
Submitted:
05 February 2024
Posted:
19 February 2024
You are already at the latest version
Abstract
Background: In 2020, the incidence of cancer was 844,778 cases among the population aged 0 to 19 years. Ninety percent of the population under 18 years of age lives in low- and middle-income countries, where cancer survivors report adverse outcomes. disease, which negatively impacts individuals’ general health, emotional state and external factors such as academic performance. Therefore, the objective of this article was to report the performance of the WCST and the sociodemographic characteristics of oncopediatric patients from Cali, Colombia. We report the reliability of the WCST instrument and indicate the association between the type of cancer and executive functioning in patients. Methods: In a cross-sectional observational study, 24 oncopediatric patients were interviewed and evaluated via the WCST. Results: The mean age was 12.08 years (3.98), 20.8% were women, 70.8% had a diagnosis of leukemia, 8 patients had acquired brain deficits, and more than 75% had adequate functioning in terms of the indicators of executive functions. Robust statistics were used to explore the differences between the types of diagnoses and performance in executive functions, and no statistically significant differences were found (p = 0.156). We accumulated evidence that the WCST has a reliable Cronbach's α of 0.804 and that oncopediatric patients without brain deficits had high scores for executive functions (p = 0.002) with a moderate effect size (0.727). Conclusions: The WCST is reliable for discriminating executive function among pediatric cancer patients. The evidence suggests that there are no differences between the types of cancer evaluated and executive functioning in the participants.
Keywords:
Wisconsin Card Sorting Test
; oncology
; neuropsychology assessment
; executive function
; pediatrics.
1. Introduction
Cancer is the second leading cause of death in the world, with a total of 10 million deaths, an incidence of 23.6 million cases and disability-adjusted life years (DALYs) of 200 million in 2019 [1]. Among the population aged 0 to 19 years, according to the size of the population, North America has the highest incidence, with a total of 16,187, followed by Europe, Oceania, Latin America and the Caribbean, Africa and Asia. In this population, the prevalence of cancer was 844,778 cases, of which leukemia was the most common, with a total of 283,466 cases in 2020 [2,3]. Approximately one child is diagnosed with cancer every minute [2,3]. In cancer survivors, adverse consequences related to cancer have been reported, for example, cognitive decline can negatively impact their general health and academic performance [4].
The typical results of cognitive deterioration reported in cancer survivors include deterioration in working memory; in the speed of information processing; in attention; and in executive functions, which has a negative impact on academic performance and, in the long term, on job support or education [5,6].
Moreover, 90% of the world's population under 18 years of age lives in low- and middle-income countries and is exposed to social factors such as poverty, inequality and violence [7], which contribute to acquired brain problems that affect brain function, quality of life and the mental health of children and adolescents [8].
The achievement of academic and work objectives depends, among other things, on the degree of regulation and control of behavior. These functions are known as executive functions and have important health outcomes [4,9]. The Wisconsin Cart Sorting Test (WCST) is the standard Gold test used in the clinical context because of its practical utility in identifying acquired brain problems linked to executive function [10].
Since there is little research related to mental health and developmental disorders in low- and middle-income countries [11], this research reports on the performance of the WCST and the sociodemographic characteristics of oncopediatric patients from Cali, Colombia. Similarly, because of the reliability of the WCST instrument in the oncopediatric population, we investigated the association between the type of cancer and executive functioning in patients. We believe that there is a statistically significant difference between cancer types and performance in executive functions.
2. Materials and Methods
The study used a cross-sectional observational design.
3.1. Context
The data were collected during 2021 and 2022. The city of Cali, Colombia, has an approximate population of 13,942,630 minors projected to date [12] and is the capital of the Department of Valle del Cauca, southeast of Bogotá. In the hospitals and clinics of Cali, the rural population is received from peripheral departments and from the city of Cali for cancer care.
3.2. Participants
The criteria for participating in the study were to have an oncological diagnosis, to be a minor at the time of application and to attend an outpatient consultation for oncological treatment. Those who did not have the consent of their legal guardian were excluded.
The entire database of pediatric patients was included in the study. All participants signed parental consent to participate in the study. During their stay in the outpatient clinic, the age at the time of the evaluation was verified. The team of researchers, AMJ, MG, and vs., was notified of the fulfillment of the inclusion criteria. The participant and the legal guardian explained the study and signed the informed consent form.
A total of 27 patients participated in the study, but 3 protocols were discarded due to errors in the registration of the information, which made it impossible to identify the criteria used by the participants during each attempt.
3.3. Data sources
The information of each patient was obtained by interviewing the main caregiver and reviewing their medical history. All the data were anonymized and guarded by researcher AMJ and her team.
The patient data included in the study were identified from 1 to 27 (all patients—including those excluded—were assigned a number for their anonymity; type of identification (civil registration or identity card); age; sex; department; city; educational link (studying or not); educational level (highest level reached); religion; health scheme (contributory or subsidized); diagnosis; type of diagnosis (large nosological groups); years since diagnosis; assessment of palliative care; radiotherapy treatment; caregiver role (role assumed; example, mother, father, etc.); age of the caregiver; occupation of the caregiver; internship in the child protection system (in Colombia, it is the Colombian Institute of Family Welfare); type of family, family functionality; personal psychopathological history; treatment objective; patient location; laterality; correct responses (classification criteria correctly fed back); complete categories; persistent errors; and failures to maintain the attitude.
3.4. Procedure
The Wisconsin Card Sorting Test (WCST) was used due to its clinical utility, sensitivity, and validity in the scientific community to discriminate functional executives between clinical and nonclinical samples [13,14]. The objective of the task is to classify 128 cards according to the following classification criteria: color (the cards can be red, yellow, blue, or green), shape (triangle, circle, cross, or star), and number (of one to four figures per card). Since the task consists of choosing a criterion, waiting for feedback (correct or incorrect) and, in relation to said feedback, maintaining or changing the classification criteria, the WCST is the gold standard test for evaluating the regulation and control of the activity. cognitive flexibility or executive functions [15].
The literature suggests estimating executive functioning to include four indicators: correct answers, complete categories, perseverative errors and failures to maintain the attitude. Each one independently provides information on an aspect of the executive functioning of the subject, which can be grouped around maintaining the action according to the objective of the task or, on the other hand, inhibiting actions unrelated to the objective.
The maintenance of the action is interpreted as follows: the higher the score is, the greater the maintenance. Here, are the correct answers and the number of correct categories. The correct answers are the number of classification actions that were made according to the stipulated classification criteria (shape, color, number), with a maximum score of 128; complete categories are the number of classification criteria completed, with a maximum score of 6. Conversely, maintenance failures are interpreted as follows: the lower the score is, the greater the maintenance. Perseverative errors, which are repetitive actions unrelated to the current classification criteria, have a maximum score of 127. Similarly, the failure to maintain an attitude, defined as an action that is consecutively consistent with the classification criterion of participant failure to maintain a maximum score of 127 [10,16].
These scores are based on the assumption that the subject can make a mistake after the change in criteria or the first feedback according to the classification rule. Similarly, according to the age, educational level, and clinical or nonclinical group, the typical score and classification can be estimated (Table 1):
Since ages vary among subjects, age scales were used; these scales are found in the supplementary material available in the Mendeley data and are briefly reviewed.
The application and qualification of the instrument were carried out by ABC, vs. and MG, trained in neuropsychology. The protocols were reviewed twice by the researchers at random, according to the rules of application and qualification of the WCST.
The data were processed in Jamovi Version 2.3. Qualitative variables are expressed as frequencies and percentages, and quantitative variables are expressed as the means and standard deviations. Hypothesis tests were performed to verify the normality of the assumptions for the quantitative variables. Since the Shapiro‒Wilk test indicates deviations from the normality of the data together with the small sample size, robust statistics were used in the Walrus module, and the trimmed mean is indicated.
The Mann‒Whitney U test was used to compare total executive function between patients with and without brain deficits according to the WCST. The hypothesis was accepted with a value of p <0.05 and an effect size (95% CI). Total executive function is estimated according to Kopp [10] as the sum of the four indicators (correct answers, complete categories, perseverative errors and failures to maintain the attitude); the last two are inversely related to executive function; that is, a lower score translates into greater performance, and perseverative errors multiplied by minus one are added, with failures for the maintenance of attitude multiplied by minus one. The reliability of the instrument in the sample was estimated using Cronbach's alpha.
3. Results
Twenty-four oncopediatric patients received a palliative care protocol and were continuous with their treatment. Table 2 shows the baseline data of the participants.
Eight oncopediatric patients were classified according to their WCST results, which indicated brain deficit. The total executive function in the group was 54.25 (SD 27.61), which was considered a relatively low score for the group of oncopediatric patients; however, no deficits were observed in the 4 indicators of executive functions in more than 75% of the patients. participants.
The reliability of the instrument in the sample had a Cronbach's α of 0.804, which is considered adequate.
Table 3 shows the association between the type of diagnosis and the total score on each of the WCST subscales.
There was no association between the type of oncological diagnosis and the total performance of executive functions (p = 0.156). The two dimensions that make up the scale of executive functions, inhibition of action and maintenance of action, are consistent with the results of the total scale and have nonsignificant values (p = 0.139 and p = 0.203, respectively). We found a statistically significant difference (p = 0.044) in the complete categories, which suggested that there was an association between the type of diagnosis and maintaining the action; however, the effect size was small (ε2 = 0.351). The two-to-two Dwass-Steel-Critchlow-Fligner comparisons indicated that there were no differences in the comparisons between pairs. For example, lymphomas-leukemias, leukemias-bone tumors, and leukemias-solid tumors can be found.
We explored the differences between patients who, according to their WCST scores, had brain deficits and total executive function scores. Given that there is ample evidence of low performance in executive functions when there is a brain deficit, the hypothesis that the group without brain deficit has a higher total score in executive functions was tested (Table 4).
The difference between the two groups was statistically significant (p = 0.002), and the effect size was moderate (0.727), which suggested that a patient who had a brain deficit according to the WCST had a lower score on the executive functions test and that this difference was not due to chance (Figure 1).
Finally, we explored the association between cancer patients by type of diagnosis and the presence of acquired brain deficits (Table 5):
Fisher's exact test showed an absence of association (p = 0.690) between the type of diagnosis and having acquired brain deficits, and the strength of the association in the sample was weak according to the contingency coefficient of 0.285.
4. Discussion
Cancer is recognized worldwide as a process of uncontrolled growth of cells that directly alters the functioning of the human body and can be cured by treatments such as surgery, radiotherapy or chemotherapy if detected at an early stage. However, both quantitative and qualitative studies have shown that this pathology affects all dimensions of life, in this case, the infant, and the possible repercussions that it has on executive functioning. The brain of an infant is more sensitive to that of an adult since its maturation process, mediated by myelination, continues to develop until approximately 20 years of age. Therefore, when a toxic effect occurs during cancer treatment, the white matter is destroyed, which affects 70% of oncopediatric patients [23]. In addition, age, family history, type of cancer present and dose administered to combat it affect the cognitive, behavioral and emotional performance of children and adolescents with this diagnosis. According to a study carried out in 2017 on 62 Spanish cancer patients, they presented greater difficulties in written communication, visual memory, cognitive flexibility and the ability to plan [24,25]. In addition, deficiencies between moderate and severe attention and between processing speed and perceptual reasoning directly affect the learning process of children in their school stage [26].
Although the performance of the WCST in oncopediatric patients allowed for cross-sectional characterization or observational reporting of 24 children, the results obtained showed relatively low executive function overall, which is consistent with the findings of other high-income countries [27]. This behavior is observed among cancer survivors due to the vulnerability of executive functions and the speed of processing during treatment, which alters the function and structure of the brain [27,28]. These cognitive deficits are related to alterations in the gene expression of microglia in the prefrontal cortex. This alteration was associated with a diagnosis of cancer at an early age and exposure to chemotherapy [29]. Although the present study did not find a relationship between the type of cancer diagnosis and overall executive functioning performance (p = 0.156), a significant relationship was found between the type of diagnosis and the number of categories completed (p = 0.044; ε2 = 0.351). Phenomenon that alludes to the ability of the subjects to maintain the action and is a useful predictor of working memory performance in each individual, while the viability of the WCST has been verified through its contrast with the Wechsler Memory Scale III. This highlights its potential in the measurement of information processing and storage, as well as a predictor of high reasoning skills, concept formation and set-shifting [30]. The test is highly sensitive in the measurement of executive and cognitive dysfunction [31], in addition to its usefulness in cognitive evaluation in individuals with schizophrenic disorders and psychoactive substance abuse [32].
Despite the size of the effect of the aforementioned relationship (ε2 = 0.351), it has been observed that oncological diagnosis is linked to working memory and executive function in subjects with noncancer. related to the central nervous system involving neuroinflammatory processes and oxidative stress [33]. This phenomenon is equally attributable to the secondary cognitive impairment of chemotherapy and radiotherapy in cognitive domains [34], which include working memory and poor frontal lobe test performance [35]. On the other hand, McDonald and colleagues found hyperactivity in frontal areas using fMRI when evaluating the working memory of patients with breast cancer in contrast to the control group after receiving chemotherapy for more than two years. This finding clarifies the role of diagnosis not related to the central (peripheral) nervous system, together with its treatment, denoting the presence of compensatory hyperarousal in brain circuits associated with working memory functioning [36].
The type of cancer has been shown to be an indicator of cognitive decline [37,38]. However, Wouters and colleagues reported that a diagnosis of lymphoma in adults tends to be associated with cognitive impairment in 16% of clinical samples (n = 106) and at least 1.5 standard deviations below the control group (n = 56), despite not registering significant neuropsychological differences between the clinical group and the control group [39]. In this vein, it is pertinent to consider the existence of cognitive deficits as a phenomenon associated with a certain degree of peripheral tumor development and treatment. Next, working memory dysfunction has been observed in children with acute lymphoblastic leukemia compared with N-backs, especially given the weakness of the answers and precision. Defects have also been observed in executive functioning and cognitive flexibility measured by the WCST [40]. However, in the case of the present study, as well as the antecedents already presented, it is essential to consider the scarce association between peripheral diagnostic typologies and brain deterioration or dysfunction, suggesting the relevance of longitudinally assessing the effects of cancer treatment according to its variant to contrast its role with that of the pediatric sample.
Despite this premise, the ability of the WCST to expand the available knowledge about its construct validity was tested. We verified that there were statistically significant differences in executive function between the patients with and without brain deficits (p = 0.002), with a moderate effect size (0.727). This phenomenon highlights the existence of a deficit in executive performance in the current sample and allows us to consider the role of family, social or school variables that contribute to explaining cognitive deficiencies. This is based on variables in addition to oncological treatment, which has been shown to influence cognitive dysfunction or deterioration according to its typology given the neurotoxic effects of chemotherapy, such as methotrexate [41]. Moreover, variables such as lifestyle, lack of care for medical factors, experimentation with distress, genetics, and molecular risks have been linked to cognitive impairment associated with cancer, in addition to showing that survivors of pediatric cancer tend to experience risk of mental health problems and cognitive dysfunction [42]. In this regard, Krull and colleagues longitudinally reported cognitive dysfunction in most cognitive and behavioral domains in patients surviving acute lymphoblastic leukemia 26 years after diagnosis. The authors noted that deficits tended to occur in subjects exposed to chemotherapy and low doses of cranial radiation therapy, associating neurocognitive impairment with variables such as full-time employability and schooling. In turn, it was shown that at an earlier age after starting treatment, there was greater progressive impairment in intellect, memory and academic performance with the passage of time [43]. Thus, considering the influence of these variables is vital in the explanatory framework of brain dysfunction in pediatric and adult oncology patients in the present study.
Second, it is pertinent to note the validity of the WCST in the process of evaluating executive dysfunction in the present sample. Premise that coincides with the findings of the antecedents that have investigated the reliability and sensitivity of this test to determine the presence or absence of deficiencies at the executive level [10,30,31]. This finding invites us to discuss the criticisms that the instrument has received regarding the limitations of its ecological validity [44,45,46] and the importance of improving the latter in the executive evaluation process [47].
It is pertinent to mention that the research was carried out in an environment whose environmental control of variables was reduced, as part of the obstacles involved in the field work typical of the hospital environment, where various alterations were found in their life dynamics that revolved around the family, social, school and disease-specific dimensions, which can influence the oncopediatric process. However, in future articles, our group will address in detail this interaction between the oncopediatric aspects and the narratives of caregivers about the family process. As has been emphasized previously, despite advances in the treatment of this disease, there are various secondary effects in the short, medium and long term that cancer patients experience, generated in their majority by the different processes and transformations involved in combatting the disease. Short-term physical effects, such as nausea, pain, fatigue, weight loss, and hair loss, are produced during treatment but end when all the procedures are concluded. On the other hand, the medium-term effects are those that appear during or after treatment, such as impairments in cognitive functions and/or processes. Finally, late side effects are symptoms that appear months or years after treatment, including heart failure or second cancer. For this reason, continuing to study and follow neuropsychologically and psychologically the process of the patients who go through this diagnosis and thus safeguard their quality of life is pertinent.
With respect to the generalization of our findings in neuropsychology and psychology, we are cautious about the generalization of our results [48]. In middle-income countries such as ours, this study is considered a starting point for describing the validity of the WCST as a diagnostic and complementary tool in palliative care services in the oncopediatric population, considering the impact that treatment and diagnosis have on brain function and executive functions, as well as on future outcomes in academics and/or work performance.
5. Conclusions
The WCST is reliable for evaluating executive functioning in oncopediatric patients. Patients with an acquired brain deficit had lower scores for executive functions; these differences were not associated with the type of oncological diagnosis or with having acquired brain deficit.
The use of the WCST in the sample makes it possible to identify patients with an acquired brain deficit in a cost‒benefit relationship, which affects brain function, executive functions and health outcomes.
Author Contributions
Conceptualization, AMJ. and ABC . ; methodology, all authors. ; software, all authors. ; validation, AMJ., VS., MG and ABC. ; formal analysis, all authors. ; investigation, VS., MG; resources, XX; data curation, all authors. Writing — original draft preparation, ABC; writing — review and editing, all authors; project administration, AMJ. ; funding acquisition, AMJ and ABC. All the authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Directorate General of Research of Universidad Santiago de Cali under call No.02-2023 and the APC was funded by the Directorate General of Research of Universidad Santiago de Cali under call No.02-2023 .
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board. Patients were blinded for pairwise review (protocol code XXX and date of approval).
Informed Consent Statement
Informed consent was obtained from all the subjects involved in the study.
Data Availability Statement
Yes, this paper reviews Mendeley data and data in brief.
Acknowledgments
All patients and their families.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analysis, or interpretation of the data; in the writing of the manuscript; or in the decision to publish the results.
References
- Global Burden of Disease 2019 Cancer Collaboration, Kocarnik JM, Compton K, et al. Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. JAMA Oncol. 2022;8(3):420-444. [CrossRef]
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021 Feb 4. Epub ahead of print. PMID: 33538338. [CrossRef]
- Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Piñeros M, Znaor A, Bray F. Cancer statistics for the year 2020: An overview. Int J Cancer. 2021 Apr 5. Epub ahead of print. PMID: 33818764. [CrossRef]
- He, Fang; Huang, Haiying; Ye, Liyan; Wen, Xiulan; Cheng, Andy S. K.1. Meta-analysis of neurocognitive rehabilitation for cognitive dysfunction among pediatric cancer survivors. Journal of Cancer Research and Therapeutics 18(7):p 2058-2065, December 2022. |. [CrossRef]
- Krull KR, Hardy KK, Kahalley LS, Schuitema I, Kesler SR. Neurocognitive Outcomes and Interventions in Long-Term Survivors of Childhood Cancer [published correction appears in J Clin Oncol. 2019 Mar 1;37(7):612]. J Clin Oncol. 2018;36(21):2181-2189. [CrossRef]
- Semendric I, Pollock D, Haller OJ, George RP, Collins-Praino LE, Whittaker AL. "Chemobrain" in childhood cancer survivors-the impact on social, academic, and daily living skills: a qualitative systematic review. Support Care Cancer. 2023;31(9):532. Published 2023 Aug 22. [CrossRef]
- WHO. World health statistics 2023: monitoring health for the SDGs, sustainable development goals https://www.who.int/publications/i/item/9789240074323.
- Kusi-Mensah K, Nuamah ND, Wemakor S, et al. Assessment Tools for Executive Function and Adaptive Function Following Brain Pathology Among Children in Developing Country Contexts: a Scoping Review of Current Tools. Neuropsychol Rev. 2022;32(3):459-482. [CrossRef]
- Sun Z, Yuan Y, Xiong X, Meng S, Shi Y, Chen A. Predicting academic achievement from the collaborative influences of executive function, physical fitness, and demographic factors among primary school students in China: ensemble learning methods. BMC Public Health. 2024;24(1):274. Published 2024 Jan 23. [CrossRef]
- Kopp B, Lange F, Steinke A. The Reliability of the Wisconsin Card Sorting Test in Clinical Practice. Assessment. 2021;28(1):248-263. [CrossRef]
- Kusi-Mensah K, Nuamah ND, Wemakor S, et al. A Systematic Review of the Validity and Reliability of Assessment Tools for Executive Function and Adaptive Function Following Brain Pathology among Children and Adolescents in Low- and Middle-Income Countries [published correction appears in Neuropsychol Rev. 2022 Apr 30;:]. Neuropsychol Rev. 2022;32(4):974-1016. [CrossRef]
- Departamento Nacional de Estadística (DANE) https://www.dane.gov.co/index.php/estadisticas-por-tema/demografia-y-poblacion/proyecciones-de-poblacion.
- BERG EA. A simple objective technique for measuring flexibility in thinking. J Gen Psychol. 1948;39:15-22. [CrossRef]
- GRANT DA, BERG EA. A behavioral analysis of degree of reinforcement and ease of shifting to new responses in a Weigl-type card-sorting problem. J Exp Psychol. 1948;38(4):404-411. [CrossRef]
- Steinke A, Lange F, Kopp B. Parallel model-based and model-free reinforcement learning for card sorting performance. Sci Rep. 2020;10(1):15464. Published 2020 Sep 22. [CrossRef]
- Kopp B, Al-Hafez B, Steinke A. Habits, Goals, and Behavioral Signs of Cognitive Perseveration on Wisconsin Card-Sorting Tasks. Brain Sciences. 2023; 13(6):919. [CrossRef]
- The jamovi project (2022). jamovi. (Version 2.3) [Computer Software]. Retrieved from https://www.jamovi.org.
- R Core Team (2021). R: A Language and environment for statistical computing. (Version 4.1) [Computer software]. Retrieved from https://cran.r-project.org. (R packages retrieved from MRAN snapshot 2022-01-01).
- Kazuki, Y. (2019). tableone: Create 'Table 1' to Describe Baseline Characteristics. [R package]. Retrieved from https://CRAN.R-project.org/package=tableone.
- Serdar Balci (2022). ClinicoPath jamovi Module. [R package]. Retrieved from https://github.com/sbalci/ClinicoPathJamoviModule. link. [CrossRef]
- Kerby, D. S. (2014). The simple difference formula: An approach to teaching nonparametric correlation. Comprehensive Psychology, 3, 2165–2228. [CrossRef]
- Sing, T., Sander, O., Beerenwinkel, N., & Lengauer, T. (2015). ROCR: Visualizing the Performance of Scoring Classifiers. [R package]. Retrieved from https://cran.r-project.org/package=ROCR.
- Hernández Martínez Montserrat, Pastor Hernández Nuria. Afectación neuropsicológica como secuela del tratamiento oncológico. Rev Pediatr Aten Primaria [Internet]. 2020 Mar [citado 2024 Feb 02] ; 22(85): e27-e30. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1139-76322020000100010&lng=es. Epub 03-Ago-2020.
- Arce B, Grañana N. Alteraciones cognitivas por quimioterapia en pacientes con cáncer de mama: una revisión bibliográfica [Cognitive deficits with chemotherapy in women with breast cancer: a bibliographic revisión]. Rev Fac Cien Med Univ Nac Cordoba. 2023 Jun 30;80(2):126-133. Spanish. PMID: 37402295; PMCID: PMC10443418. [CrossRef]
- García Gómez, R. Estudio de las funciones cognitivas en sujetos con leucemia infantil. 2017. http://hdl.handle.net/10366/137319.
- González, A., et al. "Perfil cognitivo de niños con meduloblastoma que culminaron su tratamiento oncológico: caracterización de los procesos mnésicos." Med. infant 2011: 190-197.
- Jacola LM, Litten M, Reddick WE, Krull KR. Structural and Functional Brain Imaging in Long-Term Survivors of Childhood Acute Lymphoblastic Leukemia Treated With Chemotherapy: A Systematic Review. JNCI Cancer Spectr. 2021;5(5):pkab069. Published 2021 Aug 11. [CrossRef]
- Cheung YT, Sabin ND, Reddick WE, et al. Leukoencephalopathy and long-term neurobehavioral, neurocognitive, and brain imaging outcomes in survivors of childhood acute lymphoblastic leukemia treated with chemotherapy: a longitudinal analysis. Lancet Hematol. 2016;3(10):e456-e466. [CrossRef]
- Laaker CJ, Cantelon C, Davis AB, et al. Early life cancer and chemotherapy lead to cognitive deficits related to alterations in microglial-associated gene expression in prefrontal cortex. Brain Behav Immun. 2023;113:176-188. [CrossRef]
- Kafadar, Hatice, Hasibe Arıcan Süren, and Selin Yılmaz. "A comparison of individuals whose capacity of working memory is high and low from the perspective of WCST performance." Anatomy: International Journal of Experimental & Clinical Anatomy 16 (2022).
- Mackey, WE, Devinsky, O., Doyle, WK, Meager, MR, & Curtis, CE. The Human Dorsolateral Prefrontal Cortex Is Not Necessary for Spatial Working Memory. Journal of Neuroscience, 2016, 36 (10), 2847–2856. [CrossRef]
- Faustino, B., Oliveira, J., & Lopes, P. (2019). Diagnostic precision of the Wisconsin Card Sorting Test in assessing cognitive deficits in substance use disorders. Applied Neuropsychology: Adult, 1–8. [CrossRef]
- Joly F, Giffard B, Rigal O et al. Impact of cancer and its treatments on cognitive function: advances in research from the Paris International Cognition and Cancer Task Force Symposium and update since 2012. J Pain Symptom Manage 2015; 50 (6): 830–841.
- Coomans, M. B., van der Linden, S. D., Gehring, K., & Taphoorn, M. J. B. Treatment of cognitive deficits in brain tumor patients. Current Opinion in Oncology, 2019. 1. [CrossRef]
- Lange, M., Joly, F., Vardy, J., Ahles, T., Dubois, M., Tron, L., Winocur, G., De Ruiter, M. B., & Castel, H. Cancer-related cognitive impairment: an update on state of the art, detection, and management strategies in cancer survivors. Annals of Oncology, 2019. 30(12), 1925–1940. [CrossRef]
- McDonald BC, Conroy SK, Ahles TA, West JD, Saykin AJ. Alterations in brain activation during working memory processing associated with breast cancer and treatment: a prospective functional magnetic resonance imaging study. J Clin Oncol. 2012 Jul 10;30(20):2500-8. Epub 2012 Jun 4. PMID: 22665542; PMCID: PMC3397784. [CrossRef]
- Wefel JS, Kesler SR, Noll KR, Schagen SB. Clinical characteristics, pathophysiology, and management of noncentral nervous system cancer-related cognitive impairment in adults. CA Cancer J Clin. 2015 Mar;65(2):123-38. Epub 2014 Dec 5. PMID: 25483452; PMCID: PMC4355212. [CrossRef]
- Lange M, Joly F, Vardy J, Ahles T, Dubois M, Tron L, Winocur G, De Ruiter MB, Castel H. Cancer-related cognitive impairment: an update on state of the art, detection, and management strategies in cancer survivors. Ann Oncol. 2019 Dec 1;30(12):1925-1940. PMID: 31617564; PMCID: PMC8109411. [CrossRef]
- Wouters H, Baars JW, Schagen SB. Neurocognitive function of lymphoma patients after treatment with chemotherapy. Acta Oncol. 2016 Sep-Oct;55(9-10):1121-1125. Epub 2016 Jun 22. PMID: 27333078. [CrossRef]
- Firoozi, M., & Azadfar, Z. Working Memory Performance, Attention Maintenance and Executive Function in Children with Acute Lymphoblastic Leukemia. International Journal of Cancer Management, 2017. 10(7). [CrossRef]
- Janelsins MC, Heckler CE, Peppone LJ, Kamen C, Mustian KM, Mohile SG, Magnuson A, Kleckner IR, Guido JJ, Young KL, Conlin AK, Weiselberg LR, Mitchell JW, Ambrosone CA, Ahles TA, Morrow GR. Cognitive Complaints in Survivors of Breast Cancer After Chemotherapy Compared With Age-Matched Controls: An Analysis From a Nationwide, Multicenter, Prospective Longitudinal Study. J Clin Oncol. 2017 Feb 10;35(5):506-514. Epub 2016 Dec 28. PMID: 28029304; PMCID: PMC5455314. [CrossRef]
- Vannorsdall TD. Cognitive Changes Related to Cancer Therapy. Med Clin North Am. 2017 Nov;101(6):1115-1134. Epub 2017 Aug 25. PMID: 28992858. [CrossRef] [PubMed]
- Krull KR, Brinkman TM, Li C, Armstrong GT, Ness KK, Srivastava DK, Gurney JG, Kimberg C, Krasin MJ, Pui CH, Robison LL, Hudson MM. Neurocognitive outcomes decades after treatment for childhood acute lymphoblastic leukemia: a report from the St Jude lifetime cohort study. J Clin Oncol. 2013 Dec 10;31(35):4407-15. Epub 2013 Nov 4. PMID: 24190124; PMCID: PMC3842908. [CrossRef]
- Chiu EC, Wu WC, Hung JW, Tseng YH. Validity of the Wisconsin Card Sorting Test in patients with stroke. Disabil Rehabil. 2018 Aug;40(16):1967-1971. Epub 2017 May 11. PMID: 28494623. [CrossRef]
- Adjorlolo S. Ecological validity of executive function tests in moderate traumatic brain injury in Ghana. Clin Neuropsychol. 2016 Jan-Dec;30(sup1):1517-1537. Epub 2016 Apr 13. PMID: 27071720. [CrossRef]
- Gómez-de-Regil L. Assessment of Executive Function in Patients with Traumatic Brain Injury with the Wisconsin Card-Sorting Test. Brain Sci. 2020 Oct 1;10(10):699. PMID: 33019772; PMCID: PMC7600451. [CrossRef]
- Diercks CM, Gunther KE, Teti DM, Lunkenheimer E. Ecological validity in measuring parents' executive function. Child Dev Perspect. 2022 Dec;16(4):208-214. Epub 2022 Sep 2. PMID: 36590076; PMCID: PMC9799100. [CrossRef]
- Malik HB, Norman JB. Best Practices and Methodological Strategies for Addressing Generalizability in Neuropsychological Assessment. J Pediatr Neuropsychol. 2023;9(2):47-63. Epub 2023 May 13. PMID: 37250805; PMCID: PMC10182845. [CrossRef]
Figure 1.
Descriptive plot: differences in medians between the oncopediatric groups.
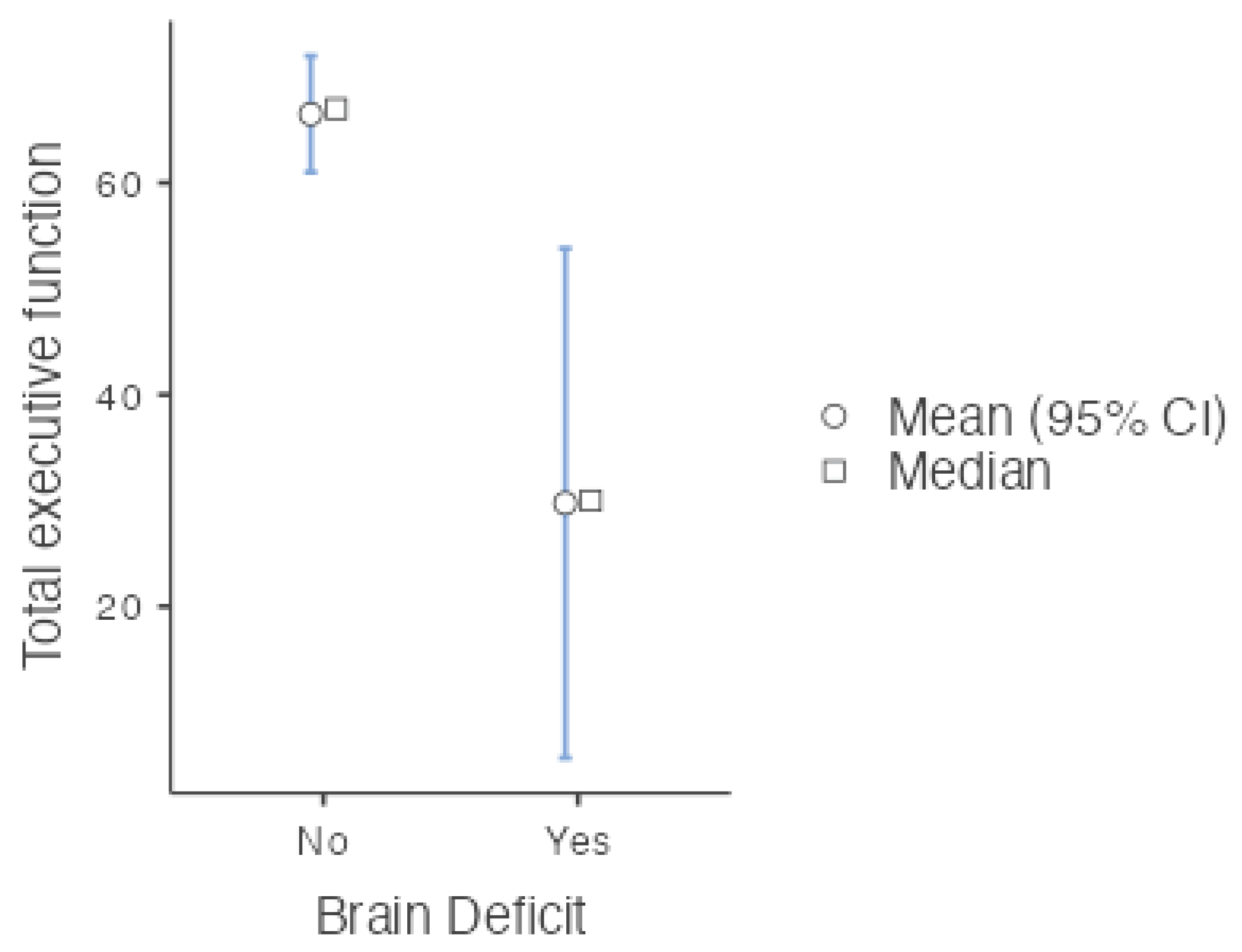

Table 1.
Classification according to the direct score obtained on the WCST.
| Classification | Threshold | Score |
| Significantly deficient | Severe impairment | 0-54 |
| Severe to moderate impairment | 55-61 | |
|
Poor |
Moderate deterioration | 62-69 |
|
Borderline Expected |
Moderate to intermediate Intermediate deterioration |
70-76 77-84 |
| Below average | 85-91 | |
| Medium | 92-106 | |
| Above average | 107 + | |
Note: In this research, scores between 0 and 84 according to the manual were assumed to indicate brain deficit. Scores between 85 and 107+ expected brain function according to age scale.
Table 2.
Sociodemographic characteristics and performance on the WCST.
| Overall |
| n 24 |
| Age (mean (SD)) 12.08 (3.98) |
| Sex = Woman (%) 5 (20.8) |
| Department (%) |
| Cauca 10 (41.7) |
| Caqueta 2 (8.3) |
| Valley 12 (50.0) |
| Study = No (%) 5 (20.8) |
| Health regime 1 = Contributory (%) 5 (20.8) |
| Typology Dx (%) |
| Leukemias 17 (70.8) |
| Lymphomas 3 (12.5) |
| Bone tumor 3 (12.5) |
| Solid tumor 1 (4.2) |
| 4 years or more Dx (%) |
| No 17 (70.8) |
| Yes 4 (16.7) |
| Does not record 3 (12.5) |
| Palliative Care Value = No. (%) 15 (62.5) |
| Radiation therapy = No. (%) 19 (79.2) |
| Step home (%) |
| Yes 12 (50.0) |
| No 10 (41.7) |
| Does not record 2 (8.3) |
| Family function (%) |
| Functional 17 (70.8) |
| Dysfunctional 3 (12.5) |
| Does not record 4 (16.7) |
| Treatment goal = Palliative (%) 2 (8.3) |
| Laterality = Left-handed (%) 2 (8.3) |
| Correct answers (mean (SD)) 74.12 (13.02) |
| Response Deficit = No (%) 18 (75.0) |
| Complete categories (mean (SD)) 4.46 (1.79) |
| Deficit Categories = No. (%) 18 (75.0) |
| Perseverative errors (mean (SD)) 22.75 (16.17) |
| Perseverative error deficit = No (%) 18 (75.0) |
| Maintaining attitude (mean (SD)) 1.58 (1.72) |
| Maintenance attitude deficit = No (%) 20 (83.3) Maintenance action (mean (SD)) 78.58 (14.19) |
| Action inhibition (mean (SD)) -24.33 (15.95) |
| Total executive function (mean (SD)) 54.25 (27.61) |
| Brain Deficit = Yes (%) 8 (33.3) |
1 The health regime in Colombia is public (subsidized) or private (contributory).
Table 3.
ANOVA of a Kruskal‒Wallis factor.
| Subscale and total | χ2 | gl | p | ε2 | |
|---|---|---|---|---|---|
| Total executive function | 5.23 | 3 | 0.156 | 0.227 | |
| Inhibition action | 5.50 | 3 | 0.139 | 0.239 | |
| Maintenance Action | 4.61 | 3 | 0.203 | 0.200 | |
| Maintain attitude | 3.02 | 3 | 0.388 | 0.131 | |
| Perseverative mistakes | 5.04 | 3 | 0.169 | 0.219 | |
| Complete categories | 8.08 | 3 | 0.044 | 0.351 | |
| Correct answers | 4.07 | 3 | 0.254 | 0.177 | |
Table 4.
Independent Samples T Test.
| 95% Confidence Interval | |||||||
|---|---|---|---|---|---|---|---|
| Statistic | p | Effect Size | Lower | Upper | |||
| Total executive function | Mann‒Whitney U | 17.5 | 0.002 | Rank biserial correlation | 0.727 | ||
Note. H ₐ μ No > μ Yes.
Table 5.
Contingency table by type of diagnosis and brain deficit.
| Brain Deficit | ||||
|---|---|---|---|---|
| Type of diagnosis | No | Yes | Total | |
| Leukemias | Observed | 12 | 5 | 17 |
| % within row | 70.6 % | 29.4 % | 100.0 % | |
| Lymphomas | Observed | 1 | 2 | 3 |
| % within row | 33.3 % | 66.7 % | 100.0 % | |
| Bone tumor | Observed | 2 | 1 | 3 |
| % within row | 66.7 % | 33.3 % | 100.0 % | |
| Solid tumor | Observed | 1 | 0 | 1 |
| % within row | 100.0 % | 0.0 % | 100.0 % | |
| Total | Observed | 16 | 8 | 24 |
| % within row | 66.7 % | 33.3 % | 100.0 % | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



