell proliferation, favoring renal tissue recovery after damage. This particular role may explain the sustained elevated urinary NGAL (uNGAL) levels observed during the days following renal injury [55]. Therefore, NGAL may also be detected in the proximal tubular epithelium due to the failure of reabsorption of filtered NGAL [56].
Surprisingly, NGAL increases rapidly in a dose-dependent manner and is detectable at early points (3 hours after kidney damage and peaks at 6-12 hours). Moreover, its elevation could persist markedly for up to 5 days if the initial injury is severe. For this reason, among all new biomarkers, NGAL is one of the most widely investigated.
One of the most ambitious studies based on large cohorts of patients, both children and adults, receiving contrast agents and undergoing cardiac catheterization, intra-arterial coronary angiography or computed tomography (CT), revealed a very good performance of plasma and uNGAL in the prediction of CI-AKI [57,58].
More recently, uNGAL monitoring studies revealed that NGAL also predicted the severity of CI-AKI into CKD and/or hemodialysis progression, demonstrating that NGAL is potentially superior compared to conventional markers of nephropathy after invasive coronary procedures with contrast agents [59,60,61,62,63]. However, ANTI-CI-AKI clinical trial study concluded that uNGAL was not able to predict CI-AKI and was an inadequate tool to guide an early intervention strategy to prevent CI-AKI outcomes [64] and further studies will be necessary.
4.3.2. Kidney Injury Molecule 1 (KIM-1)
KIM-1 is a type I transmembrane glycoprotein that is poorly expressed in the kidneys of healthy subjects. However, following ischemia/reperfusion injury (IRI) and nephrotoxic exposure, KIM-1 is dramatically overexpressed in the proximal tubular epithelium in both rodent models [65,66] and humans [67]. Following kidney injury, the extracellular domain of KIM-1 is released from the tubular epithelial cells in a metalloproteinase-dependent manner. This release, in combination with the persistent increase of renal KIM-1 synthesis, leads to a rapid increase in exclusively urinary KIM-1 after 48 hours [68].
Recent clinical studies have shown that urinary KIM-1 concentration (uKIM-1) is higher in patients with AKI due to ischemia and hypoperfusion, nephrotoxins, CIN nephropathy and cardiac surgery compared to controls, and also that it is a predictor of the risk of developing AKI [69,70,71]. Since KIM-1 is defined as an effective early biomarker in AKI, several rodent models showed that uKIM-1 concentration was elevated 12 hours following CM administration [72,73]. Furthermore, differences in uKIM-1 production were found in pre-existing kidney injury models of hypertension, diabetes and nephropathy subjected to CM administration [74]. Multiple human clinical studies confirm the potential use of uKIM-1 as an early valuable marker for CIN diagnosis. In a large study of more than 3000 patients undergoing CA, KIM-1 levels were found to be significantly increased in the urine of CIN patients at the sixth hour compared to baseline [75]. These results confirmed a previous study in which KIM-1 was measured 12 hours after cardiac catheterization in humans and exhibited a good predictive value for CI-AKI diagnosis with high sensitivity and specificity [76].
4.3.3. Insulin-like Growth Factor-Binding Protein 7 (IGFBP-7) and Tissue Inhibitor of Metalloproteinases-2 (TIMP-2)
IGFBP-7 and TIMP-2 are master regulatory biomarkers of G1 cell cycle arrest, predominantly expressed in proximal and distal tubular cells in response to DNA damage. Unlike many previously studied biomarkers, both are markers of cellular stress in an early phase of tubular cell damage caused by a wide variety of triggers and could act as a protective mechanism for cell injury [77,78]. Remarkably, these two proteins are discussed in combination because some preclinical studies demonstrated their superiority when used together to predict advanced AKI stages compared to other biomarkers [79].
In 2014, the FDA approved the first point-of-care device (NephroCheck test) that allows the determination of both urinary IGFBP-7 and TIMP-2 in critically ill patients with an increased risk of developing moderate-to-severe AKI. The NephroCheck test anticipates the diagnosis of AKI, therefore reducing the social and health care costs associated with worsening disease in these patients [80,81]. Surprisingly, other clinical and observational studies reported that the combined IGFBP-7/TIMP-2 test was the strongest predictor of AKI and significantly improved the risk assessment after major surgery [81]. Despite this, the impact of CM on these biomarkers and the evaluation of the potential development of CI-AKI have not yet been addressed.
4.3.4. Liver Fatty Acid-Binding Protein (L-FABP)
L-FABP is a protein that is expressed in several tissues, but predominantly localizes to the renal proximal tubule epithelium and is excreted into the tubular lumen before binding to peroxisomal toxic products [82,83,84]. Urinary L-FABP (uL-FABP) has been extensively studied in preclinical and clinical models and has been suggested as a potential biomarker in a variety of pathological conditions, such as AKI, CKD, diabetic nephropathy, IgA nephropathy and CI-AKI [85,86].
Nakamura et al. demonstrated that uL-FABP increase was associated with CIN. Remarkably, before angiography, uL-FABP concentration was significantly higher in 13 of 66 patients suffering from CIN compared to the non-CIN group or healthy volunteers [87], suggesting that uL-FABP levels could clinically serve as a useful predictive biomarker to detect CI-AKI onset before CM exposure.
4.3.5. N-acetyl-β-d-glucosaminidase (NAG)
NAG is a lysosomal enzyme that is expressed mainly in the brush border of proximal renal tubular cells but also is localized in the liver, brain and spleen [88]. Due to its nature, NAG does not cross the glomerular barrier and therefore, urinary NAG release reflects tubular impairment.
Increased NAG levels have been described in multiple AKI onsets showing, in all cases a high sensitivity for detecting AKI [88,89,90,91]. However, increased NAG levels have been reported in a variety of non-clinical AKI conditions, limiting the use of NAG as a marker of AKI in some settings [92].
Comparative investigations suggested that NAG is also a valuable biomarker in CI-AKI, exclusively in patients undergoing CA and/or therapeutic PCI. A robust study showed that urinary NAG (uNAG) and sCr were significantly increased on days 1 and 2 after radiocontrast injection, compared to patients without CI-AKI. Moreover, uNAG levels peaked earlier and increased more than sCr levels [93]. Clinical studies in children corroborated that uNAG detection may contribute to a more accurate diagnosis of CI-AKI by indicating increased stress on the kidneys after CA [94,95].
4.3.6. α, π glutathione S-transferase (α-GST, π-GST)
α-GST and π-GST are promising proximal and distal tubular cytosolic enzymes respectively, that are considered promising biomarkers for early detection of AKI. In AKI, a single urinary π-GST measurement performed better than α-GST at predicting dialysis requirement or death, whereas α-GST performed better in patients with AKI in stage 1 or 2. However, neither marker had good prognostic discrimination [96]. Finally, further other investigations showed that urinary GSTs predicted AKI progression or hospital mortality after cardiovascular surgery, where CM administration is correlated with kidney damage following an increase in urinary biomarkers [97,98,99].
4.4. Emerging novel biomarkers
Among the classical CI-AKI biomarkers, a large number of promising molecules have been constantly investigated to assess their predictive and intrinsic diagnostic value in a wide spectrum of renal disorders, including CI-AKI, to improve patient outcome. However, some of them are exclusively studied in animal models although some are not yet in CI-AKI models. Hence, there is an open need to discover, evaluate and validate the best-performing biomarkers in clinical trials, and, consequently, to extrapolate them to clinical practice. These include:
4.4.1. Renalase
Renalase is a novel catecholamine-metabolizing amine oxidase synthesized mainly by proximal tubular cells and secreted into the urine and bloodstream, which plays a key role in blood pressure regulation [100]. In animal models, renalase-deficient mice displayed a severe IRI reflected by higher SCr and a significant increase in tubular inflammation, apoptosis and necrosis, which was partially alleviated by renalase pretreatment [101]. Renalase was also documented to ameliorate cisplatin-induced AKI [102].
Singularly, a recent study of ioversol-induced CI-AKI showed an exceptional protective effect of renalase pretreatment on renal function and kidney morphology in rats [103]. To date, only one clinical study is available to evaluate the urinary renalase concentration in patients with preserved renal function undergoing CA/PCI interventions, in which it was observed that their urinary levels were reduced after these interventions [103]. However, further studies will be required to validate renalase as a diagnostic marker of CI-AKI, and also to assess that the exogenous recombinant renalase administration could serve as a preventive therapeutic agent [104,105].
4.4.2. Connective Tissue Growth Factor (CTGF)
CTGF is an important profibrotic factor that is upregulated in kidney diseases. When endogenous CTGF is artificially suppressed in experimental models of kidney injury, renal function is restored [106]. In a murine model of CI-AKI, CTGF gene expression levels increased 2 days after CM administration in nephrectomized mice compared to the non-CM infusion group [107]. Despite this, clinical correlations have not yet been addressed and further studies will be necessary to evaluate CTGF protein as a kidney injury biomarker in humans.
4.4.3. Uromodulin
Uromodulin, also known as Tamm-Horsfall protein, is a glycoprotein localized mainly in renal tubular cells lining the thick ascending limb of the loop of Henle. In the last decade, uromodulin has been implicated in the pathophysiology of several diseases, including AKI and CKD, showing a protective role through downregulation of interstitial inflammation [108]. Surprisingly, several publications expressed an exponential interest in the role of uromodulin in CM nephrotoxicity, showing a huge urinary decrease after CM administration in patients, but also in canine experimental models [109,110,111]. Recent publications have demonstrated that a lower uromodulin-to-creatinine ratio is associated with AKI after cardiac surgery. Overall, the consideration of uromodulin as a biomarker in clinical measures could be considered to minimize the risk of developing AKI/CI-AKI [112,113].
4.4.4. Vascular Endothelial Growth Factor (VEGF)
VEGF is an endothelial-specific growth factor that promotes endothelium proliferation, differentiation, survival and mediates vasodilatation, microvascular permeability and matrix remodeling. In the kidney, it is prominently expressed in tubular epithelial cells and glomerular podocytes and is associated with the pathophysiology of diabetic nephropathy, glomerulosclerosis and tubule-interstitial fibrosis [114].
Despite the lack of updated clinical results regarding CI-AKI, a single study of CM administration in rats suggested that VEGF protein levels in kidney tissue were significantly higher compared to controls and consequently, it was correlated with advanced kidney damage. Interestingly, paricalcitol pretreatment ameliorated kidney injury markers, including VEGF levels, thus offering the opportunity to prevent CI-AKI [115].
4.4.5. Osteopontin (OPN)
OPN is a glycoprotein expressed in bone, immune, smooth muscle, epithelial and endothelial cells and plays an important role in bone mineralization and resorption. In addition, OPN is found in the kidneys and urine and its expression results elevated in several renal pathologies [116], suggesting its potential role as a novel biomarker. Besides this, clinical trials and observational studies demonstrated that OPN had a positive association with the risk of AKI in patients undergoing CA [117] and could predict the patient outcome after cardiac arrest [118].
4.4.6. Fractional Excretion of Sodium (FENa)
FENa is the percentage of the sodium filtered by the kidney that is excreted in the urine. Principally, under normal conditions, most of the sodium is reabsorbed by intact tubular cells, but another small part is excreted in the urine. Therefore, FENa could be calculated to assess changes in renal blood flow and kidney tubular damage under pathological conditions [119].
In a clinical study, it was observed that patients with oliguric AKI presented <1% FENa in pre-renal AKI and >3% in acute tubular necrosis (ATN), demonstrating the applicability of FENa as a prognostic marker [119]. Subsequently, different studies were conducted to evaluate the effects of CM exposure in human kidneys, indicating that CM administration is associated with increased urinary FENa [120,121]. These findings were also corroborated in animal models [122,123].
4.4.7. Hepcidin
Hepcidin is a small peptide hormone principally produced in hepatocytes, but also in other tissues such as the kidney or brain. In the kidney, hepcidin is freely filtered by the glomeruli with significant tubular uptake and catabolism, which could be excreted in the urine and also found in plasma [124]. Surprisingly, clinical researchers determined that lower levels of hepcidin could predict the risk for AKI development [125,126,127]. However, in patients undergoing PCI, serum hepcidin concentration increased at 4 and 8 hours after CM administration, while urine hepcidin was significantly lower in PCI patients with CI-AKI compared with baseline [128]. Consequently, early changes in hepcidin could predict a later CI-AKI onset.
4.4.8. Retinal Binding Protein (RBP)
RBP is a carrier protein filtered mainly by the glomeruli and reabsorbed by the proximal tubules of the kidney. The relation of variation in serum RBP levels was initially studied in a small cohort of patients with kidney disease and healthy volunteers, in whom the urinary concentration of RBP was differentially excreted, leading to the conclusion that RBP could be useful for the diagnosis and monitoring of kidney disease progression [129]. Accordingly, in a randomized controlled study, urinary RBP concentration was rapidly elevated in patients undergoing peripheral arterial angiography [130].
4.4.9. Vitamin D Binding Protein (VDBP)
VDBP is filtered in the glomerulus, reabsorbed by proximal tubule epithelial cells and subsequently catabolized, thus reducing urinary excretion. After tubular injury, increased urinary VDBP (uVDBP) levels are expected to be found, reflecting renal damage. Chaykovska et al. demonstrated that uVDBP is a potent biomarker of major renal adverse effects after CA intervention, concluding that uVDBP concentration 24 hours after CM administration was predictive for dialysis and death [131].
4.4.10. Gamma Glutamyl Transferase (GGT)
GGT is an enzyme localized in the brush border of the renal proximal tubules that appears in the urine (uGGT) when damage occurs. Early clinical studies focused on tubular toxicity due to CM exposure showed a relevant early increase in uGGT enzyme activity in patients undergoing radiological examination with intravascular injection of CM [132]. Recently, the same results were obtained in patients undergoing PCI, where urinary GGT showed a predictive value for CI-AKI progression [133].
4.4.11. Midkine (MK)
MK is a heparin-binding growth factor that regulates inflammation, cell growth, survival and migration. In the kidney, MK is expressed in both proximal and distal tubular epithelial cells. Strikingly, MK was found to be significantly elevated 2, 4, and 8 hours after CM exposure, exclusively in patients undergoing PCI, and then, returned to baseline after 24 hours and started to decrease after 2 days [134], suggesting MK determination as a great opportunity for CI-AKI treatment.
4.4.12. MicroRNAs (miRNAs)
miRNAs are short, non-protein-coding RNA molecules that regulate gene expression at the post-transcriptional level by mRNA repression and are involved in multiple cell mechanisms, such as proliferation, differentiation, death or inflammation. For this reason, miRNAs differential expression is principally related to pathophysiological conditions, including kidney injury [15,135]. Among others, miR-21 has been extensively studied in the kidney, where it plays a crucial role in cell proliferation and downregulation of apoptosis after renal IRI [136], while serum and urine levels of miR-21 also predict AKI in cardiac surgery patients [137]. In particular, different preclinical studies that were validated in humans revealed that circulating levels of miR-188, miR-30a, miR-30c and miR-30e should be considered as early biomarkers in CI-AKI [138].
4.4.13. Clusterin
Clusterin is a sulfated glycoprotein mainly present in the cytoplasm of proximal and distal convoluted tubules [139]. In the context of kidney injury (nephrotoxicity, ischemia, surgery) in experimental models, it has been suggested that clusterin could play an anti-apoptotic role in favoring cell protection and regeneration [140].
In a variety of nephrotoxic models including cisplatin, higher urinary levels of clusterin outperformed BUN and SCr for detecting proximal tubular injury even in the absence of functional effects and was correlated with positive clusterin kidney immunostaining [140,141]. Interestingly, in ischemia-reperfusion models, clusterin deficiency worsens renal inflammation and kidney fibrosis after IRI, suggesting a crucial role in kidney cell repair and proliferation [142,143]. Despite the lack of studies indicating the predictive potential value of clusterin in CI-AKI, a controlled clinical trial performed by Da et al. has been recently published, suggesting for the first time that clusterin could detect early nephrotoxicity and predict AKI when compared AKI cases with non-AKI controls [144]. This study opens the possibility of using clusterin as a future biomarker in CI-AKI.
4.4.14. Calbindin
Calbindin is an intracellular protein involved in the regulation of calcium reabsorption that is commonly expressed and localized in the distal tubule and the proximal part of the collecting ducts. As a kidney injury marker, calbindin has been studied in rat and sheep nephrotoxic models, thus reflecting changes in urinary excretion without histological alterations [145,146]. In humans, calbindin concentration was significantly higher in urine from patients receiving cisplatin chemotherapy while SCr levels remained unchanged [147,148]. In correlation, calbindin was the most consistently and significantly altered urinary marker in patients following partial nephrectomy, suggesting its potential role as an early predictor of AKI and CI-AKI [149], although future studies will have to be developed to demonstrate its effectiveness.
5. Combination of Biomarkers: a Future Approach
To date, most preclinical and clinical studies on kidney diseases only validate one biomarker rather than a combination of several, limiting the ability to determine whether several specific panels of biomarkers are more specific and predictive than one biomarker alone. Biomarker combinations could be integrated into clinical practice using viable high-throughput technology to increase the ability to detect and diagnose multiple renal disorders early, unravel new pathophysiological mechanisms and consequently, prevent undesirable long-term patient outcomes.
Vaidya et al. suggested that comparative values of multiple urinary biomarkers detection (NGAL, Hepatocyte Growth Factor (HGF), VEGF, Protein and KIM-1) were associated with sensitive and specific prognosis and diagnosis of AKI in humans [92]. Furthermore, in a cross-sectional study, the combination of urinary Matrix Metalloproteinase 9 (MMP-9), KIM-1 and NAG markers allowed AKI diagnosis earlier than an increase in SCr [69]. However, the results of the SAPHIRE study demonstrated that performing exclusively urinary TIMP-2/IGFBP7 significantly improved AKI risk stratification, thus providing additional information on clinical variables [79]. In a cohort study based on major surgeries, it was proposed that urinary NGAL and L-FABP determination may improve the diagnostic yield of AKI [150]. In addition, the combination of urinary IL-18 and KIM-1 concentrations had a very good predictive value for predicting AKI stage 3 or death, thus identifying high-risk patients after cardiac surgery [151]. Moreover, in studies on obstructive nephropathy and cisplatin-induced nephrotoxicity, the combined detection of the EGF/MCP-1 ratio, urinary NGAL and urinary KIM-1 outperformed that of any of the biomarkers alone in predicting progressive renal damage, thus, avoiding undesirable long-term outcomes [46,47]. Finally, several recent investigations focusing on contrast-induced nephrotoxicity deciphered multiple biomarker combinations that successfully predicted early CI-AKI, predominantly in patients undergoing CA. While Wybraniez et al. proposed that post-procedural determination of urinary KIM-1 and IL-18 predicted CI-AKI; Connolly et al. suggested that serum L-FABP and plasma NGAL were the best combination to predict early CI-AKI [52,152]. Finally, Banda et al. stated that serum CysC at 24 hours was the best biomarker for CIN diagnosis, while baseline levels of serum IL-18, β-2M and TNFα were the best for predicting prognosis [34].
6. Conclusions
Iodinated contrast drugs are widely used in various clinical procedures, increasing the patient’s risk of mild to severe kidney alterations and the development of CI-AKI. The absence of current pharmacological treatments for AKI makes intensive care the only possible supportive tool and, therefore, new emerging therapeutic approaches are greatly needed.
However, so far there is no consensus among experts on which biomarker panel neither for AKI nor for CI-AKI diagnosis and prognosis. This is of great concern because the lack of well-established worldwide clinical guidelines for CI-AKI prevention and management, could be detrimental to patient recovery and survival. Therefore, we envision a clinical setting in which a single urine/plasma preparation will be rapidly analyzed for simultaneous measurement of a stringent panel of desired biomarkers for kidney disease, using a validated and cost-effective high-throughput assay that allows for rapid in-hospital patient monitoring, thus preventing patients from suffering poor outcomes and improving renal therapies.
Author Contributions
Conceptualization, M.A.G-N., C.G-G. and A.L.; methodology M.A.G-N. and C.G-G. ; software, M.A.G-N., C.G-G. and L.V-R.; validation, L.V-R. and A.L.; formal analysis, M.A.G-N., C.G-G. M.A.G., L.B., L. V-R., A.L.; investigation, M.A.G-N., C.G-G. M.A.G., L.B., L. V-R., A.L.; resources, M.A.G. and A.L.; data curation, L.V-R., L.B. and A.L.; writing—original draft preparation, M.A.G-N., C.G-G. and L.V-R.; writing—review and editing, L-V-R., M.A.G., L.B. and A.L.; visualization, M.A.G. and L.B.; supervision, L.V-R. and A.L.; project administration, A.L.; funding acquisition, M.A.G. and A.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Spanish Ministry of Economy and Competitiveness Instituto de Salud Carlos III-Fondo de Investigación en Salud (grant numbers:, PI20/01577, ICI21/00111 and CIBERCV, cofinanced by Fondo Europeo de Desarrollo Regional (FEDER) Funds from the European Commission, “A way of making Europe”), ISCIII-RICORS2040 (Kidney Disease, grant number RD21/0005/0029), Comunidad de Madrid (grant number 2022/BMD-7223 (CIFRA_COR-CM), and Fundación Mutua Madrileña (XX Convocatoria de Ayudas a la Investigación en Salud).
Institutional Review Board Statement
Ethical review and approval were waived for this study due to we have not conducted basic or clinical research, but rather we have conducted a literature review article and state of the art of the specific topic biomarkers in contrast-induced acute kidney injury.
Data Availability Statement
No new data have been created in this review article, only a review of the state of the art of biomarkers in acute renal failure-induced by iodinated contrast agents, and all the data noted have been extracted from the relevant literature in the article.
Acknowledgments
The Renal Physiopathology Laboratory would like to thank Dr. Alberto Tejedor, may he rest in peace, for all his efforts in the research of acute renal failure and for being an example for us.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Andreucci, M.; Solomon, R.; Tasanarong, A. Side effects of radiographic contrast media: pathogenesis, risk factors, and prevention. BioMed Res Int 2014, 2014, 741018. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Nikolsky, E. Contrast-induced nephropathy: definition, epidemiology, and patients at risk. Kidney Int Suppl 2006, 100, S11–15. [Google Scholar] [CrossRef] [PubMed]
- Weisbord, S.D.; Palevsky, P.M. Contrast-associated Acute Kidney Injury. Crit Care Clin 2015, 31, 725–735. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.J.; Tsai, S.F. Patients with Different Stages of Chronic Kidney Disease Undergoing Intravenous Contrast-Enhanced Computed Tomography-The Incidence of Contrast-Associated Acute Kidney Injury. Diagnostics (Basel) 2022, 12, 864. [Google Scholar] [CrossRef] [PubMed]
- Thomsen, H.S. Guidelines for contrast media from the European Society of Urogenital Radiology. AJR Am J Roentgenol 2003, 181, 1463–1471. [Google Scholar] [CrossRef]
- McCullough, P.A. Contrast-induced acute kidney injury. J Am Coll Cardiol 2008, 51, 1419–1428. [Google Scholar] [CrossRef]
- Andreucci, M.; Faga, T.; Pisani, A.; Sabbatini, M.; Russo, D.; Michael, A. Prevention of contrast-induced nephropathy through a knowledge of its pathogenesis and risk factors. ScientificWorldJournal 2014, 2014, 823169. [Google Scholar] [CrossRef]
- Andreucci, M.; Faga, T.; Pisani, A.; Sabbatini, M.; Michael, A. Acute kidney injury by radiographic contrast media: pathogenesis and prevention. Biomed Res Int 2014, 2014, 362725. [Google Scholar] [CrossRef] [PubMed]
- Andreucci, M.; Faga, T.; Serra, R.; De Sarro, G.; Michael, A. Update on the renal toxicity of iodinated contrast drugs used in clinical medicine. Drug Healthc Patient Saf 2017, 9, 25–37. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Dangas, G.D.; Weisbord, S.D. Contrast-Associated Acute Kidney Injury. N Engl J Med 2019, 380, 2146–2155. [Google Scholar] [CrossRef] [PubMed]
- McCullough, P.A.; Choi, J.P.; Feghali, G.A.; Schussler, J.M.; Stoler, R.M.; Vallabahn, R.C.; Mehta, A. Contrast-Induced Acute Kidney Injury. J Am Coll Cardiol 2016, 68, 1465–1473. [Google Scholar] [CrossRef] [PubMed]
- Kidney International Supplements 2012, 2(1). Available online: https://kdigo.org/wp-content/uploads/2016/10/KDIGO-2012-AKI-Guideline-English.pdf (accessed on 31 01 2024).
- Nusca, A; Miglionico, M.; Proscia, C.; Ragni, L.; Carassiti, M.; Pepe, F.L.; Di Sciascio, G. Early prediction of contrast-induced acute kidney injury by a “bedside” assessment of Neutrophil Gelatinase-Associated Lipocalin during elective percutaneous coronary interventions. PloS one 2018, 13, e0197833. [Google Scholar] [CrossRef]
- Briguori, C.; Quintavalle, C.; Donnarumma, E.; Condorelli, G. Novel biomarkers for contrast-induced acute kidney injury. BioMed Res Int 2014, 2014, 568738. [Google Scholar] [CrossRef] [PubMed]
- Andreucci, M.; Faga, T.; Riccio, E.; Sabbatini, M.; Pisani, A.; Michael, A. The potential use of biomarkers in predicting contrast-induced acute kidney injury. Int J Nephrol Renovasc Dis 2016, 9, 205–221. [Google Scholar] [CrossRef]
- Mussap, M.; Noto, A.; Fanos, V.; Van Den Anker, J.N. Emerging biomarkers and metabolomics for assessing toxic nephropathy and acute kidney injury (AKI) in neonatology. BioMed Res Int 2014, 2014, 602526. [Google Scholar] [CrossRef]
- Damman, K.; Voors, A.A.; Navis, G.; van Veldhuisen, D.J.; Hillege, H.L. Current and novel renal biomarkers in heart failure. Heart Fail Rev 2012, 17, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Cockcroft, D.W.; Gault, M.H. Prediction of creatinine clearance from serum creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med 1999, 130, 461–470. [Google Scholar] [CrossRef]
- Solomon, R.; Goldstein, S. Real-time measurement of glomerular filtration rate. Curr Opin Crit Care 2017, 23, 470–474. [Google Scholar] [CrossRef]
- QPI-1002 Phase 3 for Prevention of Major Adverse Kidney Events (MAKE) in Subjects at High Risk for AKI Following Cardiac Surgery. 2021. Available online: https://clinicaltrials.gov/study/NCT03510897 (accessed on 31 01 2024).
- Randomized double blind placebo-controlled phase II study on the effects of EA-230 on the innate immune response following on-pump cardiac surgery. 2016. Available online: https://www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2015-005600-28 (accessed on 31 01 2024).
- Kellum, J.A.; Sileanu, F.E.; Murugan, R.; Lucko, N.; Shaw, A.D.; Clermont, G. Classifying AKI by Urine Output versus Serum Creatinine Level. JAm Soc Nephrol 2015, 26, 2231–2238. [Google Scholar] [CrossRef]
- Sudarsky, D.; Nikolsky, E. Contrast-induced nephropathy in interventional cardiology. Int J of Nephrol Renovasc Dis 2011, 4, 85–99. [Google Scholar] [CrossRef]
- Slocum, J.L.; Heung, M.; Pennathur, S. Marking renal injury: can we move beyond serum creatinine? Transl Res 2012, 159, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Royakkers, A.A.; van Suijlen, J.D.; Hofstra, L.S.; Kuiper, M.A.; Bouman, C.S.C.; Spronk, P.E.; Schultz, M.J. Serum cystatin C-A useful endogenous marker of renal function in intensive care unit patients at risk for or with acute renal failure? Curr Med Chem 2007, 14, 2314–2317. [Google Scholar] [CrossRef] [PubMed]
- Briguori, C.; Visconti, G.; Rivera, N.V.; Focaccio, A.; Golia, B.; Giannone, R.; Castaldo, D.; De Micco, F.; Ricciardelli, B.; Colombo, A. Cystatin C and contrast-induced acute kidney injury. Circulation 2010, 121, 2117–2122. [Google Scholar] [CrossRef] [PubMed]
- Budano C, Andreis A, De Filippo O, Bissolino, A.; Lanfranco, G.; Usmiani, T.; Gai, M.; Levis, M.; Bergamasco, L.; Marra, S.; Rinaldi, M.; De Ferrari, G.M. A single cystatin C determination before coronary angiography can predict short and long-term adverse events. Int J Cardiol 2020, 300, 73–79. [CrossRef]
- Bachorzewska-Gajewska, H.; Malyszko, J.; Sitniewska, E.; Malyszko, J.S.; Dobrzycki, S. Neutrophil gelatinase-associated lipocalin (NGAL) correlations with cystatin C, serum creatinine and eGFR in patients with normal serum creatinine undergoing coronary angiography. Nephrol Dial Transplant 2007, 22, 295–296. [Google Scholar] [CrossRef] [PubMed]
- Rickli, H.; Benou, K.; Ammann, P.; Fehr, T.; Brunner-La Rocca, H.P.; Petridis, H.; Riesen, W.; Wüthrich, R.P. Time course of serial cystatin C levels in comparison with serum creatinine after application of radiocontrast media. Clinical Nephrol 2004, 61, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Solomon, R.J.; Mehran, R.; Natarajan, M.K.; Doucet, S.; Katholi, R.E.; Staniloae, C.S.; Sharma, S.K.; Labinaz, M.; Gelormini, J.L.; Barrett, B.J. Contrast-induced nephropathy and long-term adverse events: cause and effect? Clin J Am Soc Nephrol 2009, 4, 1162–1169. [Google Scholar] [CrossRef]
- Thiele, H.; Hildebrand, L.; Schirdewahn, C.; Eitel, I.; Adams, V.; Fuernau, G.; Erbs, S.; Linke, A.; Diederich, K-W.; Nowak, M.; Desch, S.; Gutberlet, M.; Schulere, G. Impact of high-dose N-acetylcysteine versus placebo on contrast-induced nephropathy and myocardial reperfusion injury in unselected patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. The LIPSIA-N-ACC (Prospective, Single-Blind, Placebo-Controlled, Randomized Leipzig Immediate PercutaneouS Coronary Intervention Acute Myocardial Infarction N-ACC) Trial. J Am Coll Cardiol 2010, 55, 2201–2209. [CrossRef]
- Droppa, M.; Desch, S.; Blasé, P.; Eitel, I.; Fuernau, G.; Schuler, G.; Adams, V.; Thiele, H. Impact of N-acetylcysteine on contrast-induced nephropathy defined by cystatin C in patients with ST-elevation myocardial infarction undergoing primary angioplasty. Clin Res Cardiol 2011, 100, 1037–1043. [Google Scholar] [CrossRef]
- Banda, J.; Duarte, R.; Dix-Peek, T.; Dickens, C.; Manga, P.; Naicker, S. Biomarkers for Diagnosis and Prediction of Outcomes in Contrast-Induced Nephropathy. Int J Nephrol 2020, 2020, 8568139. [Google Scholar] [CrossRef]
- Terzi, I.; Papaioannou, V.; Papanas, N.; Dragoumanis, C.; Petala, A.; Theodorou, V.; Gioka, T.; Vargemezis, V.; Maltezos, E.; Pneumatikos, I. Alpha1-microglobulin as an early biomarker of sepsis-associated acute kidney injury: a prospective cohort study. Hippokratia 2014, 18, 262–268. [Google Scholar]
- Heise, D.; Rentsch, K.; Braeuer, A.; Friedrich, M.; Quintel, M. Comparison of urinary neutrophil glucosaminidase-associated lipocalin, cystatin C, and α1-microglobulin for early detection of acute renal injury after cardiac surgery. Eur J Cardiothorac Surg 2011, 39, 38–43. [Google Scholar] [CrossRef]
- Adiyanti, S.S.; Loho, T. Acute Kidney Injury (AKI) biomarker. Acta Med Indones 2012, 44, 246–255. [Google Scholar]
- Barton, K.T.; Kakajiwala, A.; Dietzen, D.J.; Goss, C.W.; Gu, H.; Dharnidharka, V.R. Using the newer Kidney Disease: Improving Global Outcomes criteria, beta-2-microglobulin levels associate with severity of acute kidney injury. Clin kidney J 2018, 11, 797–802. [Google Scholar] [CrossRef] [PubMed]
- Levin, A.; Pate, G.E.; Shalansky, S.; Al-Shamari,A.; Webb, J.G.; Buller, C.E.; Humphries, K.H. N-acetylcysteine reduces urinary albumin excretion following contrast administration: evidence of biological effect. Nephrol Dial Transplant 2007, 22, 2520–2524. [CrossRef] [PubMed]
- Isobe, S.; Yuba, M.; Mori, H.; Suzuki, S.; Sato, K.; Ishii, H.; Murohara, T. Increased pre-procedural urinary microalbumin is associated with a risk for renal functional deterioration after coronary computed tomography angiography. Int J Cardiol 2017, 230, 599–603. [Google Scholar] [CrossRef]
- Parr, S.K.; Matheny, M.E.; Abdel-Kader, K.; Greevy Jr, R.A.; Bian, A.; Fly, J.; Chen, G.; Speroff, T.; Hung, A.M.; Ikizler, T.A.; Siew, E.D. Acute kidney injury is a risk factor for subsequent proteinuria. Kidney Int 2018, 93, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Piskinpasa, S.; Altun, B.; Akoglu, H.; Yildirim, T.; Agbaht, K.; Yilmaz, R.; Peynircioglu, B.; Cil, B.; Aytemir, K.; Turgan, C. An uninvestigated risk factor for contrast-induced nephropathy in chronic kidney disease: proteinuria. Ren Fail 2013, 35, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Parikh, C.R.; Devarajan, P. New biomarkers of acute kidney injury. Crit Care Med 2008, 36 (4 Suppl), S159–165. [Google Scholar] [CrossRef]
- Tao, Y.; Dong, W.; Li, Z.; Chen, Y.; Liang, H.; Li, R.; Mo, L.; Xu, L.; Liu, S.; Shi, W.; Zhang, L.; Liang, X. Proteinuria as an independent risk factor for contrast-induced acute kidney injury and mortality in patients with stroke undergoing cerebral angiography. J Neurointerv Surg 2017, 9, 445–448. [Google Scholar] [CrossRef]
- Munshi, R.; Johnson, A.; Siew, E.D.; Ikizler, T.A.; Ware, L.B.; Wurfel, M.M; Himmelfarb, J.; Zager, R.A. MCP-1 gene activation marks acute kidney injury. J Am Soc Nephrol 2011, 22, 165–175. [Google Scholar] [CrossRef]
- Lucarelli, G.; Mancini, V.; Galleggiante, V.; Rutigliano, M.; Vavallo, A.; Battaglia, M.; Ditonno, P. Emerging urinary markers of renal injury in obstructive nephropathy. Biomed Res Int 2014, 2014, 303298. [Google Scholar] [CrossRef] [PubMed]
- Shinke, H.; Masuda, S.; Togashi, Y.; Ikemi, Y.; Ozawa, A.; Sato, T.; Kim, Y.H.; Mishima, M.; Ichimura, T.; Bonventre, J.V.; Matsubara, K. Urinary kidney injury molecule-1 and monocyte chemotactic protein-1 are noninvasive biomarkers of cisplatin-induced nephrotoxicity in lung cancer patients. Cancer Chemother Pharmacol 2015, 76, 989–996. [Google Scholar] [CrossRef]
- Ling, W.; Zhaohui, N.; Ben, H.; Leyi, G.; Jianping, L.; Huili, D.; Jiaqi, Q. Urinary IL-18 and NGAL as early predictive biomarkers in contrast-induced nephropathy after coronary angiography. Nephron Clin Pract 2008, 108, c176–181. [Google Scholar] [CrossRef]
- He, H.; Li, W.; Qian, W.; Zhao, X.; Wang, L.; Yu, Y.; Liu, J.; Cheng, J. Urinary interleukin-18 as an early indicator to predict contrast-induced nephropathy in patients undergoing percutaneous coronary intervention. Exp Ther Med 2014, 8, 1263–1266. [Google Scholar] [CrossRef] [PubMed]
- Duan, S.B.; Liu, G.L.; Yu, Z.Q.; Pan, P. Urinary KIM-1, IL-18 and Cys-c as early predictive biomarkers in gadolinium-based contrast-induced nephropathy in the elderly patients. Clin Nephrol 2013, 80, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Bulent Gul, C.; Gullulu, M.; Oral, B.; Aydinlar, A.; Oz, O.; Budak, F.; Yilmaz, Y.; Yurtkuran, M. Urinary IL-18: a marker of contrast-induced nephropathy following percutaneous coronary intervention? Clin Biochem 2008, 41, 544–547. [Google Scholar] [CrossRef]
- Connolly, M.; Kinnin, M.; McEneaney, D.; Menown, I.; Kurth, M.; Lamont, J.; Morgan, N.; Harbinson, M. Prediction of contrast induced acute kidney injury using novel biomarkers following contrast coronary angiography. QJM 2018, 111, 103–110. [Google Scholar] [CrossRef]
- Mishra, J.; Ma, Q.; Prada, A.; Mitsnefes, M.; Zahedi, K.; Yang, J.; Barasch, J.; Devarajan, P. Identification of neutrophil gelatinase-associated lipocalin as a novel early urinary biomarker for ischemic renal injury. J Am Soc mNephrol 2003, 14, 2534–2543. [Google Scholar] [CrossRef]
- Mishra, J.; Mori, K.; Ma, Q.; Kelly, C.; Barasch, J.; Devarajan, P. Neutrophil gelatinase-associated lipocalin: a novel early urinary biomarker for cisplatin nephrotoxicity. Am J Nephrol 2004, 24, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Alge, J.L.; Arthur, J.M. Biomarkers of AKI: a review of mechanistic relevance and potential therapeutic implications. Clin J Am Soc Nephrol 2015, 10, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Paragas, N.; Qiu, A.; Zhang, Q.; Samstein, B.; Deng, S-X.; Schmidt-Ott, K.M.; Viltard, M.; Yu, W.; Forster, C.S.; Gong, G.; Liu, Y.; Kulkarni, R.; Mori,K.; Kalandadze, A.; Ratner, A.J.; Devarajan, P.; Landry, D.W.; D’Agati, V.; Lin, C-S.; Barasch, J. The Ngal reporter mouse detects the response of the kidney to injury in real time. Nat Med 2011, 17, 216–222. [CrossRef]
- Filiopoulos, V.; Biblaki, D.; Lazarou, D.; Chrisis, D.; Fatourou, M.; Lafoyianni, S.; Vlassopoulos, D. Plasma neutrophil gelatinase-associated lipocalin (NGAL) as an early predictive marker of contrast-induced nephropathy in hospitalized patients undergoing computed tomography. Clin Kidney J 2013, 6, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Filiopoulos, V.; Biblaki, D.; Vlassopoulos, D. Neutrophil gelatinase-associated lipocalin (NGAL): a promising biomarker of contrast-induced nephropathy after computed tomography. Ren Fail 2014, 36, 979–986. [Google Scholar] [CrossRef]
- Schilcher, G.; Ribitsch, W.; Otto, R.; Portugaller, R.H.; Quehenberger, F.; Truschnig-Wilders, M.; Zweiker, R.; Stiegler, P.; Brodmann, M.; Weinhandl, K.; Horina, J.H. Early detection and intervention using neutrophil gelatinase-associated lipocalin (NGAL) may improve renal outcome of acute contrast media induced nephropathy: a randomized controlled trial in patients undergoing intra-arterial angiography (ANTI-CIN Study). BMC Nephrol 2011, 12, 39. [Google Scholar] [CrossRef]
- Tasanarong, A.; Hutayanon, P.; Piyayotai, D. Urinary Neutrophil Gelatinase-Associated Lipocalin predicts the severity of contrast-induced acute kidney injury in chronic kidney disease patients undergoing elective coronary procedures. BMC Nephrol 2013, 14, 270. [Google Scholar] [CrossRef]
- Quintavalle, C.; Anselmi, C.V.; De Micco, F.; Roscigno, G.; Visconti, G.; Golia, B.; Focaccio, A.; Ricciardelli, B.; Perna, E.; Papa, L.; Donnarumma, E.; Condorelli, G.; Briguori, C. Neutrophil Gelatinase-Associated Lipocalin and Contrast-Induced Acute Kidney Injury. Cir Cardiovas Interv 2015, 8, e002673. [Google Scholar] [CrossRef]
- Kafkas, N.; Liakos, C.; Zoubouloglou, F.; Dagadaki, O.; Dragasis, S.; Makris, K. Neutrophil Gelatinase-Associated Lipocalin as an Early Marker of Contrast-Induced Nephropathy After Elective Invasive Cardiac Procedures. Clin Cardiol 2016, 39, 464–470. [Google Scholar] [CrossRef]
- Reyes, L.F.; Severiche-Bueno, D.F.; Bustamante, C.A.; Murillo, S.; Soni, N.J.; Poveda, M.; Gomez, E.; Buitrago, R.; Rodriguez, A. Serum levels of neutrophil Gelatinase associated Lipocalin (NGAL) predicts hemodialysis after coronary angiography in high risk patients with acute coronary syndrome. BMC Nephrol 2020, 21, 143. [Google Scholar] [CrossRef]
- Ribitsch, W.; Schilcher, G.; Quehenberger, F.; Pilz, S.; Portugaller, R.H.; Truschnig-Wilders, M.; Zweiker, R.; Brodmann, M.; Stiegler, P.; Rosenkranz, A.R.; Pickering, J.W.; Horina, J.H. Neutrophil gelatinase-associated lipocalin (NGAL) fails as an early predictor of contrast induced nephropathy in chronic kidney disease (ANTI-CI-AKI study). Sci Rep 2017, 7, 41300. [Google Scholar] [CrossRef] [PubMed]
- Ichimura, T.; Bonventre, J.V.; Bailly, V.; Wei, H.; Hession, C.A.; Cate, R.L.; Sanicolaet, M. Kidney injury molecule-1 (KIM-1), a putative epithelial cell adhesion molecule containing a novel immunoglobulin domain, is up-regulated in renal cells after injury. J Biol Chem 1998, 273, 4135–4142. [Google Scholar] [CrossRef] [PubMed]
- Prozialeck, W.C.; Vaidya, V.S.; Liu, J.; Waalkes, M.P.; Edwards, J.R.; Lamar, P.C.; Bernard, A.M.; Dumont, X.; Bonventre, J.V. Kidney injury molecule-1 is an early biomarker of cadmium nephrotoxicity. Kidney Int 2007, 72, 985–993. [Google Scholar] [CrossRef] [PubMed]
- Han, W.K.; Bailly, V.; Abichandani, R.; Thadhani, R.; Bonventre, J.V. Kidney Injury Molecule-1 (KIM-1): a novel biomarker for human renal proximal tubule injury. Kidney Int 2002, 62, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Ichimura, T.; Hung, C.C.; Yang, S.A.; Stevens, J.L.; Bonventre, J.V. Kidney injury molecule-1: a tissue and urinary biomarker for nephrotoxicant-induced renal injury. Am J Physiol Renal Physiol 2004, 286, F552–563. [Google Scholar] [CrossRef] [PubMed]
- Han, W.K.; Waikar, S.S.; Johnson, A.; Betensky, R.A.; Dent, C.L.; Devarajan, P.; Bonventre, J.V. Urinary biomarkers in the early diagnosis of acute kidney injury. Kidney Int 2008, 73, 863–869. [Google Scholar] [CrossRef] [PubMed]
- Parikh, C.R.; Thiessen-Philbrook, H.; Garg, A.X.; Kadiyala, D.; Shlipak, M.G.; Koyner, J.L.; Edelstein, C.L.; Devarajan, P.; Patel, U.D.; Zappitelli, M.; Krawczeski, C.D.; Passik, C.S.; Coca; S. G.; TRIBE-AKI Consortium. Performance of kidney injury molecule-1 and liver fatty acid-binding protein and combined biomarkers of AKI after cardiac surgery. Clinical J Am Soc Nephrol 2013, 8, 1079–1088. [Google Scholar] [CrossRef]
- Sabbisetti, V.; Waikar, S.S.; Antoine, D.J.; Smiles, A.; Wang, C.; Ravisankar, A.; Ito, K.; Sharma, S.; Ramadesikan, S.; Lee, M.; Briskin, R.; De Jager, P.L.; Ngo, T.T.; Radlinski, M.; Dear, J.W.; Park, K.B.; Betensky, R.; Krolewski, A.S.; Bonventre, J.V. Blood kidney injury molecule-1 is a biomarker of acute and chronic kidney injury and predicts progression to ESRD in type I diabetes. J Am Soc Nephrol 2014, 25, 2177–2186. [Google Scholar] [CrossRef]
- Rosner, M.H.; Ronco, C.; Okusa, M.D. The role of inflammation in the cardio-renal syndrome: a focus on cytokines and inflammatory mediators. Semin Nephrol 2012, 32, 70–78. [Google Scholar] [CrossRef]
- Mamoulakis, C.; Fragkiadoulaki, I.; Karkala, P.; Georgiadis, G.; Zisis, I.-E.; Stivaktakis, P.; Kalogeraki, A.; Tsiaoussis, I.; Burykina, T.; Lazopoulos, G.; Tsarouhas, K.; Kouretas, D.; Tsatsakis, A. Contrast-induced nephropathy in an animal model: Evaluation of novel biomarkers in blood and tissue samples. Toxicol Rep 2019, 6, 395–400. [Google Scholar] [CrossRef]
- Rouse, R.L.; Stewart, S.R.; Thompson, K.L.; Zhang, J. Kidney injury biomarkers in hypertensive, diabetic, and nephropathy rat models treated with contrast media. Toxicol Pathol 2013, 41, 662–680. [Google Scholar] [CrossRef] [PubMed]
- Akdeniz, D.; Celik, H.T.; Kazanci, F.; Yilmaz, H.; Yalcin, S.; Bilgic, M.A.; Ruzgaresen, N.; Akcay, A.; Eryonucu, B. Is Kidney Injury Molecule 1 a Valuable Tool for the Early Diagnosis of Contrast-Induced Nephropathy? J Investig Med 2015, 63, 930–934. [Google Scholar] [CrossRef]
- Torregrosa, I.; Montoliu, C.; Urios, A.; Andrés-Costa, M.J.; Giménez-Garzó, C.; Juan, I.; Puchades, M.J.; Blasco, M.L.; Carratalá, A.; Sanjuán, R.; Miguel, A. Urinary KIM-1, NGAL and L-FABP for the diagnosis of AKI in patients with acute coronary syndrome or heart failure undergoing coronary angiography. Heart Vessels 2015, 30, 703–711. [Google Scholar] [CrossRef] [PubMed]
- Fuhrman, D.Y.; Kellum, J.A. Biomarkers for Diagnosis, Prognosis and Intervention in Acute Kidney Injury. Contrib Nephrol 2016, 187, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Ricci, Z. The concept of risk and the value of novel markers of acute kidney injury. Crit Care 2013, 17, 117. [Google Scholar] [CrossRef]
- Kashani, K.; Al-Khafaji, A.; Ardiles, T.; Artigas, A.; Bagshaw, S.M.; Bell, M.; Bihorac, A.; Birkhahn, R.; Cely, C.M.; Chawla, L.S.; Davison, D.L.; Feldkamp, T.; Forni, L.G.; Gong, M.N.; Gunnerson, K.J.; Haase, M.; Hackett, J.; Honore, P.M.; Hoste, E.A.J.; Joannes-Boyau, O.; Joannidis, M.; Kim, P.; Koyner, J.L.; Laskowitz, D.T.; Lissauer, M.E.; Marx, G.; McCullough, P.A.; Mullaney, S.; Ostermann, M.; Rimmelé, T.; Shapiro, N.I.; Shaw, A.D.; Shi, J.; Sprague, A.M.; Vincent, J.-L.; Vinsonneau, C.; Wagner, L.; Walker, M.G.; Wilkerson, R.G.; Zacharowski, K.; Kellum, J.A. Discovery and validation of cell cycle arrest biomarkers in human acute kidney injury. Crit Care 2013, 17, R25. [Google Scholar] [CrossRef]
- Koyner, JL, Shaw, AD, Chawla, LS, Hoste, E.A.J.; Bihorac, A.; Kashani, K.; Haase, M.; Shi, J.; Kellum, J.A.; Sapphire Investigators. Tissue Inhibitor Metalloproteinase-2 (TIMP-2)⋅IGF-Binding Protein-7 (IGFBP7) Levels Are Associated with Adverse Long-Term Outcomes in Patients with AKI. J Am Soc Nephrol 2015, 26, 1747–1754. [CrossRef]
- Gocze, I.; Koch, M.; Renner, P.; Zeman, F.; Graf, B.M.; Dahlke, M.H.; Nerlich, M.; Schlitt, H.J.; Kellum, J.A.; Bein, T. Urinary biomarkers TIMP-2 and IGFBP7 early predict acute kidney injury after major surgery. PloS One 2015, 10, e0120863. [Google Scholar] [CrossRef]
- Landrier, J.F.; Thomas, C.; Grober, J.; Duez, H.; Percevault, F.; Souidi, M.; Linard, C.; Staels, B.; Besnard, P. Statin induction of liver fatty acid-binding protein (L-FABP) gene expression is peroxisome proliferator-activated receptor-alpha-dependent. J Biol Chem 2004, 279, 45512–45518. [Google Scholar] [CrossRef]
- Yamamoto, T.; Noiri, E.; Ono, Y.; Doi, K.; Negishi, K.; Kamijo, A.; Kimura, K.; Fujita, T.; Kinukawa, T.; Taniguchi, H.; Nakamura, K.; Goto, M.; Shinozaki, N.; Ohshima, S.; Sugaya, T. Renal L-type fatty acid-binding protein in acute ischemic injury. J Am Soc Nephrol 2007, 18, 2894–2902. [Google Scholar] [CrossRef]
- Kamijo-Ikemori, A.; Sugaya, T.; Matsui, K.; Yokoyama, T.; Kimura, K. Roles of human liver type fatty acid binding protein in kidney disease clarified using hL-FABP chromosomal transgenic mice. Nephrology (Carlton) 2011, 16, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Portilla, D.; Dent, C.; Sugaya, T.; Nagothu, K.K.; Kundi, I.; Moore, P.; Noiri, E.; Devarajan, P. Liver fatty acid-binding protein as a biomarker of acute kidney injury after cardiac surgery. Kidney Int 2008, 73, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.; Tangri, N.; Komenda, P.; Kausha, A.; Sood, M.; Brar, R.; Gill, K.; Walker, S.; MacDonald, K.; Hiebert, B.M.; Arora, R.C.; Rigatto, C. Urinary, Plasma, and Serum Biomarkers’ Utility for Predicting Acute Kidney Injury Associated With Cardiac Surgery in Adults: A Meta-analysis. Am J Kidney Dis 2015, 66, 993–1005. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Sugaya, T.; Node, K.; Ueda, Y.; Koide, H. Urinary excretion of liver-type fatty acid-binding protein in contrast medium-induced nephropathy. Am J Kidney Dis 2006, 47, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Liangos, O.; Perianayagam, M.C.; Vaidya, V.S.; Han, W.K.; Wald, R.; Tighiouart, H.; W MacKinnon, R.W.; Li, L.; Balakrishnan, V.S.; Pereira, B.J.G.; Bonventre, J.V.; Jaber, B.L. Urinary N-acetyl-beta-(D)-glucosaminidase activity and kidney injury molecule-1 level are associated with adverse outcomes in acute renal failure. J Am Soc Nephrol 2007, 18, 904–912. [Google Scholar] [CrossRef] [PubMed]
- Bazzi, C.; Petrini, C.; Rizza, V.; Arrigo, G.; Napodano, P.; Paparella, M.; D’Amico, G. Urinary N-acetyl-beta-glucosaminidase excretion is a marker of tubular cell dysfunction and a predictor of outcome in primary glomerulonephritis. Nephrol Dial Transplant 2002, 17, 1890–1896. [Google Scholar] [CrossRef] [PubMed]
- Mukhopadhyay, B.; Chinchole, S.; Lobo, V.; Gang, S.; Rajapurkar, M. Enzymuria pattern in early post renal transplant period: Diagnostic usefulness in graft dysfunction. Indian J Clin Biochem 2004, 19, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Arakawa, Y.; Tamura, M.; Sakuyama, T.; Aiba, K.; Eto, S.; Yuda, M.; Tanaka, Y.; Matsumoto, A.; Nishikawa, K. Early measurement of urinary N-acetyl-β-glucosaminidase helps predict severe hyponatremia associated with cisplatin-containing chemotherapy. J Infect Chemother 2015, 21, 502–506. [Google Scholar] [CrossRef]
- Vaidya, VS.; Waikar, S.S.; Ferguson, M.A.; Collings, F.B.; Sunderland, K.; Gioules, C.; Bradwin, G.; Matsouaka, R.; Betensky, R.A.; Curhan, G.C.; Bonventre, J.V. Urinary biomarkers for sensitive and specific detection of acute kidney injury in humans. Clin Transl Sci 2008, 1, 200–208. [Google Scholar] [CrossRef]
- Ren, L.; Ji, J.; Fang, Y.; Jiang, S.H.; Lin, Y.M.; Bo, J.; Qian, J.Y.; Xu, X.H.; Ding, X.Q. Assessment of urinary N-acetyl-β-glucosaminidase as an early marker of contrast-induced nephropathy. J Int Med Res 2011, 39, 647–653. [Google Scholar] [CrossRef]
- Benzer, M.; Alpay, H.; Baykan, Ö.; Erdem, A.; Demir, I.H. Serum NGAL, cystatin C and urinary NAG measurements for early diagnosis of contrast-induced nephropathy in children. Ren Fail 2016, 38, 27–34. [Google Scholar] [CrossRef]
- Nishida, M.; Kubo, S.; Morishita, Y.; Nishikawa, K.; Ikeda, K.; Itoi, T.; Hosoi, H. Kidney injury biomarkers after cardiac angiography in children with congenital heart disease. Congenit Heart Dis 2019, 14, 1087–1093. [Google Scholar] [CrossRef]
- Seabra, V.F.; Perianayagam, M.C.; Tighiouart, H.; Liangos, O.; dos Santos, O.F.; Jaber, B.L. Urinary α-GST and π-GST for prediction of dialysis requirement or in-hospital death in established acute kidney injury. Biomarkers 2011, 16, 709–717. [Google Scholar] [CrossRef]
- McMahon, B.A.; Koyner, J.L.; Murray, P.T. Urinary glutathione S-transferases in the pathogenesis and diagnostic evaluation of acute kidney injury following cardiac surgery: a critical review. Curr Opin Crit Care 2010, 16, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Susantitaphong, P.; Perianayagam, M.C.; Tighiouart, H.; Kouznetsov, D.; Liangos, O.; Jaber, B.L. Urinary α- and π-glutathione s-transferases for early detection of acute kidney injury following cardiopulmonary bypass. Biomarkers 2013, 18, 331–337. [Google Scholar] [CrossRef]
- Shu, K,H. ; Wang, C.H.; Wu, C.H.; Huang, T.M.; Wu, P.C.; Lai, C.H.; Tseng, L.J.; Tsai, P.R.; Connolly, R.; Wu, V.C. Urinary π-glutathione S-transferase Predicts Advanced Acute Kidney Injury Following Cardiovascular Surgery. Sci Rep 2016, 6, 26335. [Google Scholar] [CrossRef]
- Xu, J.; L,i G. ; Wang, P.; Velazquez, H.; Yao, X.; Li, Y.; Wu, Y.; Peixoto, A.; Crowley, S.; Desir, G.V. Renalase is a novel, soluble monoamine oxidase that regulates cardiac function and blood pressure. J Clin Invest 2005, 115, 1275–1280. [Google Scholar] [CrossRef]
- Lee, H.T.; Kim, J.Y.; Kim, M.; Wang, P.; Tang, L.; Baroni, S.; D’Agati, V.D.; Desir, G.V. Renalase protects against ischemic AKI. J Am Soc Nephrol 2013, 24, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Velazquez, H.; Moeckel, G.; Chang, J.; Ham, A.; Lee, H.T.; Safirstein, R.; Desir, G.V. Renalase prevents AKI independent of amine oxidase activity. J Am Soc Nephrol 2014, 25, 1226–1235. [Google Scholar] [CrossRef]
- Zhao, B.; Zhao, Q.; Li, J.; Xing, T.; Wang, F.; Wang, N. Renalase protects against contrast-induced nephropathy in Sprague-Dawley rats. PloS One 2015, 10, e0116583. [Google Scholar] [CrossRef] [PubMed]
- Wybraniec, M.T.; Bożentowicz-Wikarek, M.; Chudek, J.; Mizia-Stec, K. Urinary renalase concentration in patients with preserved kidney function undergoing coronary angiography. Nephrology (Carlton) 2018, 23, 133–138. [Google Scholar] [CrossRef]
- Wybraniec, M.T.; Mizia-Stec, K. Renalase and Biomarkers of Contrast-Induced Acute Kidney Injury. Cardiorenal Med 2015, 6, 25–36. [Google Scholar] [CrossRef]
- Sánchez-López, E.; Rayego, S.; Rodrigues-Díez, R.; Rodriguez, J.S.; Rodrigues-Díez, R.; Rodríguez-Vita, J.; Carvajal, G.; Aroeira, L.S.; Selgas, R.; Mezzano, S.A.; Ortiz, A.; Egido, J.; Ruiz-Ortega, M. CTGF promotes inflammatory cell infiltration of the renal interstitium by activating NF-kappaB. J Am Soc Nephrol 2009, 20, 1513–1526. [Google Scholar] [CrossRef]
- Kilari, S.; Yang, B.; Sharma, A.; McCall, D.L.; Misra, S. Increased transforming growth factor beta (TGF-β) and pSMAD3 signaling in a Murine Model for Contrast Induced Kidney Injury. Sci Rep 2018, 8, 6630. [Google Scholar] [CrossRef] [PubMed]
- El-Achkar, T.M.; Wu, X.R. Uromodulin in kidney injury: an instigator, bystander, or protector? Am J Kidney Dis 2012, 59, 452–461. [Google Scholar] [CrossRef]
- Dawnay, A.B.; Thornley, C.; Nockler, I.; Webb, J.A.; Cattell, W.R. Tamm-Horsfall glycoprotein excretion and aggregation during intravenous urography. Relevance to acute renal failure. Invest Radiol 1985, 20, 53–57. [Google Scholar] [CrossRef]
- Dawson, P.; Freedman, D.B.; Howell, M.J.; Hine, A.L. Contrast-medium-induced acute renal failure and Tamm-Horsfall proteinuria. Br J Radiol 1984, 57, 577–579. [Google Scholar] [CrossRef]
- Bakris, G.L.; Gaber, A.O.; Jones, J.D. Oxygen free radical involvement in urinary Tamm-Horsfall protein excretion after intrarenal injection of contrast medium. Radiology 1990, 175, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Garimella, P.; Jaber, B.L.; Tighiouart, H.; Liangos, O.; Bennett, M.R.; Devarajan, P.; El-Achkar, T.M.; Sarnak, M.J. Association of Preoperative Urinary Uromodulin with AKI after Cardiac Surgery. Clin J Am Soc Nephrol 2017, 12, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Bennett, M.R.; Pyles, O.; Ma, Q.; Devarajan, P. Preoperative levels of urinary uromodulin predict acute kidney injury after pediatric cardiopulmonary bypass surgery. Pediatr Nephrol 2018, 33, 521–526. [Google Scholar] [CrossRef]
- Schrijvers, B.F.; Flyvbjerg, A.; De Vriese, A.S. The role of vascular endothelial growth factor (VEGF) in renal pathophysiology. Kidney Int 2004, 65, 2003–2017. [Google Scholar] [CrossRef]
- Ari, E.; Kedrah, A.E.; Alahdab, Y.; Bulut, G.; Eren, Z.; Baytekin, O.; Odabasi, D. Antioxidant and renoprotective effects of paricalcitol on experimental contrast-induced nephropathy model. Br J Radiol 2012, 85, 1038–1043. [Google Scholar] [CrossRef]
- Kaleta, B. The role of osteopontin in kidney diseases. Inflamm Res 2019, 68, 93–102. [Google Scholar] [CrossRef]
- Ibrahim, N.E.; McCarthy, C.P.; Shrestha, S.; Gaggin, H.K.; Mukai, R.; Magaret, C.A.; Rhyne, R.F.; Januzzi Jr, J.L. A clinical, proteomics, and artificial intelligence-driven model to predict acute kidney injury in patients undergoing coronary angiography. Clin Cardiol 2019, 42, 292–298. [Google Scholar] [CrossRef]
- Beitland, S.; Nakstad, E.R.; Berg, J.P.; Trøseid, A.M.S.; Brusletto, B.S.; Brunborg, C.; Lundqvist, C.; Sunde, K. Urine β-2-Microglobulin, Osteopontin, and Trefoil Factor 3 May Early Predict Acute Kidney Injury and Outcome after Cardiac Arrest. Crit Care Res Pract 2019, 2019, 4384796. [Google Scholar] [CrossRef]
- Espinel, C.H. The FENa test. Use in the differential diagnosis of acute renal failure. Jama 1976, 236, 579–581. [Google Scholar] [CrossRef] [PubMed]
- Russo, D.; Minutolo, R.; Cianciaruso, B.; Memoli, B.; Conte, G.; De Nicola, L. Early effects of contrast media on renal hemodynamics and tubular function in chronic renal failure. J Am Soc Nephrol 1995, 6, 1451–1458. [Google Scholar] [CrossRef]
- Murakami, R.; Kumazaki, T.; Tajima, H.; Hayashi, H.; Kuwako, T.; Hakozaki, K.; Kiriyama, T. Urinary excretion of vasoactive factors following contrast media exposure in humans. Nephron Clin Pract 2005, 101, c150–154. [Google Scholar] [CrossRef] [PubMed]
- Duan, S.B.; Yang, S.K.; Zhou, Q.Y.; Pan, P.; Zhang, H.; Liu, F.; Xu, X.Q. Mitochondria-targeted peptides prevent on contrast-induced acute kidney injury in the rats with hypercholesterolemia. Ren Fail 2013, 35, 1124–1129. [Google Scholar] [CrossRef]
- Calzavacca, P.; Ishikawa, K.; Bailey, M.; May, C.N.; Bellomo, R. Systemic and renal hemodynamic effects of intra-arterial radiocontrast. Intensive Care Med Exp 2014, 2, 32. [Google Scholar] [CrossRef] [PubMed]
- Ostermann, M.; Philips, B.J.; Forni, L.G. Clinical review: Biomarkers of acute kidney injury: where are we now? Crit Care 2012, 16, 233. [Google Scholar] [CrossRef] [PubMed]
- Prowle, J.R.; Ostland, V.; Calzavacca, P.; Licari, E.; Ligabo, E.V.; Echeverri, J.E.; Bagshaw, S.M.; Haase-Fielitz, A.; Haase, M.; Westerman, M.; Bellomo, R. Greater increase in urinary hepcidin predicts protection from acute kidney injury after cardiopulmonary bypass. Nephrol Dial Transplant 2012, 27, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Prowle, J.R.; Westerman, M.; Bellomo, R. Urinary hepcidin: an inverse biomarker of acute kidney injury after cardiopulmonary bypass? Curr Opin Crit Care 2010, 16, 540–544. [Google Scholar] [CrossRef]
- Leaf, D.E.; Rajapurkar, M.; Lele, S.S.; Mukhopadhyay, B.; Boerger, E.A.S.; Mc Causland, F.R.; Eisenga, M.F.; Singh, K.; Babitt, J.L.; Kellum, J.A.; Palevsky, P.M.; Christov, M.; Waikar, S.S. Iron, Hepcidin, and Death in Human AKI. J Am Soc Nephrol 2019, 30, 493–504. [Google Scholar] [CrossRef]
- Malyszko, J.; Bachorzewska-Gajewska, H.; Malyszko, J.S.; Koc-Zorawska, E.; Matuszkiewicz-Rowinska, J.; Dobrzycki, S. Hepcidin - Potential biomarker of contrast-induced acute kidney injury in patients undergoing percutaneous coronary interventions. Adv Med Sci 2019, 64, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Ayatse, J.O. Human retinol-binding protein: its relationship to renal function in renal diseases. West Afr J Med 1991, 10, 226–231. [Google Scholar]
- Sadat, U.; Walsh, S.R.; Norden, A.G.; Gillard, J.H.; Boyle, J.R. Does oral N-acetylcysteine reduce contrast-induced renal injury in patients with peripheral arterial disease undergoing peripheral angiography? A randomized-controlled study. Angiology 2011, 62, 225–230. [Google Scholar] [CrossRef]
- Chaykovska, L, Heunisch, F, von Einem, G, Alter, M. L.; Hocher, C.F.; Tsuprykov, O.; Dschietzig, T.; Kretschmer, A.; Hocher, B. Urinary Vitamin D Binding Protein and KIM-1 Are Potent New Biomarkers of Major Adverse Renal Events in Patients Undergoing Coronary Angiography. PloS One 2016, 11, e0145723. [Google Scholar] [CrossRef]
- Donadio, C.; Tramonti, G.; Lucchesi, A.; Giordani, R.; Lucchetti, A.; Bianchi, C. Gamma-glutamyltransferase is a reliable marker for tubular effects of contrast media. Renal Fail 1998, 20, 319–324. [Google Scholar] [CrossRef]
- Oksuz, F.; Yarlioglues, M.; Cay, S.; Celik, I.E.; Mendi, M.A.; Kurtul, A.; Cankurt, T.; Kuyumcu, S.; Canpolat, U.; Turak, O. Predictive Value of Gamma-Glutamyl Transferase Levels for Contrast-Induced Nephropathy in Patients With ST-Segment Elevation Myocardial Infarction Who Underwent Primary Percutaneous Coronary Intervention. Am J Cardiol 2015, 116, 711–716. [Google Scholar] [CrossRef]
- Malyszko, J.; Bachorzewska-Gajewska, H.; Koc-Zorawska, E.; Malyszko, J.S.; Kobus, G.; Dobrzycki, S. Midkine: a novel and early biomarker of contrast-induced acute kidney injury in patients undergoing percutaneous coronary interventions. Biomed Res Int 2015, 2015, 879509. [Google Scholar] [CrossRef]
- Jones, T.F.; Bekele, S.; O’Dwyer, M.J.; Prowle, J.R. MicroRNAs in Acute Kidney Injury. Nephron 2018, 140, 124–128. [Google Scholar] [CrossRef]
- Li, Y.F.; Jing, Y.; Hao, J.; Frankfort, N.C.; Zhou, X.; Shen, B.; Liu, X.; Wang, L.; Li, R. MicroRNA-21 in the pathogenesis of acute kidney injury. Protein Cell 2013, 4, 813–819. [Google Scholar] [CrossRef] [PubMed]
- Du, J.; Cao, X.; Zou, L.; Chen, Y.; Guo, J.; Chen,bZ.; Hu, S.; Zheng, Z. MicroRNA-21 and risk of severe acute kidney injury and poor outcomes after adult cardiac surgery. PloS One 2013, 8, e63390. [CrossRef]
- Sun, S.Q.; Zhang, T.; Ding, D.; Zhang, W.F.; Wang, X.L.; Sun, Z.; Hu, L.H.; Qin, S.Y.; Shen, L.H.; He, B. Circulating MicroRNA-188, -30a, and -30e as Early Biomarkers for Contrast-Induced Acute Kidney Injury. J Am Heart Assoc 2016, 5, e004138. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Moon, A. Drug-induced nephrotoxicity and its biomarkers. Biomol Ther 2012, 20, 268–272. [Google Scholar] [CrossRef]
- Dieterle, F.; Perentes, E.; Cordier, A.; Roth, D.R.; Verdes, P.; Grenet, O.; Pantano, S.; Moulin, P.; Wahl, D.; Mahl, A.; End, P.; Staedtler, F.; Legay, F.; Carl, K.; Laurie, D.; Chibout, S.D.; Vonderscher, J.; Maurer, G. Urinary clusterin, cystatin C, beta2-microglobulin and total protein as markers to detect drug-induced kidney injury. Nat Biotechnol 2010, 28, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Vinken, P.; Starckx, S.; Barale-Thomas, E.; Looszova, A.; Sonee, M.; Goeminne, N.; Versmissen, L.; Buyens, K.; Lampo, A. Tissue Kim-1 and urinary clusterin as early indicators of cisplatin-induced acute kidney injury in rats. Toxicol Pathol 2012, 40, 1049–62. [Google Scholar] [CrossRef] [PubMed]
- Nguan, C.Y.C.; Guan, Q.; Gleave, M.E.; Du, C. Promotion of cell proliferation by clusterin in the renal tissue repair phase after ischemia-reperfusion injury. Am J Physiol Ren Physiol 2014, 306, F724–33. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Guan, Q.; Liu, X.; Wang, H.; Gleave, M.E.; Nguan, C.Y.C.; Du, C. Relationship of clusterin with renal inflammation and fibrosis after the recovery phase of ischemia-reperfusion injury. BMC Nephrol 2016, 17, 133. [Google Scholar] [CrossRef]
- Da, Y.; Akalya, K.; Murali, T.; Vathsala, A.; Tan, C.S.; Low, S.; Lim, H.N.; Teo, B.W.; Lau, T.; Ong, L.; Chua, H.R. Serial Quantification of Urinary Protein Biomarkers to Predict Drug-induced Acute Kidney Injury. Curr Drug Metab 2019, 20, 656–64. [Google Scholar] [CrossRef]
- Hoffmann, D.; Fuchs, T.C.; Henzler, T.; Matheis, K.A.; Herget, T.; Dekant, W.; Hewitt, P.; Mally, A. Evaluation of a urinary kidney biomarker panel in rat models of acute and subchronic nephrotoxicity. Toxicology 2010, 277, 49–58. [Google Scholar] [CrossRef]
- Palviainen, M.; Raekallio, M.; Rajamäki, M.M.; Linden, J.; Vainio, O. Kidney-derived proteins in urine as biomarkers of induced acute kidney injury in sheep. Vet J 2012, 193, 287–9. [Google Scholar] [CrossRef] [PubMed]
- George, B.; Wen, X.; Mercke, N.; Gomez, M.; O’Bryant, C.; Bowles, D.W.; Hu, Y.; Hogan, S.L.; Joy, M.S.; Aleksunes, L.M. Profiling of Kidney Injury Biomarkers in Patients Receiving Cisplatin: Time-dependent Changes in the Absence of Clinical Nephrotoxicity. Clin Pharmacol Ther 2017, 101, 510–518. [Google Scholar] [CrossRef]
- George, B.; Wen, X.; Mercke, N.; Gomez, M.; O’Bryant, C.; Bowles, D.W.; Hu, Y.; Hogan, S.L.; Joy, M.S.; Aleksunes, L.M. Time-dependent changes in kidney injury biomarkers in patients receiving multiple cycles of cisplatin chemotherapy. Toxicol Rep 2020, 7, 571–576. [Google Scholar] [CrossRef]
- Lane, B.R.; Babitz, S.K.; Vlasakova, K.; Wong, A.; Noyes, S.L.; Boshoven, W.; Grady, P.; Zimmerman, C.; Engerman, S.; Gebben, M.; Tanen, M.; Glaab, W.E.; Sistare, F.D. Evaluation of Urinary Renal Biomarkers for Early Prediction of Acute Kidney Injury Following Partial Nephrectomy: A Feasibility Study. Eur Urol Focus 2020, 6, 1240–1247. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.F.; Li, J.M.; Tan, Y.; Wang, Z.F.; He, Y.; Chang, J.; Zhang, H.; Zhao, H.; Bai, X.; Xie, F.; Sun, J.; Zhang, Y. Performance of urinary NGAL and L-FABP in predicting acute kidney injury and subsequent renal recovery: a cohort study based on major surgeries. Clin Chem Lab Med 2014, 52, 671–678. [Google Scholar] [CrossRef]
- Arthur, J.M.; Hill, E.G.; Alge, J.L.; Lewis, E.C.; Neely, B.A.; Janech, M.G.; Tumlin, J.A.; Chawla, L.S.; Shaw; A. D.; SAKInet Investigators. Evaluation of 32 urine biomarkers to predict the progression of acute kidney injury after cardiac surgery. Kidney Int 2014, 85, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Wybraniec, M.T.; Chudek, J.; Bożentowicz-Wikarek, M.; Mizia-Stec, K. Prediction of contrast-induced acute kidney injury by early post-procedural analysis of urinary biomarkers and intra-renal Doppler flow indices in patients undergoing coronary angiography. J Interv Cardiol. 2017, 30, 465–472. [Google Scholar] [CrossRef]
Figure 1.
Contrast-induced acute kidney injury (CI-AKI) pathophysiology. Contrast media (CM) mediates on the other hand, direct renal tubular and endothelial cytotoxicity, leading to increased intrarenal pressure and consequent increase of intratubular pressure, resulting in a vicious cycle of medullary hypoxia, oxidative stress and increased loss of function, integrity and cell death. On the other hand, the viscous properties of CM trigger vasoconstriction, increases blood viscosity that reduces urinary flow rate, decreases microvascularization and increases the risk of microvascular thrombosis. All this leads to an abrupt loss of renal function resulting in CI-AKI. P, pressure; ROS, reactive oxygen species; GFR, glomerular filtration rate.
Figure 1.
Contrast-induced acute kidney injury (CI-AKI) pathophysiology. Contrast media (CM) mediates on the other hand, direct renal tubular and endothelial cytotoxicity, leading to increased intrarenal pressure and consequent increase of intratubular pressure, resulting in a vicious cycle of medullary hypoxia, oxidative stress and increased loss of function, integrity and cell death. On the other hand, the viscous properties of CM trigger vasoconstriction, increases blood viscosity that reduces urinary flow rate, decreases microvascularization and increases the risk of microvascular thrombosis. All this leads to an abrupt loss of renal function resulting in CI-AKI. P, pressure; ROS, reactive oxygen species; GFR, glomerular filtration rate.
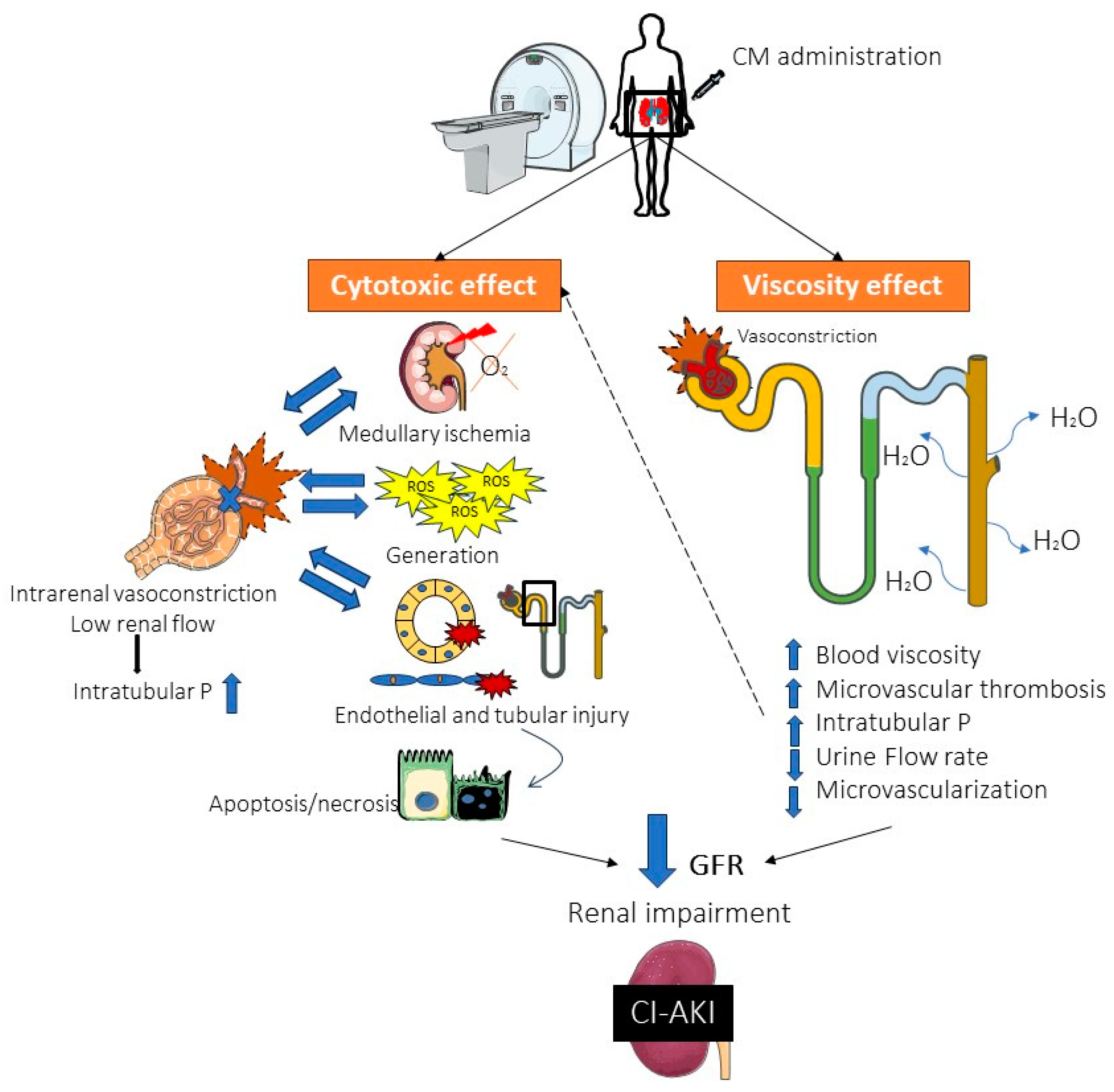
Figure 2.
Traditional and novel biomarkers classification. CysC, Cystatin C; NGAL, Neutrophil Gelatinase-Associated Lipocalin; KIM-1, Kidney Injury Molecule-1; IGFBP, Insulin-like Growth Factor-Binding Protein; TIMP, Tissue Inhibitor of Metalloproteinase; L-FABP, Liver Fatty Acid-Binding Protein; NAG, N-Acetyl-β-D-Glucosaminidase; GST, α-Glutathione S-Transferase; MCP-1, Monocyte Chemoattractant Protein-1; IL, Interleukin; CTGF, Connective Tissue Growth Factor; VEGF, Vascular Endothelial Growth Factor; OPN, Osteopontin; FENA, Fractional Excretion of Sodium; RBP, Retinol Binding Protein; VDBP, Vitamin D Binding Protein; GGT, Gamma-glutamyltransferase activity; MK, Midkine; miRNAs, microRNA.
Figure 2.
Traditional and novel biomarkers classification. CysC, Cystatin C; NGAL, Neutrophil Gelatinase-Associated Lipocalin; KIM-1, Kidney Injury Molecule-1; IGFBP, Insulin-like Growth Factor-Binding Protein; TIMP, Tissue Inhibitor of Metalloproteinase; L-FABP, Liver Fatty Acid-Binding Protein; NAG, N-Acetyl-β-D-Glucosaminidase; GST, α-Glutathione S-Transferase; MCP-1, Monocyte Chemoattractant Protein-1; IL, Interleukin; CTGF, Connective Tissue Growth Factor; VEGF, Vascular Endothelial Growth Factor; OPN, Osteopontin; FENA, Fractional Excretion of Sodium; RBP, Retinol Binding Protein; VDBP, Vitamin D Binding Protein; GGT, Gamma-glutamyltransferase activity; MK, Midkine; miRNAs, microRNA.
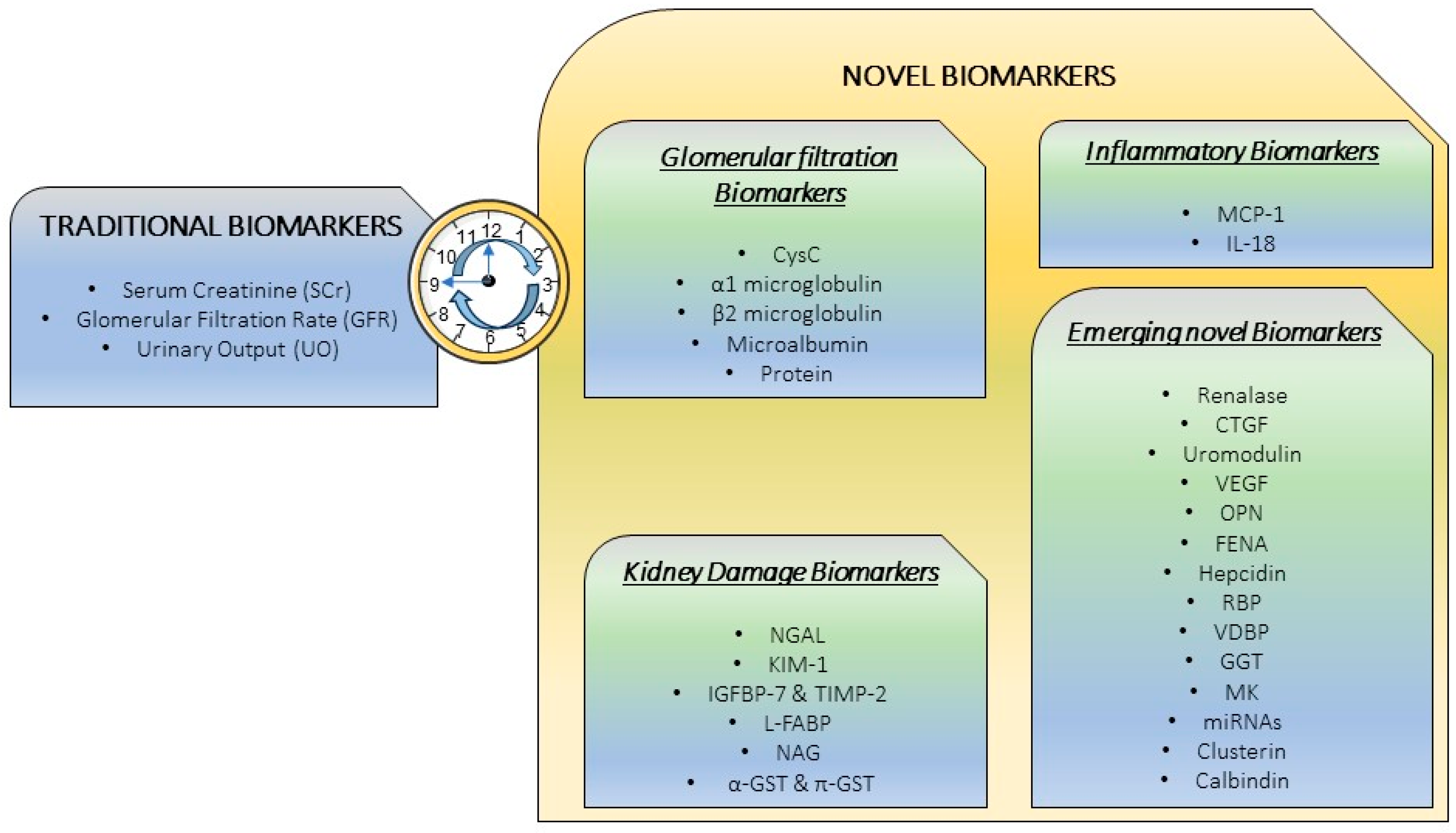
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



