
Submitted:
29 February 2024
Posted:
01 March 2024
You are already at the latest version
Abstract
Tinnitus is a symptom often associated with hearing loss (HL) and is in many cases more burdening to the individual than the HL itself. Many approaches have been made to explain the development and chronification of the phantom percept as well as different treatment strategies to lower the tinnitus related burden. In many studies, the variance of the HL data is high and therefore the interpretation of specific data might be difficult. With this retrospective study, we attempt to explain a part of this variance by investigating specifically the effects of non-auditory comorbidity categories on pure-tone audiometric data in a tinnitus patient collective that was homogeneous with respect to auditory comorbidities. We found age dependent as well as number of non-auditory comorbidity (e.g. diabetes mellitus) dependent differences in the mean HL of the tinnitus patients as well as differences in the peak HL frequency relative to the tinnitus frequency. The analysis of the age dependent HL within the different non-auditory comorbidities revealed specific – partially opposed – effects of endocrine, circulatory, muscle-skeletal and digestive disease categories on the hearing thresholds of tinnitus patients. Taken together we argue that in future tinnitus (and non-tinnitus) patient studies also non-auditory comorbidities should be taken into account as possible covariables that might explain the variance found in the auditory threshold development of these patients.
Keywords:
tinnitus
; comorbidities
; audiometry
; retrospective patient study
1. Introduction
Tinnitus – the percept of sound without a physical source – is a symptom often associated with hearing loss (HL) but can also occur without it [1,2,3,4]. Tinnitus is often the more burdening problem than the HL itself [5,6] and is responsible for yearly costs of at least 21.9 billion Euro in Germany alone [7]. It is still unclear, how tinnitus develops and chronifies exactly, even though several models try to explain these mechanisms from different angles e.g., [8,9,10,11,12,13,14,15]. Due to the individual and very complex pathologies of tinnitus and still too little knowledge there is no causal therapy for this condition. Nevertheless, recently several model-based treatment approaches have been developed and applied with more or less success e.g., [16,17,18,19,20,21,22]. Restoration of hearing is one of such approaches that leads to a reduction of the tinnitus percept loudness [23,24,25]. One of the major problems of all studies with tinnitus patients is the huge variability in the data [26,27,28]; this heterogeneity of tinnitus is also reflected in the patients’ audiograms. This is on the one hand a trivial problem, as tinnitus can be a symptom of HL, as mentioned above, and is therefore also dependent on cofactors like the patients’ age (e.g., occurrence of presbyacusis). On the other hand, other diseases of the auditory system or non-auditory comorbidities can have an influence on HL and / or the occurrence of tinnitus [29,30,31,32] and therefore add further variance to the patients’ data. All these different covariables make the measurement of “baseline” tinnitus data and successively the changes during treatments difficult and hard to interpret.
In this retrospective study, we investigate possible correlations of non-auditory comorbidities on the HL in patients that primarily came to the ENT hospital in Erlangen because of their suffering from tinnitus and without any severe auditory comorbidities except HL.
2. Materials and Methods
2.1. Patient Collective and Ethics Statement
We performed a retrospective study on anonymized audiometric data (pure-tone air conductance hearing loss, tinnitus frequency and loudness) from 136 adult tinnitus patients (56 female) with a mean age of 50.9 ± 15.5 a who came to the ENT hospital in Erlangen for medical examination between 2000 and 2018. By signing the treatment contract, all patients gave their consent that their data can be used for scientific purposes. Therefore, no further declaration of consent was necessary. Patients were specifically selected for their complain about tinnitus as the main reason for coming to the clinic. Data of auditory and non-auditory comorbidities were extracted from the patient files. None of these patients had any acute surgeries affecting the auditory system, even though 5/136 patients had such surgeries earlier in their life (e.g. tympanoplasty surgeries). Hearing aids were used by 5/136 patients (1 monaural, 4 binaural). HL of 20 dB or more was diagnosed prior to their visit in the clinics in 36/136 patients; no other acute auditory disease was reported. Nevertheless in 7/136 cases a common cold was mentioned, that could change hearing ability to a certain degree; 46/136 patients mentioned earlier episodes of vertigo. None suffered from hyperacusis as assessed by the German version of the hyperacusis questionnaire [33].
Only acute (e.g. Asthma bronchiale / Allergies, N=6) and chronic (e.g. Diabetes mellitus N=8 or Hypothyreosis N=23) non-auditory comorbidities of the patients were taken into account in this study and separated into seven categories according to the ICD-10-GM codes; the exact patient numbers for each category is given in Table 1. Category 1: Endocrine system / metabolic diseases. This included, e.g. diabetes mellitus or hypothyroidism. Category 2: psychiatric / behavioral disorders. This included, e.g. clinical depression or anxiety. Category 3: diseases of the central nervous system. This included, e.g., strokes or space-occupying tumors of the brain. Category 4: Diseases of the circulatory system. This included, e.g., patients that suffered from earlier cardiac arrests or arteriosclerosis. Category 5: Diseases of the respiratory system: This included, e.g., chronic obstructive pulmonary disease or chronic asthma. Category 6: Diseases of the digestive system. This included, e.g., inflammatory bowel disease or ulcerative colitis. Category 7: muscle-skeletal diseases. This included, e.g., disc-related spinal disorders, arthritis or osteoporosis. Patients could suffer from more than one non-auditory comorbidity (169 comorbidities in 136 tinnitus patients), for these numbers please refer to Table 2.
2.2. Data Evaluation and Statistics
For the statistical data analysis, Statistica 14 (TIBCO software, Palo Alto, CA, USA) was used. The patients were categorized according to their age at the performed measurements into young: 18 to 39 a, middle aged: 40 to 59 a and senior: 60+ a. The tinnitus related data as well as the number of comorbidities were analyzed by non-parametric statistics. Only the audiogram data of the patients’ tinnitus-affected ears were used for further analyses. All HL related data was analyzed using two-factorial ANOVAs with Tukey post-hoc tests. The distance of the tested audiometric frequency to the tinnitus frequency (TF) was calculated by log2(frequency (Hz)/TF (Hz)) rounded to the nearest integer. This was used to align the measured HL to the determined TF. Note that for the analyses only TF distances ranging from -4 to +2 octaves relative to the TF were used, as TF distances beyond this range were rare in the patient collective.
3. Results
3.1. Patient Collective
The 136 adult tinnitus patients (56 ♀, 80 ♂) included in this study had a mean age of 50.9 ± 15.5 a. Female (51.3 ± 15.5 a) and male patients (50.6 ± 15.5 a) did not differ significantly in their mean age (Student’s t-test, p=0.79). The adult patient collective was divided into three age categories of young (<39 a; n=18; mean age (± standard deviation): 23.9 ± 3.6 a), middle aged (40 – 59 a; n=85; 48.8 ± 7.6 a) and senior (60+ a; n=33; 70.6 ± 7,6 a) patients to account for age related hearing changes and comorbidity burden. The patients reported either monaural (young: n=13; middle aged: n=38; senior: n=19) or binaural (young: n=5; middle aged: n=46; senior: n=13) pure tone (young: n=12; middle aged: n=56; senior: n=21) or narrowband noise tinnitus (young: n=6; middle aged: n=28; senior: n=11). Usually, only one kind of tinnitus percept with a determinable center frequency was reported, even though in the case of a binaural percept the frequency could differ; only two patients (one middle aged and one senior) reported pure tone in one ear and narrowband noise in the other. Only the audiograms of the patients’ tinnitus-affected ears were used for the analyses described below, so different center frequencies of both ears did not affect the evaluation. The patients’ TF in the three age groups was not significantly different from each other (median frequency (interquartile range)): young: 4000 Hz (750 Hz, 8000 Hz); middle aged: 4000 Hz (2000 Hz, 6000 Hz); senior: 4000 Hz (1000 Hz, 6000 Hz); Kruskal-Wallis ANOVA: H(2, 202)=2.30, p=0.32. The same was true for the tinnitus loudness, given in dB sensation level (dB SL) (young: 7 dB SL (0 dB SL, 10 dB SL); middle aged: 7.5 dB SL (-3 dB SL, 15 dB SL); senior: 10 dB HL (2 dB SL, 19 dB SL); Kruskal-Wallis ANOVA: H (2, 196)=2.97, p=0.23). Nevertheless, patients in the three age categories showed a significant different number (Χ² (20,136)=13.58, p=0.035) of non-auditory comorbidities (cf. Methods), these are summarized in Table 2. Trivially, with increasing age the number of non-auditory comorbidities rises significantly (Kruskal-Wallis ANOVA, H(3, 136)=14.93, p<0.001) and Multiple Comparison of means post-hoc tests show that young patients show significantly less non-auditory comorbidities than middle aged (p=0.015) or senior patients (p<0.001), while those two last groups did not show significant differences in comorbidity numbers (p=0.25). When analyzing the tinnitus frequency with these non-auditory comorbidity categories in the three age groups independently, we also did not see any significant differences between the median frequency of patients with different numbers of comorbidities (young: Mann-Whitney U-test, p=0.21; middle aged: Kruskal-Wallis ANOVA, H (3, 132)=6.12, p=0.11; senior: Kruskal-Wallis ANOVA, H (3, 47)=0.94, p=0.82). This is also true for the tinnitus loudness (young: Mann-Whitney U-test, p=0.48; middle aged: Kruskal-Wallis ANOVA, H (3, 128) = 3.70, p=0.30; senior: Kruskal-Wallis ANOVA, H (3, 46)=3.54, p=0.32). In other words, neither tinnitus frequency nor tinnitus loudness did show any dependency on the patient’s age.
Those 45 (33 %) tinnitus patients without any non-auditory comorbidities were seen as “standard tinnitus patients” to which the other comorbidity groups could be compared. In the young patients group, only data of patients with one non-auditory comorbidity could be compared to them. In the two other age groups, we could compare the data of patients with one to five non-auditory comorbidities to these “standard tinnitus patients”.
3.2. Correlation of the Audiometric Data of Tinnitus Patients with and without the Presence of Non-Auditory Comorbidities
In first analyses, the pure tone air-conductance audiometric HL of the patients of the three age groups was assessed independently by two-factorial ANOVAs with the factors frequency and number of non-auditory comorbidities. As mentioned above, for the young patients group, only the comparison between zero and one comorbidity was possible. The results are summarized in Figure 1. In all patient groups we found a significant effect of the HL on frequency (not shown in Figure; young: F (10, 374)=1.92, p=0.041; middle aged: F (10, 1826)=59.49, p<0.001; senior: F (10, 672)=35.90, p<0.001). We also found a dependency of the HL on the number of non-auditory comorbidities. In the young tinnitus patients, the mean HL was significant weaker with one of these comorbidities (Figure 1A, inset; F (1, 374)=10.61, p=0.001), while the middle aged tinnitus patients did show a significantly increased HL with one non-auditory comorbidity (Figure 1B, inset; F (3, 1826)=5.05, p=0.002). Senior tinnitus patients showed a significant increased HL only with three or more non-auditory comorbidities (Figure 1C, inset; F (3, 672)=2.87, p=0.036). No interaction of the two factors could be found in the three age groups (Figure 1 A to C; young: F (10, 374)=0.22, p=0.99; middle aged: F (10, 1826)=0.69, p=0.90; senior: F (10, 672)=0.39, p=0.99). In other words, dependent on the tinnitus patients’ age and number of non-auditory comorbidities, the hearing thresholds can be significantly different, even if no further auditory comorbidities are present. Note, that only in the senior tinnitus patients we find a steadily increasing mean HL with increasing number of comorbidities while in the middle aged patients this dependency is non-linear and in young patients even inverted.
It is well known that the maximum of the HL and the TF correlate with each other. Usually the TF is found to be at the frequency of the maximum HL but comorbidities and / or age might have an influence on this correlation. Therefore, we analyzed the HL dependent on the distance of the tested frequency to the determined tinnitus frequency (TF) given in octaves and the number of non-auditory comorbidities with independent ANOVAs for each age group. For better comparison, we used only the distance range of -4 to +2 oct relative to the TF, which includes 81.5% (1812/2222 data points) of the complete HL data provided above. The reasoning behind these analyses was to investigate if the HL – as mentioned above – is dependent on the distance to the TF and if this dependency is further dependent on the number of non-auditory comorbidities. We found, first, in young tinnitus patients the expected dependency of the HL on the distance to TF (Figure 1D, inset; F (6, 179)=3.46, p=0.003) with the maximum HL at +1 oct relative to the TF (Tukey post-hoc tests, p<0.05). No difference between HL without any non-auditory comorbidities and one comorbidity was found (not shown in Figure; F (1, 179)=0.002, p=0.97) and no significant interaction was found (Figure 1D; F (6, 179)=1.74, p=0.11). Second, in the middle aged tinnitus patients again the expected dependency of HL and distance to TF was found (Figure 1E, inset; F (6, 1174)=29.24, p<0.001) with the maximum HL at the TF (Tukey post-hoc tests, p<0.001). No difference in mean HL between the number of non-auditory comorbidities was found (not shown in Figure; F (3, 1174)=0.38, p=0.77) but we found a significant interaction of both factors (Figure 1E; F (18, 1174)=2.42, p<0.001). Tukey post-hoc tests indicated that especially the HL of the tinnitus patients without any non-auditory comorbidities showed a different peak-TF location compared to the other comorbidity groups (p<0.05). Finally, in the senior age group we found a sigmoidal shaped dependency of the HL on the distance to the TF (Figure 1F, inset; F (6, 385)=15.10, p<0.001) with a maximum at the maximum of the investigated range of +2 oct relative to TF (Tukey post-hoc tests, p<0.001). We also found a significant dependency on the number of non-auditory comorbidities (not shown in Figure; F (3, 385)=7.63, p<0.001) with the “3+” category having significantly higher HL values compared to two of the other three categories (Tukey post-hoc tests, “0 vs. 3+” and “2 vs. 3+”, p<0.05; “1 vs. 3+”, p=0.075). The interaction of both factors did show a significant value as well (Figure 1F; F (18, 385)=3.48, p<0.001). Here the peak of the HL was at the TF for one and two non-auditory comorbidities, while for the two extreme cases (“0” and “3+”) the maximum HL was found at +2 oct relative to the TF (Tukey post-hoc tests, p<0.001). In other words, the statement that the maximum HL can be found at or around the TF is only partially true and dependent on the factor age and more importantly also on the number of non-auditory comorbidities. Again, no “simple” linear correlation of the data with the number of non-auditory comorbidities could be identified.
With this knowledge, we aimed to identify the possible non-auditory comorbidity (or comorbidities) that affected the HL in the different tinnitus patient age groups most. The non-auditory comorbidities were separated into seven categories (cf. Methods). The patients’ mean HL of the different age groups was then analyzed by independent two-factorial ANOVAs with the factors frequency and non-auditory comorbidity presence (i.e., with or without the specific comorbidity). The results of all analyses are given in Table 3. Note that analyses were not possible in all age groups dependent on the specific non-auditory comorbidity; we refrained from using the data of the young patients completely (cf. Table 1). From the analyses it became obvious that frequency dependent HL was mostly independent from the non-auditory comorbidity in middle aged and senior tinnitus patients, as in all cases the “standard” HL-pattern of low HL in lower frequencies and higher HL in higher frequencies was either significant or showed a tendency (column frequency in Table 3). The analyses of the factor comorbidity presence resulted in a more differentiated picture. In the case of diseases of the endocrine system / metabolism, patients of these two age groups with enough data for analysis showed significantly higher HL without that non-auditory comorbidity compared to patients with that specific comorbidity. In the remaining six categories of non-auditory comorbidities middle aged tinnitus patients showed higher HL with the specific comorbidity in two categories (digestive and muscle-skeletal system), senior patients showed this only with circulatory system comorbidities. Finally. We found interactions of both factors (i.e., frequency and presence of a comorbidity) only in one case, namely in middle aged tinnitus patients with or without muscle-skeletal system comorbidities. In other words, in all other cases with significant differences in mean HL dependent on the non-auditory comorbidity the whole audiogram was shifted in a parallel manner, which was not the case in this specific group.
4. Discussion
With this study we aimed to investigate if tinnitus patients with or without additional non-auditory comorbidities show differences in hearing loss. In summary, we found significant differences in the hearing thresholds of tinnitus patients – dependent on their age – suffering from diseases of different kinds of comorbidity categories. Not all patients with non-auditory comorbidities with significant effects on HL showed a decrease in their hearing ability, which may further increase the variance of studies on the hearing of patients with and without tinnitus.
Generally speaking the investigation of comorbidities in tinnitus patients is not new as the heterogeneity of the symptom / disease is a well-known problem [26,27]. Several studies tried to explain the variance in tinnitus patients’ data with auditory or non-auditory diseases [34,35,36]. Some of them focused on psychiatric comorbidities only [e.g., 37,38,39] but other studies combined them with several other factors [e.g., 35,40]. In further approaches, the comorbidities were used, e.g., to assess the risk factors of developing bothersome tinnitus [41] or to compare it with other diseases like chronic pain [42,43,44].
We tried to select an as homogeneous tinnitus patient collective as possible with respect to the occurrence of auditory comorbidities (cf. Methods) to reduce any HL effects of these diseases. Nevertheless, we cannot rule out that some patients might have undetected or unreported auditory or non-auditory comorbidities, as we performed an analysis on the data the patient files provided. The analysis of the tinnitus related parameters like frequency and loudness did not show any difference between the patients of the three age groups. These parameters were also not affected by the number of non-auditory comorbidities, while the number of comorbidities did trivially depend on the patients’ age. Nevertheless, we did find a significant TF-distance dependency of the peak of the HL relative to age and number of non-auditory comorbidities. This could explain differences found in different tinnitus patient groups in other studies, where the TF did or did not match the maximum HL [45,46,47,48]. Furthermore, the also trivially age dependent mean HL across all frequencies did also show further dependencies on the number of non-auditory comorbidities. In a vicious circle, the increased number of such comorbidities might increase the individual stress which in turn might increase the vulnerability for further comorbidities and vice versa. This combinatory effect of age, possible stress and vulnerability and number of comorbidities might explain differences of reported effects on HL in tinnitus patients [e.g., 49,50] and therefore might add to the explanation of at least a part of the overall heterogeneity in the data reported in the literature.
The attempt of the investigation of the single non-auditory comorbidity category effects on the HL (Table 3) has to be seen as a first analysis step. A more fine-grained investigation of single diseases in a larger patient collective and a comparison with non-tinnitus patients with the same non-auditory diseases might give much more insight in possible mechanisms on the effects of HL severity. Nevertheless, our approach on explaining a part of the variance of audiometric data in tinnitus patients revealed some candidate non-auditory comorbidity categories where such investigations might be fruitful. In our analyses especially the diseases of the endocrine or metabolic system had a strong – to our surprise positive – effect on the severity of the HL. This could indicate that there is a causal relationship here, rather than a simple aging effect. One possible explanation of this effect could be the patients receiving of medication (e.g. hormone substitutes) which in turn reduce stress [51] and therefore changes HL and / or the tinnitus percept. Negative effects on the hearing ability could be observed in the circulatory disease category in the elderly and muscle-skeletal system disease category as well as the digestive system disease category in the middle aged tinnitus patients. As the categories of the non-auditory comorbidities cover a wide range of individual diseases with different kind of expression strengths within each disease we refrain from providing any mechanistic or pathological explanation – but compare, e.g., [30,32] – although this rather is a phenomenological description.
As mentioned above, to understand the effects of the different pathologies on the hearing thresholds of tinnitus and non-tinnitus patients much more focused prospective studies have to be performed. This study can only guide the focus on the problem of the data variance in tinnitus patient research and might lead to the effect that more attention is given to non-auditory comorbidities in further tinnitus patient studies. One candidate non-auditory comorbidity category includes diseases of the endocrine or metabolic system, which provides surprising results and should be investigated more thoroughly.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, K.T. and H.S.; methodology, B.N. and A.Se.; formal analysis, K.T.; data curation, A..Se.; writing, K.T., P.K., A.Sc., P.B., B.M. and H.S.; project administration, H.S.; funding acquisition, K.T., A.Sc. and P.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by German Research Foundation (DFG), TZ 100/2-1 to KT and KR 5148/3-1 to PK project number 510395418; grant SCHI 1482/3-1 project number 451810794 to AS; grant KR 5148/2-1 project number 436456810 to PK.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Patient consent was waived due to the signature on the treatment contract with the University hospital Erlangen. With that, all patients gave their consent that their data can be used for scientific purposes. No further declaration of consent was necessary.
Data Availability Statement
All data can be obtained by request to the authors.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Biswas, R.; Lugo, A.; Akeroyd, M.A.; Schlee, W.; Gallus, S.; Hall, D.A. Tinnitus prevalence in Europe: a multi-country cross-sectional population study. The Lancet Regional Health - Europe 2022, 12, 100250. [CrossRef]
- Eggermont, J.J. Central tinnitus. Auris Nasus Larynx 2003, 30 Suppl, S7-12. [CrossRef]
- Schaette, R.; McAlpine, D. Tinnitus with a normal audiogram: physiological evidence for hidden hearing loss and computational model. J Neurosci 2011, 31, 13452-13457. [CrossRef]
- Savastano, M. Tinnitus with or without hearing loss: are its characteristics different? Eur Arch Otorhinolaryngol 2008, 265, 1295-1300. [CrossRef]
- Hebert, S.; Canlon, B.; Hasson, D. Emotional exhaustion as a predictor of tinnitus. Psychother Psychosom 2012, 81, 324-326. [CrossRef]
- Hebert, S.; Canlon, B.; Hasson, D.; Magnusson Hanson, L.L.; Westerlund, H.; Theorell, T. Tinnitus severity is reduced with reduction of depressive mood–a prospective population study in Sweden. PloS one 2012, 7, e37733. [CrossRef]
- Tziridis, K.; Friedrich, J.; Brueggemann, P.; Mazurek, B.; Schulze, H. Estimation of Tinnitus-Related Socioeconomic Costs in Germany. Int J Environ Res Public Health 2022, 19. [CrossRef]
- Eggermont, J.J.; Roberts, L.E. The neuroscience of tinnitus. Trends Neurosci 2004, 27, 676-682. [CrossRef]
- Gerken, G.M. Central tinnitus and lateral inhibition: an auditory brainstem model. Hear Res 1996, 97, 75-83. [CrossRef]
- Rüttiger, L.; Singer, W.; Panford-Walsh, R.; Matsumoto, M.; Lee, S.C.; Zuccotti, A.; Zimmermann, U.; Jaumann, M.; Rohbock, K.; Xiong, H. The reduced cochlear output and the failure to adapt the central auditory response causes tinnitus in noise exposed rats. PloS one 2013, 8, e57247. [CrossRef]
- Krauss, P.; Tziridis, K.; Metzner, C.; Schilling, A.; Hoppe, U.; Schulze, H. Stochastic resonance controlled upregulation of internal noise after hearing loss as a putative cause of tinnitus-related neuronal hyperactivity. Frontiers in neuroscience 2016, 10, 597. [CrossRef]
- Hickox, A.E.; Liberman, M.C. Is noise-induced cochlear neuropathy key to the generation of hyperacusis or tinnitus? J Neurophysiol 2014, 111, 552-564. [CrossRef]
- Tziridis, K.; Forster, J.; Buchheidt-Dorfler, I.; Krauss, P.; Schilling, A.; Wendler, O.; Sterna, E.; Schulze, H. Tinnitus development is associated with synaptopathy of inner hair cells in Mongolian gerbils. Eur J Neurosci 2021, 54, 4768-4780. [CrossRef]
- Mazurek, B.; Haupt, H.; Olze, H.; Szczepek, A.J. Stress and tinnitus—from bedside to bench and back. Frontiers in systems neuroscience 2012, 6, 47. [CrossRef]
- Schilling, A.; Sedley, W.; Gerum, R.; Metzner, C.; Tziridis, K.; Maier, A.; Schulze, H.; Zeng, F.-G.; Friston, K.J.; Krauss, P. Predictive coding and stochastic resonance as fundamental principles of auditory phantom perception. Brain 2023, 146, 4809-4825. [CrossRef]
- Knipper, M.; Ruettiger, L.; Schick, B.; Dlugaiczyk, J. Glycine receptor agonists for the treatment of phantom phenomena. 2011, US20110077239A1.
- Engineer, N.D.; Riley, J.R.; Seale, J.D.; Vrana, W.A.; Shetake, J.A.; Sudanagunta, S.P.; Borland, M.S.; Kilgard, M.P. Reversing pathological neural activity using targeted plasticity. Nature 2011, 470, 101-104. [CrossRef]
- Tziridis, K.; Brunner, S.; Schilling, A.; Krauss, P.; Schulze, H. Spectrally Matched Near-Threshold Noise for Subjective Tinnitus Loudness Attenuation Based on Stochastic Resonance. Front Neurosci 2022, 16, 831581. [CrossRef]
- Knipper, M.; van Dijk, P.; Schulze, H.; Mazurek, B.; Krauss, P.; Scheper, V.; Warnecke, A.; Schlee, W.; Schwabe, K.; Singer, W.; et al. The Neural Bases of Tinnitus: Lessons from Deafness and Cochlear Implants. J Neurosci 2020, 40, 7190-7202. [CrossRef]
- Távora-Vieira, D.; Marino, R.; Krishnaswamy, J.; Kuthbutheen, J.; Rajan, G.P. Cochlear implantation for unilateral deafness with and without tinnitus: a case series. The Laryngoscope 2013, 123, 1251-1255. [CrossRef]
- Tass, P.A.; Adamchic, I.; Freund, H.-J.; von Stackelberg, T.; Hauptmann, C. Counteracting tinnitus by acoustic coordinated reset neuromodulation. Restorative neurology and neuroscience 2012, 30, 137-159. [CrossRef]
- Mazurek, B.; Hesse, G.; Sattel, H.; Kratzsch, V.; Lahmann, C.; Dobel, C. S3 Guideline: Chronic Tinnitus: German Society for Otorhinolaryngology, Head and Neck Surgery e. V.(DGHNO-KHC). Hno 2022, 70, 795-827. [CrossRef]
- Shekhawat, G.S.; Searchfield, G.D.; Stinear, C.M. Role of hearing aids in tinnitus intervention: a scoping review. Journal of the American Academy of Audiology 2013, 24, 747-762. [CrossRef]
- Baguley, D.; McFerran, D.; Hall, D. Tinnitus. The Lancet 2013, 382, 1600-1607. [CrossRef]
- Bauer, C.A. Tinnitus. New England Journal of Medicine 2018, 378, 1224-1231. [CrossRef]
- Beukes, E.W.; Manchaiah, V.; Allen, P.M.; Andersson, G.; Baguley, D.M. Chapter 4 - Exploring tinnitus heterogeneity. In Progress in Brain Research, Schlee, W., Langguth, B., Kleinjung, T., Vanneste, S., De Ridder, D., Eds.; Elsevier: 2021; Volume 260, pp. 79-99. [CrossRef]
- Mazurek, B.; Rose, M.; Schulze, H.; Dobel, C. Systems Medicine Approach for Tinnitus with Comorbid Disorders. Nutrients 2022, 14, 4320. [CrossRef]
- Cederroth, C.R.; Gallus, S.; Hall, D.A.; Kleinjung, T.; Langguth, B.; Maruotti, A.; Meyer, M.; Norena, A.; Probst, T.; Pryss, R. Towards an understanding of tinnitus heterogeneity. Frontiers in aging neuroscience 2019, 11, 53. [CrossRef]
- Besser, J.; Stropahl, M.; Urry, E.; Launer, S. Comorbidities of hearing loss and the implications of multimorbidity for audiological care. Hearing research 2018, 369, 3-14. [CrossRef]
- Wattamwar, K.; Qian, Z.J.; Otter, J.; Leskowitz, M.J.; Caruana, F.F.; Siedlecki, B.; Spitzer, J.B.; Lalwani, A.K. Association of cardiovascular comorbidities with hearing loss in the older old. JAMA Otolaryngology–Head & Neck Surgery 2018, 144, 623-629. [CrossRef]
- Stam, M.; Kostense, P.J.; Lemke, U.; Merkus, P.; Smit, J.H.; Festen, J.M.; Kramer, S.E. Comorbidity in adults with hearing difficulties: which chronic medical conditions are related to hearing impairment? International journal of audiology 2014, 53, 392-401. [CrossRef]
- Gibrin, P.C.D.; Melo, J.J.; Marchiori, L. Prevalence of tinnitus complaints and probable association with hearing loss, diabetes mellitus and hypertension in elderly. In Proceedings of the CoDAS, 2013; pp. 176-180. [CrossRef]
- Fackrell, K.; Fearnley, C.; Hoare, D.J.; Sereda, M. Hyperacusis Questionnaire as a Tool for Measuring Hypersensitivity to Sound in a Tinnitus Research Population. Biomed Res Int 2015, 2015, 290425. [CrossRef]
- Rhee, J.; Lee, D.; Suh, M.W.; Lee, J.H.; Hong, Y.-C.; Oh, S.H.; Park, M.K. Prevalence, associated factors, and comorbidities of tinnitus in adolescents. PLOS ONE 2020, 15, e0236723. [CrossRef]
- Basso, L.; Boecking, B.; Brueggemann, P.; Pedersen, N.L.; Canlon, B.; Cederroth, C.R.; Mazurek, B. Subjective hearing ability, physical and mental comorbidities in individuals with bothersome tinnitus in a Swedish population sample. Progress in Brain Research 2021, 260, 51-78. [CrossRef]
- Bhatt, I.S.; Washnik, N.J.; Kingsbury, S.; Deshpande, A.K.; Kingsbury, H.; Bhagavan, S.G.; Michel, K.; Dias, R.; Torkamani, A. Identifying Health-Related Conditions Associated with Tinnitus in Young Adults. Audiology Research 2023, 13, 546-562. [CrossRef]
- Belli, S.; Belli, H.; Bahcebasi, T.; Ozcetin, A.; Alpay, E.; Ertem, U. Assessment of psychopathological aspects and psychiatric comorbidities in patients affected by tinnitus. European Archives of Oto-Rhino-Laryngology 2008, 265, 279-285. [CrossRef]
- Hébert, S. Psychological comorbidities of tinnitus. The Behavioral Neuroscience of Tinnitus 2021, 349-359. [CrossRef]
- Malakouti, S.K.; Mahmoudian, M.N.S.; Alifattahi, N.; Salehi, M. Comorbidity of chronic tinnitus and mental disorders. The international tinnitus journal 2011, 16, 118-122.
- Pavaci, S.; Tortorella, F.; Fioretti, A.B.; Angelone, A.M.; Businco, L.D.R.; Lauriello, M.; Eibenstein, A. Analysis of the audiological characteristics and comorbidity in patients with chronic tinnitus. Audiology Research 2019, 9, 231. [CrossRef]
- Basso, L.; Boecking, B.; Brueggemann, P.; Pedersen, N.L.; Canlon, B.; Cederroth, C.R.; Mazurek, B. Gender-specific risk factors and comorbidities of bothersome tinnitus. Frontiers in neuroscience 2020, 14, 706. [CrossRef]
- Zirke, N.; Seydel, C.; Szczepek, A.J.; Olze, H.; Haupt, H.; Mazurek, B. Psychological comorbidity in patients with chronic tinnitus: analysis and comparison with chronic pain, asthma or atopic dermatitis patients. Quality of Life Research 2013, 22, 263-272. [CrossRef]
- Boecking, B.; von Sass, J.; Sieveking, A.; Schaefer, C.; Brueggemann, P.; Rose, M.; Mazurek, B. Tinnitus-related distress and pain perceptions in patients with chronic tinnitus–Do psychological factors constitute a link? PLoS One 2020, 15, e0234807. [CrossRef]
- Biehl, R.; Boecking, B.; Brueggemann, P.; Grosse, R.; Mazurek, B. Personality Traits, Perceived Stress, and Tinnitus-Related Distress in Patients With Chronic Tinnitus: Support for a Vulnerability-Stress Model. Front Psychol 2019, 10, 3093. [CrossRef]
- Schilling, A.; Krauss, P.; Hannemann, R.; Schulze, H.; Tziridis, K. Reduktion der Tinnituslautstärke. HNO 2020, 69, 891-898. [CrossRef]
- Shetty, H.N.; Pottackal, J.M. Gain adjustment at tinnitus pitch to manage both tinnitus and speech perception in noise. Journal of Otology 2019, 14, 141-148. [CrossRef]
- McNeill, C.; Távora-Vieira, D.; Alnafjan, F.; Searchfield, G.D.; Welch, D. Tinnitus pitch, masking, and the effectiveness of hearing aids for tinnitus therapy. International journal of audiology 2012, 51, 914-919. [CrossRef]
- Vielsmeier, V.; Lehner, A.; Strutz, J.; Steffens, T.; Kreuzer, P.M.; Schecklmann, M.; Landgrebe, M.; Langguth, B.; Kleinjung, T. The Relevance of the High Frequency Audiometry in Tinnitus Patients with Normal Hearing in Conventional Pure-Tone Audiometry. [CrossRef]
- Martines, F.; Bentivegna, D.; Martines, E.; Sciacca, V.; Martinciglio, G. Assessing audiological, pathophysiological and psychological variables in tinnitus patients with or without hearing loss. European Archives of Oto-Rhino-Laryngology 2010, 267, 1685-1693. [CrossRef]
- Langguth, B.; Landgrebe, M.; Schlee, W.; Schecklmann, M.; Vielsmeier, V.; Steffens, T.; Staudinger, S.; Frick, H.; Frick, U. Different patterns of hearing loss among tinnitus patients: a latent class analysis of a large sample. Frontiers in neurology 2017, 8, 46. [CrossRef]
- Selye, H. Stress and disease. Science 1955, 122, 625-631. [CrossRef]
Figure 1.
Mean hearing loss dependent on number of non-auditory comorbidities. A Interaction plot of two-factorial ANOVA of the mean HL (dB) in young tinnitus patients (n=18) dependent on the factors frequency and number of non-auditory comorbidities (color-coded). The inset depicts the one-factorial part of HL analysis with the factor number of non-auditory comorbidities; statistics are given on the side. B, C Same plots as described above for middle aged (n=85) and senior tinnitus patients (n=33), respectively. Asterisks in insets depict the level of significant Tukey post-hoc tests, * p<0.05. D, E, F Interaction plots of two-factorial ANOVAs on mean HL (dB) in tinnitus patients of different age groups dependent on the factors distance to tinnitus frequency (TF) given in octaves and number of non-auditory comorbidities. The inset depicts the one-factorial part of HL analysis with the factor distance to TF; statistics are given on the side. For details of the analyses, see text.
Figure 1.
Mean hearing loss dependent on number of non-auditory comorbidities. A Interaction plot of two-factorial ANOVA of the mean HL (dB) in young tinnitus patients (n=18) dependent on the factors frequency and number of non-auditory comorbidities (color-coded). The inset depicts the one-factorial part of HL analysis with the factor number of non-auditory comorbidities; statistics are given on the side. B, C Same plots as described above for middle aged (n=85) and senior tinnitus patients (n=33), respectively. Asterisks in insets depict the level of significant Tukey post-hoc tests, * p<0.05. D, E, F Interaction plots of two-factorial ANOVAs on mean HL (dB) in tinnitus patients of different age groups dependent on the factors distance to tinnitus frequency (TF) given in octaves and number of non-auditory comorbidities. The inset depicts the one-factorial part of HL analysis with the factor distance to TF; statistics are given on the side. For details of the analyses, see text.
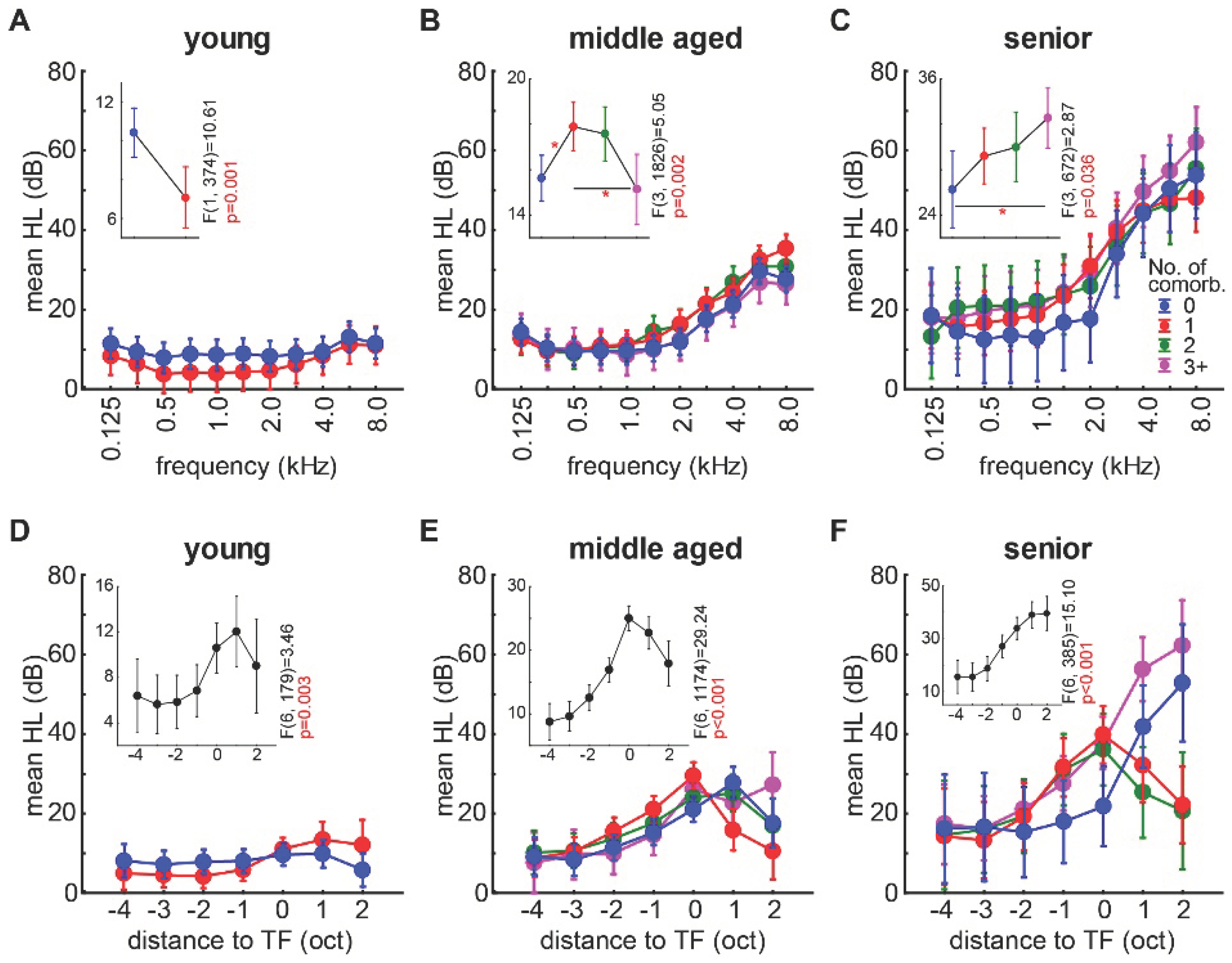

Table 1.
Overview of non-auditory comorbidity categories in patients separated by age group.
| Comorbidity Category | Young Patients | Middle Aged Patients | Senior Patients | Σ and % of all patients |
|---|---|---|---|---|
| endocrine system / metabolic diseases | 1/18 | 24/85 | 15/33 | 40/136 (29.4%) |
| psychiatric / behavioral disorders | 4/18 | 20/85 | 4/33 | 28/136 (20.6%) |
| diseases of the central nervous system | 0/18 | 6/85 | 3/33 | 9/136 (6.6%) |
| Diseases of the circulatory system | 0/18 | 22/85 | 19/33 | 41/136 (30.1%) |
| Diseases of the respiratory system | 0/18 | 5/85 | 5/33 | 10/136 (7.4%) |
| Diseases of the digestive system | 0/18 | 9/85 | 1/33 | 10/136 (7.4%) |
| muscle-skeletal diseases | 1/18 | 19/85 | 11/33 | 31/136 (22.8%) |
| Σ all comorbidity classes | 6 | 105 | 58 | 169 comorbidities in 136 patients |
Table 2.
Number of non-auditory comorbidities in patients separated by age group.
| Age Group | 0 Comorbidities | 1 Comorbidity | 2 Comorbidities | 3+ Comorbidities |
|---|---|---|---|---|
| young | 11 | 7 | 0 | 0 |
| middle | 28 | 25 | 20 | 12 |
| senior | 6 | 11 | 7 | 9 |
Table 3.
Results of two-factorial ANOVAs of HL dependent on frequency and non-auditory comorbidity presence.
Table 3.
Results of two-factorial ANOVAs of HL dependent on frequency and non-auditory comorbidity presence.
| category | age group | frequency | comorbidity presence | interaction |
|---|---|---|---|---|
| endocrine system / metabolism | middle | F(10, 1144)=7.64, p<0.001 | F(1, 1144)=7.69, p=0.006with (24): 12.97 dBwithout (61): 17.00 dB | F(10, 1144)=0.73, p=0.70 |
| senior | F(10, 694)=9.64, p<0.001 | F(1, 694)=4.55, p=0.034with (15): 20.73 dBwithout (18): 27.51 dB | F(10, 694)=0.14, p=0.99 | |
| psychiatric / behavioral | middle | F(10, 1144)=16.06, p<0.001 | F(1, 1144)=1.11, p=0.29with (20): 15.44 dBwithout (65): 16.74 dB | F(10, 1144)=0.40, p=0.95 |
| senior | F(10, 694)=3.75, p<0.001 | F(1, 694)=0.02, p=0.88with (4): 27.05 dBwithout (29): 26.26 dB | F(10, 694)=0.07, p=0.99 | |
| central nervous system | middle | F(10, 1144)=9.19, p<0.001 | F(1, 1144)=0.87, p=0.35with (6): 18.17 dBwithout (79): 16.61 dB | F(10, 1144)=0.06, p=0.99 |
| senior | F(10, 694)=12.53, p<0.001 | F(1, 694)=1.96, p=0.16with (3): 26.65 dBwithout (30): 30.11 dB | F(10, 694)=0.19, p=0.99 | |
| circulatory system | middle | F(10, 1144)=20.23, p<0.001 | F(1, 1144)=0.35, p=0.55with (22): 16.05 dBwithout (63): 16.78 dB | F(10, 1144)=0,41, p=0.94 |
| senior | F(10, 694)=12.65, p<0.001 | F(1, 694)=20.09, p<0.001with (19): 33.42 dBwithout (14): 22.39 dB | F(10, 694)=1.32, p=0.22 | |
| respiratory system | middle | F(10, 1144)=1.76, p=0.06 | F(1, 1144)=0.55, p=0.46with (5): 14.64 dBwithout (80): 16.74 dB | F(10, 1144)=0.39, p=0.95 |
| senior | F(10, 694)=17.19, p<0.001 | F(1, 694)=3.59, p=0.06with (5): 26.60 dBwithout (28): 30.37 dB | F(10, 694)=0.33, p=0.97 | |
| digestive system | middle | F(10, 1144)=3.81, p<0.001 | F(1, 1144)=3.95, p=0.047with (9): 22.23 dBwithout (76): 16.59 dB | F(10, 1144)=0.14, p=0.99 |
| muscle-skeletal system | middle | F(10, 1144)=25.37, p<0.001 | F(1,1144)=66.60,p<0.001with (19): 26.12 dBwithout (66): 15.72 dB | F(10, 1144)=2.29, p=0.01 |
| senior | F(10, 694)=3.26, p<0.001 | F(1, 694)=1.06, p=0.30with (11): 31.32 dBwithout (22): 25.99 dB | F(10, 694)=0.17, p=0.99 |
Note: the numbers in brackets behind with/without give the patients numbers included.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



