
Submitted:
08 April 2024
Posted:
09 April 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The potential advantages of plant-based interventions in decreasing the incidence and lessening the morbidity and mortality of COVID-19 are yet to be widely acknowledged. Nevertheless, recent publications propose that these interventions could be effective. Our cardiology center conducted an interventional study in which we incorporated plant-based foods and provided supplementation to 3470 elderly COVID-19 patients with multiple comorbidities. We pay close attention to the precise selection of food items, the application of appropriate processing methods, and the provision of nourishing meals to our patients. Our outcome was highly successful as we achieved a zero mortality rate, and none of our patients experienced worsening conditions or required hospitalization. In this review article we present the mechanisms how plant-based and supplement interventions can mitigate COVID-19 disease severity and mortality. And experts have validated our hypotheses very recently. The measures and methods used to address the ongoing SARS-CoV-2 pandemic through plant-based interventions and supplements are effective and may help prevent or manage future pandemics.
Keywords:
Plant-based
; COVID-19
; Inflammation
; Supplements
1. Introduction
Several studies have demonstrated that a plant-based diet (PBD) can effectively treat chronic inflammatory diseases, such as obesity, atherosclerosis, hypertension, hyperlipidemia, and hypercholesterolemia. Dietary interventions not only manage these diseases but can potentially reverse them [1,2]. By reducing the consumption of foods that promote inflammation and contribute to chronic inflammatory diseases, one can further enhance the positive impact of a healthy diet. In our cardiology practice, we have observed remarkable results in patients suffering from chronic inflammation-related illnesses. These patients achieved remission with limited medication. Patients with hyperlipidemia could also meet their lipid targets according to International guidelines. We also noticed improved kidney function and successful management of glucose for non-insulin-dependent diabetes mellitus (NIDDM) or glucose intolerance patients without the need for excessive medication or insulin. Furthermore, we witnessed a regression of coronary obstruction in numerous cardiac patients, and there was a low occurrence of in-stent restenosis (ISR).
Based on our previous successful experiences in treating our patients with chronic inflammatory diseases using a plant-based diet (PBD) and dietary supplements, we hypothesized that PBD could decrease the incidence and severity of SARS-CoV-2 infection and may save lives. Our clinical trial was conducted between April 2020 and July 2023, enrolling 3,470 mostly elderly COVID-19 patients, most of whom are cardiology patients with multiple comorbidities. More than half of our study populations had been following PBD and taking dietary supplements before they contracted the coronavirus and were enrolled in our study. Even though they have comorbidities, all their clinical, laboratory, and inflammatory profiles were satisfactorily controlled. Our research report is published separately. To the best of our knowledge, we are the pioneer in embarking on the PBD and providing dietary supplements to COVID-19 patients, which started at the beginning of the pandemic.
It is important to note that during the initial eighteen months of our investigation, no studies or recommendations emerged demonstrating the benefits of PBD and dietary supplementation in reducing the virus’s incidence, severity, and mortality. Fortunately, we observed the promising outcomes at the onset of our study. So, despite significant skepticism and opposition from our Indonesian peers towards PBD intervention, we continued our research. Later on, despite the publication of positive findings in a prestigious journal indicating the crucial role of PBD in managing the coronavirus [3], our research still gained minimal traction. Undertaking interventional research with close contact with COVID-19 patients when no medications or vaccines were available was also a high-risk endeavor and very challenging. Our perseverance in continuing our research is our firm belief in PBD and supplementations, supported by our extensive knowledge of PBD and supplementations, plus our positive experiences using such interventions to manage chronic inflammatory diseases for our cardiology patients. And most importantly, our ultimate goal is to save as many lives as possible, including ours.
We put forward the notion that PBD could potentially enhance nitric oxide (NO) availability, alter the gut microbiota, improve endothelial function, reduce inflammation, combat oxidative stress, boost mitochondrial function, extend telomeres, and facilitate caloric restriction (CR) as a means to combat COVID-19. These mechanisms can potentially decrease the incidence, morbidity, and mortality rate of COVID-19 patients. Severe inflammation and blood clotting are significant contributing factors to the high mortality rate of COVID-19 patients [4,5], and PBD may help to prevent these complications. Field experts have recently validated our hypotheses, inspiring us to share our findings and publish our study.
Our research sets itself apart from other PBD studies in several ways, including utilizing raw PBD, carefully selecting foods to maximize their potential, and paying close attention to food preparation techniques, such as avoiding high-temperature cooking of vegetables, which can negatively impact the NO content. Furthermore, we supplement our dietary intervention with vitamins, minerals, and nutraceuticals to maximize anti-inflammatory and antioxidant effects, minimize oxidative stress, improve NO availability, and repair the endothelium. These supplements are selected based on our usual supplements used for cardiology patients to fight their chronic inflammatory diseases [6,7]. However, only recently has the significance of vitamins, minerals, and nutraceuticals in relation to COVID-19 been recognized [8,9]. We hypothesize that by combining our dietary intervention with strategic supplementation, we can decrease the severity and fatality rates of the coronavirus to the greatest extent possible.
2. Mechanism of Plant-Based in Decreasing Incidence, Morbidity, and Mortality of COVID-19
2.1. Mechanism of NO in Fighting Coronavirus
NO is a naturally occurring molecule found in various cell types and organ systems and plays a crucial function in the cardiovascular. Its functions include regulating basal vascular tone, preventing platelet activation, and limiting leukocyte adhesion to the endothelium. Furthermore, it significantly contributes to regulating myocardial contractility [10]. Unfortunately, conditions like obesity, hypertension, hypercholesterolemia, and NIDDM, which are commonly linked to risk factors for atherosclerosis, can lead to a decrease in NO release into the arterial wall due to synthesis dysfunction or enormous oxidative degradation [11]. Studies on humans indicate that natural NO production reduces with age, which is relevant to the number of diseases that affect elderly people [12]. It is believed that the elderly’s NO deficiency may contribute to the severity and mortality of coronavirus and the development of comorbidities [13]. On the other hand, children and young adults (below 19 years old) have low COVID-19 mortality rates, which may be due to their high NO content [14]. To measure our study population’s, N.O.; we used a salivary strip that has a 96% accuracy rate [15]. We can improve our patients’ NO readings by modifying their diet and lifestyle [16]. Figure 1 illustrates the conversion of nitrate-rich foods to nitric oxide [17].
It has been observed that coronavirus has the potential to reduce the availability of NO in the endothelium [18], as shown in Figure 2.
It is suggested that the virus could affect the cardiovascular system, resulting in conditions like acute coronary syndrome, pulmonary embolism, and heightened COVID-19 mortality. NO plays a vital role in the lungs and serves as a vasodilator, bronchodilator, anticoagulant, anti-inflammatory, and antiviral agent [18], as demonstrated in Figure 3.
Research has indicated that NO can provide therapeutic advantages, including reducing pulmonary hypertension and increasing blood flow in ventilated lung units [13]. Furthermore, a higher baseline level of NO has been linked to fewer cold symptoms, indicating that it may enhance mucosal immunocompetence and aid in preventing airway infections [19]. Recent studies have also found that inhaled nitric oxide (iNO) may be beneficial in treating COVID-19 patients by improving arterial oxygenation. Given the high risk of refractory hypoxemia in these patients, clinical guidelines need to consider the potential advantages of iNO in managing ARDS, particularly for critically ill individuals [20].
To increase NO levels in vital organs such as the hearts, brains, and lungs of coronavirus patients, we recommend incorporating dietary nitrates from sources such as raw green leafy vegetables, beets, cabbage, pomegranate, watermelon, garlic, lemongrass, ginger, turmeric into their daily diet [21]. Our study suggests that improving NO may lower morbidity and mortality rates in coronavirus patients, as previously explained.
2.2. The Role of Microbiota in Coronavirus
The human body is home to approximately 38 trillion microorganisms, and the gut is the most diversely populated and densely organ. The gut microbiota is crucial for maintaining immune homeostasis. The gut-associated lymphoid tissue (GALT) and bronchial-associated lymphoid tissue, part of the mucosal immune system, serve as the first line of defense against infections. The GALT includes the Peyer’s patches, appendix and isolated lymphoid follicles of the intestinal mucosa. To regulate the immune system, interaction between the GALT and the gut microbiota is extremely important. Since most (70-80%) of immune cells are found in the gut, maintaining a healthy gut microbiota is essential [22]. The understanding of gut microbiota has been extensively studied compared to lung microbiota.
The relationship between the gut and lung systems, known as the “gut-lung axis,” has been extensively researched, and evidence supports the connection between gut microbiota and lung immunity. Dysfunction of gut microbiota has been linked to impaired alveolar macrophage function and reduced bacteria-killing capacity. Antibiotics can disrupt the gut microbiota, leading to the survival and growth of pathogenic microorganisms in the lungs. The gut-lung axis is bidirectional; through the bloodstream, microbial components from the gut can impact the lungs, and lung inflammation may also impact the gut microbiota. Studies have shown that exposure to the influenza virus can result in the migration of CD4 T cells from the lungs to the intestine, leading to dysbiosis of the gut microbiota and an abnormal Th17 response, intestinal damage, and gastroenteritis [23]. Chronic inflammatory diseases have also been linked to the gut microbiota composition [24].
Many simple therapeutic techniques have been proposed to modify microbiota and combat chronic illnesses. These include changes to one’s diet and the use of pre-and probiotics. These modifications have the potential to mitigate the severity of COVID-19 through a multitude of mechanisms while also impacting the course of chronic illnesses like hypertension, NIDDM, obesity, and coronary heart disease. Addressing these comorbidities can decrease the risk of developing severe coronavirus and facing mortality rates.
Disrupting beneficial microorganisms in the gut’s microbiota can lead to gut dysbiosis and may increase the risk of respiratory illnesses, sepsis, and ARDS. The intestinal barrier serves as a shield against harmful microbes and their byproducts from entering the bloodstream. However, when gut dysbiosis occurs, the gut barrier may become more permeable, resulting in a leaky gut. This condition has been linked to decreased short-chain fatty acids (SCFAs) produced by gut bacteria. This increase in gut permeability allows microbiota-derived lipopolysaccharides (LPS) and inflammatory components to enter the bloodstream, resulting in inflammation and immune activation. Toll-like receptor 4 (TLR4) has a significant role in immune activation, and its activation by LPS can exacerbate a range of clinical problems. Research has indicated that TLR4 activation by LPS can worsen mortality rates in cases of influenza infections [25].
SCFAs are essential for regulating immune and inflammatory responses. By promoting mucin production and maintaining an acidic pH in the gut environment, harmful microbes are discouraged from growing. Furthermore, SCFAs maintain the integrity of the gut epithelium. So, epithelium leakage or translocation can be avoided. SCFAs are also powerful histone deacetylase (HDAC) inhibitors that can reduce inflammation by boosting the numbers and functions of regulatory T-, T helper-, and Th17 effector- cells. SCFAs can activate G protein-coupled receptors (GPCRs) like GPR43 and inhibit the Nf-kB pathway, which has an anti-inflammatory effect. Recent research indicates a potential gut-lung axis, as small amounts of SCFAs are present in the lungs [26]. The studies have also shown that SCFAs assist in creating macrophage and dendritic cell progenitors in the bone marrow. Additionally, SCFAs protect against airway inflammation and respiratory tract infections by enhancing the function of T cells [27].
Younger people may experience less severe symptoms and less risk of developing cytokine storms due to their less inflammatory response toward the coronavirus [28]. On the other hand, the elderly are more likely to have an imbalance in their gut microbiota, so the chances of having severe inflammation and the risk of developing cytokine storms will be higher. Also, beneficial strains of microbiota like Bifidobacteria and Lactobacillus and bacteria that produce SCFAs, which help maintain intestinal barrier integrity, will be altered in the elderly. Many shreds of evidence support that gut dysbiosis is important in chronic aging-related diseases. Therefore, the morbidity and mortality rates of coronavirus in elderly patients over 65 with comorbidities such as NIDDM, obesity, hyperlipidemia, hypertension, and cardiovascular disorders are high [29].
Numerous Studies reveal that immunological aging is connected with “inflammaging,” a subclinical inflammatory state that relies heavily on Th1 immune responses. Children, on the other hand, exhibit more Th2 response, which leads to less production of pro-inflammatory molecules. Recent research has extensively studied and found that gut microbiota links to various chronic inflammatory diseases such as chronic respiratory diseases, inflammatory bowel disease, NIDDM, cardiovascular disease, depression, and hypertension [30]. Proving there is a strong correlation between gut microbiota disturbances and disease severity and clinical outcomes in elderly COVID-19 with chronic inflammatory illness [31]. Multiple studies have suggested that increased cytokine and chemokine production, leading to viral hyperinflammation (cytokine storm), is mainly responsible for coronavirus mortality [32], as illustrated in Figure 4.
Maintaining an optimized and balanced immune response is essential in preventing severe inflammatory reactions that could potentially be life-threatening. This can be achieved by cultivating a healthy gut microbiota. A well-regulated immune response is critical for determining clinical outcomes and consequences, and it must be neither overly reactive nor under-reactive. Consuming a nutritious diet and taking supplements can help achieve a harmonious immune response balance.
Research has shown that dietary carnitine, primarily found in animal protein, can negatively impact human vascular health. Gut flora converts carnitine into trimethylamine (TMA), which is then metabolized into trimethylamine N-oxide (TMAO) in the liver. Increased TMAO in the bloodstream is linked to major adverse cardiovascular events, such as stroke, myocardial infarction, congestive heart failure, and mortality. In COVID-19 patients, a correlation between elevated serum TMAO and inflammation and thrombosis has been observed. Gut dysbiosis will also produce TMAO. Various molecular mechanisms, such as the nuclear factor kappa (NF-kB) and the expression of scavenger receptors (SRs) on the surface of macrophages, will be upregulated by TMAO and lead to inflammation. TMAO can also induce the expression of pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-𝛼) and interleukin 1ß(IL-1ß), which increase the inflammatory response. Moreover, TMAO will reduce the expression of anti-inflammatory cytokines such as interleukin-10 (IL-10). TMAO can also enhance platelet aggregation and adhesion to collagen, which may increase the risk of thrombosis. Recent studies have shown that high TMAO levels may lead to coronavirus severity [33].
Previous studies revealed that those who adhere to a vegan or vegetarian diet tend to have decreased levels of TMAO. Instead, consuming red meat, processed meat, egg yolks, fish, and full-fat dairy products results in elevated TMAO levels.
The microorganisms that reside in our gastrointestinal (GI) tract, from the mouth to the anus, are an essential part of our overall health. Our well-being is maintained by the gut, which is connected to various organs in our body through the gut-organ axis. Moreover, the gut-brain axis (GBA) significantly influences our emotions and behavior. The gut-brain-immune system axis operates bi-directionally and can impact the progression of COVID-19, particularly when stress is involved. Several communication systems exist between the gut and brain, including the autonomic nervous system (ANS), the enteric nervous system (ENS), the immune system, and neuroendocrine signaling systems, which can all impact the gut microbiota. As a result, having a healthy balance of gut microbiota may help alleviate stress levels during the pandemic [34].
In light of the coronavirus pandemic, it’s crucial to maintain a healthy mood and behavior to prevent cytokine storms. Several risk factors for cardiovascular disease can lead to dysbiosis, weakening the gut barrier and causing inflammation. Recent research has shown that this can increase the severity of coronavirus symptoms. Furthermore, studies have shown a close association between gut microbiota, dietary lipid intake, and atherosclerosis development, involving metabolic and inflammatory factors. A novel pathway has been identified that connects these components, with the production of TMAO being linked to reduced bile acid synthesis and inhibited reverse cholesterol transport, ultimately contributing to the development of atherosclerosis. Microbial dysbiosis and abnormal metabolite production have been associated with exacerbation of acute heart failure [35], which can worsen the prognosis of COVID-19 patients who already suffer from both atherosclerosis and heart failure (gut-heart axis).
Numerous health benefits have been associated with healthy microbial metabolites, such as anti-inflammatory, antioxidant, anti-lipid, antiproliferative, anti-obesity, antihypertensive, and immunomodulatory. Recent research has shown that the gut microbiota can adapt rapidly following a change in diet, whether PBD or omnivorous, with noticeable alteration appearing in three days [36]. This information suggests that even those with unhealthy eating habits can improve their microbiota through dietary changes, which is especially relevant for new COVID-19 patients in acute settings. A shift in gut microbiota composition occurs when transitioning from PBD to an omnivorous diet, with increased bile acid-metabolizing species, which can induce an inflammatory process. On the other hand, PBD effectively combats inflammation, as it is shown in reducing chronic inflammation markers such as Fibrinogen, IL-6, and CRP [37]. Interestingly, individuals who primarily follow PBD do not experience increased TMAO levels when occasionally consuming animal-based foods [38]. This is postulated due to the microbiota environment established over time.
Many experts suggest that the current COVID-19 pandemic presents a rare chance to assess how nutritional interventions may help fight infectious diseases. With this in mind, conducting tests during the pandemic can yield valuable information [39]. Our studies have revealed a significant link between consuming foods that include fresh, nutrient-rich foods like vegetables, legumes, whole grains, healthy fats (seeds, avocado, and a moderate amount of oily fish), and fruits and limiting one’s intake of sugary products, high-calorie empty nutrients, and high-salt foods, leading to a decrease in COVID-19 severity and mortality.
2.3. Mechanism of Inflammation and Endothelial Dysfunction in Coronavirus
The role of chronic inflammation in developing vascular lesions cannot be overstated. This process causes endothelial dysfunction and triggers several other processes that contribute to the worsening of atherosclerosis. These processes include platelet aggregation, leucocyte adhesion, cytokine production, and increased endothelial permeability [40]. Unfortunately, atherosclerosis is often associated with acute coronary events, and COVID-19 can exacerbate this situation by inducing a severe inflammatory state that may trigger similar events. It’s important to note that coronary artery disease resulting from atherosclerosis, as well as heart failure, hypertension, and atrial fibrillation, are all considered comorbidities for COVID-19, and they are also caused by chronic inflammation [41]. Patients with heart conditions who contract coronavirus are at an increased risk of developing arrhythmia, acute coronary syndrome, and acute heart failure, which can lead to higher mortality rates.
Eating unhealthy foods such as sugary drinks, snacks, cakes, pastries, sweets, added salt, saturated fat, trans-fat, cholesterol, dairy products, processed meat, red meats, poultry, and eggs can contribute to chronic inflammation [42]. Coronavirus is classified as an acute inflammatory disorder, and it can increase inflammatory markers such as ferritin, procalcitonin, LDH, D-Dimer, and acute phase response proteins. This virus can also trigger a cytokine storm, a severe inflammatory reaction that can be fatal [43]. Coronavirus patients with chronic inflammation are at risk for severe inflammation regardless of their comorbidities. In that case, their body will have to work extra hard to combat the inflammation and its complications. Their chances of experiencing a cytokine storm and facing a higher mortality risk are understandably higher [44,45]. Conversely, eating foods that increase dietary inflammatory index (DII) is recommended to combat the inflammatory response in our coronavirus patients (Table 1).
Rich polyphenols are found in vegetables and fruits and can inhibit the binding of coronavirus spike protein to the ACE2 receptor. Thus, viral entry into host cells can be prevented, and viral RNA replication and protein processing can be suppressed [46]. Consuming red meat, refined sugar, high cholesterol, saturated and trans fats foods will promote inflammation and can expedite the binding of coronavirus to host cells [47].
Adopting a healthy lifestyle for an extended period can significantly improve chronic disease conditions. Therefore, an individual with multiple comorbidities who embraces a healthy PBD and lifestyle may observe a normalization of most of their chronic inflammatory markers. These can decrease the risk of coronavirus severity and mortality. Is PBD intervention a viable option for individuals with chronic comorbidities who contract COVID-19 in the acute setting? While research has indicated that PBD intervention can effectively reduce acute arthritic pain [48,49], our experience with COVID-19 patients has demonstrated the same efficacy. Even though inflammatory markers may not improve, patients reported symptom relief. Thus, our study supports this hypothesis.
2.4. Role of Oxidative Stress in Coronavirus
One mechanism through which the coronavirus causes imbalances within the body is by generating reactive oxygen species (ROS) and diminishing the body’s capacity to produce antioxidants that can combat the virus. Automatically, this will induce redox stress, decreasing the body’s ability to fight off the virus and increasing inflammation and cell damage. Ultimately, this will damage tissues and organs in the body. A diagram illustrating this process can be found in Figure 5.
ROS is a natural byproduct of metabolic processes in different organelles, including endoplasmic reticulum (ER), plasma and nuclear membranes, mitochondria, and peroxisomes. These ROS play an essential role in various cellular processes. ROS can cause oxidative damage to mitochondria, dysregulated gene expression, aberrant cellular signaling, and impaired host defense. Notably, the primary source of ROS is from mitochondria named mito-ROS, which are formed during energy production. ROS levels can increase during viral infections, and while they have harmful effects on tissues and cells, they are also essential as an antiviral [50].
Too much ROS in the body can harm essential parts of cells like proteins, lipids, and DNA. ROS can also affect immune functions, cause inflammation, and damage organs and tissues. Research has found that oxidative stress is crucial in viral respiratory infections like influenza and RSV. In severe cases of COVID-19, elevated oxidative stress can induce inflammation, harm endothelial cells, plus form blood clots. Eventually, it will damage multiple organs [51,52].
Research suggests that elderly patients are more susceptible to oxidative stress. There is a reciprocal link between ROS and chronic inflammation, in which chronic inflammation leads to the buildup of ROS, and ROS also contributes to chronic inflammation [53]. Consequently, older individuals who have chronic inflammatory conditions are at greater risk of experiencing serious illness in the event of contracting SARS-CoV-2 infections [54].
Research has shown that consuming meat products, refined sugars, and fats can increase ROS levels, resulting in inflammation. However, studies indicate that incorporating PBD can potentially reduce inflammation and oxidative stress, which play a significant role in coronavirus infection [55,56,57,58]. Exploring dietary changes for COVID-19 patients may be prudent as the current omnivorous or similar diets can increase oxidative stress and inflammation. Adopting PBD can help manage chronic inflammatory conditions and enhance the likelihood of surviving the COVID-19 pandemic.
2.5. The Link between Mitochondria Health and COVID-19 Severity and Mortality
As we grow older, the powerhouses of our cells, known as mitochondria, undergo changes that cause a decline in their function. This decline is caused by ROS-inducing accumulation of oxidative damage and mutations. As a result, the volume, integrity, and functionality of mitochondrial DNA (mtDNA) decrease. Moreover, the mitochondria of older adults are characterized by significant increases in ROS and decreased antioxidant defense, which lead to impaired functions. These include decreased ATP production, lowered oxidative capacity, and reduced oxidative phosphorylation. Additionally, with aging, mitochondrial biogenesis will decline. This is due to inhibition of mitophagy and alterations in mitochondrial dynamics (fission and fusion). An autophagy process that eliminates defective mitochondria will also deteriorate in aging.
Acute and chronic inflammatory diseases are characterized by an excessive generation of ROS. This may cause damage to mtDNA, mitochondrial proteins, and lipids. This, in turn, negatively affects normal mitochondrial function and dynamics. Inflammation is generated by various mitochondrial products called damage-associated molecular patterns (DAMPs) and is released into the cytosol or extracellular environment. Protective measures are in place to prevent mitochondria from triggering harmful inflammatory responses, such as disposing of damaged mitochondria through autophagy. However, if these mechanisms are overwhelmed or not functioning correctly, inflammatory reactions instigated by mitochondria can become problematic and contribute to developing disorders associated with autoimmunity. Furthermore, inefficient inflammatory pathways can exacerbate infectious diseases and impede healing.
Atherosclerosis occurs due to the dysfunction of endothelial cells and the infiltration of lipids. Mitochondrial dysfunction can negatively impact various cells within the arterial wall, including endothelial cells, smooth muscle cells, macrophages, and lymphocytes, leading to heightened ROS levels. This can cause chronic inflammation, oxidative stress, and intracellular lipid deposition. Moreover, mitochondrial dysfunction plays a significant role in chronic inflammatory diseases like hypertension, obesity, and asthma [59,60].
As we learn more about COVID-19, it becomes increasingly clear that certain factors may contribute to its severity and mortality. These include age, age-related conditions, and underlying disorders like CVD, metabolic syndrome (including NIDDM), obesity, and hypertension. In coronavirus disease development, a potential role for mitochondria has been discovered. Mitochondria and its mtDAMPs control the immune system and impact coronavirus infection. It is suggested that mitochondria hijacked by the coronavirus could significantly affect COVID-19 pathogenesis [61], potentially causing massive inflammation and damage to multiple organs. A new study in the journal Nature sheds light on why some people with COVID-19 develop these severe symptoms, revealing that the virus may be able to infect and cause fatalities in vital immune cells within the bloodstream and lungs. As we continue to investigate this virus, it has been proven that mitochondrial dysfunction significantly eliminates these immune cells [62].
Studies have proposed that people living in “blue zones” lead long and healthy lives by adhering to healthy habits such as exercising regularly, eating a balanced diet, mainly being PBD, abstaining from harmful substances, managing stress effectively, having strong social support, and getting enough rest. These lifestyle choices contribute to maintaining healthy mitochondria. Mitochondrial function can be improved by consuming PBD foods, specific natural products, caloric restriction, intermittent fasting, and exercise [63,64,65]. Our elderly coronavirus cardiology patients have been living a Blue Zone lifestyle for many years, leading us to hypothesize that this has resulted in less severe symptoms and zero mortality due to their healthy mitochondria.
2.6. Potential Benefits of Telomere Manipulation in Coronavirus Treatment
As the Centers for Disease Control and Prevention (CDC) reported, the most significant factor in determining poor outcomes and severe illness in individuals with COVID-19 is aging. Data from the National Vital Statistics System (NVSS) at the CDC reveals that people aged 50-64 with COVID-19 are 25 times more likely to die than those under 30 years old. For individuals aged 65-74, the risk of death increases to 60 times, while for those over 85, it jumps to 340 times. This data includes all deaths in America from February 2020 to July 1, 2022, regardless of vaccination status [66,67].
Short telomeres are affiliated with a higher probability of all-cause mortality and disease-specific mortality in the general population [68]. Studies suggest that COVID-19 severity in older individuals may be influenced by the same molecular pathways that cause aging. One of these pathways involves gradual telomeres shortening. Telomeres are protective structures at the ends of chromosomes. When telomeres become excessively short, they can hinder tissue regeneration and disrupt tissue homeostasis, leading to disease. Since the coronavirus infects various cell types, it triggers cell turnover and regeneration to support homeostasis. Research has shown that people with shorter telomeres are at an increased risk of experiencing severe coronavirus symptoms. The risk of developing severe coronavirus pathologies has been associated with individuals with higher percentiles of short telomeres and lower percentiles of telomere length [69,70,71]. Myeloid and lymphoid cells contribute to innate and adaptive immunity, which is essential in defending against coronavirus [72]. To resist the infection, the production of myeloid cells is rapidly activated when the virus enters the body. The length of telomeres will shorten with age; this will affect the production of T and B cells, which are crucial to clearing the virus. Understandably, older people will have a higher risk of a T-cell shortfall when contracting coronavirus compared to younger people. People with inherently short T-cell telomeres will experience poor adaptive immune response caused by a T-cell deficit, which might contribute to the severity of COVID-19. These individuals might also generate inadequate T-cell response to anti-SARS-Cov-2 vaccination, which is vital to know [73]. Furthermore, ACE2 (Angiotensin Converting Enzyme 2), the receptor for SARS-CoV-2, is upregulated by shortened telomeres. So, telomere shortening in elderly individuals increases their susceptibility to coronavirus infection and increases their risk for coronavirus severity and mortality [74].
Chronic inflammation can cause the shortening of telomeres, altering the genes related to telomeres, and decreasing telomerase enzymes, which control the release of cytokines that cause inflammation. All of these mechanisms will cause severe COVID-19 disease and mortality. There is a two-way relationship between telomere shortening and inflammation; telomere attrition and dysfunction can cause low-grade inflammation. On the other hand, inflammation can speed up telomere wear and telomere dysfunction. [75].
Chronic inflammation and oxidative stress can accelerate telomere shortening. However, consuming healthy PBD, which is full of anti-inflammatory and antioxidant properties, counteracts this process. Observational studies have indicated that adopting a healthy PBD, consuming seeds and their derivatives, and incorporating carotenoids will promote telomere lengthening. This can lead to improved overall health and longevity [76,77].
Elizabeth Blackburn, a Nobel Prize winner, discovered that switching to a vegan diet can change over 500 genes in just three months. This diet can activate genes that help prevent diseases and deactivate genes that cause chronic inflammatory diseases [78]. There are various ways to strengthen our telomeres, including exercising regularly, avoiding smoking, and consuming a diet rich in plant-based foods that protect telomeres. Dean Ornish and Elizabeth Blackburn conducted a study demonstrating how PBD can increase telomerase activity, the enzyme responsible for maintaining long telomeres. The ability to lengthen telomeres is crucial for longevity. While we cannot reverse chronological age, we can reverse biological age, which can help us reverse chronic illnesses in our patients and protect them from severe morbidity and mortality from coronavirus. Additionally, reducing our patients’ biological age by one or two decades will automatically decrease their risk of developing severe coronavirus. We hypothesized that one of the mechanisms implies that the elderly coronavirus patients in our study have milder symptoms and experience no mortality, which is linked to their telomere superiority.
2.7. Caloric Restriction is Emerging As an Essential Factor in the Fight Against Inflammation
Reducing caloric intake, commonly known as Caloric Restriction or CR, has been shown to have consistent anti-aging effects across various organisms. Age-related diseases, including chronic inflammatory disorders such as stroke, NIDDM, cardiovascular disease, hypertension, and cancer, have been shown to improve with the practice of CR. CR can reduce oxidative stress and inflammation while boosting the production and activity of antioxidant enzymes and anti-inflammatory mediators. Studies have also revealed that CR can improve overall health and well-being, reduce ROS and inflammation, enhance cellular protection, optimize energy metabolism, improve insulin sensitivity and glucose regulation, induce functional changes in the neuroendocrine systems, and even shape the gut microbiota [79].
DNA and RNA viruses, including coronavirus, use the Mammalian Target of Rapamycin (mTOR) as their signaling system to replicate and persist in host cells. CR has been found to inhibit the mTOR pathway, similar to the effect of Rapamycin in laboratory research. One of the mechanisms CR benefits in coronavirus is mTOR inhibition and autophagy promotion. Moreover, CR could help fight the virus by interrupting the viral cycle (protein synthesis) [80].
Increased glucose variability and poor glycemic control have been associated with coronavirus severity [81,82]. Metabolic syndrome and insulin resistance, as shown by elevated triglycerides and glucose (TyG) index, are associated with coronavirus severity and morbidity [83,84]. Eating healthy PBD with CR will help the patients have proper glycemic control, achieve good metabolism, and avoid insulin resistance.
In our modern society, unhealthy habits like consuming excessive calories and living a sedentary lifestyle are significant determinants of health issues and inflammatory disorders. The overconsumption of food, especially unhealthy food, can pose big problems. Therefore, COVID-19 patients who consume excessive calories with poor nutrients will struggle to fight inflammation, especially if their bodies are already inflamed [85]. We hypothesized that the whole food PBD emphasizing CR may have contributed to the mild illness and zero mortality observed in our COVID-19 elderly patients with multiple comorbidities study.
3. Supplements Their Significant Role in Managing COVID-19
In the preliminary phase of our research, we did not come across any academic literature demonstrating the role of dietary supplements in mitigating the frequency, severity, and mortality of coronavirus infection. Therefore, the literature we used to determine the types of vitamins, minerals, and nutraceuticals in our study was taken from the literature we used in previous studies, where we combatted chronic inflammatory diseases with PBD and dietary supplements. Those dietary supplements have been known to increase NO levels, reduce inflammation, serve as immunomodulatory, decrease the likelihood of cytokine storms, fight oxidative stress, and exhibit antiviral properties. We also studied extensively literature about dietary supplements that have shown their benefits in previous viral pandemics.
Most adults consume a poor-quality diet and lack essential nutrients such as magnesium, calcium, potassium, iron, vitamins A, C, D, E, fiber, and choline [86]. Therefore, we provide our patients with multivitamins based on the literature and blood levels. It is worth noting that all of our cardiology patients who follow PBD have been advised to take B12, dietary multivitamins, and supplements with anti-oxidant, anti-inflammatory, endothelial-supporting, and other properties relevant to cardiovascular health.
3.1. Vitamin C
Due to its anti-infective properties and safety, many experts have proposed vitamin C as a potential treatment for coronavirus. Studies have shown the severity and duration of colds can be reduced by taking vitamin C [87]. Numerous studies have revealed that vitamin C may support cellular health and defense against coronavirus infection. This is believed because vitamin C has anti-oxidative stress and anti-inflammatory properties [88]. In severe coronavirus cases, high doses of vitamin C help fight oxidative stress and relieve the severity of cytokine storms. A high dose of intravenous vitamin C shortens patients’ time in the ICU, and if combined with corticosteroids and thiamin, it also reduces mortality [89].
In treating patients who require mechanical ventilation caused by an acute inflammatory lung injury, vitamin C has positive effects due to its oxidative stress properties. A study from China suggested that high-dose intravenous vitamin C can effectively treat coronavirus patients. Those patients who received intravenous bolus vitamin C had their oxygenation improved, and no mortality was observed [87].
3.2. Vitamin D
In our previous experience with cardiology patients who strictly adhered to a plant-based diet, we found that most of them were deficient in vitamin D. Therefore, we recommend that our patients take vitamin D supplements and adjust the dosage based on their blood vitamin D levels. We have discovered that vitamin D plays a crucial role in chronic inflammatory diseases, including coronary heart disease, and it may also play a role in combating COVID-19, in which inflammation plays a significant role.
T regulatory lymphocytes (Tregs) are essential in fighting against uncontrolled inflammation and viral infections. However, many COVID-19 patients have low Tregs levels. One way to increase Tregs levels is through supplementation with vitamin D. Decreased vitamin D has been linked to increased inflammatory cytokines, which significantly increase the risk of infection in the upper respiratory tract, including viral and pneumonia [92]. The recent paper has acknowledged the role of vitamin D in reducing the risk of COVID-19. The proposed mechanism is the induction of cathelicidin and defensins, which decreases the risk of viral and bacterial infections and diseases, including pneumonia. Additionally, vitamin D may reduce the binding of the virus to the ACE2 receptor, which could potentially lessen the risk of cytokine storms in coronavirus infection [93].
The likelihood of thrombotic events, commonly observed in coronavirus patients, has been associated with a vitamin D deficiency [94,95]. During the pandemic, it was observed that many coronavirus patients developed severe diseases or died due to vitamin D deficiency [96]. A recent meta-analysis has suggested that vitamin D supplementation could positively impact the incidence, severity, and mortality of SARS-CoV-2 illness, especially in patients with vitamin D deficiency [97,98,99].
3.3. Vitamin B3, Precursor of NAD+
There are three primary types of vitamin B3, i.e., Nicotinic acid (NA), nicotinamide riboside (NR), and nicotinamide (NAM). These vitamins are not only helpful in preventing pellagra but may also prevent some of the physiological changes that occur with age-related diseases and promote healthy aging, particularly NR [100]. It has been suggested that increasing NAD+ levels might enhance the body’s ability to fight off viruses and reduce inflammation. NA, NR, and NAM play essential roles as precursors of NAD+ and provide the production of NAD+ through different metabolic pathways.
Studies indicate that different types of B3 vitamins will support NAD+ levels differently. To increase NAD+ concentrations, one can give NMN, which is derived from NAM and in the body will be converted into NAD+. NMN only requires one enzymatic step to be transformed into NAD+ and is currently the most effective method to raise NAD+ levels [101,102]. Research on NAD+ in vascular aging and chronic inflammatory diseases like coronary artery disease has been promising. NAD+ has been shown to reduce chronic inflammation, induce reactivate autophagy, and assist mitochondrial biogenesis. These findings suggest that supplementing with precursor NAD+ may be a useful therapeutic approach for treating these conditions [103], as we have done for our elderly cardiology patients long before the coronavirus pandemic. Further, more sophisticated research is required before recommending precursor NAD+ to reduce the morbidity and mortality of coronavirus patients.
3.4. Zinc
Oral zinc (Zn) supplementation can reduce the 30-day death rate, shorten the duration of symptoms, and decrease the ICU admission rate, as shown in a recent randomized, double-blind controlled trial [104]. Trace element zinc is crucial in stimulating innate and acquired immunity. A recent meta-analysis has found that zinc supplementation can reduce coronavirus mortality in hospitals. Due to the scientific evidence of zinc’s role in coronavirus patients, it should be considered an adjunct therapy [105].
3.5. Copper
Both copper (Cu) and zinc play an essential role in the production of an important antioxidant enzyme known as superoxide dismutase (SOD). This enzyme aids in combating free radicals and decreasing oxidative stress. Maintaining the appropriate ratio between the two is essential to ensure the optimal functioning of this enzyme. It is important to know that zinc can lead to copper deficiency. Therefore, seeking guidance from a qualified healthcare professional is crucial to prevent adverse effects [106]. Cu plays a critical role in assisting the functions of macrophages, neutrophils, and immune cells such as B cells, T helper cells, and natural killer (NK) cells. These blood cells kill infectious microbes, produce specific antibodies against pathogens, and mediate cell-mediated immunity. In humans with Cu deficiency, there is an increased risk for infections due to these blood cells’ decreased number and function.
Additionally, Cu can kill viral infections like poliovirus, human immunodeficiency virus type 1 (HIV-1), single—or double-stranded DNA or RNA, and other enveloped or non-enveloped viruses. Moreover, Cu has a potent contact-killing capacity against several viruses, including SARS-CoV-2 [107]. We always combine Zn and Cu in our center since Zn can lead to Cu deficiency.
3.6. Selenium
Several studies have suggested that lacking selenium may negatively affect viral disorders. The correlation between selenium and coronavirus disease severity research has yielded mixed results [108]. According to the report, a shortage of selenium is linked to a higher risk of chronic diseases with inflammatory pathogenesis [109]. In viral disorders, supplementing with selenium has shown promising outcomes [110]. This is assumed due to selenium’s immune-boosting, anti-inflammatory, and antithrombotic effects [111]. Most of our cardiology patients have been consuming selenium before contracting coronavirus.
3.7. Coenzyme Q10 (CoQ10)
CoQ10 benefits cardiovascular health by helping reduce total cholesterol, improving endothelial function, and fighting inflammation and oxidative stress. This also makes it a suitable option for treating COVID-19 [112,113]. A recent meta-analysis found that CoQ10 supplements taken for 10 weeks may lower malondialdehyde (MDA), IL-6, and TNF-α levels, which are all involved in COVID-19 inflammation [114].
In the course of the resurgence of the coronavirus pandemic in China in 2023, there has been a growing demand for Ubiquinol—the active form of CoQ10. Supplementing with Ubiquinol can significantly increase the level of CoQ10 in whole blood, platelets, and plasma. CoQ10 can also accelerate the regeneration of mitochondrial function [115,116]. Recent research has shown that patients recovered from coronavirus have reduced levels of platelet mitochondrial function and decreased endogenous CoQ10. Mitochondria are the energy powerhouses of our cells and are vital for cellular metabolism and immune responses. Further research has proposed that mitochondria have a role in antiviral defense [117,118]. We used CoQ10 on our cardiology patients, which may also benefit coronavirus patients.
3.8. Astaxanthin
Studies have shown that astaxanthin significantly reduces oxidative stress biomarkers, such as blood MDA levels. This effect is particularly notable in NIDDM patients, especially those who are overweight, where astaxanthin has been found to improve superoxide dismutase activity and reduce serum isoprostane, which has an antioxidant effect and can neutralize free radicals [119].
Natural astaxanthin can potentially alleviate cytokine release syndrome by regulating inflammatory cytokines. The mechanism is by inhibiting the activities of key players such as JAK/STAT-3, NF-kB, NLRP3, while regulating the expression of pro-inflammatory factors such as IL-6, IL-8, TNF-α, and IL-1ß. Additionally, natural astaxanthin can prevent oxidative damage. Given these benefits, it is reasonable to consider supplementation with astaxanthin since it has a potential therapeutic effect against inflammation and cytokine storms in coronavirus patients [120,121].
3.9. Quercetin
Quercetin may reduce the likelihood of coronavirus patients being admitted to ICU, as has been shown in recent systematic reviews and meta-analyses. It also can lower hospitalization rates and potentially decrease mortality [122,123]. Quercetin, as an antioxidant, has also been known to possess antiviral and anti-inflammatory properties. According to studies, quercetin has been found to interfere with 85% of coronavirus proteins in human cells [124]. A study recently highlighted quercetin’s capability to block ACE2 receptors, thereby interfering with viral replication. Moreover, protease enzymes that play a crucial role in virus replication may be inhibited by Quercetin [125].
Flavonoid quercetin in PBD has been found to block the active site of 6LU7, the major protease in coronavirus. This will inhibit virus replication [126,127]. In addition to its anti-inflammatory and antioxidant effects, Quercetin exhibits a potent iron-chelating property, which helps decrease the severity of coronavirus symptoms. Due to these properties, we believe Quercetin can be a valuable therapeutic option for treating COVID-19 [128].
3.10. Curcumin
Curcumin is a natural polyphenolic compound with various benefits, such as anti-inflammatory, antiviral [129], cytoprotective, anticoagulant, and antiplatelet properties. It has been proven to help reduce the progression of several inflammatory diseases [130,131]. These effects have made Curcumin a potential treatment option for coronavirus patients. The pathophysiology of COVID-19 involves severe inflammatory reactions, coagulopathy, and the development of cytokine storms. The benefits of Curcumin can be due to its anti-inflammatory effects, such as inhibiting inflammasome formation. By binding to the primary protease (Mpro) enzyme of coronavirus, which is necessary for viral replication, Curcumin has been found to have antiviral effects. Additionally, Curcumin can effectively block viral attachment to entry into human cells [132]. According to modeling studies, ACE2 receptor and spike proteins are both inhibited by Curcumin, thus preventing virus-receptor interaction [133]. In a randomized trial, it was suggested that Curcumin could speed up the recovery of acute inflammatory immune response [134].
In coronavirus patients who received nano-curcumin, the mRNA expression of interleukin-6 and interleukin- 1ß was significantly decreased, which may reduce the systemic inflammatory reaction. Moreover, further trials showed a significant reduction in gene expression, the number of Th17 cells, and serum levels of Th17-mediated cytokines upon administering curcumin. These mechanisms may benefit coronavirus patients [135,136,137]. Systematic reviews and meta-analyses of randomized trials recently concluded that oral administration of Curcumin as a supplement in coronavirus patients could significantly decrease their death risk [138].
3.11. Taurine
Various studies suggest Taurine can act as an antioxidant, anti-inflammatory, and antiviral substance. Taurine may also help regulate vascular function. Its potential effects are wide-ranging, from stopping viral invasion through the AT1R-mediated coronavirus/ACE2 endocytosis pathway to reducing vascular injury and inflammation by affecting both inflammatory and coagulation pathways. Like other infections, COVID-19 decreases Taurine levels, which limits its protective properties under normal circumstances. It is hypothesized that early Taurine administration during COVID-19 onset can halt cytokine storms, reducing morbidity and mortality. Taurine seems to be a promising, supplementary option for coronavirus patients [139,140].
4. Healthy Lifestyles Their Significant Role in Managing the COVID-19 Pandemic
As we demonstrated, the significance of PBD and supplementations in managing coronavirus patients has been emphasized. In addition to following a balanced diet, everyone must adopt certain lifestyle practices to mitigate chronic inflammatory conditions and prevent severe coronavirus and its associated mortality. These practices include maintaining a healthy weight, engaging in regular physical activity, reducing stress, abstaining from harmful substances such as smoking and alcohol, ensuring adequate sleep, and fostering positive personal relationships.
To enhance the immune system, consuming 2-3 cups of coffee daily [141] and cabbage and fermented vegetables in one’s diet is recommended. Cabbage is rich in sulforaphane, a natural and potent Nrf2 activator. Fermented vegetables are abundant in lactobacilli, another potent Nrf2 activator with antioxidant properties, helping alleviate the severity of coronavirus infections [142].
During the COVID-19 pandemic, we recommended that our patients receive sun exposure. Research has demonstrated that sunlight exposure is associated with decreased mortality rates for COVID-19 patients, independent of its role in increasing vitamin D levels. It is believed that ultraviolet A and B radiation may promote the release of NO from the skin, which can benefit cardiovascular health and reduce the risk of coronavirus infection [143,144,145].
5. Conclusions
PBD has been associated with reduced COVID-19 incidence, severity, and mortality rates over time, as demonstrated by various studies [146,147,148,149,150,151,152,153]. However, in early 2024, some experts in the field, including Rayman M, Stewart G, Mellor D, and McCoway K, strongly reacted to a recent study published in BMJ Nutrition, Prevention & Health by Acosta-Navarro et al. Their study focused on the relationship between different types of diets and COVID-19 infection. The experts specifically highlighted the deficiency of essential nutrients, such as vitamins B12 and D, and minerals like iodine, iron, zinc, selenium, and calcium, in PBD interventions, which can be detrimental, particularly for pregnant individuals. The experts also drew attention to the ambiguous definition of PBD in the study, which did not consider factors such as the quality, quantity, and food preparation methods, as well as the loose definition of PBD encompassing ovo- and pesco-vegetarians. Since most of those studies used questionnaires, further research with a clear definition of PBD and adequate supplementation is needed to provide valuable insights and shed additional light on the subject, per the expert commentary.
In the context of those criticisms, our study has given considerable importance to the expert opinions regarding the inclusion of micronutrients in our coronavirus participant’s dietary supplements, including vitamin C, vitamin D, vitamin B3/NAD+, zinc, copper, selenium, and natural anti-inflammatory products such as astaxanthin, curcumin, quercetin, as well as CoQ10, taurine, and multivitamins (containing various small doses of minerals and vitamins as recommended for daily RDA). To the best of our knowledge, as of the writing of this paper, no previous PBD studies on COVID-19 have included the use of supplements. Our study aims not only to ensure the adequacy of supplementation but also to validate our hypothesis that dietary supplements can enhance the anti-inflammatory, immune regulatory, and antiviral properties of PBD in combating coronavirus. However, in recent years, experts (not PBD experts) have highlighted the importance of using supplements in managing the virus.
The critical distinction between our research and others is that we accounted carefully for variations in food quality, quantity, and preparation methods. Additionally, we closely monitored our participants’ dietary intake throughout their illness. These factors that distinguish our study from others in the field are paramount. When considering these elements, evaluating the disparities between our research outcomes and those of other studies is crucial, particularly the lack of disease progression, hospitalization, and mortality among our participants. Our study stands out due to these unique characteristics, which merit special attention.
Our research and theories have saved the lives of COVID-19 patients and improved and reversed their chronic diseases, enhancing their quality of life and extending their lifespan. Furthermore, our findings may offer protection against future pandemics, i.e., disease, X.; as the World Health Organization (WHO) has predicted.
Reviewing the historical record from the start of the 20th century, it is evident that a diet emphasizing PBD and adopting a healthier lifestyle has safeguarded numerous individuals from various pandemics [154,155]. Furthermore, our extensive knowledge of supplementation will enrich our understanding of how to combat COVID-19 and may also motivate us to prepare for future pandemics. Numerous studies have demonstrated the importance of PBD in managing COVID-19, and our research has contributed significant evidence to support this claim. Despite this, the medical community remains cautious and skeptical about the use of PBD in treating the virus. Till the writing of this article, the World Health Organization has not endorsed PBD or supplementation specifically in their guidelines for managing coronavirus. We hope that more research will be conducted to fully understand PBD and supplementation benefits in treating viral illnesses, leading to greater acceptance and adoption by the wide medical community.
Author Contributions
Conceptualization, D.M.; Writing-original draft, D.M.; Writing-review and editing, D.M., A.M.H., N.E.L., M.K.S., and H.U. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wang, P.; Song, M.; Eliassen, A.H.; Wang, M.; Fung, T.T.; Clinton, S.K.; Rimm, E.B.; Hu, F.B.; Willett, W.C.; Tabung, F.K.; Giovannucci, E.L. Optimal dietary patterns for prevention of chronic disease. Nat Med. Erratum in: Nat Med. 2024. 2023, 29, 719–728. [Google Scholar] [CrossRef] [PubMed]
- Peña-Jorquera, H.; Cid-Jofré, V.; Landaeta-Diaz, L.; et al. Plant-Based Nutrition: Exploring Health Benefits for Atherosclerosis, Chronic Diseases, and Metabolic Syndrome- A Comprehensive Review. Nutrients 2023, 15, 3244. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Rebholz, C.M.; Hedge, S.; et al. Plant-based diets, pescatarian diets and COVID-19 severity: a population-based case-control study in six countries. BMJ Nutrition, Prevention & Health. 2021, 4, e000272. [Google Scholar]
- Oboza, P.; Ogarek, N. The main causes of death in patients with COVID-19. Eur Rev Med Pharmacol Sci. 2023, 27, 2165–2172. [Google Scholar]
- Dessie, Z.G.; Zewotir, T. Mortality-related risk factors of COVID-19: a systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect Dis. 2021, 21, 855. [Google Scholar] [CrossRef]
- Gupta, S.C.; Prasad, S.; Aggarwal, BB. Anti-inflammatory Nutraceuticals and Chronic Diseases. Advances in Experimental Medicine and Biology. 2016. [CrossRef]
- Chojnacka, K.; Skrzypczak, D.; Izydorczyk, G.; et al. Antiviral Properties of Polyphenols from Plants. Foods. 2021, 10, 2277. [Google Scholar] [CrossRef] [PubMed]
- Alesci, A.; Aragona, M.; Cicero, N.; et al. Can nutraceuticals assist treatment and improve covid-19 symptoms? Natural Product Research. [CrossRef]
- Alam, S.; Sarker, M.R.; Afrin, S. Traditional Herbal Medicines, Bioactive Metabolites, and Plant Products Against COVID-19: Update on Clinical Trials and Mechanism of Actions. Frontiers in Pharmacology 2021, 12, 671498. [Google Scholar] [CrossRef]
- Loscalzo, J.; Welch, G. Nitric Oxide and its role in cardiovascular system. Prog Cardiovasc Dis. 1995, 38, 87–104. [Google Scholar] [CrossRef]
- Cannon, R.O. , 3rd. Role of nitric oxide in cardiovascular disease: focus on the endothelium. Clin Chem. 1998, 44, 1809–1819. [Google Scholar] [CrossRef]
- Torregrossa, A.C.; Aranke, M.; Bryan, NS. Nitric Oxide and geriatrics: Implications in diagnostics and treatment of the elderly. J Geriatr Cardiol. 2011, 8, 230–242. [Google Scholar] [PubMed]
- Nikolaidis, A.; Kramer, R.; Ostojic, S. Nitric Oxide: The Missing Factor in COVID-19 Severity? Med Sci (Basel). 2022, 10, 3. [Google Scholar] [CrossRef] [PubMed]
- Flaxman, S.; Whittaker, C.; Semenova, E.; et al. Assessment of COVID-19 as the Underlying Cause of Death Among Children and Young People Aged 0 to 19 Years in the US. JAMA Netw Open. 2023, 6, e2253590. [Google Scholar] [CrossRef] [PubMed]
- Babateen, A.; Shannon, O.; Mathers, J.C.; et al. Validity and reliability of test strips for the measurement of salivary nitrite concentration with and without the use of mouthwash in healthy adults. Nitric Oxide. 2019, 91. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, J.; Ohtake, K.; Uchida, H. NO-Rich Diet for Lifestyle-Related Diseases. Nutrients. 2015, 7, 4911–4937. [Google Scholar] [CrossRef] [PubMed]
- Rajendran, S.; Shen, X.; Glawe, J.D.; et al. Nitric Oxide and Hydrogen Sulfide Regulation of Ischemic Vascular Growth and Remodeling. Chapter in Comprehensive Physiology. 3337. [Google Scholar]
- Fang, W.; Jiang, J.; Su, L.; et al. The role of NO in COVID-19 and potential therapeutic strategies. Free Radical Biology and Medicine. 2021, 163, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Ritz, T.; Trueba, A.F.; Vogel, P.D.; et al. Exhaled nitric oxide and vascular endothelial growth factor as predictors of cold symptoms after stress. Biol Psychol. 2018, 132, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, J.S.; Aldhahir, A.M.; Al Ghamdi, S.S.; et al. Inhaled Nitric Oxide for Clinical Management of COVID-19: A Systematic Review and Meta-Analysis. Int J Environ Public Health. 2022, 19, 12803. [Google Scholar] [CrossRef]
- Mir, J.M.; Maurya, RC. Nitric oxide as a therapeutic option for COVID-19 treatment: a concise perspective. New J Chem. 2021, 45, 1774. [Google Scholar] [CrossRef]
- Wiertsema, S.P.; van Bergenhenegouwen, J.; Garssen, J.; et al. The Interplay between the Gut Microbiome and the Immune System in the Context of Infectious Diseases throughout Life and the Role of Nutrition in Optimizing Treatment Strategies. Nutrients. 2021, 13, 886. [Google Scholar] [CrossRef]
- Dumas, A.; Bernard, J.; Poquet, Y.; et al. The role of the lung microbiota and the gut-lung axis in respiratory infectious diseases. Cell Microbiol. 2018, 20, e12966. [Google Scholar] [CrossRef] [PubMed]
- Vijay, A.; Valdes, AM. Role of the gut microbiome in chronic diseases: a narrative review. European Journal of Clinical Nutrition. 2022, 76, 489–501. [Google Scholar] [CrossRef] [PubMed]
- Vignesh, R.; Swathirajan, C.R. ; Tun Z-H, et al. Could Perturbation of Gut Microbiota Possibly Exacerbate the Severity of COVID-19 via Cytokine Storm? Frontiers in Immunology. 2021, 11, 607734. [Google Scholar]
- Budden, K.F.; Gellatly, S.L.; Wood, D.L.A.; et al. Emerging pathogenic links between microbiota and the gut-lung axis. Nat Rev Microbiol. 2017, 15, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Dang, A.t.; Marsland, B.J. Microbes, metabolites, and gut-lung axis. Mucosal Immunol. 2019, 12, 843–50. [Google Scholar] [CrossRef] [PubMed]
- Ramatillah, D.L.; Gan, S.-H.; Pratiwi, I. ; et al. Impact of cytokine storm on severity of COVID-19 disease in a private hospital in West Jakarta prior to vaccination. PloS One. 2022, 17, e0262438. [Google Scholar] [CrossRef] [PubMed]
- Du, R.-H.; Liang, L.-R.; Yang, C.-Q.; et al. Predictors of mortality for patients with COVID-19 pneumonia caused by SARS-CoV-2: a prospective cohort study. Eur Respir J. 2020, 56, 3. [Google Scholar] [CrossRef] [PubMed]
- Groves, H.T.; Higham, S.L.; Moffatt, M.F.; et al. Respiratory Viral Infection Alters the Gut Microbiota by Inducing Inappetence. mBio. 2020, 11, 1. [Google Scholar] [CrossRef]
- Gou, W.; Fu, Y.; Yue, L.; et al. Gut microbiota may underlie the predisposition of healthy individuals to COVID-19. MedRxiv. 2020, 22, 20076091. [Google Scholar]
- Vignesh, R.; Swathirajan, C.R.; Tun, Z.-H.; et al. Could Perturbation of Gut Microbiota Possibly Exacerbate the Severity of COVID-19 via Cytokine Storm? Frontiers in Immunology. 2021, 11, 607734. [Google Scholar] [CrossRef]
- Abadi, M.S.S.; Kodashahi, R.; Aliakbarian, M.; et al. The Association Between the Gut Microbiome and COVID-19 Severity: The Potential Role of TMAO Produced by the Gut Microbiome. Archives of Clinical Infectious Diseases. 2024, 18, e140346. [Google Scholar]
- Foster, J.A.; Baker, G.B.; Dursun, SM. The Relationship Between the Gut Microbiome- Immune System-Brain Axis and Major Depressive Disorder. Front Neurol. 2021, 12, 721126. [Google Scholar] [CrossRef] [PubMed]
- Kamo, T.; Akazawa, H.; Suda, W.; et al. Dysbiosis and compositional alterations with aging in the gut microbiota of patients with heart failure. PloS One. 2017, 12, e0174099. [Google Scholar] [CrossRef] [PubMed]
- Leeming, E.R.; Johnson, A.J.; Spector, T.D.; et al. Effect of Diet on the Gut Microbiota: Rethinking Intervention Duration. Nutrients. 2019, 11, 2862. [Google Scholar] [CrossRef] [PubMed]
- Craddock, J.C.; Neale, E.P.; Peoples, G.E.; et al. Vegetarian-Based Dietary Patterns and their Relation with Inflammatory and Immune Biomarkers: A Systematic Review and Meta-Analysis. Advances in Nutrition. 2019, 10, 433–451. [Google Scholar] [CrossRef] [PubMed]
- Sidhu, S.R.K.; Kok, C.-W.; Kunasegaran, T. ; et al. Effect of Plant-Based Diets on Gut Microbiota: A Systematic Review of Interventional Studies. Nutrients. 2023, 15, 1510. [Google Scholar] [CrossRef] [PubMed]
- Hibino, S.; Hayashida, K. Modifiable Host Factors for the Prevention and Treatment of COVID-19: Diet and Lifestyle/ Diet and Lifestyle Factors in the Prevention of COVID-19. Nutrients. 2022, 14, 1876. [Google Scholar] [CrossRef] [PubMed]
- Dovignoan, J.; Ganz, P. Role of Endothelial Dysfunction in Atherosclerosis. Circulation. 2004, 109, III–27. [Google Scholar] [CrossRef] [PubMed]
- Akinrinmade, A.O.; Obitulata-Uqwu, V.O.; Obijiofor, N.B.; et al. COVID-19 and Acute Coronary Syndrome: A Literature Review. Cureus. 2022, 14, e29747. [Google Scholar] [CrossRef]
- Margina, D.; Ungurianu, A.; Purdel, C.; et al. Chronic Inflammation in the Context of Everyday Life: Dietary Changes as Mitigating Factors. Int J Environ Res Public Health. 2020, 17, 4135. [Google Scholar] [CrossRef]
- Hojyo, S.; Uchida, M.; Tanaka, K.; et al. How COVID-19 induces cytokine storm with high mortality. Inflamm Regen. 2020, 40, 37. [Google Scholar] [CrossRef]
- Moludi, J.; Qaisar, S.A.; Alizadeh, M.; et al. The relationship between Dietary Inflammatory Index and disease severity and inflammatory status: a case-control study of COVID-19 patients. British Journal of Nutrition. 2021, 1–9. [Google Scholar] [CrossRef]
- Zhao, L.; Wirth, M.D.; Petermann-Rocha, F.; et al. Diet-Related Inflammation Is Associated with Worse COVID-19 Outcomes in the UK Biobank Cohort. Nutrients. 2023, 15, 884. [Google Scholar] [CrossRef] [PubMed]
- Paraiso, I.L.; Revel, J.S.; Stevens, JF. Potential use of polyphenols in the battle against COVID-Current Opinion in Food. Science. 2020, 32, 149–155. [Google Scholar]
- Wang, Y.; Uffelman, C.; Hill, E. The Effects of Red Meat Intake on Inflammation Biomarkers in Humans: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Curr Dev Nutr. 2022, 6 (Suppl. S1), 994. [Google Scholar] [CrossRef]
- Hofseth, L.J.; Hébert, J.R. Chapter 3- Diet and acute and chronic, systemic, low-grade inflammation. Diet, Inflammation, and Health. 2022; 85–111. [Google Scholar]
- Buck, A.N.; Vincent, H.K.; Newman, CB. Evidence-Based Dietary Practices to Improve Osteoarthritis Symptoms: An Umbrella Review. Nutrients. 2023, 15, 3050. [Google Scholar] [CrossRef] [PubMed]
- Gain, C.; Song, S.; Angtuaco, T.; et al. The role of oxidative stress in the pathogenesis of infections with coronavirus. Frontiers in Microbiology. [CrossRef]
- Li, M.; Zhu, D.; Yang, J.; et al. Clinical treatment experience in severe and critical COVID-19. Mediat Inflamm. 2021, 9924542. [Google Scholar] [CrossRef] [PubMed]
- Alam, M.S.; Czajkowsky, DM. SARS-CoV-2 infection and oxidative stress: pathophysiology insight into thrombosis and therapeutic opportunities. Cytokine Growth Factor Rev. 2022, 63, 44–57. [Google Scholar] [CrossRef] [PubMed]
- Gorni, D.; Finco, A. Oxidative stress in elderly population: A prevention screening study. Aging medicine. 2020, 3, 205–213. [Google Scholar] [CrossRef]
- Al-Zahrani, J. SARS-CoV-2 associated COVID-19 in geriatric population: A brief narrative review. Saudi Journal of Biological Sciences. 2021, 28, 738–743. [Google Scholar] [CrossRef]
- Macho-Gonzáles, A.; Garcimartín, A.; López-Oliva, M.E.; et al. Can Meat and Meat-Products Induce Oxidative Stress? Antioxidants. 2020, 9, 638. [Google Scholar] [CrossRef] [PubMed]
- Macho-Gonzáles, A.; Bastida, S.; Garcimartín, A.; et al. Functional Meat Products as Oxidative Stress Modulators: A Review. Advances in Nutrition. 2021, 12, 1514–1539. [Google Scholar] [CrossRef] [PubMed]
- Aleksandrova, K.; Koelman, L.; Rodrigues, CE. Dietary patterns and biomarkers of oxidative stress and inflammation: A systematic review of observational and intervention studies. Redox Biology. 2021, 42, 101869. [Google Scholar] [CrossRef] [PubMed]
- Baghaei-Yazdi, N.; Bahmaie, M.; Abhari, FM. The Role of plant-derived natural antioxidants in reduction of oxidative stress. BioFactors. 2022, 1–23. [Google Scholar]
- Marchi, S.; Guilbaud, E.; Galluzzi, L. Mitochondrial control of inflammation. Nature Reviews Immunology. 2023, 23, 159–173. [Google Scholar] [CrossRef] [PubMed]
- Ciccarelli, G.; Conte, S.; Cimmino, G.; et al. Mitochondrial Dysfunction: The Hidden Player in the Pathogenesis of Atherosclerosis? Int J Mol Sci. 2023, 24, 1086. [Google Scholar] [CrossRef] [PubMed]
- Shoraka, S.; Samarasinghe, A.E.; Ghaemi, A.; et al. Host mitochondria: more than an organelle in SARS-CoV-2 infection. Frontiers in Cellular and Infection Microbiology. [CrossRef]
- Junqueira, C.; Crespo, A.; Lieberman, J.; et al. FcyR-mediated SARS-CoV-2 infection of monocytes activates inflammation. Nature. 2022, 606, 576–584. [Google Scholar] [CrossRef]
- Khalil, M.; Shanmugam, H.; Abdallah, H.; et al. The Potential of the Mediterranean Diet to Improve Mitochondrial Function in Experimental Models of Obesity and Metabolic Syndrome. Nutrients. 2022, 14, 3112. [Google Scholar] [CrossRef] [PubMed]
- Pollicino, F.; Veronese, N.; Dominguez, L.; et al. Mediterranean diet and mitochondria: New findings. Experimental Gerontology. 2023, 176, 112165. [Google Scholar] [CrossRef]
- Kyriazis, I.D.; Vassi, E.; Alvanou, M.; et al. The impact of diet upon mitochondrial physiology (Review). International Journal of Molecular Medicine. 2022, 50, 135. [Google Scholar] [CrossRef]
- Ahmad, F.B.; Cisewski, J.A.; Miniño, A.; et al. Provisional Mortality Data- United States. MMWR Morb Mortal Wkly Rep. 2021, 70, 519–522. [Google Scholar] [CrossRef]
- Stokes, E.K.; Zambrano, L.D.; Anderson, K.N.; et al. Coronavirus Disease 2019 Case Surveillance—United States, January 22-May 30. MMWR Morb Mortal Wkly Rep. 2020, 69, 759–765. [Google Scholar] [CrossRef]
- Wang, Q.; Zhan, Y.; Pederson, N.L.; et al. Telomere length and all-cause mortality: a meta-analysis. Ageing Res Rev. 2018, 48, 11–20. [Google Scholar] [CrossRef]
- Sanchez-Vazquez, R.; Guío-Carrión, A.; Zapatero-Gaviria, A.; et al. Shorter telomere lengths in patients with severe COVID-19 disease. Aging (Albany NY). 2021, 13, 1–15. [Google Scholar] [CrossRef]
- Mahmoodpoor, A.; Sanale, S.; Eskandari, M.; et al. Association between leucocyte telomere length and COVID-19 severity. Egypt J Med Hum Genet. 2023, 24, 37. [Google Scholar] [CrossRef]
- Retuerto, M.; Liedó, A.; Fernandez-Varas, B.; et al. Shorter telomere length is associated with COVID-19 hospitalization and with persistence of radiographic lung abnormalities. Immunity & Ageing. 2022, 19, 38. [Google Scholar]
- Arantes dos Santos, G.; Pimenta, R.; Viana, N.I.; et al. Shorter leukocyte telomere length is associated with severity of COVID-19 infection. Biochemistry and Biophysics Reports. 2021, 27, 101056. [Google Scholar] [CrossRef]
- Aviv, A. The bullwhip effect, T-cell telomeres, and SARS-CoV-2. Lancet. 2022, 3, E715–E721. [Google Scholar] [CrossRef]
- Sepe, S.; Rossiello, F.; Cancila, V.; et al. DNA damage response at telomeres boosts the transcription of SARS-CoV-2 receptor ACE2 during aging. EMBO rep. 2022, 23, e53658. [Google Scholar] [CrossRef]
- Liu, S.; Nong, W.; Ji, L.; et al. The regulatory feedback of inflammatory signaling and telomere/telomerase complex dysfunction in chronic inflammatory disease. Experimental Gerontology. 2023, 174, 112132. [Google Scholar] [CrossRef]
- Crous-Bou, M.; Molinuevo, J.-L.; Sala-Vila, A. Plant-Rich Dietary Patterns, Plant Foods and Nutrients, and Telomere Length. Adv Nutr. 2019, 10 (Suppl. S4), S286–S303. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, S. Diet and Aging: The Role of Polyphenol-Rich Diets in Slow Down the Shortening of Telomeres: A Review. Antioxidants 2023, 12, 2086. [Google Scholar] [CrossRef] [PubMed]
- Blackburn, E.; Epel, E. The Telomere Effect: A Revolutionary Approach to Living Younger, Healthier, Longer. Grand Central Publishing. 2017.
- Kökten, T.; Hansmannel, F.; Ndiaye, N.C.; et al. Calorie Restriction as a New Treatment of Inflammatory Diseases. Adv Nutr. 2021, 12, 1558–1570. [Google Scholar] [CrossRef] [PubMed]
- Gnoni, M.; Beas, R.; Vásques-Garagatti. Is there any role of intermittent fasting in the prevention and improving clinical outcomes of COVID-19?: intersection between inflammation, mTOR pathway, autophagy and caloric restriction. VirusDis. 2021, 32, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Martin Bagos, J.P.; Erick, M.; Matawaran, B. Predictors of Poor Glycemic Control and Increased Glucose Variability Among Admitted Moderate to Critical COVID-19 Patients with Type 2 Diabetes Mellitus: A Single Center Cross-sectional Study. J ASEAN Fed Endocr Soc. 2023, 38, 57–64. [Google Scholar] [CrossRef] [PubMed]
- Sultan, K.; Kal, S.; Issagholian, L.; et al. The Effect of Glycemic Control on Morbidity and Mortality in Critically Ill COVID-19 Patients. Cureus 2023, 15, e47991. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Carretero, R.; Vazquez-Gomez, O.; Lopez-Lomba, M.; Gil-Prieto, R.; Gil-de-Miguel, A. Insulin Resistance and Metabolic Syndrome as Risk Factors for Hospitalization in Patients with COVID-19: Pilot Study on the Use of Machine Learning. Metab Syndr Relat Disord. 2023, 21, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Alvarado, M.; Campos-Campos, L.; Guerrero-Romero, F.; et al. The Triglycerides and Glucose Index Is an Independent Risk Factor for Acute Respiratory Distress Syndrome in Patients with Covid-Metab Syndr Relat Disord. [CrossRef]
- Horne, B.D.; May, H.T.; Muhlestein, J.B.; et al. Association of periodic fasting with lower severity of COVID-19 outcomes in the SARS-CoV-2 prevaccine era: an observational cohort from the INSPIRE registry. BMJ Nutrition, Prevention & Health. 2022, 0, eooo462. [CrossRef]
- U.S. Department of Agriculture, Agriculture Research Service, Scientific Report of the 2020 Dietary Guideline Advisory Committee: Advisory Report to the Secretary of Agriculture and the Secretary of Health and Human Services, Published Accessed March 18, 2023. https://www.dietaryguidelines.gov/2020-advisory-committee-report.
- Cheng, R.Z. Can early and high intravenous dose of vitamin C prevent and treat coronavirus disease 2019 (COVID_19)? Med Drug Discov. 2020, 5, 100028. [Google Scholar] [CrossRef]
- Chen, L.; Hu, C.; Hood, M.; et al. A novel combination of vitamin, C.; curcumin and glycyrrhizin acid potentially regulates immune and inflammatory response associated with coronavirus infections: a perspective from system biology analysis. Nutrients. 2020, 12, 1193. [Google Scholar] [CrossRef]
- Marik, P.E.; Khangoora, V.; Rivera, R.; et al. Hydrocortisone, vitamin, C.; and thiamine for the treatment of severe sepsis and septic shock: a retrospective before-after study. Chest. 2017, 151, 1229–1238. [Google Scholar] [CrossRef]
- Kow, S.-K.; Hasan, S.S.; Ramachandram, D.S. The effect of vitamin C on the risk of mortality in patients with COVID-19: a systematic review and meta-analysis of randomized controlled trials. Inflammopharmacology. 2023, 18, 1–6. [Google Scholar] [CrossRef]
- Olczak-Pruc, M.; Swieczkowski, D.; Ladny, J.R.; et al. Vitamin C Supplementation for the Treatment of COVID-19: A Systematic Review and Meta-Analysis. Nutrients. 2022, 14, 4217. [Google Scholar] [CrossRef]
- Fisher, S.A.; Rahimzadeh, M.; Brierley, C.; et al. The role of vitamin D in increasing circulating T regulatory cell numbers and modulating T regulatory cell phenotypes in patients with inflammatory disease or in healthy volunteers: A systematic review. PloS One. 2019, 14, e0222313. [Google Scholar] [CrossRef]
- Gönen, M.S.; Alaylıoğlu, M.; Durcan, E.; Özdemir, Y.; Şahin, S.; Konukoğlu, D.; Nohut, O.K.; Ürkmez, S.; Küçükece, B.; Balkan, İ.İ.; et al. Rapid and Effective Vitamin D Supplementation May Present Better Clinical Outcomes in COVID-19 (SARS-CoV-2) Patients by Altering Serum INOS1, IL1B, IFNg, Cathelicidin-LL37, and ICAM1. Nutrients 2021, 13, 4047. [Google Scholar] [CrossRef]
- Giannis, D.; Ziogas, I.A.; Gianni, P. Coagulation disorders in coronavirus infected patients: COVID-19, SARS-CoV-1, MERS-CoV and lessons from the past. J Clin Virol. 2020, 127, 104362. [Google Scholar] [CrossRef]
- Mohammad, S.; Mishra, A.; Ashraf, MZ. Emerging role of Vitamin D and its associated molecules in pathways related to pathogenesis of thrombosis. Biomolecules. 2019, 9, 649. [Google Scholar] [CrossRef]
- Weir, E.K.; Thenappan, T.; Bhargaya, M.; et al. Does vitamin D deficiency increase the severity of COVID-19? Clin Med (Lond). 2020, 20, e107–e108. [Google Scholar] [CrossRef]
- D’Ecclesiis, O.; Gavioli, C.; Martinoli, C.; et al. Vitamin D and SARS Cov-2 infection, severity and mortality: A systematic review and meta-analysis. PLoS One. 2022, 17, e0268396. [Google Scholar] [CrossRef]
- Meng, J.; Li, X.; Lie, W.; et al. The role of vitamin D in the prevention and treatment of SARS-CoV-2 infection: A meta-analysis of randomized controlled trials. Clinical Nutrition. 2023, 42, 2198–2206. [Google Scholar] [CrossRef]
- Sartini, M.; Del Puente, F.; Oliva, M.; Carbone, A.; Bobbio, N.; Schinca, E.; Giribone, L.; Cristina, M.L. Preventive Vitamin D Supplementation and Risk for COVID-19 Infection: A Systematic Review and Meta-Analysis. Nutrients 2024, 16, 679. [Google Scholar] [CrossRef]
- Bogan, K.L.; Brenner, C. Nicotinic acid, nicotinamide, and nicotinamide riboside: a molecular evaluation of NAD+ precursor vitamins in human nutrition. Annu Rev Nutr. 2008, 28, 115–130. [Google Scholar] [CrossRef]
- Zheng, M.; Schultz, M.B.; Sinclair, DA. NAD+ in COVID-19 and viral infections. Trends in Immunology. 2022, 43, 283–295. [Google Scholar] [CrossRef]
- Bogan-Brown, K.; Nkrumah-Elie, Y.; Ishtiaq, Y.; et al. Potential Efficacy of Nutrient Supplements for Treatment of Prevention of COVID-19. Journal of Dietary Supplements. 2022, 19, 336–365. [Google Scholar] [CrossRef]
- Abdellatif, M.; Bugger, H.; Kroemer, G.; et al. NAD+ and Vascular Dysfunction: From Mechanisms to Therapeutic Opportunities. J Lipid Atheroscler. 2022, 11, 111–132. [Google Scholar] [CrossRef]
- Abdallah, S.B.; Mhalla, Y.; Trabelsi, I.; et al. Twice-Daily Oral Zinc in the treatment of Patients With Coronavirus Disease 2019: A Randomized Doble- Blind Controlled Trial. Clin Infect Dis. 2023, 76, 185–191. [Google Scholar] [CrossRef]
- Olczak-Pruc, M.; Szarpak, L.; Navolokina, A.; et al. The effect of zinc supplementation on the course of COVID-19- A systematic review and meta-analysis. Ann Agric Environ Med. 2022, 29, 568–574. [Google Scholar] [CrossRef]
- Francis, Z.; Book, G.; Litvin, C.; et al. The COVID-19 Pandemic and Zinc-Induced Copper Deficiency: An Important Link. Am J Med. 2022, 135, e290–e291. [Google Scholar] [CrossRef]
- Raha, S.; Mallick, R.; Basak, S.; et al. Is copper beneficial for COVID-19 patients? Med Hypotheses. 2020, 142, 109814. [Google Scholar] [CrossRef] [PubMed]
- Fakhrolmobasheri, M.; Mazaheri-Tehrani, S.; Kieliszek, M.; et al. COVID-19 and Selenium Deficiency: a Systematic Review. Biol Trace Elem Res. 2022, 200, 3945–3956. [Google Scholar] [CrossRef] [PubMed]
- Gröber, U.; Holick, MF. The coronavirus disease (COVID-19)- a supportive approach with selected micronutrients. Int J Vitam Nutr Res Int Z Vitam. Ernahrungsforschung J Int Vitaminol Nutr.
- Gullin, O.M.; Vindry, C.; Ohlmann, T.; et al. Selenium, selenoproteins and viral infection. Nutrients. 2019, 11, 2101. [Google Scholar] [CrossRef]
- Kieliszek, M.; Lipinski, B. Selenium supplementation in the prevention of coronavirus infection (COVID-19). Med Hypotheses. 2020, 143, 109878. [Google Scholar] [CrossRef]
- Dludia, P.V.; Nyambuya, T.M.; Orlando, P.; et al. The impact of coenzyme Q10 on metabolic and cardiovascular disease profiles in diabetic patients: A systematic review and meta-analysis of randomized controlled trials. Endocrinol Diabetes Metab. 2020, 3, e00118. [Google Scholar] [CrossRef]
- Alarcón-Vieco, E.; Martínez-García, I.; Sequí-Domínguez, I.; et al. Effect of coenzyme Q10 on cardiac function and survival in heart failure: an overview of systematic reviews and meta-analyses. Food Funct. 2023, 14, 6302–6311. [Google Scholar] [CrossRef]
- Jorat, M.V.; Tabrizi, R.; Kolahdooz, F.; et al. The effects of coenzyme Q10 supplementation on biomarkers of inflammation and oxidative stress in among coronary artery disease: a systematic review and meta-analysis of randomized controlled trials. Inflammopharmacology. 2019, 27, 233–248. [Google Scholar] [CrossRef]
- Sue-Ling, C.B.; Abel, W.M.; Sue-Ling, K. Coenzyme Q10 as adjunctive Therapy for Cardiovascular Disease and Hypertension: A Systematic Review. The Journal of Nutrition. 2022, 152, 1666–1674. [Google Scholar] [CrossRef]
- Hargreaves, I.R.; Mantle, D. COVID-19, Coenzyme Q10, and Selenium. Adv Exp Med Biol. 2021, 168, 1327161. [Google Scholar]
- Varnousfaderani, S.D.; Musazadeh, V.; Ghalichi, F.; et al. Alleviating effects of coenzyme Q10 supplements on biomarkers of inflammation and oxidative stress: result from an umbrella meta-analysis. Frontiers in Pharmacology. 2023, 14, 1191290. [Google Scholar] [CrossRef]
- Sumbalova, Z.; Kucharská, J.; Rausová, Z.; et al. Reduced platelet mitochondrial respiration and oxidative phosphorylation in patients with pst COVID-19 syndrome are regenerated after spa rehabilitation and targeted ubiquinol therapy. Front Mol Biosci. [CrossRef]
- Ma, B.; Lu, J.; Kang, T.; et al. Astaxanthin supplementation mildly reduced oxidative stress and inflammation biomarkers: a systematic review and meta-analysis of randomized controlled trials. Nutrition Research. 2022, 99, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Talukdar, J.; Bhadra, B.; Dattaroy, T.; et al. Potential of natural astaxanthin in alleviating the risk of cytokine storm in COVID-19. Biomed Pharmacother. 2020, 132, 110886. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi A-R, Ayazi-Nasrabadi R. Astaxanthin protective barrier and its ability to improve the health in patients with COVID-19. Iran J Microbiol. 2021, 13, 434–441.
- Cheema, H.A.; Sohail, A.; Fatima, A.; et al. Quercetin for the treatment of COVID-19 patients: A systematic review and meta-analysis. Reviews in Medical Virology. 2023, 33, e2427. [Google Scholar] [CrossRef]
- Ziaei, S.; Alimohammadi-Kamalabadi, M.; Hasani, M.; et al. The effect of quercetin supplementation on clinical outcomes in COVID-19 patients: A systematic review and meta-analysis. Food Science & Nutrition. 2023, 11, 7504–7514. [Google Scholar]
- Mrityunjaya, M.; Pavithra, V.; Neelam, R.; et al. Immune-boosting, antioxidant and anti-inflammatory food supplements targeting pathogenesis of COVID-19. Front Immunol. 2020, 11, 570122. [Google Scholar] [CrossRef]
- Smith, M.; Smith, JC. Repurposing therapeutics for COVID-19: supercomputer-based docking to the SARS-CoV-2 viral spike protein and viral spike protein-human ACE2 interface. [CrossRef]
- Khaerunnisa, S.; Kurniawan, H.; Awaluddin, R.; et al. Potential inhibitor of COVID-19 main protease (Mpro) from several medicinal plant compounds by molecular docking study. [CrossRef]
- Derosa, G.; Maffioli, P.; D’Angelo, A.; et al. A role for quercetin in coronavirus disease 2019 (COVID-19). Phytother Res. 2021, 35, 1230–1236. [Google Scholar] [CrossRef]
- Lammi, C.; Arnoldi, A. Food-derived antioxidants and COVID-19. J Food Biochem. 2021, 45, 1–6. [Google Scholar] [CrossRef]
- Hassaniazad, M.; Eftekhar, E.; Inchehsablagh, B.R.; et al. A triple-blind, placebo-controlled, randomized clinical trial to evaluate the effect of curcumin-containing nanomicelles on cellular immune responses subtypes and clinical outcome in COVID-19 patients. Phytotherapy Research. 2021, 35, 6417–6427. [Google Scholar] [CrossRef]
- Sadeghi, M.; Dehnavi, S.; Asadirad, A.; et al. Curcumin and chemokines: mechanism of action and therapeutic potential in inflammatory diseases. Inflammopharmacology. 2023, 31, 1069–1093. [Google Scholar] [CrossRef]
- Rattis, B.; Ramos, S.G.; Celles, M. Curcumin as a potential treatment for COVID-19. Frontiers in Pharmacology. 2021, 12, 675287. [Google Scholar] [CrossRef] [PubMed]
- Dourado, D.; Freire, D.T.; Pereira, D.T.; et al. Will curcumin nanosystems be the next promising antiviral alternatives in COVID-19 treatment trials? Biomedicine & Pharmacotherapy. 2021, 139, 111578. [Google Scholar]
- Manoharan, Y.; Haidas, V.; Vasanthakumar, K.C.; et al. Curcumin: A wonder drug as a preventive measure for COVID-19 management. Indian Journal of Clinical Biochemistry. 2020, 35, 373–375. [Google Scholar] [CrossRef]
- Hassaniazad, M.; Eftekhar, E.; Inchehsablagh, B.R.; et al. A triple-blind, placebo-controlled, randomized clinical trial to evaluate the effect of curcumin-containing nanomicelles on cellular immune responses subtypes and clinical outcome in COVID-19 patients. Phytotherapy Research. 2021, 35, 6417–6427. [Google Scholar] [CrossRef]
- Valizadeh, H.; Abdolmohammadi-Vahid, S.; Danshina, S.; et al. Nano-curcumin therapy, a promising method in modulating inflammatory cytokines in COVID-19 patients. International Immunopharmacology. 2020, 89, 101088. [Google Scholar] [CrossRef]
- Tahmasebi, S.; El-Esawi, M.A.; Mahmoud, Z.H.; et al. Immunomodulatory effects of nanocurcumin on Th17 cell responses in mild and severe COVID-19 patients. Journal of Cellular Physiology. 2021, 236, 5325–5338. [Google Scholar] [CrossRef]
- Chia, S.-K.; Ramachandram, D.S.; Hasan, S. S.; Hasan S. The effect of curcumin on the risk of mortality in patients with COVID-19: A systematic review and meta-analysis of randomized trials. Phytotherapy Research. 2022, 36, 3365–3368. [Google Scholar]
- Shafiee, A.; Athar, M.M.T.; Shahid, A.; et al. Curcumin for the treatment of COVID-19 patients: A meta-analysis of randomized controlled trials. Phytotherapy Research. 2023, 37, 1167–1175. [Google Scholar] [CrossRef]
- van Eijk, Larissa, E.; Offringa, et al. The Disease-Modifying Role of Taurine and Its Therapeutic Potential in Coronavirus Disease 2019 (COVID-19). Taurine 2. [CrossRef]
- Rubio-Casillas, A.; Gupta, R.C.; Redwan, E.M.; et al. Early taurine administration as a mean for halting the cytokine storm progression in COVID-19 patients. Explor Med. 2022, 3, 234–48. [Google Scholar] [CrossRef]
- Vu, T.T.; Rydland, K.J.; Achenbach, C.J.; Van Horn, L.; Cornelis, MC. Dietary Behaviors and Incident COVID-19 in the UK Biobank. Nutrients. 2021, 13, 2114. [Google Scholar] [CrossRef]
- Bousquet, J.; Anto, J.M.; Czarlewski, W.; Haahtela, T.; Fonseca, S.C.; Iaccarino, G.; Blain, H.; Vidal, A.; Sheikh, A.; Akdis, C.A.; et al. Cabbage and fermented vegetables: From death rate heterogeneity in countries to candidates for mitigation strategies of severe COVID-19. Allergy. 2021, 76, 735–750. [Google Scholar] [CrossRef]
- Gorman, S.; Weller, R. Investigating the Potential for Ultraviolet Light to Modulate Morbidity and Mortality From COVID-19: A Narrative Review and Update. Frontiers in Cardiovascular Medicine. 2020, 7. [Google Scholar] [CrossRef]
- Cherrie, M.; Clemens, T.; Colandrea, C.; Feng, Z.; Webb, D.J.; Weller, R.B.; Dibben, C. Ultraviolet A radiation and COVID-19 deaths in the USA with replication studies in England and Italy. Br J Dermatol. 2021, 185, 363–370. [Google Scholar] [CrossRef]
- Pelegrino, M.T.; Paganotti, A.; Seabra, A.B.; Weller, RB. Photochemistry of nitric oxide and S-nitrosothiols in human skin. Histochem Cell Biol. 2020, 153, 431–441. [Google Scholar] [CrossRef] [PubMed]
- Acosta-Navarro, J.C.; Dias, L.F.; Gomes de Gouveia, L.A.; et al. Vegetarian and plant-based diets associated with lower incidence of COVID-19. BMJ Nutrition, Prevention & Health, 0629. [Google Scholar]
- Soltanieh, S.; Salavatizadeh, M.; Ghazanfari, T.; et al. Plant-based diet and COVID-19 severity: results from a cross-sectional study. BMJ Nutrition, Prevention & Health, 0688. [Google Scholar]
- Kendrick, K.N.; Kim, H.; Rebholz, C.M.; et al. Plant-Base Diets and Risk of Hospitalization with Respiratory Infection: Results from the Atherosclerosis Risk in Communities (ARIC) Study. Nutrients. 2023, 15, 4265. [Google Scholar] [CrossRef] [PubMed]
- Kahleova, H.; Barnard, ND. Can a plant-based diet help mitigate COVID-19? European Journal of Clinical Nutrition. 2022, 76, 911–912. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-Z.; Sato, T.; Sakuraba, A. Worldwide association of lifestyle-related factors and COVID-19 mortality. Annals of Medicine. 2021, 53, 1528–1533. [Google Scholar]
- Storz, M.A. Lifestyle Adjustments in Long-COVID Management: Potential Benefits of Plant-Based Diets. Current Nutrition Reports. 2021, 10, 352–363. [Google Scholar] [CrossRef]
- Lange, K.W.; Nakamura, Y. Lifestyle factors in the prevention of COVID-19. Global Health Journal 2020, 4, 146–152. [Google Scholar] [CrossRef]
- Moreb, N.A.; Albandary, A.; Jaiswal, S.; Jaiswal, A.K. Fruits and Vegetables in the Management of Underlying Conditions for COVID-19 High-Risk Groups. Foods 2021, 10, 389. [Google Scholar] [CrossRef]
- Khaleova, H.; Barnard, ND. The Role of Nutrition in COVID-19: Taking a Lesson from the 1918 H1N1 Pandemic. SAGE. 2022. http://www.sagepub.com/journalsPermissions.nav.
- Rust, P.; Ekmekcioglu. The Role of Diet and Specific Nutrients during the COVID-19 Pandemic: What Have We Learned over the Last Three Years? International Journal of Environmental Research and Public Health. 2023, 20, 5400. [Google Scholar] [CrossRef]
Figure 1.
Illustration of a nitrate-rich diet metabolized into nitric oxide [17].
Figure 1.
Illustration of a nitrate-rich diet metabolized into nitric oxide [17].
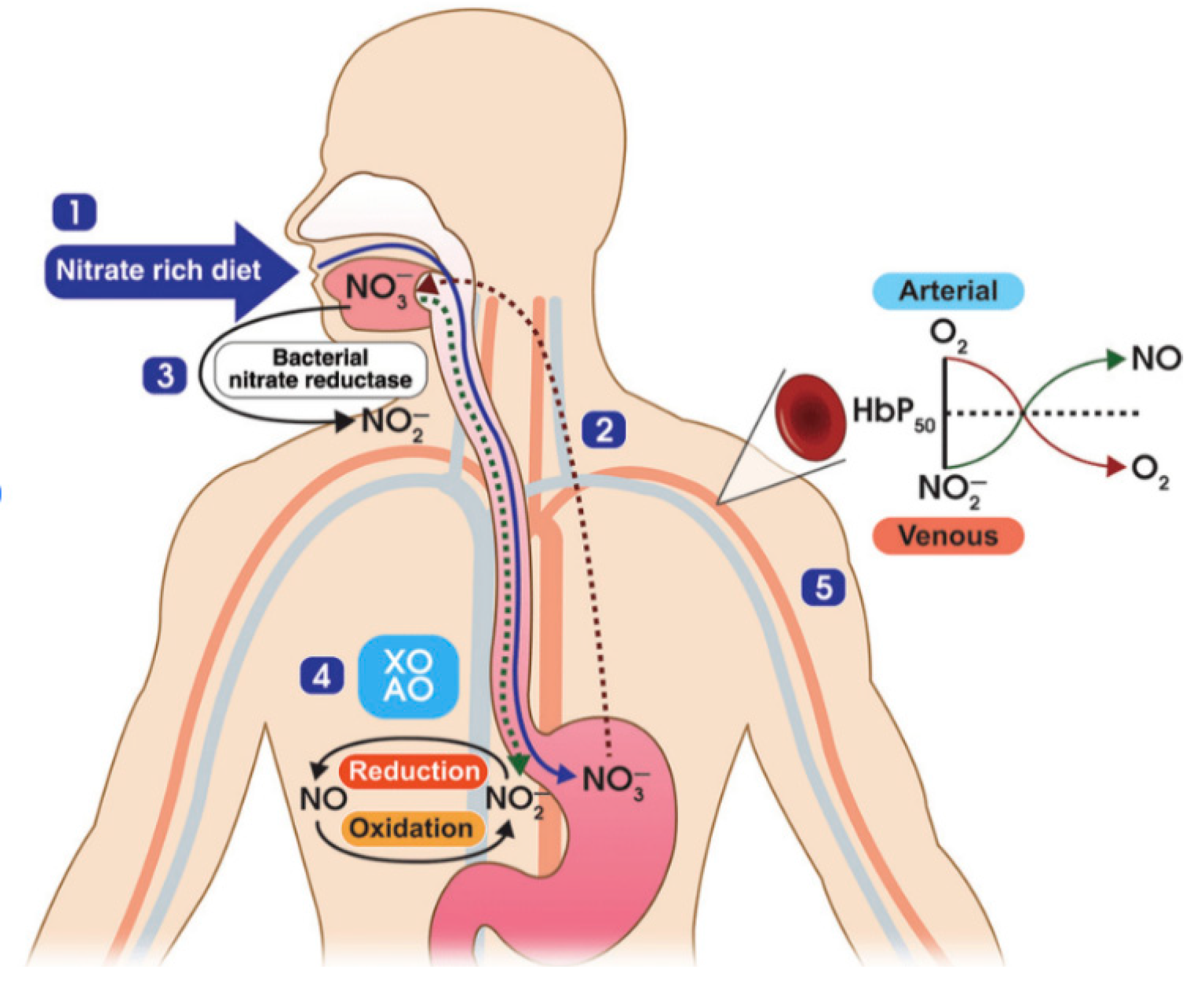
Figure 2.
Endothelial NO decreased by coronavirus-infected cells [18].
Figure 2.
Endothelial NO decreased by coronavirus-infected cells [18].
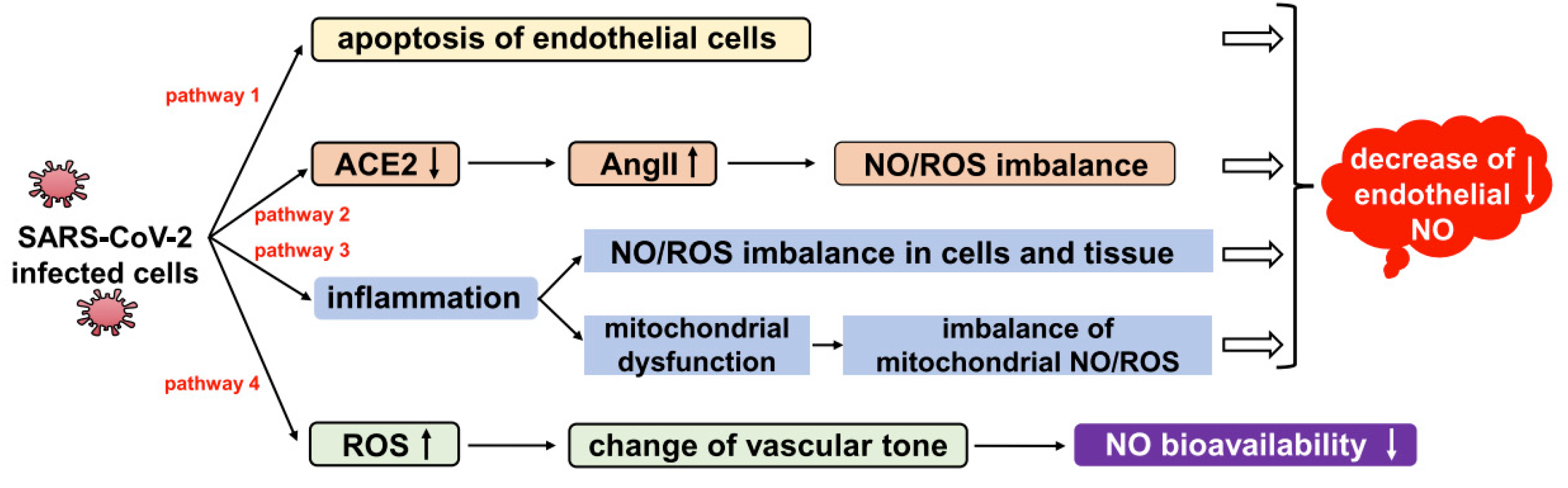
Figure 3.
NO as a vasodilator, bronchodilator, anticoagulation, anti-inflammatory, and anti-viral [18].
Figure 3.
NO as a vasodilator, bronchodilator, anticoagulation, anti-inflammatory, and anti-viral [18].
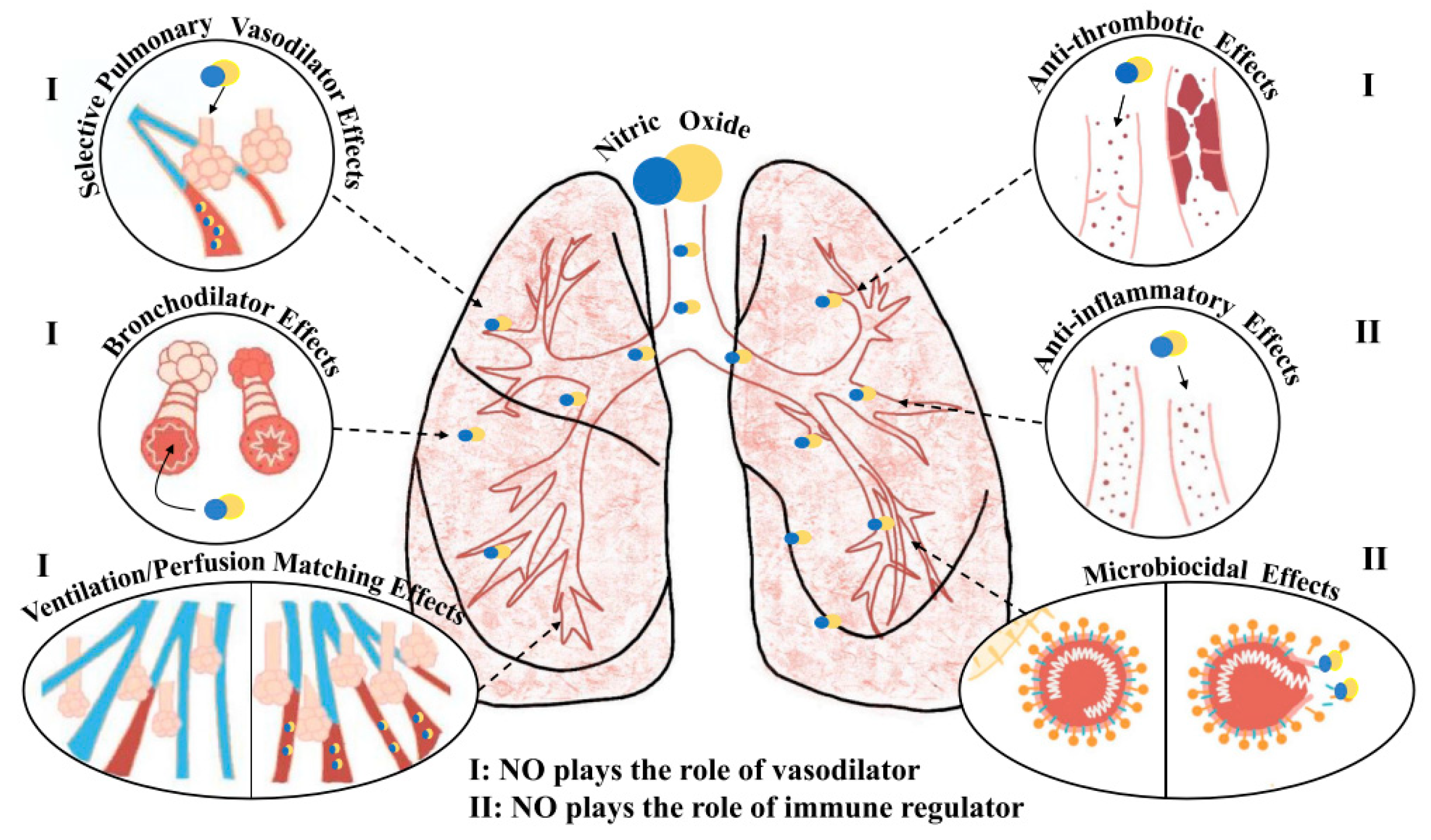
Figure 4.
Gut microbiota perturbation leading to cytokine storm causing severe COVID-19 and death [32].
Figure 4.
Gut microbiota perturbation leading to cytokine storm causing severe COVID-19 and death [32].
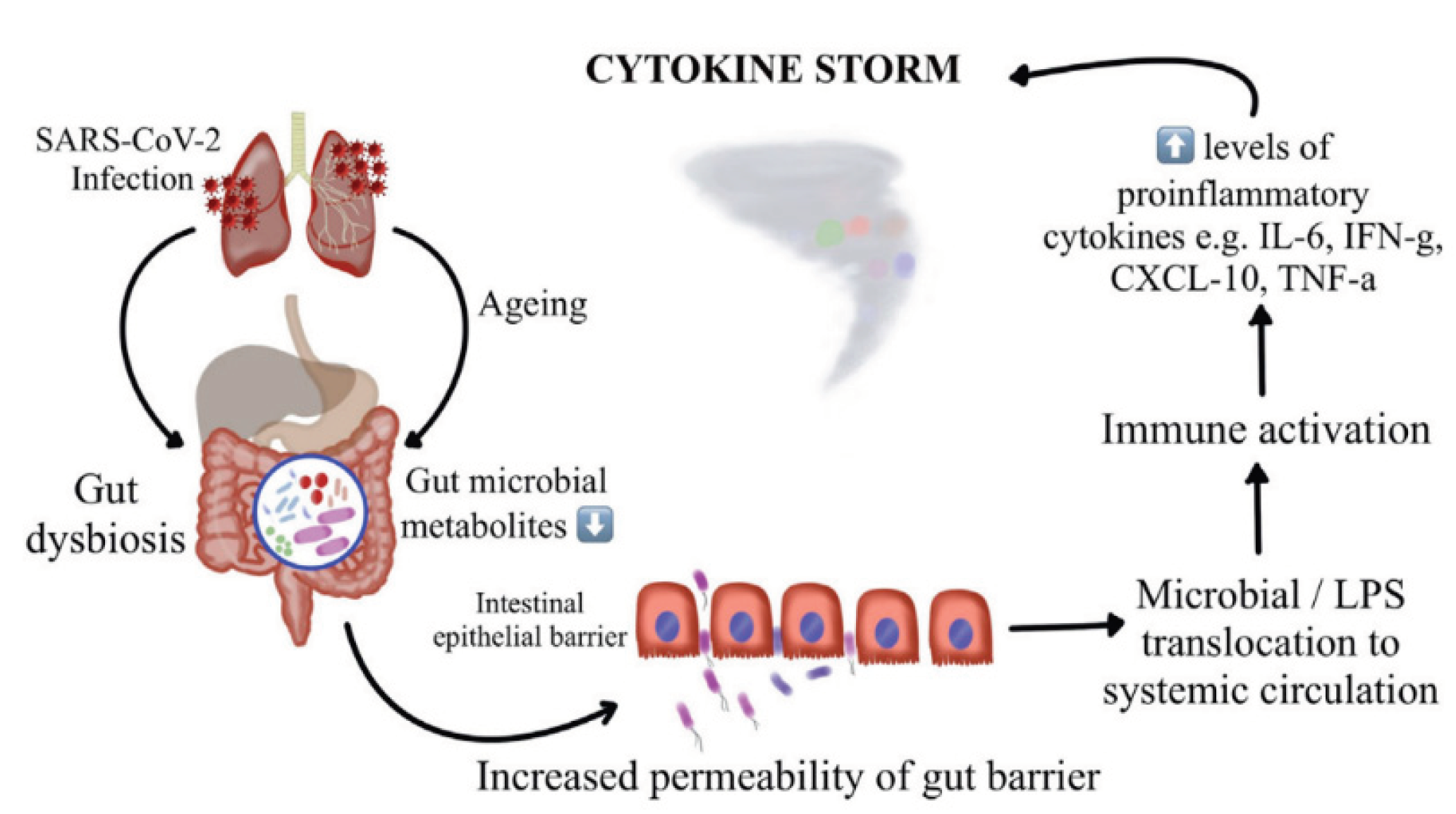
Figure 5.
Redox imbalance in coronavirus infections.
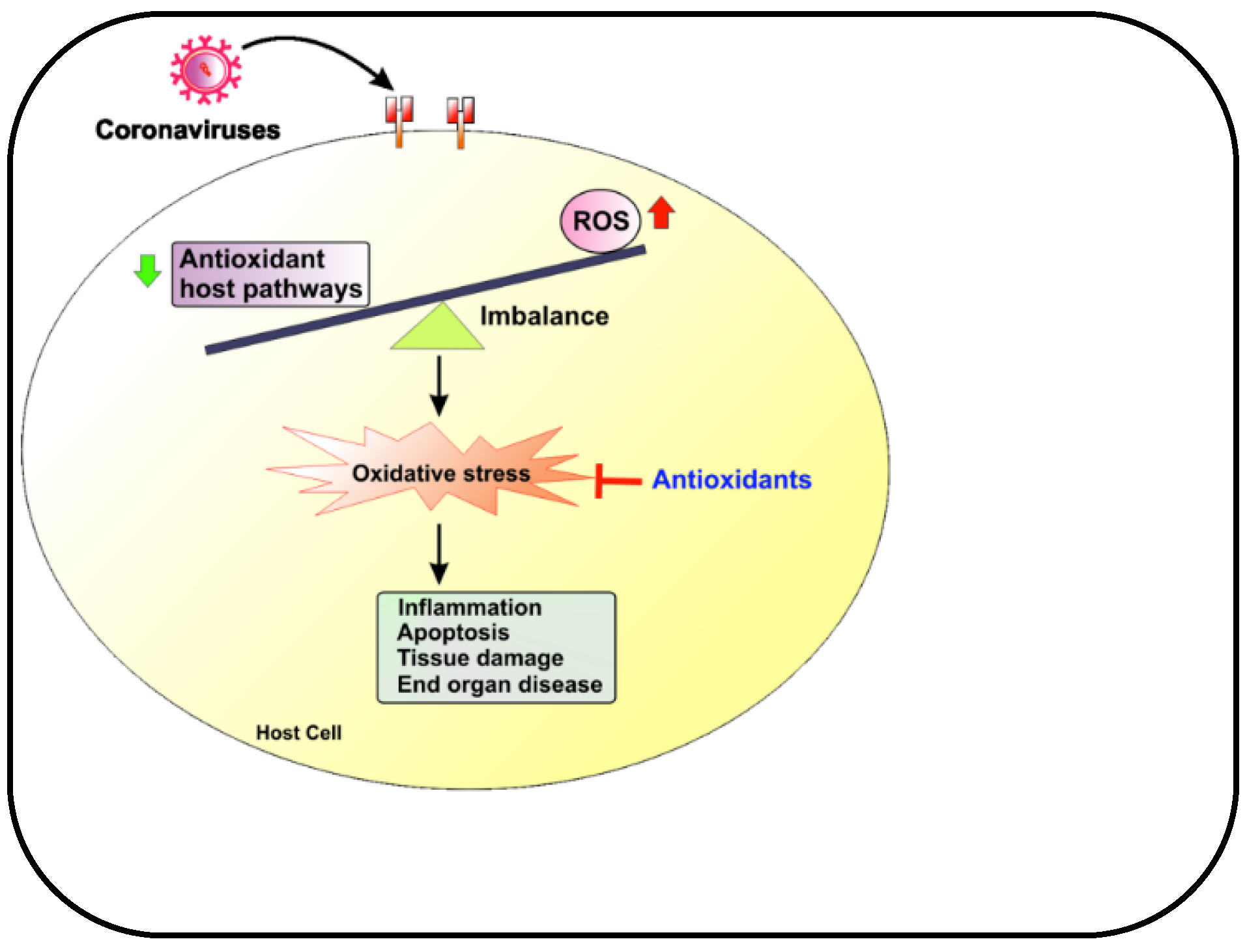

Table 1.
List of foods that reduce and increase DII.
| Foods that reduce DII | Foods that increase DII |
|---|---|
| Red meat (steak and hamburgers) Animal products (including eggs and dairy products) Processed meat Commercial baked goods White flour (bread and noodles), white rice Deep-fried foods Sugary products Products with trans-fats Saturated fats (especially animal fats) Cholesterol (red meats, processed meats, eggs, fried foods and dairy products) |
Plant-based proteins (beans, lentils, chickpeas, edamame, hemp seeds, tofu, tempeh, and nuts) Whole grains (oatmeal, buckwheat, quinoa, pigmented rice) Starchy vegetables (sweet potatoes and beets) Seeds (flaxseeds and chia seeds) Green leafy vegetables (raw) Colorful vegetables (raw) Fruits (berries, apples, grapes, oranges, peaches, figs, bananas, and kiwi) Spices and herbs (turmeric, ginger, cumin, peppermint, cinnamon, chili, parsley, bay leaf, and basil) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



