Submitted:
21 February 2024
Posted:
25 February 2024
You are already at the latest version
Abstract
Hereditary hemochromatosis (HH) is the main genetic cause of iron overload and is regarded as metal-related human toxicosis. HH may result from HFE and non-HFE gene mutations causing hepcidin deficiency or hepcidin resistance. The disorder has a high biochemical penetrance, but a low clinical prevalence. Unfortunately, the majority of patients with HH remain undiagnosed at their disease-curable stage. The main aim of HH therapy is to prevent iron overload in the early-phase disease and elimination of excess iron from the body by phlebotomy in its late stage. Raising global awareness of HH among health professionals, their training to pay attention to early HH signs and symptoms, and strict patient monitoring are critical management strategies for preventing treatment delays, upgrading its efficacy, and improving patient prognosis.
Keywords:
hereditary hemochromatosis
; iron overload
; HFE gene mutation
; non-HFE gene mutation
; phlebotomy
1. Introduction
Hereditary hemochromatosis (HH) (synonyms: congenital, primary, idiopathic hemochromatosis) is one of the most common human inherited metabolic disorders with a frequency of about 1 in 250 in Caucasians. It is the main genetic cause of iron overload and is regarded as metal-related human toxicosis [1]. The disorder was first described in 1865 by Trousseau, although twenty-four years later, von Recklinghausen, the German pathologist, used the term hemochromatosis [2,3]. In 1996 Feder et al. confirmed the location of the HFE gene on the short arm of chromosome 6 [4]. The HFE gene is responsible for proper iron absorption in the gastrointestinal (GI) tract. Iron delivery to the blood is controlled by a peptide hormone hepcidin synthesized by hepatocytes and secreted into the blood plasma. A detailed description of cellular and tissue regulation of iron homeostasis is available elsewhere [5,6,7,8]. Briefly, hepcidin binding to ferroportin, which remains the only cellular iron exporter identified in humans, blocks iron transport. In normal conditions, ferroportin exports iron from duodenal enterocytes that absorb dietary iron, iron-recycling macrophages in the spleen and the liver and iron-storing hepatocytes [9]. The hepcidin-ferroportin axis is engaged in systemic iron homeostasis by influencing hepatic hepcidin synthesis. Due to genetic mutations that cause hepcidin deficiency or disrupt its binding to ferroportin, dietary iron absorption increases [10]. HFE gene mutations lead not only to enhanced iron uptake and its increased plasma concentrations, but also to progressive iron deposition in the cytoplasm of parenchymal cells of various organs and tissues (particularly hepatocytes, pancreatic cells, cardiomyocytes, skin, joints, and other organs) causing deleterious complications with multi-organ damage years later if untreated [11,12]. The toxic impact of surplus iron stems from the development of oxidative stress and the production of free oxygen radicals (i.e., hydroxyl and peroxide radicals in the Fenton and Haber-Weiss reactions) which destroy intracellular organelle membranes, trigger DNA strand breaks, and lead to cell injury. The usual body antioxidant defense mechanisms that involve glutathione peroxidase, catalase, and superoxide dismutase are exhausted in the course of HH [13,14,15]. As a consequence, DNA damage occurs with subsequent impairment of protein synthesis and deterioration in cellular integrity.
Some factors may modify the natural course of the disease, its prevalence, and severity. They include individual patient features (age, gender, comorbidities) and environmental triggers (alcohol consumption, smoking, hepatotropic virus infections, hepatotoxic drugs, etc.) [16,17].
Although the genetic defect is present at birth, signs and symptoms of HH rarely occur until adulthood. Most individuals remain asymptomatic throughout their lives. Signs and symptoms of the disease in C282Y homozygotes usually occur over the age of 40 in men and the age of 50 in women [18]. The disorder has a high biochemical penetrance, but a low clinical prevalence. Recent studies indicate that only 10-33% of C282Y homozygotes present with overt disease, and less frequently women (probably due to the physiological loss of iron during menstruation and pregnancy). Nevertheless, HH remains a relevant illness due to its high prevalence in the Caucasian population. Also, the results of a recent study confirmed that C282Y homozygotes experience higher death and complication rates than individuals without HFE mutations, even despite treatment by phlebotomy [19].
Iron concentration is tightly regulated in the human body. As mentioned before, most dietary iron absorption takes place through mature enterocytes in the duodenum and upper jejunum [20]. Once absorbed, iron must either be used or stored because humans do not have physiological mechanisms to actively remove iron from the body. The only way to eliminate it is passive loss through menstrual blood, bleeding, exfoliation of epithelium, etc.
Gender-related differences influence the penetration of HH. Men suffer from the disease 2-3 times more often than women and more often present serious complications of the disease including diabetes and liver cirrhosis.
In summary, the main risk factors for overt HH include the following:
- a)
- HFE gene homozygosity – the greatest risk factor;
- b)
- positive family history for HH in the first-line relatives;
- c)
- Northern European ethnicity – the disease is less prevalent in populations of Afro-American, Hispanic, and Asian origin;
- d)
- male gender – men are susceptible to developing HH symptoms at an earlier age, however, females’ risk increases after menopause or a hysterectomy.
2. Gene mutations in hereditary hemochromatosis
Three main mutations of the HFE gene have been described. The most common of them is C282Y, when cysteine replaces tyrosine in position 282 of the HFE gene. This type of mutation occurs most often in the population of Northern Europe (1 in 220-250 individuals). The homozygosity of C282Y is observed in 0.3%-0.6% of the European population and is responsible for signs of iron overload in 90% of Caucasians [21,22]. The second mutation, which, in combination with C282Y, is responsible for another 5% of cases of primary hemochromatosis is H63D (substitution of histidine instead of aspartamine). The global prevalence of C292Y was estimated at 1.9%; H63D at 8.1%; and mixed heterozygosity C282Y/H63D at 1.97%. About 10% of the entire population are carriers of defective genes. The third HFE mutation was confirmed at nucleotide 193, where serine is replaced by cysteine at position 65 (S65C). Unlike C282Y/C282Y, homozygosity for H63D or S65C usually leads to mild disease or no clinical consequences at all.
3. The classification of hereditary hemochromatosis
Until recently, the classification of hemochromatosis was based on criteria that included the type of genetic defect and the age at which disease symptoms appear. In 2022 new recommendations for HH classification have been developed by panelists of the International Society for the Study of Iron in Biology and Medicine (BIOIRON Society), during a meeting in Heidelberg, Germany. The classification presented in Table 1 addresses both clinical issues and molecular complexity [25].
According to novel classification, if a patient presents with convincing features of HH phenotype without cofactors but is not a p.Cys282Tyr homozygote (or compound p.Cys282Tyr/p.His63Asp heterozygote, or p.His63Asp homozygote), a temporary diagnosis of “molecularly undefined” HH can be established, and treatment (phlebotomies) can be started. New HH classification takes into account the challenge of molecular clarification and facilitates medical communication.
4. Clinical presentation of hereditary hemochromatosis
Some individuals with HH never present the disease signs and symptoms. Homozygosity or compound heterozygosity (heterozygosity for two separate mutations) for HFE gene mutations does not ensure that the affected individual will develop signs and symptoms of iron overload in their lifetime. Furthermore, heterozygous carriers of single HFE gene mutations are not at risk of developing overt disease [26,27].
Women are more likely to develop HH symptoms after menopause when they no longer lose iron with menstruation and pregnancy. Since clinical signs of overt iron overload in homozygotes develop in adult life, testing in children is not recommended until the age of 18 [26,28].
Diagnosis of HH may be challenging due to the variety of clinical symptoms, although a common initial presentation is a symptomless patient with mildly elevated liver enzymes. The most common HH signs and symptoms are presented in Table 2.
4.1. Hereditary hemochromatosis and the skeletomuscular system
Fatigue and joint pain occur as the most common symptoms in the early phase of the disease. The majority of patients with HH develop a typical arthropathy, as described by Schumacher in 1964 in the metacarpophalangeal (MCP) and proximal interphalangeal (PIF) joints [29]. Arthropathy related to HH can affect different joints, but most frequently the 2nd/3rd MCP and the ankle joints, followed by the knee and hip [30]. Ankle arthropathy confirmed in 32–61% of HH patients can lead to foot pain during walking, swelling, and impairment of the range of motion (ROM) of the ankle [31]. It occurs frequently as the first manifestation of the disease [32]. There are no particular clinical features or radiological findings to reliably differentiate HH arthropathy from primary osteoarthritis of the ankle joint. The diagnosis is mostly based on the patient’s history [31].
4.2. Hereditary hemochromatosis and the central nervous system
Patients with HH may present with a lack of energy (lethargy), irritability, memory fog, mood swings, depression, and anxiety. Moreover, due to iron deposition in the brain, movement disorders (including those similar to Parkinson’s disease or chorea) and tremors may (rarely) occur [33,34]. Topiwala et al. found that alcohol consumption above 7 units weekly was associated with higher brain iron. Higher basal ganglia iron deposits were related to slower executive function, lower fluid intelligence, and slower reaction time. The authors indicate that iron accumulation may represent a potential mechanism for alcohol-related cognitive decline [35]. Therefore, abnormal iron homeostasis in patients with HH may be worsened by alcohol consumption leading to overt motor and cognitive impairment.
4.3. Hereditary hemochromatosis and the liver
Liver damage most frequently occurs in HFE-related hemochromatosis [21]. The clinical presentation is diverse: from asymptomatic increase of blood ALT and AST activity, through non-specific epigastric pain in the right upper quadrant of the abdomen, to signs of end-stage liver disease. SF below 1000 ng/ml at the time of HH diagnosis identifies patients at low risk of advanced liver fibrosis [26]. Several studies have confirmed the association between alcohol intake and liver cirrhosis development in HH patients. Alcohol was found to down-regulate hepcidin expression both in vitro in hepatoma cells, as well as in vivo in mice subjected to short-term alcohol exposure [36]. Therefore, hepcidin-associated mechanisms that guard the body against the detrimental impact of iron overload are disrupted by alcohol intake [37]. As reported elsewhere, both iron and alcohol consumption lead to oxidative stress and lipid peroxidation and the liver is more vulnerable to oxidative conditions in comparison to other organs and tissues [38]. Recent reports indicate that HH subjects who drink more than 60 g of alcohol per day are approximately 9 times more likely to develop liver cirrhosis, and drinking more than 80 g per day significantly reduces patient survival [39,40]. There is data on the development of fulminant hepatic failure in a young patient with minimal alcohol consumption [41].
Risk factors associated with advanced liver disease in the course of HH are presented in Table 3.
Patients with HH and liver cirrhosis are also at increased risk of hepatocellular carcinoma (HCC), which leads to about 45% of deaths in this population. The relative risk of developing malignancy in the course of HH is 20–200%, and the risk factor is SF >2000 ng/ml. The 10-year incidence of HCC in patients with liver cirrhosis secondary to HH is 6–10%, higher in men than in women [42]. However, the most recent report by Schaefer et al. after an investigation of a total of 8839 individuals from the Austrian region of Tyrol revealed that HCC incidence was not significantly higher in p.C282Y homozygotes than in controls matched for age and sex [43]. Recommendations for HCC screening in patients with liver cirrhosis due to HH are the same as in cirrhotics of other etiology, this is an ultrasound examination every 6 months with or without α-fetoprotein (AFP) measurement [44]. HCC is very rare in the absence of cirrhosis, but HH is a risk factor and patients should be closely monitored for any signs and symptoms suggestive of malignancy even after the excess iron removal as the risk of HCC remains increased [45]. Therefore, the aforementioned reports support the implementation of cancer screening programs in the majority of patients with overt HH. Currently, based on international guidelines, the diagnosis of HCC (regardless of its etiology) relies on non-invasive criteria (multiphasic contrast-enhanced CT and MRI scanning) [44]. In a retrospective study of HH patients with the C282Y mutation, Bardou-Jacquet E. et al. found that severe liver fibrosis can regress with treatment, and in patients with fibrosis regression to a stage F2 or less, the long-term risk for liver cancer was significantly reduced [46].
4.4. Hereditary hemochromatosis and the cardiovascular system
Heart damage in the course of HH may manifest as cardiomyopathy (dilated or restrictive), arrhythmias (including sinus node dysfunction and atrial fibrillation), and heart failure. Initial hypertrophy, diastolic dysfunction, heart dilatation, systolic dysfunction, and arrhythmias are possible clinical presentations of cardiac HH [47]. From the moment of symptoms of heart failure, the prognosis remains poor. Cardiomyopathy is the second most common cause of death in patients with HH. Therefore, it is crucial to prevent heart complications in advance at the preclinical phase of the disease [48,49]. In their retrospective study, Cortés et al. found that patients with a C282Y/H63D genetic mutation had a higher frequency of myocardial infarction, yet this mutation was associated with reduced odds of diastolic dysfunction compared to other genetic mutations in patients with a normal left ventricular ejection fraction (LVEF). No specific HFE genetic mutation was associated with LVEF < 55% [50]. Electrocardiography (ECG) is not very useful as a diagnostic tool since the alterations occur in the late stage of cardiac HH. They are not specific and may include signs of left ventricle hypertrophy, low QRS voltage, nonspecific ST-T changes, and atrioventricular, supraventricular (mostly atrial fibrillation), or ventricular arrhythmias. The best non-invasive method for detecting heart involvement in a patient with HH is echocardiography. Phlebotomy leads to significant improvement in cardiac parameters, including twist and torsion of the LV [47]. Emerging evidence indicates that ferroptosis which is a novel non-apoptotic cell death characterized by iron-dependence and the accumulation of lipid peroxidation causing membrane damage plays a relevant role in the development of HH-associated cardiomyopathy [51].
4.5. Hereditary hemochromatosis and the endocrine system
Diabetes in HH develops as a result of pancreatic islet damage by iron overload as well as insulin resistance secondary to liver injury [52,53]. As reported, high iron content is a risk factor for type 2 diabetes mellitus (T2DM) and affects most of its cardinal features: decreased insulin secretion, insulin resistance, and increased hepatic gluconeogenesis [54]. However, SF levels do not predict diabetes in p.C282Y homozygotes. The prevalence of diabetes in p.C282Y homozygotes identified in population screening programs is relatively low [55,56,57,58]. The adoption of HFE genotyping for early HH diagnoses after 1996 could account for the decline in diabetes prevalence. As reported, phlebotomy treatment does not improve diabetes control in HH [59].
The second most common endocrine disorder in the course of HH is hypogonadism, a consequence of selective iron deposition in the pituitary gland leading to impaired secretion of hormones. It occurs most often in adolescent HH. In men, it presents as impotence, loss of libido, and osteoporosis, while women suffer from amenorrhea or premature menopause. Cases of hypopituitarism and alterations of adrenal, thyroid, and parathyroid glands in the course of HH are rare but also reported. Osteoporosis may occur in up to 25% of HH patients [60].
4.6. Hereditary hemochromatosis and the skin
The disease has been called “bronze diabetes” due to the discoloration of the skin and its coexistence with the disease of the pancreas. Hypermelanotic pigmentation is a typical sign of overt disease and is seen in more than 70% of patients. The altered skin color (bronze or gray) is primarily due to melanin rather than iron [61,62]. HH-related pigmentation occurs more often in sun-exposed and/or scarred skin areas. There are correlations between skin manifestations and other signs of the disease. Moreover, porphyria cutanea tarda (PCT) can be associated with hepatic iron overload with HFE gene mutation prevalence of 60-80%. Therefore, if a blistering condition occurs and porphyria is suspected, testing for HFE mutations should be performed to check for HH [63,64]. Also, pigmented purpuric dermatitis and alopecia areata (AA) affecting the beard have been described in a 56-year-old man with C282Y/H63D compound heterozygosity [65]. There are few reports of patients with HH and AA suggesting that AA may be a rare early cutaneous manifestation of HH, but the genetic relationship between the two disorders is currently unclear [66].
4.7. Hereditary hemochromatosis and the immune system
Many patients with HH are affected by immune defects and an increased incidence of autoimmune diseases. Growing evidence has supported an immunological role for HFE with recent studies describing HFE specifically as it relates to MHC I antigen presentation [67]. Since iron overload alters CD8+ T cell function, HH may facilitate patient immunodeficiency and increased risk of infections of Listeria monocytogenes, Yersinia enterocolitica, Escherichia coli, and Vibrio vulnificus [68].
A recent report indicates that the p.C282Y mutation increased the risk of SARS-COV-2 infection in the Czech population [69]. Nevertheless, the other study revealed that HFE polymorphisms do not affect susceptibility/resistance to SARS-CoV-2 infection or the clinical COVID-19 course in patients with altered iron parameters [70]. In general, oral iron supplementation during infection increases mortality in humans [71]. Growing evidence indicates that hyperferritinemia, regardless of the underlying pathology, is associated with high mortality [72,73]. As a marker of significant macrophage activation and reticuloendothelial system activation, it is related to multiple organ dysfunction [74].
5. Diagnostic approach to the patient with suspected iron overload
Timely management of individuals with suggestive laboratory and/or clinical presentation of iron overload enables early diagnosis, successful treatment, and prevention of serious complications. Diagnosis of HH is noninvasive and includes clinical examination, evaluation of blood iron parameters, imaging procedures, and genetic testing. Since iron overload may be caused by a variety of hereditary or acquired factors, the disease requires a differential diagnosis with other common causes of iron overload, such as alcohol-associated liver disease, hepatitis C virus (HCV) infection, or metabolic dysfunction-associated steatotic liver disease (MASLD), formerly known as non-alcoholic fatty liver disease (NAFLD) [75]. Moreover, history of multiple transfusions (ß-thalassemia major, MDS); excessive parenteral iron supplementation (chronic digestive bleeding, chronic renal failure); ineffective erythropoiesis as well as non-HH genetic iron overload (ferroportin disease, hereditary aceruloplasminemia) should be also excluded. The differential diagnosis in a patient with clinical presentation of iron overload is presented in Figure 1.
The diagnostic approach to a patient with HH suspicion may be challenging. Early disease symptoms such as stiff joints and fatigue are nonspecific for HH and may be observed also in other disorders. Since the only alterations seen in the majority of individuals with HFE mutation are high blood iron levels, the disease may be recognized coincidentally based on incorrect results of blood tests done for other indications or when screening family members of patients diagnosed with the disease. As a rule, patients with signs and symptoms suggestive of HH, or positive family history should be referred for the assessment of serum iron parameters.
5.1. Blood tests
The first step in the diagnostic approach for HH suspicion is the assessment of serum transferrin saturation and serum ferritin. These are two crucial tests to detect iron overload:
- Serum transferrin saturation (TSAT) - the ratio between serum iron and total iron-binding capacity (TIBC), expressed as a percentage; increased transferrin saturation (>45%) is the earliest biochemical sign observed in all hemochromatosis subtypes [23]. However, other than iron overload disorders can cause increased transferrin saturation (eg. hemolysis, cytolysis) or decreased blood transferrin concentration (eg. hepatocellular failure, poor nutrition, proteinuria, genetic alterations) [76]. Normal or even low transferrin saturation can be observed in patients with ferroportin disease or hereditary aceruloplasminemia despite overt iron overload [77,78].
- Serum ferritin level (SF) - determining serum ferritin is the simplest and the most used diagnostic tool for body iron storage assessment, even if not a very specific method [79]. Since ferritin is an acute-phase protein, its concentration depends on many factors. Elevated SF levels (≥300 μg/L in men and ≥200 μg/L in women) require precise explanation before they are assigned to iron overload. Other conditions of hyperferritinemia such as metabolic syndrome, alcoholism, inflammation, and marked cytolysis should be ruled out [11]. Nevertheless, SF is an important prognostic factor in patients with HH. It is a predictor of advanced liver fibrosis and cirrhosis in patients with previously diagnosed congenital hemochromatosis.
5.2. Genetic testing
Based on the clinical picture or elevated levels of serum ferritin and transferrin, testing for HFE gene mutations remains a standard and confirmatory step of the diagnostic approach to individuals with HH suspicion. HH results from mutations causing hepcidin deficiency or hepcidin resistance. Both HFE and non-HFE mutations can lead to hepcidin deficiency. HFE-related HH associated with hepcidin deficiency results from the presence of the homozygous C282Y or the heterozygous C282Y/H63D mutations (the so-called compound heterozygote). Homozygosity for HFE C282Y is present in above 80% of patients with clinically overt disease. Neither homozygous nor heterozygous H63D or S65C mutations lead to iron overload and are not relevant for the HH diagnosis [11,26,80]. As indicated, there is no consensus on the diagnostic significance of HFE H63D mutation. The EASL guidelines indicate that H63D should not be considered a disease-causing variant and H63D-affected individuals can be managed based on their clinical signs and symptoms of iron overload, not their genotype alone. Also, environmental and other genetic risk factors should be taken into account in this patient subgroup. However, according to the guidelines, phlebotomy remains the recommended therapy in HH patients who are compound heterozygous C282Y/H63D or homozygous H63D and have proven iron overload (assessed via MRI R2/T2 or liver biopsy) even if results of randomized clinical trials are lacking [26,80].
Non-HFE HH related to hepcidin deficiency is rare and related to genes encoding proteins engaged in the hepcidin synthetic pathway including the hemojuvelin (HJV), hepcidin (HAMP), and transferrin receptor 2 (TFR2) genes. Finally, a rare type of HH related to hepcidin resistance is due to mutations of the ferroportin gene (SLC40A1) that disturb hepcidin-ferroportin interaction [81]. Pathogenic allele frequencies have been estimated to be 74/100,000 for type 2A, 20/100,000 for type 2B, 30/100,000 for type 3, and 90/100,000 for type 4 hemochromatosis classified according to the previous criteria. Although less prevalent, the non-HFE disease can be the cause of iron overload as serious as the HFE type [24]. Consequently, in patients with no C282Y mutation and clinical evidence of iron overload, the basic gene panel is recommended and should cover the following tests: rare HFE mutation, caeruloplasmin (CP), bone morphogenetic protein (BMP6), solute carrier family 40 member 1 (SLC40A1), the genes related to the early disease onset as HAMP and hemojuvelin (HJV) and those connected with abnormal transferrin, transferrin receptor 2 (TFR2) and transferrin (TF), and the hyperferritin-cataract syndrome gene (FTL). Since diagnosis based on gene panels is more easily available, the unbiased confirmation of mutation presence may help to avoid confusion and facilitate family screening [80]. Before genetic testing for non-HFE mutations, other causes of increased iron-related parameters should be excluded (i.e., alcoholic liver disease, MASLD, HCV infection), as they occur more often than the rare HH types 2-4 [82,83].
5.3. Additional diagnostic assessment for hereditary hemochromatosis
Additional diagnostic tests can be helpful to confirm the diagnosis and to look for other HH-related problems:
- Liver enzymes and function tests – the pattern of liver function alterations helps monitor liver damage in the course of HH.
- Liver biopsy – determining the hepatic iron concentration (HIC) is rarely required to establish a final HH diagnosis, therefore liver biopsy has been replaced by genetic testing and imaging findings. Seldom, it may be used to confirm or exclude other co-existing chronic liver diseases and to determine the degree of hepatic fibrosis, especially in C282Y homozygotes with SF >1000 ng/ml. The HIC may also be indicated in cases of suspected genetic iron overload with negative results towards common mutations including C282Y, H63D, and S65C. In remaining cases, liver biopsy is an option for individual consideration [84]. HIC determined in “good quality” biopsy specimen (i.e., sample gross weight ≥1 mg dry weight) is a reliable indicator of whole liver iron concentration [85].
- Magnetic resonance imaging (MRI) - the reference standard imaging modality for the detection and quantification of hepatic iron concentration (HIC); highly sensitive to the presence of tissue iron, the correlation between MRI findings and results of liver biopsy for the detection of moderate to high iron overload was excellent; the imagine technique increasingly adopted as a noninvasive alternative to biopsy for detection, severity grading, and treatment monitoring in patients with known or suspected iron overload [86,87].
6. Screening of healthy people for hereditary hemochromatosis
Genetic screening for HFE-HH is not recommended in the general population. Genetic testing should be considered in patients with chronic liver disease of unclear etiology and TSAT >45% and can be offered to patients with hepatocellular carcinoma (HCC), type 1 diabetes, porphyria cutanea tarda or chondrocalcinosis [22,89]. First-degree relatives, of patients with HFE-related HH should also be tested, not only because of the possible presence of the mutation but also because of the possibility of shared environmental factors that may increase the penetrance of this mutation. For children of one parent confirmed with HFE-related HH, testing for HFE gene mutations in the other parent is recommended. If it is not detected, the child is heterozygous and does not need to be tested. If testing of the other parent is not possible, the child does not need to be diagnosed before the age of 18 because clinical symptoms of HH rarely occur in childhood. Children are not tested for HFE gene mutations before adulthood, even as first-degree relatives of patients with known hereditary hemochromatosis [28].
Results of a recent cross-sectional study conducted on 86,601 participants revealed the possibility of genomic screening to recognize latent iron overload and promote appropriate management. They also confirmed the advantage of population screening for HFE p.Cys282Tyr homozygosity, which was uncovered in 201 participants. Fifty-seven of them (28.4%) were previously diagnosed with HH type 1, and 144 individuals learned of their status through screening [90]. However, further studies are needed to evaluate the value of genomic screening for health outcomes and cost-effectiveness.
7. Treatment of hereditary hemochromatosis
The main aim of HH therapy is to prevent iron overload in the early-phase disease and elimination of excess iron from the body by phlebotomy in its late stage. Since humans have no specific mechanisms of body iron excretion, surplus body iron is most efficiently removed by repeated blood-lettings Therefore, the first-line treatment of choice in HH patients is therapeutic phlebotomy [26]. For homozygotes/compound heterozygotes, an annual routine clinical review to screen for potential symptoms of iron overload (e.g., lethargy, arthralgia, liver disease, cardiac failure/dysrhythmia, testicular atrophy) is recommended.
7.1. Phlebotomy- the first-line treatment for iron depletion
Phlebotomy (venesection or ‘bloodletting’) is the currently recommended treatment for HH [91]. As reported elsewhere, the disease can be treated safely and effectively by removing iron from the body by repeated phlebotomies ordered based on the patient’s age, overall health, and the grade of iron overload. Treatment should be initiated when the presence of iron overload is confirmed based on serum iron parameters: TSAT >45% and ferritin >200 μg/L in females and TSAT >50% and ferritin >300 μg/L in males and postmenopausal women [26].
Initial treatment may require about 500 milliliters of blood removal (each containing 240 - 250 mg iron ) every 1 to 2 weeks. Before each blood removal, the hemoglobin level should be checked and its levels should not decrease below 11 g/dL. If its value is below 11 g/dl, the procedure is temporarily stopped; if it is 11–12 g/dl, the frequency is reduced. The ferritin concentration should be determined after 4 phlebotomies until it reaches 200 µg/l, then every 1–2 phlebotomies until it decreases to 50 µg/l [92]. The next step is maintenance treatment. Once body iron content decreases, blood can be removed less frequently on an as-needed basis, usually two to four times a year. Since elevated TSAT levels persist after iron depletion is achieved, elevated TSAT is not a target of treatment in HFE-related HH. According to the EASL guidelines, targets for phlebotomy are based on ferritin below 50 μg/L in the induction phase and below 100 μg/L in the maintenance phase of treatment [26]. Before blood removal, the patient should be well hydrated, and avoid excessive physical activity for 24 hours after the procedure.
Some patients maintain normal iron levels while others may require blood removals at regular monthly intervals. The schedule of phlebotomies should be tailored individually according to the rate of iron accumulation in the body.
The treatment can help relieve patient signs and symptoms and prevent multi-organ complications observed predominantly in the liver, heart, and pancreas. Phlebotomy may delay the progress of the disease and in some cases even reverse it.
7.2. Erythrocytapheresis as an alternative to phlebotomy
Erythrocytapheresis (EA) is an extracorporeal blood separation procedure by which erythrocytes (RBC) are selectively removed, and the remaining blood is returned to circulation. It aims to rapidly decrease RBC populations or the iron content [93]. In comparison to phlebotomy, EA removes red blood cells more efficiently and diminishes iron overload more rapidly. Therefore, it is cost-effective, particularly in the induction phase of HH therapy - fewer interventions are required in longer treatment intervals. Personalized EA may represent the preferred therapeutic option, if available, for suitable and selected HH patients presenting good antecubital venous access and fair cardiac function [91,94,95]. EA is suggested to be more suitable for subgroups of HH patients with cardiac disease as it is related to insignificant hemodynamic alterations compared with phlebotomy, and individuals with thrombocytopenia or hypoproteinaemia as other than RBCs blood components are returned to the circulation [80].
7.3. Iron chelators as a therapeutic alternative in hereditary hemochromatosis
Iron chelation therapy is not recommended for typical HH. Nevertheless, severe iron overload without proper response to phlebotomies, poor vein conditions and/or severe non-HFE HH (mainly juvenile form), anemia, or heart complications may create contraindications to venesection therapy. Instead, iron chelators may be administered although they are not commonly indicated in hemochromatosis [80,96].
Administration of chelating agents can be oral, IM, or IV to favor the elimination of toxic iron in the urine or the feces through the bile route. In Europe, three iron chelators are available, but availability varies between countries [97]. Iron chelators for clinical use include deferoxamine (DFO), deferiprone (DFP), and deferasirox (DFX). All three aforementioned have been approved by the United States Food and Drug Administration, although each of them has its advantages and disadvantages [98]. The DFO, a nontoxic parenteral iron chelator is approved for long-term treatment in clinical settings. The DFP as an oral medication remains a good alternative for patients who have not responded to DFO or DFX. The DFX is an oral tridentate iron-chelating agent that binds iron in a 2 : 1 ratio [99,100]. Some recent reports indicate that deferasirox therapy is more affordable than traditional deferoxamine therapy [101]. In general, deferasirox is the first choice, followed by deferiprone and deferoxamine in second and third place, respectively [102].
7.4. Proton pump inhibitors - an adjunct therapy for hereditary hemochromatosis?
Proton pump inhibitors (PPIs) have been shown to reduce non-heme iron absorption and can be considered as an adjunct therapy for HH. Results of the recent randomized controlled trial revealed that pantoprazole 40 mg/day versus placebo for 12 months significantly reduced the need for phlebotomies in p.C282Y homozygous patients (p= 0.0052). Given the known long-term safety profile of PPIs, they can be considered a valuable addition to standard HH therapy if medical indications for PPIs are present [103]. The aforementioned results were confirmed by meta-analysis which involved 68 patients with HH (34 in the PPI group and 34 in the placebo or non-PPI group). The minimum duration of PPI treatment was the same (1 year) [104]. However, the routine use of PPIs in the treatment of HH is not recommended.
7.5. Liver transplantation for hereditary hemochromatosis
Liver transplantation (LT) for HH should be considered in patients with end-stage liver dysfunction or HCC. Nevertheless, HH is a very uncommon indication for liver transplantation comprising only about 1% of all transplants [27]. This kind of treatment normalizes iron metabolism due to the proper hepcidin synthesis in the donor’s liver. Recently, based on the United Network for Organ Sharing registry, the analysis of waitlist and post-LT survival in adults with HH without concomitant liver disease from 2003 to 2019 has been published. It revealed, that the post-transplantation short- and long-term survival rates for HH were excellent and comparable with those of other LT recipients [105]. Moreover, patients with HCC and HH can also achieve comparable survival rates to other liver diseases following curative LT. The Barcelona Clinic Liver Cancer (BCLC) staging system accurately stratifies survival and excellent 5-year survival is possible following LT in selected patients [106].
7.6. Recommended lifestyle and diet modifications in patients with hereditary hemochromatosis
Patients who suffer from HH should be educated on how they may reduce the risk of the disease progression, but they should also know and remember that the disease cannot be treated simply by diet. Dietary restrictions should not substitute for iron removal treatment. The recommendations regarding their lifestyle and diet include the following precautions:
- withdrawal of additional iron sources such as iron supplements, iron-containing multivitamins, and iron-fortified foods and drinks (eg. breakfast cereals, sports energy bars, etc.);
- recommendation of a varied vegetarian, semi-vegetarian or flexitarian diet;
- avoidance of vitamin C supplements which increase iron absorption, but there is no need to restrict natural vitamin C in their diet (fruit and vegetables); fruit juices should be consumed between meals;
- recommendation of complete alcohol abstinence as its hepatotoxic impact aggravates liver damage, there is no safe alcohol amount;
Any additional extreme modifications of diet are not usually required for HH patients who receive blood removal treatment. Multicenter, prospective, randomized studies should further clarify the impact of dietary interventions in patients with HH [111].
Patients with iron overload should never stop checking their iron parameters and should be followed lifelong on an out-patient basis
8. Hereditary hemochromatosis in women - pregnancy and fertility issues
HH is not a gender-specific disease, but more males than females present the clinical features of the disease which manifests later in women than in men [112,113].
Therefore, most women may not be aware of the disease until their middle age, often after already passing childbearing years. However, some of them may have a relative with HH and discover their disorder earlier before any signs and symptoms appear. The diagnosis of HH may also be established incidentally while they are examined due to other medical conditions or as part of a routine blood examination. Rarely, women of all ages may develop marks of iron overload and their condition can be detected and confirmed at that time.
A recent retrospective study assessed the impact of HH on maternal and perinatal outcomes in the United States between 2010 and 2019. Data from over 36 million delivery hospitalizations revealed that there was a significant increase in HH prevalence over the studied period. A higher prevalence of gestational hypertensive complications and venous thromboembolism were observed in pregnant women with HH. Moreover, patients with HH had a longer hospital stay and higher total charges [114].
As suggested, pregnancy might temporarily reduce the iron level of a woman (even potentially to the point of anemia). However, this effect does not seem to confer any long-term benefit to overall iron deposits in a woman’s body. Scotet et al. reported that pregnancy status has no impact on iron parameter levels, and is not a protective factor against progressive iron accumulation [115]. Results obtained from the HFE-/- mice animal model also indicate that multiple pregnancies do not reduce body iron stores [116]. These results are consistent with recent experimental data suggesting that the difference in disease expression observed between men and women may be explained by other factors such as hormones [117,118,119].
Pregnant women with mild or moderate iron overload and no signs of advanced liver dysfunction should be carefully assessed for individual therapeutic decisions, but for most of them, phlebotomy can be discontinued during the whole period of pregnancy to avoid sideropenia. One should keep in mind that even women with HH may develop sideropenia during pregnancy. As a rule iron supplements should be avoided in HH, however, if iron deficiency occurs it is recommended that pregnant patients with HH should be treated similarly to other pregnant women.
In the past, pregnant women with HH were thought to have no higher risk of complications in comparison to the general population. Nevertheless, accumulating evidence indicates that feto-maternal complications may occur as a result of iron overload. A recent systematic review revealed that even in the absence of altered iron parameters, HH increased the risk of feto-maternal complications and required prenatal monitoring [120]. As reported, the absorption of lead and iron increases the risk of preeclampsia, gestational hypertension, fetal congenital abnormalities, and growth problems. There is a higher risk of fetal neurodevelopmental delays and childhood leukemia in the course of HH. Therefore, close monitoring of both mother and baby is required in every case with HH mutation.
More research exploring the impact of HH on pregnancy and fertility is required.
9. Future directions in hereditary hemochromatosis
Few studies are being conducted on HH at present. Only 4 currently recruiting trials are registered at the website https://clinicaltrials.gov/. They are focused mainly on the selection of the best criteria in guiding bloodletting and validation of the Magnetic Resonance Imaging (MRI) technique for the assessment of iron deposits in the liver. These trials are presented in Table 4.
10. Conclusions
Untreated HH continues to be a life-threatening disorder that may lead to increased morbidity and mortality due to iron overload. Unfortunately, the majority of patients with HH remain undiagnosed at the disease-curable stage. Undiagnosed, progressive iron accumulation may finally result in liver, heart, and endocrine failure. Therefore, early identification of patients with clinical features suggestive of HH and their appropriate management remain fundamental to preventing disease complications and ensuring normal life expectancy. This goal could be achieved by targeted case detection, although previous population screening studies revealed that HH penetrance is lower than expected [121]. However, screening among at least Caucasian men of Northern European ancestry seems to be reasonable. Raising global awareness of HH among health professionals, their training to pay attention to early HH signs and symptoms, and strict patient monitoring are critical management strategies for preventing treatment delays, upgrading its efficacy, and improving patient prognosis.
References
- Brissot, P.; Cavey, T.; Ropert, M.; Gaboriau, F.; Loréal, O. Hemochromatosis: A Model of Metal-Related Human Toxicosis. Environ. Sci. Pollut. Res. Int. 2018, 25, 2007–2013. [Google Scholar] [CrossRef] [PubMed]
- Bacon, B.R. Hemochromatosis: Discovery of the HFE Gene. Mo. Med. 2012, 109, 133–136. [Google Scholar] [PubMed]
- Von Recklinghausen: Uber Haemochromatose. Taggeblatt... - Google Scholar. Available online: https://scholar.google.com/scholar_lookup?journal=Tagebl+Versamml+Natur+%C3%84rzte+Heidelberg&title=%C3%9Cber+Hamochromatose&author=FD+von+Recklinghausen&volume=62&publication_year=1889&pages=324& (accessed on 18 February 2024).
- Feder, J.N.; Gnirke, A.; Thomas, W.; Tsuchihashi, Z.; Ruddy, D.A.; Basava, A. The Discovery of the New Haemochromatosis Gene. 1996. J Hepatol 2003, 38, 704–709. [Google Scholar] [CrossRef] [PubMed]
- Fleming, R.E.; Ponka, P. Iron Overload in Human Disease. N. Engl. J. Med. 2012, 366, 348–359. [Google Scholar] [CrossRef] [PubMed]
- Ganz, T.; Nemeth, E. Hepcidin and Iron Homeostasis. Biochim. Biophys. Acta 2012, 1823, 1434–1443. [Google Scholar] [CrossRef]
- Camaschella, C.; Nai, A.; Silvestri, L. Iron Metabolism and Iron Disorders Revisited in the Hepcidin Era. Haematologica 2020, 105, 260–272. [Google Scholar] [CrossRef] [PubMed]
- Muckenthaler, M.U.; Rivella, S.; Hentze, M.W.; Galy, B. A Red Carpet for Iron Metabolism. Cell 2017, 168, 344–361. [Google Scholar] [CrossRef]
- Nemeth, E.; Ganz, T. Hepcidin-Ferroportin Interaction Controls Systemic Iron Homeostasis. Int. J. Mol. Sci. 2021, 22, 6493. [Google Scholar] [CrossRef]
- Lal, A. Iron in Health and Disease: An Update. Indian. J. Pediatr. 2020, 87, 58–65. [Google Scholar] [CrossRef]
- Brissot, P.; Pietrangelo, A.; Adams, P.C.; de Graaff, B.; McLaren, C.E.; Loréal, O. Haemochromatosis. Nat. Rev. Dis. Primers 2018, 4, 18016. [Google Scholar] [CrossRef]
- Altés, A.; Sanz, C.; Bruguera, M. Hemocromatosis hereditaria. Probl. En. El Diagnóstico Y Tratamiento. Med. Clínica 2015, 144, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Kawabata, T. Iron-Induced Oxidative Stress in Human Diseases. Cells 2022, 11, 2152. [Google Scholar] [CrossRef] [PubMed]
- Abe, C.; Miyazawa, T.; Miyazawa, T. Current Use of Fenton Reaction in Drugs and Food. Molecules 2022, 27, 5451. [Google Scholar] [CrossRef] [PubMed]
- Bloomer, S.A.; Brown, K.E. Iron-Induced Liver Injury: A Critical Reappraisal. Int. J. Mol. Sci. 2019, 20, 2132. [Google Scholar] [CrossRef] [PubMed]
- Jena, A.B.; Samal, R.R.; Bhol, N.K.; Duttaroy, A.K. Cellular Red-Ox System in Health and Disease: The Latest Update. Biomed. Pharmacother. 2023, 162, 114606. [Google Scholar] [CrossRef] [PubMed]
- Anderson, G.J.; Bardou-Jacquet, E. Revisiting Hemochromatosis: Genetic vs. Phenotypic Manifestations. Ann. Transl. Med. 2021, 9, 731. [Google Scholar] [CrossRef] [PubMed]
- Cathcart, J.; Mukhopadhya, A. European Association for Study of the Liver (EASL) Clinical Practice Guidelines on Haemochromatosis. Frontline Gastroenterol. 2023, 14, 282–286. [Google Scholar] [CrossRef] [PubMed]
- Adams, P.C.; Richard, L.; Weir, M.; Speechley, M. Survival and Development of Health Conditions after Iron Depletion Therapy in C282Y-Linked Hemochromatosis Patients. Can. Liver J. 2021, 4, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Brissot, P.; Troadec, M.-B.; Loréal, O. Intestinal Absorption of Iron in HFE-1 Hemochromatosis: Local or Systemic Process? J Hepatol 2004, 40, 702–709. [Google Scholar] [CrossRef]
- Barton, J.C.; McLaren, C.E.; Chen, W.; Ramm, G.A.; Anderson, G.J.; Powell, L.W.; Subramaniam, V.N.; Adams, P.C.; Phatak, P.D.; Gurrin, L.C.; et al. Cirrhosis in Hemochromatosis: Independent Risk Factors in 368 HFE p.C282Y Homozygotes. Ann. Hepatol. 2018, 17, 871–879. [Google Scholar] [CrossRef]
- Kowdley, K.V.; Brown, K.E.; Ahn, J.; Sundaram, V. ACG Clinical Guideline: Hereditary Hemochromatosis. Am. J. Gastroenterol. 2019, 114, 1202–1218. [Google Scholar] [CrossRef] [PubMed]
- Cancado, R.D.; Alvarenga, A.M.; Santos, P.C.J. HFE Hemochromatosis: An Overview about Therapeutic Recommendations. Hematol., Transfus. Cell Ther. 2022, 44, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Turshudzhyan, A.; Wu, D.C.; Wu, G.Y. Primary Non-HFE Hemochromatosis: A Review. J. Clin. Transl. Hepatol. 2023, 11, 925–931. [Google Scholar] [CrossRef] [PubMed]
- Girelli, D.; Busti, F.; Brissot, P.; Cabantchik, I.; Muckenthaler, M.U.; Porto, G. Hemochromatosis Classification: Update and Recommendations by the BIOIRON Society. Blood 2022, 139, 3018–3029. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. Electronic address: easloffice@easloffice.eu; European Association for the Study of the Liver EASL Clinical Practice Guidelines on Haemochromatosis. J. Hepatol. 2022, 77, 479–502. [Google Scholar] [CrossRef] [PubMed]
- Crawford, D.H.G.; Ramm, G.A.; Bridle, K.R.; Nicoll, A.J.; Delatycki, M.B.; Olynyk, J.K. Clinical Practice Guidelines on Hemochromatosis: Asian Pacific Association for the Study of the Liver. Hepatol. Int. 2023, 17, 522–541. [Google Scholar] [CrossRef] [PubMed]
- Delatycki, M.B.; Powell, L.W.; Allen, K.J. Hereditary Hemochromatosis Genetic Testing of At-Risk Children: What Is the Appropriate Age? Genet Test 2004, 8, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, H.R. HEMOCHROMATOSIS AND ARTHRITIS. Arthritis Rheum. 1964, 7, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Richardson, A.; Prideaux, A.; Kiely, P. Haemochromatosis: Unexplained Metacarpophalangeal or Ankle Arthropathy Should Prompt Diagnostic Tests: Findings from Two UK Observational Cohort Studies. Scand. J. Rheumatol. 2017, 46, 69–74. [Google Scholar] [CrossRef]
- Calori, S.; Comisi, C.; Mascio, A.; Fulchignoni, C.; Pataia, E.; Maccauro, G.; Greco, T.; Perisano, C. Overview of Ankle Arthropathy in Hereditary Hemochromatosis. Med Sci (Basel) 2023, 11, 51. [Google Scholar] [CrossRef]
- Adams, P.C.; Kertesz, A.E.; Valberg, L.S. Clinical Presentation of Hemochromatosis: A Changing Scene. Am. J. Med. 1991, 90, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Loughnan, R.; Ahern, J.; Tompkins, C.; Palmer, C.E.; Iversen, J.; Thompson, W.K.; Andreassen, O.; Jernigan, T.; Sugrue, L.; Dale, A.; et al. Association of Genetic Variant Linked to Hemochromatosis With Brain Magnetic Resonance Imaging Measures of Iron and Movement Disorders. JAMA Neurol. 2022, 79, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Rizek, P.; Sadikovic, B.; Adams, P.C.; Jog, M. Movement Disorders Associated With Hemochromatosis. Can. J. Neurol. Sci. 2016, 43, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Topiwala, A.; Wang, C.; Ebmeier, K.P.; Burgess, S.; Bell, S.; Levey, D.F.; Zhou, H.; McCracken, C.; Roca-Fernández, A.; Petersen, S.E.; et al. Associations between Moderate Alcohol Consumption, Brain Iron, and Cognition in UK Biobank Participants: Observational and Mendelian Randomization Analyses. PLoS Med. 2022, 19, e1004039. [Google Scholar] [CrossRef] [PubMed]
- Harrison-Findik, D.D.; Schafer, D.; Klein, E.; Timchenko, N.A.; Kulaksiz, H.; Clemens, D.; Fein, E.; Andriopoulos, B.; Pantopoulos, K.; Gollan, J. Alcohol Metabolism-Mediated Oxidative Stress down-Regulates Hepcidin Transcription and Leads to Increased Duodenal Iron Transporter Expression. J. Biol. Chem. 2006, 281, 22974–22982. [Google Scholar] [CrossRef] [PubMed]
- Harrison-Findik, D.D. Role of Alcohol in the Regulation of Iron Metabolism. World J. Gastroenterol. 2007, 13, 4925–4930. [Google Scholar] [CrossRef] [PubMed]
- Sadasivam, N.; Kim, Y.-J.; Radhakrishnan, K.; Kim, D.-K. Oxidative Stress, Genomic Integrity, and Liver Diseases. Molecules 2022, 27, 3159. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, L.M.; Dixon, J.L.; Purdie, D.M.; Powell, L.W.; Crawford, D.H.G. Excess Alcohol Greatly Increases the Prevalence of Cirrhosis in Hereditary Hemochromatosis. Gastroenterology 2002, 122, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Adams, P.C.; Agnew, S. Alcoholism in Hereditary Hemochromatosis Revisited: Prevalence and Clinical Consequences among Homozygous Siblings. Hepatology 1996, 23, 724–727. [Google Scholar] [CrossRef]
- Alvi, A.T.; Santiago, L.E.; Nadeem, Z.; Chaudhry, A. Fulminant Hepatic Failure With Minimal Alcohol Consumption in a 25-Year-Old Female With Hereditary Hemochromatosis: A Rare Case. Cureus 2023, 15, e44544. [Google Scholar] [CrossRef]
- Kew, M.C. Hepatic Iron Overload and Hepatocellular Carcinoma. Liver Cancer 2014, 3, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, B.; Pammer, L.M.; Pfeifer, B.; Neururer, S.; Troppmair, M.R.; Panzer, M.; Wagner, S.; Pertler, E.; Gieger, C.; Kronenberg, F.; et al. Penetrance, Cancer Incidence and Survival in HFE Haemochromatosis-A Population-Based Cohort Study. Liver Int. 2024. [Google Scholar] [CrossRef] [PubMed]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Kaur, H.; Lerner, R.G.; Patel, R.; Rafiyath, S.M.; Singh Lamba, G. Hepatocellular Carcinoma in Non-Cirrhotic Liver Without Evidence of Iron Overload in a Patient with Primary Hemochromatosis. Review. J. Gastrointest. Canc 2012, 43, 36–39. [Google Scholar] [CrossRef]
- Bardou-Jacquet, E.; Morandeau, E.; Anderson, G.J.; Ramm, G.A.; Ramm, L.E.; Morcet, J.; Bouzille, G.; Dixon, J.; Clouston, A.D.; Lainé, F.; et al. Regression of Fibrosis Stage With Treatment Reduces Long-Term Risk of Liver Cancer in Patients With Hemochromatosis Caused by Mutation in HFE. Clin. Gastroenterol. Hepatol. 2020, 18, 1851–1857. [Google Scholar] [CrossRef] [PubMed]
- Daniłowicz-Szymanowicz, L.; Świątczak, M.; Sikorska, K.; Starzyński, R.R.; Raczak, A.; Lipiński, P. Pathogenesis, Diagnosis, and Clinical Implications of Hereditary Hemochromatosis—The Cardiological Point of View. Diagnostics (Basel) 2021, 11, 1279. [Google Scholar] [CrossRef] [PubMed]
- Seferović, P.M.; Polovina, M.; Bauersachs, J.; Arad, M.; Ben Gal, T.; Lund, L.H.; Felix, S.B.; Arbustini, E.; Caforio, A.L.P.; Farmakis, D.; et al. Heart Failure in Cardiomyopathies: A Position Paper from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 553–576. [Google Scholar] [CrossRef] [PubMed]
- Rozpoznanie i leczenie hemochromatozy dziedzicznej. Podsumowanie wytycznych American College of Gastroenterology (AGA). Available online: http://www.mp.pl/social/article/260811 (accessed on 18 February 2024).
- Cortés, P.; Elsayed, A.A.; Stancampiano, F.F.; Barusco, F.M.; Shapiro, B.P.; Bi, Y.; Heckman, M.G.; Peng, Z.; Kempaiah, P.; Palmer, W.C. Clinical and Genetic Predictors of Cardiac Dysfunction Assessed by Echocardiography in Patients with Hereditary Hemochromatosis. Int. J. Cardiovasc. Imaging 2024, 40, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.-H.; Fefelova, N.; Pamarthi, S.H.; Gwathmey, J.K. Molecular Mechanisms of Ferroptosis and Relevance to Cardiovascular Disease. Cells 2022, 11, 2726. [Google Scholar] [CrossRef]
- Wood, M.J.; Powell, L.W.; Dixon, J.L.; Ramm, G.A. Clinical Cofactors and Hepatic Fibrosis in Hereditary Hemochromatosis: The Role of Diabetes Mellitus. Hepatology 2012, 56, 904–911. [Google Scholar] [CrossRef]
- Altamura, S.; Müdder, K.; Schlotterer, A.; Fleming, T.; Heidenreich, E.; Qiu, R.; Hammes, H.-P.; Nawroth, P.; Muckenthaler, M.U. Iron Aggravates Hepatic Insulin Resistance in the Absence of Inflammation in a Novel Db/Db Mouse Model with Iron Overload. Mol. Metab. 2021, 51, 101235. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.V.; Lorenzo, F.R.; McClain, D.A. Iron and the Pathophysiology of Diabetes. Annu. Rev. Physiol. 2023, 85, 339–362. [Google Scholar] [CrossRef] [PubMed]
- Asberg, A.; Hveem, K.; Thorstensen, K.; Ellekjter, E.; Kannelønning, K.; Fjøsne, U.; Halvorsen, T.B.; Smethurst, H.B.; Sagen, E.; Bjerve, K.S. Screening for Hemochromatosis: High Prevalence and Low Morbidity in an Unselected Population of 65,238 Persons. Scand. J. Gastroenterol. 2001, 36, 1108–1115. [Google Scholar] [CrossRef] [PubMed]
- Beutler, E.; Felitti, V.J.; Koziol, J.A.; Ho, N.J.; Gelbart, T. Penetrance of 845G--> A (C282Y) HFE Hereditary Haemochromatosis Mutation in the USA. Lancet 2002, 359, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Allen, K.J.; Gurrin, L.C.; Constantine, C.C.; Osborne, N.J.; Delatycki, M.B.; Nicoll, A.J.; McLaren, C.E.; Bahlo, M.; Nisselle, A.E.; Vulpe, C.D.; et al. Iron-Overload-Related Disease in HFE Hereditary Hemochromatosis. N. Engl. J. Med. 2008, 358, 221–230. [Google Scholar] [CrossRef] [PubMed]
- McLaren, G.D.; McLaren, C.E.; Adams, P.C.; Barton, J.C.; Reboussin, D.M.; Gordeuk, V.R.; Acton, R.T.; Harris, E.L.; Speechley, M.R.; Sholinsky, P.; et al. Clinical Manifestations of Hemochromatosis in HFE C282Y Homozygotes Identified by Screening. Can. J. Gastroenterol. 2008, 22, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Barton, J.C.; Acton, R.T. Diabetes in HFE Hemochromatosis. J. Diabetes Res. 2017, 2017, 9826930. [Google Scholar] [CrossRef]
- Pelusi, C.; Gasparini, D.I.; Bianchi, N.; Pasquali, R. Endocrine Dysfunction in Hereditary Hemochromatosis. J. Endocrinol. Invest. 2016, 39, 837–847. [Google Scholar] [CrossRef]
- Parkash, O.; Akram, M. Hereditary Hemochromatosis. J. Coll. Physicians Surg. Pak. 2015, 25, 644–647. [Google Scholar]
- Chevrant-Breton, J.; Simon, M.; Bourel, M.; Ferrand, B. Cutaneous Manifestations of Idiopathic Hemochromatosis. Study of 100 Cases. Arch. Dermatol. 1977, 113, 161–165. [Google Scholar] [CrossRef]
- Varada, N.; Tun, K.M.; Chang, M.J.; Bomberger, S.; Calagari, R.; Varada, N.; Tun, K.M.; Chang, M.J.; Bomberger, S.; Calagari, R. A Rare Case of Hereditary Hemochromatosis Presenting With Porphyria Cutanea Tarda. Cureus 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Edwards, M.V.; Ray, J.M.; Bacon, B.R. Sporadic Porphyria Cutanea Tarda as the Initial Manifestation of Hereditary Hemochromatosis. ACG Case Rep. J. 2019, 6, e00247. [Google Scholar] [CrossRef] [PubMed]
- Sredoja Tišma, V.; Bulimbašić, S.; Jaganjac, M.; Stjepandić, M.; Larma, M. Progressive Pigmented Purpuric Dermatitis and Alopecia Areata as Unusual Skin Manifestations in Recognizing Hereditary Hemochromatosis. Acta Dermatovenerol. Croat. 2012, 20, 181–186. [Google Scholar] [PubMed]
- Leung, B.; Lindley, L.; Cruz, P.D.; Cole, S.; Ayoade, K.O. Iron Screening in Alopecia Areata Patients May Catch Hereditary Hemochromatosis Early. Cutis 2022, 110, E30–E32. [Google Scholar] [CrossRef] [PubMed]
- Reuben, A.; Chung, J.W.; Lapointe, R.; Santos, M.M. The Hemochromatosis Protein HFE 20 Years Later: An Emerging Role in Antigen Presentation and in the Immune System. Immun. Inflamm. Dis. 2017, 5, 218–232. [Google Scholar] [CrossRef] [PubMed]
- Porto, G.; Sousa, M.D. Iron Overload and Immunity. World J. Gastroenterol. 2007, 13, 4707–4715. [Google Scholar] [CrossRef] [PubMed]
- Hubacek, J.A.; Philipp, T.; Adamkova, V.; Majek, O.; Dusek, L. A Haemochromatosis-Causing HFE Mutation Is Associated with SARS-CoV-2 Susceptibility in the Czech Population. Clin. Chim. Acta 2023, 538, 211–215. [Google Scholar] [CrossRef]
- Ristić, S.; Milić, S.; Tatalović, T.; Bilobrk, M.; Rončević, D.; Ćurko-Cofek, B.; Barac-Latas, V.; Čizmarević, N.S. The Influence of Hemochromatosis Gene (HFE) Mutations on SARS-CoV-2 Susceptibility and COVID-19 Severity. Balkan Med. J. 2023, 40, 229–231. [Google Scholar] [CrossRef]
- Sazawal, S.; Black, R.E.; Kabole, I.; Dutta, A.; Dhingra, U.; Ramsan, M. Effect of Iron/Folic Acid Supplementation on the Outcome of Malaria Episodes Treated with Sulfadoxine-Pyrimethamine. Malar. Res. Treat. 2014, 2014, 625905. [Google Scholar] [CrossRef]
- Carcillo, J.A.; Sward, K.; Halstead, E.S.; Telford, R.; Jimenez-Bacardi, A.; Shakoory, B.; Simon, D.; Hall, M. ; Eunice Kennedy Shriver National Institute of Child Health and Human Development Collaborative Pediatric Critical Care Research Network Investigators A Systemic Inflammation Mortality Risk Assessment Contingency Table for Severe Sepsis. Pediatr. Crit. Care Med. 2017, 18, 143–150. [Google Scholar] [CrossRef]
- Bennett, T.D.; Hayward, K.N.; Farris, R.W.D.; Ringold, S.; Wallace, C.A.; Brogan, T.V. Very High Serum Ferritin Levels Are Associated with Increased Mortality and Critical Care in Pediatric Patients. Pediatr. Crit. Care Med. 2011, 12, e233–e236. [Google Scholar] [CrossRef] [PubMed]
- Kernan, K.F.; Carcillo, J.A. Hyperferritinemia and Inflammation. Int. Immunol. 2017, 29, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.C.; Senussi, N.H.; Fertrin, K.Y.; Kowdley, K.V. Iron Overload Disorders. Hepatol. Commun. 2022, 6, 1842–1854. [Google Scholar] [CrossRef] [PubMed]
- Beaumont-Epinette, M.-P.; Delobel, J.-B.; Ropert, M.; Deugnier, Y.; Loréal, O.; Jouanolle, A.-M.; Brissot, P.; Bardou-Jacquet, E. Hereditary Hypotransferrinemia Can Lead to Elevated Transferrin Saturation and, When Associated to HFE or HAMP Mutations, to Iron Overload. Blood Cells Mol. Dis. 2015, 54, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Montosi, G.; Donovan, A.; Totaro, A.; Garuti, C.; Pignatti, E.; Cassanelli, S.; Trenor, C.C.; Gasparini, P.; Andrews, N.C.; Pietrangelo, A. Autosomal-Dominant Hemochromatosis Is Associated with a Mutation in the Ferroportin (SLC11A3) Gene. J. Clin. Investig. 2001, 108, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Miyajima, H. Aceruloplasminemia. Neuropathology 2015, 35, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Bruzzese, A.; Martino, E.A.; Mendicino, F.; Lucia, E.; Olivito, V.; Bova, C.; Filippelli, G.; Capodanno, I.; Neri, A.; Morabito, F.; et al. Iron Chelation Therapy. Eur. J. Haematol. 2023, 110, 490–497. [Google Scholar] [CrossRef]
- Liu Yin, J.; Cussen, C.; Harrington, C.; Foskett, P.; Raja, K.; Ala, A. Guideline Review: European Association for the Study of Liver (EASL) Clinical Practice Guidelines on Haemochromatosis. J. Clin. Exp. Hepatol. 2023, 13, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Brissot, P.; Brissot, E. What’s Important and New in Hemochromatosis? Clin. Hematol. Int. 2020, 2, 143–148. [Google Scholar] [CrossRef]
- Milic, S.; Mikolasevic, I.; Orlic, L.; Devcic, E.; Starcevic-Cizmarevic, N.; Stimac, D.; Kapovic, M.; Ristic, S. The Role of Iron and Iron Overload in Chronic Liver Disease. Med. Sci. Monit. 2016, 22, 2144–2151. [Google Scholar] [CrossRef]
- Pinyopornpanish, K.; Tantiworawit, A.; Leerapun, A.; Soontornpun, A.; Thongsawat, S. Secondary Iron Overload and the Liver: A Comprehensive Review. J. Clin. Transl. Hepatol. 2023, 11, 932–941. [Google Scholar] [CrossRef] [PubMed]
- Bassett, M.L.; Hickman, P.E.; Dahlstrom, J.E. The Changing Role of Liver Biopsy in Diagnosis and Management of Haemochromatosis. Pathology 2011, 43, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Urru, S.A.M.; Tandurella, I.; Capasso, M.; Usala, E.; Baronciani, D.; Giardini, C.; Visani, G.; Angelucci, E. Reproducibility of Liver Iron Concentration Measured on a Biopsy Sample: A Validation Study in Vivo. Am. J. Hematol. 2015, 90, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Golfeyz, S.; Lewis, S.; Weisberg, I.S. Hemochromatosis: Pathophysiology, Evaluation, and Management of Hepatic Iron Overload with a Focus on MRI. Expert. Rev. Gastroenterol. Hepatol. 2018, 12, 767–778. [Google Scholar] [CrossRef] [PubMed]
- Reeder, S.B.; Yokoo, T.; França, M.; Hernando, D.; Alberich-Bayarri, Á.; Alústiza, J.M.; Gandon, Y.; Henninger, B.; Hillenbrand, C.; Jhaveri, K.; et al. Quantification of Liver Iron Overload with MRI: Review and Guidelines from the ESGAR and SAR. Radiology 2023, 307, e221856. [Google Scholar] [CrossRef] [PubMed]
- Jacobi, N.; Herich, L. Measurement of Liver Iron Concentration by Superconducting Quantum Interference Device Biomagnetic Liver Susceptometry Validates Serum Ferritin as Prognostic Parameter for Allogeneic Stem Cell Transplantation. Eur. J. Haematol. 2016, 97, 336–341. [Google Scholar] [CrossRef] [PubMed]
- European Association For The Study Of The Liver EASL Clinical Practice Guidelines for HFE Hemochromatosis. J. Hepatol. 2010, 53, 3–22. [CrossRef] [PubMed]
- Savatt, J.M.; Johns, A.; Schwartz, M.L.B.; McDonald, W.S.; Salvati, Z.M.; Oritz, N.M.; Masnick, M.; Hatchell, K.; Hao, J.; Buchanan, A.H.; et al. Testing and Management of Iron Overload After Genetic Screening-Identified Hemochromatosis. JAMA Netw. Open 2023, 6, e2338995. [Google Scholar] [CrossRef] [PubMed]
- Buzzetti, E.; Kalafateli, M.; Thorburn, D.; Davidson, B.R.; Tsochatzis, E.; Gurusamy, K.S. Interventions for Hereditary Haemochromatosis: An Attempted Network Meta-Analysis. Cochrane Database Syst. Rev. 2017, 3, CD011647. [Google Scholar] [CrossRef]
- Adams, P.; Altes, A.; Brissot, P.; Butzeck, B.; Cabantchik, I.; Cançado, R.; Distante, S.; Evans, P.; Evans, R.; Ganz, T.; et al. Therapeutic Recommendations in HFE Hemochromatosis for p.Cys282Tyr (C282Y/C282Y) Homozygous Genotype. Hepatol. Int. 2018, 12, 83–86. [Google Scholar] [CrossRef]
- Stussi, G.; Buser, A.; Holbro, A. Red Blood Cells: Exchange, Transfuse, or Deplete. Transfus. Med. Hemother 2019, 46, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Rombout-Sestrienkova, E.; Brandts, L.; Koek, G.H.; van Deursen, C.Th.B.M. Patients with Hereditary Hemochromatosis Reach Safe Range of Transferrin Saturation Sooner with Erythrocytaphereses than with Phlebotomies. J. Clin. Apher. 2022, 37, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Sundic, T.; Hervig, T.; Hannisdal, S.; Assmus, J.; Ulvik, R.J.; Olaussen, R.W.; Berentsen, S. Erythrocytapheresis Compared with Whole Blood Phlebotomy for the Treatment of Hereditary Haemochromatosis. Blood Transfus. 2014, 12, s84–s89. [Google Scholar] [CrossRef] [PubMed]
- Cançado, R.; Melo, M.R.; de Moraes Bastos, R.; Santos, P.C.J.L.; Guerra-Shinohara, E.M.; Chiattone, C.; Ballas, S.K. Deferasirox in Patients with Iron Overload Secondary to Hereditary Hemochromatosis: Results of a 1-Yr Phase 2 Study. Eur. J. Haematol. 2015, 95, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Entezari, S.; Haghi, S.M.; Norouzkhani, N.; Sahebnazar, B.; Vosoughian, F.; Akbarzadeh, D.; Islampanah, M.; Naghsh, N.; Abbasalizadeh, M.; Deravi, N. Iron Chelators in Treatment of Iron Overload. J. Toxicol. 2022, 2022, 4911205. [Google Scholar] [CrossRef] [PubMed]
- Gomber, S.; Jain, P.; Sharma, S.; Narang, M. Comparative Efficacy and Safety of Oral Iron Chelators and Their Novel Combination in Children with Thalassemia. Indian. Pediatr. 2016, 53, 207–210. [Google Scholar] [CrossRef]
- Angelucci, E. Another Step Forward in Iron Chelation Therapy. Acta Haematol. 2015, 134, 231–232. [Google Scholar] [CrossRef] [PubMed]
- Kontoghiorghe, C.N.; Kontoghiorghes, G.J. New Developments and Controversies in Iron Metabolism and Iron Chelation Therapy. World J. Methodol. 2016, 6, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Bauchner, H.; Fontanarosa, P.B.; Golub, R.M. Evaluation of the Trial to Assess Chelation Therapy (TACT): The Scientific Process, Peer Review, and Editorial Scrutiny. JAMA 2013, 309, 1291–1292. [Google Scholar] [CrossRef]
- Mobarra, N.; Shanaki, M.; Ehteram, H.; Nasiri, H.; Sahmani, M.; Saeidi, M.; Goudarzi, M.; Pourkarim, H.; Azad, M. A Review on Iron Chelators in Treatment of Iron Overload Syndromes. Int. J. Hematol. Oncol. Stem Cell Res. 2016, 10, 239–247. [Google Scholar]
- Vanclooster, A.; van Deursen, C.; Jaspers, R.; Cassiman, D.; Koek, G. Proton Pump Inhibitors Decrease Phlebotomy Need in HFE Hemochromatosis: Double-Blind Randomized Placebo-Controlled Trial. Gastroenterology 2017, 153, 678–680. [Google Scholar] [CrossRef]
- Dirweesh, A.; Anugwom, C.M.; Li, Y.; Vaughn, B.P.; Lake, J. Proton Pump Inhibitors Reduce Phlebotomy Burden in Patients with HFE-Related Hemochromatosis: A Systematic Review and Meta-Analysis. Eur. J. Gastroenterol. Hepatol. 2021, 33, 1327–1331. [Google Scholar] [CrossRef]
- Lymberopoulos, P.; Prakash, S.; Shaikh, A.; Bhatnagar, A.; Allam, A.K.; Goli, K.; Goss, J.A.; Kanwal, F.; Rana, A.; Kowdley, K.V.; et al. Long-Term Outcomes and Trends in Liver Transplantation for Hereditary Hemochromatosis in the United States. Liver Transpl. 2023, 29, 15–25. [Google Scholar] [CrossRef]
- McPhail, M.J.W.; Khorsandi, S.E.; Abbott, L.; Al-Kadhimi, G.; Kane, P.; Karani, J.; O’Grady, J.; Heaton, N.; Bomford, A.; Suddle, A. Modern Outcomes Following Treatment of Hepatocellular Carcinoma in Hereditary Hemochromatosis: A Matched Cohort Study. Am. J. Clin. Oncol. 2019, 42, 918–923. [Google Scholar] [CrossRef] [PubMed]
- Charlebois, E.; Pantopoulos, K. Nutritional Aspects of Iron in Health and Disease. Nutrients 2023, 15, 2441. [Google Scholar] [CrossRef] [PubMed]
- Zakrzewski, A.J.; Gajewska, J.; Chajęcka-Wierzchowska, W.; Załuski, D.; Zadernowska, A. Prevalence of Listeria Monocytogenes and Other Listeria Species in Fish, Fish Products and Fish Processing Environment: A Systematic Review and Meta-Analysis. Sci. Total Environ. 2024, 907, 167912. [Google Scholar] [CrossRef] [PubMed]
- Lasagabaster, A.; Jiménez, E.; Lehnherr, T.; Miranda-Cadena, K.; Lehnherr, H. Bacteriophage Biocontrol to Fight Listeria Outbreaks in Seafood. Food Chem. Toxicol. 2020, 145, 111682. [Google Scholar] [CrossRef]
- Krahulcová, M.; Cverenkárová, K.; Koreneková, J.; Oravcová, A.; Koščová, J.; Bírošová, L. Occurrence of Antibiotic-Resistant Bacteria in Fish and Seafood from Slovak Market. Foods 2023, 12, 3912. [Google Scholar] [CrossRef]
- Milman, N.T. Managing Genetic Hemochromatosis: An Overview of Dietary Measures, Which May Reduce Intestinal Iron Absorption in Persons With Iron Overload. Gastroenterology Res. 2021, 14, 66–80. [Google Scholar] [CrossRef]
- Moirand, R.; Adams, P.C.; Bicheler, V.; Brissot, P.; Deugnier, Y. Clinical Features of Genetic Hemochromatosis in Women Compared with Men. Ann. Intern. Med. 1997, 127, 105–110. [Google Scholar] [CrossRef]
- Durazzo, M.; Belci, P.; Collo, A.; Prandi, V.; Pistone, E.; Martorana, M.; Gambino, R.; Bo, S. Gender Specific Medicine in Liver Diseases: A Point of View. World J. Gastroenterol. 2014, 20, 2127–2135. [Google Scholar] [CrossRef] [PubMed]
- Niu, C.; Zhang, J.; Goldenberg, I.; Gill, S.; Saeed, H.; Iyer, C.; Dunnigan, K. Maternal and Prenatal Outcomes of Hemochromatosis in Pregnancy: A Population-Based Study. Clin. Res. Hepatol. Gastroenterol. 2023, 47, 102221. [Google Scholar] [CrossRef] [PubMed]
- Scotet, V.; Saliou, P.; Uguen, M.; L’Hostis, C.; Merour, M.-C.; Triponey, C.; Chanu, B.; Nousbaum, J.-B.; Le Gac, G.; Ferec, C. Do Pregnancies Reduce Iron Overload in HFE Hemochromatosis Women? Results from an Observational Prospective Study. BMC Pregnancy Childbirth 2018, 18, 53. [Google Scholar] [CrossRef] [PubMed]
- Neves, J.V.; Olsson, I.A.S.; Porto, G.; Rodrigues, P.N. Hemochromatosis and Pregnancy: Iron Stores in the Hfe-/- Mouse Are Not Reduced by Multiple Pregnancies. Am. J. Physiol. Gastrointest. Liver Physiol. 2010, 298, G525–G529. [Google Scholar] [CrossRef]
- Sayaf, K.; Gabbia, D.; Russo, F.P.; De Martin, S. The Role of Sex in Acute and Chronic Liver Damage. Int. J. Mol. Sci. 2022, 23, 10654. [Google Scholar] [CrossRef] [PubMed]
- Della Torre, S. Beyond the X Factor: Relevance of Sex Hormones in NAFLD Pathophysiology. Cells 2021, 10, 2502. [Google Scholar] [CrossRef] [PubMed]
- Bizzaro, D.; Crescenzi, M.; Di Liddo, R.; Arcidiacono, D.; Cappon, A.; Bertalot, T.; Amodio, V.; Tasso, A.; Stefani, A.; Bertazzo, V.; et al. Sex-Dependent Differences in Inflammatory Responses during Liver Regeneration in a Murine Model of Acute Liver Injury. Clin Sci (Lond) 2018, 132, 255–272. [Google Scholar] [CrossRef] [PubMed]
- Shamas, A.G. Primary Hereditary Haemochromatosis and Pregnancy. GastroHep 2023, 2023, e2674203. [Google Scholar] [CrossRef]
- Phatak, P.D.; Bonkovsky, H.L.; Kowdley, K.V. Hereditary Hemochromatosis: Time for Targeted Screening. Ann. Intern. Med. 2008, 149, 270–272. [Google Scholar] [CrossRef]
Figure 1.
Differential diagnosis of iron overload (HCV- hepatitis C virus; HH- hereditary hemochromatosis; MCV- mean red cell volume; MDS- myelodysplastic syndrome; SF- serum ferritin; TSAT- transferrin saturation).
Figure 1.
Differential diagnosis of iron overload (HCV- hepatitis C virus; HH- hereditary hemochromatosis; MCV- mean red cell volume; MDS- myelodysplastic syndrome; SF- serum ferritin; TSAT- transferrin saturation).
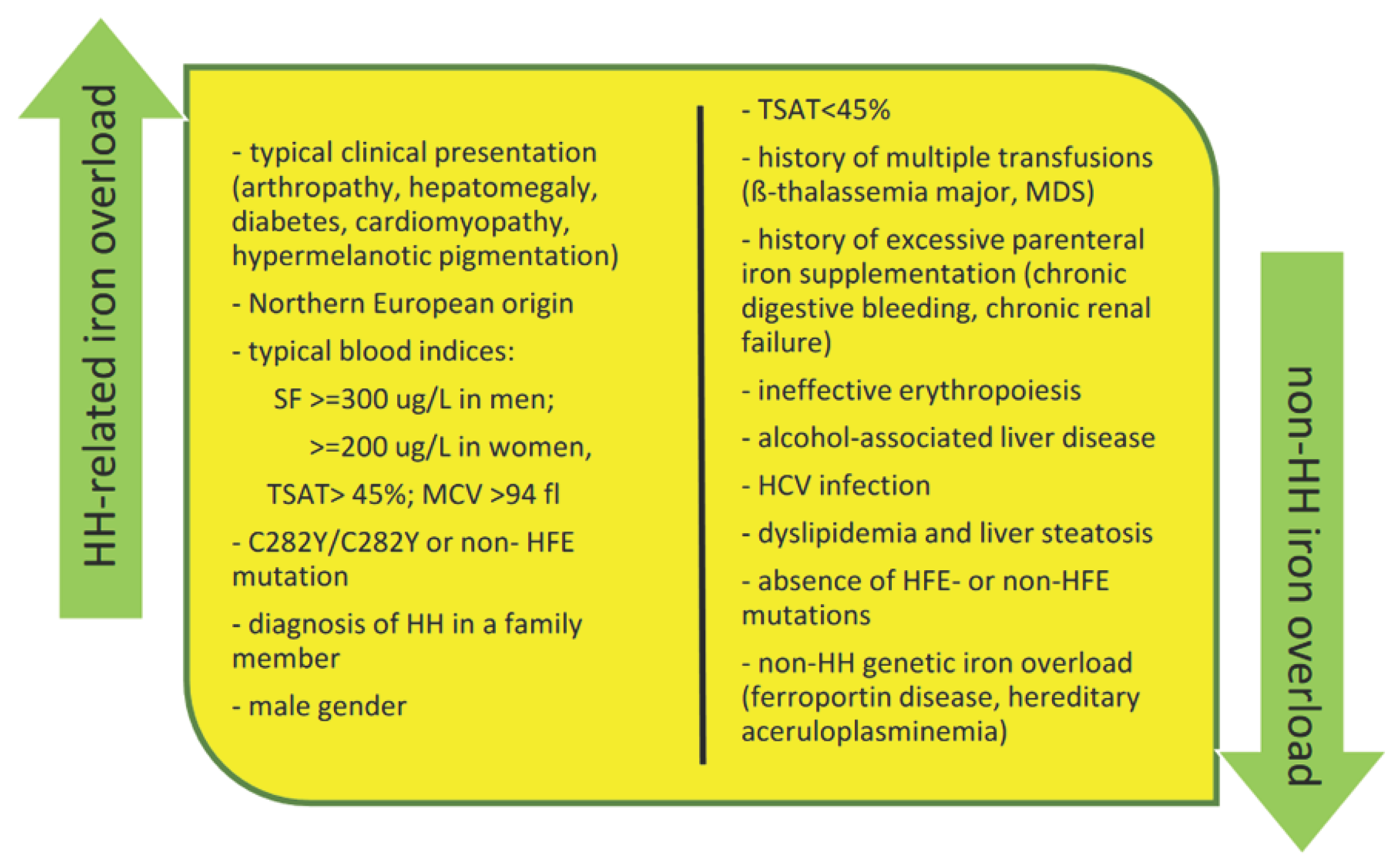

Table 1.
Novel classification of hereditary hemochromatosis (HH) proposed by the International Society for the Study of Iron in Biology and Medicine (BIOIRON Society); (adopted and modified from [25]).
Table 1.
Novel classification of hereditary hemochromatosis (HH) proposed by the International Society for the Study of Iron in Biology and Medicine (BIOIRON Society); (adopted and modified from [25]).
| Novel HH classification | Molecular pattern | Comments |
|---|---|---|
| HFE-related | p.Cys282Tyr homozygosity or compound heterozygosity of p.Cys282Tyr with other rare HFE variants or HFE deletion |
Low penetrance; consider the presence of host-related or environmental cofactors for iron overload. In subjects with other HFE genotypes (eg, p.Cys282Tyr/His63Asp compound heterozygosity or p.His63Asp homozygosity) consider second-line genetic testing for rarer variants |
| Non-HFE-related | Rare variants in “non-HFE” genes: • HJV-related • HAMP-related • TFR2-related • SLC40A1 (GOF)-related |
Potentially, mutations in any hepcidin-regulatory gene may be causative (the effects of novel mutations should be confirmed through functional and epidemiological studies) Molecular subtypes characterization only in specialized centers, but the diagnosis of non-HFE related HH is sufficient to start phlebotomies at nonspecialized centers* |
| Digenic** | Double heterozygosity and/or double homozygosity/heterozygosity for mutations in 2 different genes involved in iron metabolism (HFE and/or non-HFE) |
More commonly, p.Cys282Tyr mutation in the HFE gene might coexist with mutations in other genes; rarely, both mutations involve non-HFE genes |
| Molecularly undefined | Molecular characterization (still) not available after sequencing of known genes (provisional diagnosis) | Patients should be referred (or DNA should be sent) to specialized centers |
*Provided that iron overload (IO) is confirmed by MRI. If this is not accessible, close monitoring of Hb level is needed to avoid the occurrence of anemia. ** Data interpretation with caution as digenic inheritance results from NGS outputs reporting several variants in gene panels. Whenever possible, strict criteria for defining pathogenic variants should be adopted and corroborated by family segregation and/or functional studies.
Table 2.
Clinical presentation of hereditary hemochromatosis.
| Organ/system | Symptoms |
|---|---|
| Skeletomuscular system | arthralgia, arthritis, chondrocalcinosis, reduced bone mineral density, fatigue, weakness |
| Central nervous system | lack of energy (lethargy), irritability, memory fog, mood swings, depression, anxiety, movement disorders, tremors |
| Liver | high liver enzymes, hepatosplenomegaly, liver fibrosis and cirrhosis, hepatocellular carcinoma |
| Cardiovascular system | cardiomyopathy, arrhythmia, heart failure |
| Endocrine system | hypogonadism, testicular atrophy, reproductive disorders with loss of libido, impotence, amenorrhea, hyperglycemia, diabetes mellitus, hypopituitarism |
| Skin | bronze or gray skin tone (hypermelanotic pigmentation), hair loss, porphyria cutanea tarda (?) |
| Immune system | immune defects, infections |
Table 3.
Risk factors of severe liver disease in HFE-related hemochromatosis [26]: .
Table 3.
Risk factors of severe liver disease in HFE-related hemochromatosis [26]: .
| Risk factors related to severe liver disease |
|---|
|
Table 4.
Clinical trials currently recruiting patients with hereditary hemochromatosis and registered at the website https://clinicaltrials.gov/ (accessed on 4 February 2024).
Table 4.
Clinical trials currently recruiting patients with hereditary hemochromatosis and registered at the website https://clinicaltrials.gov/ (accessed on 4 February 2024).
| Study Title (brief description) |
NCT Number | Conditions | Interventions | Study Type | Location |
|---|---|---|---|---|---|
| Impact of Transferrin Saturation Guided Maintenance Treatment on Quality of Life in HFE Haemochromatosis (biological test results guide the treatment modification: either time schedule or volume of bloodletting according to randomization group (patients treated with bloodletting according to current guidelines “ferritin alone” versus patients treated with bloodletting according to “transferrin saturation and serum ferritin”) |
NCT04779593 | Hemochromatosis | Clinical examination SF36 Quest AIMS2_SF Quest Bloodletting - experimental group 11 more |
Interventional | France |
| Treatment of Hemochromatosis (comparison of ferritin and MCV in guiding phlebotomy in pts with HH) |
NCT00007150 | Hemochromatosis | Phlebotomy | Interventional | United States |
| MRI QSM Imaging for Iron Overload (validation of a novel technique i.e., MRI-based QSM of the abdomen, for non-invasive assessment of liver iron deposition) |
NCT04631718 | Hemochromatosis Iron Overload |
Radiation: MRI-based QSM | Observational | United States |
| Iron Overload and Endocrinological Diseases (evaluation of the prevalence of endocrinological diseases in adult pts with iron overload due to β-thalassemia or hemochromatosis and their impact on quality of life) |
NCT06137079 | Thalassemia (major or intermedia) Hereditary Hemochromatosis |
Observational | Italy |
*HH- hereditary hemochromatosis; MCV- mean corpuscular volume; MRI- Magnetic Resonance Imaging; pts- patients; QSM-Quantitative Susceptibility Mapping; Quest- questionnaire.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



