
Submitted:
14 February 2024
Posted:
15 February 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The enduring psychological effects of the COVID-19 pandemic continue to affect individuals long after the immediate health concerns have subsided. This research aims to identify specific groups within the Romanian population who are at a higher risk of experiencing mental health challenges that can interfere with everyday life and may lead to more serious mental health disorders.
Methods: Conducted as a cross-sectional survey, this study evaluated the prevalence and intensity of psychological distress using the DASS-21 questionnaire. An online survey distributed via Google Forms also gathered socio-demographic data and COVID-19-specific information. Statistical analyses included the Shapiro-Wilk test, Fisher's exact test, and Z-tests with Bonferroni correction. Quantitative independent variables that lacked a normal distribution were compared between groups using either the Mann-Whitney U test or the Kruskal-Wallis H test.
Results: Analysis of 521 questionnaires, filled out by a predominantly middle-aged cohort of 320 women and 201 men, revealed that 63.72% of participants worked outside the healthcare field. Those unemployed or retired reported significantly higher anxiety levels than individuals in other sectors. Moreover, living alone, experiencing the loss of close relatives (6.14%) or friends (33.59%), and undergoing hospitalization or reinfection due to COVID-19 were linked to significantly elevated distress scores.
Conclusion. By identifying the segments of the population most vulnerable to psychological distress, as evidenced by higher scores among the unemployed, retirees, individuals living alone, and those directly affected by COVID-19 through personal health or loss, targeted initiatives for psychological screening and therapy can be established. Such measures are essential for enhancing the post-pandemic mental well-being of Romanians, addressing the specific needs uncovered in this study.
Keywords:
COVID-19
; mental health
; anxiety
; depression
; stress
1. Introduction
Since the beginning of the pandemic, medical professionals, psychologists, and health researchers have highlighted the risks of psychological distress among the general population and healthcare workers exposed to COVID-19 pathology [1,2,3,4,5]. Even without illness, population quarantine has had adverse psychological effects, evident in previous epidemics (MERS and SARS) as well as in the recent pandemic, particularly pronounced during prolonged isolation, inadequate communication, and instances of supply shortages and financial strain [6]. Long-term studies on the psychiatric aftermath of the SARS epidemic revealed lasting psychological vulnerabilities persisting even up to 4 years after the initial outbreak [7,8,9]. When examining the repercussions of reinfections, the heightened risks extend to all-cause mortality and adverse health outcomes, encompassing mental health, during both the acute and post-acute phases of reinfection [10].
In Romania, there is a strong scientific interest in studying the impact of COVID-19, both from a medical [11] and psychological perspective [12,13,14]. Romanian researchers have examined the psychological pressure of the pandemic on the general population [12], as well as on healthcare professionals [13,14]. However, the psychological consequences of reinfection with this new pathology and the timing of reinfection concerning therapeutic possibilities have not yet been addressed in this Romanian socio-cultural context.
Furthermore, as Brenda Penninx and collaborators highlight in a review article, the monitoring of mental health status must persist beyond the pandemic due to the associated and dynamically evolving repercussions, with effects experienced long after the primary event, especially in countries where the medical and psychosocial infrastructure was previously unprepared [15].
There are numerous psychological tools used to identify psycho-emotional imbalance [16,17], nonetheless, we utilized the DASS-21 scale, a validated instrument for the adult population in our country [18].
Our study aims to investigate the following scientific hypotheses:
- The psychological burden during the COVID-19 pandemic varied according to occupation and the extent of social involvement, particularly whether an individual was actively employed or retired. Engaging in healthcare roles presented an elevated level of psychological pressure.
- Romanians residing with their families have encountered a diminished psychological impact in contrast to those living alone. Furthermore, we suggest that having a pet functions as a protective source of emotional support.
- Anxiety, stress, and depression induced by the pandemic were heightened for individuals who witnessed the death of a friend or a relative.
- Vaccination conferred an emotionally protective status by reducing stress, anxiety, and depression.
- The hospitalization of individuals with COVID-19 intensified psychological imbalance by exacerbating distress, and the persistence of symptoms further compromised the mental health of Romanians.
- The experience of going through the illness was perceived as a negative emotional burden, varying across the three phases of the pandemic.
- Reinfection with SARS-CoV-2 emotionally strained the analyzed population.
Thus, the purpose of the study is to uncover the complex relationships between the various determinants.
2. Materials and Methods
Study design.
The current study is a cross-sectional survey designed to ascertain the prevalence and severity of psychological distress, encompassing stress, anxiety, and depression, within the Romanian population. Employing an online interview format, the study was distributed cross-sectionally through the mobile messaging app WhatsApp using Google Forms.
Exclusion criteria for the study included individuals under 18 years of age (in Romania, individuals above 18 years are considered adults) and those with declared psychiatric pathology. It is important to note that respondents did not experience any benefits or secondary repercussions as a result of participating in this study. Their participation was voluntary and without constraints, and non-completion of the interview resulted in exclusion from statistical processing.
The questionnaire underlying our study encompassed socio-demographic data (age, gender, social status (employed/retired), living arrangements, pet ownership), questions related to COVID-19 pathology (experience of the illness, reinfection status, vaccination history, hospitalization, persistent symptoms, loss of a relative or friend during the pandemic, timing of illness about the three pandemic waves in Romania), and the DASS-21 questionnaire.
The Depression Anxiety Stress Scale (DASS-21) serves as a widely utilized assessment tool in both general and clinical populations globally [19]. The study utilized the short version of the self-report scale, consisting of 21 questions. Each question was rated on a 4-point Likert scale, ranging from 0 (does not apply to me at all - NEVER) to 3 (applies to me very often or most of the time - ALWAYS). The total score was computed by summing up the points for each disease category, with each category comprising 7 questions. Measuring negative emotional states is crucial for clinicians to recognize and address mental disorders. Elevated levels indicative of negative affect act as a warning sign, underscoring the necessity for proactive intervention measures to prevent the development of psychiatric disorders. Based on their responses, emotional distress could be categorized as normal, mild, moderate, severe, or extremely severe. A higher score indicates a more severe manifestation of the respective disorder.
Study population.
The analyzed population consists of socially active adults or retirees who actively engage on various social media platforms. Recruitment was conducted through general practitioners and pulmonologists across different cities in Romania. The study adhered to the relevant legislation governing the processing and free movement of personal data. This research aligns with international ethical recommendations, ensuring absolute confidentiality of the collected data and upholding the anonymity and security of participants. The institutional ethics committee at "Ovidius" University of Constanța, Romania, with protocol number DCI 54/31.05.2023, granted approval for this study. The principles outlined in the Declaration of Helsinki were appropriately adhered to. Following informed consent, participants completed a 10-minute online survey. Data collection took place from June 1 to July 1, 2023, after the World Health Organization (WHO) declared that the COVID-19 pandemic was no longer categorized as a global health emergency.
Statistical analysis.
The study data was analyzed utilizing IBM SPSS Statistics 25 software, and data visualizations were generated using Microsoft Office Excel/Word 2021. For quantitative variables, normal distribution was assessed through the Shapiro-Wilk test, and outcomes were presented as means with standard deviations or medians with interquartile ranges. Qualitative variables were expressed as counts or percentages, and group distinctions were evaluated using Fisher's exact test. To provide additional insights into the contingency table results, Z-tests with Bonferroni correction were conducted. Quantitative independent variables lacking a normal distribution were compared between groups using either the Mann-Whitney U test or the Kruskal-Wallis H test. Post-hoc Dunn-Bonferroni tests were performed for more in-depth analysis and interpretation of the results in the comparisons of quantitative independent variables.
3. Results
A total of 1000 questionnaires were disseminated through social media groups of general practitioners and pulmonologists. Out of these, 637 questionnaires were filled out by the participants. However, only 521 of these completed surveys fulfilled the criteria for inclusion in the statistical analysis, with the remaining surveys deemed invalid for various reasons.
Among the respondents, there were 201 males and 320 females, spanning ages 18 to 85 years. To better characterize the cohort, we categorized them as young adults (ages 18-24), adults (ages 25-35), middle-aged individuals (ages 36-64), and older adults (ages >65). Females constituted 61.42% of the participants, while males accounted for 38.58%. A majority of the participants fell into the middle-aged category (n=296; 56.81%), with substantial participation from adults (n=168; 32.24%). Young adults (n=37; 7.10%) and older adults (n=20; 3.83%) comprised smaller proportions of the sample.
The survey used questions from the DASS-21 questionnaire, which is designed to assess the presence of symptoms of anxiety, stress, and depression in a generally healthy population. Each condition is assessed using 7 questions resulting in scores between 0 and 21. As the shortened version of the questionnaire was used in this survey, the scores obtained will be doubled and subsequent analysis will determine the severity of these symptoms.
3.1. Comparative Analysis of Anxiety, Depression, and Stress Levels Based on Occupational Status
We analyzed, in terms of DASS parameters, the emotional impact of the pandemic distributed based on the type of occupational activity. We paid special attention to individuals working in the medical field, who not only experienced the pressure of working in an infectious risk environment but also witnessed the suffering of COVID-19 patients (Figure 1).
According to the Shapiro-Wilk test, the distribution of values was non-parametric across all groups (p<0.05). Most participants were employed outside the medical field (n=332; 63.72%), while those in the medical field constituted 24.18% (n=126), and the unemployed or retired accounted for 12.09% (n=63). Based on Kruskal-Wallis H-tests, there were significant differences in anxiety (p=0.040), depression (p=0.049), and stress (p=0.027) scores among the groups. However, post-hoc Dunn-Bonferroni tests revealed significant differences only in anxiety scores: Individuals working as domestic workers, being unemployed, or retired exhibited a significantly higher anxiety score (median = 16, IQR = 2-28) compared to those employed in various other occupational domains (median = 10, IQR = 2-18) (p=0.035). A similar statistical pattern was observed for depression or stress scores, although, in these cases, only trends toward statistical significance were noted (depression – p = 0.079, stress – p = 0.061), potentially due to the limited number of household members included in the analysis.
3.2. Comparative Analysis of Anxiety, Depression, and Stress Levels Based on Living Arrangements
Humans are social beings who communicate affectionately, empathize, and show compassion towards their fellow beings. Based on these premises, we interviewed respondents regarding whether they live alone or with other family members. We applied DASS variables over this pragmatic aspect, which holds significant influence over mental well-being, especially in crises, during travel restrictions, and interpersonal socialization limitations.
80.04% (n=417) of respondents reside with at least one other person, while 19.96% (n=104) live alone. According to the Mann-Whitney U-tests, there were significant differences in the values for anxiety (p=0.042), depression (p=0.017), and stress (p=0.021) between the groups. Patients living alone exhibited significantly higher values for the analyzed scores (anxiety: median = 13, IQR = 2.5-22; depression: median = 10, IQR = 4-20; stress: median = 13, IQR = 4-21.5) compared to patients who lived with their family (anxiety: median = 8, IQR = 2-18; depression: median = 6, IQR = 2-14; stress: median = 8, IQR = 2-18) (Figure 2).
When analyzing the impact of pets on the perception of DASS parameters, we observed an improvement in anxiety among pet owners, although without statistically significant relevance. The distribution of scores was non-parametric across all groups, as indicated by the Shapiro-Wilk tests (p<0.05). According to the Mann-Whitney U tests, the differences in anxiety (p=0.575), depression (p=0.901), and stress (p=0.733) scores were not statistically significant between persons with and without pets.
3.3. Comparative analysis of anxiety, depression, and stress levels among groups that had experienced the loss of a relative or a friend
The loss through the death of a person with whom there were channels of affective communication and a history of moments filled with intense positive emotion will result in the suffering of the social circle and mourning. The study aimed to identify the extent of these sufferings in the context of the COVID-19 Pandemic. Based on initial results, 6.14% (n=32) of respondents reported having first-degree relatives who had died from this disease.
According to the Mann-Whitney U-tests, there were significant differences in the values for anxiety (p<0.001), depression (p<0.001), and stress (p<0.001) between the groups. Patients who had lost first-degree relatives exhibited significantly higher values for the analyzed scores (anxiety: median = 22, IQR = 10.5-32; depression: median = 19, IQR = 10.5-30; stress: median = 22, IQR = 9-33.5) compared to patients who had not lost relatives (anxiety: median = 8, IQR = 2-18; depression: median = 6, IQR = 2-16; stress: median = 8, IQR = 2-18).
Additionally, the death of a friend, due to COVID-19 has destabilized the mental equilibrium of respondents compared to individuals who have not experienced grief. In our study, 33.59% (n=175) of respondents reported losing a friend.
According to the Mann-Whitney U tests, there were significant differences in the values for anxiety (p<0.001), depression (p<0.001), and stress (p<0.001) between the groups. Patients who had lost friends exhibited significantly higher values for the analyzed scores (anxiety: median = 14, IQR = 4-26; depression: median = 12, IQR = 2-22; stress: median = 14, IQR = 4-24) compared to patients who had not lost close individuals (anxiety: median = 8, IQR = 2-16.5; depression: median = 6, IQR = 2-14; stress: median = 8, IQR = 2-16).
3.4. Comparison of anxiety, depression, and stress scores between the COVID-19 vaccination groups
The advent of the vaccine has positively altered the overall mental state, instilling hope for halting the spread of the virus and associated pathologies. The analysis of DASS variables aimed to quantify these psychological changes for the analyzed population. The distribution of scores was non-parametric across all groups, as indicated by the Shapiro-Wilk tests (p<0.05).
Of the respondents, 75.43% (n=393) were vaccinated, while 24.56% (n=128) did not get the vaccine. Among the vaccinated, 27.25% (n=142) received the vaccine before contracting COVID-19, and 9.78% (n=51) were vaccinated after the COVID-19 infection. According to the Mann-Whitney U tests, differences in anxiety (p=0.211), depression (p=0.158), and stress (p=0.218) scores were not statistically significant between patients who were or were not vaccinated against SarsCov2.
3.5. Comparative Analysis of Anxiety, Depression, and Stress Levels between COVID-19 Hospitalized Patients and those Managed Outside Hospital Settings.
In the initial phase of the pandemic, patients were hospitalized for better isolation and to limit the spread of the virus in Romania. Subsequently, as the number of infection cases increased, COVID-19-positive patients were hospitalized for severe forms of the disease, requiring increased oxygen or even mechanical ventilation, necessitating invasive treatments. Moreover, individuals with chronic pathologies and compromised immune systems developed more severe forms of the illness. In this context, the daily governmental mortality reports were related to hospitalized patients. Against this factual backdrop, our study aimed to retrospectively assess the perception of COVID-19 patients regarding their hospitalization. (Table 2, Figure 3).
The scores exhibited a non-parametric distribution across all groups, as determined by the Shapiro-Wilk tests (p<0.05). According to the Mann-Whitney U tests, significant differences were observed in anxiety (p<0.001), depression (p<0.001), and stress (p<0.001) scores between the groups. Specifically, patients who were hospitalized following COVID-19 infection displayed markedly higher values for the analyzed scores (anxiety: median = 19, IQR = 8-30; depression: median = 16, IQR = 6-28; stress: median = 19, IQR = 8-32) compared to patients who were not hospitalized (anxiety: median = 8, IQR = 2-14; depression: median = 6, IQR = 2-12; stress: median = 6, IQR = 2-14).
3.6. Comparative analysis of anxiety, depression, and stress levels between the time of infection. We have classified the distinct stages of the pandemic as follows:
- The Initial Phase: This pertains to the period from the onset of the first case of COVID-19 until January 2021.
- The Middle Phase: This covers the timeframe from January 2021 to January 2022, aligning with the emergence of the Omicron variant.
- The Final Phase: This phase spans from January 2022 until May 5, 2023, coinciding with the World Health Organization's (WHO) declaration that the pandemic no longer constitutes an international concern.
When comparing anxiety, depression, and stress scores between individuals with a COVID-19 infection at the beginning of the pandemic and those without, the results are as follows: The distribution of scores was non-parametric across all groups based on the Shapiro-Wilk tests (p<0.05). According to the Mann-Whitney U tests, there are significant differences in anxiety (p<0.001), depression (p<0.001), and stress (p<0.001) scores between the groups. Patients who had a COVID-19 infection at the beginning of the pandemic had significantly higher values for the analyzed scores (anxiety: median = 20, IQR = 4-32; depression: median = 16, IQR = 6-29; stress: median = 20, IQR = 6-32) compared to patients who weren't infected at the beginning of the pandemic (anxiety: median = 10, IQR = 4-18; depression: median = 8, IQR = 4-16; stress: median = 10, IQR = 4-18).
In the middle period of the pandemic, the distribution of scores was non-parametric across all groups based on the Shapiro-Wilk tests (p<0.05). According to the Mann-Whitney U tests, differences in anxiety (p=0.095) and depression (p=0.065) were not statistically significant between patients who were or were not COVID-19 infected during this period. There were only tendencies toward statistical significance, indicating higher values of scores in cases of infected patients over non-infected patients. However, the stress score (p=0.045) was significant between groups. Patients who had a COVID-19 infection in the middle period of the pandemic had significantly higher values of the stress score (median = 14, IQR = 5-22) compared to patients who weren't infected during this period (median = 10, IQR = 4-22). These results suggest that the impact of COVID-19 on the mental health of infected patients tends to decrease as time progresses from the beginning of the pandemic.
To analyze the ending phase of the pandemic, the distribution of scores displayed non-parametric characteristics across all groups, as indicated by the Shapiro-Wilk tests (p<0.05). According to the Mann-Whitney U tests, significant differences in anxiety (p=0.042), depression (p=0.007), and stress (p<0.001) scores were observed between groups. Patients who contracted COVID-19 at the end of the pandemic exhibited notably lower values for the analyzed scores (anxiety: median = 10, IQR = 4-20; depression: median = 8, IQR = 4-14; stress: median = 8, IQR = 4-18) compared to patients who remained uninfected at the end of the pandemic (and were infected at the beginning and/or in the middle period) (anxiety: median = 14, IQR = 6-24; depression: median = 12, IQR = 4-22; stress: median = 14, IQR = 6-24). These results provide evidence that the mental health impact of COVID-19 infection diminishes even further over time, possibly reaching its lowest point at the end of the pandemic, primarily due to societal adaptation, milder forms of the disease, and effective treatments.
3.7. Comparative analysis of anxiety, depression, and stress levels concerning reinfection with SARS-CoV2
In Table 3 the scores exhibited a non-parametric distribution across all groups as per the Shapiro-Wilk tests (p<0.05). A total of 18.6% (n=97) reported experiencing the disease on multiple occasions. Based on the Mann-Whitney U tests, significant differences in anxiety (p=0.001), depression (p<0.001), and stress (p<0.001) scores were observed between groups. Patients with reinfections had notably higher scores (anxiety: median = 14, IQR = 4-26; depression: median = 12, IQR = 4-24; stress: median = 14, IQR = 5-24) compared to those without reinfections (anxiety: median = 8, IQR = 2-18; depression: median = 6, IQR = 2-14; stress: median = 8, IQR = 2-18).
4. Discussion
Recently, the onset of the COVID-19 pandemic has underscored the significant impact that a new virus can exert on human life. The substantial changes triggered by COVID-19 have presented notable societal challenges worldwide, influencing various facets of existence [1]. The protracted duration and far-reaching repercussions of this crisis have led to widespread psychological distress on a global scale.
Since the beginning of the pandemic, researchers have documented a decline in the general population's well-being, attributed to both the fear of illness and the secondary consequences of the pandemic, including imposed restrictions, and pre-existing economic, social, and medical impacts [20,21]. The present study aims to assess the mental state of the Romanian population post-pandemic, employing a validated psychological tool. Consequently, we intend to conduct a comparative analysis of the results obtained from the sampled population of similar literature.
4.1. Mental distress and occupational status
Many studies conducted across continents and throughout different phases of the pandemic have consistently shown, regardless of socio-cultural context, that healthcare workers have been more profoundly affected in terms of psychological burden compared to individuals in other life domains [13,22,23]. Our study aligns with these global scientific findings. However, the novelty lies in the fact that, despite being exposed, medical professionals exhibited lower levels of anxiety, depression, and stress compared to those who were not working at all, including retirees, homemakers, or the unemployed. This may initially seem counterintuitive, but upon closer examination, it appears that from an external perspective, the battle seems more perilous than when you are a "soldier in the fight." One possible explanation is that active involvement in a concrete medical activity eliminates the fog of misinformation and conspiracy theories. Instead, the satisfaction of aiding those in distress emerges aspects that, overall, reduce the negative emotional burden compared to those who experienced the pandemic more through media reports, amplified by personal vulnerability, such as comorbidities increasing the risk of a more severe form of the disease, and/or financial and social insecurity.
When comparing the psychological strain results of workers in various non-medical fields with those of individuals who are not employed, our findings indicate that the active population expresses lower levels of depression, anxiety, and stress. Similar results, suggesting the activation of mental protective mechanisms for the employed population across different social layers, have been recently published [23,24]. These results emphasize that active engagement in a work regimen represents a resilience strategy and reduces the negative impact of uncertainty, stress, anxiety, and depression in the general population.
4.2. Living Arrangement and its Impact on pandemic time mental health
From the perspective of the Romanian individuals who were interviewed, living alone exacerbated stress, anxiety, and depression, regardless of other contributing factors. Similar effects have been reported by other researchers. For example, a Spanish study on medical professionals during the pandemic revealed that living alone does not significantly impact mental well-being; instead, it is primarily the experienced loneliness that has unfavorable effects [25].
In a study conducted in the United States, it was found that residing in larger families had a resilience effect during the pandemic, while living alone had a negative impact on mental well-being [26]. Additionally, in China, when factors such as age, gender, and social status were analyzed alongside living alone, female loneliness and self-employment were identified as variables that negatively influence psychosocial well-being [27].
In conclusion, living alone during the pandemic period had adverse effects on mental balance, irrespective of the continent or the population studied, and this aspect was further influenced by loneliness, as well as economic and medical conditions.
Some authors have demonstrated that the human-pet relationship acts as an emotional protective factor, even during the pandemic [28]. Analyzing this hypothesis, the current study was unable to establish statistically significant correlations between the presence of a pet and improvement in mental health status within the studied population.
4.3. The Impact of Grief on Mental Health
The death of a friend or a family member abruptly alters the psychological framework of life, as the grief caused by the irreversible loss of a person influences their attitude and behavior, and can also have significant somatic manifestations. In a large-scale Australian cohort, a longitudinal study spanning 15 years has determined that the degree of connection or attachment developed over time significantly influences the manifestation of anxiety symptoms following the loss of a friend. The effect of losing a family member is further shaped by additional variables such as age, gender, ethnicity, religion, and interpersonal dynamics. These elements can lead to diverse degrees of psychological distress across different types of loss. The impact may persist for up to four years, with females being more adversely affected than males [29]. To all these aspects, the anxiety from the pandemic, fear of illness, and social restrictions add further strain on human resilience [30,31].
A study encompassing ten Latin American countries, where mortality rates during the initial wave of the pandemic reached alarming levels, investigated the effect of grief on health science students, quantifying the extent of distress about the emotional proximity to the deceased. The findings align with intuitive expectations: the closer the deceased was to the individuals, the deeper the impact on their stress, anxiety, and depression levels [32].
Our results are consistent with existing literature: individuals who have suffered the loss of a friend or a close family member display higher levels of anxiety, stress, and depression in comparison to those who have not experienced the death of a loved one. Thus, negative emotions associated with grief further destabilize individuals with a more fragile mental state, those with lower resilience to stress, or those with pre-existing medical conditions.
4.4. The Influence of Vaccination on Mental Health
The vaccine against SARS-CoV-2 was introduced with the hope of minimizing the somatic progression of the disease and, indirectly, optimizing the emotional mechanisms that govern the population's psychological state. However, the introduction of the vaccine triggered unexpected counter-reactions, ranging from hesitation and fear to outright refusal of vaccination in certain cases. The causes of this anxiety were linked to misinformation, the fact that the research behind the vaccine was not entirely transparent, and that it was not extensively tested due to global emergency reasons, as we know [33]. In this context, studies have yielded inconsistent results regarding adherence to vaccination and the alleviation of anxiety. For example, in the US, vaccination improved psychological parameters such as anxiety, stress, and depression, except among certain ethnic groups and individuals with lower educational levels [34]. On the other hand, a study in China showed that the level of anxiety and depression was not alleviated by the number of vaccinations or the timing of vaccination [32]. A study conducted in Poland, which analyzed the attitudes of healthcare professionals towards vaccination, found that 94% of healthcare workers were open to the idea of vaccination, being informed and aware of the benefits provided. The authors examined the factors contributing to vaccine hesitancy, which was more prevalent among the general population, and identified misinformation, distrust in state institutions, and a lower level of education as key determinants. [35].
In a 2021 UK study, researchers found significant mental health improvements following vaccination. These benefits were not only statistically significant but also substantial, akin to the effects of major life events. This indicates that before vaccination, widespread anxiety about catching COVID-19 was a major source of psychological distress for many. Additionally, the study emphasized that individuals with underlying health conditions (clinically vulnerable) and older adults particularly experienced significant mental health improvements from vaccination. [28].
When we analyzed the Romanian group from the perspective of vaccination, although there were improvements in mental status, these did not yield statistically significant changes, regardless of whether the vaccine was received before or after experiencing COVID-19. These findings confirm the multifaceted nature of the psycho-emotional dynamics during the pandemic.
4.5. Comparative Analysis of Distress in the Population Requiring Hospitalization versus Those Who Did Not
The findings of our study highlight the perception of stress, anxiety, and depression in COVID patients who required hospitalization in a statistically significant manner, compared to those who managed the illness at home. This aspect aligns with other published medical reports, regardless of the pandemic phase or nationality [36,37].
Starting from the host immune response to SARS-CoV-2 infection, the persistent psychological stress before and during infection, and a possible direct viral infection of the central nervous system, a group of Italian researchers have proposed the hypothesis of potential mechanisms inducing neuropsychiatric sequelae [38]. This concept is bolstered by findings that elevated immune/inflammatory baselines, marked by increased circulating inflammation biomarkers, are identified in mood disorders without apparent triggering events. These findings are currently explored as fundamental pathogenic mechanisms behind depressive disorders [39]. Peripheral cytokines involved in the host's anti-viral response may induce psychiatric symptoms by triggering inflammation both peripherally and in the central nervous system [38]. Moreover, major stress factors including the fear of severe and unfamiliar illnesses, isolation, and social stigma, may play an important role in the extensive emotional turmoil and heightened likelihood of mental health disorders among COVID-19 hospitalized patients.
4.6. Mental strain according to the timing of infection, concerning the pandemic waves
In our study, we found that patients who contracted COVID-19 at the beginning of the pandemic had higher levels of anxiety, depression, and stress. These psychological symptoms gradually decreased as the pandemic progressed. The mitigation of the psychological impact on the population has several causes: firstly, the emergence of effective therapeutic strategies; secondly, the decrease in the virulence of the pathogen over time; and thirdly, the development of adaptation mechanisms and mental flexibility to the imposed regulations.
In Italy, research focused on psychological distress during the first wave of the COVID-19 lockdown assessed levels of stress, depression, and anxiety at the beginning and end of the lockdown period, spanning two months. The study revealed that anxiety levels remained relatively unchanged, whereas stress and depression levels increased over this period. Additionally, individuals with initially higher depression and stress levels were found to be more likely to report elevated levels at the end of the lockdown [40].
Contrary to the results from Italy, a longitudinal study of two UK cohorts indicates that depression rates during the pandemic mirrored those before the pandemic. However, the rate of anxiety almost doubled, compared to the pre-pandemic times. For both cohorts, the levels of anxiety and depression during the pandemic were elevated in younger people, women, individuals with existing mental or physical health issues, and those experiencing socio-economic challenges [5].
To reduce the contradiction, the variable of time must be introduced, in the sense that the Italian study was published in November 2020, and the British study in June 2021, both pieces of research being conducted during the pandemic when the psychological impact was fully felt by the population.
4.7. The consequences of reinfection
Reinfection with COVID-19, defined as a positive RT-PCR test occurring at least 90 days after the primary infection, was initially rare; the first documented case was reported in Hong Kong, China, in August 2020, after 142 days had passed between infections [41].
A meta-analysis research on COVID-19 reinfection, published in 2022 and analyzing 91 studies, concludes that strong natural immunity develops after the primary infection and can persist for more than a year. Even though reinfection rates notably increased during the Omicron variant surge, the probability of encountering a severe or deadly disease from a subsequent infection stayed exceedingly low [42].
Another meta-analysis published in 2023 in a Chinese journal concludes that, although the possibility of reinfection exists, it affects the general population at a rate of less than 3%, and healthcare workers at a rate of 6.02% [43].
A study from the US, utilizing the Department of Veterans Affairs national healthcare database, found that reinfection with SARS-CoV-2 poses additional risks of mortality, hospitalization, and various sequelae, including issues related to the lungs, heart, blood, diabetes, gastrointestinal system, kidneys, mental health, muscles and bones, and nervous system. These risks were observed regardless of one's vaccination status and were most significant during the acute phase but continued to be present six months into the post-acute phase. Compared to individuals who were never infected, the cumulative risks and health impacts escalated with each subsequent infection. Therefore, strategies to prevent reinfection are essential to reduce the overall disease burden caused by SARS-CoV-2 [44].
The results of a systematic review on SARS-CoV-2 reinfection indicate that reinfection is possible either due to the host immune system's inability or the aggressiveness of other viral variants. However, there is also published literature that identifies reinfection solely based on RT-PCR without viral genetic sequencing, which introduces a source of bias in validating conclusions. Consequently, the authors recommend that patients who have recovered from the disease and have been vaccinated continue to adhere to biological safety measures [45].
The psychological effects of reinfection, especially in Romania, have not yet been sufficiently researched. In our study group, only 18.6% of participants reported having been infected with SARS-CoV-2 multiple times, and these individuals had higher levels of anxiety, depression, and stress compared to those who had not been repeatedly infected.
In summary, reinfection with COVID-19 poses risks of both physical and psychological disability, with the mental health component acting like a difficult-to-estimate halo in terms of magnitude, yet having a long-term influence on the well-being of the global population.
The limitations of the study
Despite the considerable effort put into this study, we must acknowledge its limitations. First, its cross-sectional nature captured only a snapshot of the dynamic mental health state of Romania's population. Secondly, participants were selected based on their use of the internet and technology, resulting in the underrepresentation of the elderly and socio-economically disadvantaged populations. The third sensitive point involves personal perception and the anonymous declaration of the absence of prior mental health conditions; the authors could not verify the accuracy of this information, relying on the honesty of participants. Finally, self-assessment of COVID-19 infection/reinfection and its severity may introduce biases that could either understate or overstate symptoms.
Further research is essential for understanding the dynamics and relationships between factors existing before the pandemic and those specific to COVID-19 that influence mental health throughout the pandemic period. It is important to continue tracking depression and anxiety, as well as their associated impairments, to assess the crisis's long-term repercussions.
This effort will help ensure that future strategies are designed to optimally maintain both mental and physical well-being. The results of this survey are best viewed as a qualitative and descriptive analysis of how the pandemic has affected the citizens of Romania. Future longitudinal studies spanning multiple years will yield more detailed information regarding the mental health of the population.
5. Conclusions
The pandemic has led to significant psychological distress, manifesting as anxiety, stress, and depression, often reaching levels of clinical concern. Therefore, addressing and reducing the negative psychological effects of COVID-19 should be an urgent public health priority. Understanding these psychological impacts is crucial for providing appropriate support and care to those at risk. In the socio-economic context of Romania, we have identified that elderly individuals, retirees, or those unemployed, who live alone, have been hospitalized for COVID-19, have suffered the loss of a loved one during the pandemic, and have experienced reinfection, regardless of vaccination status, remain psychologically vulnerable even after the pandemic has ended.
Author Contributions
Conceptualization: A.M. and A.H. and R.G.E.; Methodology: A.M., A.H., A.C. and E.D.; Software: A.M. and A.H.; Validation: A.M., A.H., A.C., R.G.E. and E.D.; Formal analysis: A.M., A.H., A.C., R.G.E. and E.D.; Investigation: A.M. and A.H.; Resources: A.M. and A.H.; Data curation: A.M., A.H. and A.C.; Writing—original draft preparation: A.M. and A.H.; Writing—review and editing: A.M., A.H., A.C. and E.D.; Visualization: A.M., A.H., A.C., R.G.E. and E.D.; Supervision: A.C., R.G.E. and E.D.; Project administration: A.M., A.H., A.C, R.G.E. and E.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted following the Declaration of Helsinki, and approved by the institutional Ethics Committee ("Universitatea Ovidius Constanța", Romania, no. DCI 54/31.05.2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The online interview, distributed via Google Forms, was applied through this link, which is closed at the present time. https://docs.google.com/forms/d/e/1FAIpQLSeIOPkABS031tjimCk8SKFVSDchhUs4-ppUyJkRnb3kSfqgFQ/viewform?fbclid=IwAR06utiriEkJmt0bubYVJygMSYPFSazHYyPr97TnktigaCyjtad4378cUlE The responses that form the basis of this study can be found through this link. https://docs.google.com/forms/d/1cDFLnq8Br8FKLVG5GeCaqQBA3ezJO90-7pvF90pCtSg/edit#responses.
Acknowledgments
We are grateful to Dr. Andrei Condurache for his skilled advice on biostatistical analysis.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Holmes, E.A.; O'Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; Ford, T.; John, A.; Kabir, T; King, K.; Madan, I.; Michie, S.; Przybylski, A.K.; Shafran, R.; Sweeney, A.; Worthman, C.M.; Yardley, L.; Cowan, K.; Cope, C.; Hotopf, M.; Bullmore, E. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry, 2020, Jun; 7(6):547-560. [CrossRef]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry, 2020, Jul; 7(7):611-627. [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. Gen Psychiatr, 2020, 33(2): e100213. [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open, 2020, 3(3): e203976. [CrossRef]
- Kwong, A.S.F.; Pearson, R.M.; Adams, M.J.; Northstone, K.; Tilling, K.; Smith, D.; Fawns-Ritchie, C.; Bould, H.; Warne, N.; Zammit, S.; Gunnell, D.J.; Moran, P.A.; Micali, N.; Reichenberg, A.; Hickman, M.; Rai, D.; Haworth, S.; Campbell, A.; Altschul, D.; Flaig, R.; McIntosh, A.M.; Lawlor, D.A.; Porteous, D.; Timpson, N.J. Mental health before and during the COVID-19 pandemic in two longitudinal UK population cohorts. Br J Psychiatry, 2021, Jun; 218(6):334-343. [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet, 2020, Mar 14; 395(10227):912-920. [CrossRef]
- Lam, M.H.; Wing, Y.K.; Yu, M.W.; Leung, C.M.; Ma, R.C.; Kong, A.P.; So, W.Y.; Fong, S.Y.; Lam, S.P. Mental morbidities and chronic fatigue in severe acute respiratory syndrome survivors: long-term follow-up. Arch Intern Med, 2009, Dec 14; 169(22):2142-7.
- Cheung, Y.T.; Chau, P.H.; Yip, P.S. A revisit on older adults suicides and Severe Acute Respiratory Syndrome (SARS) epidemic in Hong Kong. Int J Geriatr Psychiatry, 2008, Dec 23; (12):1231-8. [CrossRef]
- Mak, I.W.; Chu, C.M.; Pan, P.C.; Yiu, M.G.; Chan, V.L. Long-term psychiatric morbidities among SARS survivors. Gen Hosp Psychiatry, 2009, Jul-Aug; 31(4):318-26. [CrossRef]
- Bowe, B.; Xie, Y.; Al-Aly, Z. Acute and postacute sequelae associated with SARS-CoV-2 reinfection. Nat Med, 2022, Nov; 28(11):2398-2405.
- Musat, O.; Sorop, V.B.; Sorop, M.I.; Lazar, V.; Marti, D.T.; Susan, M.; Avram, C.R.; Oprisoni, A.;Vulcanescu, D.D.; Horhat, F.G.; et al. COVID-19 and Laboratory Markers from Romanian Patients—A Narrative Review. Life, 2023, 13, 1837. [CrossRef]
- Popa, E.; Tetia, T.; Poroch, M.; Ungureanu, M.; Cosmescu, A.; Barbacariu, L.; Slanina, A.M.; Bacusca, A.; Petroae, A.; Novac, O.; Manole, M.; Anton-Paduraru, D.; Popa, A.E.; Coman, E.A. The Effects of the COVID-19 Pandemic on Mental Health: A Web-Based Study Among Romanian Adults. Cureus, 2022, Nov 10; 14(11):e31331. [CrossRef]
- Hăisan, A.; Hogaș, S.; Măirean, C.; Punei, M.O.; Volovăț, S.R.; Hogaș, M.; Kantor, C.; Cimpoeșu, D. Compassion fatigue and compassion satisfaction among Romanian emergency medicine personnel. Front Med (Lausanne), 2023, Jul 24; 10:1189294. https://doi.org/10.3389/fmed.2023.1189294. [CrossRef]
- Stafie, C.S.; Profire, L.; Apostol, M.M.; Costache, I.I. The Professional and Psycho-Emotional Impact of the COVID-19 Pandemic on Medical Care—A Romanian GPs’ Perspective. Int. J. Environ. Res. Public Health, 2021, 18, 2031. [CrossRef]
- Penninx, B.W.J.H.; Benros, M.E.; Klein, R.S.; et al. How COVID-19 shaped mental health: from infection to pandemic effects. Nat Med, 2022, 28; 2027–2037. [CrossRef]
- Ali, A.M.; Alkhamees, A.A.; Hori, H.; Kim, Y.; Kunugi, H. The Depression Anxiety Stress Scale 21: Development and Validation of the Depression Anxiety Stress Scale 8-Item in Psychiatric Patients and the General Public for Easier Mental Health Measurement in a Post COVID-19 World. Int J Environ Res Public Health, 2021, Sep 27; 18(19):10142. [CrossRef]
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychol. Assess, 1998, 10 (2); 176–181.
- Zanon, C.; Brenner, R.E.; Baptista, M.N.; Vogel, D.L.; Rubin, M.; Al-Darmaki, F.R.; Gonçalves, M.; Heath, P.J.; Liao, H.Y.; Mackenzie, C.S.; Topkaya, N.; Wade, N.G.; Zlati, A. Examining the Dimensionality, Reliability, and Invariance of the Depression, Anxiety, and Stress Scale-21 (DASS-21) Across Eight Countries. Assessment, 2021, Sep; 28(6):1531-1544.
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales, 2nd ed.; Sydney: Psychology Foundation, Australia, 1995.
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [CrossRef]
- Wang, C.; Tee, M.; Roy, A.E.; et al. The impact of COVID-19 pandemic on physical and mental health of Asians:A study of seven middle-income countries in Asia. PLoS One, 2021, 16(2):e0246824. [CrossRef]
- Petrino, R.; Riesgo, L.G.; Yilmaz, B. Burnout in emergency medicine professionals after 2 years of the COVID-19 pandemic: a threat to the healthcare system?. Eur J Emerg Med, 2022, Aug 1;29(4):279-284. [CrossRef]
- Casjens, S.; Taeger, D.; Brüning, T.; Behrens, T. Altered Mental Distress Among Employees From Different Occupational Groups and Industries During the COVID-19 Pandemic in Germany. J Occup Environ Med, 2022, Oct 1; 64(10):874-880. [CrossRef]
- Foti, G.; Bondanini, G.; Finstad, G.L.; Alessio, F.; Giorgi, G. The Relationship between Occupational Stress, Mental Health and COVID-19-Related Stress: Mediation Analysis Results. Adm. Sci., 2023, 13, 116. [CrossRef]
- Cabello, M.; Izquierdo, A.; Leal, I. Loneliness and not living alone is what impacted on the healthcare professional's mental health during the COVID-19 outbreak in Spain. Health Soc Care Community, 2022, May; 30(3):968-975. [CrossRef]
- Ghimire, J.; Carswell, A.T.; Ghimire, R.; Turner, P.R. The Impact of U.S. Housing Type and Residential Living Situations on Mental Health during COVID-19. Int J Environ Res Public Health, 2021, Aug 5; 18(16):8281. [CrossRef]
- Xu, J.; Zhang, L. The effect of living alone on the mental health of the economically active floating population during the COVID-19 pandemic. Front Public Health, 2022, Aug 11; 10:931425. [CrossRef]
- Ratschen, E.; Shoesmith, E.; Shahab, L.; Silva, K.; Kale, D.; Toner, P.; Reeve, C.; Mills, D. S. Human-animal relationships and interactions during the Covid-19 lockdown phase in the UK: Investigating links with mental health and loneliness. PLoS One, 2020, 15 (9), e0239397. [CrossRef]
- Liu, W.-M.; Forbat, L.; Anderson, K. Death of a close friend: Short and long-term impacts on physical, psychological and social well-being. PLoS ONE, 2019, 14, e0214838.
- Araujo Hernández, M.; García Navarro, S.; García-Navarro, E.B. Approaching grief and death in family members of patients with COVID-19: Narrative review. Enferm. Clin., 2021, 31, S112–S116.
- Joaquim, R.M.; Pinto, A.L.C.B.; Guatimosim, R.F.; de Paula, J.J.; Souza Costa, D.; Diaz, A.P.; da Silva, A.G.; Pinheiro, M.I.C.; Serpa, A.L.O.; Miranda, D.M.; et al. Bereavement and psychological distress during COVID-19 pandemics: The impact of death experience on mental health. Curr. Res. Behav. Sci., 2021, 2, 100019. [CrossRef]
- Zhang, X.; Cai, Y.; Zhu, K.; Liu, Z.; Zhou, Q.; Zhu, Y.; Zhou, C.; Zhong, Z.; Liu, Y.; Xiao, W. Prevalence and risk factors of depression and anxiety among Chinese adults who received SARS-CoV-2 vaccine - A cross-sectional survey. J Affect Disord., 2023, Mar 1; 324:53-60.
- Pandey, K.; Thurman, M.; Johnson, S.D.; Acharya, A.; Johnston, M.; Klug, E.A.; Olwenyi, O.A.; Rajaiah, R.; Byrareddy, S.N. Mental Health Issues During and After COVID-19 Vaccine Era. Brain Res Bull., 2021, Nov; 176:161-173. [CrossRef]
- Chen, S.; Aruldass, A.R.; Cardinal, R.N. Mental health outcomes after SARS-CoV-2 vaccination in the United States:A national cross-sectional study. J Affect Disord. 2022, 298(Pt A):396-399.
- Szmyd, B.; Karuga, F.F.; Bartoszek, A.; et al. Attitude and Behaviors towards SARS-CoV-2 Vaccination among Healthcare Workers:A Cross-Sectional Study from Poland. Vaccines (Basel), 2021, 9(3):218.
- Moseholm, E.; Midtgaard, J.; Bollerup, S.; Apol, Á.D.; Olesen, O.B.; Jespersen, S.; Weis, N. Psychological Distress among Hospitalized COVID-19 Patients in Denmark during the First 12 Months of the Pandemic. Int J Environ Res Public Health, 2022, Aug 15; 19(16):10097. [CrossRef]
- Veazie, S.; Lafavor, B.; Vela, K.; Young, S.; Sayer, N.A.; Carlson, K.F.; O’Neil, M.E. Mental Health Outcomes of Adults Hospitalized for COVID-19: A Systematic Review. J. Affect Disord. Rep., 2022, 8, 100312. [CrossRef]
- Mazza, M.G.; Palladini, M.; De Lorenzo, R.; Magnaghi, C.; Poletti, S.; Furlan, R.; Ciceri, F. COVID-19 BioB Outpatient Clinic Study group; Rovere-Querini, P.; Benedetti, F. Persistent psychopathology and neurocognitive impairment in COVID-19 survivors: Effect of inflammatory biomarkers at three-month follow-up. Brain Behav Immun., 2021, May; 94:138-147. [CrossRef]
- Poletti, S.; Vai, B.; Mazza, M.G.; Zanardi, R.; Lorenzi, C.; Calesella, F.; Cazzetta, S.; Branchi, I.; Colombo, C.; Furlan, R.; Benedetti, F. A peripheral inflammatory signature discriminates bipolar from unipolar depression: a machine learning approach. Prog. Neuropsychopharmacol. Biol. Psychiatry, 2020, 105, 110136. [CrossRef]
- Roma, P.; Monaro, M.; Colasanti, M.; et al. A 2-Month Follow-Up Study of Psychological Distress among Italian People during the COVID-19 Lockdown. Int J Environ Res Public Health, 2020, 17(21):8180. [CrossRef]
- Centers for Disease Control and Prevention Investigative Criteria for Suspected Cases of SARS-CoV-2 Reinfection (ICR). Available online: https://stacks.cdc.gov/view/cdc/96072 (accessed on 1 November 2023).
- Flacco, M.E.; Acuti Martellucci, C.; Baccolini, V.; De Vito, C.; Renzi, E.; Villari, P.; Manzoli, L. Risk of reinfection and disease after SARS-CoV-2 primary infection: Meta-analysis. Eur. J. Clin. Investig., 2022, 52:e13845.
- MA, Yi-rui.; DENG, Jie.; LIANG, Wan-nian.; LIU, Min.; LIU, Jue. Meta-analysis of SARS-CoV-2 reinfection rate in the world. CHINESE JOURNAL OF DISEASE CONTROL & PREVENTION, 2023, 27(2): 127-135.
- Bowe, B.; Xie, Y.; Al-Aly, Z. Acute and postacute sequelae associated with SARS-CoV-2 reinfection. Nat. Med., 2022, 28:2398–2405.
- Ren, X.; Zhou, J.; Guo, J.; et al. Reinfection in patients with COVID-19: a systematic review. Glob. health res. policy., 2022, 7, 12. [CrossRef]
Figure 1.
Comparison of Anxiety, Depression, and Stress Scores Across Different Occupational Activities.
Figure 1.
Comparison of Anxiety, Depression, and Stress Scores Across Different Occupational Activities.
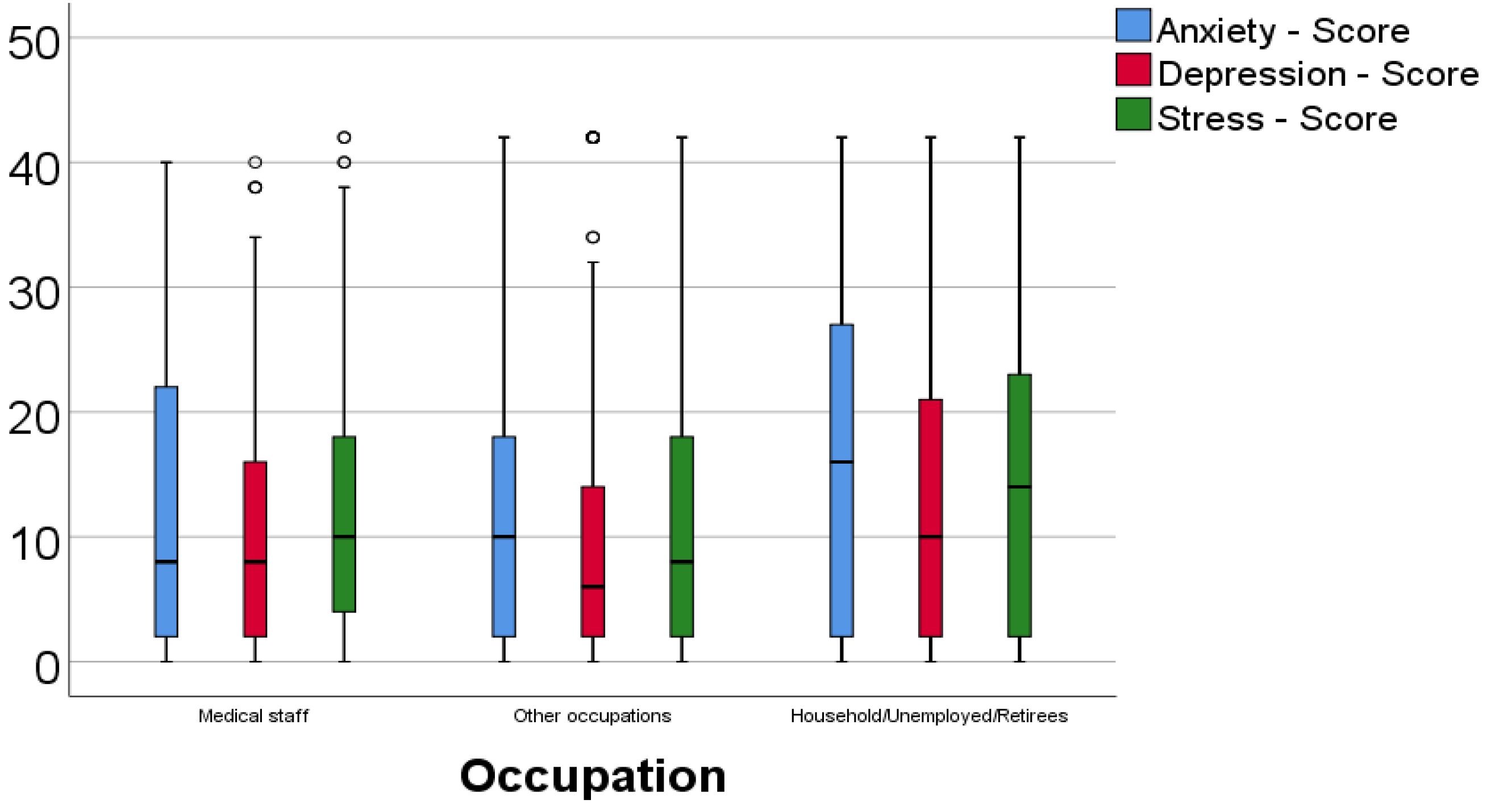
Figure 2.
Analysis of anxiety, depression, and stress scores across different living arrangements.
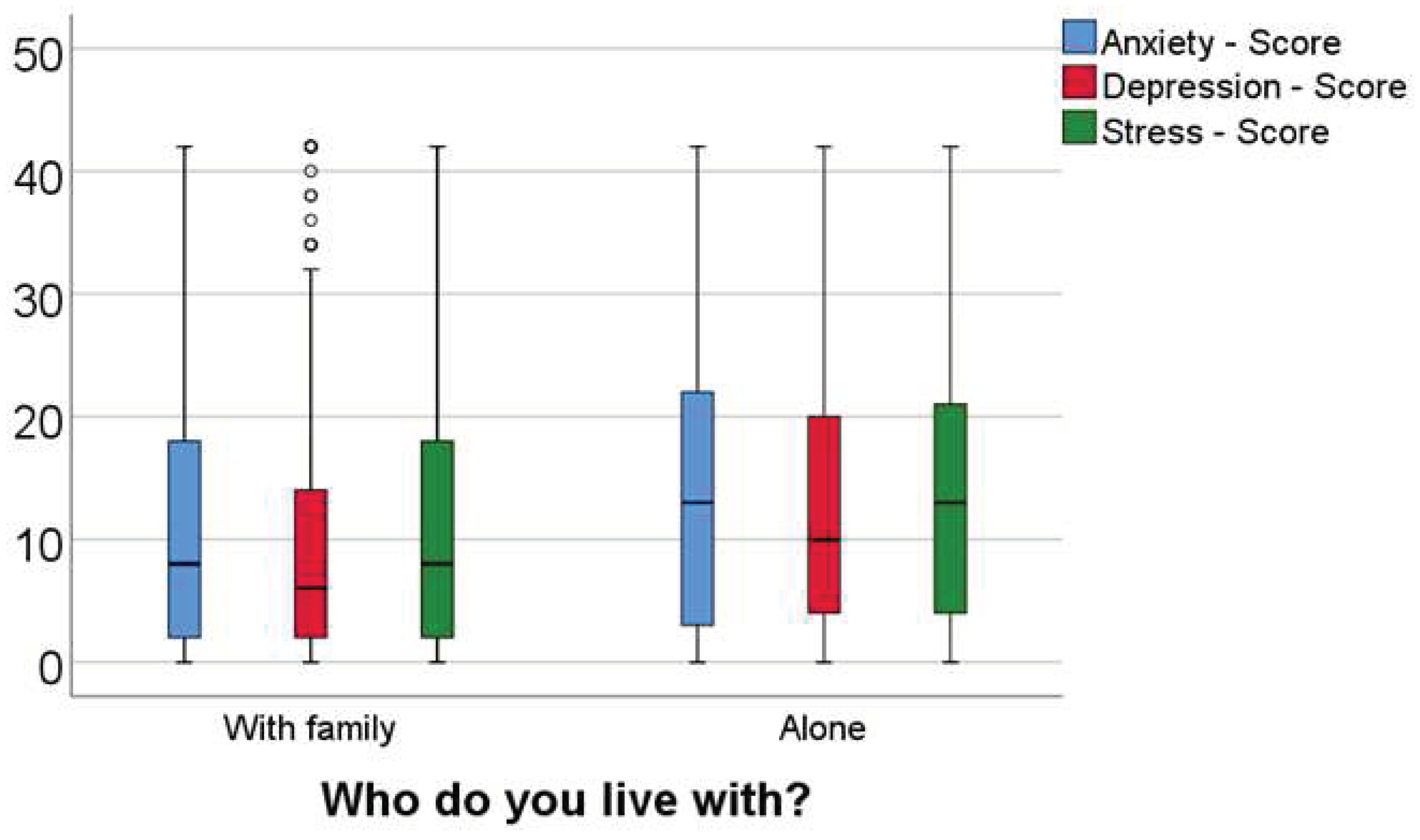
Figure 3.
Comparison of anxiety, depression, and stress scores between the hospitalized groups.
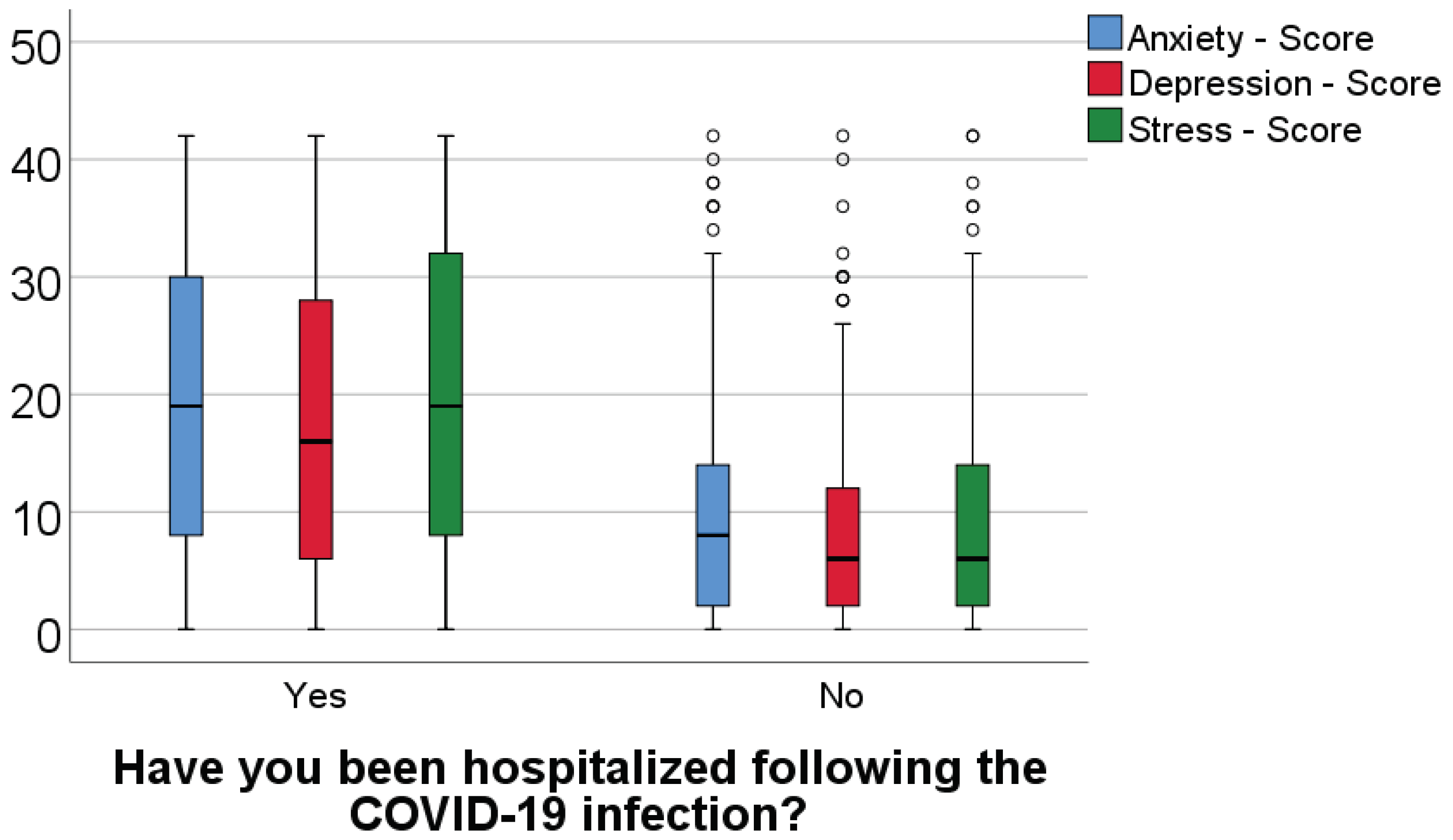

Table 1.
Illustration of the Depression Anxiety Stress Scale (DASS) according to severity [19].
Table 1.
Illustration of the Depression Anxiety Stress Scale (DASS) according to severity [19].
| Severity | Depression | Anxiety | Stress |
|---|---|---|---|
| Normal | 0-9 | 0-7 | 0-14 |
| Mild | 10-13 | 8-9 | 15-18 |
| Moderate | 14-20 | 10-14 | 19-25 |
| Severe | 21-27 | 15-19 | 26-33 |
| Extremely Severe | 28+ | 20+ | 34+ |
Table 2.
Comparison of anxiety, depression, and stress levels between the hospitalized groups.
| HospitalizationAnxiety score | Average ± SD | Median (IQR) | Average rank | p* |
| Present (p<0.001**) | 19.75 ± 13.22 | 19 (8-30) | 345.43 | <0.001 |
| Absent (p<0.001**) | 9.51 ± 9.18 | 8 (2-14) | 226.07 | |
| Hospitalization / Depression score | Average ± SD | Median (IQR) | Average rank | p* |
| Present (p<0.001**) | 18.01 ± 12.94 | 16 (6-28) | 351.07 | <0.001 |
| Absent (p<0.001**) | 7.55 ± 7.83 | 6 (2-12) | 223.78 | |
| Hospitalization / Stress score | Average ± SD | Median (IQR) | Average rank | p* |
| Present (p<0.001**) | 19.85 ± 13.55 | 19 (8-32) | 348.89 | <0.001 |
| Absent (p<0.001**) | 8.93 ± 8.76 | 6 (2-14) | 224.67 |
*Mann-Whitney U Test, **Shapiro-Wilk Test.
Table 3.
Comparison of anxiety, depression, and stress scores between groups with and without reinfection.
Table 3.
Comparison of anxiety, depression, and stress scores between groups with and without reinfection.
| Reinfection / Anxiety score | Average ± SD | Median (IQR) | Average rank | p* |
| Present (p<0.001**) | 16.39 ± 12.75 | 14 (4-26) | 308.51 | 0.001 |
| Absent (p<0.001**) | 11.57 ± 10.97 | 8 (2-18) | 250.13 | |
| Reinfection / Depression score | Average ± SD | Median (IQR) | Average rank | p* |
| Present (p<0.001**) | 15.46 ± 12.07 | 12 (4-24) | 329.52 | <0.001 |
| Absent (p<0.001**) | 9.46 ± 10.02 | 6 (2-14) | 245.32 | |
| Reinfection / Stress score | Average ± SD | Median (IQR) | Average rank | p* |
| Present (p<0.001**) | 16.31 ± 12.75 | 14 (5-24) | 314.79 | <0.001 |
| Absent (p<0.001**) | 11.12 ± 10.95 | 8 (2-18) | 248.69 |
*Mann-Whitney U Test, **Shapiro-Wilk Test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



