
Submitted:
01 March 2024
Posted:
04 March 2024
You are already at the latest version
Abstract
During pregnancy, profound physiological changes occur in the maternal body, including those affecting oral health. Dental stem cells (DSCs) have emerged as promising candidates for regenerative therapies in dentistry. This manuscript delves into the intricate interplay between DSC behavior and maternal oral health during pregnancy. We provide an overview of current knowledge concerning the impact of pregnancy on DSCs, highlighting their potential roles in maintaining oral homeostasis and responding to pathological conditions. Additionally, we identify key research gaps and propose future directions for investigating novel therapeutic strategies leveraging DSCs to improve maternal and fetal oral health outcomes. By elucidating this relationship, we aim to pave the way for innovative approaches in preventive and regenerative dentistry tailored to the unique needs of pregnant women.
Keywords:
Dental stem cells
; maternal oral health
; pregnancy
; oral microbiota
; regenerative potential
; hormonal changes
; preventive strategies
1. Introduction
Maintaining optimal oral health during pregnancy is crucial for the well-being of both the expectant mother and the developing fetus, with significant implications for maternal and child health outcomes. Hormonal fluctuations, characterized by elevated levels of estrogen and progesterone, play a pivotal role in influencing the oral cavity during pregnancy [1]. These changes can lead to alterations in the oral microbiota and increase susceptibility to specific oral health conditions and diseases. Managing and understanding these hormonal shifts is imperative to prevent complications such as gingivitis and periodontal disease [2].
The oral microbiota undergoes transformations influenced by hormonal variations and altered immune responses during pregnancy, heightening the risk of dental issues and emphasizing the need for comprehensive oral care [3]. Research has established connections between poor maternal oral health and adverse pregnancy outcomes, with conditions like periodontal disease being linked to an increased risk of preterm delivery and low birth weight [4,5].
Maternal oral health is intricately linked to systemic health, and maintaining good oral hygiene is paramount for preventing the exacerbation of existing conditions or the onset of new ones [6]. Furthermore, pathogens associated with maternal oral infections have been identified in the placenta and amniotic fluid, suggesting the potential for transplacental transmission [7,8].
In addition to its physiological aspects, the oral health of expectant mothers profoundly impacts their psychological well-being and overall quality of life during pregnancy. Addressing oral health concerns not only promotes physical well-being but also contributes to a positive maternal experience, nurturing a sense of overall well-being [9]. Recognizing the multifaceted impact of maternal oral health during pregnancy underscores the importance of comprehensive care to safeguard the health of both the expectant mother and the developing fetus.
In recent years, the field of regenerative medicine has witnessed substantial advancements, with Dental Stem Cells (DSCs) emerging as promising contributors. These cells, present in various oral tissues, possess unique regenerative properties, offering novel opportunities for revolutionizing therapeutic approaches in dentistry and beyond. DSCs encompass diverse types, including dental pulp stem cells (DPSCs) [10], stem cells from human exfoliated deciduous teeth (SHED) [11], periodontal ligament stem cells (PDLSCs) [12], and dental follicle progenitor cells (DFPCs) [13], each demonstrating distinct regenerative capabilities tailored for specific dental tissues.
A hallmark feature of DSCs lies in their remarkable ability to differentiate into various specialized cell types, even within the oral cavity [14]. These include odontoblasts for dentin formation, osteoblasts for bone regeneration, adipocytes for fat tissue formation, and neural cells [14]. The unique regenerative potential of DSCs positions them as pivotal players in tissue engineering and regenerative medicine applications within dentistry [15]. The versatility of DSCs has led to innovative applications aimed at addressing a wide array of oral health challenges, including regenerating damaged or lost tooth structures and enhancing periodontal tissues [16]. Moreover, the therapeutic potential of DSCs extends beyond dentistry, offering promising avenues for treating craniofacial disorders and injuries [17]. By harnessing the regenerative capacity of DSCs, it may be possible to develop innovative therapeutic strategies for managing pregnancy-related oral health issues. For example, DSC-based therapies could be utilized to promote periodontal tissue regeneration, enhance wound healing following dental procedures, or even regenerate lost dental tissues such as enamel and dentin [18,19]. However, while considerable progress has been made in understanding the regenerative properties of DSCs, there remain several research gaps that need to be addressed. For instance, further investigations are needed to elucidate how pregnancy influences the behavior and regenerative potential of DSCs in the oral cavity. Additionally, studies exploring the safety and efficacy of DSC-based therapies in pregnant individuals are warranted to ensure their suitability for clinical applications [20,21].
This comprehensive review aims to unravel the complex interplay between DSCs and maternal oral health during pregnancy. By synthesizing existing literature, it delves into the dynamics of maternal oral health changes, provides insights into the diverse types of DSCs, evaluates their regenerative potential, elucidates their clinical applications, and emphasizes the significance of interdisciplinary collaboration in this context. Additionally, it identifies gaps in current knowledge and proposes avenues for future research to deepen our understanding of this pivotal relationship.
2. Maternal Oral Health during Pregnancy
Elevated levels of estrogen and progesterone during pregnancy exert significant influences on various physiological processes, including vascularization and immune responses within the oral cavity [22,23]. These hormonal changes not only affect the structural integrity of oral tissues but also intricately influence the host's defense mechanisms, potentially altering susceptibility to oral diseases and conditions (Table 1) [22].
The interplay between hormonal shifts and the oral microbiota during pregnancy presents a compelling narrative for heightened vigilance in periodontal health monitoring among expectant mothers. Emerging evidence suggests that hormonally-induced alterations in the oral microbiota may exacerbate the risk of periodontal diseases in pregnant women [24,25]. Therefore, stringent oral health monitoring protocols are imperative to mitigate the heightened risk of periodontal diseases in pregnant women, underscoring the importance of integrated dental care within prenatal health management.
By elucidating how hormonal changes can influence the oral microbiome, dental professionals can design targeted interventions aimed at mitigating potential oral health risks during gestation [26,27]. These preventive measures may encompass personalized oral care plans that account for the heightened susceptibility to gingival inflammation and microbial dysbiosis characteristic of pregnancy. Furthermore, integrating regular dental check-ups and professional cleanings into prenatal care protocols can facilitate early detection and prompt management of periodontal conditions, thereby safeguarding maternal oral health and potentially reducing the risk of adverse pregnancy outcomes [26,27]. Acknowledging the intricate nexus between hormonal fluctuations, oral microbiota dynamics, and overall health underscores the imperative of fostering seamless collaboration between obstetric care providers and oral health professionals [26,27]. This integrative model of care transcends traditional disciplinary boundaries, recognizing oral health as a fundamental pillar of maternal well-being with far-reaching implications for both the mother and the developing fetus. Furthermore, this holistic model emphasizes the importance of comprehensive health education and preventive interventions tailored to the unique needs of pregnant individuals.
To minimize pregnancy-related complications, the following clinical implications may be drawn from the above-mentioned conditions. Monitoring oral health indicators during prenatal care allows for early intervention, potentially mitigating the risk of pregnancy-related complications [28,29]. Educating pregnant women about the importance of oral hygiene practices and regular dental check-ups is crucial in preventing potential complications [6,30]. Implementing comprehensive oral health education programs can empower women to adopt preventive measures and enhance their overall well-being during pregnancy.
3. DSCs
3.1. Types and Sources of DSCs
DSCs represent a promising frontier in regenerative medicine, offering diverse applications in dentistry and beyond [14]. Table 2 summarizes various types of DSCs, their respective sources, and key characteristics, thus facilitating a better understanding of their potential applications in regenerative medicine [15,31,32,33,34].
3.2. Clinical Significance of DSCs in Regenerative Dentistry
The clinical significance of DSCs resides in their exceptional regenerative potential and their wide-ranging applications in tissue engineering. Ongoing research and clinical trials are actively exploring the therapeutic possibilities of DSCs across diverse dental and systemic conditions, with a focus on refining protocols for their isolation, expansion, and differentiation [35]. With their remarkable regenerative capabilities, DSCs have the potential to revolutionize restorative dentistry by facilitating tooth regeneration and the repair of damaged dental pulp. Stem cells sourced from various dental tissues, including deciduous teeth and periodontal ligaments, offer promising avenues for addressing craniofacial disorders and injuries [36,37]. Efforts to raise awareness about DSC banking for future therapies, along with the continual optimization of isolation and differentiation protocols, are essential for fully realizing the clinical implications of these remarkable cells [38].
3.3. Standardization of Protocols
In the quest to advance DSC research, the standardization of experimental protocols is of utmost importance [38]. The subsequent sections will delineate standardized procedures for the isolation and differentiation of DSCs, quality control measures, strategies for interdisciplinary collaboration, and avenues for accessing these protocols.
3.3.1. Isolation of DSCs
Distinct protocols and procedures have been proposed to isolate the different types of cells. Here below, the anatomical sources and the key passages are summarized.
DPSCs: The isolation of DPSCs typically involves collecting dental tissues from the oral cavity, such as dental pulp, periodontal ligament, or dental follicle, from extracted or deciduous teeth [10,39,40]. The process begins with the extraction of teeth under aseptic conditions. Subsequently, the dental tissues are enzymatically digested or mechanically dissociated to release the stem cells from the extracellular matrix [10,39]. The dissociated cells are then cultured in specific growth media supplemented with fetal bovine serum (FBS) and additional growth factors to promote their proliferation and expansion [10,39]. Various isolation methods, including enzymatic digestion with collagenase and dispase, have been employed to isolate DSCs effectively [41]. Additionally, magnetic-activated cell sorting (MACS) or fluorescence-activated cell sorting (FACS) techniques may be utilized to isolate specific subpopulations of DSCs based on surface marker expression [42,43].
SHEDs: The isolation of SHEDs typically involves a sequential process starting with the collection of deciduous teeth from pediatric patients who undergo tooth extraction due to natural exfoliation or clinical indications [44]. Once collected, the dental pulp tissue within the teeth is accessed and dissociated enzymatically or mechanically under sterile conditions to release the stem cells [44]. Enzymatic digestion using collagenase and dispase is commonly employed to break down the extracellular matrix and liberate the cells. Following digestion, the cell suspension is centrifuged to pellet the cells, and the supernatant is discarded. The collected cells are then cultured in specialized growth media containing FBS and growth factors, such as basic fibroblast growth factor (bFGF) and epidermal growth factor (EGF), to promote their proliferation and expansion [45]. Such optimized culture conditions support the maintenance of stem cell properties and facilitate their propagation in vitro. Additionally, MACS or FACS techniques can be utilized to isolate specific subpopulations of SHEDs based on the expression of surface markers, allowing for the enrichment of the desired cell populations [42].
PDLSCs: The isolation of PDLSCs involves obtaining tissue from the periodontal ligament, which connects the tooth root to the alveolar bone. Typically, PDLSCs are harvested either from extracted teeth or obtained during periodontal surgeries. The collected tissue is subjected to enzymatic digestion using collagenase and dispase or other proteolytic enzymes to dissociate the cells from the extracellular matrix [46]. Mechanical scraping or shaking may also be employed to aid in the release of cells. Following digestion, the cell suspension is filtered to remove debris, and the dissociated cells are cultured in specialized growth media supplemented with FBS and growth factors such as platelet-derived growth factor (PDGF) and insulin-like growth factor (IGF) [46]. These culture conditions support the proliferation and maintenance of PDLSCs' stemness properties. Additionally, PDLSCs can be isolated using techniques like MACS or FACS based on specific surface marker expression, allowing for the enrichment of the desired cell population [42].
DFPCs: The isolation of DFPCs typically involves collecting dental follicle tissues from extracted or impacted teeth, particularly those associated with developing permanent teeth [47]. The process begins with the extraction of the tooth containing the dental follicle under aseptic conditions. Subsequently, the dental follicle tissues are carefully dissected and enzymatically digested or mechanically dissociated to release the progenitor cells from the extracellular matrix [48]. Enzymatic digestion using collagenase and dispase is commonly employed to break down the tissue and liberate the cells [42]. Following digestion, the cell suspension is centrifuged to isolate the cells, and the supernatant is discarded. The collected cells are then cultured in specialized growth media containing FBS and growth factors, such as fibroblast growth factor (FGF) and PDGF, to promote cell proliferation and expansion [42]. These optimized culture conditions support the maintenance of stem cell properties and facilitate their propagation in vitro [49]. Additionally, MACS or FACS techniques can be utilized to isolate specific subpopulations of DFPCs based on surface marker expression, allowing for the enrichment of desired cell populations [42].
3.3.2. Enhancing Research Efficiency: Protocols, Quality Control, Collaboration, and Accessibility
Table 3 presents the fundamental components for navigating the intricate landscape of stem cell research methodologies and collaborative practices. Adherence to these standardized protocols, by means of well-established methodologies [13,49,50], will contribute to the robustness and reproducibility of DSC research, fostering advancements in regenerative dentistry.
3.4. Translating research findings into clinically relevant therapies
Achieving standardized protocols for DSC isolation and differentiation is essential for translating research findings into clinically viable therapies [51]. Table 4 provides a structured overview of the main steps aimed at translating basic research data into clinically relevant approaches for dental stem cell management. DSC isolation, differentiation, and quality control measures are considered. Each step is accompanied by a description of the actions involved in that particular stage of the process.
3.5. DSCs Behavior during Pregnancy
3.5.1. Understanding the Impact of Pregnancy on DSC Behavior: Current Knowledge and Research Gaps
During pregnancy, profound hormonal changes and immune modulation occur, potentially influencing the behavior of DSCs [1,2]. While emerging evidence suggests a link between pregnancy and alterations in DSC function, precise mechanisms and implications remain poorly understood. Research efforts have focused on elucidating the effects of pregnancy-related factors on DSC proliferation, differentiation, and immunomodulatory properties, yet significant knowledge gaps persist.
Some studies suggest enhanced regenerative potential of DSCs during pregnancy, while others indicate compromised functionality [10,11,12,13,14,15]. Factors such as trimester-specific hormonal changes, maternal age, and systemic conditions may contribute to variations in DSC behavior. Moreover, alterations in the oral microenvironment, including changes in salivary composition and immune responses, may further modulate DSC activity.
To address research gaps, longitudinal studies are needed to assess DSC behavior throughout pregnancy and postpartum periods. Standardized experimental models are essential for elucidating underlying mechanisms and predicting clinical outcomes accurately. Investigations into the implications of pregnancy-induced alterations in DSC behavior for maternal oral health and regenerative therapies are warranted.
Understanding the impact of pregnancy on DSC behavior is crucial for advancing knowledge of maternal oral health and developing effective regenerative strategies tailored to pregnant individuals.
4. Future Directions and Research Recommendations
Moving forward, several avenues for future research and recommendations emerge regarding the impact of pregnancy on DSC behavior. By pursuing these research directions, we can deepen our understanding of how pregnancy influences DSC behavior and pave the way for innovative regenerative therapies to enhance maternal oral health outcomes (Flowchart 1).
4.1. Novel Therapeutic Strategies Leveraging DSCs for Maternal Oral Health Enhancement
A) Dental Stem Cell-Based Periodontal Therapy: Periodontal diseases, such as gingivitis and periodontitis, are prevalent among pregnant women and have been associated with adverse pregnancy outcomes [12]. Dental stem cell-based periodontal therapy involves the use of DSCs, such as PDLSCs and DPSCs, to regenerate periodontal tissues damaged by disease [10]. Preclinical studies have demonstrated the efficacy of DSC-based therapies in promoting periodontal tissue regeneration and reducing inflammation, offering a potential treatment modality for pregnant women with periodontal disease.
B) Dental Stem Cell-Mediated Pulp Regeneration: Pulpal diseases, including pulpitis and pulp necrosis, can pose significant challenges during pregnancy due to limited treatment options that are safe for both the mother and fetus [52]. Dental stem cell-mediated pulp regeneration involves the transplantation of DSCs, such as stem cells from the apical papilla (SCAP) or DPSCs, into the pulp chamber to promote pulp tissue regeneration and repair [53]. This approach holds promise for preserving the vitality of compromised teeth and avoiding invasive procedures during pregnancy.
C) Immunomodulatory Effects of Dental Stem Cells: In addition to their regenerative properties, DSCs possess potent immunomodulatory capabilities that can modulate the maternal immune response and mitigate inflammation-associated complications during pregnancy [54]. DSCs exert immunomodulatory effects through the secretion of anti-inflammatory cytokines and the suppression of immune cell activation. Harnessing these immunomodulatory properties may offer novel therapeutic strategies for managing oral inflammatory conditions in pregnant women, such as gingivitis and periodontitis.
D) Salivary Gland Regeneration Using Dental Stem Cells: Xerostomia, or dry mouth, is a common oral health issue experienced by pregnant women, often attributed to hormonal changes and dehydration [55]. Severe cases of xerostomia can lead to oral infections and compromised oral health. Dental stem cell-based approaches for salivary gland regeneration offer a potential solution for restoring salivary gland function and alleviating xerostomia in pregnant women.
6. Conclusions
The utilization of DSCs holds significant promise in advancing regenerative dentistry and addressing oral health issues during pregnancy. To develop tailored therapeutic interventions for pregnant women, it's crucial to deepen our understanding of how pregnancy influences DSC behavior and its impact on oral health outcomes. By leveraging the regenerative and immunomodulatory properties of DSCs, innovative strategies can be devised to effectively manage oral health conditions in expectant mothers prioritizing the safety and well-being of both mother and fetus.
Author Contributions
“Conceptualization, Aida Meto and A.S.; methodology, Agron Meto; software, A.S.; validation Aida Meto, S.P. and E.B.; formal analysis, A.S.; investigation, A.S.; resources, Aida Meto; data curation, Agron Meto.; writing—original draft preparation, Aida Meto; writing—review and editing, E.B.; visualization, S.P.; supervision, S.P. and Agron Meto. All authors have read and agreed to the published version of the manuscript.”
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Steinberg, B.J. Women's oral health issues. J Calif Dent Assoc. 2000, 28, 663–7. [Google Scholar] [CrossRef]
- Hartnett, E.; Haber, J.; Krainovich-Miller, B.; Bella, A.; Vasilyeva, A.; Lange Kessler, J. Oral Health in Pregnancy. J Obstet Gynecol Neonatal Nurs. 2016, 45, 565–73. [Google Scholar] [CrossRef]
- Saadaoui, M.; Singh, P.; Al Khodor, S. Oral microbiome and pregnancy: A bidirectional relationship. J Reprod Immunol. 2021, 145, 103293. [Google Scholar] [CrossRef]
- Boggess, K.A. Choosing the left fork: Steven Offenbacher and understanding maternal periodontal disease and adverse pregnancy outcomes. J Periodontol. 2020, 91, S40–S44. [Google Scholar] [CrossRef]
- Daskalakis, G.; Psarris, A.; Koutras, A, et al. Maternal Infection and Preterm Birth: From Molecular Basis to Clinical Implications. Children (Basel) 2023, 10, 907. [CrossRef]
- Bushehab, N.M.E.; Sreedharan, J.; Reddy, S.; D'souza, J.; Abdelmagyd, H. Oral Hygiene Practices and Awareness of Pregnant Women about the Effects of Periodontal Disease on Pregnancy Outcomes. Int J Dent. 2022, 2022, 5195278. [Google Scholar] [CrossRef]
- Han, Y.W.; Redline, R.W.; Li, M.; Yin, L.; Hill, G.B.; McCormick, T.S. Fusobacterium nucleatum induces premature and term stillbirths in pregnant mice: implication of oral bacteria in preterm birth. Infect Immun. 2004, 72, 2272–9. [Google Scholar] [CrossRef]
- Vidmar Šimic, M.; Maver, A.; Zimani, A.N.; Hočevar, K.; Peterlin, B.; Kovanda, A.; Premru-Sršen, T. Oral microbiome and preterm birth. Front Med (Lausanne). 2023, 10, 1177990. [Google Scholar] [CrossRef]
- Lagadec, N.; Steinecker, M.; Kapassi, A.; Magnier, A.M.; Chastang, J.; Robert, S.; et al. Factors influencing the quality of life of pregnant women: a systematic review. BMC Pregnancy Childbirth 2018, 18, 455. [Google Scholar] [CrossRef]
- Gronthos, S.; Mankani, M.; Brahim, J.; Robey, P.G.; Shi, S. Postnatal human dental pulp stem cells (DPSCs) in vitro and in vivo. Proc Natl Acad Sci U S A. 2000, 97, 13625–30. [Google Scholar] [CrossRef]
- Miura, M.; Gronthos, S.; Zhao, M.; Lu, B.; Fisher, L.W.; Robey, P.G.; Shi, S. SHED: stem cells from human exfoliated deciduous teeth. Proc Natl Acad Sci U S A. 2003, 100, 5807–12. [Google Scholar] [CrossRef]
- Seo, B.M.; Miura, M.; Gronthos, S.; Bartold, P.M.; Batouli, S.; Brahim, J.; Young, M.; Robey, P.G.; Wang, C.Y.; Shi, S. Investigation of multipotent postnatal stem cells from human periodontal ligament. Lancet 2004, 364, 149–55. [Google Scholar] [CrossRef] [PubMed]
- Morsczeck, C.; Götz, W.; Schierholz, J.; Zeilhofer, F.; Kühn, U.; Möhl, C.; Sippel, C.; Hoffmann, K.H. Isolation of precursor cells (PCs) from human dental follicle of wisdom teeth. Matrix Biol. 2005, 24, 155–65. [Google Scholar] [CrossRef]
- Botelho, J.; Cavacas, M.A.; Machado, V.; Mendes, J.J. Dental stem cells: recent progresses in tissue engineering and regenerative medicine. Ann Med. 2017, 49, 644–651. [Google Scholar] [CrossRef]
- Zhai, Q.; Dong, Z.; Wang, W.; Li, B.; Jin, Y. Dental stem cell and dental tissue regeneration. Front Med. 2019, 13, 152–159. [Google Scholar] [CrossRef]
- Miran, S.; Mitsiadis, T.A.; Pagella, P. Innovative Dental Stem Cell-Based Research Approaches: The Future of Dentistry. Stem Cells Int. 2016, 2016, 7231038. [Google Scholar] [CrossRef]
- Vaswani, B.K.; Mundada, B.P.; Bhola, N.; Paul, P.; Reche, A.; Ahuja, K.P. Stem-Cell Therapy: Filling Gaps in Oro-Maxillofacial Region. Cureus 2023, 15, e47171. [Google Scholar] [CrossRef]
- Bansal, R.; Jain, A. Current overview on dental stem cells applications in regenerative dentistry. J Nat Sci Biol Med. 2015, 6, 29–34. [Google Scholar] [CrossRef]
- Moshaverinia, A.; Chen, C.; Xu, X.; et al. Regulation of the Stem Cell-Host Immune System Interplay Using Hydrogel Coencapsulation System with an Anti-Inflammatory Drug. Adv Funct Mater. 2015, 25, 2296–2307. [Google Scholar] [CrossRef]
- Huang, G.T.; Gronthos, S.; Shi, S. Mesenchymal stem cells derived from dental tissues vs. those from other sources: their biology and role in regenerative medicine. J Dent Res. 2009, 88, 792–806. [Google Scholar] [CrossRef]
- Volponi, A.A.; Pang, Y.; Sharpe, P.T. Stem cell-based biological tooth repair and regeneration. Trends Cell Biol. 2010, 20, 715–22. [Google Scholar] [CrossRef]
- Offenbacher, S.; Lieff, S.; Boggess, K.A.; et al. Maternal periodontitis and prematurity. Part I: Obstetric outcome of prematurity and growth restriction. Ann Periodontol. 2001, 6, 164–74. [Google Scholar] [CrossRef]
- Beckers, K.F.; Sones, J.L. Maternal microbiome and the hypertensive disorder of pregnancy, preeclampsia. Am J Physiol Heart Circ Physiol. 2020, 318, H1–H10. [Google Scholar] [CrossRef]
- Ye, C.; Kapila, Y. Oral microbiome shifts during pregnancy and adverse pregnancy outcomes: Hormonal and Immunologic changes at play. Periodontol 2000. 2021, 87, 276–281. [Google Scholar] [CrossRef]
- Balan, P.; Chong, Y.S.; Umashankar, S.; et al. Keystone Species in Pregnancy Gingivitis: A Snapshot of Oral Microbiome During Pregnancy and Postpartum Period. Front Microbiol. 2018, 9, 2360. [Google Scholar] [CrossRef]
- Iida, H. Oral Health Interventions During Pregnancy. Dent Clin North Am. 2017, 61, 467–481. [Google Scholar] [CrossRef]
- Steinberg, B.J.; Hilton, I.V.; Iida, H.; Samelson, R. Oral health and dental care during pregnancy. Dent Clin North Am. 2013, 57, 195–210. [Google Scholar] [CrossRef] [PubMed]
- Hartnett, E.; Haber, J.; Krainovich-Miller, B.; Bella, A.; Vasilyeva, A.; Lange Kessler, J. Oral Health in Pregnancy. J Obstet Gynecol Neonatal Nurs. 2016, 45, 565–73. [Google Scholar] [CrossRef] [PubMed]
- Krukowski, R.A.; Jacobson, L.T.; John, J.; et al. Correlates of Early Prenatal Care Access among U. S. Women: Data from the Pregnancy Risk Assessment Monitoring System (PRAMS). Matern Child Health J. 2022, 26, 328–341. [Google Scholar] [CrossRef] [PubMed]
- Przeklasa-Bierowiec, A.; Jakubik, A.; Szczeklik, K.; Majewska, I.; Marcinek, A.; Pytko-Polończyk, J. Awareness of oral health prophylaxis in pregnant women. Folia Med Cracov. 2020, 60, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Sui, B.; Wu, D.; Xiang, L.; Fu, Y.; Kou, X.; Shi, S. Dental Pulp Stem Cells: From Discovery to Clinical Application. J Endod. 2020, 46, S46–S55. [Google Scholar] [CrossRef] [PubMed]
- Bar, J.K.; Lis-Nawara, A.; Grelewski, P.G. Dental Pulp Stem Cell-Derived Secretome and Its Regenerative Potential. Int J Mol Sci. 2021, 22, 12018. [Google Scholar] [CrossRef] [PubMed]
- Tomokiyo, A.; Wada, N.; Maeda, H. Periodontal Ligament Stem Cells: Regenerative Potency in Periodontium. Stem Cells Dev. 2019, 28, 974–985. [Google Scholar] [CrossRef] [PubMed]
- Bi, R.; Lyu, P.; Song, Y.; Li, P.; Song, D.; Cui, C.; Fan, Y. Function of Dental Follicle Progenitor/Stem Cells and Their Potential in Regenerative Medicine: From Mechanisms to Applications. Biomolecules. 2021, 11, 997. [Google Scholar] [CrossRef]
- Song, W.P.; Jin, L.Y.; Zhu, M.D.; Wang, H.; Xia, D.S. Clinical trials using dental stem cells: 2022 update. World J Stem Cells. 2023, 15, 31–51. [Google Scholar] [CrossRef]
- Rai, S.; Kaur, M.; Kaur, S. Applications of stem cells in interdisciplinary dentistry and beyond: an overview. Ann Med Health Sci Res. 2013, 3, 245–54. [Google Scholar] [CrossRef]
- Chalisserry, E.P.; Nam, S.Y.; Park, S.H.; Anil, S. Therapeutic potential of dental stem cells. J Tissue Eng. 2017, 8, 2041731417702531. [Google Scholar] [CrossRef]
- Hilkens, P.; Driesen, R.B.; Wolfs, E.; et al. Cryopreservation and Banking of Dental Stem Cells. Adv Exp Med Biol. 2016, 951, 199–235. [Google Scholar] [CrossRef]
- Gronthos, S.; Arthur, A.; Bartold, P.M.; Shi, S. A method to isolate and culture expand human dental pulp stem cells. Methods Mol Biol. 2011, 698, 107–21. [Google Scholar] [CrossRef]
- Smith, J.G.; Smith, A.; Shelton, R.M.; Cooper, P.R. Dental Pulp Cell Behavior in Biomimetic Environments. J Dent Res. 2015, 94, 1552–9. [Google Scholar] [CrossRef]
- Pisciotta, A.; Carnevale, G.; Meloni, S.; et al. Human dental pulp stem cells (hDPSCs): isolation, enrichment and comparative differentiation of two sub-populations. BMC Dev Biol. 2015, 15, 14. [Google Scholar] [CrossRef]
- Bacon, K.; Lavoie, A.; Rao, B.M.; Daniele, M.; Menegatti, S. Past, Present, and Future of Affinity-based Cell Separation Technologies. Acta Biomater. 2020, 112, 29–51. [Google Scholar] [CrossRef]
- Dieterle, M.P.; Gross, T.; Steinberg, T.; et al. Characterization of a Stemness-Optimized Purification Method for Human Dental-Pulp Stem Cells: An Approach to Standardization. Cells 2022, 11, 3204. [Google Scholar] [CrossRef]
- Wang, X.; Sha, X.J.; Li, G.H.; et al. Comparative characterization of stem cells from human exfoliated deciduous teeth and dental pulp stem cells. Arch Oral Biol. 2012, 57, 1231–40. [Google Scholar] [CrossRef]
- Jeon, M.; Song, J.S.; Choi, B.J.; Choi, H.J.; Shin, D.M.; Jung, H.S.; Kim, S.O. In vitro and in vivo characteristics of stem cells from human exfoliated deciduous teeth obtained by enzymatic disaggregation and outgrowth. Arch Oral Biol. 2014, 59, 1013–23. [Google Scholar] [CrossRef]
- Behfarnia, P.; Fazlalizadeh, S.; Nasr-Esfahani, M.H.; Ejeian, F.; Mogharehabed, A. Isolation and characterization of human periodontal ligament stem cells under the terms of use in clinical application: A pilot study. Dent Res J (Isfahan). 2023, 20, 105. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Xu, X.; Lin, J.; Fan, L.; Zheng, Y.; Kuang, W. Dental Stem Cell in Tooth Development and Advances of Adult Dental Stem Cell in Regenerative Therapies. Curr Stem Cell Res Ther. 2015, 10, 375–83. [Google Scholar] [CrossRef]
- Aydin, S.; Şahin, F. Stem Cells Derived from Dental Tissues. Adv Exp Med Biol. 2019, 1144, 123–132. [Google Scholar] [CrossRef]
- Karaöz, E.; Doğan, B.N.; Aksoy, A.; et al. Isolation and in vitro characterisation of dental pulp stem cells from natal teeth. Histochem Cell Biol. 2010, 133, 95–112. [Google Scholar] [CrossRef] [PubMed]
- Chouaib, B.; Cuisinier, F.; Collart-Dutilleul, P.Y. Dental stem cell-conditioned medium for tissue regeneration: Optimization of production and storage. World J Stem Cells. 2022, 14, 287–302. [Google Scholar] [CrossRef] [PubMed]
- Dominici, M.; Le Blanc, K.; Mueller, I.; et al. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–7. [Google Scholar] [CrossRef]
- Sonoyama, W.; Liu, Y.; Yamaza, T.; Tuan, R.S.; Wang, S.; Shi, S.; Huang, G.T. Characterization of the apical papilla and its residing stem cells from human immature permanent teeth: a pilot study. J Endod. 2008, 34, 166–71. [Google Scholar] [CrossRef]
- Huang, G.T.; Sonoyama, W.; Liu, Y.; Liu, H.; Wang, S.; Shi, S. The hidden treasure in apical papilla: the potential role in pulp/dentin regeneration and bioroot engineering. J Endod. 2008, 34, 645–51. [Google Scholar] [CrossRef]
- Tatullo, M.; Marrelli, M.; Shakesheff, K.M.; White, L.J. Dental pulp stem cells: function, isolation and applications in regenerative medicine. J Tissue Eng Regen Med. 2015, 9, 1205–16. [Google Scholar] [CrossRef]
- Lombaert, I.M.; Brunsting, J.F.; Wierenga, P.K.; et al. Rescue of salivary gland function after stem cell transplantation in irradiated glands. PLoS One 2008, 3, e2063. [Google Scholar] [CrossRef]
Figure 1.
Overview of factors influencing DSC behavior during pregnancy.
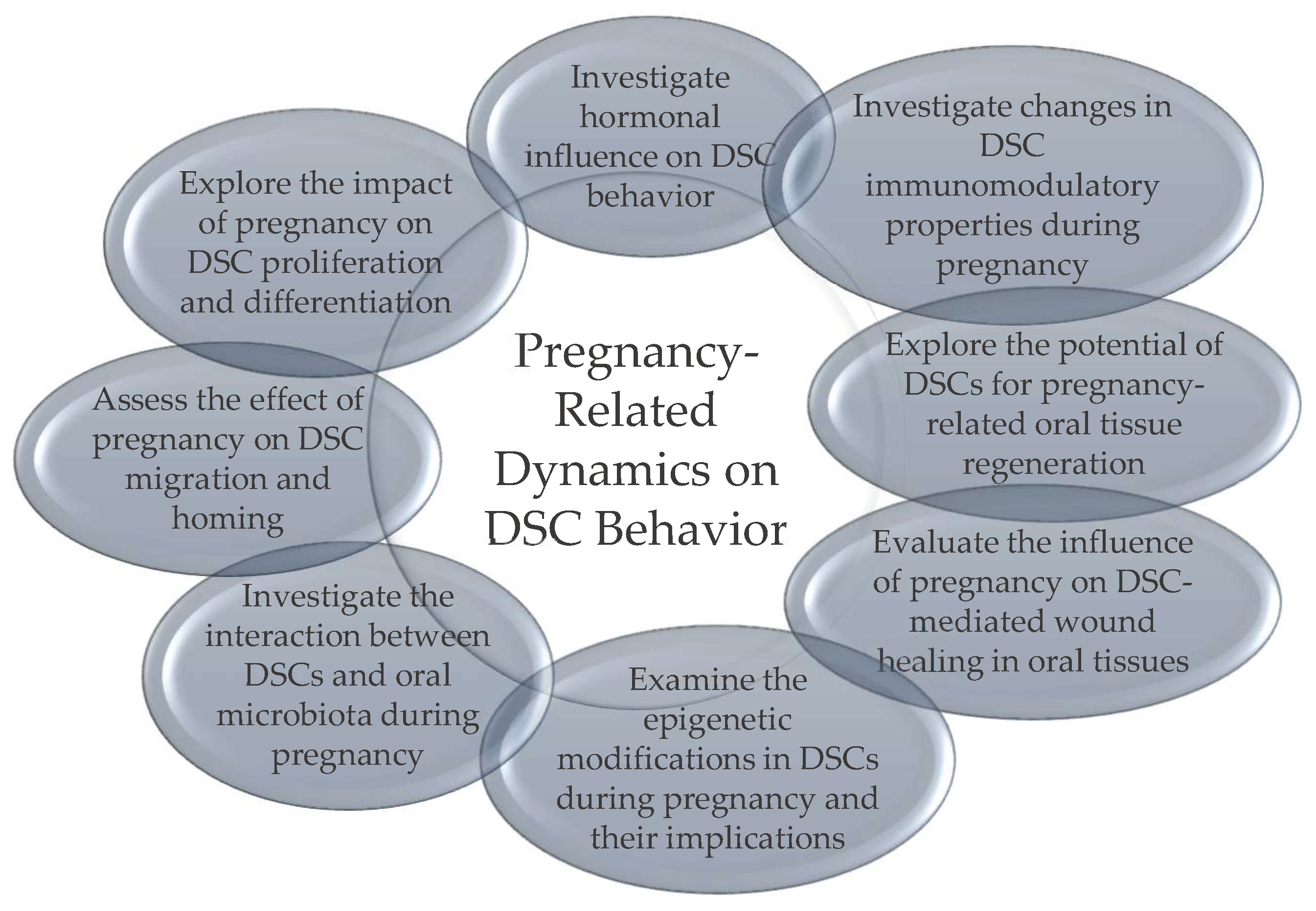

Table 1.
Oral health indicators and their association with pregnancy-related complications.
| Oral Health Indicator | Description | Correlation with Pregnancy-Related Complications |
|---|---|---|
| Gingival Inflammation | Swelling, redness, and tenderness of the gingiva | Increased risk of preterm birth, low birth weight |
| Periodontal Disease | Inflammation and infection of the gums and surrounding tissues | Linked to preterm birth, preeclampsia, and gestational diabetes |
| Dental Caries | Tooth decay resulting from bacterial acid demineralization | May exacerbate the risk of preterm birth and low birth weight |
| Pregnancy Gingivitis | Gingival inflammation exacerbated by hormonal changes | Associated with adverse pregnancy outcomes, including preterm birth |
| Oral Candidiasis | Fungal infection characterized by white patches in the mouth | May indicate immunosuppression, potential risk factor for preterm birth |
| Oral Lesions | Abnormalities in the oral mucosa, including ulcers, red or white patches | Linked to nutritional deficiencies, may affect maternal health and fetal development |
| Pregnancy Tumors | Also known as pyogenic granulomas or granuloma gravidarum | Presence may indicate hormonal imbalances; typically resolve postpartum |
| Salivary Changes | Altered salivary composition, dry mouth | Changes in salivary flow and composition may impact oral health and contribute to the development of gestational diabetes |
Table 2.
Overview of types and sources of DSCs.
| DSC Type | Source | Characteristics |
|---|---|---|
| Dental Pulp Stem Cells (DPSCs) | Dental pulp of teeth | - Multipotent mesenchymal stem cells########- Self-renewal capabilities########- Differentiation into odontoblasts, osteoblasts, adipocytes, and neural cells########- High proliferative capacity########- Expression of mesenchymal stem cell markers (CD73, CD90, CD105) |
| Stem Cells from Human Exfoliated Deciduous Teeth (SHEDs) | Dental pulp of deciduous teeth | - High proliferation rates########- Multipotent differentiation capabilities########- Differentiation into odontoblasts, adipocytes, and neural cells########- Accessibility and ease of isolation########- Robust regenerative potential |
| Periodontal Ligament Stem Cells (PDLSCs) | Periodontal ligament | - Self-renewal capacity########- Multilineage differentiation potential (osteoblasts, chondrocytes, adipocytes)########- Crucial role in maintaining periodontal tissue homeostasis########- Potential in regenerative therapies for periodontal tissue repair |
| Dental Follicle Progenitor Cells (DFPCs) | Dental follicle surrounding tooth germ | - Self-renewal ability########- Multilineage differentiation potential (osteoblasts, adipocytes, cementoblasts)########- Vital role in tooth eruption and periodontal tissue formation########- Potential for tooth and periodontal tissue regeneration |
Table 3.
Overview of stem cell research methodologies and collaborative practices.
| Specific Aspect | Description |
|---|---|
| Standardized Differentiation Protocols | Protocols established for obtaining differentiated cells from various lineages |
| - Odontoblastic Differentiation | Induce differentiation with specific odontogenic medium; monitor gene expression and mineralization |
| - Osteogenic Differentiation | Culture cells in osteogenic medium containing dexamethasone and β-glycerophosphate; assess osteogenic markers and mineralized matrix |
| - Adipogenic Differentiation | Induce adipogenesis using adipogenic medium; confirm differentiation by lipid staining and adipogenic marker expression |
| - Neurogenic Differentiation | Expose cells to neurogenic differentiation medium; evaluate neural marker expression and neurite formation |
| Quality Control Measures | Measures ensuring the correctness of produced data |
| - Viability Assessment | Employ assays (e.g., Trypan Blue exclusion) to determine cell viability |
| - Phenotypic Characterization | Confirm stem cell markers (e.g., CD146, STRO-1) via flow cytometry |
| - Sterility Testing | Regularly perform microbial testing to ensure aseptic conditions |
| - Functional Assays | Validate stem cell functionality through differentiation assays |
| Interdisciplinary Collaboration | Enhanced potential of studies through multidisciplinary collaboration |
| - Regular Consultation | Engage with experts in stem cell biology, dentistry, and regenerative medicine |
| - Open Communication | Establish platforms for sharing protocols and research findings. |
| - Collaborative Research Projects | Foster joint initiatives to refine and optimize protocols collaboratively |
| Access to Protocols | Methods to access and share protocols effectively |
| - Online Repositories | Contribute to and utilize online platforms for protocol sharing. |
| - Scientific Journals | Encourage publication of detailed protocols alongside research articles |
| - Consortium Initiatives | Support consortiums promoting standardized protocols in dental stem cell research |
Table 4.
Summary of translational steps for DSC therapies.
| Steps | Description |
|---|---|
| DSC ########Isolation | - Following the International Society for Cellular Therapy guidelines for minimal criteria [51] ########- Source cells from well-established locations such as dental pulp, deciduous teeth, periodontal ligament, and dental follicle [10,11,12,13] ########- Ensure ethical considerations and regulatory approvals ########- Use aseptic techniques during tissue collection and cell isolation |
| DSC Differentiation | - Choose appropriate differentiation protocols based on desired cell type (e.g., odontoblasts, osteoblasts, adipocytes, neural cells) ########- Optimize culture conditions for specific lineage differentiation########- Validate differentiation outcomes through morphological, molecular, and functional assays ########- Adjust protocols based on assessment results |
| Quality Control | - Implement rigorous quality control measures at each step of isolation and differentiation ########- Monitor cell viability, morphology, and phenotype throughout the process########- Use standardized assays to confirm multipotency and differentiation potential |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



