
Submitted:
20 February 2024
Posted:
21 February 2024
You are already at the latest version
Abstract
Recently, immunotherapy has arisen as a novel treatment approach for patients with colorectal cancer (CRC), but the effectiveness of immunotherapy varies in these patients. We hypothesized that immune checkpoint molecules (ICMs), which are the targets of immunotherapy, are often exhibit concomitantly. Our objective was to investigate the patterns of ICM expression in patients with CRC and the differences in ICM expression based on the microsatellite instability status. Immunohistochemical expression of programmed cell death protein 1 (PD-1), programmed cell death ligand 1 (PD-L1), T cell immunoglobulin and mucin-domain containing-3 (TIM-3), and lymphocyte-activation gene 3 (LAG-3) in the tumor center and periphery was assessed in patients with non-metastatic colorectal cancer. We enrolled 83 patients with CRC: 40 with microsatellite stable (MSS) and 43 with microsatellite instability-high (MSI-H). PD-L1 was more frequently expressed in the tumor center in patients with MSI-H than that in patients with MSS (18 [41.9 %] vs. 3 [7.5 %], respectively; P < 0.001), and the same trend was observed for TIM-3 expression (30 [69.8 %] vs. 19 [47.5 %], respectively; P = 0.047). Concomitant expression of two or more ICMs was more frequently observed than no expression or expression of a single molecule in both MSS and MSI-H groups; 34 (79.7 %) patients with MSI-H and 23 (57.5 %) with MSS showed ICM expression at the tumor center, whereas 34 (79.7 %) patients with MSI-H and 22 (55 %) with MSS showed expression at the tumor periphery. Patients with the genetic characteristics of MSI-H showed higher expression levels of ICMs than that in patients with MSS, and predominantly, two or more ICMs were concurrently expressed. Our findings highlight the potential efficacy of the dual-blockade approach in immunotherapy, particularly in patients with MSI-H CRC.
Keywords:
colorectal neoplasms
; microsatellite instability
; immune checkpoint proteins
; immunotherapy
1. Introduction
Radical surgical resection stands as the principal therapy for colorectal cancer (CRC), and for advanced CRC, the use of cytotoxic chemotherapy and target agents has played a crucial role in treating the disease. However, currently, CRC has an overall recurrence rate of 25 %, and metastatic lesions are found in 20 % of the patients at the time of diagnosis [1,2]. Overall, the treatment of recurrent or metastatic CRC remains a challenge.
Recently, immune checkpoint inhibitors (ICIs), which inhibit immune checkpoint molecules (ICMs), have emerged as novel therapeutic choices for patients with CRC. Interactions between tumors and tumor-specific T cells via ICMs have been identified as key underlying mechanisms within the tumor microenvironment [3,4,5]. Genetic and epigenetic changes during carcinogenesis induce the expression of multiple tumor antigens; however, tumors can survive the immune response by inducing tolerance [6,7]. Immunotherapy using ICIs can counteract tumor immune escape by inhibiting immune checkpoint pathways and reactivating the body's capacity to initiate an effective antitumor immune response [8]. The effectiveness of ICIs has been proven in other malignant disease such as melanoma, lung cancer, and prostate cancer [9,10,11].
Although immunotherapy is effective in treating patients with CRC, it specifically displays partial efficacy in a subset of individuals who have genetic features of microsatellite instability, which accounts for approximately 10 % of patients with CRC [12,13,14]. This may be attributed to enhanced tumor resistance due to the lack of tumor-infiltrating lymphocytes and the presence of inhibitory myeloid cells. Additionally, low expression levels of PD-L1, which is the primary target of immunotherapy, in tumors may restrict the effectiveness of treatment [15,16,17,18,19,20,21]. Assessing the expression patterns of ICMs other than PD-L1, which can be targeted using ICIs, and tailoring the treatment based on these expression patterns can potentially enhance the therapeutic outcomes in patients with CRC. Immunotherapy, which focuses on multiple ICMs simultaneously, is already being studied and applied to various cancer types, including CRC [22,23].
Therefore, our objective was to study the expression patterns of ICMs via immunohistochemical staining in patients with CRC and assess whether the expression patterns of the identified markers correlated with the clinicopathological characteristics. By analyzing the expression patterns of ICMs, we intended to obtain theoretical support for the multi-blockade of ICMs in CRC treatment.
2. Materials and Methods
2.1. Patient Selection
We enrolled individuals diagnosed with stage I–III CRC, according to the American Joint Committee on Cancer (AJCC) guidelines, who underwent curative surgical resection between January 2006 and December 2017. Patients who received only palliative bypass surgery without radical resection, those with cancers in other organs, and those with a history of CRC were excluded. The Institutional Review Board of Wonju Severance Christian Hospital approved this study (approval number: CR:318334), and every participant gave their written informed consent. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
2.2. Data Collection: Clinicopathological Data
The patients’ clinical information, including age, sex, medical history, classification recommended by the American Society of Anesthesiologists (ASA), tumor location, carcinoembryonic antigen (CEA) level, pathologic stage, tumor differentiation, and lymphatic invasion, was obtained from medical records. Low-grade tumors were defined as poorly-differentiated mucinous tumors, whereas high-grade tumors were defined as well- or moderately-differentiated tumors. Patient survival data were obtained from the colorectal cancer databases of Wonju Severance Christian Hospital and the Korean National Cancer Center.
2.3. Tissue Sample Preparation and Microarray Analysis
Paraffin-embedded, formalin-fixed specimens of 83 cases of CRC were acquired from the records of the Department of Pathology at Wonju Severance Christian Hospital (2006–2017). Tissue microarrays (TMAs) were constructed by reviewing archived tumor slides. A core of 0.5-mm diameter was inserted into the paraffin block; for each patient, one sample each was obtained from the tumor center and another from the margin of tumor invasion. Each core was processed into blocks in a 1-mm-spaced grid covering approximately 1 square inch, and 5-micron thick sections were cut. The number of tissue cores in the TMA was 5 × 4. Tissues were arrayed using a manual arraying instrument (Unitma, South Korea).
2.4. Immunohistochemical Analysis
Paraffin-embedded tissue samples were sectioned from each block and warmed at 75 °C for 4 min. The slides underwent deparaffinization with EZPrep (Ventana Medical Systems, Tucson, AZ, USA), followed by antigen retrieval for 60 minutes using a cell-conditioning solution provided by Ventana Medical Systems. To reduce endogenous peroxidase activity, the sections were treated with an ultraviolet inhibitor for a duration of 4 minutes. Following this, the sections were rinsed repeatedly with reaction buffer at ambient temperature. For the purpose of immunohistochemical (IHC) staining, the ultraView Universal DAB Detection Kit provided by Ventana Medical Systems was employed. The sections were incubated with the primary antibodies against programmed cell death ligand 1 (PD-L1; 1:200; Cell Signaling Technology; catalog no.: 13687), programmed cell death protein 1 (PD-1; 1:200; Cell Signaling Technology; catalog no.: 86163), T cell immunoglobulin and mucin-domain containing-3 (TIM-3; 1:100; Abcam; catalog no.: ab185703), and lymphocyte-activation gene 3 (LAG-3; 1:200; LifeSpan BioSciences; catalog no.: LS-C340186-100) for 2 h at 37 °C in an autostainer (Benchmark XT; Ventana Medical Systems). Subsequently, the slides were washed using the reaction buffer, and a series of reagents from Ventana Medical Systems, including HRP UNIV MULT, DAB, and DAB H2O2, were applied in sequence to each slide, allowing 8 minutes for each reagent, with intermittent washing using the reaction buffer. A copper solution was then applied to the slides for 4 minutes. A bluing reagent was added subsequently, after which the slides were again washed with the reaction buffer. For nuclear staining, the sections were counterstained with hematoxylin.
The protein expression was manually analyzed in selected hotspot fields. PD-L1, PD-1, and TIM-3 showed membrane expression, whereas LAG-3 was mainly localized in the cytoplasm. The PD-L1 expression level was defined as either low (≤ 40 %) or high (> 41 %) [24]. A high degree of lymphocyte infiltration in PD-1-expressing tumors was defined as a measure of > 1.43 tumor-infiltrating lymphocytes per square millimeter [25]. TIM-3 expression level was evaluated using the HSCORE system (HSCORE = stain intensity × percentage of positive cells), and the cut-off points were defined [26,27,28]. LAG-3 expression level was defined as low (< 5 %) or high (< 5 %) [29]. The IHC staining outcomes were independently evaluated by two pathologists who had no knowledge of the patients' clinical and pathological data. Discrepancies between the pathologists' findings were resolved by mutual agreement. The IHC staining results are shown in Figure 1.
2.5. Statistical Analysis
Patients were classified into two groups according to their microsatellite status, and a comparative analysis was performed. Categorical variables are presented as frequencies and percentages and were analyzed using the chi-square test. If the expected frequency of the data was less than five, Fisher's exact test was used. Continuous variables are described as means and standard deviations and were analyzed using the Student’s t-test. Statistical analyses were carried out using SPSS software (version 25.0; IBM, Armonk, USA), and statistical significance established at a P-value of less than 0.05.
3. Results
3.1. Differences in Baseline Characteristics between Patients with Microsatellite Stable (MSS) and Microsatellite Instability-High (MSI-H)
Our analysis included 83 eligible patients, of whom 40 exhibited genetic characteristics consistent with MSS and 43 exhibited MSI-H. The two groups exhibited well-balanced distributions in terms of age, sex ratio, ASA classification, and pathologic stage; the numbers of women in the MSS and MSI-H groups were 25 (58.1 %) and 21 (52.5 %), respectively, and the mean ages at diagnosis of patients in the two groups were 66.3 and 67.4 years, respectively; the proportions of patients with ASA scores of 3 were 16 (37.2 %) and 12 (30 %), respectively. In each group, 60 and 65.1 % of the patients, respectively, were diagnosed with pathologic stage I–II CRC.
In the MSS group, rectal cancer was the most frequent, affecting 17 patients (42.5 %), whereas in the MSI-H group, right-sided colon cancer was the most prevalent, accounting for 29 patients (67.4 %). Low-grade differentiation, including poorly differentiated and mucinous adenocarcinomas, was more frequent in the MSI-H group than that in the MSS group (12 [27.9 %] vs. 2 [5 %], respectively; P = 0.007). The median follow-up duration for patients was 48 months (interquartile range [IQR]: 30, 73). During the follow-up period, in the MSS group, 11 cases of recurrence were observed (27.5 %), whereas in the MSI-H group, five cases of recurrence were identified (11.6 %; P = 0.067). Regarding cancer-related deaths, two deaths (5 %) occurred in the MSS group and five (11.6 %) in the MSI-H group, and no statistically significant difference was observed (P = 0.435; Table 1).
3.2. Differential Expression of Immune Checkpoint Molecules between MSS and MSI-H Groups
Assessment of ICM expression in the center of the tumor tissue in MSI-H and MSS groups revealed that the expression levels of PD-L1 (18 [41.9 %] vs. 3 [7.5 %, respectively; P < 0.001) and TIM-3 (30 [69.8 %] vs. 19 [47.5 %], respectively; P = 0.047) were significantly higher in the MSI-H group than those in the MSS group; the expression levels of PD-1 (12 [30 %] vs. 16 [37.2 %], respectively; P = 0.643) and LAG-3 (30 [75 %] vs. 33 [76.7 %], respectively; P = 1) were not significantly different between the two groups. At the margin of the tumor tissue, the ICM expression levels were higher in the MSI-H group than those in the MSS group, but the difference was not statistically significant (Table 2).
3.3. Concomitant Expression of Immune Checkpoint Molecules
In numerous cases, concomitant expression of two or more ICMs was confirmed. At the tumor center, concurrent expression of two or more ICMs was observed in 57 individuals (68.7 %). Concurrent expression of all four ICMs was observed in nine cases (10.3 %), whereas high expression levels of a single marker were observed in 16 cases (19.2 %). Conversely, the absence of expression of all four ICMs was observed in 10 patients (12 %). In the MSS group, two or more ICMs were co-expressed in 23 individuals (57.5 %), whereas in the MSI-H group, 34 individuals (79.1 %) demonstrated co-expression of two or more ICMs (Table 3).
At the tumor border, concurrent expression of two or more ICMs was observed in 56 individuals (67.5 %), and concurrent expression of all four ICMs was observed in eight individuals (9.6 %), whereas a single marker was highly expressed in 18 individuals (21.7 %). No expression of all four ICMs was observed in nine individuals (10.8 %). In the MSS group, 22 individuals (55 %) exhibited co-expression of two or more ICMs, whereas in the MSI-H group, 34 individuals (79.1 %) demonstrated co-expression of two or more ICMs (Table 3). The results indicate that patients with CRC showed concomitant expression of various types of ICMs. Notably, in the MSI-H group, a significantly higher degree of concurrent expression of ICMs was observed than that in the MSS group at the tumor border (55 vs. 79.1 %, respectively; P = 0.03) and tumor center (57.5 vs. 79.1 %, respectively; P = 0.06) (Table 4 and Figure 2).
4. Discussion
Our analysis revealed that the majority of patients with CRC (73 out of 83; approximately 87.95 %) exhibited high ICM expression levels. According to the microsatellite status, patients with genetic characteristics of MSI-H showed higher levels of ICM expression. This was particularly noticeable in the tumor center, where the expression levels of PD-L1 and TIM-3 were significantly higher in the MSI-H group than those in the MSS group. Additionally, the expression of ICMs was predominantly characterized by the concurrent expression of two or more markers, accounting for over 68 % of cases, as compared to that for single marker expression. Several overlapping expression patterns of TIM-3 and LAG-3 were observed. Remarkably, within both the tumor center and border, the MSI-H group demonstrated higher concurrent expression rates of ICMs than those observed in the MSS group.
Various types of ICMs are involved in malignant diseases [30,31], including PD-1 and PD-L1, which are representative ICMs that are highly expressed in the tumor microenvironment, and ICIs targeting these molecules are utilized in immunotherapy. Studies have related the overexpression of these markers to the prognosis of tumors, but the conclusions are still debatable. Li et al. reported that PD-L1 expression in colorectal tumor cells and PD-1 expression in tumor-infiltrating cells are associated with favorable 5-year overall survival (OS) and disease-free survival (DFS) in patients with CRC [32]. Conversely, several studies have shown that the overexpression of PD-L1 is associated with adverse clinicopathological characteristics, including poor differentiation, lymphovascular invasion, and poor OS [33,34]. TIM-3 is an immune checkpoint receptor that is predominantly found on the surface of T cells, particularly CD4+ and CD8+ T cells. According to previous studies, TIM-3 is known to be overexpressed in CRC, and its overexpression is correlated with tumor progression [35,36]. Yu et al. documented that increased TIM-3 expression in CRC was correlated with tumor size, TNM stage, and distant metastasis. Furthermore, the suppression of TIM-3 expression substantially decreased cell proliferation, migration, and invasion, and these findings were consistent with those obtained from analysis of clinical tissues [35]. In this study, we observed higher expression levels of LAG-3 compared to those of other molecules in the tumor center and periphery in both MSI-H and MSS groups. LAG-3, a surface molecule belonging to the immunoglobulin superfamily, has been detected in tumor-infiltrating lymphocytes (TILs) in various cancer types, including breast, ovarian, and lung cancers. LAG-3 expression is frequently associated with elevated PD-1 expression levels in T cells [37]. LAG-3 is a pivotal checkpoint molecule that potentially exhibits synergistic interaction with PD-1 and PD-L1 during cancer immunotherapy [38,39]. LAG-3, closely linked to CD4, modulates T cell proliferation, activation, and homeostasis. Several studies have indicated that elevated LAG-3 expression in TILs is related to unfavorable prognosis in various cancers [40,41]. Tavana et al. [42] conducted a study to assess the expression levels of LAG-3 and the prognostic impact of LAG-3 expression on patients with CRC and showed that a high number of LAG-3 + TILs was associated with poor clinicopathological features, especially in patients with left-sided colon cancer. Since LAG-3 was predominantly expressed in patients with CRC in our study, and LAG-3 has been regarded as an important prognostic factor, LAG-3 should be regarded as a potential therapeutic target for the treatment of CRC.
In this study, we not only observed expression of single ICMs in different individuals, but also observed concurrent expression of two or more markers in the same individual [30,31]. In our study, the concurrent expression rate of two or more ICMs was over 68 %. Additionally, our preliminary study, in which we analyzed gene expression in tissue samples obtained from 30 patients with CRC using quantitative polymerase chain reaction (qPCR), confirmed the expression of two or more immune-related genes in 29 patients (96.7 %) [43]. Concurrent expression of ICMs has been reported not only in CRC, but also in other malignant tumors. Datar et al. assessed the expression levels and clinical significance of PD-1, LAG-3, and TIM-3 proteins in non-small cell lung cancer (NSCLC) [44]. They observed co-expression of ICMs, and this co-expression was linked to T cell activation markers and apoptotic signal receptors. However, the proportion of samples exhibiting dual expression was lower than that of samples displaying a single expression pattern.
Currently, immunotherapy targeting ICMs is used for the treatment of metastatic and recurrent CRC. However, immunotherapy is only administered to patients with genetic characteristics of deficient mismatch repair (dMMR)/MSI-H. Furthermore, studies have reported the effectiveness of neoadjuvant immunotherapy in patients with advanced-stage MSI-H CRC [45,46]. The National Comprehensive Cancer Network (NCCN) guidelines recommend neoadjuvant immunotherapy for patients with MSI-H CRC. However, patients with CRC having the genetic characteristics of MSI-H constitute only approximately 5–10% of the total population, limiting the applicability and effectiveness of this treatment. In a phase II clinical trial conducted by Le et al., the partial objective response rate, following the administration of pembrolizumab, for patients with dMMR CRC was 40 %, and 0% for those with proficient mismatch repair (pMMR) CRC [12]. In a phase II trial conducted by Overman et al., which was the largest immunotherapy trial for CRC, a partial response to nivolumab (an anti-PD-1 antibody) administered either alone or in combination with ipilimumab was observed in 31 % of the patients with MSI and in 10% of the patients with MSS [13]. Additionally, in a phase III study conducted to compare the effects of pembrolizumab and chemotherapy in patients with MSI-H CRC (KEYNOTE-177), the pembrolizumab group demonstrated a greater progression-free survival (PFS) advantage compared to the chemotherapy group; however, OS did not differ significantly between the two groups [47]. Our results support the theory that ICMs operate via complex mechanisms involving multiple molecules rather than via a single mechanism.
As noted in our study, in numerous instances, two or more ICMs were expressed concurrently. Therefore, theoretically, blocking of two or more ICMs simultaneously would be effective. Numerous studies have focused on assessing the effectiveness of the simultaneous inhibition of two ICMs in CRC. The CheckMate 142 study, a phase 2 single-arm study investigating the efficacy of nivolumab and ipilimumab combination therapy in patients with MSI-H mCRC, showed convincing results in terms of a durable objective response rate (65 %), encouraging survival rates, and manageable safety [23,48,49]. Another phase 2 study, the GERCOR NIPICOL study, involving administration of nivolumab plus ipilimumab in patients with MSI-H mCRC, reported a 12-week disease control rate of 86 % and 12-month PFS and OS rates of 72.9 and 84 %, respectively [50]. The NICHE study, in which the effect of dual blockade with nivolumab and ipilimumab in neoadjuvant immunotherapy was investigated, reported that 19 out of 20 patients with dMMR CRC showed a major pathologic response (≤ 10 % residual viable tumor), whereas three out of 15 patients with pMMR CRC demonstrated a major pathologic response [45]. Further investigations involving a larger patient cohort are necessary to confirm the efficacy of dual blockade in CRC treatment. Research on the effectiveness of dual-blockade therapy for other malignant diseases has been conducted. Hellmann et al. observed that first-line treatment with nivolumab (anti-PD 1 antibodies) combined with ipilimumab (anti-CTLA4 antibodies) resulted in longer overall survival than that observed with chemotherapy in individuals with NSCLC, independent of the PD-L1 expression level [51]. Additionally, Paz-Ares et al. showed that combining nivolumab and ipilimumab with two cycles of chemotherapy significantly enhanced overall survival compared to that observed with chemotherapy alone and led to a favorable risk–benefit profile [11].
The four ICMs investigated in this study showed higher expression in the MSI-H group than that in the MSS group. Particularly, PD-L1 expression at the center of the tumor was significantly higher in the MSI-H group than that in the MSS group. This finding aligns with the findings of numerous prior studies. Valentini et al. reported that the proportion of PD-L1-expressing tumor cells and infiltrating immune cells was higher in patients with MSI-H CRC than that in patients with MSS CRC [17]. Ho et al. demonstrated that PD-L1 expression in stromal tumor-infiltrating immune cells and intraepithelial tumor-infiltrating immune cells was more frequent in the MSI-H group than that in the MSS group [18]. Therefore, when selecting an immunotherapy target for colorectal cancer, targeting the MSI-H group rather than the MSS group may show a better therapeutic effect. Additionally, our study revealed that in the MSI-H patient cohort, cases with concomitant expression of two or more types of ICMs were more prevalent than those showing expression of a single ICM. To the best of our knowledge, this issue has not been addressed in previous studies.
This study had several limitations. First, the limited sample size and absence of a validated independent cohort could have biased the findings. Second, given the concern of multiple comparisons, the risk of Type I errors cannot be dismissed. Additionally, IHC staining was conducted on a tissue array, which could introduce a selection bias.
Despite these limitations, this study is meaningful because the results provide information on the expression patterns of ICMs. In summary, patients with the genetic characteristics of MSI-H showed a higher tendency for ICM expression, and predominantly, two or more ICMs were concurrently expressed. Our findings highlight the potential efficacy of the dual-blockade approach in immunotherapy, particularly in patients with MSI-H CRC. Although several studies have already been undertaken to assess the effectiveness of dual blockade in patients with CRC, further investigations with a larger number of participants are necessary, and research must be conducted to obtain fundamental evidence that can advance our understanding and treatment strategies.
Author Contributions
Conceptualization, S.A., K.K., and Y.K.; methodology, S.A., W.L., K.K., Y.K., and M.Y.C; data curation, S.A., W.L., H.Y.K., H.D., B.K., K.K., Y.K., and M.Y.C.; analysis and interpretation, S.A., W.L., H.Y.K., H.D., B.K., K.K., Y.K., and M.Y.C.; writing—original draft preparation, S.A., K.K., and Y.K.; writing—review and editing, S.A., K.K., and Y.K.; supervision, S.A., K.K., Y.K, and M.Y.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Institutional Review. Board of Wonju Severance Christian Hospital (CR: 318334).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Biller, L.H.; Schrag, D. Diagnosis and treatment of metastatic colorectal cancer: A review. JAMA 2021, 325, 669–685. [Google Scholar] [CrossRef]
- Kunst, N.; Alarid-Escudero, F.; Aas, E.; Coupe, V.M.H.; Schrag, D.; Kuntz, K.M. Estimating population-based recurrence rates of colorectal cancer over time in the united states. Cancer Epidemiol. Biomarkers Prev. 2020, 29, 2710–2718. [Google Scholar] [CrossRef]
- Lee, K.S.; Kwak, Y.; Ahn, S.; Shin, E.; Oh, H.K.; Kim, D.W.; Kang, S.B.; Choe, G.; Kim, W.H.; Lee, H.S. Prognostic implication of CD274 (PD-L1) protein expression in tumor-infiltrating immune cells for microsatellite unstable and stable colorectal cancer. Cancer Immunol. Immunother. 2017, 66, 927–939. [Google Scholar] [CrossRef]
- Lee, K.S.; Kim, B.H.; Oh, H.K.; Kim, D.W.; Kang, S.B.; Kim, H.; Shin, E. Programmed cell death ligand-1 protein expression and CD274/PD-L1 gene amplification in colorectal cancer: Implications for prognosis. Cancer Sci. 2018, 109, 2957–2969. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Jun, S.Y.; Lee, I.H.; Kang, B.W.; Park, S.Y.; Kim, H.J.; Park, J.S.; Choi, G.S.; Yoon, G.; Kim, J.G. CD274, LAG3, and IDO1 expressions in tumor-infiltrating immune cells as prognostic biomarker for patients with MSI-high colon cancer. J. Cancer Res. Clin. Oncol. 2018, 144, 1005–1014. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.R.; Tykodi, S.S.; Chow, L.Q.M.; Hwu, W.-J.; Topalian, S.L.; Hwu, P.; Drake, C.G.; Camacho, L.H.; Kauh, J.; Odunsi, K.; et al. Safety and activity of anti–PD-L1 antibody in patients with advanced cancer. N. Engl. J. Med. 2012, 366, 2455–2465. [Google Scholar] [CrossRef] [PubMed]
- Topalian, S.L.; Hodi, F.S.; Brahmer, J.R.; Gettinger, S.N.; Smith, D.C.; McDermott, D.F.; Powderly, J.D.; Carvajal, R.D.; Sosman, J.A.; Atkins, M.B.; et al. Safety, activity, and immune correlates of anti–PD-1 antibody in cancer. N. Engl. J. Med. 2012, 366, 2443–2454. [Google Scholar] [CrossRef] [PubMed]
- Boukouris, A.E.; Theochari, M.; Stefanou, D.; Papalambros, A.; Felekouras, E.; Gogas, H.; Ziogas, D.C. Latest evidence on immune checkpoint inhibitors in metastatic colorectal cancer: A 2022 update. Crit. Rev. Oncol. Hematol. 2022, 173, 103663. [Google Scholar] [CrossRef] [PubMed]
- Carlino, M.S.; Larkin, J.; Long, G.V. Immune checkpoint inhibitors in melanoma. Lancet 2021, 398, 1002–1014. [Google Scholar] [CrossRef]
- Venkatachalam, S.; McFarland, T.R.; Agarwal, N.; Swami, U. Immune checkpoint inhibitors in prostate cancer. Cancers (Basel) 2021, 13, 2187. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Ciuleanu, T.-E.; Cobo, M.; Schenker, M.; Zurawski, B.; Menezes, J.; Richardet, E.; Bennouna, J.; Felip, E.; Juan-Vidal, O.; et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): An international, randomised, open-label, phase 3 trial. The Lancet Oncology 2021, 22, 198–211. [Google Scholar] [CrossRef]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef]
- Overman, M.J.; McDermott, R.; Leach, J.L.; Lonardi, S.; Lenz, H.-J.; Morse, M.A.; Desai, J.; Hill, A.; Axelson, M.; Moss, R.A.; et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): An open-label, multicentre, phase 2 study. The Lancet Oncology 2017, 18, 1182–1191. [Google Scholar] [CrossRef]
- Gatalica, Z.; Vranic, S.; Xiu, J.; Swensen, J.; Reddy, S. High microsatellite instability (MSI-H) colorectal carcinoma: A brief review of predictive biomarkers in the era of personalized medicine. Fam. Cancer 2016, 15, 405–412. [Google Scholar] [CrossRef]
- Wang, L.; Ren, F.; Wang, Q.; Baldridge, L.A.; Monn, M.F.; Fisher, K.W.; Sheng, W.; Zhou, X.; Du, X.; Cheng, L. Significance of programmed death ligand 1 (PD-L1) immunohistochemical expression in colorectal cancer. Mol. Diagn. Ther. 2016, 20, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Li, L.; Jiang, X.; Li, Q. Mismatch repair deficiency/microsatellite instability-high as a predictor for anti-PD-1/PD-L1 immunotherapy efficacy. J. Hematol. Oncol. 2019, 12, 54. [Google Scholar] [CrossRef] [PubMed]
- Valentini, A.M.; Di Pinto, F.; Cariola, F.; Guerra, V.; Giannelli, G.; Caruso, M.L.; Pirrelli, M. PD-L1 expression in colorectal cancer defines three subsets of tumor immune microenvironments. Oncotarget 2018, 9, 8584–8596. [Google Scholar] [CrossRef]
- Ho, H.-L.; Chou, T.-Y.; Yang, S.-H.; Jiang, J.-K.; Chen, W.-S.; Chao, Y.; Teng, H.-W. PD-L1 is a double-edged sword in colorectal cancer: The prognostic value of PD-L1 depends on the cell type expressing PD-L1. J. Cancer Res. Clin. Oncol. 2019, 145, 1785–1794. [Google Scholar] [CrossRef] [PubMed]
- Pyo, J.S.; Ko, S.H.; Ko, Y.S.; Kim, N.Y. Clinicopathological significance of PD-L1 expression in colorectal cancer: Impact of PD-L1 expression on pFOXO1 expression. Pathol. Res. Pract. 2020, 216, 152764. [Google Scholar] [CrossRef]
- Jung, D.H.; Park, H.J.; Jang, H.H.; Kim, S.H.; Jung, Y.; Lee, W.S. Clinical impact of PD-L1 expression for survival in curatively resected colon cancer. Cancer Invest. 2020, 38, 406–414. [Google Scholar] [CrossRef]
- Inaguma, S.; Lasota, J.; Wang, Z.; Felisiak-Golabek, A.; Ikeda, H.; Miettinen, M. Clinicopathologic profile, immunophenotype, and genotype of CD274 (PD-L1)-positive colorectal carcinomas. Mod. Pathol. 2017, 30, 278–285. [Google Scholar] [CrossRef]
- Ahern, E.; Harjunpää, H.; O'Donnell, J.S.; Allen, S.; Dougall, W.C.; Teng, M.W.L.; Smyth, M.J. RANKL blockade improves efficacy of PD1-PD-L1 blockade or dual PD1-PD-L1 and CTLA4 blockade in mouse models of cancer. Oncoimmunology 2018, 7, e1431088. [Google Scholar] [CrossRef]
- Andre, T.; Lonardi, S.; Wong, K.Y.M.; Lenz, H.J.; Gelsomino, F.; Aglietta, M.; Morse, M.A.; Van Cutsem, E.; McDermott, R.; Hill, A.; et al. Nivolumab plus low-dose ipilimumab in previously treated patients with microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer: 4-year follow-up from CheckMate 142. Ann. Oncol. 2022, 33, 1052–1060. [Google Scholar] [CrossRef]
- Marginean, E.C.; Melosky, B. Is there a role for programmed death ligand-1 testing and immunotherapy in colorectal cancer with microsatellite instability? Part i—Colorectal cancer: Microsatellite instability, testing, and clinical implications. Arch. Pathol. Lab. Med. 2017, 142, 17–25. [Google Scholar] [CrossRef]
- Lee, L.H.; Cavalcanti, M.S.; Segal, N.H.; Hechtman, J.F.; Weiser, M.R.; Smith, J.J.; Garcia-Aguilar, J.; Sadot, E.; Ntiamoah, P.; Markowitz, A.J.; et al. Patterns and prognostic relevance of PD-1 and PD-L1 expression in colorectal carcinoma. Mod. Pathol. 2016, 29, 1433–1442. [Google Scholar] [CrossRef]
- Zhou, E.; Huang, Q.; Wang, J.; Fang, C.; Yang, L.; Zhu, M.; Chen, J.; Chen, L.; Dong, M. Up-regulation of Tim-3 is associated with poor prognosis of patients with colon cancer. Int. J. Clin. Exp. Pathol. 2015, 8, 8018–8027. [Google Scholar] [PubMed]
- Teng, F.; Meng, X.; Kong, L.; Mu, D.; Zhu, H.; Liu, S.; Zhang, J.; Yu, J. Tumor-infiltrating lymphocytes, forkhead box P3, programmed death ligand-1, and cytotoxic T lymphocyte–associated antigen-4 expressions before and after neoadjuvant chemoradiation in rectal cancer. Transl. Res. 2015, 166, 721–732. [Google Scholar] [CrossRef]
- Brandacher, G.; Perathoner, A.; Ladurner, R.; Schneeberger, S.; Obrist, P.; Winkler, C.; Werner, E.R.; Werner-Felmayer, G.; Weiss, H.G.; G√∂bel, G.; et al. Prognostic value of indoleamine 2,3-dioxygenase expression in colorectal cancer: Effect on tumor-infiltrating T cells. Clin. Cancer Res. 2006, 12, 1144–1151. [Google Scholar] [CrossRef] [PubMed]
- Taube, J.M.; Young, G.D.; McMiller, T.L.; Chen, S.; Salas, J.T.; Pritchard, T.S.; Xu, H.; Meeker, A.K.; Fan, J.; Cheadle, C.; et al. Differential expression of immune-regulatory genes associated with PD-L1 display in melanoma: Implications for PD-1 pathway blockade. Clin. Cancer Res. 2015, 21, 3969–3976. [Google Scholar] [CrossRef] [PubMed]
- Talaat, I.M.; Elemam, N.M.; Zaher, S.; Saber-Ayad, M. Checkpoint molecules on infiltrating immune cells in colorectal tumor microenvironment. Front. Med. (Lausanne) 2022, 9, 955599. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, J.; Smits, E.; Lardon, F.; Pauwels, P.; Deschoolmeester, V. Immune checkpoint modulation in colorectal cancer: What's new and what to expect. J. Immunol. Res. 2015, 2015, 158038. [Google Scholar] [CrossRef]
- Li, Y.; Liang, L.; Dai, W.; Cai, G.; Xu, Y.; Li, X.; Li, Q.; Cai, S. Prognostic impact of programed cell death-1 (PD-1) and PD-ligand 1 (PD-L1) expression in cancer cells and tumor infiltrating lymphocytes in colorectal cancer. Mol. Cancer 2016, 15, 55. [Google Scholar] [CrossRef]
- Shan, T.; Chen, S.; Wu, T.; Yang, Y.; Li, S.; Chen, X. PD-L1 expression in colon cancer and its relationship with clinical prognosis. Int. J. Clin. Exp. Pathol. 2019, 12, 1764–1769. [Google Scholar]
- Ntomi, V.; Foukas, P.; Papaconstantinou, D.; Antonopoulou, I.; Pikoulis, A.; Panagiotides, I.; Pikoulis, E.; Syrigos, K. The clinical significance of PD-L1 in colorectal cancer (Review). Oncol. Rep. 2021, 45, 92. [Google Scholar] [CrossRef]
- Yu, M.; Lu, B.; Liu, Y.; Me, Y.; Wang, L.; Zhang, P. Tim-3 is upregulated in human colorectal carcinoma and associated with tumor progression. Mol. Med. Rep. 2017, 15, 689–695. [Google Scholar] [CrossRef]
- Mokhtari, Z.; Rezaei, M.; Sanei, M.H.; Dehghanian, A.; Faghih, Z.; Heidari, Z.; Tavana, S. Tim3 and PD-1 as a therapeutic and prognostic targets in colorectal cancer: Relationship with sidedness, clinicopathological parameters, and survival. Front. Oncol. 2023, 13, 1069696. [Google Scholar] [CrossRef] [PubMed]
- Burugu, S.; Asleh-Aburaya, K.; Nielsen, T.O. Immune infiltrates in the breast cancer microenvironment: Detection, characterization and clinical implication. Breast Cancer (Auckl) 2017, 24, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Triebel, F.; Jitsukawa, S.; Baixeras, E.; Roman-Roman, S.; Genevee, C.; Viegas-Pequignot, E.; Hercend, T. LAG-3, a novel lymphocyte activation gene closely related to CD4. J. Exp. Med. 1990, 171, 1393–1405. [Google Scholar] [CrossRef] [PubMed]
- Anderson, Ana C. ; Joller, N.; Kuchroo, Vijay K. Lag-3, tim-3, and tigit: Co-inhibitory receptors with specialized functions in immune regulation. Immunity 2016, 44, 989–1004. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Yu, H.; Rozeboom, L.; Rivard, C.J.; Ellison, K.; Dziadziuszko, R.; Suda, K.; Ren, S.; Wu, C.; Hou, L.; et al. Lag-3 protein expression in non–small cell lung cancer and its relationship with PD-1/PD-L1 and tumor-infiltrating lymphocytes. J. Thorac. Oncol. 2017, 12, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Rhyner Agocs, G.; Assarzadegan, N.; Kirsch, R.; Dawson, H.; Galvan, J.A.; Lugli, A.; Zlobec, I.; Berger, M.D. Lag-3 expression predicts outcome in stage ii colon cancer. J. Pers. Med. 2021, 11, 749. [Google Scholar] [CrossRef] [PubMed]
- Tavana, S.; Mokhtari, Z.; Sanei, M.H.; Heidari, Z.; Dehghanian, A.R.; Faghih, Z.; Rezaei, M. Clinicopathological significance and prognostic role of LAG3 + tumor-infiltrating lymphocytes in colorectal cancer; relationship with sidedness. Cancer Cell Int. 2023, 23, 23. [Google Scholar] [CrossRef] [PubMed]
- Bang, H.J.; Sohn, J.H.; Kim, S.K.; Kim, C.S.; Cho, M.Y.; Kim, B.; An, S.; Kim, K.; Kim, Y. Concurrent upregulation of immune checkpoint molecule genes in colorectal cancer. Mol. Cell. Toxicol. 2022, 19, 521–529. [Google Scholar] [CrossRef]
- Datar, I.; Sanmamed, M.F.; Wang, J.; Henick, B.S.; Choi, J.; Badri, T.; Dong, W.; Mani, N.; Toki, M.; Mejías, L.D.; et al. Expression analysis and significance of PD-1, lag-3, and tim-3 in human non–small cell lung cancer using spatially resolved and multiparametric single-cell analysis. Clin. Cancer Res. 2019, 25, 4663–4673. [Google Scholar] [CrossRef]
- Chalabi, M.; Fanchi, L.F.; Dijkstra, K.K.; Van den Berg, J.G.; Aalbers, A.G.; Sikorska, K.; Lopez-Yurda, M.; Grootscholten, C.; Beets, G.L.; Snaebjornsson, P.; et al. Neoadjuvant immunotherapy leads to pathological responses in MMR-proficient and MMR-deficient early-stage colon cancers. Nat. Med. 2020, 26, 566–576. [Google Scholar] [CrossRef]
- Han, K.; Tang, J.H.; Liao, L.E.; Jiang, W.; Sui, Q.Q.; Xiao, B.Y.; Li, W.R.; Hong, Z.G.; Li, Y.; Kong, L.H.; et al. Neoadjuvant immune checkpoint inhibition improves organ preservation in t4bm0 colorectal cancer with mismatch repair deficiency: A retrospective observational study. Dis. Colon Rectum 2023, 66, e996–e1005. [Google Scholar] [CrossRef]
- Diaz, L.A., Jr.; Shiu, K.K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab versus chemotherapy for microsatellite instability-high or mismatch repair-deficient metastatic colorectal cancer (KEYNOTE-177): Final analysis of a randomised, open-label, phase 3 study. Lancet Oncol. 2022, 23, 659–670. [Google Scholar] [CrossRef] [PubMed]
- Overman, M.J.; Lonardi, S.; Wong, K.Y.M.; Lenz, H.J.; Gelsomino, F.; Aglietta, M.; Morse, M.A.; Van Cutsem, E.; McDermott, R.; Hill, A.; et al. Durable clinical benefit with nivolumab plus ipilimumab in DNA mismatch repair-deficient/microsatellite instability-high metastatic colorectal cancer. J. Clin. Oncol. 2018, 36, 773–779. [Google Scholar] [CrossRef]
- Morse, M.A.; Overman, M.J.; Hartman, L.; Khoukaz, T.; Brutcher, E.; Lenz, H.J.; Atasoy, A.; Shangguan, T.; Zhao, H.; El-Rayes, B. Safety of nivolumab plus low-dose ipilimumab in previously treated microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer. Oncologist 2019, 24, 1453–1461. [Google Scholar] [CrossRef]
- Cohen, R.; Bennouna, J.; Meurisse, A.; Tournigand, C.; De La Fouchardiere, C.; Tougeron, D.; Borg, C.; Mazard, T.; Chibaudel, B.; Garcia-Larnicol, M.L.; et al. RECIST and iRECIST criteria for the evaluation of nivolumab plus ipilimumab in patients with microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer: The GERCOR NIPICOL phase II study. J. Immunother. Cancer 2020, 8, e001499. [Google Scholar] [CrossRef]
- Hellmann, M.D.; Paz-Ares, L.; Bernabe Caro, R.; Zurawski, B.; Kim, S.-W.; Carcereny Costa, E.; Park, K.; Alexandru, A.; Lupinacci, L.; de la Mora Jimenez, E.; et al. Nivolumab plus ipilimumab in advanced non–small-cell lung cancer. N. Engl. J. Med. 2019, 381, 2020–2031. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Immunohistochemical analysis of immune check point proteins. (A) Negative PD-L1 expression. (B) Positive PD-L1 expression in tumor cells. (C) Negative PD-1 expression. (D) Positive PD-1 expression in tumor cells. (E) Negative LAG-3 expression. (F) Positive LAG-3 expression in tumor cells. (G) Negative TIM-3 expression. (H) Positive TIM-3 expression. PD-L1, programmed cell death-ligand 1; PD-1, programmed cell death protein 1; TIM-3, T cell immunoglobulin and mucin domain-containing protein 3; LAG-3, lymphocyte-activation gene 3.
Figure 1.
Immunohistochemical analysis of immune check point proteins. (A) Negative PD-L1 expression. (B) Positive PD-L1 expression in tumor cells. (C) Negative PD-1 expression. (D) Positive PD-1 expression in tumor cells. (E) Negative LAG-3 expression. (F) Positive LAG-3 expression in tumor cells. (G) Negative TIM-3 expression. (H) Positive TIM-3 expression. PD-L1, programmed cell death-ligand 1; PD-1, programmed cell death protein 1; TIM-3, T cell immunoglobulin and mucin domain-containing protein 3; LAG-3, lymphocyte-activation gene 3.
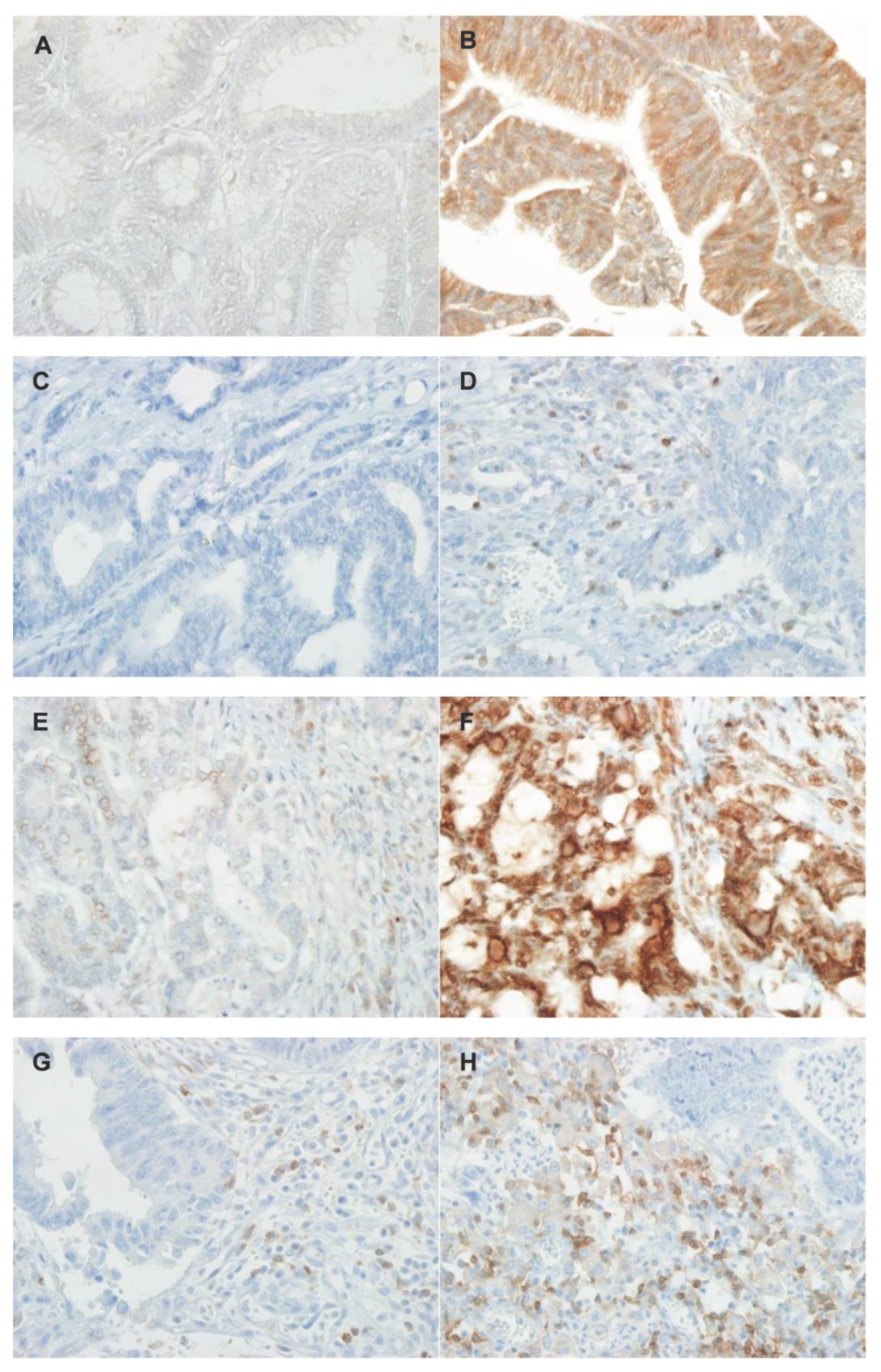
Figure 2.
Concurrent expression of multiple immune checkpoint molecules. (A) Center of tumor. (B) Border of tumor. MSS, microsatellite stable; MSI-H, microsatellite instability high.
Figure 2.
Concurrent expression of multiple immune checkpoint molecules. (A) Center of tumor. (B) Border of tumor. MSS, microsatellite stable; MSI-H, microsatellite instability high.
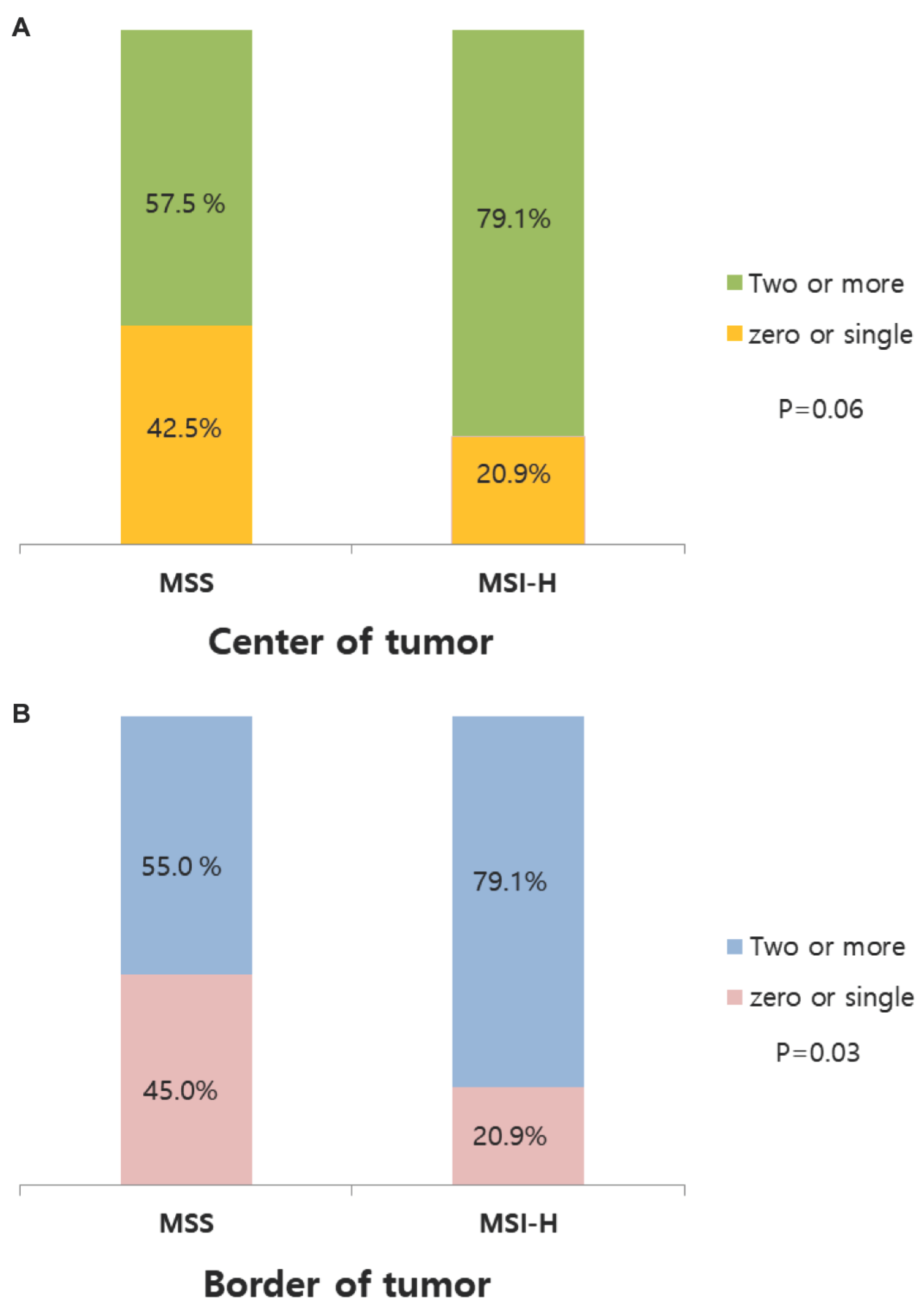

Table 1.
Comparison of the baseline demographics of patients with colorectal cancer stratified into the MSS or MSI-H groups.
Table 1.
Comparison of the baseline demographics of patients with colorectal cancer stratified into the MSS or MSI-H groups.
| MSS (%) (n = 40) |
MSI-H (%) (n = 43) |
P value | |
|---|---|---|---|
| Age (year) | |||
| Mean (SD) | 67.4 (13) | 66.3 (14.5) | 0.305 |
| Gender | |||
| Female | 21 (52.5) | 25 (58.1) | 0.662 |
| Male | 19 (47.5) | 18 (41.9) | |
| ASA score | |||
| 1 | 5 (12.5) | 5 (11.6) | 0.784 |
| 2 | 23 (57.5) | 22 (51.2) | |
| 3 | 12 (30.0) | 16 (37.2) | |
| Tumor location | |||
| Proximal | 10 (25.0) | 29 (67.4) | 0.001 |
| Distal | 13 (32.5) | 7 (16.3) | |
| Rectum | 17 (42.5) | 7 (16.3) | |
| CEA | |||
| <5 | 26 (65.0) | 31 (72.1) | 0.636 |
| 5≥ | 14 (35.0) | 12 (27.9) | |
| T stage | |||
| 2-3 | 29 (72.5) | 28 (65.1) | 0.489 |
| 4 | 11 (27.5) | 15 (34.9) | |
| N stage | |||
| 0 | 25 (62.5) | 28 (65.1) | 0.823 |
| 1-2 | 15 (37.5) | 15 (34.9) | |
| TNM stage | |||
| I-II | 24(60.0) | 28(65.1) | 0.656 |
| III | 16(40.0) | 15(34.9) | |
| Differentiation | |||
| High grade | 38 (95.0) | 31 (72.1) | 0.007 |
| Low grade | 2 (5.0) | 12 (27.9) | |
| Lymphatic invasion | |||
| No | 22 (55.0) | 22 (51.2) | 0.827 |
| Yes | 18 (45.0) | 21 (48.8) | |
| Lymph node harvest | |||
| Mean (SD) | 25.48 (11.79) | 33.2 (13.37) | 0.320 |
| Recurrence | |||
| No | 29 (72.5) | 38 (88.4) | 0.067 |
| Yes | 11 (27.5) | 5 (11.6) | |
| Cancer related Mortality | |||
| No | 38 (95.0) | 38 (88.4) | 0.435 |
| Yes | 2 (5.0) | 5 (11.6) |
MSS, microsatellite stable; MSI-H, microsatellite instability high; SD, standard deviation; ASA, American Society of Anesthesiologists; CEA, carcinoembryonic antigen.
Table 2.
Expression of immune checkpoint molecules (ICMs) in patients with MSS and MSI-H colorectal cancer.
Table 2.
Expression of immune checkpoint molecules (ICMs) in patients with MSS and MSI-H colorectal cancer.
| MSS (%) (n = 40) |
MSI-H (%) (n = 43) |
P value | |
|---|---|---|---|
| Center of tumor | |||
| PD-L1 | |||
| negative | 37 (92.5) | 25 (58.1) | < 0.001 |
| positive | 3 (7.5) | 18 (41.9) | |
| PD-1 | |||
| negative | 28(70.0) | 27 (62.8) | 0.643 |
| positive | 12(30.0) | 16 (37.2) | |
| TIM-3 | |||
| negative | 21 (55.2) | 13 (30.2) | 0.047 |
| Positive | 19 (47.5) | 30 (69.8) | |
| LAG-3 | |||
| negative | 10 (30.0) | 10 (23.3) | 1.000 |
| positive | 30 (75.0) | 33 (76.7) | |
| Border of tumor | |||
| PD-L1 | |||
| negative | 32 (80.0) | 31 (72.1) | 0.450 |
| positive | 8 (20.0) | 12 (27.9) | |
| PD-1 | |||
| negative | 24 (60.0) | 19 (44.2) | 0.189 |
| positive | 16 (40.0) | 24 (55.8) | |
| TIM-3 | |||
| negative | 22 (55.0) | 20 (46.5) | 0.512 |
| Positive | 18 (45.0) | 23 (53.5) | |
| LAG-3 | |||
| negative | 11 (27.5) | 6 (14.0) | 0.175 |
| positive | 29 (72.5) | 37 (86.0) |
MSS, microsatellite stable; MSI-H, microsatellite instability high; PD-L1, programmed cell death-ligand 1; PD-1, programmed cell death protein 1; TIM-3, T cell immunoglobulin and mucin domain-containing protein 3; LAG-3, lymphocyte-activation gene 3.
Table 3.
Concurrent expression of multiple immune checkpoint molecules.
| Center of tumor | MSS (n = 40) | MSI-H (n = 43) | Total (n = 83) |
|---|---|---|---|
| PD-L1+PD1+TIM3+LAG3 | 1 | 8 | 9 |
| PD-L1+PD1+TIM3 | 0 | 0 | 0 |
| PD-L1+PD1+LAG3 | 1 | 0 | 1 |
| PD-L1+TIM3+LAG3 | 0 | 4 | 4 |
| PD-1+TIM3+LAG3 | 5 | 3 | 8 |
| PD-L1+PD1 | 0 | 2 | 2 |
| PD-L1+TIM3 | 0 | 0 | 0 |
| PD-L1+LAG3 | 1 | 3 | 4 |
| PD1+TIM3 | 0 | 1 | 1 |
| PD1+LAG3 | 3 | 1 | 4 |
| TIM3+LAG3 | 12 | 12 | 24 |
| PD-L1 | 0 | 1 | 1 |
| PD1 | 2 | 1 | 3 |
| TIM3 | 1 | 2 | 3 |
| LAG3 | 7 | 2 | 9 |
| All negative | 7 | 3 | 10 |
| Border of tumor | |||
| PD-L1+PD1+TIM3+LAG3 | 4 | 4 | 8 |
| PD-L1+PD1+TIM3 | 0 | 0 | 0 |
| PD-L1+PD1+LAG3 | 4 | 6 | 10 |
| PD-L1+TIM3+LAG3 | 0 | 0 | 0 |
| PD1+TIM3+LAG3 | 5 | 6 | 11 |
| PD-L1+PD1 | 0 | 1 | 1 |
| PD-L1+TIM3 | 0 | 0 | 0 |
| PD-L1+LAG3 | 0 | 1 | 1 |
| PD1+TIM3 | 1 | 1 | 2 |
| PD1+LAG3 | 1 | 4 | 5 |
| TIM3+LAG3 | 7 | 11 | 18 |
| PD-L1 | 0 | 0 | 0 |
| PD1 | 1 | 2 | 3 |
| TIM3 | 1 | 1 | 2 |
| LAG3 | 8 | 5 | 13 |
| All negative | 8 | 1 | 9 |
MSS, microsatellite stable; MSI-H, microsatellite instability high; PD-L1, programmed cell death-ligand 1; PD-1, programmed cell death protein 1; TIM-3, T cell immunoglobulin and mucin domain-containing protein 3; LAG-3, lymphocyte-activation gene 3.
Table 4.
Expression of multiple immune checkpoint molecules in patients with MSS and MSI-H colorectal cancer.
Table 4.
Expression of multiple immune checkpoint molecules in patients with MSS and MSI-H colorectal cancer.
| zero or single | Two or more | P-value | |
|---|---|---|---|
| Center of tumor | |||
| MSS | 17 (42.5) | 23 (57.5) | |
| MSI-H | 9 (20.9) | 34 (79.1) | 0.06 |
| Border of tumor | |||
| MSS | 18 (45.0) | 22 (55.0) | |
| MSI-H | 9 (20.9) | 34 (79.1) | 0.03 |
MSS, microsatellite stable; MSI-H, microsatellite instability high.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



