
Submitted:
17 February 2024
Posted:
19 February 2024
You are already at the latest version
Abstract
Type 2 diabetes (T2DM) presents an enormous global healthcare challenge, especially among rural communities due to limited access. To overcome this, many low- and middle-income countries are resorting to task shifting, using community health workers (CHWs) for diabetes management. However, its successful implementation depends on the practice behaviours and knowledge of these workers.
This cross-sectional study from rural South India aimed to evaluate the proficiency of 275 CHWs in diabetes screening and management. A customized questionnaire, developed through experts and government was used to evaluate the practice behaviours and knowledge. Analytical methodologies consisted of descriptive statistics, logistic regression, and mosaic plots for comprehensive data interpretation.
Results showed significant deficiencies of mean correct practice behaviours at 48 and 50% respectively. The identified gaps included diabetes diagnosis, HbA1c testing, diet, self-management, complications screening and risk assessment. In several areas, correct practice behaviour was reported by a relatively large number of CHWs despite incorrect answers to the related knowledge questions such as referral to the health centres, self-management and calculation of diabetes risk assessment.
Addressing these deficiencies requires a thorough needs assessment and tailored training for improved diabetes management by CHWs. Training of CHWs, should not only identify prior knowledge and/or behaviour but also their interrelationship to help create a robust and flexible set of practice behaviours.
Keywords:
Community Health Workers
; Health worker Diabetes Knowledge
; Health worker Diabetes Practice
; Health worker Diabetes Behaviour
; South-East Asia
1. Introduction
Type 2 diabetes mellitus (T2DM) is a pressing global health concern, with an estimated 537 million adults living with the condition worldwide, and 74.2 million cases in India alone [1]. The World Bank data estimates that in 2021, the prevalence of T2DM in Indian adults was 5 per cent [2]. The International Diabetes Federation (IDF) reported that nearly 50% of persons are living with undiagnosed diabetes in India[1]. The report also estimates that this Indian burden is set to grow to 125 million by 2045 significantly affecting a major proportion of its population[1]. Recent trends have indicated the growing prevalence of diabetes amongst lower socioeconomic stratum and rural populations especially in LMICs[3]. With nearly 65% of Indians residing in such areas[4], diabetes poses a huge threat to the population. Prolonged exposure to high blood glucose levels can lead to severe health consequences, particularly micro- and macrovascular complications often leading to morbidity and mortality[1]. An Indian study showed that patients already have some form of diabetic retinopathy at the time of their eye clinic visits with a potential for blindness if left untreated[5]. Thus, detection and management of T2DM in these areas is extremely critical but is a challenge due to factors like limited access to healthcare services especially in rural areas, lack of trained personnel, unsatisfactory health-seeking behaviour and long travel distances [3,6,7,8,9]. Therefore, healthcare systems must develop innovative service models to overcome these barriers.
Task shifting of certain duties of medically trained healthcare workers in rural areas to frontline community health workers (CHWs) is one of the methods to improve the accessibility of care and to reduce the burden on the more qualified health workforce [10]. This approach is being carried out by several developing countries [11,12,13,14,15,16]. In India Multipurpose Health Workers/Assistants and Accredited Social Health Activists, typically members of the local communities, are nowadays involved in task shifting in various national health programs for the prevention and management of diabetes, cardiovascular disease, cancer, and stroke[11,17,18,19,20,21]. However, before entrusting the CHWs with the management of the entire spectrum of diabetes screening & management, along with the medical officers, we need to ascertain their capabilities in carrying out the prescribed duties. Evidence reveals a lack of knowledge among these health workers [22,23,24] and we need to better understand what these gaps in knowledge and associated practice behaviours are.
The current study was undertaken to define the current practice behaviours of CHWs responsible for screening and managing diabetes in rural South India and to determine if these behaviours were associated with specific gaps in knowledge. These data would be used as the starting point for the development of a specific training program tailored to the needs of these healthcare workers.
Hence the research question of this study is: what are the existing gaps in the practice behaviours and knowledge of the CHWs involved in screening and management of diabetes in rural South India?
2. Methodology
This study had a cross-sectional design and included the CHWs involved in diabetes screening and management at the community level and working in eight healthcare administrative regions of Telangana, South India between August 2021 to March 2022. Telangana has approximately 21,400,000 (21.4 million) rural inhabitants, which is almost 62% of its total population. These workers are primarily tasked with population enumeration, home screening and motivating patients to maintain a healthy lifestyle and attend regular complication screening supervision of tasks undertaken by junior cadres conduct meetings with local essential stakeholders, oversee the data from their health centre and share the data with the authorities.
We used a questionnaire to assess practice behaviour of the participants and associated knowledge. To develop this questionnaire, we first interviewed senior government officials and medical officers about the common situations faced by CHWs in the community. In these interviews, the most important practice behaviours of the CHWs were identified and the knowledge deemed conditional for these practice behaviours. The questionnaire was developed in both English and Telugu (vernacular language) consisting of 19 questions. This was then piloted with 10 CHWs not included in the study. Based on the feedback received, it was edited and eventually, the validated questionnaire consisted of 17 questions, 10 on practice behaviours and 7 on associated knowledge, as shown in Table A1 and summarized in Table 1.
We administered the questionnaire to 275 CHWs on paper in a face-to-face manner. Because of the diversity, in reading and linguistic skills (due to differences in dialects) the content of the questionnaire was explained by two research assistants during group sessions of approximately 25-30 CHWs per session. After all the queries of the CHWs were answered by the research assistants, participants were asked to fill in the answers individually and arrangements were made to ensure no discussion among the participants during this phase of the meeting was possible. The duration of each session was approximately 3.5-4 hours. Each session was presided over by two research associates and 8 meetings were held, in the region where the CHWs were working. The two research associates were trained beforehand and were provided with a handbook to assist them in their roles.
A digital version of the questionnaire was created for each participant in Microsoft (MS) Access and data were imputed by coding for correct and incorrect answers along with missing values. The imputed data were cross-verified by the lead researcher and wherever an error was discovered, those physical forms were accessed again to rectify the error. To ensure the veracity of the data, 10% of participants were contacted telephonically for verification. Once confirmed, the data were saved as an Excel workbook which was exported to STATA version 17 for analysis. For scoring the answers to each question, each correct answer was graded as 1 and a wrong, a double answer or no answer was graded as zero. In the initial phase, we asked the government officials and the doctors involved in the development of the questionnaire for the minimal number of correct answers and they formulated a benchmark of 75% correct answers, which we used as an external benchmark for sufficient practice behaviours and knowledge.
2.1. Statistical Analysis
The data were analyzed using mean + standard deviation, median with interquartile ranges (IQR) and frequencies wherever appropriate. The association between correct practice behaviours and their associated knowledge was explored using logistic regression to better understand the relationship between specific gaps in the practice behaviours and knowledge. Finally, to study the relation of correct practice behaviors with incorrect knowledge we used mosaic plots as graphical representations. These plots are divided into four parts, each part depicts the relationship between participants’ practice behaviours (Correct or Incorrect) with the participant’s knowledge (Correct or Incorrect). All the significant results were tabulated and are presented in the results section. More details on the plots and the relationships can be found in Appendix A.3.
3. Results
All participants (n=275) filled in the questionnaire; all were females with a mean age of 38.0 + 7.1 years. A majority (approx. 94%) completed high school. The median (IQR) work experience was 10 years (6-15 years). The median overall number of correct answers was 8 (7-10) out of 17 questions. Only 11 participants (4%) crossed the 75% external benchmark of correct answers (two participants had 14 and nine had 13 correct answers).
In the practice behaviour questionnaire the median overall number of correct answers was 5 (IQR 4-6) out of 10; only 9 participants (3.3%) crossed the 75% benchmark. The correctly answered percentages for each of the questions are depicted in Table A2 of the Appendix A. The participants reported sufficient practice behaviours for hypoglycemia management (78% had correct answers) and frequency of risk screening (75%) while the score for health centre referral, self-management and diabetes signs & symptoms were insufficient (9.8% to 51.3%).
In the knowledge questionnaire the median overall number of correct answers was 4 (IQR 3-4) out of 7, only 15 participants (5.5%) crossed the 75% benchmark. The correctly answered percentages for each of the questions are depicted in Table A3 in the Appendix A. The knowledge about diabetes diet (89.5% correct answers) and diabetic retinopathy/ hypoglycemia (85.1%) was sufficient. The knowledge about diabetes diagnosis & referral, types & self-management and microvascular complications and their screening was insufficient, (30.6% to 57.0% correct answers).
In order to study the association between practice behaviour with knowledge, their overall mean scores were standardized to a scale of 10 with overall mean scores of 5.5 and 4.8 respectively. Practice behaviour was associated with knowledge with an odds ratio of 1.64 and a standardized regression coefficient (beta) of 0.50 with a p-value <0.01. Subsequently, we examined for each pair of questions the association between practice behaviour and knowledge to determine to which extent specific practice behaviour was associated with the knowledge on this topic. In Table 2 the associations with p value below 0.2 are shown. The highest odds ratio (1.99) was observed for the association of microvascular complication screening with the knowledge question on this topic (beta-coefficient of 0.68) with a p-value of 0.09. Nearly the same association was observed for microvascular screening & peripheral neuropathy management with an odds ratio of 1.97 and beta of 0.68 (p= 0.01). The only other pair for which a significant association was observed was for HbA1c testing and diabetes, diagnosis and referral with an odds ratio of only 0.53 and a beta of -0.61 (p=0.04).
We used the mosaic plots to analyze the relationship between correct answers to practice behaviours questions with incorrect knowledge to determine common misconceptions and myths in diabetes care amongst community health workers. There were indeed four such instances where the CHWs answered more than 50% of the correctly answered practice behaviour questions and incorrectly answered knowledge questions. Table 3 depicts these relationships and their frequencies in detail. The mosaic plots can be found in the Appendix A.1.
4. Discussion
The study revealed insufficient practice behaviours and knowledge in ≥ 95% CHWs working in rural areas in India and who are responsible for diabetes screening and management. The identified areas of insufficiency were broadly representative of the core competencies required for effective diabetes management, encompassing diabetes diagnosis and referral, HbA1c testing, diabetes diet, diabetes type and self-management, microvascular complications and their screening, peripheral neuropathy management, and diabetes risk assessment.
Our observations align with existing literature [25,26,27,28,29] documenting incorrect practices among CHWs due to limited or insufficient knowledge. This underscores the need for thorough needs assessments to identify existing knowledge gaps and incorrect practices among CHWs. By addressing these gaps, we can enhance the effectiveness of CHW training programs and ultimately improve diabetes management outcomes.
The summary score of knowledge revealed a stronger association (OR 9.03, p=0.09) with the summary score of practice behaviours compared to associations of knowledge with practice behaviour when each pair of questions was analyzed separately (highest OR 1.99, p=0.09). This observation suggests that while overall knowledge levels tended to positively influence practice behaviours, the relationship was not as evident at the level of specific questions. To further investigate this discrepancy, we employed mosaic plots, which provided insights into potential associations between correct practice behaviours as reported by the respondents and incorrect knowledge. Interestingly, we identified several instances where CHWs reported correct practice behaviours despite possessing incorrect knowledge. This could be attributed to several factors, including prior training, educational differences, or the non-essential nature of specific knowledge for certain practices after adequate training. However, it is crucial to note that even in these cases, incorrect knowledge may hinder the long-term sustainability of the observed correct practice behaviours as it is more likely to push forth incorrect or out-of-date practice behaviours. Thus, focusing solely on either knowledge or behaviour may not yield the desired long-term outcomes. Instead, an integrated, comprehensive approach focusing on both components is essential for effectively equipping CHWs to provide quality diabetes care.
The major strengths of the study were that the questionnaire was developed in close cooperation with the medical staff ultimately responsible for diabetes care as well as using input and feedback from the target group studied. We were therefore able to develop the questionnaire into an accessible tool that could be readable and understandable for all CHWs. In addition, we recruited a relatively large number of participants from multiple rural areas increasing the external validity of our observations. The study also has high generalizability in similar geographies of rural Southeast Asia which bear similarities to our study site like similar diversities of linguistics, education, cultures, practices and socio-demographic factors. Given the time necessary to explain and subsequently fill in the questionnaire, we had to restrict the number of questions for each domain. Moreover, in a few cases, we had to combine two questions into one question, which might have caused difficulty in comprehension for the CHWs and which may have weakened the associations between knowledge and practice behaviour for a specific topic.
Finally, some areas require further exploration, like the correct practice behaviours linked with the incorrect practice behaviours and vice-versa; the barriers and enablers for such relationships also need exploration. The analysis surprisingly discovered that the use of HbA1c testing in daily practice was negatively associated with knowledge of diabetes, diagnosis, and referral: with an odds ratio of 0.53, beta-coefficient of 0.61 and p-value 0.04. This finding, which is currently difficult to explain, needs further exploration in order to improve future training.
5. Conclusions
To conclude, the vast majority of the CHWs involved in diabetes screening and management in rural areas reported inadequate practice behaviour and had insufficient knowledge underlying these behaviours. Defining these gaps in knowledge and practice behaviour is very informative in setting up tailored education programs. However, in several areas, correct practice behaviour was reported by a relatively large number of CHWs despite incorrect answers to the related knowledge questions. Hence, training of CHWs, should not only identify prior knowledge and/or behavior but also their interrelationship to help create a robust and flexible set of practice behaviors that are in line with guidelines on diabetes care, that are continuously changing over time.
Author Contributions
Conceptualization: Anirudh Gaurang Gudlavalleti, Giridhara R. Babu, Nicolaas C Schaper, OCP van Schayck. Validation: Nicolaas Schaper, Giridhara R. Babu, Onno CP van Schayck. Data curation: Anirudh Gaurang Gudlavalleti, Varun Agiwal. Funding acquisition: Anirudh Gaurang Gudlavalleti, Giridhara R. Babu, G.V.S Murthy. Methodology: Anirudh Gaurang Gudlavalleti, Giridhara R. Babu, G.V.S Murthy, Nicolaas C. Schaper, Onno CP van Schayck. Project administration: Anirudh Gaurang Gudlavalleti. Resources: Anirudh Gaurang Gudlavalleti, Giridhara R. Babu, Nicolaas C. Schaper, Onno CP van Schayck. Software: Anirudh Gaurang Gudlavalleti, Varun Agiwal. Supervision: Giridhara R. Babu, G.V. S Murthy, Nicolaas C. Schaper, Onno CP van Schayck. Writing—original draft: Anirudh Gaurang Gudlavalleti. Writing—review & editing: Anirudh Gaurang Gudlavalleti, Giridhara R. Babu, G.V.S Murthy, Nicolaas C. Schaper, Onno CP van Schayck.
Funding
This research received funding from the Department of Science & Technology, India, under the Scheme for Young Scientist and Technologist (SYST) file number: SP/YO/2019/1021 and the APC was funded by PushpagiriVitreo Retinal Institute.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional ethics committee of the Indian Institute of Public Health Hyderabad, with the registration number: IIPHH/TRCIEC/218/2020. The trial has also been registered under the Clinical trial registry of India (CTRI) on 27th July 2020. The registration number of the trial is: CTRI/2020/07/026828. The URL of the registry trial is: http://ctri.nic.in/Clinicaltrials/showallp.php?mid1=45342&EncHid=&userName=CTRI/2020/07/026828.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Consent was also obtained to publish the data anonymously.
Data Availability Statement
The anonymized data will be available on request for those interested due to ethical considerations.
Acknowledgments
The authors would like to express their heartfelt gratitude to Pushpagiri Vitreo Retina Institute for its administrative support, technical support and article processing charges support.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Appendix A

Table A1.
Questionnaire Used for Data Collection.
| General Information of CHWs | |||
|---|---|---|---|
| Name of CHW | Name of PHC | ||
| Age of CHW | Designation of CHW | ||
| Gender of CHW | Educational Qualification of CHW | ||
| Marital Status of CHW | Work Experience of CHW (in Yrs) | ||
| Address of VHW (village Name) | Diatance of residence from PHC | ||
| Practice Behaviour & Knowledge Assessment | |||
| Question | Answer Options | ||
| Q1. Which of these signs indicate diabetes, how is it diagnosed, and where should someone go for treatment?? | 1. Increased Blood Glucose levels, diagnosed using HbA1c and managed at Primary Health Centre (PHC) 2. Increased Blood pressure, diagnosed using HbA1c and managed at PHC 3. Random blood glucose values above or equal to 200mg/dl, diagnosed using Random or fasting glucose and managed at PHC 4. Both 1. and 3 |
||
| Q2. A 40-year-old woman has a condition where her body doesn’t make enough insulin. She experiences more urination at night, and increased hunger, and thirst. What’s this condition called, and what can she do to feel better? | 1). Type 1 Diabetes; only exercise 2). Type 2 Diabetes; exercise, medication & diet control with medicines 3). Gestational Diabetes; do nothing 4). Monogenic Diabetes; only medication |
||
| Q3- A 38-year-old patient with diabetes is under your care. However, he does not get his blood glucose levels checked regularly due to a fear of multiple pricks. What will you do in this case to get to know his blood glucose control? | 1. Advise Fasting blood glucose test at the nearest facility 2. Advise Glycosylated Hemoglobin- HbA1c test at the nearest facility 3. Advise Random blood glucose test at the nearest facility 4. Both 1. and 3. |
||
| Q4- A 65-year-old known diabetic is under your care. How often will you recommend herself be screened for diabetes-associated chronic complications? What should you advise to prevent/manage COVID-19? | 1). Once every 2 years/ Exercise 2). Once every 3 months/ COVID Medicine 3). Once every year (Annually)/ COVID-vaccination 4). Once every 3 years/ Nothing can be done |
||
| Q5- A 57-year-old diabetic patient under your care has been on insulin for 5 years. Suddenly at night, his wife calls to tell you that he is suffering from Sweating, Tremors, Hunger, Fast heartbeat, Dizziness, Confusion What will you advise the wife to improve the patient’s condition immediately |
1. Advise the patient to take more Insulin 2. Advise the patient to take glucose or sugar dissolved in water immediately 3. Advise the patient to sleep and it will be fine in the morning 4. Will not give any advice to the patient |
||
| Q6- A 47-year-old male with diabetes for 15 years comes to you with a complaint of tingling sensations in the feet and sometimes a burning sensation in the feet. What could this be, and how often should he get checked for it? | 1). Hypoglycemia; Checked once every year 2). Peripheral Neuropathy; Checked once every year 3). Diabetic Ketoacidosis; Checked twice every year 4). Diabetic Retinopathy; Checked twice every year |
||
| Q7- Your friend has been troubled over the past few days and approaches you in tears. She tells you that her 71-year-old mother who has been a diabetic for 12 years and is on medicines has been experiencing dizziness, burning sensation in her feet, overall lethargy and getting tired easily. She thinks her mother’s medicines are not having any effect and wants your help. What can you do to help her mother? |
1. Change/Modify her medicine based on her blood glucose values 2. Send her to the ANM to get her medicines changed/modified 3. Refer her to the Medical Officer at the nearest health centre 4. Ask her to change/modify her medicines as per the pharmacist’s advise |
||
| Q8-Which of the following foods will you advise for any person with diabetes or at risk of developing diabetes? | 1. Samosas 2. Bajjis/Pakodas 3. Black Chana 4. Laddoos |
||
| Q9- A 46-year-old patient with diabetes who is under your care is constantly taking sweets and sugarcane juice. What can you suggest as a natural alternative to satisfy their sweet tooth? | 1. Mangoes 2. Chikus/Sapotas 3. Grapes 4. Apples |
||
| Q10- A 48-year-old patient with diabetes for the last 3 years has come to you with his blood glucose readings for the past two months. You observe that most of his readings are over 200 mg/dl. In such case what can you advise the patient to help them improve their glucose control? | 1. Regular exercise for at least 30 mins for five days a week 2. Consuming a diet rich in proteins 3. Reducing or eliminating habits like smoking, alcohol, tobacco chewing, etc 4. All of the above |
||
|
Q11- What will you advise for a Diabetic patient during the COVID-19 Pandemic? |
1. To maintain blood glucose levels within the prescribed range (< 140 mg/dl) 2. To keep a stock of all important medicines 3. To consult a doctor if they have any flu-like symptoms 4. All of the above |
||
| Q12- Which of the following organs or body parts is affected by uncontrolled Diabetes and what is an unexpected fall in blood glucose called | 1). Stomach; Hyperglycemia 2). Retina; Hypoglycemia 3). Both the above are correct 4). None of the above are correct |
||
|
Q13- A 69-year-old farmer who has been diabetic for the last 10 years has been complaining to you about a burning sensation in his feet for the last couple of weeks. You sent him to the nearest health facility where the doctor treated it. Now what should be your advice to ensure that this condition does not arise for the patient again? |
1. To be barefoot all the time 2. To wash and inspect feet daily 3. To use boiling water to clean feet 4. To leave the feet dry |
||
| Q14- A 40-year-old person, with a height of 5’4 and weight of 87kgs presents to you with the following problems: Frequent urination, Excessive thirst Increased hunger & Sudden weight loss. What would you advise? |
1. Refer to the nearest health centre for random blood glucose testing/HbA1C testing 2. Refer to the nearest health centre for blood pressure testing/ 3. Refer to the nearest health centre for thyroid hormone tests 4. None of the above |
||
| Q15- A 53-year-old male who leads a sedentary lifestyle with a family history of Diabetes, a waist circumference of more than 100cm and habits of smoking, and consuming alcohol daily has undergone CBAC Assessment. What will be the total score? | 1. Seven 2. Fifteen 3. Four 4. Ten |
||
|
Q16- What does a score less than four in the CBAC Assessment imply? |
1. The person is free from NCDs 2. The person is at higher risk of getting NCDs 3. The person still needs to be screened for NCDs annually 4. The person may not attend the weekly NCD Meeting |
||
| Q17- You are a part of the NCD screening in your village this year. A 41-year-old female comes to enquire about what is happening. On further interaction, you learn that she has no history of diabetes or hypertension and also does not share any signs/symptoms of either. In such a case what will be your plan of action? | 1. Screen the person every year (annually) 2. No need to screen the person again 3. Screen the person after 2 years 4. Screen the person every 5 years |
||
Table A2.
Question-wise practice behaviour scores of the community health workers.
| Practice Behaviour scores | |||
|---|---|---|---|
| Themes | Questions | Percentage of participants with correct answers % (n) | Confidence intervals |
| Practice behaviour | Diabetes signs & symptoms | 51.3% (141) | 45%-57% |
| Referral to health centre | 66.5% (183) | 60%-72% | |
| HbA1c testing | 31.6% (87) | 26%-37% | |
| Diabetes diet | 41.8% (115) | 35%-47% | |
| Self-management | 52% (143) | 45%-58% | |
| Hypoglycemia management | 78% (215) | 72%-82% | |
| Microvascular complication screening | 9.8% (27) | 6%-13% | |
| Peripheral neuropathy management | 29.5% (81) | 24%-35% | |
| Calculation of diabetes risk score | 26.6% (73) | 21%-32% | |
| Frequency risk screening | 75.6% (208) | 70%-80% | |
Table A3.
Question-wise knowledge scores of the community health workers.
| Knowledge Score | |||
|---|---|---|---|
| Themes | Questions | Percentage of participants with correct answers % (n) | Confidence intervals |
| Knowledge questions | Diabetes, diagnosis & referral | 31.6% (87) | 26%-37% |
| Diabetes: types & self-management | 30.6% (84) | 25%-36% | |
| Diabetes diet | 89.5% (246) | 85%-92% | |
| Diabetic retinopathy and Hypoglycemia (combined question) | 85.1% (234) | 80%-89% | |
| Microvascular complications: signs & screening | 36.7% (101) | 31%-42% | |
| Diabetes & COVID | 57.1% (157) | 51%-63% | |
| Diabetes risk assessment | 44% (121) | 38%- 50% | |
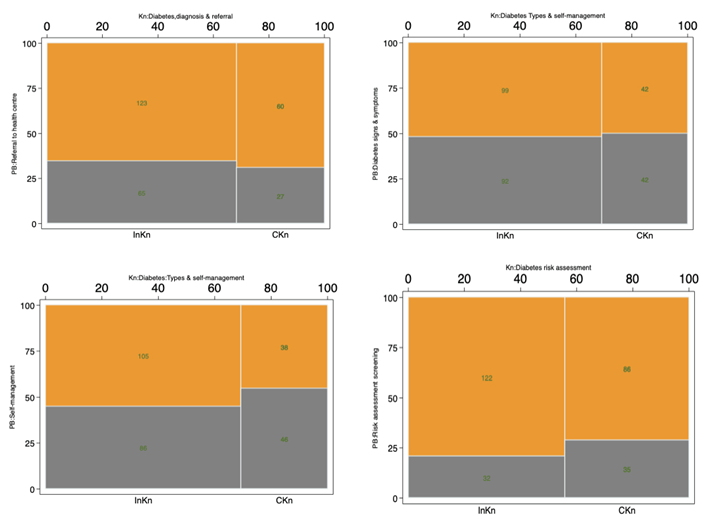
Appendix A.1. Mosaic Plots Depicting the Strong Relationship between Correct Practice Behaviour and Incorrect Knowledge
Each mosaic plot consists of four sections. Each plot has the number of participants answering knowledge questions on the X-axis and practice behaviour questions on the Y-axis. In the plot, there are two columns, each divided into two parts. The left column shows the number of participants who answered knowledge questions incorrectly. The right column shows the same for correctly answered knowledge questions. The upper part of each column shows the number of participants who answered practice behaviour questions correctly and the lower part who answered incorrectly. Further, the upper right section shows the number of participants who answered both knowledge and practice behaviour questions correctly, and the upper left section shows the number of participants who answered the practice behaviour questions correctly but the knowledge questions incorrectly. The lower left section shows the number of participants who answered both the knowledge and practice behaviour questions incorrectly. The lower right section shows the number of participants who answered knowledge questions correctly but practice behaviour questions incorrectly.
References
- Federation, ID. IDF Diabetes Atlas. 10th edition. 2021. www.diabetesatlas.org.
- The World Bank Group. Population, total- India. 2022. https://data.worldbank.org/indicator/SP.POP.TOTL?locations=IN. Accessed 1 Aug 2022.
- Anjana RM, Deepa M, Pradeepa R, Mahanta J, Narain K, Das HK, et al. Prevalence of diabetes and prediabetes in 15 states of India: results from the ICMR–INDIAB population-based cross-sectional study. Lancet Diabetes Endocrinol. 2017;5:585–96.
- Statistics Division M of H&, FW. Rural Health Statistics. New Delhi; 2021. https://hmis.nhp.gov.in/downloadfile?filepath=publications/Rural-Health-Statistics/RHS 2020-21.pdf.
- Shukla R, Gudlavalleti MVS, Bandyopadhyay S, Anchala R, Gudlavalleti ASV, Jotheeswaran AT, et al. Perception of care and barriers to treatment in individuals with diabetic retinopathy in India: 11-city 9-state study. Indian J Endocrinol Metab. 2016;20:S33–41.
- Jacobs B, Ir P, Bigdeli M, Annear PL, Van Damme W. Addressing access barriers to health services: An analytical framework for selectingappropriate interventions in low-income Asian countries. Health Policy Plan. 2012;27:288–300.
- Baru R V, Acharya A, Acharya S, Shiva Kumar A, Nagaraj K. Inequities in Access to Health Services in India. Econ Polit Wkly. 2010;xlv:49–58. http://www.mendeley.com/research/inequities-access-health-services-india/.
- Kumar V, Singh P. Access to healthcare among the Empowered Action Group (Eag) states of India: Current status and impeding factors. Natl Med J India. 2016;29:267–73.
- Correction: Prevalence of diabetes and prediabetes in 15 states of India: results from the ICMR–INDIAB population-based cross-sectional study (The Lancet Diabetes and Endocrinology (2017) 5(8) (585–596)(S2213858717301742)(10.1016/S2213-8587(17)30174-2)). Lancet Diabetes Endocrinol. 2017;5:e5.
- WHO. Task Shifting. Global Recomendations and Guidelines. 2008.
- Balasubramanya B, Isaac R, Philip S, Prashanth HR, Abraham P, Poobalan A, et al. Task shifting to frontline community health workers for improved diabetes care in low-resource settings in India: a phase II non-randomized controlled clinical trial. J Glob Heal Reports. 2020;4:1–9.
- Joshi R, Alim M, Kengne AP, Jan S, Maulik PK, Peiris D, et al. Task shifting for non-communicable disease management in low and middle income countries - A systematic review. PLoS One. 2014;9.
- Jeemon P, Narayanan G, Kondal D, Kahol K, Bharadwaj A, Purty A, et al. Task shifting of frontline community health workers for cardiovascular risk reduction: Design and rationale of a cluster randomised controlled trial (DISHA study) in India. BMC Public Health. 2016;16:1–11. [CrossRef]
- Lekoubou A, Awah P, Fezeu L, Sobngwi E, Kengne AP. Hypertension, diabetes mellitus and task shifting in their management in sub-Saharan Africa. Int J Environ Res Public Health. 2010;7:353–63.
- Maria JL, Anand TN, Dona B, Prinu J, Prabhakaran D, Jeemon P. Task-sharing interventions for improving control of diabetes in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Glob Heal. 2021;9:e170–80. [CrossRef]
- Lekoubou A, Awah P, Fezeu L, Sobngwi E, Kengne AP, Joshi R, et al. Hypertension, diabetes mellitus and task shifting in their management in sub-Saharan Africa. J Interprof Care. 2010;7:353–63. [CrossRef]
- National Health Mission. Operational Guidelines: Prevention, Screening and Control of Common Non-Communicable Diseases: Hypertension, Diabetes and Common Cancers (Oral, Breast, Cervix)(Part of Comprehensive Primary Health Care. New Delhi: National Health Mission; 2016. http://nhsrcindia.org/sites/default/files/Operational Guideline Comprehensive Primary Health Care.pdf.
- NHM, NPCDCS. Training manual for NCD program manager at State and District level. 2017. https://main.mohfw.gov.in/sites/default/files/Training Manual for NCD Programme Managers at State and Disctrict Level_0.pdf.
- WHO. Community health workers : What do we know about them ? 2007. https://www.who.int/hrh/documents/community_health_workers_brief.pdf.
- Kartar Singh Committee. Report of the committee on multipurpose workers under health and family planning programs. New Delhi; 1972. https://www.nhp.gov.in/sites/default/files/pdf/Kartar_Singh_Committee_Report.pdf.
- NHM, NHSRC. ASHA Which Way Forward...? New Delhi: Macrographics; 2011. https://nhm.gov.in/images/pdf/communitisation/asha/Studies/Evaluation_of_ASHA_Program_2010-11_Report.pdf.
- Lopes SC, Cabral AJ, de Sousa B. Community health workers: To train or to restrain? A longitudinal survey to assess the impact of training community health workers in the Bolama Region, Guinea-Bissau. Hum Resour Health. 2014;12:1–9.
- Tsolekile LP, Schneider H, Puoane T. The roles, training and knowledge of community health workers about diabetes and hypertension in Khayelitsha, Cape Town. Curationis. 2018;41:1–8.
- Abrahams-Gessel S, Denman CA, Montano CM, Gaziano TA, Levitt N, Rivera-Andrade A, et al. The Training and Fieldwork Experiences of Community Health Workers Conducting Population-Based, Noninvasive Screening for CVD in LMIC. Glob Heart. 2015;10:45. [CrossRef]
- Hughes GD, Puoane T, Bradley H. Ability to manage diabetes - Community health workers’ knowledge, attitudes and beliefs. J Endocrinol Metab Diabetes South Africa. 2006;11:10–4.
- Ferguson WJ, Lemay CA, Hargraves JL, Gorodetsky T, Calista J. Developing community health worker diabetes training. Health Educ Res. 2012;27:755–65.
- Tripathy JP, Thakur JS, Jeet G, Chawla S, Jain S, Pal A, et al. Prevalence and risk factors of diabetes in a large community-based study in North India: results from a STEPS survey in Punjab, India. Diabetol Metab Syndr. 2017;9:1–8.
- Rendrayani F, Alfian SD, Wahyudin W, Puspitasari IM. Pharmacists’ Knowledge, Attitude, and Practice of Medication Therapy Management: A Systematic Review. Healthc. 2022;10.
- Ferguson E, Mills R. Exploring the nuances of cooperation in public health – a critical reflection on default policies and reputation effects: a reply to ‘Nurturing, nudging and navigating the increasingly precarious nature of cooperation in public health: the cases of vaccin. Glob Discourse. 2023;XX Xx:1–21. [CrossRef]
Table 1.
The Associations of Practice Behaviour with Knowledge in the Questionnaire (Complete Questionnaire in Table A1). Bold is indicating a correct answer.
Table 1.
The Associations of Practice Behaviour with Knowledge in the Questionnaire (Complete Questionnaire in Table A1). Bold is indicating a correct answer.
| Practice behaviour & related knowledge questions with correct answers in bold | |
|---|---|
| Practice Behaviour Questions | Knowledge Questions |
| PbQ1: You encounter a 40-year-old individual who is 5 feet 4 inches tall and weighs 87 kg. This person reports the following concerns: 1. Frequent urination 2. Excessive thirst 3. Increased appetite 4. Unexplained rapid weight loss What guidance or recommendations would you offer in response to these symptoms?: Answer options: 1). Refer to the nearest health centre for random blood glucose/ HbA1c testing 2). Refer to the nearest health centre for blood pressure testing 3). Refer to the nearest health centre for thyroid hormone tests 4). None of the above |
KnQ1: A 40-year-old woman has a condition where her body doesn’t make enough insulin. She experiences more urination at night, and increased hunger, and thirst. What’s this condition called, and what can she do to feel better? Answer Options 1). Type 1 Diabetes; only exercise 2). Type 2 Diabetes; exercise, medication & diet control with medicines 3). Gestational Diabetes; do nothing 4). Monogenic Diabetes; only medication This knowledge question, KnQ1 is associated with practice behaviour questions: PbQ1 and PbQ3 |
| PbQ2: How would you approach the assessment of blood glucose control for a 38-year-old patient with diabetes who refrains from regular blood glucose checks due to a fear of multiple pricks? Answer Options: 1). Advise Fasting blood glucose test at the nearest facility 2). Advise Glycosylated Hemoglobin- HbA1c test at the nearest facility 3). Advise Random blood glucose test at the nearest facility 4). Both 1. and 2 |
KnQ2: Which of these signs indicate diabetes, how is it diagnosed, and where should someone go for treatment? Answer Options 1). Increased Blood Glucose levels, diagnosed using HbA1c and managed at Primary Health Centre (PHC) 2). Increased Blood pressure, diagnosed using HbA1c and managed at PHC 3). Random blood glucose values above or equal to 200mg/dl, diagnosed using Random or fasting glucose and managed at PHC 4). Both 1. and 3 This knowledge question, KnQ2 is associated with practice behaviour questions: PbQ2 and PbQ7 |
| PbQ3: You have a 48-year-old patient who has had diabetes for three years. They have given you their blood sugar readings from the past two months, and most of them are consistently over 200 mg/dL. What would you suggest to help this patient improve their blood glucose control? Answer Options 1). Regular exercise for at least 30 mins for five days a week 2). Consuming a diet rich in proteins 3). Reducing or eliminating habits like smoking, alcohol, tobacco chewing, etc 4). All of the above |
KnQ3: Which of the following organs or body parts is affected by uncontrolled Diabetes and what is an unexpected fall in blood glucose called Answer Options 1). Stomach; Hyperglycemia 2). Retina; Hypoglycemia 3). Both the above are correct 4). None of the above are correct This knowledge question, KnQ3 is associated with practice behaviour questions: PbQ4 |
| PbQ4: A 57-year-old diabetic patient, on insulin for 5 years, experiences symptoms like sweating, tremors, hunger, a fast heartbeat, dizziness, and confusion at night. If his wife calls you for help, what would you advise her to do immediately to improve his condition? Answer Options: 1). Advise the patient to take more Insulin 2). Advise the patient to take glucose or sugar dissolved in water immediately 3). Advise the patient to sleep and it will be fine in the morning 4). Will not give any advice to the patient |
KnQ4: A 47-year-old man, diabetic for 15 years, reports tingling and burning sensations in his feet. What could this be, and how often should he get checked for it? Answer Options 1). Hypoglycemia; Checked once every year 2). Peripheral Neuropathy; Checked once every year 3). Diabetic Ketoacidosis; Checked twice every year 4). Diabetic Retinopathy; Checked twice every year This knowledge question, KnQ4 is associated with practice behaviour questions: PbQ5 and PbQ6 |
| PbQ5: You’re overseeing the care of a 65-year-old diabetic patient. How frequently should you remind her to undergo screening for diabetes-related chronic complications of the eye & kidneys? What should you advise to prevent/manage COVID-19? Answer Options 1). Once every 2 years/ Exercise 2). Once every 3 months/ COVID Medicine 3). Once every year (Annually)/ COVID-vaccination 4). Once every 3 years/ Nothing can be done |
KnQ5: What will you advise for a Diabetic patient during the COVID-19 Pandemic? Answer Options 1). To maintain blood glucose levels within the prescribed range (< 140 mg/dl) 2). To keep a stock of all important medicines 3). To consult a doctor if they have any flu-like symptoms 4). All of the above This knowledge question, KnQ5 is associated with practice behaviour questions: PbQ5 |
| PbQ6: A 69-year-old farmer, who has had diabetes for 10 years, had a burning sensation in his feet for a few weeks. He received treatment at a nearby clinic. What advice would you provide to ensure this problem doesn’t come back? Answer Options 1). To be barefoot all the time 2). To wash and inspect feet daily 3). To use boiling water to clean feet 4). To leave the feet dry |
KnQ6: What foods would you recommend for individuals with diabetes or those at risk of developing diabetes? Answer Options 1). Samosas (Indian fried snack) 2). Bajji/Pakodas (Indian Fritters) 3). Black Chana (Black Grams) 4). Laddoos (Indian Dessert) This knowledge question, KnQ6 is associated with practice behaviour questions: PbQ8 |
| PbQ7: Your friend is upset and tells you that her 71-year-old diabetic mother, who has been on medication for 12 years, is experiencing dizziness, burning sensations in her feet, overall tiredness, and easy fatigue. She thinks the medicines aren’t working and asks for your help. What can you do to assist her mother? Answer Options 1). Change her medicine based on her blood glucose values 2). Send her to the ANM to get her medicines changed/modified 3). Refer her to the Medical Officer at the nearest health centre to change her medicines if needed 4). Ask her to change her medicines as per the pharmacist’s advise |
KnQ7: What does a score below four in the Community Based Assessment Checklist (CBAC)* Assessment mean, and what should be done if the score is less than four? Answer Options 1). The person is free from Non-Communicable Diseases (NCDs) 2). The person is at higher risk of getting NCDs 3). The person still needs to be screened for NCDs annually 4). The person may not attend the weekly NCD Meeting This knowledge question, KnQ7 is associated with practice behaviour questions: PbQ9 & PbQ10 |
| PbQ8: Your patient, aged 46 with diabetes, indulges in sweets and sugarcane juice. Which food can you recommend for satisfying their sweet cravings naturally without impacting their diabetes? Answer Options 1). Mangoes 2). Chikus/Sapotas 3). Grapes 4). Apples |
|
| PbQ9: 53-year-old man, who does not move around much, has a family history of diabetes, a waist size over 100 cm, and smokes while drinking alcohol daily. When using the Community Based Assessment Checklist (CBAC), what will be his total score? Answer Options 1). Seven 2). Fifteen 3). Four 4). Ten |
|
| PbQ10: As a Community Health Worker (CHW) doing health checks in your village. A 41-year-old woman comes up to you, saying she does not have a history of diabetes or high blood pressure, and she doesn’t seem to have any symptoms of these conditions. What should you do in this situation? Answer Options 1). Screen the person every year (annually) 2). No need to screen the person again 3). Screen the person after 2 years 4). Screen the person every 5 years |
|
Table 2.
Logistic Regression Between Practice Behaviour & Knowledge Questions.
| Practice Behaviour Question | Knowledge Question | Odds Ratio | Coefficient | p-value |
|---|---|---|---|---|
| HbA1c Testing | Diabetes, Diagnosis & referral | 0.53 | -0.61 | 0.04 |
| Self-Management | Diabetes: Types & Self-Management | 0.67 | -0.39 | 0.13 |
| Microvascular Complication Screening | Microvascular Complications: Signs & Screening | 1.99 | 0.68 | 0.09 |
| Peripheral Neuropathy Management | Microvascular Complications: Signs & Screening | 1.97 | 0.68 | 0.01 |
| Risk Assessment Screening | Diabetes Risk Assessment | 0.64 | -0.43 | 0.12 |
Table 3.
Relationship of incorrect knowledge and correct practice behaviours among CHWs.
| Knowledge | Practice Behaviour | Correct Practice Behaviours Despite Incomplete/ Incorrect Knowledge Responses |
|---|---|---|
| Knowledge about referral criterion and pathway | Practice Behaviour about Referral to the Health Centre | 123 out of 183 participants (67.2%) displayed correct practice behaviour despite incomplete knowledge responses |
| Knowledge about types of Diabetes | Practice Behaviour about Self-Management | 105 out of 143 participants (73.4%) displayed correct practice behaviour despite incomplete knowledge responses |
| Knowledge about types of diabetes | Practice Behaviour about identifying type 2 diabetes signs & symptoms | 99 out of 141 participants (70.2%) displayed correct practice behaviour despite incomplete knowledge responses |
| Knowledge about diabetes risk assessment | Risk Assessment Screening | 122 out of 208 participants (58.7%) displayed correct practice behaviour despite incomplete knowledge responses |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



