
Submitted:
27 February 2024
Posted:
28 February 2024
You are already at the latest version
Abstract
Thromboprophylaxis of hospitalized patients at risk of venous thromboembolism (VTE) presents challenges owing to patient heterogeneity and lack of adoption of evidence-based methods. Intuitive practices for thromboprophylaxis have resulted in many patients being inappropriately prophylaxed. Multiple interventions for thromboprophylaxis have been tested, including use of multifaceted approaches such as national VTE prevention programs with audits, use of passive alerts (either human or electronic), and more recently use of active clinical decision support (CDS) tools incorporated into electronic health records (EHRs). Multifaceted health-system interventions have shown mixed results in their ability to increase appropriate thromboprophylaxis and reduce VTE, unless mandated through a national VTE prevention program, though the latter approach is potentially costly, effort- and time-dependent. Studies utilizing passive human or electronic alerts have also shown mixed results in increasing appropriate thromboprophylaxis and reducing VTE. The use of active CDS tools holds the greatest promise, especially with further refinement and widespread implementation within various EHRs and clinical workflows. Recent-ly a universal cloud-based and EHR-agnostic CDS VTE tool revealed high adoption and effectiveness in increasing appropriate thromboprophylaxis and reducing major thromboembolism. This narrative review summarizes the literature on system-wide thromboprophylaxis interventions in hospitalized patients, with a focus on CDS tools.
Keywords:
Venous Thromboembolism
; Clinical Decision Support Tools
; Thromboprophylaxis
; Hospitalized Patients
; Electronic Health Records
1. Introduction
Venous Thromboembolism (VTE), encompassing deep vein thrombosis (DVT) and pulmonary embolism (PE), is the third most common cause of cardiovascular mortality [1] and substantially increases morbidity worldwide [2]. Approximately 60% of all VTE events are associated with a recent hospital admission, with the majority of VTE events - including most fatal PE - occurring in medical inpatients [3]. At the same time, VTE is associated with increased healthcare expenditure, especially in US healthcare systems [4,5].
Thromboprophylaxis of hospitalized patients necessitates complex clinical management strategies that incorporate both patient-specific and disease-specific risk factors [6]. VTE risk models in surgical and medical patients have now undergone extensive external validation, including the Caprini VTE risk score in surgical patients and the Padua, IMPROVE, and IMPROVE-DD VTE scores in medical patients [7,8,9]. However, decreased average hospital length of stay, especially among medical inpatients (4-5 days) both in the US and other advanced health systems has dampened the treatment effects of in-hospital thromboprophylaxis [8,10], with <4% of hospitalized patients receiving any form of post-discharge thromboprophylaxis [11].
Although antithrombotic clinical practice guidelines have given clear recommendations on the need for anticoagulant thromboprophylaxis in at-VTE-risk hospitalized patients [3,6,12,13], current hospital-wide thromboprophylaxis using systematic and evidence-based approaches remain sub-par [7,14,15,16,17]. Factors for underuse of evidence-based approaches include the complexity of appropriate clinical management, the lack of incorporation of validated VTE risk models into clinical care pathways [18], and both underutilization of thromboprophylaxis in high VTE-risk patients due to concerns of bleeding, and overutilization of thromboprophylaxis in low VTE-risk patients in the absence of formal VTE risk stratification [18,19].
Multiple approaches to improve uptake of appropriate thromboprophylaxis in hospitalized patients have been assessed: quality improvement programs that include educational activities and audits, national VTE prevention programs [20,21,22], passive human or electronic alert systems using clinical rules [23,24]; and more recently, active and computerized clinical decision support (CDS) tools [25]. CDS rules and algorithms have included digital, paper-based, or in-person modalities, or multimodal approaches [20,21]. More recently a cloud-based and EHR-agnostic universal CDS tool incorporating a validated VTE risk model in hospitalized medical patients has been developed [26].
This narrative review will discuss various system-wide thromboprophylaxis interventions for hospitalized patients, with a focus on cross-platform CDS tools embedded into EHRs. The review will also outline evolving patterns in the literature that contribute to shaping future iterations of these tools, highlighting practices that are evidence-based and patient-centered.
2. Methods
Literature searches of the MEDLINE database were iteratively undertaken during the initial drafting of this paper, looking for relevant articles published between 1990 and 2023 with the following keywords and MeSH terms: “Venous Thromboembolism”, “thromboprophylaxis”, “risk assessment”, “clinical decision support”, “computerized systems”, “human alerts”, “paper-based systems”, “quality improvement”, “hospitalized patients” and “major bleeding”. Observational studies and randomized controlled trials on the topic of a system-of-care approach to VTE prevention in hospitalized patients were included, as were meta-analyses and systematic reviews. Observational studies with fewer than 500 patients and randomized controlled trials with fewer than 100 patients were excluded.
3. Results
As shown in the Table, there were 26 studies that met criteria across four types of system-wide approaches for thromboprophylaxis in hospitalized patients: multifaceted interventions, use of pre-printed order sets, passive alerts (human or electronic), and active CDS tools.

| Study | Type | P | I | C | Risk model | O |
|---|---|---|---|---|---|---|
| Multifaceted | ||||||
| Anderson 1994 N = 798 |
Cluster RCT |
Medical and surgical |
CME only: grand rounds slide lecture with local data by physician expert + mailed materials + telephone line for immediate VTE consults. CME + QA: additionally, data from manual retrospective chart reviews reported at medical staff meetings, individual physician feedback concerning compliance. | Usual care |
Generic screening for the selection of high-risk patients and adequate thromboprophylaxis rates. Generic risk factor screening. | Changes in prophylaxis among the control, CME, and CME + QA hospitals maintained significance. Multivariate adjusted odds ratios were 2.1 (95% confidence limits, 1.6,2.9) for control hospitals, 3.6 (95% confidence limits, 2.7,4.7) for CME hospitals, and 3.8 (95% confidence limits, 2.9,5.0) for CME+QA hospitals. |
| Streubel 2009 N = 345 |
Pretest-posttest | Surgical | Prospective VTE protocol adherence and event rate monitoring. Results presented every two months. | Usual care |
N/A | VTE prophylaxis adherence failure reduction: 15% vs 1.6% (P = 0.002), VTE rates trend for improvement (P = 0.37). |
| Labarere 2007 N = 812 |
Cluster RCT |
Medical | Educational presentations with local data, educational material, audit/feedback components directed at physicians and nurses. | Physicians only | Evidence derived, non-validated | No significant differences in radiology-verified DVT (two-level OR, 1.21; 95% CI, 0.70 – 2.11; P = 0.50; intra-cluster correlation coefficient, 0.08). |
| Hinchey 2010 N = 2071 |
Cluster, Quasi-RCT |
Medical | Audit, feedback and benchmark information along with site-selected components from the below: evidence synthesis as educational resource, alerts, standing orders, grand round reporting of audits, individualized clinician feedback. Knowledge and attitude, barrier to adherence audit and discussion, with suggestions for improvement. | Audit with feedback | Unknown | Nonsignificant trend for appropriate thromboprophylaxis - no more data available. Extracted from figure with web plot digitizer (apps.automeris.io/wpd/): Intervention baseline 79%, outcome 87.1%. Control: baseline, 81%utcome, 86%. |
| Pai 2013 N = 2611 |
Pilot cluster RCT | Medical | Paper based VTE risk assessment forms, educational sessions and material for all staff, real-time chart audits within 24h of admission used for instructional feedback at 4, 12 and 16 weeks. | Usual care | non-validated, evidence derived ACCP 8th ed. | No significant difference in appropriate thromboprophylaxis, over- or under-prescription rates. Significant qualitative components: interviews and questionnaires of stakeholders, including patients. No significant difference rates of appropriate thromboprophylaxis between groups was found (OR = 0.80; 95% CI: 0.50, 1.28; P = 0.36). |
| Cavalcanti 2016 N = 6761 |
Cluster RCT | Medical and Surgical | Goals of care discussions at ICU level. Daily Checklist in daily grand rounds with single item confirming thromboprophylaxis orders. Online and offline education. Involvement of the whole clinical team. Checklist adherence feedback. Periodic text message reminders. Directors contacted when adherence was low. | Usual care | N/A | VTE prophylaxis rates 74.8% vs 75.0% of patient-days; adjusted RR, 1.05; 95% CI, 0.91-1.22; P = 0.5 favoring intervention. |
| Roy 2016 N = 15351 |
Cluster RCT | Medical | Educational lectures, educational resources. In a second phase, a CDSS with alerts incorporating medical diagnosis code for risk stratification and tailored thromboprophylaxis suggestions used in only 2 of 13 centers. | Usual care | Non-validated | No difference in VTE/major bleeding composite, thromboembolic events, major bleeding, and all-cause mortality. Thromboprophylaxis rates post-intervention similar between groups. Adjusted difference in thromboprophylaxis rates: 6.6% [1.6-11.6] favoring intervention. |
| Roberts 2017 NHS Centers in UK |
Observational pretest-posttest | Medical and surgical | See text. | Usual care | Paper-based, non-validated, evidence-derived national tool- lists of risk factors. | Median risk assessment rate 2010: 51% (IQR 27-71%), March 2012: 93% (IQR 91-96%). Hospitals with >90% assessment rate: 15% reduction in hospital associated thrombosis, 12% lower avoidable VTE, VTE related mortality reduction post-discharge: 15% for >3 days hospitalizations (95% CI 0.75-0.96), 39% for <3 days hospitalizations (CI 0.48-0.79), excluding outpatient. 90-day readmissions with VTE: 4% reduction, secondary VTE diagnosis: 9%reduction, mean mortality rate: 9% reduction, maintained at 8% less than 2012 estimates, long-term data unavailable. |
| Pre-Printed Order Sheets | ||||||
| Fontaine et al. 2006 N = 719 |
Cluster RCT | Medical | Evidence-derived, locally compiled thromboprophylaxis prescription guidelines. Anonymous anticoagulant prescription forms including patient characteristics (age, sex, body weight, date of admission), presence or absence of venous thromboembolic risk factors, 10 cm visual analogical scale of the patient’s risk of anticoagulation and hemorrhagic complications risk. | Usual care | Non-validated, evidence derived, weighted risk factor based | Overprophylaxis increased by 17% (from 22 to 26%) in the control group and decreased by 44% (from 25% to 15%) in the intervention group. Appropriate thromboprophylaxis rates were similar (around 63%) before and after the intervention. No differences in undertreatment, with both groups showing minor reductions. |
| Passive Alerts (Human or Electronic) | ||||||
| Dexter 2001 N = 1326 |
Cluster RCT | Medical | EHR order entry CDS providing rule-based reminders and prewritten orders with explanatory text. Rules integrated the demographics, EHR codes and pharmacy records to alert and provide decision support, that could be accepted or not by the physician. Disabled escape key and attention-grabbing color schemes used to increase use. Simulated use test and provider interviews for design. | Usual care | Non-validated, evidence derived | Appropriate LMWH ordering rates increased by 13.3% (18.9% vs 32.2%) favoring intervention (P < 0.001). |
| Kucher 2005 N = 2506 |
Quasi-RCT | Medical and surgical | CDS integrated into database performing daily automatic patient screening. Physicians of at-risk patients not on prophylaxis would receive alerts to physicians that had to be acknowledged and provide a list of generic prophylaxis order options. No forcing components. VTE guidelines made available in the EHR. | VTE guidelines made available in the EHR. | Weighted score based on common risk factors and lab results | VTE rates at 90 days favored intervention with a hazard ratio of 0.59 (95% CI, 0.43 to 0.81; P=0.001). Mortality and bleeding rates were similar. |
| Garcia 2009 N = 140 |
Cluster, Quasi RCT | Medical | Pharmacist manual chart review via a standardized risk-assessment form. Weighted and scored list of comorbidities/risk factors, contraindications, and relevant prophylaxis options. Standardized script for informing physician of patient VTE risk level, no specific therapy recommendations. No further alerts after the first. | Usual care | Weighted score based on common risk factors and lab results | Thromboprophylaxis rates similar (P = 0.15). In at-risk patients: Low-dose unfractionated heparin use rate: 56%. Prophylactic dose enoxaparin use: 11%. Sequential Compression Device use: 64% in intervention vs 50% in control group, often in combination with pharmacologic strategies. |
| Piazza 2009 N = 2493 |
RCT | Medical and surgical | Manual weighted screening for VTE risk factors based on ICD-9 codes and laboratory values by staff. Alerting physicians if at-risk patient had no prescription with a recommendation for mechanical prophylaxis. Contraindications and bleeding risk not considered. No specific modalities, agents, doses, frequencies, or durations were recommended. | Usual care | Weighted score based on common risk factors and lab results | Thromboprophylaxis rates increase: 25.35% (95% CI: 21.8-28.9%). No differences in hard outcomes overall or in high-risk subgroups. |
| Mahan 2011 N = 3525 |
Observational pretest-posttest | Medical and surgical | Rounds discusions, manual pharmacist VTE risk assessments, alerts to physicians, monthly performance reviews. Printed risk assessment forms assessing risk factors, overall risk level and contraindications, with prophylactic recommendations: enoxaparin, UFH, mechanical prophylaxis or none based on bleeding risk and eGFR. Risk assessment forms added to the patient records. In cases of non-compliance, contact was repeated by the lead pharmacist and then escalated to a physician champion. | Usual care | Paper-based, non-validated, guideline-derived risk assessment form. | Appropriate prophylaxis rates: OR 2.5 (critical care), 1.6 (surgical), 2.1 (medical), 1.8 (overall discharges), P < 0.0001. Preventable VTE rates reduction: 74%, P = 0.0006. Overall VTE reduction: 44%, P = 0.0624. |
| Piazza 2013 N = 2513 |
RCT | Medical | Pre-discharge manual screening of medical inpatients close to discharge. Staff page alerts and calls to attending physicians of high-risk patients with no active thromboprophylaxis orders. Contraindications, bleeding risk assessment and specific regimen recommendations not provided. | Usual care | Weighted score based on common risk factors and lab results | Intervention group thromboprophylaxis rates: 22.0% vs control 9.7%, P < 0.0001. Pharmacoprophylaxis rates: Intervention 19% vs control 7.7%, P < 0.0001. Symptomatic DVT/PE at 90 days: HR 1.12 (95% CI 0.74-1.69), not significantly different. Mortality and bleeding rates at 90 days similar. |
| Computerized CDSS | ||||||
| Galanter 2010 N = 38647 |
Observational pretest-posttest | Medical and surgical | Evidence-based, locally compiled, EMR-integrated mandatory VTE risk assessment form, launched via alert at order entry until risk assessment completed. Could be dismissed for first 8 hours. Form adapted based on previous answers and provided prophylaxis recommendations by risk level. Batch reviews of alerts printed at nursing station, if patients were found to be at risk and have no valid orders based on automatic screening. Same alerts also sent to the clinical EMR mailbox of treating physicians. | Usual care | Evidence-based, locally compiled, non-validated. | VTE pharmacoprophylaxis rate increased from 25.9% to 36.8% (p < 0.0001). Orthopedics only saw no increase. Intervention group prophylaxis rate higher for all medications except warfarin. Post-intervention odds of receiving prophylaxis: OR = 2.02, 95% CI = 1.92–2.13. Compared to medical patients, increased odds of prophylaxis for all patient types except obstetrics and gynecology. VTE rate declined from 0.51% to 0.43% (p = 0.22) Absolute VTE risk in medical patients declined from 0.55% to 0.33% (p = 0.02). NNT: 450 patients. Minor bleeding event rate post-CDS: 1.75% to 1.60% (p = 0.27). |
| MaCauely 2012 N = 4669 |
Observational pretest-posttest | Medical and surgical | Electronic admission order CDS. First screen: risk stratification as high, moderate, or low risk via point based VTE risk assessment displayed as text along with relative and absolute pharmacoprophylaxis contraindications. Second screen: alert displayed for patients with moderate or high risk and no VTE prophylaxis. Option to order or indicate contraindication. | Usual care | Caprini surgical score | Post-implementation cohorts: Low-risk: 48%, Moderate-risk: 31%, High-risk: 7%, Higher manual risk classification than computer-generated: 38%, Deferred/missing provider risk assessment: 14%, Pharmacoprophylaxis rate from 27% to 53%, Increase in VTE prophylaxis: 26% (P < 0.0001), VTE incidence declined from 0.98% to 0.42%, RRR 57%, P < 0.02) |
| Mitchell 2012 N = 5238 |
Observational pretest-posttest | Medical and surgical | Electronic alert in EMR history and physical note at admission. Asked whether patient is receiving prophylaxis, is low, medium, or high-risk for VTE. Displayed sample order choices for each level and listed contraindications. Note could not be saved without filling in the alert. Could not link to order screen due to software limitations. | Historical controls | None | Overall prophylaxis rate increase from 42.8% to 60.0%, P < 0.001. Not significant in renal failure, hip fracture/replacement patients. VTE rate decrease from 1.1% to 0.34%, P = 0.001. Non-significant DVT rate reduction from 0.42% to 0.13%, P = 0.053. Pulmonary embolism rate reduced from 0.74% to 0.22%, P = 0.009. Bleeding rate trend from 1.1% to 0.6%, P = 0.09. |
| Bhalla 2012 N = 36500 |
Observational pretest-posttest | Medical and surgical | Mandatory VTE risk alert in admission EHR note: prophylaxis status, risk level. Sample orders for each risk category and contraindications displayed. Alert completion required to save note. Direct linking to order screen restricted by software limitations. Repeated every 5 days if no prophylaxis. | Usual care | None | (Medicine services) VTE prophylaxis order rates: 61.9% to 82.1%, P < 0.001, pharmacologic VTE prophylaxis rate: 59.0% to 74.5%, P < 0.001, hospital acquired VTE incidence: 0.65% to 0.42%, P = 0.008, bleeding rates: 2.9% to 4.0%, P < 0.001. (Non-medicine services) VTE prophylaxis ordering rates: 70.5% to 73.6%, P < 0.001, pharmacologic prophylaxis rates: 59.3% to 63.3%, P < 0.001, bleeding rates: 7.7% to 8.6%, P = 0.043, hospital acquired VTE incidence change nonsignificant. |
| Umscheid 2012 N = 223062 |
Quasi-experimental pretest-posttest | Medical and surgical | EHR integrated CDS tools: list of 11 risk factors simply presented along with option to accept or decline VTE prophylaxis based on informed intuitive assessment, along with display of contraindications. Upon declining thromboprophylaxis, a specific reason had to be provided as free text in the first of two periods, changed to a choice between prewritten options during the third. The system disallowed two anticoagulants to be ordered simultaneously. An eGFR calculator prevented LMWH use in patients with stage 4 or higher renal disease. Risk estimation was intuitive. | Usual care | None | Thromboprophylaxis rates (control, 1st intervention period, 2nd intervention period): 27.1% to 43.0% to 51.9%, P < 0.01. Appropriate thromboprophylaxis rates: 42.0% to 47.6% to 54.4%, P < 0.01. VTE incidence and bleeding rates: unchanged. DVT decrease: 1.77% to 1.75% to 1.15%, P < 0.01. Overall VTE decrease: 2.18 to 2.15 to 1.73, P < 0.01. PE incidence increase: 0.52 to 0.53 to 0.74, P < 0.01. Physician guideline adherence increase for positively predisposed: 89.0% to 93.8%, P < 0.01. Physician guideline adherence increase for not predisposed: 63.7% to 74.1%, P < 0.01. Non-compliance reasons: No risk factors 58%, on therapeutic anticoagulation 35%, peri-procedural concerns 4%, bleeding risk 2%. |
| Fuzinatto 2013 N = 523 |
Observational pretest-posttest | Medical and surgical | Educational lecture, consensus meeting, EHR-based CDS tool. At EHR launch every 48 hours thereafter, if no thromboprophylaxis was prescribed, the physician could choose between 3 risk levels and indicate if thromboprophylaxis was contraindicated, aided by displayed text. Each level of risk was linked to appropriate UFH regimens, automatically prescribed in the background. Physicians could override the CDS by providing written justification. | Usual care | Evidence-based, locally compiled, non-validated | Thromboprophylaxis rate increase: from 46.2% to 57.9%, difference: 11.7% (95% CI: 3.2% - 20.3%, P = 0.01). Surgical patient VTE prophylaxis increase not statistically significant. Appropriate VTE prophylaxis pre- to post-implementation in cancer patients: 18.1% to 44.1%, absolute difference 26%, 95% CI: 9.9% to 42.3%, p = 0.002. Surgical patients postoperative appropriate VTE prophylaxis pre- to post-implementation: 53.6% to 60.4%, absolute difference 6.8%, 95% CI: −13.6% to 27.2%, p = 0.6. Medical patients appropriate VTE prophylaxis pre- to post-implementation: 44.2% to 57.2%, absolute difference 13%, 95% CI: 3.0% to 23.1%, p = 0.011. |
| Eijgenraam 2015 N = 128 |
Observational pretest-posttest | Medical | Button on first EHR, launching a risk assessment form, including a non-validated bleeding risk assessment model. Neither mandatory nor linked to the ordering system. Suggested appropriate prophylaxis regimens. | Usual care | Padua VTE risk score | Guideline adherence pre- and post-intervention: 59.4%, underprophylaxis decrease: OR 0.48 (95% CI: 0.18-1.30, P = 0.14), overprophylaxis increase: OR 1.66 (95% CI: 0.74–3.73, P = 0.22), CDS LMWH dose non-adherence: 12.5%, Physician self-reported non-adherence reason mean, SD: 2.4/5, 0.5 due to patient preferences. CDS mistrusted for complicated cases by 2/5 physicians, 3/5 questioned evidence base 3/5, 4/5 perceived improved patient outcomes, 2/5 believed automated ordering would reduce errors. |
| Amland 2015 N = 45046 |
Observational pretest-posttest | Medical and surgical | Three distinct periods separated by washout: 1. Nursing staff workflow standardized (thromboprophylaxis orders, interventions, documentation, outcome tracking) 2. CDS tool for risk stratification, contraindication documentation, evidence-based recommendations 3. Alert if patient not assessed or at increased VTE risk, given that initial tool utilization was non-measurable. | Usual care | Evidence-derived, non-validated risk assessment | VTE risk assessment rates within 24 hours from admission: increased from 49.7% to 78.4%, percentage of at-risk patients identified: increased from 42.8% to 64%, at-risk patients prescribed thromboprophylaxis: increased from 25.4% to 47.7%, VTE rates per 1000 patient days at baseline: 0.954, after nursing intervention: 0.734, after CDS availability: 0.790, after alert implementation: 0.434 (55% lower than baseline), sustained VTE rate at study end: 0.407 per 1000 patient days. Full implementation reduced VTE prevalence from 0.36% to 0.17% (OR 0.65, 95% CI 0.49-0.87, p = 0.0039), likelihood of VTE per patient after full intervention 35% lower compared to baseline, alerts crucial for significant results. |
| Spirk 2017 N = 1593 |
RCT | Medical | EHR alert 24 hours after admission prompting physicians to verify whether patient was on/had indications for therapeutic anticoagulation. EHR alert repeated at most three times promted risk stratification. A few patient characteristics were prepopulated (e.g. age). Anticoagulation recommendations for LMWH, UFH or mechanical prophylaxis based on creatinine clearance and bleeding risk, if appropriate based on risk. | Usual care | Geneva risk score | Similar rates of thromboprophylaxis, over- and underprophylaxis, and hard outcomes. 55.5% with inconsistent risk assessment leading to 9.2% lower rates of appropriate prophylaxis (62.6% vs 71.8%, P = 0.006) |
| Mathers 2017 N = 576 |
Observational pretest-posttest | Medical and surgical | Single-issue EHR-integrated alert at admission, mandating validated risk assessment. If patients were classified as medium or high risk, thromboprophylaxis prescription was required. The CDS could be overridden in cases of critical bleed or coagulopathy (INR > 2). | Usual care | Caprini surgical score | Pharmacoprophylaxis overall rate increase: 60% to 81.2% (P < 0.001), Medical service increase: 26.3% to 62.8% (P < 0.001), Surgical service increase: 83.7% to 95.5% (P < 0.001), Non-adherence in medical patients: 12.7%, Non-adherence in surgical patients: 3.6%, Common reasons for missing doses: patient preference (57%), provider overrides (25%), patient absence (15%), Hospitalization post-CDS associated with higher pharmacoprophylaxis odds: OR 4.72 (95% CI 2.94-7.57), Admission in surgical service associated with higher odds: OR 14.3 (95% CI 8.62-24.39), Blood transfusions associated with lower pharmacoprophylaxis odds: OR 0.28 (95% CI 0.12-0.63). |
| Spyropoulos 2023 N = 10699 |
Cluster RCT | Medical | EHR-agnostic CDS tool incorporating a validated VTE risk score for medical inpatient classification as low-, moderate- and high-risk. Multiple trigger points (admission, VTE prophylaxis order entry, discharge medication reconciliation). Automatically populating risk score calculator. Directed prescribers to order-entry for appropriate pharmacologic thromboprophylaxis, including extended post-discharge thromboprophylaxis. System overrides available only for patients at high bleed risk and non-medical inpatients. | Education | IMPROVE-DD - validated for medical patients | Inpatient thromboprophylaxis rates increased: 80.1% vs 72.5%, OR 1.52, 95% CI 1.39 to 1.67, P < 0.001. Appropriate discharge thromboprophylaxis rates in high-risk patients: 13.6% vs 7.5%, OR 1.93, 95% CI 1.60-2.33, P < 0.001. ATE events: 0.25% vs 0.70%, OR 0.35, P < 0.001. Mortality in the intervention group: 9.1% vs 7.0%, OR 1.32, P < 0.001. Outpatient arterial thromboembolic events: 0.86% to 0.32%, OR 0.37, 95% CI 0.21-0.65, P < 0.001. Total thromboembolic events: 4.5% to 3.3%, OR 0.72, 95% CI 0.59-0.88, P = 0.001. Mortality or VTE readmission rates at intervention sites: 4.9% vs 3.7%, OR 1.34, 95% CI 1.10-1.63, P < 0.004. |
3.1. Multifaceted Interventions
The SENTRY pilot cluster randomized trial conducted by Pai et al. examined VTE prophylaxis methods including paper based VTE risk assessment forms, educational sessions, and real-time chart audits used for instructional feedback [27]. No significant difference was found in appropriate thromboprophylaxis rates, or over- or under-prescription of thromboprophylaxis. A significant contribution of this study is the incorporation of qualitative analysis components, including small interviews and/or questionnaires directed towards all stakeholders, including patients.
A broad intervention by the PREVENU study group in France incorporated educational lectures, educational material dissemination and, in a second phase, a CDS tool with alerts incorporating medical diagnosis code information for risk stratification and tailored prescription choices [28]. The results of the study most likely reflect educational and informational interventions, as software infrastructure and policy barriers led to only 2 of 13 centers implementing the CDS tool. There was no difference between the intervention and control group in terms of the composite of VTE or major bleeding. Similarly, no difference was found in thromboembolic events, major bleeding, or all-cause mortality. Appropriate thromboprophylaxis rates were similar between groups post-intervention. The adjusted difference in rates of thromboprophylaxis was 6.6% [1.6-11.6%], with the intervention group having a larger increase compared to the control group.
Labarere et al. compared the effects of a multifaceted intervention including educational presentations with local data and educational material and audit components when directed at physicians only versus at physicians and nurses [29]. There were no significant differences between the study groups regarding radiology-verified DVT (OR 1.21; 95% CI, 0.70 – 2.11; P = 0.50).
As part of interventions targeted at improving various clinical outcomes, The Stroke Practice Improvement Network implemented alerts, standardized orders, grand rounds reporting with local data, educational resource provision, as well as individualized clinician feedback targeting DVT prophylaxis [30]. A non-significant trend favoring appropriate thromboprophylaxis was reported.
The Writing Group for the CHECKLIST-ICU Investigators and the Brazilian Research in Intensive Care Network (BRICNet) implemented a daily intensive care unit (ICU) checklist including a simple item on whether thromboprophylaxis had been ordered. This was combined with daily rounds discussions, review of patient goals of care, and checklist adherence feedback [31]. Periodic text message reminders to use the checklist were sent to providers, and directors were contacted if adherence was low. VTE prophylaxis rates were not affected (74.8% vs 75.0% of patient-days; adjusted RR, 1.05; 95% CI, 0.91-1.22; p = 0.50).
Streubel et al. compared a historic control period to a prospective audit and feedback intervention for VTE prophylaxis protocol adherence for patients undergoing primary total hip replacement surgery [32]. Results with local data were presented every two months. VTE prophylaxis adherence failure was reduced from 15% to 1.6% (p = 0.002) and VTE rates showed a non-significant trend toward improvement (p = 0.37)
Anderson et al. compared three groups: A) usual care, B) local-data-enriched educational and informational interventions alone, and C) in combination with an audit and feedback component, consisting of retrospective chart review data reported at staff meetings and individual physician compliance feedback [33]. Changes in rates of prophylaxis among groups A, B, and C were significant after adjusting for confounders: multivariate adjusted odds ratios were 2.1 (95% CI, 1.6-2.9) for A, 3.6 (95% CI, 2.7-4.7) for B, and 3.8 (95% CI, 2.9-5.0) for C.
The National VTE Prevention Program was developed in two pilot centers in the UK National Health System (NHS) and afterwards expanded to all NHS centers in 2010 [22], combining educational programs, quality standards, reporting requirements with audits, localization initiatives and financial incentives. The national VTE risk assessment tool used included lists of patient- and admission-related risk factors for VTE and bleeding. Hospitals were fined for not reaching the 95% screening rate target. Hospital-level data was collated and reported on a digital platform monthly and assessed on a quarterly basis, and root cause analyses were performed for a locally specified number of cases. The program resulted in a sustained increase in risk assessment rates by almost 50 percentage points in the first two years. Hospitals converged in terms of risk assessment rates from 51% (Inter quartile range (IQR) 27-71%), to 93% (IQR 91-96%). Hospitals achieving >90% risk assessment rates had 15% lower hospital-associated thrombosis, 12% lower chance of avoidable VTE and related mortality up to 90 days post-discharge. Non-fatal VTE readmissions and inpatient VTE-related mortality remained unchanged.
3.2. Preprinted Order Sets
An intervention by Fontaine et al. was informed by evidence-based, locally compiled prescription guidelines [34]. Physicians filled in anonymous questionnaires with data including patient characteristics, VTE risk factors, physician clinical impressions, and a visual analog scale for rating the risk of hemorrhagic complications. Over-prophylaxis decreased by 44% (from 25% to 15%) in the intervention group and increased by 17% (from 22% to 26%) in the control group. Appropriate thromboprophylaxis rates were not affected, while undertreatment showed minor reductions in both groups. The number of VTE risk factors was a significant factor affecting thromboprophylaxis prescriptions.
3.3. Passive Alerts (Human or Electronic)
An early study by Piazza et al. implemented manual weighted screening for VTE risk factors based on ICD-9 codes and laboratory values by staff [24]. Thromboprophylaxis contraindications and bleeding risk were not explicitly included. No specific thromboprophylaxis recommendations were made. Appropriate thromboprophylaxis rates increased across study periods in all hospitals and services from 27.1% to 51.9% (p < 0.01). There was no difference in overall VTE incidence or bleeding, however there were significant reductions in DVT and overall VTE (p < 0.01), with an increase in PE (0.52 to 0.74, p < 0.01).
A CDS tool integrated with EHR order entry was implemented by Dexter et al [35]. The tool provided physicians with national guideline-based reminders and prewritten orders with explanatory text, to be accepted or rejected. Datapoints informing the recommendations included demographics, EHR codes and prescriptions. Measures were taken to capture user attention (e.g., use of high contrast color schemes, disabling escape key). Subcutaneous heparin ordering for eligible patients increased from 18.9% in the to 32.2 percent (p<0.001).
Mahan et al. tested an intervention that combined rounds discussions, manual clinical pharmacist VTE risk assessments, and alerts to physicians with monthly performance reviews [5]. Printed risk assessment forms with risk factors and contraindications, plus prophylaxis recommendations based on bleeding risk and estimated glomerular filtration rate (eGFR) were incorporated. In cases of non-compliance, lead pharmacists and physician champions were alerted. Appropriate prophylaxis rates increased significantly, for critical care (OR 2.5), surgical (OR 1.6), medical (OR 2.1) patients and overall discharges (OR 1.8) (p < 0.0001 for all). There was a 74% reduction in preventable VTE rates (p = 0.0006).
Garcia et al. implemented a pharmacist manual chart review process based on a standardized and scored VTE risk assessment form, with weighted comorbidities/risk factors, contraindications, and prophylaxis options [36]. Physicians were only contacted once for each patient with scores of 4 or more. They were provided with information on VTE risk level but without specific recommendations for prescription. The difference in thromboprophylaxis rates between the two groups was not statistically significant (p = 0.15).
In a 2013 study of human alerts, Piazza et al. implemented discharge manual screening of medical inpatients [37]. Staff were tasked with paging alerts and called attending physicians of high-VTE risk patients to promote thromboprophylaxis. Contraindications, bleeding risk assessment and specific thromboprophylaxis regimen recommendations were not provided. Thromboprophylaxis rates were significantly higher in the intervention group (22.0% vs 9.7%, p < 0.0001), as were rates of pharmacologic prophylaxis (19% vs 7.7%, p < 0.0001). Symptomatic DVT or PE rates at 90 days were not significantly higher (HR 1.12; 95% CI 0.74-1.69). Mortality rates and bleeding rates at 90 days were similar.
In a landmark study, Kucher et al. devised a computer program to perform daily automatic patient screening and scoring using ICD-9 codes and a weighted VTE scoring system [23]. For intervention patients with a score ≥ 4 not on thromboprophylaxis, physicians received alerts and a list of generic prophylaxis options, and VTE guidelines available on screen. DVT or PE at 90 days occurred in 4.9% of the intervention group vs. 8.2% of the control group (p<0.001). There was a 41% reduced risk of VTE at 90 days (hazard ratio 0.59, 95% CI, 0.43 to 0.81; p=0.001). No differences were found in mortality and hemorrhage.
3.4. Computerized CDS System (CDSS) Interventions
Galanter et al. implemented an EHR VTE risk assessment form that would trigger alerts on order entry [38]. Prophylaxis options were recommended based on VTE risk level and compared to orders. A second alert was sent to the EHR inbox and printed so that it was reviewed in batch. Overall, pharmacologic prophylaxis rates increased from 25.9% to 36.8% (p < 0.0001). The odds ratio of thromboprophylaxis pre- vs post-intervention was 2.02, (95% CI 1.92-2.13). VTE rate reduction was significant only in medical patients (0.55% vs 0.33%, p = 0.02) with an absolute risk reduction of 0.22% and a number needed to treat of 450 patients. Bleeding rates were unaffected.
MaCauley et al. created an EHR-based CDS tool in the admission order process for all hospitalized patients [39]. VTE risk stratification (high vs moderate vs low VTE risk) was presented on the first screen upon order entry at admission. Relevant risk factors and their weights for a risk score were displayed, as were generic options to order prophylaxis or verify pharmacologic contraindications. Rates of pharmacologic thromboprophylaxis increased from 26% to 34% post-intervention (p < 0.0001), with a 57% relative risk reduction in VTE (p < 0.02).
Mitchell et al. added an extra CDS component to the admission note history and physical to force risk stratification of patients as low, medium, or high-risk for VTE [40]. A list of thromboprophylaxis contraindications and sample orders for each risk level was also displayed on the same screen, but not linked to order entry. The overall rate of appropriate pharmacologic prophylaxis increased from 42.8% to 60.0% (p < 0.001). The overall VTE rate was significantly lower in the control group (1.1% vs 0.34%, p = 0.001), though DVT rate differences alone did not reach significance. There was a trend toward lower bleeding rates after a reminder was added (1.1% vs 0.6%, p = 0.09).
Umscheid et al. implemented a CDS tool presenting 11 thrombotic risk factors and the option to provide VTE prophylaxis based on intuitive assessment [41]. Providers who declined CDS were required to enter a specific reason as free text or select among prewritten options. Contraindications were displayed on the following admission order entry screen. The system did not allow two anticoagulants to be ordered, and an eGFR calculator was used to prevent low molecular weight heparin (LMWH) use in patients with advanced renal disease. Thromboprophylaxis rates increased from 27.1% in the first to 51.9% in the third period (P < 0.01). Appropriate prophylaxis rates showed a similar increase (from 42.0% to 54.4%, P < 0.01). VTE incidence and bleeding rates were unaffected.
In an intervention by Bhalla et al., order sets for medicine inpatients, as denoted by admission codes, were populated with choices regarding pharmacologic prophylaxis, planned prophylactic anticoagulation, lack of indication and contraindications to prophylaxis [42]. This order set framework would repeat every 5 days if no prophylaxis was provided. Thromboprophylaxis ordering saw significant increases in both medicine and non-medicine services. The incidence of hospital-associated thrombosis was decreased from 0.65% to 0.42% (p = 0.008) for medicine patients but was non-significant for patients on non-medicine services. Bleeding rates increased from 2.9 to 4.0% on medicine services (p < 0.001) and from 7.7% to 8.6% on non-medicine services (p = 0.043).
In 2013 Fuzinatto et al. adapted existing guidelines into a local protocol to standardize risk factors, contraindications for heparin, and VTE risk-appropriate prophylaxis [43]. An EHR-based CDS tool was also developed and deployed after a lecture and a consensus meeting. At EHR launch and then every 48 hours if no thromboprophylaxis was prescribed, the physician could choose between 3 risk levels and indicate if thromboprophylaxis was contraindicated, aided by displayed information. Each level of risk was linked to appropriate unfractionated heparin regimens that were automatically prescribed in the background. Physicians could override the CDS tool by providing written justification. Appropriate thromboprophylaxis rates increased from 46.2% to 57.9%, a significant 11.7% difference (95% CI: 3.2% - 20.3%, p = 0.01). The increase appropriate VTE prophylaxis among surgical patients was not statistically significant.
Amland et al., implemented thromboprophylaxis interventions in three steps across three distinct periods separated by a washout [44]. First, a nursing staff workflow standardized care components including thromboprophylaxis orders and interventions. Next, a CDS tool allowing physicians to complete VTE risk stratification with guideline-derived criteria and thromboprophylaxis options was deployed. Finally, an alert was added for patients not assessed or at increased risk of VTE, given undetectable utilization in the first two periods. VTE risk assessment rates within 24 hours from admission increased from 49.7% to 78.4%, VTE rates per 1000 patient days were 0.954 at baseline and ultimately decreased to 0.434 in the alert period, 35% lower compared to baseline, (OR 0.65, CI 0.49–0.87, P = 0.0039). The likelihood of VTE per patient after the full intervention was 29% lower compared to baseline (OR 0.71, 95% CI 0.55-0.93, P = 0.014).
Eijgenraam et al. piloted a button on the first page of the electronic patient record that would deploy a risk assessment form based on the validated Padua VTE risk score [45]. The use of the CDS was neither mandatory nor linked to the ordering system, though it did suggest appropriate prophylaxis regimens. The included bleeding risk assessment model was not validated. Adherence to guidelines was similar before and after the intervention (59.4% in both cases), but under-prophylaxis decreased (OR 0.48, 95% CI: 0.18-1.30, p = 0.14), while over-prophylaxis increased (OR 1.66, 95% CI 0.74 – 3.73, p = 0.22). 12.5% of patients on whom the CDS tool was used did not receive the LMWH dose prescribed by the system. On a scale measuring how often non-adherence was due to patient preferences, ranging from 1 (‘never’) to 5 (‘very often’), physicians responded with an average of 2.4 (standard deviation [SD] 0.5). Physicians questioned the validity of CDS advice for complicated patients, including those with multiple comorbidities, as well as whether the CDS was evidence-based, while 40% thought that automated ordering would reduce errors.
Spirk et al. implemented an EHR alert prompting physicians 24 hours after admission to verify whether a patient was on or had indications for prophylactic anticoagulation [46]. If not, the Geneva VTE risk score was presented, with some demographic data pre-populated. The alert would be repeated 3 times if dismissed. A score ≥ 3 led to anticoagulant thromboprophylaxis recommendations based on renal function and bleeding risk factors. 55.5% of intervention patients had inconsistent or absent score calculations and lower appropriate thromboprophylaxis rates than those with consistent scores (62.6% vs 71.8%, p = 0.006). Alerts showed an increase in thromboprophylaxis prescription from 63.1% to 70.4%, P = 0.028. No difference was found in rates of appropriate prophylaxis, inpatient mortality, rates of inpatient thromboprophylaxis, over- and underprophylaxis, inpatient all-cause mortality, inpatient VTE rates, and bleeding requiring medical attention.
Mathers et al. tested a single-issue EHR-integrated alert at admission, mandating risk assessment of surgical and medical patients with the validated surgical Caprini VTE score [47]. If patients were classified as medium or high VTE risk, a prophylactic intervention was required. The CDS tool could be overridden in cases of critical bleed or coagulopathy. Overall rates of pharmacologic prophylaxis increased from 60% to 81.2% (p < 0.001), and the increase was significant both in medical (26.3% vs 62.8%, p < 0.001) and surgical services (83.7% v 95.5% p < 0.001). Non-adherence to CDS-recommended pharmacologic prophylaxis was higher in medical patients, with 12.7% not receiving the doses ordered, versus only 3.6% of surgical patients. Patient preference (57%), provider overrides (25%) and patient absence for procedures or tests (15%) were common reasons for missing doses. Multivariate regression showed that hospitalization after the CDS was deployed was associated with higher odds of receiving pharmacologic prophylaxis (OR 4.72, 95% CI 2.94-7.57), as was being admitted to a surgical service (OR 14.3, 95% CI 8.62-24.39). Requiring blood transfusions was associated with lower odds of pharmacologic prophylaxis (OR 0.28, 95% CI 0.12-0.63).
A recent large cluster randomized trial- IMPROVE-DD -by Spyropoulos et al. in medical inpatients evaluated a cloud based, EHR-agnostic CDS tool incorporating the validated and weighted IMPROVE-DD VTE score after multiple rounds of usability testing [26]. The tool was triggered at admission, VTE prophylaxis order entry, and at discharge medication reconciliation. A mostly auto-populating calculator stratified patients into low, moderate, and high VTE risk and actively guided prescribers to appropriate pharmacologic thromboprophylaxis, including extended post-discharge thromboprophylaxis in high VTE risk patients with a score ≥ 4. Overrides were available only for high bleed risk cases and non-medical inpatients. Tool adoption rate was 77.8%, leading to increased inpatient (OR: 1.52, 95% CI: 1.39 to 1.67, p < 0.001) and at-discharge appropriate extended thromboprophylaxis (OR: 1.93, 95% CI: 1.60-2.33, p < 0.001). At 30 days post-discharge, there were fewer venous (2.7% versus 3.3%, OR 0.80, 95% CI 0.64-1.00), arterial (0.25% versus 0.70%, OR 0.35, 95% CI 0.19-0.67), and total thromboembolisms (2.9% versus 4.0%, OR 0.71, 95% CI 0.58-0.88) at intervention hospitals. Major bleeding was rare and did not differ between groups. Mortality was higher at intervention hospitals (9.1% versus 7.0%, OR 1.32, 95% CI 1.15-1.53), which included more patients hospitalized with COVID-19.
3.5. Systematic Reviews and Meta-Analyses
An early Cochrane systematic review and meta-analysis of randomized trials and observational studies showed that multifaceted interventions were effective at increasing rates of thromboprophylaxis (Risk Difference (RD) 95% CI: 0.17, 0.09 – 0.25) [48]. However, there was substantial heterogeneity among studies, and the included four non-randomized studies reporting VTE or DVT risk showed no difference. There was a significant increase in patients receiving appropriate prophylaxis with educational interventions (RD 0.11 (95% CI 0.06 to 0.17), although assessment by non-randomized studies and the pooled effect showed no statistical significance. Alerts increased rates of overall thromboprophylaxis based on four randomized trials (RD 0.13, 95% CI: 0.01, 0.25, I-squared = 94.9%) and five non-randomized studies (RD 0.09, 95% CI: -0.00 - 0.19, I-squared = 97.8%). Electronic alerts tended to be more effective than the preprinted counterparts. Appropriate thromboprophylaxis rates were also increased by alerts, based on 10 non-randomized studies, (RD 0.18, 95% CI 0.12 to 0.24), though there was substantial heterogeneity. All interventions increased rates of thromboprophylaxis, with multifaceted interventions combined with alerts showing the greatest effect size Absolute differences were moderate (less than 20%), with greatest effect size in non-academic settings.
An updated Cochrane systematic review and meta-analysis by the same group included 11 randomized trials on interventions to increase appropriate inpatient thromboprophylaxis [49]. Studies investigated multifaceted interventions, preprinted orders, and alerts (human or electronic). Though there was substantial heterogeneity of patient populations, hospital settings, and alert type between studies, alerts (human or computer) overall increased the proportion of patients who received appropriate thromboprophylaxis by 16% and decreased the relative risk of symptomatic VTE by 36%. Although multifaceted interventions increased the proportion of patients who received prophylaxis, they were found to be less effective than alerts interventions.
A recent systematic review and meta-analysis evaluated the impact of CDS tools versus routine care on VTE prophylaxis guideline adherence and VTE rates in hospitalized non-surgical patients [25]. CDS interventions resulted in significantly increased rates of appropriate prophylaxis based on three non-randomized studies (OR 1.69, 95% CI: 1.25-2.28, p = 0.001, I 2 = 59.3%, p = 0.085) and increased overall rates of pharmacologic prophylaxis, based on 7 non-randomized studies (OR = 2.02, 95% CI: 1.66-2.45, p < 0.001; I2 = 97.1%, p < 0.001). CDS tool use was also associated with significantly decreased rates of VTE events based on three non-randomized studies (OR = 0.68, 95% CI: 0.54-0.85, p = 0.001, I2 = 31.5%, p = 0.211).
4. Critical Synthesis and Discussion
System-wide interventions to increase appropriate thromboprophylaxis in hospitalized patients require multimodal quality improvement efforts. These include an educational component, which increases provider motivation by providing regular automated reports, provides current information on best practices, and can be augmented by computerized, targeted education [50]. Motivational interviewing by clinicians and patient education can also be part of quality improvement efforts if patient hesitancy is a bottleneck. This may be especially important in increasing appropriate extended post-discharge thromboprophylaxis, where the patient has greater control over the medication they take.
Identifying patients with an appropriate risk-benefit ratio is another important component of system-wide thromboprophylaxis interventions. The use of externally validated VTE risk models that are weighted and scored represent an important improvement over intuitive, unweighted and checklist based VTE risk assessment strategies. Validated VTE risk models such as the Caprini score in surgical inpatients and the Padua or IMPROVE/IMPROVE-DD score in medical inpatients have been incorporated in both passive alert systems as well as computerized CDS tools, resulting in increased appropriate inpatient thromboprophylaxis in at- or moderate-VTE risk patients, and in the case of IMPROVE-DD, increased appropriate at discharge extended thromboprophylaxis in high VTE-risk patients [26]. Importantly, incorporation of these validated VTE risk scores has resulted in reduction of VTE risk without a concomitant increase in major bleeding, by careful patient selection.
An important multimodal component of a system-wide thromboprophylaxis intervention is use of an active CDS tool over other interventions. Although passive (human or electronic) alert systems have been shown to be more effective than multifaceted interventions in increasing appropriate thromboprophylaxis, active computerized CDS tools – especially if the CDS tool can auto-populate both a VTE risk score as well as an order entry for thromboprophylaxis – appear to be effective in both increasing appropriate thromboprophylaxis based on VTE risk level and reducing major thromboembolism.
4.1. Multifaceted
Providing passive information to clinicians through lectures, printed, mailed, or emailed literature, pocket cards, grand rounds, links to guidelines, and continuing medical education self-assessments has an overall negligible impact on thromboprophylaxis [29,33,41,43,51,52,53]. This holds true even if the information is available at the point of care in the form of a free decision support hotline [33] or a system that provides educational feedback in the medication order entry screen [54]. This has partly been attributed to barriers like patient preferences and time restrictions [29]. Educational interventions can be more engaging and effective when organized in small groups in the form of “academic detailing” [55], when incorporating hospital-specific data [33], targeting the whole clinical team and when repeated as teams turn over [29,51,56]. Educational interventions have led to increased rates of appropriate thromboprophylaxis by informing compliant physicians on the latest best practices [57] and the rates of over-prophylaxis when not paired with other interventions to guide or monitor prescription [28].
Consensus building and collaboration in the quality improvement process, along with the incorporation of a champion, a respected and knowledgeable staff member for each intervention center, can increase success [29,33,51]. Tasks like entering data in risk-scoring systems is error prone if undertaken by humans [58]. Reminders by staff members may also be easily ignored by physicians [51]. Screening rate or thromboprophylaxis rate targets and ward-level feedback may be important in achieving adoption and increasing staff motivation [33,55,59]. Audits, even on their own, are effective in increasing thromboprophylaxis but require major time and staff investment [59]. Lastly, educational and consensus building are not effective unless audited [52,57]. Overall, although multifaceted interventions, including educational initiatives, appear to increase appropriate inpatient thromboprophylaxis, these efforts show mixed results in reducing rates of VTE, are time and resource intensive, and are less effective than alert-based interventions.
4.2. Preprinted Order Sets
Preprinted admission order sets used voluntarily have resulted in significant increases in thromboprophylaxis, though with low overall rates of thromboprophylaxis [60,61]. Preprinted forms are not necessarily a bottleneck in achieving high rates of thromboprophylaxis [60], but they can be easily ignored [27].
4.3. Passive Alerts (Human or Electronic) and Order Entry Components
Passive alerts have been found to be moderately useful as system-wide thromboprophylaxis interventions, originally taking the form of stickers on patient files [59], printed schedule alerts [62,63] and eventually electronic and critiquing alerts that are activated when thromboprophylaxis was inconsistent with the patient’s risk profile [54]. EHR alerts used as a VTE risk assessment point for all inpatients via a checklist interface resulted only in marginal improvements in appropriate thromboprophylaxis [46]. The lack of efficacy was attributed to the Hawthorne effect [64] and alert fatigue [46]. Alerts that are not mandatory or involve workflow barriers such as requiring physician action to be displayed or separate logins lead to low utilization rates [45], while repeat alerts increase thromboprophylaxis in high-risk patients compared to single alerts [65]. In addition, passive alerts prompting for verification in case of no prescription and a third verification by nursing staff resulted in sustained increases in appropriate prophylaxis [66]. Manual VTE risk assessment of patients that were automatically categorized as low-risk resulted in better outcomes compared to a non-validated, ad hoc point-based scoring system alone [39]. However, the manual intuitive risk assessment that was not based on a risk score was also not sensitive enough to correctly identify moderate-risk patients. Daily risk stratification paired with an alerting system resulted in decreased thromboembolism while the system was in use [67]. Additionally, prepopulating the order entry with relevant choices encouraged use and increased effectiveness [66]. Overall, alerts, especially in electronic form, appear to be more effective than multifaceted interventions. Making alert responses and order entry tool use mandatory and embedding them in a multifaceted approach leads to improved outcomes on its own or in combination with other interventions [41,60].
4.2. Computerized CDS Systems
Active CDS tools that incorporate individual clinical data were tested initially by printing alerts on surgical schedules for patients undergoing high-risk procedures [62]. Alerting for patients according to medical diagnosis codes has also been tested with variable results [28,35,42]. Subsequently, inextensible computerized software infrastructure and hospital policy have been identified as barriers to research efforts and widespread adoption [23,28]. Auto-displaying alert and pre-populated order sets where a CDS tool could also auto-populate a patient’s prescription has shown the greatest effectiveness in increasing appropriate thromboprophylaxis and reducing VTE [25,35]. Thus, computerized CDS tools that are active are the most promising in implementing evidence-based medicine at the point-of-care based on accepted antithrombotic guidelines [39]. However, a major limitation of CDS technology was that it was limited to individual healthcare centers based on informatics technology support, with inability to export to other health system EHRs, and thus impacting generalizability [68]. The most recent large cluster randomized trial on the topic was able to demonstrate effectiveness of a novel CDS platform for VTE prevention in hospitalized medical patients utilizing a widely validated VTE risk score that was EHR-agnostic and cloud-based (thus able to be housed externally from a particular healthcare informatics network) [26]. Compared to usual medical care in hospitalized patients, CDS tools significantly increase rates of appropriate thromboprophylaxis and reduce major thromboembolism, including VTE and arterial thromboembolism. These results, coupled with workflow efficiency of CDS tools that auto-populate a patient’s thrombotic risk and actively recommend thromboprophylaxis prescriptions based on level of thrombotic risk, appear the most effective system-wide interventions for thromboprophylaxis of hospitalized patients. The ability to export a particular CDS tool to multiple EHRs using an EHR-agnostic platform and the ability to further refine and adapt a CDS tool based on local workflow requirements holds promise in effectively providing system-wide evidence-based recommendations for thromboprophylaxis of hospitalized patients at the point-of-care.
5. Future Directions
The updated 2024 International Union of Angiology Consensus Guidelines on VTE prevention and management for the first time recommended the use of health informatics technology in the form of electronic alerts or CDS tools to identify key populations of medical inpatients that may benefit from inpatient and extended post-discharge pharmacologic thromboprophylaxis, based on moderate quality evidence [69]. Antithrombotic guideline recommendations would thus encourage health system-wide adoption and implementation of validated CDS tools, and a recent National Institute of Health (NIH) R01 funding announcement calls for dissemination and implementation of validated CDS tools across multiple health-care environments (https://public.era.nih.gov). The previously discussed CDS platform - called EvidencePoint – utilized in the IMPROVE-DD trial is EHR-agnostic, thus theoretically be interoperable within any EHR, and adaptable, thus able to be modified based on local usability testing to accommodate a variety of clinical workflows and health-care environments [70,71,72] (Figure 1). The platform could sit on top of any informatics infrastructure using internationally standardized SMART on FHIR and health level (HL) 7 applications [73]. CDS hook protocols integrate with informatics systems to access information not only within the EHR, but also across the health system informatics exchange environment. Single sign-on functionality is able to eliminate barriers that discouraged adoption. Data is not only retrieved, but also updated and created with minimal need for bespoke software. Importantly, this cloud-based EHR-agnostic CDS tool built as an online service is able to solve the tension between deep EHR integration and portability, by using standardized secure protocols and application programming interfaces to pull and push data irrespective of the underlying informatics environment. The platform is able to retrieve data that auto-populates a specific VTE risk score and assist providers in determining VTE risk at the point-of-care, as shown in Figure 2 [72]. Thus, the portability and deep integration of the CDS tool would allow flexible and seamless workflow integration into clinical care pathways utilizing formal usability testing with rapid iteration over designs, based on standardized metrics and feedback gathered through live testing sessions and interviews with volunteer clinicians. The flexibility of the platform would be in accordance with the "five rights" directive: the right information, to the right person, in the right format, through the right channel, at the right time [74]. For example, given the need for improved post-discharge thromboprophylaxis in high VTE risk patients, adding a discharge trigger point would require minimal effort.
Future research efforts for system-wide thromboprophylaxis interventions should focus on comprehensive quantitative and qualitative assessments of active CDS tools that have shown effectiveness and incorporate validated VTE risk score implementations, workflow components, and patient outcomes. Widespread refinement and implementation of active CDS tools across various EHR environments using EHR-agnostic platforms, with workflow mapping and usability testing of the CDS tools in diverse sites and in different clinical settings, will allow for identification of barriers and opportunities for improvement. Lastly, there is potential for the use of artificial intelligence based CDS using machine learning to increase CDS tool accuracy and improve model discrimination that can lead to fewer false alerts and missed patients [75]. Rapid dissemination of effective, accurate, and adaptable CDS tools will enable incorporating current evidence at the point of care and thus promote thromboprophylaxis standardization across hospitals and health systems.
5. Conclusions
System-wide implementation of thromboprophylaxis includes use of multifaceted approaches including educational components, pre-printed order sheets, human or electronic passive alerts, and active computerized CDS. Of all these, the use of active computerized CDS that incorporates a validated VTE risk score appears the most effective and efficient intervention to increase appropriate thromboprophylaxis and reduce thromboembolism. Refinement of effective CDS tools with usability testing across various workflows that are deeply integrated across EHRs using agnostic methods, with widespread implementation of these tools, can potentiate dissemination of best practices of evidence-based thromboprophylaxis in hospitalized patients.
Author Contributions
Conceptualization, A.C.S., M.G., N.T.S.; methodology, N.T.S, A.C.S; data curation, N.T.S., A.C.S.; writing—original draft preparation, N.T.S., A.C.S., M.G.; writing—review and editing, A.C.S., M.G., N.T.S.; supervision, A.C.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by funding from the Broxmeyer Fellowship in Clinical Thrombosis.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable.
Acknowledgments
The authors are grateful to Jeffrey Solomon, et al. for allowing the use of figures from their publication [72], which greatly enhanced this work. Thank you for your generosity and collaboration.
Conflicts of Interest
Dr. Spyropoulos reports honoraria from Janssen, Bayer, Bristol Myers Squibb, Pfizer, and Sanofi and research grants from Janssen and Boehringer Ingelheim. He also is a member of the ATLAS group, an academic research organization. Dr. Goldin reports grant support from Janssen and AstraZeneca outside of the submitted work. Dr. Tsaftaridis reports no conflicts. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Wolberg, A.S.; Rosendaal, F.R.; Weitz, J.I.; Jaffer, I.H.; Agnelli, G.; Baglin, T.; Mackman, N. Venous Thrombosis. Nat. Rev. Dis. Primer 2015, 1, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Raskob, G.E.; Angchaisuksiri, P.; Blanco, A.N.; Buller, H.; Gallus, A.; Hunt, B.J.; Hylek, E.M.; Kakkar, A.; Konstantinides, S.V.; McCumber, M.; et al. Thrombosis: A Major Contributor to Global Disease Burden. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 2363–2371. [Google Scholar] [CrossRef] [PubMed]
- Kahn, S.R.; Lim, W.; Dunn, A.S.; Cushman, M.; Dentali, F.; Akl, E.A.; Cook, D.J.; Balekian, A.A.; Klein, R.C.; Le, H.; et al. Prevention of VTE in Nonsurgical Patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th Ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012, 141, e195S–e226S. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, M.; Chan, N.; Bhagirath, V.; Ginsberg, J. Prevention of Venous Thromboembolism in 2020 and Beyond. J. Clin. Med. 2020, 9, 2467. [Google Scholar] [CrossRef]
- Mahan, C.E.; Holdsworth, M.T.; Welch, S.M.; Borrego, M.; Spyropoulos, A.C. Deep-Vein Thrombosis: A United States Cost Model for a Preventable and Costly Adverse Event. Thromb. Haemost. 2011, 106, 405–415. [Google Scholar] [CrossRef]
- Schünemann, H.J.; Cushman, M.; Burnett, A.E.; Kahn, S.R.; Beyer-Westendorf, J.; Spencer, F.A.; Rezende, S.M.; Zakai, N.A.; Bauer, K.A.; Dentali, F.; et al. American Society of Hematology 2018 Guidelines for Management of Venous Thromboembolism: Prophylaxis for Hospitalized and Nonhospitalized Medical Patients. Blood Adv. 2018, 2, 3198–3225. [Google Scholar] [CrossRef]
- Barbar, S.; Noventa, F.; Rossetto, V.; Ferrari, A.; Brandolin, B.; Perlati, M.; Bon, E.D.; Tormene, D.; Pagnan, A.; Prandoni, P. A Risk Assessment Model for the Identification of Hospitalized Medical Patients at Risk for Venous Thromboembolism: The Padua Prediction Score. J. Thromb. Haemost. 2010, 8, 2450–2457. [Google Scholar] [CrossRef]
- Spyropoulos, A.C.; Lipardi, C.; Xu, J.; Peluso, C.; Spiro, T.E.; De Sanctis, Y.; Barnathan, E.S.; Raskob, G.E. Modified IMPROVE VTE Risk Score and Elevated D-Dimer Identify a High Venous Thromboembolism Risk in Acutely Ill Medical Population for Extended Thromboprophylaxis. TH Open 2020, 04, e59–e65. [Google Scholar] [CrossRef]
- Bahl, V.; Hu, H.M.; Henke, P.K.; Wakefield, T.W.; Campbell, D.A.J.; Caprini, J.A. A Validation Study of a Retrospective Venous Thromboembolism Risk Scoring Method. Ann. Surg. 2010, 251, 344. [Google Scholar] [CrossRef]
- Flanders, S.A.; Greene, M.T.; Grant, P.; Kaatz, S.; Paje, D.; Lee, B.; Barron, J.; Chopra, V.; Share, D.; Bernstein, S.J. Hospital Performance for Pharmacologic Venous Thromboembolism Prophylaxis and Rate of Venous Thromboembolism : A Cohort Study. JAMA Intern. Med. 2014, 174, 1577–1584. [Google Scholar] [CrossRef]
- Mahan, C.E.; Fisher, M.D.; Mills, R.M.; Fields, L.E.; Stephenson, J.J.; Fu, A.-C.; Spyropoulos, A.C. Thromboprophylaxis Patterns, Risk Factors, and Outcomes of Care in the Medically Ill Patient Population. Thromb. Res. 2013, 132, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Nicolaides, A.; Fareed, J.; Kakkar, A.K.; Comerota, A.J.; Goldhaber, S.Z.; Hull, R.; Myers, K.; Samama, M.; Fletcher, J.; Kalodiki, E.; et al. Prevention and Treatment of Venous Thromboembolism: International Consensus Statement (Guidelines According to Scientific Evidence). Clin. Appl. Thromb. 2013, 19, 116–118. [Google Scholar] [CrossRef]
- Stevens, S.M.; Woller, S.C.; Kreuziger, L.B.; Bounameaux, H.; Doerschug, K.; Geersing, G.-J.; Huisman, M.V.; Kearon, C.; King, C.S.; Knighton, A.J.; et al. Executive Summary: Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report. CHEST 2021, 160, 2247–2259. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulos, A.C.; Anderson, F.A.; FitzGerald, G.; Decousus, H.; Pini, M.; Chong, B.H.; Zotz, R.B.; Bergmann, J.-F.; Tapson, V.; Froehlich, J.B.; et al. Predictive and Associative Models to Identify Hospitalized Medical Patients at Risk for VTE. CHEST 2011, 140, 706–714. [Google Scholar] [CrossRef]
- Mahan, C.E.; Liu, Y.; Turpie, A.G.; Vu, J.T.; Heddle, N.; Cook, R.J.; Dairkee, U.; Spyropoulos, A.C. External Validation of a Risk Assessment Model for Venous Thromboembolism in the Hospitalised Acutely-Ill Medical Patient (VTE-VALOURR). Thromb. Haemost. 2014, 112, 692–699. [Google Scholar] [CrossRef]
- Greene, M.T.; Spyropoulos, A.C.; Chopra, V.; Grant, P.J.; Kaatz, S.; Bernstein, S.J.; Flanders, S.A. Validation of Risk Assessment Models of Venous Thromboembolism in Hospitalized Medical Patients. Am. J. Med. 2016, 129, 1001.e9–1001.e18. [Google Scholar] [CrossRef]
- Nendaz, M.R.; Chopard, P.; Lovis, C.; Kucher, N.; Asmis, L.M.; Dörffler, J.; Spirk, D.; Bounameaux, H. Adequacy of Venous Thromboprophylaxis in Acutely Ill Medical Patients (IMPART): Multisite Comparison of Different Clinical Decision Support Systems. J. Thromb. Haemost. 2010, 8, 1230–1234. [Google Scholar] [CrossRef]
- Spyropoulos, A.C.; Raskob, G.E. New Paradigms in Venous Thromboprophylaxis of Medically Ill Patients. Thromb. Haemost. 2017, 117, 1662–1670. [Google Scholar] [CrossRef]
- Raskob, E.G.; Day, I.S.C. for W.T. Venous Thromboembolism: A Call for Risk Assessment in All Hospitalised Patients. Thromb. Haemost. 2016, 116, 777–779. [Google Scholar] [CrossRef]
- Zhen, K.; Dong, F.; Fang, F.; Gao, Q.; Zhang, Z.; Xia, L.; Wang, W.; Yang, P.; Jia, C.; Liu, P.; et al. Evaluation of In-Hospital Venous Thromboembolism Prevention and Management System Using Hospital-Level Metrics: A Nationwide Cross-Sectional Survey in China. J. Patient Saf. 2022, 18, e626. [Google Scholar] [CrossRef] [PubMed]
- Bright, T.J.; Wong, A.; Dhurjati, R.; Bristow, E.; Bastian, L.; Coeytaux, R.R.; Samsa, G.; Hasselblad, V.; Williams, J.W.; Musty, M.D.; et al. Effect of Clinical Decision-Support Systems. Ann. Intern. Med. 2012, 157, 29–43. [Google Scholar] [CrossRef] [PubMed]
- Roberts, L.N.; Durkin, M.; Arya, R. Annotation: Developing a National Programme for VTE Prevention. Br. J. Haematol. 2017, 178, 162–170. [Google Scholar] [CrossRef] [PubMed]
- Kucher, N.; Koo, S.; Quiroz, R.; Cooper, J.M.; Paterno, M.D.; Soukonnikov, B.; Goldhaber, S.Z. Electronic Alerts to Prevent Venous Thromboembolism among Hospitalized Patients. N. Engl. J. Med. 2005, 352, 969–977. [Google Scholar] [CrossRef] [PubMed]
- Piazza, G.; Rosenbaum, E.J.; Pendergast, W.; Jacobson, J.O.; Pendleton, R.C.; McLaren, G.D.; Elliott, C.G.; Stevens, S.M.; Patton, W.F.; Dabbagh, O.; et al. Physician Alerts to Prevent Symptomatic Venous Thromboembolism in Hospitalized Patients. Circulation 2009, 119, 2196–2201. [Google Scholar] [CrossRef] [PubMed]
- Karajizadeh, M.; Hassanipour, S.; Sharifian, R.; Tajbakhsh, F.; Saeidnia, H.R. The Effect of Information Technology Intervention on Using Appropriate VTE Prophylaxis in Non-Surgical Patients: A Systematic Review and Meta-Analysis. Digit. Health 2022, 8, 20552076221118828. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulos, A.C.; Goldin, M.; Koulas, I.; Solomon, J.; Qiu, M.; Ngu, S.; Smith, K.; Leung, T.; Ochani, K.; Malik, F.; et al. Universal EHRs Clinical Decision Support for Thromboprophylaxis in Medical Inpatients. 2023. [Google Scholar]
- Pai, M.; Lloyd, N.S.; Cheng, J.; Thabane, L.; Spencer, F.A.; Cook, D.J.; Haynes, R.B.; Schünemann, H.J.; Douketis, J.D. Strategies to Enhance Venous Thromboprophylaxis in Hospitalized Medical Patients (SENTRY): A Pilot Cluster Randomized Trial. Implement. Sci. IS 2013, 8, 1. [Google Scholar] [CrossRef] [PubMed]
- Roy, P.-M.; Rachas, A.; Meyer, G.; Gal, G.L.; Durieux, P.; Kouri, D.E.; Honnart, D.; Schmidt, J.; Legall, C.; Hausfater, P.; et al. Multifaceted Intervention to Prevent Venous Thromboembolism in Patients Hospitalized for Acute Medical Illness: A Multicenter Cluster-Randomized Trial. PLOS ONE 2016, 11, e0154832. [Google Scholar] [CrossRef]
- Labarere, J.; Bosson, J.-L.; Sevestre, M.-A.; Sellier, E.; Richaud, C.; Legagneux, A. Intervention Targeted at Nurses to Improve Venous Thromboprophylaxis. Int. J. Qual. Health Care 2007, 19, 301–308. [Google Scholar] [CrossRef]
- Hinchey, J.A.; Shephard, T.; Tonn, S.T.; Ruthazer, R.; Hermann, R.C.; Selker, H.P.; Kent, D.M. The Stroke Practice Improvement Network: A Quasiexperimental Trial of a Multifaceted Intervention to Improve Quality. J. Stroke Cerebrovasc. Dis. 2010, 19, 130–137. [Google Scholar] [CrossRef]
- Writing Group for the CHECKLIST-ICU Investigators and the Brazilian Research in Intensive Care Network (BRICNet); Cavalcanti, A.B.; Bozza, F.A.; Machado, F.R.; Salluh, J.I.F.; Campagnucci, V.P.; Vendramim, P.; Guimaraes, H.P.; Normilio-Silva, K.; Damiani, L.P.; et al. Effect of a Quality Improvement Intervention With Daily Round Checklists, Goal Setting, and Clinician Prompting on Mortality of Critically Ill Patients: A Randomized Clinical Trial. JAMA 2016, 315, 1480. [Google Scholar] [CrossRef]
- Streubel, P.N.; Pachón, M.; Kerguelén, C.A.; Navas, J.; Portocarrero, J.; Pesantez, R.F.; Zayed, G.; Carrillo, G.; Llinás, A.M. Prospective Monitoring Improves Outcomes of Primary Total Hip Replacement: A Cohort Study. Patient Saf. Surg. 2009, 3, 7. [Google Scholar] [CrossRef]
- Anderson, F.A.; Wheeler, H.B.; Goldberg, R.J.; Hosmer, D.W.; Forcier, A.; Patwardhan, N.A. Changing Clinical Practice. Prospective Study of the Impact of Continuing Medical Education and Quality Assurance Programs on Use of Prophylaxis for Venous Thromboembolism. Arch. Intern. Med. 1994, 154, 669–677. [Google Scholar] [CrossRef]
- Fontaine, A.; Mahé, I.; Bergmann, J.F.; Fiessinger, J.N.; Dhote, R.; Cohen, P.; Vinceneux, P. Effectiveness of Written Guidelines on the Appropriateness of Thromboprophylaxis Prescriptions for Medical Patients: A Prospective Randomized Study. J. Intern. Med. 2006, 260, 369–376. [Google Scholar] [CrossRef]
- Dexter, P.R.; Perkins, S.; Overhage, J.M.; Maharry, K.; Kohler, R.B.; McDonald, C.J. A Computerized Reminder System to Increase the Use of Preventive Care for Hospitalized Patients. N. Engl. J. Med. 2001, 345, 965–970. [Google Scholar] [CrossRef]
- Garcia, D.A.; Highfill, J.; Finnerty, K.; Varoz, E.; McConkey, S.; Hutchinson, K.; Libby, E. A Prospective, Controlled Trial of a Pharmacy-Driven Alert System to Increase Thromboprophylaxis Rates in Medical Inpatients. Blood Coagul. Fibrinolysis 2009, 20, 541. [Google Scholar] [CrossRef]
- Piazza, G.; Anderson, F.A.; Ortel, T.L.; Cox, M.J.; Rosenberg, D.J.; Rahimian, S.; Pendergast, W.J.; McLaren, G.D.; Welker, J.A.; Akus, J.J.; et al. Randomized Trial of Physician Alerts for Thromboprophylaxis after Discharge. Am. J. Med. 2013, 126, 435–442. [Google Scholar] [CrossRef]
- Galanter, W.L.; Thambi, M.; Rosencranz, H.; Shah, B.; Falck, S.; Lin, F.-J.; Nutescu, E.; Lambert, B. Effects of Clinical Decision Support on Venous Thromboembolism Risk Assessment, Prophylaxis, and Prevention at a University Teaching Hospital. Am. J. Health. Syst. Pharm. 2010, 67, 1265–1273. [Google Scholar] [CrossRef]
- MaCauley, M.J.; Showalter, J.W.; Beck, M.J.; Chuang, C.H. The Effect of a Provider-Enhanced Clinical Decision Support Tool for Guiding Venous Thromboembolism Pharmacoprophylaxis in Low-Risk Patients. Hosp. Pract. 2012, 40, 7–12. [Google Scholar] [CrossRef]
- Mitchell, J.D.; Collen, J.F.; Petteys, S.; Holley, A.B. A Simple Reminder System Improves Venous Thromboembolism Prophylaxis Rates and Reduces Thrombotic Events for Hospitalized Patients1. J. Thromb. Haemost. 2012, 10, 236–243. [Google Scholar] [CrossRef]
- Umscheid, C.A.; Hanish, A.; Chittams, J.; Weiner, M.G.; Hecht, T.E. Effectiveness of a Novel and Scalable Clinical Decision Support Intervention to Improve Venous Thromboembolism Prophylaxis: A Quasi-Experimental Study. BMC Med. Inform. Decis. Mak. 2012, 12, 92. [Google Scholar] [CrossRef]
- Bhalla, R.; Berger, M.A.; Reissman, S.H.; Yongue, B.G.; Adelman, J.S.; Jacobs, L.G.; Billett, H.; Sinnett, M.J.; Kalkut, G. Improving Hospital Venous Thromboembolism Prophylaxis with Electronic Decision Support. J. Hosp. Med. 2013, 8, 115–120. [Google Scholar] [CrossRef]
- Fuzinatto, F.; Waldemar, F.S.D.; Wajner, A.; Elias, C.A.A.; Fernandez, J.F.; Hopf, J.L.D.S.; Barreto, S.S.M. A Clinical Decision Support System for Venous Thromboembolism Prophylaxis at a General Hospital in a Middle-Income Country. J. Bras. Pneumol. 2013, 39, 138–146. [Google Scholar] [CrossRef]
- Amland, R.C.; Dean, B.B.; Yu, H.; Ryan, H.; Orsund, T.; Hackman, J.L.; Roberts, S.R. Computerized Clinical Decision Support to Prevent Venous Thromboembolism Among Hospitalized Patients: Proximal Outcomes from a Multiyear Quality Improvement Project. J. Healthc. Qual. JHQ 2015, 37, 221. [Google Scholar] [CrossRef]
- Eijgenraam, P.; Meertens, N.; Van Den Ham, R.; Ten Cate, H.; Ten Cate-Hoek, A.J. The Effect of Clinical Decision Support on Adherence to Thrombosis Prophylaxis Guidelines in Medical Patients; A Single Center Experience. Thromb. Res. 2015, 135, 464–471. [Google Scholar] [CrossRef]
- Spirk, D.; Stuck, A.K.; Hager, A.; Engelberger, R.P.; Aujesky, D.; Kucher, N. Electronic Alert System for Improving Appropriate Thromboprophylaxis in Hospitalized Medical Patients: A Randomized Controlled Trial. J. Thromb. Haemost. JTH 2017, 15, 2138–2146. [Google Scholar] [CrossRef]
- Mathers, B.; Williams, E.; Bedi, G.; Messaris, E.; Tinsley, A. An Electronic Alert System Is Associated With a Significant Increase in Pharmacologic Venous Thromboembolism Prophylaxis Rates Among Hospitalized Inflammatory Bowel Disease Patients. J. Healthc. Qual. JHQ 2017, 39, 307. [Google Scholar] [CrossRef]
- Kahn, S.R.; Morrison, D.R.; Cohen, J.M.; Emed, J.; Tagalakis, V.; Roussin, A.; Geerts, W. Interventions for Implementation of Thromboprophylaxis in Hospitalized Medical and Surgical Patients at Risk for Venous Thromboembolism. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Kahn, S.R.; Diendéré, G.; Morrison, D.R.; Piché, A.; Filion, K.B.; Klil-Drori, A.J.; Douketis, J.; Emed, J.; Roussin, A.; Tagalakis, V.; et al. Effectiveness of Interventions for the Implementation of Thromboprophylaxis in Hospitalised Patients at Risk of Venous Thromboembolism: An Updated Abridged Cochrane Systematic Review and Meta-Analysis of Randomised Controlled Trials. BMJ Open 2019, 9, e024444. [Google Scholar] [CrossRef]
- Lenchus, J.D. Transitions in the Prophylaxis, Treatment and Care of Patients with Venous Thromboembolism. Adv. Ther. 2016, 33, 29–45. [Google Scholar] [CrossRef]
- Lee-Ann Hawkins, T.; Lange, I.R.; Gibson, P.S. Compliance With a Perinatal Prophylaxis Policy for Prevention of Venous Thromboembolism After Caesarean Section. J. Obstet. Gynaecol. Can. 2008, 30, 1110–1117. [Google Scholar] [CrossRef]
- Peterson, G.M.; Drake, C.I.; Jupe, D.M.L.; Vial, J.H.; Wilkinson, S. Educational Campaign to Improve the Prevention of Postoperative Venous Thromboembolism. J. Clin. Pharm. Ther. 1999, 24, 279–287. [Google Scholar] [CrossRef]
- Sellier, E. Effectiveness of a Guideline for Venous Thromboembolism Prophylaxis in Elderly Post–Acute Care Patients: A Multicenter Study With Systematic Ultrasonographic Examination. Arch. Intern. Med. 2006, 166, 2065. [Google Scholar] [CrossRef]
- Durieux, P.; Nizard, R.; Ravaud, P.; Mounier, N.; Lepage, E. A Clinical Decision Support System for Prevention of Venous Thromboembolism: Effect on Physician Behavior. JAMA 2000, 283, 2816. [Google Scholar] [CrossRef]
- Roberts, G.W.; Adams, R. Impact of Introducing Anticoagulation-Related Prescribing Guidelines in a Hospital Setting Using Academic Detailing. Ther. Clin. Risk Manag. 2006, 2, 309–316. [Google Scholar] [CrossRef]
- Dobesh, P.P.; Stacy, Z.A. Effect of a Clinical Pharmacy Education Program on Improvement in the Quantity and Quality of Venous Thromboembolism Prophylaxis for Medically Ill Patients. J. Manag. Care Pharm. 2005, 11, 755–762. [Google Scholar] [CrossRef]
- Rashid, S.T.; Thursz, M.R.; Razvi, N.A.; Voller, R.; Orchard, T.; Rashid, S.T.; Shlebak, A.A. Venous Thromboprophylaxis in UK Medical Inpatients. 2005; 98. [Google Scholar]
- Taylor, G.M.; McKenzie, C.A.; Mires, G.J. Use of a Computerised Maternity Information System to Improve Clinical eVectiveness: Thromboprophylaxis at Caesarean Section. 2000. [Google Scholar]
- McEleny, P.; Bowie, P.; Robins, J.B.; Brown, R.C. Getting a Validated Guideline into Local Practice: Implementation and Audit of the Sign Guideline on the Prevention of Deep Vein Thrombosis in a District General Hospital. Scott. Med. J. 1998, 43, 23–25. [Google Scholar] [CrossRef]
- Bullock-Palmer, R.P.; Weiss, S.; Hyman, C. Innovative Approaches to Increase Deep Vein Thrombosis Prophylaxis Rate Resulting in a Decrease in Hospital-acquired Deep Vein Thrombosis at a Tertiary-care Teaching Hospital. J. Hosp. Med. 2008, 3, 148–155. [Google Scholar] [CrossRef]
- O’Connor, C.; Adhikari, N.K.J.; DeCaire, K.; Friedrich, J.O. Medical Admission Order Sets to Improve Deep Vein Thrombosis Prophylaxis Rates and Other Outcomes. J. Hosp. Med. 2009, 4, 81–89. [Google Scholar] [CrossRef]
- Patterson, R. A Computerized Reminder for Prophylaxis of Deep Vein Thrombosis in Surgical Patients. Proc. AMIA Symp. 1998, 573–576. [Google Scholar]
- Mosen, D.; Elliott, C.G.; Egger, M.J.; Mundorff, M.; Hopkins, J.; Patterson, R.; Gardner, R.M. The Effect of a Computerized Reminder System on the Prevention of Postoperative Venous Thromboembolism. Chest 2004, 125, 1635–1641. [Google Scholar] [CrossRef]
- Sedgwick, P.; Greenwood, N. Understanding the Hawthorne Effect. BMJ 2015, h4672. [Google Scholar] [CrossRef]
- Fiumara, K.; Piovella, C.; Hurwitz, S.; Piazza, G.; Niles, C.; Fanikos, J.; Paterno, M.; Labreche, M.; Stevens, L.-A.; Baroletti, S.; et al. Multi-Screen Electronic Alerts to Augment Venous Thromboembolism Prophylaxis. Thromb. Haemost. 2010, 103, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Maynard, G.A.; Morris, T.A.; Jenkins, I.H.; Stone, S.; Lee, J.; Renvall, M.; Fink, E.; Schoenhaus, R. Optimizing Prevention of Hospital-acquired Venous Thromboembolism (VTE): Prospective Validation of a VTE Risk Assessment Model. J. Hosp. Med. 2010, 5, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Lecumberri, R.; Marqués, M.; Díaz-Navarlaz, M.; Panizo, E.; Toledo, J.; García-Mouriz, A.; Páramo, J.A. Maintained Effectiveness of an Electronic Alert System to Prevent Venous Thromboembolism among Hospitalized Patients. Thromb. Haemost. 2008, 100, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Al-Jaghbeer, M.; Dealmeida, D.; Bilderback, A.; Ambrosino, R.; Kellum, J.A. Clinical Decision Support for In-Hospital AKI. J. Am. Soc. Nephrol. JASN 2018, 29, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Nicolaides, A.; Fareed, J.; Spyropoulos, A.C.; Kakkar, A.K.; Antignani, P.; Avgerinos, E. Prevention and Management of Venous Thromboembolism. Int. Angiol. 2024. (In press) [Google Scholar]
- Hostler, D.C.; Marx, E.S.; Moores, L.K.; Petteys, S.K.; Hostler, J.M.; Mitchell, J.D.; Holley, P.R.; Collen, J.F.; Foster, B.E.; Holley, A.B. Validation of the International Medical Prevention Registry on Venous Thromboembolism Bleeding Risk Score. Chest 2016, 149, 372–379. [Google Scholar] [CrossRef]
- Rosenberg, D.J.; Press, A.; Fishbein, J.; Lesser, M.; McCullagh, L.; McGinn, T.; Spyropoulos, A.C. External Validation of the IMPROVE Bleeding Risk Assessment Model in Medical Patients. Thromb. Haemost. 2016, 116, 530–536. [Google Scholar] [CrossRef]
- Solomon, J.; Dauber-Decker, K.; Richardson, S.; Levy, S.; Khan, S.; Coleman, B.; Persaud, R.; Chelico, J.; King, D.; Spyropoulos, A.; et al. Integrating Clinical Decision Support Into Electronic Health Record Systems Using a Novel Platform (EvidencePoint): Developmental Study. JMIR Form. Res. 2023, 7, e44065. [Google Scholar] [CrossRef]
- Mandel, J.C.; Kreda, D.A.; Mandl, K.D.; Kohane, I.S.; Ramoni, R.B. SMART on FHIR: A Standards-Based, Interoperable Apps Platform for Electronic Health Records. J. Am. Med. Inform. Assoc. 2016, 23, 899–908. [Google Scholar] [CrossRef]
- Jenders, J.A.O. , Jonathan Teich, Donald Levick, Luis Saldana, Ferdinand Velasco, Dean Sittig, Kendall Rogers, Robert Improving Outcomes with Clinical Decision Support: An Implementer’s Guide, Second Edition; 2nd ed.; HIMSS Publishing: New York, 2012; ISBN 978-0-367-80612-5. [Google Scholar]
- Ramgopal, S.; Sanchez-Pinto, L.N.; Horvat, C.M.; Carroll, M.S.; Luo, Y.; Florin, T.A. Artificial Intelligence-Based Clinical Decision Support in Pediatrics. Pediatr. Res. 2023, 93, 334–341. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schematics of the flow of data between the health care system, electronic health record (EHR), and health information exchange (HIE). Published with permission from (Solomon, 2023). Doctors launch an EvidencePoint clinical decision support tool from an EHR front-end workflow. The request includes the desired clinical prediction rule (e.g., the Well’s criteria) and the patient’s visit-specific ID. The clinical decision support tool forwards the request to the EvidencePoint application programming interface, which retrieves patient data, prepopulates evaluation answers, and sets the clinical prediction rule calculation logic. After calculating the patient score, the clinical decision support tool returns the score to the EHR front-end workflow.
Figure 1.
Schematics of the flow of data between the health care system, electronic health record (EHR), and health information exchange (HIE). Published with permission from (Solomon, 2023). Doctors launch an EvidencePoint clinical decision support tool from an EHR front-end workflow. The request includes the desired clinical prediction rule (e.g., the Well’s criteria) and the patient’s visit-specific ID. The clinical decision support tool forwards the request to the EvidencePoint application programming interface, which retrieves patient data, prepopulates evaluation answers, and sets the clinical prediction rule calculation logic. After calculating the patient score, the clinical decision support tool returns the score to the EHR front-end workflow.
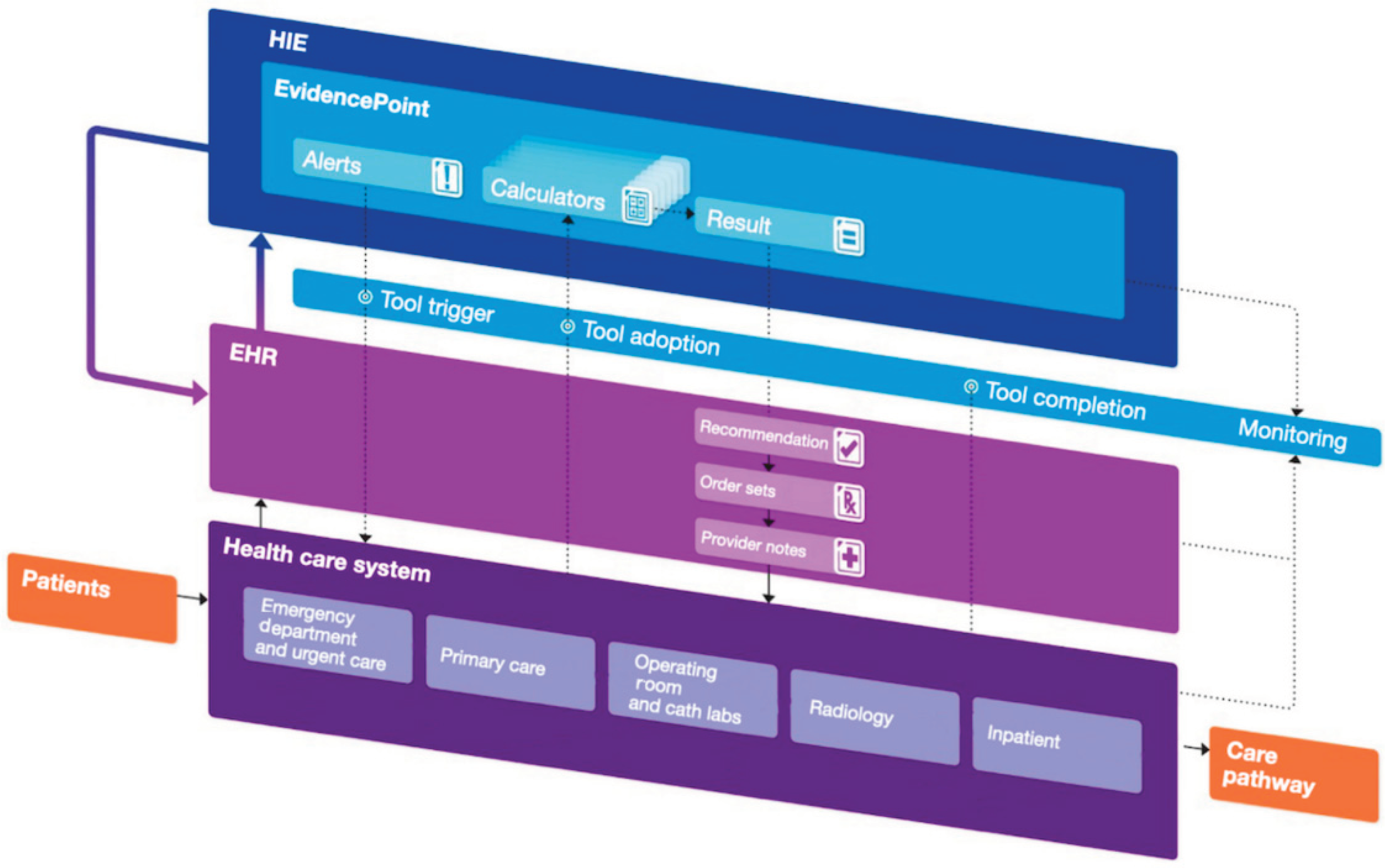
Figure 2.
EvidencePoint platform structure (left) and communication scheme (right). API: application programming interface; CDS: clinical decision support; EHR: electronic health record. (looks low-quality).
Figure 2.
EvidencePoint platform structure (left) and communication scheme (right). API: application programming interface; CDS: clinical decision support; EHR: electronic health record. (looks low-quality).
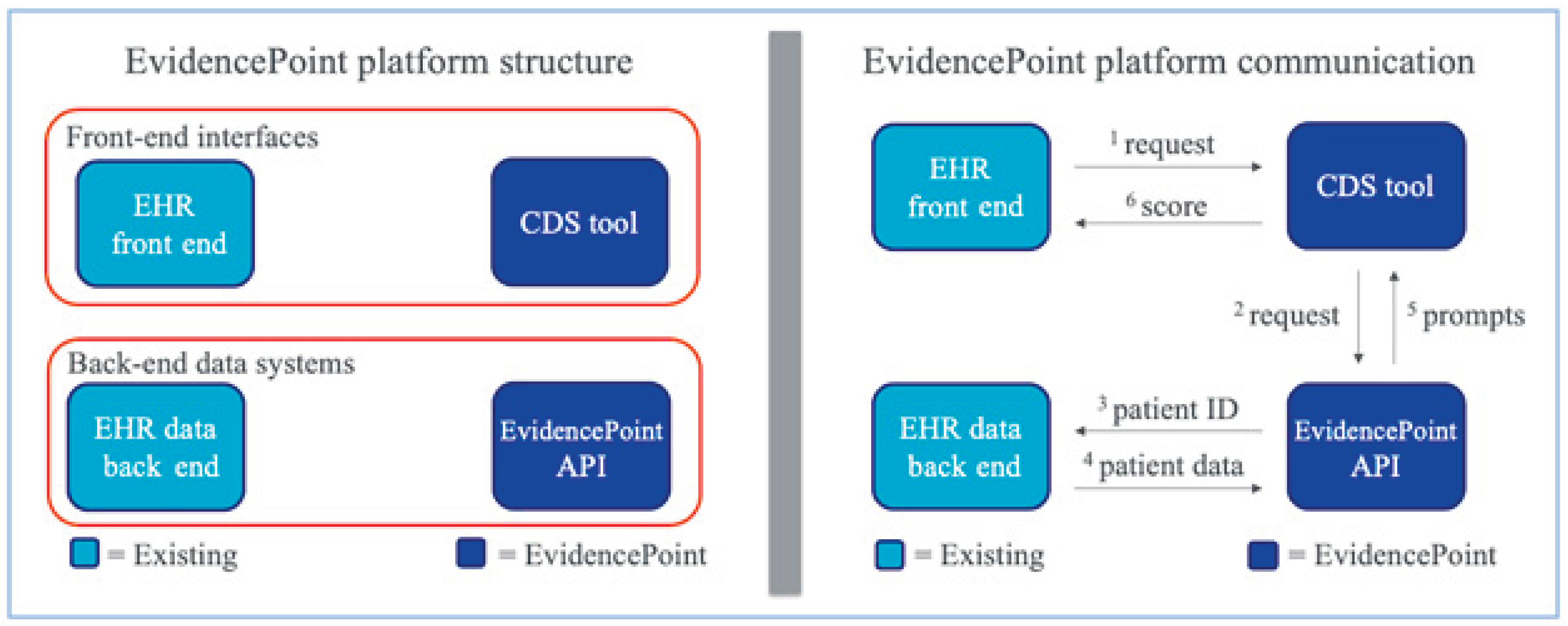
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



