
Submitted:
26 February 2024
Posted:
26 February 2024
You are already at the latest version
Abstract
Proton-pump inhibitors (PPIs) are the most administered first-line treatment for eosinophilic esophagitis (EoE). However, only around half of EoE patients respond histologically to PPI at double dosage. In addition, 70% of responders maintain EoE in remission after tapering the PPI dose. In order to avoid endoscopy with biopsies − the only accurate method of assessing PPI response − efforts have been made to identify PPI responder patients. Clinical or endoscopic features and biomarkers evaluated so far however, have not proved good enough in predicting PPI response. Although new approaches based on omics technologies have uncovered promising biomarkers, the specialized and complex procedures required are difficult to implement in clinical settings. Alternatively, PPI pharmacogenetics based on identifying variations in CYP2C19 and STAT6 genes have shown promising results in EoE, and could easily be performed in most laboratories. Other genetic variations have also been associated with PPI response and may explain those cases not related to CYP2C19 or STAT6. Here, we give an overview of PPI treatment in EoE and evidence of how genetic variations in CYP2C19 and other genes could affect PPI effectiveness, and also discuss studies evaluating the role of pharmacogenetics in predicting PPI response in patients with EoE.
Keywords:
Proton-pump inhibitors
; eosinophilic esophagitis
; pharmacogenetics
; CYP219 gene
; STAT6 gene.
1. General Characteristics of Proton-Pump Inhibitors
Proton-pump inhibitors (PPIs) are a class of acid-suppressing agents which are among the most utilized drugs worldwide. They are used to treat gastroesophageal disorders, predominantly gastroesophageal reflux disease (GERD), peptic ulcer disease, Helicobacter pylori infection, erosive esophagitis, Zollinger-Ellison syndrome and eosinophilic esophagitis (EoE) [1].
PPIs are benzimidazole derivates which, after being absorbed in the small intestine, become its active form in the gastric parietal cells; they irreversibly block gastric H+/K+ adenosine triphosphatase (ATPase) pump after covalently binding to cysteine residues, thus inhibiting acid secretion. This inhibition is only reversible through the production of new proton pumps, which can take up to 54 hours [2]. Despite their short half-life of approximately one hour, the effect of PPIs lasts for 48 hours and reaches an acid suppression steady-state in 2-3 days, capable of inhibiting around 70% of daily acid production in the stomach [2].
The main pathway of metabolism of PPIs is cytochrome P450 (CYP450), specifically CYP2C19 and, to a lesser extent, CYP3A4/5 enzymes [3]. These two enzymes mediate the hydroxylation and sulfoxidation of PPIs required for their clearance, and determine the pharmacokinetic (PK) and pharmacodynamic (PD) profile of PPIs [4].
There are 5 PPI drugs approved in most developed countries: the first-generation PPIs include omeprazole, lansoprazole and pantoprazole, while the second-generation consists of esomeprazole (stereoisomer of omeprazole) and rabeprazole. There are also two further second-generation PPIs approved in some countries, dexlansoprazole in the USA and ilaprazole in Korea and China. Second generation PPIs are more effective, faster in achieving acid suppression and less dependent on CYP450 enzymatic metabolism [5].
Although they are proven safe and their prescription has been extended to other diseases, some side effects have been noted in long-term use; these include increased risk of osteoporosis in post-menopausal women, kidney damage, increased risk of certain infections (pneumonia and Clostridium difficile), and nutritional deficiencies or lower counts of platelets and hemoglobin [6]. However, most of the putative adverse outcomes associated with PPI use are not supported by high-quality evidence and are likely to have been affected by underlying confounding factors [7,8].
2. PPI Treatment in Eosinophilic Esophagitis
2.1. Brief Description of EoE Pathophysiology
EoE is a chronic, local immunity-mediated esophageal disorder, characterized clinically by symptoms of esophageal dysfunction, and histologically by an eosinophil-predominant inflammation restricted to the esophagus [9], defined by ≥15 eosinophils per high-power field (eos/HPF) at any esophageal level. First described 3 decades ago [10], EoE currently represents the leading cause of dysphagia and food impaction among children and young adults [11]. Patients with EoE commonly have concomitant atopies, resulting in allergy being involved in the origin of the disease [12]; indeed, EoE was initially characterized as a particular form of non-IgE mediated food allergy [13,14]. An increased expression of T-helper (Th)-2 cytokines in the esophageal inflammatory infiltrate, including interleukin (IL)-5, IL-4, IL-13 and thymic stromal lymphopoietin (TSLP), are involved in the pathophysiology of EoE [15], as in other type 2 inflammatory diseases [12]. These cytokines are responsible for lymphocytes differentiation, Th2 polarization in the esophageal mucosa (IL-4), proliferation, maturation and release of eosinophils from bone marrow (IL-5), production and release of eotaxins which are potent eosinophil chemoattractants (IL-13), increased permeability of the epithelial barrier (IL-3) and maturation of antigen presenting cells (TSLP), among other functions [16]. Eotaxin-3 is the highest up-regulated gene in the esophageal mucosa of EoE patients [17], its transcription depending on the STAT6 nuclear factor [18]. This results in a long-lasting inflammatory response, which affects the different layers of the esophageal wall [19], causing esophageal dysmotility [20] and promoting a fibrous remodeling that may progress into esophageal strictures [21,22].
Apart from dietary therapy to avoid food culprits from triggering and maintaining esophageal inflammation, drug therapy, mainly based on topical corticosteroids and PPIs [23], has been used to treat EoE since the first descriptions of the disease. Due to their wide availability, easy administration, convenience, and positive safety profile, PPIs represent the most commonly used first-line therapy for EoE - as repeatedly documented by series of patients of all ages and from different settings [24,25,26,27,28,29].
2.2. The Evolving Concept of PPI Response in EoE
The presence of eosinophils in the esophageal mucosa was erroneously linked to GERD in early literature [30,31]; the use of PPIs as the initial treatment, therefore excluded EoE as a diagnosis in responder patients [32]. However, a prospective series in 2011 revealed that clinical, endoscopic and histological features of EoE were not distinguishable between patients who did and did not respond to PPI therapy; whereas in a subset of patients who resolved eosinophilic infiltration in esophageal biopsies, GERD could not be demonstrated by esophageal pH-monitoring [33]. This gave rise to a provisional entity called “PPI responsive esophageal eosinophilia”, or PPI-REE, to define those patients who resolved an apparent food allergy through the use of a drug able to block gastric acid secretion [34].
Over the next few years, cumulative evidence demonstrated that patients with so-called PPI-REE and those with “classic” EoE were identical at baseline in terms of symptoms [35,36], endoscopy appearance [35,36,37], and esophageal biopsy features [36,38,39], and even showed the same altered gene expression in esophageal samples [40]. Furthermore, among responders, PPI therapy downregulated Th2 cytokines gene expression [41], reversed the abnormal EoE gene transcriptomic signature [40] and the changes induced by IL-13 responses [42], in the same way as swallowed topical steroids in EoE patients. Consequently, an international position paper [43], and European [9] and American [44] guidelines recognized PPI therapy as a true first-line therapy for patients with EoE.
2.3. PPI Dosages, Treatment Duration and Effectiveness to Induce Remission
By analogy with reflux disease, double doses of PPI for a period of 8 weeks were initially proposed for the treatment of patients with EoE [34]. This therapy had proved effective in curing peptic erosions in most patients with erosive GERD [45] and was also considered suitable for EoE.
The first prospective study that evaluated systematically the response to double dose PPI therapy in these patients revealed a 50% histological response – defined by <15 eos/HPF [33]. This rate of effectiveness was reproduced in two small randomized controlled trials [46,47] and by the first meta-analysis of 33 studies with 619, mostly European and US, EoE patients [48]. Large registries, based on data obtained from real world practice, have been recently made available: a retrospective study in 236 adult patients from Denmark disclosed histological remission in 49% of patients after treatment with an 8-week high-dose PPI trial [49]; and prospective data from the EoE CONNECT registry on 630 European patients reproduced an overall clinical plus histological remission rate of 49% [24], both studies defining histological remission as a peak eosinophil count below 15 eos/HPF. When higher histological criteria (<5 eos/HPF) were considered, remission was achieved by 33% to 40% of patients after double PPI doses [24,46,47]. In addition, in those PPI-responsive patients, PPIs proved effective in reversing endoscopic features of fibrosis and in improving esophageal distensibility [50].
The effectiveness of PPI in pediatric EoE patients has been shown to be similar, although the studies have, in general, presented more heterogeneous results, most likely due to their smaller sample sizes. In the first prospective study conducted in 51 children treated with high-dose PPI (esomeprazole 1 mg/kg, twice daily), 68% were found to have <15 eos/HPF after an 8-week trial [51]. The abovementioned meta-analysis included 188 children, among whom PPI therapy resulted in a summary estimate effectiveness of 54% [48]. More recently, an analysis of the prospective Spanish nationwide RENESE registry found that histological and clinico-histological remission was observed in 51.4% and 46.5% of the 346 children included [52].
To optimize PPI-effectiveness, extending treatment duration up to 12 weeks has shown to increase effectiveness by up to 65.2% (odds ratio=2.7, 95% CI: 1.3–5.3, compared to treatment between 8 to 10 weeks) [24]. The use of double doses in induction, compared to standard, determined the effectiveness in children [50] and adults [23]. In contrast, no significant differences in remission rates were shown for the different PPI drugs when used at equivalent doses [24]. Dividing the total PPI dose into two intakes also showed a non-significant trend in increasing its effectiveness in remission, compared to once-daily dosing [48].
2.4. Long-Term Maintenance Therapy with EoE: Effectiveness and Monitoring
Several observational studies have provided consistent data on the effectiveness of tapering doses of PPIs in maintaining long-term EoE remission among initially responding patients. In adults, 73% to 81% of patients remained in remission after 1 year with half the effective induction dose [53,54]. As for pediatric patients, 70% to 78% of initial responders to double doses remained in clinical and histological remission on tapering maintenance doses of 1 mg/kg/day after one year [51,55]. These figures have been nicely reproduced by large registries of clinical practice [24,52].
Importantly, relapsing esophageal inflammation (>15 eos/HPF) on tapering PPI doses among initial PPI responders can be effectively managed by resuming the initial higher doses [53]. Therefore, only a minimal proportion of initial PPI responders may require high-dose maintenance PPI in order to keep a sustained response.
In terms of histological remission [56], EoE symptoms have been repeatedly shown not to be reliable enough to monitor treatment response; and for PPI therapy, clinical remission rates repeatedly exceed those of histological remission. Despite considerable effort to identify non- or minimally-invasive methods to assess esophageal inflammation in EoE [57], endoscopy with biopsies currently remains the only accurate procedure. Therefore, follow-up assessment based on endoscopy with biopsies should be performed 8 to 12 weeks after the initiation of any induction treatment based on PPIs for active EoE, or after any major treatment change (eg, dose reduction or withdrawal of maintenance therapy) [58].
2.5. Clinical Predictors of PPI Effectiveness in EoE
An initial response to PPI therapy has been associated with some clinical and endoscopic aspects. Neither the age nor the sex of the patient determines the effectiveness of this therapy, nor does its use as the first or subsequent lines of treatment (after failure of dietary therapy or swallowed topical corticosteroids) [52,59,60]. On the other hand, increased body mass index was found to reduce the chances of achieving remission with PPIs [61]. The presence of fibro-stricturing endoscopic features (esophageal rings or strictures) has consistently been shown to reduce the chances of response to PPI [24,52,59,62], which could explain that patients who debuted with food impaction also had a higher probability of PPI therapy failure (adjusted odds ratio=2.8, 95% confidence interval [CI]: 1.1-7.4) [63]. Edema and vertical lines were also endoscopic features found more commonly in children who did not respond to PPIs [64].
Regarding histopathological findings, a higher score in the EoE Histology Scoring System in the middle esophagus [65] and a lower immunostaining score of filaggrin [66] were associated with reduced PPI response.
The frequency or type of concomitant atopy to EoE has not been shown to determine response to PPI [52,62]; however, higher peripheral eosinophilia at baseline independently predicted failure to PPI response in adult EoE patients in two retrospective series [61,63], and rhinoconjunctivitis (odds ratio=8.6, 95% CI: 1.5-48.7) was found to be a predictor of loss of response to PPIs during maintenance, after dose reduction [53]. In addition, higher levels of eosinophil-derived neurotoxin (EDN) were found in samples from esophageal brushing of child/young adult PPI non-responders before treatment, compared to responders [67].
2.6. Prediction of PPI Response by Omics Studies
The wide access to omics technologies have favored the application of these methodologies in studies trying to determine which patients will respond to PPIs at the point of EoE diagnosis. The first studies evaluated the transcriptome profile, but no differences were found [40,69]; a result that was later confirmed [70,71].
Although transcriptomics was unsuccessful in classifying patients into PPI responders or non-responders, a gene expression analysis did identify that EoE patients could be classified into 3 endotypes, according to the results of the EoE Diagnostic Panel composed of 95 genes [72]. Using this strategy, it might be expected that patients with the milder EoE endotype (named EoEe1) would have a greater probability of responding to PPIs than the other two endotypes.
Other approaches have also been successful in this purpose. For example, a study in a population of 39 children with EoE identified a profile of esophageal micro-RNAs, composed of miR-7-5p, miR-375-3p and miR-223-3p, able to predict the response to esomeprazole with an area under the ROC curve (AUC) of 0.90 [73].
Similarly, our group collaborated in a study that discovered a proteomic signature composed of 28 proteins that were differentially accumulated in esophageal biopsies from responder and non-responder patients [71]. This study also confirmed previous evidence with regard to no difference between PPI responders and non-responders in transcriptomic analysis.
The main limitation for clinical implementation of these three strategies is that they still require endoscopy, since esophageal biopsy is the starting material, and the specialized techniques needed for gene/miRNA/protein characterization.
3. Role of CYP2C19 in Response to PPI
Cytochrome CYP2C19 is an enzyme, and part of the CYP450 super family that contributes to the metabolism of many drugs, including antidepressant, benzodiazepines, mephenytoin, clopidogrel, and as previously mentioned, PPIs [74]. Variations in the gene encoding for CYP2C19 are the most important and well-studied pharmacogenetic factors affecting response to PPIs. Despite other possible factors, CYP2C19 genotype is responsible for a large percentage of the PK variability for PPIs [75].
3.1. Genetic Variants, Phenotypes and Populations’ Frequencies
The CYP2C19 gene is located on chromosome 10p23.33 [76] and is highly polymorphic, with 36 known variant alleles [77]. These alleles are classified into functional groups, which are based on reported in vivo or in vitro information, when available, as follows: normal function (CYP2C19*1); no function (eg. CYP2C19*2, *3, *4); decreased function (eg. CYP2C19*9); increased function (CYP2C19*17); and uncertain function (eg. CYP2C19*12, *14). Table 1 summarizes the main genetic variations of CYP2C19.
The frequency of these alleles varies between populations [77]. Among the no functional alleles, CYP2C19*2 is the most common, with a frequency of approximately 60% in Oceanians, 27-29% in Asians, 12-18% in Europeans, Africans and Americans, and around 11% in populations with Latino or Near Eastern origins. CYP2C19*3 also has a high presence in some populations, with an allele frequency of 15% in Oceanians and 2-7% in Asians, but rarely found in others. Most of the other variant alleles have below 1% frequency. Increased function allele CYP2C19*17 is present in 15-20% of African, European, Near Eastern and Latino populations, but in only 2% of East Asians and 5% of Oceanians. According to data from 2.29 million people in a study assessing the three most frequent variants (CYP2C19*2, *3, and *17), 58.3% of the participants expressed at least one increased or decreased allele function [78]. However, these allele frequency data may not be entirely accurate as they are based on published data that is limited for some populations; and most studies only test for the most common alleles, which can lead to underestimating certain alleles [76].
The combination of different alleles of the CYP2C19 gene leads to various phenotypes that are categorized according to the enzyme’s activity level (Table 2) [3,77]. Individuals with two normal function alleles are classified as CYP2C19 normal metabolizers (NM), and those individuals carrying two non-function alleles are classified as CYP2C19 poor metabolizers (PM). Individuals with one normal and one non-function allele or one non-function and one increased function allele are considered CYP2C19 intermediate metabolizers (IM). Data suggest that the loss of function caused by allele *2 has a much greater impact on the phenotype than the gain of function of allele *17, resulting in an IM phenotype [79]. Individuals carrying one normal and one increase function allele are classified as CYP2C19 rapid metabolizers (RM) and those carrying two increased function alleles are considered CYP2C19 ultrarapid metabolizers (UM). As there are limited data available for decreased function alleles, individuals carrying one decreased function and one non-function allele are classified as “likely PM”; and those carrying one normal function and one decreased function allele, or one increased function and one decreased function allele, or two decreased function alleles are currently classified as “likely IM”. Finally, those individuals carrying one or two uncertain function alleles are assigned an “indetermined metabolizer” phenotype.
The frequency of these phenotypes also differs among populations [77]. Phenotypes with non-function alleles, such as CYP2C19 PM and IM, have the highest prevalence in East Asia (13% and 46%, respectively) and Oceania (57% and 37%, respectively), and are less common in Europe (2% for PM and 26% for IM) and Africa (4% for PM and 31% for IM). Conversely, RM and UM phenotypes have a high prevalence in Europeans and Near Eastern populations (25-27% and 3-4%, respectively), and are rarely found in other populations such as East Asians (2% and 0.5%, respectively). Overall, most individuals in any part of the world have a phenotype other than NM (between 48-67%) [80].
3.2. Clinical implications of CYP2C19 phenotypes
The impact of CYP2C19 genotype on the PK and PD characteristics of PPIs varies depending on the contribution of this enzyme to the metabolism of each PPI drug [75]. In first-generation PPIs (omeprazole, lansoprazole and pantoprazole), CYP2C19 is responsible for more than 80% of their metabolism [81], making these drugs more susceptible to the impact of CYP2C19 genetic variations. The metabolism of the 2nd-generation PPI esomeprazole is less reliant on CYP2C19 compared to omeprazole [82], and therefore less affected by genetic variations in this enzyme. Rabeprazole, the other 2nd-generation PPI, is the least influenced by the genetic variations in CYP2C19, as it is mainly metabolized via a non-enzymatic pathway [83].
Several studies have shown that individuals with CYP2C19 IM and PM phenotypes exhibit decreased clearance and increased PPI plasma concentrations, when compared to NMs, which results in higher PPI exposure and leads to a more pronounced acid suppression effect, measured by intragastric pH [3,75]. The AUC of omeprazole and lansoprazole was 4 to 12 folds higher in PM than in NM phenotype carriers; and in the case of lansoprazole and rabeprazole, the AUC was 6 and 2-fold higher in PM than in NM, respectively [75]. The median intra-gastric pH was also higher in PM compared to the other phenotypes, when standard doses were given [84]. In contrast, those individuals with CYP2C19 RM and UM phenotypes have increased clearance and decreased plasma concentration compared to NM, resulting in lower PPI exposure, which may lead to an increased risk of treatment failure [3]. For these phenotypes, there is less data regarding the association with the PK/PD parameters of PPIs. This is due to the fact that most studies were carried out in populations with a low prevalence of the CYP2C19*17 allele or conducted prior to its discovery [85]. However, it has been reported that those with RM and UM phenotypes have lower AUC than those with NM, IM and PM [3,75,84].
The resulting different exposure to the drug influences PPI effectiveness in the treatment of several diseases. In the case of GERD, a meta-analysis that included 19 studies, demonstrated that the efficacy rates of PPIs varied significantly among CYP2C19 phenotypes (52,2% in NMs; 56.7% in IMs; 61.3% in PMs; p=0.047); and also, that those subjects carrying a RM phenotype had an increased risk of being refractory to PPI therapy when compared with PMs (odds ratio=1.7, 95% CI: 1.0-2.7) [86].
For the efficacy of H. pylori infection eradication therapy, a meta-analysis including 39 studies showed that regardless of the type of PPI used, treatment duration or treatment regimens, there were significant differences in eradication rates, according to CYP2C19 phenotypes, between extensive metabolizers (EM, which includes those with NM or RM phenotypes) and IMs (79.2% vs. 84.0%, odds ratio=0.7, 95 CI: 0.6-0.9,), and also between EMs and PMs (79.2% vs. 87.0%, odds ratio=0.6, 95 CI: 0.5-0.7), but not between IMs and PMs [87]. Furthermore, when different PPI drugs were evaluated, these differences were found in patients treated with omeprazole, lansoprazole and esomeprazole but not in those treated with rabeprazole (due to its mainly non-enzymatic metabolism) or pantoprazole (probably due to the small number of studies that evaluated this drug) [87].
As the influence of CYP2C19 phenotype on the clinical efficacy of PPI treatment is well documented, some clinical guidelines have included recommendations to adjust PPI dosage in certain diseases. The Clinical Pharmacogenetics Implementation Consortium (CPIC) elaborated an evidence-based guideline, which included strong recommendations for most CYP2C19 phenotypes when treated with first-generation PPIs [3]. Also, guidelines from the Dutch Pharmacogenetics Working Group (DPWG) made recommendations according to patients’ CYP2C19 phenotype, but limited them to the usage of first-generation PPIs in H. pylori eradication, and affecting only the UM phenotype [88].
4. Other Genetic Variations Influencing Response to PPIs
4.1. CYP2C18
The association between an haplotype of two SNPs close to CYP2C18 gene (rs2860840 C>T and rs11188059 G>A), CYP2C:TG, and an UM CYP2C19 phenotype was recently established by assessing escitalopram metabolism [89]. One year later, another group found that the same haplotype was also associated with treatment failure to omeprazole in GERD [90]. Specifically, they described a higher proportion of homozygous patients for CYP2C:TG compared to the reference population (New Zealand European) among patients with objective GERD, despite treatment with omeprazole (≥ 40 mg/day) for a minimum of 8 weeks (p=0.03).
Interestingly, all homozygous CYP2C:TG/TG patients did not have the variant CYP2C19*17 in both studies, thus suggesting that this haplotype could be a new genetic variant, which may explain rapid metabolism of PPIs in patients lacking of CYP2C19*17 allele.
4.2. CYP3A4/5
As mentioned previously, the CYP3A family is a secondary enzyme participating in the metabolism of most PPIs. The two main enzymes are CYP3A4 and CYP3A5, and are also involved in the biotransformation of multiple drugs (anti-depressants, calcium antagonists, immunosuppressants, opiates, statins, steroids, etc.) [91]. Although genetic variations are rare for CYP3A4, a variant for CYP3A5 implying a splicing defect is common in all populations, except African [92]. The most studied variations are CYP3A4*22 (rs35599367 C>T), which causes decreased function [93], and CYP3A5*3 (rs776746 T>C), which showed lack of activity [94].
To date, no proven relevant effect of genetic variants in CYP3A4/5 on PPI metabolism has been found, excepting CYP3A5*3/*3 genotype influence on ilaprazole clearance, described in a Chinese population [95]. However, CYP3A4/5 variants could be important in certain situations due to drug-drug-gene interactions [80]. For example, the proportion of PPI metabolized by CYP3A is higher in CYP2C19 IMs and PMs [96,97]; thus, treatments with other drugs metabolized by CYP3A could mutually affect their concentrations, or concomitant treatment with any drug inhibiting CYP3A could lead to increased risk of PPI adverse events [98]. Another case in which CYP3A4/5 genetic variants could have more influence in PPI response is in CYP2C19 inhibition by drugs such as fluvoxamine. As rabeprazole is rarely metabolized by these pathways, it is suggested as the PPI to be chosen for patients concomitantly treated with drugs metabolized by CYP2C19, and/or CYP3A or inhibiting these enzymes [98].
4.3. ABCB1
ABCB1 gene, (ATP-binding cassette, sub-family B, member 1; formerly known as multidrug resistance transporter gene 1 or MDR1), codifies a P-glycoprotein involved in the absorption of PPIs in the small intestine. This protein is also involved in the bioavailability of multiple drugs, and some of its genetic variations are associated with clinical implications [99].
One of its most studied SNPs, rs1045642 (C3435T), has been investigated in two studies assessing its influence in lansoprazole PK and PD. In the first of these, higher plasma levels of lansoprazole were found in 15 Japanese subjects (all CYP2C19*1/*1) with the rs1045642-TT genotype, but no effect was observed regarding intragastric pH [100]. In the other study, including 24 healthy Chinese volunteers, only a trend to improved absorption and rapid elimination for rs1045642 wild type subjects was detected, while the effect on PK parameters was significant for different CYP2C19 genotypes [101]. Therefore, according to these results, although rs1045642 could have a role in PPI effectiveness, its effect would be minor and less important than that exerted by CYP2C19 variations.
4.4. ATP4A
The gastric H+/K+-ATPase pump is responsible for generating the acidic environment in the stomach and it is the main target of PPIs [102]. Therefore, it makes sense that genetic variations on this pump could affect PPI effectiveness. This issue was investigated by a Chinese group, which analyzed the influence of the rs2733743 (ATP4A A>G) in acid suppression by dexlansoprazole injections in 51 healthy subjects [103].
Firstly, they found that this variation was quite common in their population, with 35% in heterozygosis and 38% in homozygosis. Secondly, they compared gastric acid inhibition among different genetic variations for CYP2C19, ABCB1 and the aforementioned rs2733743, and discovered that the inhibitory effect was affected by CYP2C19 genotypes and in rs2733743 homozygotes (GG genotype), with the latter showing a greater inhibition [103]. To date, no other studies have confirmed this association in other populations.
4.5. STAT6
Signal Transducer and Activator of Transcription 6 (STAT6) is a mediator of T helper type 2 cell-response and its synthesis is stimulated by certain interleukins, mainly IL-4 and IL-13. STAT6 has thus an important role in atopy and allergic diseases, including EoE [104,105]. Precisely, eosinophilic infiltration in the esophagus is led by eotaxin-3, whose expression is stimulated by STAT6. As PPIs can block STAT6 binding to the eotaxin-3 promoter [106], it is feasible to consider that genetic variations in STAT6 could affect PPI response in EoE.
This hypothesis was investigated by Mougey et al. in two studies that recruited children with EoE, in whom 8 SNPs of STAT6 were determined [68,107]. Their results are described in detail in the next section of this review and summarized jointly with the other genetic variations affecting PPI response in Table 3.
5. Pharmacogenetic Studies on PPI Effectiveness in EoE
To date, only four studies - three full papers and one congress abstract - have evaluated the role of pharmacogenetics in PPI response in EoE. Two of these analyzed CYP2C19 genotypes only, while the other two, performed by the same research group, determined genetic variants in CYP2C19 and STAT6.
The first study analyzing the influence of pharmacogenetics in the response to PPIs in EoE was carried out in 2015 [53]. In this study, 75 adult patients with EoE from 8 hospitals in 4 different countries were included. CYP2C19 was genotyped in 50 patients who initially achieved remission with PPIs, and its association with loss of histological response after dose reduction was evaluated. Maintenance treatment length until effectiveness assessment was highly variable (minimum one year, mean of 26 months), as were PPI drugs used (omeprazole, esomeprazole and pantoprazole) and dosages (60% double doses and 40% single dose). In univariate analysis, subjects with *1/*1 genotype and those with at least one *17 allele (66% of patients) were more frequent in the group of patients who experience EoE recurrence (36% vs. 6%). In the multivariate model, these patients showed a 12.5-fold increase in the odds of losing response.
The next two studies were undertaken by the same researchers in a cohort of children with EoE from two Spanish hospitals, and evaluated the influence of CYP2C19 and STAT6 in the histological response to PPIs [68,107].
In the first, 92 children were included, mainly treated with esomeprazole (96%) at different doses (ranging between 0.46 and 2.40 mg/Kg/day) to induce EoE remission [107]. Regarding CYP2C19, subjects carrying the CYP2C19*17 allele had 7.7 times greater probability of not responding to PPIs. Interesting findings were observed for STAT6 variations. Firstly, SNP rs324011 (which is in linkage disequilibrium with rs167769 and rs12368672) showed association with the peak of eos/HPF in distal biopsies before treatment, with a 1.7-fold increase in subjects with TT genotype. In addition, this SNP showed a synergistic effect with CYP2C19*17, as having this allele and 1 or 2 copies of the variant for rs324011 (genotypes CT/TT) increased to 8.7 times the odds of not responding to PPIs. Another SNP, the rs1059513 also displayed relevant results, as carrying 1 or 2 copies of the variant (genotypes TC/CC) was independently associated with response to PPIs; with a 6.2-fold increase of achieving histological response in the full cohort and 14.9-fold better odds for individuals who do not carry the CYP2C19*17 allele.
In the following study by Mougey et al. performed two years later [68], a group of 73 child responders to PPI (mostly from the same cohort used in the previous study), who had dose reduction in their PPI treatment for maintenance of remission (dose range for maintenance was 0.23 to 1.22 mg/Kg/day) were included. Endoscopic assessment was carried out after 1 year and the influence of variants in CYP2C19 and STAT6 were again analyzed. The CT/TT genotypes of rs324011 showed higher probability of EoE relapse, with a 2.8-fold increase of having ≥15 eos/HPF after PPI reduction. A similar effect was observed for the other two SNPs in linkage disequilibrium (rs167769 and rs12368672). Interestingly, they did not detect significant associations between CYP2C19*17 (or combinations of this allele with the former 3 SNPs of STAT6) and maintenance of EoE remission.
Although providing relevant data about the effect of CYP2C19 and STAT variants in the response to PPIs, both for induction and maintenance of remission in EoE, the studies of Mougey et al. had limitations. These included small sample size, variation in PPI dose and length of therapy for induction, including only pediatric populations, and not assessing the adherence to PPI therapy.
Finally, Bortolin et al. described CYP2C19 genotyping in a group of 37 Canadian children with EoE, and found a high proportion of RM and UM variants (32% and 11%, respectively) [108]. In this cohort, pharmacogenetic testing to guide PPI dosing resulted in treatment change in 78% of patients - mainly dose increase and PPI switch to rabeprazole in RM (25% dose increase and 42% PPI switch) and UM (100% PPI switch) carrier children. However, results relating to effectiveness before and after CYP2C19 genotyping were not available, and have not been published as a full paper as yet.
In summary, 3 out of the 4 studies were only carried out in pediatric populations; and with regard to the influence of SNPs on PPI response, 1 study provided data on induction of remission, 2 on maintenance of remission after dose decrease, and the abstract described no information at all. Furthermore, all studies were limited by a low number of patients with heterogeneous management of dosing, PPI drug and treatment length.
6. Conclusions and Future Perspectives
PPIs are widely recognized as a treatment option for patients with EoE, being the first preferred alternative in many countries and sites. Previous studies are concordant with the fact that PPIs at double dosage are effective in achieving histological response in approximately half of patients; and that in approximately 70% of these remission is maintained after dose reduction to standard ones. However, it is not possible, in the clinical setting today, to predict which patient will respond to this therapy. Clinical and molecular variables could help in identifying some patients with reduced chances of response, but their predictive power is far from being adequate (Figure 1). No biomarkers have been established for this purpose and, although miRNA and proteomic profiles from esophageal biopsies have shown some predictive capacity, it seems unlikely that these procedures could be applied in the clinical laboratory routine.
On the other hand, pharmacogenetics represents an interesting option, being successful for other drugs, does not require invasive testing and may be performed in most laboratories. Currently, the effect of CYP2C19 variants on PPI effectiveness in other diseases (such as GERD and H. pylori eradication) is well-described and included in clinical guidelines. However, pharmacogenetics of PPIs in EoE began only recently, with just four studies focused on this issue, analyzing CYP2C19 and STAT6 variants in small cohorts (Figure 1). Results are promising, but limited by the low number of patients and the heterogenous characteristics of PPI treatments.
Consequently, current evidence suggests that there may be a role for genetic variants in CYP2C19 and STAT6 genes in determining PPI response. Additional studies including higher cohorts, with adult patients, in more controlled conditions, and analysis of more SNPs related to EoE and PPI metabolism however are needed to establish whether these findings could be applied in routine clinical practice.
Nevertheless, the response to treatment with PPIs most likely depends on a combination of different clinical, molecular and genetic factors, and to date no integrative model has been proposed to allow an effective and personalized approach for patients.
Author Contributions
Conceptualization: LRA, AJL and EJLM; writing—original draft preparation: LRA, AJL and EJLM; writing—review and editing: LRA, PN, LAG, EGN, AJL and EJLM. All authors have read and agreed to the published version of the manuscript.
Funding
Leticia Rodríguez-Alcolado is a recipient of a predoctoral contract for Health Research Training – PFIS grant (FI22/00013) from the Instituto de Salud Carlos III (ISCIII), Spanish Ministry of Health – Social Services and Equality, which is partly funded by the European Social Fund. This work was supported by two grants from the ISCIII to Alfredo J Lucendo (PI21/01036) and Emilio J Laserna Mendieta (PI21/00579).
Acknowledgments
We are grateful to Melanie Radcliff for English language revision.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the in the writing of the manuscript; or in the decision to publish the results.
References
- Strand, D.S.; Kim, D.; Peura, D.A. 25 Years of Proton Pump Inhibitors: A Comprehensive Review. Gut Liver 2017, 11, 27–37. [CrossRef]
- Shin, J.M.; Sachs, G. Pharmacology of Proton Pump Inhibitors. Curr Gastroenterol Rep 2008, 10, 528–534. [CrossRef]
- Lima, J.J.; Thomas, C.D.; Barbarino, J.; Desta, Z.; Van Driest, S.L.; El Rouby, N.; Johnson, J.A.; Cavallari, L.H.; Shakhnovich, V.; Thacker, D.L.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C19 and Proton Pump Inhibitor Dosing. Clin Pharmacol Ther 2021, 109, 1417–1423. [CrossRef]
- Zhang, H.-J.; Zhang, X.-H.; Liu, J.; Sun, L.-N.; Shen, Y.-W.; Zhou, C.; Zhang, H.-W.; Xie, L.-J.; Chen, J.; Liu, Y.; et al. Effects of Genetic Polymorphisms on the Pharmacokinetics and Pharmacodynamics of Proton Pump Inhibitors. Pharmacological Research 2020, 152, 104606. [CrossRef]
- Robinson, M. New-Generation Proton Pump Inhibitors: Overcoming the Limitations of Early-Generation Agents. Eur J Gastroenterol Hepatol 2001, 13 Suppl 1, S43-47.
- Yu, L.-Y.; Sun, L.-N.; Zhang, X.-H.; Li, Y.-Q.; Yu, L.; Yuan, Z.-Q.-Y.; Meng, L.; Zhang, H.-W.; Wang, Y.-Q. A Review of the Novel Application and Potential Adverse Effects of Proton Pump Inhibitors. Adv Ther 2017, 34, 1070–1086. [CrossRef]
- Vaezi, M.F.; Yang, Y.-X.; Howden, C.W. Complications of Proton Pump Inhibitor Therapy. Gastroenterology 2017, 153, 35–48. [CrossRef]
- Veettil, S.K.; Sadoyu, S.; Bald, E.M.; Chandran, V.P.; Khuu, S.A.T.; Pitak, P.; Lee, Y.Y.; Nair, A.B.; Antony, P.T.; Ford, A.C.; et al. Association of Proton-Pump Inhibitor Use with Adverse Health Outcomes: A Systematic Umbrella Review of Meta-Analyses of Cohort Studies and Randomised Controlled Trials. Br J Clin Pharmacol 2022, 88, 1551–1566. [CrossRef]
- Lucendo, A.J.; Molina-Infante, J.; Arias, A.; von Arnim, U.; Bredenoord, A.J.; Bussmann, C.; Amil Dias, J.; Bove, M.; Gonzalez-Cervera, J.; Larsson, H.; et al. Guidelines on Eosinophilic Esophagitis: Evidence-Based Statements and Recommendations for Diagnosis and Management in Children and Adults. United European Gastroenterol J 2017, 5, 335–358. [CrossRef]
- Attwood, S.E.; Smyrk, T.C.; Demeester, T.R.; Jones, J.B. Esophageal Eosinophilia with Dysphagia. A Distinct Clinicopathologic Syndrome. Dig. Dis. Sci. 1993, 38, 109–116. [CrossRef]
- Arias, Á.; Lucendo, A.J. Epidemiology and Risk Factors for Eosinophilic Esophagitis: Lessons for Clinicians. Expert Review of Gastroenterology & Hepatology 2020, 14, 1069–1082. [CrossRef]
- McCormick, J.P.; Lee, J.T. Insights into the Implications of Coexisting Type 2 Inflammatory Diseases. J Inflamm Res 2021, 14, 4259–4266. [CrossRef]
- Kelly, K.J.; Lazenby, A.J.; Rowe, P.C.; Yardley, J.H.; Perman, J.A.; Sampson, H.A. Eosinophilic Esophagitis Attributed to Gastroesophageal Reflux: Improvement with an Amino Acid-Based Formula. Gastroenterology 1995, 109, 1503–1512. [CrossRef]
- Simon, D.; Cianferoni, A.; Spergel, J.M.; Aceves, S.; Holbreich, M.; Venter, C.; Rothenberg, M.E.; Terreehorst, I.; Muraro, A.; Lucendo, A.J.; et al. Eosinophilic Esophagitis Is Characterized by a Non-IgE-Mediated Food Hypersensitivity. Allergy 2016, 71, 611–620. [CrossRef]
- Underwood, B.; Troutman, T.D.; Schwartz, J.T. Breaking down the Complex Pathophysiology of Eosinophilic Esophagitis. Ann Allergy Asthma Immunol 2023, 130, 28–39. [CrossRef]
- Racca, F.; Pellegatta, G.; Cataldo, G.; Vespa, E.; Carlani, E.; Pelaia, C.; Paoletti, G.; Messina, M.R.; Nappi, E.; Canonica, G.W.; et al. Type 2 Inflammation in Eosinophilic Esophagitis: From Pathophysiology to Therapeutic Targets. Front Physiol 2021, 12, 815842. [CrossRef]
- Blanchard, C.; Wang, N.; Stringer, K.F.; Mishra, A.; Fulkerson, P.C.; Abonia, J.P.; Jameson, S.C.; Kirby, C.; Konikoff, M.R.; Collins, M.H.; et al. Eotaxin-3 and a Uniquely Conserved Gene-Expression Profile in Eosinophilic Esophagitis. J. Clin. Invest. 2006, 116, 536–547. [CrossRef]
- Mishra, A.; Rothenberg, M.E. Intratracheal IL-13 Induces Eosinophilic Esophagitis by an IL-5, Eotaxin-1, and STAT6-Dependent Mechanism. Gastroenterology 2003, 125, 1419–1427. [CrossRef]
- Fontillon, M.; Lucendo, A.J. Transmural Eosinophilic Infiltration and Fibrosis in a Patient with Non-Traumatic Boerhaave’s Syndrome Due to Eosinophilic Esophagitis. Am J Gastroenterol 2012, 107, 1762. [CrossRef]
- Visaggi, P.; Ghisa, M.; Marabotto, E.; Venturini, A.; Stefani Donati, D.; Bellini, M.; Savarino, V.; de Bortoli, N.; Savarino, E. Esophageal Dysmotility in Patients with Eosinophilic Esophagitis: Pathogenesis, Assessment Tools, Manometric Characteristics, and Clinical Implications. Esophagus 2023, 20, 29–38. [CrossRef]
- Aceves, S.S.; Alexander, J.A.; Baron, T.H.; Bredenoord, A.J.; Day, L.; Dellon, E.S.; Falk, G.W.; Furuta, G.T.; Gonsalves, N.; Hirano, I.; et al. Endoscopic Approach to Eosinophilic Esophagitis: American Society for Gastrointestinal Endoscopy Consensus Conference. Gastrointest Endosc 2022, 96, 576-592.e1. [CrossRef]
- Arias-González, L.; Rodríguez-Alcolado, L.; Laserna-Mendieta, E.J.; Navarro, P.; Lucendo, A.J.; Grueso-Navarro, E. Fibrous Remodeling in Eosinophilic Esophagitis: Clinical Facts and Pathophysiological Uncertainties. Int J Mol Sci 2024, 25, 927. [CrossRef]
- Tamarit-Sebastian, S.; Ferrer-Soler, F.M.; Lucendo, A.J. Current Options and Investigational Drugs for the Treatment of Eosinophilic Esophagitis. Expert Opin Investig Drugs 2022, 1–18. [CrossRef]
- Laserna-Mendieta, E.J.; Casabona, S.; Guagnozzi, D.; Savarino, E.; Perelló, A.; Guardiola-Arévalo, A.; Barrio, J.; Pérez-Martínez, I.; Lund Krarup, A.; Alcedo, J.; et al. Efficacy of Proton Pump Inhibitor Therapy for Eosinophilic Oesophagitis in 630 Patients: Results from the EoE Connect Registry. Alimentary Pharmacology & Therapeutics 2020, 52, 798–807. [CrossRef]
- Tourlamain, G.; Garcia-Puig, R.; Gutiérrez-Junquera, C.; Papadopoulou, A.; Roma, E.; Kalach, N.; Oudshoorn, J.; Sokollik, C.; Karolewska-Bochenek, K.; Oliva, S.; et al. Differences in Management of Eosinophilic Esophagitis in Europe: An Assessment of Current Practice. J Pediatr Gastroenterol Nutr 2020, Publish Ahead of Print. [CrossRef]
- Chang, J.W.; Saini, S.D.; Mellinger, J.L.; Chen, J.W.; Zikmund-Fisher, B.J.; Rubenstein, J.H. Management of Eosinophilic Esophagitis Is Often Discordant with Guidelines and Not Patient-Centered: Results of a Survey of Gastroenterologists. Dis. Esophagus 2019, 32. [CrossRef]
- Hannan, N.; Steel, A.; McMillan, S.S.; Tiralongo, E. Health Service Use and Treatment Choices for Pediatric Eosinophilic Esophagitis: Findings From a Cross-Sectional Survey of Australian Carers. Frontiers in Pediatrics 2020, 8. [CrossRef]
- Miehlke, S.; von Arnim, U.; Schlag, C.; Frieling, T.; Madisch, A.; Loibl, R.; Mainz, D.; Labenz, J. Clinical Management of Eosinophilic Esophagitis - a Nationwide Survey among Gastroenterologists in Germany. Z Gastroenterol 2019, 57, 745–752. [CrossRef]
- Zifman, E.; Banai, H.; Shamir, R.; Ringel-Kulka, T.; Zevit, N. Practice Differences in the Diagnosis and Management of Eosinophilic Esophagitis Among Adult and Pediatric Gastroenterologists in Israel. J Pediatr Gastroenterol Nutr 2018, 67, 34–39. [CrossRef]
- Winter, H.S.; Madara, J.L.; Stafford, R.J.; Grand, R.J.; Quinlan, J.E.; Goldman, H. Intraepithelial Eosinophils: A New Diagnostic Criterion for Reflux Esophagitis. Gastroenterology 1982, 83, 818–823. [CrossRef]
- Brown, L.F.; Goldman, H.; Antonioli, D.A. Intraepithelial Eosinophils in Endoscopic Biopsies of Adults with Reflux Esophagitis. Am J Surg Pathol 1984, 8, 899–905. [CrossRef]
- Furuta, G.T.; Liacouras, C.A.; Collins, M.H.; Gupta, S.K.; Justinich, C.; Putnam, P.E.; Bonis, P.; Hassall, E.; Straumann, A.; Rothenberg, M.E.; et al. Eosinophilic Esophagitis in Children and Adults: A Systematic Review and Consensus Recommendations for Diagnosis and Treatment. Gastroenterology 2007, 133, 1342–1363. [CrossRef]
- Molina-Infante, J.; Ferrando-Lamana, L.; Ripoll, C.; Hernandez-Alonso, M.; Mateos, J.M.; Fernandez-Bermejo, M.; Dueñas, C.; Fernandez-Gonzalez, N.; Quintana, E.M.; Gonzalez-Nuñez, M.A. Esophageal Eosinophilic Infiltration Responds to Proton Pump Inhibition in Most Adults. Clin. Gastroenterol. Hepatol. 2011, 9, 110–117. [CrossRef]
- Liacouras, C.A.; Furuta, G.T.; Hirano, I.; Atkins, D.; Attwood, S.E.; Bonis, P.A.; Burks, A.W.; Chehade, M.; Collins, M.H.; Dellon, E.S.; et al. Eosinophilic Esophagitis: Updated Consensus Recommendations for Children and Adults. Journal of Allergy and Clinical Immunology 2011, 128, 3–20. [CrossRef]
- Dellon, E.S.; Speck, O.; Woodward, K.; Gebhart, J.H.; Madanick, R.D.; Levinson, S.; Fritchie, K.J.; Woosley, J.T.; Shaheen, N.J. Clinical and Endoscopic Characteristics Do Not Reliably Differentiate PPI-Responsive Esophageal Eosinophilia and Eosinophilic Esophagitis in Patients Undergoing Upper Endoscopy: A Prospective Cohort Study. Am J Gastroenterol 2013, 108, 1854–1860. [CrossRef]
- Moawad, F.J.; Schoepfer, A.M.; Safroneeva, E.; Ally, M.R.; Chen, Y.-J.; Maydonovitch, C.L.; Wong, R.K.H. Eosinophilic Oesophagitis and Proton Pump Inhibitor-Responsive Oesophageal Eosinophilia Have Similar Clinical, Endoscopic and Histological Findings. Alimentary Pharmacology and Therapeutics 2014, 39, 603–608. [CrossRef]
- Warners, M.J.; van Rhijn, B.D.; Curvers, W.L.; Smout, A.J.P.M.; Bredenoord, A.J. PPI-Responsive Esophageal Eosinophilia Cannot Be Distinguished from Eosinophilic Esophagitis by Endoscopic Signs. Eur J Gastroenterol Hepatol 2015, 27, 506–511. [CrossRef]
- van Rhijn, B.D.; Weijenborg, P.W.; Verheij, J.; van den Bergh Weerman, M.A.; Verseijden, C.; van den Wijngaard, R.M.J.G.J.; de Jonge, W.J.; Smout, A.J.P.M.; Bredenoord, A.J. Proton Pump Inhibitors Partially Restore Mucosal Integrity in Patients with Proton Pump Inhibitor-Responsive Esophageal Eosinophilia but Not Eosinophilic Esophagitis. Clin. Gastroenterol. Hepatol. 2014, 12, 1815-1823.e2. [CrossRef]
- Jung, D.H.; Yun, G.-W.; Lee, Y.J.; Jo, Y.; Park, H. Clinicopathologic Analysis of Proton Pump Inhibitor-Responsive Esophageal Eosinophilia in Korean Patients. Gut Liver 2016, 10, 37–41. [CrossRef]
- Wen, T.; Dellon, E.S.; Moawad, F.J.; Furuta, G.T.; Aceves, S.S.; Rothenberg, M.E. Transcriptome Analysis of Proton Pump Inhibitor-Responsive Esophageal Eosinophilia Reveals Proton Pump Inhibitor-Reversible Allergic Inflammation. J. Allergy Clin. Immunol. 2015, 135, 187–197. [CrossRef]
- Molina-Infante, J.; Rivas, M.D.; Hernandez-Alonso, M.; Vinagre-Rodríguez, G.; Mateos-Rodríguez, J.M.; Dueñas-Sadornil, C.; Perez-Gallardo, B.; Ferrando-Lamana, L.; Fernandez-Gonzalez, N.; Bañares, R.; et al. Proton Pump Inhibitor-Responsive Oesophageal Eosinophilia Correlates with Downregulation of Eotaxin-3 and Th2 Cytokines Overexpression. Alimentary Pharmacology and Therapeutics 2014, 40, 955–965. [CrossRef]
- Rochman, M.; Xie, Y.M.; Mack, L.; Caldwell, J.M.; Klingler, A.M.; Osswald, G.A.; Azouz, N.P.; Rothenberg, M.E. Broad Transcriptional Response of the Human Esophageal Epithelium to Proton Pump Inhibitors. J Allergy Clin Immunol 2021, 147, 1924–1935. [CrossRef]
- Molina-Infante, J.; Bredenoord, A.J.; Cheng, E.; Dellon, E.S.; Furuta, G.T.; Gupta, S.K.; Hirano, I.; Katzka, D.A.; Moawad, F.J.; Rothenberg, M.E.; et al. Proton Pump Inhibitor-Responsive Oesophageal Eosinophilia: An Entity Challenging Current Diagnostic Criteria for Eosinophilic Oesophagitis. Gut 2016, 65, 521–531. [CrossRef]
- Dellon, E.S.; Liacouras, C.A.; Molina-Infante, J.; Furuta, G.T.; Spergel, J.M.; Zevit, N.; Spechler, S.J.; Attwood, S.E.; Straumann, A.; Aceves, S.S.; et al. Updated International Consensus Diagnostic Criteria for Eosinophilic Esophagitis: Proceedings of the AGREE Conference. Gastroenterology 2018. [CrossRef]
- Sontag, S.J.; Hirschowitz, B.I.; Holt, S.; Robinson, M.G.; Behar, J.; Berenson, M.M.; McCullough, A.; Ippoliti, A.F.; Richter, J.E.; Ahtaridis, G. Two Doses of Omeprazole versus Placebo in Symptomatic Erosive Esophagitis: The U.S. Multicenter Study. Gastroenterology 1992, 102, 109–118. [CrossRef]
- Peterson, K.A.; Thomas, K.L.; Hilden, K.; Emerson, L.L.; Wills, J.C.; Fang, J.C. Comparison of Esomeprazole to Aerosolized, Swallowed Fluticasone for Eosinophilic Esophagitis. Dig. Dis. Sci. 2010, 55, 1313–1319. [CrossRef]
- Moawad, F.J.; Veerappan, G.R.; Dias, J.A.; Baker, T.P.; Maydonovitch, C.L.; Wong, R.K.H. Randomized Controlled Trial Comparing Aerosolized Swallowed Fluticasone to Esomeprazole for Esophageal Eosinophilia. Am. J. Gastroenterol. 2013, 108, 366–372. [CrossRef]
- Lucendo, A.J.; Arias, A.; Molina-Infante, J. Efficacy of Proton Pump Inhibitor Drugs for Inducing Clinical and Histologic Remission in Patients With Symptomatic Esophageal Eosinophilia: A Systematic Review and Meta-Analysis. Clin Gastroenterol Hepatol 2016, 14, 13-22.e1. [CrossRef]
- Frandsen, L.T.; Westmark, S.; Melgaard, D.; Krarup, A.L. Effectiveness of PPI Treatment and Guideline Adherence in 236 Patients with Eosinophilic Oesophagitis-Results from the Population-Based DanEoE Cohort Shows a Low Complication Rate. United European Gastroenterol J 2021, 9, 910–918. [CrossRef]
- Navarro, P.; Laserna-Mendieta, E.J.; Guagnozzi, D.; Casabona, S.; Perelló, A.; Savarino, E.; de la Riva, S.; Olalla, J.M.; Ghisa, M.; Serrano-Moya, N.; et al. Proton Pump Inhibitor Therapy Reverses Endoscopic Features of Fibrosis in Eosinophilic Esophagitis. Dig Liver Dis 2021, 53, 1479–1485. [CrossRef]
- Gutiérrez-Junquera, C.; Fernández-Fernández, S.; Cilleruelo, M.L.; Rayo, A.; Echeverría, L.; Quevedo, S.; Bracamonte, T.; Román, E. High Prevalence of Response to Proton-Pump Inhibitor Treatment in Children With Esophageal Eosinophilia. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 704–710. [CrossRef]
- Gutiérrez-Junquera, C.; Fernández-Fernández, S.; Domínguez-Ortega, G.; Vila Miravet, V.; García-Puig, R.; La Orden-Izquierdo, E.; Peña Quintana, L.; Barrio Torres, J.; Medina Benítez, E.; Leis, R.; et al. Proton Pump Inhibitor Therapy in Pediatric Eosinophilic Esophagitis: Predictive Factors and Long-Term Step-Down Efficacy. J Pediatr Gastroenterol Nutr 2023, 76, 191–198. [CrossRef]
- Molina-Infante, J.; Rodriguez-Sanchez, J.; Martinek, J.; van Rhijn, B.D.; Krajciova, J.; Rivas, M.D.; Barrio, J.; Moawad, F.J.; Martinez-Alcalá, C.; Bredenoord, A.J.; et al. Long-Term Loss of Response in Proton Pump Inhibitor-Responsive Esophageal Eosinophilia Is Uncommon and Influenced by CYP2C19 Genotype and Rhinoconjunctivitis. Am J Gastroenterol 2015, 110, 1567–1575. [CrossRef]
- Gómez-Torrijos, E.; García-Rodríguez, R.; Castro-Jiménez, A.; Rodríguez-Sanchez, J.; Méndez Díaz, Y.; Molina-Infante, J.; Gomez-Torrijos, E.; Garcia-Rodriguez, R.; Castro-Jimenez, A.; Rodriguez-Sanchez, J.; et al. The Efficacy of Step-down Therapy in Adult Patients with Proton Pump Inhibitor-Responsive Oesophageal Eosinophilia. Alimentary Pharmacology & Therapeutics 2016, 43, 534–540. [CrossRef]
- Gutiérrez-Junquera, C.; Fernández-Fernández, S.; Cilleruelo, M.L.; Rayo, A.; Echeverría, L.; Borrell, B.; Román, E. Long-Term Treatment With Proton Pump Inhibitors Is Effective in Children With Eosinophilic Esophagitis. Journal of Pediatric Gastroenterology & Nutrition 2018, 67, 210–216. [CrossRef]
- Lucendo, A.J.; Molina-Infante, J. Limitation of Symptoms as Predictors of Remission in Eosinophilic Esophagitis: The Need to Go Beyond Endoscopy and Histology. Gastroenterology 2016, 150, 547–549. [CrossRef]
- Grueso-Navarro, E.; Navarro, P.; Laserna-Mendieta, E.J.; Lucendo, A.J.; Arias-González, L. Blood-Based Biomarkers for Eosinophilic Esophagitis and Concomitant Atopic Diseases: A Look into the Potential of Extracellular Vesicles. Int J Mol Sci 2023, 24, 3669. [CrossRef]
- Arnim, U. von; Biedermann, L.; Aceves, S.S.; Bonis, P.A.; Collins, M.H.; Dellon, E.S.; Furuta, G.T.; Gonsalves, N.; Gupta, S.; Hirano, I.; et al. Monitoring Patients With Eosinophilic Esophagitis in Routine Clinical Practice - International Expert Recommendations. Clin Gastroenterol Hepatol 2023, 21, 2526–2533. [CrossRef]
- Laserna-Mendieta, E.J.; Casabona, S.; Savarino, E.; Perelló, A.; Pérez-Martínez, I.; Guagnozzi, D.; Barrio, J.; Guardiola, A.; Asensio, T.; de la Riva, S.; et al. Efficacy of Therapy for Eosinophilic Esophagitis in Real-World Practice. Clinical Gastroenterology and Hepatology 2020, 18, 2903-2911.e4. [CrossRef]
- Dranove, J.E.; Horn, D.S.; Davis, M.A.; Kernek, K.M.; Gupta, S.K. Predictors of Response to Proton Pump Inhibitor Therapy among Children with Significant Esophageal Eosinophilia. J Pediatr 2009, 154, 96–100. [CrossRef]
- Alexander, R.; Alexander, J.A.; Akambase, J.; Harmsen, W.S.; Geno, D.; Tholen, C.; Katzka, D.A.; Ravi, K. Proton Pump Inhibitor Therapy in Eosinophilic Esophagitis: Predictors of Nonresponse. Dig Dis Sci 2021, 66, 3096–3104. [CrossRef]
- Goldin, A.H.; Muftah, M.; Mangla, S.; Hornick, J.L.; Hsu Blatman, K.; Hamilton, M.J.; Lo, W.-K.; Chan, W.W. Assessment of the Clinical and Allergy Profiles of PPI Responsive and Non-Responsive Eosinophilic Esophagitis. Dis Esophagus 2023, 36, doac098. [CrossRef]
- Muftah, M.; Barshop, K.; Redd, W.D.; Goldin, A.H.; Lo, W.-K.; Chan, W.W. Baseline Peripheral Eosinophil Count Independently Predicts Proton Pump Inhibitor Response in Eosinophilic Esophagitis. J Clin Gastroenterol 2023. [CrossRef]
- Vieira, G.G.; Ribeiro, L.B.M.; Truppel, S.K.; Rosário Filho, N.A.; Vieira, M.C. Endoscopic and Histological Characteristics in Patients with Eosinophilic Esophagitis Responsive and Non-Responsive to Proton Pump Inhibitors. J Pediatr (Rio J) 2020, 96, 638–643. [CrossRef]
- Jevtić, J.; Ristić, N.; Pavlović, V.; Svorcan, J.; Milovanovich, I.; Radusinović, M.; Popovac, N.; Simić, L.; Ćirović, A.; Đuknić, M.; et al. The Usefulness of the Eosinophilic Esophagitis Histology Scoring System in Predicting Response to Proton Pump Inhibitor Monotherapy in Children with Eosinophilic Esophagitis. Diagnostics (Basel) 2023, 13, 3445. [CrossRef]
- Nagano, N.; Araki, A.; Ishikawa, N.; Nagase, M.; Adachi, K.; Ishimura, N.; Ishihara, S.; Kinoshita, Y.; Maruyama, R. Immunohistochemical Expression of Filaggrin Is Decreased in Proton Pump Inhibitor Non-Responders Compared with Proton Pump Inhibitor Responders of Eosinophilic Esophagitis. Esophagus 2021, 18, 362–371. [CrossRef]
- Irastorza, L.E.; Hopson, P.; Nabar, S.; Deb, C.; Smadi, Y. Eosinophil-Derived Neurotoxin Predicts Response to Proton-Pump Inhibitor Treatment in Pediatric Eosinophilic Esophagitis. J Pediatr Gastroenterol Nutr 2022, 74, 267–271. [CrossRef]
- Mougey, E.B.; Nguyen, V.; Gutiérrez-Junquera, C.; Fernández-Fernández, S.; Cilleruelo, M.L.; Rayo, A.; Borrell, B.; Román, E.; González-Lois, C.; Chao, M.; et al. STAT6 Variants Associate With Relapse of Eosinophilic Esophagitis in Patients Receiving Long-Term Proton Pump Inhibitor Therapy. Clin Gastroenterol Hepatol 2021, 19, 2046-2053.e2. [CrossRef]
- Shoda, T.; Matsuda, A.; Nomura, I.; Okada, N.; Orihara, K.; Mikami, H.; Ishimura, N.; Ishihara, S.; Matsumoto, K.; Kinoshita, Y. Eosinophilic Esophagitis versus Proton Pump Inhibitor-Responsive Esophageal Eosinophilia: Transcriptome Analysis. J Allergy Clin Immunol 2017, 139, 2010-2013.e4. [CrossRef]
- Hamilton, M.J.; Muftah, M.; Goldin, A.H.; Lo, W.-K.; Hsu Blatman, K.S.; Chan, W.W.; Srivastava, A. Overlapping Transcriptional Profile in Proton Pump Inhibitor Responsive and Nonresponsive Eosinophilic Esophagitis. Clin Transl Gastroenterol 2022, 13, e00540. [CrossRef]
- Molina-Jiménez, F.; Ugalde-Triviño, L.; Arias-González, L.; Relaño-Rupérez, C.; Casabona, S.; Moreno-Monteagudo, J.A.; Pérez-Fernández, M.T.; Martín-Domínguez, V.; Fernández-Pacheco, J.; Laserna-Mendieta, E.J.; et al. Proton Pump Inhibitor Effect on Esophageal Protein Signature of Eosinophilic Esophagitis, Prediction and Evaluation of Treatment Response 2023, 2023.11.21.23298292. [CrossRef]
- Shoda, T.; Wen, T.; Aceves, S.S.; Abonia, P.J.; Atkins, D.; Bonis, P.A.; Caldwell, J.M.; Capocelli, K.E.; Carpenter, C.L.; Collins, M.H.; et al. Eosinophilic Esophagitis Endotype Classification by Molecular, Clinical, and Histopathological Analyses: A Cross Sectional Study by the Consortium of Eosinophilic Gastrointestinal Disease Researchers (CEGIR). Lancet Gastroenterol Hepatol 2018, 3, 477–488. [CrossRef]
- Cañas, J.A.; Tabares, A.; Barbero, C.; García-Sánchez, D.; Sastre, B.; Rodrigo-Muñoz, J.M.; Mahíllo-Fernández, I.; Rayo, A.; Borrell, B.; Cilleruelo, M.L.; et al. Proton-Pump Inhibitor Response Prediction Using Esophageal microRNAs in Children With Eosinophilic Esophagitis. J Pediatr Gastroenterol Nutr 2020, 71, 755–763. [CrossRef]
- Scott, S.A.; Sangkuhl, K.; Shuldiner, A.R.; Hulot, J.-S.; Thorn, C.F.; Altman, R.B.; Klein, T.E. PharmGKB Summary: Very Important Pharmacogene Information for Cytochrome P450, Family 2, Subfamily C, Polypeptide 19. Pharmacogenet Genomics 2012, 22, 159–165. [CrossRef]
- El Rouby, N.; Lima, J.J.; Johnson, J.A. Proton Pump Inhibitors: From CYP2C19 Pharmacogenetics to Precision Medicine. Expert Opin Drug Metab Toxicol 2018, 14, 447–460. [CrossRef]
- Botton, M.R.; Whirl-Carrillo, M.; Del Tredici, A.L.; Sangkuhl, K.; Cavallari, L.H.; Agúndez, J.A.G.; Duconge, J.; Lee, M.T.M.; Woodahl, E.L.; Claudio-Campos, K.; et al. PharmVar GeneFocus: CYP2C19. Clin Pharmacol Ther 2021, 109, 352–366. [CrossRef]
- Gene-Specific Information Tables for CYP2C19. Available online: https://www.pharmgkb.org/page/cyp2c19RefMaterials (accessed on 26 January 2024).
- Ionova, Y.; Ashenhurst, J.; Zhan, J.; Nhan, H.; Kosinski, C.; Tamraz, B.; Chubb, A. CYP2C19 Allele Frequencies in Over 2.2 Million Direct-to-Consumer Genetics Research Participants and the Potential Implication for Prescriptions in a Large Health System. Clin Transl Sci 2020, 13, 1298–1306. [CrossRef]
- Sibbing, D.; Gebhard, D.; Koch, W.; Braun, S.; Stegherr, J.; Morath, T.; Von Beckerath, N.; Mehilli, J.; Schömig, A.; Schuster, T.; et al. Isolated and Interactive Impact of Common CYP2C19 Genetic Variants on the Antiplatelet Effect of Chronic Clopidogrel Therapy. J Thromb Haemost 2010, 8, 1685–1693. [CrossRef]
- Eken, E.; Estores, D.S.; Cicali, E.J.; Wiisanen, K.K.; Johnson, J.A. A Pharmacogenetics-Based Approach to Managing Gastroesophageal Reflux Disease: Current Perspectives and Future Steps. Pharmgenomics Pers Med 2023, 16, 645–664. [CrossRef]
- Andersson, T.; Holmberg, J.; Röhss, K.; Walan, A. Pharmacokinetics and Effect on Caffeine Metabolism of the Proton Pump Inhibitors, Omeprazole, Lansoprazole, and Pantoprazole. Br J Clin Pharmacol 1998, 45, 369–375. [CrossRef]
- Andersson, T.; Hassan-Alin, M.; Hasselgren, G.; Röhss, K.; Weidolf, L. Pharmacokinetic Studies with Esomeprazole, the (S)-Isomer of Omeprazole. Clin Pharmacokinet 2001, 40, 411–426. [CrossRef]
- Lim, P.W.Y.; Goh, K.L.; Wong, B.C.Y. CYP2C19 Genotype and the PPIs--Focus on Rabeprazole. J Gastroenterol Hepatol 2005, 20 Suppl, S22-28. [CrossRef]
- Harris, D.M.; Stancampiano, F.F.; Burton, M.C.; Moyer, A.M.; Schuh, M.J.; Valery, J.R.; Bi, Y. Use of Pharmacogenomics to Guide Proton Pump Inhibitor Therapy in Clinical Practice. Dig Dis Sci 2021, 66, 4120–4127. [CrossRef]
- Sim, S.C.; Risinger, C.; Dahl, M.-L.; Aklillu, E.; Christensen, M.; Bertilsson, L.; Ingelman-Sundberg, M. A Common Novel CYP2C19 Gene Variant Causes Ultrarapid Drug Metabolism Relevant for the Drug Response to Proton Pump Inhibitors and Antidepressants. Clin Pharmacol Ther 2006, 79, 103–113. [CrossRef]
- Ichikawa, H.; Sugimoto, M.; Sugimoto, K.; Andoh, A.; Furuta, T. Rapid Metabolizer Genotype of CYP2C19 Is a Risk Factor of Being Refractory to Proton Pump Inhibitor Therapy for Reflux Esophagitis. J Gastroenterol Hepatol 2016, 31, 716–726. [CrossRef]
- Zhao, X.; Zhang, Z.; Lu, F.; Xiong, M.; Jiang, L.; Tang, K.; Fu, M.; Wu, Y.; He, B. Effects of CYP2C19 Genetic Polymorphisms on the Cure Rates of H. Pylori in Patients Treated with the Proton Pump Inhibitors: An Updated Meta-Analysis. Front Pharmacol 2022, 13, 938419. [CrossRef]
- Dutch Pharmacogenetics Working Group Recommendations Royal Dutch Pharmacists Association (KNMP). Dutch Pharmacogenetics Working Group (DPWG). Pharmacogenetic Guidelines.
- Bråten, L.S.; Haslemo, T.; Jukic, M.M.; Ivanov, M.; Ingelman-Sundberg, M.; Molden, E.; Kringen, M.K. A Novel CYP2C-Haplotype Associated With Ultrarapid Metabolism of Escitalopram. Clinical Pharmacology & Therapeutics 2021, 110, 786–793. [CrossRef]
- Kee, P.S.; Maggo, S.D.S.; Kennedy, M.A.; Barclay, M.L.; Miller, A.L.; Lehnert, K.; Curtis, M.A.; Faull, R.L.M.; Parker, R.; Chin, P.K.L. Omeprazole Treatment Failure in Gastroesophageal Reflux Disease and Genetic Variation at the CYP2C Locus. Frontiers in Genetics 2022, 13. [CrossRef]
- Daly, A.K. Significance of the Minor Cytochrome P450 3A Isoforms. Clin Pharmacokinet 2006, 45, 13–31. [CrossRef]
- Zhou, Y.; Ingelman-Sundberg, M.; Lauschke, V.M. Worldwide Distribution of Cytochrome P450 Alleles: A Meta-Analysis of Population-Scale Sequencing Projects. Clin Pharmacol Ther 2017, 102, 688–700. [CrossRef]
- Wang, D.; Guo, Y.; Wrighton, S.A.; Cooke, G.E.; Sadee, W. Intronic Polymorphism in CYP3A4 Affects Hepatic Expression and Response to Statin Drugs. Pharmacogenomics J 2011, 11, 274–286. [CrossRef]
- Kuehl, P.; Zhang, J.; Lin, Y.; Lamba, J.; Assem, M.; Schuetz, J.; Watkins, P.B.; Daly, A.; Wrighton, S.A.; Hall, S.D.; et al. Sequence Diversity in CYP3A Promoters and Characterization of the Genetic Basis of Polymorphic CYP3A5 Expression. Nat Genet 2001, 27, 383–391. [CrossRef]
- Li, Y.; Zhang, W.; Guo, D.; Zhou, G.; Zhou, H.; Xiao, Z. Pharmacokinetics of the New Proton Pump Inhibitor Ilaprazole in Chinese Healthy Subjects in Relation to CYP3A5 and CYP2C19 Genotypes. Clin Chim Acta 2008, 391, 60–67. [CrossRef]
- Desta, Z.; Zhao, X.; Shin, J.-G.; Flockhart, D.A. Clinical Significance of the Cytochrome P450 2C19 Genetic Polymorphism. Clin Pharmacokinet 2002, 41, 913–958. [CrossRef]
- Denisenko, N.P.; Sychev, D.A.; Sizova, Z.M.; Smirnov, V.V.; Ryzhikova, K.A.; Sozaeva, Z.A.; Grishina, E.A. CYP3A and CYP2C19 Activity in Urine in Relation to CYP3A4, CYP3A5, and CYP2C19 Polymorphisms in Russian Peptic Ulcer Patients Taking Omeprazole. Pharmgenomics Pers Med 2018, 11, 107–112. [CrossRef]
- Wedemeyer, R.-S.; Blume, H. Pharmacokinetic Drug Interaction Profiles of Proton Pump Inhibitors: An Update. Drug Saf 2014, 37, 201–211. [CrossRef]
- Brambila-Tapia, A. MDR1 (ABCB1) Polymorphisms: Functional Effects and Clinical Implications. Rev Invest Clin 2013, 65, 445–454.
- Kodaira, C.; Sugimoto, M.; Nishino, M.; Yamade, M.; Shirai, N.; Uchida, S.; Ikuma, M.; Yamada, S.; Watanabe, H.; Hishida, A.; et al. Effect of MDR1 C3435T Polymorphism on Lansoprazole in Healthy Japanese Subjects. Eur J Clin Pharmacol 2009, 65, 593–600. [CrossRef]
- Li, C.-Y.; Zhang, J.; Chu, J.-H.; Xu, M.-J.; Ju, W.-Z.; Liu, F.; Zou, J.-D. A Correlative Study of Polymorphisms of CYP2C19 and MDR1 C3435T with the Pharmacokinetic Profiles of Lansoprazole and Its Main Metabolites Following Single Oral Administration in Healthy Adult Chinese Subjects. Eur J Drug Metab Pharmacokinet 2014, 39, 121–128. [CrossRef]
- Abe, K.; Tani, K.; Fujiyoshi, Y. Conformational Rearrangement of Gastric H+,K+-ATPase Induced by an Acid Suppressant. Nat Commun 2011, 2, 155. [CrossRef]
- Sun, L.-N.; Cao, Y.; Li, Y.-Q.; Fang, Y.-Q.; Zhang, H.-W.; Wang, M.-F.; Xie, L.-J.; Chen, J.; Yang, Z.-C.; Bian, M.-L.; et al. Impact of Gastric H+/K+-ATPase Rs2733743 on the Intragastric pH-Values of Dexlansoprazole Injection in Chinese Subjects. Frontiers in Pharmacology 2017, 8. [CrossRef]
- Karpathiou, G.; Papoudou-Bai, A.; Ferrand, E.; Dumollard, J.M.; Peoc’h, M. STAT6: A Review of a Signaling Pathway Implicated in Various Diseases with a Special Emphasis in Its Usefulness in Pathology. Pathology - Research and Practice 2021, 223, 153477. [CrossRef]
- Zhang, X.; Cheng, E.; Huo, X.; Yu, C.; Zhang, Q.; Pham, T.H.; Wang, D.H.; Spechler, S.J.; Souza, R.F. Omeprazole Blocks STAT6 Binding to the Eotaxin-3 Promoter in Eosinophilic Esophagitis Cells. PLoS One 2012, 7, e50037. [CrossRef]
- Cheng, E.; Zhang, X.; Huo, X.; Yu, C.; Zhang, Q.; Wang, D.H.; Spechler, S.J.; Souza, R.F. Omeprazole Blocks Eotaxin-3 Expression by Oesophageal Squamous Cells from Patients with Eosinophilic Oesophagitis and GORD. Gut 2013, 62, 824–832. [CrossRef]
- Mougey, E.B.; Williams, A.; Coyne, A.J.K.; Gutiérrez-Junquera, C.; Fernández-Fernández, S.; Cilleruelo, M.L.; Rayo, A.; Echeverría, L.; Román, E.; González Lois, C.; et al. CYP2C19 and STAT6 Variants Influence the Outcome of Proton Pump Inhibitor Therapy in Pediatric Eosinophilic Esophagitis. J Pediatr Gastroenterol Nutr 2019, 69, 581–587. [CrossRef]
- Bortolin, K.A.; Cohn, I.; Da Silva, S.; Ito, S.; Marcon, P.; Afzal, N.; Scodellaro, S.; Verstegen, R.; Hulst, J. A129 CYP2C19 Pharmacogenetic testing in paediatric patients with eosinophilic esophagitis influences dosing of proton-pump-inhibitors and response to therapy. J Can Assoc Gastroenterol 2022, 5, 152–153. [CrossRef]
Figure 1.
Clinical and molecular factors, omics features and genetic variations associated by previous research with usefulness to predict response to proton-pump inhibitors (PPI) in patients with eosinophilic esophagitis. a: only to predict response after PPI dose reduction for maintenance; b: this genetic variation had a synergistic effect with CYP2C19*17 allele. EoE-HSS: eosinophilic esophagitis histology scoring system; HPF: high power field.
Figure 1.
Clinical and molecular factors, omics features and genetic variations associated by previous research with usefulness to predict response to proton-pump inhibitors (PPI) in patients with eosinophilic esophagitis. a: only to predict response after PPI dose reduction for maintenance; b: this genetic variation had a synergistic effect with CYP2C19*17 allele. EoE-HSS: eosinophilic esophagitis histology scoring system; HPF: high power field.
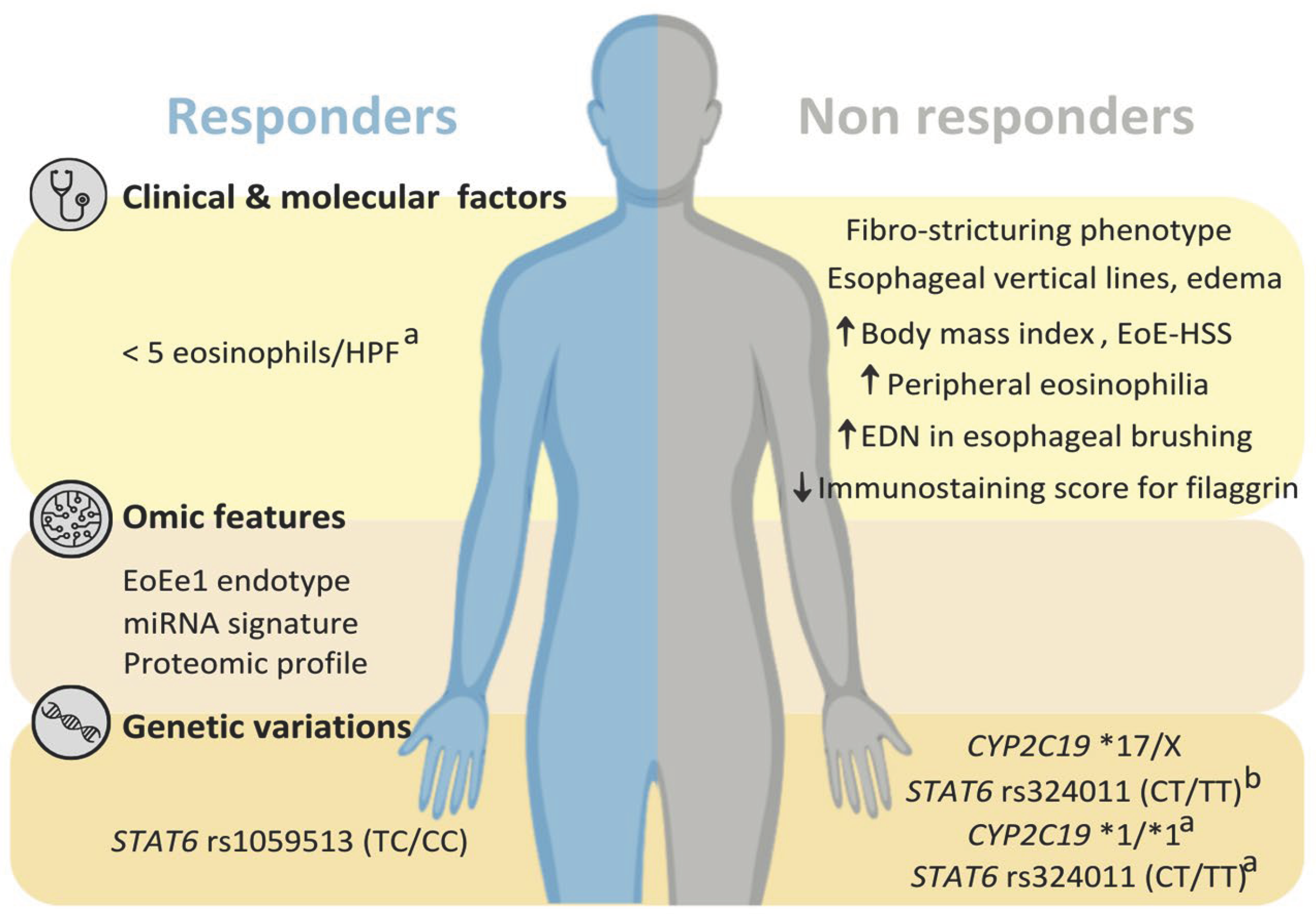

Table 1.
Main genetic variants of CYP2C19 gene that affect the response to proton-pump inhibitors (PPI).
Table 1.
Main genetic variants of CYP2C19 gene that affect the response to proton-pump inhibitors (PPI).
| Genotype | SNP | Nucleotide Change | Amino Acid Change | Functionality |
|---|---|---|---|---|
| CYP2C19*2a | rs4244285 | g.24179G>A c.681G>A |
Splicing defect | Non-functional protein |
| rs12769205 | g.17687A>G c.332-23A>G |
|||
| CYP2C19*3 | rs4986893 | g.22973G>A c.636G>A |
Trp212Ter (stop gained) | Non-functional protein |
| CYP2C19*4 | rs28399504 | g.5026A>G c.1A>G |
Met1Val (initiation codon variant) | Non-functional protein |
| CYP2C19*17 | rs12248560 | g.4220C>T c.-806C>T |
None (upstream variant) | Increased expression of the protein |
a CYP2C19*2 is represented in the table with 2 different SNPs as all CYP2C19*2 suballeles share those two SNPs. SNP: single nucleotide polymorphism.
Table 2.
CYP2C19 phenotypes according to the functionality of alleles.
| Phenotype | Genotype | Dyplotype example |
|---|---|---|
| Poor metabolizers (PM) | 2 non-function alleles | CYP2C19*2/*2 |
| “Likely” poor metabolizers (Likely PM)a | 1 non-function + 1 decreased function alleles | CYP2C19*2/*9 |
| Intermediate metabolizers (IM) | 1 normal function + 1 non-function alleles | CYP2C19*1/*2 |
| 1 non-function + 1 increased function alleles | CYP2C19*2/*17 | |
| “Likely” intermediate metabolizers (Likely IM)a | 1 normal function + 1 decreased function alleles | CYP2C19*1/*9 |
| 1 decreased function + 1 increased function alleles | CYP2C19*9/*17 | |
| 2 decreased function alleles | CYP2C19*9/*9 | |
| Normal metabolizers (NM) | 2 normal function alleles | CYP2C19*1/*1 |
| Rapid metabolizers (RM) | 1 normal function + 1 increased function alleles | CYP2C19*1/*17 |
| Ultrarapid metabolizers (UM) | 2 increased function alleles | CYP2C19*17/*17 |
| Indetermined metabolizers | 1 or 2 uncertain function alleles | CYP2C19*12/*14 |
a There are limited data to conclusively characterize decreased function alleles.
Table 3.
Summary of other genetic variations different from CYP2C19 that have been associated with response to proton-pump inhibitors (PPI).
Table 3.
Summary of other genetic variations different from CYP2C19 that have been associated with response to proton-pump inhibitors (PPI).
| Gene | SNP | Disease | Type of PPI | Functionality | Commentary |
|---|---|---|---|---|---|
| CYP2C18 | rs2860840 rs11188059 |
GERD | Omeprazole | Increased (ultrarapid phenotype) | Haplotype CYP2C:TG |
| CYP3A5 | rs776746 | Healthy volunteers | Ilaprazole | Lack of activity (but increased drug clearance) | CYP3A5*3 |
| ABCB1 | rs1045642 | Healthy volunteers | Lansoprazole | Decreased (lower clearance) | Lower effect than CYP2C19 genotypes |
| ATP4A | rs2733743 | Healthy volunteers | Dexlansoprazole | Increased (higher inhibition of acid gastric secretion) | Higher effect than CYP2C19 genotypes |
| STAT6 | rs167769 rs324011 rs12368672 |
Eosinophilic esophagitis | Esomeprazole (mainly) | Increased (higher odds of no response to PPIs during maintenance) | These 3 SNPs are in linkage disequilibrium; synergistic effect with CYP2C19*17 in induction |
| rs1059513 | Decreased (higher odds of response to PPIs in induction) | Independent from CYP2C19 genotypes |
GERD: gastroesophageal reflux disease; SNP: single nucleotide polymorphism.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



