
Submitted:
27 February 2024
Posted:
27 February 2024
You are already at the latest version
Abstract
The role of inflammation in the pathophysiology of acute myocardial infarction (AMI) is well established. Recognizing inflammation's pivotal role in AMI, this manuscript systematically traces historical studies, spanning from early attempts to the present landscape. Several anti-inflammatory trials targeting inflammation in post-AMI have been performed. The review includes key trials, examining their designs, patient demographics, and primary outcomes. Efficacy and challenges are analyzed, shedding light on the translational implications of trial outcomes. The article also discusses emerging trends, ongoing research, and potential future directions in the field. Practical applications and implications for clinical practice are considered, providing a holistic view of the evolving landscape of anti-inflammatory interventions in the context of AMI.
Keywords:
Acute myocardial infarction
; anti-inflammatory interventions
; canakinumab
; colchicine
; coronary artery disease
; IL-6
; inflammation
1. Introduction
Acute myocardial infarction (AMI) stands as a primary contributor to mortality and morbidity in cardiovascular disease (CVD) [1]. AMI is characterized by a complex interplay of physiological responses, including inflammation. The significance of inflammation in AMI is underlined by its role in aggravating tissue damage, influencing plaque stability, and contributing to adverse cardiac remodeling [2,3]. Recognizing inflammation as a key player in the outcome of AMI has prompted a growing interest in anti-inflammatory interventions as potential therapeutic strategies [4].
Early attempts to address inflammation in the context of AMI were marked by a gradual understanding of the complex relationship between inflammation and cardiac events [5,6]. Initial interventions primarily focused on broad-spectrum anti-inflammatory agents, aiming to mitigate the inflammatory response associated with AMI [7,8]. Over time, as our understanding of the inflammatory pathways developed, interventions evolved to target specific components of the inflammatory cascade [9], shifting towards more dedicated strategies, including the exploration of cytokine modulation, antiplatelet agents [10,11], and immune-modulating therapies [12]. The evolution of these interventions reflects a growing awareness of the multifaceted nature of inflammation in AMI, leading to more refined and targeted approaches to address this crucial aspect of cardiovascular (CV) pathology [13].
This comprehensive review aims to explore various strategies targeting inflammation post-AMI, providing insights into their mechanisms and clinical outcomes, emphasizing their importance in enhancing CV health. The scope encompasses an exploration of various agents, mechanisms, and clinical outcomes, shedding light on the evolving landscape of therapeutic interventions aimed at mitigating inflammation in the context of AMI.
2. Classification of Anti-Inflammatory Trials in AMI
Organizing and classifying anti-inflammatory trials in CVD can be approached systematically. Anti-inflammatory trials can be classified according to the targeted inflammatory pathway, according to the class of anti-inflammatory drugs under investigation, according to the patient population, the outcome measures or even the trial phase (Table 1). This methodical approach enhances a thorough comprehension of the landscape and provides systematic organization for researchers, clinicians, and policymakers engaged in AMI-related inflammation research.
From the pathophysiology viewpoint, the ideal approach is to categorize inflammatory trials based on the specific inflammatory pathways or mediators targeted. Based on this, anti-inflammatory strategies can be classified into two main groups: those targeting the central interleukin-1 (IL-1), tumor necrosis factor-a (TNF-α), and interleukin-6 (IL-6) inflammatory signaling pathway and those that operate independently of it [14]. The central IL-6 pathway plays a crucial role in the inflammatory signaling involved in the onset and advancement of CVD [15]. IL-6 coordinate the recruitment of immune cells to the injured myocardium [16]. It promotes the production of acute-phase proteins, such as C-reactive protein (CRP), which serve as markers of inflammation [17]. Additionally, IL-6 influences the differentiation and activation of immune cells, contributing to the inflammatory environment in the infarcted tissue [18,19]. In the other inflammatory cascade during AMI, key molecules outside the IL-6 pathway include matrix metalloproteinase-9 (MMP-9) [20], phospholipase-2 (PLA2) [21], P-selectin, E-selectin, intercellular cell adhesion molecule-1 (ICAM-1) [22], growth differentiation factor-15 (GDF-15) [23,24], and p38-mitogen-activated protein kinase (MAPK) [25]. These molecules collectively contribute to the interplay responses observed in the outcome of AMI, showing the complex nature of the inflammatory cascade in CV pathology. Therefore, addressing these elements within the central IL-6 signaling pathway or alternative inflammatory signaling pathways has the potential to delay the advancement of CV and systemic inflammation, thereby improving CV prognosis [26].
Pathophysiology organization of the anti-inflammatory trials is actual and reasonable but increases the complexity and might create confusion. For the purposes of this review, we decided to present the available studies based on the class of anti-inflammatory drugs under investigation and the studies are divided in two categories: specific target ant-inflammatory agents and broad-spectrum anti-inflammatory agents (Table 2 and Table 3). The review encompassed late-phase trials meeting specific criteria: 1) conducted in individuals with established CVD; 2) comparing anti-inflammatory therapies to a placebo; 3) designed to evaluate CV clinical outcomes and report on CV events and/or infarct size, and not only on the effect on specific inflammatory biomarkers.
3. Studies with Specific-Target Anti-Inflammatory Agents
3.1. CANTOS Study (Canakinumab Anti-inflammatory Thrombosis Outcomes Study)
The canakinumab anti-inflammatory thrombosis outcome study (CANTOS), was a randomized, double-blind, placebo-controlled trial involving stable patients with previous myocardial infarction (MI), evaluated whether canakinumab could prevent recurrent vascular events in men and women who have a persistent proinflammatory response [27].
Canakinumab, is an interleukin-1 beta (IL-1β) inhibitor, approved for use in several rare heritable pediatric conditions associated with IL-1β over-expression [28]. CANTOS trial examined the efficacy of canakinumab, in reducing CV events among 10,061 patients with a history of MI and elevated high-sensitivity C-reactive protein (hsCRP). The primary endpoint included major adverse CV events (MACE) – a composite of non-fatal MI, stroke, and CV death. The trial demonstrated a significant reduction in MACE in the canakinumab group, with a hazard ratio (HR) of 0.85 [95% confidence interval (CI) 0.74–0.98] and a p-value below 0.05. This landmark trial highlighted the link between inflammation, as indicated by hsCRP levels, and CV risk, paving the way for targeted anti-inflammatory therapies in CVD [29]. The CANTOS trial demonstrated that inflammation plays a treatable role in atherosclerosis. By pinpointing IL-1β as a viable therapeutic target, it is poised to stimulate additional clinical investigations and the development of anti-inflammatory agents for CV prevention [30].
3.2. VISTA-16 Trial (Vascular Inflammation Suppression to Treat Acute Coronary Syndrome for 16 Weeks)
The plasma level of secretory PLA2 is a known risk factor for CAD and is associated with adverse outcomes in patients with stable CAD and acute coronary syndromes (ACS) [31,32,33]. The VISTA-16 trial, initiated in 2006, set out to investigate the efficacy of varespladib, a potent anti-inflammatory agent by interfering with arachidonic acid metabolism (inhibitor of secretory PLA2), in suppressing vascular inflammation among patients with ACS. This randomized, double-blind trial enrolled 5,145 participants and aimed to evaluate the impact of varespladib on MACE [34].
The trial was prematurely terminated in 2012 due to futility, as varespladib failed to demonstrate a statistically significant reduction in CV events compared to the placebo group (6.1% vs. 5.1%; HR, 1.25; 95% CI, 0.97-1.61; p-value = 0.08). Of note, the composite secondary outcome of CV mortality, MI, and stroke was higher in the varespladib arm (4.6% vs. 3.8%, HR, 1.36; 95% CI, 1.02-1.82; p-value = 0.04). This was due primarily to a greater incidence of MI in the varespladib arm (3.4% vs. 2.2%; p = 0.005) [35]. The absence of a meaningful clinical benefit, coupled with the trial’s termination, underscored the limitations and challenges associated with targeting secretory PLA2 as a therapeutic approach in ACS [36]. The findings prompted a critical reevaluation of the potential role of this pathway in ACS treatment strategies.
3.3. LATITUDE-TIMI 60 Trial (Losmapimod to Inhibit p38 MAP Kinase as a Therapeutic Target and Modify Outcomes After an Acute Coronary Syndrome)
Losmapimod is a selective, reversible, competitive inhibitor of p38 MAPK [37]. MAPK-mediated inflammatory augmentation has been implicated in atherogenesis, plaque destabilization, and detrimental processes in infarction and recovery [38], and is considered an alternative inflammatory signaling pathway that acts outside the IL-6 pathway [39,40]. Preliminary data showed that the use of losmapimod in non ST elevation MI (NSTEMI) patients attenuates inflammation and may improve outcomes [41].
The LATITUDE-TIMI 60 trial, was a pivotal multinational investigation that delved into the efficacy and safety of losmapimod, administered at a dosage of 7.5 mg twice daily, in a cohort of 3503 patients presenting with ACS [42]. Contrary to expectations, the trial did not reveal a significant reduction in MACEs, including CV death, MI, and stroke (8.1% vs 7.0%, HR, 1.16; 95% CI, 0.91-1.47; p-value = 0.24) [42]. Losmapimod did not demonstrate a risk reduction for recurrent MACEs events over the 12-week treatment period in patients hospitalized with ACS. Additionally, there was no indication that losmapimod influenced the occurrence of secondary outcomes, including all-cause mortality. Consequently, this study does not endorse the adoption of a strategy involving p38 MAPK inhibition with losmapimod for patients admitted with MI [43].
3.4. SOLID-TIMI 52 Trial (Stabilization of plaques using Darapladib-Thrombolysis in Myocardial Infarction 52)
Lipoprotein-associated phospholipase A2 (Lp-PLA2) has been proposed as a potential causal factor in atherosclerosis development and suggested to contribute to plaque instability via pathways associated with inflammation [32,44]. Darapladib is an oral selective Lp-PLA2 inhibitor that reduces Lp-PLA2 activity in plasma5 and in atherosclerotic plaques [45]. The use of darapladib in stable coronary artery patients did not show a significant reduction in the primary composite endpoint [46].
The SOLID-TIMI 52 trial, initiated in 2010, and it was a randomized, double-blind, placebo-controlled, multicenter, event-driven trial, focusing to investigate the role of darapladib, to stabilize atherosclerotic plaques and reduce CV events [47]. Enrolling over 13,000 patients, the trial aimed to evaluate darapladib’s impact on MACEs, such as CV death, MI, and stroke. However, the trial did not meet its primary endpoint, as darapladib did not significantly reduce the risk of MACE compared to placebo [48]. The findings of SOLID-TIMI 52 raised questions about the role of Lp-PLA2 inhibition as a therapeutic target and prompted further exploration of alternative approaches to address CV risk in patients with chronic CAD.
3.5. ASSAIL-MI-Trial (ASSessing the Effect of Anti-IL-6 Treatment in Myocardial Infarction)
IL-6 is the crucial pro-inflammatory cytokine that is upregulated during MI and affects both plaque destabilization and myocardial remodeling [49,50]. Tocilizumab, an IL-6 receptor antagonist, can attenuated the inflammatory response and primarily PCI-related TnT release in NSTEMI patients [12]. The ASSAIL-MI trial, a randomized, double-blind, placebo-controlled study, was conducted at three high-volume PCI centers in Norway, designed to evaluate the effect of tocilizumab on myocardial salvage in patients with acute ST-elevation MI (STEMI) [51,52]. Eligible participants included patients admitted with STEMI within 6 hours of symptom onset. In a 1:1 randomization, consenting patients received a single infusion of either 280 mg tocilizumab or placebo promptly. The primary endpoint, evaluated using magnetic resonance imaging after 3 to 7 days, was the myocardial salvage index [52].
Out of the total, 101 patients were randomized to receive tocilizumab, and 98 patients received the placebo. The tocilizumab group exhibited a larger myocardial salvage index compared to the placebo group, with an adjusted between-group difference of 5.6 (95% CI: 0.2 to 11.3) percentage points (p-value = 0.04). While microvascular obstruction was less extensive in the tocilizumab arm, there was no significant difference in the final infarct size between the tocilizumab and placebo arms (7.2% vs. 9.1% of myocardial volume, p-value = 0.08). Adverse events were evenly distributed across the treatment groups. In conclusion, tocilizumab demonstrated an increase in myocardial salvage among patients with acute STEMI in the ASSAIL-MI trial [52].
3.6. SELECT-ACS (Effects of the P-Selectin Antagonist Inclacumab on Myocardial Damage After Percutaneous Coronary Intervention for Non-ST-Elevation Myocardial Infarction)
The SELECT ACS trial aimed to assess the efficacy of inclacumab in reducing myocardial damage during percutaneous coronary intervention (PCI) in patients with NSTEMI[53]. P-selectin, an adhesion molecule involved in cellular interactions, particularly among endothelial cells, platelets, and leukocytes, served as the target [54]. Inclacumab, a recombinant monoclonal antibody against P-selectin, was evaluated for its potential anti-inflammatory, antithrombotic, and antiatherogenic properties [55].
In this randomized trial involving 544 NSTEMI patients scheduled for coronary angiography and possible ad hoc PCI, participants received one pre-procedural infusion of inclacumab at either 5 or 20 mg/kg or a placebo. The primary endpoint, assessed in patients who underwent PCI and received the study medication with available efficacy data (n = 322), was the change in troponin I from baseline at 16 and 24 hours after PCI.
Results indicated that inclacumab at 20 mg/kg demonstrated a significant reduction in troponin I levels, with a placebo-adjusted geometric mean percent change of -24.4% at 24 hours (p-value = 0.05) and -22.4% at 16 hours (p-value = 0.07). Similar trends were observed in peak troponin I levels and the area under the curve over 24 hours. Creatine kinase-myocardial band also showed reductions with inclacumab at 20 mg/kg [53]. Notably, adverse events did not significantly differ between the groups. In conclusion, inclacumab appears to effectively diminish myocardial damage following PCI in patients with NSTEMI [56].
4. Studies with Broad-Spectrum Anti-Inflammatory Agents
4.1. COLCOT Trial (Colchicine Cardiovascular Outcomes Trial)
Published in 2019, the COLCOT trial investigated the use of colchicine, in 4,745 post-MI patients [57]. Colchicine has a broad cellular effect that include inhibition of tubulin polymerization and alteration of leukocyte responsiveness[58]. The primary endpoint, a composite of CV death, MI, stroke, resuscitated cardiac arrest, and urgent hospitalization for angina leading to coronary revascularization, exhibited an HR of 0.77 (95% CI 0.61–0.96), with a statistically significant p-value of 0.02. In individuals who recently experienced a MI, the use of low-dose colchicine demonstrated efficacy in preventing MACEs when compared to a placebo. The primary benefit stemmed from a notable reduction in the occurrence of stroke and the need for urgent hospitalization due to unstable angina leading to revascularization. Notably, colchicine exhibited positive effects, particularly among patients with diabetes. The study drug was well-tolerated and exhibited a similar incidence of infection and diarrhea compared to the placebo (9.7% vs 8.9%, p-value=0.35). Additionally, colchicine was deemed cost-effective. The observed advantages of colchicine were attributed to the anti-inflammatory properties inherent in the drug. This trial underscored the potential of colchicine in preventing major CV events in this high-risk population, shedding light on a novel anti-inflammatory approach in post-MI care [59].
4.2. LoDoCo2 Trial (Low-Dose Colchicine after Myocardial Infarction)
LoDoCo trial was designed to determine whether colchicine 0.5 mg/day, a broad spectrum anti-inflammatory agent, could minimize the risk of CV events in patients with clinically stable coronary disease [60]. The study was not placebo-controlled, and the primary outcome was the composite incidence of ACS, out-of-hospital cardiac arrest, or non-cardioembolic ischemic stroke. 532 patients were included in the study. The primary outcome occurred in 15 of 282 patients (5.3%) who received colchicine and 40 of 250 patients (16.0%) assigned no colchicine (hazard ratio: 0.33; 95% confidence interval [CI] 0.18 to 0.59; p < 0.001; number needed to treat: 11)[60].
The larger LoDoCo2 trial aimed to confirm the result of the LoDoCo trial. It was conducted in 2020 and enrolled 5,522 post-myocardial infarction participants, focusing to assess the impact of low-dose colchicine on MACEs [61]. The primary endpoint, a composite of CV death, MI, ischemic stroke, or urgent hospitalization for angina requiring revascularization, exhibited a hazard ratio of 0.69 (95% CI 0.50–0.96), with a statistically significant p-value of 0.02 [62]. This trials not only confirmed the efficacy of colchicine in reducing CV risk but also highlighted the potential benefits of using a lower colchicine dose in post-MI patients [63].
4.3. COPS Trial (Colchicine in Patients With Acute Coronary Syndrome)
COPS was multicenter, randomized, double-blind, placebo-controlled trial involving 17 hospitals in Australia that provide acute cardiac care service [64]. The study enrolled 795 participants with ACS investigated the potential utility of colchicine. The patients were randomized to receive colchicine or placebo, in addition to standard secondary prevention pharmacotherapy, and were followed up for a minimum of 12 months. The primary outcome, a composite of all-cause mortality, ACS, unplanned urgent revascularization, and noncardioembolic ischemic stroke, did not significantly differ between the colchicine and placebo groups at 12 months (24 vs 38 events, p-value = 0.09). Of note, the colchicine group showed a higher rate of total death, particularly non-CV death (p-value= 0.024). Adverse effects were similar between groups. In conclusion, colchicine did not significantly impact CV outcomes and was associated with a higher mortality rate in ACS patients.
4.4. CIRT Trial (Cardiovascular Inflammation Reduction Trial)
The Cardiovascular Inflammation Reduction Trial (CIRT), initiated in 2019, investigated the impact of low-dose methotrexate on CV events among individuals with a history of MI or multi-vessel CAD and either type 2 diabetes or metabolic syndrome [65]. Enrolling a sizable population of 4786 patients, the trial aimed to discern the potential benefits of methotrexate in reducing MACE for a median follow up period of 2.3 years. The primary end point at the onset of the trial was a composite of nonfatal MI, nonfatal stroke, or CV death and hospitalization for unstable angina. Methotrexate did not result in lower IL-1β, IL-6, or CRP levels than placebo. The final primary end point occurred in 201 patients in the methotrexate group and in 207 in the placebo group (4.13 vs. 4.31 per 100 person-years; HR, 0.96; 95% CI, 0.79 to 1.16). The original primary end point occurred in 170 patients in the methotrexate group and in 167 in the placebo group (, 3.46 vs. 3.43 per 100 person-years; hazard ratio, 1.01; 95% CI, 0.82 to 1.25) [66].
4.5. AIM-HIGH (Atherothrombosis Intervention in Metabolic Syndrome with Low HDL/High Triglycerides: Impact on Global Health Outcomes)
Conducted in 2011, the AIM-HIGH trial assessed extended-release niacin in 3,414 patients with a history of CVD and dyslipidemia. The trial did not demonstrate additional CV benefit from niacin therapy compared to the placebo. The hazard ratio for the primary composite endpoint of cardiovascular events was 1.02 (95% CI 0.87–1.21), with a non-significant p-value of 0.79 [67]. AIM-HIGH raised questions about the efficacy of niacin in improving cardiovascular outcomes in this specific patient population, influencing subsequent considerations regarding niacin therapy in CV care [68].
4.6. ALL-Heart Study (Allopurinol versus Usual Care in UK Patients with Ischemic Heart Disease)
Elevated levels of serum uric acid have been linked to unfavorable CV outcomes [69]. While certain observational studies propose that therapy aimed at lowering uric acid may decrease CV risk [70], conflicting evidence exists as other studies have not observed similar benefits [71]. Allopurinol, a xanthine oxidase inhibitor, is approved for gout prophylaxis, symptomatic hyperuricemia treatment, and hyperuricemia prevention related to cancer chemotherapy. Allopurinol’s potential benefits for patients with ischemic heart disease may extend beyond its ability to lower serum uric acid levels. This includes its impact on decreasing vascular oxidative stress mediated by xanthine oxidase, which could be a separate mechanism from its uric acid-lowering effects [72,73].
The ALL-HEART trial, a multicenter, prospective, randomized study, aimed to investigate the impact of allopurinol therapy in patients aged 60 years or older with ischemic heart disease and no history of gout. The primary outcome, a composite of non-fatal myocardial infarction, non-fatal stroke, or CV death, showed no significant difference between the allopurinol and usual care groups. Over a mean follow-up of 4.8 years, rates of the primary endpoint and overall mortality were similar between the groups, suggesting that allopurinol therapy did not confer additional CV benefits in this specific population [74].
5. Discussion
The studies reviewed above, demonstrate that only CANTOS with canakinumab, and COLCOT, and LoDoCo2 with colchicine, achieved favorable clinical outcomes. The smaller trials like ASSAIL-MI with tocilizumab and SELECT-ACS with inclacumab, which assessed myocardial damage using CMR or troponin levels, showed promising results but need larger controlled studies to fully examine their impact on clinical outcomes.
Conversely, the remaining randomized trials did not show evidence that anti-inflammatory therapies can alter the prognosis in patients with CVD. This emphasizes that not all anti-inflammatory treatments are equivalent, and the method by which inflammation is reduced probably determines whether a particular anti-inflammatory drug will lower CV events. Therefore, a thorough examination and analysis of each study’s design can yield valuable insights.
When comparing CANTOS and CIRT, significant differences may contribute to their divergent outcomes [29,66]. While, both trials primarily enrolled patients already on statin therapy, the patients in CIRT study achieved better LDL-C control, falling below the current guideline target (<70 mg/dL). Moreover, CANTOS required participants to have hsCRP levels of ≥2 mg/L, while CIRT did not mandate elevated hsCRP levels. Consequently, baseline hsCRP values were higher in CANTOS, indicating a population with greater residual inflammatory risk. The most notable contrast lies in how these trials addressed inflammation: while CANTOS directly targeted the IL-1β pathway, reducing downstream mediators IL-6 and hsCRP, CIRT lowered inflammation (lower WBC) without altering IL-1β, IL-6, or hsCRP. Hence, the efficacy of anti-inflammatory therapies may vary, with the mechanism of inflammation reduction likely determining their impact on CV events.
The extent of hsCRP decrease after a single dose of canakinumab could offer a straightforward clinical approach to pinpoint individuals who may gain the greatest advantage from ongoing treatment [75]. Extracting this discovery in the design of all the other trials, could explain that the inability to show effectiveness could also be linked to the mechanism, highlighting the importance of selecting the appropriate inflammatory target or drug when inhibiting inflammation in CVD.
The remarkable outcome from the CANTOS trial demonstrated the successful reduction of CV risk with canakinumab therapy, highlighting the crucial inflammatory targets likely concentrated within the IL-1β to IL-6 to CRP pathway [76]. Theoretically, colchicine, the other effective broad anti-inflammatory medication, has the potential to irreversibly inhibit the NLRP3 inflammasome, leading to neutrophil dysfunction. This mechanism results in decreased circulating levels of IL-1β, IL-6, and CRP [77]. However, the mechanism of the CV benefit from colchicine needs further evaluation.
Based on the LoDoCo2 and CLCOT trials, low-dose colchicine is considered the ideal anti-inflammatory treatment in patient with stable CAD [78]. Of note, a recent meta-analysis included the four major randomized clinical trials, COLCOT and the COPS in ACS patient LoDoCo and LoDoCo2 in stable CAD including more than 11,550 patients showed in the secondary prevention of CV events, augmenting standard medical therapy with low-dose colchicine decreases the occurrence of major CV events, with the exception of CV mortality, in comparison to standard medical therapy alone [79]. The decrease in inflammation could be a critical factor in the effectiveness of low-dose colchicine in reducing the risk of recurrent cardiovascular events post-MI. Regular monitoring of hs-CRP levels before and after colchicine treatment could be significant [80].
6. Future Directions and Emerging Trends
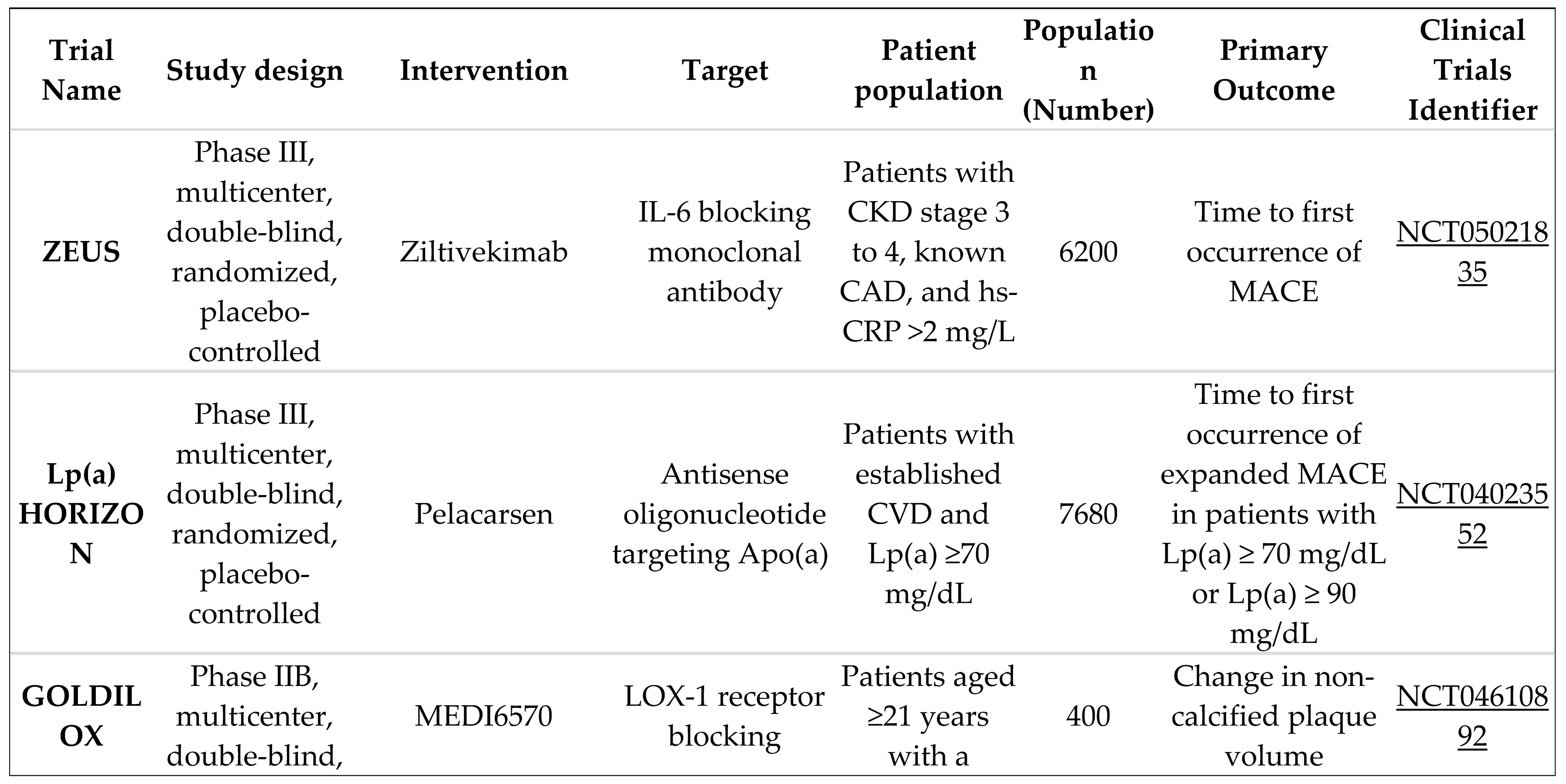
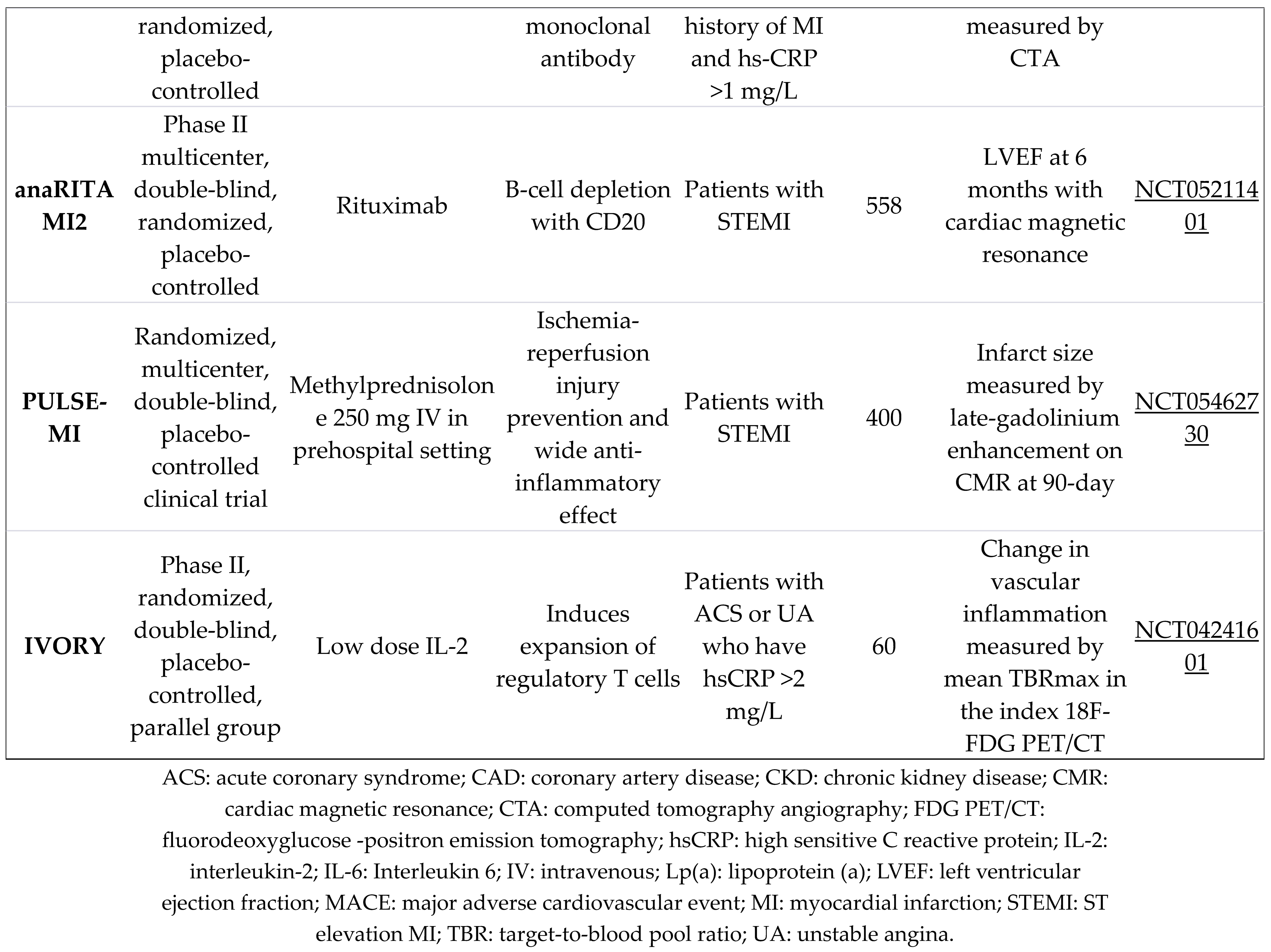
Looking into the future of inflammation-targeted strategies in CV health, the trajectory is guided by several key elements. Ongoing research and upcoming trials are composed to unravel deeper insights into the complexities of inflammatory pathways, providing a novel understanding of their role in CV dynamics [81,82]. As the scientific community strives to expand its knowledge base, innovative approaches are anticipated to take center stage. These may encompass precision medicine [83], advanced imaging techniques [84], and evolving pharmacotherapies designed to modulate inflammation with greater specificity [85]. The Table 4, summarizes all the ongoing clinical studies of treatments targeting inflammation in the context of atherosclerosis and AMI.
The landscape is also marked by emerging trends that signify a paradigm shift in addressing inflammation-related CV risks. From harnessing the potential of artificial intelligence in data analysis to exploring the role of microbiota in CV health, these trends underscore the multidimensional nature of ongoing investigations [86,87].
These potential advancements not only hold implications for scientific understanding but also bear a profound impact on future clinical practice. A shift towards personalized, targeted interventions may redefine treatment strategies, offering more effective and tailored approaches to patients [88]. As these trends unfold, they are set to shape the landscape of CV care, paving the way for a new era in the prevention and management of CVD.
7. Implications for Clinical Practice
In considering the implications for clinical practice, the integration of anti-inflammatory strategies into the management of AMI emerges as a transformative avenue. The practical applications of these strategies, explored in this section, shed light on their potential to redefine how we approach AMI treatment. As we navigate the intricacies of AMI management, understanding the significance of incorporating anti-inflammatory interventions into existing protocols becomes paramount [89]. This involves not only recognizing the specific clinical scenarios where such strategies prove most effective but also ensuring a seamless integration that aligns with the broader treatment landscape [90].
In this direction, the new 2021 guidelines on CVD prevention issued by the European Society of Cardiology, suggested the consideration of low-dose colchicine (0.5 mg once daily) for secondary prevention of CVD, especially in cases where recurrent events persist despite optimal therapy [91].
Moreover, the discussion extends beyond general applications to delve into the realm of personalized medicine. Tailoring anti-inflammatory interventions to the unique characteristics of individual patients represents a paradigm shift in clinical practice. By acknowledging patient-specific considerations, such as comorbidities, genetic predispositions, and lifestyle factors, clinicians can optimize the efficacy of anti-inflammatory strategies while minimizing potential risks. As we advance, these considerations forge a path toward a more patient-centered approach in the realm of AMI management, promising not only improved outcomes but also a more tailored and compassionate form of CV care.
The ideal AMI target might be the patient with a large inflammatory burden. Extensive MIs, characterized by significant ischemic damage, release higher levels of inflammatory mediators, leading to a more pronounced acute inflammatory response. These patients with extensive MIs, and consequently elevated inflammatory burden, might experience greater advantages from early anti-inflammatory treatments. Thus, selection of patients with STEMI rather than NSTEMI, or selection of patients with elevated levels of cardiac troponins might be a useful approach, In order to promptly identify individuals with substantial AMI and identify the most suitable surrogate markers for anti-inflammatory therapy [92]. Additionally, the use of available biomarkers of inflammation (e.g. CRP and IL-6) could further improve the identification of individuals with large inflammatory burden post-AMI and benefit by anti-inflammatory strategies. Finally, the ideal patient, would benefit by administration of anti-inflammatory therapy at early stages after the acute event. A treatment plan aimed at addressing the initial stages of excessive and harmful post-AMI inflammation could potentially restrict further myocardial damage [92].
8. Conclusion
In conclusion, through meticulous examination of pivotal trials, we uncovered diverse approaches, ranging from therapies targeting the central IL-6 pathway to broad-spectrum anti-inflammatory interventions. Despite the undoubted complexities in trial designs, patient populations, and primary outcomes, an understanding emerges, highlighting both successes and challenges in the pursuit of effective anti-inflammatory interventions post-AMI. As we navigate this evolving field, our review not only synthesizes existing knowledge but also underscores the need for continued exploration and innovation. This comprehensive overview sets the stage for future research and clinical endeavors, providing a foundation for refining anti-inflammatory strategies and improving CV outcomes in AMI patients.
Author Contributions
A.M., S.T., and G.K. (George Kassimis), were involved in the conceptualization, writing, and editing. M.K, S.S., G.K. (Georgia Karmioti), M.D., M.M., and A.Z. were involved in editing and reviewing. Supervision was by S.T., and G.K (George Kassimis). All authors have read and agreed to the published version of the manuscript.
Funding
No funding for this research.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- McManus, D.D.; Gore, J.; Yarzebski, J.; Spencer, F.; Lessard, D.; Goldberg, R.J. Recent Trends in the Incidence, Treatment, and Outcomes of Patients with STEMI and NSTEMI. Am J Med 2011, 124, 40–47. [CrossRef]
- Libby, P. Mechanisms of Acute Coronary Syndromes and Their Implications for Therapy. N Engl J Med 2013, 368, 2004–2013. [CrossRef]
- Libby, P. The Changing Landscape of Atherosclerosis. Nature 2021, 592, 524–533. [CrossRef]
- Mitsis, A.; Kadoglou, N.P.E.; Lambadiari, V.; Alexiou, S.; Theodoropoulos, K.C.; Avraamides, P.; Kassimis, G. Prognostic Role of Inflammatory Cytokines and Novel Adipokines in Acute Myocardial Infarction: An Updated and Comprehensive Review. Cytokine 2022, 153, 155848. [CrossRef]
- Ross, R. Atherosclerosis--an Inflammatory Disease. N Engl J Med 1999, 340, 115–126. [CrossRef]
- Berk, B.C.; Weintraub, W.S.; Alexander, R.W. Elevation of C-Reactive Protein in “Active” Coronary Artery Disease. Am J Cardiol 1990, 65, 168–172. [CrossRef]
- Ridker, P.M.; Cushman, M.; Stampfer, M.J.; Tracy, R.P.; Hennekens, C.H. Inflammation, Aspirin, and the Risk of Cardiovascular Disease in Apparently Healthy Men. N Engl J Med 1997, 336, 973–979. [CrossRef]
- Ridker, P.M.; Rifai, N.; Clearfield, M.; Downs, J.R.; Weis, S.E.; Miles, J.S.; Gotto, A.M.; Air Force/Texas Coronary Atherosclerosis Prevention Study Investigators Measurement of C-Reactive Protein for the Targeting of Statin Therapy in the Primary Prevention of Acute Coronary Events. N Engl J Med 2001, 344, 1959–1965. [CrossRef]
- Lindmark, E.; Diderholm, E.; Wallentin, L.; Siegbahn, A. Relationship between Interleukin 6 and Mortality in Patients with Unstable Coronary Artery Disease: Effects of an Early Invasive or Noninvasive Strategy. JAMA 2001, 286, 2107–2113. [CrossRef]
- Al-Bahrani, A.; Taha, S.; Shaath, H.; Bakhiet, M. TNF-Alpha and IL-8 in Acute Stroke and the Modulation of These Cytokines by Antiplatelet Agents. Curr Neurovasc Res 2007, 4, 31–37. [CrossRef]
- Heinzmann, A.C.A.; Coenen, D.M.; Vajen, T.; Cosemans, J.M.E.M.; Koenen, R.R. Combined Antiplatelet Therapy Reduces the Proinflammatory Properties of Activated Platelets. TH Open 2021, 5, e533–e542. [CrossRef]
- Kleveland, O.; Kunszt, G.; Bratlie, M.; Ueland, T.; Broch, K.; Holte, E.; Michelsen, A.E.; Bendz, B.; Amundsen, B.H.; Espevik, T.; et al. Effect of a Single Dose of the Interleukin-6 Receptor Antagonist Tocilizumab on Inflammation and Troponin T Release in Patients with Non-ST-Elevation Myocardial Infarction: A Double-Blind, Randomized, Placebo-Controlled Phase 2 Trial. Eur Heart J 2016, 37, 2406–2413. [CrossRef]
- Wollenweber, T.; Roentgen, P.; Schäfer, A.; Schatka, I.; Zwadlo, C.; Brunkhorst, T.; Berding, G.; Bauersachs, J.; Bengel, F.M. Characterizing the Inflammatory Tissue Response to Acute Myocardial Infarction by Clinical Multimodality Noninvasive Imaging. Circ Cardiovasc Imaging 2014, 7, 811–818. [CrossRef]
- Ridker, P.M.; Lüscher, T.F. Anti-Inflammatory Therapies for Cardiovascular Disease. Eur Heart J 2014, 35, 1782–1791. [CrossRef]
- Gabriel, A.S.; Martinsson, A.; Wretlind, B.; Ahnve, S. IL-6 Levels in Acute and Post Myocardial Infarction: Their Relation to CRP Levels, Infarction Size, Left Ventricular Systolic Function, and Heart Failure. Eur J Intern Med 2004, 15, 523–528. [CrossRef]
- Libby, P. Targeting Inflammatory Pathways in Cardiovascular Disease: The Inflammasome, Interleukin-1, Interleukin-6 and Beyond. Cells 2021, 10, 951. [CrossRef]
- Ridker, P.M. From C-Reactive Protein to Interleukin-6 to Interleukin-1: Moving Upstream To Identify Novel Targets for Atheroprotection. Circ Res 2016, 118, 145–156. [CrossRef]
- Ridker, P.M.; Rane, M. Interleukin-6 Signaling and Anti-Interleukin-6 Therapeutics in Cardiovascular Disease. Circ Res 2021, 128, 1728–1746. [CrossRef]
- Anzai, A.; Ko, S.; Fukuda, K. Immune and Inflammatory Networks in Myocardial Infarction: Current Research and Its Potential Implications for the Clinic. Int J Mol Sci 2022, 23, 5214. [CrossRef]
- Halade, G.V.; Jin, Y.-F.; Lindsey, M.L. Matrix Metalloproteinase (MMP)-9: A Proximal Biomarker for Cardiac Remodeling and a Distal Biomarker for Inflammation. Pharmacol Ther 2013, 139, 32–40. [CrossRef]
- Gerber, Y.; McConnell, J.P.; Jaffe, A.S.; Weston, S.A.; Killian, J.M.; Roger, V.L. Lipoprotein-Associated Phospholipase A2 and Prognosis after Myocardial Infarction in the Community. Arterioscler Thromb Vasc Biol 2006, 26, 2517–2522. [CrossRef]
- Kerner, T.; Ahlers, O.; Reschreiter, H.; Bührer, C.; Möckel, M.; Gerlach, H. Adhesion Molecules in Different Treatments of Acute Myocardial Infarction. Crit Care 2001, 5, 145–150. [CrossRef]
- Tzikas, S.; Palapies, L.; Bakogiannis, C.; Zeller, T.; Sinning, C.; Baldus, S.; Bickel, C.; Vassilikos, V.; Lackner, K.J.; Zeiher, A.; et al. GDF-15 Predicts Cardiovascular Events in Acute Chest Pain Patients. PLoS One 2017, 12, e0182314. [CrossRef]
- Tzikas, S.; Vassilikos, V.; Keller, T. GDF-15 as a Risk Stratification Biomarker for Cardiovascular Disease. Int J Cardiol 2019, 292, 246–247. [CrossRef]
- Abe, J. i; Baines, C.P.; Berk, B.C. Role of Mitogen-Activated Protein Kinases in Ischemia and Reperfusion Injury : The Good and the Bad. Circ Res 2000, 86, 607–609. [CrossRef]
- Wang, J.; Wang, M.; Lu, X.; Zhang, Y.; Zeng, S.; Pan, X.; Zhou, Y.; Wang, H.; Chen, N.; Cai, F.; et al. IL-6 Inhibitors Effectively Reverse Post-Infarction Cardiac Injury and Ischemic Myocardial Remodeling via the TGF-Β1/Smad3 Signaling Pathway. Exp Ther Med 2022, 24, 576. [CrossRef]
- Ridker, P.M.; Thuren, T.; Zalewski, A.; Libby, P. Interleukin-1β Inhibition and the Prevention of Recurrent Cardiovascular Events: Rationale and Design of the Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS). Am Heart J 2011, 162, 597–605. [CrossRef]
- Welzel, T.; Oefelein, L.; Twilt, M.; Pfister, M.; Kuemmerle-Deschner, J.B.; Benseler, S.M. Tapering of Biological Treatment in Autoinflammatory Diseases: A Scoping Review. Pediatr Rheumatol Online J 2022, 20, 67. [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N Engl J Med 2017, 377, 1119–1131. [CrossRef]
- Hansson, G.K. Inflammation and Atherosclerosis: The End of a Controversy. Circulation 2017, 136, 1875–1877. [CrossRef]
- Kugiyama, K.; Ota, Y.; Sugiyama, S.; Kawano, H.; Doi, H.; Soejima, H.; Miyamoto, S.; Ogawa, H.; Takazoe, K.; Yasue, H. Prognostic Value of Plasma Levels of Secretory Type II Phospholipase A2 in Patients with Unstable Angina Pectoris. Am J Cardiol 2000, 86, 718–722. [CrossRef]
- Mallat, Z.; Lambeau, G.; Tedgui, A. Lipoprotein-Associated and Secreted Phospholipases A₂ in Cardiovascular Disease: Roles as Biological Effectors and Biomarkers. Circulation 2010, 122, 2183–2200. [CrossRef]
- Fras, Z.; Tršan, J.; Banach, M. On the Present and Future Role of Lp-PLA2 in Atherosclerosis-Related Cardiovascular Risk Prediction and Management. Arch Med Sci 2021, 17, 954–964. [CrossRef]
- Nicholls, S.J.; Cavender, M.A.; Kastelein, J.J.P.; Schwartz, G.; Waters, D.D.; Rosenson, R.S.; Bash, D.; Hislop, C. Inhibition of Secretory Phospholipase A2 in Patients with Acute Coronary Syndromes: Rationale and Design of the Vascular Inflammation Suppression to Treat Acute Coronary Syndrome for 16 Weeks (VISTA-16) Trial. Cardiovasc Drugs Ther 2012, 26, 71–75. [CrossRef]
- Nicholls, S.J.; Kastelein, J.J.P.; Schwartz, G.G.; Bash, D.; Rosenson, R.S.; Cavender, M.A.; Brennan, D.M.; Koenig, W.; Jukema, J.W.; Nambi, V.; et al. Varespladib and Cardiovascular Events in Patients With an Acute Coronary Syndrome: The VISTA-16 Randomized Clinical Trial. JAMA 2014, 311, 252. [CrossRef]
- Mani, P.; Puri, R.; Schwartz, G.G.; Nissen, S.E.; Shao, M.; Kastelein, J.J.P.; Menon, V.; Lincoff, A.M.; Nicholls, S.J. Association of Initial and Serial C-Reactive Protein Levels With Adverse Cardiovascular Events and Death After Acute Coronary Syndrome: A Secondary Analysis of the VISTA-16 Trial. JAMA Cardiol 2019, 4, 314. [CrossRef]
- Denise Martin, E.; De Nicola, G.F.; Marber, M.S. New Therapeutic Targets in Cardiology: P38 Alpha Mitogen-Activated Protein Kinase for Ischemic Heart Disease. Circulation 2012, 126, 357–368. [CrossRef]
- Seeger, F.H.; Sedding, D.; Langheinrich, A.C.; Haendeler, J.; Zeiher, A.M.; Dimmeler, S. Inhibition of the P38 MAP Kinase in Vivo Improves Number and Functional Activity of Vasculogenic Cells and Reduces Atherosclerotic Disease Progression. Basic Res Cardiol 2010, 105, 389–397. [CrossRef]
- Muslin, A.J. MAPK Signaling in Cardiovascular Health and Disease: Molecular Mechanisms and Therapeutic Targets. Clin Sci (Lond) 2008, 115, 203–218. [CrossRef]
- Clerk, A.; Sugden, P.H. Inflame My Heart (by P38-MAPK). Circ Res 2006, 99, 455–458. [CrossRef]
- Newby, L.K.; Marber, M.S.; Melloni, C.; Sarov-Blat, L.; Aberle, L.H.; Aylward, P.E.; Cai, G.; de Winter, R.J.; Hamm, C.W.; Heitner, J.F.; et al. Losmapimod, a Novel P38 Mitogen-Activated Protein Kinase Inhibitor, in Non-ST-Segment Elevation Myocardial Infarction: A Randomised Phase 2 Trial. Lancet 2014, 384, 1187–1195. [CrossRef]
- O’Donoghue, M.L.; Glaser, R.; Cavender, M.A.; Aylward, P.E.; Bonaca, M.P.; Budaj, A.; Davies, R.Y.; Dellborg, M.; Fox, K.A.A.; Gutierrez, J.A.T.; et al. Effect of Losmapimod on Cardiovascular Outcomes in Patients Hospitalized With Acute Myocardial Infarction: A Randomized Clinical Trial. JAMA 2016, 315, 1591. [CrossRef]
- Cavender, M.A.; O’Donoghue, M.L.; Abbate, A.; Aylward, P.; Fox, K.A.; Glaser, R.X.; Park, J.-G.; Lopez-Sendon, J.; Steg, P.G.; Sabatine, M.S.; et al. Inhibition of P38 MAP Kinase in Patients with ST-Elevation Myocardial Infarction - Findings from the LATITUDE-TIMI 60 Trial. Am Heart J 2022, 243, 147–157. [CrossRef]
- Jabor, B.; Choi, H.; Ruel, I.; Hafiane, A.; Mourad, W.; Genest, J. Lipoprotein-Associated Phospholipase A(2) (Lp-PLA(2)) in Acute Coronary Syndrome: Relationship with Low-Density Lipoprotein Cholesterol. Can J Cardiol 2013, 29, 1679–1686. [CrossRef]
- Johnson, J.L.; Shi, Y.; Snipes, R.; Janmohamed, S.; Rolfe, T.E.; Davis, B.; Postle, A.; Macphee, C.H. Effect of Darapladib Treatment on Endarterectomy Carotid Plaque Lipoprotein-Associated Phospholipase A2 Activity: A Randomized, Controlled Trial. PLoS One 2014, 9, e89034. [CrossRef]
- STABILITY Investigators; White, H.D.; Held, C.; Stewart, R.; Tarka, E.; Brown, R.; Davies, R.Y.; Budaj, A.; Harrington, R.A.; Steg, P.G.; et al. Darapladib for Preventing Ischemic Events in Stable Coronary Heart Disease. N Engl J Med 2014, 370, 1702–1711. [CrossRef]
- O’Donoghue, M.L.; Braunwald, E.; White, H.D.; Serruys, P.; Steg, Ph.G.; Hochman, J.; Maggioni, A.P.; Bode, C.; Weaver, D.; Johnson, J.L.; et al. Study Design and Rationale for the Stabilization of pLaques usIng Darapladib—Thrombolysis in Myocardial Infarction (SOLID-TIMI 52) Trial in Patients after an Acute Coronary Syndrome. American Heart Journal 2011, 162, 613-619.e1. [CrossRef]
- O’Donoghue, M.L.; Braunwald, E.; White, H.D.; Steen, D.P.; Lukas, M.A.; Tarka, E.; Steg, P.G.; Hochman, J.S.; Bode, C.; Maggioni, A.P.; et al. Effect of Darapladib on Major Coronary Events After an Acute Coronary Syndrome: The SOLID-TIMI 52 Randomized Clinical Trial. JAMA 2014, 312, 1006. [CrossRef]
- Ridker, P.M.; Libby, P.; MacFadyen, J.G.; Thuren, T.; Ballantyne, C.; Fonseca, F.; Koenig, W.; Shimokawa, H.; Everett, B.M.; Glynn, R.J. Modulation of the Interleukin-6 Signalling Pathway and Incidence Rates of Atherosclerotic Events and All-Cause Mortality: Analyses from the Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS). Eur Heart J 2018, 39, 3499–3507. [CrossRef]
- Alter, C.; Henseler, A.-S.; Owenier, C.; Hesse, J.; Ding, Z.; Lautwein, T.; Bahr, J.; Hayat, S.; Kramann, R.; Kostenis, E.; et al. IL-6 in the Infarcted Heart Is Preferentially Formed by Fibroblasts and Modulated by Purinergic Signaling. J Clin Invest 133, e163799. [CrossRef]
- Anstensrud, A.K.; Woxholt, S.; Sharma, K.; Broch, K.; Bendz, B.; Aakhus, S.; Ueland, T.; Amundsen, B.H.; Damås, J.K.; Hopp, E.; et al. Rationale for the ASSAIL-MI-Trial: A Randomised Controlled Trial Designed to Assess the Effect of Tocilizumab on Myocardial Salvage in Patients with Acute ST-Elevation Myocardial Infarction (STEMI). Open Heart 2019, 6, e001108. [CrossRef]
- Broch, K.; Anstensrud, A.K.; Woxholt, S.; Sharma, K.; Tøllefsen, I.M.; Bendz, B.; Aakhus, S.; Ueland, T.; Amundsen, B.H.; Damås, J.K.; et al. Randomized Trial of Interleukin-6 Receptor Inhibition in Patients With Acute ST-Segment Elevation Myocardial Infarction. Journal of the American College of Cardiology 2021, 77, 1845–1855. [CrossRef]
- Tardif, J.-C.; Tanguay, J.-F.; Wright, S.R.; Duchatelle, V.; Petroni, T.; Grégoire, J.C.; Ibrahim, R.; Heinonen, T.M.; Robb, S.; Bertrand, O.F.; et al. Effects of the P-Selectin Antagonist Inclacumab on Myocardial Damage after Percutaneous Coronary Intervention for Non-ST-Segment Elevation Myocardial Infarction: Results of the SELECT-ACS Trial. J Am Coll Cardiol 2013, 61, 2048–2055. [CrossRef]
- Blann, A.D.; Nadar, S.K.; Lip, G.Y.H. The Adhesion Molecule P-Selectin and Cardiovascular Disease. Eur Heart J 2003, 24, 2166–2179. [CrossRef]
- Tanguay, J.-F.; Geoffroy, P.; Sirois, M.G.; Libersan, D.; Kumar, A.; Schaub, R.G.; Merhi, Y. Prevention of In-Stent Restenosis via Reduction of Thrombo-Inflammatory Reactions with Recombinant P-Selectin Glycoprotein Ligand-1. Thromb Haemost 2004, 91, 1186–1193. [CrossRef]
- Stähli, B.E.; Gebhard, C.; Duchatelle, V.; Cournoyer, D.; Petroni, T.; Tanguay, J.-F.; Robb, S.; Mann, J.; Guertin, M.-C.; Wright, R.S.; et al. Effects of the P-Selectin Antagonist Inclacumab on Myocardial Damage After Percutaneous Coronary Intervention According to Timing of Infusion: Insights From the SELECT-ACS Trial. J Am Heart Assoc 2016, 5, e004255. [CrossRef]
- Tardif, J.-C.; Kouz, S.; Waters, D.D.; Bertrand, O.F.; Diaz, R.; Maggioni, A.P.; Pinto, F.J.; Ibrahim, R.; Gamra, H.; Kiwan, G.S.; et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. New England Journal of Medicine 2019, 381, 2497–2505. [CrossRef]
- Leung, Y.Y.; Yao Hui, L.L.; Kraus, V.B. Colchicine--Update on Mechanisms of Action and Therapeutic Uses. Semin Arthritis Rheum 2015, 45, 341–350. [CrossRef]
- Bouabdallaoui, N.; Tardif, J.-C.; Waters, D.D.; Pinto, F.J.; Maggioni, A.P.; Diaz, R.; Berry, C.; Koenig, W.; Lopez-Sendon, J.; Gamra, H.; et al. Time-to-Treatment Initiation of Colchicine and Cardiovascular Outcomes after Myocardial Infarction in the Colchicine Cardiovascular Outcomes Trial (COLCOT). Eur Heart J 2020, 41, 4092–4099. [CrossRef]
- Nidorf, S.M.; Eikelboom, J.W.; Budgeon, C.A.; Thompson, P.L. Low-Dose Colchicine for Secondary Prevention of Cardiovascular Disease. J Am Coll Cardiol 2013, 61, 404–410. [CrossRef]
- Nidorf, S.M.; Fiolet, A.T.L.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.J.; Bax, W.A.; Budgeon, C.A.; Tijssen, J.G.P.; Mosterd, A.; Cornel, J.H.; et al. The Effect of Low-Dose Colchicine in Patients with Stable Coronary Artery Disease: The LoDoCo2 Trial Rationale, Design, and Baseline Characteristics. Am Heart J 2019, 218, 46–56. [CrossRef]
- Nidorf, S.M.; Fiolet, A.T.L.; Mosterd, A.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.J.; The, S.H.K.; Xu, X.-F.; Ireland, M.A.; Lenderink, T.; et al. Colchicine in Patients with Chronic Coronary Disease. N Engl J Med 2020, 383, 1838–1847. [CrossRef]
- Bouabdallaoui, N.; Blondeau, L.; Tardif, J.-C. Lessons from COLCOT and LoDoCo2: Colchicine for Secondary Prevention in Coronary Artery Disease. Eur Heart J 2021, 42, 2800–2801. [CrossRef]
- Tong, D.C.; Quinn, S.; Nasis, A.; Hiew, C.; Roberts-Thomson, P.; Adams, H.; Sriamareswaran, R.; Htun, N.M.; Wilson, W.; Stub, D.; et al. Colchicine in Patients With Acute Coronary Syndrome: The Australian COPS Randomized Clinical Trial. Circulation 2020, 142, 1890–1900. [CrossRef]
- Everett, B.M.; Pradhan, A.D.; Solomon, D.H.; Paynter, N.; Macfadyen, J.; Zaharris, E.; Gupta, M.; Clearfield, M.; Libby, P.; Hasan, A.A.K.; et al. Rationale and Design of the Cardiovascular Inflammation Reduction Trial: A Test of the Inflammatory Hypothesis of Atherothrombosis. Am Heart J 2013, 166, 199-207.e15. [CrossRef]
- Ridker, P.M.; Everett, B.M.; Pradhan, A.; MacFadyen, J.G.; Solomon, D.H.; Zaharris, E.; Mam, V.; Hasan, A.; Rosenberg, Y.; Iturriaga, E.; et al. Low-Dose Methotrexate for the Prevention of Atherosclerotic Events. N Engl J Med 2019, 380, 752–762. [CrossRef]
- AIM-HIGH Investigators; Boden, W.E.; Probstfield, J.L.; Anderson, T.; Chaitman, B.R.; Desvignes-Nickens, P.; Koprowicz, K.; McBride, R.; Teo, K.; Weintraub, W. Niacin in Patients with Low HDL Cholesterol Levels Receiving Intensive Statin Therapy. N Engl J Med 2011, 365, 2255–2267. [CrossRef]
- Guyton, J.R.; Slee, A.E.; Anderson, T.; Fleg, J.L.; Goldberg, R.B.; Kashyap, M.L.; Marcovina, S.M.; Nash, S.D.; O’Brien, K.D.; Weintraub, W.S.; et al. Relationship of Lipoproteins to Cardiovascular Events: The AIM-HIGH Trial (Atherothrombosis Intervention in Metabolic Syndrome With Low HDL/High Triglycerides and Impact on Global Health Outcomes). J Am Coll Cardiol 2013, 62, 1580–1584. [CrossRef]
- Weisman, A.; Tomlinson, G.A.; Lipscombe, L.L.; Perkins, B.A.; Hawker, G.A. Association between Allopurinol and Cardiovascular Outcomes and All-Cause Mortality in Diabetes: A Retrospective, Population-Based Cohort Study. Diabetes Obes Metab 2019, 21, 1322–1329. [CrossRef]
- Lai, S.-W.; Lin, C.-L.; Liao, K.-F. Case-Control Study Examining the Association between Allopurinol Use and Ischemic Cerebrovascular Disease. J Investig Med 2019, 67, 48–51. [CrossRef]
- Ju, C.; Lai, R.W.C.; Li, K.H.C.; Hung, J.K.F.; Lai, J.C.L.; Ho, J.; Liu, Y.; Tsoi, M.F.; Liu, T.; Cheung, B.M.Y.; et al. Comparative Cardiovascular Risk in Users versus Non-Users of Xanthine Oxidase Inhibitors and Febuxostat versus Allopurinol Users. Rheumatology (Oxford) 2020, 59, 2340–2349. [CrossRef]
- George, J.; Carr, E.; Davies, J.; Belch, J.J.F.; Struthers, A. High-Dose Allopurinol Improves Endothelial Function by Profoundly Reducing Vascular Oxidative Stress and Not by Lowering Uric Acid. Circulation 2006, 114, 2508–2516. [CrossRef]
- Rajendra, N.S.; Ireland, S.; George, J.; Belch, J.J.F.; Lang, C.C.; Struthers, A.D. Mechanistic Insights into the Therapeutic Use of High-Dose Allopurinol in Angina Pectoris. J Am Coll Cardiol 2011, 58, 820–828. [CrossRef]
- Mackenzie, I.S.; Hawkey, C.J.; Ford, I.; Greenlaw, N.; Pigazzani, F.; Rogers, A.; Struthers, A.D.; Begg, A.G.; Wei, L.; Avery, A.J.; et al. Allopurinol versus Usual Care in UK Patients with Ischaemic Heart Disease (ALL-HEART): A Multicentre, Prospective, Randomised, Open-Label, Blinded-Endpoint Trial. Lancet 2022, 400, 1195–1205. [CrossRef]
- Ridker, P.M.; MacFadyen, J.G.; Everett, B.M.; Libby, P.; Thuren, T.; Glynn, R.J.; Ridker, P.M.; MacFadyen, J.G.; Everett, B.M.; Libby, P.; et al. Relationship of C-Reactive Protein Reduction to Cardiovascular Event Reduction Following Treatment with Canakinumab: A Secondary Analysis from the CANTOS Randomised Controlled Trial. The Lancet 2018, 391, 319–328. [CrossRef]
- Ridker, P.M. From CANTOS to CIRT to COLCOT to Clinic: Will All Atherosclerosis Patients Soon Be Treated With Combination Lipid-Lowering and Inflammation-Inhibiting Agents? Circulation 2020, 141, 787–789. [CrossRef]
- Hemkens, L.G.; Ewald, H.; Gloy, V.L.; Arpagaus, A.; Olu, K.K.; Nidorf, M.; Glinz, D.; Nordmann, A.J.; Briel, M. Colchicine for Prevention of Cardiovascular Events. Cochrane Database Syst Rev 2016, 2016, CD011047. [CrossRef]
- Nelson, K.; Fuster, V.; Ridker, P.M. Low-Dose Colchicine for Secondary Prevention of Coronary Artery Disease: JACC Review Topic of the Week. J Am Coll Cardiol 2023, 82, 648–660. [CrossRef]
- Samuel, M.; Tardif, J.-C.; Bouabdallaoui, N.; Khairy, P.; Dubé, M.-P.; Blondeau, L.; Guertin, M.-C. Colchicine for Secondary Prevention of Cardiovascular Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Can J Cardiol 2021, 37, 776–785. [CrossRef]
- Sun, M.; Dubé, M.-P.; Hennessy, T.; Schultz, C.J.; Barhdadi, A.; Rhainds, D.; Hillis, G.S.; Tardif, J.-C. Low-Dose Colchicine and High-Sensitivity C-Reactive Protein after Myocardial Infarction: A Combined Analysis Using Individual Patient Data from the COLCOT and LoDoCo-MI Studies. Int J Cardiol 2022, 363, 20–22. [CrossRef]
- Mitsis, A.; Avraamides, P.; Lakoumentas, J.; Kyriakou, M.; Sokratous, S.; Karmioti, G.; Drakomathioulakis, M.; Theodoropoulos, K.C.; Nasoufidou, A.; Evangeliou, A.; et al. Role of Inflammation Following an Acute Myocardial Infarction: Design of INFINITY. Biomark Med 2023, 17, 971–981. [CrossRef]
- Malick, W.A.; Goonewardena, S.N.; Koenig, W.; Rosenson, R.S. Clinical Trial Design for Lipoprotein(a)-Lowering Therapies: JACC Focus Seminar 2/3. J Am Coll Cardiol 2023, 81, 1633–1645. [CrossRef]
- Distler, O.; Ludwig, R.J.; Niemann, S.; Riemekasten, G.; Schreiber, S. Editorial: Precision Medicine in Chronic Inflammation. Front Immunol 2021, 12, 770462. [CrossRef]
- West, H.W.; Dangas, K.; Antoniades, C. Advances in Clinical Imaging of Vascular Inflammation: A State-of-the-Art Review. JACC: Basic to Translational Science 2023. [CrossRef]
- Stanke-Labesque, F.; Gautier-Veyret, E.; Chhun, S.; Guilhaumou, R. Inflammation Is a Major Regulator of Drug Metabolizing Enzymes and Transporters: Consequences for the Personalization of Drug Treatment. Pharmacol Ther 2020, 215, 107627. [CrossRef]
- Vilne, B.; Ķibilds, J.; Siksna, I.; Lazda, I.; Valciņa, O.; Krūmiņa, A. Could Artificial Intelligence/Machine Learning and Inclusion of Diet-Gut Microbiome Interactions Improve Disease Risk Prediction? Case Study: Coronary Artery Disease. Front Microbiol 2022, 13, 627892. [CrossRef]
- Gupta, A.; Slater, J.J.; Boyne, D.; Mitsakakis, N.; Béliveau, A.; Druzdzel, M.J.; Brenner, D.R.; Hussain, S.; Arora, P. Probabilistic Graphical Modeling for Estimating Risk of Coronary Artery Disease: Applications of a Flexible Machine-Learning Method. Med Decis Making 2019, 39, 1032–1044. [CrossRef]
- Litman, T. Personalized Medicine—Concepts, Technologies, and Applications in Inflammatory Skin Diseases. APMIS 2019, 127, 386–424. [CrossRef]
- Charo, I.F.; Taub, R. Anti-Inflammatory Therapeutics for the Treatment of Atherosclerosis. Nat Rev Drug Discov 2011, 10, 365–376. [CrossRef]
- Soehnlein, O.; Libby, P. Targeting Inflammation in Atherosclerosis - from Experimental Insights to the Clinic. Nat Rev Drug Discov 2021, 20, 589–610. [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Eur Heart J 2021, 42, 3227–3337. [CrossRef]
- Matter, M.A.; Paneni, F.; Libby, P.; Frantz, S.; Stähli, B.E.; Templin, C.; Mengozzi, A.; Wang, Y.-J.; Kündig, T.M.; Räber, L.; et al. Inflammation in Acute Myocardial Infarction: The Good, the Bad and the Ugly. Eur Heart J 2024, 45, 89–103. [CrossRef]

Table 1.
Approaches to organize and classify anti-inflammatory trials.
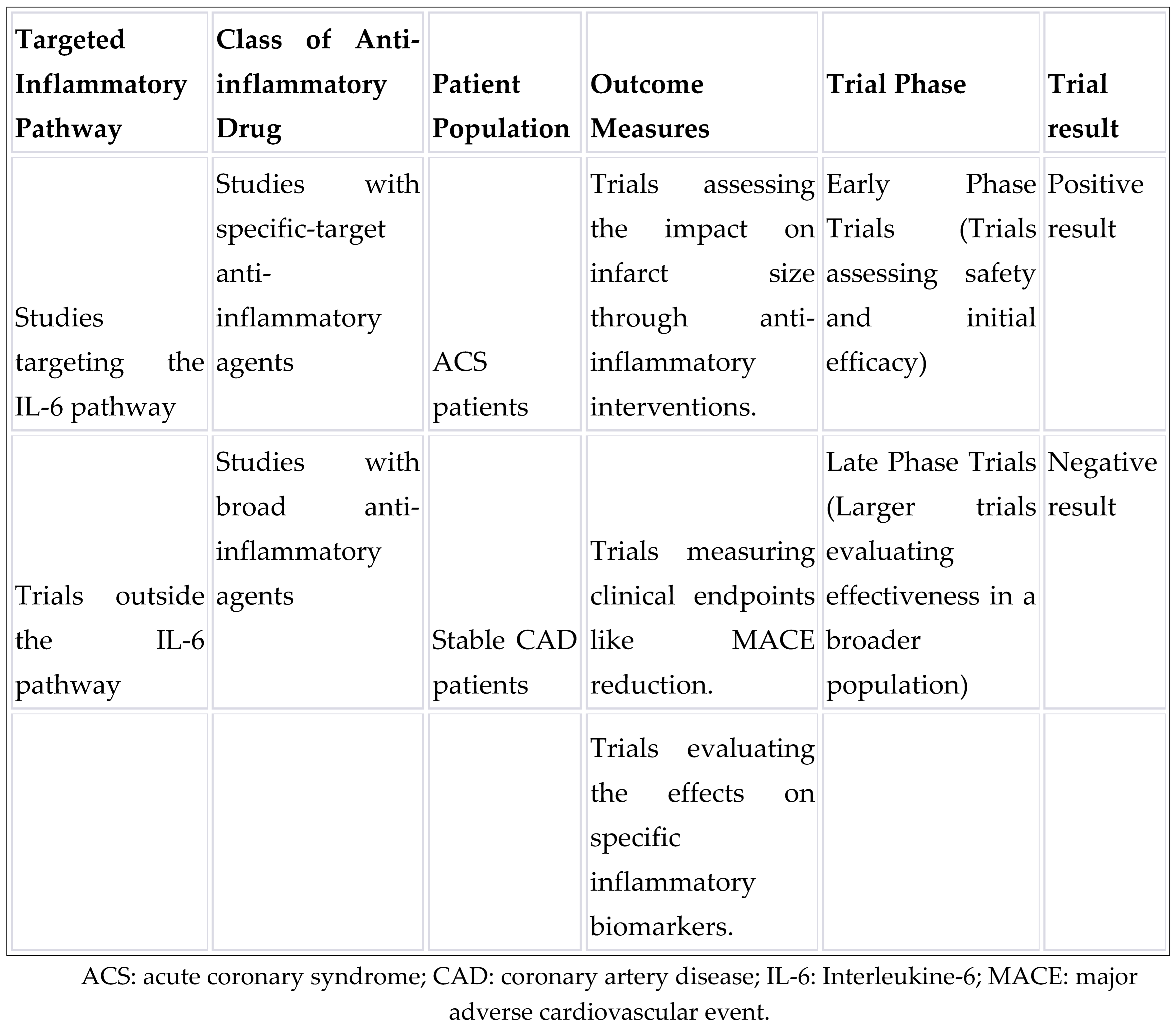
Table 2.
Summary of clinical studies with specific-target anti-inflammatory agents.
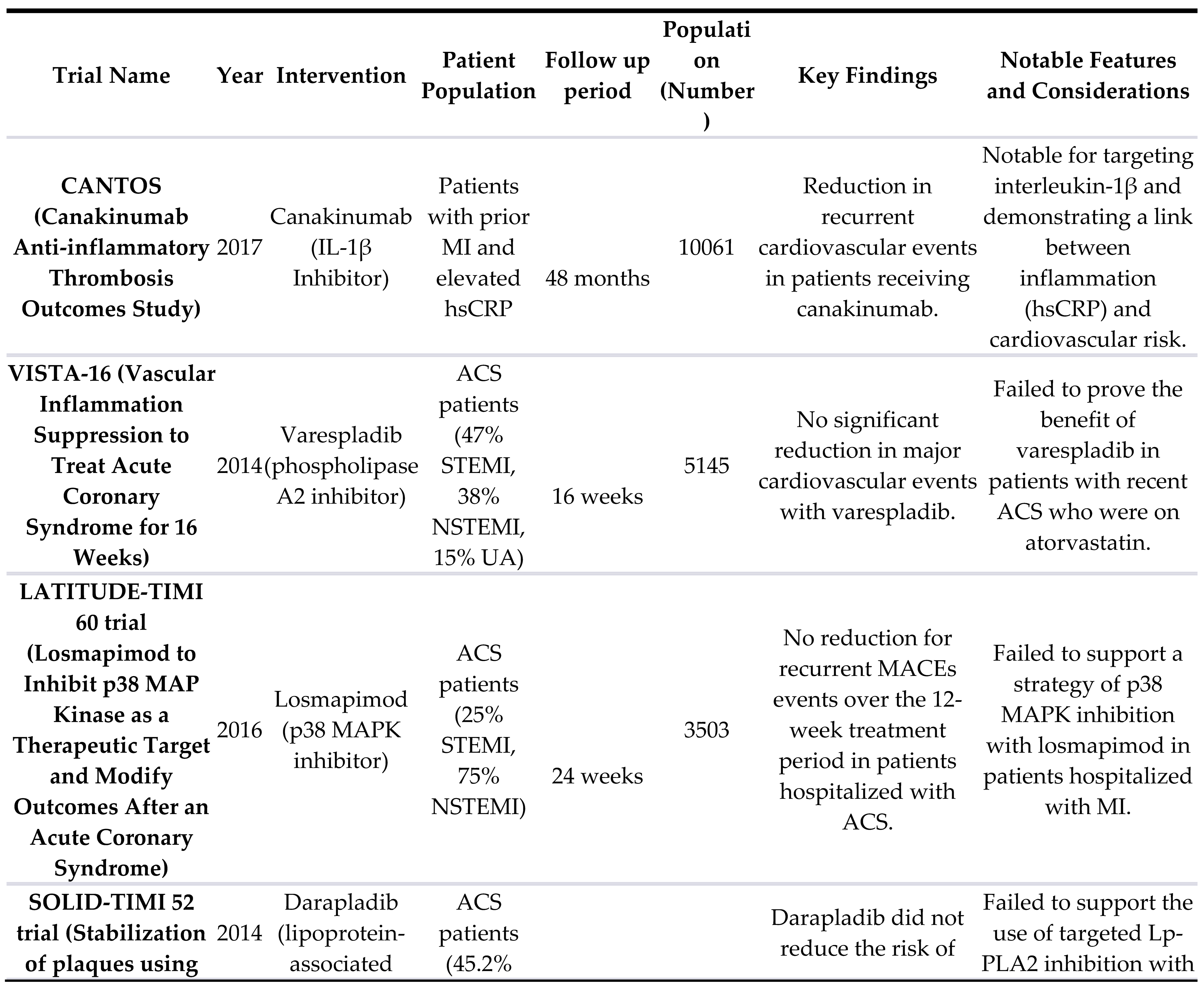
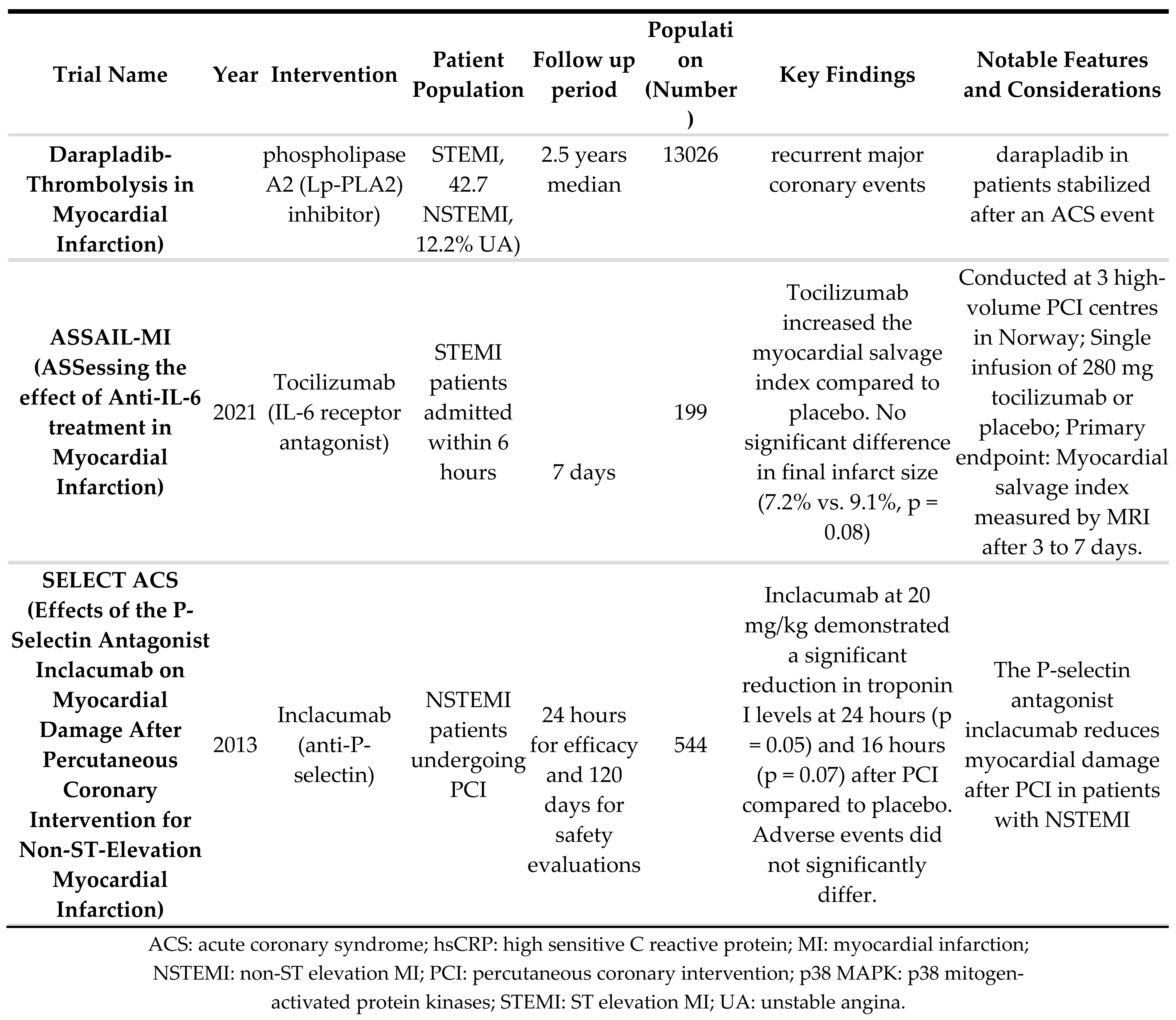
Table 3.
Summary of clinical studies with broad spectrum anti-inflammatory agents.
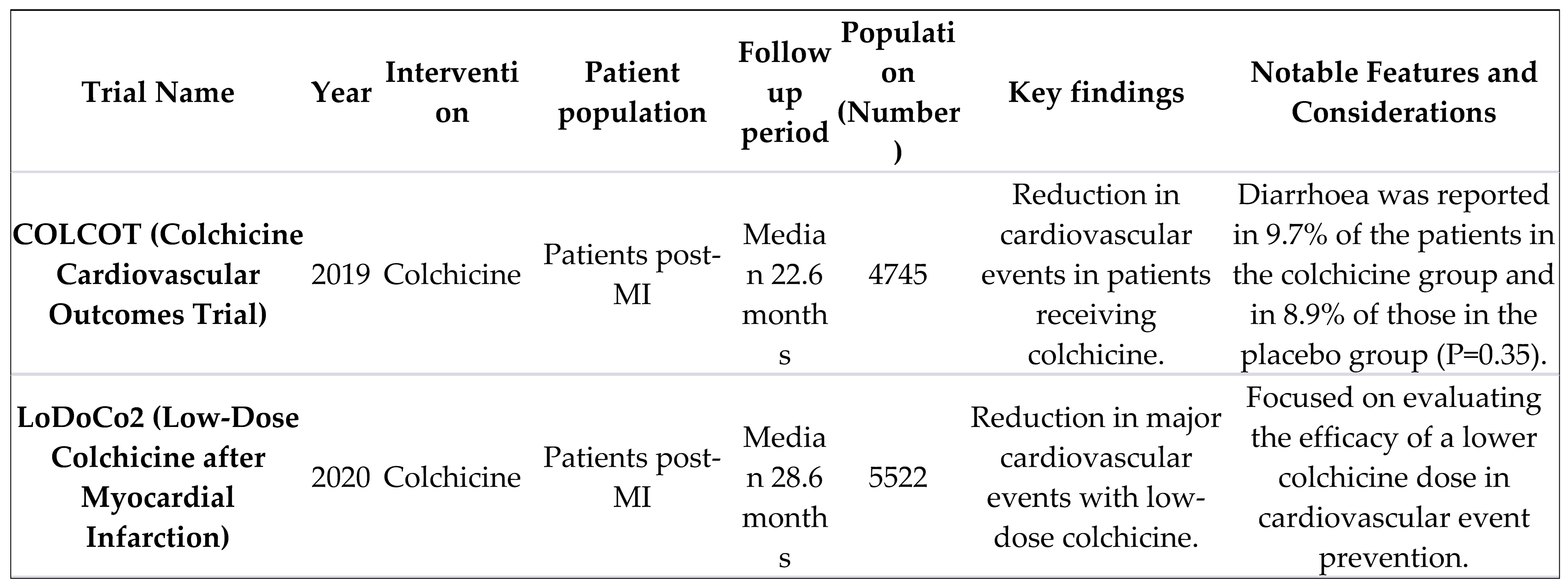
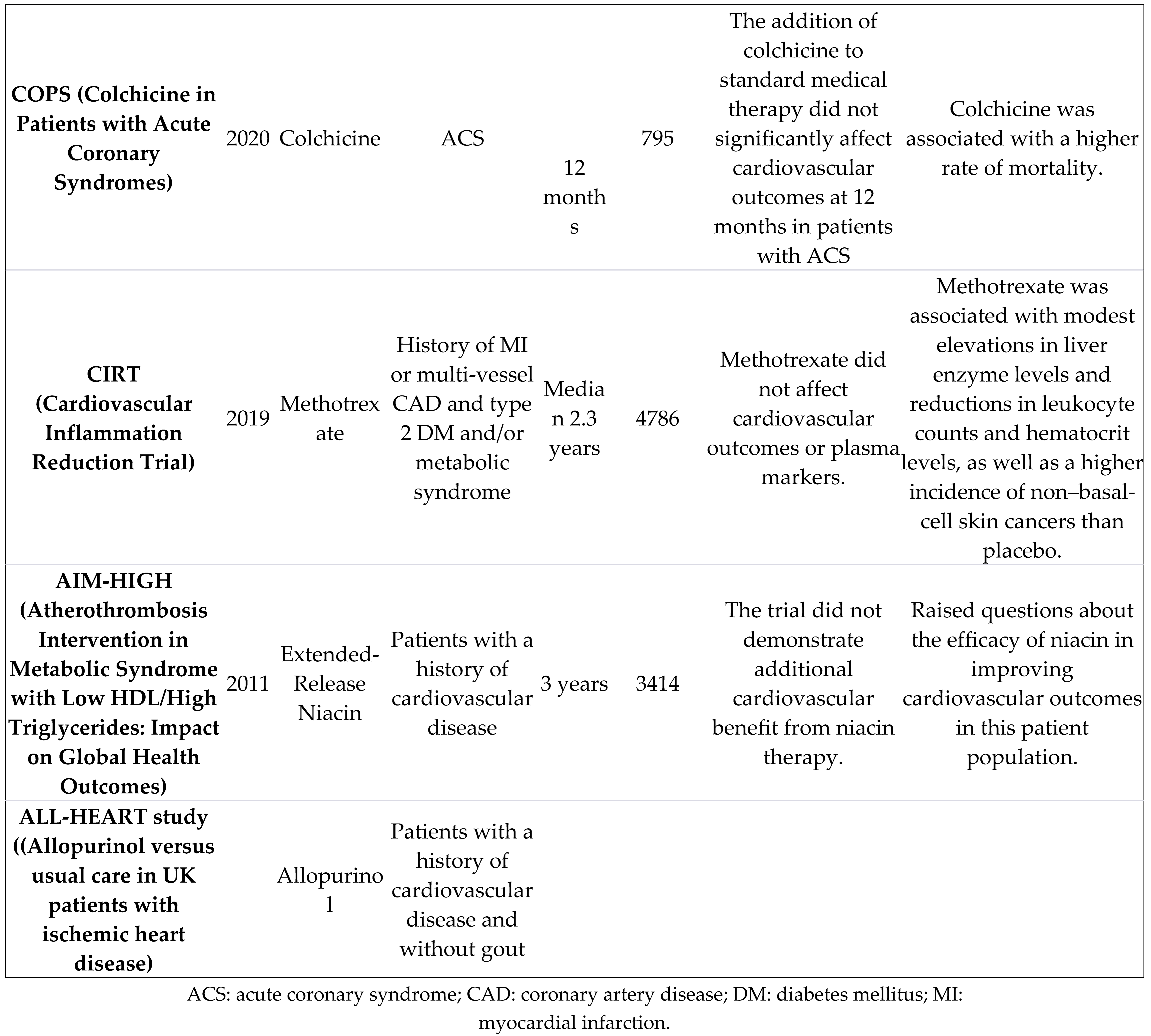
Table 4.
Summary of ongoing clinical studies of treatments targeting inflammation in the context of atherosclerosis and acute myocardial infarction.
Table 4.
Summary of ongoing clinical studies of treatments targeting inflammation in the context of atherosclerosis and acute myocardial infarction.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



