
Submitted:
18 February 2024
Posted:
19 February 2024
You are already at the latest version
Abstract
Landiolol is an ultra-short-acting, selective ß1- adrenergic receptor blocker that was originally approved by Japan for the treatment of intraoperative tachyarrhythmias. It has gained attention for its use in the management of tachyarrhythmias and perioperative tachycardia, especially atrial fibrillation for both cardiac and non-cardiac surgeries. It can be the ideal agent for heart rate control due to its high β1‐selectivity, the potent negative chronotropic effect, a limited negative inotropic potential, and an ultrashort elimination half‐life (around 4 min); moreover, it may have a potential therapeutic effect for sepsis and pediatric patients. Landiolol seems to be superior to other short‐acting and selective beta‐blockers such as esmolol. This review aims to provide a comprehensive overview of landiolol, a new ultra-short-acting ß1 selective antagonist, including its pharmacology, clinical applications, efficacy, safety profile, and future directions in research and clinical data.
Keywords:
landiolol
; atrial fibrillation
; beta-blockers
; perioperative tachyarrhythmias
; cardiac surgery
; arrhythmias
1. Introduction
Tachyarrhythmias, the most frequent one being atrial fibrillation (AF), may bring significant risks to patients, especially those with underlying cardiovascular conditions. While various ß-blockers options exist, the need for a rapid and effective intervention has led to the development of ultra-short-acting ß-blocker such as landiolol. This review will explore the pharmacological properties, clinical applications, potential benefits, challenges, and perspectives of landiolol in the management of tachyarrhythmias.
Atrial fibrillation, whose mechanism consists of a concept using Coumel’s Triangle that requires a trigger for initiation, a catalyst agent, and an arrhythmogenic substrate for the perpetuation and maintenance of the trigger, increases heart rate (HR), oxygen consumption and implicates the loss of atrial systole, which will bring a poorer prognosis for frail patients, such as perioperative patients. This required the study and development of a ß -blocker such as landiolol, which has been primarily studied and utilized in the management of tachyarrhythmias, not only AF but also atrial flutter (AFL), because of its rapid onset and offset of action. In this way, it is the perfect candidate for acute situations, where immediate HR control is required [1,2].
Several clinical studies have demonstrated the efficacy of landiolol in controlling HR in patients with tachyarrhythmias. Its rapid onset of action and short half-life allow for precise titration to control HR control without the risk of prolonged ß-blockade. Landiolol has shown favorable safety and tolerability profiles, with minimal negative inotropic effects, making it suitable for patients with compromised cardiac function. Compared with esmolol, another intravenous ß-blocker, the high β1 selectivity (β1/β2 ratio of 255:1) of landiolol allows it to bring a more rapid HR decrease, avoiding in the same time, the decreases in mean arterial blood pressure (BP). That is the reason, landiolol has been also found useful in left ventricular dysfunction patients and fatal arrhythmia requiring emergency treatment [3].
A meta-analysis showed landiolol is effective in the prevention of AF after cardiac surgery (especially coronary artery bypass grafting) and without increasing the risk of major complications. Also, this ß-blocker can manage postoperative atrial fibrillation (POAF) in non-cardiac surgeries, such as esophagectomy. Ojima et al., showed that administration of landiolol 3 μg/kg/ min from the first postoperative day in patients who had an esophagectomy, may reduce the incidence of POAF (landiolol: 30% vs placebo: 10%, p=0.012), postoperative complications (landiolol: 40% vs placebo: 60%, p=0.046) and even the reduction of IL-6 cytokine, which is a promotor for inflammation [4].
Regarding percutaneous coronary intervention, another study showed that using 3 μg/kg/min may be an independent predictor of an ST-segment resolution and may prevent Killip class grade progression without important cardiac complications, such as severe bradycardia, hypotension, or atrioventricular block [5,6].
In septic patients, it is known that tachycardia is associated with a poor outcome and the use of catecholamine vasopressor may increase cardiac adverse events; that is why a β-adrenergic blocker could significantly decrease mortality, by preserving HR and heart load. Landiolol can be the ideal solution in this case, especially for its ability to decrease serum levels of TNF-α and IL-6 in rat models, according to Seki et al. [7,8].
Landiolol may be also used to control HR in pediatric patients with non-arrhythmic sinus tachycardia, heart failure, and pulmonary hypertension. According to Schroeder et al., landiolol administration is well tolerated and safe in pediatric patients, being able to achieve a quick HR control; it is associated with an improvement of ventricular dysfunction and pulmonary hypertension severity in critically ill infants [9].
2. Overview of Pharmacodynamics and Pharmacokinetics in Comparison with Other ß-Blockers
Landiolol hydrochloride is an ultra-short-acting ß1-adrenergic receptor blocker with a rapid onset and offset of action. It exerts its effects by competitively blocking ß1-adrenergic receptors, leading to a reduction in HR, myocardial contractility, and conduction velocity. It specifically targets the beta-1 adrenergic receptors, which are predominantly found in the myocardium, in this way competing with endogenous catecholamines (epinephrine and norepinephrine). Following the blockade of ß-adrenergic receptors, several intracellular molecules and signaling pathways are affected (as shown in Figure 1):
1. G protein-coupled receptor signaling: ß-1 adrenergic receptors are G protein-coupled receptors, meaning that their activation leads to the activation of intracellular signaling pathways through G proteins. When catecholamines (e.g., epinephrine and norepinephrine) bind to ß -1 receptors, they activate stimulatory G proteins, leading to the production of cyclic adenosine monophosphate (cAMP) from adenosine triphosphate by the enzyme adenylyl cyclase.
2. cAMP production: Cyclic AMP, a second messenger, plays a central role in mediating the effects of ß -adrenergic receptor activation. Increased levels of cAMP lead to the activation of protein kinase A (PKA), a key enzyme involved in regulating cellular function. PKA phosphorylates a variety of target proteins, leading to changes in cellular function and gene expression, one of the major intracellular effects of ß-1 receptor activation being the regulation of intracellular calcium levels in cardiac myocytes. Activation of ß-1 receptors leads to an increase in intracellular calcium levels through several mechanisms, including enhanced calcium release from the sarcoplasmic reticulum and increased calcium entry through L-type calcium channels in the cell membrane. The increase in intracellular calcium levels and the subsequent activation of PKA through the ryanodine receptor 2, sarcoplasmic/endoplasmic reticulum calcium ATPase 2 and phospholamban lead to enhanced contractility and increased HR in cardiac myocytes [10].
When ß-blockers like landiolol block ß-1 receptors, they interfere with all of these intracellular signaling pathways. Specifically, the inhibition of ß-1 adrenergic receptors leads to reduced cAMP production, decreased activation of PKA, and altered calcium handling in cardiac myocytes, which will create (detailed in Table 1)[11]:
- A negative bathmotropic effect (by blocking INa channels responsible for the rapid depolarization phase of the cardiac action potential).
- A negative dromotropic effect (it decreases the speed of impulse conduction through the atrioventricular node by blocking especially IKs channels).
- A negative chronotropic effect (blocking the ß-1 receptors in the sinoatrial node and modulating the activity of various ion channels, including If- funny current).
- A negative inotropic effect: due to its blockade of the ß-1 receptors in the myocardium and in this way blocking the release of calcium, necessary for cardiomyocyte contraction.
- An antiarrhythmic effect: due to its suppression of triggered activity and prolongation of refractory period by blocking IKs channels. In this way, it may help prevent the re-entry of electrical impulses that can lead to certain types of arrhythmias such as AF, AFL, atrioventricular re-entry tachycardia, or atrioventricular nodal reentry tachycardia [12].
Compared to other ß-blockers, landiolol has a unique pharmacokinetic profile, characterized by its short half-life of approximately 4 minutes, which allows for rapid titration and termination of its effects. It distinguishes it from other ß-blockers in terms of pharmacodynamics and pharmacokinetics (detailed in Table 2).

Table 2.
An overview of Landiolol in comparison with other beta-blockers.
| Property | Landiolol[13] | Esmolol[13] | Metoprolol[14] | Nebivolol[15] | Bisoprolol[15] | Atenolol[16] | Carvedilol[17] | Propranolol[18] |
| Drug class | Ultra-short-acting selective ß-1 blocker | Short-acting selective ß-1 blocker | Selective ß -1 blocker | Highly cardio selective ß -1 blocker with vasodilator properties | Highly cardio-selective ß -1 blocker | Cardio selective ß -1 blocker | Non-selective ß blocker with alpha-1 blocking activity | Non-selective ß blocker |
| Half-life | Very short (about 4 minutes) | Very short (about 9 minutes) | 3-7 hours | 10-12 hours |
10-12 hours |
6-7 hours |
7-10 hours |
4-6 hours |
| Pharmacokinetics | Rapid onset and offset of action | Rapid onset and offset of action | Rapidly and completely absorbed | Absorbed rapidly and extensively metabolized | Slowly and completely absorbed | Absorbed slowly but almost completely | Extensive l y metabolized | Rapidly and completely absorbed |
| Pharmacodynamics | Selective ß1-blocker, short-acting |
Selective ß1-blocker, short-acting |
Selective ß1-blocker, long-acting |
ß1-blocker with vasodilator effects | Selective ß1-blocker, long-acting |
Selective ß1-blocker, long-acting |
Non-selective ß-blocker with ß1-blockade |
Non-selective ß-blocker, membrane-stabilizing activity |
| Cardio selectivity | Highly | Highly | Highly | Highly with vasodilator properties | Highly | Highly | Non-selective | Non-selective |
| Dose Range | 1-40 μg/kg/min | 50-300 μg/kg/min |
25-200 mg/day |
2.5-10 mg/day |
2.5-10 mg/day |
25-100 mg/day |
6.25-25 mg/day |
20-320 mg/day |
| Vasodilator effects | Minimal | Minimal | Minimal | Significant | Minimal | Minimal | Strong | Minimal |
| Indications | Rapid heart rate control in critical care settings | Acute heart rate control, intraoperative and postoperative tachycardia | Hypertension, angina, heart failure, post-myocardial infarction | Hypertension, angina, heart failure | Hypertension, angina, heart failure | Hypertension, angina, arrhythmias | Hypertension, angina, heart failure | Hypertension, angina, arrhythmias |
| Adverse effects | Rarely Hypotension, bradycardia, | Hypotension, bradycardia, bronchospasm | Hypotension, bradycardia, fatigue, dizziness | Hypotension, bradycardia, fatigue, dizziness, headache | Hypotension, bradycardia, fatigue, dizziness | Hypotension, bradycardia, fatigue, dizziness | Hypotension, bradycardia, fatigue, dizziness, heart block | Hypotension, bradycardia, fatigue, dizziness, bronchospasm |
| Contraindication | Severe bradycardia, heart block | Heart block, severe bradycardia, heart failure, asthma | Bradycardia, heart block, heart failure, hypotension | Severe bradycardia, heart block, hepatic impairment | Heart block, severe bradycardia, heart failure, asthma | Bradycar dia, heart block, heart failure, asthma | Asthma, heart block, severe bradycard ia | Asthma, heart block, bradycardia |
Regarding pharmacodynamics, it is more cardio-selective than many other ß-blockers, having a greater affinity for ß-1 adrenergic receptors relative to ß-2 receptors. This selectivity may result in a decreased risk of bronchoconstriction in patients with asthma or chronic obstructive pulmonary disease compared to non-selective ß-blockers. Then, it has rapid onset and short duration of action making it suitable for rapid titration and discontinuation as needed. This is in contrast to other ß-blockers, which often have longer half-lives and durations of action.
Regarding pharmacokinetics, landiolol undergoes rapid metabolism by esterase in the tissues rather than by the liver, leading to its short half-life (about 4 minutes). This rapid metabolism allows for quick clearance from the body, making it suitable for use in situations where rapid titration or discontinuation is necessary. It is primarily eliminated renally, and its rapid clearance contributes to its short duration of action. Other ß-blockers, such as metoprolol and propranolol, are predominantly eliminated through hepatic metabolism and have longer half-lives. Moreover, due to its rapid metabolism, landiolol has limited penetration into tissues and organs, which may contribute to its shorter duration of action and decreased potential for systemic side effects compared to other ß-blockers [13].
Recent studies showed also the anti-ischemic, anti-inflammatory, antioxidant, and cardioprotective effects of landiolol: PASCAL, PLATON, and BABYLON trials sustained significantly decreased levels of biomarkers for both inflammation, such as interleukin-6 and -8, high-sensitive C-reactive protein and for myocardial ischemia, such as creatine kinase isoenzyme MB, troponin-I and human heart fatty acid binding protein [19,20,21].
Another study claims the ability to attenuate acute lung injury and cardiac dysfunction in a rat model of endotoxin-induced sepsis. Co-treatment with landiolol protected against acute lung injury and cardiac dysfunction in a rat model of lipopolysaccharide-induced systemic inflammation. The treatment was associated with a significant reduction in serum levels of the inflammation mediator high-mobility group and histological lung damage [22].
Landiolol stands out from other ß-blockers due to its rapid onset, short duration of action, cardioselectivity, rapid metabolism, and renal elimination. These unique pharmacodynamics and pharmacokinetic properties make it a valuable option in certain clinical scenarios, such as for the management of acute tachyarrhythmias or perioperative tachycardia such as POAF, but it seems that other properties such as anti-ischemic, anti-inflammatory, and antioxidant effects make it also useful in other situations (sepsis, pediatric patients).
3. The Use of Landiolol in Clinical Practice
Landiolol, with a half-life of 3-4 minutes, is a β1 blocker characterized as an ultra-short-acting agent. It has received approval in Japan for addressing sinus tachycardia, AFL, and AF. In terms of cardioselectivity, landiolol hydrochloride demonstrates a high degree (β1/β2=255) in comparison to esmolol (β1/β2 = 33) or propranolol (β1/β2 = 0.68). For the reasons mentioned earlier, landiolol could be an appealing substitute for long-acting β-blockers in both the perioperative environment and among critically ill patients [13].
3.1. Postoperative Atrial Fibrillation Prevention and Treatment in Cardiac Surgery
Atrial fibrillation is among the most common complications following heart surgery, with an estimated incidence ranging from 16% to 85% [21]. This potentially life-threatening complication is linked to heightened risks of adverse neurological events, congestive heart failure, perioperative heart failure, myocardial infarction, prolonged length of hospitalization, and higher hospital costs [23]. It poses challenges in the postoperative period and has an impact on the long-term mortality of patients [21]. Sympathetic activation or an exaggerated response to adrenergic stimulation serves as a significant trigger for POAF [23]. β-blockers play a crucial role in both preventing and treating postoperative AF [23]. In this regard, the European Society of Cardiology, in conjunction with the American Heart Association, the American College of Cardiology, and the American College of Chest Physicians, advocates employing β-blockers to prevent AF in patients undergoing cardiac surgery [24,25].
One meta-analysis that incorporated thirty-three studies and encompassed a total of 4698 participants who underwent cardiac surgery, examined the impact of β-blockers on POAF. These results indicated a noteworthy reduction in POAF within the group that received β-blockers (16.3%) compared to the placebo group (31.7%) (OR 0.33; 95% CI 0.26 to 0.43; I2 = 55%) [26]. Moreover, in another recent systematic review involving 688 patients, it was revealed that administering β-blockers before elective cardiac surgery resulted in a notable reduction in the risk of POAF. Additionally, this preoperative intervention had an impact on the risk of stroke and all-cause mortality [27].
Recent research indicates that the intravenous administration of an ultra-short-acting β-blocker, like landiolol, is associated with a reduced likelihood of developing AF following cardiac surgery.
The PASCAL study was undertaken to assess the effectiveness of intravenous landiolol treatment in preventing POAF. The study comprised 140 patients undergoing coronary artery bypass grafting. Within the landiolol group, AF occurred in 7 patients (5%), whereas in the placebo group, the incidence of AF was observed in 24 patients (34.3%) [20]. Furthermore, the group treated with landiolol exhibited a decrease in inflammatory and ischemic parameters. It can be concluded that the inhibition of sympathetic hypertonia by landiolol led to a reduction in the incidence rate of AF [20].
The PELTA study, conducted from 2010 to 2014, involved 150 consecutive patients aged over 70 who underwent cardiovascular surgery for valvular, ischemic heart disease, and aortic disease. These patients were divided into three groups: Group 1 (landiolol at 1 μg/kg/min), Group 2 (landiolol at 2 μg/kg/min), and the control group (no landiolol). Landiolol hydrochloride was administered intravenously for a period of 4 days postoperatively. Continuous electrocardiography monitoring took place throughout the study, and cardiologists subsequently assessed whether AF occurred postoperatively. AF was observed in 24.4% of patients in the control group, 18.2% of patients in Group 1, and 11.1% of patients in Group 2. The conducted statistical analysis revealed a clear correlation between the incidence of POAF and the dosage of landiolol. This suggests that a higher dose of landiolol might be more efficacious in preventing the occurrence of AF following cardiac surgery [28].
Studies assessing the effectiveness of landiolol in preventing AF after cardiovascular surgery have been conducted across various patient profiles. One such study, the PLATON study, involved 60 patients with a preoperative left ventricular ejection fraction of less than 35% [19]. Among these patients, AF occurred in 10% of those treated with landiolol, as opposed to 40% in those without landiolol (p = 0.002). Additionally, the study group exhibited lower levels of brain natriuretic peptide and ischemic biomarkers, along with a shorter duration of hospitalization. The study concludes that utilizing a low dose (1 mcg/kg/min) of landiolol is both safe and beneficial for patients with left ventricular dysfunction. This approach proves effective in preventing episodes of AF that may occur after cardiac surgery [19].
A meta-analysis conducted by Hao et al. affirms the positive impact of landiolol in preventing AF in patients undergoing cardiac surgery. Furthermore, the analysis notes favorable effects in terms of fewer adverse events associated with landiolol use. Additionally, the administration of landiolol to prevent AF after cardiac surgery was found to reduce mortality in comparison to using landiolol for treating AF after cardiac surgery [29].
When compared to other active substances, landiolol was found to be more effective and safer for administration in patients with POAF. A study conducted in Japan investigated the effects of landiolol compared to diltiazem in patients who developed AF after heart surgery. Out of a total of 335 patients, 71 experienced AF. The conversion to sinus rhythm (SR) occurred in 54.3% of patients treated with intravenous landiolol, in contrast to 30.6% of patients treated with diltiazem. Furthermore, hypotension and bradycardia, as side effects, were less common in the group of patients receiving landiolol [30].
In all the above studies, landiolol was well tolerated, with minimal adverse effects, and a low incidence of hypotension, bradycardia, or respiratory symptoms, which did not require stopping treatment or lowering the dose. Thus, landiolol proved to be a β-blocker with a well-established safety profile [31].
3.2. Postoperative Atrial Fibrillation Prevention and Treatment in Non-Cardiac Surgery
The reasons behind AF occurrence after thoracic or gastrointestinal surgery remain uncertain, but potential contributors may involve the combined impact of heightened vagal tone, hypoxemia, pulmonary hypertension, atrial inflammation, and right heart dilation. Risk factors for POAF encompass factors related to both the patient and the surgical procedure itself, with AF carrying the potential to give rise to additional severe complications [4,32].
Individuals undergoing lung resection and experiencing AF also face additional challenges related to pulmonary complications, such as acute respiratory failure or pneumonia. These complications contribute to an elevated risk of both mortality and morbidity [33]. Additionally, POAF extends the duration of hospitalization, accompanied by an associated rise in costs [32]. There is a limited number of studies assessing the efficacy of landiolol in preventing [4,34,35,36,37] and treating [32,33,38,39] AF following non-cardiac surgery.
Due to its very short action time and significant cardioselectivity, with minimal action on alpha receptors, landiolol can be used in patients with respiratory diseases [40]. Considering these factors, Nakano et al. explored the utility and effectiveness of using landiolol in cases of AF following pulmonary resection. The continuous intravenous infusion of landiolol resulted in a reduction of HR in these individuals from 135 ± 24 bpm to 85 ± 19 bpm (p<0.0001), with 56% of patients experiencing a conversion to SR [32] (Table 3).
Table 3.
Studies that used landiolol for the treatment of post-operatory atrial fibrillation in non-cardiac surgery.
Table 3.
Studies that used landiolol for the treatment of post-operatory atrial fibrillation in non-cardiac surgery.
| Study name | Type of surgery | Number of patients | Design study | Outcomes |
|---|---|---|---|---|
| Nojiri et al.[33] | Lung surgery | 30 |
Study group (n=15) – landiolol 5 mcg/kg/min or 10 mcg/kg/min Control group (n=15) – 0.25 mg digoxin and 5 mg verapamil |
Rate of conversion to SR: Study group: at 2 h: 8/15 (53%) at 12 h 11/15 (73%) Control group: at 2 h: 3/15 (20%) at 12 h 8/15 (53%) Time of conversion to SR: Study group: 8.1± 11.0 h Control group: 23.0 ± 26.0 h |
| Niwa et al.[39] | Esophagectomy | 24 |
Study group (n=11) – landiolol 6.5 ± 3.4 mcg/kg/min, increased to 7.7 ± 4.4 mcg/kg/min Control group (n=13) – digoxin and calcium channel blockers. |
Rate of conversion to SR: Study group: at 2 h 5/8 (62.5%) at 12 h 8/8 (100%) Control group: at 2 h: at 2 h 1/13 (7.7%) at 12 h 7/13 (53.8%) Time of conversion to SR: Study group: 3.6 6 ±6.6 h Control group: 23.3 ± 5.2 h |
| Mori et al.[38] | Esophagectomy | 74 | Study group (n=13) – landiolol 0.01 mg/kg/min increased to 0.04 mg/kg/min | Rate of conversion to SR: 10/13 (77%) |
| Nakano et al.[32] | Pulmonary resection | 25 | Study group (n=25) - landiolol 5–10 mcg/kg/min or o 1–5 mcg/kg/min |
Rate of conversion to SR: 14/25 (56%) – at 1 h 4/14 (28.6%) and at 12 h 5/14 (35.7%) HR control: from 135 ± 24 bpm to 85 ± 19 bpm |
SR: sinus rhythm; HR: heart rate.
In another study, the effectiveness of landiolol treatment was assessed in comparison to the standard approach for managing AF following pulmonary resection. The study revealed a significant reduction in HR within the landiolol-treated group compared to the control group. Additionally, the time taken for the restoration of SR was significantly shorter in the landiolol-treated group. Furthermore, there were no statistically significant differences in BP between the two groups, and no need for discontinuation of treatment due to adverse effects was observed [33].
Two other studies exploring the impact of landiolol hydrochloride on treating AF after thoracic surgery have yielded consistent findings. Landiolol has demonstrated superiority over traditional therapy in effectively managing HR and facilitating the restoration of SR [38,39].
Landiolol has also been used successfully to prevent the onset of AF after non-cardiac surgery. In a double-blind, randomized trial involving 100 cancer patients undergoing esophageal surgery, landiolol was administered for the prevention of AF. In patients receiving landiolol for prophylaxis, AF occurred in 5 (10%), whereas in the control group, 15 patients (30%) experienced AF. Moreover, in the landiolol group, HR was significantly lower than in the placebo group [41]. Comparable outcomes were noted in patients undergoing lung resection. Administering a low dose of landiolol at 5 mcg/kg/min before the induction of general anesthesia and maintaining it until discharge from the intensive care unit led to a notable reduction in HR. Notably, in this study, the initiation of AF was entirely prevented, with no patients in this group experiencing this tachyarrhythmia [34].
Okita et al. conducted a study comparing a group that received landiolol before lung resection surgery to a control group without AF prophylaxis. The incidence of AF after landiolol prophylaxis was 5.2%, while the control group had a higher percentage at 14.2%. Risk factors linked to AF occurrence included older age, ischemic heart failure, longer surgery duration, and lymph node removal. Importantly, the administration of landiolol did not lead to a significant reduction in BP or marked bradycardia [37].
3.3. Treatment of Atrial Fibrillation in Patients with Cardiac Dysfunction
Heart failure (HF) and AF frequently coexist, contributing to the deterioration of cardiac function and jeopardizing hemodynamic stability. Acute HF results from the loss of atrial contraction, a rapid ventricular contraction rate, left ventricular underfilling, and increased left atrial pressures[42]. The prevalence of AF in patients with acute HF ranges from 25% to 40%. Its presence exacerbates symptoms, resulting in adverse outcomes, prolonged hospital stays, and increased mortality [42].
To address the necessity for HR control, the guidelines for HF recommend β-blocker treatment for patients with reduced ejection fraction (EF) or mild reduced EF [43]. Landiolol has been shown to be an interesting option in patients with cardiac dysfunction and AF [42]. The Japanese Circulation Society advocates for the use of landiolol, along with bisoprolol or carvedilol, as the primary treatment for controlling HR in AF (Class IB), for patients with HF, particularly in cases without an accessory pathway [44,45].
In a prospective, multicenter study comparing landiolol to digoxin (J-Land study), it was observed that a dosage ranging from 1-10 mcg/kg/min of landiolol proved more effective in patients with AF or AFL and an EF of 25-50% compared to digoxin. In nearly half of the patients, a decrease in HR exceeding 20% and achieving an HR below 110 bpm were accomplished within 2 hours following the administration of landiolol. In contrast, the digoxin group exhibited this therapeutic success in only 13.9% of patients [46].
A recent study conducted retrospectively across multiple medical centers, examined 39 patients with HF with left ventricle ejection fraction (LVEF) between 34 ± 16% and rapid AF, AFL, or atrial tachycardia. Intravenous landiolol led to a significant reduction in HR by approximately 40% from the initial level in 29 individuals and 9 of them experienced spontaneous termination of AF after receiving landiolol. In these patients, a higher initial LVEF was identified as a positive indicator of the effectiveness and safety of landiolol [47].
In a prospective study involving 101 patients experiencing acute decompensated heart failure classified as NYHA class IV, with an ejection fraction below 40%, associated AF, the use of landiolol was associated with a reduced risk of cardiac death, deterioration of renal function, and extended hospital stays. A better prognosis among these patients was correlated with lower left ventricular volume and high mean BP [48].
A recent study investigated the effectiveness of combining landiolol treatment with milrinone in nine patients experiencing acute decompensated heart failure with an ejection fraction ranging from 28% to 8%, with a “wet and cold” phenotype and rapid AF. Positive outcomes were noted with low doses of landiolol, which not only lowered HR by 11% without affecting systolic BP but also led to a reduction in pulmonary capillary wedge pressure and an increase in stroke volume index. However, higher doses of 3 mcg/kg/min landiolol in conjunction with milrinone were linked to decreased BP, stroke volume index, and cardiac index [49].
3.4. Treatment of Sepsis-Related Atrial Fibrillation
Cardiovascular abnormalities occurring in sepsis may be due to changes in circulating volume, venous tone, and tachycardia, all of which can lead to impaired cardiac function and changes in HR [50]. Sepsis can trigger tachyarrhythmias like AF due to heightened sympathetic system activity and elevated inflammatory cytokine levels. Once AF sets in, the prognosis for patients becomes even more uncertain [51]. An improved prognosis is associated with reducing the ventricular rate to less than 95 beats per minute within 24 hours of occurrence in a patient with sepsis [50]. Several studies in the literature have highlighted the effectiveness of using the β-blocker treatment landiolol in patients experiencing AF during episodes of sepsis.
A study involving 61 septic patients admitted to the intensive care unit (ICU) with AF/AFL (39 receiving landiolol and 22 not receiving landiolol) revealed notable differences between the two study groups. With an initial dose of 6.3 ± 3.3 g/kg/min, the HR significantly decreased in the landiolol group during the first hour from 145 ± 14 bpm to 119 ± 28 bpm, with no occurrence of hypotension or severe bradycardia. Conversely, there were no changes in HR observed in the control group. In the landiolol group, 25.6% of patients converted to SR, while none in the control group returned to SR [44]. The study concludes that, in patients experiencing sepsis and AF/AFL, the administration of a low dose of landiolol can effectively decrease HR and facilitate the conversion to SR. This intervention maintains a good safety profile, avoiding the induction of hypotension or reduction in cardiac output [44].
In another recent multicenter, randomized study, a total of 151 patients admitted to the intensive care unit for sepsis and subsequently developing AF or AFL during hospitalization were included. Landiolol significantly lowered the HR in 55% of patients to a range of 60-94/min within 24 hours and considerably lowered the likelihood of a recurrence of arrhythmia. Additionally, among patients in whom the HR was successfully reduced, the 28-day mortality was lower (9% vs. 24%) [50].
The beneficial effects of β-blockers stem from their pleiotropic action, leading to the modulation of inflammation, protection of cardiomyocytes, and enhanced organ function[52].
4. Challenges and Perspectives
In clinical trials currently documented in the literature, the use of landiolol was found to be safe and well-tolerated. The most frequently reported side effects after landiolol treatment are hypotension and bradycardia [53].
In clinical trials, the prevalence of hypotension in the landiolol group (n = 948), active comparator, no landiolol, and placebo cohorts was 8.5%, 8.5%, 5.7%, and 2.1%, respectively. The frequency of bradycardia was 2.1%, 2.5%, 2.4%, and 0%. In uncontrolled trials, hypotension and bradycardia manifested in 8.6% and 0.5% of 581 recipients of landiolol. Nevertheless, in post-marketing investigations (n = 1257), the frequency of hypotension was comparably lower (0.8%), with bradycardia documented in 0.7% of patients. All instances of hypotension and bradycardia either ameliorated or resolved spontaneously without any intervention or within minutes after discontinuation of landiolol, with or without additional treatment [53].
Some studies have reported noteworthy adverse effects. For instance, in a patient experiencing substantial active bleeding, severe hypotension after landiolol treatment led to shock. Discontinuation of landiolol was necessary to improve the patient’s condition. Additional significant complications post-landiolol treatment have been documented, particularly in elderly patients or those with other cardiovascular pathologies, such as cardiac arrest and complete atrioventricular block [53]. The primary drawbacks of this β-blocker lie in its negative inotropic and chronotropic properties, which stem from reduced sympathetic activity. These properties may lead to a deceleration of atrioventricular activity [13].
In some cases, landiolol treatment has been responsible for worsening heart failure, or the development of pneumonia [54]. Several alterations in laboratory parameters, including elevated ALT, AST, and bilirubin, have been noted in patients treated with landiolol. However, these changes did not exhibit significant clinical manifestations and were subsequently resolved [46,53]. Other adverse effects reported in the literature are shown in Table 4.
Table 4.
Adverse effects reported with landiolol treatment.
| Hypotension [19,28,47,48,55,56] | Dyspnea [55] |
| Bradycardia [48,55,57] | Asthma [46] |
| Aggravation of cardiac failure [48,50,55] | Hypokalemia [54] |
| Ventricular tachycardia [55] | Hypoglycemia [54] |
| Complete atrioventricular block [48,53] | Hepatic enzyme increased [53,54] |
| Cardiorespiratory arrest [50,55] | Gamma-glutamyl transferase [54] |
| Cardiogenic shock [53,55] | Blood uric acid increased [54] |
| Embolic stroke [46] | Blood alkaline phosphatase increased [54] |
| Pneumonia [33,55] | Increased serum creatinine [48,56] |
| Respiratory failure [33,55] | Vomiting and nausea [46] |
AF can arise from multiple factors, including associated comorbidities, surgical trauma, ischemia, and reperfusion during surgery, as well as electrical and pressure changes at the atrial level. However, compelling evidence suggests that inflammation and oxidative stress play significant roles in the development of AF [58]. Landiolol showed a protective effect on lipopolysaccharide (LPS)-induced systemic inflammation model in an animal study, being associated with a decrease of high mobility group box-1 protein (HMGB-1) and decreasing interleukin-6 (IL-6) levels and inhibiting tumor necrosis factor-alpha (TNF-alpha) levels [58,59]. The animal model demonstrated that landiolol’s anti-inflammatory effect extends to the inhibition of the inflammatory and vasoconstrictor peptide endothelin (ET) 1 [60]. These data emphasize the anti-inflammatory effects of landiolol, through which it helps prevent AF. However, evidence is limited, so further studies are needed to investigate this effect.
5. Conclusion
Landiolol, a new ultra-short-acting ß1 selective antagonist, shows promise in various clinical scenarios, ranging from cardiac and non-cardiac surgeries to preventing and treating AF, in the presence of heart failure or sepsis. While its ultra-short-acting nature provides advantages in specific settings, careful consideration of potential adverse effects is crucial. Further research is needed to explore its anti-inflammatory effects and fully understand its role in preventing AF. Despite challenges, landiolol presents itself as a valuable tool in managing specific cardiac conditions in clinical practice.
Author Contributions
Conceptualization, A.F.O., P.C.M., D.M.T., V.S. and M.F.; methodology, A.B., M.F. and D.M.T.; software, A.F.O., D.E.I., C.S.S., M.C.; validation, G.L.B., D.E.I. and M.F.; formal analysis, A.B., V.S., C.P.C.; investigation, A.F.O. and P.C.M.; resources, D.E.I.; data curation, G.L.B.; writing—original draft preparation, A.F.O. and P.C.M.; writing—review and editing, A.F.O., P.C.M. and M.F.; visualization, D.M.T., V.S., C.P.C., C.S.S., M.C. and M.F.; supervision, D.M.T., A.B., C.P.C., V.S.
Funding
This research received no external funding.
Data Availability Statement
Non applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Oancea, A.F.; Jigoranu, R.A.; Morariu, P.C.; Miftode, R.-S.; Trandabat, B.A.; Iov, D.E.; Cojocaru, E.; Costache, I.I.; Baroi, L.G.; Timofte, D.V.; et al. Atrial Fibrillation and Chronic Coronary Ischemia: A Challenging Vicious Circle. Life 2023, 13, 1370. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, A; Kobayashi, Y; Katsube,T. Effect of Landiolol for Atrial Fibrillation after Open Heart Surgery. The Japanese Journal of Thoracic Surgery 2023, 75, 339–342.
- Kinjo, T.; Kimura, M.; Kaname, N.; Horiuchi, D.; Itoh, T.; Ishida, Y.; Nishizaki, K.; Toyama, Y.; Sasaki, S.; Tomita, H. Landiolol, an Intravenous Β1-selective Blocker, Is Useful for Dissociating a Fusion of Atrial Activation via Accessory Pathway and Atrioventricular Node. J Arrhythm 2023, 39, 937–946. [Google Scholar] [CrossRef] [PubMed]
- Ojima, T.; Iwahashi, M.; Nakamori, M.; Nakamura, M.; Katsuda, M.; Iida, T.; Hayata, K.; Yamaue, H. Atrial Fibrillation after Esophageal Cancer Surgery: An Analysis of 207 Consecutive Patients. Surg Today 2014, 44, 839–847. [Google Scholar] [CrossRef] [PubMed]
- Kiyokuni, M.; Konishi, M.; Sakamaki, K.; Kawashima, C.; Narikawa, M.; Doi, H.; Iwata, K.; Tomari, S.; Nakayama, N.; Komura, N.; et al. Beneficial Effect of Early Infusion of Landiolol, a Very Short-Acting Beta-1 Adrenergic Receptor Blocker, on Reperfusion Status in Acute Myocardial Infarction. Int J Cardiol 2016, 221, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Hoshi, T.; Sato, A.; Nishina, H.; Kakefuda, Y.; Wang, Z.; Noguchi, Y.; Aonuma, K. Acute Hemodynamic Effects of Landiolol, an Ultra-Short-Acting Beta-Blocker, in Patients with Acute Coronary Syndrome: Preliminary Study. J Cardiol 2012, 60, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Morelli, A.; Ertmer, C.; Westphal, M.; Rehberg, S.; Kampmeier, T.; Ligges, S.; Orecchioni, A.; D’Egidio, A.; D’Ippoliti, F.; Raffone, C.; et al. Effect of Heart Rate Control With Esmolol on Hemodynamic and Clinical Outcomes in Patients With Septic Shock. JAMA 2013, 310, 1683. [Google Scholar] [CrossRef] [PubMed]
- Seki, Y.; Jesmin, S.; Shimojo, N.; Islam, Md.M.; Rahman, Md.A.; Khatun, T.; Sakuramoto, H.; Oki, M.; Sonobe, A.; Kamiyama, J.; et al. Significant Reversal of Cardiac Upregulated Endothelin-1 System in a Rat Model of Sepsis by Landiolol Hydrochloride. Life Sci 2014, 118, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, L.; Monno, P.; Unger, M.; Ackerl, J.; Shatilova, O.; Schmitt, J.; Dresbach, T.; Mueller, A.; Kipfmueller, F. Heart Rate Control with Landiolol Hydrochloride in Infants with Ventricular Dysfunction and Pulmonary Hypertension. ESC Heart Fail 2023, 10, 385–396. [Google Scholar] [CrossRef]
- Chalkias, A.; O’Donnell, E.P. Mechanisms of Landiolol-Mediated Positive Inotropy in Critical Care Settings. Eur J Clin Pharmacol 2023, 79, 1607–1612. [Google Scholar] [CrossRef]
- Oliver, E.; Mayor Jr, F.; D’Ocon, P. Beta-Blockers: Historical Perspective and Mechanisms of Action. Revista Española de Cardiología (English Edition) 2019, 72, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Grandi, E.; Ripplinger, C.M. Antiarrhythmic Mechanisms of Beta Blocker Therapy. Pharmacol Res 2019, 146, 104274. [Google Scholar] [CrossRef] [PubMed]
- Poveda-Jaramillo, R.; Monaco, F.; Zangrillo, A.; Landoni, G. Ultra-Short–Acting β-Blockers (Esmolol and Landiolol) in the Perioperative Period and in Critically Ill Patients. J Cardiothorac Vasc Anesth 2018, 32, 1415–1425. [Google Scholar] [CrossRef] [PubMed]
- Morris J; Awosika AO; Dunham A Metoprolol. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2023.
- AlHabeeb, W.; Mrabeti, S.; Abdelsalam, A.A.I. Therapeutic Properties of Highly Selective β-Blockers With or Without Additional Vasodilator Properties: Focus on Bisoprolol and Nebivolol in Patients With Cardiovascular Disease. Cardiovasc Drugs Ther 2022, 36, 959–971. [Google Scholar] [CrossRef] [PubMed]
- Kirch, W.; Görg, K.G. Clinical Pharmacokinetics of Atenolol — A Review. Eur J Drug Metab Pharmacokinet 1982, 7, 81–91. [Google Scholar] [CrossRef] [PubMed]
- Wisler, J.W.; DeWire, S.M.; Whalen, E.J.; Violin, J.D.; Drake, M.T.; Ahn, S.; Shenoy, S.K.; Lefkowitz, R.J. A Unique Mechanism of β-Blocker Action: Carvedilol Stimulates β-Arrestin Signaling. Proceedings of the National Academy of Sciences 2007, 104, 16657–16662. [Google Scholar] [CrossRef] [PubMed]
- Lewis, P. The Essential Action of Propranolol in Hypertension. Am J Med 1976, 60, 837–852. [Google Scholar] [CrossRef] [PubMed]
- Sezai, A.; Osaka, S.; Yaoita, H.; Ishii, Y.; Arimoto, M.; Hata, H.; Shiono, M. Safety and Efficacy of Landiolol Hydrochloride for Prevention of Atrial Fibrillation after Cardiac Surgery in Patients with Left Ventricular Dysfunction: Prevention of Atrial Fibrillation after Cardiac Surgery with Landiolol Hydrochloride for Left Ventricular Dysfunction (PLATON) Trial. Journal of Thoracic and Cardiovascular Surgery 2015, 150, 957–964. [Google Scholar]
- Sezai, A.; Minami, K.; Nakai, T.; Hata, M.; Yoshitake, I.; Wakui, S.; Shiono, M.; Hirayama, A. Landiolol Hydrochloride for Prevention of Atrial Fibrillation after Coronary Artery Bypass Grafting: New Evidence from the PASCAL Trial. J Thorac Cardiovasc Surg 2011, 141, 1478–1487. [Google Scholar] [CrossRef]
- Sezai, A.; Nakai, T.; Hata, M.; Yoshitake, I.; Shiono, M.; Kunimoto, S.; Hirayama, A. Feasibility of Landiolol and Bisoprolol for Prevention of Atrial Fibrillation after Coronary Artery Bypass Grafting: A Pilot Study. J Thorac Cardiovasc Surg 2012, 144, 1241–1248. [Google Scholar] [CrossRef]
- Hagiwara, S.; Iwasaka, H.; Maeda, H.; Noguchi, T. LANDIOLOL, AN ULTRASHORT-ACTING Β1-ADRENOCEPTOR ANTAGONIST, HAS PROTECTIVE EFFECTS IN AN LPS-INDUCED SYSTEMIC INFLAMMATION MODEL. Shock 2009, 31, 515–520. [Google Scholar] [CrossRef]
- Oprea, A.D.; Lombard, F.W.; Kertai, M.D. Perioperative β-Adrenergic Blockade in Noncardiac and Cardiac Surgery: A Clinical Update. J Cardiothorac Vasc Anesth 2019, 33, 817–832. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C.; Conti, J.B.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: Executive Summary. Circulation 2014, 130, 2071–2104. [Google Scholar] [CrossRef] [PubMed]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.-A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the Diagnosis and Management of Atrial Fibrillation Developed in Collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2021, 42, 373–498. [Google Scholar] [CrossRef]
- Arsenault, K.A.; Yusuf, A.M.; Crystal, E.; Healey, J.S.; Morillo, C.A.; Nair, G.M.; Whitlock, R.P. Interventions for Preventing Post-Operative Atrial Fibrillation in Patients Undergoing Heart Surgery. Cochrane Database of Systematic Reviews 2013, 2021. [Google Scholar]
- Thein, P.M.; White, K.; Banker, K.; Lunny, C.; Mirzaee, S.; Nasis, A. Preoperative Use of Oral Beta-Adrenergic Blocking Agents and the Incidence of New-Onset Atrial Fibrillation After Cardiac Surgery. A Systematic Review and Meta-Analysis. Heart Lung Circ 2018, 27, 310–321. [Google Scholar] [CrossRef]
- Sasaki, K.; Kumagai, K.; Maeda, K.; Akiyama, M.; Ito, K.; Matsuo, S.; Katahira, S.; Suzuki, T.; Suzuki, Y.; Kaiho, Y.; et al. Preventive Effect of Low-Dose Landiolol on Postoperative Atrial Fibrillation Study (PELTA Study). Gen Thorac Cardiovasc Surg 2020, 68, 1240–1251. [Google Scholar] [CrossRef] [PubMed]
- Hao, J.; Zhou, J.; Xu, W.; Chen, C.; Zhang, J.; Peng, H.; Liu, L. Beta-Blocker Landiolol Hydrochloride in Preventing Atrial Fibrillation Following Cardiothoracic Surgery: A Systematic Review and Meta-Analysis. Annals of Thoracic and Cardiovascular Surgery 2022, 28, 18–31. [Google Scholar] [CrossRef]
- Sakamoto, A.; Kitakaze, M.; Takamoto, S.; Namiki, A.; Kasanuki, H.; Hosoda, S. Landiolol, an Ultra-Short-Acting Β1-Blocker, More Effectively Terminates Atrial Fibrillation than Diltiazem after Open Heart Surgery: Prospective, Multicenter, Randomized, Open-Label Study (JL-KNIGHT Study). Circulation Journal 2012, 76, 1097–1101. [Google Scholar] [CrossRef]
- Balik, M.; Sander, M.; Trimmel, H.; Heinz, G. Landiolol for Managing Post-Operative Atrial Fibrillation. European Heart Journal Supplements 2018, 20, A10–A14. [Google Scholar] [CrossRef]
- Nakano, T.; Shimizu, K.; Kawashima, O.; Kamiyoshihara, M.; Nagashima, T.; Ibe, T.; Takeyoshi, I. Effect of Landiolol Hydrochloride, an Ultra-Short-Acting Beta 1-Selective Blocker, on Supraventricular Tachycardia, Atrial Fibrillation and Flutter after Pulmonary Resection. J Clin Pharm Ther 2012, 37, 431–435. [Google Scholar] [CrossRef]
- Nojiri, T.; Yamamoto, K.; Maeda, H.; Takeuchi, Y.; Funakoshi, Y.; Maekura, R.; Okumura, M. Efficacy of Low-Dose Landiolol, an Ultrashort-Acting β-Blocker, on Postoperative Atrial Fibrillation in Patients Undergoing Pulmonary Resection for Lung Cancer. Gen Thorac Cardiovasc Surg 2011, 59, 799–805. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Nozaki, M.; Sakamoto, R.; Suzuki, T.; Masuda, R.; Iwazaki, M. Safety of Landiolol Infusion in Patients Undergoing Lung Resection. Open J Anesthesiol 2014, 04, 183–190. [Google Scholar] [CrossRef]
- Aoyama, H.; Otsuka, Y.; Aoyama, Y. Landiolol Infusion during General Anesthesia Does Not Prevent Postoperative Atrial Fibrillation in Patients Undergoing Lung Resection. Gen Thorac Cardiovasc Surg 2016, 64, 735–741. [Google Scholar] [CrossRef]
- Yoshida T; Furukita Y; Yamamoto Y; Nishino T; Inoue S; Morimoto M; Okumura K; Toba H; Yoshida M; Takizawa H; et al. A Randomized, Open Label Study of the Efficacy of Prophylactic 24-h Low-Dose Landiolol for Atrial Fibrillation in Transthoracic Esophagectomy. Esophagus 2017, 14, 97–103.
- Okita, T.; Uji, M.; Shinjo, T.; Morioka, M.; Kumano, H.; Ishimura, N.; Nishiwada, M. [Use of Landiolol Hydrochloride for the Prevention of Atrial Fibrillation after Lung Resection]. Masui 2008, 57, 953–958. [Google Scholar] [PubMed]
- Mori, K.; Yamada, K.; Fukuda, T.; Mitsui, T.; Kitamura, T.; Yamaguchi, D.; Ando, J.; Wada, I.; Nomura, S.; Shimizu, N.; et al. Landiolol Hydrochloride for Early Postoperative Tachycardia after Transthoracic Esophagectomy. Surg Today 2014, 44, 848–854. [Google Scholar] [CrossRef]
- Niwa, Y.; Koike, M.; Iwata, N.; Kobayashi, D.; Tanaka, C.; Fujii, T.; Nakayama, G.; Sugimoto, H.; Fujiwara, M.; Kodera, Y. Effect of Landiolol Hydrochloride on Tachyarrhythmia after Esophagectomy. Hepatogastroenterology 2014, 61, 1546–1551. [Google Scholar]
- Wariishi, S.; Yamashita, K.; Nishimori, H.; Fukutomi, T.; Yamamoto, M.; Radhakrishnan, G.; Sasaguri, S. Postoperative Administration of Landiolol Hydrochloride for Patients with Supraventricular Arrhythmia: The Efficacy of Sustained Intravenous Infusion at a Low Dose☆. Interact Cardiovasc Thorac Surg 2009, 9, 811–813. [Google Scholar] [CrossRef]
- Ojima, T.; Nakamori, M.; Nakamura, M.; Katsuda, M.; Hayata, K.; Kato, T.; Kitadani, J.; Tabata, H.; Takeuchi, A.; Yamaue, H. Randomized Clinical Trial of Landiolol Hydrochloride for the Prevention of Atrial Fibrillation and Postoperative Complications after Oesophagectomy for Cancer. British Journal of Surgery 2017, 104, 1003–1009. [Google Scholar] [CrossRef]
- Bezati, S.; Velliou, M.; Polyzogopoulou, E.; Boultadakis, A.; Parissis, J. The Role of Landiolol in the Management of Atrial Tachyarrhythmias in Patients with Acute Heart Failure and Cardiogenic Shock: Case Reports and Review of Literature. European Heart Journal, Supplement 2022, 24, D22–D33. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur Heart J 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Okajima, M.; Takamura, M.; Taniguchi, T. Landiolol, an Ultra-Short-Acting Β1-Blocker, Is Useful for Managing Supraventricular Tachyarrhythmias in Sepsis. World J Crit Care Med 2015, 4, 251. [Google Scholar] [CrossRef]
- Rehberg, S.; Joannidis, M.; Whitehouse, T.; Morelli, A. Landiolol for Managing Atrial Fibrillation in Intensive Care. European Heart Journal, Supplement 2018, 20, A15–A18. [Google Scholar] [CrossRef]
- Nagai, R.; Kinugawa, K.; Inoue, H.; Atarashi, H.; Seino, Y.; Yamashita, T.; Shimizu, W.; Aiba, T.; Kitakaze, M.; Sakamoto, A.; et al. Urgent Management of Rapid Heart Rate in Patients with Atrial Fibrillation/Flutter and Left Ventricular Dysfunction - Comparison of the Ultra-Short-Acting Β1-Selective Blocker Landiolol with Digoxin (J-Land Study) -. Circulation Journal 2013, 77, 908–916. [Google Scholar] [CrossRef] [PubMed]
- Wada, Y.; Aiba, T.; Tsujita, Y.; Itoh, H.; Wada, M.; Nakajima, I.; Ishibashi, K.; Okamura, H.; Miyamoto, K.; Noda, T.; et al. Practical Applicability of Landiolol, an Ultra-Short-Acting Β1-Selective Blocker, for Rapid Atrial and Ventricular Tachyarrhythmias with Left Ventricular Dysfunction. J Arrhythm 2016, 32, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Iwahashi, N.; Takahashi, H.; Abe, T.; Okada, K.; Akiyama, E.; Matsuzawa, Y.; Konishi, M.; Maejima, N.; Hibi, K.; Kosuge, M.; et al. Urgent Control of Rapid Atrial Fibrillation by Landiolol in Patients With Acute Decompensated Heart Failure With Severely Reduced Ejection Fraction. Circ Rep 2019, 1, 422–430. [Google Scholar] [CrossRef]
- Kobayashi, S.; Myoren, T.; Kajii, T.; Kohno, M.; Nanno, T.; Ishiguchi, H.; Nishimura, S.; Fukuda, M.; Hino, A.; Fujimura, T.; et al. Addition of a Β1-Blocker to Milrinone Treatment Improves Cardiac Function in Patients with Acute Heart Failure and Rapid Atrial Fibrillation. Cardiology (Switzerland) 2019, 142, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Kakihana, Y.; Nishida, O.; Taniguchi, T.; Okajima, M.; Morimatsu, H.; Ogura, H.; Yamada, Y.; Nagano, T.; Morishima, E.; Matsuda, N. Efficacy and Safety of Landiolol, an Ultra-Short-Acting Β1-Selective Antagonist, for Treatment of Sepsis-Related Tachyarrhythmia (J-Land 3S): A Multicentre, Open-Label, Randomised Controlled Trial. Lancet Respir Med 2020, 8, 863–872. [Google Scholar] [CrossRef]
- Matsuda, N.; Nishida, O.; Taniguchi, T.; Okajima, M.; Morimatsu, H.; Ogura, H.; Yamada, Y.; Nagano, T.; Ichikawa, A.; Kakihana, Y. Impact of Patient Characteristics on the Efficacy and Safety of Landiolol in Patients with Sepsis-Related Tachyarrhythmia: Subanalysis of the J-Land 3S Randomised Controlled Study. EClinicalMedicine 2020, 28. [Google Scholar] [CrossRef]
- Unger, M.; Morelli, A.; Singer, M.; Radermacher, P.; Rehberg, S.; Trimmel, H.; Joannidis, M.; Heinz, G.; Cerny, V.; Dostál, P.; et al. Landiolol in Patients with Septic Shock Resident in an Intensive Care Unit (LANDI-SEP): Study Protocol for a Randomized Controlled Trial. Trials 2018, 19. [Google Scholar] [CrossRef] [PubMed]
- Syed, Y.Y. Landiolol: A Review in Tachyarrhythmias. Drugs 2018, 78, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, T.; Nakasu, Y.; Mizutani, H.; Sumitani, K. A Prospective Observational Survey on Landiolol in Atrial Fibrillation/Atrial Flutter Patients with Chronic Heart Failure – AF-CHF Landiolol Survey. J Cardiol 2019, 74, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, T.; Saitoh, T.; Matsushita, M. Design of a Prospective Observational Survey on Landiolol in Atrial Fibrillation/Atrial Flutter Patients with Chronic Heart Failure - AF-CHF Landiolol Survey. J Cardiol 2015, 66, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Stix, G.; Wolzt, M.; Domanovits, H.; Kadlecová, P.; Husch, B.; Trebs, M.; Hodisch, J.; Unger, M.; Krumpl, G. Open-Label Two-Dose Pilot Study of Landiolol for the Treatment of Atrial Fibrillation/Atrial Flutter in Caucasian Patients. Circulation Journal 2019, 84, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Shibata, S.C.; Uchiyama, A.; Ohta, N.; Fujino, Y. Efficacy and Safety of Landiolol Compared to Amiodarone for the Management of Postoperative Atrial Fibrillation in Intensive Care Patients. J Cardiothorac Vasc Anesth 2016, 30, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Horikoshi, Y.; Goyagi, T.; Kudo, R.; Kodama, S.; Horiguchi, T.; Nishikawa, T. The Suppressive Effects of Landiolol Administration on the Occurrence of Postoperative Atrial Fibrillation and Tachycardia, and Plasma IL-6 Elevation in Patients Undergoing Esophageal Surgery: A Randomized Controlled Clinical Trial. J Clin Anesth 2017, 38, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Schnaubelt, S.; Eibensteiner, F.; Oppenauer, J.; Tihanyi, D.; Neymayer, M.; Brock, R.; Kornfehl, A.; Veigl, C.; Al Jalali, V.; Anders, S.; et al. Hemodynamic and Rhythmologic Effects of Push-Dose Landiolol in Critical Care—A Retrospective Cross-Sectional Study. Pharmaceuticals 2023, 16. [Google Scholar] [CrossRef]
- Matsuishi, Y.; Jesmin, S.; Kawano, S.; Hideaki, S.; Shimojo, N.; Mowa, C.N.; Akhtar, S.; Zaedi, S.; Khatun, T.; Tsunoda, Y.; et al. Landiolol Hydrochloride Ameliorates Acute Lung Injury in a Rat Model of Early Sepsis through the Suppression of Elevated Levels of Pulmonary Endothelin-1. Life Sci 2016, 166, 27–33. [Google Scholar] [CrossRef]
Figure 1.
The mechanism of action for Landiolol. This image wase created with Biorender.com (accessed on 11 February 2024). ß –ADR: ß adrenergic receptor; Ina: sodium current; IKs: slow delayed rectifier potassium current; If: funny current; INaK: sodium-potassium pump current; PKA: protein kinase A; cAMP: cyclic adenosine monophosphate; SERCA2: sarcoplasmic/endoplasmic reticulum calcium ATPase 2; RyR2: ryanodine receptor 2; PLB: phospholamban; ATP: adenosine triphosphate; AC: adenylyl cyclase.
Figure 1.
The mechanism of action for Landiolol. This image wase created with Biorender.com (accessed on 11 February 2024). ß –ADR: ß adrenergic receptor; Ina: sodium current; IKs: slow delayed rectifier potassium current; If: funny current; INaK: sodium-potassium pump current; PKA: protein kinase A; cAMP: cyclic adenosine monophosphate; SERCA2: sarcoplasmic/endoplasmic reticulum calcium ATPase 2; RyR2: ryanodine receptor 2; PLB: phospholamban; ATP: adenosine triphosphate; AC: adenylyl cyclase.
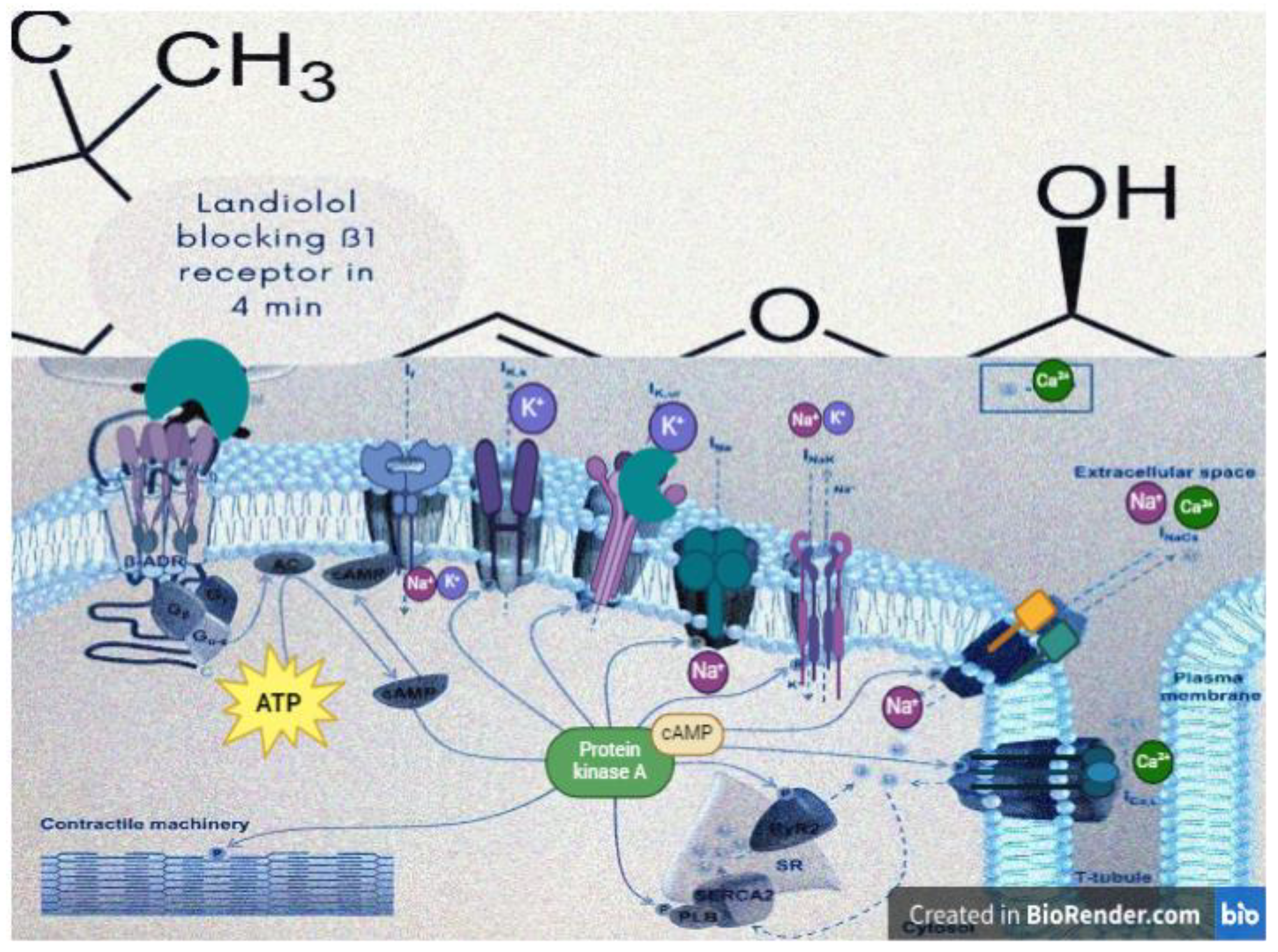
Table 1.
The impact of beta-blockers upon If, IKs, INa, and INaK channels.
| Current channel | If | IKs | INa | INaK |
|---|---|---|---|---|
| Role | A mixed cation current is carried by both Na+ and K+. It is mainly involved in the pacemaker activity of the sinoatrial node, contributing to the diastolic depolarization and spontaneous firing of action potentials. | A delayed rectifier potassium current plays a role in repolarizing the cardiac action potential. It contributes to the plateau phase of the action potential in cardiac myocytes. | The fast inward sodium current is responsible for the rapid depolarization phase of the cardiac action potential. It plays a critical role in initiating and propagating action potentials in cardiac myocytes. | The sodium-potassium pump (Na+/K+-ATPase) plays a crucial role in maintaining the resting membrane potential of cardiac myocytes by actively transporting 3 atoms of sodium out of the cell and 2 atoms of potassium into the cell. |
| The influence of landiolol1 | Indirect- by blocking ß-1 receptors, landiolol reduces the stimulatory effects of endogenous catecholamines, leading to a decrease in If activity and a subsequent decrease in heart rate. | May have minor effects on IKs, primarily through downstream signaling pathways influenced by the blockade of ß-1 adrenergic receptors. | Indirect- by blocking ß-1 receptors, landiolol reduces the stimulatory effects of catecholamines on INa, leading to a decrease in the rate of rise of the action potential and a reduction in myocardial excitability. | Not well-documented, its effects on intracellular calcium levels and ion handling in cardiac myocytes, mediated through ß-1 receptor blockade, may indirectly influence the activity of the sodium-potassium pump. |
1availabe for all beta-blockers. If: funny current; IKs: slow delayed rectifier potassium current; INa: sodium current; INaK: sodium-potassium pump current.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



