
Submitted:
21 February 2024
Posted:
23 February 2024
You are already at the latest version
Abstract
Biomechanical changes such as increased knee adduction moment (KAM) during walking are known to be involved in the development and severity of knee osteoarthritis (OA). Although various foot progression angle (FPA) modifications during gait have been applied to reduce peak KAM, few studies have investigated effects of applying toe-in or toe-out walking modifications for knee OA on peak KAM and three-dimensional (3D) moments of the ankle joint. Kinetic moment variables were acquired from 35 individuals with medial knee compartment OA. A 3D motion analysis system and two force platforms were used to acquire KAM and 3D moments of both ankle joints during gait. Visual3D motion analysis program was used to obtain final moment data for statistical processing. Repeated-measures analysis of variance with Bonferroni adjustment was used to compare kinetic and kinematic values for each FPA walking condition. The first peak KAM of an internal rotation foot position of the FPA walking condition showed significant decrease compared to normal foot position walking (p < 0.01). The second peak KAM of an external rotation foot position walking showed significant decrease compared to normal foot position walking (p < 0.01). Compared to a normal foot position, peak ankle inversion moment of the external rotation foot position walking showed a significantly decrease (p < 0.05). There were no interactive effects between FPA condition and limb sides for any KAM values (p > 0.05). These results suggest that clinical application of toe-in or toe-out gait modification walking in individuals with knee OA should be performed based on biomechanical evaluations such as peak KAM.
Keywords:
adduction moment
; foot progression angle
; knee joint
; osteoarthritis
1. Introduction
Knee osteoarthritis (OA), one of the degenerative diseases, is rapidly increasing due to recent increase in human average lifespan and an aging society [1,2]. In Korea, knee OA is a common disease that occurs in about one-third of people over the age of 60, with a prevalence rate of 20.2% in men and 50.1% in women [3]. Biomechanical changes such as increases of knee adduction moment (KAM) and knee varus shear force during walking are known to be involved in the development and severity of knee OA [4,5,6]. Because it is generally difficult to measure joint loads directly, joint moments such as KAM are often used as alternative measures of the force applied to a joint [7]. Knee moments that occur in real time during the stance phase, when the body weight is supported on the ground while walking, are biomechanical variables calculated by multiplying the magnitude of the three-dimensional ground reaction force and the lever arm distance from the knee joint center. Clinically, KAM is used for diagnosing knee OA and predicting knee pain, knee deformity, and the degree of knee OA progression [8,9]. KAM is a coronal kinetic variable. It typically has two distinct peaks during the stance phase of gait. The first peak occurs around the 25% stance phase during walking. The second peak elicits around the 75% stance phase [3]. The first peak KAM is typically greater than the second one. It is larger for patients with medial knee OA than for age-matched healthy individuals [10]. Peak KAMs during walking are determined by various factors such as gait pattern, knee pain avoidance strategy, and foot progression angle (FPA). Abnormally increased KAM during gait is closely related to worsening of musculoskeletal diseases such as knee OA [4,11,12].
From a biomechanical perspective, changes in kinematic and kinetic variables of any joints or segments during gait may affect ergonomic variables of all other connected joints and segments of the musculoskeletal system [13,14]. Therefore, changes in FPA such as internal rotation or external rotation of the foot in contact with the floor during the stance phase of gait may affect the KAM [6,14]. Since a study of Wang et al. [15], many studies have been conducted on biomechanical effects of lower extremity joints according to changes in FPA during walking. A previous study has demonstrated that the effect of FPA on KAM, in particular, self-selected over 15° of increasing toe-out angle in pain free individuals with knee OA, can significantly decrease the second peak KAM during gait except the first peak [6]. Additionally, the first KAM in internal rotation of FPA during gait is significantly decreased in patients with medial compartment knee OA [16]. Although many previous studies have reported that tiptoe walking and tiptoe walking interventions can reduce first and second peak KAMs in patients with medial compartment osteoarthritis of the knee joint, peak KAM change varies significantly between individuals in response to the achievement of the target FPA, anatomical variations, and biomechanical influence of the motor link [5]. Therefore, limiting exogenous variables that have a negative impact on measurement and evaluating objective and quantitative peak KAMs according to changes in FPA during gait are important for obtaining positive clinical outcomes of patients with knee OA.
Studies verifying effects of foot
rotation modifications during gait have mainly focused on effects of FPA during
gait on biomechanics of the knee joint
[7,17]. There is a need to evaluate effects of these modifications on other
lower extremity joints. Most of related studies have mainly examined effects of
gait modification on KAM and biomechanical values of the hip joint
[7,18,19]. However, there have been
few studies on effects of foot modification angle during walking on kinematics
and kinetics of the ankle joint along with its effect on KAM. Although it is
not known how FPA changes affect the ankle joint, increased ankle joint moments
in three dimensional planes of motion may increase biomechanical loads on soft
tissues around the ankle joint and increase the incidence of musculoskeletal
disorders such as ankle OA
[20]. Therefore, the purpose of this study was to investigate effects of
different FPA conditions during free walking on kinetics of the ankle and knee
joints in pain-free individuals with knee osteoarthritis using a 3D motion
analysis system with two force platforms.
2. Materials and Methods
2.1. Study Subjects
Thirty-five subjects (9 males and 26 females)
diagnosed with knee OA participated in this study. All participants had knee OA
without pain. Their average Kellgren-Lawrence grade was 1.8 ± 0.58 (Grade I: n
= 10, Grade II: n = 22, Grade III: n = 3). They were recruited from an area
orthopedic clinic. The mean illness duration of knee OA after initial diagnosis
was 5.2 ± 2.4 years. Inclusion criteria were: 1) no surgical
history of knee or ankle joints; 2) no severe pain of the lower extremity
joints or segments; 3) Kellgren-Lawrence grade 3 or less; and 4) able to walk
free and unaided according to instructions. If participants had neurologic
conditions affecting walking, painful knee OA, or systemic rheumatoid
arthritis, they were excluded from this study. Participants had an average age
of 62.2 years, a height of 159.3 cm, and a weight of 64.8 kg (Table 1). Average walking speeds
in NFP, IFP, and EFP gait trials were 1.24 ± 0.20 m/s, 1.21 ± 0.27 m/s, and
1.23 ± 0.19 m/s, respectively. There were no significant differences in walking
speed, cadence, or step length between FPA walking conditions (all p
> 0.05). An experienced researcher fully explained the research purpose and
experimental procedures of this study to study subjects. All subjects
voluntarily agreed to participate in this study. Written informed consents were
obtained from all participants. The study assessment protocol and design were
approved by the Institutional Review Board of Jeonju University
(jjIRB-200714-HR-2020-0708).
2.2. Instrumentation for gait analysis and data acquisition
Biomechanical data during gait were acquired from
motion analysis experimental laboratory at Jeonju university. A 3D motion
analysis system (Vicon Inc., Oxford, England) based on eight infrared cameras
and 8 m walking pathway was used to acquire KAM and 3D moments of both ankle
joints during gait (Figure 1). The
sampling rate of the motion capture camera system was set at 100 Hz. The lab
had two force platforms (AMTI, Watertown, MA, USA) for sampling data at 500 Hz.
Those were placed in the center of the walking way to obtain 3D ground reaction
force to calculate knee and ankle moments for three different FPA conditions:
normal foot position (NFP), maximal possible internal rotation foot position
(IFP), and maximal possible external foot position (EFP).
A T-frame bar (0.75 m) was used to recognize the
origin of the 3D spatial coordinates of the laboratory and for initial
calibration of the object and motion analysis system. Analog kinetic and
kinematic data obtained from two force platforms and eight capture cameras were
converted to digital data and processed through Nexus program (ver. 1.8.5,
Vicon Inc., Oxford, England) on the main computer. Anatomical labeling of
reflective markers and a lower limb segment model, which was the basis for gait
analysis, were created through the Nexus program [21].
In addition, the final c3d file for each gait trial was created through
integrated processing of all kinetic and kinematic data.
Visual3D (C-Motion Inc., Germantown, MD, USA), a
motion analysis program, was used with the final c3d data exported in the Nexus
program to obtain finals quantitative moment data for statistical processing
and 3D graphic results of knee and ankle moments (Figure 2). Visual3D software created a virtual
skeletal model for each subject based on reflective marker settings. It was
able to analyze knee moment and foot angle for each of the three FPA walking
trials (Figure 3). The X-Y-Z Cardan order
was used to decide the sequence of rotations according to the Right-Hand Rule
about the segment coordinate system’s axes [3].
All biomechanical data were low-pass filtered using a fourth-order Butterworth
filter with cutoff frequencies set to 15 Hz and 6 Hz, respectively [22].
Figure 1.
Motion analysis laboratory equipped with 3D motion capture cameras and two force platforms embedded in the center of the experimental 8 m walking pathway.
Figure 1.
Motion analysis laboratory equipped with 3D motion capture cameras and two force platforms embedded in the center of the experimental 8 m walking pathway.

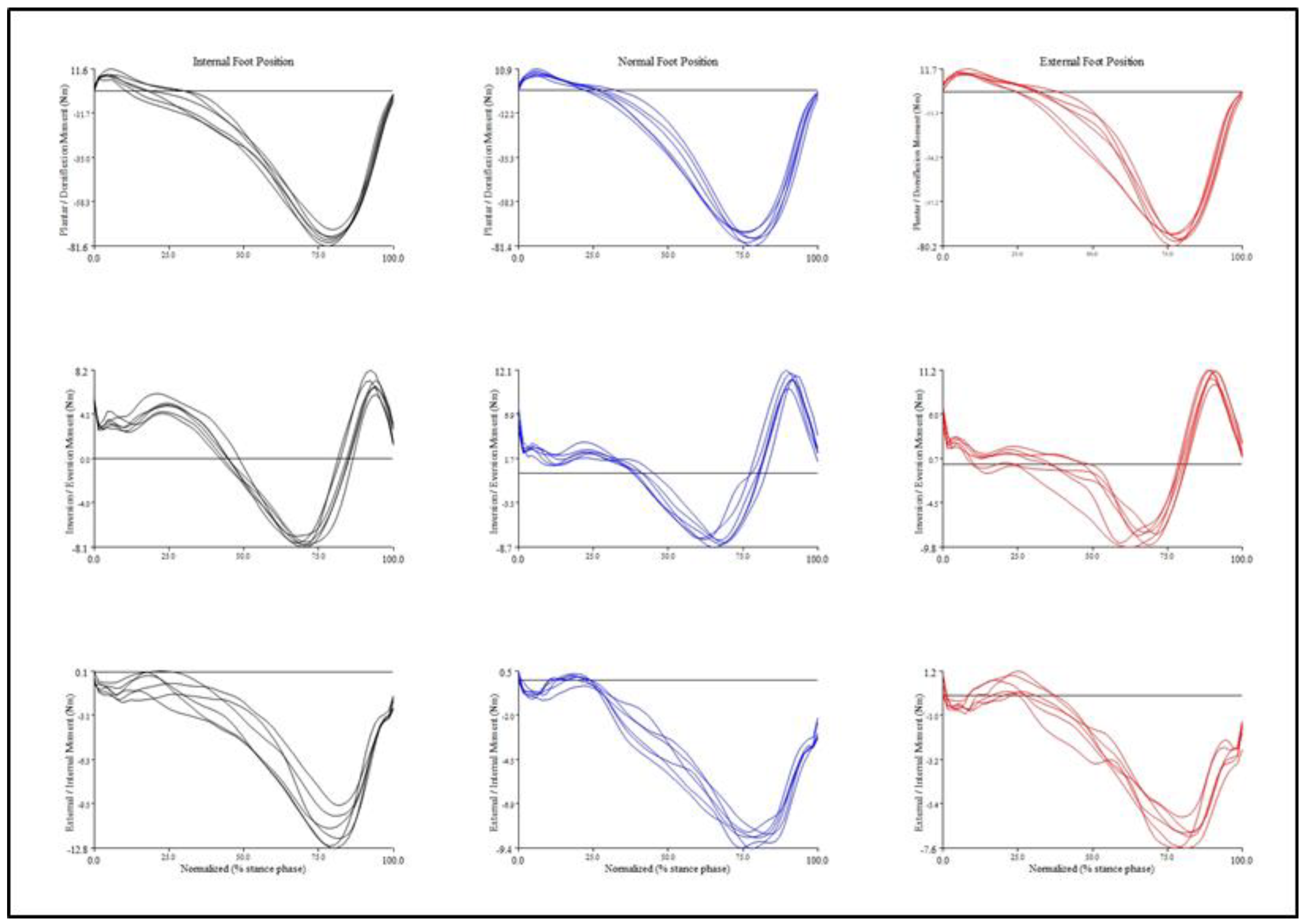
Figure 2.
Intra-individual variability in three-dimensional ankle joint net moments according to each foot position condition during walking trials.
Figure 2.
Intra-individual variability in three-dimensional ankle joint net moments according to each foot position condition during walking trials.
Ten reflective markers (14 mm) were attached
bilaterally on the medial and lateral malleoli, medial and lateral femoral
epicondyles, and greater trochanters to create joint positions. Four cluster
markers were attached bilaterally on the lower leg and thigh segments according
to six degrees of freedom (6DOF) model to present lower skeletal segments [22]. Additionally, five reflective markers were
attached to foot segments to measure FPA. Foot markers were attached onto the
first and fifth metatarsophalangeal joints, the dorsal center of the midfoot,
and medial and lateral hind foot. After setting the marker, static calibration
was executed to acquire dynamic moment data of the ankle and knee joints. The
average FPA value in each walking condition was calculated through 100% of
stance phase.
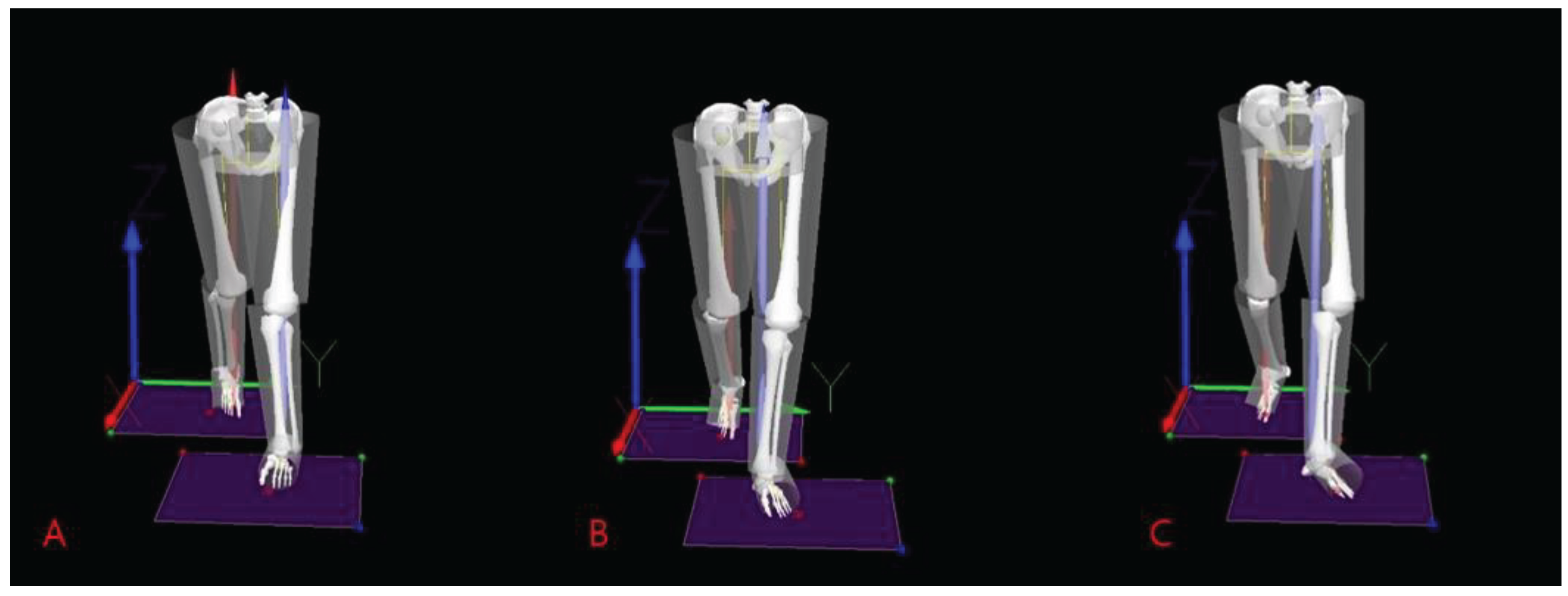
Figure 3.
Visual3D representation of virtual musculoskeletal model according to three different foot progression angles in each walking trial. A: Internal rotation foot position; B: Normal foot position; C: External rotation foot position.
Figure 3.
Visual3D representation of virtual musculoskeletal model according to three different foot progression angles in each walking trial. A: Internal rotation foot position; B: Normal foot position; C: External rotation foot position.
2.3. Gait analysis
Before attempting FPA walking trials, static
capture of reflective marker settings, which served as the standard for dynamic
gait analysis, was performed for each subject. To maintain a consistent foot
rotation angle in each FPA walking trail, the foot rotation when each subject
walked naturally was set as the baseline NFP. IFP and EFP conditions were then
set by adding or subtracting about 20° to this angle [23].
Additionally, to ensure consistent walking speed and step width, a tape line
was attached to the walking pathway so that each subject could know the degree
of FPA rotation achieved during walking practice. For each walking condition
(NFP, IFP, and EFP), a total of 8–10 walking trials that achieved the target
FPA line were analyzed. Kinetic and kinematic data were calculated for every
walking trial and averaged over each FPA gait condition. If the trial was not
completed successfully in an FPA condition, an additional walking trial was
performed. We applied a modified anatomical systems technique to analyze
biomechanical changes that occurred in the knee and ankle joints during
comfortable gait trials in different FPA conditions. All kinetic moment data of
the knee and ankle joints were normalized by each participant’s body weight and
analysis time of moment normalized to 100% of the stance phase during gait. The
experimental order of each FPA condition was randomly assigned.
2.4. Statistical analysis
Knee and ankle moments were normalized by subject
weight [7]. Knee moments val-ues were compared
between main FPA conditions: 1st peak KAM during 0-50% of stance phase, peak
KAM at mid stance, and 2nd peak KAM during 50-100% of stance phase. For
comparative analysis of ankle moments for each FPA walking condition,
characteristic peak moment variables generated in each 3D motion plane were
used. Peak ankle moment variables used in the analysis were dorsiflexion,
plantar flexion, inversion, eversion, internal rotation, and external rotation
moment that occurred in a specific period of stance phase.
G*Power (version 3.1.9.7) analysis was used to
estimate the appropriate sample size. A sample size of 25 was obtained based on
an effect size enough to identify the estimated significance based on a
previous study [5] that examined effects of
toe-in and toe-out gait retraining on biomechanical variables. Because all
analysis variables satisfied the para-metric test, the Kolmogorov-Smirnov test
used to verify normal distribution, two-way repeated-measures analysis of
variance (ANOVA) with Bonferroni adjustment was used to compare biomechanical values
for each FPA walking condition. If the significance of the main effect (FPA
condition or limb side) was confirmed in the ANOVA, pairwise comparisons were
performed using post hoc tests. All analyses were performed using SPSS version
26 (IBM Corp, Armonk, NY, USA).
3. Results
3.1. Peak knee moments occurring in coronal motion plane
All knee joint moment data required for analysis satisfied Mauchly's sphericity assumption. There were significant differences in repeated measures ANOVA results of the peak knee moment occurring in the coronal plane during the stance phase depending on FPA gait and bilateral knee conditions (p < 0.01) (Table 2). Specifically, the first peak KAM (F = 9.753, p = 0.004) and the second peak KAM (F = 27.624, p = 0.00006) were significantly different according to FPA walking trials (Table 2). The first peak KAM of the IFP walking condition showed a significant decrease compared to that of the NFP condition (p < 0.01) (Table 3, Figure 4). Additionally, the second peak KAM of the EFP condition showed a significant decrease compared to that of the NFP condition (p < 0.01) (Table 3, Figure 4). There were no significant differences in knee coronal moment variables among all other FPA walking conditions (p > 0.05). There were no interactive effects between FPA condition and knee sides for any KAM values (p > 0.05) (Table 2).
3.2. Moment results of ankle joint according to FPA condition
There was a significant difference only in the peak inversion moment generated at the ankle joint in the stance phase during walking depending on FPA conditions (F = 6.107, p = 0.019) (Table 4). Table 5 shows mean and standard deviation of peak moments occurring at the ankle joint according to the three FPA conditions in the stance phase during walking. Compared to the NFP condition, the peak inversion moment of the EFP walking condition generated at 50-75% stance phase showed a significantly decrease moment (p = 0.034, 95% CI = -0.07 ~ -0.01) (Table 5). On the other hand, except for the inversion peak moment value, there were no significant differences in other ankle peak moment values according to FPA walking conditions (p > 0.05). There were no interactive effects between FPA condition and ankle sides for any ankle moment variables (p > 0.05) (Table 4).
4. Discussion
This study was conducted to determine effects of gait modifications such as toe-in and toe-out walking on knee KAM and 3D moment characteristics occurring at the ankle joint during the stance phase in subjects with knee osteoarthritis. Increased KAM during walking not only increases the loading force imposed on the medial compartment of the knee joint, but also promotes the development of clinical symptoms of knee OA such as pain and inflammation [24,25,26]. Therefore, various gait modification methods such as medial knee thrust, lateral trunk lean, and toe-in or out gait have been applied to patients with knee OA to reduce KAM and alleviate clinical symptoms [16,27,28,29]. Comparison of effects between gait modifications in previous studies is limited by diverse sample characteristics and difficulties in consistently applying gait modifications [27,30]. To complement these methodological limitations of previous studies, this study clearly established inclusion criteria for study participants with knee osteoarthritis through pain severity and clinical evaluation as the Kellgren-Lawrence test. Additionally, guidelines were set for the walking pathway so that three different FPA walking conditions were applied as equally and consistently as possible to all participants.
This study analyzed how changes in FPA conditions affected knee joint and ankle joint moments during walking in 35 patients with medial knee osteoarthritis. Results of this study showed that the first peak value of KAM in the IFP walking condition was significantly decreased by 19.1% compared to that of NFP as the baseline walking condition. These results demonstrate the clinical effectiveness of specific gait modifications in reducing knee joint discomfort during walking, in which participants who have a choice of different gait modifications prefer toe-in gait the most [27,29,31]. In general, the value of the first peak of the KAM that occurred in the early stance phase was greater than the second peak of the KAM. Results of this study showed that toe-in gait modification was closely related to the decrease in the first peak of the KAM. The reason why the FPA condition of toe-in gait significantly reduced the first peak of the KAM was because the loading center moved to the lateral side as the knee joint central axis moved medially [16]. The second peak of the KAM (-0.50 Nm/kg) of the FPA condition of toe-in gait tended to increase compared to that of the NFP condition (-0.44 Nm/kg), although they showed no significant difference. In a study on the second peak KAM according to the application of FPA in 50 patients with knee osteoarthritis, both the 10° toe-in gait and the baseline gait showed the same moment value (-0.46 Nm/kg) without a significant difference [7]. In addition, like the current study, there was no significant difference between the two FPA walking conditions on the second peak KAM during toe-in gait and baseline gait in twelve patients with medial compartment knee osteoarthritis [16]. However, Lynn et al. [23] reported a significantly greater KAM value of the late stance in internal foot position walking than in normal foot position walking. The reason for such conflicting results of the second peak KAM might be because Lynn et al.'s study was conducted with a small number of healthy individuals without knee OA.
As a result of this study, in contrast to toe-in gait that showed a significant decrease in the first peak KAM, the toe-out gait showed a significant reduction in the second peak KAM compared to the NFP condition in individuals with knee OA. However, there was no significant difference in the first peak KAM value between NFP (-0.42 Nm/kg) and EFP (-0.47 Nm/kg) gait conditions. These results were similar to previous studies reporting reduction of the second peak KAM during toe-out gait in patients with knee OA [6,16,32,33]. Unlike results of this study, Lin et al. [34] reported that applying a 30° self-selected toe-out gait to participants caused a significant increase in the first peak KAM. The current study applied a toe-out walking trial, which was increased by 20° compared to NFP angle. Characteristics of the present study subjects were also individuals with knee osteoarthritis, not healthy participants. Peak KAM values of the present study for the FPA toe-out walking condition were somewhat different from previous studies [35,36,37,38]. These differences might be attributed to different characteristics of study subjects, clinical severity of knee OA, and variations in study design. Specifically, most subjects of the present study were patients with mild knee OA. However, there were studies conducted on patients with moderate knee osteoarthritis of K-L grade IV or higher [35,36]. There were also studies conducted on knee OA patients with severe clinical symptoms [37,38].
Many studies have determined effects of toe-in or toe-out walking conditions on biomechanical variables of the knee and hip joints in people with medial compartment knee OA. However, very few studies have examined effects of these walking conditions on the moment of the ankle joint. The present study analyzed effects of different walking conditions on 3D ankle moments along with their effects on peak KAM according to FPA during walking in individuals with knee OA. Results showed that there was no significant increase in ankle joint moment value according to changes in FPA walking conditions. Only the peak ankle inversion moment value of the EFP walking condition decreased compared to that of the NFP condition. In a previous study conducted on 15 patients with medial compartment knee OA, there was no change in the peak external ankle inversion moment value (0.02 Nm/kg) of 10° toe-out walking compared to the baseline condition. The peak external ankle inversion moment value (0.01 Nm/kg) of 20° toe-out walking was not changed either [20]. On the other hand, the toe-in gait condition showed an increase of peak inversion moment value (0.04 Nm/kg) of the ankle joint compared to all other FPA conditions [20]. As such, ankle moment results of previous studies in the toe-in gait condition did not match results of this study. The reason for such conflicting results was presumed to be due to differences in the number of study subjects, clinical characteristics of subjects, and inter-individual variability in biomechanical variables such as moments.
Although toe-in gait trials showed a significant decrease in the first peak KAM with a significantly decreased second peak KAM in toe-out walking, clinical application of the FPA walking modification for patients with knee osteoarthritis requires a cautious approach. Because the first peak KAM is more closely related to current clinical symptoms, severity, and prognosis of knee OA than the second peak KAM, the decrease in the first peak KAM is considered more important [16]. However, considering the impact of a 1% increase in KAM on knee OA symptoms [39], it will not be possible to overlook the tendency to increase the first peak KAM during EFP walking condition and the tendency to increase the second peak KAM during IFP walking. Results showed no significant increase in the ankle joint moment value in the stance phase during walking for both 20° toe-in and 20° toe-out modifications. However, in some participants, the IFP gait modification increased the peak ankle adduction moment when ankle joint contact forces peaked. This indicates that for patients with musculoskeletal deficits of the ankle joint such as ankle OA, the effectiveness of toe-in or toe-out walking trials at the ankle joint should be verified case by case before adopting FPA gait to improve the KAM.
The current study has some strengths. Previous studies related to KAM and FPA modifications have investigated effects of foot internal or external rotation condition on kinematics and kinetics of the knee joint itself during gait [5,6,16,23,40]. The study was performed to determine effects on two peak KAMs and 3D moments of the ankle joint using three different FPA modifications in individuals with knee OA through a reliable and objective 3D motion analysis system and force platforms. The present study showed that in participants with mild or moderate knee OA, FPA walking modifications affected peak KAMs without affecting the increase in peak ankle moment. Therefore, clinical application of FPA modification should be approached cautiously through quantitative analysis of the two peak KAMs in patients with knee osteoarthritis. Although abnormally high the peak KAM is a risk factor for medial compartment knee OA, abnormally reduced peak KAM might also be a risk factor for lateral compartment knee OA [23]. Limitations of this study are as follows. Because most participants had mild knee OA without severe knee pain or clinical symptoms, results of this study cannot be applied to all knee OA patients. In addition, various research methodological techniques were used to apply consistent FPA walking modifications. However, there were difficulties with consistency in some walking trials. Future research will need to verify the impact of clinical application of walking aids such as foot and ankle orthoses or insoles and integrated intervention of gait modification retraining on the first and second peak KAMs and biomechanics of lower extremity joints.
5. Conclusions
In conclusion, this study showed that IFP walking modification reduced the first peak KAM and that EFP walking reduced the second peak KAM. Additionally, any type of FPA modification conditions did not affect the increase in ankle moment. However, the impact of this FPA walking retraining intervention on other types of knee musculoskeletal disorders such as lateral compartment knee OA cannot be overlooked. Therefore, clinical application of toe-in or toe-out gait modification to patients with knee osteoarthritis should be performed based on biomechanical evaluations such as peak KAM. It is also necessary to consider additional applications of foot and ankle orthoses or modified insoles, which have a positive impact on clinical intervention.
References
- Yang, G.; Wang, J.; Liu, Y.; Lu, H.; He, L.; Ma, C.; Zhao, Z. Burden of knee osteoarthritis in 204 countries and territories, 1990–2019: Results from the global burden of disease study 2019. Arthritis Care Res. 2023, 75, 2489–2500. [Google Scholar] [CrossRef]
- Deshpande, B.R.; Katz, J.N.; Solomon, D.H.; Yelin, E.H.; Hunter, D.J.; Messier, S.P.; Suter, L.G.; Losina, E. Number of persons with symptomatic knee osteoarthritis in the us: impact of race and ethnicity, age, sex, and obesity: symptomatic knee OA in the US. Arthritis Care Res. 2016, 68, 1743–1750. [Google Scholar] [CrossRef]
- Kim, Y.; Richards, J.; Lidtke, R.H.; Trede, R. Characteristics of clinical measurements between biomechanical responders and non-responders to a shoe designed for knee osteoarthritis. Gait Posture 2018, 59, 23–27. [Google Scholar] [CrossRef]
- D’Souza, N.; Charlton, J.; Grayson, S.; Kobayashi, L.; Hutchison, M.; Hunt, M.; Simic, M. Are biomechanics during gait associated with the structural disease onset and progression of lower limb osteoarthritis? A systematic review and meta-analysis. Osteoarthritis Cartilage 2022, 30, 381–394. [Google Scholar] [CrossRef]
- Hutchison, L.; D'Souza, N.; Grayson, J.; Hiller, C.; Kobayashi, S.; Simic, M. Toe-in and toe-out gait retraining interventions to reduce proxy measures of medial knee joint load in people with medial knee osteoarthritis: Protocol for a randomised placebo-controlled trial. Contemp. Clin. Trials 2023, 134, 107355. [Google Scholar] [CrossRef]
- Guo, M.; Axe, M.J.; Manal, K. The influence of foot progression angle on the knee adduction moment during walking and stair climbing in pain free individuals with knee osteoarthritis. Gait Posture 2007, 26, 436–441. [Google Scholar] [CrossRef]
- Seagers, K.; Uhlrich, S.D.; Kolesar, J.A.; Berkson, M.; Kaneda, J.M.; Beaupre, G.S.; Delp, S.L. Changes in foot progression angle during gait reduce the knee adduction moment and do not increase hip moments in individuals with knee osteoarthritis. J. Biomech. 2022, 141, 111204. [Google Scholar] [CrossRef]
- Chehab, E.F.; Favre, J.; Erhart-Hledik, J.C.; Andriacchi, T.P. Baseline knee adduction and flexion moments during walking are both associated with 5-year cartilage changes in patients with medial knee osteoarthritis. Osteoarthritis Cartilage 2014, 22, 1833–1839. [Google Scholar] [CrossRef]
- Robbins, S.M.; Birmingham, T.B.; Callaghan, J.P.; Jones, G.R.; Chesworth, B.M.; Maly, M.R. Association of pain with frequency and magnitude of knee loading in knee osteoarthritis. Arthritis Care Res. 2011, 63, 991–997. [Google Scholar] [CrossRef]
- Hurwitz, D.E.; Ryals, A.B.; Case, J.P.; Block, J.A.; Andriacchi, T.P. The knee adduction moment during gait in subjects with knee osteoarthritis is more closely correlated with static alignment than radiographic disease severity, toe out angle and pain. J. Orthop. Res. 2002, 20, 101–107., 63, 405-426. [Google Scholar] [CrossRef]
- Hinman, R.S.; Wrigley, T.V.; Metcalf, B.R.; Hunter, D.J.; Campbell, P.; Paterson, K.; Staples, M.P.; Bennell, K.L. Unloading shoes for osteoarthritis of the knee: protocol for the SHARK randomised controlled trial. BMC Musculoskelet. Disord. 2014, 15, 48. [Google Scholar] [CrossRef]
- Simic, M.; Hinman, R.S.; Wrigley, T.V.; Bennell, K.L.; Hunt, M.A. Gait modification strategies for altering medial knee joint load: a systematic review. Arthritis Care Res. (Hoboken) 2011. [Google Scholar] [CrossRef]
- Kepple, T.M.; Segel, K.L.; Stanhope, S.J. Relative contributions of the lower extremity joint moments to forward progression and support during gait. Gait Posture 1997, 6, 1–8. [Google Scholar] [CrossRef]
- Ro, D.H.; Lee, J.; Lee, J.; Park, J.Y.; Han, H.S.; Lee, M.C. Effects of knee osteoarthritis on hip and ankle gait mechanics. Adv. Orthop. 2019, 2019, 9757369. [Google Scholar] [CrossRef]
- Wang, J.W.; Kuo, K.N.; Andriacchi, T.P.; Galante, J.O. The influence of walking mechanics and time on the results of proximal tibial osteotomy. J. Bone Joint Surg. Am. 1990, 72, 905–909. [Google Scholar] [CrossRef]
- Shull, P.B.; Shultz, R.; Silder, A.; Dragoo, J.L.; Besier, T.F.; Cutkosky, M.R.; Delp, S.L. Toe-in gait reduces the first peak knee adduction moment in patients with medial compartment knee osteoarthritis. J. Biomech. 2013, 46, 122–128. [Google Scholar] [CrossRef]
- Mündermann, A.; Dyrby, C.O.; Andriacchi, T.P. Secondary gait changes in patients with medial compartment knee osteoarthritis: Increased load at the ankle, knee, and hip during walking. Arthritis Rheum. 2005, 52, 2835–2844. [Google Scholar] [CrossRef]
- Legrand, T.; Younesian, H.; Equey, N.; Campeau-Lecours, A.; Turcot, K. Trunk lean and toe out gait strategies impact on lower limb joints. J. Biomech. 2021, 129, 110740. [Google Scholar] [CrossRef]
- Wesseling, M.; de Groote, F.; Meyer, C.; Corten, K.; Simon, J.P.; Desloovere, K.; Jonkers, I. Gait alterations to effectively reduce hip contact forces. J. Orthop. Res. 2015, 33, 1094–1102. [Google Scholar] [CrossRef]
- Charlton, J.M.; Hatfield, G.L.; Guenette, J.A.; Hunt, M.A. Ankle joint and rearfoot biomechanics during toe-in and toe-out walking in people with medial compartment knee osteoarthritis. PM R. 2019, 11, 503–511. [Google Scholar] [CrossRef]
- Kim, Y. Effects of foot-toe orthoses on moment and range of motion of knee joint in individuals with hallux valgus. Life (Basel) 2023, 13, 1162. [Google Scholar] [CrossRef]
- Collins, T.D.; Ghoussayni, S.N.; Ewins, D.J.; Kent, J.A. A six degrees-of-freedom marker set for gait analysis: repeatability and comparison with a modified Helen Hayes set. Gait Posture 2009, 30, 173–180. [Google Scholar] [CrossRef]
- Lynn, S.K.; Kajaks, T.; Costigan, P.A. The effect of internal and external foot rotation on the adduction moment and lateral-medial shear force at the knee during gait. J. Sci. Med. Sport 2008, 11, 444–451. [Google Scholar] [CrossRef]
- Dainese, P.; Wyngaert, K.V.; De Mits, S.; Wittoek, R.; Van Ginckel, A.; Calders, P. Association between knee inflammation and knee pain in patients with knee osteoarthritis: a systematic review. Osteoarthritis Cartilage 2022, 30, 516–534. [Google Scholar] [CrossRef]
- Hall, M.; Bennell, K.L.; Wrigley, T.V.; Metcalf, B.R.; Campbell, P.K.; Kasza, J.; Paterson, K.L.; Hunter, D.J.; Hinman, R.S. The knee adduction moment and knee osteoarthritis symptoms: relationships according to radiographic disease severity. Osteoarthritis Cartilage 2017, 25, 34–41. [Google Scholar] [CrossRef]
- Thorp, L.E.; Sumner, D.R.; Block, J.A.; Moisio, K.C.; Shott, S.; Wimmer, M.A. Knee joint loading differs in individuals with mild compared with moderate medial knee osteoarthritis. Arthritis Rheum. 2006, 54, 3842–3849. [Google Scholar] [CrossRef]
- Lindsey, B.; Eddo, O.; Caswell, S.V.; Prebble, M.; Cortes, N. Reductions in peak knee abduction moment in three previously studied gait modification strategies. Knee 2020, 27, 102–110. [Google Scholar] [CrossRef]
- Hunt, M.A.; Simic, M.; Hinman, R.S.; Bennell, K.L.; Wrigley, T.V. Feasibility of a gait retraining strategy for reducing knee joint loading: increased trunk lean guided by realtime biofeedback. J. Biomech. 2011, 44, 943–947. [Google Scholar] [CrossRef]
- Shull, P.B.; Silder, A.; Shultz, R.; Dragoo, J.L.; Besier, T.F.; Delp, S.L.; Cutkosky, M.R. Six-week gait retraining program reduces knee adduction moment, reduces pain, and improves function for individuals with medial compartment knee osteoarthritis. J. Orthop. Res. 2013, 31, 1020–1025. [Google Scholar] [CrossRef]
- Eddo, O.; Lindsey, B.; Caswell, S.V.; Cortes, N. Current evidence of gait modification with real-time biofeedback to alter kinetic, temporospatial, and function-related outcomes: a review. International Journal of Kinesiology and Sports Science 2017, 5, 35–55. [Google Scholar] [CrossRef]
- Wheeler, J.W.; Shull, P.B.; Besier, T.F. Real-time knee adduction moment feedback for gait retraining through visual and tactile displays. J. Biomech. Eng. 2011, 133, 041007. [Google Scholar] [CrossRef]
- Lynn, S.K.; Costigan, P.A. Effect of foot rotation on knee kinetics and hamstring activation in older adults with and without signs of knee osteoarthritis. Clin. Biomech. (Bristol, Avon) 2008, 23, 779–786. [Google Scholar] [CrossRef]
- Hurwitz, D.E.; Ryals, A.B.; Case, J.P.; Block, J.A.; Andriacchi, T.P. The knee adduction moment during gait in subjects with knee osteoarthritis is more closely correlated with static alignment than radiographic disease severity, toe out angle and pain. J. Orthop. Res. 2002, 20, 101–107. [Google Scholar] [CrossRef]
- Lin, C.J.; Lai, K.A.; Chou, Y.L.; Ho, C.S. The effect of changing the foot progression angle on the knee adduction moment in normal teenagers. Gait Posture 2001, 14, 85–91. [Google Scholar] [CrossRef]
- Baliunas, A.J.; Hurwitz, D.E.; Ryals, A.B.; Karrar, A.; Case, J.P.; Block, J.A.; Andriacchi, T.P. Increased knee joint loads during walking are present in subjects with knee osteoarthritis. Osteoarthritis Cartilage. 2002, 10, 573–579. [Google Scholar] [CrossRef]
- Costigan, P.A.; Deluzio, K.J.; Wyss, U.P. Knee and hip kinetics during normal stair climbing. Gait Posture 2002, 16, 31–37. [Google Scholar] [CrossRef]
- Gok, H.; Ergin, S.; Yavuzer, G. Kinetic and kinematic characteristics of gait in patients with medial knee arthrosis. Acta. Orthop. Scand. 2002, 73, 647–52. [Google Scholar] [CrossRef]
- Kaufman, K.R.; Hughes, C.; Morrey, B.F.; Morrey, M.; An, K.N. Gait characteristics of patients with knee osteoarthritis. J. Biomech. 2001, 34, 907–915. [Google Scholar] [CrossRef]
- Baghaei Roodsari, R.; Esteki, A.; Aminian, G.; Ebrahimi, I.; Mousavi, M.E.; Majdoleslami, B.; Bahramian, F. The effect of orthotic devices on knee adduction moment, pain and function in medial compartment knee osteoarthritis: A literature review. Disabil. Rehabil. Assist. Technol. 2017, 12, 441–449. [Google Scholar] [CrossRef]
- Simic, M.; Wrigley, T.V.; Hinman, R.S.; Hunt, M.A.; Bennell, K.L. Altering foot progression angle in people with medial knee osteoarthritis: the effects of varying toe-in and toe-out angles are mediated by pain and malalignment. Osteoarthritis Cartilage 2013, 21, 1272–1280. [Google Scholar] [CrossRef]
Figure 4.
Mean and standard deviation of knee adduction moment for all three foot rotation positions in stance phase during gait. *, Significant main effect for foot progression angle position at p < 0.01.
Figure 4.
Mean and standard deviation of knee adduction moment for all three foot rotation positions in stance phase during gait. *, Significant main effect for foot progression angle position at p < 0.01.
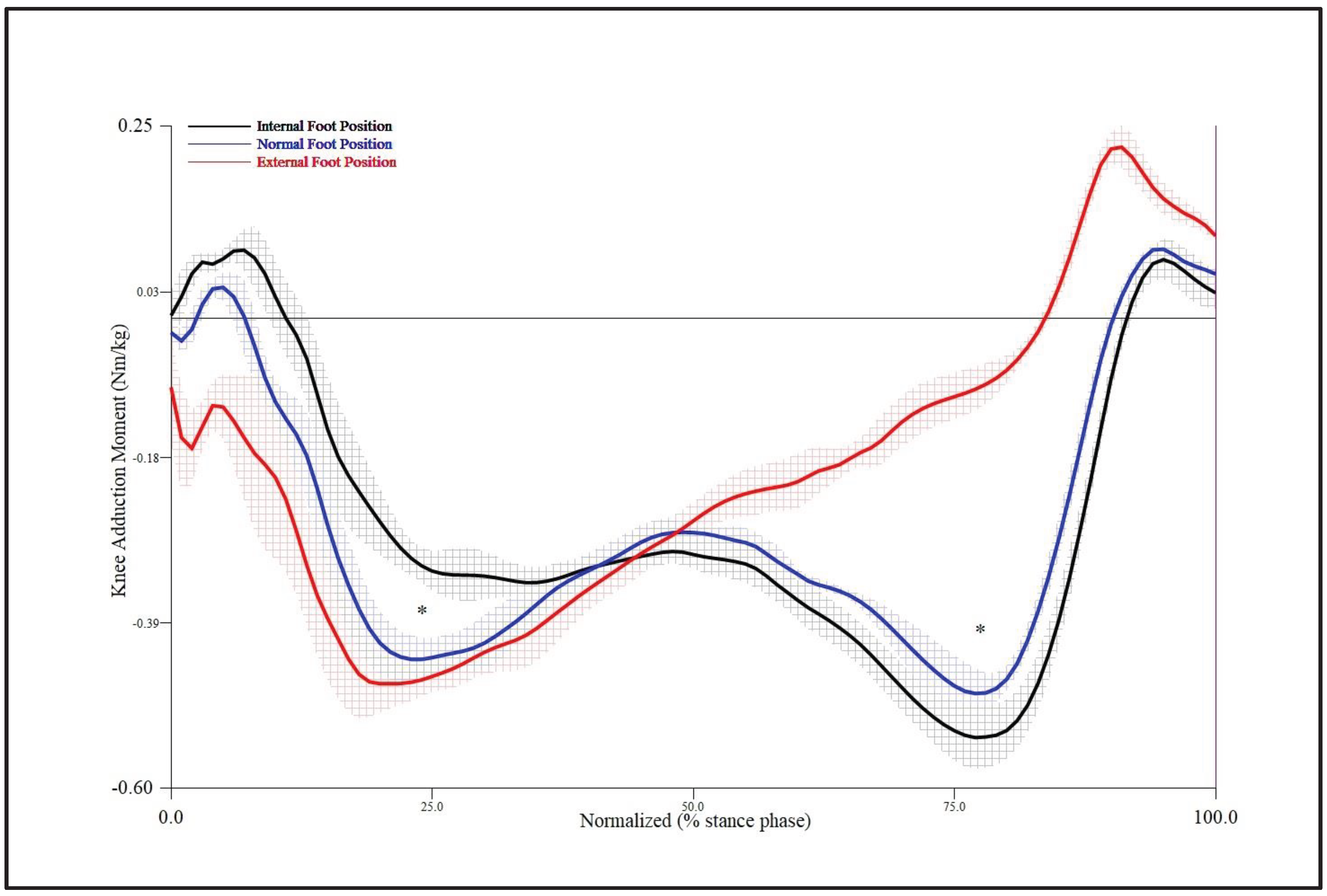

Table 1.
General characteristics of study participants (standard deviation (SD) is presented in parentheses).
Table 1.
General characteristics of study participants (standard deviation (SD) is presented in parentheses).
| Characteristics (N=35) | Mean (SD) |
|---|---|
| Age (yr) | 61.2 (2.1) |
| Height (cm) | 159.3 (9.5) |
| Weight (kg) | 64.8 (10.2) |
| Gender | Male: 9, Female: 26 |
| Foot rotation angle (deg) | NFP: 17.84 (7.12), IFP: -10.09 (5.55), EFP: 42.76 (6.80) |
| Velocity (m/s) | NFP: 1.19 (0.13), IFP: 1.16 (0.13), EFP: 1.20 (0.14) |
NFP: normal foot position; IFP: internal foot position; EFP: external foot position.
Table 2.
Comparisons of peak knee moments of coronal plane by foot progression angle and knee side in stance phase during gait.
Table 2.
Comparisons of peak knee moments of coronal plane by foot progression angle and knee side in stance phase during gait.
| Moment values | Level | F | p-value |
|---|---|---|---|
| Knee adduction moment ait 1st peak 0-25% stance (Nm/kg) |
Foot positions | 9.753 | 0.003 |
| Knee sides | 1.375 | 0.218 | |
| Positions*sides | 2.540 | 0.101 | |
| Knee adducton moment at mid stance 25-70% stance (Nm/kg) | Foot positions | 0.984 | 0.326 |
| Knee sides | 0.077 | 0.734 | |
| Positions*sides | 0.183 | 0.657 | |
| Knee adduction moment at 2nd peak 75-100% stance (Nm/kg) | Foot positions | 27.624 | 0.000 |
| Knee sides | 1.779 | 0.166 | |
| Positions*sides | 1.343 | 0.255 |
Table 3.
Mean (SD) values of knee adduction moments presented for all three foot progression coditions in stance phase during gait.
Table 3.
Mean (SD) values of knee adduction moments presented for all three foot progression coditions in stance phase during gait.
| Moment values (Nm∙kg-1) | NFP | IFP | EFP | p-value |
|---|---|---|---|---|
| 1st peak knee adduction moment at around 25% stance | -0.42* (0.11) | -0.34 (0.08) | -0.47 (0.10) | 0.003 |
| Knee adducton moment at mid 50% stance | -0.27 (0.09) | -0.30 (0.08) | -0.27 (0.09) | 0.326 |
| 2nd peak knee adduction moment at around 75% stance | -0.44† (0.14) | -0.50 (0.16) | -0.11 (0.11) | 0.000 |
*Significant difference between NFP and IFP conditions, p < 0.01. †Significant difference between NFP and EFP conditions, p < 0.01. NFP: normal foot position; IFP: internal foot position; EFP: external foot position.
Table 4.
Repeated measures ANOVA comparing three-dimensional ankle movement by foot rotation conditions and foot side during gait.
Table 4.
Repeated measures ANOVA comparing three-dimensional ankle movement by foot rotation conditions and foot side during gait.
| Ankle moment (Nm∙kg-1) | Level | F | p-value |
|---|---|---|---|
| Dorsiflexion moment peak 0-50% stance |
Foot position | 0.761 | 0.486 |
| Ankle sides | 1.122 | 0.299 | |
| Positions*sides | 2.744 | 0.078 | |
| Plantar flexion moment peak 50-100% stance |
Foot position | 0.529 | 0.571 |
| Ankle sides | 1.161 | 0.254 | |
| Positions*sides | 0.188 | 0.815 | |
| Inversion moment peak 50-75% stance |
Foot position | 6.107 | 0.019 |
| Ankle sides | 1.230 | 0.281 | |
| Positions*sides | 0.019 | 0.843 | |
| Eversion moment peak 0-50% stance |
Foot position | 2.347 | 0.102 |
| Ankle sides | 0.294 | 0.758 | |
| Positions*sides | 1.003 | 0.359 | |
| Internal rotation moment peak 0-50% stance |
Foot position | 0.888 | 0.390 |
| Ankle sides | 0.554 | 0.568 | |
| Positions*sides | 0.290 | 0.692 | |
| External rotation moment peak 50-100% stance |
Foot position | 1.453 | 0.197 |
| Ankle sides | 0.482 | 0.475 | |
| Positions*sides | 2.111 | 0.120 |
Table 5.
Mean (SD) ankle moment values presented for all three foot progression coditions in stance phase during gait.
Table 5.
Mean (SD) ankle moment values presented for all three foot progression coditions in stance phase during gait.
| Ankle moment (Nm∙kg-1) | NFP | IFP | EFP |
|---|---|---|---|
| Dorsiflexion peak 0-50% stance | 0.18 (0.08) | 0.18 (0.09) | 0.17 (0.09) |
| Plantarflexion peak 50-100% stance | -1.34 (0.26) | -1.34 (0.27) | -1.37 (0.26) |
| Inersion peak 50-75% stance | -0.09* (0.04) | -0.11 (0.06) | -0.04 (0.05) |
| Eversion peak 0-50% stance | 0.32 (0.26) | 0.32 (0.25) | 0.30 (0.26) |
| Internal rotation peak 0-50% stance | 0.05 (0.08) | 0.05 (0.07) | 0.03 (0.05) |
| External rotation peak 50-100% stance | -0.24 (0.16) | -0.27 (0.19) | 0.23 (0.16) |
*Significant difference between NFP and EFP conditions, p < 0.05. NFP: normal foot position; IFP: internal foot position; EFP: external foot position.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



