
Submitted:
15 February 2024
Posted:
15 February 2024
You are already at the latest version
Abstract
To better understand anogenital warts (AGW) natural history and dynamic of HPV6/11 infection in regional hairs, 32 newly diagnosed AGW male patients and 32 age-matched healthy controls were closely followed. During enrollment and six follow-up visits (every 2.6 months) 43 AGW tissue and 1,232 anogenital and eyebrow hair samples were collected. This represents the closest longitudinal monitoring of AGW patients to date. Patients were treated according to standard-of-care. HPV6/11 prevalence was 19.9% in patients’ hair samples (HPV6 B1 in 87.5%) and 0% in controls. The highest HPV6/11 prevalence was found in pubic hairs (29.0%) and lowest in eyebrows (7.1%). Odds for HPV6/11-positive hairs increased with smoking, shaving anogenital region and age. A close association between HPV6/11 presence in hairs and clinically visible AGW was observed. The proportion of patients with visible AGW and HPV6/11-positive hairs declined during follow-up with similar trends. No particular HPV6/11 variant was linked with increased AGW recurrence, but sublineage HPV6 B1 showed significantly higher clearance from hairs. Despite treatment, 78.1% and 62.5% of AGW patients experienced one and two/more post-initial AGW episodes, respectively. Patients having HPV6/11-positive hairs or visible AGW at preceding visit demonstrated substantially higher odds for presenting with visible AGW in subsequent visit.
Keywords:
human papillomavirus
; HPV
; HPV6
; HPV11
; genetic variants
; anogenital warts
; persistence
; recurrence
; prospective study
1. Introduction
Anogenital warts (AGW) are common benign tumors which typically present as flesh-colored exophytic lesions on the external genitalia. The etiological agents of AGW are human papillomaviruses (HPV), with HPV types 6 and 11 (HPV6/11) causing more than 95% of cases [1,2,3,4,5,6,7,8,9]. AGW frequently recur, but it is not clear whether this is due to inadequacy of treatment or to some particular feature(s) of its causing agents [4,8]. All available AGW treatments are nonspecific and do not eradicate the HPV infection [1,2]. Since lifetime prevalence of AGW is estimated between 4 and 10% [4,10,11,12,13], their recurrences are a considerable healthcare problem and contribute to emotional distress, psychosocial stigma, reduced quality of life, and financial burden [14,15,16,17].
Prior research has suggested that the recurrence of AGW may be attributed to latent HPV infection reservoirs in the surrounding epithelium [18] or in nearby anogenital hair follicles [19]. Furthermore, our pilot cross-sectional study involving 53 male patients revealed that 43.7% of anogenital hair samples from patients with AGW were positive for the presence of Alphapapillomaviruses, which was much higher in comparison to their presence in apparently healthy controls (4.5%) [20]. Notably, in the mentioned pilot study, the HPV types identified in AGW and corresponding hairs were congruent at both HPV type and genomic variant levels [20]. Similar cross-sectional study from China found a higher incidence of HPV infection in pubic hair follicles of patients with AGW compared to healthy men (32.55%, vs. 17.21% respectively), with HPV6 and HPV11 being predominantly identified across both groups [21].
To gain a deeper understanding of AGW natural history and dynamic of HPV6 and HPV11 infection in regional hairs and eyebrows, including follicles, among men with AGW, we conducted a prospective study and longitudinally followed a cohort of 32 male patients newly diagnosed with histologically confirmed AGW (cases) and 32 age-matched healthy male volunteers (controls) for a period of up to two years. We aimed to assess: (i) the duration of AGW clinical presence and HPV dynamic (HPV persistence, clearance and recurrence) in hair samples during the ongoing treatment, (ii) the cross-sectional and longitudinal concordance between HPV types and genomic variants present in AGW and corresponding hair samples, and (iii) whether specific HPV types or genomic variants could be associated with a prolonged persistence or higher AGW recurrence rates. To meet study aims more than 1,200 hair samples as well as 43 AGW tissues were tested for HPV and all HPV positive samples further characterized. With scheduled seven visits and a mean interval of 2.6 months between individual visits, to the best of our knowledge, our study represents the closest longitudinal monitoring of patients with AGW reported to date.
2. Materials and Methods
2.1. Study design
The present prospective longitudinal investigation of HPV infection in male patients with AGW and apparently healthy controls, were conducted at the Department of Dermatovenereology, University Medical Centre Ljubljana, Slovenia, in accordance with the Declaration of Helsinki. Ethical approval for the study was granted by the national Ethics Committee of the Ministry of Health of the Republic of Slovenia (consent reference 120-21/2016/15, date of approval: 17 July 2018). Written informed consent was obtained from all study participants.
The study enrolled a total of 32 patients with newly diagnosed AGW who were monitored across seven visits, scheduled two months apart. The control group comprised 32 age-matched, sexually active healthy male volunteers with no personal history of AGW and no present history of AGW in their current sexual partners. Control subjects were sampled at enrolment and, when possible, at additional time points over the subsequent two-year period.
During each visit, patients underwent a detailed examination for the presence of AGW. Tissue samples were collected from any visible AGW, taking meticulous precautions to prevent cross-contamination between samples, unless the AGW were too small to obtain appropriate samples. Each collected tissue sample was bisected using a scalpel; one half was sent for histopathological confirmation of the clinical diagnosis, while the other half was used for HPV determination.
Additionally, at each visit (at enrolment and six follow-up visits), hair samples, including follicles, were collected from three anogenital sites: pubic, scrotal, and perianal regions as well as eyebrows in both study groups. The sampling was performed by plucking a pool of 3–5 hairs using disposable gloves and sterile tweezers.
After hair sampling, AGW patients received treatment in accordance with standard care protocols, as deemed appropriate by the treating clinician. Treatment options included cryotherapy, electrodessication, local imiquimod, or other topical treatments [22]. Most of participating AGW patients were treated using cryotherapy, since this is a preferred treatment for AGW in Slovenia.
2.2. DNA extraction and HPV testing
Following total DNA extraction, performed using the High Pure PCR Template Preparation Kit (Roche Diagnostics, Mannheim, Germany) [20], samples’ integrity was verified by real-time polymerase chain reaction (RT-PCR), enabling amplification of the 150 bp of the human beta-globin gene [23]. Beta-globin-positive DNA isolates were further tested for the presence of HPV6 and HPV11, using the HPV6/11 real-time polymerase chain reaction (RT-PCR) [24], and HPV6/11-negative samples were further tested for additional HPV types using the conventional GP5+/6+/68 PCR in combination with Sanger sequencing of PCR-products, as described previously [23].
2.3. HPV6 and HPV11 genomic variant characterization
HPV6 and HPV11 variants were determined based on the 960- and 208-bp representative regions for whole-genome-based phylogenetic clustering [25,26], using newly developed type-specific PCRs. The HPV6 type-specific primers (HPV6-961-bp-FW: 5’-CCAGATGTAATTCCTAAGGTG-3’ in combination with HPV6-961-bp-RW: 5’-GACAATGGAACTGTGGTGTTAC-3’ (1,088 bp), and if necessary followed by HPV6-961-bp-FW in combination with HPV6-961-bp-RWs: 5’-TGTCCATAAAAGCCTCATCA-3’ (751 bp) and HPV6-961-bp-FWs: 5’-TTACAATTACATCCTCTGAAACA-3’ in combination with HPV6-961-bp-RW (787 bp)), were designed manually, based on the multiple alignment (mafft v7.453) [27,28] of HPV6 L2 nucleotide sequences of the 48 most diverse complete HPV6 genomes [25]. Similarly, multiple alignment of the target region (partial E2 gene and non-coding region 2) of 78 complete HPV11 genome sequences was used as a base for the design of HPV11 type-specific primers (HPV11-208bp-FW: 5’-TAGCATCTTCAACGTGGCA-3’ and HPV11-208bp-RW: 5’-TGTTAGTACCAGCACAGATGTATAT-3’ (361 bp)). The selected primers’ specificity was subsequently verified using the BLAST (http://blast.ncbi.nlm.nih.gov/Blast.cgi) and MFEprimer-2.0 (http://mfeprimer.com/docs/mfeprimer-2.0/) web-based services. The HPV6/11 viral variant PCRs were performed in a Veriti Thermal Cycler (Thermo Fisher Scientific, Wilmington, DE), using the FastStart High Fidelity PCR system (Roche Diagnostics). Briefly, each reaction mixture contained 1–5 μl of template DNA (tissues up to 100 ng) or 3 μl of outer PCR products in case of HPV6-positive samples with low DNA concentrations, 2.5 μl of 10 × FastStart High Fidelity Reaction Buffer (+ 1,8 mM MgCl2), additional 1,2 mM of MgCl2 stock solution (for outer PCRs), 200μM of dNTPs, 0.5μM of each primer, 1.25 U of FastStart High Fidelity Enzyme Blend, and water up to 25 μl. The cycling conditions were as follows: 2 min at 95°C, followed by 40 cycles of 30 s at 95°C, 30 s at 52°C, 1 min (HPV6)/30 s (HPV11) at 72°C, followed by a final elongation step of 7 min at 72°C, and cooling of the reaction mixture to 4°C. The obtained PCR products were viewed on a 2% agarose gel, Sanger sequenced, and analyzed as described previously [25].
Phylogenetic trees used for the determination of HPV6 and HPV11 genomic variants in newly obtained nucleotide sequences were prepared based on the target nucleotide sequence alignments (mafft v7.453) of reference genomes (HPV6: n=144 [25]; HPV11: n=78; [26]), nucleotide sequences obtained in our previous studies (HPV6: n=15; HPV11: n=9; unpublished data), and isolates obtained in the present study (HPV6: n=28; HPV11: n=3), using the IQtree (2.0-rc1) [29], adopting K3P+R2 and GTR+G+I model parametrizations for HPV6 and HPV11, respectively. Node support values were estimated based on the approximate likelihood ratio (aLRT) [30] and Ultrafast bootstrap (UFBootstrap) [31] methods, with 1,000 iterations, and using the abayes approach [30]. Subsequently, identification and naming of HPV6 and HPV11 genomic variant lineages and sublineages was performed, as described previously [25,26].
2.4. Statistical analysis
Sociodemographic characteristics of study participants were compared using univariate logistic regression. Based on prior experience with similar patient populations, we anticipated irregular attendance and varying intervals between study visits, and adjusted our statistical analysis for this real-life situation by allowing each patient up to two years to complete the seven scheduled study visits.
Recurrence of AGW was defined as the clinical re-emergence of AGW after at least one study visit where the treating physician found no evidence of the disease, and for the analysis of recurrence rates, we only considered the time frame for which data was available for all patients.
Likelihood ratio test examined the link between HPV types and AGW recurrence, and agreement between presence of HPV in AGW and hair samples was calculated as the proportion of patients that had each HPV lineage or sublineage present or absent in both types of samples. McNemar test evaluated HPV6 and HPV11 lineage consistency in AGW and hair samples. Mixed effect logistic regression model analyzed the clearance rate of HPV, considering time and hair sampling area, and association between patients’ age, smoking, shaving of the anogenital area. A significance level of 0.05 was used, and analyses were conducted using SPSS version 26.
3. Results
3.1. Characteristics of study participants and follow-up visits
All enrolled 32 AGW patients, aged 17–66 (mean 30.8) years, completed seven visits with a mean 2.6-month interval between two visits and a total follow-up duration of 11–25.1 months (mean follow-up 15.6 months). The 32 enrolled controls aged 21–52 (mean 30.7) years, had a mean 2.6 visits, mean 4.5-month interval between two visits and a total follow-up duration was 0–21.9 months (mean follow-up 7.3 months). Most participants were heterosexual, in stable relationships, with <11 lifetime sexual partners. No significant sociodemographic or sexual behavior differences were noted between AGW patients and controls (Table 1). However, significant difference in partner AGW history was reported (P < 0.001), as 15.6% (5/32) of patients' partners experienced AGW and 21.9% (7/32) were unsure if they had them, while not a single control had partners with AGW. In addition, more patients than controls had or were unsure about current sexually transmitted infections (two patients reported genital herpes, and one chlamydial urethritis).
3.2. HPV infection in anogenital warts and corresponding hair samples
A total of 43 DNA samples were obtained from AGW tissue: 32 at baseline and 11 during follow-up visits. Additionally, DNA was extracted from total of 1,232 collected hair samples: 896 from patients and 336 from controls. All samples tested beta-globin gene.
As shown in Table 2, all 32 baseline AGW samples exhibited a single Alphapapillomavirus infection, among which 31/32 (96.9%) tested positive for HPV6 or HPV11, while one sample was positive for HPV40. The most frequently observed HPV lineage among HPV6-positive samples was HPV6 B, with the dominant sublineage being HPV6 B1 (Table 2). All HPV11-positive AGWs contained sublineage HPV11 A2. No cases of HPV6 sublineages B4, B5, or HPV11 sublineage A1 were found (Table 2).
Among all 896 hair samples collected from AGW patients during enrollment and six follow-up visits, a total of 178 (19.9%) hair samples tested positive for HPV6 or HPV11. At least one HPV6/11-positive hair sample was identified in 31/32 (96.8%) of patients with AGW, with a mean of 5.6 HPV6/11-positive hair samples per patient. As shown in Figure 1, the highest prevalence of HPV6/11 was found in pubic hair samples (29.0%; 65/224), followed by perianal hair samples (23.7%; 53/224), scrotal hair samples (19.6%; 44/224), and eyebrow hair samples (7.1%; 16/224).
In contrast to patients with AGW, not a single out of 336 hair samples collected from controls tested HPV6/11 positive.
Out of 118 visits at which patients presented with clinically visible AGW, in 89 (75.4%) visits at least one HPV6/11-positive hair sample was found at the same visit. In contrast, out of 100 visits when patients had no clinically visible AGW, only in 8 (8.0%) visits patients had HPV6/11-positive hair sample(s) (P < 0.0001).
The proportion of agreement between the presence or absence of HPV6/11, their lineages and sublineages in AGW and corresponding hairs, in total exceeded 92%. 100% agreement was found in patients with HPV6 A, HPV6 B2, and HPV6 B3 sublineages, 96.6% in patients with HPV11 and HPV6 B, 96.3% in patients with HPV6 B1 and 90.6% overall in patients with HPV 6. However, all recorded differences were not statistically significant.
3.3. Dynamic of HPV6/11 infection in hair samples
Five out of 32 patients (15.6%) presented with AGW only at the baseline visit. In addition to presenting with AGW on the baseline visit, seven (21.9%) and 20 (62.5%) patients presented with clinically visible AGW at one, and two or more follow-up visits, respectively.
As shown in Table 3, when analyzing pairs of two consecutive visits for presence of AGW in relation to AGW and HPV6/11 status in hair samples at the preceding visit, among the 96/186 pairs of visits when any of the patient’s hair samples tested positive or negative for HPV6/11, 70 (37.6%) and 19 (10.2%) of cases had clinically visible AGW at their subsequent visit, respectively. A similar pattern was observed with AGW presence at two consecutive visits, with 73/185 (39.5%) of cases with and 12 (6.5%) without AGW also had AGW at their subsequent visit, respectively. Both associations are highly statistically significant (P < 0.0001) (Table 3).
Out of the 26/32 patients whose hair samples were initially positive for HPV6/11, 6 (23.1%) remained positive after 11 months (Table 4). At the 11-month mark, significant reductions in the proportion of HPV6/11-positive hair samples were observed for HPV6 (P = 0.001), HPV6 lineage B (P = 0.001), and HPV6 sublineage B1 (P = 0.003).
As shown in Figure 2, the proportion of patients with clinically visible AGW and HPV6/11-positive hair samples decreased over the course of follow-up visits. Despite fluctuating intervals between visits, we observed similar decreasing trends in the presence of clinically visible AGW and HPV6/11-positive hair samples, the decreasing trends seem to be similar for all four hair sampling areas. The likelihood of detecting HPV6/11 in hair samples decreased over time (OR, 0.82 [95% CI, 0.76–0.89], P < 0.001). For patients who initially had HPV6-positive AGW, compared to other two HPV types (HPV11 and HPV40), no significant differences in the rate of HPV6/11-negative final hair samples were found (OR, 1.05 [95% CI, 0.10–11.08], P = 0.97).
Results of mixed effect logistic regression model showed that interaction between time (measured as continuous variable in months to accommodate unequal time spacing per subject between visits) and hair sampling was not statistically significant. As shown in Table 5, the odds for HPV6/11 positive sample from eyebrows were statistically significantly lower in comparison to other hair sampling areas (P = 0.034). The odds for HPV positive hair sample significantly decreased through time (P = 0.007) (Table 6).
Another mixed effect logistic regression model with random intercept was built from which interaction effect of time of follow-up and hair sample area was omitted and fixed effects of age, smoking and shaving of the anogenital region were added (Table 6). Beside follow-up time and hair sampling area, also patients’ age, smoking and shaving of the anogenital region were statistically significantly associated with HPV6/11 positivity. As shown in Table 6, the odds for HPV6/11 positive hair samples increased with patients’ age at enrolment (P < 0.001), smoking status (P = 0.002) and shaving of the anogenital region (P = 0.022).

Table 5.
Association between patients’ age at enrolment, smoking, shaving of the anogenital area, and presence of HPV6/11 in collected hairs. Lifestyle factors included participant’s age at the enrolment, smoking status and shaving of the anogenital region.
Table 5.
Association between patients’ age at enrolment, smoking, shaving of the anogenital area, and presence of HPV6/11 in collected hairs. Lifestyle factors included participant’s age at the enrolment, smoking status and shaving of the anogenital region.
| Hair sampling area/age/lifestyle factors | OR (95% CI) | P |
| Perianal hairs | 1 | |
| Eyebrow hairs | 0.17 (0.08–0.34) | < 0.001 |
| Pubic hairs | 1.42 (0.68–2.98) | 0.354 |
| Scrotal hairs | 0.71 (0.37–1.34) | 0.29 |
| Follow-up time | 0.84 (0.78–0.91) | < 0.001 |
| Patients’ age at enrolment | 1.06 (1.04–1.08) | < 0.001 |
| Non-cigarette smoking | 1 | |
| Cigarette smoking | 3.04 (1.49–6.22) | 0.002 |
| Shaving – no | 1 | |
| Shaving – yes | 2.34 (1.13–4.82) | 0.022 |
Abbreviations: OR, odds ratio; 95% CI, 95% confidence interval; P, p value; statistically significant associations (P < 0.05) are shown in bold.
3.4. Recurrence of anogenital warts
Out of 32 AGW patients enrolled, two had missing data on AGW presence on some of the intermediate study visits and were excluded from the analysis of AGW recurrence. Of the remaining 30 patients, eight (26.7%) experienced AGW recurrence, defined as reappearance of AGW following at least one visit when no AGW were clinically apparent. As shown in Table 7, no significant differences were found in AGW recurrence rates across any of the HPV6 and HPV11 lineages and sublineages (P > 0.05).
4. Discussion
In the present prospective study of dynamic of HPV6/11 infection in plucked anogenital and eyebrow hair samples obtained from 32 men with AGW undergoing treatment and tightly followed for up to two years, a close association was seen between the presence of HPV6/11 in hair samples and clinically visible AGW. The proportion of patients with clinically visible AGW and HPV6/11-positive hairs declined over the course of follow-up with similar trends and no particular HPV6/11 genomic variant was linked with increased AGW recurrence rate; however, sublineage HPV6 B1 showed significantly higher clearance rate from hair samples.
All, but one baseline AGW samples tested positive for HPV6/11 (31/32, 96.9%), with the predominance of single HPV6 B1 infections, accounting for 87.5% of the cases. Previous research also reported the predominance of sublineage HPV6 B1 in European populations and its close association with anogenital infections [25,32,33]. Only a minor fraction (9.4%) of our patients were infected with the sublineage HPV11 A2, which is generally the most commonly detected genomic variant among HPV11 infections worldwide [26,32,34]. In addition, HPV40, commonly detected in AGW as a HPV6/11 co-infection [7], was detected in this study in a single AGW patient as the only HPV type present.
The predominance of HPV6 B1 infections in our study population prompts further investigation into evolutionary advantages that this sublineage may possess over other HPV6 genomic variants, as suggested recently [33,35,36]. The HIM (“HPV infection in men”) study, large prospective study of the natural history of HPV infections in men in three countries (United States, Mexico and Brazil), also found increased risk of AGW development associated with HPV6 B1 genital infections compared to sublineage HPV6 B3 [33]. Additionally, the transcriptional activity of HPV6 B1 long control region (LCR) reference variant was found to be approximately 11 times more active than the HPV6 B3 LCR reference variant [35]. These findings suggest that HPV6 B1 may persist longer as a subclinical infection, thereby contributing to an elevated risk of AGW development. In contrast, the genomic variability of HPV11 appears to be more conserved [26] and less understood, possibly due to substantially fewer HPV11 genomes sequenced from AGW [34,37].
In this study, there was a high level of agreement (>90%) between HPV6/11 presence or absence as well as presence of particular HPV lineage and sublineage in AGW and corresponding hair samples, suggesting that the identical HPV genomic variant is responsible for HPV persistence in hair samples and subsequent AGW development. These observations are consistent with findings of our pilot cross-sectional study [20] and align with the outcomes of the above mentioned HIM study which demonstrated that a genital swab collected prior to the appearance of clinically visible AGW harbored the identical HPV6 or HPV11 genomic variant as detected in the subsequently developed AGW lesion [33,34].
In the present study, overall prevalence of HPV6/11 infection in 896 hair samples collected from AGW patients during enrollment and six follow-up visits was 19.9% and out of 336 hair samples collected from controls not a single specimen tested HPV6/11 positive. The latter finding contrasts with previously reported "background" HPV6/11 prevalence in hair samples of apparently healthy “controls”, which ranged from 1.3% to 16.4% [20,21]. Similarly, a 10.4% prevalence of HPV6/11 in subjects without AGW was found by thorough swabbing anogenital surfaces in the HIM study [38]. The discrepancy in findings could be due to variations in study populations (MSM/MSWM versus MSW), sampling techniques (hairs versus thorough swabbing of wide anogenital area), anti-contamination measures used during sampling, DNA extraction and PCR testing as well as HPV detection methodologies employed.
Some previous studies labeled hair plucking samples as "hair follicles” [19,21]. However, such samples include extrafollicular hair shaft segments, potentially carrying HPV DNA from adjacent skin or lesions, therefore it is difficult to determine whether positive HPV results are solely from the hair follicle or surface contamination of the hair. Therefore, in line with our previous work [20], we refer to such samples as "hair samples" rather than "hair follicles." Plucked hair may contain intrafollicular HPV, undetectable by swabbing, however this seems unlikely in productive low-risk HPV infection as intrafollicular keratinocytes are shed outside of the follicle along the growing hair shaft. In addition, swabbing is less discomforting for the patient and allows sampling of a larger area. This advantage might make swabbing a preferred method in clinical and research settings, balancing scientific accuracy with patient comfort.
Odds for HPV6/11-positive hair samples in our study increased with two previously established risk factors for genital HPV infection: smoking and shaving of the anogenital region [39], as well as with the patients’ age. The significance of the latter remains to be clarified as it was previously found that although the burden of genital HPV infections in men remains constant throughout their lifespan, older men achieve the clearance of infection faster [40] and less likely develop AGW after newly acquired HPV infection [41,42].
This study outlines the anatomical distribution of HPV6/11 in hair samples, predominantly in the pubic region as a more reliable site for HPV6/11 detection, then the perianal area, scrotum, and eyebrows, similar to our previous findings [20]. Additionally, the significantly lower HPV6/11 detection rate in eyebrow hair aligns with the higher susceptibility of anogenital hairs to HPV, given their close proximity to the highly infectious surface of AGW [19,20,43].
Our patients exhibiting HPV6/11-positive hair samples or clinically visible AGW at preceding visit demonstrated substantially increased odds (10- and 11-fold respectively, P < 0.0001 for both) of presenting with clinically visible AGW in subsequent visits. Interestingly, similar odds were also observed in the HIM study, where HPV-positive men without prevalent AGW were nearly 12 times more likely to develop AGW compared to their HPV-negative counterparts [41]. These findings suggest similar predictive value of hair sampling, skin swabbing, and historical data of AGW in forecasting future AGW development. The correlation between AGW and presence of HPV6/11 in hair samples is further underscored by observation that over 95% of our patients had at least one HPV6/11-positive hair sample; in contrast, no HPV6/11 infections were detected in hair samples obtained from control subjects.
A high share of our 32 patients had more than one AGW episode (defined as a study visit with clinically visible AGW), as 25 (78.1%) and 20 (62.5%) experienced one, and two or more post-initial AGW episodes, respectively. This is substantially more frequent that reported in the HIM study where only 44% of men had more than one post-initial AGW episode recorded [44]. The most likely explanation for the observed difference is substantially closer longitudinal monitoring of our patients e.g. every 2.6 months (mean) compared to every 6 months in the HIM study. Also, the number of AGW episodes in men undergoing treatment might differ by the standard of care used. In the HIM study, a smaller proportion of men from Brazil experienced multiple AGW events compared to men residing in Mexico and the United States, and this might be partially due to different standards of care used: in Brazil, excision is the preferred treatment modality, compared with topical treatment in Mexico and the United States [44]. In Slovenia, the preferred treatment for newly diagnosed AGW is cryotherapy which was also used in most of our patients.
In this study, AGW recurrence after no visible AGW for at least two months of follow-up was found in 33.3% of patients, reflecting a common proportion of AGW recurrences in other studies [45,46]. No association were found between infection with particular HPV6/11 genomic variant and AGW recurrence, probably due to the predominance of a single HPV6 genomic variant (sublineage HPV6 B1) and possibly due to limited number of participants.
Our AGW patients and healthy controls significantly differed in two previously identified risk factors for anogenital HPV infection. More AGW patients than controls reported current STDs or uncertainty about their STD status, and a higher incidence of AGW in their sexual partners, emphasizing the importance of their thorough assessment in clinical settings. Interestingly, some of our patients reported current chlamydial infection and genital herpes, which were also associated with prevalent HPV infection in the HIM study [47].
Our study has strengths and limitations. The key strength of our study is its prospective design with very frequent patient monitoring, enabling a deeper and more detailed insight into the dynamic (HPV persistence, clearance and recurrence) of HPV6/11 infections and their correlation with AGW. With a mean interval of 2.6 months between patient visits, to the best of our knowledge, our study represents, by far, the closest longitudinal monitoring of patients with AGW reported to date. Another strength of our study is that in contrast to other similar studies, clinical diagnosis of AGW was confirmed in all patients by histological assessment to ensure accurate diagnosis and to avoid the issue of misidentifying other benign skin lesions as AGW [48]. Additionally, when defining HPV type that causes AGW, HPV detection was performed in AGW tissue specimens and not from e.g. AGW surface smears as in great majority of previous studies. Our approach provides more precise assessment of the HPV type etiologically linked to AGW since it allows differentiation between wart-causing HPV types and those only colonizing the skin surface, which may not have clinical significance [49,50].
The main limitations of our study are relatively small number of patients enrolled and non-equal intervals between study visits which potentially restricted the study's power to investigate in more detail association(s) between specific HPV6/11 genomic variant(s) and AGW recurrence rates. Further, since our study was conducted only on males, the results cannot be generalized to female patients and/or other populations.
5. Conclusions
To provide better understanding of AGW natural history and dynamic of HPV6 and HPV11 infection in anogenital hairs and eyebrows we longitudinally followed a cohort of 32 male patients newly diagnosed with AGW and the same number of age-matched healthy male volunteers for up to two years. All AGW tissue specimens were HPV positive, with sublineage HPV6 B1 causing 87.5% of the cases. In addition to AGW tissues, 1,232 hair samples were prospectively collected. Overall HPV6/11 prevalence in 896 hair samples collected from AGW patients was 19.9% while not a single hair sample from controls (336 hair samples) tested HPV6/11 positive. With a mean of 5.6 HPV6/11-positive hair samples per patient, the highest HPV6/11 prevalence was found in pubic hair samples (29.0%) and lowest in eyebrows (7.1%). Odds for HPV6/11-positive hair samples increased with smoking, shaving of the anogenital region and with the patients’ age. Our study, which represents the closest longitudinal monitoring of patients with AGW reported to date, showed a close association between the presence of HPV6/11 in hair samples and clinically visible AGW. The proportion of patients with clinically visible AGW and HPV6/11-positive hairs declined over the course of six follow-up visits with similar trends. Patients having HPV6/11-positive hairs or clinically visible AGW at preceding visit demonstrated substantially increased odds (10- and 11-fold, respectively) of presenting with clinically visible AGW in subsequent visit. No particular HPV6/11 genomic variant was linked with increased AGW recurrences rate, but sublineage HPV6 B1 showed significantly higher clearance rate from hair samples. Due to very close patient’s monitoring (7 visits every 2.6 months) we demonstrated that despite treatment (mainly cryotherapy) over 78% and over 62% of patients with newly diagnosed AGW experience one and two or more post-initial AGW episodes, respectively, which is substantially more frequent than previously reported in the peer-reviewed literature. Our findings underscore the need for further research to provide more comprehensive understanding of the dynamic of HPV6/11 anogenital infections and natural history of AGW, to raise public awareness about AGW and provide free access to gender-neutral HPV vaccination and vaccination across wider age groups.
Author Contributions
V.T is the lead author. M.Polj. is the corresponding author. V.T. conceptualized and designed the study, participated in data acquisition, interpreted data, searched the literature, and drafted the manuscript. L.H. participated in laboratory analyses, provided expertise in interpreting microbiological data, interpreted the data, and drafted the manuscript. M.K., T.M.Z., and K.S. participated in data acquisition and laboratory analyses, provided expertise in interpreting microbiological data, and reviewed the manuscript. B.L. performed histopathological assessment, and reviewed the manuscript. M.Pot. and J.M. supervised the study, and reviewed the manuscript. M.Polj. conceptualized, designed and supervised the study, interpreted data, provided expertise in interpreting microbiological data, and drafted the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Institute of Microbiology and Immunology, Faculty of Medicine, University of Ljubljana and the Slovenian Research and Innovation Agency ARIS (grant number P3-00083).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the national Ethics Committee of the Ministry of Health of the Republic of Slovenia (consent reference 120-21/2016/15, date of approval: 17 July 2018). .
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The vast majority of generated data are presented in the manuscript. Further data generated in this study are available on request from the corresponding author.
Acknowledgments
The authors would like to express their sincere gratitude to all patients with AGW and healthy volunteers for the participation in the study and to Vanja Ida Erčulj from Faculty of Criminal Justice and Security, University of Maribor, Ljubljana, Slovenia for her help with statistical analyses.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lacey, C.J.; Lowndes, C.M.; Shah, K.V. Chapter 4: Burden and management of non-cancerous HPV-related conditions: HPV-6/11 disease. Vaccine 2006, 24, 35–41. [Google Scholar] [CrossRef]
- Potočnik, M.; Kocjan, B.; Seme, K.; Poljak, M. Distribution of human papillomavirus (HPV) genotypes in genital warts from males in Slovenia. Acta Dermatovenerol. Alp. Pannonica Adriat. 2007, 16, 91–96. [Google Scholar]
- Bouvard, V.; Baan, R.; Straif, K.; Grosse, Y.; Secretan, B.; El Ghissassi, F.; Benbrahim-Tallaa, L.; Guha, N.; Freeman, C.; Galichet, L.; et al.; WHO International Agency for Research on Cancer Monograph Working Group. A review of human carcinogens--Part B: biological agents. Lancet Oncol. 2009, 10, 321–322. [CrossRef]
- Garland, S.M.; Steben, M.; Sings, H.L.; James, M.; Lu, S.; Railkar, R.; Barr, E.; Haupt, R.M.; Joura, E.A. Natural history of genital warts: analysis of the placebo arm of 2 randomized phase III trials of a quadrivalent human papillomavirus (types 6, 11, 16, and 18) vaccine. J. Infect. Dis. 2009, 199, 805–814. [Google Scholar] [CrossRef] [PubMed]
- Ball, S.L.; Winder, D.M.; Vaughan, K.; Hanna, N.; Levy, J.; Sterling, J.C.; Stanley, M.A.; Goon, P.K. Analyses of human papillomavirus genotypes and viral loads in anogenital warts. J. Med. Virol. 2011, 83, 1345–1350. [Google Scholar] [CrossRef] [PubMed]
- Forman, D.; de Martel, C.; Lacey, C.J.; Soerjomataram, I.; Lortet-Tieulent, J.; Bruni, L.; Vignat, J.; Ferlay, J.; Bray, F.; Plummer, M.; et al. Global burden of human papillomavirus and related diseases. Vaccine 2012, 30, F12–F23. [Google Scholar] [CrossRef] [PubMed]
- Komloš, K.F.; Kocjan, B.J.; Košorok, P.; Luzar, B.; Meglič, L.; Potočnik, M.; Hočevar-Boltežar, I.; Gale, N.; Seme, K.; Poljak, M. Tumor-specific and gender-specific pre-vaccination distribution of human papillomavirus types 6 and 11 in anogenital warts and laryngeal papillomas: a study on 574 tissue specimens. J. Med. Virol. 2012, 84, 1233–1241. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.R.; Nyitray, A.G.; Kreimer, A.R.; Pierce Campbell, C.M.; Goodman, M.T.; Sudenga, S.L.; Monsonego, J.; Franceschi, S. EUROGIN 2014 roadmap: differences in human papillomavirus infection natural history, transmission and human papillomavirus-related cancer incidence by gender and anatomic site of infection. Int. J. Cancer 2015, 136, 2752–2760. [Google Scholar] [CrossRef] [PubMed]
- Patel, C.; Brotherton, J.M.; Pillsbury, A.; Jayasinghe, S.; Donovan, B.; Macartney, K.; Marshall, H. The impact of 10 years of human papillomavirus (HPV) vaccination in Australia: what additional disease burden will a nonavalent vaccine prevent? Euro Surveill. 2018, 23, 1700737. [Google Scholar] [CrossRef]
- Grulich, A.E.; de Visser, R.O.; Smith, A.M.; Rissel, C.E.; Richters, J. Sex in Australia: sexually transmissible infection and blood-borne virus history in a representative sample of adults. Aust. N. Z. J. Public Health 2003, 27, 234–241. [Google Scholar] [CrossRef]
- Kjaer, S.K.; Tran, T.N.; Sparen, P.; Tryggvadottir, L.; Munk, C.; Dasbach, E.; Liaw, K.L.; Nygård, J.; Nygård, M. The burden of genital warts: a study of nearly 70,000 women from the general female population in the 4 Nordic countries. J. Infect. Dis. 2007, 196, 10, 1447–1454. [Google Scholar] [CrossRef]
- Dinh, T.H.; Sternberg, M.; Dunne, E.F.; Markowitz, L.E. Genital warts among 18- to 59-year-olds in the United States, national health and nutrition examination survey, 1999--2004. Sex. Transm. Dis. 2008, 35, 357–360. [Google Scholar] [CrossRef]
- Munk, C.; Nielsen, A.; Liaw, K.L.; Kjaer, S.K. Genital warts in men: a large population-based cross-sectional survey of Danish men. Sex. Transm. Infect. 2012, 88, 640–644. [Google Scholar] [CrossRef]
- Jeynes, C.; Chung, M.C.; Challenor, R. 'Shame on you'--the psychosocial impact of genital warts. Int. J. STD. AIDS 2009, 20, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Lee Mortensen, G.; Larsen, H.K. Quality of life of homosexual males with genital warts: a qualitative study. BMC Res. Notes 2010, 4, 280. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, J.; Pista, A.; Lisboa, C.; Santo, I.; Azevedo, L.; Cunha, M.J.; HERCOLES Study Group. Epidemiology of human papillomavirus on anogenital warts in Portugal - The HERCOLES study. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1342–1348. [CrossRef]
- O'Mahony, C.; Gomberg, M.; Skerlev, M.; Alraddadi, A.; de Las Heras-Alonso, M.E.; Majewski, S.; Nicolaidou, E.; Serdaroğlu, S.; Kutlubay, Z.; Tawara, M.; et al. Position statement for the diagnosis and management of anogenital warts. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 1006–1019. [Google Scholar] [CrossRef] [PubMed]
- Ferenczy, A.; Mitao, M.; Nagai, N.; Silverstein, S.J.; Crum, C.P. Latent papillomavirus and recurring genital warts. N. Engl. J. Med. 1985, 313, 784–788. [Google Scholar] [CrossRef]
- Boxman, I.L.; Hogewoning, A.; Mulder, L.H.; Bouwes Bavinck, J.N.; ter Schegget, J. Detection of human papillomavirus types 6 and 11 in pubic and perianal hair from patients with genital warts. J. Clin. Microbiol. 1999, 37, 2270–2273. [Google Scholar] [CrossRef] [PubMed]
- Poljak, M.; Kocjan, B.J.; Potocnik, M.; Seme, K. Anogenital hairs are an important reservoir of alpha-papillomaviruses in patients with genital warts. J. Infect. Dis. 2009, 199, 1270–1274. [Google Scholar] [CrossRef]
- Wang, Y.B.; Han, T.; Zhao, C.X. [Prevalence of human papillomavirus in the pubic hair follicles of healthy men and male patients with genital warts]. Zhonghua Nan. Ke. Xue. 2010, 16, 783–785. Chinese.
- Lacey, C.J.; Woodhall, S.C.; Wikstrom, A.; Ross, J. 2012 European guideline for the management of anogenital warts. J. Eur. Acad. Dermatol. Venereol. 2013, 27, e263–e270. [Google Scholar] [CrossRef] [PubMed]
- Mlakar, J.; Kocjan, B.J.; Hošnjak, L.; Pižem, J.; Beltram, M.; Gale, N.; Drnovšek-Olup, B.; Poljak, M. Morphological characteristics of conjunctival squamous papillomas in relation to human papillomavirus infection. Br. J. Ophthalmol. 2015, 99, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Kocjan, B.J.; Seme, K.; Poljak, M. Detection and differentiation of human papillomavirus genotypes HPV-6 and HPV-11 by FRET-based real-time PCR. J. Virol. Methods 2008, 153, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Jelen, M.M.; Chen, Z.; Kocjan, B.J.; Burt, F.J.; Chan, P.K.; Chouhy, D.; Combrinck, C.E.; Coutlée, F.; Estrade, C.; Ferenczy, A.; et al. Global genomic diversity of human papillomavirus 6 based on 724 isolates and 190 complete genome sequences. J. Virol. 2014, 88, 7307–7316. [Google Scholar] [CrossRef]
- Jelen, M.M.; Chen, Z.; Kocjan, B.J.; Hošnjak, L.; Burt, F.J.; Chan, P.K.S.; Chouhy, D.; Combrinck, C.E.; Estrade, C.; Fiander, A.; et al. Global Genomic Diversity of Human Papillomavirus 11 Based on 433 Isolates and 78 Complete Genome Sequences. J. Virol. 2016, 90, 5503–5513. [Google Scholar] [CrossRef]
- Katoh, K.; Misawa, K.; Kuma, K.; Miyata, T. MAFFT: a novel method for rapid multiple sequence alignment based on fast Fourier transform. Nucleic Acids Res. 2002, 30, 3059–3066. [Google Scholar] [CrossRef]
- Katoh, K.; Standley, D.M. MAFFT multiple sequence alignment software version 7: improvements in performance and usability. Mol. Biol. Evol. 2013, 30, 772–780. [Google Scholar] [CrossRef]
- Nguyen, L.T.; Schmidt, H.A.; von Haeseler, A.; Minh, B.Q. IQ-TREE: a fast and effective stochastic algorithm for estimating maximum-likelihood phylogenies. Mol. Biol. Evol. 2015, 32, 268–274. [Google Scholar] [CrossRef]
- Anisimova, M.; Gil, M.; Dufayard, J.F.; Dessimoz, C.; Gascuel, O. Survey of branch support methods demonstrates accuracy, power, and robustness of fast likelihood-based approximation schemes. Syst. Biol. 2011, 60, 685–699. [Google Scholar] [CrossRef]
- Hoang, D.T.; Chernomor, O.; von Haeseler, A.; Minh, B.Q.; Vinh, L.S. UFBoot2: Improving the Ultrafast Bootstrap Approximation. Mol. Biol. Evol. 2018, 35, 518–522. [Google Scholar] [CrossRef]
- Danielewski, J.A.; Garland, S.M.; McCloskey, J.; Hillman, R.J.; Tabrizi, S.N. Human papillomavirus type 6 and 11 genetic variants found in 71 oral and anogenital epithelial samples from Australia. PLoS One 2013, 8, e63892. [Google Scholar] [CrossRef]
- Flores-Díaz, E.; Sereday, K.A.; Ferreira, S.; Sirak, B.; Sobrinho, J.S.; Baggio, M.L.; Galan, L.; Silva, R.C.; Lazcano-Ponce, E.; Giuliano, A.R.; et al.; HIM Study group. HPV-6 Molecular Variants Association With the Development of Genital Warts in Men: The HIM Study. J. Infect. Dis. 2017, 215, 559–565. [CrossRef]
- Flores-Díaz, E.; Sereday, K.A.; Ferreira, S.; Sirak, B.; Sobrinho, J.S.; Baggio, M.L.; Galan, L.; Silva, R.C.; Lazcano-Ponce, E.; Giuliano, A.R.; et al; The Him Study Group. HPV-11 variability, persistence and progression to genital warts in men: the HIM study. J. Gen. Virol. 2017, 98, 2339–2342. [CrossRef]
- Measso do Bonfim, C.; Simão Sobrinho, J.; Lacerda Nogueira, R.; Salgado Kupper, D.; Cardoso Pereira Valera, F.; Lacerda Nogueira, M.; Villa, L.L.; Rahal, P.; Sichero, L. Differences in Transcriptional Activity of Human Papillomavirus Type 6 Molecular Variants in Recurrent Respiratory Papillomatosis. PLoS One 2015, 10, e0132325. [Google Scholar] [CrossRef]
- Szinai, M.; Nagy, Z.; Máté, P.; Kovács, D.; Laczkó, L.; Kardos, G.; Sápy, T.; Szűcs, A.; Szarka, K. Comparative analysis of human papillomavirus type 6 complete genomes originated from head and neck and anogenital disorders. Infect. Genet. Evol. 2019, 71, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Steben, M.; Garland, S.M. Genital warts. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 1063–1073. [Google Scholar] [CrossRef] [PubMed]
- Giuliano, A.R.; Lazcano-Ponce, E.; Villa, L.L.; Flores, R.; Salmeron, J.; Lee, J.H.; Papenfuss, M.R.; Abrahamsen, M.; Jolles, E.; Nielson, C.M.; el, al. The human papillomavirus infection in men study: human papillomavirus prevalence and type distribution among men residing in Brazil, Mexico, and the United States. Cancer Epidemiol. Biomarkers Prev. 2008, 17, 2036–2043. [Google Scholar] [CrossRef] [PubMed]
- Schabath, M.B.; Villa, L.L.; Lin, H.Y.; Fulp, W.J.; Lazcano-Ponce, E.; Salmerón, J.; Abrahamsen, M.E.; Papenfuss, M.R.; Quiterio, M.; Giuliano, A.R. A prospective analysis of smoking and human papillomavirus infection among men in the HPV in Men Study. Int. J. Cancer 2014, 134, 2448–2457. [Google Scholar] [CrossRef] [PubMed]
- Ingles, D.J.; Lin, H.Y.; Fulp, W.J.; Sudenga, S.L.; Lu, B.; Schabath, M.B.; Papenfuss, M.R.; Abrahamsen, M.E.; Salmeron, J.; Villa, L.L.; et al. An analysis of HPV infection incidence and clearance by genotype and age in men: The HPV Infection in Men (HIM) Study. Papillomavirus Res. 2015, 1, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Anic, G.M.; Lee, J.H.; Villa, L.L.; Lazcano-Ponce, E.; Gage, C.; José C Silva, R.; Baggio, M.L.; Quiterio, M.; Salmerón, J.; Papenfuss, M.R.; et al. Risk factors for incident condyloma in a multinational cohort of men: the HIM study. J. Infect. Dis. 2012, 205, 789–793. [Google Scholar] [CrossRef] [PubMed]
- Sudenga, S.L.; Ingles, D.J.; Pierce Campbell, C.M.; Lin, H.Y.; Fulp, W.J.; Messina, J.L.; Stoler, M.H.; Abrahamsen, M.; Villa, L.L.; Lazcano-Ponce, E.; et al. Genital Human Papillomavirus Infection Progression to External Genital Lesions: The HIM Study. Eur. Urol. 2016, 166–173. [Google Scholar] [CrossRef]
- Kocjan, B.J.; Poljak, M.; Seme, K.; Potocnik, M.; Fujs, K.; Babic, D.Z. Distribution of human papillomavirus genotypes in plucked eyebrow hairs from Slovenian males with genital warts. Infect. Genet. Evol. 2005, 5, 255–259. [Google Scholar] [CrossRef]
- Giuliano, A.R.; Sirak, B.; Abrahamsen, M.; Silva, R.J.C.; Baggio, M.L.; Galan, L.; Cintra, R.C.; Lazcano-Ponce, E.; Villa, L.L. Genital Wart Recurrence Among Men Residing in Brazil, Mexico, and the United States. J. Infect. Dis. 2019, 219, 703–710. [Google Scholar] [CrossRef]
- Pamnani, S.J.; Sudenga, S.L.; Rollison, D.E.; Ingles, D.J.; Abrahamsen, M.; Villa, L.L.; Lazcano-Ponce, E.; Huang, Y.; Borenstein, A.; Giuliano, A.R. Recurrence of Genital Infections With 9 Human Papillomavirus (HPV) Vaccine Types (6, 11, 16, 18, 31, 33, 45, 52, and 58) Among Men in the HPV Infection in Men (HIM) Study. J. Infect. Dis. 2018, 218, 1219–1227. [Google Scholar] [CrossRef]
- Widschwendter, A.; Böttcher, B.; Riedl, D.; Coban, S.; Mutz-Dehbalaie, I.; Matteucci Gothe, R.; Ciresa-König, A.; Marth, C.; Fessler, S. Recurrence of genitals warts in pre-HPV vaccine era after laser treatment. Arch. Gynecol. Obstet. 2019, 300, 661–668. [Google Scholar] [CrossRef]
- Alberts, C.J.; Schim van der Loeff, M.F.; Papenfuss, M.R.; da Silva, R.J.; Villa, L.L.; Lazcano-Ponce, E.; Nyitray, A.G.; Giuliano, A.R. Association of Chlamydia trachomatis infection and herpes simplex virus type 2 serostatus with genital human papillomavirus infection in men: the HPV in men study. Sex. Transm. Dis. 2013, 40, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Trčko, K.; Hošnjak, L.; Kušar, B.; Zorec, T.M.; Kocjan, B.J.; Križmarić, M.; Seme, K.; Miljković, J.; Luzar, B.; Poljak, M. Clinical, histopathological, and virological evaluation of 203 patients with a clinical diagnosis of molluscum contagiosum. Open Forum Infect. Dis. 2018, 5, ofy298. [Google Scholar] [CrossRef]
- Anic, G.M.; Messina, J.L.; Stoler, M.H.; Rollison, D.E. , Stockwell, H., Villa, L.L., Lazcano-Ponce, E., Gage, C., Silva, R.J., Baggio, M.L.; et al. Concordance of human papillomavirus types detected on the surface and in the tissue of genital lesions in men. J. Med. Virol. 2013, 85, 1561–1566. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, M.G.; Winder, D.M.; Ball, S.L.; Vaughan, K.; Sonnex, C.; Stanley, M.A.; Sterling, J.C.; Goon, P.K. Detection of specific HPV subtypes responsible for the pathogenesis of condylomata acuminata. Virol. J. 2013, 10, 137. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Proportions of HPV6/11-positive hair samples in 32 patients with anogenital warts, collected over the course of the seven study visits (at enrollment and six follow-up visits), by sampling location (eyebrow hairs, pubic hairs, scrotal hairs, and perianal hairs), n = 224 for each sampling area; n = 896 total number of tested hair samples.
Figure 1.
Proportions of HPV6/11-positive hair samples in 32 patients with anogenital warts, collected over the course of the seven study visits (at enrollment and six follow-up visits), by sampling location (eyebrow hairs, pubic hairs, scrotal hairs, and perianal hairs), n = 224 for each sampling area; n = 896 total number of tested hair samples.
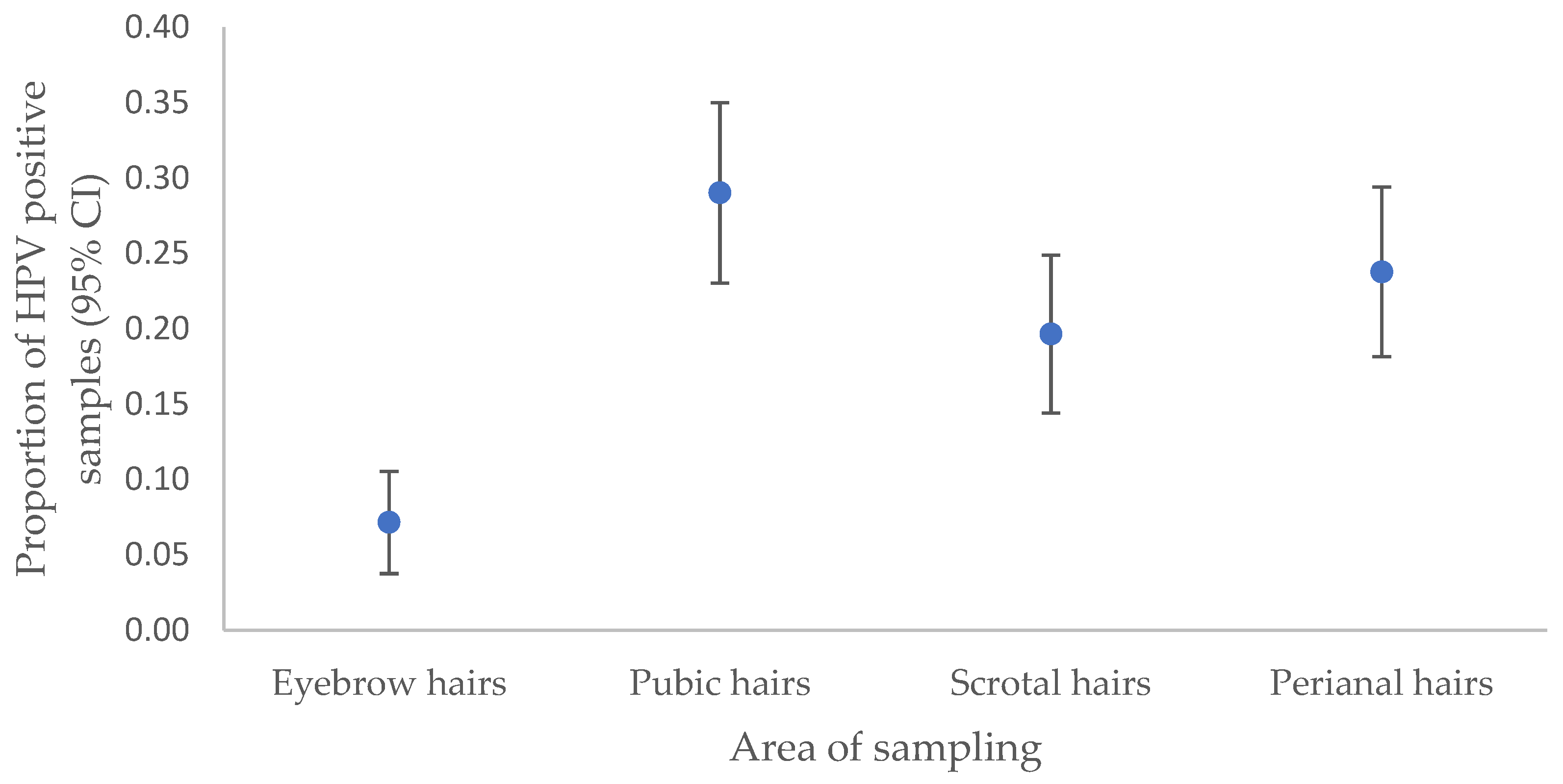
Figure 2.
Presence of clinically visible anogenital warts (AGW) and HPV6/11 positivity rate in collected hair samples through time: at enrolment (visit 1) and during six follow-up visits (visits 2-7). AGW: proportion of patients with clinically visible AGW during particular visit; Any hair sample: proportion of patients with any HPV positive hair sample collected during particular visit; Pubic hairs, Scrotal hairs, Perianal hairs, Eyebrow hairs: proportion of patients with HPV positive hair sample collected from certain collection site during particular visit. Precautions should be taken when interpreting the graph as the time intervals between visits overall and per patient were unequal.
Figure 2.
Presence of clinically visible anogenital warts (AGW) and HPV6/11 positivity rate in collected hair samples through time: at enrolment (visit 1) and during six follow-up visits (visits 2-7). AGW: proportion of patients with clinically visible AGW during particular visit; Any hair sample: proportion of patients with any HPV positive hair sample collected during particular visit; Pubic hairs, Scrotal hairs, Perianal hairs, Eyebrow hairs: proportion of patients with HPV positive hair sample collected from certain collection site during particular visit. Precautions should be taken when interpreting the graph as the time intervals between visits overall and per patient were unequal.
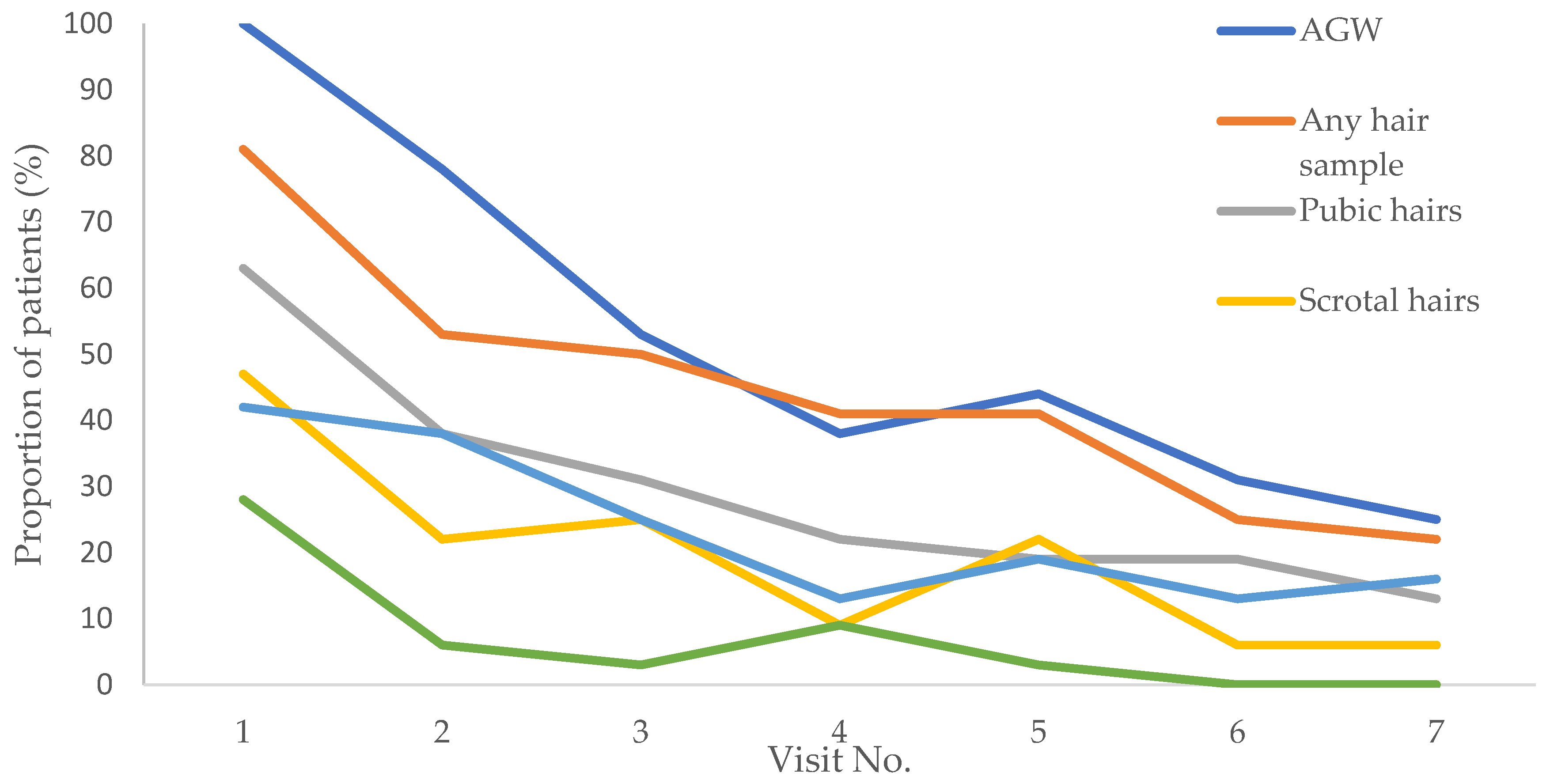
Table 1.
Sociodemographic characteristics and risk factors for anogenital HPV infection in patients with anogenital warts and controls.
Table 1.
Sociodemographic characteristics and risk factors for anogenital HPV infection in patients with anogenital warts and controls.
| Controls (n=32) | Patients (n=32) | OR (95%CI) | P | |
|---|---|---|---|---|
| Mean age (years) ± SD | 30.7± 8 | 30.8± 10 | 1 (0.9; 1.1) | 0.955 |
| ≥14 years of education | 12 (37.5) | 13 (40.6) | 1.1 (0.4; 3.1) | 0.798 |
| Currently employed | 21 (65.6) | 20 (62.5) | 0.9 (0.3; 2.4) | 0.795 |
| Marital status | ||||
| Married | 7 (21.9) | 4 (12.5) | 1 | |
| Cohabiting | 10 (31.3) | 15 (46.9) | 2.6 (0.6; 11.4) | 0.197 |
| Single | 15 (46.9) | 13 (40.6) | 1.5 (0.4; 6.4) | 0.570 |
| Cigarette smoking | 14 (43.8) | 19 (59.4) | 1.9 (0.7; 5.1) | 0.213 |
| History of skin disease | ||||
| No | 20 (62.5) | 15 (46.9) | 1 | |
| Yes | 7 (21.9) | 14 (43.8) | 2.7 (0.9; 8.2) | 0.088 |
| Unsure | 5 (15.6) | 3 (9.4) | 0.8 (0.2; 3.9) | 0.782 |
| Current STI other than AGW | 0.034* | |||
| No | 29 (90.6) | 22 (68.8) | ||
| Yes | 0 | 3 (9.4) | ||
| Unsure | 3 (9.4) | 7 (21.9) | ||
| Past STIb | 0.329 | |||
| No | 30 (93.8) | 27 (84.4) | ||
| Yes | 2 (6.3) | 4 (12.5) | ||
| Unsure | 0 | 1 (3.1) | ||
| Ever tested for STI | 8 (25) | 8 (25) | 1 (0.3; 3.1) | 1 |
| Mean age at first sexual intercourse (years) ± SD | 17.2 ± 2.2 | 17.7 ± 2 | 1.1 (0.9; 1.4) | 0.373 |
| Currently sexually active | 26 (81.3) | 23 (71.9) | 0.6 (0.2; 1.9) | 0.379 |
| Partners with present history of AGW | ||||
| No | 32 (100) | 20 (62.5) | <0.001* | |
| Yes | 0 | 5 (15.6) | ||
| Unsure | 0 | 7 (21.9) | ||
| Lifetime No. of sexual partners | ||||
| 1 | 6 (18.8) | 3 (9.4) | 1 | |
| <5 | 6 (18.8) | 8 (25) | 2.7 (0.5; 15.3) | 0.270 |
| 6–10 | 9 (28.1) | 10 (31.3) | 2.2 (0.4; 11.6) | 0.344 |
| >10 | 11 (34.4) | 11 (34.4) | 2 (0.4; 10.1) | 0.401 |
| No. of sexual partners in the past year | 0.202* | |||
| 0 | 0 | 3 (9.4) | ||
| 1 | 22 (68.8) | 18 (56.3) | ||
| 1–5 | 8 (25) | 9 (28.1) | ||
| >5 | 2 (6.3) | 2 (6.3) | ||
| Sexual orientation | 0.220* | |||
| MSW | 30 (93.7) | 27 (84.4) | ||
| MSM | 2 (6.3) | 3 (9.4) | ||
| MSWM | 0 | 2 (6.3) | ||
| Condom use | ||||
| Never | 4 (12.5) | 4 (12.5) | 1 | |
| Occasionally | 22 (68.8) | 24 (75) | 1.1 (0.2; 4.9) | 0.910 |
| Always | 6 (18.8) | 4 (12.5) | 0.7 (0.1; 4.4) | 0.672 |
| Circumcised | 2 (6.7) | 8 (25) | 4.7 (0.9; 24.1) | 0.066 |
| Shaving of anogenital region | 18 (58.1) | 18 (56.3) | 0.9 (0.3; 2.5) | 0.884 |
Data are presented as n (%) unless otherwise indicated. Abbreviations: OR, odds ratio; 95% CI, 95% confidence interval; P, p value; SD, standard deviation; AGW, anogenital warts; STI, sexually transmitted infection; MSW, men who have sex only with women, MSM, men who have sex only with men; MSWM, men who have sex with women and men; *likelihood ratio test. Statistically significant associations (P < 0.05) are shown in bold.
Table 2.
Distribution of HPV types, lineages and sublineages in baseline anogenital wart tissue samples of the 32 patients.
Table 2.
Distribution of HPV types, lineages and sublineages in baseline anogenital wart tissue samples of the 32 patients.
| HPV type, lineage and sublineage | No. (%) of samples |
|---|---|
| HPV6 | 28 (87.5) |
| HPV6 A* | 2 (7.1) |
| HPV6 B | 26 (92.9) |
| HPV6 B1 | 17 (65.4) |
| HPV6 B2 | 5 (19.2) |
| HPV6 B3 HPV6 B untypable |
2 (7.7) 2 (7.7) |
|
HPV11 HPV11A2 |
3 (9.4) 3 (100.0) |
| HPV40 | 1 (3.1) |
*HPV6 sublineage could not be determined in both HPV6 lineage A positive samples.
Table 3.
Presence of clinically visible anogenital warts (AGW) in relation to HPV6/11 in hair samples and AGW at the preceding visit. For AGW vs. HPV in hair samples at the preceding visit, n = 186. For AGW vs. AGW at the preceding visit, n = 185.
Table 3.
Presence of clinically visible anogenital warts (AGW) in relation to HPV6/11 in hair samples and AGW at the preceding visit. For AGW vs. HPV in hair samples at the preceding visit, n = 186. For AGW vs. AGW at the preceding visit, n = 185.
| Previous visit | AGW | OR (95% CI) | P | |||
|---|---|---|---|---|---|---|
| YES | NO | |||||
| n | % | n | % | |||
| Hairs YES | 70 | 37.6% | 26 | 14.0% | 10.06 (5.11–19.8) | <0.0001 |
| Hairs NO | 19 | 10.2% | 71 | 38.2% | ||
| AGW YES | 73 | 39.5% | 35 | 18.9% | 11.30 (5.41–23.58) | <0.0001 |
| AGW NO | 12 | 6.5% | 65 | 35.1% | ||
Abbreviations: OR, odds ratio; 95% CI, 95% confidence interval; P, p-value; Hairs YES, HPV6/11 detected in at least one hair sample at the preceding visit; Hair NO, no HPV6/11 detected in hair at the preceding visit; AGW YES, presence of clinically visible AGW at the preceding visit; AGW NO, no clinically visible AGW at the preceding visit; statistically significant associations (P < 0.05) are shown in bold.
Table 4.
The number and proportion (%) of participants with HPV infection in hair samples by HPV lineage at enrollment in the study and after 11 months of follow-up.
Table 4.
The number and proportion (%) of participants with HPV infection in hair samples by HPV lineage at enrollment in the study and after 11 months of follow-up.
| Baseline | After 11 months* | P | ||
|---|---|---|---|---|
| No | Yes | |||
| HPV6 | No | 5 (62.5) | 3 (37.5) | 0.001 |
| Yes | 19 (79.2) | 5 (20.8) | ||
| HPV 6 A | No | 29 (100) | 0 (0) | 0.48 |
| Yes | 2 (100) | 0 (0) | ||
| HPV 6 B | No | 7 (77.8) | 2 (22.2) | 0.001 |
| Yes | 17 (77.3) | 5 (22.7) | ||
| HPV 6 B1 | No | 13 (92.9) | 1 (7.1) | 0.003 |
| Yes | 12 (80) | 3 (20) | ||
| HPV 6 B2 | No | 25 (96.2) | 1 (3.8) | 1 |
| Yes | 1 (33.3) | 2 (66.7) | ||
| HPV 6 B3 | No | 27 (100) | 0 (0) | 0.48 |
| Yes | 2 (100) | 0 (0) | ||
| HPV 11 A2 | No | 30 (100) | 0 (0) | 1 |
| Yes | 1 (50) | 1 (50) | ||
*Due to unequal time intervals between patient follow-up visits, the cross-sectional time point was analyzed for which follow-up data were available for all 32 unrolled patients with AGW (11 months); statistically significant associations (P < 0.05) are shown in bold.
Table 5.
Association between follow-up time, hair sampling area, their interaction, and HPV positivity (results of mixed model logistic regression analysis).
Table 5.
Association between follow-up time, hair sampling area, their interaction, and HPV positivity (results of mixed model logistic regression analysis).
| Hair sampling area/follow-up time | OR (95% CI) | P |
|---|---|---|
| Perianal region | 1 | |
| Eyebrows | 0.36 (0.14; 0.92) | 0.034 |
| Pubis | 1.48 (0.68; 3.25) | 0.324 |
| Scrotum | 0.83 (0.38; 1.82) | 0.634 |
| Follow-up time | 0.86 (0.78; 0.96) | 0.007 |
| Perianal region | 1 | |
| Eyebrows | 0.81 (0.65; 1.00) | 0.055 |
| Pubis | 0.99 (0.89; 1.11) | 0.874 |
| Scrotum | 0.97 (0.88; 1.07) | 0.566 |
Abbreviations: OR, odds ratio; 95% CI, 95% confidence interval; P, p value; statistically significant associations (P < 0.05) are shown in bold. .
Table 7.
Anogenital wart recurrences (AGW), by HPV lineages and sublineages.
| HPV type, lineage and sublineage |
AGW recurrence | P | ||
|---|---|---|---|---|
| No (n (%)) | Yes (n (%)) | |||
| HPV6 | No | 1 (4.5) | 0 (0) | 0.425 |
| Yes | 21 (95.5) | 8 (100) | ||
| HPV6 A | No | 18 (90.0) | 7 (100) | 0.263 |
| Yes | 2 (10.0) | 0 (0) | ||
| HPV6 B | No | 3 (15.0) | 0 (0) | 0.165 |
| Yes | 17 (85.0) | 7 (100) | ||
| HPV6 B1 | No | 8 (42.1) | 2 (33.3) | 0.700 |
| Yes | 11 (57.9) | 4 (66.7) | ||
| HPV6 B2 | No | 16 (84.2) | 4 (66.7) | 0.369 |
| Yes | 3 (15.8) | 2 (33.3) | ||
| HPV6 B3 | No | 17 (89.5) | 6 (100) | 0.283 |
| Yes | 2 (10.5) | 0 (0) | ||
| HPV11 A2* | No | 20 (90.9) | 7 (87.5) | 0.787 |
| Yes | 2 (9.1) | 1 (12.5) | ||
| HPV40** | Yes | 1 (100) | 0 (0) | – |
*All HPV11 positive AGW samples harbored sublineage HPV11 A2. **Since only a single AGW patient tested HPV40 positive, the association between the presence of this HPV type and AGW recurrence was not tested.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



