
Submitted:
26 February 2024
Posted:
27 February 2024
You are already at the latest version
Abstract
Background: The practice of self-medication is common worldwide and is an important component of medical self-care. However, the practice can be dangerous and is linked to various risks for the patients and the entire community. This study aimed to estimate the prevalence and factors associated with self-medication among Bangladeshi adults. Methods: A cross-sectional survey was conducted between April and June 2021 among Bangladeshi adults (aged >19 years) using convenient sampling. A total of 1320 data were collected through face-to-face interviews using a standardized questionnaire. Multivariable logistic regression analysis was used to identify factors associated with self-medication practice (SMP). Results: Overall, 41% of adults in our survey reported SMP. The most common illnesses that prompted SMP were common cold/flu (66.4%), gastric problems (65%), and headache (64.4%). The most frequent reasons for SMP were to get better services (30.59%), perceive SMP without side effects (23.28%), and save time with effectiveness (14.56%). Potential risk factors included 10 years (AOR = 1.91; 95% CI: 1.04 - 3.50) and >12 years of schooling (AOR = 5.03; 95% CI: 2.27 - 11.15), being a businessman (AOR = 4.64; 95% CI: 1.74 - 12.37), having ≤6 family members (AOR = 2.13; 95% CI: 1.40 - 3.24), being a member of a social group (AOR = 1.53; 95% CI: 1.10 - 2.12), a health status check after every six months (AOR = 1.52; 95% CI: 1.08 - 2.13), and current ill-health (AOR = 1.41; 95% CI: 1.06 - 1.87). Protective factors identified included ≤30 years of age (AOR = 0.40; 95% CI: 0.17 - 0.93), and practice of modern (AOR = 0.39; 95% CI: 0.22- 0.69) and herbal (AOR = 0.45; 95% CI: 0.21- 0.97) healing types. Conclusion: More than one-third of the study participants reported practicing self-medication. Increasing the community’s awareness of the extreme consequences of SMP and not just the average experience might sway individuals away from SMP, and implementing strict jurisdiction could be a way to minimize the SMP.
Keywords:
Self-medication
; Prevalence
; Risk factors
; Bangladesh
1. Introduction
The World Health Organization (WHO) defines self-medication as when a person takes medications based on their self-diagnosis of an illness without going to a doctor or doing any clinical tests to support their beliefs [1]. Self-medication encompasses not only taking medications for acute symptoms but also repeatedly administering medications for chronic illnesses [2]. Self-medication practice (SMP), selecting and ingesting medications without consulting a physician for disease prevention, diagnosis, or treatment, is a worldwide phenomenon [3]. In 2013, it was estimated that 246 million people, or one in every 20 people aged 15-64 years worldwide, had self-medicated [4]. Insufficient drug regulation, the easy availability of over-the-counter medications, and unequal distribution of healthcare have been shown to contribute to the prevalence of this practice [5], while additional factors, such as direct marketing of drugs to the public, are also suspected.
SMP is common across nations independent of developmental or economic rank. For example, in the West, 70.1% of Americans [6], 16.1% of Brazilians [7], and 69.2% of Italians [8] self-medicate. Meanwhile, in Asia, 32.5% of Indians [9], 84.8% of Pakistanis [10], and 38.2% of Nepalis [11] self-medicate. In Bangladesh, a recent study found that among the higher-educated population in metropolitan areas (16–81%), SMP is common [12]. Another study carried out in Bangladesh’s Comilla area found that 73.6% of adults regularly self-medicated, and they did so specifically for mild illnesses due to their familiarity with the medications [13]. According to research among Savar residents in Bangladesh, pharmacy outlets, prior experience or prescriptions, and peer (friend or relative) consultation were the most common influences on SMP, with a reported incidence of 60.2% [14]. In a cross-sectional study on Bangladeshi people’s knowledge, attitudes, and awareness of self-medication, 80% of respondents admitted to buying or using medications without a prescription. Socioeconomic and lifestyle factors were the leading influences on this behavior [15].
The self-reported reasons for choosing SMP are varied and include insufficient time to consult with medical personnel, inability to schedule a quick appointment, long distances and travel times to reach the nearest hospitals and clinics, limited openings for immediate treatment from a hospital during busy hours, lack of healthcare services, and unaffordable consulting fees for medical doctors [16]. Studies conducted in Europe [17], South West Ethiopia [18], and Bangladesh [19] show that individuals choose self-medication for common ailments like fever, cold, acidity, abdominal pain, cough, headache, back pain, typhoid, typhus, cough, community-acquired pneumonia, diarrhea, amebiasis, tonsillitis, wounds, allergies, and diarrhea.
Healthcare systems have become increasingly expensive, and developing nations typically have limited healthcare facilities, making SMP an obvious choice for health care services at that time. The individual benefits of SMP are cost savings, especially considering that medical consultations will be reduced or eliminated [20], convenience, and the agency provided by participation in one’s own health care. At the community level, the benefits include avoiding the waste of scarce medical resources for minor conditions, reducing the costs of programs funded by the community for healthcare, reducing the burden on medical services in areas with inadequate healthcare personnel, and increasing the availability of affordable healthcare for rural and remote populations [20]. Thus, there are many situations where SMP is a reasonably safe alternative to professionally managed care.
However, despite the evident advantages, SMP can have detrimental consequences to both individual and community health [21]. SMP may result in health hazards such as adverse drug reactions [21], inaccurate or delayed diagnosis, and extended suffering associated with the disease [22]. As in other countries, Bangladesh has experienced high levels of bacterial resistance to widely and overused antimicrobials resulting from SMP [23]. This means that higher rates of resistant bacterial infections continue because antibiotics are not administered appropriately in the context of self-administration practices [24,25]. Antimicrobial resistance is thought to be at the heart of up to 80% of infections-related fatalities, prompting a recent petition to the Bangladesh High Court seeking a ruling barring the sale of drugs without moral justification [26].
Improving individual and community health care requires an understanding of the common practices, reasons for, and factors that impact SMP. Adult behavior has a significant impact on household and community health choices. Understanding the reasons for self-medication can help shape policies that encourage safe self-care habits, leading to better public health for adults. Unfortunately, minimal information is available on the prevalence of practicing self-medication among adults and its associated factors in Bangladesh. Therefore, the study aimed to explore (i) the prevalence of SMP among Bangladeshi adults and (ii) the associated factors leading to SMP.
2. Methods
2.1. Study Design and Period
A cross-sectional study was carried out to investigate the prevalence, indications, disease conditions, presence or absence of adverse effects, and perceived reasons for SMP among adults in Bangladesh. This study only included those who voluntarily took part in the survey. The data collection was carried out from April to June 2021. This study was conducted according to the International Conference of Harmonization (ICH) guidelines for good clinical practice [27].
2.2. Study Area
The study was carried out in two administrative Kurigram and Comilla districts found in the Northern and Eastern regions of Bangladesh, respectively. The districts are located at 337 km and 100 km from Dhaka, the capital of Bangladesh, respectively. The districts were chosen based on the accessibility and availability of the participants.
2.3. Study Tools and Data Collection
An interviewer-administered questionnaire was used to collect data from the participants. The draft version of the questionnaire was pre-tested on 50 adults from the Kurigram district to eliminate confusing and unclear items that were not included in the final analysis. For example, we removed independent variables such as decision-maker, access to healthcare services, and past medical history. The questionnaire was structured and adopted from recent existing literature [28]. To evaluate research theme, the questionnaire was divided into three domains, including sociodemographic and clinical information, indications and reasons for SMP, and disease conditions and presence or absence of adverse effects of SMP. The data were collected by trained interviewers after receiving consent from the participants. Any questions and doubts of the interviewers were communicated quickly face-to-face by the principal investigator. The interview took approximately 20-25 minutes for each participant.
2.4. Sampling and Sample Size
Participants who met inclusion criteria (Bangladeshi by birth, lived at least six months in the selected districts, and aged >19 years) were recruited via home visits. We excluded individuals who were critically ill, incapable of hearing and speaking during the survey, and absent in the home during data collection. The sample size was determined by the single proportion formula (n = Z2× P (1-P)/d2) using the following assumptions: 95% confidence level (1.96), 5% margin of error, and 73.6% SMP extent in Bangladesh [13]. Based on the equation, the final required sample size was 300. However, we included 1,320 participants to reach a more accurate conclusion in our research. We used a convenient sampling method to select the participants.
2.5. Outcomes and Covariates
The dependent variable, self-medication, was evaluated as a dichotomous variable three months prior to the survey, with responses denoting “self-medication” or “no self-medication.” To address the recall bias that is frequently observed in retrospective studies, this methodology was implemented [29]. Self-medication refers to the independent selection and application of over-the-counter medications by individuals to treat themselves or perceive themselves as having disorders or symptoms [28,30]. The covariates are socio-demographic factors such as gender, age (Age were classified as ≤30, 31-60, and >60 years), year of schooling, marital status, occupation, household income, residence, number of family members, and religion. The major health-related factors were coverage of health insurance, health status checks after every six months, present illness, and mostly used healing types. In addition, data about current smoking was assessed by asking the question “Do you currently smoke any tobacco products, such as cigarettes?”. Knowledge of drug use, member of a social group, and current treatment status were also used. To facilitate the interpretation of the results, drug use knowledge was reclassified as a dichotomous variable: inadequate knowledge of drugs (a combination of “none” and “insufficient”), and adequate (a combination of “sufficient” and “excellent”).
2.6. Statistical Analysis
Before analyzing the dataset, data cleaning and management were performed. The survey data were analyzed using IBM SPSS version 28.0. Simple descriptive analyses were used to determine the frequencies, percentages, and mean ±SD to explain different variables. Then, Chi-square and Fisher’s exact tests were conducted to identify the significant differences among variables. Multicollinearity was checked by a correlation coefficient, and a cut-off value of 0.80 was used to select independent variables. Next, both the bi-variable and multi-variable logistic regression analyses were performed to examine the factors associated with SMP by our selected independent variables. The logistic regression was validated by the Hosmer-Lemeshow test (χ2 =10.17, 10df, p = 0.252). The adjusted odds ratio (AOR) at 95% confidence intervals was used to measure association (p-value <0.05. A forest plot was used for the graphical display of the significant findings.
3. Results
The socio-demographic profiles of the respondents are presented in Table 1. A total of 1,320 respondents were included in this study, with a response rate of 78.6%. About 50.9% of participants were male, 69.3% were ≤30 years old, and 87.8% were from rural areas. Most participants (71.1%) had incomes of <15,000 BDT a month; however, only 6% were covered by health insurance.
Despite having inadequate knowledge of the drugs involved, just less than half of respondents chose SMP. A large number (98.3%) of respondents reported not having adequate knowledge of the drug used. During the study, less than half (35.8%) of the respondents were under treatment by a doctor. The extent of self-medication was 51.2% among male respondents and 31% among female respondents. The overall prevalence of SMP was 41.28%. Among the study participants, the highest SMP was observed in businessmen (74%), 72.8% in those who had > 12 years of schooling, followed by 63.6% in the respondents who had household income >30000-50000 BDT.
The SMP of respondents were significantly associated with a host of socio-demographic factors including gender (χ2=55.38, p = 0.001), age (χ2=16.22, p = 0.001), years of schooling (χ2=43.31, p = 0.001), occupation (χ2=107.41, p = 0.001), household income (χ2=20.57, p = 0.001), residence (χ2=12.30, p = 0.001), religion (χ2=5.07, p = 0.024), family member (χ2=24.83, p = 0.001) and with clinical factors like smoking status (χ2=29.35, p = 0.001), health insurance (χ2=14.91, p = 0.001), member of a social group (χ2=34.65, p = 0.001), regular check-ups (after every 6 months) (χ2=24.14, p = 0.001), present illness (χ2=19.33, p = 0.001), knowledge of drug used (χ2=5.53, p =0.019) under treatment (χ2=19.33, p = 0.001) and healing types (χ2=37.24, p = 0.001) (Table 1).
The medical reasons for seeking treatment are largely common ailments. The most frequently found illnesses treated by SMP were common cold/flu, cough (66.4%), gastric problems (65%), followed by headache (62.4%), anxiety/depression (60.7%), and insomnia (50%). The lowest levels of SMP were associated with eye infections (19.4%) and ear problems (19.3%), abnormal blood pressure (22.8%), and skin problems (22.6%) (Figure 1).
We found that quality issues topped the reasons for choosing SMP, with “improved services” being the most common reason for choosing SMP and “with less adverse side effects” being the second (30.59% and 23.28%, respectively). Next, we found that immediacy issues were reported, and the responses “rapid effectiveness” (14.56%) and “quick relief” (10.34%) were common reasons for choosing SMP (Figure 2).
Among respondents, SMP was found to be highly successful. The self-reported healing rate (93%) (Figure 3) among those choosing SMP was significant and 61.8% of respondents did not find any adverse effects in practicing self-medication (Figure 4). Only 3.1% of respondents experienced side effects of SMP, and around one-third (35%) of the total respondents did not note the magnitude of side effects (Figure 4).
We performed univariable and multivariable logistic regression analysis and regressed socio-economic and clinical factors upon SMP (Table 2 and Figure 5). The factors significantly associated with SMP included age, years of schooling, occupation, family members, members of a social group, health status check, present illness, and healing types. In this study, the younger age group (≤30 years) had practiced approximately 60% less self-medication (AOR = 0.40; 95% CI: 0.17-0.93) compared to the older age group (>60 years). The respondents with > 12 years of schooling had more than 5 times higher chance of SM than those without schooling (AOR = 5.03; 95% CI: 2.27-11.15). Those who worked in private business had 4.64 times (AOR = 4.64; 95% CI: 1.74-12.37) higher SMP than those involved in government service.
Similarly, families having 3 to 4 family members or 5 to 6 family members had 2.52 times (AOR = 2.52; 95% CI: 1.65-3.84) and 2.13 times (AOR = 2.13; CI: 1.40-3.24) higher chance to practice self-medication, respectively. Among the respondents, those who were members of a social group were 1.53 times more likely to have SMP (AOR = 1.53; 95% CI: 1.10-2.12) behavior than those not engaged with a social group. Likewise, respondents who checked their health status (after every 6 months) had 1.52 times more likely to practice self-medication than those who didn’t check their health status (AOR = 1.52; 95% CI: 1.08-2.13), and who had present illness had 1.41 times self-medication (AOR = 1.41; 95% CI: 1.06-1.87). This study also found that those who use modern treatment and herbal treatments as healing types were approximately 62 % (AOR = 0.38; 95% CI: 0.22-0.68) and 55% (AOR: 0.45; 95% CI: 0.21-0.96) less likely to practice self-medication than quackery, respectively.
4. Discussion
According to the current study, the SMP among the Bangladeshi adult population is substantial at 41.28%. This discovery aligns with a previous study in Bangladesh, which reported a prevalence of 49.9% [31], and a study in Gondar town, Northwest Ethiopia, with a similar rate of 50.2% [32]. Our findings show a higher prevalence of SMP compared to studies carried out in the Meket district, Northeast Ethiopia (35.9%) [29], Eastern Ethiopia (15.8%), Brazil (16.1%) [7], India (32.5%) [9], and Nepal (38.2%) [11]. Contrary to that, the SMP in our study (41.28%) is lower compared to studies in Bangladesh (60.2%) [14], Malaysia (62.7%) [33], the United States (70.1%) [6], Italy (69.2%) [8], and Pakistan (84.8%) [10]. The variations in SMP prevalence underscore how SMP choices are impacted by demographic factors like cultural beliefs, social determinants of health, variation in recall periods used in every study, socioeconomic gaps, settings, and law enforcement. The current study offers valuable insights into the prevalence of self-medication in Bangladesh, giving a nuanced perspective compared to national and international studies.
Our research shows that the most common reasons for self-medication were the common cold/flu and cough, with gastric issues also playing a significant role. It is in line with the idea that people may turn to self-medication for illnesses with similar symptoms because of inadequate health-seeking habits among the participants in our study [34]. In addition, our findings closely resemble previous research, where fever, body aches, common cold, headache, and cough were identified as significant reasons for self-medication [35,36], including cough and cold remedies, pain relief drugs, diarrhea treatments, allergy medications, constipation remedies, weight loss products, and heartburn medications [33]. The difference in common diseases that result in self-medication could be due to the varying prevalence of disease in different countries, highlighting the impact of cultural, environmental, and healthcare system factors on SMP.
This study highlights the most frequent reasons for choosing SMP, including improving service quality, reducing side effects, and saving time while maintaining effectiveness. In Ethiopia, households cited reasons such as the severity of illnesses, emergency cases, reducing medical costs, lack of trust in prescribers, and saving time [32]. In India, the common reasons for self-medication include saving time and not considering the condition severe enough to require a doctor’s visit [35]. The current study found that a small percentage (3.1%) experienced adverse effects after SMP. This aligns with earlier studies, where 28.2% of the subjects experienced adverse effects from the medication [37]. The relatively lower incidence of reported adverse effects indicates that the study participants may be more aware or careful, emphasizing the importance of further investigating the factors that influence SMP in Bangladesh.
The current study revealed that the older age group is more prone to SMP than other age groups regarding associated factors. This finding is consistent with a similar survey conducted in Brazil [38], but contrasts with previous research conducted in Ethiopia, which found that the younger age group was more prone to SMP [34]. However, some other studies reported no association between age and SMP [28,39]. The possible reason for the higher prevalence of SMP among older adults is the elevated risk of various diseases at an older age. Also, comorbidity in this age group can contribute to increased practice of self-medication [40], which may need to be resolved with special attention.
In the present study, participants with higher educational attainment practice more self-medication. This finding agrees with the study conducted in India [41], and several studies also underlined the fact that education level is the dominant factor for the practice of self-medication [30] but differed from the Ethiopian sample [39]. Higher-educated individuals may be more inclined to self-medicate due to their knowledge base and ability to access information online. It is crucial to consider that the influence of education on self-medication behaviors may differ based on the cultural setting and healthcare system of the respondents’ countries [42]. This study provides valuable insights into how educational background can impact self-medication behaviors and highlights the importance of tailored interventions for promoting responsible self-care in Bangladesh.
Our findings indicate that SMP among businessmen was 4.64 times higher than that of the respondents who are government sector workers. This finding is strongly supported by the study in India [41]. A lack of flexible time for businessmen to consult with health professionals may be a possible reason for utilizing SMP. One reason businessmen may have a higher SMP is due to their limited time to consult with health professionals. It suggests that busy schedules or other constraints may lead businessmen to self-medicate instead of seeking consultation from healthcare professionals. In such situations, people might choose self-medication as a fast and convenient way to deal with their health issues.
Furthermore, the research also shows that the highest prevalence is among families with less than six members. It appears that smaller families are more inclined to resort to SMP than larger families. One possible reason for this finding is that larger families might have a heightened awareness of their health-related quality of life because of the various viewpoints and contributions from multiple family members [43]. On the other hand, smaller families may have fewer individuals contributing to understanding family health as a whole. This may lead to a limited understanding of health matters within the family, which could increase the tendency to self-medicate. Interestingly, a study conducted in Northeast Ethiopia did not find a notable connection between family size and SMP among family members [32]. This emphasizes the significance of taking into account regional and cultural differences in the connection between family size and SMP. Investigating this connection in various cultural settings and geographic areas could offer valuable insights into the factors that impact SMP within families.
According to the present study, the SMP is higher among people engaged with a social group and might be influenced by the behaviors and thoughts of other people within that group. However, this is not reported in the literature and needs further verification. Another interesting finding of our study is that SMP was higher among respondents who had regular check-ups (after every 6 months). Indeed, a regular medical check-up helps to keep track of individual health and assists in identifying various risk factors at an early stage that might influence SMP to treat and manage the symptoms early. However, an earlier study reported quite the opposite finding that routine medical check-ups are negatively associated with SMP [44]. This difference highlights the complex relationship between health-seeking behaviors, routine check-ups, and SMP. It highlights the significance of taking into account different factors like cultural differences, healthcare systems, and individual attitudes to comprehend the dynamics of self-medication in various contexts.
Quacks (persons unauthorized to practice medicine) of Bangladesh usually do not charge consultation fees; medicine selling profit is their primary source of income [45]. People from rural areas with lower income might prefer the treatment of quacks because of their poverty [45]. The current study revealed that persons who use quackery as a healing type practice more self-medication, suggesting that those persons might fall into the trap of quacks and find quackery as an alternative to medical services offered by more expensive allopathy, at least for cold and cough, fever, diarrhea, and dysentery. This could be due to a lack of access to or price of mainstream medical services, prompting consumers to seek alternative, perhaps less reliable, healthcare providers.
Our results would suggest that educated adults who are short on time and money resort to SMP. Primarily, they are afflicted with common medical issues, for which they have prior experience, and are comfortable applying treatments that they have heard of or even previously taken themselves. The correctness of this decision is reinforced by high rates of success and low rates of side effects.
It would seem difficult to find fault with decisions that seem quite logical, and while education often helps to discourage improper behavior, here it seems to encourage it. They are using sound reasoning and find the likelihood of negative outcomes of SMP to be low. However, they concluded that the small likelihood of a negative event means the risk of SMP is low. These well-meaning individuals are not properly considering the tragic consequences of missed or incorrect diagnosis, potential drug interactions, or effects of counterfeit drugs which, though, rare, may be catastrophic. Taking their medical treatment into their own hands puts them and their communities at risk for events of low frequency but extreme severity.
This study has several limitations, and we confronted some constraints. Firstly, this study used a cross-sectional design; therefore, it cannot prove causality. Secondly, we assessed only common illnesses like headache, common cold/flu, cough, anxiety/depression, etc., to determine SMP and exclude contagious diseases like COVID-19, Norovirus, sexually transmitted infections (STIs), etc., from our study. Thirdly, we did not collect data on drugs used and the duration of drugs used for a specific disease. Additionally, there was very limited research on this emerging topic to carry out any final conclusion. Moreover, we collected data from two selected districts of Bangladesh. Therefore, the prevalence of SMP in other districts might be different. Finally, this study had a limited age group of people as respondents, and we did not collect data for adolescents or children for SMP.
5. Conclusions
The main finding of this study was that nearly half of adults practiced self-medication in Bangladesh. Several factors were associated with SMP, for example, years of schooling, being a businessman, having larger family members, being a member of a social group, checking health status every six months, older adults, present illness, and using quackery as a healing type. Therefore, people should be educated on the potential risks of SMP. Moreover, the general public needs to be aware of the differentiation between certified medical practitioners and quacks. To mitigate the potential risk of SMP, healthcare policymakers should promote awareness programs on the rational use of medications and enforce laws to dispense prescription medication by registered physicians. Moreover, improving community awareness during public health emergencies may help people cope with their fears about the pandemic might make the practice a survival of the fittest choice and incorporate a lesson on how to handle different types of emergencies.
Author Contributions
Conceptualization, N.R.; methodology, N.R, MA, MMH, AS and SMI.; formal analysis, N.R.; data curation, N.R.; writing-original draft preparation, B.T.R, N.R, MNI, and AS.; writing-review and editing, N.R, MNI, MS, AS, SMI, MA, MMH, KKB and EH.; supervision, N.R. All authors have read and agreed to the published version of the manuscript.
Funding
The author (s) received no specific funding for this work.
Ethics Statement
This research protocol was evaluated and approved by the Research Ethical Committee (REC) of the Department of Biochemistry and Food Analysis, Patuakhali Science and Technology University, Bangladesh (Approval Number: BFA: 12/03/2021:03). Each of the surveyed individuals was aware of the purpose and further maneuver of the collected data, and written agreements justifying the consent are kept.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The data of the study are available upon request to the corresponding author.
Acknowledgments
The authors would like to thank all the participants for their cooperation in taking part in this study. We would like to acknowledge all individuals involved in the data collection process.
Conflicts of Interest
The authors have no conflicts of interest associated with the material presented in this paper.
References
- Organization WH. Guidelines for the regulatory assessment of medicinal products for use in self-medication. World Health Organization; 2000. p. WHO/EDM/QSM/00.1.
- Ruiz, M. Risks of Self-Medication Practices. Curr Drug Saf. 2010;5: 315–323. [CrossRef]
- Baracaldo-Santamaría, D.; Trujillo-Moreno, M.J.; Pérez-Acosta, A.M.; Feliciano-Alfonso, J.E.; Calderon-Ospina, C.A.; Soler, F. Definition of self-medication: a scoping review. Ther Adv Drug Saf 2022, 13, 20420986221127501. [Google Scholar] [CrossRef]
- UNODC (United Nations Office on Drugs and Crime). World Drug Report. Vienna. 2012. https://www.unodc.org/unodc/en/data-and-analysis/statistics/drug.
- Kumari, R.; Kiran, K.; Kumar, D.; Bahl, R.; Gupta, R. Study of knowledge and practices of self-medication among medical students at Jammu. Jms Skims 2012, 15(2), 141–144. [Google Scholar] [CrossRef]
- Behzadifar, M.; Behzadifar, M.; Aryankhesal, A.; Ravaghi, H.; Baradaran, H.R.; Sajadi, H.S.; et al. Prevalence of self-medication in university students: systematic review and meta-analysis. East Mediterr Health J 2020, 26(7), 846–857. [Google Scholar] [CrossRef]
- Arrais, P.S.; Fernandes, M.E.; Pizzol, T.D.; Ramos, L.R.; Mengue, S.S.; Luiza, V.L.; Tavares, N.U.; Farias, M.R.; Oliveira, M.A.; Bertoldi, A.D. Prevalence of self-medication in Brazil and associated factors. Rev Saude Publica 2016, 50, 13s. [Google Scholar] [CrossRef]
- Garofalo, L.; Di Giuseppe, G.; Angelillo, I.F. Self-medication practices among parents in Italy. Biomed Res Int 2015, 2015, 580650. [Google Scholar] [CrossRef]
- Shalini, A.; Logaraj, M. Prevalence and determinants of self-medication use among the adult population residing in suburban areas near Chennai, Tamil Nadu. J Family Med Prim Care 2021, 10, 1835–1838. [Google Scholar] [CrossRef]
- Afridi, M.I.; Rasool, G.; Tabassum, R.; Shaheen, M.; Siddiqullah; Shujauddin, M. Prevalence and pattern of self-medication in Karachi: A community survey. Pak J Med Sci 2015, 31, 1241–1245. [Google Scholar] [CrossRef]
- Paudel, S.; Aryal, B. Exploration of self-medication practice in Pokhara valley of Nepal. BMC Public Health 2020, 20, 714. [Google Scholar] [CrossRef]
- Seam, M.O.R.; Bhatta, R.; Saha, B.L.; Das, A.; Hossain, M.M.; Uddin, S.M.N.; Karmakar, P.; Choudhuri, M.S.K.; Sattar, M.M. Assessing the Perceptions and Practice of Self-Medication among Bangladeshi Undergraduate Pharmacy Students. Pharmacy (Basel) 2018, 6, 6. [Google Scholar] [CrossRef]
- Ira, I.J. Present condition of self-medication among the general population of Comilla district, Bangladesh. The Pharma Innovation 2015, 4, 87. [Google Scholar]
- Moonajilin, M.S.; Mamun, M.A.; Rahman, M.E.; Mahmud, M.F.; Al Mamun, A.H.M.S.; Rana, M.S.; Gozal, D. Prevalence and Drivers of Self-Medication Practices among Savar Residents in Bangladesh: A Cross-Sectional Study. Risk Manag Healthc Policy 2020, 13, 743–752. [Google Scholar] [CrossRef]
- Jami, M.A.; Biswas, K. A cross-sectional study regarding the knowledge, attitude, and awareness about self-medication among Bangladeshi people. Health Policy and Technology 2023, 100715. [Google Scholar] [CrossRef]
- Gualano, M. R.; Bert, F.; Passi, S.; Stillo, M.; Galis, V.; Manzoli, L.; Siliquini, R. Use of self-medication among adolescents: a systematic review and meta-analysis. Eur. J. Public Health 2015, 25, 444–450. [Google Scholar] [CrossRef]
- Grigoryan, L.; Haaijer-Ruskamp, F. M.; Burgerhof, J. G.; Mechtler, R.; Deschepper, R.; Tambic-Andrasevic, A.; ... Birkin, J. Self-medication with antimicrobial drugs in Europe. Emerg. Infect. Dis. 2006, 12, 452. [CrossRef]
- Demissie, F.; Ereso, K.; Paulos, G. Self-medication practice with antibiotics and its associated factors among the community of Bule-Hora Town, South West Ethiopia. Drug, Healthc. Patient Saf. 2022; 9–18. [Google Scholar] [CrossRef]
- Islam, M. S. Self-medications among higher educated population in Bangladesh: an email-based exploratory study. Internet J. Health 2007, 5, 20–25. [Google Scholar]
- World Health Organization. Guidelines for the Regulatory Assessment of Medicinal Products for Use in Self-Medication. World Health Organization, 2000.
- Bennadi, D. Self-medication: A current challenge. J. Basic Clin. Pharm. 2013, 5, 19. [Google Scholar] [CrossRef]
- Montastruc, J. L.; Bondon-Guitton, E.; Abadie, D.; Lacroix, I.; Berreni, A.; Pugnet, G.; Durrieu, G.; Sailler, L.; Giroud, J. P.; Damase-Michel, C.; Montastruc, F. Pharmacovigilance, risks, and adverse effects of self-medication. Therapies 2016, 71, 257–262. [Google Scholar] [CrossRef]
- Babu, M. M. Factors contributing to the purchase of over-the-counter (OTC) drugs in Bangladesh: an empirical study. Internet J. Third World Med. 2008, 6, 9–24. [Google Scholar]
- Montastruc, J. L.; Bondon-Guitton, E.; Abadie, D.; Lacroix, I.; Berreni, A.; Pugnet, G.; Durrieu, G.; Sailler, L.; Giroud, J. P.; Damase-Michel, C.; Montastruc, F. Pharmacovigilance, risks, and adverse effects of self-medication. Therapie 2016, 71, 257–262. [Google Scholar] [CrossRef]
- Biswas, M.; Roy, M. N.; Manik, M. I. N.; et al. Self-medicated antibiotics in Bangladesh: a cross-sectional health survey conducted in the Rajshahi City. BMC Public Health 2014, 14, 847. [Google Scholar] [CrossRef]
- The Daily Star. Take steps to stop sale of antibiotic drugs without prescriptions, HC tells govt, 2019. Available from: https://www.thedailystar.net/city/take-steps-to-stop-sale-of-antibiotics-without-prescriptions-1734625.
- Gajic, A.; Herrmann, R.; Salzberg, M. The international quality requirements for the conduct of clinical studies and the challenges for study centers to implement them. Ann. Oncol. 2004, 15, 1305–1309. [Google Scholar] [CrossRef]
- Kassie, A. D.; Bifftu, B. B.; Mekonnen, H. S. Self-medication practice and associated factors among adult household members in Meket district, Northeast Ethiopia, 2017. BMC Pharmacol. Toxicol. 2018, 19, 15. [Google Scholar] [CrossRef]
- Colombo, D.; Suso-Ribera, C.; Fernández-Álvarez, J.; Cipresso, P.; Garcia-Palacios, A.; Riva, G.; Botella, C. Affect recall bias: Being resilient by distorting reality. Cogn. Ther. Res. 2020, 44, 906–918. [Google Scholar] [CrossRef]
- Jafari, F.; Khatony, A.; Rahmani, E. Prevalence of self-medication among the elderly in Kermanshah, Iran. Global J. Health Sci. 2015, 7, 360–365. [Google Scholar] [CrossRef]
- Saha, A.; Marma, K. K. S.; Rashid, A.; Tarannum, N.; Das, S.; Chowdhury, T.; ... Mistry, S. K. Risk factors associated with self-medication among the indigenous communities of Chittagong Hill Tracts, Bangladesh. PLoS One 2022, 17, e0269622. [CrossRef]
- Jember, E.; Feleke, A.; Debie, A.; Asrade, G. Self-medication practices and associated factors among households at Gondar town, Northwest Ethiopia: a cross-sectional study. BMC Res. Notes 2019, 12, 1–7. [Google Scholar] [CrossRef]
- Hassali, M. A.; Shafie, A. A.; Al-Qazaz, H.; Tambyappa, J.; Palaian, S.; Hariraj, V. Self-medication practices among the adult population attending community pharmacies in Malaysia: an exploratory study. Int. J. Clin. Pharm. 2011, 33, 794–799. [Google Scholar] [CrossRef]
- Tekeba, A.; Ayele, Y.; Negash, B.; Gashaw, T. Extent of and Factors Associated with Self-Medication among Clients Visiting Community Pharmacies in the Era of COVID-19: Does It Relieve the Possible Impact of the Pandemic on the Health-Care System? Risk Manag Healthc Policy 2021, 14, 4939–4951. [Google Scholar] [CrossRef] [PubMed]
- Rathod, P.; Sharma, S.; Ukey, U.; Sonpimpale, B.; Ughade, S.; Narlawar, U.; ... Gaikwad Jr, S. D. Prevalence, Pattern, and Reasons for Self-Medication: A Community-Based Cross-Sectional Study From Central India. Cureus 2023, 15. [CrossRef]
- Araia, Z. Z.; Gebregziabher, N. K.; Mesfun, A. B. Self-medication practice and associated factors among students of Asmara College of Health Sciences, Eritrea: a cross-sectional study. J. Pharm. Policy Pract. 2019, 12, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kifle, Z. D.; Mekuria, A. B.; Anteneh, D. A.; Enyew, E. F. Self-medication practice and associated factors among private health sciences students in Gondar Town, North West Ethiopia. A Cross-Sectional Study. Inquiry 2021, 58, 00469580211005188. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, M. A.; Francisco, P. M. S. B.; Costa, K. S.; Barros, M. B. de A. Automedicação em idosos residentes em Campinas, São Paulo, Brasil: prevalência e fatores associados. Cad. Saúde Pública. 2012, 28, 335–345. [Google Scholar] [CrossRef] [PubMed]
- Mathewos, T.; Daka, K.; Bitew, S.; Daka, D. Self-medication practice and associated factors among adults in Wolaita Soddo town, Southern Ethiopia. Int. J. Infect. Control 2021, 17. [Google Scholar] [CrossRef]
- Vali, L.; Pourreza, A.; Foroushani, A. R.; Sari, A. A.; Honarm, D. H. An Investigation on Inappropriate Medication Applied among Elderly Patients. World Appl. Sci. J. 2012, 16, 819–825. [Google Scholar]
- Kumar, V.; Mangal, A.; Yadav, G.; Raut, D.; Singh, S. Prevalence and pattern of self-medication practices in an urban area of Delhi, India. Med. J. Dr. DY Patil Univ. 2015, 8(1), 16–20. [Google Scholar] [CrossRef]
- Coelho Filho, J. M.; Marcopito, L. F.; Castelo, A. Medication use patterns among elderly people in an urban area in Northeastern Brazil. Rev. Saude Publica [Internet]. 2004 [cited 2022 Apr 21]; 38(4), 557–564.
- Paavilainen, E.; Lehti, K.; Åstedt-Kurki, P.; Tarkka, M. T. Family functioning assessed by family members in Finnish families of heart patients. Eur. J. Cardiovasc. Nurs. 2006, 5, 54–59. [Google Scholar] [CrossRef]
- Ngo, T. T.; Hoang, P. N.; Pham, H. V.; Nguyen, D. N.; Bui, H. T. T.; Nguyen, A. T.; Do, T. D.; Dang, N. T.; Dinh, H. Q.; Truong, D. Q.; Le, T. A. Routine Medical Check-Up and Self-Treatment Practices among Community-Dwelling Living in a Mountainous Area of Northern Vietnam. BioMed Res. Int. 2021, 2021. [Google Scholar] [CrossRef]
- Das, TK. Quack: Their Role in Health Sector. SSRN Electronic Journal. 2008. Available from: https://papers.ssrn.com/abstract=1292712.
Figure 1.
Indications of symptoms of illness for self-medication practice.
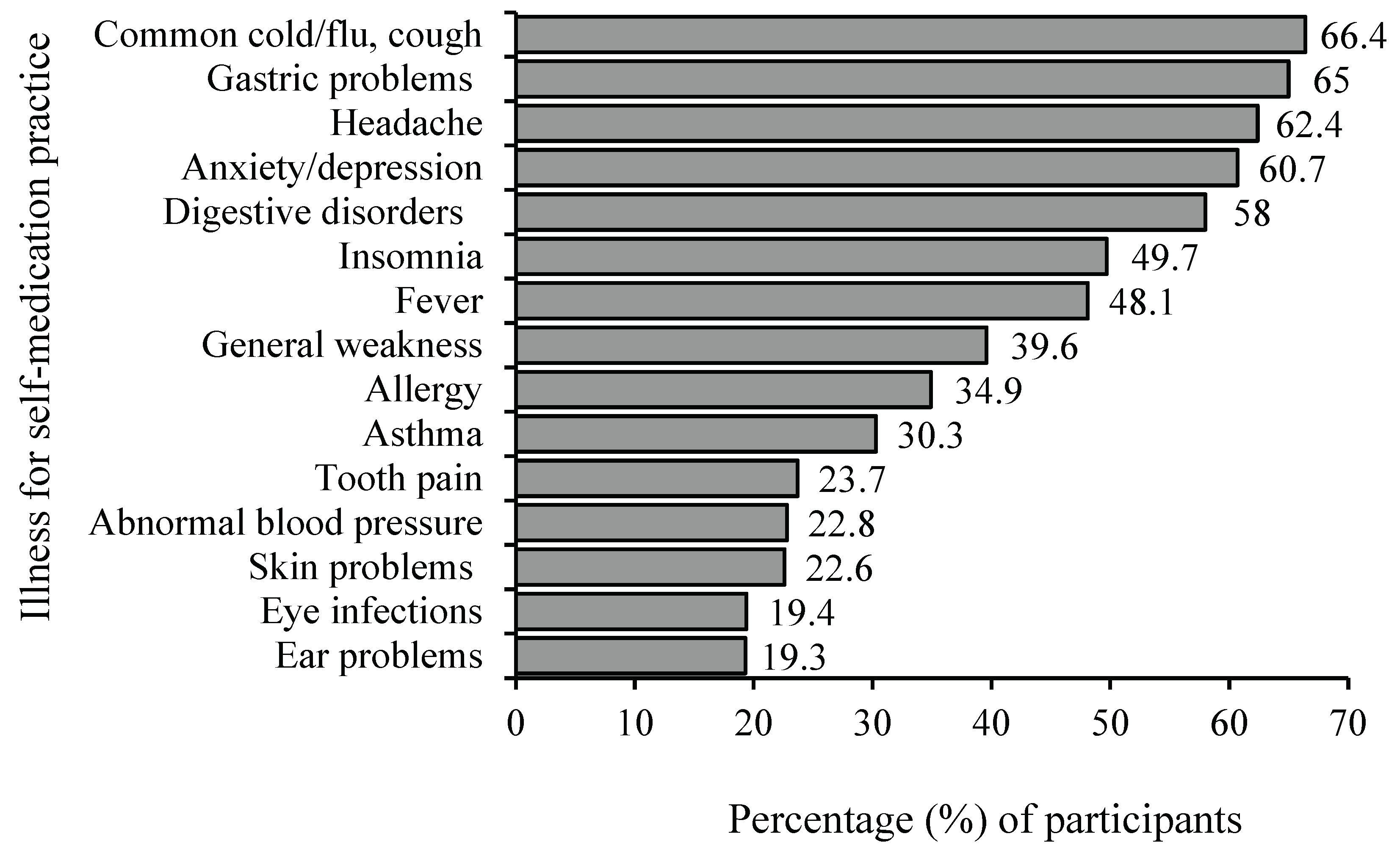
Figure 2.
Reasons for choosing the self-medication.
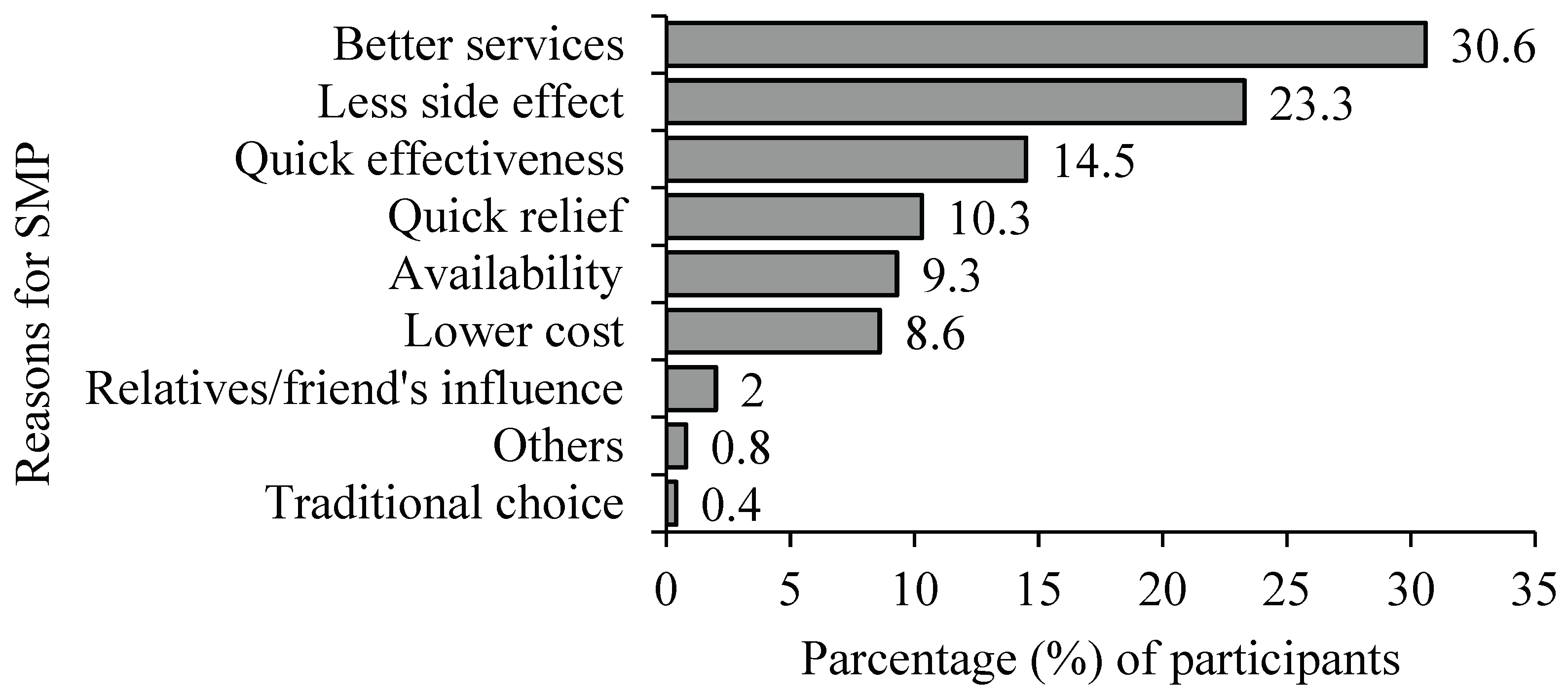
Figure 3.
Disease conditions after self-medication practice.
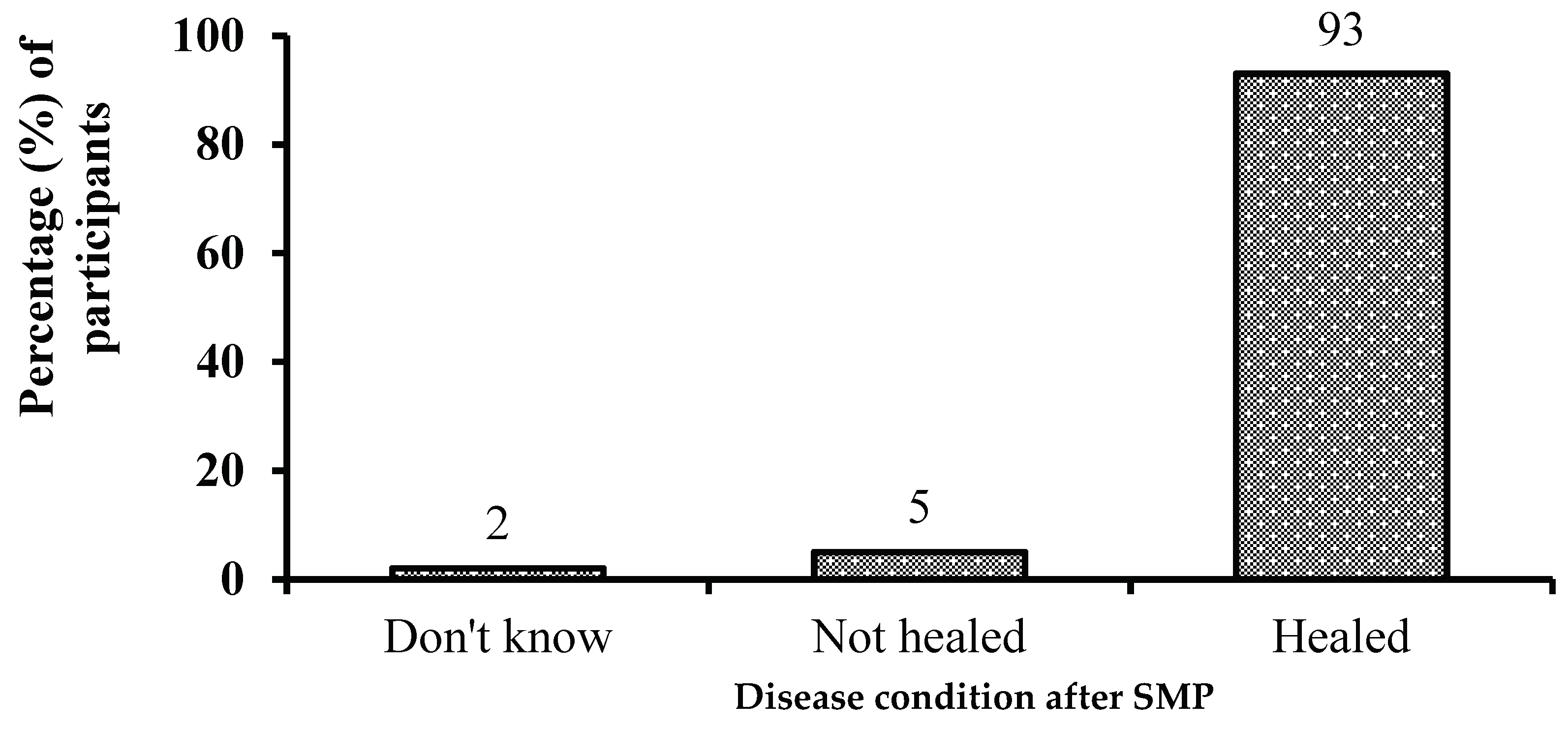
Figure 4.
Side effects after self-medication practice.
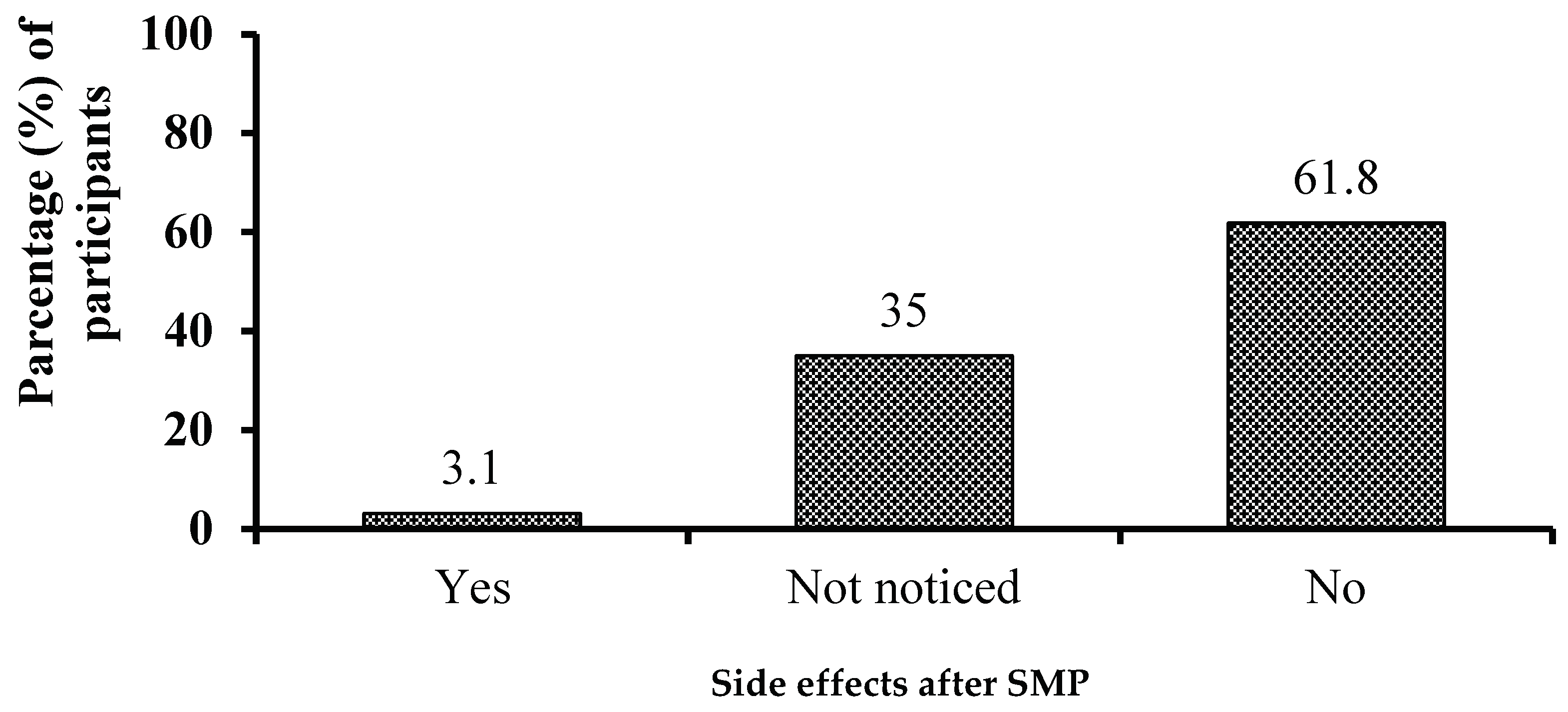
Figure 5.
Forest plot of odds ratios and 95% CI representing the correlation between predictors and practice of self-medication.
Figure 5.
Forest plot of odds ratios and 95% CI representing the correlation between predictors and practice of self-medication.
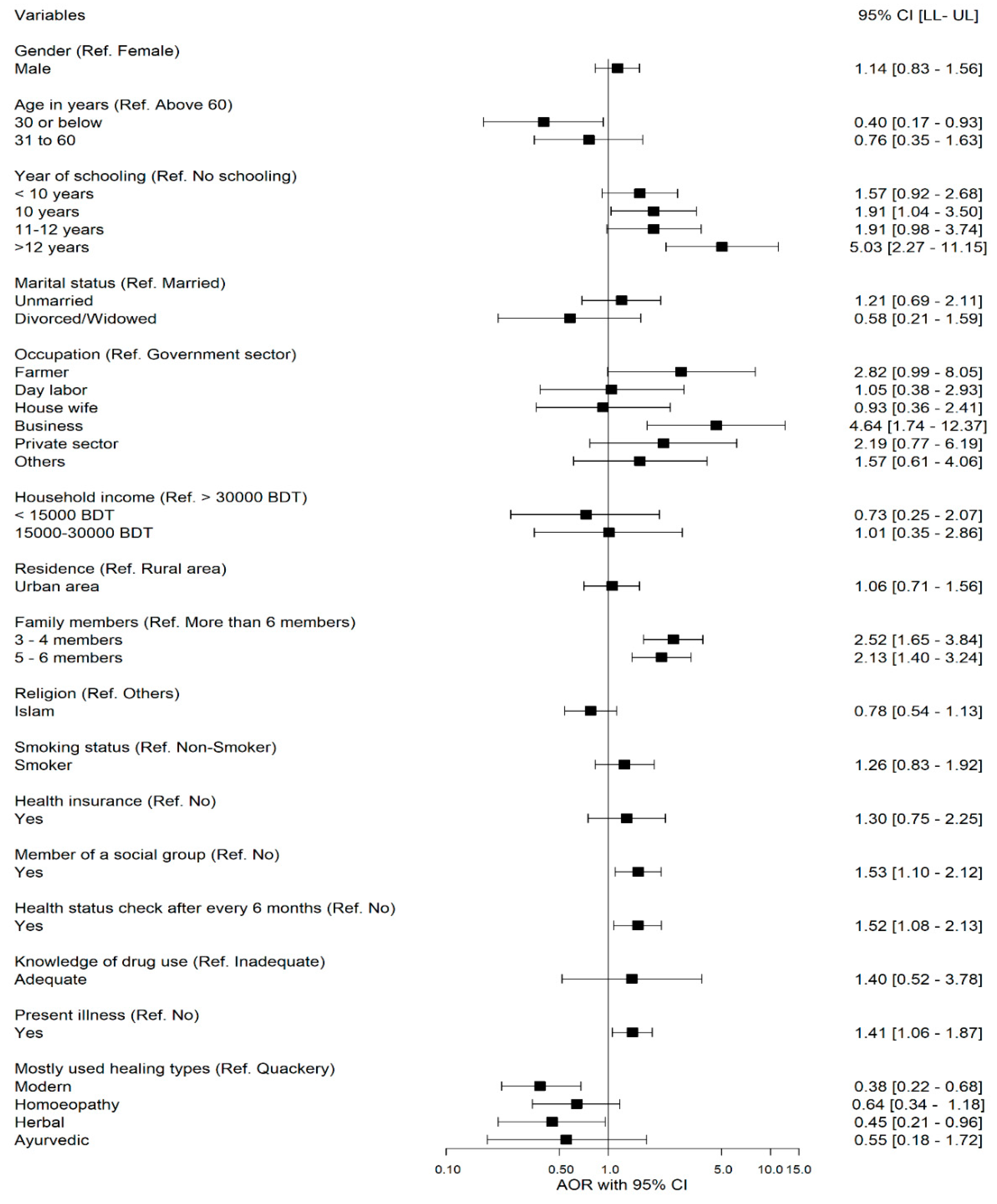

Table 1.
Association of socio-demographic and clinical variables with self-medication practice.
| Variables | Total N = 1320 |
Self-medication | χ2 | p-value | ||||
|---|---|---|---|---|---|---|---|---|
| No | Yes | |||||||
| n | % | n | % | n | % | |||
| Gender | ||||||||
| Male | 672 | 50.9 | 328 | 48.8 | 344 | 51.2 | 55.38 | <0.001 |
| Female | 648 | 49.1 | 447 | 69.0 | 201 | 31.0 | ||
| Age in years | ||||||||
| ≤30 | 915 | 69.3 | 569 | 62.2 | 346 | 37.8 | 16.22 | <0.001 |
| 31 to 60 | 361 | 27.3 | 180 | 49.9 | 181 | 50.1 | ||
| >60 | 44 | 3.3 | 26 | 59.1 | 18 | 40.9 | ||
| Years of schooling | ||||||||
| <10 years 10 years 11-12 years >12 years No Schooling |
510 | 38.6 | 315 | 61.8 | 195 | 38.2 | 43.31 | <0.001 |
| 425 | 32.2 | 254 | 59.8 | 171 | 40.2 | |||
| 172 | 13.0 | 100 | 58.1 | 72 | 41.9 | |||
| 92 | 7.0 | 25 | 27.2 | 67 | 72.8 | |||
| 121 | 9.2 | 81 | 66.9 | 40 | 33.1 | |||
| Marital status | ||||||||
| Unmarried Divorced/Widowed Married |
682 | 51.7 | 406 | 59.5 | 276 | 40.5 | 1.09 | 0.580 |
| 21 | 1.6 | 14 | 66.7 | 7 | 33.3 | |||
| 617 | 46.7 | 355 | 57.5 | 262 | 42.5 | |||
| Occupation | ||||||||
| Farmer | 63 | 4.8 | 23 | 36.5 | 40 | 63.5 | 107.41 | <0.001 |
| Day labor | 76 | 5.8 | 50 | 65.8 | 26 | 34.2 | ||
| House wife | 307 | 23.3 | 231 | 75.2 | 76 | 24.8 | ||
| Business | 104 | 7.9 | 27 | 26.0 | 77 | 74.0 | ||
| Private | 49 | 3.7 | 18 | 36.7 | 31 | 63.3 | ||
| Othersa | 690 | 52.3 | 412 | 59.7 | 278 | 40.3 | ||
| Government | 31 | 2.3 | 14 | 45.2 | 17 | 54.8 | ||
| Household income per month | ||||||||
| <15000 BDT | 938 | 71.1 | 586 | 62.5 | 352 | 37.5 | 20.57 | <0.001 |
| 15000-30000 BDT | 360 | 27.3 | 181 | 50.3 | 179 | 49.7 | ||
| >30000 BDT | 22 | 1.7 | 8 | 36.4 | 14 | 63.6 | ||
| Residence | ||||||||
| Urban area | 161 | 12.2 | 74 | 46.0 | 87 | 54.0 | 12.30 | <0.001 |
| Rural area | 1159 | 87.8 | 701 | 60.5 | 458 | 39.5 | ||
| Religion | ||||||||
| Islam | 1156 | 87.6 | 692 | 59.9 | 464 | 40.1 | 5.07 | 0.024 |
| Othersb | 164 | 12.4 | 83 | 50.6 | 81 | 49.4 | ||
| Family members | ||||||||
| 3-4 members 5 - 6 members Above 6 members |
592 | 44.8 | 322 | 54.4 | 270 | 45.6 | 24.83 | <0.001 |
| 553 | 41.9 | 321 | 58.0 | 232 | 42.0 | |||
| 175 | 13.3 | 132 | 75.4 | 43 | 24.6 | |||
| Smoking status | ||||||||
| Smoker Non-Smoker |
187 | 14.2 | 76 | 40.6 | 111 | 59.4 | 29.35 | <0.001 |
| 1133 | 85.8 | 699 | 61.7 | 434 | 38.3 | |||
| Health insurance | ||||||||
| Yes No |
79 | 6.0 | 30 | 38.0 | 49 | 62.0 | 14.91 | <0.001 |
| 1241 | 94.0 | 745 | 60.0 | 496 | 40.0 | |||
| Member of a social group | ||||||||
| Yes No |
249 | 18.9 | 105 | 42.2 | 144 | 57.8 | 34.65 | <0.001 |
| 1071 | 81.1 | 670 | 62.6 | 401 | 37.4 | |||
| Health status check (after every 6 months) | ||||||||
| Yes No |
223 | 16.9 | 98 | 43.9 | 125 | 56.1 | 24.14 | <0.001 |
| 1097 | 83.1 | 677 | 61.7 | 420 | 38.3 | |||
| Knowledge of drug used | ||||||||
| Adequate Inadequate |
23 | 1.7 | 8 | 34.8 | 15 | 65.2 | 5.53 | 0.019 |
| 1297 | 98.3 | 767 | 59.1 | 530 | 40.9 | |||
| Present illness | ||||||||
| Yes No |
483 | 36.6 | 246 | 50.9 | 237 | 49.1 | 19.02 | <0.001 |
| 837 | 63.4 | 529 | 63.2 | 308 | 36.8 | |||
| Under treatment | ||||||||
| Yes | 473 | 35.8 | 240 | 50.7 | 233 | 49.3 | 19.33 | <0.001 |
| No | 847 | 64.2 | 535 | 63.2 | 312 | 36.8 | ||
| Most frequent healing methods | ||||||||
| Modern Homeopathy Herbal Ayurvedic Quackery |
873 | 66.1 | 563 | 64.5 | 310 | 35.5 | 37.24 | <0.001 |
| 284 | 21.5 | 139 | 48.9 | 145 | 51.1 | |||
| 69 | 5.2 | 34 | 49.3 | 35 | 50.7 | |||
| 19 | 1.4 | 8 | 42.1 | 11 | 57.9 | |||
| 75 | 5.7 | 31 | 41.3 | 44 | 58.7 | |||
Note: a = includes fishermen, garments workers, vehicles driver, swipers, and unemployed b = includes Hindu, Christian, Buddhist.
Table 2.
Bivariate analysis of the factors affecting self-medication practice.
| Variables & Categories | p-value | COR 95% CI [LL- UL] |
|---|---|---|
| Gender Ref. (Female) | ||
| Male | <0.001 | 2.33 [1.86- 2.92] |
| Age (Ref. >60 Years) | ||
| ≤30 Years | 0.680 | 0.88 [0.48- 1.63] |
| 31 to 60 years | 0.250 | 1.45 [0.77- 2.74] |
| Years of schooling (Ref. No schooling) | ||
| < 10 years | 0.290 | 1.25 [0.83- 1.91] |
| 10 years | 0.153 | 1.36 [0.89- 2.09] |
| 11-12 years | 0.128 | 1.46 [0.90- 2.37] |
| >12 years | <0.001 | 5.43 [2.99- 9.84] |
| Marital status (Ref. Married) | ||
| Unmarried | 0.466 | 0.92 [0.74- 1.15] |
| Divorced/Widowed | 0.407 | 0.68 [0.27- 1.70] |
| Occupation (Ref. Government sector) | ||
| Farmer | 0.420 | 1.43 [0.60- 3.43] |
| Day labor | 0.051 | 0.43 [0.18- 1.00] |
| House wife | 0.001 | 0.27 [0.13- 0.58] |
| Business | 0.044 | 2.35 [1.02- 5.40] |
| Private sector | 0.454 | 1.42 [0.57- 3.54] |
| Others | 0.111 | 0.56 [0.27- 1.15] |
| Household income (Ref. >30000 BDT) | ||
| <15000 BDT | 0.017 | 0.34 [0.14- 0.83] |
| >15000-30000 BDT | 0.210 | 0.57 [0.23- 1.38] |
| Residence (Ref. Rural area) | ||
| Urban area | 0.001 | 1.80 [1.29- 2.51] |
| Family members (Ref. More than 6 members) | ||
| 3 - 4 members | <0.001 | 2.57 [1.76- 3.77] |
| 5 - 6 members | <0.001 | 2.22 [1.51- 3.26] |
| Religion (Ref. Others) | ||
| Islam | 0.025 | 0.69 [0.50- 0.95] |
| Smoking status (Ref. Non-Smoker) | ||
| Smoker | <0.001 | 2.35 [1.72- 3.23] |
| Health insurance (Ref. No) | ||
| Yes | <0.001 | 2.45 [1.54- 3.92] |
| Member of a social group (Ref. No) | ||
| Yes | <0.001 | 2.29 [1.73- 3.03] |
| Health status check (after every 6 months) (Ref. No) | ||
| Yes | <0.001 | 2.06 [1.54- 2.75] |
| Knowledge of drug used (Ref. Inadequate) | ||
| Adequate | 0.024 | 2.71 [1.14- 6.45] |
| Present illness (Ref. No) | ||
| Yes | <0.001 | 1.66 [1.32- 2.08] |
| Most frequent healing methods (Ref. Quackery) | ||
| Modern | <0.001 | 0.39 [0.24- 0.63] |
| Homeopathy | 0.241 | 0.74 [0.44- 1.23] |
| Herbal | 0.339 | 0.73 [0.38- 1.40] |
| Ayurvedic | 0.951 | 0.97 [0.35- 2.69] |
Note: COR: Crude odds ratio, CI: Confidence interval, LL: Lower limit, UL: Upper limit.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



