
Submitted:
15 February 2024
Posted:
16 February 2024
You are already at the latest version
Abstract
(1) Background: Sleep disordered breathing represent a growing public health concern, especially among children and adolescents. Full-night polysomnography is considered the gold standard for diagnosing obstructive sleep apnea. Our goals are to identify personal and environmental risk factors for the onset and persistence of sleep respiratory disorders. We also want to investigate the differences in neuropsychological profiles; (2) Methods: This is an observational, retrospective cohort study. We collected information on adenoidectomy or adenotonsillectomy. We reviewed the clinical history and preoperative visits and collected data through a telephone questionnaire. Pediatric Sleep Questionnaire (PSQ) and the Pediatric Quality of Life Inventory (PedsQL) are questionnaires used for screening sleep respiratory disorders in children. The data were statistically analyzed it using SPSS version 22.0 for Windows (SPSS Inc., Chicago, IL); (3) Results: The study involved 138 patients, but only 100 parents participated. A higher percentage of patients with sleep disordered breathing were observed to have mothers who smoked during pregnancy. A smaller proportion of patients with sleep disordered breathing had a habit of using a pacifier. A rise in physical results is associated with a reduction in the PSQ at follow-up (p=0.051). An increase of overall academic achievement is associated with an average decrease in the PSQ at follow-up (p<0.0001). A more significant proportion of patients undergoing adenotonsillectomy were observed to have a history of prematurity and cesarean birth (4) Conclusions: These results provide essential information on the effectiveness and effects of adenotonsillectomy intervention compared to adenoidectomy intervention and the factors associated with SDB in children undergoing these interventions.
Keywords:
adenoidectomy
; adenotonsillectomy
; breastfeeding
; children
; obstructive sleep apnea
; quality of life
; Pediatric Sleep Questionnaire
; sleep-disordered breathing
1. Introduction
Sleep-disordered breathing (SDB) is becoming an increasingly common public health problem, especially among children and adolescents [1,2]. Pediatric SDB is associated with various complications, including growth deficits [3], neurocognitive problems [4], metabolic alterations [5], cardiovascular disorders [6], and impairment of quality of life (QoL) [7,8]. The primary treatment for SDB is adenoidectomy, with or without tonsillectomy [9]. Some studies have suggested that combined adenoidectomy and antibiotic therapy may be more effective than adenoidectomy alone [4,10,11,12]. The American Academy of Pediatrics and the American Academy of Otolaryngology-Head and Neck Surgery recommend adenotonsillectomy (A&T) as an intervention to treat obstructive sleep apnea syndrome (OSAS) in children over two years of age [1,2]. The SDB is associated with various complications, including growth deficits [13], neurocognitive issues [4], metabolic alterations [14], cardiovascular disorders [6], and compromise of quality of life (QoL) in both children [15,16] and adults [17]. Il trattamento primario per il SDB è l’adenoidectomia, con o senza tonsillectomia [9]. Alcuni studi hanno suggerito che l’adenoidectomia combinata e la terapia antibiotica possono essere più efficaci della sola adenoidectomia [4,10,11,12]. The American Academy of Pediatrics and the American Academy of Otolaryngology-Head and Neck Surgery recommend A&T as an intervention to treat obstructive sleep apnea syndrome (OSAS) in children over two years of age [18,19].
The main indications for ENT surgery are tonsillar and adenoidal hypertrophy, which can cause SDB, as well as recurrent tonsillitis, recurrent otitis, and secondary hearing loss [19,20,21]. A meta-analysis has shown improved quality of life in patients who underwent A&T [16]. However, not all patients benefit from surgery; in some cases, OSAS may persist [20].
In pediatric patients, the Pediatric Sleep Questionnaire (PSQ) is one of the questionnaires that can be used for screening SDB [22,23]. Full overnight polysomnography (PSG) is considered the reference method for diagnosing obstructive sleep apnea (OSA) [24]. Evaluating the effect of surgery on the quality of life of patients with SDB can provide helpful information for identifying risk factors and improving patient management for this condition. The Pediatric Quality of Life Inventory (PedsQL), which measures health-related quality of life in pediatric populations, can be applied in clinical practice [25].
The main objective of this study is to thoroughly investigate and analyze a myriad of risk factors and protective elements in children with SDB compared to those without SDB after ENT surgery.
2. Materials and Methods
Study Design
This is a retrospective observational cohort study involving 138 children aged 2 to 11 years who were initially recruited from the Pediatric Sleep Disorders Outpatient Clinic and underwent tonsillectomy or A&T at the Otorhinolaryngology Unit of the Hospital of Verona in Italy between November 2018 and December 2021. Clinical information was collected through two methods: first, by consulting medical records, and subsequently, by conducting telephone interviews with the parents/caregivers of children who had previously undergone ENT surgery. In our study, we considered a wide range of factors, including predictive elements of SDB development and potential consequences of the condition. We acknowledge that certain factors, such as birth weight, gender, and maternal smoking, may indeed influence the risk of SDB, while also considering factors that could be affected or modified in the presence of such disorders. The Ethics Committee approved the protocol for clinical studies in the provinces of Verona and Rovigo at the Integrated University Hospital (3766CESC). All parents/caregivers provided informed consent for the scientific use of the data.
Medical Records
ENT characteristics before surgery.
In our comprehensive analysis of medical records, historical data, and preoperative visits, we meticulously compiled the following essential information:
1. Historical cases of recurrent tonsillitis, with tonsil classification based on estimation using the Brodsky scale. Tonsillar hypertrophy was explicitly defined as grades III and IV [18].
2. Adenoidal hypertrophy.
3. History of recurrent ear infections and/or hearing loss.
4. Diagnosis of hearing loss, carefully assessed through clinical presentations and audiometric tests. Pathological conditions were identified using type B and C tympanograms.
5. Antibiotic therapy undertaken as a treatment for recurrent tonsillitis before surgery was considered.
6. Preoperative PSG was conducted to evaluate sleep-related issues, mainly snoring, sleep apnea, and noisy breathing. In cases where PSG was unavailable, these symptoms were recorded in medical records and classified as SDB or OSA.
The motivation for the surgery was classified into four main groups:
(I) Tonsillar and adenoidal hypertrophy, carefully assessed through comprehensive preoperative physical examinations.
(II) Documented history of recurrent adenoiditis or tonsillitis.
(III) History of recurrent middle ear infections and hearing loss.
(IV) Evidence of SDB or OSA, either instrumental or clinical.
Respiratory polysomnography
During the overnight assessment, limited-channel polysomnography (PSG) was conducted using a portable ambulatory device (SOMNOscreen PSG, developed by SOMNOmedics GmbH in Randersacker, Germany). This advanced device continuously monitored various key physiological parameters relevant to sleep-related studies. These parameters included nasal airflow, thoracic and abdominal respiratory movements (measured using thoracic and abdominal belts), arterial oxygen saturation (SpO2), heart rate (measured via a finger probe), electrocardiogram (ECG), body position (measured via a mercury sensor), and tracheal sounds (recorded through a microphone) [26].
The device was affixed to the participant between 9:00 PM and 8:00 AM, capturing data throughout the night while the individual remained comfortably at home. The recorded data underwent manual and automatic evaluations to ensure a comprehensive analysis. The DOMINO software, specifically SOMNOmedics v.2.6.0, was used for automated analysis. Additionally, experienced technicians manually reviewed the data to obtain accurate results. Respiratory events were assessed following the guidelines provided by the American Academy of Sleep Medicine (AASM), as described in the study of Marcus, Brooks et al. (2012) [10].
To assess the severity of OSA, the total number of obstructive apneas, mixed apneas, and hypopneas was calculated and then divided by the real estimated sleep time per hour. This calculation provided the Obstructive Apnea-Hypopnea Index (oAHI), expressed as the number of events per hour. Desaturation was considered if there was a minimum 3% decrease in oxygen levels. All oxygen desaturations (SpO2) were quantified relative to the baseline SpO2 (%) mean and minimum SpO2 (%). The Oxygen Desaturation Index (ODI) was determined by dividing the total desaturations by the full estimated sleep time per hour. This metric provided additional information about the severity and frequency of oxygen level fluctuations during sleep.
Questionnaire at follow-up
The telephone questionnaire was divided into three sections: 1) questions about general and perinatal history, 2) administration of the PSQ; and 3) PedsQL—physical and school domains.
Anamnestic information
The first part of the questionnaire consisted of general questions regarding the perinatal period. In particular, the following information was investigated: birth weight and length, gestational age [26], and pacifier use. Participants were divided into those who did not use a pacifier or used it for less than two years compared to those who maintained the habit longer [27]. Other information included active maternal smoking during pregnancy, atopy, malocclusion, and neuropsychiatric disorders. Information regarding COVID-19 infection (symptomatic or asymptomatic) was also collected. Parameters at follow-up included the child’s weight, height, and BMI.
Pediatric Sleep Questionnaire (PSQ)
The Pediatric Sleep Questionnaire (PSQ) is a comprehensive tool consisting of 22 questions regarding various aspects of sleep problems in children, including snoring frequency, loud snoring, observed apneas, breathing difficulties during sleep, daytime sleepiness, distractible or hyperactive behaviour, and other common symptoms associated with pediatric OSAS. These questions can be methodically divided into three distinct groups, namely nighttime symptoms, daytime symptoms, and cognitive symptoms. The PSQ facilitates the identification of potential cases of pediatric OSAS through careful assessment of these symptoms.
Each question within the PSQ requires responses in the form of “yes,” “no,” or “don’t know,” reflecting the participant’s perception of the child’s sleep-related experiences. Consequently, the total score is calculated by dividing the sum of positive responses (yes) by the total number of reactions, excluding those “don’t know.” This standardized approach ensures a fair and accurate representation of the child’s sleep-related problems.
As a result, the derived total score ranges from 0 to 1, with a critical cutoff point of 0.33 used to distinguish patients exhibiting OSAS symptoms from those who do not. This established threshold has been validated and endorsed by Chervin et al. (2000) [23].
It is important to note that the PSQ has garnered considerable recognition for its high diagnostic value in effectively screening patients suspected of having OSAS. Its ability to comprehensively assess various aspects of sleep disorders, combined with the reliability of the calculated total score, confirms its utility as a robust screening tool [27,28,29].
Questionnaire on quality of life in children (PedsQL)
The PedsQL 4.0 Generic Core Scales is a comprehensive questionnaire to assess Health-Related Quality of Life (HRQOL) in children and adolescents aged 2 to 18. This instrument consists of 23 questions divided into four distinct domains. The assessment involves two parallel versions of the questionnaire, one to be completed by the child and the other by the parent or primary caregiver.
Each question asks participants to rate the frequency of occurrence of a specific problem over the past month on a scale from 0 to 4. These ratings reflect the perceived impact of various health-related aspects on the child’s life. The sum of all scores obtained for each question is divided by the total number of responses given to get the final score. This systematic approach ensures a comprehensive and reliable assessment of the child’s HRQOL across the specified domains. [30].
It is essential to emphasize that in cases where more than 50% of responses are missing or not provided by the participant, the overall score cannot be accurately calculated.
Statistical Analysis
The statistical analysis described focuses on exploring differences in the percentage distributions of categorical variables among different groups of patients. The chi-square test was used for categorical variables. The percentages of patients with defined categorical variables within the PSQ- and PSQ+ groups are compared. Additionally, the percentages of patients with defined categorical variables between the Ad and A&T patient groups are compared.
Statistical analysis of continuous variables in the PSQ- and PSQ+ patient groups is performed. The mean and standard deviation (S.D.) are provided for each group, along with 98% confidence intervals (C.I. 98%) for the mean. Furthermore, the result of the Mann-Whitney test, including the associated p-value, is reported.
Multiple linear regression analysis is conducted. In this analysis, the dependent variable is the percentage of PSQ% at follow-up, including the independent variables (or predictors). For each independent variable, several parameters are provided T, indicating the value of the estimated coefficient for each independent variable in the regression; Standard Error, meaning the standard error of the estimated coefficient; Beta, representing the standardized beta coefficient, indicating how much the dependent variable changes in terms of standard deviations when the independent variable increases by one standard deviation; t, representing the t-value, which is the ratio of the estimated coefficient to the standard error of the coefficient; and P, indicating the associated p-value for each independent variable, i.e., the statistical significance of the variable’s effect on the dependent variable; the 95% C.I. for B, representing the 95% confidence interval for the estimated coefficient of the independent variable.
A value of P < 0.05 was considered statistically significant for all tests employed. However, we acknowledge that the P-value in our study may be influenced by factors such as the small sample size, risk of bias, and random error. Therefore, we will also consider statistical significance with a P-value between 0.05 and 0.1, providing a reasonable explanation for this value and other evidence supporting the relationship [31].
The data were recorded in a Microsoft® Excel® database for Windows 11 and statistically analyzed using SPSS version 22.0 for Windows (SPSS Inc., Chicago, IL).
3. Results
Out of the 138 enrolled patients (65% male), 100 parents participated in the study. Therefore, 38 patients (27.5%) declined to participate in the survey or were not contacted and were thus excluded from the analysis. Peri/postoperative complications were observed in 5 children who experienced issues such as coughing, bleeding, or incomplete adenoid removal after surgery.
Figure 1.
(panel A) displays the percentage of patients for each categorical variable included in the PSQ- (orange bars; n=76) and PSQ+ (green bars; n=24) categories. Legend: PSQ, paediatric sleep questionnaire; SDB, sleep-disordered breathing. (panel B) illustrates the percentage of patients for each categorical variable included in the adenoidectomy (grey bars; n=61) and adenotonsillectomy (blue bars; n=39) categories.
Figure 1.
(panel A) displays the percentage of patients for each categorical variable included in the PSQ- (orange bars; n=76) and PSQ+ (green bars; n=24) categories. Legend: PSQ, paediatric sleep questionnaire; SDB, sleep-disordered breathing. (panel B) illustrates the percentage of patients for each categorical variable included in the adenoidectomy (grey bars; n=61) and adenotonsillectomy (blue bars; n=39) categories.
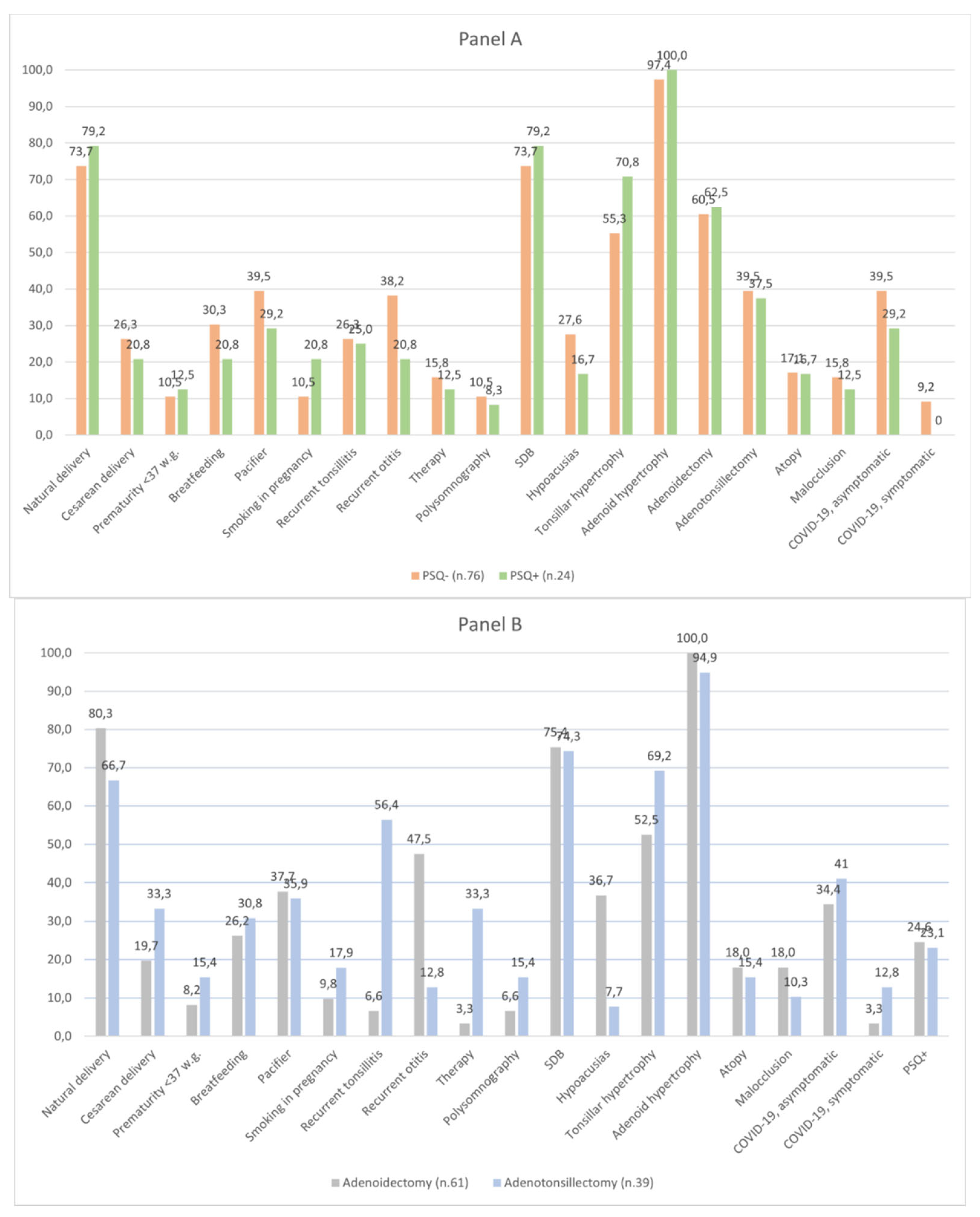
Post-operative follow-up revealed a lower percentage of children with a history of recurrent ear infections in the PSQ+ group (20.8%) compared to those with PSQ- (32.8%) and of hearing loss in the PSQ+ group (16.7%) compared to those with PSQ- (27.6%) at follow-up. A higher percentage of patients with PSQ+ had mothers who smoked during pregnancy (20.8%) compared to those with PSQ- (10.5%). Additionally, a lower proportion of patients with PSQ+ had a pacifier use habit (29.2%) than those with PSQ- (39.5%).

Table 1.
displays the results of a statistical analysis of continuous variables in two patient groups: those exhibiting symptoms of SDB (PSQ+, n = 76) and those who did not (PSQ-, n = 24). The variables’ mean and standard deviation (SD) are reported for each group, along with a 98% confidence interval (CI 98%) of the mean, indicated by the lower and upper limits. The Mann-Whitney test was conducted to determine whether the two groups had significant differences for the continuous variables.
Table 1.
displays the results of a statistical analysis of continuous variables in two patient groups: those exhibiting symptoms of SDB (PSQ+, n = 76) and those who did not (PSQ-, n = 24). The variables’ mean and standard deviation (SD) are reported for each group, along with a 98% confidence interval (CI 98%) of the mean, indicated by the lower and upper limits. The Mann-Whitney test was conducted to determine whether the two groups had significant differences for the continuous variables.
| Continue variables | PSQ- (n.76) | PSQ+ (n.24) | |||
| Mean (S.D.) | C.I. 98% (lower-upper) | Mean (S.D.) | C.I. 98% (lower-upper) | Mann-Whitney test (p) | |
| PSQ (%), T1 | 16.2 (9.0) | -34.3 ÷ (-25.7) | 46.2 (10.0) | -34.7 ÷ (-25.4) | < 0.001 |
| Birth weight (grams), T-1 | 3249 (575) | -537 ÷ (- 21) | 3507 (677) | -570 ÷ 53 | 0.086 |
| Length (cm), T-1 | 50.57 (2.95) | -1.41 ÷ 1.46 | 50.54 (3.53) | -1.59 ÷ 1.64 | 0.267 |
| Age of intervention (years), T0 | 5.20 (1.6) | -0.70 ÷ 0.73 | 5.13 (1.44) | -0.68 ÷ 0.71 | 0.904 |
| Age follow-up (years), T1 | 7.13 (1.69) | -0.07 ÷ 1.47 | 6.42 (1.54) | -0.05 ÷ 1.44 | 0.061 |
| BMI z-score, T1 | 0.13 (1.56) | -1.28 ÷ 0.20 | 0.67 (1.67) | -1.32–0.24 | 0.086 |
| Physical score (%), T1 | 0.91 (0.09) | 0.05 ÷ 0.18 | 0.81 (0.23) | 0.01 ÷ 0.21 | 0.022 |
| School score (%), T1 | 0.86 (0.16) | 0.08 ÷ 0.26 | 0.68 (0.27) | 0.05 ÷ 0.29 | 0.003 |
No significant differences were found in birth weight, age at follow-up, and BMI z-score. However, physical and school scores show substantial differences between the two groups. Birth weight, age at follow-up, and BMI z-score values may not be influenced by belonging to the two groups, while physical and school scores appear to be influenced by PSQ scores.
Table 2.
displays the results of a statistical analysis of continuous variables in two patient groups: those exhibiting symptoms of SDB (PSQ+, n = 76) and those who did not (PSQ-, n = 24). The variables’ mean and standard deviation (SD) are reported for each group, along with a 98% confidence interval (CI 98%) of the mean, indicated by the lower and upper limits. The Mann-Whitney test was conducted to determine whether the two groups had significant differences for the continuous variables.
Table 2.
displays the results of a statistical analysis of continuous variables in two patient groups: those exhibiting symptoms of SDB (PSQ+, n = 76) and those who did not (PSQ-, n = 24). The variables’ mean and standard deviation (SD) are reported for each group, along with a 98% confidence interval (CI 98%) of the mean, indicated by the lower and upper limits. The Mann-Whitney test was conducted to determine whether the two groups had significant differences for the continuous variables.
| Variables entered | Dependent variable: PSQ (%), follow-up | T | Error std | Beta | t | P | 95% C.I. per B | |
| Birth weight, birth length, age at surgery, age at follow-up, BMI z-score at follow-up, physical quality of life, and school quality of life. | Lower limit | Upper limit | ||||||
| Surgery age (years), T0 | 3.503 | 1.667 | 0.337 | 2.101 | 0.038 | 0.193 | 6.812 | |
| Age at follow-up, T1 | -3.811 | 1.515 | -0.404 | -2.516 | 0.014 | -6.818 | -0.804 | |
| Physical results (%), T1 | -20.892 | 10.577 | -0.195 | -1.975 | 0.051 | -41.890 | 0.105 | |
| Educational attainment (%), Q1 | -30.891 | 7.680 | -0.399 | -4.022 | <0.0001 | -46.138 | -15.644 |
The regression results can be interpreted as follows:
“Surgical intervention age (years), T0”: An increase of one year in the age of surgical intervention is associated with a mean increase of 3.5% in PSQ at follow-up, holding all other variables constant. This result is statistically significant (p=0.038).
Age at follow-up, T1”: An increase of one year in the age at follow-up is associated with a mean decrease of 3.8% in PSQ at follow-up, holding all other variables constant. This result is statistically significant (p=0.014).
Physical outcomes (%), T1”: An increase of one percentage point in physical outcomes is associated with a mean decrease of 20.9% in PSQ at follow-up, holding all other variables constant. This result is at the threshold of statistical significance (p=0.051).
Academic achievement (%), Q1”: An increase of one percentage point in educational achievement is associated with a mean decrease of 30.9% in PSQ at follow-up, holding all other variables constant. This result is statistically very significant (p<0.0001)
4. Discussion
The study involved 138 patients, of whom 65% were male, but only 100 parents participated. The results showed a lower percentage of children with SDB and a history of recurrent otitis and hearing loss after Ad compared to A&T. Additionally, children with recurrent tonsillitis were more likely to have undergone A&T surgery. Despite the different surgical approaches, both A&T and Ad led to comparable postoperative outcomes, as indicated by the absence of significant disparities in PSQ+ incidence. A higher percentage of patients with SDB had mothers who smoked during pregnancy, while a smaller proportion had a pacifier use habit. A history of prematurity and caesarean birth was more frequent in children who had undergone A&T. Physical outcomes and academic achievement at follow-up are associated with SDB. Specifically, an increase of one percentage point in physical outcomes and academic achievement at follow-up is associated with a mean decrease of 21% and 31%, respectively, in PSQ%.
Examining the complexities of OSAS in the young, it is essential to consider various risk factors and comorbidities. Children and adolescents with comorbidities such as obesity, neurological/developmental/craniofacial abnormalities, asthma, or severe OSAS are at high risk for residual OSAS [32]. Additionally, children with otitis media with effusion exhibit significant symptoms of OSAS. [33]. At a follow-up appointment, children with a history of recurrent tonsillitis more frequently underwent A&T rather than Ad, in line with Tatlipinar et al. [34]. Finally, a reduced percentage of children with a history of recurrent otitis media and hearing loss had persistent SDB after Ad surgery, as also suggested by Schupper et al. [9].
A child’s age plays a crucial role in the development of OSAS. According to Nosetti et al., the primary causes of SDB vary between children below and above 2 years old [35]. In younger children, there is a greater propensity to exhibit more severe OSAS, presumably due to age-related anatomical and physiological differences. Consequently, it is advisable to monitor younger children closely after A&T [37]. It’s interesting to note that the persistence of OSAS after otorhinolaryngology procedures has been associated with the presence of allergic rhinitis [36,37,38]. In the context of our study, children with SDB were, on average, younger than those without SDB, and no significant differences were found regarding allergies between the two groups, with or without SDB.
Assessing the head and neck area is crucial to determining other causes of upper airway obstruction besides tonsils and adenoids. Evidence suggests a connection between upper airway obstruction and specific patterns of oral breathing stemming from craniofacial development. This implies an intertwined interdependence between the two factors [39]. Improper alignment of teeth and jaw, known as malocclusion, can also contribute to SDB by restricting air passage through the nose and throat [40]. However, in our study, no significant differences were found in the percentage of children with malocclusion between those with and without persistent SDB. However, malocclusion was associated with specific behavioural habits, such as lack of pacifier use and breastfeeding [41]. Agreed, in our study, children without SDB more frequently had a history of pacifier use in infancy. However, despite some evidence, it is impossible to definitively conclude an association between specific malocclusion traits and SDB [42]. Although breastfeeding has been associated with a lower risk of developing SDB in children [43], we did not observe a significant difference between breastfed and non-breastfed infants for the persistence of SDB.
In our study, many children with a history of maternal smoking during pregnancy exhibited persistent SDB. According to Jara et al., passive smoke exposure during pregnancy is more common in children with SDB symptoms [44]. Ramirez et al. found a significant correlation between passive smoking and mild symptoms of SDB during early childhood, with both prenatal and childhood exposures to tobacco smoke showing a dose-dependent effect [45]. Tobacco smoke exposure during pregnancy can lead to various adverse perinatal outcomes, such as low birth weight, preterm birth, and perinatal mortality. Additionally, Tan et al. reported that children whose mothers were exposed to smoke during pregnancy had a 2.6 times higher risk of developing OSAS [46]. Rapaport Pasternak et al. have also reported similar results. [47].
Pediatric OSAS can have some behavioural consequences during childhood, both externalizing and internalizing, such as difficulties regulating behaviours, aggression, impulsivity, and hyperactivity [48]. Other neuropsychological symptoms previously reported as associated with SDB include internalizing problems such as anxiety, depression, and difficulty in controlling emotions [49]; attention-deficit/hyperactivity disorder (ADHD), daytime sleepiness, somatization, depression, aggression, and non-compliant social behaviours are also reported as associated with SDB [10,50,51]. Joosten et al. argue that comorbidities related to OSAS, such as hyperactivity, poor attention, hypertension, growth defects, or enuresis, should raise a physician’s suspicion of the presence of SDB [52]. Consistent with this, we found that poorer physical and academic performances are associated with the persistence of SDB. Specifically, a one-point increase in physical and educational outcomes is related to a decrease in PSQ% scores on average. Finally, delaying the age of ENT intervention was associated with an increase in PSQ% scores at follow-up.
The findings of our study could help identify children at higher risk of persistent SDB and implement appropriate preventive or therapeutic measures. However, our study has some limitations, such as being based on a specific analysis in a single reference centre, which may limit the generalizability of our conclusions to all pediatric patients with OSAS. Therefore, further research is needed to confirm and expand upon these results.
Another limitation of our study is its observational and retrospective design. Data collected via telephone interviews may be subject to information bias. Additionally, the loss of participants during follow-up may have influenced the validity of our results, as lost participants may differ in unknown conditions from those who were enrolled. However, the study’s strengths include exploring the association between ENT intervention and persistent SDB, and monitoring health trends in the population over time, such as changes in SDB incidence and associated factors. Ultimately, the findings of our study, supported by other reported studies, are crucial as they can assist clinicians in identifying patients at higher risk of OSAS and implementing appropriate preventive or therapeutic measures.
5. Conclusions
In conclusion, compared to Ad intervention, A&T intervention showed a lower incidence of SDB and a history of recurrent otitis and hearing loss. Additionally, a delay in ENT intervention was associated with increased PSQ% scores at follow-up. SDB at follow-up was correlated with maternal smoking during pregnancy and lower pacifier use, and there were no differences in SDB persistence between breastfed and non-breastfed infants. Prematurity and cesarean delivery were more common in children undergoing A&T. Physical outcomes and school performance at follow-up were associated with SDB, with a decrease in PSQ% for every percentage point of improvement. Lastly, these results provide important insights into the efficacy and effects of A&T intervention compared to Ad intervention and factors associated with SDB in children undergoing these interventions. They can help guide clinical decisions for treating SDB and otorhinolaryngological conditions in children.
Author Contributions
Conceptualization, M.Z. and A.P.; methodology, L.Z. and L.S.; software, M.Z. and M.P.; validation, L.N., G.P. and L.S.; formal analysis, M.Z.; investigation, M.Z. and L.S.; data curation, M.Z. and M.P.; writing—original draft preparation, M.Z.; writing—review and editing, A.P., L.Z., L.S, and L.N.; visualization, M.P.; supervision, A.P. and G.P. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Institutional Review Board Statement
The Ethics Committee approved the protocol for clinical studies in the provinces of Verona and Rovigo at the Integrated University Hospital (3766CESC).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lyons, M.M.; Bhatt, N.Y.; Pack, A.I.; Magalang, U.J. Global burden of sleep-disordered breathing and its implications. Respirology 2020, 25, 690-702. [CrossRef]
- Zaffanello, M.; Lippi, G.; Arman, N.; Piazza, M.; Tenero, L.; Piacentini, G. Popularity of sleep disordered breathing in childhood: an analysis of worldwide search using Google Trends. Transl Pediatr 2019, 8, 383-390. [CrossRef]
- M, Z.; G, P.; S, L.G. Beyond the growth delay in children with sleep-related breathing disorders: a systematic review. Panminerva medica 2020, 62. [CrossRef]
- Lo Bue, A.; Salvaggio, A.; Insalaco, G. Obstructive sleep apnea in developmental age. A narrative review. Eur J Pediatr 2020, 179, 357-365. [CrossRef]
- Lagravère, M.O.; Zecca, P.A.; Caprioglio, A.; Fastuca, R. Metabolic effects of treatment in patients with obstructive sleep apnea: a systematic review. Minerva Pediatr 2019, 71, 380-389. [CrossRef]
- Tagetti, A.; Bonafini, S.; Zaffanello, M.; Benetti, M.V.; Vedove, F.D.; Gasperi, E.; Cavarzere, P.; Gaudino, R.; Piacentini, G.; Minuz, P.; et al. Sleep-disordered breathing is associated with blood pressure and carotid arterial stiffness in obese children. J Hypertens 2016. [CrossRef]
- Brockmann, P.E.; Gozal, D. Neurocognitive Consequences in Children with Sleep Disordered Breathing: Who Is at Risk? Children (Basel) 2022, 9. [CrossRef]
- Todd, C.A.; Bareiss, A.K.; McCoul, E.D.; Rodriguez, K.H. Adenotonsillectomy for Obstructive Sleep Apnea and Quality of Life: Systematic Review and Meta-analysis. Otolaryngol Head Neck Surg 2017, 157, 767-773. [CrossRef]
- Schupper, A.J.; Nation, J.; Pransky, S. Adenoidectomy in Children: What Is the Evidence and What Is its Role? Curr Otorhinolaryngol Rep 2018, 6, 64-73. [CrossRef]
- Marcus, C.L.; Brooks, L.J.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Schechter, M.S.; Sheldon, S.H.; Spruyt, K.; Ward, S.D.; et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012, 130, 576-584. [CrossRef]
- Gulotta, G.; Iannella, G.; Vicini, C.; Polimeni, A.; Greco, A.; de Vincentiis, M.; Visconti, I.C.; Meccariello, G.; Cammaroto, G.; De Vito, A.; et al. Risk Factors for Obstructive Sleep Apnea Syndrome in Children: State of the Art. Int J Environ Res Public Health 2019, 16. [CrossRef]
- Tam, C.S.; Wong, M.; McBain, R.; Bailey, S.; Waters, K.A. Inflammatory measures in children with obstructive sleep apnoea. J Paediatr Child Health 2006, 42, 277-282. [CrossRef]
- Zaffanello, M.; Piacentini, G.; La Grutta, S. The cardiovascular risk in paediatrics: the paradigm of the obstructive sleep apnoea syndrome. Blood Transfus 2020, 1-9. [CrossRef]
- Lagravère, M.O.; Zecca, P.A.; Caprioglio, A.; Fastuca, R. Metabolic effects of treatment in patients with obstructive sleep apnea: a systematic review. Minerva pediatrica 2019, 71, 380-389. [CrossRef]
- Brockmann, P.E.; Gozal, D. Neurocognitive Consequences in Children with Sleep Disordered Breathing: Who Is at Risk? Children (Basel, Switzerland) 2022, 9, 1278.
- Todd, C.A.; Bareiss, A.K.; McCoul, E.D.; Rodriguez, K.H. Adenotonsillectomy for Obstructive Sleep Apnea and Quality of Life: Systematic Review and Meta-analysis. Otolaryngology–head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery 2017, 157, 767–773 %U https://pubmed.ncbi.nlm.nih.gov/28675097/.
- Agrafiotis, M.; Galanou, A.; Fletsios, D.; Chassiotou, A.; Chloros, D.; Steiropoulos, P. Functional Comorbidity Index and health-related quality of life in patients with obstructive sleep apnea. Adv Respir Med 2022. [CrossRef]
- Marcus, C.L.; Brooks, L.J.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Schechter, M.S.; Ward, S.D.; Sheldon, S.H.; Shiffman, R.N.; et al. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012, 130, e714-755. [CrossRef]
- Mitchell, R.B.; Archer, S.M.; Ishman, S.L.; Rosenfeld, R.M.; Coles, S.; Finestone, S.A.; Friedman, N.R.; Giordano, T.; Hildrew, D.M.; Kim, T.W.; et al. Clinical Practice Guideline: Tonsillectomy in Children (Update)-Executive Summary. Otolaryngol Head Neck Surg 2019, 160, 187-205. [CrossRef]
- Galluzzi, F.; Garavello, W. Impact of adenotonsillectomy in children with severe obstructive sleep apnea: A systematic review. Auris, nasus, larynx 2021, 48, 549–554 %U https://pubmed.ncbi.nlm.nih.gov/33109425/.
- Gozal, D.; Tan, H.L.; Kheirandish-Gozal, L. Treatment of Obstructive Sleep Apnea in Children: Handling the Unknown with Precision. J Clin Med 2020, 9. [CrossRef]
- Corrêa, C.C.; Weber, S.A.T.; Evangelisti, M.; Villa, M.P. Sleep Clinical Record application in Brazilian children and its comparison with Italian children. Sleep Med X 2019, 1, 100008. [CrossRef]
- Chervin, R.D.; Hedger, K.; Dillon, J.E.; Pituch, K.J. Pediatric sleep questionnaire (PSQ): validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med 2000, 1, 21-32. [CrossRef]
- Bitners, A.C.; Arens, R. Evaluation and Management of Children with Obstructive Sleep Apnea Syndrome. Lung 2020, 198, 257-270. [CrossRef]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PedsQL 4.0: reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Medical care 2001, 39, 800–812 %U https://pubmed.ncbi.nlm.nih.gov/11468499/.
- Tagetti, A.; Bonafini, S.; Zaffanello, M.; Benetti, M.V.; Vedove, F.D.; Gasperi, E.; Cavarzere, P.; Gaudino, R.; Piacentini, G.; Minuz, P.; et al. Sleep-disordered breathing is associated with blood pressure and carotid arterial stiffness in obese children. J Hypertens 2017, 35, 125-131. [CrossRef]
- Ferry, A.M.; Wright, A.E.; Ohlstein, J.F.; Khoo, K.; Pine, H.S. Efficacy of a Pediatric Sleep Questionnaire for the Diagnosis of Obstructive Sleep Apnea in Children. Cureus 2020, 12, e12244. [CrossRef]
- Umano, G.R.; Rondinelli, G.; Luciano, M.; Pennarella, A.; Aiello, F.; Mangoni di Santo Stefano, G.; Di Sessa, A.; Marzuillo, P.; Papparella, A.; Miraglia Del Giudice, E. Pediatric Sleep Questionnaire Predicts Moderate-to-Severe Obstructive Sleep Apnea in Children and Adolescents with Obesity. Children (Basel) 2022, 9. [CrossRef]
- Chervin, R.D.; Weatherly, R.A.; Garetz, S.L.; Ruzicka, D.L.; Giordani, B.J.; Hodges, E.K.; Dillon, J.E.; Guire, K.E. Pediatric sleep questionnaire: prediction of sleep apnea and outcomes. Arch Otolaryngol Head Neck Surg 2007, 133, 216-222. [CrossRef]
- Varni, J.W.; Burwinkle, T.M.; Seid, M.; Skarr, D. The PedsQL 4.0 as a pediatric population health measure: feasibility, reliability, and validity. Ambul Pediatr 2003, 3, 329-341. [CrossRef]
- Thiese, M.S.; Ronna, B.; Ott, U. P value interpretations and considerations. J Thorac Dis 2016, 8, E928-e931. [CrossRef]
- Imanguli, M.; Ulualp, S.O. Risk factors for residual obstructive sleep apnea after adenotonsillectomy in children. Laryngoscope 2016, 126, 2624-2629. [CrossRef]
- Huang, C.C.; Wu, P.W.; Chiu, C.H.; Lee, T.J.; Chen, C.L. Assessment of sleep-disordered breathing in pediatric otitis media with effusion. Pediatr Neonatol 2022, 63, 25-32. [CrossRef]
- Tatlıpınar, A.; Kınal, E. Links and risks associated with adenotonsillectomy and obesity. Pediatric Health Med Ther 2015, 6, 123-127. [CrossRef]
- Nosetti, L.; Zaffanello, M.; De Bernardi, F.; Piacentini, G.; Roberto, G.; Salvatore, S.; Simoncini, D.; Pietrobelli, A.; Agosti, M. Age and Upper Airway Obstruction: A Challenge to the Clinical Approach in Pediatric Patients. International Journal of Environmental Research and Public Health 2020, 17, E3531. [CrossRef]
- Wilhelm, C.P.; deShazo, R.D.; Tamanna, S.; Ullah, M.I.; Skipworth, L.B. The nose, upper airway, and obstructive sleep apnea. Ann Allergy Asthma Immunol 2015, 115, 96-102. [CrossRef]
- Shafiek, H.; Fawzy, N.; Mahmoud, M.I. Prevalence of obstructive sleep apnea in asthmatic school-aged children. European Respiratory Journal 2018, 52. [CrossRef]
- Alsufyani, N.; Isaac, A.; Witmans, M.; Major, P.; El-Hakim, H. Predictors of failure of DISE-directed adenotonsillectomy in children with sleep disordered breathing. J Otolaryngol Head Neck Surg 2017, 46, 37. [CrossRef]
- Nosetti, L.; Zaffanello, M.; De Bernardi di Valserra, F.; Simoncini, D.; Beretta, G.; Guacci, P.; Piacentini, G.; Agosti, M. Exploring the Intricate Links between Adenotonsillar Hypertrophy, Mouth Breathing, and Craniofacial Development in Children with Sleep-Disordered Breathing: Unraveling the Vicious Cycle. Children (Basel) 2023, 10. [CrossRef]
- Caruso, S.; Lisciotto, E.; Caruso, S.; Marino, A.; Fiasca, F.; Buttarazzi, M.; Sarzi Amadè, D.; Evangelisti, M.; Mattei, A.; Gatto, R. Effects of Rapid Maxillary Expander and Delaire Mask Treatment on Airway Sagittal Dimensions in Pediatric Patients Affected by Class III Malocclusion and Obstructive Sleep Apnea Syndrome. Life (Basel) 2023, 13. [CrossRef]
- Pegoraro, N.A.; Santos, C.M.D.; Colvara, B.C.; Rech, R.S.; Faustino-Silva, D.D.; Hugo, F.N.; Hilgert, J.B. Prevalence of malocclusion in early childhood and its associated factors in a primary care service in Brazil. Codas 2021, 34, e20210007. [CrossRef]
- Hansen, C.; Markström, A.; Sonnesen, L. Sleep-disordered breathing and malocclusion in children and adolescents-a systematic review. J Oral Rehabil 2022, 49, 353-361. [CrossRef]
- Gorlanova, O.; Thalmann, S.; Proietti, E.; Stern, G.; Latzin, P.; Kühni, C.; Röösli, M.; Frey, U. Effects of Breastfeeding on Respiratory Symptoms in Infancy. J Pediatr 2016, 174, 111-117.e115. [CrossRef]
- Jara, S.M.; Benke, J.R.; Lin, S.Y.; Ishman, S.L. The association between secondhand smoke and sleep-disordered breathing in children: a systematic review. Laryngoscope 2015, 125, 241-247. [CrossRef]
- Ramirez, F.D.; Groner, J.A.; Ramirez, J.L.; McEvoy, C.T.; Owens, J.A.; McCulloch, C.E.; Cabana, M.D.; Abuabara, K. Prenatal and Childhood Tobacco Smoke Exposure Are Associated With Sleep-Disordered Breathing Throughout Early Childhood. Acad Pediatr 2021, 21, 654-662. [CrossRef]
- Tan, Y.; Zhang, D.; Mei, H.; Mei, H.; Qian, Z.; Stamatakis, K.A.; Jordan, S.S.; Yang, Y.; Yang, S.; Zhang, B. Perinatal risk factors for obstructive sleep apnea syndrome in children. Sleep Med 2018, 52, 145-149. [CrossRef]
- Rapaport Pasternak, H.; Sheiner, E.; Goldbart, A.; Wainstock, T. Short and long interpregnancy interval and the risk for pediatric obstructive sleep apnea in the offspring. Pediatr Pulmonol 2021, 56, 1085-1091. [CrossRef]
- Conners, C.K.; Sitarenios, G.; Parker, J.D.; Epstein, J.N. The revised Conners’ Parent Rating Scale (CPRS-R): factor structure, reliability, and criterion validity. Journal of Abnormal Child Psychology 1998, 26, 257-268. [CrossRef]
- Blechner, M.; Williamson, A.A. Consequences of Obstructive Sleep Apnea in Children. Current Problems in Pediatric and Adolescent Health Care 2016. [CrossRef]
- Bucks, R.S.; Olaithe, M.; Eastwood, P. Neurocognitive function in obstructive sleep apnoea: a meta-review. Respirology 2013, 18, 61-70. [CrossRef]
- Testa, D.; Carotenuto, M.; Precenzano, F.; Russo, A.; Donadio, A.; Marcuccio, G.; Motta, G. Evaluation of neurocognitive abilities in children affected by obstructive sleep apnea syndrome before and after adenotonsillectomy. Acta Otorhinolaryngol Ital 2020, 40, 122-132. [CrossRef]
- Joosten, K.F.; Larramona, H.; Miano, S.; Van Waardenburg, D.; Kaditis, A.G.; Vandenbussche, N.; Ersu, R. How do we recognize the child with OSAS? Pediatr Pulmonol 2017, 52, 260-271. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



