
Submitted:
27 February 2024
Posted:
28 February 2024
You are already at the latest version
Abstract
Chronic diseases, such as type 2 diabetes (T2D), are difficult to manage because they demand continuous therapeutic review and monitoring. Beyond achieving the target HbA1c, new guidelines for the therapy of T2D have been introduced with the new groups of antidiabetics (GLP-1ra and SGLT2-in). Despite new guidelines, clinical inertia, that can be caused by physicians, patients or healthcare system, results in T2D not being effectively managed. This opinion paper explores the shift in T2D treatment, challenging assumptions and evidence-based recommendations, particularly for family physicians, considering the patient's overall situation in decision-making. We looked for the possible reasons of clinical inertia and poor application of guidelines in the management of T2D. Guidelines for antidiabetic drugs should be more precise, providing case studies and clinical examples to define clinical contexts and contraindications. Knowledge communication can improve confidence and should include clear statements on areas of decision-making not supported by evidence. Precision medicine initiative in diabetes aims to identify subcategories of T2D patients (including frail patients) using clustering techniques from data science applications, focusing on CV and poor treatment outcomes. Clear, unconditional recommendations for personalized T2D management may encourage drug prescription, especially for family physicians dealing with diverse patient contexts and clinical settings.
Keywords:
type 2 diabetes
; therapeutic inertia
; clinical guidelines
; sodium-glucose cotransporter-2 inhibitors
; glucagon-like peptide-1 receptor agonists
; primary health care
1. Introduction
Managing chronic diseases is challenging, as they require continuous monitoring and evaluation of therapy. Guidelines for managing these diseases are rapidly changing, but due to clinical inertia, chronic diseases are often not well-controlled in clinical practice [1]. The term clinical inertia refers to healthcare professionals' inability to initiate or intensify therapy when desired therapeutic goals are not achieved, and is considered a medical error with adverse effects on health-related outcomes and healthcare costs [2].
Type 2 diabetes (T2D) is a prevalent disease among the older population and is expected to increase due to the epidemic of obesity and global population aging [3]. Apart from well-known cardiovascular (CV) complications, T2D is also associated with a higher risk of other age-related conditions such as sarcopenia, malnutrition, falls, urinary incontinence, and cognitive impairment [4]. It is therefore among the most disabled illnesses. Multiple comorbidities and complicated care regimens affect the quality of life of these patients, while healthcare providers face challenges in delivering quality care [5]. Family physicians are under immense pressure in their role to provide comprehensive and patient-centered care [6]. Clinical inertia and low adherence to evidence-based recommendations are common issues in managing T2D [7,8].
Factors that contribute to clinical inertia can be attributed to doctors, patients, or the healthcare system, but they are often interconnected [2,9,10] (Table 1). In a narrow sense, clinical inertia refers to poor adherence to evidence-based recommendations for medication therapy, by healthcare providers, which is termed "therapeutic inertia" [10,11]. This distinction is important because it helps differentiate doctor-related causes of clinical inertia from patient non-adherence to pharmacological treatment [12].
With the emergence of new groups of antidiabetic drugs, such as glucagon-like peptide 1 receptor agonists (GLP-1ra) and sodium-glucose cotransporter-2 inhibitors (SGLT2-in), which have significant cardio- and renal-protective effects, the pharmacological treatment of T2D has begun to undergo revolutionary changes [13]. It appeared that the framework outlined in international actionable documents to efficiently combat cardiovascular disease (CVD) in patients with T2D has come to be realized [14]. The integrated management of T2D and CVD would be of the utmost importance for public health, as both conditions were found to share common risk factors and pathophysiology pathways. This is especially significant since CVD is a leading cause of death worldwide [15,16]. Despite the proven efficacy of novel antidiabetic drugs in reducing CV morbidity and mortality in T2D patients, their prescription rates remain low in many countries and across clinical disciplines [17].
The new approach to treating T2D patients has undergone a shift that challenges some fundamental assumptions of clinical practice for T2D and the belief that following evidence-based recommendations can reduce clinical inertia. This conflict is particularly relevant for family physicians, which need to consider the patient's overall situation in their decision-making. In this opinion paper, we will explore some of these issues, with a particular focus on the family physician's perspective. This critical viewpoint refers primarily to the common guidelines of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD), and their recent updates, as widely used among providers in European countries [18,19,20]. We will also illustrate some of our critiques using data collected through our research.
2. Hesitancy in delivering a new antidiabetic drug treatment strategy related to postulates of clinical inertia
To determine the extent of clinical inertia, three postulates are crucial: 1) the specific clinical outcomes that the treatment is intended to achieve, 2) the recommended therapy regimen that should be administered, and 3) the timeframe for timely intensification of therapy [2]. Regarding the first postulate, intermediate biomarkers, that measure the quality of care in T2D patients, like hemoglobin A1c (HbA1c), blood pressure, and low-density lipoprotein (LDL)-cholesterol have been preferred in most studies over end-point clinical outcomes, like general or cardiovascular mortality, or hospital admission rates, as the latter requires long-term prospective follow-up [8,11]. The laboratory marker, HbA1c, has been traditionally used as a standard to guide medication therapy in clinical guidelines and practice [13]. The development of novel anti-diabetic medications with cardiovascular advantages caused a change in treatment goals, with the main objective now being to reduce CV risk rather than just controlling glucose [18,20]. Healthcare providers might have faced an internal problem while making decisions regarding this switch. Even more so, the current ADA/EASD guidelines still recommend achieving optimal glycemic control, to minimize the risk of cardiac events in the long term [19,21]. Therefore, there is a need to meet the dual goal.
The question being considered is whether combining a classical hypoglycemic drug with a new-class drug, when optimal HbA1c is not achieved, is beneficial in the long run or the episodes of hypoglycemia, as evidence suggested, may rather cause harm, also regarding long-term health outcomes [22]. It might be a dilemma especially in older T2D patients with multiple health conditions, who are however the right candidates for new-class drugs [18,21]. On the other hand, does maintaining a suboptimal HbA1c diminish the positive CV effect of the new-class drug, in any manner, to avoid hypoglycemia? Two lines of concern that healthcare providers face are evident in this dilemma. The first one is fear of over-treating and resulting hypoglycaemia – a known reason for clinical inertia when managing T2D patients [23,24]. The second is the uncertainty associated with long-term outcomes, which is difficult to predict in individual patients, as multiple factors that characterize patients, and variations in treatment, can influence them [25]. Beyond the providers` hesitancy to intensify or change the therapy is not always indolence, but the fear of harming, or the difficulty of deciding conditions of uncertainty. The abovementioned is supported by studies demonstrating that therapeutic inertia increases with the prescription of more antidiabetic drugs over time and decreases when HbA1c levels rise [11].
Regarding the time from the problem detection to therapy intensification, the studies that were conducted before the advent of new antidiabetic drugs reported a long time delay despite the suboptimal glycaemic control [26,27]. How to know whether some of the GLP-1ra or SGLT2-in is delivered timely when there is more than one criterion to follow? Is early therapy intensification the right choice in treating newly diagnosed, usually obese, T2D patients, and do they need to be treated with new antidiabetic drugs immediately or when clear signs of heart failure or renal function impairment become visible? How these choices fit into the national health strategy in terms of financial restraints is also crucial. However, the intensification of therapy for newly diagnosed T2D patients has always been a challenge [28]. The 2018 update of ADA/EASD guidelines provides an alternative prescribing policy for low-income countries, which is not based on evidence-based recommendations [18]. Sharing the results of cost-effectiveness studies on new antidiabetic drugs with national healthcare authorities could help overcome therapeutic inertia [29].
The primary healthcare system's ability to systemically screen T2D patients with low renal function—information that is crucial for evaluating T2D patients with chronic kidney disease (CKD)—remains an obstacle, particularly for family physicians. In particular, to obtain information on quantified heart failure (whether it is with preserved or reduced ejection fraction), an ultrasound examination is required, making it unreliable to assume that all T2D patients have this information. The recent trials, examining the structured model of care - that is the model with standardized elements of the care process, have shown benefits for quality of care, clinical outcomes, and cost-effectiveness [30,31].
Finally, considering that some patients may meet more than one set of indication criteria, how can the proportion of T2D patients who qualify for therapy with novel antidiabetic drugs be determined? (Figure 1).
The clinical guidelines offer recommendations for delivering standardized and optimal care to patients based on scientific evidence. Adherence to guidelines by healthcare providers is considered the principal way to limit clinical inertia [10]. Despite the proven benefits, implementation rates remain below 50% historically across clinical disciplines [10,32]. Many attempts have been made to identify barriers that limit the implementation of clinical guidelines in daily medical practice [33,34]. It has been found that many guidelines manuals are too long and complicated, making it difficult to implement them effectively. Furthermore, they often fail to offer solutions for specific patient scenarios. Research on implementation strategies for guidelines needs to be intensified. Implementing guidelines should be part of a wider process of knowledge translation that results in the creation of protocols and workflows. Given the abundance of guidelines available, there is a growing need for continuous quality assessment and improvement of the development process. In today's era of healthcare system digitalization, online tools such as websites, alerting systems, interactive platforms, and clinical decision support systems are being used to aid in the access and implementation of clinical guidelines. However, the effects on practice and clinical outcomes from these tools are still unknown.
In the diagnosis, treatment, and follow-up of chronic diseases, primary healthcare providers, mostly family physicians, play a central role [9]. They are even more concerned than specialist endocrinologists with decisions on when is the right time to change or intensify therapy in T2D patients because their decision-making is more complex and involves the care of the whole patient [35]. This may be particularly challenging in circumstances such as starting insulin therapy, introducing new medications in the treatment plan, or attempting to achieve glycemic control by combining two or more oral antidiabetic drugs, as it is usual in older patients with multiple comorbidities [36]. In such cases, family physicians tend to pass the responsibility of choosing the treatment to endocrinologists, trying to avoid any anxiety that may arise due to the side effects of intensifying the therapy or using medications that they have less experience with [37].
It can be challenging to implement clinical guidelines in primary care and family medicine due to the specific nature of the workflow, which involves a holistic approach to patient care, by considering patient preferences for treatment, their ability to take medications independently, and predicting their adherence to suggested treatment [25]. It is assumed that education on psychological factors that influence patient behavior in care uptake would reduce the providers` uncertainties during decision-making and should become a part of implementation strategies [38]. In addition, family physicians may have strong attitudes towards certain medications that they have experience with and that are well accepted by patients and may be hesitant to try new treatments, despite the evidence of their efficacy [37]. Based on that, it is important to research the psychological factors that may influence family doctors' attitudes towards their behavioural intentions and decisions for action, as well as on doctor-patient communication that can shape behavioral changes. This research should be an integral part of the process of clinical guidelines development [39].
Overall, clinical guidelines are generally not designed to suit the working style of primary care providers and family physicians [35,40]. In addition, there is a lack of competency-based workflow and effective communication models between different disciplines, which can also contribute to the non-adherence of family physicians to the guidelines [37]. Research performed thus far has identified several categories of barriers and enablers to the implementation of clinical guidelines in primary care [7,41,42]. Suboptimal inter-professional communication, non-transparent division of professional responsibilities, time constraints, limited applicability of the guidelines in real-life practice, lack of knowledge and skills of primary care providers (the lack of implementation strategies), poor motivation to use guidelines in everyday workouts, and inadequate reinforcement were among the most commonly reported barriers. The most frequently reported enablers were the presence of technical support, timely education, and training for both primary care providers and patients. It is widely assumed that conducting qualitative research among primary care providers and family physicians could be a valuable way of information gathering on guidelines gaps and barriers in implementation strategies that concern them specifically [42].
3. Trends in the ADA/EASD guidelines on T2D patient management strategy and the effect on new antidiabetic drug uptake
The recent updates of the ADA/EASD guidelines (2018, 2019, and 2022), and the position statements drawn from them, have brought several areas of improvement for managing T2D patients [18,19,20,43]. First, the requirement is emphasized for the systematic screening of T2D patients for CVD and increased CV risk and the treatment of these patients with antidiabetic drugs with proven CV efficacy. It marked the end of the long-standing paradigm that T2D is the risk equivalent of coronary artery disease (CAD) or, in other words that all patients diagnosed with T2D have the same risk for atherosclerotic CVD (ASCVD). The studies conducted in the past two decades have revealed that risk levels in T2D patients approach the CAD risk levels after a decade of T2D duration or in patients with target organ damage (proteinuria, estimated glomerular filtration rate <30 mL/min/1.73 m2, left ventricular hypertrophy or retinopathy) or in those with three or more CV risk factors [44]. This finding allowed the grading of CV risk in T2D patients in three categories, very high, high, and moderate levels. The target management, of those at high and very high CV risk, has become possible thanks to the results of CV outcome trials (CVOTs), that have become mandatory for all novel drugs used to treat T2D patients [45].
Up to date, significant CV benefits have been proven for several GLP-1ra and SGLT2-in drugs, and they are advised as a preferred treatment choice for patients with T2D and established ASCVD or those at increased risk for ASCVD, independently of the glucose control level and the background use of metformin (the first-line medication). The therapy with SGLT2-in takes precedence over GLP-1ra for T2D patients with chronic heart failure (CHF) and chronic kidney disease (CKD) [21,45]. In addition, increased CV risk can be ameliorated through the potent effect of these drugs, in particular, GLP-1ra and emerging insulin secretion stimulating drugs tirzepatide, on body weight reduction [46,47].
Nevertheless, the uptake rates of GLP-1ra and SGLT2-in drugs remain low. The potential barriers in their prescribing, that refer to the gaps in the guidelines, include safety concerns, lack of clarity about when is the right time, and to whom, exactly, the therapy with either of these drugs should be initiated, as well as the lack of understanding of the treatment effects such as glycaemic, cardiac, and renal outcomes, including possible side-effects, concerning the specific sociodemographic, clinical, and laboratory characteristics of patients to whom these drugs are to be prescribed (48 - 50). For example, differences in patient socioeconomic status may be important for the uptake of SGLT2-in, if the costs are a concern [48]. A lesser glycaemic response can be expected for SGLT2-in in case of lower renal function and for GLP1-ra in case of patient reduced insulin secretion ability [49]. The knowledge is still insufficient on the full range of health effects of new antidiabetic drugs, in particular, SGLT2-in, and safety issues cannot be predicted with sufficient confidence [51,52,53]. An introduction of these drugs into the existent therapeutic scheme, in particular of older patients with multiple comorbidities and polypharmacy, may potentially cause interactions with other treatments or disease-related conditions, which may cause concerns among providers and family physicians about indications for these medications' therapy [49,54,55,56] (Table 2).
The question that needs to be clarified is how much variations between drugs, trial designs, or patient characteristics may influence the differences in the treatment effects of these drugs. In trial designs significant differences between CVOTs have been detected. Post-hoc analyses, with patient re-grouping into different CV risk categories, have been suggested as a solution to overcome these disparities [50]. In addition, the structure of patients included in CVOTs does not match the characteristics of T2D patients in real-life conditions, which could undermine the providers` confidence in recommendations provided by the guidelines [57]. Recognizing this problem, the CVOT Summit 2022 has issued a Report with recommendations to analyze the real-world data (that are routinely collected in practices), to complement the results of CVOTs, by providing more specific information on treatment options, patient risks, and safety issues related to these medications, which could help the decision-making process [58]. For example, an insight into the safety of SGLT2-in in specific patient groups such as elderly individuals has been obtained this way [59].
The general expert view is that the guidelines should be more precise in terms of how to use these drugs in specific situations, by providing case studies and clinical examples, to more specifically define clinical contexts in which to initiate their use or for which contraindications may exist [48]. Similarly, family physicians assume that their confidence can be improved by strategies such as appropriate knowledge communication with them. They also assume that the guidelines should contain clear statements about which areas of decision-making are not sufficiently supported by evidence, and for which subgroup of patients the harm-benefit ratio when using new antidiabetic drugs is not well understood [42,60].
Many of these gaps, which can lead to difficulties in making decisions about individualized therapy for T2D patients, are the result of a lack of study data. Nevertheless, in the development of the recent updates to the ADA/EASD guidelines for the management of T2D patients, there is a clear intent to promote a patient-centered approach that could help healthcare providers, particularly family physicians, alleviate concerns in decision-making and ultimately reduce clinical inertia [18,19,20]. According to these updated guidelines, the choice of antidiabetic drugs should be made with the patient in mind. Consideration should be given to comorbidities, but also to the risk of hypoglycemia, the impact on weight, the treatment cos, the side effects, and the patient's preferences. In addition, the 2022 ADA/EASD guidelines focus on the social determinants of health and healthcare systems and provide the necessary evidence for counseling patients on non-pharmacological treatment and behaviour change, including physical activity, sleep hygiene, weight management, and nutrition [19]. While the ADA/EASD guidelines still do not explain the need for systematic assessment of mental health and well-being in T2D patients, the openness for continued knowledge development and implementation into practice is clearly outlined.
4. T2D patient complexity and endeavor towards precision medicine
The possibilities of medication treatment of T2D patients are expanding, and advances in technology support such as continuous or intermittent scanning of glucose levels, mobile health, digital support, and visualization systems are leading to improvement in the management of these patients [18,19,20]. On the other hand, the requirements for a high standard of care, which include patient-centered and personalized approaches, may be constrained by still insufficient understanding of patient complexity. The complexity means a great variability among patients in clinical characteristics, comorbidity patterns, organ damage degrees, and the potential for negative health outcomes, and is in particular characteristic of elderly patients (65+), who in turn involve a major part of T2D patients [4,61]. This group experiences T2D alongside aging and accumulation of comorbidities and geriatric syndromes such as sarcopenia, malnutrition, cognitive impairment, and frailty, which can alter the pathophysiology of T2D, treatment effects, and outcomes [4].
In particular, older T2D patients with frailty are more prone to hypoglycaemia and its adverse consequences, including falls, fractures, hospitalization, CV events, and mortality. Consideration should be given to simplification, switching, or de-escalation of the therapeutic regimen in these patients [62,63]. However, if insufficiently treated, hyperglycemia can lead to acute complications such as dehydration, poor wound healing, and hyperglycaemic hyperosmolar coma, which should be avoided [63]. There is a delicate balance between over-treating and suboptimal treating, which requires an individualized treatment approach, by carefully planning both pharmacological and non-pharmacological treatments [64]. Sometimes, it is not clear how much under-prescription of the guideline-recommended therapy to frail patients, and how much the frailty status per se, contributes to poor outcomes [65].
Frailty is considered a state of failure of homeostasis in multiple organs and systems and is manifested by non-specific symptoms and signs such as muscle mass reduction, slow walking, low activity, and a feeling of exhaustion that are progressive in number and severity with aging and the presence of comorbidities [66]. Experts agree that an assessment of frailty should become a part of older T2D patients' examination so that glycaemic targets and therapeutic choices can be modified accordingly [63]. Nevertheless, knowledge is still insufficient to allow the formal guidelines development to help healthcare providers in their decisions of how to precisely manage these patients. One of the reasons may be the complex interplay between T2D, CVD, CKD, sarcopenia, and frailty (Figure 2). These conditions share common pathophysiology pathways and can potentiate the development of each other [64,67,68].
Frailty is associated with incident T2D in an older population and increased risk of comorbidities and poor outcomes; and vice versa, T2D predicts transition to higher frailty levels, while vascular complications of T2D and associated malnutrition accelerate functional decline associated with frailty [64].
Frailty contributes to the heterogeneity of patients with T2D. At least two frailty phenotypes exist in older T2D patients. One is associated with obesity and high insulin resistance (sarcopenic obese phenotype) and another is associated with weight loss, the body`s shrinking, and low insulin resistance (anorexic malnourished phenotype) [69]. The growing evidence indicates that the clinical expression of frailty is sex-dependent, which means that women are more prone to frailty and frailty-related physical disability than men, while men experience frailty at older ages than women [70,71] (Figure 3). Contrary to what is the case in the general population, women with T2D are more prone than men with T2D to CVD, but preferably for a non-atherosclerotic type of CAD and CHD [72,73].
In summary, the relationship between T2D and frailty is complex, and many questions are still unanswered, which makes the treatment of older T2D patients challenging. This can also be applied to the treatment of these patients with new antidiabetic drugs, GLP-1ra and SGLT2-in (Table 3).
Although the common conclusion of the studies performed so far is that SGLT2-in and GLP-1ra improve CV outcomes in older (≥65) and frail patients, concerns remain when narrowly defined patient subgroups are used for analysis such as older men and those older than 70 years [74]. In addition, frailty may change the harm-benefit balance of these drugs. One of the main concerns about their use in older or frail patients, in particular regarding GLP-1ra, is the effect of these drugs on weight loss, which in these patients could be counterproductive. For SGLT2-in, it is also important to take care of the presence of urinary incontinence, a disorder often associated with frailty, since the use of SGLT2-in may lead to worsening of this disorder, or cause serious infections in these patients [55]. In addition, the reduced hypoglicaemic effect of SGLT2-in patients with low renal function may potentially increase the risk of diabetic ketoacidosis [55,63].
Following increased awareness of the heterogeneity of T2D patients and the requirement for individualized treatment, an initiative has been launched for precision medicine in diabetes [80,81]. Studies that assess the feasibility of using clustering techniques from data science application areas are underway, wanting to identify subcategories of patients with T2D that can be discriminated against in terms of CV and other poor outcomes and responses to treatment. Our research group has contributed to these efforts [82−84]. Regarding treatment, precision medicine looks at variations in drug effectiveness in specific patient subgroups and seeks markers (especially genetic markers) that can predict adverse drug events [80]. However, many challenges still need to be overcome before it will be possible to implement precision medicine in the management of T2D patients [71].
5. Discussion
Taken together, the evidence is still limited on how different patient features, including age, sex, body mass and shape, comorbidity patterns, frailty status, and the level of renal function decline, may impact differences in how individuals respond to GLP-1ra and SGLT2-in. This is partly due to the traditionally inadequate characterization of participants in clinical trials, who are not systematically assessed for comorbidities, functional status, and frailty. Clinical inertia is known to be exacerbated by ambiguous guidelines and pathways. On the other hand, being aware of the broader patient context, and how it may predict responses to certain treatments, will allow for better-informed decisions for personalized management of patients with T2D.
According to the above discussion, the heterogeneity of older patients with T2D and an insufficient understanding of factors that influence treatment outcomes in older patients with T2D, might be a key barrier to individualized patient care and a reason for poor adherence of healthcare providers and family physicians to guidelines. For healthcare professionals to safely prescribe antidiabetic medications and make decisions about when to escalate or de-escalate treatment, the guidelines should be designed to assist the treatment of older adults with type 2 diabetes. This would be especially important for family physicians, who usually do not feel confident to radically change therapy by themselves. The international authorities emphasize the necessity of comprehensive patient assessment, which would allow the multilayered and holistic approach to managing these patients [80]. Data indicating comorbidities, co-medications, functional disabilities, mental health disorders, doctor-patient communication, patient health literacy, issues such as a willingness to change or a preference for a certain type of therapy, and the patient's need for support, are all things to take into account. Many of these factors have an impact on medication uptake rates, and ultimately on the patient response to treatment and the outcomes.
Evidence from epidemiologic research indicates that the time perspective of disease progression is critical to consider for hyperglycemia management, treatment regimen planning, and the prediction of CV events in T2D patients [85]. Variables such as T2D duration, patient age, and age at T2D diagnosis showed prognostically meaningful, considering that the diagnosis earlier in the life course, younger age, but longer T2D duration, carry out higher CV risk [104]. The fact that CKD, which usually accompanies T2D, is regarded as an independent CV risk factor, is also an important issue to take care of [86,87]. The variables specifically significant for the prognosis of T2D patients are age at T2D onset, eGFR, and HbA1c. These variables were aligned with the latest classification system for CV event risk estimation (SCORE2), which comprises classical CV risk factors such as age, sex, smoking, systolic blood pressure, total and HDL-cholesterol, and re-calibrated into a new system, SCORE-2 Diabetes, used for estimating the ten-year risk of CV events in T2D patients of European countries [21,88].
By allowing T2D patients to be included in CV risk assessments as those who are most at risk for CVD, the model mentioned provides important advancements in the prevention of CVD [89]. Many CV risk prediction models applicable to patients with T2D have been developed so far, but they could not accurately predict individuals who will probably experience CVD [90,91]. The applicability of SCORE-2 Diabetes has yet to be proved, concerning the accuracy of the prediction and the adequacy of the risk factors that have been included in the model [92]. In-depth evaluation of T2D patients is still necessary to precisely identify individuals with subclinical CVD who are at very high CV risk and are, therefore, also candidates for introducing therapy with new antidiabetic drugs [18,93]. Once cardiac biomarkers are approved for routine usage, routine testing using them will be a more straightforward method of accurately screening these patients [93,94].
The classical CV risk factors (which make up the SCORE2 model) do not perform well as CV risk predictors in this group, while some new variables like pharmacologic treatments, cognitive decline, and frailty have been proven to be better predictors. This makes the SCORE-2 Diabetes model particularly uncertain when it comes to predicting CV risk in elderly T2D patients. [95,96]. There are also uncertainties related to the effect of sex on CV outcomes in T2D patients and on the expression of frailty phenotypes, which may have implications on responses to treatment [72,97,98].
6. Future directions
Precision medicine hoped to improve the health of individuals or specific population subgroups by identifying biomarkers (genetic, epigenetic, or biochemical) for early detection of important diseases which, in turn, would guide interventions [99]. The success of this approach has been shown partially. One of the primary causes is the potential for exceedingly complex disease etiology, particularly in the case of prevalent non-communicable diseases. In chronic complex diseases, genetic associations have a small effect size on the expression of phenotypes, in contrast to the more robust contribution of behavioral and social factors [80]. Moreover, these diseases develop as a part of the aging process, by sharing common pathophysiological pathways with aging and with each other, showing a tendency to cluster together [100]. Knowing the clinical, biological, and sociodemographic characteristics that are consistently linked to variations in clinical outcomes is essential for treating patients with chronic complicated diseases on an individual basis [49].
Today, there is an emerging trend in using large-scale person-generated health data from electronic health records, smartphones, and wearables, to characterize different patient subgroups, and to improve the health and well-being of particular patient subgroups through strategies customized to their specific characteristics [101]. Based on our own experience, we recommend the implementation of Artificial Intelligence (AI) and data-driven research methods in primary care and family medicine, to become a part of the routine healthcare workflows [102]. As an answer to doubts about the accuracy and repeatability of the results of these methods, it is worth mentioning that the techniques in the field of AI applications that already exist can guarantee the generalizability of findings or can consider the patient effect heterogeneity. It might diminish uncertainties associated with patient complexity, and support family physicians in more individualized decisions, especially in areas where guidelines cannot provide clear recommendations. The search for simple-to-obtain biomarkers of CVD or frailty that can be used in population-based studies could also help harness uncertainty.
In addition to CVOTs, further research efforts should focus on preparing real-life studies, aimed at addressing complex issues such as different comorbidity patterns. Priority should also be given to advancing translational and implementation sciences, which should obligatorily include qualitative research including primary care providers and family physicians. This will hopefully help remove obstacles to the practical application of the guidelines in practice and tailored recommendations.
To summarize, the unresolved issue of how to manage the heterogeneity of patients with T2D and to define subgroups with different levels of CV risk is the main barrier to individualized treatment and the reason for low uptake of GLP-1ra and SGLT2-in drugs, despite accumulating evidence on their CV benefits and decreasing costs. The shortcomings of the guidelines primarily reflect the methodological limitations of the current evidence base. Intensification of research, with the introduction of new research methods and approaches is necessary to fill the current research gaps and allow the translation of new evidence into the guidelines` recommendations and clinical practice. This ultimately involves the discovery of new biomarkers for CVD and frailty.
We summarized priorities for future work that should fill the gaps in the current evidence-based recommendations, as identified by this review, including strategies that refer to designing future research, the process of the guidelines development, and knowledge implementation strategies (Table 4).
7. Conclusions
Current evidence on treatment effect heterogeneity for GLP1-ra and SGLT2-in therapies is limited, reflecting the methodological limitations of the underlying research. The introduction of new research methods and approaches is necessary to fill the current research gaps and allow for an understanding of treatment effect heterogeneity in T2D patients. The translation of new evidence into the guidelines` recommendations and clinical practice needs to involve different methods and more active approaches. Clear and unconditional recommendations for individualized management of patients with T2D may encourage the prescription of these drugs by the providers, which is especially crucial for family physicians who deal with a wide range of specific patient contexts daily, as well as various clinical and social settings.
Author Contributions
Conceptualization, T.K., D.Š., Z.B., and LJ.T.M; methodology, B.M.; software, Z.B., and B.M.; validation, T.K., D.Š., and LJ.T.M.; formal analysis, S.C.V; investigation, T.K.; resources, LJ.T.M.; data curation, D.Š.; writing—original draft preparation, T.K., D.Š., Z.B. and LJ.T.M.; writing—review and editing, T.K., B.M., LJ.T.M. and S.C.V; visualization, B.M.; supervision, S.C.V. and LJ.T.M.; project administration, LJ.T.M.; funding acquisition, LJ.T.M. All authors have read and agreed to the published version of the manuscript.
Funding
Research was funded by the University of Osijek, grant number IP-23 “Integrated Models of Chronic Diseases”.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
| T2D | type 2 diabetes |
| CV | cardiovascular |
| GLP-1ra | glucagon-like peptide 1 receptor agonists |
| SGLT-2in | sodium-glucose cotransporter-2 inhibitors |
| CVD | cardiovascular disease |
| ADA | American Diabetes Association |
| EASD | European Association for the Study of Diabetes |
| HbA1c | hemoglobin A1c |
| LDL | low-density lipoprotein |
| CAD | coronary artery disease |
| ASCVD | atherosclerotic cardiovascular disease |
| CVOT's | cardiovascular outcome trials |
| CHF | chronic hearth failure |
| CKD | chronic kidney disease |
| AI | Artificial Intelligence |
| DKA | diabetic ketoacidosis |
References
- Phillips L.S.; Branch W.T.; Cook C.B.; Doyle J.P.; El-Kebbi I.M.; Gallina D.L.; Miller C.D.; Ziemer D.C.; Barnes C.S. Clinical Inertia. Ann Intern Med. 2001; 135(9): 825-34. [CrossRef]
- O'Connor P.J.; Sperl-Hillen J.M.; Johnson P.E.; Rush W.A.; Biltz G. Clinical Inertia and Outpatient Medical Errors. Henriksen K.; Battles J.B.; Marks E.S.; Lewin D.I.; et al, editors. Advances in Patient Safety: From Research to Implementation (Volume 2: Concepts and Methodology). Rockville (MD), USA: Agency for Healthcare Research and Quality (US) (2005).
- GBD 2021 Diabetes Collaborators. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021 [published correction appears in Lancet. 2023 Sep 30;402(10408):1132]. Lancet. 2023;402(10397):203-234. [CrossRef]
- Bellary S.; Kyrou I.; Brown J.E.; Bailey C.J. Type 2 diabetes mellitus in older adults: clinical considerations and management. Nat Rev Endocrinol. 2021; 17(9) :534-548. [CrossRef]
- Jing X.; Chen J.; Dong Y.; Han D.; Zhao H.; Wang X.; Gao F.; Li C.; Cui Z.; Liu Y.; et al. Related factors of quality of life of type 2 diabetes patients: a systematic review and meta-analysis. Health Qual Life Outcomes. 2018;16(1):189. [CrossRef]
- Rutten G.E.H.M.; Alzaid A. Person-centred type 2 diabetes care: time for a paradigm shift. Lancet Diabetes Endocrinol. 2018;6(4):264-266. [CrossRef]
- de Belvis A.G.; Pelone F.; Biasco A.; Ricciardi W.; Volpe M. Can Primary Care Professionals' Adherence to Evidence Based Medicine Tools Improve Quality of Care in Type 2 Diabetes Mellitus? A Systematic Review. Diabetes Res Clin Pract. 2009;85(2):119-31. [CrossRef]
- Stone M.A.; Charpentier G.; Doggen K.; Kuss O.; Lindblad U.; Kellner C.; Nolan J.; Pazderska A., Rutten G., Trento M., et al; GUIDANCE Study Group. Quality of care of people with type 2 diabetes in eight European countries: findings from the Guideline Adherence to Enhance Care (GUIDANCE) study. Diabetes Care. 2013;36(9):2628-38. [CrossRef]
- Byrnes P.D. Why Haven't I Changed That? Therapeutic Inertia in General Practice. Aust Fam Physician. 2011;40(1-2):24-8.
- Lavoie K.L.; Rash J.A.; Campbell T.S. Changing Provider Behavior in the Context of Chronic Disease Management: Focus on Clinical Inertia. Annu Rev Pharmacol Toxicol. 2017;57:263-83. [CrossRef]
- Khunti K.; Gomes M.B.; Pocock S.; Shestakova M.V.; Pintat S.; Fenici P.; Hammar N., Medina J. Therapeutic inertia in the treatment of hyperglycaemia in patients with type 2 diabetes: A systematic review. Diabetes Obes Metab. 2018;20(2):427-437. [CrossRef]
- Allen J.D.; Curtiss F.R.; Fairman K.A. Nonadherence, Clinical Inertia, or Therapeutic Inertia? J Manag Care Pharm. 2009;15(8):690-5. [CrossRef]
- Inzucchi S.E.; Bergenstal R.M.; Buse J.B.; Diamant M.; Ferrannini E.; Nauck M.; Peters AL.; Tsapas A.; Wender R.; Matthews DR. Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2015;38(1):140-9. [CrossRef]
- Mitchell S.; Malanda B.; Damasceno A.; Eckel RH.; Gaita D.; Kotseva K.; Januzzi J.L.; Mensah G.; Plutzky J.; Prystupiuk M.; et al. Roadmap on the Prevention of Cardiovascular Disease Among People Living With Diabetes. Glob Heart. 2019;14(3):215-240. [CrossRef]
- Sharma A.; Mittal S.; Aggarwal R.; Chauhan MK. Diabetes and cardiovascular disease: inter-relation of risk factors and treatment. Futur J Pharm Sci. 2020;6:130. [CrossRef]
- Li Y.; Liu Y.; Liu S.; Gao M.; Wang W.; Chen K.; Huang L.; Liu Y. Diabetic vascular diseases: molecular mechanisms and therapeutic strategies. Signal Transduct Target Ther. 2023;8(1):152. [CrossRef]
- Schernthaner G.; Shehadeh N.; Ametov AS.; Bazarova AV.; Ebrahimi F.; Fasching P.; Janež A.; Kempler P.; Konrāde I.; Lalić N.M.; et al. Worldwide inertia to the use of cardiorenal protective glucose-lowering drugs (SGLT2i and GLP-1 RA) in high-risk patients with type 2 diabetes. Cardiovasc Diabetol. 2020;19(1):185. [CrossRef]
- Davies M.J.; D'Alessio D.A.; Fradkin J.; Kernan W.N.; Mathieu C.; Mingrone G.; Rossing P.; Tsapas A.; Wexler D.J.; Buse J.B. Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2018;41(12):2669-701. [CrossRef]
- Davies M.J.; Aroda V.R.; Collins B.S.; Gabbay R.A.; Green J.; Maruthur N.M.; Rosas S.E.; Del Prato S.; Mathieu C.; Mingrone G.; et al. Management of Hyperglycemia in Type 2 Diabetes, 2022. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2022;45(11):2753-86. [CrossRef]
- Buse J.B.; Wexler D.J.; Tsapas A.; Rossing P.; Mingrone G.; Mathieu C.; D'Alessio D.A.; Davies M.J.; 2019 Update to: Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care. 2020;43(2):487-93. [CrossRef]
- Marx N.; Federici M.; Schütt K.; Müller-Wieland D.; Ajjan R.A.; Antunes M.J.; Christodorescu R.M.; Crawford C.; Di Angelantonio.; Eliasson B.; et al; ESC Scientific Document Group. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes. Eur Heart J. 2023;44(39):4043-4140. [CrossRef]
- Boussageon R.; Bejan-Angoulvant T.; Saadatian-Elahi M.; Lafont S.; Bergeonneau C.; Kassaï B.; Erpeldinger S.; Wright J.M.; Gueyffier F.; Cornu C.; Effect of intensive glucose lowering treatment on all cause mortality, cardiovascular death, and microvascular events in type 2 diabetes: meta-analysis of randomised controlled trials. BMJ. 2011;343:d4169. [CrossRef]
- Khunti K.; Davies M.J. Clinical Inertia Versus Overtreatment in Glycaemic Management. Lancet Diabetes Endocrinol. 2018;6(4):266-8. [CrossRef]
- Mata-Cases M.; Mauricio D.; Real J.; Vlacho B.; Romera-Liebana L.; Molist-Brunet N.; Cedenilla M.; Franch-Nadal J. Potential Risk of Overtreatment in Patients with Type 2 Diabetes Aged 75 Years or Older: Data from a Population Database in Catalonia, Spain. J Clin Med. 2022;11(17):5134. [CrossRef]
- Gimeno J.A.; Cánovas G.; Durán A. Factors Associated with Adherence to Clinical Practice Guidelines for Patients with Type 2 Diabetes Mellitus: Results of a Spanish Delphi Consensus. J Diabetes Res. 2021:9970859. [CrossRef]
- Pantalone K.M.; Wells B.J.; Chagin K.M.; Ejzykowicz F.; Yu C.; Milinovich A.; Bauman JM.; Kattan MW.; Rajpathak S.; Zimmerman R.S. Intensification of Diabetes Therapy and Time Until A1C Goal Attainment Among Patients With Newly Diagnosed Type 2 Diabetes Who Fail Metformin Monotherapy Within a Large Integrated Health System. Diabetes Care. 2016;39(9):1527-34. [CrossRef]
- Khunti K.; Wolden M.L.; Thorsted B.L.; Andersen M.; Davies M.J. Clinical Inertia in People with Type 2 Diabetes: A Retrospective Cohort Study of More Than 80,000 People. Diabetes Care. 2013 36(11):3411-7. [CrossRef]
- Suraci C.; Mulas F.; Rossi M.C.; Gentile S.; Giorda C.B.; Management of Newly Diagnosed Patients with Type 2 Diabetes: What Are the Attitudes of Physicians? A Subito!Amd Survey on the Early Diabetes Treatment in Italy. Acta Diabetol. 2012;49(6):429-33. [CrossRef]
- Pawaskar M.; Bilir S.P.; Kowal S.; Li Q.; Weiss T.; Davies G. Cost-effectiveness of intensification with SGLT2 inhibitors for type 2 diabetes. Am J Manag Care. 2021;27(8):e269-e277. [CrossRef]
- Farcher R.; Graber S.M.; Thüring N.; Blozik E.; Huber C.A. Does the Implementation of an Incentive Scheme Increase Adherence to Diabetes Guidelines? A Retrospective Cohort Study of Managed Care Enrollees. BMC Health Serv Res. 2023;3(1):707. [CrossRef]
- Höglinger M.; Wirth B.; Carlander M.; Caviglia C.; Frei C.; Rhomberg B.; Rohrbasser A.; Trottmann M.; Eichler K. Impact of a diabetes disease management program on guideline-adherent care, hospitalization risk and health care costs: a propensity score matching study using real-world data. Eur J Health Econ. 2023;24(3):469-478. [CrossRef]
- Qumseya B.; Goddard A.; Qumseya A.; Estores D.; Draganov P.V.; Forsmark C. Barriers to Clinical Practice Guideline Implementation among Physicians: A Physician Survey. Int J Gen Med. 2021; 14:7591-8. [CrossRef]
- Lugtenberg M.; Burgers J.S.; Westert G.P. Effects of Evidence-Based Clinical Practice Guidelines on Quality of Care: A Systematic Review. Qual Saf Health Care. 2009;18(5):385-92. [CrossRef]
- Wang W.; Choi D.; Yu C.H. Effective Web-Based Clinical Practice Guidelines Resources: Recommendations from a Mixed Methods Usability Study. BMC Prim Care. 2023;24(1):29. [CrossRef]
- Thomas H.; Mitchell G.; Rich J.; Best M. Definition of Whole Person Care in General Practice in the English Language Literature: A Systematic Review. BMJ Open. 2018;8(12):e023758. [CrossRef]
- Vlacho B.; Simarro F.L.; Mata-Cases M.; Miravet S.; Escribano-Serrano J.; Asensio D.; Cortes X.; Franch-Nadal J. Adherence to antidiabetic treatment among patients managed in primary care centres in Spain: the INTENSE study. Prim Care Diabetes. 2022;16(6):760-767. [CrossRef]
- Dankers M.; van den Berk-Bulsink M.J.E.; van Dalfsen-Slingerland M.; Nelissen-Vrancken H.J.M.G.; Mantel-Teeuwisse A.K.; van Dijk L. Non-Adherence to Guideline Recommendations for Insulins: A Qualitative Study Amongst Primary Care Practitioners. BMC Prim Care. 2022;23(1):150. [CrossRef]
- Holmes-Truscott E.; Blackberry I.; O'Neal D.N.; Furler J.S.; Speight J. Willingness to Initiate Insulin among Adults with Type 2 Diabetes in Australian Primary Care: Results from the Stepping up Study. Diabetes Res Clin Pract. 2016;114:126-35. [CrossRef]
- Albarracin D.; Shavitt S. Attitudes and Attitude Change. Annu Rev Psychol. 2018;69:299-327. [CrossRef]
- Wangler J.; Jansky M. What Is the Significance of Guidelines in the Primary Care Setting? : Results of an Exploratory Online Survey of General Practitioners in Germany. Wien Med Wochenschr. 2021;171(13-14):321-9. [CrossRef]
- Wang T.; Tan J.B.; Liu X.L.; Zhao I. Barriers and Enablers to Implementing Clinical Practice Guidelines in Primary Care: An Overview of Systematic Reviews. BMJ Open. 2023; 13(1):e062158. [CrossRef]
- Rushforth B.; McCrorie C.; Glidewell L.; Midgley E.; Foy R. Barriers to Effective Management of Type 2 Diabetes in Primary Care: Qualitative Systematic Review. Br J Gen Pract. 2016; 66(643):e114-27. [CrossRef]
- Diabetes and Nutrition Study Group (DNSG) of the European Association for the Study of Diabetes (EASD). Evidence-based European recommendations for the dietary management of diabetes. Diabetologia. 2023;66(6):965-85. [CrossRef]
- Cosentino F.; Grant P.J.; Aboyans V.; Bailey C.J.; Ceriello A.; Delgado V.; Federici M.; Filippatos G.; Grobbee D.E.; Hansen T.B.; et al; ESC Scientific Document Group. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020 ;41(2):255-323. [CrossRef]
- McGuire D.K.; Marx N.; Johansen O.E.; Inzucchi S.E.; Rosenstock J.; George J.T.; FDA Guidance on Antihyperglyacemic Therapies for Type 2 Diabetes: One Decade Later. Diabetes Obes Metab 2019;1(5):1073-8. [CrossRef]
- Lundgren J.R.; Janus C.; Jensen S.B.K.; Juhl C.R.; Olsen L.M.; Christensen R.M.; Svane M.S.; Bandholm T.; Bojsen-Møller K.N.; Blond M.B.; et al. Healthy Weight Loss Maintenance with Exercise, Liraglutide, or Both Combined. N Engl J Med. 2021;384(18):1719-1730. [CrossRef]
- Jastreboff A.M.; Aronne L.J.; Ahmad N.N. Wharton S, Connery L, Alves B, Kiyosue A, Zhang S, Liu B, Bunck MC, et al; SURMOUNT-1 Investigators. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387(3):205-216. [CrossRef]
- Khunti K.; Jabbour S.; Cos X.; Mudaliar S.; Mende C.; Bonaca M.; Fioretto P. Sodium-Glucose Co-Transporter-2 Inhibitors in Patients with Type 2 Diabetes: Barriers and Solutions for Improving Uptake in Routine Clinical Practice. Diabetes Obes Metab. 2022;24(7):1187-96. [CrossRef]
- Young K.G.; McInnes E.H.; Massey R.J.; Kahkoska A.R.; Pilla S.J.; Raghavan S.; Stanislawski M.A.; Tobias D.K.; McGovern A.P.; Dawed A.Y.; et al. Treatment Effect Heterogeneity Following Type 2 Diabetes Treatment with GLP1-Receptor Agonists and SGLT2-inibitors: A Systematic Review. Commun Med (Lond). 2023;3(1):131. [CrossRef]
- Melo M.; Gavina C.; Silva-Nunes J.; Andrade L.; Carvalho D. Heterogeneity Amongst GLP-1 RA Cardiovascular Outcome Trials Results: Can Definition of Established Cardiovascular Disease Be the Missing Link? Diabetol Metab Syndr. 2021;13(1):81. [CrossRef]
- Schönberger E.; Mihaljević V.; Steiner K.; Šarić S.; Kurevija T.; Majnarić L.T.; Bilić Ćurčić I.; Canecki-Varžić S. Immunomodulatory Effects of SGLT2 Inhibitors-Targeting Inflammation and Oxidative Stress in Aging. Int J Environ Res Public Health. 2023;20(17). [CrossRef]
- Tilinca M.C.; Tiuca R.A.; Tilea I.; Varga A. The SGLT-2 Inhibitors in Personalized Therapy of Diabetes Mellitus Patients. J Pers Med. 2021;11(12):1249. [CrossRef]
- Grant R.; Adams A.S.; Trinacty C.M.; Zhang F.; Kleinman K.; Soumerai S.B.; Meigs J.B.; Ross-Degnan D. Relationship between Patient Medication Adherence and Subsequent Clinical Inertia in Type 2 Diabetes Glycemic Management. Diabetes Care. 2007;30(4):807-12. [CrossRef]
- Khunti K.; Aroda V.R.; Bhatt D.L.; Bozkurt B.; Buse J.B.; Heerspink H.L.; Inzucchi S.E.; Lam C.S.P.; Marx N.; McMurray J.J.V.; et al. Re-examining the widespread policy of stopping sodium-glucose cotransporter-2 inhibitors during acute illness: A perspective based on the updated evidence. Diabetes Obes Metab. 2022;24(11):2071-80. [CrossRef]
- Faillie JL. Pharmacological aspects of the safety of gliflozins. Pharmacol Res. 2017;118:71-81. [CrossRef]
- Bechmann L.E.; Emanuelsson F.; Nordestgaard B.G.; Benn M. SGLT2-inibition increases total, LDL, and HDL cholesterol and lowers triglycerides: Meta-analyses of 60 randomized trials, overall and by dose, ethnicity, and drug type. Atherosclerosis. 2023:117236. [CrossRef]
- Castellana M.; Procino F.; Sardone R.; Trimboli P.; Giannelli G. Generalizability of Sodium-Glucose Co-Transporter-2 Inhibitors Cardiovascular Outcome Trials to the Type 2 Diabetes Population: A Systematic Review and Meta-Analysis. Cardiovasc Diabetol. 2020;19(1):87. [CrossRef]
- Schnell O.; Battelino T.; Bergenstal R.; Birkenfeld A.L.; Ceriello A.; Cheng A.; Davies M.; Edelman S.; Forst T.; Giorgino F.; et al. CVOT Summit 2022 Report: new cardiovascular, kidney, and glycemic outcomes. Cardiovasc Diabetol. 2023;22(1):59. [CrossRef]
- Goldman A.; Fishman B.; Twig G.; Raschi E.; Cukierman-Yaffe T.; Moshkovits Y.; Pomerantz A.; Ben-Zvi I.; Dankner R.; Maor E. The real-world safety profile of sodium-glucose co-transporter-2 inhibitors among older adults (≥ 75 years): a retrospective, pharmacovigilance study. Cardiovasc Diabetol. 2023;22(1):16. [CrossRef]
- Lugtenberg M.; Zegers-van Schaick J.M.; Westert G.P.; Burgers J.S. Why Don't Physicians Adhere to Guideline Recommendations in Practice? An Analysis of Barriers among Dutch General Practitioners. Implement Sci. 2009;4:54. [CrossRef]
- Morley J.E.; Abbatecola A.M.; Woo J. Management of comorbidities in older persons with type 2 diabetes. J. Am. Med. Dir Assoc. 2017;18(8):639–45. [CrossRef]
- Nguyen T.N.; Harris K.; Woodward M.; Chalmers J.; Cooper M.; Hamet P.; Harrap S.; Heller S.; MacMahon S.; Mancia G.; et al. The Impact of Frailty on the Effectiveness and Safety of Intensive Glucose Control and Blood Pressure-Lowering Therapy for People With Type 2 Diabetes: Results From the ADVANCE Trial. Diabetes Care. 2021;44(7):1622-1629. [CrossRef]
- Strain W.D.; Down S.; Brown P.; Puttanna A.; Sinclair A. Diabetes and Frailty: An Expert Consensus Statement on the Management of Older Adults with Type 2 Diabetes. Diabetes Ther. 2021;12(5):1227-47. [CrossRef]
- Abd Ghafar M.Z.A.; O'Donovan M.; Sezgin D.; Moloney E.; Rodríguez-Laso Á.; Liew A.; O'Caoimh R. Frailty and Diabetes in Older Adults: Overview of Current Controversies and Challenges in Clinical Practice. Front Clin Diabetes Healthc. 2022;3:895313. [CrossRef]
- Kondo T.; Adachi T.; Kobayashi K.; Okumura T.; Izawa H.; Murohara T.; et al. Physical Frailty and Use of Guideline-Recommended Drugs in Patients with Heart Failure and Reduced Ejection Fraction. J Am Heart Assoc. 2023;12(12):e026844. [CrossRef]
- Fried L.P.; Tangen C.M.; Walston J.; Newman A.B.; Hirsch C.; Gottdiener J.; Seeman T.; Tracy R.; Kop W.J.; Burke G.; et al; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146-56. [CrossRef]
- Nixon A.C.; Bampouras T.M.; Pendleton N.; Woywodt A.; Mitra S.; Dhaygude A.; Frailty and Chronic Kidney Disease: Current Evidence and Continuing Uncertainties. Clin Kidney J. 2018;11(2):236-45. [CrossRef]
- Kleipool E.E.; Hoogendijk E.O.; Trappenburg M.C.; Handoko M.L.; Huisman M.; Peters M.J.; Muller M. Frailty in Older Adults with Cardiovascular Disease: Cause, Effect or Both? Aging Dis. 2018;9(3):489-97. [CrossRef]
- Abdelhafiz A.H.; Emmerton D., Sinclair A.J. Impact of Frailty Metabolic Phenotypes on the Management of Older People with Type 2 Diabetes Mellitus. Geriatr Gerontol Int. 2021;21(8):614-22. [CrossRef]
- Gordon E.H.; Peel N.M.; Samanta M.; Theou O.; Howlett S.E.; Hubbard R.E. Sex Differences in Frailty: A Systematic Review and Meta-Analysis. Exp Gerontol. 2017;89:30-40. [CrossRef]
- Cohen A.A.; Legault V.; Li Q.; Fried L.P.; Ferrucci L. Men Sustain Higher Dysregulation Levels Than Women without Becoming Frail. J Gerontol A Biol Sci Med Sci. 2018;73(2):175-84. [CrossRef]
- Wang Y.; O'Neil A.; Jiao Y.; Wang L.; Huang J.; Lan Y.; Zhu Y.; Yu C. Sex differences in the association between diabetes and risk of cardiovascular disease, cancer, and all-cause and cause-specific mortality: a systematic review and meta-analysis of 5,162,654 participants. BMC Med. 2019;17(1):136. [CrossRef]
- Denfeld Q.E.; Habecker B.A.; Camacho S.A.; Roberts Davis M.; Gupta N.; Hiatt S.O.; Medysky M.E.; Purnell J.Q.; Winters-Stone K.; Lee C.S. Characterizing Sex Differences in Physical Frailty Phenotypes in Heart Failure. Circ Heart Fail. 2021;14(9):e008076. [CrossRef]
- Lin T.K.; Lee M.C.; Cheng Y.H.; Ma T.; Chen M.C.; Yang T.Y.; Jong G.P. The Association between SGLT2 Inhibitors and New-Onset Acute Coronary Syndrome in the Elderly: A Population-Based Longitudinal Cohort Study. Diabetol Metab Syndr. 2023;15(1):170. [CrossRef]
- Leong D.P.; Joseph P.; McMurray J.J.V.; Rouleau J.; Maggioni A.P.; Lanas F.; Sharma S.K.; Núñez J.; Mohan B.; Celik A.; et al. Frailty and outcomes in heart failure patients from high-, middle-, and low-income countries. Eur Heart J. 2023;44(42):4435-4444. 4435. [CrossRef]
- Kutz A.; Kim D.H.; Wexler D.J.; Liu J.; Schneeweiss S.; Glynn R.J.; Patorno E. Comparative Cardiovascular Effectiveness and Safety of SGLT-2 Inhibitors, GLP-1 Receptor Agonists, and DPP-4 Inhibitors According to Frailty in Type 2 Diabetes. Diabetes Care. 2023;46(11):2004-14. [CrossRef]
- Strain W.; Griffiths J. A Systematic Review and Meta-Analysis of the Impact of GLP-1 Receptor Agonists and SGLT-2 Inhibitors on Cardiovascular Outcomes in Biologically Healthy Older Adults. The British Journal of Diabetes. 2021;21(1). [CrossRef]
- Karagiannis T.; Tsapas A.; Athanasiadou E.; Avgerinos I.; Liakos A.; Matthews D.R.; Bekiari E. GLP-1 Receptor Agonists and SGLT2 Inhibitors for Older People with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Diabetes Res Clin Pract. 2021;174:108737. [CrossRef]
- Vart P.; Butt J.H.; Jongs N.; Schechter M.; Chertow G.M.; Wheeler D.C.; Pecoits-Filho R.; Langkilde A.M.; Correa-Rotter R.; Rossing P.; et al. Efficacy and Safety of Dapagliflozin in Patients With Chronic Kidney Disease Across the Spectrum of Frailty. J Gerontol A Biol Sci Med Sci. 2024;79(2):glad181. [CrossRef]
- Chung W.K., Erion K., Florez J.C.; Hattersley A.T.; Hivert M.F.; Lee C.G.; McCarthy M.I.; Nolan J.J.; Norris J.M.; Pearson E.R.; et al. Precision medicine in diabetes: a Consensus Report from the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia. 2020;63(9):1671-1693. [CrossRef]
- Griffin S. Diabetes precision medicine: plenty of potential, pitfalls and perils but not yet ready for prime time. Diabetologia. 2022;65(11):1913-21. [CrossRef]
- Bosnić Z.; Yildirim P.; Babič F.; Šahinović I.; Wittlinger T.; Martinović I.; Majnaric L.T.; Clustering Inflammatory Markers with Sociodemographic and Clinical Characteristics of Patients with Diabetes Type 2 Can Support Family Physicians' Clinical Reasoning by Reducing Patients' Complexity. Healthcare (Basel). 2021;9(12). [CrossRef]
- Bosnić Z.; Babič F.; Anderková V.; Štefanić M.; Wittlinger T.; Majnarić L.T. A Critical Appraisal of the Diagnostic and Prognostic Utility of the Anti-Inflammatory Marker IL-37 in a Clinical Setting: A Case Study of Patients with Diabetes Type 2. Int J Environ Res Public Health. 2023;20(4). [CrossRef]
- Bosnić Z.; Babič F.; Wittlinger T.; Anderková V.; Šahinović I.; Majnarić L.T. Influence of Age, Gender, Frailty, and Body Mass Index on Serum IL-17a Levels in Mature Type 2 Diabetic Patients. Med Sci Monit. 2023:29:e940128. [CrossRef]
- Zoungas S.; Woodward M.; Li Q.; Cooper M.E.; Hamet P.; Harrap S.; Heller S.; Marre M.; Patel A.; Poulter N.; et al; ADVANCE Collaborative group. Impact of age, age at diagnosis and duration of diabetes on the risk of macrovascular and microvascular complications and death in type 2 diabetes. Diabetologia. 2014;57(12):2465-74. [CrossRef]
- Matsushita K.; Kaptoge S.; Hageman S.H.J.; Sang Y.; Ballew S.H.; Grams M.E.; Surapaneni A.; Sun L.; Arnlov J.; Bozic M.; et al. Including measures of chronic kidney disease to improve cardiovascular risk prediction by SCORE2 and SCORE2-OP. Eur J Prev Cardiol. 2023;30(1):8-16. [CrossRef]
- de Boer I.H.; Khunti K.; Sadusky T.; Tuttle K.R.; Neumiller J.J.; Rhee C.M.; Rosas S.E.; Rossing P.; Bakris G. Diabetes management in chronic kidney disease: a consensus report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2022;102(5):974-989. [CrossRef]
- SCORE2-Diabetes Working Group and the ESC Cardiovascular Risk Collaboration, SCORE2-Diabetes: 10-year cardiovascular risk estimation in type 2 diabetes in Europe. European Heart Journal. 2023;44(28):2544-56. [CrossRef]
- Cebrián-Cuenca A.M.; Mata-Cases M.; Franch-Nadal J.; Mauricio D.; Orozco-Beltrán D.; Consuegra-Sánchez L. Half of patients with type 2 diabetes mellitus are at very high cardiovascular risk according to the ESC/EASD: data from a large Mediterranean population. Eur J Prev Cardiol. 2022;28(18):e32-e34. [CrossRef] [PubMed]
- Galbete A.; Tamayo I..; Librero J.; Enguita-Germán M.; Cambra K.; Ibáñez-Beroiz B.; CONCEPT group. Cardiovascular risk in patients with type 2 diabetes: A systematic review of prediction models. Diabetes Res Clin Pract. 2022;184:109089. [CrossRef]
- Dziopa K.; Asselbergs F.W.; Gratton J.; Chaturvedi N.; Schmidt A.F. Cardiovascular Risk Prediction in Type 2 Diabetes: A Comparison of 22 Risk Scores in Primary Care Settings. Diabetologia. 2022;65(4):644-56. [CrossRef]
- Rydén L.; Ferrannini G.; Standl E. Risk prediction in patients with diabetes: is SCORE 2D the perfect solution? Eur Heart J. 2023;44(28):2557-2559. [CrossRef]
- Fang M.; Wang D.; Tang O.; McEvoy J.W.; Echouffo-Tcheugui J.B.; Christenson R.H.; Selvin E. Subclinical Cardiovascular Disease in US Adults With and Without Diabetes. J Am Heart Assoc. 2023;12(11):e029083. [CrossRef]
- De Rosa S.; Arcidiacono B.; Chiefari E.; Brunetti A.; Indolfi C.; Foti DP. Type 2 Diabetes Mellitus and Cardiovascular Disease: Genetic and Epigenetic Links. Front Endocrinol (Lausanne). 2018;9:2. [CrossRef]
- van Bussel E.F.; Richard E.; Busschers W.B.; Steyerberg E.W.; van Gool W.A.; Moll van Charante E.P.; Hoevenaar-Blom M.P. A Cardiovascular Risk Prediction Model for Older People: Development and Validation in a Primary Care Population. J Clin Hypertens (Greenwich). 2019;21(8):1145-52. 1145. [CrossRef]
- van Bussel E.F.; Hoevenaar-Blom M.P.; Poortvliet R.K.E.; Gussekloo J.; van Dalen J.W.; van Gool W.A.; Richard E.; Moll van Charante E.P. Predictive value of traditional risk factors for cardiovascular disease in older people: A systematic review. Prev Med. 2020;132:105986. [CrossRef]
- Madonna R.; Balistreri C.R.; De Rosa S.; Muscoli S.; Selvaggio S.; Selvaggio G.; Ferdinandy P.; De Caterina R. Impact of Sex Differences and Diabetes on Coronary Atherosclerosis and Ischemic Heart Disease. J Clin Med. 2019;8(1):98. [CrossRef]
- Frisoli A. Jr.; Ingham S.J.; Paes Â.T.; Tinoco E.; Greco A.; Zanata N.; Pintarelli V.; Elber I.; Borges J.; Camargo Carvalho A.C. Frailty predictors and outcomes among older patients with cardiovascular disease: Data from Fragicor. Arch Gerontol Geriatr. 2015;61(1):1-7. [CrossRef]
- Khoury M.J.; Galea S. Will Precision Medicine Improve Population Health? JAMA. 2016;316(13):1357-8. [CrossRef]
- Franceschi C.; Garagnani P.; Morsiani C.; Conte M.; Santoro A.; Grignolio A.; Monti D.; Capri M.; Salvioli S. The Continuum of Aging and Age-Related Diseases: Common Mechanisms but Different Rates. Front Med (Lausanne). 2018;5:61. [CrossRef]
- Chaturvedi R.R.; Angrisani M.; Troxel W.M.; Gutsche T.; Ortega E.; Jain M.; Boch A.; Kapteyn A. American Life in Realtime: a benchmark registry of health data for equitable precision health. Nat Med. 2023;29(2):283-286. [CrossRef]
- Majnarić L.T.; Babič F.; O'Sullivan S.; Holzinger A. AI and Big Data in Healthcare: Towards a More Comprehensive Research Framework for Multimorbidity. J Clin Med. 2021;10(4). [CrossRef]
Figure 1.
The overlap rates among the eligible patients for treatment with GLP-1ra or SGLT2inh. The results from our research (N=170, F: M = 95:75, age 50–89 years, median 66). The simplified criteria for prescribing GLP-1ra or SGLT2inh: C1: Atherosclerotic CVD (Coronary artery disease, or Periphery artery disease, or Cerebrovascular disease); C2: Age ≥55 years + chronic heart disease; C3: estimated glomerular filtration rate (eGFR) < 60 ml/min).
Figure 1.
The overlap rates among the eligible patients for treatment with GLP-1ra or SGLT2inh. The results from our research (N=170, F: M = 95:75, age 50–89 years, median 66). The simplified criteria for prescribing GLP-1ra or SGLT2inh: C1: Atherosclerotic CVD (Coronary artery disease, or Periphery artery disease, or Cerebrovascular disease); C2: Age ≥55 years + chronic heart disease; C3: estimated glomerular filtration rate (eGFR) < 60 ml/min).
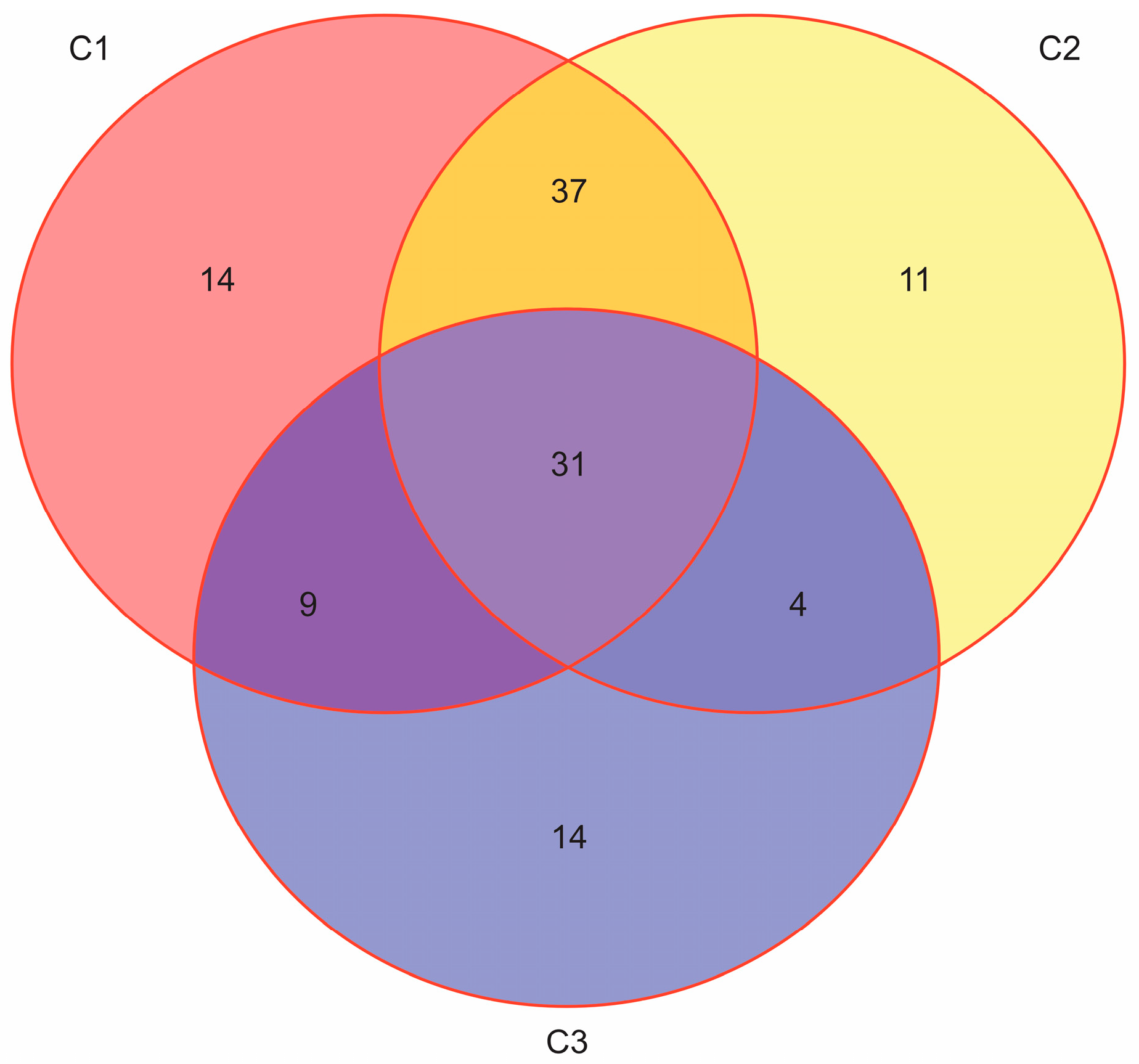
Figure 2.
Distribution of patients with T2D and diagnosed with CVD (red: no CAD or CHD; blue: both CAD and CHD; green: only CHD; red: only CAD) according to frailty status (A: nonfrail, B: pre-frail, C: frail); Fisher Test p-value (0.003). The results from our research (N=170, F: M = 95:75, age 50–89 years, median 66).
Figure 2.
Distribution of patients with T2D and diagnosed with CVD (red: no CAD or CHD; blue: both CAD and CHD; green: only CHD; red: only CAD) according to frailty status (A: nonfrail, B: pre-frail, C: frail); Fisher Test p-value (0.003). The results from our research (N=170, F: M = 95:75, age 50–89 years, median 66).
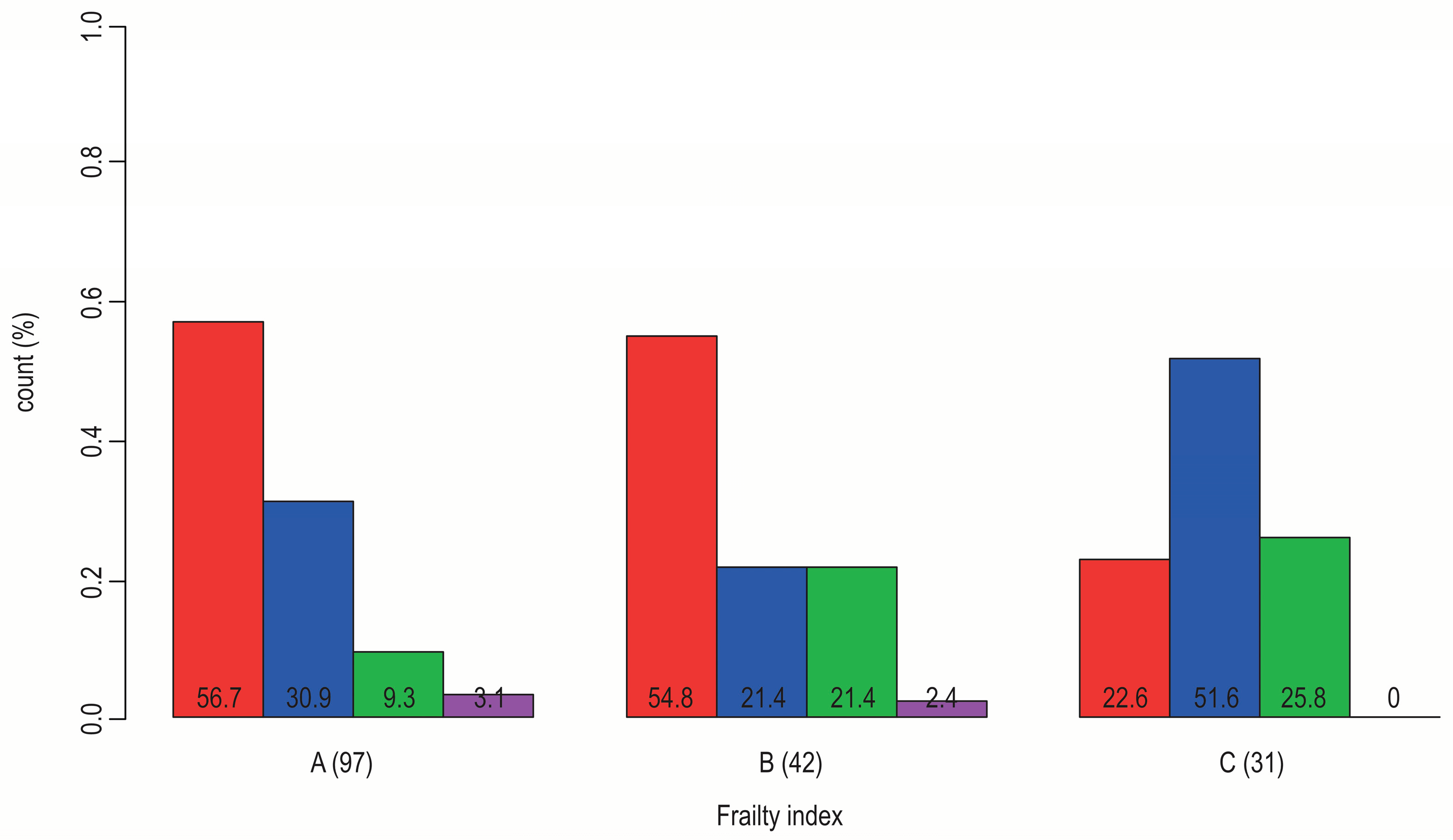
Figure 3.
Sex-dependent distribution (blue: men, red: women) of patients with T2D according to their frailty status (A: nonfrail, B: pre-frail, C: frail); Pearson Chi-Square (p-value = 0.02). The results from our research (N=170, F: M = 95:75, age 50–89 years, median 66).
Figure 3.
Sex-dependent distribution (blue: men, red: women) of patients with T2D according to their frailty status (A: nonfrail, B: pre-frail, C: frail); Pearson Chi-Square (p-value = 0.02). The results from our research (N=170, F: M = 95:75, age 50–89 years, median 66).
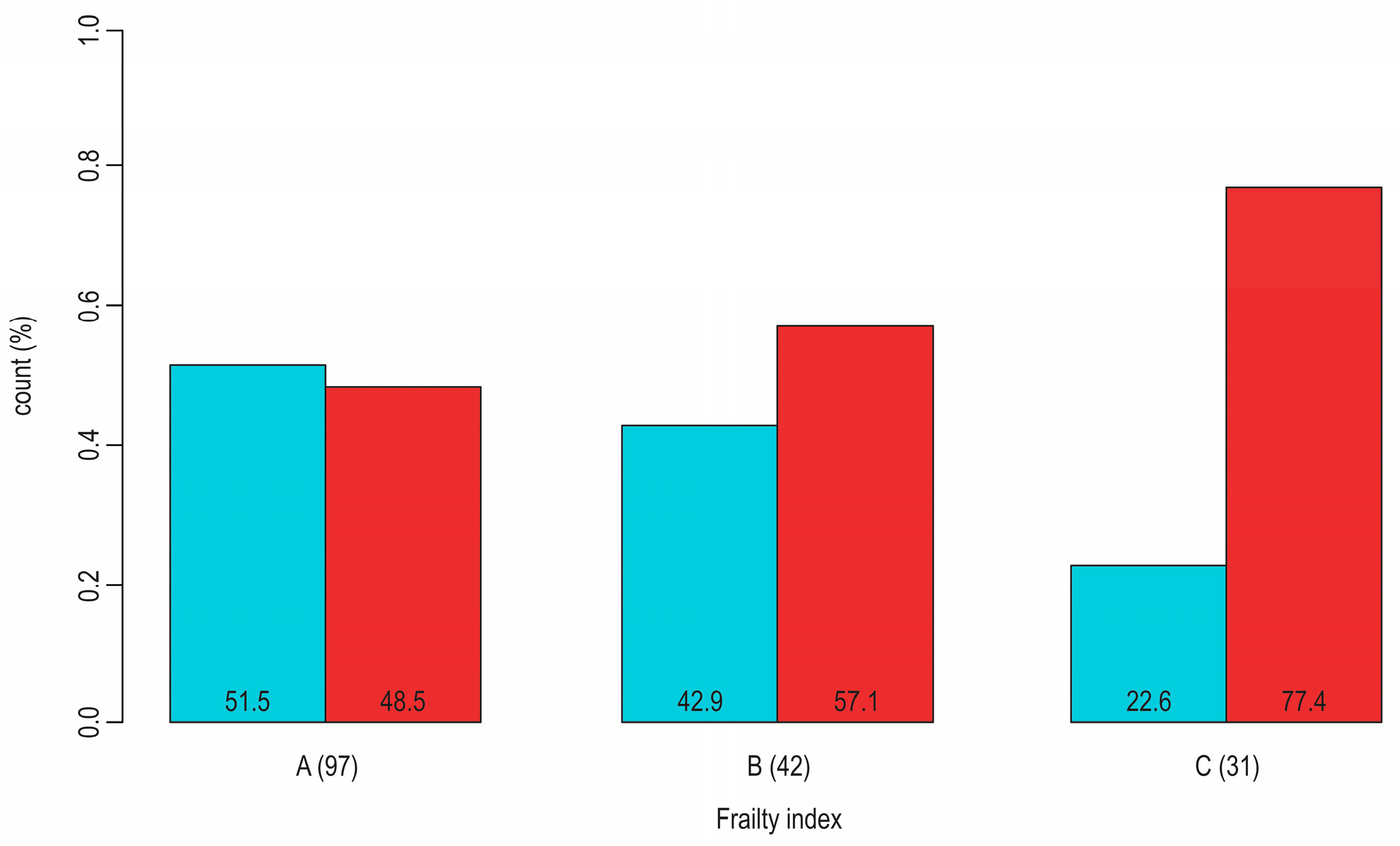

Table 1.
Factors influencing therapeutic/clinical inertia.
| Physician-related factors: | Patient-related factors: | Healthcare-related factors: |
|---|---|---|
| Lack of knowledge about the illness Overlooking the seriousness of the symptoms Not starting the treatment Inability to identify clinical outcomes Not adjusting the treatment until the intended result has been attained Inability to recognize and address comorbid condition Patient takes over the therapeutic discussion and decision Lack of knowledge about the illness Reactive care as opposed to a proactive treatment strategy |
Refuse to accept having the illness Non-existence of symptoms Inadequate knowledge regarding the health Considering that the illness is not severe Taking too many medications Financial limitation (cost of medications) The negative effects of medications Aspects of lifestyle Ineffective patient-doctor communication (lack of trust) |
The absence of clinical guidelines No database of morbidity or illness registries No visit strategy (not scheduling appointments) Absence of decision assistance and team-based careInsufficient funds and time Technical deficiency |
Table 2.
Possible side effects and heterogeneous treatment effects for SGLT2-in and GLP-1ra.
| Heterogeneous treatment effects | Possible side effects |
|---|---|
|
Higher baseline HbA1c values are associated with greater glycaemic response. GLP-1ra: there is no proof that renal function affects the response to glucose; SGLT2-in: lessened glycaemic response in patients with diminished kidney function. There isn't any reliable proof that body mass index significantly modifies the glycaemic response. GLP-1ra: less glycaemic response is linked to longer duration of diabetes; SGLT2-in: the length of diabetes does not consistently affect glycaemic response. GLP-1ra: no proof that aging affects glycaemic response; SGLT2-in: some research indicates that an older age may be linked to a lower glycaemic response. No reliable proof that gender or ethnicity significantly modifies the glycaemic response. SGLT2-in: no indication of variation in the reaction to treatment for patients with obstructive sleep apnea or for insulin secretion and insulin; GLP-1ra: studies indicate that lower fasting C-peptide and lower urine C-peptide-to-creatinine ratio, are linked to a reduced glycaemic response. |
Concerns regarding the start of SGLT2-in in patients with CVD or kidney illness, as well as the necessity of close observation of diabetic ketoacidosis (DKA) in cases of COVID-19 or other acute conditions requiring hospitalization. There is a higher risk of genital and urinary tract infections, which can be attributed to prolonged and increased glycosuria. Raised concerns about gliflozin-induced cancers (bladder and breast cancer), even though causality cannot be established. More research is required. Gliflozins cannot rule out drug-induced liver damage. Due to SGLT1 transporters' reduced inhibition there may be a lower risk of severe hypoglycemia when using gliflozins. Hypovolemic events are frequent with gliflozins and DKA can appear infrequently and be more challenging to diagnose. Gliflozins-associated fracture risk is likely influenced by a number of variables that require additional research. Symptoms of glucose-galactose malabsorption were uncommon in clinical trials. Renal function needs to be regularly monitored due to a possible reduction in GFR. Elderly patient and with renal impairment should use much more caution. There is a link to a greater rise in the less atherogenic significant LDL-C subfraction. The ratio of LDL-C to HDL-C remains nearly unaltered because of a concurrent rise in HDL-C. |
Table 3.
A list of studies indicating the effect of older age and/or frailty on treatment effects with GLP-1ra and SGLT-2-in in patients with T2D.
Table 3.
A list of studies indicating the effect of older age and/or frailty on treatment effects with GLP-1ra and SGLT-2-in in patients with T2D.
| Study (design) |
Findings summary |
|---|---|
| Lin TK, et al., 2023. (population-based longitudinal cohort study) [74] |
SGLT2-in use was associated with a non-significantly decreased risk of ACS. No difference in the SGLT2-in subtype was observed in subgroup analyses. The results indicated an increased risk for the incidence of ACS in male and older (> 70 years) patients. |
| Leong DP, et al., 2023. (population-based longitudinal cohort study) [75] |
Frailty confers substantial incremental prognostic information to prognostic variables for predicting death and hospitalization in heart failure patients. The relationship between frailty and these outcomes is consistent across countries at all income levels. |
| Kutz A, et al, 2023. (1:1 propensity score-matched cohort studies) [76] |
SGLT2-in and GLP-1ra safely improved CV outcomes and all-cause mortality, with the largest absolute benefits among frail people. |
|
Young KG, et al., 2023. (a systematic review) [49] |
Current evidence on treatment effect heterogeneity for SGLT2-in and GLP-1ra therapies is limited, likely reflecting the methodological limitations of published studies. Robust and appropriately powered studies are required to understand T2D treatment effect heterogeneity. |
| Strain WD, Griffiths J, 2021. (a systematic review and meta-analysis) [77] |
GLP-1ra and SGLT2-in reduced MACE outcomes in older adults who were eligible to participate in clinical trials. Whereas this is reassuring for the biologically robust, it should not be extrapolated to frail older adults without further investigation. |
|
Karagiannis T, et al., 2021. (a systematic review and meta-analysis) [78] Vart P, et al., 2023. (a randomized controlled trial) [79] |
In older adults (≥65) with T2D, GLP-1ra reduced MACE and its components. SGLT2-in reduced MACE, heart failure, and renal outcomes. The relative benefit of dapagliflozin in patients with chronic kidney disease (with/without T2D) for all outcomes was consistent across all frailty categories, with no difference in associated safety. |
ACS: acute coronary syndrome; MACE: major cardiovascular event; T2D: type 2 diabetes; CV: cardiovascular; HF: heart failure.
Table 4.
Future directions for overcoming T2D patient heterogeneity and increasing uptake of GLP-1ra and SGLT2-in drugs.
Table 4.
Future directions for overcoming T2D patient heterogeneity and increasing uptake of GLP-1ra and SGLT2-in drugs.
| Research | Guidelines development | Knowledge implementation |
|---|---|---|
| More comprehensive patient profiling for CVOTs Real-world data-driven research Patient clustering based on multiple descriptors (including comorbidity patterns) Research intensification on the treatment effects of non-pharmacological interventions, in particular including psychological factors New biomarkers exploration Integrated models of care Qualitative research – assessing family doctors` attitudes Translation research intensification |
Clear division of areas where there is no support by evidence Case report, Examples dealing with real-life experience Monitoring for the side effects of the treatment regimens The effects of comorbidity and frailty on treatment outcomes Evidence provided by cluster-analyses Clear recommendations on when to intensify and when to de-escalate therapy Clear statements on when to start with the cardio-protective therapy in the course of the disease The effects on outcomes of non-pharmacological interventions, in particular, concerning psychological factors Problem-solving approach Guidelines adaptation for use in primary care |
Continuous knowledge translation Educational training modules for healthcare providers, health policy officials, and patients Learning on case reports Audit analysis of real-world data with the support of information technology Implementation of care protocols and workflows Empowerment of family doctors in life science knowledge The establishment of the platform for data collection and curation from electronic health records, smartphones, and wearables; Data selection for data-driven modeling The results of data modeling become visible in the workplace by using AI visual techniques |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



