
Submitted:
21 February 2024
Posted:
22 February 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Exposure to vaccine lipid nanoparticles, mRNA, adenoviral DNA, and or Spike protein from one of the approved Covid-19 vaccines, or through secondary exposure, as through blood transfusion, is a potential source of harm. Blood reactions are an acknowledged side-effect of Covid-19 vaccination, not limited to hemolysis, paroxysmal nocturnal hemoglobinuria, chronic cold agglutinin disease, immune thrombocytopenia, haemophagocytosis, hemophagocytic lymphohistiocytosis, and many other blood related conditions. The observation of adverse events has motivated investigation into the cardiovascular mechanisms of harm by Covid-19 vaccines, and the biodistribution of vaccine contents. Biodistribution may not be limited to the body of the vaccine recipient, as a growing body of evidence demonstrates the possibility of secondary exposure to vaccine particles. These can be via bodily fluids and include the following routes of exposure: blood transfusion, organ transplantation, breastfeeding, and possibly other means. As covid-19 vaccines are associated with an increased risk of stroke, the persistence of vaccine artifacts in the blood presents a possible threat to a recipient of a blood donation from a vaccinated donor who suffered from vaccine induced thrombosis or thrombocytopenia. (VITT) We assess the feasibility and significance of these risks through an overview of the case report literature of blood disorders in vaccinated individuals, pharmacovigilance reports from the US Vaccine Adverse Events Reporting System (VAERS) and a meta-analysis of the available literature on organ transplants from vaccinated organ donors. Our analysis establishes biological mechanistic plausibility, a coherent safety signal in pharmacovigilance databases for secondary vaccine contents exposure (for the cases of blood transfusion and breastfeeding) and also an elevated level of adverse events in organ transplants from VITT-deceased donors, echoing increases in organ transplantation related complications seen in national statistics for some countries. Secondary exposure to vaccine artifacts is a potential explanation for some of the cases put forth, and requires a deeper investigation.
Keywords:
Covid-19 vaccination
; mRNA vaccine
; lipid nanoparticles
; blood transfusion
; breastfeeding exposure
; pharmacovigilance
1. Introduction
Since the introduction of Covid-19 vaccines, much attention has been given to the safety signal of myocarditis, as well as the development of blood clots and hemolysis. SARS-CoV-2 exerts its pernicious impacts via the cardiovascular system1–4, and most of the fatalities from Covid-19 were associated with cardiovascular inflammation and clotting5–9. Vaccines developed during 2020 showed promising levels of protection in the clinical trials leading to their approval in many nations10,11, however, a cardiovascular safety signal emerged, first with the AstraZeneca vaccine12–14, leading to its suspension in several nations15. A thrombotic safety signal was also found in the Johnson and Johnson adenovirus-vectored vaccine16–18, leading to its suspension in the USA19.
Later on, a similar safety signal was observed for the Moderna and Pfizer mRNA vaccines20, both messenger RNA (mRNA) vaccines encapsulated in lipid nanoparticles (LNPs). Currently, several countries no longer promote the use of Covid-19 vaccines in younger populations, owing to the low likelihood of risk from Covid-19 and the increased risk of vaccine injury, disability, and death for these populations. Cardiovascular events were much higher than any previously approved vaccines in use, based on analyses of the various pharmacovigilance schemes. Several nations discontinued vaccination in younger people, notably Denmark 21.
Immune activation cascades occurring in the circulatory system, either in the blood through thrombosis or thrombocytopenia, or in the epithelial cells of the vasculature, can alter the normal flow of blood. In extreme cases, this can lead to a stroke. Given the fact that vaccines show a safety signal consistent with alterations in blood properties, it is reasonable to examine the possibility for carry-over effects into blood transfusion.
Given the focus on cardiovascular risks from the vaccines, and one route of exposure, albeit uncommon, to Covid-19 vaccine products and their after-effects is via blood transfusion and organ transplantation. Limited literature exists on the comparisons between the blood of vaccinated people and that of unvaccinated people22,23; nonetheless, despite the paucity of evidence, many blood banks claim that there are no significant differences24–26.
Materials and Methods
We propose that the question of secondary exposure to vaccine particles is yet unresolved and requires further investigation. This is based on four classes of argument:
- Firstly, the persistence of vaccine mRNA/adenoviral DNA lipid nanoparticles and their products (ie spike protein) for long periods following vaccinations lends plausibility to this mechanism of harm. This review of the literature evidence establishes biological plausibility. As vaccine particles and altered blood parameters are found months after inujection, these may potentially be passed onto a blood donation recipient.
- Secondly, the case report literature demonstrates many circulatory disorders manifesting in differed blood characteristics in cases of the primary recipient of the injection, as well as adverse events following exposure to the bodily fluids of vaccinees. The modalities of transmission for which there is a pharmacovigilance signal are blood transfusion and breastfeeding. These establish a pharmacovigilance signal from exposure to vaccinees blood (in the case of blood donation) and breastmilk, in the case of breastfeeding.
- Lastly, recipients of organ transplant from donors deceased due to Vaccine Induced Thrombosis and Thrombocytopenia (VITT), encountered blood clotting and thrombotic events, suggesting a possible danger for organ donation, as well as blood transfusion. National monitoring for adverse events following organ transplantation also showed an increased rate of adverse events in temporal relationship to mass vaccination, but others show no increase.
2. Results
2.1. Mechanisms of Harm
The conditions of natural infection and vaccination are similar and distinct in several important ways. They are similar in that both conditions involve the expression of the spike protein in the cells via the vaccine or viral RNA. The spike protein is identified as the etiological agent for a significant portion of the cardiovascular damage of both SARS-CoV-2 infection1,27 and vaccination against Covid-1928,29.
The first Covid-19 vaccine to be investigated for cardiovascular damage was the AstraZeneca vaccine, which caused clotting disorders in several of its recipients30, and leading to its restriction in several countries31. Afterwards, the Johnson and Johnson vaccines32, as well as the Moderna mRNA COVID-19 vaccines33 demonstrated cardiovascular safety signals, leading to their suspensions in the USA34 and in Scandinavian nations (for young people)35 respectively
The proposed mechanism for cardiovascular injury from Covid-19 vaccines has been advanced in recent reviews36,37. Spike protein induced clotting, being an unanticipated side effect of the vaccines, warrants attention and caution when transfusing blood from one person to the other, depending on the time since vaccination, there may still be vaccine particles or spike protein present in the blood. It was previously assumed that the vaccine particles would remain at the site of injection38 and break down rapidly39. However, both vaccine spike antigen and mRNA have been found in vaccine recipients 60 days40 post-vaccination and spike protein antigen has been found 120 days post-vaccination41. The Red Cross claimed in a wishful public statement that vaccine particles do not enter the bloodstream42, which has been contradicted by biodistribution studies43.
One potential cause for concern is the observation that anti-platelet factor 4 antibodies have been measured are elevated 7 months post vaccination in a subset of vaccine recipients44, and other studies show a small percentage of vaccinated patients maintain elevated levels long term45,46. Most patients have a transient response47–49, but approximately 1% of patients maintain elevated anti-PF4 levels45, which can lead to clotting50. This remains cause for concern, as the triggering of this immune response can well lead to a clotting cascade51.
2.2. Pharmacovigilance
The large-scale administration of covid-19 vaccine products requires post marketing surveillance to monitor any safety signal emerging from adverse event reports. Pharmacovigilance databases have observed an unprecedented number of adverse event (AE) reports since the rollout of vaccines. These include the USA Vaccine Adverse Events Reporting System (VAERS)52, the US-based V-safe database53, the UK based yellow card scheme54, the European EudraVigilance system55 and the World Health Organization’s (WHO’s) VigiBase56. These resources were developed for the purpose of monitoring the safety profile of vaccines after approval. Despite a large number of AE reports for the Covid-19 vaccines57, the vaccines are still approved for use and recommended in the USA and other countries as of this writing (July 30, 2023).
2.2.1. Case Reports of Blood Manifestations
Recent reviews cover cardiovascular adverse events, finding an increased rate compared to previous vaccines58–62. In addition to these monitoring systems, there are also hundreds of case reports in the medical literature which have been linked to the vaccine by the medical provider (Table 1). These can broadly fall into the categories of VITT63,
Postmortem data also supports a causative role for the vaccine in the death of the patient. These autopsies, by immunohistochemically staining for both spike (S) protein and nucleocapsid (N) protein, can determine if a case is vaccine caused or caused by SARS-CoV-2 infection273. As the vaccines mentioned above only contain the spike protein, whereas natural infection results in both S and N proteins, observing S in the absence of N protein highly suggests that the proteins came from vaccines, and not SARS-CoV-2 infection274.
2.2.2. Blood Transfusions
Since vaccine contents and their downstream manifestations (e.g. microclots) remain in the bloodstream for long periods of time41, blood transfusion is a potential (secondary) route of exposure to vaccine particles.
There are 1352 transfusion reports in VAERS as of May 15, 2023 (Figure 1). In 2019, there were 10,852,000 blood transfusions performed in the USA275. Taking that as the per-year rate, roughly 24 million blood transfusions were performed since the beginning of mass-vaccination campaigns in Spring 2021. If roughly ¾ of the donors were vaccinated, that makes the denominator 18, 000, 000 transfusions. The adverse event rate is roughly 1/13 000 transfusions, or 1/429 taking into account the under reporting factor of 31 as estimated by Rose276.
As of May 25, 2023, according to the Worldometer277, the population in the United States is 336,688,028. And according to Our World in Data, the number of Americans who have received at least one dose of the COVID-19 injectable products is 270,230,000, or 80% of the US population278. Considering the time course of vaccination; from the period of 1st March, 2021 to May 25, 2023, the time-averaged vaccination percentage is 70%278. A 2019 statistic puts the number of blood transfusions occurring yearly in the USA at 10,852,000275, putting the approximate number of blood transfusions during the above period at 24.2 million. Of the 24.2 million, approximately 17 million would have received a Covid-19 vaccine. Using the number of individuals who had received both an injection and a transfusion, and the number of reports of adverse events in VAERS of transfusions, we get a rate of 1/12,570 and with an under-reporting of 31, this becomes 1/405.
2.2.3. Breastfeeding and Maternal Exposure
Given that vaccine contents have been observed in breast milk279, breastfeeding presents a possible, albeit likely transient, route of secondary exposure for nursing babies.
In VAERS as of May 15, 2023, the search terms (“Breast feeding”, “Breast milk discolouration”, “Exposure via breast milk”, “Maternal exposure during breast feeding”) return N = 1,835 total reports of adverse events (Figure 2).
Although the absolute count of reports is not very high, the under-reporting factor is not accounted for here. If we use the under-reporting factor of 31 as estimated by Rose276, the number of incidents becomes N = 56,885. This means that of the population of women who were injected who were also breast-feeding at the time, a likely meaningful proportion reported an adverse event to VAERS. Between December 14, 2020 and May 10, 2023, 60,615,370 women between the ages of 18 and 49 were reported to have been injected with at least one dose of the COVID products280. The age groups 18-24 and 25-49, as per the CDC grouping, span the child-bearing years appropriately.
Since the estimated fertility rate for women of childbearing age (15-44 years) in the United States in 2021 was 56.3 births per thousand women per year281, we can estimate that the number of women who gave birth (in the window of December 14, 2020 to May 10, 2023) of the number injected was 8,326,855. We can also estimate the number of women breastfeeding of those births since ~83% of infants are breastfed immediately, according to the CDC breastfeeding report card released in 2022 (based off 2019 data)282. Therefore, by these rates, there were approximately 6,911,289 women breastfeeding at the time of injection with COVID products. This is a rough estimate, but it is based on recent data provided by the CDC. If we use this number and compare it with the number of reports in VAERS using an under-reporting factor of 31, we get 56,885 women succumbing to adverse events out of 6,911,289. That’s a rate of 1/121, approximately. Even without the under-reporting factor, we still get a reporting rate of 1/3766.
Of the 1,835 reports, 6.6% are made for infants 4 years of age or less and of these reports, 25% are considered severe adverse events (SAEs). The VAERS handbook states that approximately 7% of reported AEs are classified as severe283, so here the proportion of serious events to total events is 18 percentage points above the norm. To be clear, neither these infants nor their mothers required the COVID-19 injections since the Infection Fatality Rate (IFR) is 0.05% for individuals less than 70 years of age284. The infants would have inherited existing immunity from neutralizing IgA antibodies, for example, from their mother’s milk since their mother likely would have generated robust and long-lasting immunity involving both antibody and T cell responses from exposure to SARS-CoV-2285. Instead, it appears as though they are suffering from severe adverse events from their mother’s milk that contains not only SARS-CoV-2 antibody proteins286,287 but traces of the injection materials279 and likely spike proteins as well. It is critical that we examine the connection between the emergence of these SAEs in infants due to exposure to the COVID-19 injectable products via breast milk.
2.2.4. Other routes of exposure
While dosage would likely be minimal, it is possible that others be exposed to vaccine particles via other routes. Shedding is observed in adenovirus vectored vaccines288, which would apply to Johnson & Johnson and the AstraZeneca vaccines289. One important distinction is that while viral shedding can be ruled out with mRNA vaccines, because they only contain the mRNA encoding the spike protein, exposure to the vaccine particles themselves can occur, albeit in very miniscule quantities.
In households where one person was vaccinated, other family members developed spike protein antibodies290. While the cited article explained this in terms of the transfer of antibodies themselves, this would likely not be persistent. In cases where the antigen (spike protein) is transferred, this may possibly explain the presence of anti-spike antibodies in the serum of unvaccinated and unexposed (to SARS-CoV-2) individuals.
Sexual intercourse is a possible mode of transmission as spike protein RNA has been observed in semen during SARS-CoV-2 infection291. Inactivated viral vector Covid-19 vaccines have been observed to decrease sperm morphology292 and motility293, and increase DNA fragmentation292, though studies do not see this effect with mRNA vaccines294,295.
Transfer through either exhalation or skin-to-skin contact has anecdotal accounts supporting it, but limited published evidence exists. Mechanistically, the lipid nanoparticles of the mRNA injections are very similar to endogenous exosomes, which can be transmitted trans-dermally, via inhalation, via breast milk and across the placenta (Figure 3)296.
Spike protein can importantly be packaged into exosomes297, and precedent exists for the presence of RNA-containing exosomes in breath 298–300. A recent review has summarized the persistence of vaccine components in different bodily fluids 301, finding evidence for persistence of spike protein in lymph nodes40, on skin302 and in blood40,303, and persistent spike protein mRNA in lymph nodes40 and in blood plasma304.
2.3. Organ Transplant Safety
Another source of information on the safety of blood transfusions is the organ transplant literature. Blood type matching is necessary for organ transplantation, in addition to other criteria, such as organ size. Current approaches are lowering the risk of transplant rejection by matching donor and recipient human leukocyte antigen (HLA)305–307.
There are several case reports of transplants from vaccinated donors. This literature focuses mostly on donors who died due to VITT. In the case of organ transplantation, with few exceptions, such as the kidney, the donor must be deceased. Considering these donors were classified as having died from VITT by a medical professional, these donations are more likely to present safety issues than blood donation, where the donor does not have manifested VITT, as this would deem them ineligible or at the very least reluctant to donate.
Vaccination mandates with respect to transplantation, especially for recipients, have been a source of controversy during the Covid-19 pandemic308–313. Several centers have refused to provide transplants to unvaccinated prospective recipients.
Our search returns 8 articles focusing on transplants from donors deemed deceased from VITT314–320 (Table 2).
Several people, having died from likely VITT, have donated their organs for medical transplantation. While the blood used during a transplant operation is typically given by a separate donor, still, this high rate of complications in recipients is cause for concern. Transplantation of organs from those suffering stroke is a common occurrence and has a low failure rate. In a Canadian study of kidney transplant recipients, where the donor died of stroke, only 5% of recipients were on dialysis after 1 year and there were no deaths in hospital323, so the vast majority of the kidney transplants worked.
A study calculated the rate of microthrombi formation in recipients where the donor dies from a cardiac death (DCD) as 3.3%324. This was not significantly different from the rate of microthrombi formation in recipients where the donor dies due to brain death (DBD), which is 11.3% 324. The rate of microthrombi and thrombotic complications is much higher in recipients of donors deceased due to VITT, at 30% of recipients (Table 2).Another study observed rates of vascular complications in the recipients of liver transplants from donors deceased due to cardiovascular events in 7 to 14% of transplant recipients325. The uncertainty is because there are two categories of vascular complications, ‘hepatic artery thrombosis’ and ‘other’, and it is not specified what the degree of overlap (recipients experiencing both types of complications) there is. Another study of recipients of liver transplants from DCD cases showed a rejection rate due to thrombotic complications of 2%, comparable with 3% of recipients of DBD326. Another Swedish study reported rates of hepatic artery thrombosis in 8 of 24 liver graft recipients from DCD donors, or 33%327. A large meta-analysis found vascular thrombosis of 3% in DCD liver graft recipients, and 2% in DBD liver graft recipients328. The same meta-analysis observed rates of vascular stenosis of 4% in DCD and 2% in DBD liver graft recipients.
These operations have mixed success, as many of these transplantations are successful, still, there remain several cases where the recipient experienced thrombotic events which persisted over long term. Still, all considered, the risks of organ transplantation may be outweighed by the definite dangers of not going through with a transplant.
Data monitoring for increases in transfusion reactions is limited. Several national hemovigilance systems do not observe a significant increase in adverse event rates in 2021 compared to previous years 329,330. Other systems have not yet published hemovigilance for 2021331, though Austria reported a 49% increase in transfusion reactions (49 in 2020 to 73 in 2021) from 2020 to 2021332, Denmark saw a significant increase in adverse reactions between 2020 and 2021333 and UK hemovigilance data shows an increase in blood component issues from 2020 to 2021334. Additionally transplantation adverse event rates in Canada rose significantly, from less than 3 transfusion adverse events per year to 12 between 2020 and 2021335. In Japan there was a slight increase of 7% from 2020 to 2021336
3. Discussion
In total, we did not find evidence to support the safety of COVID-19 vaccine recipients to donate blood.. Questions remain over the safety of associated blood products and secondary exposure to vaccine particles. Circulatory AEs associated with C19 vaccination far outstrip any previous vaccine, and may be cause for concern, as clotting can exist at a subclinical level and evade detection for many years, unless explicitly tested for, through measurements of D-dimer or troponin, for example.
One open question is if the waiting period to donate blood post vaccination is sufficient to ensure the safety for the recipient. Most countries have limited or nonexistent waiting periods for donations post vaccination, though some ask their donors to refrain from donating blood for a few weeks after vaccination. Given that vaccine particles are in principle non-replicating, we expect them to decay once in the body, where their concentration gradually drops. The time curve of vaccine particle decay still requires more investigation, as studies observe both circulating spike protein at least two months after vaccination41.
One recommendation of this report is the development of hemovigilance systems to provide summary statistics on blood properties during donor intake. Additionally, the passive monitoring for transfusion related adverse events from vaccinated donors should be addressed in a passive monitoring study whereby donors voluntarily provide their Covid-19 vaccination study on an intake form. Comparisons of vaccinated and unvaccinated blood should be made at two levels, both the properties of the blood itself as well as its interaction with its recipient. Summary statistics on both types of measurements can be calculated to determine if there exist any statistically significant differences between blood products from vaccinated and unvaccinated donors. Reporting of donor’s vaccination status can be done on a voluntary basis, out of respect for medical privacy.
Questions remain as to the safety of transfusions and transplants from vaccinated donors, and this question carries significant implications for national health systems, blood banks and organ transplant pools. A survey of blood parameters, as well as recipient adverse events would require only recording the donor vaccination status, and analysis of such data is straightforward from a statistical perspective. The low cost of such a study, combined with the importance of the questions that it would address is significant motivation to perform such a study. We ask the relevant authorities (blood donation clinics and transplant clinics) to consider adding an optional questionnaire for donors, on whether they have been vaccinated, and the dose schedule and type of vaccination. This presents a completely non-invasive way to address questions of significant public health importance.
Conclusion
Concerns remain over not only primary exposure to vaccine particles via injection, but also of secondary exposure through bodily fluids. Several lines of evidence, including mechanistic understanding, pharmacovigilance, case reports of blood manifestations in vaccine recipients and case reports of autopsies from vaccinated donors suggest that it may be a possibility. Persistence of vaccine contents and/or their expression products has been observed in blood40,41 and breast milk279. Additionally, there are adverse event reports which support bodily fluids exposure (via blood transfusion or breastfeeding) as an aetiological factor.
Further support is given by the comparatively high rate of thrombotic complications in organ donation recipients from donors deceased due to VITT, which appears higher than rates of thrombotic complications in people dying of comparable cause, only not vaccine related. The rate of thrombotic complications for the case of vaccinated donors deceased due to VITT is 30% (Table 2), whereas a pre-Covid-19 vaccine study observed a rate of thrombotic complications of 3% in recipients of liver grafts from donors deceased due to cardiovascular complications, including stroke324. While different studies have found a variety of rates for thrombotic complications, the rates of thrombotic complications in recipients of organ transplants from VITT donors (30%, Table 2) are higher than most comparable historical rates of thrombotic complications in recipients of organ transplants from DCD donors 324,326,328. One study’s reported rates327 (33%) were similar to our reported rates of thrombotic complication(30%, Table 2).
Future monitoring is important for maintaining transfusion safety, as well as the safety of breastfeeding. At this point, harms cannot be definitively ruled out and the question deserves more attention. Given these concerns, blood donors should consider refraining from donation until more information is published on the safety of blood from vaccinated donors.
Ethics approval and informed consent
This article is based on published data. No ethical approval is required.
Consent for Publication
All figures are original productions and do not require approval.
Data Availability
The datasets studied in this article are available at their respective citations.
Acknowledgements
We thank the donors to the World Council for Health for enabling this research. We thank those who support this work and enable us to curate this information. We thank Pierre Kory for his pioneering work in this regard. We thank Cristof Plothe for comments and suggestions about improvement in transfusion.
Competing Interests
Non-financial competing interests M.T.J.H. is a member of the World Council for Health.
Abbreviations
| AE: adverse events |
| CDC: Centers for Disease Control (USA) |
| HLA: human leukocyte antigen |
| IFR: Infection Fatality Rate |
| VAERS: Vaccine adverse event reporting system |
| VITT: vaccine-induced thrombosis and thrombocytopenia |
| WHO: World Health Organization |
References
- Lei Y, Zhang J, Schiavon CR, et al. SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE 2. Circulation Research. 2021;128(9):1323-1326. [CrossRef]
- Stenmark KR, Frid MG, Gerasimovskaya E, et al. Mechanisms of SARS-CoV-2-induced lung vascular disease: potential role of complement. Pulm Circ. 2021;11(2):20458940211015799. [CrossRef]
- Aid M, Busman-Sahay K, Vidal SJ, et al. Vascular Disease and Thrombosis in SARS-CoV-2-Infected Rhesus Macaques. Cell. 2020;183(5):1354-1366.e13. [CrossRef]
- Teuwen LA, Geldhof V, Pasut A, Carmeliet P. COVID-19: the vasculature unleashed. Nat Rev Immunol. 2020;20(7):389-391. [CrossRef]
- Elsoukkary SS, Mostyka M, Dillard A, et al. Autopsy Findings in 32 Patients with COVID-19: A Single-Institution Experience. Pathobiology. 2021;88(1):56-68. [CrossRef]
- Yao XH, Luo T, Shi Y, et al. A cohort autopsy study defines COVID-19 systemic pathogenesis. Cell Res. 2021;31(8):836-846. [CrossRef]
- Hanley B, Lucas SB, Youd E, Swift B, Osborn M. Autopsy in suspected COVID-19 cases. Journal of Clinical Pathology. 2020;73(5):239-242. [CrossRef]
- Stillfried S von, Bülow RD, Röhrig R, et al. First report from the German COVID-19 autopsy registry. The Lancet Regional Health – Europe. 2022;15. [CrossRef]
- Ducloyer M, Gaborit B, Toquet C, et al. Complete post-mortem data in a fatal case of COVID-19: clinical, radiological and pathological correlations. Int J Legal Med. 2020;134(6):2209-2214. [CrossRef]
- Ghasemiyeh P, Mohammadi-Samani S, Firouzabadi N, Dehshahri A, Vazin A. A focused review on technologies, mechanisms, safety, and efficacy of available COVID-19 vaccines. International Immunopharmacology. 2021;100:108162. [CrossRef]
- Francis AI, Ghany S, Gilkes T, Umakanthan S. Review of COVID-19 vaccine subtypes, efficacy and geographical distributions. Postgraduate Medical Journal. 2022;98(1159):389-394. [CrossRef]
- Tobaiqy M, Elkout H, MacLure K. Analysis of Thrombotic Adverse Reactions of COVID-19 AstraZeneca Vaccine Reported to EudraVigilance Database. Vaccines. 2021;9(4):393. [CrossRef]
- Wise J. Covid-19: Rare immune response may cause clots after AstraZeneca vaccine, say researchers. BMJ. 2021;373:n954. [CrossRef]
- Geeraerts T, Montastruc F, Bonneville F, Mémier V, Raposo N. Oxford-AstraZeneca COVID-19 vaccine-induced cerebral venous thrombosis and thrombocytopaenia: A missed opportunity for a rapid return of experience. Anaesth Crit Care Pain Med. 2021;40(4):100889. [CrossRef]
- WHO statement on AstraZeneca COVID-19 vaccine safety signals. Accessed December 7, 2022. https://www.who.int/news/item/17-03-2021-who-statement-on-astrazeneca-covid-19-vaccine-safety-signals.
- Shay DK. Safety Monitoring of the Janssen (Johnson & Johnson) COVID-19 Vaccine — United States, March–April 2021. MMWR Morb Mortal Wkly Rep. 2021;70. [CrossRef]
- Mahase E. Covid-19: Unusual blood clots are “very rare side effect” of Janssen vaccine, says EMA. BMJ. 2021;373:n1046. [CrossRef]
- Malik B, Kalantary A, Rikabi K, Kunadi A. Pulmonary embolism, transient ischaemic attack and thrombocytopenia after the Johnson & Johnson COVID-19 vaccine. BMJ Case Reports CP. 2021;14(7):e243975. [CrossRef]
- Mahase E. Covid-19: US suspends Johnson and Johnson vaccine rollout over blood clots. BMJ. 2021;373:n970. [CrossRef]
- Tobaiqy M, MacLure K, Elkout H, Stewart D. Thrombotic Adverse Events Reported for Moderna, Pfizer and Oxford-AstraZeneca COVID-19 Vaccines: Comparison of Occurrence and Clinical Outcomes in the EudraVigilance Database. Vaccines. 2021;9(11):1326. [CrossRef]
- Vaccination against covid-19. Accessed October 1, 2022. https://www.sst.dk/en/english/corona-eng/vaccination-against-covid-19.
- Alawed AA. Evaluation of Platelet and D.dimer among covid-19 Vaccinated Individuals in Shandi Town. Thesis. Elfatih Mohammed Abdallah; 2022. Accessed December 4, 2022. http://localhost:8080/xmlui/handle/123456789/1306.
- Mahmoud MAK, Khudhair N. Comparison of Complete Blood Counts between four Groups: a COVID-19 Patient, a Healthy and Healthy Vaccine Recipient, and Patient Vaccinated Recipients in Anbar Province. HIV Nursing. 2022;22(2):1988-1994.
- Ltd TIS. JPAC - Transfusion Guidelines. Accessed December 7, 2022. https://transfusionguidelines.org.uk/.
- Info about COVID-19 vaccines and blood donation. Accessed December 7, 2022. https://www.blood.ca/en/covid19/vaccines-and-blood-donation.
- EBMT COVID Vaccine Information.; 2022. https://www.ebmt.org/sites/default/files/2022-01/COVID%20vaccines%20version%208.3%20-%202022-01-03.pdf.
- Avolio E, Carrabba M, Milligan R, et al. The SARS-CoV-2 Spike protein disrupts human cardiac pericytes function through CD147 receptor-mediated signalling: a potential non-infective mechanism of COVID-19 microvascular disease. Clin Sci (Lond). 2021;135(24):2667-2689. [CrossRef]
- Trougakos IP, Terpos E, Alexopoulos H, et al. Adverse effects of COVID-19 mRNA vaccines: the spike hypothesis. Trends Mol Med. 2022;28(7):542-554. [CrossRef]
- Cosentino M, Marino F. Understanding the Pharmacology of COVID-19 mRNA Vaccines: Playing Dice with the Spike? International Journal of Molecular Sciences. 2022;23(18):10881. [CrossRef]
- Muir KL, Kallam A, Koepsell SA, Gundabolu K. Thrombotic Thrombocytopenia after Ad26.COV2.S Vaccination. New England Journal of Medicine. 2021;384(20):1964-1965. [CrossRef]
- Vogel G, Kupferschmidt K. New problems erode confidence in AstraZeneca’s vaccine. Science. 2021;371(6536):1294-1295. [CrossRef]
- See I, Su JR, Lale A, et al. US Case Reports of Cerebral Venous Sinus Thrombosis With Thrombocytopenia After Ad26.COV2.S Vaccination, March 2 to April 21, 2021. JAMA. 2021;325(24):2448-2456. [CrossRef]
- Karlstad Ø, Hovi P, Husby A, et al. SARS-CoV-2 Vaccination and Myocarditis in a Nordic Cohort Study of 23 Million Residents. JAMA Cardiology. 2022;7(6):600-612. [CrossRef]
- Hsieh YL, Rak S, SteelFisher GK, Bauhoff S. Effect of the suspension of the J&J COVID-19 vaccine on vaccine hesitancy in the United States. Vaccine. 2022;40(3):424-427. [CrossRef]
- Paterlini M. Covid-19: Sweden, Norway, and Finland suspend use of Moderna vaccine in young people “as a precaution.” BMJ. 2021;375:n2477. [CrossRef]
- De Michele M, Kahan J, Berto I, et al. Cerebrovascular Complications of COVID-19 and COVID-19 Vaccination. Circ Res. 2022;130(8):1187-1203. [CrossRef]
- McGonagle D, De Marco G, Bridgewood C. Mechanisms of Immunothrombosis in Vaccine-Induced Thrombotic Thrombocytopenia (VITT) Compared to Natural SARS-CoV-2 Infection. Journal of Autoimmunity. 2021;121:102662. [CrossRef]
- Lindsay KE, Bhosle SM, Zurla C, et al. Visualization of early events in mRNA vaccine delivery in non-human primates via PET–CT and near-infrared imaging. Nat Biomed Eng. 2019;3(5):371-380. [CrossRef]
- Spike Protein Behavior. Accessed October 1, 2022. https://www.science.org/content/blog-post/spike-protein-behavior.
- Röltgen K, Nielsen SCA, Silva O, et al. Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination. Cell. 2022;185(6):1025-1040.e14. [CrossRef]
- Bansal S, Perincheri S, Fleming T, et al. Cutting Edge: Circulating Exosomes with COVID Spike Protein Are Induced by BNT162b2 (Pfizer–BioNTech) Vaccination prior to Development of Antibodies: A Novel Mechanism for Immune Activation by mRNA Vaccines. The Journal of Immunology. 2021;207(10):2405-2410. [CrossRef]
- Jaramillo C. Red Cross Accepts Blood Donations From People Vaccinated Against COVID-19. FactCheck.org. Published April 27, 2022. Accessed December 11, 2022. https://www.factcheck.org/2022/04/scicheck-red-cross-accepts-and-uses-blood-donations-from-people-vaccinated-against-covid-19/.
- Ogata AF, Cheng CA, Desjardins M, et al. Circulating Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients. Clinical Infectious Diseases. 2022;74(4):715-718. [CrossRef]
- Montague SJ, Smith CW, Lodwick CS, et al. Anti-platelet factor 4 immunoglobulin G levels in vaccine-induced immune thrombocytopenia and thrombosis: Persistent positivity through 7 months. Res Pract Thromb Haemost. 2022;6(3):e12707. [CrossRef]
- Sørvoll IH, Horvei KD, Ernstsen SL, et al. An observational study to identify the prevalence of thrombocytopenia and anti-PF4/polyanion antibodies in Norwegian health care workers after COVID-19 vaccination. J Thromb Haemost. 2021;19(7):1813-1818. [CrossRef]
- Panagiota V, Dobbelstein C, Werwitzke S, et al. Long-Term Outcomes after Vaccine-Induced Thrombotic Thrombocytopenia. Viruses. 2022;14(8):1702. [CrossRef]
- Al-Samkari H, Leaf RK, Goodarzi K. Transient Thrombocytopenia With Glycoprotein-Specific Platelet Autoantibodies After Ad26.COV2.S Vaccination: A Case Report. Ann Intern Med. 2021;174(11):1632-1633. [CrossRef]
- Vayne C, Rollin J, Gruel Y, et al. PF4 Immunoassays in Vaccine-Induced Thrombotic Thrombocytopenia. New England Journal of Medicine. 2021;385(4):376-378. [CrossRef]
- Schönborn L, Thiele T, Kaderali L, et al. Most anti-PF4 antibodies in vaccine-induced immune thrombotic thrombocytopenia are transient. Blood. 2022;139(12):1903-1907. [CrossRef]
- Gerotziafas GT, Elalamy I, Lecrubier C, et al. The role of platelet factor 4 in platelet aggregation induced by the antibodies implicated in heparin-induced thrombocytopenia. Blood Coagul Fibrinolysis. 2001;12(7):511-520. [CrossRef]
- Warkentin TE. Platelet-activating anti-PF4 disorders: An overview. Semin Hematol. 2022;59(2):59-71. [CrossRef]
- Vaccine Adverse Event Reporting System (VAERS). Accessed December 7, 2022. https://vaers.hhs.gov/.
- CDC. Enroll in v-safe after vaccination health checker. Centers for Disease Control and Prevention. Published November 14, 2022. Accessed December 7, 2022. https://www.cdc.gov/vaccinesafety/ensuringsafety/monitoring/v-safe/index.html.
- Coronavirus vaccine - summary of Yellow Card reporting. GOV.UK. Accessed December 7, 2022. https://www.gov.uk/government/publications/coronavirus-covid-19-vaccine-adverse-reactions/coronavirus-vaccine-summary-of-yellow-card-reporting.
- EMA. EudraVigilance system overview. European Medicines Agency. Published September 17, 2018. Accessed December 7, 2022. https://www.ema.europa.eu/en/human-regulatory/research-development/pharmacovigilance/eudravigilance/eudravigilance-system-overview.
- Centre UM. VigiBase Services. Accessed December 7, 2022. https://who-umc.org/vigibase/vigibase-services/.
- Ceacareanu AC, Wintrob ZAP. Summary of COVID-19 Vaccine-Related Reports in the Vaccine Adverse Event Reporting System. J Res Pharm Pract. 2021;10(3):107-113. [CrossRef]
- Parmar K, Subramanyam S, Del Rio-Pertuz G, Sethi P, Argueta-Sosa E. Cardiac Adverse Events after Vaccination—A Systematic Review. Vaccines. 2022;10(5):700. [CrossRef]
- Jeet Kaur R, Dutta S, Charan J, et al. Cardiovascular Adverse Events Reported from COVID-19 Vaccines: A Study Based on WHO Database. Int J Gen Med. 2021;14:3909-3927. [CrossRef]
- Hajjo R, Sabbah DA, Bardaweel SK, Tropsha A. Shedding the Light on Post-Vaccine Myocarditis and Pericarditis in COVID-19 and Non-COVID-19 Vaccine Recipients. Vaccines. 2021;9(10):1186. [CrossRef]
- Welsh KJ, Baumblatt J, Chege W, Goud R, Nair N. Thrombocytopenia including immune thrombocytopenia after receipt of mRNA COVID-19 vaccines reported to the Vaccine Adverse Event Reporting System (VAERS). Vaccine. 2021;39(25):3329-3332. [CrossRef]
- Yan MM, Zhao H, Li ZR, et al. Serious adverse reaction associated with the COVID-19 vaccines of BNT162b2, Ad26.COV2.S, and mRNA-1273: Gaining insight through the VAERS. Front Pharmacol. 2022;13:921760. [CrossRef]
- Abrams CS, Barnes GD. SARS-CoV-2 Vaccination-Induced Thrombotic Thrombocytopenia: A Rare But Serious Immunologic Complication. Annual Review of Medicine. 2023;74(1):null. [CrossRef]
- Al-Maqbali JS, Rasbi SA, Kashoub MS, et al. A 59-Year-Old Woman with Extensive Deep Vein Thrombosis and Pulmonary Thromboembolism 7 Days Following a First Dose of the Pfizer-BioNTech BNT162b2 mRNA COVID-19 Vaccine. Am J Case Rep. 2021;22:e932946-1-e932946-4. [CrossRef]
- Wiest NE, Johns GS, Edwards E. A Case of Acute Pulmonary Embolus after mRNA SARS-CoV-2 Immunization. Vaccines. 2021;9(8):903. [CrossRef]
- Fazio S, Vaccariello M, Affuso F. A Case of Adverse Reaction to Booster Dose of COVID-19 Vaccination: Could D-Dimer Elevation Suggest Increased Clotting Risk? Health. 2022;14(2):204-208. [CrossRef]
- Malayala SV, Papudesi BN, Sharma R, Vusqa UT, Raza A. A Case of Idiopathic Thrombocytopenic Purpura After Booster Dose of BNT162b2 (Pfizer-Biontech) COVID-19 Vaccine. Cureus. 2021;13(10). [CrossRef]
- van Dijk MMH, Veldman HD, Aarts F, Barten DG, van den Bergh JP, Dielis AWJH. A case of unusual mild clinical presentation of COVID-19 vaccine-induced immune thrombotic thrombocytopenia with splanchnic vein thrombosis. Ann Hepatol. 2022;27(1):100590. [CrossRef]
- Lee CSM, Liang HPH, Connor DE, et al. A novel flow cytometry procoagulant assay for diagnosis of vaccine-induced immune thrombotic thrombocytopenia. Blood Adv. 2022;6(11):3494-3506. [CrossRef]
- Agbariah N, Bütler VA, Wieland A, Andina N, Hammann F, Kremer Hovinga JA. Acquired immune-mediated thrombotic thrombocytopenic pur-pura (iTTP) following mRNA-based COVID-19 vaccination (BNT162b2). Swiss Medical Weekly. Published online 2021:20S-20S.
- Ruhe J, Schnetzke U, Kentouche K, et al. Acquired thrombotic thrombocytopenic purpura after first vaccination dose of BNT162b2 mRNA COVID-19 vaccine. Ann Hematol. 2022;101(3):717-719. [CrossRef]
- Yoshida K, Sakaki A, Matsuyama Y, et al. Acquired Thrombotic Thrombocytopenic Purpura Following BNT162b2 mRNA Coronavirus Disease Vaccination in a Japanese Patient. Internal Medicine. 2022;61(3):407-412. [CrossRef]
- Ben Saida I, Maatouk I, Toumi R, et al. Acquired Thrombotic Thrombocytopenic Purpura Following Inactivated COVID-19 Vaccines: Two Case Reports and a Short Literature Review. Vaccines (Basel). 2022;10(7):1012. [CrossRef]
- McFadyen JD, Sharma P, Moon MJ, et al. Activation of circulating platelets in vaccine-induced thrombotic thrombocytopenia and its reversal by intravenous immunoglobulin. British Journal of Haematology. 2022;196(1):234-237. [CrossRef]
- Sung PS, Oh JS, Choi J. Acute Budd-Chiari syndrome with thrombotic thrombocytopenia after BNT162b2 mRNA vaccination. Liver Int. 2022;42(6):1447-1448. [CrossRef]
- Tajstra M, Jaroszewicz J, Gąsior M. Acute Coronary Tree Thrombosis After Vaccination for COVID-19. JACC: Cardiovascular Interventions. 2021;14(9):e103-e104. [CrossRef]
- Walter U, Fuchs M, Grossmann A, et al. Adenovirus-Vectored COVID-19 Vaccine–Induced Immune Thrombosis of Carotid Artery: A Case Report. Neurology. 2021;97(15):716-719. [CrossRef]
- Kolahchi Z, Khanmirzaei M, Mowla A. Acute ischemic stroke and vaccine-induced immune thrombotic thrombocytopenia post COVID-19 vaccination; a systematic review. J Neurol Sci. 2022;439:120327. [CrossRef]
- Costentin G, Ozkul-Wermester O, Triquenot A, et al. Acute Ischemic Stroke Revealing ChAdOx1 nCov-19 Vaccine-Induced Immune Thrombotic Thrombocytopenia: Impact on Recanalization Strategy. J Stroke Cerebrovasc Dis. 2021;30(9):105942. [CrossRef]
- Chen PW, Tsai ZY, Chao TH, Li YH, Hou CJY, Liu PY. Addressing Vaccine-Induced Immune Thrombotic Thrombocytopenia (VITT) Following COVID-19 Vaccination: A Mini-Review of Practical Strategies. Acta Cardiol Sin. 2021;37(4):355-364. [CrossRef]
- Lioudaki S, Kontopodis N, Pontikoglou C, et al. Multiple Sites of Arterial Thrombosis in A 35-Year Old Patient after ChAdOx1 (AstraZeneca) Vaccination, Requiring Emergent Femoral and Carotid Surgical Thrombectomy. Annals of Vascular Surgery. 2022;79:438.e1-438.e4. [CrossRef]
- Islam A, Bashir MS, Joyce K, Rashid H, Laher I, Elshazly S. An Update on COVID-19 Vaccine Induced Thrombotic Thrombocytopenia Syndrome and Some Management Recommendations. Molecules. 2021;26(16):5004. [CrossRef]
- Ahmed SH, Shaikh TG, Waseem S, Qadir NA, Yousaf Z, Ullah I. Vaccine-induced thrombotic thrombocytopenia following coronavirus vaccine: A narrative review. Annals of Medicine and Surgery. 2022;73:102988. [CrossRef]
- Bourguignon A, Arnold DM, Warkentin TE, et al. Adjunct Immune Globulin for Vaccine-Induced Immune Thrombotic Thrombocytopenia. New England Journal of Medicine. 2021;385(8):720-728. [CrossRef]
- Huynh A, Kelton JG, Arnold DM, Daka M, Nazy I. Antibody epitopes in vaccine-induced immune thrombotic thrombocytopaenia. Nature. 2021;596(7873):565-569. [CrossRef]
- Reilly-Stitt C, Kitchen S, Jennings I, et al. Anti-PF4 testing for vaccine-induced immune thrombocytopenia and thrombosis and heparin induced thrombocytopenia: Results from a UK National External Quality Assessment Scheme exercise April 2021. Journal of Thrombosis and Haemostasis. 2021;19(9):2263-2267. [CrossRef]
- Marcucci R, Marietta M. Vaccine-induced thrombotic thrombocytopenia: the elusive link between thrombosis and adenovirus-based SARS-CoV-2 vaccines. Intern Emerg Med. 2021;16(5):1113-1119. [CrossRef]
- Mancuso M, Lauretti DL, Cecconi N, et al. Arterial intracranial thrombosis as the first manifestation of vaccine-induced immune thrombotic thrombocytopenia (VITT): a case report. Neurol Sci. 2022;43(3):2085-2089. [CrossRef]
- Sessa A, Gattamorta M, Punginelli M, Maggioni G. Arterial Thrombosis in an Unusual Site (Ulnar Artery) after COVID-19 Vaccination—A Case Report. Clinics and Practice. 2022;12(3):237-242. [CrossRef]
- Chen VM, Curnow JL, Tran HA, Choi PY. Australian and New Zealand approach to diagnosis and management of vaccine-induced immune thrombosis and thrombocytopenia. Medical Journal of Australia. 2021;215(6):245. [CrossRef]
- Rodríguez Y, Rojas M, Beltrán S, et al. Autoimmune and autoinflammatory conditions after COVID-19 vaccination. New case reports and updated literature review. J Autoimmun. 2022;132:102898. [CrossRef]
- Gaignard ME, Lieberherr S, Schoenenberger A, Benz R. Autoimmune Hematologic Disorders in Two Patients After mRNA COVID-19 Vaccine. Hemasphere. 2021;5(8):e618. [CrossRef]
- Elrashdy F, Tambuwala MM, Hassan SkS, et al. Autoimmunity roots of the thrombotic events after COVID-19 vaccination. Autoimmunity Reviews. 2021;20(11):102941. [CrossRef]
- Ryan E, Benjamin D, McDonald I, et al. AZD1222 vaccine-related coagulopathy and thrombocytopenia without thrombosis in a young female. Br J Haematol. 2021;194(3):553-556. [CrossRef]
- Waqar U, Ahmed S, Gardezi SMHA, et al. Thrombosis with Thrombocytopenia Syndrome After Administration of AZD1222 or Ad26.COV2.S Vaccine for COVID-19: A Systematic Review. Clin Appl Thromb Hemost. 2021;27:10760296211068487. [CrossRef]
- Cari L, Fiore P, Naghavi Alhosseini M, Sava G, Nocentini G. Blood clots and bleeding events following BNT162b2 and ChAdOx1 nCoV-19 vaccine: An analysis of European data. Journal of Autoimmunity. 2021;122:102685. [CrossRef]
- Ihnatko M, Truchla I, Ihnatková L, Prohászka Z, Lazúrová I. Case Report: A Case of COVID Vaccine-Induced Thrombotic Thrombocytopenia Manifested as Pulmonary Embolism and Hemorrhagia. A First Reported Case From Slovakia. Front Med (Lausanne). 2021;8:789972. [CrossRef]
- Braun T, Viard M, Juenemann M, et al. Case Report: Take a Second Look: Covid-19 Vaccination-Related Cerebral Venous Thrombosis and Thrombotic Thrombocytopenia Syndrome. Frontiers in Neurology. 2021;12. Accessed December 4, 2022. https://www.frontiersin.org/articles/10.3389/fneur.2021.763049.
- Su PH, Yu YC, Chen WH, et al. Case Report: Vaccine-Induced Immune Thrombotic Thrombocytopenia in a Pancreatic Cancer Patient After Vaccination With Messenger RNA−1273. Front Med (Lausanne). 2021;8:772424. [CrossRef]
- See I, Lale A, Marquez P, et al. Case Series of Thrombosis With Thrombocytopenia Syndrome After COVID-19 Vaccination—United States, December 2020 to August 2021. Ann Intern Med. 2022;175(4):513-522. [CrossRef]
- Siegler JE, Klein P, Yaghi S, et al. Cerebral Vein Thrombosis With Vaccine-Induced Immune Thrombotic Thrombocytopenia. Stroke. 2021;52(9):3045-3053. [CrossRef]
- Adekoya A, Adelekan-Popoola F, Fabamwo A, et al. Chadox1 Ncov-19 Vaccination: A Clinico-Pathological Review of Coagulation Derangement in Four Cases. 2022;9:11-21. [CrossRef]
- Suresh P, Petchey W. ChAdOx1 nCOV-19 vaccine-induced immune thrombotic thrombocytopenia and cerebral venous sinus thrombosis (CVST). BMJ Case Reports CP. 2021;14(6):e243931. [CrossRef]
- Greinacher A, Schönborn L, Siegerist F, et al. Pathogenesis of vaccine-induced immune thrombotic thrombocytopenia (VITT). Seminars in Hematology. 2022;59(2):97-107. [CrossRef]
- Sánchez van Kammen M, Aguiar de Sousa D, Poli S, et al. Characteristics and Outcomes of Patients With Cerebral Venous Sinus Thrombosis in SARS-CoV-2 Vaccine-Induced Immune Thrombotic Thrombocytopenia. JAMA Neurol. 2021;78(11):1314-1323. [CrossRef]
- Lee AYY, Al Moosawi M, Peterson EA, et al. Clinical care pathway for the evaluation of patients with suspected VITT after ChAdOx1 nCoV-19 vaccination. Blood Adv. 2022;6(11):3315-3320. [CrossRef]
- Rizk JG, Gupta A, Sardar P, et al. Clinical Characteristics and Pharmacological Management of COVID-19 Vaccine-Induced Immune Thrombotic Thrombocytopenia With Cerebral Venous Sinus Thrombosis: A Review. JAMA Cardiol. 2021;6(12):1451-1460. [CrossRef]
- Mungmunpuntipantip R, Wiwanitkit V. COVID-19, neurovascular thrombotic problem and short summary on blood coagulation disorder: a brief review. Egypt J Neurol Psychiatr Neurosurg. 2022;58(1):6. [CrossRef]
- Khan Z, Besis G, Candilio L. COVID-19 Vaccine-Induced Thrombotic Thrombocytopaenia With Venous and Arterial Thrombosis: A Case Report. Cureus. 2022;14(8):e28535. [CrossRef]
- Pishko AM, Bussel JB, Cines DB. COVID-19 vaccination and immune thrombocytopenia. Nat Med. 2021;27(7):1145-1146. [CrossRef]
- Carli G, Nichele I, Ruggeri M, Barra S, Tosetto A. Deep vein thrombosis (DVT) occurring shortly after the second dose of mRNA SARS-CoV-2 vaccine. Intern Emerg Med. 2021;16(3):803-804. [CrossRef]
- Ledford H. COVID vaccines and blood clots: five key questions. Nature. 2021;592(7855):495-496. [CrossRef]
- Greinacher A. COVID vaccine-induced immune thrombotic thrombocytopenia: Rare but relevant. Eur J Intern Med. 2022;105:20-22. [CrossRef]
- Lai CC, Ko WC, Chen CJ, et al. COVID-19 vaccines and thrombosis with thrombocytopenia syndrome. Expert Rev Vaccines. 2021;20(8):1027-1035. [CrossRef]
- Pavord S, Scully M, Hunt BJ, et al. Clinical Features of Vaccine-Induced Immune Thrombocytopenia and Thrombosis. New England Journal of Medicine. 2021;385(18):1680-1689. [CrossRef]
- Alam W. COVID-19 vaccine-induced immune thrombotic thrombocytopenia: A review of the potential mechanisms and proposed management. Sci Prog. 2021;104(2):368504211025927. [CrossRef]
- Deucher W, Sukumar S, Cataland SR. Clinical relapse of immune-mediated thrombotic thrombocytopenic purpura following COVID-19 vaccination. Research and Practice in Thrombosis and Haemostasis. 2022;6(1):e12658. [CrossRef]
- Scully M, Singh D, Lown R, et al. Pathologic Antibodies to Platelet Factor 4 after ChAdOx1 nCoV-19 Vaccination. N Engl J Med. 2021;384(23):2202-2211. [CrossRef]
- Hwang J, Han YJ, Yon DK, et al. Clinical significance of hepatosplenic thrombosis in vaccine-induced immune thrombotic thrombocytopenia after ChAdOx1 nCoV-19 vaccination. International Journal of Infectious Diseases. 2022;116:114-121. [CrossRef]
- Günther A, Brämer D, Pletz MW, et al. Complicated Long Term Vaccine Induced Thrombotic Immune Thrombocytopenia-A Case Report. Vaccines (Basel). 2021;9(11):1344. [CrossRef]
- Mekheal EM, Millet C, Mekheal N, Ghrewati M, Mechineni A, Maroules M. Coincidental or causal? A case report of acquired thrombotic thrombocytopenic purpura following mRNA-1273 Covid-19 vaccination. Hematology, Transfusion and Cell Therapy. Published online November 28, 2022. [CrossRef]
- Gan G, Liu H, Liang Z, Zhang G, Liu X, Ma L. Vaccine-associated thrombocytopenia. Thromb Res. 2022;220:12-20. [CrossRef]
- Alsmady MM, Al-Qaryouti RA, Sultan NG, Khrais OI, Khrais H. Upper Limb Ischemia Due to Arterial Thrombosis after COVID-19 Vaccination. Case Rep Med. 2022;2022:4819131. [CrossRef]
- Laroche A, Soulet D, Bazin M, et al. Live imaging of platelets and neutrophils during antibody-mediated neurovascular thrombosis. Blood Advances. 2022;6(12):3697-3702. [CrossRef]
- Bandapaati S, Bobba H, Navinan MR. Coeliac artery and splenic artery thrombosis complicated with splenic infarction 7 days following the first dose of Oxford vaccination, causal relationship or coincidence? BMJ Case Reports CP. 2021;14(7):e243799. [CrossRef]
- Chang JC, Hawley HB. Vaccine-Associated Thrombocytopenia and Thrombosis: Venous Endotheliopathy Leading to Venous Combined Micro-Macrothrombosis. Medicina. 2021;57(11):1163. [CrossRef]
- Pavord S, Hunt BJ, Horner D, Bewley S, Karpusheff J. Vaccine induced immune thrombocytopenia and thrombosis: summary of NICE guidance. BMJ. 2021;375:n2195. [CrossRef]
- Yamada S, Asakura H. Coagulopathy and Fibrinolytic Pathophysiology in COVID-19 and SARS-CoV-2 Vaccination. International Journal of Molecular Sciences. 2022;23(6):3338. [CrossRef]
- Abdel-Bakky MS, Amin E, Ewees MG, et al. Coagulation System Activation for Targeting of COVID-19: Insights into Anticoagulants, Vaccine-Loaded Nanoparticles, and Hypercoagulability in COVID-19 Vaccines. Viruses. 2022;14(2):228. [CrossRef]
- Franchini M, Liumbruno GM, Pezzo M. COVID-19 vaccine-associated immune thrombosis and thrombocytopenia (VITT): Diagnostic and therapeutic recommendations for a new syndrome. European Journal of Haematology. 2021;107(2):173-180. [CrossRef]
- Thachil J. COVID-19 Vaccine-Induced Immune Thrombosis with Thrombocytopenia (VITT) and the Shades of Grey in Thrombus Formation. Semin Thromb Hemost. 2022;48(1):15-18. [CrossRef]
- Thaler J, Jilma P, Samadi N, et al. Long-term follow-up after successful treatment of vaccine-induced prothrombotic immune thrombocytopenia. Thrombosis Research. 2021;207:126-130. [CrossRef]
- Abrignani MG, Murrone A, De Luca L, et al. COVID-19, Vaccines, and Thrombotic Events: A Narrative Review. J Clin Med. 2022;11(4):948. [CrossRef]
- Danish F i A, Rabani AE, Subhani F e R, Yasmin S, Koul SS. COVID-19: Vaccine-induced immune thrombotic thrombocytopenia. European Journal of Haematology. 2022;109(6):619-632. [CrossRef]
- Napoli R, Visonà E. Deep vein thrombosis and acute hepatitis after ChAdOx1 nCov-19 vaccination in a Charcot-Marie-Tooth patient: a case report. Clin Exp Vaccine Res. 2022;11(3):294-297. [CrossRef]
- Mouta Nunes de Oliveira P, Mendes-de-Almeida DP, Bertollo Gomes Porto V, et al. Vaccine-induced immune thrombotic thrombocytopenia after COVID-19 vaccination: Description of a series of 39 cases in Brazil. Vaccine. 2022;40(33):4788-4795. [CrossRef]
- Herrera-Comoglio R, Lane S. Vaccine-Induced Immune Thrombocytopenia and Thrombosis after the Sputnik V Vaccine. New England Journal of Medicine. 2022;387(15):1431-1432. [CrossRef]
- Dotan A, Shoenfeld Y. Perspectives on vaccine induced thrombotic thrombocytopenia. Journal of Autoimmunity. 2021;121:102663. [CrossRef]
- Lavin M, Elder PT, O’Keeffe D, et al. Vaccine-induced immune thrombotic thrombocytopenia (VITT) – a novel clinico-pathological entity with heterogeneous clinical presentations. British Journal of Haematology. 2021;195(1):76-84. [CrossRef]
- Hrastelj J, Robertson NP. Vaccine-induced immune thrombosis and thrombocytopaenia: incidence, mechanism and treatment. J Neurol. 2021;268(11):4396-4397. [CrossRef]
- De Michele M, Iacobucci M, Chistolini A, et al. Malignant cerebral infarction after ChAdOx1 nCov-19 vaccination: a catastrophic variant of vaccine-induced immune thrombotic thrombocytopenia. Nat Commun. 2021;12(1):4663. [CrossRef]
- Smadja DM, Yue QY, Chocron R, Sanchez O, Louet ALL. Vaccination against COVID-19: insight from arterial and venous thrombosis occurrence using data from VigiBase. European Respiratory Journal. 2021;58(1). [CrossRef]
- Atoui A, Jarrah K, Al Mahmasani L, Bou-Fakhredin R, Taher AT. Deep venous thrombosis and pulmonary embolism after COVID-19 mRNA vaccination. Ann Hematol. 2022;101(5):1111-1113. [CrossRef]
- Wiedmann M, Skattør T, Stray-Pedersen A, et al. Vaccine Induced Immune Thrombotic Thrombocytopenia Causing a Severe Form of Cerebral Venous Thrombosis With High Fatality Rate: A Case Series. Frontiers in Neurology. 2021;12. Accessed December 4, 2022. https://www.frontiersin.org/articles/10.3389/fneur.2021.721146.
- Bérezné A, Bougon D, Blanc-Jouvan F, et al. Deterioration of vaccine-induced immune thrombotic thrombocytopenia treated by heparin and platelet transfusion: Insight from functional cytometry and serotonin release assay. Research and Practice in Thrombosis and Haemostasis. 2021;5(6):e12572. [CrossRef]
- Furie KL, Cushman M, Elkind MSV, Lyden PD, Saposnik G, null null. Diagnosis and Management of Cerebral Venous Sinus Thrombosis With Vaccine-Induced Immune Thrombotic Thrombocytopenia. Stroke. 2021;52(7):2478-2482. [CrossRef]
- Pai M, Grill A, Ivers N, et al. Vaccine Induced Prothrombotic Immune Thrombocytopenia (VIPIT) Following AstraZeneca COVID-19 Vaccination. Ontario COVID-19 Science Advisory Table; 2021. [CrossRef]
- Oldenburg J, Klamroth R, Langer F, et al. Diagnosis and Management of Vaccine-Related Thrombosis following AstraZeneca COVID-19 Vaccination: Guidance Statement from the GTH. Hamostaseologie. 2021;41(3):184-189. [CrossRef]
- Long B, Bridwell R, Gottlieb M. Thrombosis with thrombocytopenia syndrome associated with COVID-19 vaccines. The American Journal of Emergency Medicine. 2021;49:58-61. [CrossRef]
- Ceschia N, Scheggi V, Gori AM, et al. Diffuse prothrombotic syndrome after ChAdOx1 nCoV-19 vaccine administration: a case report. J Med Case Reports. 2021;15(1):496. [CrossRef]
- Klok FA, Pai M, Huisman MV, Makris M. Vaccine-induced immune thrombotic thrombocytopenia. Lancet Haematol. 2022;9(1):e73-e80. [CrossRef]
- Pai M. Epidemiology of VITT. Seminars in Hematology. 2022;59(2):72-75. [CrossRef]
- Brazete C, Aguiar A, Furtado I, Duarte R. Thrombotic events and COVID-19 vaccines. The International Journal of Tuberculosis and Lung Disease. 2021;25(9):701-707. [CrossRef]
- Berlot G, Tomasini A, La Fata C, Pintacuda S, Rigutti S, Falanga A. Widespread Arterial Thrombosis after ChAdOx1 nCov-19 Vaccination. Case Reports in Critical Care. 2022;2022:e6804456. [CrossRef]
- Taylor P, Allen L, Shrikrishnapalasuriyar N, Stechman M, Rees A. Vaccine-induced thrombosis and thrombocytopenia with bilateral adrenal haemorrhage. Clin Endocrinol (Oxf). 2022;97(1):26-27. [CrossRef]
- Makris M, Pavord S, Lester W, Scully M, Hunt B. Vaccine-induced Immune Thrombocytopenia and Thrombosis (VITT). Res Pract Thromb Haemost. 2021;5(5):e12529. [CrossRef]
- Guditi S, Setty G, Verma M, et al. Vaccine-Induced Thrombotic Thrombocytopenia Due to Coronavirus Disease 2019 Vaccine From a Deceased Donor: A Case Report. Transplant Proc. 2022;54(6):1534-1538. [CrossRef]
- Salih F, Schönborn L, Kohler S, et al. Vaccine-Induced Thrombocytopenia with Severe Headache. New England Journal of Medicine. 2021;385(22):2103-2105. [CrossRef]
- Lai CMB, Lee AYY, Parkin SBI. Vaccine-induced prothrombotic immune thrombocytopenia without thrombosis may not require immune modulatory therapy: A case report. Research and Practice in Thrombosis and Haemostasis. 2022;6(4):e12716. [CrossRef]
- Al Rawahi B, BaTaher H, Jaffer Z, Al-Balushi A, Al-Mazrouqi A, Al-Balushi N. Vaccine-induced immune thrombotic thrombocytopenia following AstraZeneca (ChAdOx1 nCOV19) vaccine–A case report. Research and Practice in Thrombosis and Haemostasis. 2021;5(6):e12578. [CrossRef]
- Dalan R, Boehm BO. Thrombosis post COVID-19 vaccinations: Potential link to ACE pathways. Thrombosis Research. 2021;206:137-138. [CrossRef]
- Sachs UJ, Cooper N, Czwalinna A, et al. PF4-Dependent Immunoassays in Patients with Vaccine-Induced Immune Thrombotic Thrombocytopenia: Results of an Interlaboratory Comparison. Thromb Haemost. 2021;121(12):1622-1627. [CrossRef]
- Curcio R, Gandolfo V, Alcidi R, et al. Vaccine-induced massive pulmonary embolism and thrombocytopenia following a single dose of Janssen Ad26.COV2.S vaccination. International Journal of Infectious Diseases. 2022;116:154-156. [CrossRef]
- Aladdin Y, Algahtani H, Shirah B. Vaccine-Induced Immune Thrombotic Thrombocytopenia with Disseminated Intravascular Coagulation and Death following the ChAdOx1 nCoV-19 Vaccine. Journal of Stroke and Cerebrovascular Diseases. 2021;30(9):105938. [CrossRef]
- Charidimou A, Samudrala S, Cervantes-Arslanian AM, Sloan JM, Dasenbrock HH, Daneshmand A. Vaccine-Induced Immune Thrombotic Thrombocytopenia with Concurrent Arterial and Venous Thrombi Following Ad26.COV2.S Vaccination. Journal of Stroke and Cerebrovascular Diseases. 2021;30(12). [CrossRef]
- Connors JM, Iba T. Vaccine-induced immune thrombotic thrombocytopenia and patients with cancer. Thrombosis Research. 2022;213:S77-S83. [CrossRef]
- Sharifian-Dorche M, Bahmanyar M, Sharifian-Dorche A, Mohammadi P, Nomovi M, Mowla A. Vaccine-induced immune thrombotic thrombocytopenia and cerebral venous sinus thrombosis post COVID-19 vaccination; a systematic review. Journal of the Neurological Sciences. 2021;428:117607. [CrossRef]
- Mohseni Afshar Z, Babazadeh A, Janbakhsh A, et al. Vaccine-induced immune thrombotic thrombocytopenia after vaccination against Covid-19: A clinical dilemma for clinicians and patients. Reviews in Medical Virology. 2022;32(2):e2273. [CrossRef]
- Warkentin TE, Pai M. The Epidemiology of Thrombosis With Thrombocytopenia Syndrome: Analogies With Heparin-Induced Thrombocytopenia. Ann Intern Med. 2022;175(4):604-605. [CrossRef]
- Kuter DJ. Exacerbation of immune thrombocytopenia following COVID-19 vaccination. British Journal of Haematology. 2021;195(3):365-370. [CrossRef]
- Graça LL, Amaral MJ, Serôdio M, Costa B. Extensive thrombosis after COVID-19 vaccine: cause or coincidence? BMJ Case Reports CP. 2021;14(8):e244878. [CrossRef]
- Gresele P, Marietta M, Ageno W, et al. Management of cerebral and splanchnic vein thrombosis associated with thrombocytopenia in subjects previously vaccinated with Vaxzevria (AstraZeneca): a position statement from the Italian Society for the Study of Haemostasis and Thrombosis (SISET). Blood Transfus. 2021;19(4):281-283. [CrossRef]
- Toom S, Wolf B, Avula A, Peeke S, Becker K. Familial thrombocytopenia flare-up following the first dose of mRNA-1273 Covid-19 vaccine. Am J Hematol. 2021;96(5):E134-E135. [CrossRef]
- de Bruijn S, Maes MB, De Waele L, Vanhoorelbeke K, Gadisseur A. First report of a de novo iTTP episode associated with an mRNA-based anti-COVID-19 vaccination. Journal of Thrombosis and Haemostasis. 2021;19(8):2014-2018. [CrossRef]
- Lee E, Cines DB, Gernsheimer T, et al. Thrombocytopenia following Pfizer and Moderna SARS-CoV-2 vaccination. Am J Hematol. 2021;96(5):534-537. [CrossRef]
- Marietta M, Coluccio V, Luppi M. Potential mechanisms of vaccine-induced thrombosis. Eur J Intern Med. 2022;105:1-7. [CrossRef]
- Anderson A, Seddon M, Shahzad K, Lunevicius R. Post-COVID-19 vaccination occurrence of splenic infarction due to arterial thrombosis. BMJ Case Reports CP. 2021;14(12):e243846. [CrossRef]
- Sangli S, Virani A, Cheronis N, et al. Thrombosis With Thrombocytopenia After the Messenger RNA–1273 Vaccine. Ann Intern Med. 2021;174(10):1480-1482. [CrossRef]
- Kenda J, Lovrič D, Škerget M, Milivojević N. Treatment of ChAdOx1 nCoV-19 Vaccine-Induced Immune Thrombotic Thrombocytopenia Related Acute Ischemic Stroke. J Stroke Cerebrovasc Dis. 2021;30(11):106072. [CrossRef]
- Othman M, Baker AT, Gupalo E, et al. To clot or not to clot? Ad is the question—Insights on mechanisms related to vaccine-induced thrombotic thrombocytopenia. Journal of Thrombosis and Haemostasis. 2021;19(11):2845-2856. [CrossRef]
- Hosseinzadeh R, Barary M, Mehdinezhad H, Sio TT, Langer F, Khosravi S. Thrombotic thrombocytopenia After Sinopharm BBIBP-CorV COVID-19 vaccination. Research and Practice in Thrombosis and Haemostasis. 2022;6(4):e12750. [CrossRef]
- Gabarin N, Arnold DM, Nazy I, Warkentin TE. Treatment of vaccine-induced immune thrombotic thrombocytopenia (VITT). Semin Hematol. 2022;59(2):89-96. [CrossRef]
- Rzymski P, Perek B, Flisiak R. Thrombotic Thrombocytopenia after COVID-19 Vaccination: In Search of the Underlying Mechanism. Vaccines. 2021;9(6):559. [CrossRef]
- Stoll SE, Werner P, Wetsch WA, et al. Transjugular intrahepatic portosystemic shunt, local thrombaspiration, and lysis for management of fulminant portomesenteric thrombosis and atraumatic splenic rupture due to vector-vaccine-induced thrombotic thrombocytopenia: a case report. Journal of Medical Case Reports. 2022;16(1):271. [CrossRef]
- Kim AY, Woo W, Yon DK, et al. Thrombosis patterns and clinical outcome of COVID-19 vaccine-induced immune thrombotic thrombocytopenia: A Systematic Review and Meta-Analysis. International Journal of Infectious Diseases. 2022;119:130-139. [CrossRef]
- Iba T, Levy JH. Thrombosis and thrombocytopenia in COVID-19 and after COVID-19 vaccination. Trends in Cardiovascular Medicine. 2022;32(5):249-256. [CrossRef]
- Schultz NH, Sørvoll IH, Michelsen AE, et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. New England Journal of Medicine. 2021;384(22):2124-2130. [CrossRef]
- Nicolai L, Leunig A, Pekayvaz K, et al. Thrombocytopenia and splenic platelet-directed immune responses after IV ChAdOx1 nCov-19 administration. Blood. 2022;140(5):478-490. [CrossRef]
- Wolf ME, Luz B, Niehaus L, Bhogal P, Bäzner H, Henkes H. Thrombocytopenia and Intracranial Venous Sinus Thrombosis after “COVID-19 Vaccine AstraZeneca” Exposure. Journal of Clinical Medicine. 2021;10(8):1599. [CrossRef]
- Patriquin CJ, Laroche V, Selby R, et al. Therapeutic Plasma Exchange in Vaccine-Induced Immune Thrombotic Thrombocytopenia. New England Journal of Medicine. 2021;385(9):857-859. [CrossRef]
- Thaler J, Ay C, Gleixner KV, et al. Successful treatment of vaccine-induced prothrombotic immune thrombocytopenia (VIPIT). Journal of Thrombosis and Haemostasis. 2021;19(7):1819-1822. [CrossRef]
- Helms JM, Ansteatt KT, Roberts JC, et al. Severe, Refractory Immune Thrombocytopenia Occurring After SARS-CoV-2 Vaccine. J Blood Med. 2021;12:221-224. [CrossRef]
- Ling VWT, Fan BE, Lau SL, Lee XH, Tan CW, Lee SY. Severe Thrombocytopenia, Thrombosis and Anti-PF4 Antibody after Pfizer-BioNTech COVID-19 mRNA Vaccine Booster—Is It Vaccine-Induced Immune Thrombotic Thrombocytopenia? Vaccines. 2022;10(12):2023. [CrossRef]
- Afshar ZM, Barary M, Babazadeh A, et al. SARS-CoV-2-related and Covid-19 vaccine-induced thromboembolic events: A comparative review. Reviews in Medical Virology. 2022;32(4):e2327. [CrossRef]
- Hsiao PJ, Wu KL, Chen YC, et al. The role of anti-platelet factor 4 antibodies and platelet activation tests in patients with vaccine-induced immune thrombotic thrombocytopenia: Brief report on a comparison of the laboratory diagnosis and literature review. Clin Chim Acta. 2022;529:42-45. [CrossRef]
- Cines DB, Bussel JB. SARS-CoV-2 Vaccine–Induced Immune Thrombotic Thrombocytopenia. New England Journal of Medicine. 2021;384(23):2254-2256. [CrossRef]
- Liu Y, Shao Z, Wang H. SARS-CoV-2 vaccine-induced immune thrombotic thrombocytopenia. Thrombosis Research. 2022;209:75-79. [CrossRef]
- Kashir J, Ambia AR, Shafqat A, Sajid MR, AlKattan K, Yaqinuddin A. Scientific premise for the involvement of neutrophil extracellular traps (NETs) in vaccine-induced thrombotic thrombocytopenia (VITT). Journal of Leukocyte Biology. 2022;111(3):725-734. [CrossRef]
- Kalaska B, Miklosz J, Swieton J, Jakimczuk A, Pawlak D, Mogielnicki A. The effect of ChAdOx1 nCov-19 vaccine on arterial thrombosis development and platelet aggregation in female rats. Vaccine. 2022;40(13):1996-2002. [CrossRef]
- Pavenski K. Relapse of Immune Thrombotic Thrombocytopenic Purpura Following Vaccination with COVID19 mRNA Vaccine. TH Open. 2021;05(3):e335-e337. [CrossRef]
- Rock G, Weber V, Stegmayr B. Therapeutic plasma exchange (TPE) as a plausible rescue therapy in severe vaccine-induced immune thrombotic thrombocytopenia. Transfusion and Apheresis Science. 2021;60(4):103174. [CrossRef]
- Okada Y, Sakai R, Sato-Fitoussi M, et al. Potential Triggers for Thrombocytopenia and/or Hemorrhage by the BNT162b2 Vaccine, Pfizer-BioNTech. Front Med (Lausanne). 2021;8:751598. [CrossRef]
- Chong KM, Yang CY, Lin CC, Lien WC. Severe immune thrombocytopenia following COVID-19 vaccination (Moderna) and immune checkpoint inhibitor. The American Journal of Emergency Medicine. 2022;56:395.e1-395.e3. [CrossRef]
- Schettle S, Frantz R, Stulak J, Villavicencio M, Rosenbaum A. HeartWare Thrombosis After mRNA COVID-19 Vaccination. Mayo Clinic Proceedings. 2022;97(7):1399-1401. [CrossRef]
- Jacob C, Rani KA, Holton PJ, et al. Malignant middle cerebral artery syndrome with thrombotic thrombocytopenia following vaccination against SARS-CoV-2. Journal of the Intensive Care Society. 2022;23(4):479-484. [CrossRef]
- Cliff-Patel N, Moncrieff L, Ziauddin V. Renal Vein Thrombosis and Pulmonary Embolism Secondary to Vaccine-induced Thrombotic Thrombocytopenia (VITT). Eur J Case Rep Intern Med. 2021;8(6):002692. [CrossRef]
- Melas N. “Portal vein thrombosis occurring after the first dose of mRNA SARS-CoV-2 vaccine in a patient with antiphospholipid syndrome.” Thrombosis Update. 2021;5:100069. [CrossRef]
- Marchandot B, Carmona A, Trimaille A, Curtiaud A, Morel O. Procoagulant microparticles: a possible link between vaccine-induced immune thrombocytopenia (VITT) and cerebral sinus venous thrombosis. J Thromb Thrombolysis. 2021;52(3):689-691. [CrossRef]
- Favaloro EJ, Pasalic L, Lippi G. Review and evolution of guidelines for diagnosis of COVID-19 vaccine induced thrombotic thrombocytopenia (VITT). Clinical Chemistry and Laboratory Medicine (CCLM). 2022;60(1):7-17. [CrossRef]
- Franceschi AM, Petrover DR, McMahon TM, et al. Retrospective review COVID-19 vaccine induced thrombotic thrombocytopenia and cerebral venous thrombosis-what can we learn from the immune response. Clin Imaging. 2022;90:63-70. [CrossRef]
- Lindhoff-Last E, Schoenborn L, Piorkowski M, et al. Heterogeneity of Vaccine-Induced Immune Thrombotic Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination and Safety of Second Vaccination with BNT162b2. Thromb Haemost. 2022;122(2):304-307. [CrossRef]
- Sissa C, Al-Khaffaf A, Frattini F, et al. Relapse of thrombotic thrombocytopenic purpura after COVID-19 vaccine. Transfusion and Apheresis Science. 2021;60(4). [CrossRef]
- Leung HHL, Perdomo J, Ahmadi Z, et al. NETosis and thrombosis in vaccine-induced immune thrombotic thrombocytopenia. Nat Commun. 2022;13(1):5206. [CrossRef]
- Wang CA, Yeh JS, Hong CY. Repeated Coronary Artery Thrombosis after mRNA-1273 COVID-19 Vaccination. Acta Cardiol Sin. 2022;38(6):793-795. [CrossRef]
- Refractory vaccine-induced immune thrombotic thrombocytopenia (VITT) managed with delayed therapeutic plasma exchange (TPE). [CrossRef]
- Iba T, Levy JH, Warkentin TE. Recognizing Vaccine-Induced Immune Thrombotic Thrombocytopenia. Crit Care Med. 2022;50(1):e80-e86. [CrossRef]
- Julian JA, Mathern DR, Fernando D. Idiopathic Thrombocytopenic Purpura and the Moderna Covid-19 Vaccine. Annals of Emergency Medicine. 2021;77(6):654-656. [CrossRef]
- Paul M, Abraham L, Sophy M, Varghese D, Thomas J. Idiopathic Thrombotic Microangiopathy with ChAdOx1 nCov-19 Vaccination in a Middle Aged Male: A Clinical Challenge in the Covid Era. Published online July 25, 2021:431.
- Pasin F, Calabrese A, Pelagatti L. Immune thrombocytopenia following COVID-19 mRNA vaccine: casuality or causality? Intern Emerg Med. 2022;17(1):295-297. [CrossRef]
- Choi PYI, Hsu D, Tran HA, et al. Immune thrombocytopenia following vaccination during the COVID-19 pandemic. Haematologica. 2021;107(5):1193-1196. [CrossRef]
- Tarawneh O, Tarawneh H. Immune thrombocytopenia in a 22-year-old post Covid-19 vaccine. Am J Hematol. 2021;96(5):E133-E134. [CrossRef]
- Condorelli A, Markovic U, Sciortino R, Di Giorgio MA, Nicolosi D, Giuffrida G. Immune Thrombocytopenic Purpura Cases Following COVID-19 Vaccination. Mediterr J Hematol Infect Dis. 2021;13(1):e2021047. [CrossRef]
- Kelton JG, Arnold DM, Nazy I. Lessons from vaccine-induced immune thrombotic thrombocytopenia. Nat Rev Immunol. 2021;21(12):753-755. [CrossRef]
- Favaloro EJ. Laboratory testing for suspected COVID-19 vaccine–induced (immune) thrombotic thrombocytopenia. International Journal of Laboratory Hematology. 2021;43(4):559-570. [CrossRef]
- Thiele T, Weisser K, Schönborn L, et al. Laboratory confirmed vaccine-induced immune thrombotic thrombocytopenia: Retrospective analysis of reported cases after vaccination with ChAdOx-1 nCoV-19 in Germany. Lancet Reg Health Eur. 2022;12:100270. [CrossRef]
- Al-Ahmad M, Al Rasheed M, Altourah L, Rodriguez-Bouza T, Shalaby N. Isolated thrombosis after COVID-19 vaccination: case series. Int J Hematol. 2022;115(2):153-157. [CrossRef]
- Malayala SV, Mohan G, Vasireddy D, Atluri P. Purpuric Rash and Thrombocytopenia After the mRNA-1273 (Moderna) COVID-19 Vaccine. Cureus. 2021;13(3). [CrossRef]
- Mendes-de-Almeida DP, Martins-Gonçalves R, Morato-Santos R, et al. Intracerebral hemorrhage associated with vaccine-induced thrombotic thrombocytopenia following ChAdOx1 nCOVID-19 vaccine in a pregnant woman. Haematologica. 2021;106(11):3025-3028. [CrossRef]
- Passariello M, Vetrei C, Amato F, De Lorenzo C. Interactions of Spike-RBD of SARS-CoV-2 and Platelet Factor 4: New Insights in the Etiopathogenesis of Thrombosis. Int J Mol Sci. 2021;22(16):8562. [CrossRef]
- Greinacher A, Selleng K, Palankar R, et al. Insights in ChAdOx1 nCoV-19 vaccine-induced immune thrombotic thrombocytopenia. Blood. 2021;138(22):2256-2268. [CrossRef]
- Zheng X, Gao F, Wang L, Meng Y, Ageno W, Qi X. Incidence and outcomes of splanchnic vein thrombosis after diagnosis of COVID-19 or COVID-19 vaccination: a systematic review and meta-analysis. J Thromb Thrombolysis. Published online November 19, 2022:1-14. [CrossRef]
- Dix C, McFadyen J, Huang A, Chunilal S, Chen V, Tran H. Understanding vaccine-induced thrombotic thrombocytopenia (VITT). Internal Medicine Journal. 2022;52(5):717-723. [CrossRef]
- Tsilingiris D, Vallianou NG, Karampela Ι, Dalamaga Μ. Vaccine induced thrombotic thrombocytopenia: The shady chapter of a success story. Metabolism Open. 2021;11:100101. [CrossRef]
- Blauenfeldt RA, Kristensen SR, Ernstsen SL, Kristensen CCH, Simonsen CZ, Hvas AM. Thrombocytopenia with acute ischemic stroke and bleeding in a patient newly vaccinated with an adenoviral vector-based COVID-19 vaccine. Journal of Thrombosis and Haemostasis. 2021;19(7):1771-1775. [CrossRef]
- Al-Mayhani T, Saber S, Stubbs MJ, et al. Ischaemic stroke as a presenting feature of ChAdOx1 nCoV-19 vaccine-induced immune thrombotic thrombocytopenia. J Neurol Neurosurg Psychiatry. 2021;92(11):1247-1248. [CrossRef]
- Cascio Rizzo A, Giussani G, Agostoni EC. Ischemic Stroke and Vaccine-Induced Immune Thrombotic Thrombocytopenia following COVID-19 Vaccine: A Case Report with Systematic Review of the Literature. Cerebrovasc Dis. Published online May 5, 2022:1-13. [CrossRef]
- Ferro JM, Sousa DA de, Coutinho JM, Martinelli I. European stroke organization interim expert opinion on cerebral venous thrombosis occurring after SARS-CoV-2 vaccination. European Stroke Journal. 2021;6(3):CXVI-CXXI. [CrossRef]
- Mereuta OM, Rossi R, Douglas A, et al. Characterization of the ‘White’ Appearing Clots that Cause Acute Ischemic Stroke. Journal of Stroke and Cerebrovascular Diseases. 2021;30(12):106127. [CrossRef]
- Rahmig J, Altarsha E, Siepmann T, Barlinn K. Acute Ischemic Stroke in the Context of SARS-CoV-2 Vaccination: A Systematic Review. Neuropsychiatr Dis Treat. 2022;18:1907-1916. [CrossRef]
- Saleh M, Zimmermann J, Lehnen NC, Pötzsch B, Weller JM. Late-Onset Vaccine-Induced Immune Thombotic Thrombocytopenia (VITT) with Cerebral Venous Sinus Thrombosis. J Stroke Cerebrovasc Dis. 2022;31(4):106311. [CrossRef]
- Stefanou MI, Palaiodimou L, Sousa DA de, et al. Acute Arterial Ischemic Stroke Following COVID-19 Vaccination: A Systematic Review and Meta-analysis. Neurology. 2022;99(14):e1465-e1474. [CrossRef]
- Wills A, Swallow G, Kirkman MA, Rajan K, Subramanian G. Arterial and venous thrombotic stroke after ChAdOx1 nCoV-19 vaccine. Clin Med (Lond). 2022;22(2):184-186. [CrossRef]
- van de Munckhof A, Lindgren E, Kleinig TJ, et al. Outcomes of Cerebral Venous Thrombosis due to Vaccine-Induced Immune Thrombotic Thrombocytopenia After the Acute Phase. Stroke. 2022;53(10):3206-3210. [CrossRef]
- Alonso Castillo R, Martínez Castrillo JC. Neurological manifestations associated with COVID-19 vaccine. Neurologia (Engl Ed). Published online October 23, 2022:S2173-5808(22)00141-9. [CrossRef]
- Mohseni Afshar Z, Sharma A, Babazadeh A, et al. A review of the potential neurological adverse events of COVID-19 vaccines. Acta Neurol Belg. Published online November 16, 2022:1-36. [CrossRef]
- Dutta S, Kaur R, Charan J, et al. Analysis of Neurological Adverse Events Reported in VigiBase From COVID-19 Vaccines. Cureus. 2022;14(1):e21376. [CrossRef]
- Mirandola L, Arena G, Pagliaro M, et al. Massive cerebral venous sinus thrombosis in vaccine-induced immune thrombotic thrombocytopenia after ChAdOx1 nCoV-19 serum: case report of a successful multidisciplinary approach. Neurol Sci. 2022;43(3):1499-1502. [CrossRef]
- Sriwastava S, Sharma K, Khalid SH, et al. COVID-19 Vaccination and Neurological Manifestations: A Review of Case Reports and Case Series. Brain Sci. 2022;12(3):407. [CrossRef]
- Dutta A, Ghosh R, Bhattacharya D, et al. Anti-PF4 antibody negative cerebral venous sinus thrombosis without thrombocytopenia following immunization with COVID-19 vaccine in an elderly non-comorbid Indian male, managed with conventional heparin-warfarin based anticoagulation. Diabetes & Metabolic Syndrome: Clinical Research & Reviews. 2021;15(4):102184. [CrossRef]
- Park J, Park MS, Kim HJ, Song TJ. Association of Cerebral Venous Thrombosis with mRNA COVID-19 Vaccines: A Disproportionality Analysis of the World Health Organization Pharmacovigilance Database. Vaccines. 2022;10(5):799. [CrossRef]
- Taquet M, Husain M, Geddes JR, Luciano S, Harrison PJ. Cerebral venous thrombosis: a retrospective cohort study of 513,284 confirmed COVID-19 cases and a comparison with 489,871 people receiving a COVID-19 mRNA vaccine. :23.
- Fan BE, Shen JY, Lim XR, et al. Cerebral venous thrombosis post BNT162b2 mRNA SARS-CoV-2 vaccination: A black swan event. Am J Hematol. 2021;96(9):E357-E361. [CrossRef]
- Franchini M, Testa S, Pezzo M, et al. Cerebral venous thrombosis and thrombocytopenia post-COVID-19 vaccination. Thrombosis Research. 2021;202:182-183. [CrossRef]
- de Gregorio C, Colarusso L, Calcaterra G, et al. Cerebral Venous Sinus Thrombosis following COVID-19 Vaccination: Analysis of 552 Worldwide Cases. Vaccines. 2022;10(2):232. [CrossRef]
- Omidian N, Mohammadi P, Sadeghalvad M, Mohammadi-Motlagh HR. Cerebral microvascular complications associated with SARS-CoV-2 infection: How did it occur and how should it be treated? Biomed Pharmacother. 2022;154:113534. [CrossRef]
- De Michele M, Iacobucci M, Nicolini E, et al. Malignant Cerebral Infarction, Systemic Venous Thrombosis and Thrombocytopenia after ChAdOx1 nCov Vaccination: A Possible Catastrophic Variant of Vaccine Induced Thrombotic Thrombocytopenia. In Review; 2021. [CrossRef]
- Schulz JB, Berlit P, Diener HC, et al. COVID-19 Vaccine-Associated Cerebral Venous Thrombosis in Germany. Annals of Neurology. 2021;90(4):627-639. [CrossRef]
- Fadul A, Abdalla Elm, Abdelmahmuod E, et al. COVID-19 Vaccine-Induced Cerebral Sinus Thrombosis: Coincidence vs. Cause? Cureus. 2022;14(6):e26436. [CrossRef]
- Bs T. Acute Hemoglobin Decline with Signs of Hemolysis in Chronically Transfused Beta-thalassemia Patient Post Pfizer-BioNTech COVID-19 (BNT162b2) Vaccine: A Case Report. :4.
- Kumar TA, Sunka S. A Rare Case of M-RNA Vaccine (COVID-19) Induced Autoimmune Hemolytic Anaemia. Indian Journal of Critical Care Medicine. Published online 2022:S13-S13.
- Delaporta P, Lampropoulou E, Moschoviti A, et al. Adverse Events Following COVID-19 Vaccination in Transfusion-Dependent -Thalassemia Patients. Blood. 2021;138:2015. [CrossRef]
- Ferrer F, Roldão M, Figueiredo C, Lopes K. Atypical Hemolytic Uremic Syndrome after ChAdOx1 nCoV-19 Vaccination in a Patient with Homozygous CFHR3/CFHR1 Gene Deletion. NEF. 2022;146(2):185-189. [CrossRef]
- Fattizzo B, Barcellini W. Autoimmune hemolytic anemia: causes and consequences. Expert Review of Clinical Immunology. 2022;18(7):731-745. [CrossRef]
- Rico AC, Ferreirol AG, Zorilla SR, Gonzalez AM. Drug-induced autoimmune hemolytic anemia, as an adverse effect to a vaccine against COVID-19, description of 1 case and review of the literature. Galicia Clinica. Published online 2021:218-219.
- Kamura Y, Sakamoto T, Yokoyama Y, et al. Hemolysis induced by SARS-CoV-2 mRNA vaccination in patients with paroxysmal nocturnal hemoglobinuria. Int J Hematol. 2022;116(1):55-59. [CrossRef]
- Al-kuraishy HM, Al-Gareeb AI, Kaushik A, Kujawska M, Batiha GES. Hemolytic anemia in COVID-19. Ann Hematol. 2022;101(9):1887-1895. [CrossRef]
- Pérez-Lamas L, Moreno-Jiménez G, Tenorio-Núñez MC, et al. Hemolytic crisis due to Covid-19 vaccination in a woman with cold agglutinin disease. Am J Hematol. 2021;96(8):E288-E291. [CrossRef]
- Shakoor MT, Birkenbach MP, Lynch M. ANCA-Associated Vasculitis Following Pfizer-BioNTech COVID-19 Vaccine. American Journal of Kidney Diseases. 2021;78(4):611-613. [CrossRef]
- Mücke VT, Knop V, Mücke MM, Ochsendorf F, Zeuzem S. First description of immune complex vasculitis after COVID-19 vaccination with BNT162b2: a case report. BMC Infect Dis. 2021;21(1):958. [CrossRef]
- Chen CY, Chen TT, Hsieh CY, Lien MY, Yeh SP, Chen CC. Case reports of management of aplastic anemia after COVID-19 vaccination: a single institute experience in Taiwan. Int J Hematol. Published online September 4, 2022. [CrossRef]
- Suzuki Y, Shiba T. Chronic cold agglutinin disease after a third COVID-19 mRNA vaccination. Int J Hematol. Published online October 29, 2022. [CrossRef]
- Camacho-Domínguez L, Rodríguez Y, Polo F, et al. COVID-19 vaccine and autoimmunity. A new case of autoimmune hepatitis and review of the literature. Journal of Translational Autoimmunity. 2022;5:100140. [CrossRef]
- Mörz M. A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against COVID-19. Vaccines. 2022;10(10):1651. [CrossRef]
- Gill JR, Tashjian R, Duncanson E. Autopsy Histopathologic Cardiac Findings in 2 Adolescents Following the Second COVID-19 Vaccine Dose. Archives of Pathology & Laboratory Medicine. 2022;146(8):925-929. [CrossRef]
- Number of blood transfusions U.S. 2019. Statista. Accessed May 25, 2023. https://www.statista.com/statistics/1204079/number-blood-tranfusions-us/.
- Rose J. Critical Appraisal of VAERS Pharmacovigilance: Is the U.S. Vaccine Adverse Events Reporting System (VAERS) a Functioning Pharmacovigilance System? Published online April 21, 2023.
- United States Population (2023) - Worldometer. Accessed May 26, 2023. https://www.worldometers.info/world-population/us-population/.
- Ritchie H, Mathieu E, Rodés-Guirao L, et al. Coronavirus Pandemic (COVID-19). Our World in Data. Published online March 5, 2020. Accessed July 25, 2022. https://ourworldindata.org/covid-deaths.
- Hanna N, Heffes-Doon A, Lin X, et al. Detection of Messenger RNA COVID-19 Vaccines in Human Breast Milk. JAMA Pediatrics. Published online September 26, 2022. [CrossRef]
- CDC. COVID Data Tracker. Centers for Disease Control and Prevention. Published March 28, 2020. Accessed May 26, 2023. https://covid.cdc.gov/covid-data-tracker.
- NVSS - Birth Data. Published May 3, 2023. Accessed May 26, 2023. https://www.cdc.gov/nchs/nvss/births.htm.
- 2022 Breastfeeding Report Card. Centers for Disease Control and Prevention. Published April 13, 2023. Accessed May 26, 2023. https://www.cdc.gov/breastfeeding/data/reportcard.htm.
- Shimabukuro TT, Nguyen M, Martin D, DeStefano F. Safety monitoring in the Vaccine Adverse Event Reporting System (VAERS). Vaccine. 2015;33(36):4398-4405. [CrossRef]
- Ioannidis JPA. Infection fatality rate of COVID-19 inferred from seroprevalence data. Bull World Health Organ. 2021;99(1):19-33F. [CrossRef]
- Abas AH, Marfuah S, Idroes R, et al. Can the SARS-CoV-2 Omicron Variant Confer Natural Immunity against COVID-19? Molecules. 2022;27(7):2221. [CrossRef]
- Young BE, Seppo AE, Diaz N, et al. Association of Human Milk Antibody Induction, Persistence, and Neutralizing Capacity With SARS-CoV-2 Infection vs mRNA Vaccination. JAMA Pediatrics. 2022;176(2):159-168. [CrossRef]
- Narayanaswamy V, Pentecost BT, Schoen CN, et al. Neutralizing Antibodies and Cytokines in Breast Milk After Coronavirus Disease 2019 (COVID-19) mRNA Vaccination. Obstet Gynecol. 2022;139(2):181-191. [CrossRef]
- Schenk-Braat EAM, van Mierlo MMKB, Wagemaker G, Bangma CH, Kaptein LCM. An inventory of shedding data from clinical gene therapy trials. The Journal of Gene Medicine. 2007;9(10):910-921. [CrossRef]
- Mendonça SA, Lorincz R, Boucher P, Curiel DT. Adenoviral vector vaccine platforms in the SARS-CoV-2 pandemic. npj Vaccines. 2021;6(1):1-14. [CrossRef]
- Kedl RM, Hsieh EWY, Morrison TE, et al. Evidence for Aerosol Transfer of SARS-CoV-2–Specific Humoral Immunity. Immunohorizons. 2023;7(5):307-309. [CrossRef]
- Purpura LJ, Alukal J, Chong AM, et al. SARS-CoV-2 RNA Shedding in Semen and Oligozoospermia of Patient with Severe Coronavirus Disease 11 Weeks after Infection. Emerg Infect Dis. 2022;28(1):196-200. [CrossRef]
- Lestari SW, Restiansyah G, Yunihastuti E, Pratama G. Comparison of sperm parameters and DNA fragmentation index between infertile men with infection and vaccines of COVID-19. Asian Journal of Andrology.:10.4103/aja202310. [CrossRef]
- Dong Y, Li X, Li Z, et al. Effects of inactivated SARS-CoV-2 vaccination on male fertility: A retrospective cohort study. Journal of Medical Virology. 2023;95(1):e28329. [CrossRef]
- Olana S, Mazzilli R, Salerno G, et al. 4BNT162b2 mRNA COVID-19 vaccine and semen: What do we know? Andrology. 2022;10(6):1023-1029. [CrossRef]
- Ma YC, Cheng C, Yuan C, Xiang LY, Wen J, Jin X. The effect of COVID-19 vaccines on sperm parameters: a systematic review and meta-analysis. Asian Journal of Andrology. 2023;25(4):468. [CrossRef]
- Banoun H. Current state of knowledge on the excretion of mRNA and spike produced by anti-COVID-19 mRNA vaccines; possibility of contamination of the entourage of those vaccinated by these products. Infectious Diseases Research. 2022;2022;3(4):22. [CrossRef]
- Craddock V, Mahajan A, Spikes L, et al. Persistent circulation of soluble and extracellular vesicle-linked Spike protein in individuals with postacute sequelae of COVID-19. Journal of Medical Virology. 2023;95(2):e28568. [CrossRef]
- Dobhal G, Datta A, Ayupova D, Teesdale-Spittle P, Goreham RV. Isolation, characterisation and detection of breath-derived extracellular vesicles. Sci Rep. 2020;10(1):17381. [CrossRef]
- Sinha A, Yadav AK, Chakraborty S, et al. Exosome-enclosed microRNAs in exhaled breath hold potential for biomarker discovery in patients with pulmonary diseases. Journal of Allergy and Clinical Immunology. 2013;132(1):219-222.e7. [CrossRef]
- Lucchetti D, Santini G, Perelli L, et al. Detection and characterisation of extracellular vesicles in exhaled breath condensate and sputum of COPD and severe asthma patients. European Respiratory Journal. 2021;58(2). [CrossRef]
- Parry PI, Lefringhausen A, Turni C, et al. ‘Spikeopathy’: COVID-19 Spike Protein Is Pathogenic, from Both Virus and Vaccine mRNA. Biomedicines. 2023;11(8):2287. [CrossRef]
- Yamamoto M, Kase M, Sano H, Kamijima R, Sano S. Persistent varicella zoster virus infection following mRNA COVID-19 vaccination was associated with the presence of encoded spike protein in the lesion. Journal of Cutaneous Immunology and Allergy. 2023;6(1):18-23. [CrossRef]
- Yonker LM, Swank Z, Bartsch YC, et al. Circulating Spike Protein Detected in Post–COVID-19 mRNA Vaccine Myocarditis. Circulation. 2023;147(11):867-876. [CrossRef]
- Castruita JAS, Schneider UV, Mollerup S, et al. SARS-CoV-2 spike mRNA vaccine sequences circulate in blood up to 28 days after COVID-19 vaccination. APMIS. 2023;131(3):128-132. [CrossRef]
- Duquesnoy RJ. Are We Ready for Epitope-Based HLA Matching in Clinical Organ Transplantation? Transplantation. 2017;101(8):1755-1765. [CrossRef]
- Aita KSU, Monte SJH, Silva AS, et al. Time is life: EpAssistant - a new tool for the automatic identification of anti-HLA antibody epitope specificity in transplant programs. Transplant Immunology. 2018;51:1-5. [CrossRef]
- Opelz G, Wujciak T, Döhler B, Scherer S, Mytilineos J. HLA compatibility and organ transplant survival. Collaborative Transplant Study. Rev Immunogenet. 1999;1(3):334-342.
- Harhay MN, Klassen AC, Zaidi H, et al. Living Organ Donor Perspectives and Sources of Hesitancy about COVID-19 Vaccines. Kidney360. 2021;2(7):1132-1140. [CrossRef]
- Pullen LC. COVID-19 Spurs Transplant Vaccination Policy. American Journal of Transplantation. 2021;21(12):3817-3818. [CrossRef]
- Kates OS, Stohs EJ, Pergam SA, et al. The limits of refusal: An ethical review of solid organ transplantation and vaccine hesitancy. American Journal of Transplantation. 2021;21(8):2637-2645. [CrossRef]
- Hippen BE, Axelrod DA, Maher K, et al. Survey of current transplant center practices regarding COVID-19 vaccine mandates in the United States. American Journal of Transplantation. 2022;22(6):1705-1713. [CrossRef]
- Kute V, Meshram HS, Sharma A, et al. Update on Coronavirus 2019 Vaccine Guidelines for Transplant Recipients. Transplantation Proceedings. 2022;54(6):1399-1404. [CrossRef]
- Kute VB, Asthana S, Gupta S, et al. NOTTO guidelines for vaccine-induced thrombotic thrombocytopenia in organ donation and transplantation. Indian Journal of Transplantation. 2022;16(1):3. [CrossRef]
- Uzun G, Bohnert BN, Althaus K, et al. Organ Donation From a Brain Dead Donor With Vaccine-induced Immune Thrombotic Thrombocytopenia After Ad26.COV2.S: The Risk of Organ Microthrombi. Transplantation. 2022;106(3):e178-e180. [CrossRef]
- Hann A, Hartog H, Nutu A, et al. Liver graft outcomes from donors with vaccine induced thrombosis and thrombocytopenia (VITT): United Kingdom multicenter experience. American Journal of Transplantation. 2022;22(3):996-998. [CrossRef]
- Greenhall GHB, Ushiro-Lumb I, Pavord S, et al. Kidney Transplantation From Deceased Donors With Vaccine-induced Immune Thrombocytopenia and Thrombosis: An Updated Analysis of the UK Experience. Transplantation. 2022;106(9):1824-1830. [CrossRef]
- Greenhall GHB, Ushiro-Lumb I, Pavord S, et al. Organ transplantation from deceased donors with vaccine-induced thrombosis and thrombocytopenia. Am J Transplant. 2021;21(12):4095-4097. [CrossRef]
- Loupy A, Goutaudier V, Jacquelinet C, Kerbaul F. Solid organ procurement and transplantation from deceased donors with vaccine-induced thrombosis and thrombocytopenia. American Journal of Transplantation. 2021;21(12):4098-4101. [CrossRef]
- van Bruchem M, van Rosmalen M, Warmerdam A, et al. Outcome After Organ Transplantation From Brain-dead Donors After a Cerebral Insult Following SARS-CoV-2 Vaccination Within the Eurotransplant Region. Transplantation. 2022;106(1):e100. [CrossRef]
- Centonze L, Lauterio A, De Carlis R, Ferla F, De Carlis L. Successful Liver Transplantation From a Deceased Donor With Vaccine-Induced Thrombotic Thrombocytopenia Causing Cerebral Venous Sinus and Hepatic Veins Thrombosis After ChAdOx1 nCov-19 Vaccination. Transplantation. 2021;105(10):e144. [CrossRef]
- Valsecchi M, Lauterio A, Crocchiolo R, et al. New-Onset Antibodies to Platelet Factor 4 Following Liver Transplantation From a Donor With Vaccine-Induced Thrombotic Thrombocytopenia. Liver Transpl. 2022;28(2):314-316. [CrossRef]
- Jamme M, Elalamy I, d’Izarny Gargas T, et al. Transplantation Outcome in Recipients Engrafted With Organs Recovered From the First French Deceased Donor With a SARS-COV-2 Vaccine-induced Thrombotic Thrombocytopenia. Transplantation. 2021;105(8):e84. [CrossRef]
- Kramer AH, Baht R, Doig CJ. Time trends in organ donation after neurologic determination of death: a cohort study. CMAJ Open. 2017;5(1):E19-E27. [CrossRef]
- Verhoeven CJ, Simon TC, de Jonge J, et al. Liver grafts procured from donors after circulatory death have no increased risk of microthrombi formation. Liver Transplantation. 2016;22(12):1676-1687. [CrossRef]
- Dubbeld J, Hoekstra H, Farid W, et al. Similar liver transplantation survival with selected cardiac death donors and brain death donors. British Journal of Surgery. 2010;97(5):744-753. [CrossRef]
- Grewal HP, Willingham DL, Nguyen J, et al. Liver transplantation using controlled donation after cardiac death donors: An analysis of a large single-center experience. Liver Transplantation. 2009;15(9):1028-1035. [CrossRef]
- Yamamoto S, Wilczek HE, Duraj FF, Groth CG, Ericzon BG. Liver Transplantation with Grafts from Controlled Donors after Cardiac Death: A 20-Year Follow-up at a Single Center. American Journal of Transplantation. 2010;10(3):602-611. [CrossRef]
- Vivalda S, Zhengbin H, Xiong Y, Liu Z, Wang Z, Ye Q. Vascular and Biliary Complications Following Deceased Donor Liver Transplantation: A Meta-analysis. Transplantation Proceedings. 2019;51(3):823-832. [CrossRef]
- Swissmedic 2019 © Copyright. Evaluation of haemovigilance reports in 2021. Accessed December 11, 2022. https://www.swissmedic.ch/swissmedic/en/home/humanarzneimittel/marktueberwachung/haemovigilance/haemovigilance-publications-events/haemovigilance-report-2021.html.
- Actualité - Rapport d’activité hémovigilance 2021 - ANSM. Accessed December 11, 2022. https://ansm.sante.fr/actualites/rapport-dactivite-hemovigilance-2021.
- Funk M, Heiden M, Müller S, et al. Hämovigilanz-Bericht Des Paul-Ehrlich-Instituts 2020: Auswertung Der Meldungen von Reaktionen Und Zwischenfällen Nach § 63i AMG. Accessed December 11, 2022. www.pei.de/haemovigilanzbericht.
- Martina V. Hämovigilanzbericht 2021.
- Danish Hemovigilance Committee. Blood Donation Adverse Reactions and Events Annual Report 2021. Accessed May 25, 2023. https://dski.dk/wp-content/uploads/2023/03/blood-donation-adverse-reaction-and-events-annual-report-2021.pdf.
- S Narayan (Ed) D Poles et al. The 2021 Annual SHOT Report. Serious Hazards of Transfusion (SHOT) Steering Group; 2022. Accessed December 11, 2022. https://www.shotuk.org/wp-content/uploads/myimages/SHOT-REPORT-2021-FINAL-bookmarked-V3-November.pdf.
- 2020 to 2021 Cells, tissues, and organs surveillance system (CTOSS). Published December 22, 2022. Accessed May 25, 2023. https://www.canada.ca/en/public-health/services/surveillance/blood-safety-contribution-program/cells-tissues-organs-surveillance-system-2020-2021-infographic.html.
- Haemovigilance by JRCS 2021. Japanese Red Cross Accessed May 25, 2023. https://www.jrc.or.jp/mr/english/pdf/Haemovigilance%20by%20JRCS%202021.pdf.
Figure 1.
VAERS domestic and foreign reports as of May 15, 2023 queried using keyword ‘transfusions’. Source: https://vaers.hhs.gov.
Figure 1.
VAERS domestic and foreign reports as of May 15, 2023 queried using keyword ‘transfusions’. Source: https://vaers.hhs.gov.
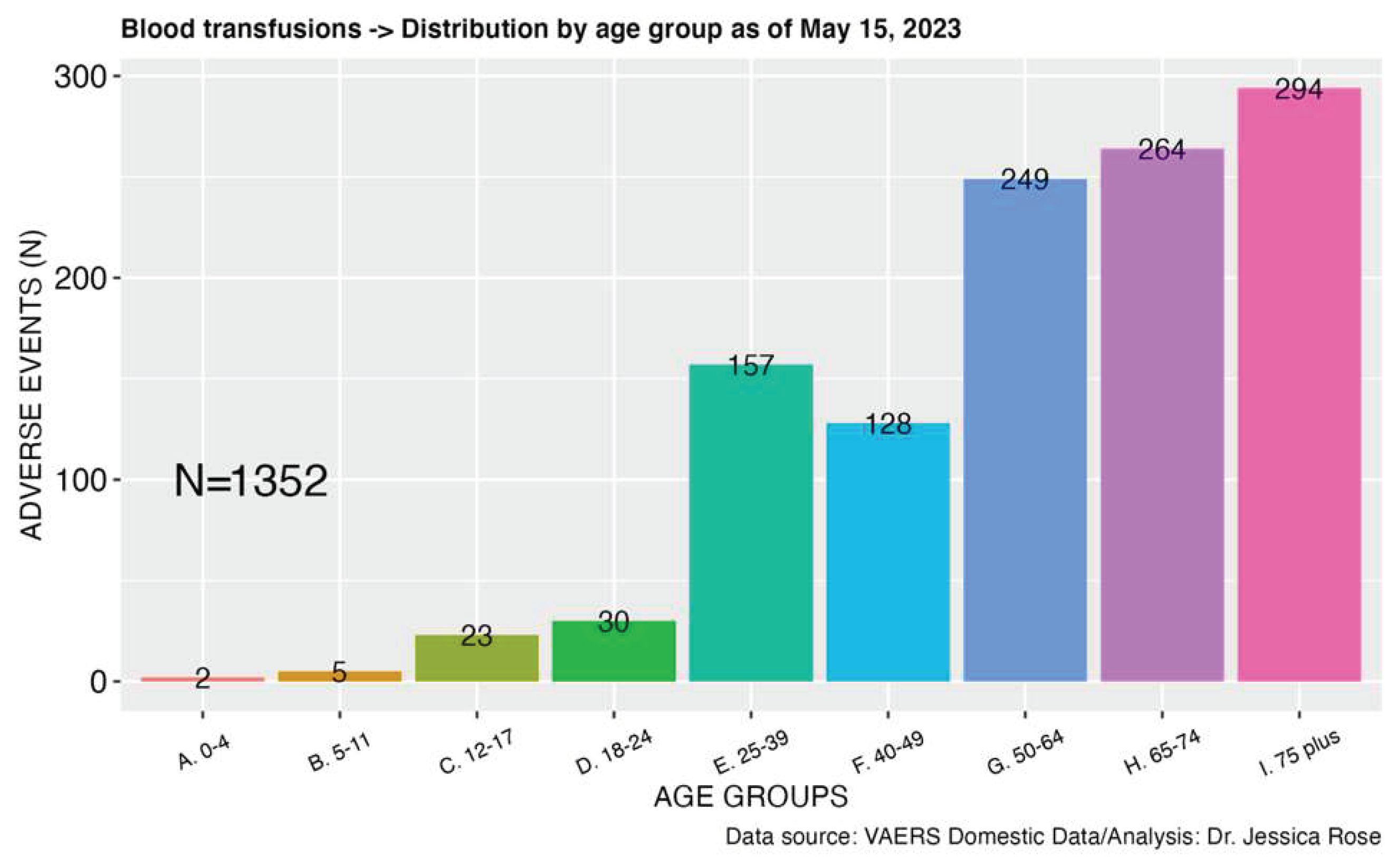
Figure 2.
VAERS domestic and foreign reports as of May 15, 2023 queried using MedDRA keywords “Breast feeding”, “Breast milk discolouration”, “Exposure via breast milk”, “Maternal exposure during breast feeding”. Source: https://vaers.hhs.gov.
Figure 2.
VAERS domestic and foreign reports as of May 15, 2023 queried using MedDRA keywords “Breast feeding”, “Breast milk discolouration”, “Exposure via breast milk”, “Maternal exposure during breast feeding”. Source: https://vaers.hhs.gov.
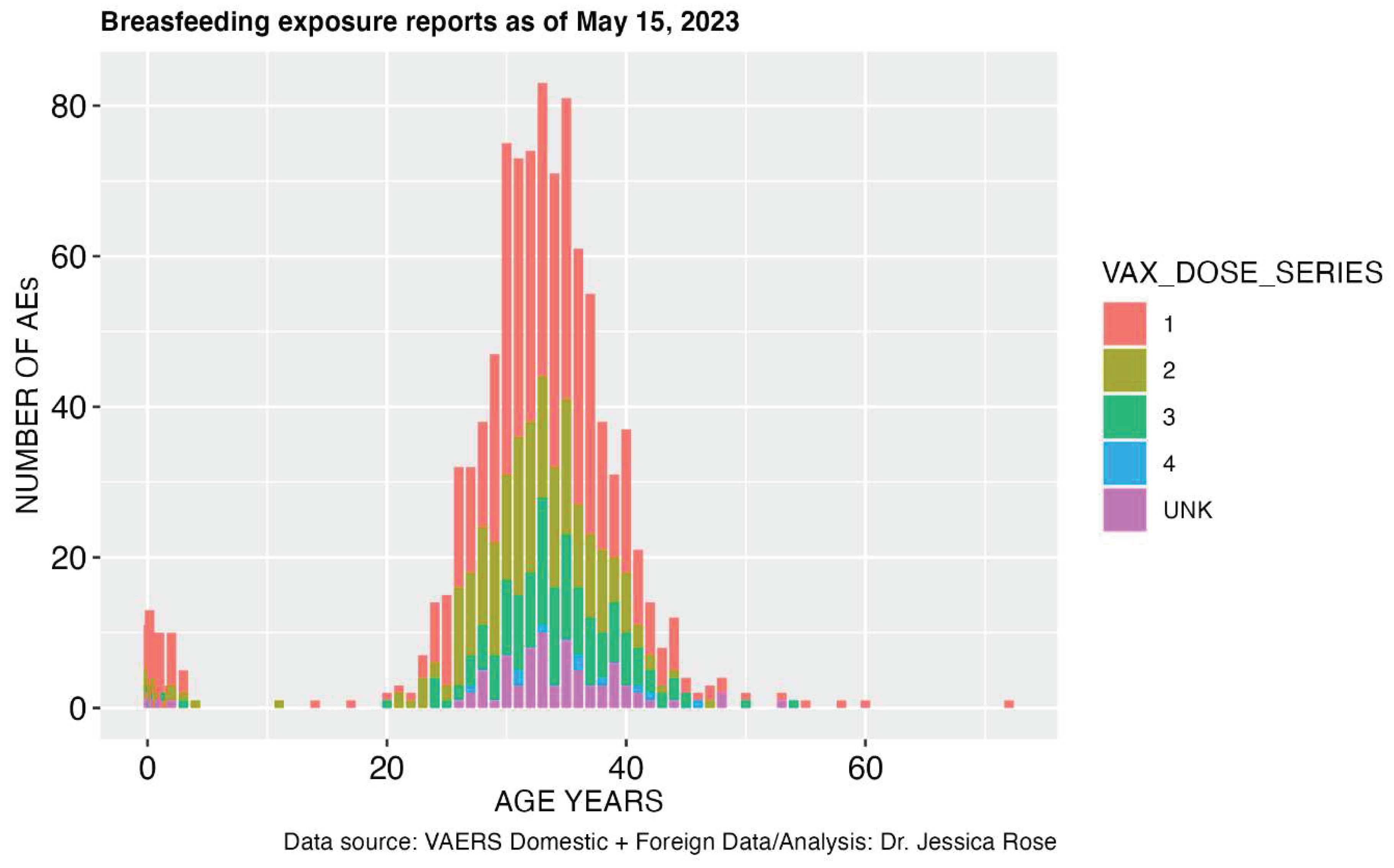
Figure 3.
Possible routes of secondary exposure to vaccine artifacts.
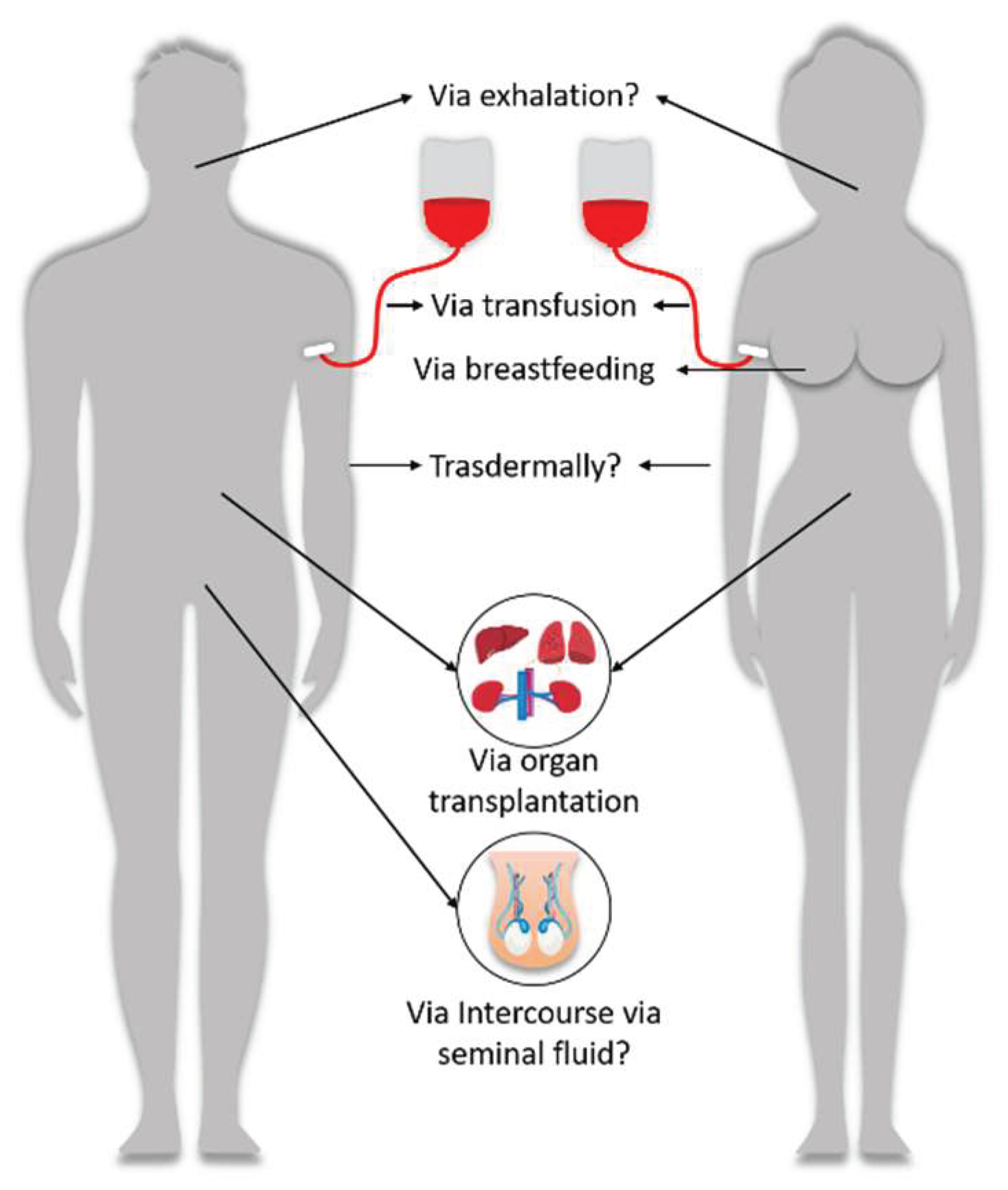

Table 1.
An overview of case reports for blood conditions related to Covid-19 vaccines.
| Condition | Case Reports |
| VITT | 12,14,30,37,44,45(p4),61,63–101,102(p1),103–233 |
| Stroke | 36,78,79,88,98,101,108,146,234–250,251(p284),252–258 |
| Hemolysis | 92,259–267 |
| Vasculitis | 4,268,269 |
| Anemia | 270 |
| Cold agglutinin disease | 271 |
| Hepatitis | 135,272 |
Table 2.
A summary of transplantation trials from donors deceased from VITT.
| Study | Donor | Organ | Recipient | Outcome | Thrombotic AE rate [AE rate including microthrombi, organ/graft rejection and Positive anti-PF4] |
| 314 | 50 year female with VITT | Heart | Unknown | No thrombosis or thrombocytopenia Anti-PF4 antibodies negative 3 weeks after transplantation |
0/1 [0/1] |
| 321 | 18 year old brain-dead female who dies from VITT-related intracranial hemorrhage | Liver | 58 year old female | Rapid drop in platelet count from 104x109/liter to 30x109/liter Anti-PF4 IgG strongly positive Grade 3 (severe) thrombocytopenia |
1/1 [1/1] |
| 315 | (n = 8, aged between 22 and 55 years) Died of catastrophic intracerebral hemorrhage or thrombosis, had received the first dose of ChAdOx1 nCOV-19 vaccine 9 to 19 days before hospital admission, and had detectable anti-PF4, low fibrinogen and elevated D-Dimers |
Liver | (n = 9, aged 2–43 years) | Four recipients with positive anti-PF4 antibodies without bleeding or thrombotic complications Two recipients with severe thrombotic events, requiring emergency retransplantation. Anti-PF4 antibodies negative. |
2/9 [6/9] |
| 316 | N=16 Median age 44 75% female |
Kidney Microthrombi observed in 4/11 biopsies |
N=30 Median age 48 47% female |
2 recipients with anti-PF4 antibodies but no clinical disease Major hemorrhagic complications in 3 recipients w/ independent risk factors |
3/30 [5/30] |
| 318 | Male, 41 Female, 69 Male, 67 All deceased from VITT |
Heart Kidney Liver Lungs |
N=9 Median age 58 (40-70) 44% female |
Glomerular microthrombi in 2 kidney recipients Pulmonary embolism in lung recipient No anti-PF4 antibodies observed |
1/9 [3/9] |
| 319 | N=6 Aged 37-72 years 50% female |
Liver Kidney Lung Heart |
N=17 Aged <1 to 77 years 42% female |
Liver cell necrosis and re-transplantation in one recipient Microangiopathy in one kidney recipient Two recipients (11.8%) developed thrombosis-related complications |
2/17 [4/17] |
| 320 | 32-year-old female deceased from VITT-induced stroke | Liver | 69-year-old female | No adverse events, operation successful | 0/1 [0/1] |
| 317 | N=13 Median age 34 (21 to 63) 85% female |
Kidney Liver Heart Lung Pancreas |
N=26 Median age 40 (2 to 63) |
Thrombsis Thromboembolism in 7/26 recipients (3 liver recipients and 4 Kidney/SPK/islet recipients) Graft dysfunction in 4/26 recipients Anti-PF4 antibodies positive in 3/13 (23%) tests with results |
7/26 [10/26] |
| 322 | Female aged 60-69 | Liver & Heart Lungs Right Kidney Left Kidney |
63-year-old male 58-year-old woman 70-year-old man 52-year-old man |
No AEs No AEs Thrombi is pre-implantation biopsy, uneventful transplantation Glomerular inflammation and hemorrhagic suffusion |
0/4 [2/4] |
| Summary | 16/98, 16% [29/98, 30%] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



