Submitted:
26 February 2024
Posted:
26 February 2024
You are already at the latest version
Abstract
Melasma is a challenging skin condition which involves both structural and functional skin alterations. Despite the availability of various treatment options, the management remains complex. This is the first study to investigate topical application of Rosa Damascena stem cell exosomes when used concomitantly with microneedling in women and men with facial melasma. We recruited 20 subjects with Fitzpatrick skin types I-III, exhibiting melasma of varying severity. The modified Melasma Area and Severity Index (mMASI) and Global Aesthetic Improvement Scale (GAIS) were utilized to evaluate treatment response. The treatment protocol involved microneedling followed by exosome application over four or five sessions, at 4-week intervals. Ninety percent of subjects demonstrated a significant improvement in mMASI scores, while only 10% showed no change. GAIS assessment further supports overall improvement, with just 10% categorized as "not changed". Tolerability was favorable, with mild, transient side effects. Our findings suggest promising outcomes with this combined therapy, underscoring its potential as a safe and effective approach for treating melasma, particularly in severe and moderate cases. However, further research with larger sample sizes and control arms is warranted to validate these findings and explore long-term efficacy.
Keywords:
Melasma
; hyperpigmentation
; exosomes
; RSCEs
; microneedling.
; mMASI
; GAIS
1. Introduction
Melasma is a chronic, acquired skin condition characterized by irregular and symmetrical distributed hyperpigmented spots that affects sun-exposed areas, especially the face. It is most commonly found in darker skin types (Fitzpatrick classification III–VI), particularly in Asian women of reproductive age. Melasma is a multifactorial disorder resulting from external factors such as ultraviolet radiation (UVR) exposure, oxidative status and female hormone stimulation, in genetically predisposed individuals [1]. Wood's lamp examination classifies melasma into epidermal, dermal, or mixed types based on pigment location. However, laser confocal microscopy studies reveal that all melasma types are mixed, suggesting a shared pathophysiology [2]. Although it was initially believed that melasma affected only melanocytes, subsequent histopathological studies of the affected skin have revealed structural and functional alterations across all skin layers [3]. Evidence of solar elastosis, thinning of the Stratum Corneum (SC), disruption of the basal membrane (BM), and heightened dermal blood vessels suggests that melasma may be a skin condition resulting from "photoaging". Pendulous melanocytes associated with basal membrane abnormality were identified as a distinctive histological feature in melasma [4]. These changes synergistically contribute to hypermelanogenesis [5]. Transcriptomic analyses performed in melasma lesions highlighted the involvement of at least 300 genes, impacting melanocytes and dermal components [6]. Genes involved in melanogenesis, such as tyrosinase (TYR), tyrosinase-related protein 1 (TYRP1), melanocortin 1 receptor (MC1R) and PDZ domain-containing protein 1 (PDZK1), seem to be upregulated. Downregulation of H19 gene impacts melanogenesis and melanin transfer, along with reduced expression of miR-675, which targets microphthalmia-associated transcription factor (MITF), a critical regulator of melanocytic cells. The decreased expression of miR-675 appears to influence cadherin-11 (CDH11), potentially contributing to BM damage [3,5]. UVR and VL act as a direct stimulants for melanogenesis. Prolonged sun exposure induces fibroblasts to secrete melanogenic and proinflammatory factors, including stem cell factor (SCF), a ligand for the tyrosine kinase receptor c-kit, which contributes to the increase in melanogenesis [7]. UVB has a significant impact on the epidermis and basal membrane; it induces the upregulation of proopiomelanocortin (POMC) in the epidermis, causing melanogenesis and the translocation of melanosomes to keratinocytes. Furthermore, UVB induces the release of inflammatory mediators such as prostaglandins and vascular endothelial growth factor (VEGF), fostering endothelial proliferation and elevating the levels of matrix metalloproteinases, which degrade type IV and VI collagen in the skin. UVA, despite being less erythemogenic, exerts a more significant impact on the superficial dermis through the generation of reactive species, proving to be more efficient in inducing pigment darkening and delayed tanning, especially in individuals with darker phenotypes. Also, VL penetrates the deep dermis and subcutis but only shorter wavelengths (420-470 nm) can induce pigmentation in darker phototypes by activating opsin 3 (OPN3) receptors in melanocytes [3]. Melasma is challenging to treat, and currently, there is no known cure. Several treatment options are available, such as chemical peels, lasers, lights, and systemic and topical approaches such as tranexamic acid, corticosteroids, tretinoin, and hydroquinone combined with broad-spectrum sunscreen protecting against UVB, long-wave UVA and high-energy VL [8]. Kligman's Trio (KT), initially introduced by Kligman in 1975, is acknowledged as the foremost treatment for melasma. This cream incorporates a blend of 5% hydroquinone, tretinoin, and corticosteroid. Nevertheless, this topical solution is linked to discomforting side effects, such as erythema, desquamation, and a burning sensation. Recently the use of a new triple combination cream containing isobutylamido-thiazolyl-resorcinol, retinoic acid, and corticosteroid has been introduced as a well-tolerated alternative to KT [9]. Chemical peels are an effective procedure in treating melasma as they exfoliate superficial skin layers, reducing hyperpigmentation. Various acid substances like salicylic acid, glycolic acid, and trichloroacetic acid, among others, are used at different concentrations to achieve improvement of the disease. They are often used in combination with other treatments, such as laser therapy or topical therapies, to optimize results. The use of deep and medium-depth peels in subjects with darker skin phototypes is not recommended due to the risk of hyperpigmentation [10]. Various types of lasers have become available in melasma treatment, particularly non ablative lasers, being widely utilized due to their lower incidence of post-inflammatory hyperpigmentation. The effectiveness of laser therapy is significantly augmented when combined with complementary topical treatments [11,12]. Microneedling is a minimally invasive procedure that causes microperforations in the skin using very thin needles. Micro-injuries stimulate neocollagenesis, neo elastogenesis and transcutaneous elimination of melanin [13]. Over the past years, this technique, alone or in combination with topical agents, has demonstrated efficacy and safety in melasma treatment, with a growing body of literature supporting its effectiveness. After a single session of microneedling using a dermaroller with 1.5 mm needles, a reduction in melanin density and pendulous melanocyte was observed, along with an improvement in MASI and quality of life [14]. Moreover, microneedling improves the effectiveness of topical therapies by increasing their transcutaneous penetration. [15] The addition of topical TXA and a depigmententing solution containing TXA, N-acetyl glucosamine, vitamin C, and idebenone to microneedling resulted in further reductions in MASI compared to microneedling alone [16] [17]. The advantages of microneedling include a low complication rate and a very low risk of post-inflammatory hyperpigmentation, making it safe even for darker phototypes [18]. Exosomes are lipid bilayer-enclosed nanovesicles released by almost all types of cells carrying proteins, DNA, long non coding RNAs (lncRNA), micro-RNAs (miRNA) and other bioactive molecules. These nano-sized vesicles typically range in diameter from 30 to 200 nanometers [19]. and are formed inside cells in endosomal compartments knowns as multivesicular bodies (MVBs). Upon fusion of MVBs with the plasma membrane, exosomes are released into the extracellular space. They play a crucial role in intercellular communication and can influence various physiological and pathological processes [20]. Exosomes exert local paracrine or distant effects and can be found in various body fluid including plasma, urine, amniotic fluid, and saliva [21]. The cargo of exosomes is dependent on the cell of origin, reflecting its physiological state, type, and environment. It can influence the behavior of recipient cells in several ways, including modulation of gene expression and alteration of cellular processes. Exosomes can be isolated and purified from different sources, such as blood, urine, mesenchymal stem cells, and adipose tissue stem cells. The isolation and characterization of exosomes involve techniques such as ultracentrifugation, size-exclusion chromography, and flow cytometry. The interest in exosomes spans across various fields of biomedical research and clinical application, especially due to their role in signaling mechanism, their potential as biomarkers for disease diagnosis, and their possible role as therapeutic agents and as vehicles for drug delivery. In the field of dermatology and aesthetic medicine, exosomes are emerging as a promising therapeutic option in various conditions, such as hair loss, scar treatment, wound healing, skin aging and pigmentation disorders [22,23]. In the skin, endogenous exosomes facilitate a complex network of interactions involving keratinocytes, fibroblast, melanocytes, macrophages, adipocytes and immune cells. They are necessary to maintain cellular functions and tissue homeostasis [24]. Exogenous exosomes, such as stem cells exosomes, can serve as novel treatment options to repair and rejuvenate skin tissues [25]. Exosomes can influence skin cell behavior, promoting wound healing, collagen synthesis, and modulating melanogenesis. Exosomes carry Wnt proteins to induce Wnt signaling activity in target cells [26]. Wnt signaling is essential for skin development and maintenance, as well as regulation of skin stem cells. Human umbilical cord mesenchymal stem-cell exosomes (hUCMSC-Exos) enhances wound closure by delivering Wnt4 to activate Wnt/β-catenin in skin cells, and inhibits acute heat stress-induced skin cell apoptosis via activation of AKT pathway [27]. In vitro and in vivo studies demonstrated the therapeutic effect of exosomes in photodamaged skin by decreasing TNF-α, while upregulating TGF-β and tissue inhibitor of MMP (TIMP). This leads to overall increased collagen I and elastin and decreased collagen III [28]. The keratinocyte-derived exosomes increase melanocyte pigmentation via miR-3196 and MITF-dependent signaling pathways or miR-203 and MITF-independent signaling pathway. On the other hand, the miR-330–5p overexpressing in keratinocyte-derived exosomes decreased the melanin production and TYR expression in melanocytes, and the miR-675 from keratinocyte exosomes involved in H19 lncRNA downregulation-stimulated melanogenesis, by inhibiting MITF expression [25]. Exosomes derived from human adipose tissue-derived mesenchymal stem/stromal cells (ASC-exosomes) are able to reduce intracellular melanin content in vitro, via affecting downstream factors of TYR (TYRP-1, TYRP-2). However, clinically relevant brightening effects are not evident, suggesting an enhancement in transdermal delivery for more meaningful efficacy [29]. A 12-week split-face study demonstrated that combined treatment with human adipose tissue stem cell-derived exosomes (HASC) and microneedling is effective for facial skin aging, showing improvement in skin hydration, elasticity, and pigmentation. In particular, the melanin index significantly decreased in the skin area treated with exosomes and microneedling compared to the area treated with microneedling alone [30]. Another study investigated the therapeutic effects and the percutaneous penetration of hUCMSC-Exos combined with microneedles, 1565 nm nonablative fractional laser (NAFL), and a plasma named Peninsula Blue Aurora Shumin Master (PBASM) for treating melasma both in rat models and human patients. In the animal study, about the effect of penetration, hUCMSC-Exos can penetrate the deep dermis under microneedles, NAFL, and PBASM treatments. All the patients showed significant clinical improvement in melasma compared to baseline, assessed through the MASI score, degree of improvement rate, and physician global assessment score (PGA). No statistically significant differences were found among the three therapeutic approaches [31]. More recently, it has been demonstrated that rose stem cell exosomes (RSCEs) harbor anti-inflammatory and regenerative properties. Research on plant exosomes is still relatively new. Plants-derived exosomes are similar in structure and function to animal exosomes and they are studied for drug delivery, cancer treatment, inflammatory diseases, and neurodegenerative disorders offering a novel, cell-free, and sustainable approach to various conditions [32]. Rose stem cells release their exosomes into the conditioned media during callus culture. The size and shape closely resemble exosomes derived from human stem cells. RSCEs are obtained by separating and refining the RSC culture supernatant. The physical characteristic of the lipid membrane and the size of 30-200 nanometers are confirmed through Nano Tracking Analysis (NTA) and Trasmission Electron Microscope (TEM). RSCE could increase the collagen production of human dermal fibroblasts by 40–120% in a dose-dependent manner and promote cellular migration by more than 20%. RSCE was found to have an anti-inflammatory function that the IL-6 production of macrophages was also reduced to 50–60%, depending on its concentration. The RSCEs are also taken up by melanocytes, leading to a reduced melanin content in the cells, suggesting that the RSCEs may have a whitening function. The exact molecular mechanism of this function is unclear, but is likely to involve multiple molecules contained in the RSCEs cargo. In summary, RSCEs contain miRNA and peptides with anti-inflammatory properties, promoting fibroblast proliferation, collagen production, and dose-dependent reduction in melanin accumulation [33]. The aim of our study was to evaluate the efficacy and safety of exosomes derived from Rosa Damascena stem cells, when used concomitantly with microneedling in women and men with facial melasma.
2. Materials and Methods
2.1. Study Design
This monocentric, observational, pilot study was conducted in a private dermatocosmetology practice and was performed during the autumn and winter season, from September 2023 to January 2024. Twenty subjects (sixteen women and four men) from eighteen to sixty-nine years of age, with Fitzpatrick skin type I-III, and facial melasma ranging from mild to severe were enrolled in this study. Subjects with the following conditions were excluded: skin marks in the experimental area (scars, hypertrichosis, nevi, tattoo), current pregnancy or lactation, history of allergy or reactivity of topical products and any previous or current topical or systemic therapies for melasma. All the subjects gave their consent before entering the study.
2.2. Study Device
The microneedling device was used with sterile, individually packaged needle cartridges that were disposable. To prevent contamination of the microneedling device, a nonsterile, disposable sheath was employed at the interface between the pen and the needle cartridge (SkinPen Precision System). The device featured 14 solid needles, each with a diameter of 0.25 mm, operating at a speed ranging from 6300 to 7700 rpm. The maximum extension of the cartridge needles was less than 2.5 mm.
2.3. Intervention
Each subject received microneedling treatment utilizing a dermapen equipped with 1.5 mm long needles, followed by topical application of exosomes (ASCE plus ®) at 4 weeks intervals, up to a maximum of five sessions. Only the facial areas affected by melasma have been treated. All subjects were advised for strict sun protection.
2.4. Photographic Documentation
Standardized photography was obtained at baseline and during follow-up visits using the VectraH1camera system (CanfieldScientific, Inc., Fairfield, NewJersey), to achieve more homogeneous and reproducible illumination. Images were taken with standard lighting, with angles set at right lateral 37°, left lateral 37°, frontal, left side and right-side views.
Skin analysis is a possible application of VECTRA technology.
2.5. mMASI
mMASI (modified Melasma Area and Severity Index) was scored by dermatologist assessment according to the method developed by Pandya et al [34]. Total mMASI score range is 0-24 and it has been categorized as follows: mild (0-8), moderate (9-16), severe (17-24). The following formula was used to calculate the mMASI:
where A is proportion of melasma area, D is darkness, F is forehead, LM is the left check, RM is the right check, and C is the chin.
mMASI = 0.3 (AF)(DF) + 0.3 (ALM)(DLM) + 0.3 (ARM)(DRM) + 0.1 (AC)(DC)
2.6. GAIS
Global Aesthetic Improvement Scale was graded by dermatologist assessment as much improved (50% or above), improved (less than 50%), and no improved, regarding the enhancement of the overall cutaneous appearance, in particular skin texture and chromatic homogeneity as compared with the original condition at baseline before treatment. The elaboration of GAIS also relied on the observation of specific parameters collected by the VECTRA at T0 and T1: spots, wrinkles, texture and brown spots.
2.7. Evaluation of Tolerability
Tolerability was evaluated by visual inspection of the skin region under experimentation, performed by a dermatologist. Assessment occurred before treatment and subsequently every 4 weeks before the treatment session, until the end of the study. Subjects were encouraged to report any potential discomfort arising from product application (burning, stinging, itching) and any adverse reaction (dryness, erythema, edema, discoloration) along with their severity (mild, moderate, severe).
2.8. Statistical Analysis
Demographic and clinical characteristics are presented as counts and percentages for categorical variables.
3. Results
3.1. Subjects
Twenty subjects were included in the study and completed it. Population characteristics and number of treatment sessions are listed in Table 1.

Table 1.
| Number of subjects (%) | ||
|---|---|---|
| Age | 18-40 | 2 (10) |
| 41-50 | 8 (40) | |
| 51-60 >60 |
6 (30) 4 (20) |
|
| Sex | Male | 4 (20) |
| Female | 16 (80) | |
| Fitzpatrick Phototype | I | 1 (5) |
| II | 12(60) | |
| III | 7(35) | |
| Number of sessions | 4 | 7 (35) |
| 5 | 13 (65) |
* Subjects baseline characteristic and total number of sessions conducted every 4 weeks.
3.2. mMASI
The mMASI was evaluated at the baseline (T0) and at the end of treatment sessions (T1)
(Figure 1). At T0, only one subject exhibited mild mMASI, maintaining this status until the end of the treatment (T1). Among the nine subjects initially classified with moderate MASI at T0, a significant 88.9% transitioned to mild mMASI at T1. Similarly, of the ten subjects with severe mMASI at T0, 40% progressed to mild mMASI (Figure 2), while 60% transitioned to moderate mMASI at T1. Remarkably, 10% of subjects showed no change in mMASI, while 90% of subjects demonstrated improvement.
3.3. GAIS
GAIS was scored by dermatologist assessment at the end of the treatment (T1).
At the end of the treatment sessions, 90% of subjects manifested improvement according to the Global Aesthetic Improvement Scale. In particular, 70% of subjects exhibited an improvement <50% and 20% of subjects showed an improvement >50% compared to the baseline, respectively. 10% of patients showed no improvement (Table 2). Skin parameters obtained with VECTRA acquisitions also confirmed the improvement (Figure 3). No statistically significant associations were found between GAIS and the other variables.
Table 2.
|
Much Improved 4 (20%) |
GAIS Improved 14 (70%) |
No Change 2 (10%) |
||
|---|---|---|---|---|
| Age (yrs) | 18-40 | 0 (0.0%) | 1 (7.1%) | 1 (50.0%) |
| 41-50 | 3 (75.0%) | 5 (35.7%) | 0 (0.0%) | |
| 51-60 >60 |
1 (25.0%) 0 (0.0%) |
4 (28.6%) 4 (28.6%) |
1 (50.0%) 0 (0.0%) |
|
| Sex | Male | 1 (25.0%) | 3 (25.0%) | 0 (0.0%) |
| Female | 3 (75.0%) | 11 (78.6%) | 2 (100%) | |
| Fitzpatrick Phototype | I | 0 (0.0%) | 1 (7.1%) | 0 (0.0%) |
| II | 4 (100%) | 6 (42.9%) | 2 (100%) | |
| III | 0 (0.0%) | 7 (50.0%) | 0 (0.0%) | |
| Number of sessions | 4 | 1 (25.0%) | 4 (28.6%) | 2 (100%) |
| 5 | 3 (75.0%) | 10 (71.4%) | 0 (0.0%) |
* Percentage and number of subjects categorized based on GAIS score according to the baseline characteristics and total number of sessions.
3.4. Evaluation of Tolerability
All subjects reported mild erythema and burning sensation in the first days following the treatment. No subject reported severe adverse reactions. All subjects reported the treatment as well-tolerated.
4. Discussion
Melasma is a challenging dermatological condition characterized by a tendency for recurrence and difficulties in achieving effective treatment. The condition entails both structural and functional alterations in the epidermis, basement membrane, and upper dermis, resulting in a distinctive hyper melanogenic phenotype. Current therapeutic approaches focus on reducing melanin production and inhibiting melanin synthesis pathways. However, the efficacy of most treatments is limited, and adverse effects are not uncommon [35] Notably, the epidermal changes associated with melasma go beyond hypermelanosis. Recent histopathological studies have unveiled additional dimensions, exposing solar elastosis, a thinner SC, atrophic granular layer, and modifications in basal keratinocytes [5]. Sun exposure emerges as a pivotal environmental factor in melasma, with both UV and visible light playing substantial roles in fostering melanin synthesis, activating tyrosinase activity, and contributing to skin photoaging [7]. The increased vascularity, coupled with heightened VEGF expression, indicates angiogenic involvement in the pathogenesis of melasma. Perivascular mast cells and infiltrating leukocytes contribute to chronic skin inflammation, potentially influencing melanocyte activity and vascular changes [36]. Consequently, an effective therapeutic approach should not only address melanin production but also target the photoaging aspects of the skin. Originally developed in the 1990s for the treatment of scars, striae, and laxity [37], microneedling has evolved into a well-known procedure for effectively managing melasma. By creating controlled micro-injuries in the epidermis and papillary dermis, a complex local regenerative response is initiated. This encompasses the proliferation of keratinocytes, leading to an increased transepidermal elimination of melanin, improvement in solar elastosis, and repair of the damaged basal membrane [38]. Furthermore, microneedling enhances the transcutaneous delivery of topical agents, creating microchannels that improves the penetration of active ingredients into the skin strata [39]. In fact, a substantial body of studies have evaluated its combination with topical or oral tranexamic acid, retinoic acid, and vitamin C, yielding encouraging results [10,40]. Due to its swift post-treatment recovery, minimal side effects, its safety in darker skin phototypes [41], and notable clinical outcomes, microneedling stands as a valuable alternative to more invasive approaches like laser skin resurfacing and deep chemical peeling [42]. Stem cell-derived exosomes (SC-Exos) are lipid-bilayer nanovesicles with 30–200 nm molecular diameter. They are produced and secreted from the cells and act as extracellular messengers. SC-Exos share attributes to stem cells (SCs), in addition to the advantages of enhanced stability and low immunogenicity. With antiaging, anti-inflammatory, and antioxidation properties, SC-Exos contribute to skin whitening and promote skin regeneration. In particular, Rose Stem Cell Exosomes (RSCEs) promote growth of skin fibroblasts and collagen production, reduced melanin production in melanocytes, and inhibition of inflammation [33].However, exosomes encounter difficulty penetrating the skin barrier. Recently, it has been demonstrated that microneedling is an effective and safe penetration-promoting method in the treatment of melasma, enhancing the percutaneous penetration of SC-Exos [31]. The presented study underscores the potential efficacy of the combination of Rosa Damascena stem cell exosomes and microneedling in addressing melasma. It is noteworthy to emphasize that our work benefits from a highly diversified patient sample, representing a strong point of our research. The analysis encompassed both male and female participants, individuals spanning various age groups, and those with different Fitzpatrick skin types. Ninety percent of subjects demonstrated a significant improvement in mMASI scores, while only 10% showed no change. GAIS assessment further supports overall improvement, with just 10% categorized as "not changed". Tolerability was favorable, marked by mild and transient side effects. It's essential to highlight the variability in responses among subjects, particularly the distinctions between those experiencing better outcomes (transition to mild mMASI) and those with less improvement (transition to moderate mMASI). Notably, half of the subjects not improving in mMASI had a mild form at baseline. This could be attributed to their condition being closer to the desired outcome with fewer pigmentary changes. The totality of subjects with moderate melasma at baseline responded well to treatment, transitioning to mild mMASI. This indicates that this kind of patient may be more receptive to the combined therapy, possibly due to less entrenched melanin deposition or more responsive skin physiology. Fifty percent of the subjects exhibited severe melasma, and all demonstrated a positive response, indicating the efficacy of the combined therapy even in challenging cases. This raises optimism for individuals traditionally deemed to have less favorable prognosis. However, within the severe melasma group, diverse responses were observed. While 40% showed improvement to mild mMASI, 60% transitioned to moderate mMASI, possibly indicating a subgroup less responsive to the intervention, influenced by intrinsic factors or a longer history of melasma. Notably, the absence of severe adverse reactions and post-inflammatory hyperpigmentation, with increased attention to individuals with darker skin types (Fitzpatrick III), along with the perception of the treatment as well-tolerated, indicates a positive safety profile. Finally, the observation that the only subjects not experiencing improvement in GAIS were those who did not undergo the maximum five sessions raises questions about the correlation between the number of sessions and treatment efficacy. This suggests that completing the entire treatment course is crucial for achieving optimal outcomes and discontinuing prematurely might limit the intervention's effectiveness.
5. Conclusions
This is the first study to investigate the clinical treatment with microneedling with topical application of Rosa Damascena stem cell exosomes. The therapeutic approach outlined in this study has proven to be both safe and effective, requiring no anesthesia and showing no allergic reactions. This makes it a promising option in melasma treatment, especially in patients with severe and moderate melasma at risk of post-inflammatory hyperpigmentation. Limitations of the study include a small sample size and the absence of a control arm with microneedling or topical exosomes application alone. Considering the positive outcome of this pilot study, a randomized control trial with increased sample size could be considered in the future to further evaluate the efficacy of this combined therapeutic approach.
Author Contributions
I.P., C.B., F.S. participated in the study design and drafting of the manuscript; image assessment, I. P.; data curation, C. I.; statistical analysis, A. S.; supervision, C.P. All authors contributed to the review and final approval of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
No ethical approval was required since our study was based on the application of a topical product which is not a drug and the utilization of a regenerative aesthetic procedure which did not require a doctor’s prescription.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets created and analyzed during this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Zhou LL, Baibergenova A. Melasma: systematic review of the systemic treatments. Int J Dermatol. 2017 Sep;56(9):902-908. Epub 2017 Feb 27. PMID: 28239840. [CrossRef]
- Kang WH, Yoon KH, Lee ES, Kim J, Lee KB, Yim H, Sohn S, Im S. Melasma: histopathological characteristics in 56 Korean patients. Br J Dermatol. 2002 Feb;146(2):228-37. PMID: 11903232. [CrossRef]
- Espósito ACC, Cassiano DP, da Silva CN, Lima PB, Dias JAF, Hassun K, Bagatin E, Miot LDB, Miot HA. Update on Melasma-Part I: Pathogenesis. Dermatol Ther (Heidelb). 2022 Sep;12(9):1967-1988. Epub 2022 Jul 29. PMID: 35904706; PMCID: PMC9464278. [CrossRef]
- Lee DJ, Park KC, Ortonne JP, Kang HY. Pendulous melanocytes: a characteristic feature of melasma and how it may occur. Br J Dermatol. 2012 Mar;166(3):684-6. Epub 2012 Feb 6. PMID: 21936855. [CrossRef]
- Kwon SH, Hwang YJ, Lee SK, Park KC. Heterogeneous Pathology of Melasma and Its Clinical Implications. Int J Mol Sci. 2016 May 26;17(6):824. PMID: 27240341; PMCID: PMC4926358. [CrossRef]
- Kang HY, Hwang JS, Lee JY, Ahn JH, Kim JY, Lee ES, Kang WH. The dermal stem cell factor and c-kit are overexpressed in melasma. Br J Dermatol. 2006 Jun;154(6):1094-9. PMID: 16704639. [CrossRef]
- Kapoor R, Dhatwalia SK, Kumar R, Rani S, Parsad D. Emerging role of dermal compartment in skin pigmentation: comprehensive review. J Eur Acad Dermatol Venereol. 2020 Dec;34(12):2757-2765. Epub 2020 May 13. PMID: 32243635. [CrossRef]
- Rendon M, Berneburg M, Arellano I, Picardo M. Treatment of melasma. J Am Acad Dermatol. 2006 May;54(5 Suppl 2):S272-81. PMID: 16631968. [CrossRef]
- Bertold C, Fontas E, Singh T, Gastaut N, Ruitort S, Wehrlen Pugliese S, Passeron T. Efficacy and safety of a novel triple combination cream compared to Kligman's trio for melasma: A 24-week double-blind prospective randomized controlled trial. J Eur Acad Dermatol Venereol. 2023 Dec;37(12):2601-2607. Epub 2023 Sep 4. PMID: 37620285. [CrossRef]
- Neagu, N., Conforti, C., Agozzino, M., Marangi, G. F., Morariu, S. H., Pellacani, G., Persichetti, P., Piccolo, D., Segreto, F., Zalaudek, I., & Dianzani, C. (2022). Melasma treatment: a systematic review. In Journal of Dermatological Treatment. [CrossRef]
- Abdel-Raouf Mohamed H, Ali Nasif G, Saad Abdel-Azim E, Abd El-Fatah Ahmed M. Comparative study of fractional Erbium: YAG laser vs combined therapy with topical steroid as an adjuvant treatment in melasma. J Cosmet Dermatol. 2019 Apr;18(2):517–23.
- Lee M-C, Chang C-S, Huang Y-L, Chang S-L, Chang C-H, Lin Y-F, et al. Treatment of melasma with mixed parameters of 1,064-nm Q-switched Nd:YAG laser toning and an enhanced effect of ultrasonic application of vitamin C: a split-face study. Lasers Med Sci. 2015 Jan;30(1):159–63.
- Jung, J. W., Kim, W. O., Jung, H. R., Kim, S. A., & Ryoo, Y. W. (2019). A face-split study to evaluate the effects of microneedle radiofrequency with Q-switched Nd:YAG laser for the treatment of melasma. Annals of Dermatology. [CrossRef]
- Cassiano DP, Esposito AC, Hassun KM, Lima EV, Bagatin E, Miot HA (2019). Early clinical and histological changes induced by microneedling in facial melasma: A pilot study. Indian J Dermatol Venereol Leprol 2019;85:638-641.
- Singh, A., & Yadav, S. (2016). Microneedling: Advances and widening horizons. Indian Dermatology Online Journal. [CrossRef]
- Saleh FY, Abdel-Azim ES, Ragaie MH, Guendy MG. Topicaltranexamic acid with microneedling versus microneedlingalone in treatment of melasma: clinical, histopathologic, and immunohistochemical study. J Egypt Women’s Dermatol Soc.2019;16(2). [CrossRef]
- Farshi S, Mansouri P. Study of efficacy of microneedling and mesoneedling in the treatment of epidermal melasma: A pilot trial. J Cosmet Dermatol. 2020; 19: 1093–1098. [CrossRef]
- Cohen, B. E., & Elbuluk, N. (2016). Microneedling in skin of color: A review of uses and efficacy. Journal of the American Academy of Dermatology. [CrossRef]
- Ha DH, Kim HK, Lee J, Kwon HH, Park GH, Yang SH, Jung JY, Choi H, Lee JH, Sung S, Yi YW, Cho BS. Mesenchymal Stem/Stromal Cell-Derived Exosomes for Immunomodulatory Therapeutics and Skin Regeneration. Cells. 2020 May 7;9(5):1157. PMID: 32392899; PMCID: PMC7290908. [CrossRef]
- From the American Association of Neurological Surgeons (AANS), American Society of Neuroradiology (ASNR), Cardiovascular and Interventional Radiology Society of Europe (CIRSE), Canadian Interventional Radiology Association (CIRA), Congress of Neurological Surgeons (CNS), European Society of Minimally Invasive Neurological Therapy (ESMINT), European Society of Neuroradiology (ESNR), European Stroke Organization (ESO), Society for Cardiovascular Angiography and Interventions (SCAI), Society of Interventional Radiology (SIR), Society of NeuroInterventional Surgery (SNIS), and World Stroke Organization (WSO); Sacks D, Baxter B, Campbell BCV, Carpenter JS, Cognard C, Dippel D, Eesa M, Fischer U, Hausegger K, Hirsch JA, Shazam Hussain M, Jansen O, Jayaraman MV, Khalessi AA, Kluck BW, Lavine S, Meyers PM, Ramee S, Rüfenacht DA, Schirmer CM, Vorwerk D. Multisociety Consensus Quality Improvement Revised Consensus Statement for Endovascular Therapy of Acute Ischemic Stroke. Int J Stroke. 2018 Aug;13(6):612-632. Epub 2018 May 22. PMID: 29786478. [CrossRef]
- Bano R, Ahmad F, Mohsin M. A perspective on the isolation and characterization of extracellular vesicles from different biofluids. RSC Adv. 2021 Jun 1;11(32):19598-19615. PMID: 35479207; PMCID: PMC9033677. [CrossRef]
- Thakur, A.; Shah, D.; Rai, D.; Parra, D.C.; Pathikonda, S.; Kurilova, S.; Cili, A. Therapeutic Values of Exosomes in Cosmetics, Skin Care, Tissue Regeneration, and Dermatological Diseases. Cosmetics 2023, 10, 65. [CrossRef]
- Olumesi KR, Goldberg DJ. A review of exosomes and their application in cutaneous medical aesthetics. J Cosmet Dermatol. 2023 Oct;22(10):2628-2634. Epub 2023 Jul 27. PMID: 37498301. [CrossRef]
- Yin, L.; Liu, X.; Shi, Y.; Ocansey, D.K.W.; Hu, Y.; Li, X.; Zhang, C.; Xu, W.; Qian, H. Therapeutic Advances of Stem Cell-Derived Extracellular Vesicles in Regenerative Medicine. Cells 2020, 9, 707. [CrossRef]
- Xiong M, Zhang Q, Hu W, Zhao C, Lv W, Yi Y, Wang Y, Tang H, Wu M, Wu Y. The novel mechanisms and applications of exosomes in dermatology and cutaneous medical aesthetics. Pharmacol Res. 2021 Apr;166:105490. Epub 2021 Feb 12. PMID: 33582246. [CrossRef]
- Gross, J., Chaudhary, V., Bartscherer, K. et al. Active Wnt proteins are secreted on exosomes. Nat Cell Biol 14, 1036–1045 (2012). [CrossRef]
- Zhang B, Wu X, Zhang X, Sun Y, Yan Y, Shi H, Zhu Y, Wu L, Pan Z, Zhu W, Qian H, Xu W. Human umbilical cord mesenchymal stem cell exosomes enhance angiogenesis through the Wnt4/β-catenin pathway. Stem Cells Transl Med. 2015 May;4(5):513-22. Epub 2015 Mar 30. PMID: 25824139; PMCID: PMC4414225. [CrossRef]
- Ku YC, Omer Sulaiman H, Anderson SR, Abtahi AR. The Potential Role of Exosomes in Aesthetic Plastic Surgery: A Review of Current Literature. Plast Reconstr Surg Glob Open. 2023 Jun 12;11(6):e5051. PMID: 37313480; PMCID: PMC10259637. [CrossRef]
- Cho, B. S., Lee, J., Won, Y., Duncan, D. I., Jin, R. C., Lee, J., Kwon, H. H., Park, G. H., Yang, S. H., Park, B. C., Park, K. Y., Youn, J., Chae, J., Jung, M., & Yi, Y. W. (2020). Skin brightening efficacy of exosomes derived from human adipose tissue-derived stem/stromal cells: A prospective, split-face, randomized placebo-controlled study. Cosmetics. [CrossRef]
- Park GH, Kwon HH, Seok J, Yang SH, Lee J, Park BC, Shin E, Park KY. Efficacy of combined treatment with human adipose tissue stem cell-derived exosome-containing solution and microneedling for facial skin aging: A 12-week prospective, randomized, split-face study. J Cosmet Dermatol. 2023 Dec;22(12):3418-3426. Epub 2023 Jun 28. PMID: 37377400. [CrossRef]
- Wang T, Gao H, Wang D, Zhang C, Hu K, Zhang H, Lin J, Chen X. Stem cell-derived exosomes in the treatment of melasma and its percutaneous penetration. Lasers Surg Med. 2023 Feb;55(2):178-189. Epub 2022 Dec 27. PMID: 36573453. [CrossRef]
- Mu N, Li J, Zeng L, You J, Li R, Qin A, Liu X, Yan F, Zhou Z. Plant-Derived Exosome-Like Nanovesicles: Current Progress and Prospects. Int J Nanomedicine. 2023 Sep 5;18:4987-5009. PMID: 37693885; PMCID: PMC10492547. [CrossRef]
- Won Yu Jin, Lee Esther, Min Seon Young, Cho Byong Seung (2023). Biological Function of Exosome-like Particles Isolated from Rose (Rosa Damascena) Stem Cell Culture Supernatant. InbioRxiv - Cell Biology 2023-10-19 . [CrossRef]
- Pandya, A. G., Hynan, L. S., Bhore, R., Riley, F. C., Guevara, I. L., Grimes, P., Nordlund, J. J., Rendon, M., Taylor, S., Gottschalk, R. W., Agim, N. G., & Ortonne, J. P. (2011). Reliability assessment and validation of the Melasma Area and Severity Index (MASI) and a new modified MASI scoring method. Journal of the American Academy of Dermatology. [CrossRef]
- Ma W, Gao Q, Liu J, Zhong X, Xu T, Wu Q, Cheng Z, Luo N, Hao P. Efficacy and safety of laser-related therapy for melasma: A systematic review and network meta-analysis. J Cosmet Dermatol. 2023 Nov;22(11):2910-2924. Epub 2023 Sep 22. PMID: 37737021. [CrossRef]
- Zhu JW, Ni YJ, Tong XY, Guo X, Wu XP. Activation of VEGF receptors in response to UVB promotes cell proliferation and melanogenesis of normal human melanocytes. Exp Cell Res. 2020 Feb 15;387(2):111798. Epub 2019 Dec 23. PMID: 31874175. [CrossRef]
- ORENTREICH, D. S., & ORENTREICH, N. (1995). Subcutaneous Incisionless (Subcision) Surgery for the Correction of Depressed Scars and Wrinkles. Dermatologic Surgery. [CrossRef]
- Cassiano, D. P., Espósito, A. C. C., Hassun, K. M., de Andrade Lima, M. M. D., de Andrade Lima, E. V., Miot, L. D. B., Miot, H. A., & Bagatin, E. (2022). Histological changes in facial melasma after treatment with triple combination cream with or without oral tranexamic acid and/or microneedling: A randomised clinical trial. Indian Journal of Dermatology, Venereology and Leprology. [CrossRef]
- Hou, A., Cohen, B., Haimovic, A., & Elbuluk, N. (2017). Microneedling: A Comprehensive Review. In Dermatologic Surgery. [CrossRef]
- Brasil dos Santos, J., Nagem Lopes, L. P., de Lima, G. G., Teixeira da Silva, R., da Silva e Souza Lorca, B., Miranda Pinheiro, G., & Faria de Freitas, Z. M. (2022). Microneedling with cutaneous delivery of topical agents for the treatment of melasma: A systematic review. Journal of Cosmetic Dermatology. [CrossRef]
- Rivas, S., & Pandya, A. G. (2013). Treatment of melasma with topical agents, peels and lasers: An evidence-based review. In American Journal of Clinical Dermatology. [CrossRef]
- Alster, T. S., & Graham, P. M. (2018). Microneedling: A review and practical guide. In Dermatologic Surgery. [CrossRef]
Figure 1.
Graphical representation of the percentage of subjects categorized based on mMASI score at T0 and T1.
Figure 1.
Graphical representation of the percentage of subjects categorized based on mMASI score at T0 and T1.
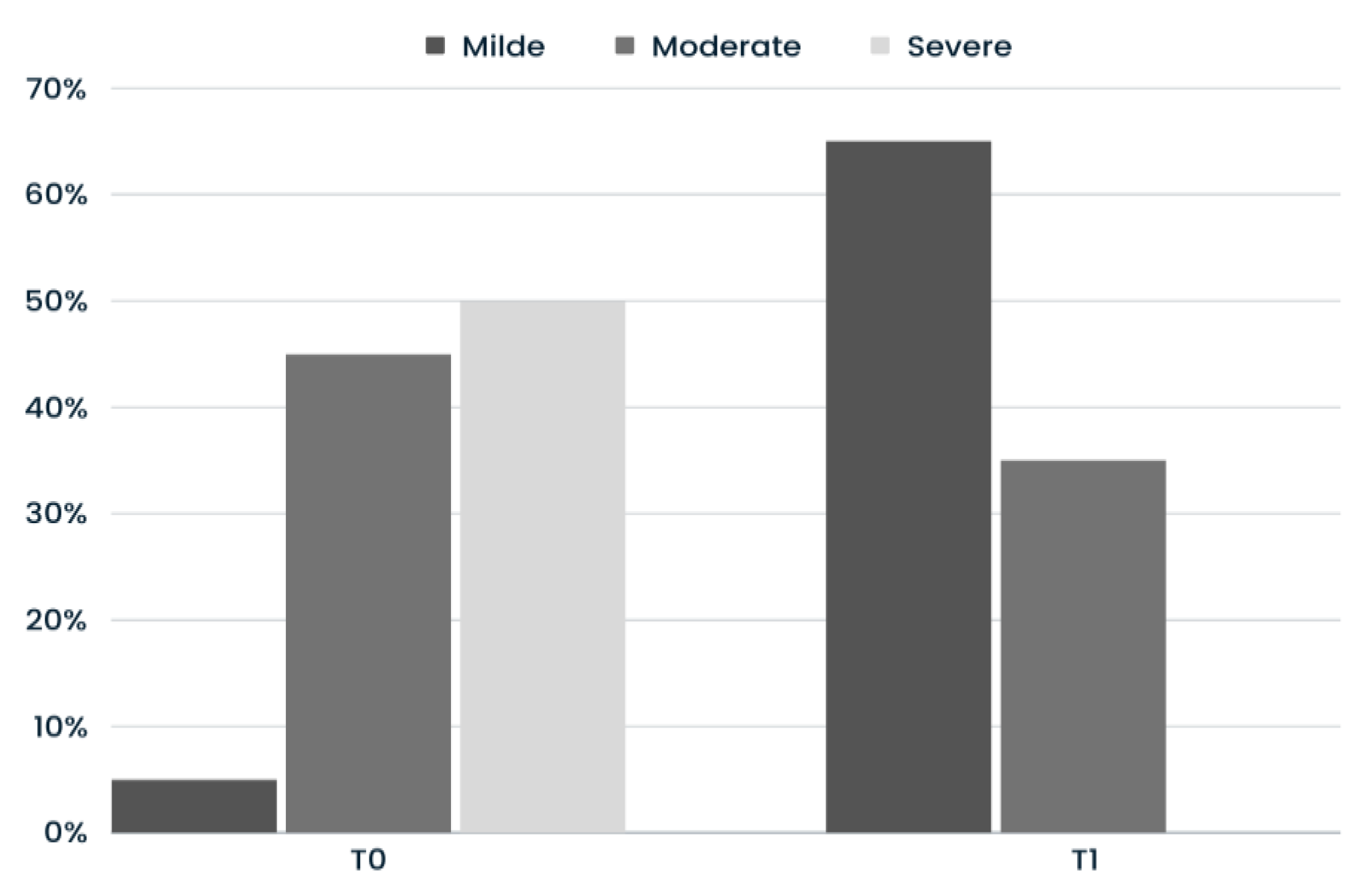
Figure 2.
VECTRA® pictures of a patient with severe mMASI at T0 who progressed to mild mMASI at T1. Frontal, right lateral 37°, right side, left lateral 37° and left side views at baseline (A,B,C,D,E); frontal, right lateral 37°, right side, left lateral 37° and left side views after five sessions of treatment (4 months) (F,G,H,I,J).
Figure 2.
VECTRA® pictures of a patient with severe mMASI at T0 who progressed to mild mMASI at T1. Frontal, right lateral 37°, right side, left lateral 37° and left side views at baseline (A,B,C,D,E); frontal, right lateral 37°, right side, left lateral 37° and left side views after five sessions of treatment (4 months) (F,G,H,I,J).
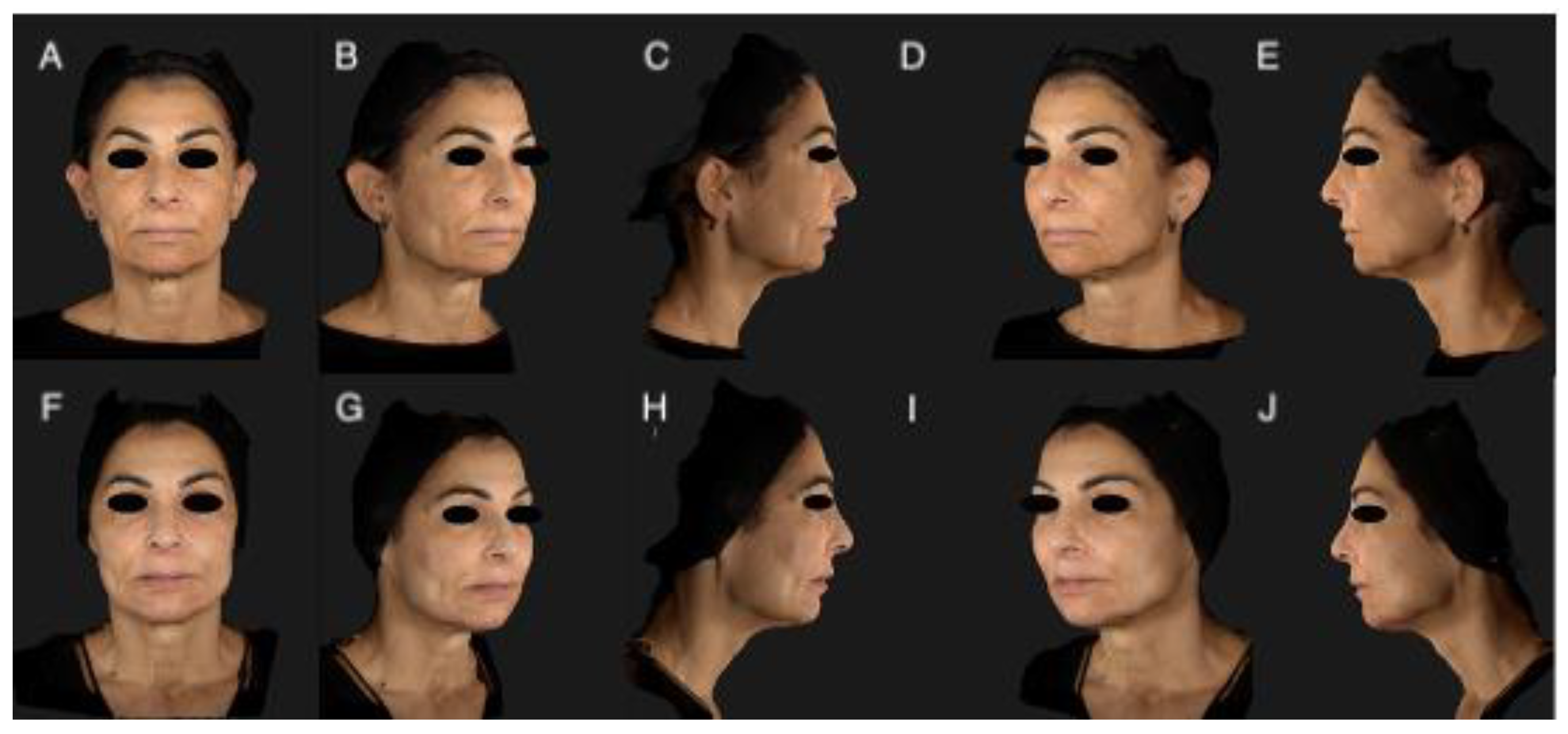
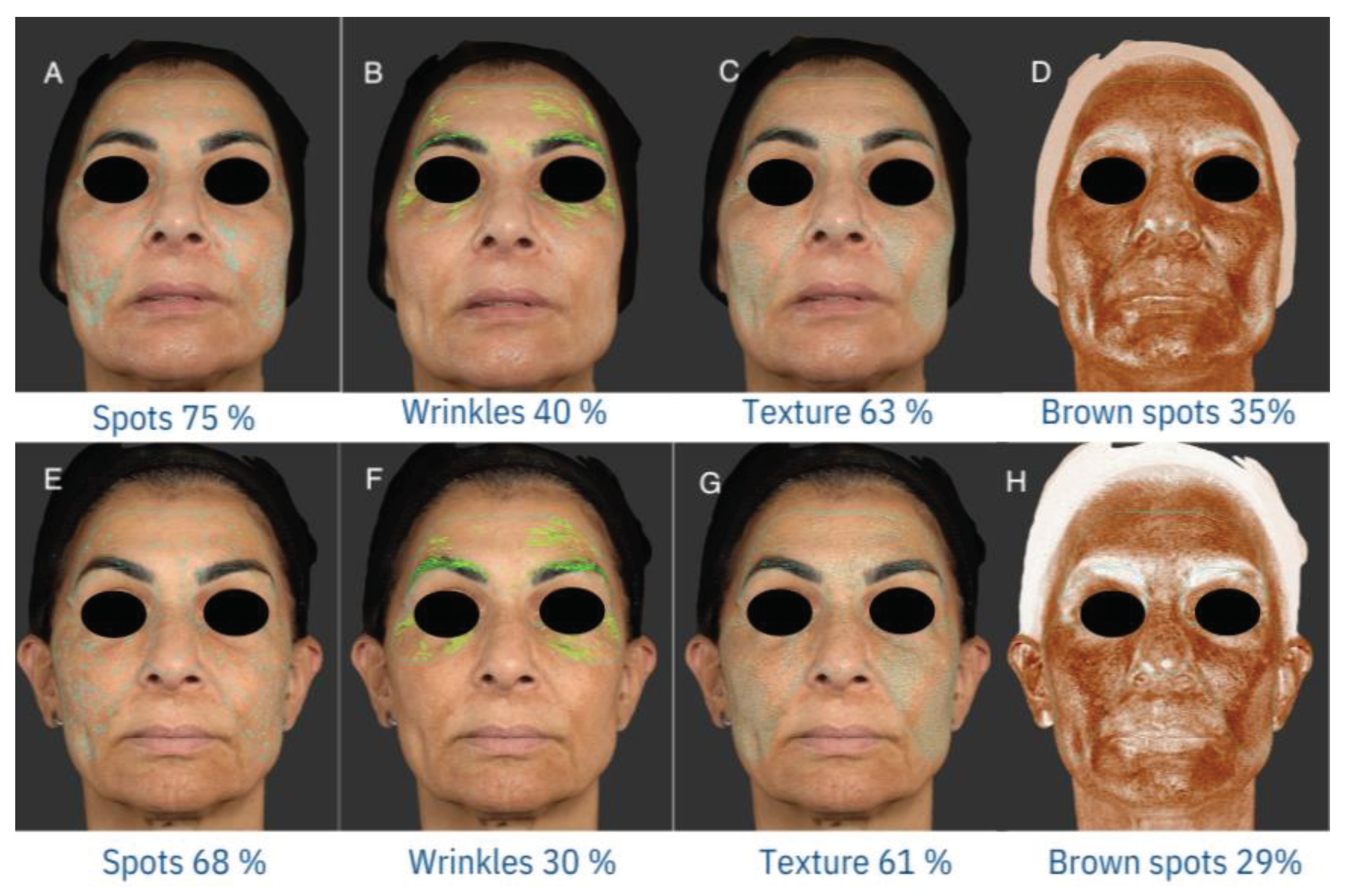
Figure 3.
VECTRA evaluation of skin parameters (spots, wrinkles, texture and brown spots) at T0 (A, B,C,D,) and T1 (E,F,G,H): a reduction in the percentage values related to all 4 analyzed parameters emerges, in particular a significant improvement in spots and brown spots is observed.
Figure 3.
VECTRA evaluation of skin parameters (spots, wrinkles, texture and brown spots) at T0 (A, B,C,D,) and T1 (E,F,G,H): a reduction in the percentage values related to all 4 analyzed parameters emerges, in particular a significant improvement in spots and brown spots is observed.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



