
Submitted:
20 February 2024
Posted:
21 February 2024
You are already at the latest version
Abstract
In patients with primary central nervous system lymphoma (PCNSL), the choice of surgical strategy for histopathologic assessment is still controversial, particularly in terms of preoperative corticosteroid (CS) therapy. To provide further evidence for clinical decision-making, we retrospectively analyzed data from 148 consecutive patients who underwent surgery at our institution. Although patients treated with corticosteroids preoperatively were significantly more likely to require a second or third biopsy (p=0.049), it was only necessary in less than 10% of the cases with preoperative corticosteroid treatment. The choice of surgical procedure did not affect diagnostic accuracy (p>0.05). Preoperative CSF sampling did not provide additional information but was associated with delayed surgery (p=0.02). Surprisingly, diagnostic accuracy was significantly lower when patients were treated with anticoagulation or dual antiplatelet therapy (p=0.015). In conclusion, preoperative CS therapy can challenge the histological diagnosis of PCNSL. At the same time, our data suggest that preoperative CS treatment only presents a relative contraindication for an early surgical intervention. The standard surgical approach is stereotactic biopsy, but other approaches can be individually considered. If a definitive diagnosis cannot be made after the first surgical intervention, the timing of a repeat biopsy after discontinuation of CS remains a case-by-case decision.
Keywords:
primary central nervous system lymphoma
; stereotactic biopsy
; corticosteroid
; histopathology
; brain tumor
1. Introduction
Primary Central Nervous System B-cell lymphoma (PCNSL) is a subtype of extranodal non-Hodgkin lymphoma confined to the brain, leptomeninges, spinal cord and eyes without a systemic manifestation [1]. It accounted for approximately 1.9% (incidence of 0.43 per 100.000) of primary brain tumors in the United States of America between 2011 and 2015 [2], has shown a continuous rise in its incidence in the past decades and can occur in immunocompetent or immunocompromised patients [3]. Therapeutically, it represents a significant challenge, with approximately only every second patient surviving the first 12 months after diagnosis [2].
To verify the diagnosis of PCNSL, a histopathological diagnosis is essential [3]. However, the preferred surgical approach remains a controversial topic. A randomized phase III study showed a partial benefit of PCNSL resection for patients’ outcomes [4,5]. Subsequently, tumor resection might be a feasible option in some cases yet bares the risk of unintentionally resecting non-cancerous tissue or other brain tumors as they can often not be distinguished from PCNSL by clinical presentation or Magnet Resonance Imaging (MRI) alone [6]. Therefore, stereotactic biopsy remains the most common surgical approach to verify the diagnosis of PCNSL today [3]. One problem with the histopathological diagnosis of PCNSL that is not seen in the majority of other primary brain tumors is their strong response to corticosteroids (CS).
In cases of unclear intracranial mass lesions or autoimmune neuroinflammation, which are common differential diagnoses of PCNSL, high-dose CS are a practical and frequently used preoperative treatment. [7,8]. While CS lead to a decrease in symptomatic tumor-associated edema without significantly affecting the tumor cells in most other brain tumors, they have an additional tumor-destructive effect in PCNSL. Via the glucocorticoid receptor, mitogen-activated protein kinases are activated, ultimately resulting in apoptosis of the PCNSL cells. [9,10,11] (Figure 1).
While the CS effect may be desirable for short-term improvement of neurological symptoms, it carries the risk of obscuring the diagnosis, thus significantly impairing the necessary therapy and the long-term outcome. Preoperative treatment with CS may even mimic inflammatory diseases in PCNSL [12]. Therefore, clinical guidelines recommend avoiding the application of CS when PCNSL is suspected and patients’ clinical condition does not obligate CS treatment [3].
This dilemma leads to numerous problems in everyday clinical practice that need to be resolved by case-by-case decisions: should CS be used at the risk of prolonging diagnosis and causal treatment? Or should CS be avoided at the risk of depriving patients of effective symptomatic treatment? In addition, the feasibility of diagnosing PCNSL patients treated with CS may influence the decision on the optimal timing of surgery. Should the histopathologic diagnosis be rushed to allow earlier postoperative CS treatment? Or should surgery be delayed if patients have received preoperative CS to increase the chances of a definite histopathologic diagnosis?
In this study, we aimed to (1) compare the accuracy rate of histopathologic diagnosis of PCNSL with or without preoperative CS treatment, (2) investigate the accuracy rate of histopathologic diagnosis after CS treatment depending on the time interval from the last CS application, (3) analyze whether different surgical approaches (e.g., stereotactic vs. open biopsy) provide an advantage for histopathologic diagnosis of PCNSL, and (4) extrapolate possible implications for clinical decision-making.
2. Materials and Methods
This retrospective single-center observational study comprised all consecutive patients who underwent biopsy or resection of PCNSL between October 2008 and November 2022. The study was conducted under the Declaration of Helsinki, was compliant with the Health Insurance Portability and Accountability Act of 1996 (HIPAA) guidelines, and was approved by the Institutional Review Board of the University of Essen (protocol code 22-11037-BO, date of approval: 09.01.2023). All patients included were referred to us with an unclear brain lesion from other regional health care providers or departments after our interdisciplinary neurooncological tumor board had recommended a neurosurgical intervention. Therefore, the preoperative diagnostics and therapy (including the application of CS) were highly heterogeneous. The histopathological diagnosis was classified by routine histology following WHO criteria [13]. Only the cases with histological confirmation of PCNSL diagnosis were included. PCNSL that were diagnosed without a biopsy at our institution were excluded. Basic demographic and clinical data, such as type of surgical intervention, CS treatment, suspected diagnosis and surgical intervention success, obtained within the routine clinical assessment framework, were collected from the hospital database. Preoperative imaging consisted of MRI with at least T1- and T2-weighted sequences with and without contrast agent as well as Fluid Attenuated Inversion Recovery (FLAIR) sequences and were independently evaluated by two experienced neuroradiologists.
Statistical analysis was done using IBM SPSS Statistics 28 (IBM Corporation, Armonk, NY, USA). For demographic data, we reported numbers, percentages, medians and interquartile ranges. Normality was tested by the Shapiro-Wilk test. As normal distribution was always rejected, differences between groups were determined using the Kruskal Wallis test (KW) with posthoc Dunn’s test (D-B)/the Mann-Whitney-U-test (MWU-B) with correction of the significances according to Bonferroni for ordinal and metric variables or the chi-squared and Fisher’s exact test for categorical variables. Correlations were evaluated using Spearman’s correlation coefficient. The significance level was set to p < 0.05.
3. Results
3.1. The majority of PCNSL were diagnosed by stereotactic biopsies
In total, we identified 148 patients who underwent a neurosurgical procedure at our institution between October 2008 and November 2022 to confirm the histopathologic diagnosis of PCNSL. A slight majority of these patients were male (n=88, 59.5 %), and the median age in our cohort was 70 years (interquartile range: 60 - 76 years). In most cases, a stereotactic biopsy was performed to confirm the diagnosis (n=96, 64.9%). In the remaining cases, sampling was performed by open biopsy (n=25, 16.9%), partial or complete tumor resection (n=22, 14.9%), or other surgical procedures (n=5, 3.4%), such as endoscopic biopsy. Most patients required only one biopsy to confirm the diagnosis (n=138, 93.2 %). Eight patients underwent a second surgery (5.4 %), and two patients required three biopsies (1.4 %). The tissue sample was most frequently taken from the frontal lobe (n=66, 44.6%), followed by basal ganglia/thalamus (n=21, 14.2%), occipital (n=16, 10.8%), parietal (n=13, 8.8%) and temporal lobe (n=9, 6.1%). Nine patients had infratentorial biopsies (6.1%), and 14 had other locations (9.5%), e.g. intraventricular. In the majority of cases (n=109, 73.6%), the treating physicians already suspected PCNSL preoperatively, while 39 (26.4%) procedures were performed under different assumptions (e.g., suspected glioma). PCNSL were highly proliferative with a median Ki67 staining of 80% (quartiles: 70-80%, not determined in two cases) and were surgically treated at a median of eight days after MRI diagnosis (4-17 days). Regarding the preoperative clinical status, 32 patients (21.6%) had ECOG status 0, 61 patients (41.2%) had ECOG status 1, 29 patients (19.6%) had ECOG status 2, 20 patients (13.5%) had ECOG status 3 and 6 patients (4.1%) had ECOG status 4.
3.2. Patients treated with CS had a slightly higher risk of an unsuccessful first biopsy
Fifty-seven (38.5%) patients received preoperative CS treatment. Information on the type and dosage of the corticosteroid was rarely available as most patients were previously treated at external hospitals and referred for surgical biopsy after MRI diagnosis. In fifty of the 57 cases (87.7 %), the diagnosis of PCNSL was confirmed after the first biopsy despite preoperative CS therapy. Five patients (8.8%) required two biopsies, and two (3.6%) required a total of three surgical procedures to confirm the diagnosis of PCNSL. In the 91 patients who had not received corticosteroids, the first biopsy was successful in 88 cases (96.7%), which was a slightly higher rate than in the CS group (p=0.049, Fisher’s exact test), and only three patients (3.3%) required a second operation.
CS was in median discontinued 11 days (quartiles 4 – 15 days) before a successful first biopsy. In contrast, CS was discontinued 1, 4, 6, 8, 8, and 30 days (information missing for one patient) before surgery in the subgroup of patients who had an unsuccessful first biopsy after administration of CS (Table 1). The time at which CS was discontinued preoperatively did not differ significantly between patients with successful and unsuccessful first biopsies (p>0.05, MWU). Not surprisingly, patients that were treated with CS had a considerably longer time between initial MRI and surgery (13 days [quartiles 6-26 days] vs. seven days [quartiles 3-14.5 days], p < 0.01, MWU)—this time correlated to the time that CS was paused (r=0.53, p<0.01, Spearman, Figure 2a).
3.3. The surgical approach did not influence the accuracy of the histopathologic diagnosis and depended mainly on the suspected diagnosis
Interestingly, we did not observe a significant difference regarding successful tissue sampling between stereotactic and open surgery techniques (p>0.05, Fisher’s exact test). However, the surgical methods chosen significantly differed depending on the patients’ CS treatment. In patients with preoperative CS, open biopsies (12/57, 21.1% compared to 13/91, 14.3%) and especially tumor resections (14/57, 24.6%, compared to 8/91, 8.8%) were more common. In contrast, patients not treated with CS underwent stereotactic biopsies (65/91, 71.4% compared to 31/57, 54.4%) and other interventions (e.g., endoscopic biopsies; 5/91, 5.5% compared to 0/57, 0%) more often. However, it should be noted that surgical intervention was primarily related to the preoperative assessment of whether PCNSL was suspected. Accordingly, most patients received a stereotactic biopsy (82/109, 75.2% compared to 14/39, 35.9%) or other surgical intervention (5/109, 4.6%, compared to 0/39, 0%) when PCNSL was suspected. In contrast, resections were more frequently chosen when other differential diagnoses were suspected (18/39, 46.2% vs. 4/109, 3.7%, p<0.01, Fisher’s exact test). Open biopsies were equally frequent in both groups (17.9% vs. 16.5%). We also observed a slight tendency for patients with suspected PCNSL to have received CS less frequently (p>0.05, chi-square test).
3.4. Anticoagulation or platelet inhibition delayed surgery and was associated with the lower success of the biopsy
Next, we wondered whether patients treated with antiplatelet therapy (PI) or anticoagulation (AC) may have had a disadvantage, such as additional delay or impaired diagnostic accuracy due to a more cautious surgical approach. Although most of the patients were treated with neither PI nor AC (n=104, 70.3%), 27 received single PI (18.2%), and four received double PI (2.7%). Twelve patients received AC (6 / 4.1 % with coumarin derivatives, 1 / 0.7 % with heparin, 4 / 2.7 % with direct oral AC, and 1 0.7 % in combination with PI; no information was available for one patient). In 36 cases (24.3%), AC or PI treatment was entirely suspended before surgery. Twice (1.4%), one of multiple medications was continued while the others were discontinued, and five patients (3.4%) required surgery while receiving AC or PI. Not surprisingly, the time between MRI and surgery was significantly longer in patients treated with double PI or AC than in those treated with neither medication (p=0.012, KW; p=0.028, D-B; Figure 2b). Simple PI showed a non-significant tendency towards a longer preoperative time. The surgical methods chosen were independent of AC/PI (p<0.05, Fisher’s exact test). On the other hand, the biopsy success rate was not. Five of the patients who were treated with neither AC/PI (4.8%) and one patient with single PI (3.7%) required a second biopsy, while the first biopsy was unsuccessful in 4 of the 16 patients treated with double PI or AC (25%, p=0.015, Fisher’s exact test). In addition, both patients with PCNSL diagnosed after the third biopsy were treated with PI/AC prior to surgery.
3.5. Cerebrospinal fluid (CSF) diagnostics were independent of previous CS treatment
Preoperative diagnostics included a histopathological examination of the cerebrospinal fluid in almost half of our cases (n=65, 43.9%). Twenty-nine of these (44.6%) showed no abnormalities, 30 showed mild (46.2%) and four severe pleocytosis (6.2%). Only twice (3.1%) did the pathologists find cells strongly suspicious for PCNSL. Fluorescence-activated cell sorting (FACS) was reported for 32 cases (21.6 %). Of these, 26 were classified as unremarkable (81.3 %), while FACS identified malignant or suspicious cells in six patients (18.8 %). Though CSF diagnostics indicated suspicious results in a few of our cases, neither pathological examination nor FACS were sufficient to reach a definitive diagnosis. CSF findings were independent of previous CS treatment, whether analyzed by a pathologist or FACS (p>0.05, Fisher’s exact test). Interestingly, the time between MRI and surgery differed between patients who underwent preoperative lumbar puncture (median: 10d [quartiles 6.75-19.5d]) and those who did not (median: 6.5d [quartiles: 2-15 d], p=0.02; MWU; Figure 2c).
4. Discussion
In line with previously published data, stereotactic biopsies were performed on most patients in the presented cohort [3,5]. The surgical approach was not associated with a successful histopathologic diagnosis, which is consistent with most previous studies. However, a small meta-analysis by Scheichel et al. found an inconclusive stereotactic biopsy rate of 8.6% after CS treatment and 1.9% without CS treatment [14]. In their analysis, open surgical procedures yielded the histopathologic diagnosis in all cases, largely similar to our observations [14]. We suspect that the presented cohort is too small to detect the marginal difference in diagnostic accuracy concerning surgical technique.
Nevertheless, the choice of surgical approach remains an individual decision. The traditional view that resection of PCNSL might even be an unfavorable prognostic factor has been challenged by Weller et al., who described the benefit of tumor resection [5,15,16,17,18]. More recent studies have supported the hypothesis that at least a subgroup of patients may benefit from tumor resection [19,20,21]. However, a retrospective analysis of the French oculo-cerebral lymphoma network, which included over 1,000 subjects, showed no association between tumor resection and patient outcomes [22]. Still, stereotactic biopsies offer high diagnostic accuracy with comparatively low risk and may be preferred when there are no specific reasons for an open approach [23,24].
Interestingly, PCNSL was not the suspected diagnosis in one out of four biopsies. Most patients who underwent tumor resection also belonged to this group, suggesting that the decision for tumor resection instead of stereotactic biopsy was often made under the assumption of a different diagnosis. An alternative way to detect a PCNSL and an essential part of the diagnostic work-up is CSF cytomorphology and FACS. Previous studies reported that CSF diagnostics can only verify the correct diagnosis in a minority of cases [25]. However, we could neither confirm nor refute these observations, as patients whose PCNSL could be diagnosed without a surgical intervention were excluded from our study by design. Notably, the detection rate of suspicious cells via FACS was superior to conventional cytopathology, as already hypothesized before [26,27,28] and was not influenced by previous CS treatment. However, it deserves to be noted that newer methods of CSF diagnostics, such as ultrasensitive circulating tumor DNA sequencing, show promising results to set a new standard [29]. The time to surgery was significantly longer for patients who received a lumbar puncture. While it seems reasonable to perform preoperative CSF diagnostics because it might avoid surgical intervention, the decision should be weighed against the potential risk of a diagnostic delay [25].
One of the most essential clinical questions when PCNSL is a possible differential diagnosis is whether patients should be treated with CS and whether a prompt biopsy after CS administration is still useful. Our analysis showed a slightly lower success in confirming the diagnosis when CS was given before surgery. While this trend was to be expected, it is surprising that the success rate of the first biopsy was above 90% in both groups. Previous studies on this topic have provided mixed results: Brück et al. reported non-specific changes without clear evidence of PCNSL in 112 of 221 (>50%) biopsy specimens after CS therapy and concluded that CS should be avoided if possible [30]. In contrast, Porter et al. reported that only 8/68 (12%) of their cohort required a second biopsy after CS [31], suggesting that a biopsy under CS can be performed with high diagnostic accuracy if contrast enhancement is preserved on MRI. It should be noted that 42 of their patients even underwent surgery during CS treatment [31]. Bullis et al. agree with the conclusions of Porter et al., while Haldorsen et al. report that repeat biopsies are required in 22% of patients [32,33].
Manoj et al. provide a differentiated observation by dividing their collective depending on the duration of CS treatment: Similar to the reports from Brück et al., biopsies were inconclusive in up to 57% of their collective of patients that received CS for over one week [34]. A possible explanation for these discrepancies might, except from regional differences, lie in the high degree of interobserver variability, as reported by Önder et al. [35]. Velasco et al. examined additional aspects [36]. Similar to our collective, they reported that patients treated with CS required a second biopsy more frequently. However, the rate of an unsuccessful biopsy in both groups was low compared to other trials (12% vs. 4%). Secondly, they investigated the effect of pausing CS before surgery and stated that CS tapering and the duration of CS pause before surgery did not influence the likelihood of a false-negative result, which is supported by our observations [36].
Further, despite the high diagnostic accuracy after CS treatment, patients of their cohort who received CS suffered a diagnostic delay that was, once again, mirrored in our collective [36]. The reasons for this delay cannot be answered with certainty. Still, one might speculate that a delay before surgery due to CS withdrawal, as noticeable in the study by Velasoco et al., might play a significant role [36]. Also, clinical practice suggests that there is a collective of patients who are initially misdiagnosed and might receive CS as a therapeutic option before a biopsy is finally performed.
In 2021, Scheichel et al. conducted a small meta-analysis that included data from their own cohort and several of the studies mentioned above. Interestingly, they found that CS had no effect on diagnostic accuracy in their own cohort but concluded that CS treatment led to an increased risk of inconclusive biopsies in the meta-analysis with an odds ratio of about 3.1. The success of the biopsy did not differ in the meta-analysis, regardless of whether CS was continued or paused [14].
A delay in diagnosis, e.g., due to a delay in surgery because of CS treatment, has been described as a negative prognostic factor in PCNSL [37]. In clinical practice, a common reason for delayed surgery is the use of anticoagulant medication. As expected, we observed a longer interval between the first MRI and surgery in patients treated with AC or dual PI, whereas single PI seemed to delay surgery only slightly.
However, to our surprise, a second or third biopsy was more frequently required to verify PCNSL in patients treated with AC or dual PI. Coagulation-related complications are not uncommon in lymphoma patients, but to our knowledge, there is no known impact on tumor growth or diagnostic accuracy [38,39,40]. Although the surgical methods did not differ significantly between the two groups, it could be hypothesized that an increased risk of bleeding may have prompted surgeons to proceed more cautiously. Also, the delay before surgery may have led to the use of higher doses of CS. Apart from an unknown bias, we cannot exclude the possibility of statistical chance and, therefore, look forward to future studies to reproduce or refute this observation.
Most immunocompetent PCNSL patients have neuropsychiatric deficits as their primary symptom. However, one in three patients shows signs of increased intracranial pressure, and one in six patients suffers from seizures at an early stage [15,41]. These symptoms can significantly impair the patient’s quality of life or even lead to life-threatening situations. They can also improve dramatically after the administration of glucocorticoids due to the reduction of brain edema and cytotoxic activity [42]. In our collective of patients treated preoperatively with CS, unsuccessful biopsies were more frequent. Nevertheless, PCNSL could be correctly diagnosed in over 90% of cases, and the diagnostic accuracy could be further increased by additional molecular diagnostics [43].
We hypothesize that the widespread concern about jeopardizing the histologic diagnosis by preoperative CS therapy may be overly cautious. When necessary, the pursuit of ideal biopsy conditions should not lead clinicians to withhold effective treatment from patients with suspected PCNSL and severe symptoms. Our data suggest that preoperative CS treatment does not present a definitive contraindication for an early surgical intervention. If the first biopsy was unsuccessful, a second biopsy after CS therapy was discontinued yielded the correct diagnosis with few exceptions. However, like other authors, we could not establish a threshold for the ideal duration of discontinuation of CS [14]. Therefore, if a definitive diagnosis cannot be made after the first surgical intervention, a second biopsy after discontinuation of CS appears sensible but remains an individual case-by-case decision.
This study has some limitations that need to be considered: (1) Only patients whose PCNSL was diagnosed in our institute were included. Therefore, we cannot exclude that patients with PCNSL and an unsuccessful first biopsy may have died or refused reoperation and are therefore not included in the study population. (2) As patients were referred to us from regional centers, we cannot exclude a selection bias, which may have led us to overestimate the number of inconclusive biopsies. Data on the duration and dosage of CS treatment were also incomplete and could not be analyzed in more detail. However, as these observations relate to real-life situations where physicians often have to make decisions with incomplete data, we still consider them very valuable. (3) The study might be biased due to its retrospective and monocentric nature. (4) The study included patients treated over a decade and a half. Changes in clinical standards or procedures may also have affected the observations.
5. Conclusions
Preoperative treatment with CS for suspected PCNSL should be avoided, if possible, but should not be withheld from patients at all costs. Even after CS treatment, an early biopsy is justified, as the diagnostic accuracy remains high. Therefore, our data suggest that preoperative CS treatment only presents a relative contraindication for an early surgical intervention. The standard surgical procedure is stereotactic biopsy. If a definitive diagnosis cannot be made after the first surgical intervention, the timing of a repeat biopsy after discontinuation of CS remains a case-by-case decision.
Author Contributions
Conceptualization, J.F., and K.H.W.; methodology, J.F., C.D., A.J. and K.H.W.; software, J.F. and J.A.F..; validation, R.J., C.D., A.J., U.S. and K.H.W.; formal analysis, J.F., M.D.O. and J.A.F.; investigation, J.F..; resources, U.S and K.H.W.; data curation, J.F. and R.J.; writing—original draft preparation, J.F. and K.H.W.; writing—review and editing, K.H.W., U.S., W.D.O., A.K.U., O.G., Y.A., and J.A.F.; visualization, J.F., C.D., A.J. and J.A.F.; supervision, K.H.W. and U.S.; project administration, K.H.W. and U.S.; funding acquisition, K.H.W. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of the University of Essen (protocol code: 22-11037-BO; date of approval: 09.01.2023).
Informed Consent Statement
Not applicable.
Data Availability Statement
All data are contained within the manuscript. Raw data are available on reasonable request from the corresponding author. The data are not publicly available due to ethical restrictions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Batchelor, T.; Loeffler, J.S. Primary CNS lymphoma. J Clin Oncol 2006, 24, 1281–1288. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Gittleman, H.; Truitt, G.; Boscia, A.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2011-2015. Neuro Oncol 2018, 20, iv1–iv86. [Google Scholar] [CrossRef]
- Hoang-Xuan, K.; Bessell, E.; Bromberg, J.; Hottinger, A.F.; Preusser, M.; Rudà, R.; Schlegel, U.; Siegal, T.; Soussain, C.; Abacioglu, U.; et al. Diagnosis and treatment of primary CNS lymphoma in immunocompetent patients: guidelines from the European Association for Neuro-Oncology. The Lancet Oncology 2015, 16, e322–e332. [Google Scholar] [CrossRef] [PubMed]
- Thiel, E.; Korfel, A.; Martus, P.; Kanz, L.; Griesinger, F.; Rauch, M.; Röth, A.; Hertenstein, B.; von Toll, T.; Hundsberger, T.; et al. High-dose methotrexate with or without whole brain radiotherapy for primary CNS lymphoma (G-PCNSL-SG-1): a phase 3, randomised, non-inferiority trial. Lancet Oncol 2010, 11, 1036–1047. [Google Scholar] [CrossRef] [PubMed]
- Weller, M.; Martus, P.; Roth, P.; Thiel, E.; Korfel, A. Surgery for primary CNS lymphoma? Challenging a paradigm. Neuro Oncol 2012, 14, 1481–1484. [Google Scholar] [CrossRef] [PubMed]
- Krebs, S.; Barasch, J.G.; Young, R.J.; Grommes, C.; Schöder, H. Positron emission tomography and magnetic resonance imaging in primary central nervous System lymphoma-a narrative review. Ann Lymphoma 2021, 5. [Google Scholar] [CrossRef] [PubMed]
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat Rev Clin Oncol 2021, 18, 170–186. [Google Scholar] [CrossRef] [PubMed]
- Abboud, H.; Probasco, J.C.; Irani, S.; Ances, B.; Benavides, D.R.; Bradshaw, M.; Christo, P.P.; Dale, R.C.; Fernandez-Fournier, M.; Flanagan, E.P.; et al. Autoimmune encephalitis: proposed best practice recommendations for diagnosis and acute management. J Neurol Neurosurg Psychiatry 2021, 92, 757–768. [Google Scholar] [CrossRef]
- Miller, A.L.; Webb, M.S.; Copik, A.J.; Wang, Y.; Johnson, B.H.; Kumar, R.; Thompson, E.B. p38 Mitogen-activated protein kinase (MAPK) is a key mediator in glucocorticoid-induced apoptosis of lymphoid cells: correlation between p38 MAPK activation and site-specific phosphorylation of the human glucocorticoid receptor at serine 211. Mol Endocrinol 2005, 19, 1569–1583. [Google Scholar] [CrossRef] [PubMed]
- Roth, P.; Wick, W.; Weller, M. Steroids in neurooncology: actions, indications, side-effects. Curr Opin Neurol 2010, 23, 597–602. [Google Scholar] [CrossRef]
- Sionov, R.V.; Spokoini, R.; Kfir-Erenfeld, S.; Cohen, O.; Yefenof, E. Mechanisms regulating the susceptibility of hematopoietic malignancies to glucocorticoid-induced apoptosis. Adv Cancer Res 2008, 101, 127–248. [Google Scholar] [CrossRef] [PubMed]
- Barrantes-Freer, A.; Engel, A.S.; Rodríguez-Villagra, O.A.; Winkler, A.; Bergmann, M.; Mawrin, C.; Kuempfel, T.; Pellkofer, H.; Metz, I.; Bleckmann, A.; et al. Diagnostic red flags: steroid-treated malignant CNS lymphoma mimicking autoimmune inflammatory demyelination. Brain Pathol 2018, 28, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol 2021. [Google Scholar] [CrossRef] [PubMed]
- Scheichel, F.; Marhold, F.; Pinggera, D.; Kiesel, B.; Rossmann, T.; Popadic, B.; Woehrer, A.; Weber, M.; Kitzwoegerer, M.; Geissler, K.; et al. Influence of preoperative corticosteroid treatment on rate of diagnostic surgeries in primary central nervous system lymphoma: a multicenter retrospective study. BMC Cancer 2021, 21, 754. [Google Scholar] [CrossRef] [PubMed]
- Bataille, B.; Delwail, V.; Menet, E.; Vandermarcq, P.; Ingrand, P.; Wager, M.; Guy, G.; Lapierre, F. Primary intracerebral malignant lymphoma: report of 248 cases. Journal of neurosurgery 2000, 92, 261–266. [Google Scholar] [CrossRef]
- Henry, J.M.; Heffner Jr, R.R.; Dillard, S.H.; Earle, K.M.; Davis, R.L. Primary malignant lymphomas of the central nervous System. Cancer 1974, 34, 1293–1302. [Google Scholar] [CrossRef]
- DeAngelis, L.M.; Yahalom, J.; Heinemann, M.H.; Cirrincione, C.; Thaler, H.T.; Krol, G. Primary CNS lymphoma: combined treatment with chemotherapy and radiotherapy. Neurology 1990, 40, 80–86. [Google Scholar] [CrossRef]
- Hoang-Xuan, K.; Bessell, E.; Bromberg, J.; Hottinger, A.F.; Preusser, M.; Rudà, R.; Schlegel, U.; Siegal, T.; Soussain, C.; Abacioglu, U.; et al. Diagnosis and treatment of primary CNS lymphoma in immunocompetent patients: guidelines from the European Association for Neuro-Oncology. Lancet Oncol 2015, 16, e322–332. [Google Scholar] [CrossRef]
- Rae, A.I.; Mehta, A.; Cloney, M.; Kinslow, C.J.; Wang, T.J.C.; Bhagat, G.; Canoll, P.D.; Zanazzi, G.J.; Sisti, M.B.; Sheth, S.A.; et al. Craniotomy and Survival for Primary Central Nervous System Lymphoma. Neurosurgery 2019, 84, 935–944. [Google Scholar] [CrossRef]
- Schellekes, N.; Barbotti, A.; Abramov, Y.; Sitt, R.; Di Meco, F.; Ram, Z.; Grossman, R. Resection of primary central nervous system lymphoma: impact of patient selection on overall survival. J Neurosurg 2021, 1–10. [Google Scholar] [CrossRef]
- Wu, S.; Wang, J.; Liu, W.; Hu, F.; Zhao, K.; Jiang, W.; Lei, T.; Shu, K. The role of surgical resection in primary central nervous system lymphoma: a single-center retrospective analysis of 70 patients. BMC Neurol 2021, 21, 190. [Google Scholar] [CrossRef]
- Houillier, C.; Soussain, C.; Ghesquières, H.; Soubeyran, P.; Chinot, O.; Taillandier, L.; Lamy, T.; Choquet, S.; Ahle, G.; Damaj, G.; et al. Management and outcome of primary CNS lymphoma in the modern era: An LOC network study. Neurology 2020, 94, e1027–e1039. [Google Scholar] [CrossRef] [PubMed]
- Hall, W.A. The safety and efficacy of stereotactic biopsy for intracranial lesions. Cancer 1998, 82, 1749–1755. [Google Scholar] [CrossRef]
- Shooman, D.; Belli, A.; Grundy, P.L. Image-guided frameless stereotactic biopsy without intraoperative neuropathological examination. J Neurosurg 2010, 113, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Morell, A.A.; Shah, A.H.; Cavallo, C.; Eichberg, D.G.; Sarkiss, C.A.; Benveniste, R.; Ivan, M.E.; Komotar, R.J. Diagnosis of primary central nervous system lymphoma: a systematic review of the utility of CSF screening and the role of early brain biopsy. Neurooncol Pract 2019, 6, 415–423. [Google Scholar] [CrossRef]
- Schroers, R.; Baraniskin, A.; Heute, C.; Vorgerd, M.; Brunn, A.; Kuhnhenn, J.; Kowoll, A.; Alekseyev, A.; Schmiegel, W.; Schlegel, U.; et al. Diagnosis of leptomeningeal disease in diffuse large B-cell lymphomas of the central nervous System by flow cytometry and cytopathology. Eur J Haematol 2010, 85, 520–528. [Google Scholar] [CrossRef]
- Quijano, S.; López, A.; Manuel Sancho, J.; Panizo, C.; Debén, G.; Castilla, C.; Antonio García-Vela, J.; Salar, A.; Alonso-Vence, N.; González-Barca, E.; et al. Identification of leptomeningeal disease in aggressive B-cell non-Hodgkin’s lymphoma: improved sensitivity of flow cytometry. J Clin Oncol 2009, 27, 1462–1469. [Google Scholar] [CrossRef]
- Hegde, U.; Filie, A.; Little, R.F.; Janik, J.E.; Grant, N.; Steinberg, S.M.; Dunleavy, K.; Jaffe, E.S.; Abati, A.; Stetler-Stevenson, M.; et al. High incidence of occult leptomeningeal disease detected by flow cytometry in newly diagnosed aggressive B-cell lymphomas at risk for central nervous system involvement: the role of flow cytometry versus cytology. Blood 2005, 105, 496–502. [Google Scholar] [CrossRef]
- Heger, J.M.; Mattlener, J.; Schneider, J.; Gödel, P.; Sieg, N.; Ullrich, F.; Lewis, R.I.; Bucaciuc-Mracica, T.; Schwarz, R.F.; Rueß, D.; et al. Entirely noninvasive outcome prediction in central nervous system lymphomas using circulating tumor DNA. Blood 2023. [Google Scholar] [CrossRef]
- Brück, W.; Brunn, A.; Klapper, W.; Kuhlmann, T.; Metz, I.; Paulus, W.; Deckert, M. [Differential diagnosis of lymphoid infiltrates in the central nervous System: experience of the Network Lymphomas and Lymphomatoid Lesions in the Nervous System]. Pathologe 2013, 34, 186–197. [Google Scholar] [CrossRef]
- Porter, A.B.; Giannini, C.; Kaufmann, T.; Lucchinetti, C.F.; Wu, W.; Decker, P.A.; Atkinson, J.L.D.; O’Neill, B.P. Primary central nervous system lymphoma can be histologically diagnosed after previous corticosteroid use: A pilot study to determine whether corticosteroids prevent the diagnosis of primary central nervous system lymphoma. Annals of Neurology 2008, 63, 662–667. [Google Scholar] [CrossRef]
- Bullis, C.L.; Maldonado-Perez, A.; Bowden, S.G.; Yaghi, N.; Munger, D.; Wood, M.D.; Barajas, R.F.; Ambady, P.; Neuwelt, E.A.; Han, S.J. Diagnostic impact of preoperative corticosteroids in primary central nervous system lymphoma. J Clin Neurosci 2020, 72, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Haldorsen, I.S.; Espeland, A.; Larsen, J.L.; Mella, O. Diagnostic delay in primary central nervous system lymphoma. Acta Oncologica 2005, 44, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Manoj, N.; Arivazhagan, A.; Mahadevan, A.; Bhat, D.I.; Arvinda, H.R.; Devi, B.I.; Sampath, S.; Chandramouli, B.A. Central nervous system lymphoma: patterns of incidence in Indian population and effect of steroids on stereotactic biopsy yield. Neurol India 2014, 62, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Önder, E.; Arıkök, A.T.; Önder, S.; Han, Ü.; Sorar, M.; Kertmen, H.; Yılmaz, E.D.; Fesli, R.; Alper, M. Corticosteroid pre-treated primary CNS lymphoma: a detailed analysis of stereotactic biopsy findings and consideration of interobserver variability. Int J Clin Exp Pathol 2015, 8, 7798–7808. [Google Scholar] [PubMed]
- Velasco, R.; Mercadal, S.; Vidal, N.; Alañá, M.; Barceló, M.I.; Ibáñez-Juliá, M.J.; Bobillo, S.; Caldú Agud, R.; García Molina, E.; Martínez, P.; et al. Diagnostic delay and outcome in immunocompetent patients with primary central nervous system lymphoma in Spain: a multicentric study. J Neurooncol 2020, 148, 545–554. [Google Scholar] [CrossRef]
- Cerqua, R.; Balestrini, S.; Perozzi, C.; Cameriere, V.; Renzi, S.; Lagalla, G.; Mancini, G.; Montanari, M.; Leoni, P.; Scerrati, M.; et al. Diagnostic delay and prognosis in primary central nervous system lymphoma compared with glioblastoma multiforme. Neurol Sci 2016, 37, 23–29. [Google Scholar] [CrossRef]
- Falanga, A.; Marchetti, M.; Russo, L. Venous thromboembolism in the hematologic malignancies. Curr Opin Oncol 2012, 24, 702–710. [Google Scholar] [CrossRef]
- Yokoyama, K. Thrombosis in Lymphoma Patients and in Myeloma Patients. The Keio Journal of Medicine 2015, 64, 37–43. [Google Scholar] [CrossRef]
- Gazal, S.; Lebel, E.; Kalish, Y.; Makranz, C.; Gatt, M.E.; Goldschmidt, N.; Nachmias, B. Venous Thromboembolism Prophylaxis with Low-Molecular-Weight Heparin in Primary Central Nervous System Lymphoma. Oncol Res Treat 2021, 44, 52–57. [Google Scholar] [CrossRef]
- Gerstner, E.; Batchelor, T. Primary CNS lymphoma. Expert Review of Anticancer Therapy 2007, 7, 689–700. [Google Scholar] [CrossRef]
- Weller, M. Glucocorticoid treatment of primary CNS lymphoma. J Neurooncol 1999, 43, 237–239. [Google Scholar] [CrossRef]
- Shaw, A.; Iyer, V.; Rooney, N.; Wragg, R.; Waits, P.; Roberts, E.; Haynes, H.R.; Kurian, K.M. Diagnosis of primary cerebral lymphomas: possible value of PCR testing in equivocal cases requiring rebiopsy. Br J Neurosurg 2014, 28, 214–219. [Google Scholar] [CrossRef]
Figure 1.
Consequences of corticosteroid treatment on PCNSL. Upper row: Exemplary hematoxylin-eosin staining of (a) untreated PCNSL, (b) PCNSL after high-dose CS treatment and (c) PCNSL after an interval of discontinued high-dose CS treatment Bottom row: Exemplary T1-weighed contrast-enhanced Magnetic Resonance Image of (d) untreated PCNSL, (e) PCNSL after high-dose CS treatment and (f) PCNSL after interval of discontinued high-dose CS treatment.
Figure 1.
Consequences of corticosteroid treatment on PCNSL. Upper row: Exemplary hematoxylin-eosin staining of (a) untreated PCNSL, (b) PCNSL after high-dose CS treatment and (c) PCNSL after an interval of discontinued high-dose CS treatment Bottom row: Exemplary T1-weighed contrast-enhanced Magnetic Resonance Image of (d) untreated PCNSL, (e) PCNSL after high-dose CS treatment and (f) PCNSL after interval of discontinued high-dose CS treatment.
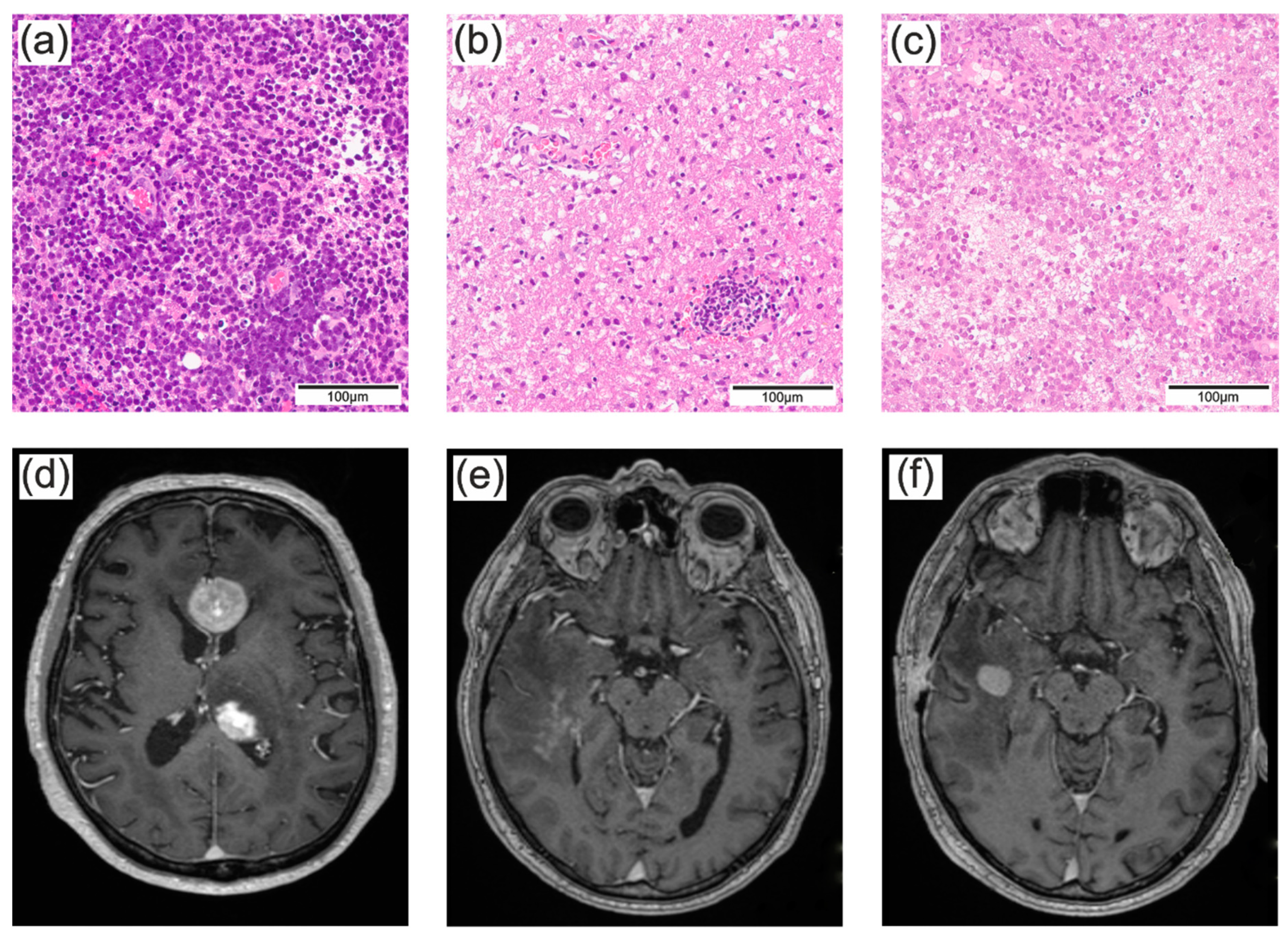
Figure 2.
The time between the initial MRI and surgery. Boxplots show the period between MRI and surgery depending on whether patients were treated with (a) corticosteroids, (b) anticoagulation or platelet inhibition, or received (c) diagnostics of the cerebrospinal fluid preoperatively. Abbreviations: CS, corticosteroids; PI, platelet inhibition; AC, anticoagulation; CSF, cerebrospinal fluid.
Figure 2.
The time between the initial MRI and surgery. Boxplots show the period between MRI and surgery depending on whether patients were treated with (a) corticosteroids, (b) anticoagulation or platelet inhibition, or received (c) diagnostics of the cerebrospinal fluid preoperatively. Abbreviations: CS, corticosteroids; PI, platelet inhibition; AC, anticoagulation; CSF, cerebrospinal fluid.
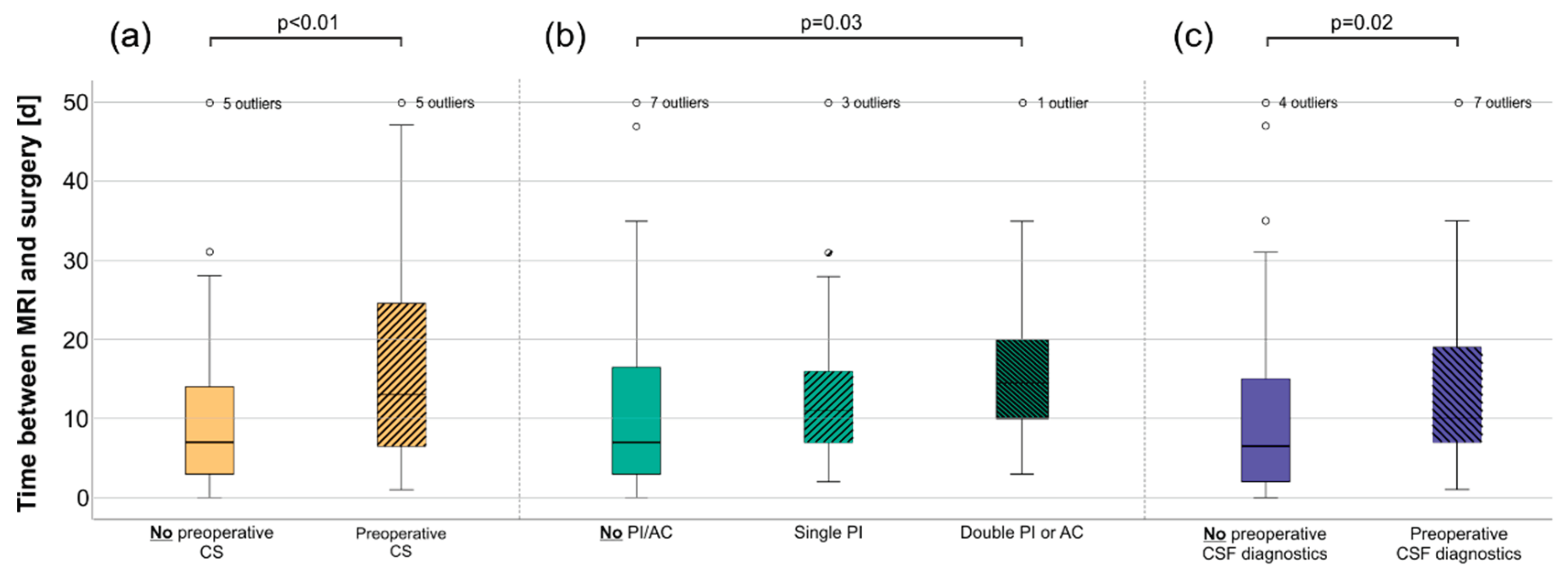

Table 1.
PCNSL patients with unsuccessful first biopsy after CS therapy.
| Patient | CS paused before 1st surgery [d] | 1st surgery | CS paused before 2nd surgery [d] | 2nd surgery | CS paused before 3rd surgery [d] | 3rd surgery |
|---|---|---|---|---|---|---|
| 1 | 30 | STB | 88 | STB | ||
| 2 | m.i. | OSB | ≥259 | STB | ||
| 3 | 4 | STB | 71 | Resection | ||
| 4 | 8 | OSB | 19 | OSB | 48 | STB |
| 5 | 1 | STB | 11 | STB | ||
| 6 | 8 | OSB | 21 | Resection | 141 | Resection |
| 7 | 6 | STB | 3 | Resection |
Abbreviations: STB, Stereotactic biopsy; OSB, Open surgery biopsy; Resection, (Partial) tumor resection; m.i., missing information due to initial surgery at an external institution.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



