
Submitted:
18 February 2024
Posted:
19 February 2024
You are already at the latest version
Abstract
Aim: To analyze a single center's experience with Short Bowel Syndrome/ Chronic Intestinal Failure (SBS/CIF) in adult patients treated with Home Parenteral Nutrition (HPN).
Materials and methods: In the last thirty years, 13 patients with SBS/CIF were included in an HPN program.
Results: Between 1992 and 2023, 13 patients were included in an HPN program. The primary underlying pathology was acute mesenteric ischemia. The median age of the starting HPN was 44 years old. Most are submitted to several surgeries of extensive intestinal resection with posterior intestinal reconstruction. Five of the 13 patients have died while on HPN for a median of 42 months. The causes of death HPN-related were catheter sepsis, endocarditis with cardiac failure, or hepatic failure. One patient died due to underlying pathology: pelvic abscesses and bleeding related to radiotherapy. Eight patients remain alive with a median time of HPN of 173 months. During the HPN support, the most frequent complications were venous catheter infection and venous territory thrombosis. None of the eight patients alive have hepatic failure. Two patients recently started teduglutide, with good tolerance, and need reduction of HPN support. All these eight patients have a satisfactory quality of life (parenteral support needs range between five to two nutrition bags per week).
Conclusion: HPN remains the gold standard of SBS/CIF treatment, although Teduglutide may reduce HPN needs and HPN complications and provide a better quality of life. An HPN multidisciplinary healthcare group support is essential to ensure these patients' survival and quality of life.
Keywords
Short bowel Syndrome, Chronic Intestinal failure, Home Parenteral Nutrition, Teduglutide, Complications of Parenteral Support.
Keywords:
Keywords
; Short bowel Syndrome
; Chronic Intestinal failure
; Home Parenteral Nutrition
; Teduglutide
; Complications of Parenteral Support
1. Introduction
Intestinal failure is characterized by the inability to maintain adequate nutrition via the intestine. It can be subdivided into three groups: acute, usually self-limiting, of short duration and appearing in the postoperative period; subacute, for patients who are metabolically unstable, usually septic, and need of prolonged artificial nutrition; and chronic, which requires long-term parenteral nutrition or IVS to maintain health and/or growth,, appearing in metabolically stable patients who are incapable of maintaining adequate absorption of macronutrients and/or water and electrolytes through the intestine [1,2]. Short Bowel Syndrome is a subgroup of chronic intestinal failure, a rare entity usually resulting from extensive intestinal resections requiring prolonged parenteral nutrition as the primary therapy, ideally performed at home [3,4]. Home parenteral nutrition means the patient does it at home through a central access (long-term central catheter), a nutritional bag, and/or fluids and electrolytes bag, and all the medication necessary to survive. Home parenteral nutrition, the basis for treating short bowel syndrome, is not free of serious complications, such as infection and thrombosis of central venous accesses, metabolic disturbances, and liver failure. The risk of mortality in these cases can reach 10 to 15% when this type of nutrition lasts more than two years [5]. The guidelines for HPN are well established and help in a correct SBD/CIF patient orientation [6,7].
In Portugal, the experience with Short Bowel Syndrome/Chronic Intestinal failure in adult patients in Hospital Centers nationwide is minimal. Centro Hospitalar Universitário de Santo António is the only national public institution that has maintained a home parenteral nutrition program for this type of patient over the last 30 years [8].
Given that SBS/CIF is a rare condition and difficult to handle, a reflection on this entity and the best way to treat it is the purpose of this article based on the experience gained.
2. Materials and Methods
A retrospective single-center analysis of all consecutive patients with SBS/CIF was included in an HPN between January 1994 and August 2023. Primary outcomes were patient survival; secondary outcomes were the main difficulties in the HPN implementation, complications related to HPN, and quality of life.
Inclusion criteria:
Patients with SBS/CIF treated in the last 30 years could be included in an HPN program at Centro Hospitalar Universitário de Santo António.
Exclusion criteria:
Patients with sub-acute intestinal failure evolved favorably without needing home parenteral support, and those who evolved unfavorably died without the opportunity to be included in this program.
Patients
The characterization of patients is described in Table 1.
The primary underlying pathology was acute mesenteric ischemia. All are submitted to several surgeries with intestinal reconstruction. In most patients, the small intestine remains between 10 to 60 cm (jejunum or Ilion), with the left colon preserved. The intestinal extent varies between patients; the smallest consists only of the duodenum and colon (patients 1 and 8), and the largest consists of 60 cm of jejunum plus 10 cm of ileum and the left colon (patient 12). Only two have the ileocecal valve preserved (patients 4 and 12). Most cases resulted from intestinal vascular ischemia, but we also have a case of volvulus, a case of desmoid tumor, a case of radiation enteritis, and one case of intestinal dysmotility. Of the patients in the program, one has an ileostomy due to intestinal aganglionosis, one an ileostomy and a high output jejunum fistula, and one a colostomy; all others have colon continuity.
The first patient with CIF in that innovative program in Portugal emerged in 1994; a case report was previously published [9]. The patient remained in that condition for five years, having died of Intravascular catheter-related bloodstream infection (CRBSI). The third patient arose in 1996, and he is still in this program, accompanied by other cases that have appeared over this time. The incidence of CIF in our hospital has been decreasing. Overall, 13 patients were included in the HPN program from the beginning, of which eight are currently alive. 62.5% are females, age at CIF diagnosis was 43.7 years old. The median age of the starting HPN was 44 years old. At the date of this manuscript, the average age of participants was 58.4 years (minimum 48 and maximum 68 years). None of these patients have higher education, and one is illiterate.
Patient education and training program for HPN administration
During the hospitalization, the patients were learning how to administer HPN and to recognize the main alarm signs to go to the Hospital. Eleven of thirteen became autonomous without needing nursing help with parenteral nutrition at home - self-management of the CVC by patients. The other two have problems with learning, and parenteral nutrition is made with nursing help.
Central venous access and nutritional support
The patients usually have a long-term catheter, a tunnelled one, placed in the right subclavian vein for parenteral nutrition administration. The catheter is flushed with heparin after IV administration of parenteral nutrition. We don´t routinely use taurolidine 4% at each catheter disconnection.
Patients are independent in preparing the nutrient bags and undergo a cyclical infusion, on average, for 10 hours at night.
All patients supplement the standard bag with water-soluble vitamins and fat-soluble and trace elements in each parenteral nutrition administration. Some patients need to supplement electrolytes in addition to those present in the nutritive admixture, particularly magnesium.
Apart from one patient who has recently started personalized parenteral nutrition, all others use standardized tri-compartmentalized bags.
Teduglutide therapy
Two of these patients started this therapy in 2022 as a small percentage of patients meet the criteria for health conditions and socio-intellectual conditions.
Culinary food support
Only patient 7 has an oral intake limited to liquid foods, all others follow family eating routines.
Follow-up
These patients are regularly followed in a multidisciplinary approach, including Nutrition appointments. In each consultation, the nutritional status, including weight, body mass index (BMI), and whole-body composition, are assessed using bioelectrical impedance (RJL Systems, Quantum II Body Composition Analyser). Eating and bowel habits are evaluated with a high degree of detail. Food consumption is evaluated using the 24-hour-recall method and a food frequency questionnaire, although patients fill out food diaries whenever clinically necessary.
Blood tests with a large nutritional profile are regularly performed, according to the updated ESPEN guidelines on long-term HPN [10], and allow the monitoring of adherence and therapeutic adequacy. Nutritional interventions are based on the results of all these assessments.
Various medical exams are conducted routinely to assess the health of the liver, kidneys, and other body organs. These exams include abdominal echography, bone scintigraphy, and upper and lower endoscopy. In case of complications related or unrelated to HPN, additional tests such as chest and abdominal CT scan, liver MRI, or capsule endoscopy may also be performed.
In the event of hospitalization, patients are evaluated closely by the same team that follows them in an outpatient clinic.
3. Results
Nutritional support
Patients in the HPN program administer parenteral nutrition on average 4.9 days a week (minimum: 2 and maximum 7). The mean daily volume administered is 922 mL (minimum: 282 and maximum 1500 mL), corresponding to 6452 mL per week (min 1972 and maximum 10500 mL). The mean daily energy intake is 986 kcal, 120 g of carbohydrates, 39 g of protein, and 35 g of lipids. All patients supplement the standard bag with water-soluble vitamins and fat-soluble and trace elements in each parenteral nutrition administration. Some patients need to supplement electrolytes in addition to those present in the nutritive admixture, particularly magnesium.
Differences between sexes are presented in Table 2.
Apart from one patient recently starting individualized parenteral nutrition (compounded PN), all others use standardized commercially available multi-chamber bags. The need for a special formulation tailored to the patient arose due to a chronic renal disease that required specific water volumes and a lower load of amino acid, potassium, and phosphorus.
Teduglutide therapy
Two (patients 9 and 12) of the eight patients recently started teduglutide with good tolerance and reduction needs for HPN support. One of the patients has already reduced parenteral energy intake by 50 %. After six months, Teduglutide treatment significantly reduced PN days, caloric needs, infusion time, and infusion volume. The other had an infectious intercurrence (pleural tuberculosis) with prolonged hospitalization and changes in nutrition, which influenced the result, maintaining the initial intake today. It should be noted that the patient who reduced the intake maintained her weight and body composition.
Nutritional status
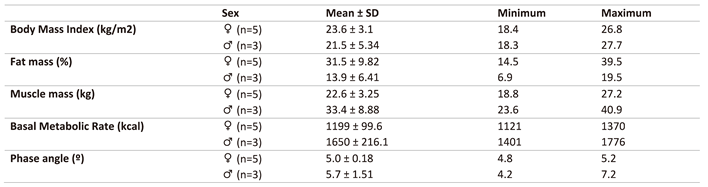
Table 3 contains a description of the anthropometric assessment of HPN patients.
Data from the last evaluation of each patient show a mean BMI of 22.8 kg/m2 (two patients at the upper limit of the malnutrition WHO classification and three at the lower limit of the overweight classification, data not shown). The phase angle was 5.0 in females and 5.7 in males, only below the limit in patient 13, possibly because she was still in an adaptation phase. A mean fat mass of 13.9% was obtained for the male sex (below the limit established by the bioimpedance equipment) and 32.0% for the female sex (above the limit established by the bioimpedance equipment). Regarding muscle mass, male sex patients presented a mean of 33.4 kg compared to 22.0 kg female sex patients (Table 4).
Complications related and unrelated to HPN
Five of the 13 patients were deceased. These five deceased patients were on HPN for 42 months (87 – 13). The causes of death related to HPN were catheter sepsis (2), endocarditis and cardiac failure (1), and hepatic failure (1); the causes of death unrelated to HPN were necrosis tissue, sepsis, pelvic abscesses, and pelvic bleeding due to radiation enteritis (1).
Eight patients remain alive with a median time of HPN of 173 months (320 – 43). Three of the eight have health comorbidities, making the HPN's management difficult.
In these eight patients, during the HPN support, the main complications related to HPN were the venous catheter infection and the venous territory thrombosis. The frequency of the CVC infection is not the same in all patients. One of the patients kept the same catheter without complications for more than eight years. Catheter changes occur due to material deterioration. Urosepsis and metabolic dysfunction were the second most frequent problems. None of the eight patients alive have hepatic failure.
In these eight patients, the main complications unrelated to HPN were an auricular flutter with cardiac insufficiency, urosepsis with chronic renal dysfunction, acute cholecystitis, tuberculosis, and COVID-19 infection. The infection of COVID-19 in those patients was a severe problem during the pandemic period. Four of our eight patients had COVID-19 infection. One of them had a severe infection with Intensive care hospitalization: lung infection (Figure 1) and posterior thrombosis of the central venous territory.
The problem was fixed by introducing a thoracic venous catheter using the surfacer inside-out technique (Figure 2).
Quality of Life
All these eight patients have a satisfactory quality of life with needs for parenteral support that varies between five to two nutrition bags per week.
None of the patients practice scheduled and regular physical activity; they only do activities of daily living.
Regarding occupation, although very active in their daily lives, two work in their own companies. Another patient visits her daughter, who lives in another European country, traveling by plane.
4. Discussion
Short Bowel Syndrome with Chronic Intestinal Failure (SBS-CIF) is the inability to maintain protein-energy, fluid, electrolyte, or micronutrient balance due to a short bowel [3].
In Portugal, extensive intestinal resections that lead to Short Bowel Syndrome are generally performed in urgent situations due to acute mesenteric ischemia. Other pathological entities may require extensive intestinal resections performed on an elective or urgent basis, such in Crohn's disease [11,12,13], radiation enteritis [14], and severe complications of digestive, severe gastrointestinal dysmotility disorders [15], digestive surgical complications, or intestinal bypass preparations due to oncological disease [16] can also result in SBS. Our experience is minimal in those cases; we haven’t experienced oncologic intestinal obstruction patients.
We have a small but interesting experience of 13 patients with SBS-IF. Nine of these thirteen patients had acute mesenteric ischemia that led to SBS. The other four patients, the SBS/CIF, result from radiation enteritis (two), extensive intestinal resection due to a mesenteric desmoid tumor, and intestinal aganglionosis. This small number of patients in HPN and the type of underlying pathology can result from some negative factors of clinical practice and some positive ones. As negatives, we can include the later diagnosis, elderly patients, and multiple comorbidities leading to the death of many patients with acute mesenteric ischemia. As positives, the advances in the treatment of some pathologic conditions, such as the biological treatment of Crohn's disease, the implementation of radiotherapy neoadjuvant and not adjuvant in locally advanced rectal cancer with reduction of the radiation enteritis, and the collaboration of the vascular surgery in the management of acute and chronic mesenteric ischemia, leading to the reduction of the number of patients with SBS/CIF. The absence of oncologic patients with intestinal obstruction in our HPN program is probably due to the poor survival of these specific patients and the difficulty of providing the home-efficacy home care support they need.
Although SBS/CIF is rare, its clinical management is complex, challenging, expensive, and time-consuming. It is necessary to have a correct approach to this condition, a multidisciplinary team [17], an HPN program implementation, and open SOS phone contact.
These patients have in common the need for several surgeries of intestinal resections, and most need intensive care hospitalization. In most cases, the remnant intestine of the patients operated on due to acute mesenteric ischemia was a small amount of small bowel (10 to 60 cm) and the left colon. When possible, elective intestinal reconstruction was made to make HPN management easier [18]. In our series, the absence of stomas was possible in 10 of 13 patients. Doing intestinal reconstruction seems to be a good achievement and allows for the reduction of hydro electrolytic imbalance and cardiac and renal dysfunction.
On the other hand, HPN remains the standard care of those patients with SBS/CIF, but the complications related to HPN are frequent and life-threatening [5]. Implementing an HPN program since the SBS/CIF patient was metabolically balanced and non-septic is difficult. We took some strategies to reduce HPN complications: implementation of a patient education and training program for HPN administration, the patient's monitorization by the same team in medical appointments and during the hospitalization, the correct use of parenteral and enteral support, and the utilization of the analog of human glucagon-like peptide-2 (GLP-2), whenever indicated.
These patients require long-term and lifelong vascular access and are at considerable risk of developing central line-associated bloodstream infections. In our experience, the most frequent complication was the central venous catheter infection. This type of infection is a frequent and severe problem. It can provoke severe sepsis, territory venous thrombosis, and even threaten patient life. In our patients, central venous catheter infection results in multiple hospital admissions for sepsis, three patients with extensive thrombosis of venous territory, and the death of two patients. Some catheter sepsis was also related to urinary tract infection and bacterial endocarditis, worsening the renal or cardiac function or leading to renal or cardiac failure. It happens in four of our patients
In our center, the CVC changes are realized with echography control to reduce the risk of catheter infection and thrombosis in the venous territory. Catheter-related bloodstream infections (CRBSI) are a serious complication in HPN. Antibiotic salvage of central venous catheters (CVCs) in CRBSI is recommended; however, this is based on limited reports [19]. In our center, in case of infection, a standardized 10 to 14-day catheter salvage treatment protocol, including antibiotic CVC locks, stopping bag perfusion, and systemic antibiotic administration, was used to salvage infected CVCs as appropriate. The CVC was not used for systemic therapy for the duration of the salvage protocol. We don’t routinely use taurolidine + 4% citrate after the nutrition bag infusion as infection prevention, although other centers do it with good results [20]. Relatively to thrombosis central venous, the vascular surgeon with special skills in vascular access approach has resolved the problems (Figure 2).
To avoid metabolic complications, we select and prescribe the nutrition bags, monitor the patient's nutritional and health status, and try the precocious detection of HPN side effects. Moreover, we use the enteral route whenever possible. It is essential to highlight the possible nutrient absorption via the enteral route, contributing to the total intake depending on the patient's characteristics. This route is also important in maintaining enterohepatic circulation, reducing the risk of parenteral nutrition-associated complications, namely hepatic failure. Specific oral nutritional supplementation can also be a strategy to reduce parenteral intake. Considering the oral nutritional apport is necessary to avoid over-nourishing patients, but we cannot accurately quantify this. Still, we can confirm this happens because body weight is maintained with parenteral administrations lower than the calculated energy expenditure.
The use of individualized bags can contribute not only to the reduction of metabolic complications but also to the reduction of catheter infections and hydro electrolytic imbalances. We have recently started using custom bags to reduce the complications of NPD. Whenever indicated to reduce the volume/number of PNH bags per week [21], Teduglutide is an important aid in managing these patients [22]. In addition to reducing the number of bags, it reduces the long-term complications of PNH and significantly improves the patient's quality of life [23,24]. This analog of human glucagon-like peptide-2 (GLP-2) has been referred to as improving structural and functional intestinal adaptation following intestinal resection by decelerating a rapid gastric emptying, decreasing gastric hypersecretion, increasing intestinal blood flow, and promoting intestinal growth [25]. It was approved in Portugal only in 2019. In our series, it was possible to introduce teduglutide in two patients. Although still recently introduced, this drug was well tolerated, with a reduction in the number of bags per week.
Liver failure with progression to cirrhosis is the HPN complication most fear. The bag composition (calory, the ratio glucose/lipide, and fish oil emulsion) can interfere with liver function [26,27,28,29]. The monitorization and the bag composition readjustment are essential tasks in outpatient appointments. Careful monitoring of fluid, electrolyte, macronutrient, and micronutrient status can minimize major organ dysfunction and metabolic complications. It should be noted that the eight patients on HPN do not show signs of liver dysfunction, with progression to cirrhosis. Hepatic cirrhosis was one of the complications that arose in one of the first patients in the series, and he died before having the opportunity to undergo the liver and intestinal transplant for which he was proposed.
Other issues that appear during and related to HPN support include kidney acute and chronic insufficiency, cardiac insufficiency, cholelithiasis, hyperglycemia, vitamin D insufficiency, and osteoporosis, resolved or controlled with the indicated measures.
In general terms, in our center, although with a small group of patients with various comorbidities, HPN has performed with considerable patient survival combined with a reasonable quality of life. In our series, patients have an average of 173 months of NPD. This outcome is identical to the other centers with an enormous experience [30,31,32,33]. This result was and is only possible through the joint action of a multidisciplinary group, including general surgery, vascular surgery, nutritionist, nursing, pharmacy and nephrology, cardiology, and anesthesiology, to effectively treat patients with SBS/ICF.
5. Conclusions
HPN remains the gold standard of SBS/CIF treatment, although Teduglutide may reduce HPN needs and HPN complications and provide a better quality of life. A multidisciplinary healthcare group for HPN support is essential to ensure these patients' survival and quality of life.
Author Contributions
All the authors contributed to the patient's clinical observations in their respective areas. M.D. Santos and V. Magalhães contributed to the conception, design, and drafting of the manuscript; L. Loureiro, P. Pina, A. Castro, P. Aguiar, A. Gomes, and D. Soares contributed to the acquisition and analysis of the data; M. D. Santos and A. Rocha contributed to the interpretation of the data and supervision of the manuscript. All authors critically revised the manuscript, agreed to be fully accountable for ensuring the integrity and accuracy of the work, and read and approved the final manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.Written informed consent for publication must be obtained from participating patients who can be identified.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Gardiner, K.R. Management of acute intestinal failure. The Proceedings of the Nutrition Society 2011, 70, 321–328. [Google Scholar] [CrossRef]
- Pironi, L.; Cuerda, C.; Jeppesen, P.B.; Joly, F.; Jonkers, C.; Krznaric, Z.; Lal, S.; Lamprecht, G.; Lichota, M.; Mundi, M.S.; et al. ESPEN guideline on chronic intestinal failure in adults - Update 2023. Clin Nutr 2023, 42, 1940–2021. [Google Scholar] [CrossRef]
- 3. Ballesteros Pomar MD, Vidal Casariego A. [Short bowel syndrome: definition, causes, intestinal adaptation and bacterial overgrowth]. Nutricion hospitalaria : organo oficial de la Sociedad Espanola de Nutricion Parenteral y Enteral. 2007;22 Suppl 2:74-85.
- Guillen, B.; Atherton, N.S. Short Bowel Syndrome. In StatPearls, Treasure Island (FL), 2021.
- D'Eusebio, C.; Merlo, F.D.; Ossola, M.; Bioletto, F.; Ippolito, M.; Locatelli, M.; De Francesco, A.; Anro, M.; Romagnoli, R.; Strignano, P.; et al. Mortality and parenteral nutrition weaning in patients with chronic intestinal failure on home parenteral nutrition: A 30-year retrospective cohort study. Nutrition 2023, 107, 111915. [Google Scholar] [CrossRef]
- Pironi, L.; Boeykens, K.; Bozzetti, F.; Joly, F.; Klek, S.; Lal, S.; Lichota, M.; Muhlebach, S.; Van Gossum, A.; Wanten, G.; et al. ESPEN practical guideline: Home parenteral nutrition. Clin Nutr 2023, 42, 411–430. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, S.C.; Austin, P.; Boeykens, K.; Chourdakis, M.; Cuerda, C.; Jonkers-Schuitema, C.; Lichota, M.; Nyulasi, I.; Schneider, S.M.; Stanga, Z.; et al. ESPEN guideline on home enteral nutrition. Clin Nutr 2020, 39, 5–22. [Google Scholar] [CrossRef] [PubMed]
- Silva, R.; Guerra, P.; Rocha, A.; Correia, M.; Ferreira, R.; Fonseca, J.; Lima, E.; Oliveira, A.; Gomes, M.; Ramos, D.; et al. Clinical, Economic, and Humanistic Impact of Short-Bowel Syndrome/Chronic Intestinal Failure in Portugal (PARENTERAL Study). GE Port J Gastroenterol 2022, 293–304. [Google Scholar] [CrossRef] [PubMed]
- Rocha, A. , Pereira, I., Ramalhão AM. Home total parenteral nutrition by absence of jejune and ileum (case report) [original title in portuguese: Nutrição paretérica total dominciliária por ausência de jejuno-íleo (caso clínico)]. Arquivos Portugueses de Cirurgia 1995, 4, 101–104. [Google Scholar]
- Pironi, L.; Boeykens, K.; Bozzetti, F.; Joly, F.; Klek, S.; Lal, S.; Lichota, M.; Mühlebach, S.; Van Gossum, A.; Wanten, G.; et al. ESPEN practical guideline: Home parenteral nutrition. Clinical Nutrition 2023, 42, 411–430. [Google Scholar] [CrossRef] [PubMed]
- Bakhshi, Z.; Yadav, S.; Salonen, B.R.; Bonnes, S.L.; Varayil, J.E.; Harmsen, W.S.; Hurt, R.T.; Tremaine, W.J.; Loftus, E.V., Jr. Incidence and Outcomes of Home Parenteral Nutrition in Patients With Crohn Disease in Olmsted County, Minnesota. Crohns Colitis 360 2020, 2, otaa083. [Google Scholar] [CrossRef]
- Calvert, C.R.; Lal, S. Approaches to intestinal failure in Crohn's disease. The Proceedings of the Nutrition Society 2011, 70, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Gerlach, U.A.; Vrakas, G.; Reddy, S.; Baumgar, D.C.; Neuhaus, P.; Friend, P.J.; Pascher, A.; Vaidya, A. Chronic intestinal failure after crohn disease: when to perform transplantation. JAMA surgery 2014, 149, 1060–1066. [Google Scholar] [CrossRef] [PubMed]
- Kalaiselvan, R.; Theis, V.S.; Dibb, M.; Teubner, A.; Anderson, I.D.; Shaffer, J.L.; Carlson, G.L.; Lal, S. Radiation enteritis leading to intestinal failure: 1994 patient-years of experience in a national referral centre. European journal of clinical nutrition 2014, 68, 166–170. [Google Scholar] [CrossRef]
- Salazar, E.; Clermont-Dejean, N.M.; Schwenger, K.J.P.; Noelting, J.; Lu, Z.; Lou, W.; Allard, J.P. Patients With Severe Gastrointestinal Dysmotility Disorders Receiving Home Parenteral Nutrition Have Similar Survival As Those With Short-Bowel Syndrome: A Prospective Cohort Study. JPEN. Journal of parenteral and enteral nutrition 2021, 45, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Culine, S.; Chambrier, C.; Tadmouri, A.; Senesse, P.; Seys, P.; Radji, A.; Rotarski, M.; Balian, A.; Dufour, P. Home parenteral nutrition improves quality of life and nutritional status in patients with cancer: a French observational multicentre study. Supportive care in cancer: official journal of the Multinational Association of Supportive Care in Cancer 2014, 22, 1867–1874. [Google Scholar] [CrossRef] [PubMed]
- Corcos, O.; Castier, Y.; Sibert, A.; Gaujoux, S.; Ronot, M.; Joly, F.; Paugam, C.; Bretagnol, F.; Abdel-Rehim, M.; Francis, F.; et al. Effects of a multimodal management strategy for acute mesenteric ischemia on survival and intestinal failure. Clinical gastroenterology and hepatology: the official clinical practice journal of the American Gastroenterological Association 2013, 11, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Cruz, R.J., Jr.; McGurgan, J.; Butera, L.; Poloyac, K.; Roberts, M.; Stein, W.; Minervini, M.; Jorgensen, D.R.; Humar, A. Gastrointestinal Tract Reconstruction in Adults with Ultra-Short Bowel Syndrome: Surgical and Nutritional Outcomes. Surgery 2020, 168, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Dibb, M.J.; Abraham, A.; Chadwick, P.R.; Shaffer, J.L.; Teubner, A.; Carlson, G.L.; Lal, S. Central Venous Catheter Salvage in Home Parenteral Nutrition Catheter-Related Bloodstream Infections: Long-Term Safety and Efficacy Data. JPEN. Journal of parenteral and enteral nutrition 2014. [Google Scholar] [CrossRef]
- Ait Hammou Taleb, M.H.; Mahmutovic, M.; Michot, N.; Malgras, A.; Nguyen-Thi, P.L.; Quilliot, D. Effectiveness of salvage catheters in home parenteral nutrition: A single-center study and systematic literature review. Clin Nutr ESPEN 2023, 56, 111–119. [Google Scholar] [CrossRef]
- Schonenberger, K.A.; Reber, E.; Huwiler, V.V.; Durig, C.; Muri, R.; Leuenberger, M.; Muhlebach, S.; Stanga, Z. Quality of Life in the Management of Home Parenteral Nutrition. Annals of nutrition & metabolism 2023. [Google Scholar] [CrossRef]
- de Dreuille, B.; Nuzzo, A.; Bataille, J.; Mailhat, C.; Billiauws, L.; Le Gall, M.; Joly, F. Post-Marketing Use of Teduglutide in a Large Cohort of Adults with Short Bowel Syndrome-Associated Chronic Intestinal Failure: Evolution and Outcomes. Nutrients 2023, 15. [Google Scholar] [CrossRef]
- Chen, K.; Joly, F.; Mu, F.; Kelkar, S.S.; Olivier, C.; Xie, J.; Seidner, D.L. Predictors and timing of response to teduglutide in patients with short bowel syndrome dependent on parenteral support. Clin Nutr ESPEN 2021, 43, 420–427. [Google Scholar] [CrossRef]
- Jones, D.; Lal, S.; French, C.; Sowerbutts, A.M.; Gittins, M.; Gabe, S.; Brundrett, D.; Culkin, A.; Calvert, C.; Thompson, B.; et al. Investigating the Relationship between Home Parenteral Support and Needs-Based Quality of Life in Patients with Chronic Intestinal Failure: A National Multi-Centre Longitudinal Cohort Study. Nutrients 2023, 15. [Google Scholar] [CrossRef]
- Jeppesen, P.B. New approaches to the treatments of short bowel syndrome-associated intestinal failure. Current opinion in gastroenterology 2014, 30, 182–188. [Google Scholar] [CrossRef]
- Goulet, O.J. Intestinal failure-associated liver disease and the use of fish oil-based lipid emulsions. World review of nutrition and dietetics 2015, 112, 90–114. [Google Scholar] [CrossRef]
- Nandivada, P.; Chang, M.I.; Potemkin, A.K.; Carlson, S.J.; Cowan, E.; O'Loughlin A, A.; Mitchell, P.D.; Gura, K.M.; Puder, M. The Natural History of Cirrhosis From Parenteral Nutrition-Associated Liver Disease After Resolution of Cholestasis With Parenteral Fish Oil Therapy. Annals of surgery 2013. [Google Scholar] [CrossRef]
- Chang, M.I.; Puder, M.; Gura, K.M. The use of fish oil lipid emulsion in the treatment of intestinal failure associated liver disease (IFALD). Nutrients 2012, 4, 1828–1850. [Google Scholar] [CrossRef] [PubMed]
- Lawinski, M.; Bzikowska, A.; Omidi, M.; Majewska, K.; Zielinska-Borkowska, U. Liver disease in patients qualified for home parenteral nutrition - a consequence of a failure to adjust RTU bags in the primary centre? Polski przeglad chirurgiczny 2014, 86, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Reber, E.; Staub, K.; Schonenberger, K.A.; Stanga, A.; Leuenberger, M.; Pichard, C.; Schuetz, P.; Muhlebach, S.; Stanga, Z. Management of Home Parenteral Nutrition: Complications and Survival. Annals of nutrition & metabolism 2021, 77, 46–55. [Google Scholar] [CrossRef]
- Noelting, J.; Gramlich, L.; Whittaker, S.; Armstrong, D.; Marliss, E.; Jurewitsch, B.; Raman, M.; Duerksen, D.R.; Stevenson, D.; Lou, W.; et al. Survival of Patients With Short-Bowel Syndrome on Home Parenteral Nutrition: A Prospective Cohort Study. JPEN. Journal of parenteral and enteral nutrition 2021, 45, 1083–1088. [Google Scholar] [CrossRef] [PubMed]
- Joly, F.; Baxter, J.; Staun, M.; Kelly, D.G.; Hwa, Y.L.; Corcos, O.; De Francesco, A.; Agostini, F.; Klek, S.; Santarpia, L.; et al. Five-year survival and causes of death in patients on home parenteral nutrition for severe chronic and benign intestinal failure. Clin Nutr 2018, 37, 1415–1422. [Google Scholar] [CrossRef] [PubMed]
- Dibb, M.; Soop, M.; Teubner, A.; Shaffer, J.; Abraham, A.; Carlson, G.; Lal, S. Survival and nutritional dependence on home parenteral nutrition: Three decades of experience from a single referral centre. Clin Nutr 2017, 36, 570–576. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Covid-19 infection (patient 2).
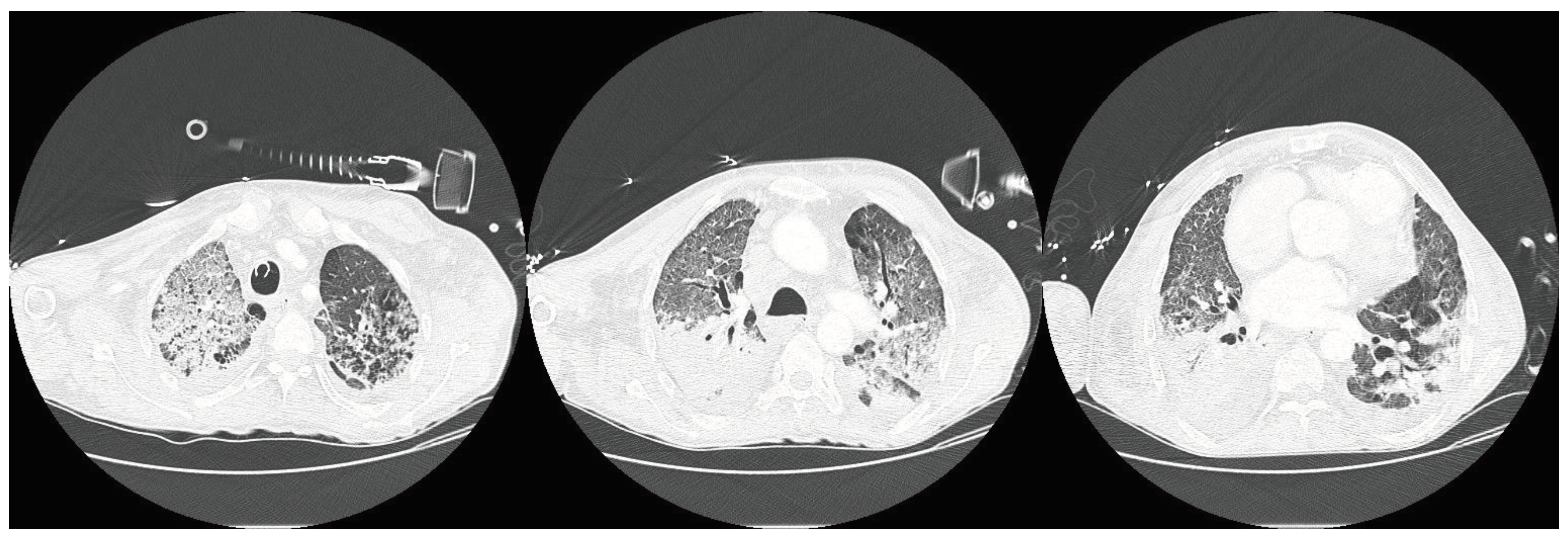
Figure 2.
New right thoracica venous access after vein recanalization with surfacer inside-out system. Procedure realized in Patient 2.
Figure 2.
New right thoracica venous access after vein recanalization with surfacer inside-out system. Procedure realized in Patient 2.
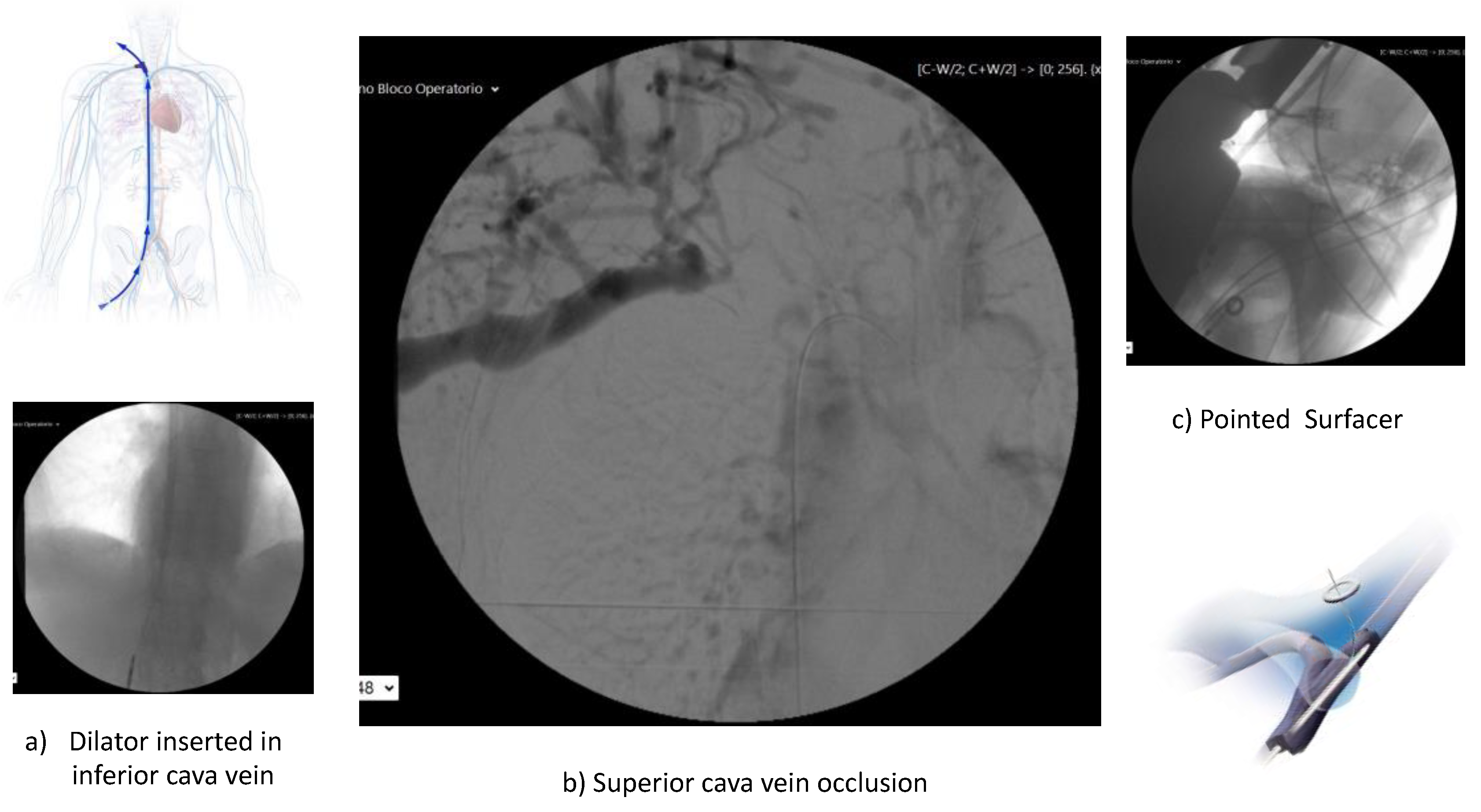

Table 1.
Patients’ characteristics.
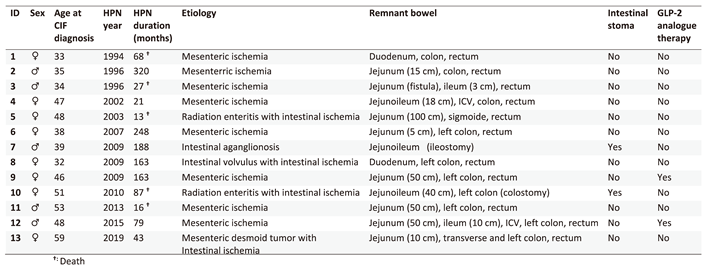
Table 2.
Other patients’ characteristics.
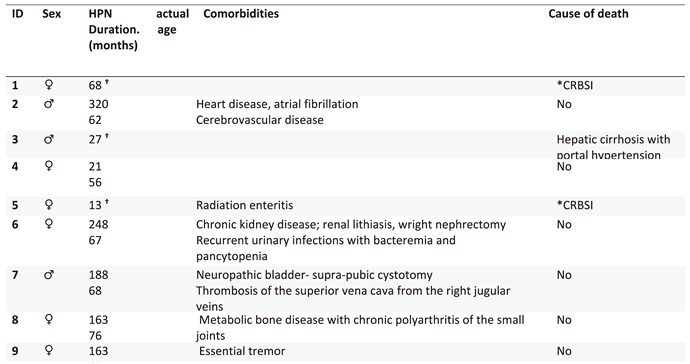
Table 3.
Current parenteral nutritional supply of the cohort of patients with chronic intestinal failure in a home parenteral nutrition program managed by the Colorectal Surgery Unit.
Table 3.
Current parenteral nutritional supply of the cohort of patients with chronic intestinal failure in a home parenteral nutrition program managed by the Colorectal Surgery Unit.
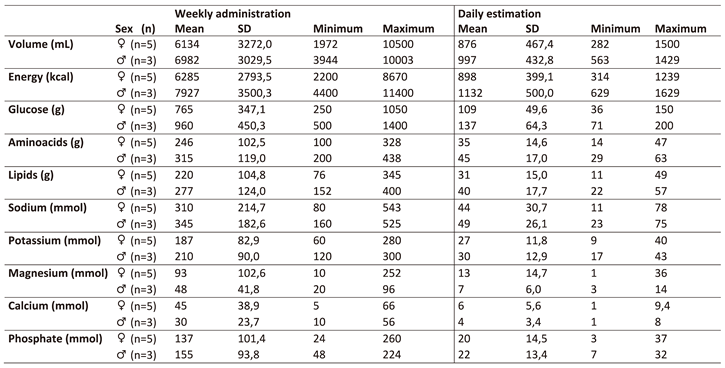
Table 4.
Current nutritional status of the cohort of patients with chronic intestinal failure in a home parenteral nutrition program, managed by the Colorectal Surgery Unit.
Table 4.
Current nutritional status of the cohort of patients with chronic intestinal failure in a home parenteral nutrition program, managed by the Colorectal Surgery Unit.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



