
Submitted:
29 February 2024
Posted:
01 March 2024
You are already at the latest version
Abstract
The aim of this study is to evaluate the efficacy of taking a daily supplement based on active compounds (AUDISTIM® Day Night: A D/N) in alleviating tinnitus-related disability, as suggested by previous real-life studies. This double-blind randomized placebo-controlled study was conducted in adult with mild to severe tinnitus receiving a 3 month-supplementation. Tinnitus-related handicap (THI), psychological stress (MSP-9) and sleep quality (PSQI) were assessed at baseline and during intervention, perceived impression of tinnitus improvement at the end of the follow-up. The full set analysis included 114 patients (59 A D/N, 55 placebo) aged 53.8±11.4 years, 58% women, with fluctuating (45%) or permanent (55%) tinnitus from 9.3±9.4 years. A D/N supplementation led to greater changes in THI (-13.2±16.0 vs -6.2±14.4, p=0.0158, Cohen’s d=0.44) at 3 months, especially with continuous tinnitus (-15.0±16.3 vs -4.6±12.8, p=0.0065), and, to a lesser extent, at 1 month (-9.8±13.1 for A vs -4.3±12.1, p=0.0213). PSQI significantly improved over time in both groups, MSP-9 only with A D/N. In lines with previous observational studies, both clinical (THI score > 7 pts) and statistical (vs. placebo) improvement, more pronounced in permanent tinnitus, demonstrate the effectiveness of the combination of active compounds and support its use in the management of mild to severe tinnitus.
Keywords:
Tinnitus
; THI
; Tinnitus Handicap Inventory
; Permanent
; Fluctuating
; food supplement
; antioxidant
1. Introduction
Tinnitus has been defined in many ways, i.e., in the WHOS’s ICD11 [1] or in scientific literature [2,3,4], but not all of them capture its complex characteristics. To compensate for the lack of a complete, precise and consensual definition of tinnitus, and to distinguish between tinnitus without suffering and tinnitus with associated suffering, a group of international experts recently proposed the following definitions: “Tinnitus is the conscious awareness of a tonal or composite noise for which there is no identifiable corresponding external acoustic source, which becomes Tinnitus Disorder “when associated with emotional distress, cognitive dysfunction, and/or autonomic arousal, leading to behavioral changes and functional disability” [5]. Heterogeneity of forms, genetic and environmental etiological factors, associated condition or disease, and assessment for diagnosis make it challenging not only to specify accurate tinnitus prevalence over the general population, but also to provide effective standardized treatments. However, all types together, it has been estimated that around 740 million adults worldwide may be affected by tinnitus [6], and 65 million in European Union, meaning more than 1 in 7 adults in a gender-balanced way [7].
When extremely loud or bothersome, tinnitus is a major source of distress with well-established functional and psychological effects [8,9,10] and impaired quality of life [11,12]. Of adverse effect of tinnitus, sleep disturbance has been reported as the most common [13] but tinnitus could also affect daily activities or led to depression and anxiety [3,14].
A wide range of drugs or non-pharmacological alternatives are offered to patients presented with tinnitus [9,15,16,17]. Review of scientific data highlights that there is no effective treatment for all patients with tinnitus [15,17,18]. As an example, recent meta-analysis reported encouraging conclusions regarding the beneficial effects of drugs with brain acting effects or anti-inflammatory/antioxidant effect on certain primary tinnitus [16]. In a recent double-blind, randomized, placebo-controlled study, an antioxidant-based dietary supplement was shown to be effective in reducing the discomfort and intensity of tinnitus [19].
Consistent results were reported in two observational studies which assessed the effectiveness of AUDISTIM Day/Night, a food supplement marketed since 2015 [20,21]. This supplement combines several active ingredients and antioxidants that may exert beneficial effects on tinnitus and related disorders. Claims of the different components of the food supplement are provided in detail in our previous works [20,21]. Conducted in France and Belgium, the two studies included a total of 421 patients with persistent subjective tinnitus enrolled by Ear Nose Throat practitioners in community settings or hospital facilities. Both studies displayed converging results in terms regarding the effectiveness of the supplement on reducing tinnitus-related impairment on daily life, psychological stress, and sleep quality. In both studies, tinnitus impairment on daily life was assessed using the THI (Tinnitus Handicap Inventory) [22], the questionnaire being the most frequently used in practice [18].
However, as pointed out by authors of the above-mentioned systematic reviews and meta-analyses, well-conducted randomized controlled trials that consider the subjective character of tinnitus are essential to assess efficacy of the interventions. The present double-blind randomized controlled trial (RCT) aimed at confirming the efficacy of A D/N on tinnitus in patients with mild to severe persistent tinnitus. The study methodology, as outlined by Kikidis et al. [23], follows the latest recommendations for RCTs in tinnitus. Changes in THI score at 3 months was chosen as primary endpoint, objective measurement such changes in hearing loss having been reported as not the most relevant outcome of treatment response [23]. The THI questionnaire which is a validated in French version [24], is widely used tool for assessing efficacy in tinnitus, allowing for comparison with our work and others’.
2. Materials and Methods
Study design. This study was a double-blind, randomized, placebo-controlled with 1.1 ratio, parallel-arm, and monocentric. The study was set up at a clinical investigation center (CEN Experimental, Dijon, France) under principal investigator supervision. Having been duly informed about the study and in accordance with national provisions and the General Data Protection Regulation (GDPR), each patient has given written and informed consent to their participation in the study and to the processing of their personal data. After baseline data collection (M0), patients meeting all entry criteria were allocated to the A D/N and placebo groups. Patients took part in study assessments on three occasions, once at enrolment (visit M0) and twice during follow-up, i.e., after 1 (M1) and 3 months (M3) following the start of daily supplementation with their allocated intervention.
Participants. Patients aged 30 to 75 suffering from mild to severe tinnitus, as assessed by a THI (Tinnitus Handicap Inventory) score of 12 to 76 [22], for at least 6 months may be included if they did not meet the following main exclusion criteria: tinnitus treatment (pharmacological or alternative), deafness, hearing aid, hearing disease or ototoxic treatments, chronic metabolic or progressive disease, psychiatric disorder. Shift workers, pregnant or breastfeeding women were excluded.
Randomization and blinding. Eligible patients were assigned 1:1 to either A D/N or placebo. Randomization was generated using the block 4-randomization of the random function of the SAS software version 9.4 (SAS Enterprise Miner 13.1. SAS Institute Inc., Cary, NC.). All clinical investigation, data collection, assessments and data analyses were blinded to randomization allocation.
Interventions. At M0 visit, depending on their allocated group, patients received 3 boxes of A D/N or placebo tablets containing 30 “Day” tablets and 30 “Night” tablets in blister packs, corresponding to 3 months’ supplementation. Supplementation should start the next day after M0 visit. AUDISTIM® day/night consists of two “Day” and “Night” tablets to be taken daily in the morning and 30-60 minutes before bedtime, respectively. The Day tablet contained 515.6 mg of excipients including coating (maltodextrin, microcrystalline cellulose, sodium croscarmellose, magnesium stearate, silicon dioxide, hydroxypropylmethylcellulose, calcium sulfate, magnesium carbonate, hydroxypropylcellulose, stearic acid) and magnesium (124.5 mg), L-theanine (50.0 mg), Ginkgo biloba (40.0 mg), Crataegus laevigata (37.5 mg), quercetin (25.0 mg), and vitamins: nicotinamide (19.2 mg), cyanocobalamine (3.0 mg) (1.4 mg), pyridoxine (2.04 mg), thiamine (1.68 mg). The Night tablet contained 483.1 mg of excipients including coating (same as Day plus Spirulina used as a colorant), (Melissa officinalis L. (80.0 mg), magnesium (62.25 mg), Ginkgo biloba L. (40.0 mg), Eschscholtzia californica Cham. (40.0 mg), L-tryptophan (40.0 mg), zinc (31.95 mg), quercetin (25.0 mg), and melatonin (1.0 mg). Both tablets covered 100% of the French Recommended Daily Allowance [25] for vitamins and zinc, 50% for magnesium. Placebo day and night tablets were indistinguishable from A D/N tablets and contained 742 mg of their respective excipients. Compliance with supplementation was assessed at M1 and M3.
Outcomes. THI score changes from baseline at 3 months was chosen as meaningful primary endpoint. The Tinnitus Handicap Inventory [22] and its French version [24] is a 25-item self-report measure to determine perceived tinnitus handicap severity which is classified as very mild (score 0–16), mild (score 18–36), moderate (score 38–56), severe (score 58–76) and catastrophic (78–90). A change score of at least seven points has been considered to denote reliable clinically significant improvement on the THI [26]. Secondary efficacy criteria included changes from baseline at M1 and M3 of the subjective measures of psychological stress using MSP-9 (shorter nine-items version of the Psychological Stress Measurement) [27], with scores ranging from 9 to 72 (maximum stress), and sleep quality using the PSQI (Pittsburgh Sleep Quality Index) questionnaire [28] with scores ranging from 0 to 21 (poorer sleep quality). Patient were asked to subjectively assess their impression of tinnitus improvement using the PGII (Patient Global Impression of Improvement). Safety endpoints were assessed throughout the study.
Sample size. The sample size assumed a 10-point difference in the mean change at M3 in THI scores between A D/N and placebo. With a standard deviation of 15 [20,21], a reduction from baseline of 5 in the placebo arm and of 15 in the A D/N arm, at risk alpha=0.05, with a power of 90 and in a bilateral situation, the sample size reached 98 subjects (49 per arm), increased to 110 subjects in total to account for dropouts.
Statistical analysis. Statistics were conducted according to the Statistical Principles for Clinical Trials ICH-E9 guidance [29]. Quantitative variables were described by mean and standard deviation (SD) or median and 95% confidence interval (95CI). Qualitative variables were described by number and percentage. Full set analysis was used as main efficacy analysis. Analyses were also conducted in the subsets of patients with fluctuant or permanent tinnitus. THI, MSP-9, and PSQI changes from baseline were compared between groups using a two-way (Time x Treatment) ANOVA, and their scores at M0, M1 or M3 using Chi2 test. Where same group, M0, M1 and M3 scores were compared using paired t-test. Effect size was estimated for primary outcome and using Cohen’s d [30], and related classification: small (d = 0.2), medium (d = 0.5), and large (d ≥ 0.8). PGII was compared between groups and subsets using Fisher test. The alpha risk for the significance level was set at 5%.
3. Results
3.1. Patient Disposition
From April 2022 to May 2023, 136 patients were screened at the clinical trial site, of them, 120 were randomized. The Full analysis set (FAS) included 114 patients who all received interventions and had assessable primary endpoint (Figure 1). Patients were equally allocated to A D/N (n=59) or placebo (n=55) groups, thus respecting sample size assumptions.
3.2. Description of Patients and Tinnitus at Baseline
Baseline demographics and clinical characteristics of the patients did not differ between A D/N and placebo groups (Table 1). On overall, patients (58.0% women) had a mean (SD) age of 53.8 (11.4) years, 94.7% (n= 112) did not present clinical abnormalities and 68.4% (n= 78) no concomitant pathologies. As shown in Table 2, tinnitus characteristics did not differ between groups. Mean (SD) duration of tinnitus was 9.9 (10.5) years, and tinnitus were classified as permanent for 55.3% (n=63) of patients, fluctuating for 44.7% (n=51). In overall FAS, mean (SD) tinnitus-induced annoyance in daily life was rated 5.1 (1.7), corresponding to a moderate impact, and 67.5% (n=77) reported associated symptoms (data not shown). Mean (SD) THI score in FAS was 37.4 (16.9) of 100, and 34.2% (n=39) and 13.2% (n=15) had moderate to severe tinnitus-related handicap (data not shown).
3.3. Changes in Tinnitus-Related Handicap under Dietary Supplementation
Changes from baseline at 3 months are presented in Table 3. Variation in THI score was significantly higher in A D/N group vs placebo (-13.2±16.0 vs -6.2±14.4, p=0.0158, Cohen’s d=0.44). Greater improvement was observed in patients with permanent tinnitus (-15.0±16.3 vs -4.6±12.8, p=0.0065, Cohen’s d=0.71). As suggested by Figure 2, to a lesser extent, significant variations of THI score were also reported from M1 in all patients (-9.8±13.1 vs -4.3±12.1, p=0.0213, Cohen’s d=0.44) and patients with permanent tinnitus (-11.5±13.6 vs -2.7±10.5, p=0.0057, Cohen’s d=0.72). Similar but not significant trend was observed in patients with fluctuant tinnitus (-7.8±12.6 for vs -6.3±13.9, p=0.6818). Irrespective of the duration of intervention and type of permanent/fluctuating tinnitus, all variations in THI scores were above the minimum clinical significance of 7 points in the A D/N group, never in the placebo group. All tinnitus combined, the rate of patients with at least a 20% reduction in THI score at M3 was significantly higher in the A D/N group. Probably due to the limited sample size of this subset, a higher but non-significant rate was reported in the subset of patients with permanent tinnitus.
3.4. Psychological Stress, Sleep Quality and Subjective Assessment of Tinnitus improvement
3.4.1. Psychological Stress and Sleep Quality
Evolution of psychological stress and sleep quality assessed using MSP-9 and PSQI questionnaires, respectively, over the study is detailed in Table 4. All patients had comparable moderate levels of stress, as suggested by MSP-9 score values (Lemyre & Tessier, 2003). MSP-9 scores were significantly lower by -3.9 (10.7) points at M3 (p=0.008) compared to M0 in A D/N group but not in placebo. Similar trend was observed in patients under A D/N with permanent and fluctuating tinnitus. However, the modest variations from baseline at 3 months observed in A D/N group did not achieve clinical significance for psychological stress reduction. At baseline, mean FAS PSQI score was just above the threshold of 5 that separates good from bad sleepers, suggesting that the study population was did not have significant sleep disorders. At the end of the follow-up, PSQI scores were modestly but significantly lower in all patients, except placebo patients with permanent tinnitus.
3.4.2. Subjective Assessment
Subjective assessments of tinnitus improvement reported by the patients are presented in Figure 3. A non-significant trend in favor of the A D/N was observed in both subsets of patients with permanent tinnitus and with fluctuating tinnitus. However, when 65% (n=17) in A D/N group vs 55% (n=12) in placebo group of patients with fluctuating tinnitus reported improvement, 33% (n=10) in A D/N group vs 20% (n=6) in placebo group of patients with permanent tinnitus also reported improvement.
3.5. Safety
During intervention, 15% (n=9) patients in A D/N group and 18% (n=11) in placebo experienced adverse events with relationship to treatment classified as possible or probable by the investigator. In placebo group, 6 of the 12 adverse events were tinnitus worsening. In A D/N group, 4 of 11 adverse reactions were gastrointestinal troubles. Other, headache (n=2) or insomnia (n=2) were also reported by placebo patients.
4. Discussion
Over the past decade, tinnitus has become one of the most common causes of disability [31]. As mentioned in the introduction, despite the discomfort and distress, some patients remain without effective treatment. It is becoming increasingly clear that no treatment is not an acceptable solution for patients, and that all attempts to improve tinnitus and relieve related symptoms and suffering will benefit patients. AUDISTIM® Day/Night was developed with this in mind. Thanks to its combination of active compounds, this food supplement aims to offer a non-pharmacological treatment for subjective tinnitus of various etiologies.
One of the main findings of this RCT is that results confirmed the effectiveness of AUDISTIM® Day/Night on tinnitus-related impairment in daily life reported in the two real-world studies, in patients suffering from chronic subjective tinnitus [20,21]. Results also support the favorable effect of the food supplement on psychological stress and sleep quality already observed in the two observational studies, whether statistical significance was not always achieved for this both criteria. Other finding of interest of the current RCT is that response to the supplementation was majored in patients with permanent compared to fluctuating tinnitus.
In the French and Belgium observational studies, THI scores were significantly decreased by -17.9 points and -9.9 points, respectively, versus -13.2 points in patients of the present RCT consuming A D/N. Thus, all changes in THI scores under A D/N supplementation reached the clinical meaningful [26] whereas placebo did not. These differences in THI changes between studies may be explained by patient tinnitus heterogeneity. As an example, only the Belgium study included patients with extremely severe tinnitus based on THI scores indicating “catastrophic handicap” in which response to treatment is poorly expected. In the French study, mean (SD) baseline THI score was close to the one (44.6 (23.4)) of the present RCT (38.9 (16.2)) but changes in THI score was slightly higher. It cannot be ruled out that selection and/or evaluation bias, inherent in observational studies, may have led to an overestimation of the real effectiveness.
AUDISTIM® Day/Night is a combination of nutrients, phytochemicals, and plant extracts with recognized antioxidant properties or nutritional claims. Beneficial effects of antioxidant association were also shown by other in patients of similar profile than those of this RCT. In Petridou’s RCT, taking multivitamin and mineral tablets once a day and alpha-lipoic acid tablets twice a day for three months induced a non-clinical but significant 6.1-point reduction in THI scores [19]. However, there was no significant difference with placebo, probably due to a strong response in this arm. Another randomized controlled trial reported a 10.0-point reduction in THI score after 3 months’ consumption of 100 mg of the higher antioxidant-rich extract of Euterpe oleracea martius (Açaí) once a day [32]. Overall, these results provide clinical evidence for antioxidant molecules in tinnitus that should not be ignored. The dietary supplement studied contains Ginko biloba, the effectiveness of which on tinnitus is still uncertain, as concluded by the latest Cochrane review [33]. It should be noted that the poor quality of the 12 RCTs included in this systematic review meant that no further conclusions could be drawn. The same could be said of zinc’s controversial efficacy. The supplement also contains melatonin which promising beneficial effect on tinnitus has been reported [34], and antioxidant activity [35]. It is well established that melatonin helps people fall asleep and relieves sleep disorders as well as lemon balm (Melissa officinalis), thanks to its traditional use to relieve mild symptoms of mental stress and to promote sleep [36]. Based on PSQI scores, the patients in our study had only mild sleep disturbances. The modest variations in sleep quality alone cannot account for the variations in THI scores. We can therefore assume that sleep-inducing ingredients such as melatonin and extract of lemon balm leaves are not the active ingredients of A D/N that have played a major role in improving tinnitus severity. Studies carried out on patients with markedly poor sleep quality could help support this hypothesis. To date, the three studies carried out on the food supplement do not make it possible to determine whether the effect observed is due to certain compounds alone, or whether the effects have been potentiated.
While experts have stressed the need to separately evaluate responses to intervention in patients with chronic/persistent tinnitus, meaning lasting from at least 3 months [5], either continuously perceived or with intermittent occurrence, very few studies have focused on it [23]. This RCT differ from other as the efficacy of AUDISTIM® Day/Night supplementation was investigated in two subsets of the FAS, namely patients with permanent or fluctuating tinnitus. In the absence of a well-defined wording and to avoid confusion with transient ear noise, in the present study, tinnitus lasting all day or present almost all the time was classified as “permanent”, tinnitus over 5 minute-duration which occurs occasionally as “fluctuating”. The results of our study showed that the variation in THI scores from baseline at 3 months was greater in patients with permanent tinnitus, suggesting that supplementation is beneficial for patients with greater day-to-day tinnitus-related discomfort or suffering. Results also highlighted that the placebo effect was lower in patients with permanent tinnitus than in those with fluctuating tinnitus. Higher placebo-effect and lower effectiveness of the supplementation may explain why variations in THI scores did not differ between A D/N and placebo in this subset.
Similar figures were obtained when sleep quality was assessed in both subsets. In patients with permanent tinnitus, sleep quality improved significantly, but not in the placebo group. Interestingly, the PSQI was below the threshold that distinguishes “good sleepers” from “bad sleepers” at the end of the A D/N intervention [28]. By contrast, in patients with fluctuating tinnitus, sleep quality was significantly and comparably improved in patients taking the supplement or placebo. As well as sleep quality, which was more impaired in patients with fluctuating tinnitus, the psychosocial stress was also greater in these patients. In line with the results of the two observational studies, regardless the type of tinnitus, psychosocial stress was improved in patients receiving the supplementation but not the placebo. Significance was only reported on overall patients of the A D/N group, suggesting that the small size of the subsets failed to achieve statistical significance.
Patients’ subjective assessment of tinnitus improvement also showed a trend in favor of the A D/N over placebo. Among patients with permanent tinnitus, only a third perceived a positive change in tinnitus, while THI score increased by at least 20% in three-quarters of patients, and sleep quality for most of them. In contrast, the results from one assessment to the next were consistent in patients with fluctuating tinnitus. This observation is hardly surprising, and once again raises the difficulties of evaluating the efficacy of tinnitus intervention in this condition of highly subjective nature [9,17,23]. In this context, it is worth remembering that the Tinnitus Handicap Inventory, used in this RCT, remains validated tool with predefined clinical meaningful, and that clinically significant effect was achieved with A D/N supplementation in overall patients as well as patients with permanent or fluctuating tinnitus [26,37].
Finally, data from the present study also shown the safe profile of the supplement. In this study, few adverse events reported with doubtful relationship to the food supplement as it appeared not possible to clearly state that it was side effects.
This study has some limitations. The first is that the sample size proved too small to achieve statistical significance when variations from baseline in the secondary endpoints were compared between the A D/N and placebo groups. Sample size calculation assumptions were based on THI changes, chosen as primary endpoint, measured in the two observational studies. Even, the sample size usually not considers the secondary endpoints, such high placebo effect was not anticipated. This high placebo effect may also explain the moderate sample effect on primary endpoint. The second limitation is that confounded factors such as mood disorder or anxiety were not collected. Groups being comparable at enrollment, it is assumed that randomization and blinding have limit this risk of bias. Finally, annoyance using VAS as part of perceptual aspects of tinnitus was only collected at baseline as part of the evaluation of tinnitus severity, but any changes were not investigated during the intervention. Despite these limitations, we are reasonably confident with the conclusions of the study.
5. Conclusions
In lines with the two observational studies, significant clinical and statistical improvement over placebo demonstrate the effectiveness of AUDISTIM® Day/Night on tinnitus severity. The combination of active compounds is supposed to be more effective in permanent tinnitus. Beneficial trends on psychological stress and sleep quality deserve to be investigated in further studies. To conclude, results of the present study support the use of AUDISTIM® Day/Night in the management of mild to severe tinnitus.
Author Contributions
Conceptualization, D.P., B.F. and M-J.E-F.; methodology, F.H. and C.J.; validation, D.P., B.F. and M-J.E-F.; F.R.,; data curation, F.R.; writing—original draft preparation, C.J..; writing—review and editing, C.J.; D.P., B.F. and M-J.E-F, X.X.; project administration, F.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by by MEDIWEB-AUDISTIMPHARMA, France.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by a French national Ethics Committee (“Comité de Protection des Personnes (CPP) Sud-Ouest-Outre-Mer”, 13 December 2021 under the number 21.03103.000060) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available from CEN (contact@groupecen.com), upon reasonable request.
Acknowledgments
Investigation team of CEN Experimental for study implementation, patient enrolment and follow-up.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Author 1, A.B.; ICD11, 2019, Tinnitus. Available online: https://icd.who.int/ct11/icd11_mms/en/remease.
- McFadden, D., 1982. Tinnitus: Facts, Theories, and Treatments. National Academy of Sciences Press, Washington DC.
- Baguley, D.; McFerran, D.; Hall, D. Tinnitus. Lancet 2013, 382, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Langguth, B.; Kreuzer, P.M.; Kleinjung, T.; De Ridder, D. Tinnitus: causes and clinical management. Lancet Neurol. 2013, 12, 920–930. [Google Scholar] [CrossRef] [PubMed]
- De Ridder D, Schlee W, Vanneste S; et al. Tinnitus and tinnitus disorder: Theoretical and operational definitions (an international multidisciplinary proposal). Prog Brain Res. 2021, 260, 1–25. [Google Scholar] [CrossRef]
- Jarach CM, Lugo A, Scala M; et al. Global Prevalence and Incidence of Tinnitus: A Systematic Review and Meta-analysis. JAMA Neurol. 2022, 79, 888–900. [Google Scholar] [CrossRef] [PubMed]
- Biswas R, Lugo A, Akeroyd MA, Schlee W, Gallus S, Hall DA. Tinnitus prevalence in Europe: a multi-country cross-sectional population study. Lancet Reg Health Eur. 2022, 12, 100250. [CrossRef]
- Tunkel DE, Bauer CA, Sun GH; et al. Clinical practice guideline: tinnitus. Otolaryngol Head Neck Surg 2014, 151 (Suppl. S2), S1–S40. [Google Scholar] [CrossRef]
- Bauer, CA. Tinnitus. N Engl J Med. 2018, 378, 1224–1231. [Google Scholar] [CrossRef]
- Henry JA, Reavis KM, Griest SE; et al. Tinnitus: An Epidemiologic Perspective. Otolaryngol Clin North Am. 2020, 53, 481–499. [Google Scholar] [CrossRef]
- Méric C, Gartner M, Collet L, Chéry-Croze S. Psychopathological Profile of Tinnitus Sufferers: Evidence Concerning the Relationship between Tinnitus Features and Impact on Life. Audiology and Neurotology 1998, 3, 240–252. [CrossRef]
- Tinnitus Retraining Therapy Trial Research Group, Scherer RW, Formby C. Effect of Tinnitus Retraining Therapy vs Standard of Care on Tinnitus-Related Quality of Life: A Randomized Clinical Trial. JAMA Otolaryngol Head Neck Surg. 2019, 145, 597–608. [Google Scholar] [CrossRef]
- Meikle M, Taylor-Walsh E. Characteristics of tinnitus and related observations in over 1800 tinnitus clinic patients. J. Laryngol Otol Suppl 1984, 9, 17–21. [Google Scholar] [CrossRef]
- Reavis K.M., Henry J.A., Marshall L.M., Carlson K.F. Prevalence of self-reported depression symptoms and perceived anxiety among community-dwelling U.S. adults reporting tinnitus. Perspect. ASHA Spec. Interest Groups 2020, 5, 959–970. [CrossRef]
- Langguth B, Elgoyhen AB, Cederroth CR. Therapeutic Approaches to the Treatment of Tinnitus. Annu Rev Pharmacol Toxicol. 2019, 59, 291–313. [Google Scholar] [CrossRef]
- Chen JJ, Chen YW, Zeng BY; et al. Efficacy of pharmacologic treatment in tinnitus patients without specific or treatable origin: A network meta-analysis of randomised controlled trials. EClinicalMedicine. 2021, 39, 101080. [Google Scholar] [CrossRef] [PubMed]
- Langguth B, Kleinjung T, Schlee W, Vanneste S, De Ridder D. Tinnitus Guidelines and Their Evidence Base. J. Clin. Med 2023, 12, 3087. [CrossRef] [PubMed]
- Person OC, Junior FVA, Altoé J, Portes LM, Lopes PR, Puga ME dos S. O que revisões sistemáticas Cochrane dizem sobre terapêutica para zumbido? ABCS Health Sciences 2022, 47, e022301. [CrossRef]
- Petridou AI, Zagora ET, Petridis P; et al. The Effect of Antioxidant Supplementation in Patients with Tinnitus and Normal Hearing or Hearing Loss: A Randomized, Double-Blind, Placebo Controlled Trial. Nutrients. 2019, 11, 3037. [Google Scholar] [CrossRef]
- Frachet B, Portmann D, Allaert F. Observational Study to assess the effect of Audistim® on the quality of life of patients presenting with chronic tinnitus. Revue de laryngologie - otologie - rhinologie 2017, 138. [Google Scholar]
- Van Becelaere T, Zahti H, Polet T, Glorieux P, Portmann D, Rigaudier F, Herpin F, Decat M. Improving quality of life in subjective tinnitus patients with Audistim®. Rev Laryngol Otol Rhinol. 2019, 140, 1, 3–7.
- Newman CW, Sandridge SA, Jacobson GP. Psychometric adequacy of the Tinnitus Handicap Inventory (THI) for evaluating treatment outcome. J Am Acad Audiol. 1998, 9, 153–160. [Google Scholar] [PubMed]
- Kikidis D, Vassou E, Schlee W; et al. Methodological Aspects of Randomized Controlled Trials for Tinnitus: A Systematic Review and How a Decision Support System Could Overcome Barriers. J Clin Med. 2021, 10, 1737. [Google Scholar] [CrossRef] [PubMed]
- Ghulyan-Bédikian V, Paolino M, Giorgetti-D’Esclercs F, Paolino F. [Psychometric properties of a French adaptation of the Tinnitus Handicap Inventory]. Encephale. 2010, 36, 390–396. [CrossRef] [PubMed]
- Available online: https://www.anses.fr/fr/content/les-r%C3%A9f%C3%A9rences-nutritionnelles-en-vitamines-et-min%C3%A9raux.
- Zeman F, Koller M, Figueiredo R; et al. Tinnitus handicap inventory for evaluating treatment effects: which changes are clinically relevant? Otolaryngol Head Neck Surg. 2011, 145, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Lemyre, L.; Tessier, R. La mesure de stress psychologique en recherche de première lgne : concept, modèle et mesure. Canadian Family Psysician – Le Médecin de famille canadien 2003, 49, 1166–1168. [Google Scholar]
- Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [CrossRef]
- International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use. ICH Harmonised Tripartite Guideline: Statistical Principles for Clinical Trials E9. London, England: European Medicines Agency; 1998. 1998.
- Cohen, J. Things I have learned (so far). Am. Psychol. 1990, 45, 1304–1312. [Google Scholar] [CrossRef]
- Wilson BS, Tucci DL, Merson MH, O’Donoghue GM. Global hearing health care: new findings and perspectives. Lancet. 2017, 390, 2503–2515. [CrossRef]
- Oppitz SJ, Garcia MV, Bruno RS; et al. Supplementation with açaí (Euterpe Oleracea Martius) for the treatment of chronic tinnitus: effects on perception, anxiety levels and oxidative metabolism biomarkers. Codas. 2022, 34, e20210076. [Google Scholar] [CrossRef]
- Sereda M, Xia J, Scutt P, Hilton MP, El Refaie A, Hoare DJ. Ginkgo biloba for tinnitus. Cochrane Database Syst Rev. 2022, 11, CD013514. [CrossRef]
- Hosseinzadeh A, Kamrava SK, Moore BCJ; et al. Molecular Aspects of Melatonin Treatment in Tinnitus: A Review. Curr Drug Targets. 2019, 20, 1112–1128. [Google Scholar] [CrossRef] [PubMed]
- Reiter RJ, Mayo JC, Tan DX, Sainz RM, Alatorre-Jimenez M, Qin L. Melatonin as an antioxidant: under promises but over delivers. J Pineal Res. 2016, 61, 253–278. [CrossRef] [PubMed]
- Community herbal monograph on Melissa officinalis L. folium. EMA/HMPC/196745/2012.
- Landgrebe M, Azevedo A, Baguley D; et al. Methodological aspects of clinical trials in tinnitus: a proposal for an international standard. J Psychosom Res. 2012, 73, 112–121. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Study flow-chart.
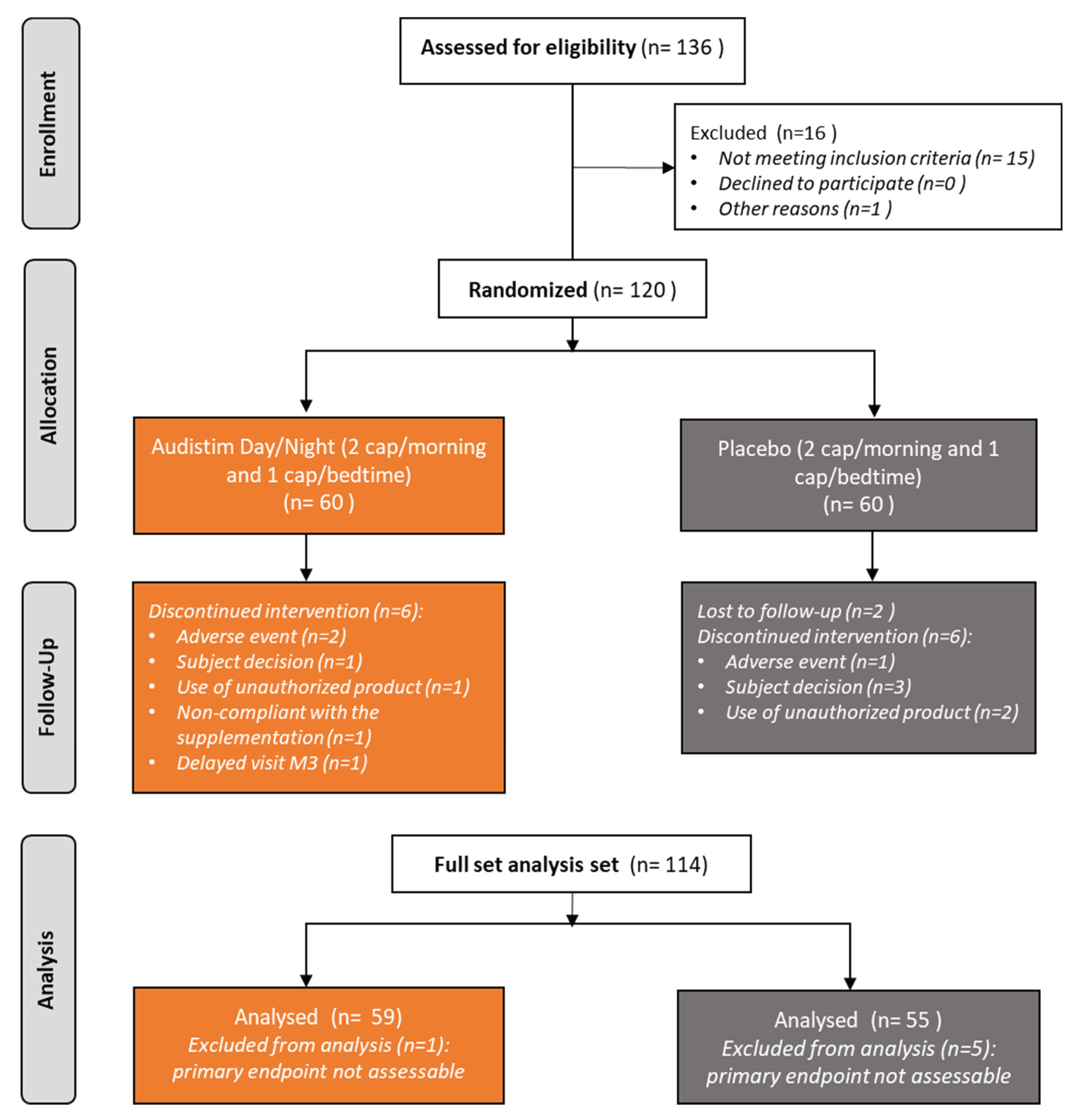
Figure 2.
THI scores over 3 months of supplementation with A D/N (AUDISTIM Day/Night) or placebo, a) all tinnitus (A D/N, n=59; placebo, n=55), b) permanent tinnitus (A D/N, n=32; placebo, n=31) and c) fluctuating tinnitus (A D/N, n=27; placebo, n=24). * and **mean significant difference between M0 and M1, or M0 and M3 with paired t-test at p value <0.05 and < 0.0001, respectively.
Figure 2.
THI scores over 3 months of supplementation with A D/N (AUDISTIM Day/Night) or placebo, a) all tinnitus (A D/N, n=59; placebo, n=55), b) permanent tinnitus (A D/N, n=32; placebo, n=31) and c) fluctuating tinnitus (A D/N, n=27; placebo, n=24). * and **mean significant difference between M0 and M1, or M0 and M3 with paired t-test at p value <0.05 and < 0.0001, respectively.
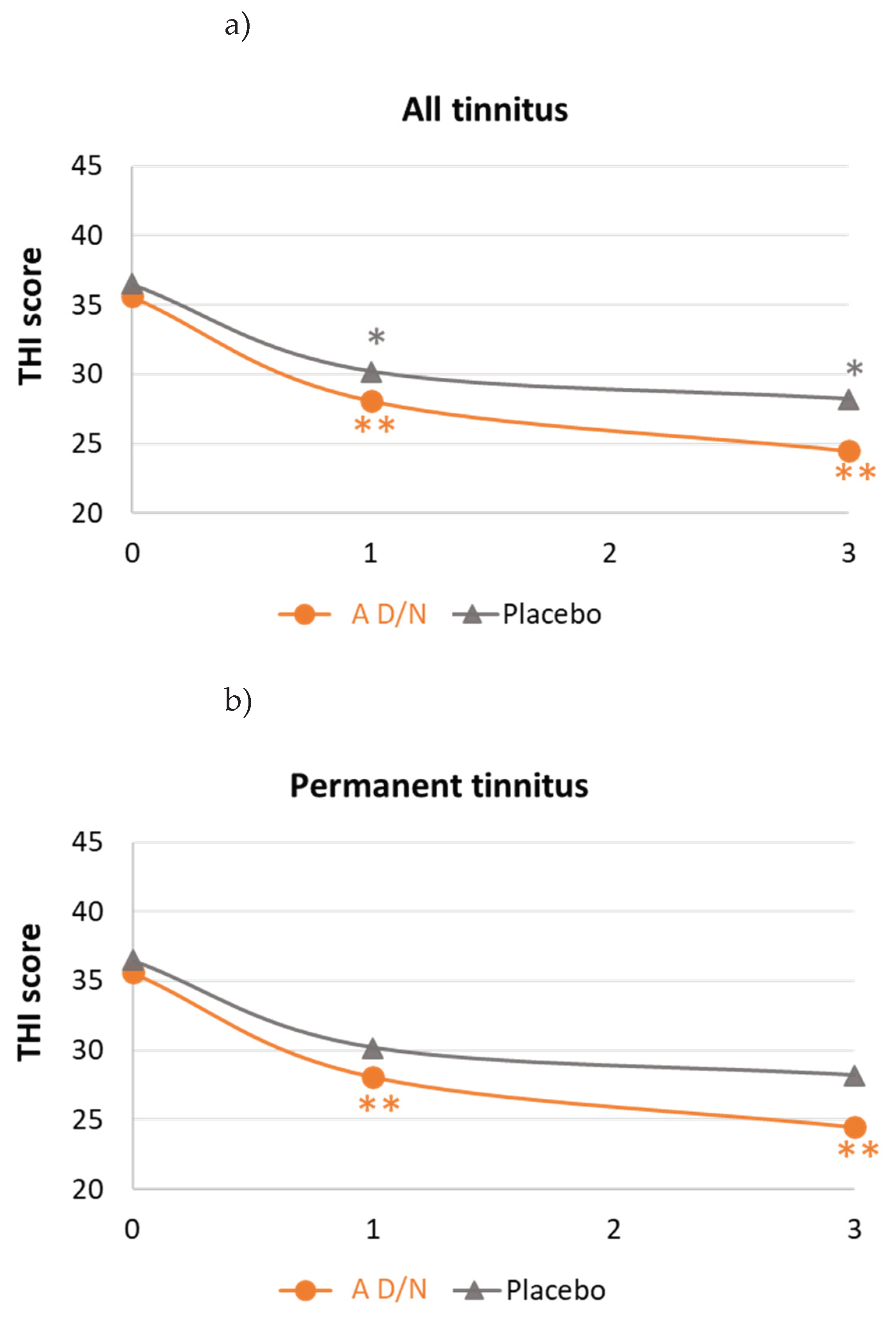
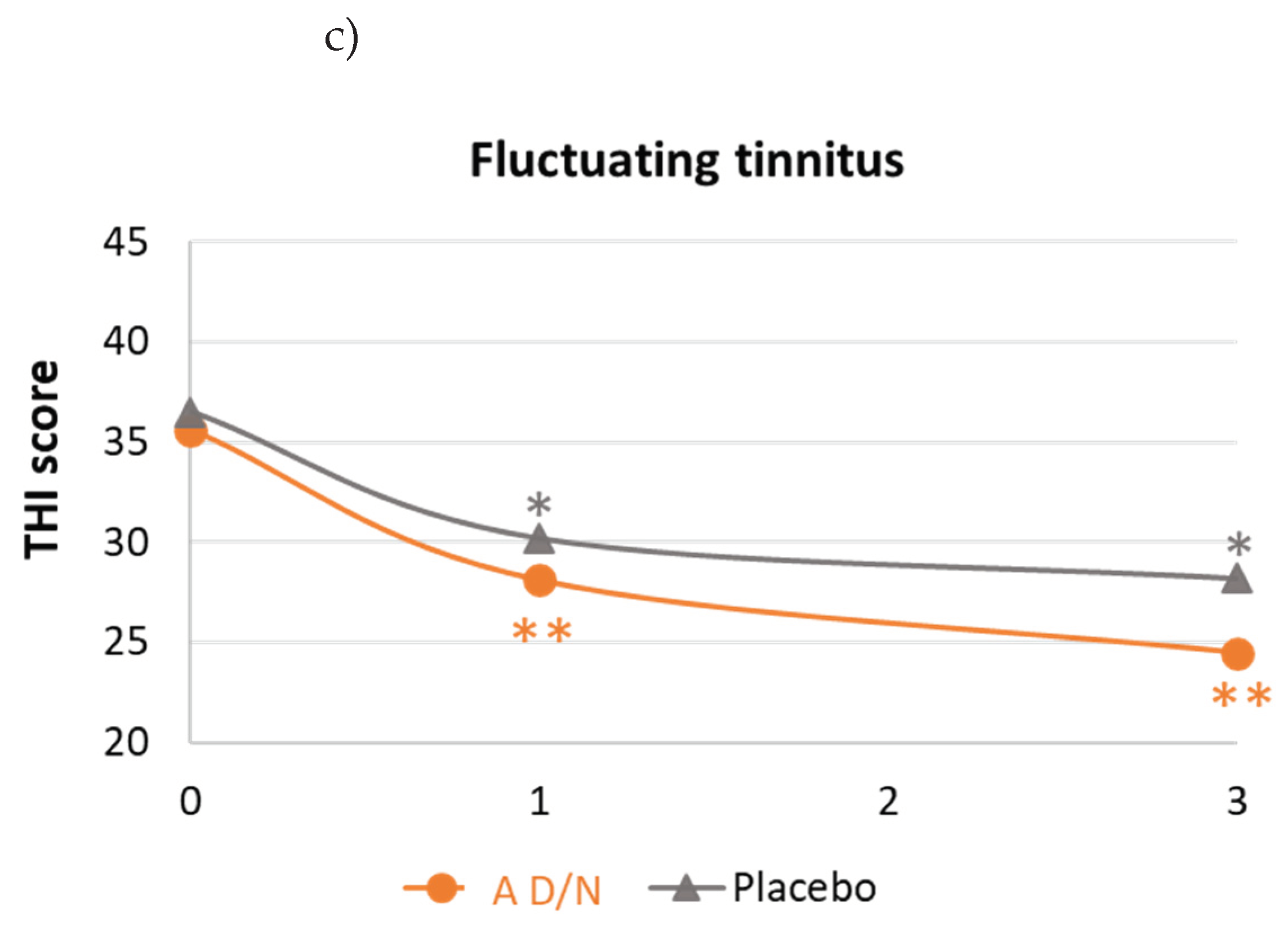
Figure 3.
Patient subjective assessment of improvement of tinnitus after 3 months of supplementation with A D/N (AUDISTIM Day/Night) or placebo, all tinnitus (A D/N, n=59; placebo, n=55), permanent tinnitus (A D/N, n=30; placebo, n=30) and fluctuating tinnitus (A D/N, n=27; placebo, n=24).
Figure 3.
Patient subjective assessment of improvement of tinnitus after 3 months of supplementation with A D/N (AUDISTIM Day/Night) or placebo, all tinnitus (A D/N, n=59; placebo, n=55), permanent tinnitus (A D/N, n=30; placebo, n=30) and fluctuating tinnitus (A D/N, n=27; placebo, n=24).
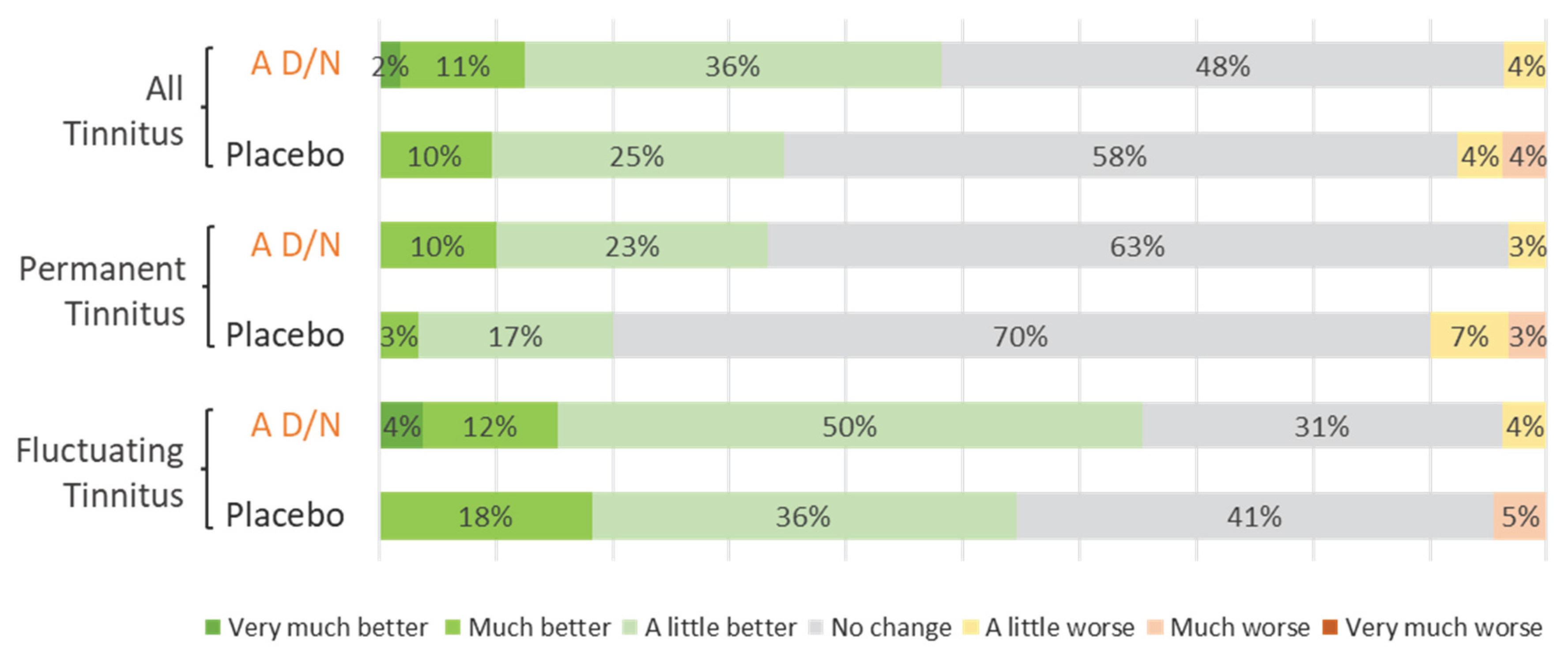

Table 1.
Description of patients (n=114).
| Patient description | A D/N (n=59) | Placebo (n=55) | p-value |
|---|---|---|---|
| Age (years) | |||
| Mean (SD) | 54.6 (12.5) | 52.9 (10.1) | 0.4281* |
| Median (IQR) | 59.0 (43.0 ; 65.0) | 53.0 (44.0 ; 59.0) | |
| Gender (% male/% female) | 37.3/ 62.7 | 47.3 / 52.7 | 0.2806** |
| Concomitant disorder (Yes) (n (%)) | 23 (39.0) | 13 (23.6) | 0.1693** |
| Clinical abnormalities (Yes) (n (%)) | 1 (1.7) | 5 (9.1) | 0.1047** |
* Student paired test, ** Chi-squared test or Fisher Test.
Table 2.
Description of tinnitus at baseline (n=114).
| Tinnitus description | A D/N(n=59) | Placebo(n=55) | p-value |
|---|---|---|---|
| Duration (years) Mean (SD) Median (IQR) |
9.5 (9.7) 6.0 (3.0 ; 13.0) |
9.0 (9.3) 5.0 (2.0 ; 15.0) |
0.7862* |
| Main aetiology | |||
| Idiopathic (n (%)) | 25 / 42.4 | 18 / 32.7 | 0.7529** |
| Acoustic trauma (n (%)) | 18 / 30.5 | 20 / 36.4 | 0.5075** |
| ENT/Viral infection (n (%)) | 6 / 10.2 | 6 / 10.9 | 0.7529** |
| Presbycusis (n (%)) | 5 / 8.5 | 2 / 3.6 | 0.4404** |
| Vascular disorders (n (%)) | 2 /3.4 | 5 / 9.1 | 0.2597** |
| Location | |||
| Both ears (n (%)) | 37 / 62.7 | 38 / 69.1 | 0.2105** |
| Right or Left ear (n (%)) | 19 / 32.2 | 17 / 30.9 | |
| Head (n (%)) | 3 / 5.1 | 0 /0.0 | |
| Tinnitus onset | |||
| Permanent (n (%)) | 32 / 54.2 | 31 / 56.4 | 0.8195** |
| Fluctuating (n (%)) | 27 / 45.8 | 24 / 43.6 | |
| Associated symptoms (Yes) (n (%)) | 41 / 69.5 | 36 / 65.5 | |
| Hypoacusis/hyperacusis | 25 / 42.4 | 25 / 45.5 | 0.8885** |
| Headache | 13 / 22.0 | 8 / 14.5 | 0.3027** |
| Annoyance (0-10 VAS) | |||
| Mean (SD) Median (IQR) |
5.3 (1.5) 5.0 (4.0 ; 6.7) |
4.9 (1.8) 5.0 (3.0 ; 7.0) |
0.1913* |
| THI total score | |||
| Mean (SD) | 38.9 (16.2) | 35.7 (17.5) | 0.3180* |
| Median (IQR) | 36.0 (26.0 ; 54.0) | 30.0 (22.0 ; 48.0) | |
| THI classification | |||
| No handicap (n (%)) | 7 (11.9) | 7 (12.7) | 0.6329** |
| Mild handicap (n (%)) | 23 (39.0) | 23 (41.8) | |
| Moderate handicap (n (%)) | 23 (39.0) | 16 (29.1) | |
| Severe handicap (n (%)) | 6 (10.2) | 9 (16.4) | |
| Catastrophic handicap (n (%)) | 0 (0.0) | 0 (0.0) |
THI: Tinnitus Handicap Inventory questionnaire, ENT: ear, nose throat infection or viral infection by SARS-Cov2.* Student paired test, ** Chi-squared test or Fisher Test.
Table 3.
Changes in tinnitus-related handicap at 3 months.
| A D/N | Placebo | p-value | |
|---|---|---|---|
| All tinnitus (n=104) | (n=59) | (n=55) | |
| Changes in THI scores | |||
| Mean (SD) | -13.2 (16.0) | -6.2 (14.4) | 0.0158* |
| 95%CI | -17.4/-9.1 | -10.1/-2.3 | |
| THI score reduction ≥20% | |||
| n (%) | 40 (67.8) | 26 (47.3) | 0.0266** |
| Permanent tinnitus (n=63) | (n=32) | (n=31) | |
| Changes in THI scores | |||
| Mean (SD) | -15.0 (16.3) | -4. (12.8) | 0.0065* |
| 95%CI | -20.9/-9.1 | -9.3/0.1 | |
| THI score reduction ≥20% | |||
| n (%) | 23 (71.9) | 15 (48.4) | 0.0568** |
| Fluctuating tinnitus (n=51) | (n=27) | (n=24) | |
| Changes in THI scores | |||
| Mean (SD) | -11.1 (15.7) | -8.3 (16.3) | 0.5384* |
| 95%CI | -17.3/-4.9 | -15.2/-1.5 | |
| THI score reduction ≥20% | |||
| n (%) | 17 (63.0) | 11 (45.8) | 0.2198** |
* ANOVA Time x Treatment, ** Chi-squared test or Fisher Test.
Table 4.
Psychological stress and sleep quality.
| A D/N | Placebo | A D/N vs Placebo | |||||
|---|---|---|---|---|---|---|---|
|
Baseline Mean (SD) |
Final Mean (SD) |
p-value* | Baseline Mean (SD) |
Final Mean (SD) |
p-value* | p-value** | |
| All tinnitus | (n=56) | (n=52) | |||||
| MSP-9 scores | 35.4 (12.6) | 31.4 (11.2) | 0.008 | 34.1 (11.2) | 32.2 (11.1) | 0.1947 | 0.3190 |
| PSQI scores | 7.4 (3.5) | 6.0 (3.2) | 0.0014 | 7.3 (3.5) | 6.3 (3.0) | 0.0374 | 0.3979 |
| Permanent tinnitus | (n=30) | (n=30) | |||||
| MSP-9 scores | 33.5 (10.4) | 29.4 (9.8) | 0.0655 | 32.5 (10.8) | 31.8 (11.1) | 0.6561 | 0.2062 |
| PSQI scores | 6.7 (3.6) | 5.3 (2.5) | 0.0154 | 6.4 (3.4) | 6.0 (3.4) | 0.4077 | 0.1855 |
| Fluctuating tinnitus | (n=26) | (n=22) | |||||
| MSP-9 scores | 37.5 (14.5) | 33.7 (12.4) | 0.0586 | 36.1 (11.5) | 32.6 (11.4) | 0.2026 | 0.9359 |
| PSQI scores | 8.2 (3.3) | 6.7 (3.8) | 0.0385 | 8.4 (3.3) | 6.8 (2.3) | 0.0458 | 0.9128 |
* Student paired test, ** ANOVA Time X Treatment.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



