
Submitted:
27 February 2024
Posted:
28 February 2024
Read the latest preprint version here
Abstract
Newborn screening (NBS) is hailed as a public health success, but little is known about what happens to these children after diagnosis. There has been difficulty gathering long-term follow-up (LTFU) data consistently, reliably, and with minimal effort by state NBS programs from clinicians. Six programs have been working towards a core minimal LTFU dataset, starting with data elements proposed by the Advisory Committee on Heritable Disorders in Newborns and Children’s Follow-up and Treatment workgroup (ACHDNC FUTR). This minimal data set could begin to address the impact of early diagnosis by NBS. After three rounds of data collection and revision to a data collection tool that defines the minimal LTFU data elements, the group agreed that it was most important for the dataset to capture two items for the denominator--diagnosis and if the child moved or died—with three outcomes: if the child was still alive, if the child had contact with a specialist, and if they received appropriate care specific to their diagnosis within the year. All six programs were able to provide these data. In 2022, about 83.8% (563/672) of the children in these LTFU programs were alive, 92.0% saw a specialist, and 87.7% received appropriate care.
Keywords:
newborn screening
; public health
; equity
; long-term follow-up data
1. Introduction
Infants born in the United States (US) are universally offered newborn screening (NBS) for specific medical conditions shortly after birth [1,2]. As of January, 2024 there are 37 core conditions and 26 secondary conditions on the Recommended Uniform Screening Panel (RUSP) [3]. Upwards of 6,500 newborns who have NBS blood spot screening are identified with a significant condition each year. That number increases to approximately 13,000 a year when hearing screening is included [4,5]. The goal of NBS is to identify children who are at increased risk of having a condition that can result in death or significant developmental delay before symptoms appear, and can be managed or reversed with prompt efficacious available treatment [1]. Ultimately, the goal is to improve the quality of life for individuals as a result of early detection and treatment commencement [1]. The Centers for Disease Control and Prevention (CDC) has identified NBS as one of the significant public health achievements of the 21st Century [6] yet the efficacy of this program has not yet been tested [1].
NBS is a complex system [2] that involves public health programs, hospitals, birthing providers, couriers, families, insurers, and healthcare providers. This system is intended to be comprehensive, encompassing screening, diagnosis, and long-term care for children with a condition identified through an abnormal screen [7]. Follow-up of affected infants with an out-of-range NBS encompasses two time periods: first from the abnormal screening result until a diagnosis is made (short-term follow-up) and then ongoing clinical care and treatment following a diagnosis (long-term follow-up). As Hoff et al. (2006) state, identifying that an infant has a genetic or metabolic condition is not valuable if that infant is unable to receive timely, appropriate care [8]. The role of follow-up, both short-term and long-term, in NBS is to ensure that newborns identified receive the necessary treatment [9]. NBS follow-up is becoming more difficult and more important as new conditions are added to the RUSP. The most recent additions to the RUSP include severe combined immunodeficiency (SCID) (2010), glycogen storage disease, type II (Pompe) (2015), X-linked adrenoleukodystrophy (X-ALD) (2016), mucopolysaccharidosis, type I (MPS I) (2016), spinal muscular atrophy (SMA) (2018), mucopolysaccharidosis, type II (MPS II) (2022), and guanidinoacetate methyltransferase deficiency (GAMT) (2023) [10]. Treatments for some of the conditions on the RUSP are more complex and expensive, especially for some of the new conditions added (e.g., enzyme replacement therapy and hematopoietic stem cell transplantation) [11]. Additionally, infants may now be identified with a condition shortly after birth (e.g., X-ALD, Pompe disease) that might not require treatment until late childhood or early adulthood [11].
Since 2006, it has been argued that long-term follow-up (LTFU) is needed for NBS to be a meaningful public health activity (Hoff et al., 2006). Currently, the success of NBS in the US is measured using quality indicators which focus on process measures [1]. One of the quality indicators tied to follow-up, focuses on ensuring there is a final resolution for all infants (e.g., screening, diagnosis, or diagnosis ruled out) (Quality Indicator 4) (Newborn Screening Technical assistance and Evaluation Program (NewSTEPs) [12]. The field has had a difficult time, however, gathering data reliably and consistently to determine the impact of NBS on the quality of life for children / adults who were identified with a condition through NBS and determining if they are connected to and receiving care for their condition. A system designed to collect LTFU data could provide insight needed to improve and refine the NBS system.
1.1. Measuring LTFU in NBS
Historically LTFU has been defined as starting once a child has a confirmed diagnosis as a result of an abnormal NBS [13]. The length of LTFU can vary from up until school age, to 18 years of life, or to the entire lifespan [13,14,15]. This definition of the length of LTFU may vary because there are two pieces to LTFU -- public health LTFU and clinical care LTFU [13]. Public health is interested in assessments of health outcomes, care coordination, and ensuring access to treatments / interventions [7], while clinical LTFU focuses on overall health, developmental outcomes, and improving evidence-based treatment [13].
Regardless of the length of time a child is followed, there is agreement that gathering LTFU data is important. There have been many publications on what metrics should be measured for LTFU: (1) whether the child is still alive [1,15,16,17]; (2) health care utilization for both specialty care and primary care (e.g., linked to care; receiving appropriate clinical monitoring and treatment for condition) [8,11,14,15,16,17,18] (3) child’s health status (e.g., growth, development, function) [1,17]; (4) quality of life for the child and family [1,17]; (5) referral to early intervention[1]; and (6) ensuring all families get care (no disparities in LTFU) [17].
While there have been a few research projects that have gathered and looked at LTFU data ([15,19] and one tool, the Longitudinal Pediatric Data Resource (LPDR) which captures genomic and phenotypic data over the lifespan of NBS-identified newborns assessing the impact of early detection and treatment [20], there has been difficulty gathering data consistently and reliably from state NBS programs. This may be because not all NBS programs conduct LTFU [13,15]. Of the 33 states who provided data in the NewSTEPs LTFU Taskforce survey conducted in January and February of 2020, five (15%) reported they fully implemented LTFU and another five (15%) said they had partially implemented a LFTU program [13]. It should be noted that it is unclear from the report if the respondents in this survey were provided with a LTFU definition given that the Taskforce was using the data to create one. There is also a lack of standards for data elements, sources, and case definitions [15]. The lack of standards may be due to different stakeholder groups who can provide insight into the effectiveness of LTFU; these groups can provide data from sources they have access to and bring their own perspectives to what successful LTFU looks like. While different stakeholders can have different ideas on what to collect for LTFU or have different abilities to collect data; these systems may converge around a few key LTFU indicators.
1.2. Minimal LTFU Data Set
There has been difficulty gathering LTFU data reliably and consistently from the majority of NBS programs because of the variety of data elements suggested and tested for in LTFU. While this variety mirrors the complexity of LTFU, the authors of this paper feel that it may be more important to find a starting place that allows more states to contribute data, and then start work towards gathering the more complex data elements. As Lloyd-Puryear & Brower [2] recommended, we are attempting to start in an incremental fashion, allowing us to create concrete data definitions, thus we proposed the NBS LTFU minimal data set. The goal is to identify data elements of interest to all LTFU that can be gathered reliably, consistently, and with minimal burden to the existing NBS infrastructures. We recognize that these data will generate more questions, but it is a beginning to answer if affected children reap the intended benefits of NBS for improving long-term health by first quantifying how many receive appropriate care over time.
2. Materials and Methods
Six programs—four state programs (CT, CO/WY, NY, ND), one university program (UCSF), and one professional foundation (the American College of Medical Genetics(ACMG)) were funded by HRSA (HRSA-21-079) to “expand the ability of state public health agencies to provide screening, counseling and services” to the families of newborns and children diagnosed with a condition as a result of an abnormal newborn screen. “The purpose of the program is to support comprehensive models of long-term follow-up that demonstrate collaborations between clinicians, public health agencies, and families” (HRSA-21-079 funding opportunity announcement, pg. i).
During a regularly scheduled meeting between all six programs, there was discussion on working towards a core LTFU dataset. As part of these discussions, the six programs talked to different stakeholders who would use LTFU data (See Figure 1) and what questions each stakeholder group might ask from LTFU data. As part of this discussion, a diagram was created (See Figure 1) and goals around creating a core LTFU dataset were created. The group decided that the minimal data set discussed by the Advisory Committee of Heritable Disorders in Newborns and Children’s Follow-Up and Treatment Workgroup (ACHDNCs FUTR) [16], would be data all stakeholders would use and therefore this was represented in the diagram at the convergence point.
A smaller group then met to identify the core LTFU data set that could be tested by the six programs. To start, the six programs compared the data their program was gathering, how the data was gathered (e.g., source), and the format of the data collected (e.g., drop-down list, yes/no, numeric value). Because of the lack of consistency between the programs’ LTFU data, the decision was made to focus on the core data set and test whether the six programs could gather a minimal LTFU data set to address the effectiveness of NBS.
2.1. Approach
The six programs then met on May 9-10, 2023; five attended in person and one program attended virtually. The goal for the meeting was to identify the minimum needed data set that the majority of states, reliably, consistently, and with minimum burden, could collect. The participants looked at what data had been collected by previous programs as well as their own and discussed the feasibility of gathering the data elements that had been proposed by the ACHDNC FUTR (2019) meeting as a minimal LTFU data set: (1) diagnosis, (2) if the child was still alive, (3) date of appropriate first intervention, and (4) if the child received care and treatment within the last 12 months specific to the diagnosis, and if yes, (5) the type of care provider the child saw. As part of this discussion, the group looked at each LTFU data element proposed and discussed the (1) data element, (2) potential data sources, (3) if the element could be obtained from all participating programs reliably and efficiently, and (4) what were the lowest common data values that could be gathered. Next, the group discussed what was needed to create a common denominator so that percentages could be generated.
The group agreed to pull 2022 data, meet again to discuss the process, and make clarifications to definitions and the data elements as needed. For the data pull, children were put into age groups based on their age on the last day of the evaluation year, December 31, 2022. Rather than looking at individual children, the group decided to look at age groups within that calendar year. Specifically, we grouped children born in 2018 (4 year to < 5 years), 2019 (3 years to <4 years), 2020 (2 year to <3 years), 2021 (1 year to <2 years), and 2022 (<1 year) and reported on their status in 2022 for the 5 questions mentioned above. Each participating team was assigned a condition to provide data.
2.2. LTFU Data Collection
To date (February 2024), the group has pulled data three times to test and refine the process. All six programs have developed systems to extract data. Table 2 shows the sources used to pull data and the limitations noted by each program.
3. Results
3.1. Defining Data Elements
The full minimal LTFU dataset that was initially tested included (1) diagnosis, (2) if the child was still alive, deceased, or had moved, (3) age of first documented contact per the NewSTEPs definition, (4) data about cause of death, if applicable, (5) if the child received appropriate care specific to the diagnosis within the last 12 months and is the receiving LTFU care (6) number of children lost to follow up, (7) the number actively engaged (for opt-in programs), and if the child is being seen, (8) the type of care provider who provided care and treatment to the child (PCP, specialist, or both). However, it became clear that it was difficult to gather all eight data elements; the group agreed that it was most important for a minimal LTFU dataset to capture two data elements to create a denominator –diagnosis and how many children moved or died the previous year—and three data elements to measure outcome--if the child was still alive, if the child had contact with the specialist within the last 12 months, and if the child received appropriate care specific to the diagnosis within the last 12 months.
3.1.1. Denominator
To calculate percentages reliably across NBS follow-up programs, the minimal data set must include a comparable denominator. For the minimal LTFU dataset, the denominator represents the number of children within the birth cohort who have been diagnosed as having the condition, including those cases which were diagnosed after the NBS but are known to the NBS program, minus those who died or moved their care out of the jurisdiction prior to the year being reported (i.e., in our case those who died or moved prior to January 1, 2022).
Diagnosis was a descriptive variable to pull, report, and analyze. It was included for two reasons (1) the data may come from different clinics and (2) it informs what health care the child should receive (appropriate care specific to the diagnosis) and allows for data users to see if there is an outcome difference by disorder. The group categorized NBS disorders as follows: (1) metabolic conditions; (2) congenital adrenal hyperplasia (CAH); (3) congenital hypothyroidism (CH), (4) hemoglobinopathies, (5) cystic fibrosis (CF), (6) SCID, (7) T-Cell lymphopenia, (8) SMA, and (9) X-ALD. The metabolic conditions were categorized together due to similar follow-up recommendations and clinical specialists; the same was done for the hemoglobinopathies. A child was determined to fit into the diagnosis category if the program providing information confirmed the child had that diagnosis using the established NBS public health case definitions [21].
3.1.2. Numerators
Initially, the team tested seven outcomes -- (1) if the child was still alive, (2) age of first documented contact per the NewSTEPs definition, (3) if the child received appropriate care specific to the diagnosis within the last 12 months and is the child receiving LTFU care, (4) the number of children lost to follow up, (5) the number actively engaged in LTFU (for opt-in programs), (6) if the child was seen by a primary care provider and/or specialist, and (7) the type of care provider who provided care and treatment to the child (PCP, specialist, or both). After round one of data collection, it became clear it was too difficult to gather age of first documented contact per the NewSTEPs definition, the number actively engaged in LTFU (for opt-in programs), and if the child is being seen by the PCP. At the outset, the group had also proposed collecting data on the cause of death to better understand the role of NBS; however, these data were challenging to collect and thus, were not included in the final analysis.
3.1.2.1. Alive
The primary outcome variable discussed for the minimal data set is whether the child is alive or not. A child was counted as being alive if they were not classified as deceased in the clinic’s electronic health record (EHR). This variable was included in the final minimal LTFU data set.
3.1.2.2. Received Care and Treatment Specific to Diagnosis
Another outcome variable considered was connection to treatment. The group discussed that not every condition requires seeing a specialist annually, and as a result, the minimal data set should capture the number of cases receiving appropriate care for their condition based on recommendations within a 12-month period. This was altered during discussion to answer two questions (1) did the child have at least one contact with a specialist either in-person, via telehealth, email, or a phone call and (2) did the child see the appropriate specialist on the recommended cadence for care within the state/jurisdiction (e.g., quarterly visits for children with cystic fibrosis). For the final data set, appropriate care was defined as the number of children seeing the appropriate specialist on the recommended cadence for care within their state/jurisdiction. In some cases, it may also include obtaining laboratory test results or procedures at the frequency appropriate for their condition.
3.2. Analysis of LTFU Data
Long-term follow-up data for 672 children were submitted by the six programs for 2022. Five birth cohorts were shared (2018-2022), although not all programs were able to report for all birth cohorts (Table 3). A large proportion of children had data provided in 2022 across all cohorts and disorders. Some children moved their care out of the jurisdiction or died prior to 2022, leaving 563 in LTFU during the reporting year. Of those 563, over 90% had at least one documented contact with an appropriate care provider; this proportion decreased slightly in older age cohorts (Table 3). Across all disorders, this number drops to 85% for the 2018 cohort. This contact may have been in the form of a clinic visit, a telehealth visit, or a phone call; these visits were documented to confirm that the specialist was still in contact with the child.
Programs also reported the number of children who met the program-defined condition-specific recommendations for care. While fewer children met those guidelines, 87% did in aggregate and >82% met the guidelines across all age groups when looking at all NBS disorders.
Disorder-specific numbers are presented for each cohort, but due to small numbers and differences between the disorders reported by programs, no comparisons can be made.
Follow-up and connection with clinical providers at specific ages demonstrates that most children are being seen by appropriate clinical providers at age three years using the 2019 birth cohort, for example, with greater than 94% success.
4. Discussion
Since 2006 there has been a call for the NBS field to gather and analyze LTFU data to evaluate the impact of newborn screening. While many have worked towards this goal [2,8,11,15,16,17,18] it has become clear that there is a need to codify a minimal data set to make data collection more feasible. Our team started with the five LTFU questions posed by ACHDNCs FUTR in 2019 [6] and quickly learned that it was too difficult to gather data to address all those questions. Our team was able to address three questions – (1) is the child alive, (2) is the child getting care for their condition, and (3) is the care the child is receiving appropriate for their condition. This basic insight also allows all stakeholder groups – public health programs, research groups, and clinical care providers – to look more closely at the data and determine if there is inequity in groups who are deceased or are not connected to care after diagnosis of a newborn screening condition. Furthermore, once a system is in place and the minimal LTFU data is being gathered, there is an opportunity to start exploring the other questions that may be more difficult to answer at present.
All six programs- four state newborn screening programs, a university research program, and a national research program--were able to provide LTFU data. Overall, the results from our analysis look promising for the impact of NBS. In 2022, 83.8% of the children in these LTFU programs were alive and still living in the jurisdiction of the follow-up system, 92% of those had contact with a specialist, and 87.7% were receiving appropriate care.
Determining the well-being of children identified by newborn screening has been a topic of discussion since the founding advisory committee members started discussion a national recommendation panel [22,23]. The LTFU data presented here provides evidence that children can be identified through public health long-term follow-up systems, and the vast majority are being followed by the appropriate clinical providers and meeting the recommended guidelines for follow-up. The challenge for the public health system moving forward is to identify those who are not receiving the appropriate care and seek solutions to any barriers families may be encountering. The next step is to expand LTFU data collection to more newborn screening programs; this will help determine the feasibility of the minimal LTFU data set proposed and could help in discussions around setting benchmarks around what the rate/goals should be for each outcome.
4.1. Limitations
There are a few limitations for this project. First, two programs are consent-based and therefore their samples may not be representative for their states. For the UCSF program follow-up rates are high. Patients who have not consented may be receiving care outside of the seven Immunology Centers of Excellence in the state and are not reflected in our report.
For other programs, the data relies on children within a healthcare system, potentially excluding those not connected to any healthcare system, leading to the potential underrepresentation of specific demographic groups. Most programs did not have a process for tracking patients who had moved their care out of state or to a provider not affiliated with the state NBS. Future efforts may need to establish a national system to follow patients who relocate and move their care out of jurisdiction.
Another notable limitation in determining if patients have had a visit in the past 12 months is the restricted connectivity of PCPs and specialists to health information exchange (HIE). It can be particularly difficult to collect these data from PCP sites that still rely on paper records or non-interfacing Electronic Health Record (EHR) systems with HIEs. However, this limitation could decrease over time as more practices adopt electronic health records, and HIEs become more interoperable. Lastly, the sample size is small, as data collection focused on specific conditions over a limited timeframe. There is potential for a more comprehensive understanding of the impact of newborn screening with an expanded data collection effort over time.
5. Conclusion
While a minimal LTFU data set is not ideal to fully answer the question about the impact of NBS on the public, it is a feasible starting point. Ensuring that children are followed by care providers and receiving appropriate care as established within their states is reassuring for public health professionals. It is not the responsibility of public health to monitor changes in clinical care or to ensure a child is following all the clinical recommendations for care. Rather, it is the duty of the public health system to confirm that children with a disorder diagnosed as the result of an abnormal NBS have access to appropriate care [7], and when children are not receiving care to identify and remove barriers. This should be seen as the responsibility of the public health system and not just the newborn screening programs, as ensuring access to care can be a monumental task that requires the input of all interested parties.
Author Contributions
Conceptualization, YKG, MS, formal analysis, MS, KR, KC, LB, ABu, KN, SF funding acquisition, all authors; investigation, KR, KC, LB, ABu, KN, SF; methodology, all authors; project administration, all authors; supervision, YKG, MS; writing—original draft, YKG, MS, LB, KR, SF, KN, MC; writing—review and editing, GN, MC, KC, MD, ABr, ABu, KC, ML, JT, MD; All authors have read and agreed to the published version of the manuscript.
Funding
The programs who took part are supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) as part of an award totaling $6,392,409 with 0% financed with non-governmental sources. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the U.S. Government. For more information, please visit HRSA.gov.
Institutional Review Board
Five underwent review by the respective Institutional Review Board – the University of California San Francisco group, the New York state team, the Colorado/Wyoming team, Connecticut’s Children team, and the American College of Medical Genetics (ACMG). The University of California San Franscico got IRB approval. The other IRBs determined the projects to be not human subjects research. In addition, the seven clinical sites that submitted data to the ACMG effort also discussed the project with their Institutional Review Boards and all of them determined that this was not human subjects’ research. The other program did not require IRB approval. It should be noted that no personally identifiable information was shared by or between programs.
Data Availability
Data are available upon request to the primary (Yvonne.kellarguenther@CPHInnovation.org) or senior author (Marci.sontag@CPHInnovation.org).
References
- Bailey Jr: Donald B. “Early Intervention and Newborn Screening: Parallel Roads or Divergent Highways?” Infants & Young Children 34, no. 1 (2021): 3-16. [CrossRef]
- Lloyd-Puryear, M. A., and A. Brower. “Long-Term Follow-up in Newborn Screening: A Systems Approach for Improving Health Outcomes.” Genet Med 12, no. 12 Suppl (2010): S256-60. [CrossRef]
- Advisory Committee on Heritable Disorders in Newborns and Children. “Recommended Uniform Screening Panel.” https://www.hrsa.gov/advisory-committees/heritable-disorders/rusp (accessed January 2024).
- Gaviglio, A., S. McKasson, S. Singh, and J. Ojodu. “Infants with Congenital Diseases Identified through Newborn Screening-United States, 2018-2020.” Int J Neonatal Screen 9, no. 2 (2023). [CrossRef]
- Sontag, M. K., C. Yusuf, S. D. Grosse, S. Edelman, J. I. Miller, S. McKasson, Y. Kellar-Guenther, M. Gaffney, C. F. Hinton, C. Cuthbert, S. Singh, J. Ojodu, and S. K. Shapira. “Infants with Congenital Disorders Identified through Newborn Screening - United States, 2015-2017.” MMWR Morb Mortal Wkly Rep 69, no. 36 (2020): 1265-68. [CrossRef]
- Domestic Public Health Achievements Team, CDC. “Ten Great Public Health Achievements — United States, 2001–2010.” MMWR Morb Mortal Wkly Rep 60, no. 19 (2011): 619-23.
- Clinical Laboratory and Standards Institute. “Clsi: Newborn Screening Follow-up and Education, 3rd Edition, Nbs02.” 2023.
- Hoff, T., and A. Hoyt. “Practices and Perceptions of Long-Term Follow-up among State Newborn Screening Programs.” Pediatrics 117, no. 6 (2006): 1922-9. [CrossRef]
- Darby, E., J. Thompson, C. Johnson, S. Singh, and J. Ojodu. “Establishing a National Community of Practice for Newborn Screening Follow-Up.” Int J Neonatal Screen 7, no. 3 (2021). [CrossRef]
- Singh, S., J. Ojodu, A. R. Kemper, W. K. K. Lam, and S. D. Grosse. “Implementation of Newborn Screening for Conditions in the United States First Recommended During 2010-2018.” Int J Neonatal Screen 9, no. 2 (2023). [CrossRef]
- Kemper, A. R., C. A. Boyle, J. P. Brosco, and S. D. Grosse. “Ensuring the Life-Span Benefits of Newborn Screening.” Pediatrics 144, no. 6 (2019). [CrossRef]
- Yusuf, C., M. K. Sontag, J. Miller, Y. Kellar-Guenther, S. McKasson, S. Shone, S. Singh, and J. Ojodu. “Development of National Newborn Screening Quality Indicators in the United States.” Int J Neonatal Screen 5, no. 3 (2019): 34. [CrossRef]
- NewSTEPs Long-Term Follow-up Workforce. “Long Term Follow-up Taskforce Activities.” https://www.newsteps.org/sites/default/files/resources/download/LTFU%20Taskforce%20Report_EducationalResource_February2021.pdf (accessed January 2023).
- Kemper, A. R., C. A. Boyle, J. Aceves, D. Dougherty, J. Figge, J. L. Fisch, A. R. Hinman, C. L. Greene, C. A. Kus, J. Miller, D. Robertson, J. Telfair, B. Therrell, M. Lloyd-Puryear, P. C. van Dyck, and R. R. Howell. “Long-Term Follow-up after Diagnosis Resulting from Newborn Screening: Statement of the Us Secretary of Health and Human Services’ Advisory Committee on Heritable Disorders and Genetic Diseases in Newborns and Children.” Genet Med 10, no. 4 (2008): 259-61. [CrossRef]
- Hinton, C. F., C. T. Mai, S. K. Nabukera, L. D. Botto, L. Feuchtbaum, P. A. Romitti, Y. Wang, K. N. Piper, and R. S. Olney. “Developing a Public Health-Tracking System for Follow-up of Newborn Screening Metabolic Conditions: A Four-State Pilot Project Structure and Initial Findings.” Genet Med 16, no. 6 (2014): 484-90. [CrossRef]
- Advisory Committee on Heritable Disorders in Newborn and Children Follow Up and Treatment Workgroup. “Workgroup Report April 2019.” https://public3.pagefreezer.com/browse/health-resources-and-services-administration/10-08-2022T13:11/https://www.hrsa.gov/sites/default/files/hrsa/advisory-committees/heritable-disorders/meetings/20190423/Day2-Kus-FollowupTreatment.pdf (accessed January 2024).
- Hinton, C. F., C. J. Homer, A. A. Thompson, A. Williams, K. L. Hassell, L. Feuchtbaum, S. A. Berry, A. M. Comeau, B. L. Therrell, A. Brower, K. B. Harris, C. Brown, J. Monaco, R. J. Ostrander, A. E. Zuckerman, C. Kaye, D. Dougherty, C. Greene, N. S. Green, up Follow, Newborns Treatment Sub-committee of the Advisory Committee on Heritable Disorders in, and Children. “A Framework for Assessing Outcomes from Newborn Screening: On the Road to Measuring Its Promise.” Mol Genet Metab 118, no. 4 (2016): 221-9.
- Hoff, T., M. Ayoob, and B. L. Therrell. “Long-Term Follow-up Data Collection and Use in State Newborn Screening Programs.” Arch Pediatr Adolesc Med 161, no. 10 (2007): 994-1000. [CrossRef]
- Chan, K., Z. Hu, L. W. Bush, H. Cope, I. A. Holm, S. F. Kingsmore, K. Wilhelm, C. Scharfe, and A. Brower. “Nbstrn Tools to Advance Newborn Screening Research and Support Newborn Screening Stakeholders.” Int J Neonatal Screen 9, no. 4 (2023). [CrossRef]
- Brower, A., K. Chan, M. Hartnett, and J. Taylor. “The Longitudinal Pediatric Data Resource: Facilitating Longitudinal Collection of Health Information to Inform Clinical Care and Guide Newborn Screening Efforts.” Int J Neonatal Screen 7, no. 3 (2021). [CrossRef]
- Sontag, M. K., D. Sarkar, A. M. Comeau, K. Hassell, L. D. Botto, R. Parad, S. R. Rose, K. A. Wintergerst, K. Smith-Whitley, S. Singh, C. Yusuf, J. Ojodu, S. Copeland, and C. F. Hinton. “Case Definitions for Conditions Identified by Newborn Screening Public Health Surveillance.” Int J Neonatal Screen 4, no. 2 (2018): 16. [CrossRef]
- Coleman, C. L., M. Morrison, S. K. Perkins, J. P. Brosco, and E. L. Schor. “Quality of Life and Well-Being for Children and Youth with Special Health Care Needs and Their Families: A Vision for the Future.” Pediatrics 149, no. Suppl 7 (2022). [CrossRef]
- American College of Medical Genetics Newborn Screening Expert, Group. “Newborn Screening: Toward a Uniform Screening Panel and System--Executive Summary.” Pediatrics 117, no. 5 Pt 2 (2006): S296-307. [CrossRef]
Figure 1.
LTFU Stakeholders and Potential LTFU Data.
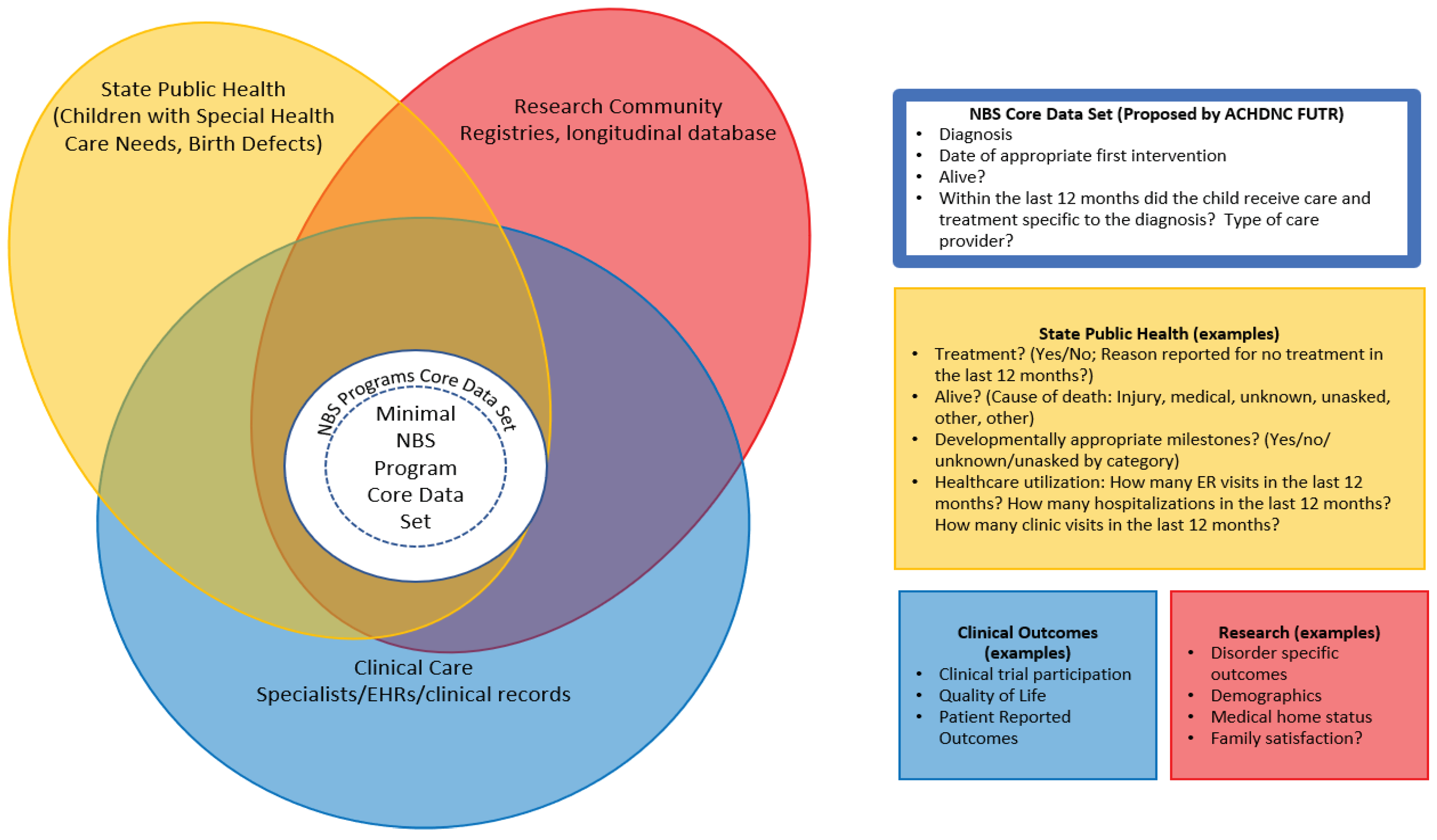

Table 1.
LTFU Focus of the Six Collaborating Programs for this Project.
| Program | LTFU Program Focus (overall goal, conditions focused on, time period) |
| CO/WY | To ensure all children identified through newborn screening in Colorado/Wyoming are receiving appropriate follow-up for their disorders, and to identify barriers leading to a child not receiving appropriate care. The program tracks all newborn screened conditions, 2002 – present, except for CH, these patients are followed separately. |
| CT | The Connecticut Newborn Screening Network aims to ensure timely and appropriate follow-up care for people diagnosed with a condition through newborn screening in CT. Utilizing electronic health record-based registries and dashboards, the network emphasizes comprehensive care coordination for optimal long-term outcomes. The Network’s LTFU registry currently tracks patients identified with a condition through newborn screening in CT since March 1, 2019, except for CF, CCHD, or hearing screen; as those patients are followed by separate programs. |
| NY | The goal of NY’s LTFU project is to develop a sustainable infrastructure to expand the newborn screening LTFU patient registry to include all the inherited metabolic disorders (IMD) on the newborn screening panel. |
| ND | To ensure that newborns and children identified through newborn screening (NBS) achieve the best possible outcomes by utilizing a comprehensive model of LTFU that demonstrates collaborations between clinicians, public health agencies and families to create a system of care that can assess and coordinate follow-up and treatment of newborn screening conditions. |
| UCSF | To design and implement a comprehensive, family-centered LTFU program that becomes the standard for following clinical outcomes, supporting child and caregiver well-being, and anticipating future needs of children with Severe Combined Immunodeficiency (SCID) and T-cell lymphopenia (TCL) disorders. |
| ACMG | To develop a comprehensive LTFU model system demonstrating collaborations between clinicians, public health agencies, and families and assure the best possible outcomes for individuals identified through newborn screening. The project uses spinal muscular atrophy (SMA) as a model collecting data on cases within the first five years of life, engaging with up to five clinical sites, and reporting annual, de-identified aggregated data to state programs through the use of online dashboards. The type and scope of data collected was informed by parents and families with a family member who has SMA. |
Table 2.
Data Sources Utilized by Program.
| Programs | Data Source(s) | Data Limitations |
| CO/WY | Clinic data EHR (EPIC) | Follow-up with specialists outside of primary children’s hospital may be missed |
| CT | Clinic data EHR (EPIC) and Epic Care Everywhere Health Information Exchange | Follow-up with specialists outside of primary children’s hospital can be missed if not sent to health information exchange |
| NY | Lab Information System, Electronic Medical Record (EHR) Data System from Specialty Centers | Need Informed Consent |
| ND | Vital Records, Care Coordination Module within the North Dakota Health Information Network (NDHIN), LTFU records | Starting screening for Pompe/MPSI in 2024, Limited data for SMA |
| UCSF | EHR (EPIC) | Need Informed Consent, unable to report on deceased patients. |
| ACMG | Pediatric neurologists | Only retrospective data based on a REDCap survey with 81 questions (53/81 longitudinal) with up to five years of life per case; minimum of one case per center |
Table 3.
Findings from the Long-Term Follow-Up Data Submitted by the Six Programs.
| Birth Cohort | Diagnosis as determined by published case definitions [21] | Children known to be alive and living in the jurisdiction/number of children with disorder | Children who had at least one contact with specialist/ number of children known to be alive and in jurisdiction | Children receiving appropriate care/number of children know to be alive and in jurisdiction |
| All Birth Cohorts | All NBS Disorders Reported | 563/672(83.8%) | 518/563(92.0%) | 494/563(87.7%) |
| 2018 | All NBS Disorders Reported | 67/91(73.6%) | 57/67(85.1%) | 55/67(82.1%) |
| 2019 | 100/132(75.8%) | 94/100(94.0%) | 94/100(94.0%) | |
| 2020 | 129/155(83.2%) | 121/129(93.8%) | 114/129(88.4%) | |
| 2021 | 139/155(89.7%) | 124/139(89.2%) | 116/139(83.5%) | |
| 2022 | 128/139(92.1%) | 122/128(95.3%) | 115/128(89.8%) | |
| 2018 | Metabolic Conditions | 20/24(83.3%) | 15/20(75.0%) | 15/20(75.0%) |
| 2019 | 18/24(75.0%) | 14/18(77.8%) | 14/18(77.8%) | |
| 2020 | 29/34(85.3%) | 26/29(89.7%) | 20/29(69.0%) | |
| 2021 | 38/40(95.0%) | 29/38(76.3%) | 25/38(65.8%) | |
| 2022 | 28/29(96.6%) | 24/28(85.7%) | 21/28(75.0%) | |
| 2018 | Congenital Adrenal Hyperplasia | 8/10(80.0%) | 8/8(100.0%) | 7/8(87.5%) |
| 2019 | 8/11(72.7%) | 8/8(100.0%) | 8/8(100.0%) | |
| 2020 | 8/8(100.0%) | 7/8(87.5%) | 7/8(87.5%) | |
| 2021 | 10/10(100.0%) | 9/10(90.0%) | 8/10(80.0%) | |
| 2022 | 6/6(100.0%) | 6/6(100.0%) | 6/6(100.0%) | |
| 2018 | Congenital Hypothyroidism | None reported | None reported | None reported |
| 2019 | 16/26(61.5%) | 16/16(100.0%) | 16/16(100.0%) | |
| 2020 | 29/37(78.4%) | 29/29(100.0%) | 29/29(100.0%) | |
| 2021 | 32/39(82.1%) | 32/32(100.0%) | 32/32(100.0%) | |
| 2022 | 29/35(82.9%) | 29/29(100.0%) | 27/29(93.1%) | |
| 2018 | Hemoglobinop-athies | 10/19(52.6%) | 9/10(90.0%) | 8/10(80.0%) |
| 2019 | 19/26(73.1%) | 18/19(94.7%) | 18/19(94.7%) | |
| 2020 | 22/29(75.9%) | 19/22(86.4%) | 18/22(81.8%) | |
| 2021 | 18/21(85.7%) | 15/18(83.3%) | 13/18(72.2%) | |
| 2022 | 20/21(95.2%) | 20/20(100.0%) | 18/20(90.0%) | |
| 2018 | Cystic Fibrosis | 17/21(81.0%) | 16/17(94.1%) | 16/17(94.1%) |
| 2019 | 23/27(85.2%) | 23/23(100.0%) | 23/23(100.0%) | |
| 2020 | 21/22(95.5%) | 21/21(100.0%) | 21/21(100.0%) | |
| 2021 | 14/17(82.4%) | 13/14(92.9%) | 13/14(92.9%) | |
| 2022 | 20/21(95.2%) | 20/20(100.0%) | 20/20(100.0%) | |
| 2018 | Severe Combined Immunodeficiency (SCID) | 6/11(54.5%) | 3/6(50.0%) | 3/6(50.0%) |
| 2019 | 6/8(75.0%) | 5/6(83.3%) | 5/6(83.3%) | |
| 2020 | 11/14(78.6%) | 10/11(90.9%) | 10/11(90.9%) | |
| 2021 | 4/4(100.0%) | 3/4(75.0%) | 3/4(75.0%) | |
| 2022 | 9/10(90.0%) | 7/9(77.8%) | 7/9(77.8%) | |
| 2018 | non-SCID T cell lymphopenia | 4/4(100.0%) | 4/4(100.0%) | 4/4(100.0%) |
| 2019 | 4/4(100.0%) | 4/4(100.0%) | 4/4(100.0%) | |
| 2020 | 1/1(100.0%) | 1/1(100.0%) | 1/1(100.0%) | |
| 2021 | 4/4(100.0%) | 4/4(100.0%) | 4/4(100.0%) | |
| 2022 | 8/8(100.0%) | 8/8(100.0%) | 8/8(100.0%) | |
| 2018 | Spinal Muscular Atrophy | 2/2(100.0%) | 2/2(100.0%) | 2/2(100.0%) |
| 2019 | 6/6(100.0%) | 6/6(100.0%) | 6/6(100.0%) | |
| 2020 | 8/10(80.0%) | 8/8(100.0%) | 8/8(100.0%) | |
| 2021 | 19/20(95.0%) | 19/19(100.0%) | 18/19(94.7%) | |
| 2022 | 8/9(88.9%) | 8/8(100.0%) | 8/8(100.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



