Submitted:
26 February 2024
Posted:
28 February 2024
You are already at the latest version
Abstract
Background: Endoscopic sphincterotomy (EST) has been employed for the endoscopic treatment of common bile duct stones (CBDSs), and a high success rate of stone removal has been reported. However, EST is associated with the risk of bleeding, perforation, and sphincter of Oddi function disruption. To avoid these risks, endoscopic papillary balloon dilation (EPBD) is an option for CBDS. Sphincter of Oddi function preservation decreases long-term biliary infection and gallstone recurrence. EPBD may have advantages in children who require a long follow-up. However, there have been few reports on pediatric cases, particularly in infants.
Methods: From September 2017 to December 2023, we performed EPBD for four pediatric CBDSs. The patients were aged from 5 months to 8 years; including two infants aged 5 and 6 months. Furthermore, we reviewed the stone removal rate and complications of 545 ESTs performed at high-volume centers and 13 EPBD-reported cases in children with CBDSs.
Results: CBDSs of all patients who underwent EPBD in our institution were successfully removed. No bleeding or perforation was noted, and pancreatitis was observed in three patients. In an analysis of 545 ESTs in children, the stone removal rate was high, ranging from 83% to 100% (mean, 96%). The incidence of pancreatitis was 0%–9.6% (mean, 4.4%), and the grade of pancreatitis was almost mild. The bleeding frequency was 1.3%–5.4% (mean, 2.7%). According to the grade of bleeding, seven and four cases were mild (64%) and moderate (36%), respectively, Compared with adult cases who underwent EST, the frequency of pancreatitis and bleeding was almost similar in children.; however once bleeding occur, it has a higher risk of leading to blood transfusion in children. Stone removal by EPBD in children was 100% successful. All complications were pancreatitis, and its frequency was 46% (6/13 patients, including five mild cases and one moderate case), which is higher than that of EST and adult cases who underwent EPBD. In most children with pancreatitis, pancreatic enzyme levels returned to normal within 2–3 days following EPBD, and no severe cases caused by EPBD were reported.
Conclusions: CBDS removal by EPBD in children has a high success rate with very low risk of bleeding and perforation. Although pancreatitis frequently occurs, most cases are mild. Sphincter of Oddi function preservation by EPBD is expected to prevent long-term stone recurrence and biliary tract infection, and EPBD is considered an effective method for CBDS removal in children.
Keywords:
endoscopic papillary balloon dilation
; common bile duct stone
; choledocholithiasis
; children
; endoscopic retrograde cholangiopancreatography
1. Introduction
Gallbladder stones (GBSs) in children are less common than in adults, with a reported prevalence of 0.13%–0.2% in Italy [1], 0.13% in Japan [2], and 1.9% in the Netherlands [3]. Recently, the prevalence of GBS has increased from 1.9% to 4% in children [4]. In infants, the most common causes of cholelithiasis are preterm birth, total parenteral nutrition, and abdominal surgery, whereas in children, the main causes are hemolytic disease and hereditary erythrocytosis [4,5]. Obesity and oral contraceptive use have been recently identified as risk factors in adolescents [5]. More than 80% of adults with GBSs are asymptomatic [6]. In contrast, 17%–50% of children are symptomatic [6,7,8,9]. Common bile duct stones (CBDSs) require urgent treatment. Surgical treatment is invasive, and endoscopic sphincterotomy (EST) has been employed to remove CBDSs in children [7,8,9,10,11,12,13,14,15,16,17]. However, as EST performs incision of the main papilla, there are risks of perforation and bleeding. Moreover, sphincter of Oddi function disruption could cause bacterial invasion and growth in the bile ducts and reflux of digestive juices [18,19,20], which are believed to be factors in bile duct stone recurrence [21,22,23].
In contrast, endoscopic papillary balloon dilation (EPBD) has lower risk of bleeding and perforation [22,23]; in addition, it preserves sphincter of Oddi function [24,25]. In children, the sphincter of Oddi function preservation is desirable owing to the long clinical course required. Therefore, we previously performed EST for CBDSs, and since September 2017, we have selected EPBD to preserve the sphincter of Oddi function. Only a few studies of EPBD for pediatric CBDSs have been conducted [26,27,28], especially in infants. In this study, we performed EPBD for stone removal in four children with CBDSs, two of whom were infants. We report our experience with a review of literature on EPBD and EST in children with CBDSs.
2. Materials and Methods
From September 2017 to December 2023, four pediatric CBDSs requiring endoscopic treatment presented to our institution. Their ages ranged from 5 months to 8 years, two of whom were infants aged 5 and 6 months. A 5-month-old girl had no specific medical history and a 6-month-old girl had undergone open heart surgery for cardiac disease. The other two cases were 7- and 8-year-old boys. The CBDSs were 3–4 mm in size and 1–2 in number. The details of these cases are presented in Table 1.
Endoscopic retrograde cholangiopancreatography (ERCP) was performed under general anesthesia using PJF 240 (Olympus, Tokyo, Japan) in infants and TJFQ180 or JF260v (Olympus) in older children. The PJF 240 uses a video system and has a narrow tip diameter of 8.8 mm, making it useful for ERCP in infants. For older children, a balloon catheter with a 4–6-mm diameter and a 30-mm-long balloon was used (ZARA; Century Medical Inc., Tokyo, Japan). The 30-mm-long balloon is sufficiently long to be used for EPBD in infants. Shorter endoscopic papillary balloons are not available in the market. Therefore, we used a percutaneous transluminal coronary angioplasty (PCTA) balloon with the consent of the family for use in infants. The PCTA balloon is available in short balloon lengths. For infants, a catheter with a 3–4-mm diameter and a 15-mm-long balloon (Ryurei; Terumo Inc., Tokyo, Japan) was used. The balloon was inflated for 30 s or 1 min. Following balloon dilatation, the balloon was deflated and inserted into the hepatic duct. To remove the bile stones, the balloon was subsequently reinflated and pulled back into the duodenum. Basket forceps and mechanical lithotripsy tool were not used. Following EPBD, a 4- or 5-Fr endoscopic nasobiliary drainage (ENBD) tube was prophylactically inserted in all patients. The grading of endoscopic complications (pancreatitis and hemorrhage) [29] was classified according to Cotton et al [30]. The Revised Atlanta classification of post-ERCP pancreatitis (PEP) was also used [31]. In this classification, the evaluation of abdominal pain is a criterion. We assumed that determining whether an infant has abdominal pain was difficult; therefore, we used the classification by Cotton et al.
This study was approved by the Ethics Committee of Tokyo Women’s Medical University (approval number: 5728) in accordance with the Declaration of Helsinki of 1964 (revised in 2013).
3. Results
3.1.1 Pateint1: A 6-month-old girl presented with jaundice due to CBDS. She had undergone open heart surgery under cardiopulmonary bypass at the age of 5 months. Her body weight was 5 kg when she underwent EPBD. Her common bile duct was dilated because of impaction of stones up to 9.4 mm in diameter. By EPBD, the bile stones were removed twice using a balloon catheter, and no complications were observed.
3.1.2 Patient2: A 5-month-old girl presented with vomiting. Ultrasonography (US) revealed GBSs and gallbladder wall thickness. She presented with sepsis and urgently underwent gallbladder drainage (Figure 1a). During surgery, one CBDS impacting the distal common duct was observed, and an ENBD tube was inserted (Figure 1b). After recovery from cholecystitis and sepsis, EPBD was performed for CBDSs (Figure 2a,b). As the stone was 3 mm in size, the papilla was dilated by 3 mm in 30 s, and the stone was removed by one balloon pulling. The next day after EPBD, serum lipase levels increased to 1,695 IU/L and returned to normal on the fifth day.
3.1.3 Patient3: An 8-year-old boy with trisomy 13 complained of jaundice and abdominal pain. Computed tomography revealed gallbladder wall swelling and multiple stones in the gallbladder and CBD (Figure 3a). Percutaneous transhepatic gallbladder drainage and ENBD tube insertion were performed for cholangitis and bile stones. After the improvement of cholecystitis, the patient simultaneously underwent laparoscopic cholecystectomy and EPBD. During surgery, 55 small bile stones in the gallbladder and 2 stones in the CBD were observed (Figure 3b). By EPBD, all bile stones were removed twice using a balloon catheter. One day after EPBD, lipase levels increased to 4,999 IU/L but returned to normal on the second day.
3.1.4 Patient4: A 7-year-old boy complained of abdominal pain and vomiting. Blood examination showed pancreatic enzyme level elevation, and US revealed pancreatic swelling. Magnetic resonance cholangiopancreatography showed no abnormality in the pancreaticobiliary system. ERCP showed a relatively long common channel with one stone seen in the lower part of CBD. The stone was successfully removed by EPBD. One day after EBPD, serum lipase levels increased to 1,923 IU/L and returned to normal on the third day.
All cases of CBD removal by EPBD were completed without complications of bleeding or perforation. Post-EPBD follow-up ranged from 2 to 75 (mean, 35) months, with no EPBD-associated complications.
Figure 1. A 5-month-old girl who presented with vomiting and revealed gallbladder and common bile duct stones on ultrasonography.
Figure 2. A 5-month-old girl who presented with vomiting and revealed gallbladder and common bile duct stones on ultrasonography.
Figure 3. An 8-year-old boy complained of gallbladder and common bile duct stones.
4. Discussion
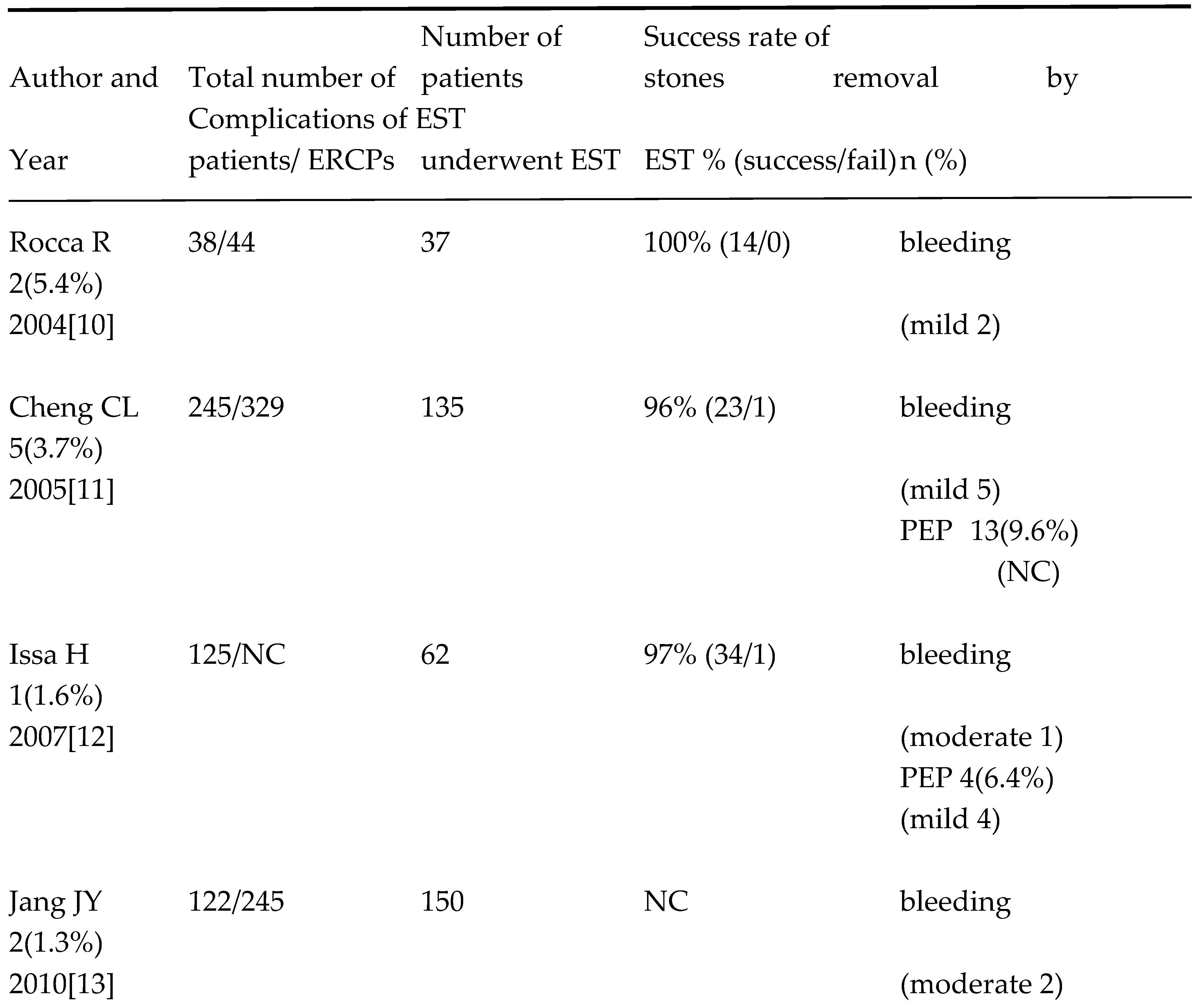
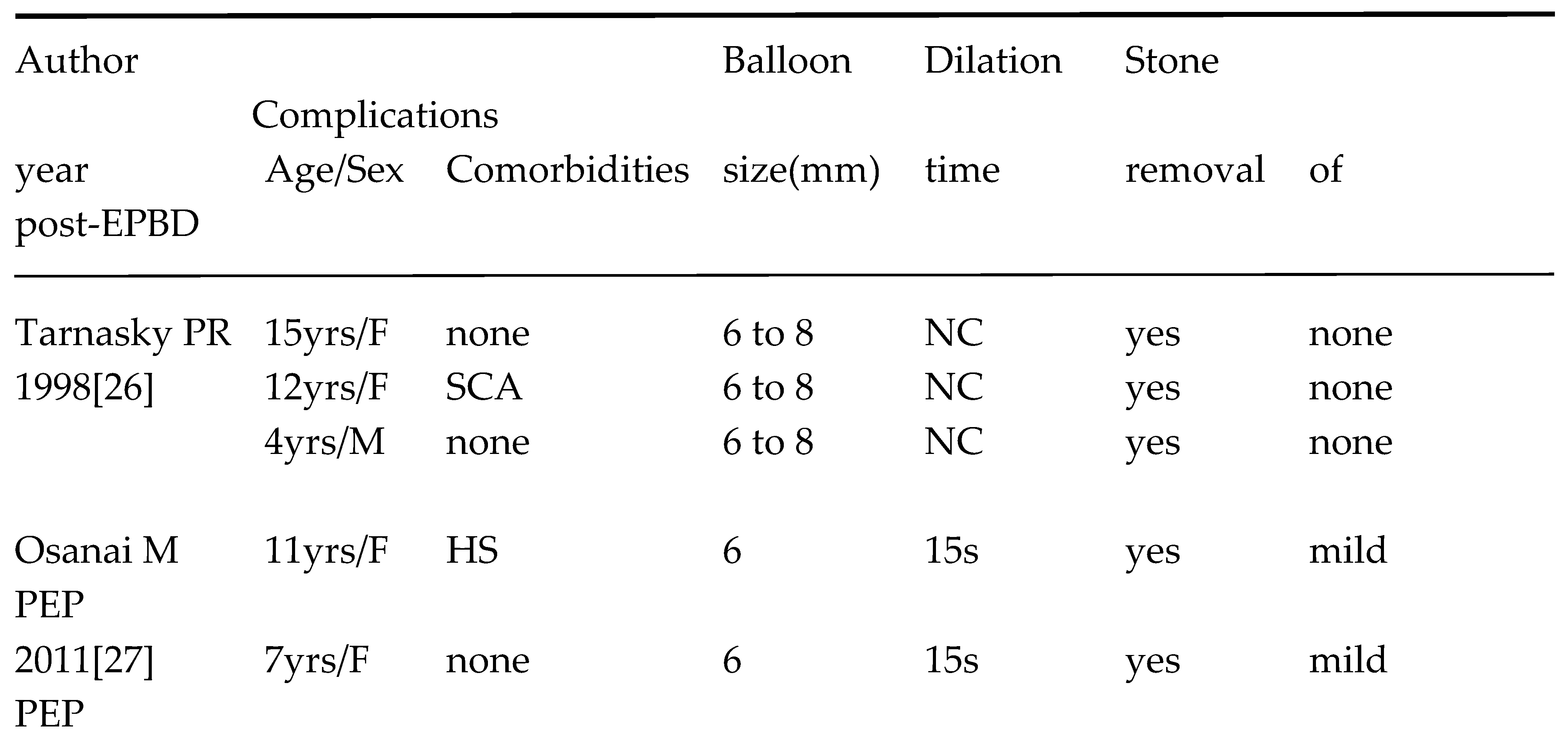
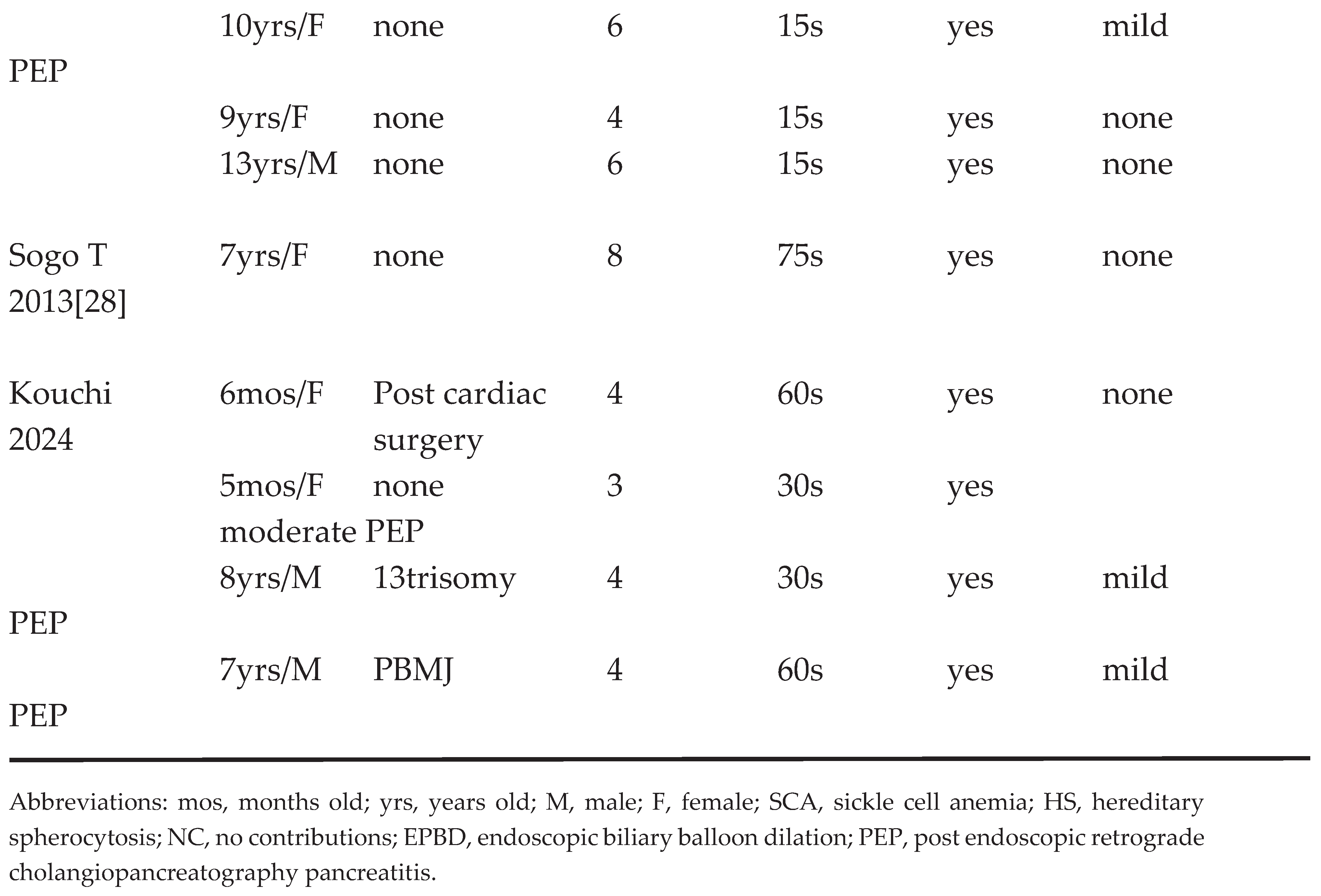
EPBD for CBDSs was first reported in 1982 by Staritz et al [32]. EPBD has the advantages of preserving the function of the sphincter of Oddi and a low risk of hemorrhage and perforation compared with EST [21,22,23]. Yasuda et al [25] compared the basal and maximal pressures and contraction frequencies of the sphincter muscles of the papilla in the EST and EPBD groups at 1 week and 1 year after endoscopic treatment using manometry. Sphincter pressure at 1 week was low in both groups. After 1 year, the EST group showed no recovery in basal or maximal pressure, whereas the EPBD group showed an obvious recovery of both pressures; however, the recovery was lower than the previous value. It is considered that the loss of papillary function causes reflux of digestive fluids and bacteria into the bile ducts [18,19,20], thereby leading to various complications. Several studies have attributed the lower incidence of long-term stone recurrence and cholangitis in the EPBD group compared with that in the EST group to papillary function preservation [21,22,23]. In contrast, the risk of PEP has been reported to be higher than that of EST [21,22,23,33]. Therefore, the European Society of Gastrointestinal Endoscopy (ESGE) clinical guidelines for CDBSs state that EPBD without EST is primarily indicated for patients with abnormalities in coagulation and stones smaller than 8 mm [34]. Children with CBDSs have mainly been treated by EST. Reports of children treated by EST in high-volume centers since 2000 are presented in Table 2 [7,8,9,10,11,12,13,14,15,16,17]. The success rate of stone removal was high, ranging from 83% to 100% (mean, 96%). To the best of our knowledge, the youngest reported case of stone removal by EST is a 3-month-old boy who developed CBDSs following chemotherapy for a malignant tumor [35]. In contrast, only a few reports of EPBD in children less than 15 years of age have been conducted (Table 3) [26,27,28]. This may be due to the high PEP incidence in Europe and the United States, which is why it is not aggressively performed. Although the number of EPBD cases in children is small, the success rate of stone removal was 100%. The PEP incidence by EST at high-volume centers of pediatric facilities is described by dividing the number of PEP cases by the total number of ERCPs [11,12,15,16]. In this study, the percentages were calculated by dividing the number of PEP cases by the number of EST cases performed. This method of calculation is considered to be a more realistic estimate of PEP incidence in children, with rates ranging from 1.3% to 5.4% (mean, 4.4%). According to a meta-analysis of adults, the frequency of PEP ranged from 0% to 18.8% [22,23,36], suggesting that PEP frequency is not much different from that in children. The frequency of bleeding following EST in children ranged from 1.3% to 5.4% (mean, 2.7%), and this frequency was calculated in the same way as for PEP. The frequency of bleeding in adults was approximately 0%–26% (mean, 3.4%) [22,23,36], and the frequency of occurrence was not expected to differ from that in children. In adult cases, grade of bleeding after EST was reported as moderate (45.8%–71%) and severe (25%–29%) [37,38]. Anticoagulants, cirrhosis, and end-stage renal disease were noted as a risk factor for bleeding [38]. However, the grade of post EST bleeding was mostly mild (87%) in average risk adult patients [39]. Generally, the risk factors of post-EST bleeding in children are rare; seven cases of bleeding were mild (64%) and four cases were moderate (36%), indicating a high rate of moderate bleeding. In children, bleeding following EST is associated with a high risk of blood transfusion. Conversely, in EPBD in children [26,27,28], all complications were PEP, with a frequency of 6 of the 13 cases (46%) (five mild cases and one moderate case), which is clearly higher than that of EST. This PEP frequency in children is also higher than that in adults who underwent EPBD [0%–11.3% (mean, 7.0%)] [22,23,36]. Balloon diameter and dilation time have been identified as factors associated with PEP following EPBD [34]. Regarding balloon diameter, a comparison has been made between EPBD and endoscopic papillary large balloon dilation (EPLBD) in adults [40]. The frequency of PEP is lower with EPLBD than with EPBD [41,42]. Even with the use of a small-diameter balloon (3–8 mm), the situation in infants may be similar to that in which EPLBD is performed. The ESGE [34] and the American Society for Gastrointestinal Endoscopy [43] also state that a dilation time longer than 2 min carries less risk of PEP. In contrast, Wang et al. (2021) [44] reported a systematic review and meta-analysis of EPBD according to balloon dilation time. They classified the dilation times into short dilation times of <1 min and long dilation times of >1 min and noted no difference in complications or successful stone removal rates between the short and long dilation times. In children who underwent EPBD [26,27,28], the dilation time was relatively short, ranging from 15 to 75 s. This is believed to be because children have softer tissues than adults, which may have led to the shorter balloon dilation time. Furthermore, we set a short dilation time (30 s) for infants. PEP frequently occurred in children who underwent EPBD, mostly with mild cases, with a rapid increase in pancreatic enzyme levels following EPBD; however, most children had a rapid return to normal range within a few days. No mortality or severe pediatric cases of PEP due to EPBD were reported. Therefore, we supposed that papillary edema rapidly improves owing to soft tissues in children following EPBD.
This study had some limitations. The most significant point was the small number of pediatric EPBD cases, particularly in infants. Only a few studies on pediatric EPBD have been conducted in Europe and the United States, and we need to wait for more cases to be accumulated in the future. Moreover, the balloon dilation time for pediatric EPBD was relatively short. Performing dilatations of 2 min or longer to compare cases will be necessary.
5. Conclusions
Stone removal by EBPD in children is expected to have a high success rate with very low risk of bleeding and perforation. The frequency of PEP is high, with most of them being mild; the posttreatment course is uneventful when post-EBPD management is correctly performed. In children who require a long clinical follow-up after CBDS removal, papillary function preservation is expected to prevent stone recurrence and biliary tract infection and is considered an effective method.
Author Contributions
Conceptualization, Kouchi K.; methodology, Kouchi K.; software, Matsuoka A.; validation, Yoshizawa H., Yabe K. and Fujishiro J.; formal analysis, Nakata C.; investigation, Yabe K. and Yoshizawa H.; resources, Fujishiro J.; data curation, Matsuoka A.; writing—original draft preparation, Kouchi K.; writing—review and editing, Kouchi K.; visualization, Takenouchi A.; supervision, Sugiyama H.; project administration, Kouchi K.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Tokyo Women’s Medical University (approval number: 5728).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data generated or analyzed during this study are available from the corresponding author by request subject to institutional review and a data use agreement.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Palasciano, G.; Portincasa, P.; Vinciguerra, V.; Velardi, A.; Tardi, S.; Baldassarre, G.; Albano, O. Gallstone prevalence and gallbladder volume in children and adolescents: an epidemiological ultrasonographic survey and relationship to body mass index. Am. J. Gastroenterol. 1989, 84, 1378–1382. [Google Scholar] [PubMed]
- Nomura H.; Kashiwagi S.; Hayashi J.; Kajimaya W.; Ikematsu H.; Noguchi A, et al. Prevalence of gallstone disease in general population of Okinawa, Japan. Am J Epidemiol. 1988, 128:598-605. [CrossRef]
- Wesdorp I; Bosman D.; de Graaff A.; Aronson D.; van der Blij F.; Taminiau J. Clinical presentations and predisposing factors of cholelithiasis and sludge in children. J Pediatr Gastroenterol Nutr. 2000, 31,411-7.
- Zdanowicz K.; Daniluk J.; Lebensztejn DM.; Daniluk U. The Etiology of Cholelithiasis in Children and Adolescents-A Literature Review. Int J Mol Sci. 2022, 23, 13376. [CrossRef] [PubMed]
- Koebnick C.; Smith N.; Black MH.; Porter AH.; Richie BA.; Hudson S.; Gililland D.; Jacobsen SJ.; Longstreth GF. Pediatric obesity and gallstone disease. J Pediatr Gastroenterol Nutr. 2012, 55:328-33. [CrossRef]
- Grace, W.A.; Ransohoff, D.F. Natural history of silent gallstone: the innocent gallstone is not a myth. N. Engl. J. Med. 1982, 23, 798–800. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Park, Y.S.; Park, J.H. Cholecystectomy is feasible in children with small-sized or large numbers of gallstones and in those with persistent symptoms despite medical treatment. Pediatr. Gastroenterol. Hepatol. Nutr. 2020, 23, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Bogue, C.O.; Murphy, A.J.; Gerstle, J.T.; Moineddin, R.; Daneman, A. Risk factors, complications, and outcomes of gallstone in children. J. Pediatr. Gastroenterol. Nutr. 2010, 50, 303–308. [Google Scholar] [CrossRef] [PubMed]
- Serdaroglu, F.; Koca, Y.S.; Saltik, F.; Koca, T.; Dereci, S.; Akcam, M.; Akcam, F.Z. Gallstones in childhood: etiology, clinical features, and prognosis. Eur. J. Gastroenterol. Hepatol. 2016, 28, 1468–1472. [Google Scholar] [CrossRef] [PubMed]
- Rocca, R.; Castellino, F.; Dapermo, F.; Masoero, G.; Sostegni, R.; Ercole, E.; et al. Therapeutic ERCP in paediatric patients. Digestive and Liver Disease 2005, 37, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Cheng, C.L.; Fogel, E.L.; Sherman, S.; McHenry, L.; Watkins, J.L.; Croffie, J.M.; et al. Diagnostic and therapeutic endoscopic retrograde cholangiopancreatography in children: a large series report. J. Pediatr. Gastroenterol. Nutr. 2005, 41, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Issa, H.; Al-Haddad, A.; Al-Salem, A.H. Diagnostic and therapeutic ERCP in the pediatric age group. Pediatr. Surg. Int. 2007, 23, 111–116. [Google Scholar] [CrossRef]
- Jang, J.Y.; Yoon, C.H.; Kim, K.M. Endoscopic retrograde cholangiopancreatography in pancreatic and biliary tract disease in Korean children. World J. Gastroenterol. 2010, 28, 490–495. [Google Scholar] [CrossRef]
- Otto AK, Neal MD, Slivka AN, Kane TD. (2011) An appraisal of endoscopic retrograde cholangiopancreatography (ERCP) for pancreaticobiliary disease in children: our institutional experience in 231 cases. Surg Endosc 25:2536-2540. [CrossRef]
- Troendle, D.M.; Barth, B.A. ERCP can be safely and effectively performed by a pediatric gastroenterologist for choledocholithiasis in a pediatric facility. J. Pediatr. Gastroenterol. Nutr. 2013, 57, 655–658. [Google Scholar] [CrossRef] [PubMed]
- Fishman, D.S.; Chumpitazi, B.P.; Raijman, I.; Tsai, C.M.; Smith, E.O.; et al. Endoscopic retrograde cholangiopancreatography for pediatric choledocholithiasis: assessing the need for endoscopic intervention. World J. Gastroenterol. 2016, 8, 425–432. [Google Scholar]
- Keane, M.G.; Kumar, M.; Cieplik, N.; Thorburn, D.; Johnson, G.J.; Webster, G.J.; Chapman, M.H.; Lindley, K.J.; Pereira, S.P. Paediatric pancreaticobiliary endoscopy: a 21-year experience from a tertiary hepatobiliary centre and systematic literature review. BMC Pediatr. 2018, 18, 42. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, M.; Atomi, Y. Does endoscopic sphincterotomy cause prolonged pancreatobiliary reflux? Am J Gastroenterol. 1999, 94, 795–798. [Google Scholar] [CrossRef]
- Gregg, J.A.; Girolami, P.D.; Carr-Locke, D.L. Effects of sphincteroplasty and endoscopic sphincterotomy on the bacteriologic characteristics of the common bile duct. Am. J. Surg. 1985, 149, 668–671. [Google Scholar] [CrossRef] [PubMed]
- Sand, J.; Airo, I.; Hiltunen, K.M.; Mattila, J. Nordback I. Changes in biliary bacteria after endoscopic cholangiography and sphincterotomy. Am. Surg. 1992, 58, 324–328. [Google Scholar]
- Weinberg, B.M.; Shindy, W.; Lo, S. Endoscopic balloon dilatation (sphincteroplasty) versus sphincterotomy for bile duct stones. Review Cochrane Database Syst Rev. 2006, 18, CD004890. [Google Scholar]
- Zhao, H.C.; He, L.; Zhou, D.C.; Geng, X.P.; Pan, F.M. Meta-analysis comparison of endoscopic papillary balloon dilatation and endoscopic sphincteropapillotomy. World J. Gastroenterol. 2013, 19, 3883–3891. [Google Scholar] [CrossRef]
- Sakai, Y.; Tsuyuguchi, T.; Sugiyama, H.; Hayashi, M.; Senoo, J.; Kusakabe, Y.; Yasui, S.; Mikata, R.; Yokosuka, O. Comparison of endoscopic papillary balloon dilatation and endoscopic sphincterotomy for bile duct stones. World J. Gastrointest Endosc. 2016, 8, 395–401. [Google Scholar] [CrossRef]
- Sato, H.; Kodama, T.; Takaaki, J.; Tatsumi, Y.; Maeda, T.; Fujita, S.; Fukui, Y.; Ogasawara, H.; Mitsufuji, S. Endoscopic papillary balloon dilatation may preserve sphincter of Oddi function after common bile duct stone management: evaluation from the viewpoint of endoscopic manometry. Gut. 1997, 41, 541–544. [Google Scholar] [CrossRef]
- Yasuda, I.; Tomita, E.; Enya, M.; Kato, T.; Moriwaki, H. Can endoscopic papillary balloon dilation really preserve sphincter of Oddi function? Gut. 2001, 49, 686–691. [Google Scholar] [CrossRef]
- Tarnasky, P.R.; Tagge, E.P.; Hebra, A.; Othersen, B.; Adams, D.B.; Cunningham, J.T.; Cotton, P.B.; Hawes, R.H. minimally invasive therapy for choledocholithiasis in children. Gastrointest Endosc. 1998, 47, 189–192. [Google Scholar] [CrossRef] [PubMed]
- Osanai, M.; Maguchi, H.; Takahashi, K.; Katanuma, A.; Yane, K.; Kaneko, M.; Hashigo, S.; Katoh, S.; Harada, R.; Katoh, R.; Tanno, S. Safety and long-term outcomes of endoscopic papillary balloon dilation in children with bile duct stones. Gastrointest Endosc. 2011, 73, 619–623. [Google Scholar] [CrossRef]
- Sogo, T.; Kondo, T.; Tsunoda, T.; Murayama, A.; Komatsu, H.; Inui, A.; Fujisawa, T. Endoscopic papillary balloon dilatation for a 7-year-old girl with choledocholithiasis. Pediatr Int. 2013, 55, e1–e3. [Google Scholar] [CrossRef]
- ASGE Standards of Practice Committee. Adverse events associated with ERCP. Gastrointest Endosc. 2017, 85, 32-47.
- Cotton, P.B.; Lehman, G.; Vennes, J.; Geenen, J.E.; Russell, R.C.; Meyers, W.C.; Liguory, C.; Nickl, N. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 1991, 37, 383–393. [Google Scholar] [CrossRef]
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, Tsiotos GG, Vege SS; Acute Pancreatitis Classification Working Group. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013, 62, 102-11. [CrossRef]
- Staritz M, Ewe K, Meyer zum Büschenfelde KH. Endoscopic papillary dilatation, a possible alternative to endoscopic papillotomy. Lancet 1982; 1: 1306-7. [CrossRef]
- Disario JA, Freeman ML, Bjorkman DJ, et al. Endoscopic balloon dilatation compared with sphincterotomy for extraction of bile stones. Gastroenterol 2004; 127: 1291-9. [CrossRef]
- Manes G.; Paspatis G.; Aabakken L.; Anderloni A.; Arvanitakis M.; Ah-Soune P.; Barthet M.; Domagk D.; Dumonceau J-M, Gigot J-F; et al. Endoscopic management of common bile duct stones: European Society of Gastrointestinal Endoscopy (ESGE) guideline. Endoscopy. 2019, 51, 472-491. [CrossRef]
- Lou, Q.; Sun, J.; Zhang, X.; Shen, H. Successful therapeutic ERCP in a 99-day-old child with common bile duct stones: a case report and discussions on the particularities of the ERCP in children. Front Pediatr. 2020, 28, 435. [Google Scholar] [CrossRef] [PubMed]
- Zhao HC, He L, Zhou DC, Geng XP, Pan FM. Meta-analysis comparison of endoscopic papillary balloon dilatation and endoscopic sphincteropapillotomy. World J Gastroenterol. 2013, 19, 3883-91.
- Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher PJ, Moore JP, Fennerty MB, Ryan ME, Shaw MJ, Lande JD, Pheley AM. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 1996, 335:909-18. [CrossRef]
- Dumonceau JM, Kapral C, Aabakken L, Papanikolaou IS, Tringali A, Vanbiervliet G, Beyna T, Dinis-Ribeiro M, Hritz I, Mariani A, Paspatis G, Radaelli F, Lakhtakia S, Veitch AM, van Hooft JE. ERCP-related adverse events: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2020, 52:127-149. [CrossRef]
- Bae SS, Lee DW, Han J, Kim HG. Risk factor of bleeding after endoscopic sphincterotomy in average risk patients. Surg Endosc. 2019, 33:3334-3340. [CrossRef]
- Ersoz, G.; Tekesin, O.; Ozutemiz, A.O.; Gunsar, F. Biliary sphincterotomy plus dilation with a large balloon for bile duct stones that are difficult to extract. Gastrointest Endosc. 2003, 57, 156–159. [Google Scholar] [CrossRef]
- Jang SI, Yun GW, Lee DK. Balloon dilation itself may not be a major determinant of post-endoscopic retrograde cholangiopancreatography pancreatitis. World J Gastroenterol. 2014, 20, 16913-24. [CrossRef]
- Fujisawa, T.; Kagawa, K.; Hisatomi, K.; Kubota, K.; Nakajima, A.; Matsuhashi, N. Is endoscopic papillary balloon dilatation really a risk factor for post-ERCP pancreatitis? World J Gastroenterol. 2016, 22, 5909–5916. [Google Scholar] [CrossRef]
- ASGE Standards of Practice Committee; Buxbaum JL.; Abbas Fehmi SM.; Sultan S.; Fishman DS.; Qumseya BJ.; Cortessis VK.; Schilperoort H.; Kysh L.; Matsuoka L.; Yachimski P.; et al. ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis. Gastrointest Endosc. 2019, 89, 1075-1105. [CrossRef]
- Wang Q, Fu L, Wu T, Ding X. The ballooning time in endoscopic papillary balloon dilation for removal of bile duct stones: A systematic review and meta-analysis. Medicine (Baltimore). 2021, 100:e24735.
Figure 1.
(a) Enhanced computed tomography (CT) showing multiple small gallstones and gallbladder swelling. (b) The patient developed septic shock due to cholangitis. Emergency gallbladder drainage was performed, and a bile stone impacting the distal common bile duct (white arrow head) was noted. A 4-Fr ENBD tube was inserted.
Figure 1.
(a) Enhanced computed tomography (CT) showing multiple small gallstones and gallbladder swelling. (b) The patient developed septic shock due to cholangitis. Emergency gallbladder drainage was performed, and a bile stone impacting the distal common bile duct (white arrow head) was noted. A 4-Fr ENBD tube was inserted.

Figure 2.
(a) After recovery from cholecystitis and sepsis, EPBD was performed, and the stone was removed by one balloon pulling. (b) After EPBD, a 5-Fr prophylactic ENBD tube was inserted, and no residual stone was detected by cholangiography.
Figure 2.
(a) After recovery from cholecystitis and sepsis, EPBD was performed, and the stone was removed by one balloon pulling. (b) After EPBD, a 5-Fr prophylactic ENBD tube was inserted, and no residual stone was detected by cholangiography.
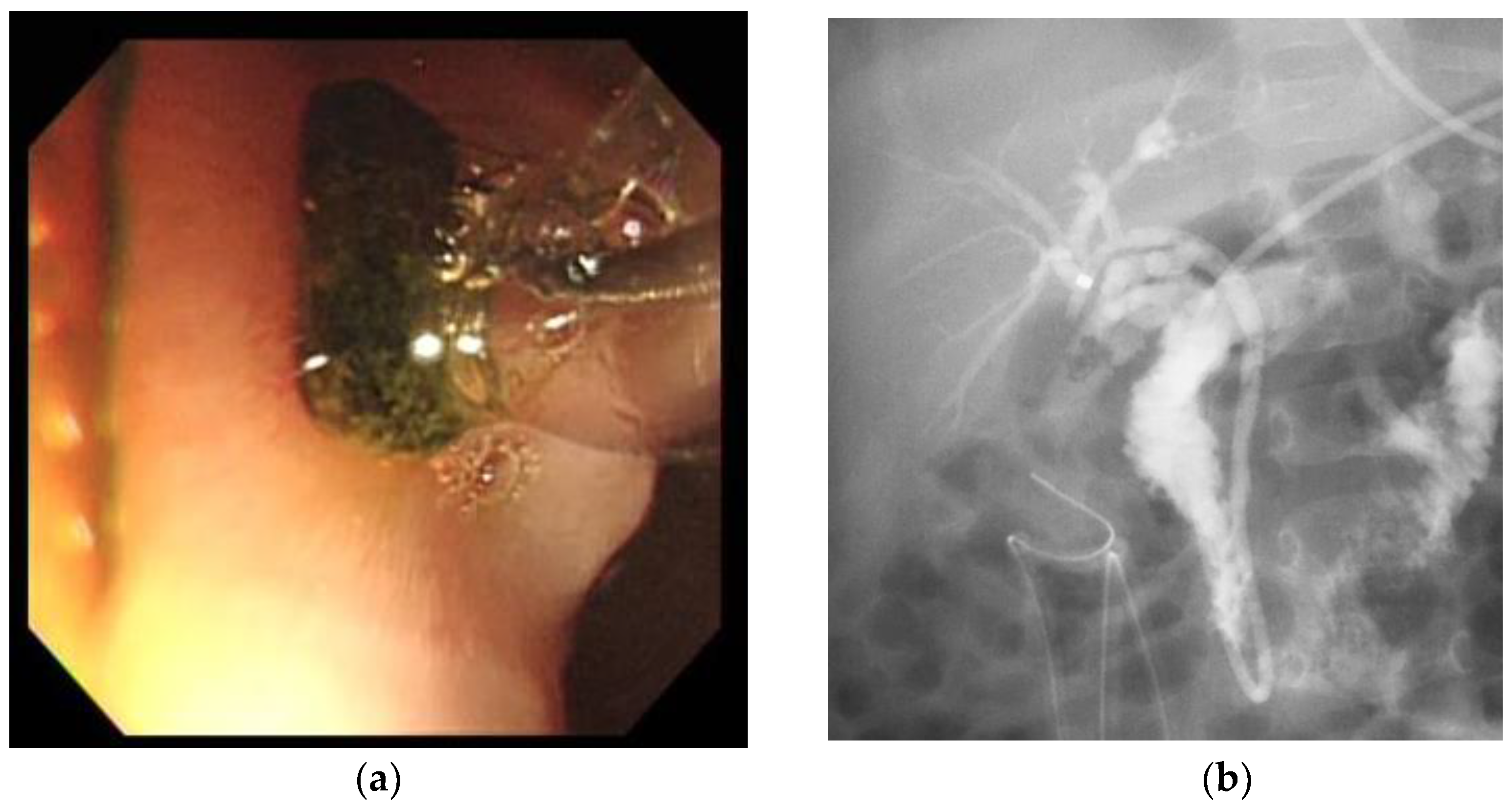
Figure 3.
(a) Enhanced CT showing multiple bile stones in the gallbladder and thickening of the wall. (b) EPBD soon after laparoscopic cholecystectomy revealed two bile stones (white arrow head) in the common bile duct. We removed the bile stones using EPBD.
Figure 3.
(a) Enhanced CT showing multiple bile stones in the gallbladder and thickening of the wall. (b) EPBD soon after laparoscopic cholecystectomy revealed two bile stones (white arrow head) in the common bile duct. We removed the bile stones using EPBD.
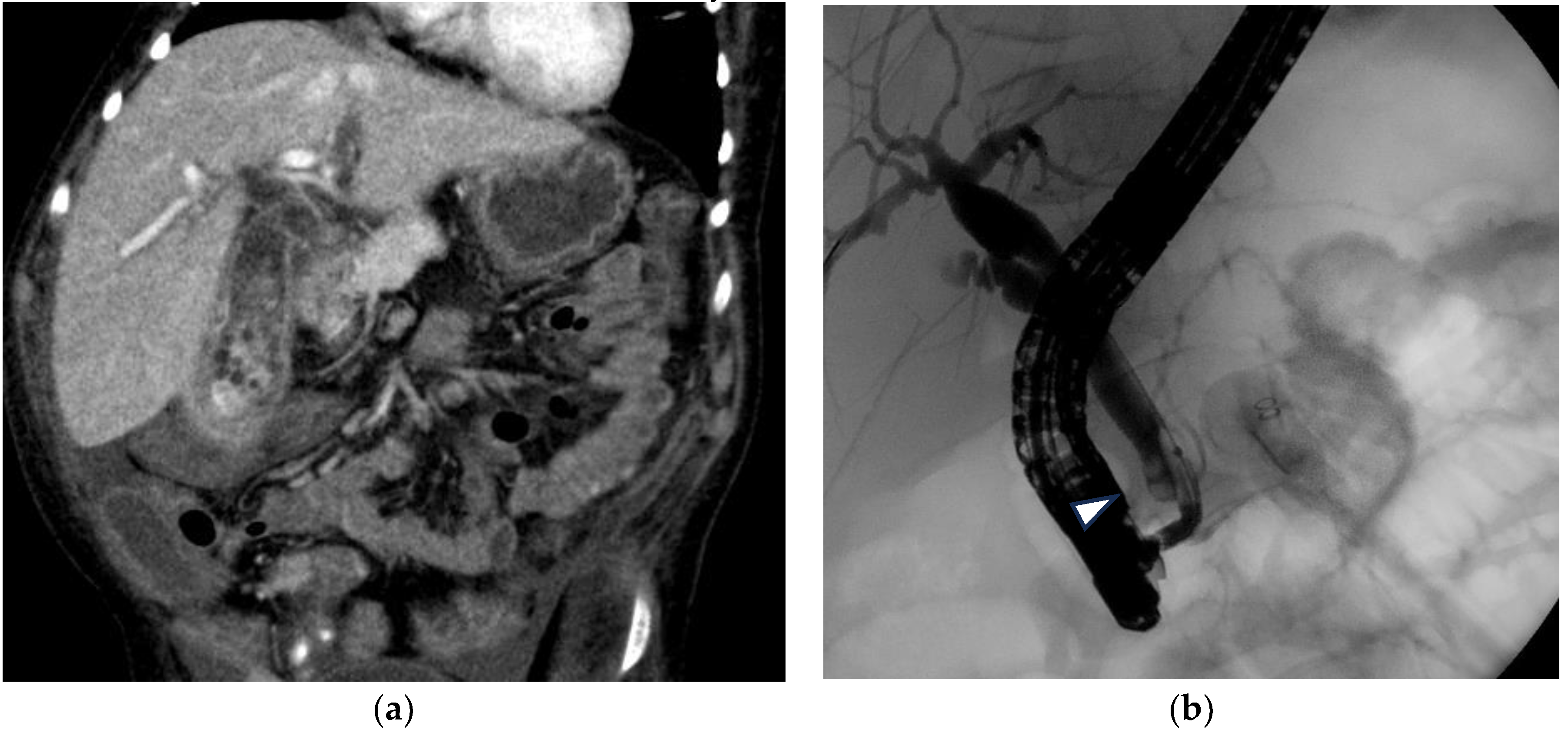

Table 1.
Features of pediatric patients with common bile duct stones treated with endoscopic papillary balloon dilatation.
Table 1.
Features of pediatric patients with common bile duct stones treated with endoscopic papillary balloon dilatation.
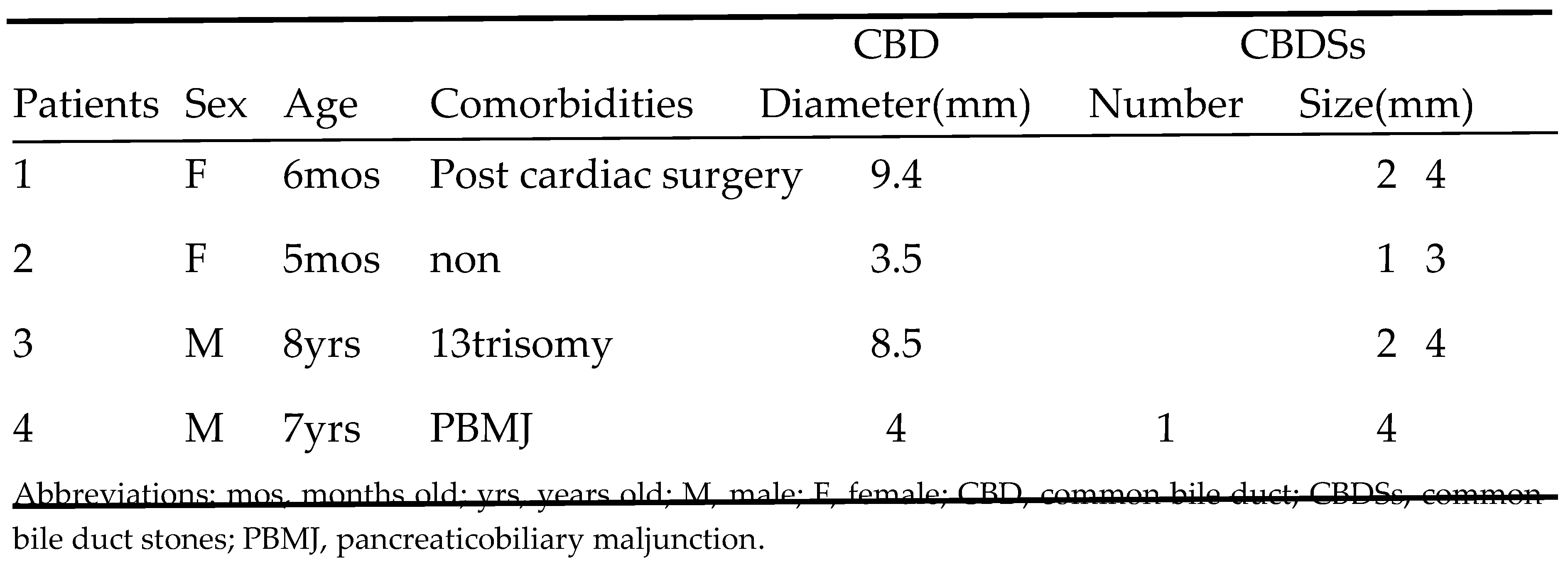 |
Table 2.
Reports of endoscopic retrograde cholangiopancreatography and endoscopic sphincterotomy in children with common bile duct stones in a high-volume center.
Table 2.
Reports of endoscopic retrograde cholangiopancreatography and endoscopic sphincterotomy in children with common bile duct stones in a high-volume center.
 |
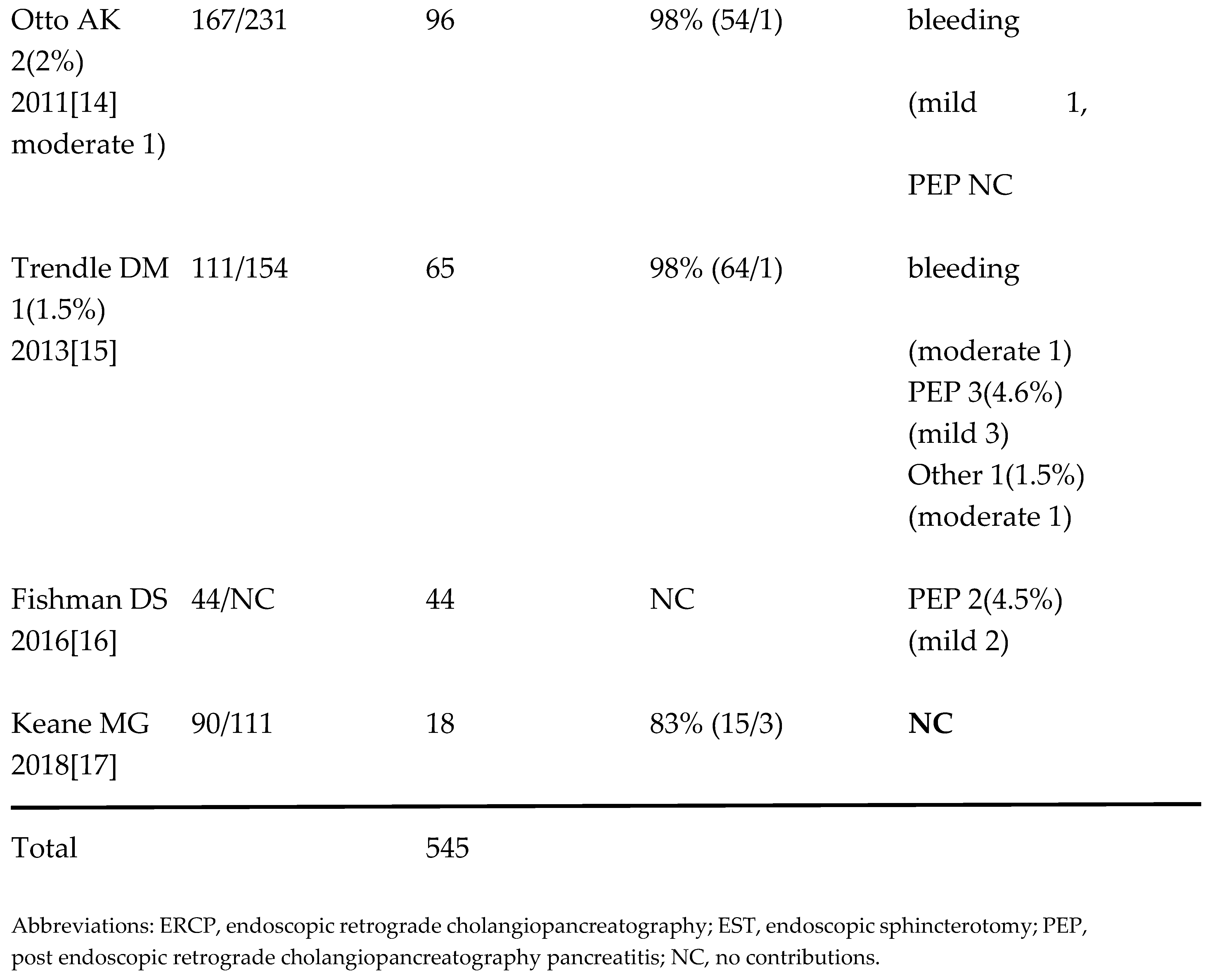 |
Table 3.
Endoscopic papillary balloon dilation in children under 15 years of age with common bile duct stones.
Table 3.
Endoscopic papillary balloon dilation in children under 15 years of age with common bile duct stones.
 |
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



