
Submitted:
01 March 2024
Posted:
04 March 2024
You are already at the latest version
Abstract
Our aim was to determine the secondary antibody deficiency profiles of patients in a mesoregion of São Paulo state, Brazil, focusing on infectious diseases. Demographic characteristics, clinical and laboratory data were obtained from electronic files; infections were classified as organ-specific and graded as mild, moderate, life-threatening, and fatal. Non-Hodgkin lymphoma (NHL) accounted for 30% of patients, nephrotic syndrome (NS) 25%; chronic lymphocyte leukemia 20%, and multiple myeloma 15%. Patients with NS were younger than those in other groups, and hypo-γ-globulinemia was detected in 94.1%, IgG <400 mg/dL in 60.0%, IgA <40 mg/dL in 55.0%, and CD19 <20 cells/mm3 in 30.0%. One hundred and one infections were found; 82.1% were classified as mild or moderate, 7.9% as life-threatening, and 1.9% as fatal. Respiratory tract infections were more prevalent (41.5%), and pneumonia accounted for 19.8%. Lower levels of infections were found in patients with NS compared with NHL (P=0.0001). Most patients progressed to hypo-γ-globulinemia and secondary antibody deficiency after treatment with immunosuppressants, and mild and moderate infections were predominant. These therapies are increasing in patients with different diseases, therefore monitoring hypo-γ-globulinemia and infections may help to identify patients at high risk for severe complications, antibiotic prophylaxis or treatment, and immunoglobulin replacement
Keywords:
Secondary Antibody Deficiency
; hypo-γ-globulinemia
; infectious diseases
1. Introduction
Secondary immunodeficiency (SID) is an impairment of the immune system due to extrinsic factors and underlying medical conditions. SID is up to 30 times more common than inborn errors of immunity (IEI) and can occur as a consequence of hematologic malignancies, autoimmune diseases, immunosuppressive therapies, malnutrition, metabolic disorders, chronic infections, and severe trauma. Furthermore, SIDs are becoming increasingly common as new therapies are available [1]. Several mechanisms induce SIDs. In onco-hematology malignancies, SID is induced due to systemic disorders that include aplastic anemia; hematologic malignancies, such as chronic lymphocytic leukemia (CLL), multiple myeloma (MM), Hodgkin’s disease, non-Hodgkin lymphoma (NHL); graft vs. host disease, and sickle cell disease. One of the leading causes of SID in onco-hematology is iatrogenic disorders caused by biological agents such as chemotherapy, immunosuppressants, corticosteroids, monoclonal antibodies, including anti-CD20 agents, and B cell differentiation and maturation inhibitors, as well as other conditions; radiation therapy, splenectomy, and bone marrow ablation before transplant [2]. In a large cohort of onco-hematologic diseases, biological agents have become one of the best early therapeutic options. They block inflammatory pathways, which reduces pathologic inflammation through various mechanisms such as cytokine inhibition, monoclonal cell deletion, and co-stimulatory inhibition [3,4]. Consequently, most of these biological agents cause immunosuppression leading to hypo-γ-globulinemia with decreased antibody production and increased risks of infections [1,2,3,4]. In addition to onco-hematologic malignancies, autoimmune diseases are becoming one of the most prevalent causes of SID and secondary antibody deficiency (SAD). B cells play a pivotal role in both cases [1,5].
Germinal center B cells proliferate quickly and, due to their mutagenesis program, can transform normal cells into cancer cells. Thus, reagents that bind to B cell surface glycoproteins, such as CD20+, have been widely used to target B cell lymphomas by removing cancerous and non-cancerous CD20+ cells [4]. Anti-CD20-mediated B cell depletion has also been well documented for the treatment of autoimmune diseases such as nephrotic syndrome (NS), systemic lupus erythematosus, rheumatoid arthritis, immune thrombocytopenia (ITP), autoimmune hemolytic anemia, anti-neutrophil cytoplasmic antibody-associated vasculitis, myasthenia gravis, and autoimmune bullous dermatoses [5].
Rituximab (RTX) and bispecific antibody treatments targeted against B lymphocytes may induce hypo-γ-globulinemia and reduce antibody production and have been widely reported in different diseases such as onco-hematologic malignancies and autoimmune diseases. Low IgG levels after treatment with RTX have been reported; 27% to 50% in children and 3.5% to 40% in adults [6,7]. Several risk factors have been reported to induce hypo-γ-globulinemia after treatment with RTX. Low baseline serum immunoglobulin level; the number of RTX treatment cycles (i.e., longer-term RTX treatment); association with glucocorticoids; mycophenolate mofetil; cyclophosphamide; purine analogs; fludarabine; younger age in children, and older age in adults. The potential risk for increasing infectious disease complications with monoclonal antibodies used in cancer therapy and autoimmune diseases has been a preoccupation of physicians since their introduction in clinical practice [6,7].
Immunoglobulin replacement therapy (IGRT) for secondary hypo-γ-globulinemia is increasing worldwide [2]. In developing countries in Latin America, not all doctors are prepared to diagnose SIDs and to deal with hypo-γ-globulinemia after treatment with immunosuppressors. Currently, consensus guidelines are not available, and the European guidelines are followed [8]. In Brazil, immunoglobulin replacement therapy is reserved mainly for regional centers. SIDs are underdiagnosed although more prevalent than IEIs, and doctors have difficulties directing these patients to reference centers [9]. In the western region of São Paulo state, the Regional Hospital of Presidente Prudente (RH) has been the reference center for immunotherapy since 2014 for patients of the Unified Health System (SUS). Here, our aim was to determine the SAD profile of patients in a mesoregion followed in a public reference center and a private specialized clinic of São Paulo state, focusing on infectious diseases.
2. Materials and Methods
2.1. Regional Characteristics
2.2. Demographic, Clinical, and Laboratory Characteristics of the Participants
This retrospective, long-term study cohort included 20 patients between January 2014 and December 2023 living in different municipalities of RNHA11, with a diagnosis of secondary immunodeficiencies, who were treated with different regimens. The patients were followed in the immunodeficiency outpatient clinic of the Regional Hospital of Presidente Prudente and in a specialized private clinic located in Presidente Prudente, Sao Paulo state, Brazil. Participants' demographics, baseline clinical characteristics, different treatment regimens, and laboratory data, including serum electrophoresis, immunophenotyping blood counts, and immunoglobulin (Ig) levels after chemotherapy, were abstracted from electronic health records. Infections were further classified as organ-specific infections and severity was graded as mild, moderate, life-threatening, or fatal. Mild infection was defined as requiring oral antimicrobial therapy; moderate infection the patient was hospitalized; life-threatening infection was defined as the presence of end-organ or cardiovascular compromise and treatment in Intensive Care Unit; in fatal infection the patient died.
2.3. Immunoglobulin Replacement
Immunoglobulin replacement, endovenous or subcutaneous, when indicated, was given at a 28-day interval, and few patients received IgG replacement at intervals longer than 28 days. Patients followed at RH received different brands and quantities of immunoglobulin (5 g/50 mL or 5 g/100 mL) as provided by SUS. Patients treated in the private clinic received Endobulin Kiovig 10% (Takeda Pharmaceutical) or recombinant human hyaluronidase-facilitated subcutaneous immunoglobulin (HyQvia, Takeda Pharmaceutical). The initial dose was 400 mg/kg and was adjusted when necessary.
2.4. Inclusion and Exclusion Criteria
Only patients defined with SAD were screened. There is an enigmatic border between primary and secondary immunodeficiencies. In these situations, the case was discussed with a professional from the Immunodeficiencies Reference Center of Children's Hospital (ICr), HCFMUSP, São Paulo, Brazil. Patients treated in Presidente Prudente but followed in other centers were excluded.
2.5. Statistical Analysis
The results are shown as means ± standard deviation (SD) (for normally distributed variables) and confidence intervals (95% CIs). Dichotomous and nominal variables are expressed as frequencies and percentages. Statistical analysis was performed using GraphPad (San Diego, CA, USA, version 8.2.1) and GraphPad InStat 3 (San Diego, CA, USA).
2.6. Study Approval
This study was approved by the Ethics Committee of the University of Oeste Paulista, Presidente Prudente, São Paulo, Brazil (number 8008; 08/11/2023).
3. Results
3.1. Demographics, Clinical, and Laboratory Characteristics of the Participants at Baseline
The most frequent form of SAD was NHL (30%) followed by NS (25%); CLL (20%); MM (15%), protein-losing enteropathy (5%), and ITP (5%). The mean age was 41.87±27.63 years (95% CI, 28.56–55.19 years). When distributed by groups, patients with NS were younger than patients with NHL (13.40±4.82 years; interquartile range [IQR], 7.40–19.39 years vs 66.83±11.02 years; IQR, 55.26–78.39 years), CLL (66.75±11.35 years; IQR, 47.68–83.82 years), and MM (52.0±10.58; IQR, 25.71–78.29 years). Males were more prevalent than females with a ratio of 1.5:1, and European descendants were found in higher numbers. Hematologic malignancies accounted for 13 patients (65.0%), followed by autoimmune diseases in 6 patients (30.0%) and metabolic disorders in 1 patient (5.0%). At baseline, the mean IgG levels were 389.6±185.20 mg/dL (95% CI, 302.9–476.3 mg/dL), and 60.0% of patients had an IgG level <400 mg/dL. The mean IgA level was 52.04±54.46 mg/dL (95% CI, 24.04–80.05 mg/dL), and 55.0% of the patients had an IgA level <40 mg/dL. Patient 6 was excluded due to MM hyper-γ-globulinemia induced by IgA (2.210 mg/dL). Of 17 patients available for γ-globulins, 16 (94.1%) had hypo-γ-globulinemia. The mean γ-globulin levels were 0.357±0.20 (95% CI, 0.25–0.46). The mean CD19 level was 120.0±156.2 cells/mm3 (95% CI, 39.71–200.3 mm3) (normal range in children, >200 mm3; adults, >140 mm3) (Table 1). There were no differences between public and private services regarding the origin of the patients and the replacement of immunoglobulin. The prevalent route of replacement of immunoglobulin was endovenous, however, four patients received the subcutaneous form (Table 1). Concerning treatment, RTX was used in 9 (45%) patients (Table 2). Immunological markers were analyzed separately (Figure 2). Most patients showed IgG levels <400 mg/dL in all groups, but notably in the NHL group (Figure 2A). Similar results were found for IgA and γ-globulin levels (Figure 2B,C). In the patients with hematologic malignancies, after treatment with RTX/ibrutinib and teclistamab, 91.0% showed hypo-γ-globulinemia, 84.7% had low levels of IgG, and 72.3% had low levels of CD19. However, when CD19 was analyzed, these cells were not found in 4/6 (67.0%) patients with NHL (Figure 2D). Considering the main risk factors for NHL (age, >65 years old; gender, male, ethnicity, white), 50.0% of our patients were older than 65 years; all of them were white; and 50.0% were men.
3.2. Impact of Infections on Patients with Secondary Antibody Deficiency after Treatment with Immunosuppressants
Table 2 shows the impact of infections at baseline after treatment with immunosuppressants and before the replacement of intravenous immunoglobulin. In twenty patients analyzed, there were 101 infection events (62 bacterial, 31 viral, and 6 fungal). Most of the infections, 83/101 (82.1%) were classified as mild or moderate, 8 (7.92%) as life-threatening, and 2 (1.9%) as fatal. Pneumonia was the most prevalent and accounted for 20 cases (19.8%), followed by 14 cases of sinusitis (13.8%); 10 cases of sepsis (9.9%); 9 cases of urinary tract infection (8.9%); 8 cases of tonsillitis (7.9%); 8 cases of herpes simplex (7.9%), 7 cases each of herpes zoster, gastroenteritis, and COVID-19 (6.9%), 6 cases of skin mycosis (5.9%); 1 tongue lesion and I case of otitis (1.0%). When the infections were distributed by organ involvement, respiratory tract infections were more prevalent accounting for 42 cases (41.6%) followed by 21 cases of skin disease and 21 cases of soft tissue infection (20.8%). A significant number of infections with dengue virus (2.9%) and COVID-19 (6.9%) was found. The number of patients with infections by organs is shown in Figure 3. A higher mean number of infections distributed by the diagnosis group was found for NHL, 7.00±3.89 (IQR, 2.90–11.09), followed by 5.25±4.64 (IQR, −2.13 to 12.64) for CLL, 3.66±3.51 (IQR, −5.05 to 12.39) for MM, and 3.00±4.47 (IQR, −2.55 to 8.55) for NS. Patients with NS showed significantly lower levels of infections than those with NHL (43 vs 15; P=0.0001). Patient 8 is a child who moved from Presidente Prudente to another state and was lost to follow-up, patient 16 was also lost to follow-up. Patient 19 died at the age of 6 months and patient 15 died at 65 years of age.
4. Discussion
The main findings of the study show that onco-hematologic malignancies and autoimmune diseases accounted for 65% and 30% of cases, respectively; hypo-γ-globulinemia was present in 94.1%, and 101 infection events were found.
Regarding the demographic characteristics of the study population, the patients with NS were younger than those with NHL, CLL, and MM. NS is the most common glomerular disease in the pediatric age group, and most patients progress until adulthood [10]. Age is the single biggest risk factor for hematologic malignancies. In Europe, the median age at diagnosis across all hematologic malignancies is 69 years and the incidence generally increases with age, reaching a maximum at 75–99 years [11]. In our study, males were found to be more prevalent than females in a ratio of 1.5:1. Males are at increased risk of hematologic malignancies and have a worse prognosis with consistently poorer survival compared with females. According to the GLOBOCAN statistics, currently, 304,151 males versus 240,201 females have NHL; 98.613 versus 77.791 have MM [12]. In a study conducted in Martinica, the incidence of hematologic malignancies was higher in males, with rates close to 6 per 100,000 for MM and NHL, compared with 5 per 100,000 for females [13]. In São Paulo state, the adjusted rate of incidence of NHL per 100,000 men is estimated to be 5.38–9,47 for males and 3.60–359 for females for 2023 [14]. The reasons for increased cancer susceptibility for hematologic malignancies in men are not well understood. In a recent review, possible causes include differences in environmental exposures, lifestyle, endogenous hormones, sex chromosomes, epigenetics, and probably complex multidirectional interactions between these factors [14]. In our cohort, the underlying risk factors were not addressed. Another interesting finding was that 50% of the patients were European and 10% were of Asian descent. The ethnic and racial composition of Brazilian society is the result of a confluence of people from several different ethnic origins, making it difficult to compare with other countries. No differences were found in the number of patients treated in the private specialized clinic compared with the public reference center, highlighting the role of RH in the diagnosis and treatment of patients with SAD in the context of RRAS11.
Hematologic malignancies accounted for 65.0% of cases of SAD; NHL was more prevalent (30.0%) than CLL (20%) and MM (15%). In Brazil, NHL is also the more prevalent hematologic malignancy. In 2023, 10,180 new cases of NHL were diagnosed in the country and were more prevalent in men [14]. According to GLOBOCAN, in 2020, the incidence of NHL was 544,352 cases and 176,404 cases for MM [12]. However, these results are different from studies on hematologic malignancies in Martinique, in which 47.8% were MM and 36% were NHL [13]. Due to a diverse class of B cell and T cell proliferation, NHL is the most common hematologic malignancy worldwide, accounting for nearly 3% of cancer diagnoses and deaths; it is the seventh most prevalent cancer and has the sixth highest mortality rate among cancers in the United States [15]. Among the non-modifiable risk factors, age >65 years has a more than double cumulative lifetime risk; white and non-Hispanic race/ethnicity has a higher risk, and family history, immunosuppression, and autoimmune diseases have been associated with various subtypes of NHL [15]. All our patients with NHL were white, representing the only risk factor, and only one patient was diagnosed with autoimmune disease (hypothyroidism). No previous immunosuppression was found before the diagnosis of NHL and treatment with RTX.
In our patients with hematologic malignancies, after treatment with RTX/ibrutinib and teclistamab, 91.0% showed hypo-γ-globulinemia, 84.7% had low levels of IgG, and 72.3% had low levels of CD19. Our findings on hypo-γ-globulinemia are higher than reported in other studies in which persistent or transient hypo-γ-globulinemia was expected after treatment with anti-CD20 biologics. In a study on RTX-associated hypo-γ-globulinemia in patients with multi-system autoimmune disease, 56% had hypo-γ-globulinemia during follow-up [16]. In a large cohort of patients treated with RTX who presented normal, mild, or moderate hypo-γ-globulinemia before treatment, 63.9% evolved to moderate or severe hypo-γ-globulinemia after RTX treatment [17,18]. One reason why these results were so different from ours may be the different pathologies among the patients. Different autoimmune diseases were screened, and the subgroups included hematologic malignancies (NHL and CLL), autoimmune/rheumatologic diseases, hematologic conditions, and primary immunodeficiencies [19,20]. Some probable mechanisms are suggested for RTX-induced hypo-γ-globulinemia, such as impaired immune recovery that halted differentiation from naive to memory B cells, increased B cell apoptosis, and altered T lymphocyte homeostasis [16].
A total of 101 infections were registered in patients with SAD; 82.1% were classified as mild or moderate, 7.9% as life-threatening, and 1.9% as fatal (two patients died from sepsis). Our study presents similar results to those for patients treated with CART-cells therapy, in which 71% of all infections were considered mild to moderate [20]. In a large cohort of 1261 patients treated with RTX for different pathologies, 28.2% had severe infections after treatment [17]. In our study, pneumonia was the most prevalent infection followed by sinusitis. When the infections were distributed according to organ involvement, respiratory tract infections were more prevalent, followed by skin and soft tissue infections, triggered mainly by herpes simplex and herpes zoster viruses. Among hematologic malignancies, NHL showed a higher mean prevalence of infection, followed by CLL and MM. In line with our results, increased rates of respiratory tract infections, pneumonia, and sinusitis were demonstrated in patients with NHL treated with RTX [6]. Respiratory tract infections were the most common infection observed in patients with SID treated with different biologics and immunomodulatory therapies, including tumor necrosis factor-α inhibitors, interleukin-12/interleukin-23 inhibitors, anti-T-lymphocyte therapies, anti-B-lymphocyte therapies [21]. The mechanisms underlying RTX-induced respiratory tract infections are unclear, but abnormalities in IL-2 production and IL-2R expression, associated with decreased antigen-induced lymphocyte proliferation, late-onset neutropenia, and delayed onset cytopenia are described [21].
One of the most important findings in our study was the significant number of patients with NS accounting for 30.0% of cases of infection. Four of our patients (80.0%) were treated with RTX, however, hypo-γ-globulinemia, low levels of IgG, and CD19 were present in all patients before the treatment. Although hypo-γ-globulinemia in NS is regarded as a risk factor for infections, our patients showed lower levels compared with NHL (P=0.0001). Our results are in line with 140 patients with childhood-onset idiopathic steroid-sensitive nephrotic syndrome treated with RTX; hypo-γ-globulinemia was not associated with an increase or the severity of infections [22]. NS is characterized by proteinuria, hypoalbuminemia, hyperlipidemia, generalized edema, and hypo-γ-globulinemia is a frequent finding. Some probable mechanisms leading to this phenomenon are suggested, such as the relapsing course, often triggered by infections or allergies, the response to immunosuppressive regimens, such as steroids, cyclophosphamide, and cyclosporine, and the absence of structural abnormalities of the glomerular basement membrane. Hypo-γ-globulinemia was believed to be caused by urinary loss of IgG, however, it is known that the parallel increase in IgM suggests a defect in the switch from IgM to IgG synthesis due to an unknown immunologic defect, leading to low levels of immunoglobulins [11].
The main strength of this study was the inclusion of different types of SAD in the cohort who received different immunosuppressive agents. As far as we know, no data with these characteristics have been published before. Our region harbors a great number of small municipalities in a developing region with a regional health reference center, therefore the study has global relevance and may be applied in Brazilian regions or countries with similar social and epidemiological characteristics to RRAS11.
Several shortcomings must be mentioned. Some immunologic data were lost because some patients moved from RRAS-11 or died at the beginning or during the follow-up. The duration of the study varied for each patient, generating a bias in the results. Some groups had very few patients such as MM, autoimmune thrombocytopenia, and protein-losing enteropathy. The low number of patients assessed in these analyses allows for low statistical power. It is a retrospective analysis, subject to selection and misclassification bias.
5. Conclusion
In our cohort, most patients progressed to hypo-γ-globulinemia and low levels of IgG and CD19 after treatment with immunosuppressants, and mild and moderate infections were predominant. These therapies are increasing in different diseases, and in developing countries, therefore monitoring hypo-γ-globulinemia and infections may help to identify patients at high risk for severe complications by introducing antibiotic prophylaxis or treatment, and immunoglobulin replacement. Furthermore, the study shows the importance of public reference hospitals in the diagnosis and treatment of SAD patients from SUS in Brazil.
Author Contributions
Conceptualization, L.E.P.C.; methodology, L.E.P.C.; formal analysis, L.E.P.C.; writing—original draft preparation, L.E.P.C.; writing—review and editing, L.E.P.C., P.A.M.C., D.F.H.B.T., J.A.N.B., A.C.G.P., P.H.M., F.M.C.S. and M.D.F.
Funding
This research received no external funding.
Institutional Review Board Statement
Permission to conduct the study and its publication was obtained from the Institutional Ethics Committee of the University of Oeste Paulista (protocol 8008 approved on November 7, 2023).
Informed Consent Statement
Informed consent was obtained from all patients involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Tuano KS, Seth N, Chinen J. Secondary immunodeficiencies: An overview. Ann Allergy Asthma Immunol. 2021;127(6):617-626. [CrossRef]
- Sánchez-Ramón S, Bermúdez A, González-Granado LI, Rodríguez-Gallego C, Sastre A, Soler-Palacín P; ID-Signal Onco-Haematology Group. Primary and Secondary Immunodeficiency Diseases in Oncohaematology: Warning Signs, Diagnosis, and Management. Front Immunol. 2019; 26;10:586. [CrossRef]
- Kaplan B, Bonagura VR. Secondary Hypogammaglobulinemia: An Increasingly Recognized Complication of Treatment with Immunomodulators and After Solid Organ Transplantation. Immunol Allergy Clin North Am. 2019;39(1):31-47. [CrossRef]
- Axelrod H, Adams M. Biologic Agents and Secondary Immune Deficiency. Immunol Allergy Clin North Am. 2021;41(4):639-652. [CrossRef]
- Crickx E, Weill JC, Reynaud CA, Mahévas M. Anti-CD20-mediated B-cell depletion in autoimmune diseases: successes, failures and future perspectives. Kidney Int. 2020;97(5):885-893. [CrossRef]
- de Souza KJ, Ferro RS, Prestes-Carneiro LE, Carrilho PAM, Vasconcelos DM. Infectious diseases and immunological markers associated with patients with non-Hodgkin lymphoma treated with rituximab. Immunopharmacol Immunotoxicol. 2018;40(1):13-17. [CrossRef]
- Stabler S, Giovannelli J, Launay D, Cotteau-Leroy A, Heusele M, Lefèvre G, Terriou L, Lambert M, Dubucquoi S, Hachulla E, Sobanski V. Serious Infectious Events and Immunoglobulin Replacement Therapy in Patients With Autoimmune Disease Receiving Rituximab: A Retrospective Cohort Study. Clin Infect Dis. 2021;72(5):727-737. [CrossRef]
- Jolles S, Michallet M, Agostini C, Albert MH, Edgar D, Ria R, Trentin L, Lévy V. Treating secondary antibody deficiency in patients with haematological malignancy: European expert consensus. Eur J Haematol. 2021;106(4):439-449. [CrossRef]
- Boton Pereira DH, Primo LS, Pelizari G, Flores E, de Moraes-Vasconcelos D, Condino-Neto A, Prestes-Carneiro LE. Primary Immunodeficiencies in a Mesoregion of São Paulo, Brazil: Epidemiologic, Clinical, and Geospatial Approach. Front Immunol. 2020;11:862. [CrossRef]
- Han JW, Lee KY, Hwang JY, Koh DK, Lee JS. Antibody status in children with steroid-sensitive nephrotic syndrome. Yonsei Med J. 2010 Mar;51(2):239-43. Epub 2010 Feb 12. PMID: 20191016; PMCID: PMC2824870. [CrossRef]
- Ben-Batalla I, Vargas-Delgado ME, Meier L, Loges S. Sexual dimorphism in solid and hematological malignancies. Semin Immunopathol. 2019 Mar;41(2):251-263. Epub 2018 Oct 25. [CrossRef]
- World Health Organization, International Agency for Research on Cancer, Global Cancer Observatory. Available online: https://gco.iarc.fr/en (accessed on 23 January 2023).
- Houpert R, Almont T, Belahreche R, Faro M, Okouango J, Vestris M, Macni J, Pierre-Louis O, Montabord C, Beaubrun-Renard M, Soumah N, Boisseau M, Véronique-Baudin J, Joachim C. A population-based analysis of hematological malignancies from a French-West-Indies cancer registry's data (2009-2018). BMC Cancer. 2023;23(1):1197. [CrossRef]
- Ministério da Saúde, Instituto Nacional de Câncer Incidência de Câncer no asil. Available online: https://www.inca.gov.br/sites/ufu.sti.inca.local/files/media/document/estimativa-2023.pdf (accessed on 10 February 2023).
- Thandra KC, Barsouk A, Saginala K, Padala SA, Barsouk A, Rawla P. Epidemiology of Non-Hodgkin's Lymphoma. Med Sci (Basel). 2021;9(1):5. [CrossRef]
- Roberts DM, Jones RB, Smith RM, Alberici F, Kumaratne DS, Burns S, Jayne DR. Rituximab-associated hypogammaglobulinemia: incidence, predictors and outcomes in patients with multi-system autoimmune disease. J Autoimmun. 2015 Feb;57:60-5. Epub 2014 Dec 31. PMID: 25556904. [CrossRef] [PubMed]
- Barmettler S, Ong MS, Farmer JR, Choi H, Walter J. Association of Immunoglobulin Levels, Infectious Risk, and Mortality With Rituximab and Hypogammaglobulinemia. JAMA Netw Open. 2018 Nov 2;1(7):e184169. PMID: 30646343; PMCID: PMC6324375. [CrossRef]
- Ottaviano G, Sgrulletti M, Moschese V. Secondary rituximab-associated versus primary immunodeficiencies: The enigmatic border. Eur J Immunol. 2022;52(10):1572-1580. [CrossRef]
- Roberts DM, Jones RB, Smith RM, Alberici F, Kumaratne DS, Burns S, Jayne DR. Rituximab-associated hypogammaglobulinemia: incidence, predictors and outcomes in patients with multi-system autoimmune disease. J Autoimmun. 2015 Feb;57:60-5. Epub 2014 Dec 31. PMID: 25556904. [CrossRef] [PubMed]
- Wudhikarn K, Palomba ML, Pennisi M, Garcia-Recio M, Flynn JR, Devlin SM, Afuye A, Silverberg ML, Maloy MA, Shah GL, Scordo M, Dahi PB, Sauter CS, Batlevi CL, Santomasso BD, Mead E, Seo SK, Perales MA. Infection during the first year in patients treated with CD19 CAR T cells for diffuse large B cell lymphoma. Blood Cancer J. 2020;10(8):79. [CrossRef]
- Cannon L, Pan A, Kovalick L, Sarkissian A, Wu EY. Secondary immunodeficiencies and infectious considerations of biologic immunomodulatory therapies. Ann Allergy Asthma Immunol. 2023 Jun;130(6):718-726. Epub 2023 Feb 18. PMID: 36801438; PMCID: PMC10247415. [CrossRef]
- Han JW, Lee KY, Hwang JY, Koh DK, Lee JS. Antibody status in children with steroid-sensitive nephrotic syndrome. Yonsei Med J. 2010;51(2):239-43. [CrossRef]
Figure 1.
The study setting.
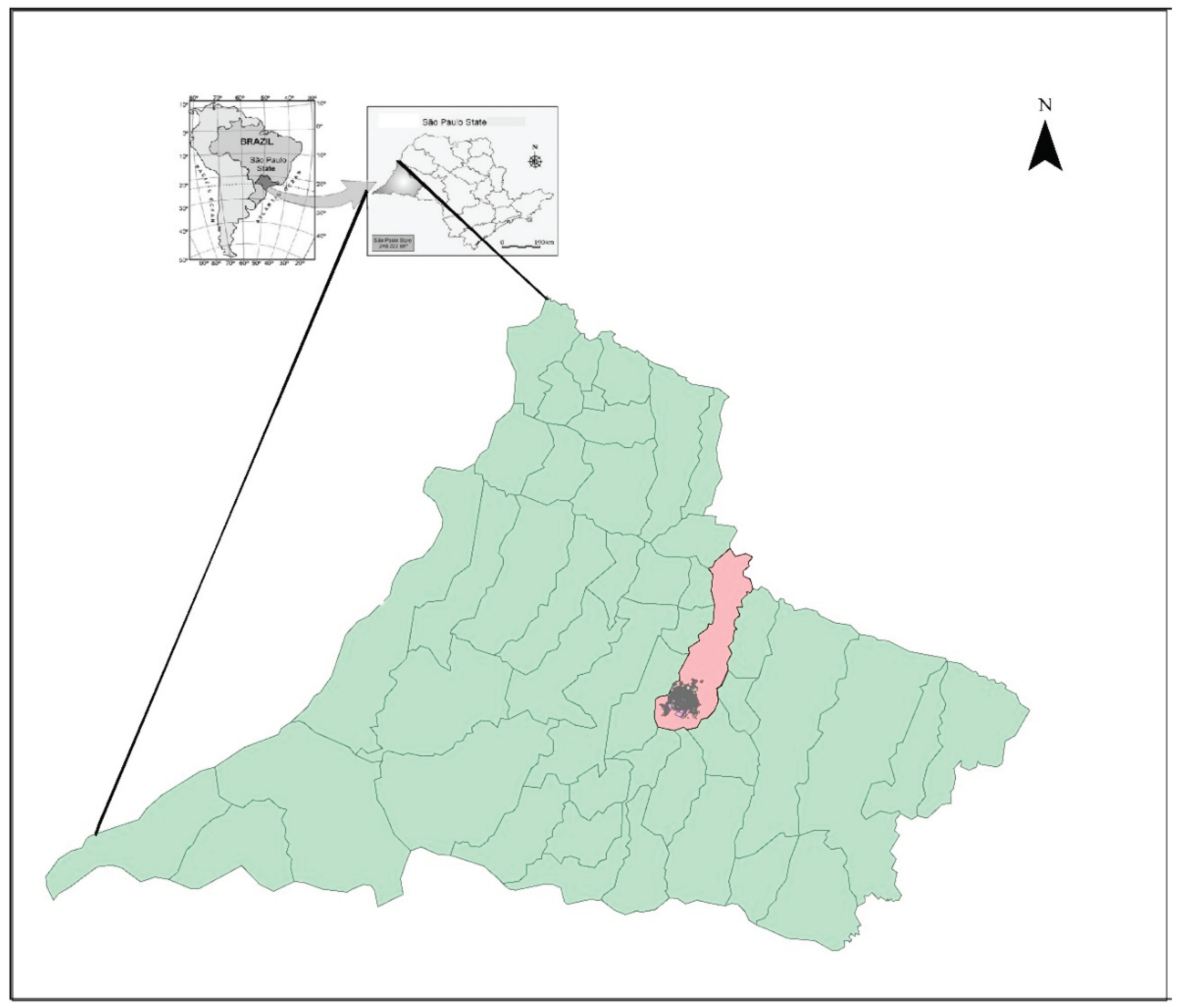
Figure 2.
Immunological markers in different groups of patients with secondary immunodeficiency.
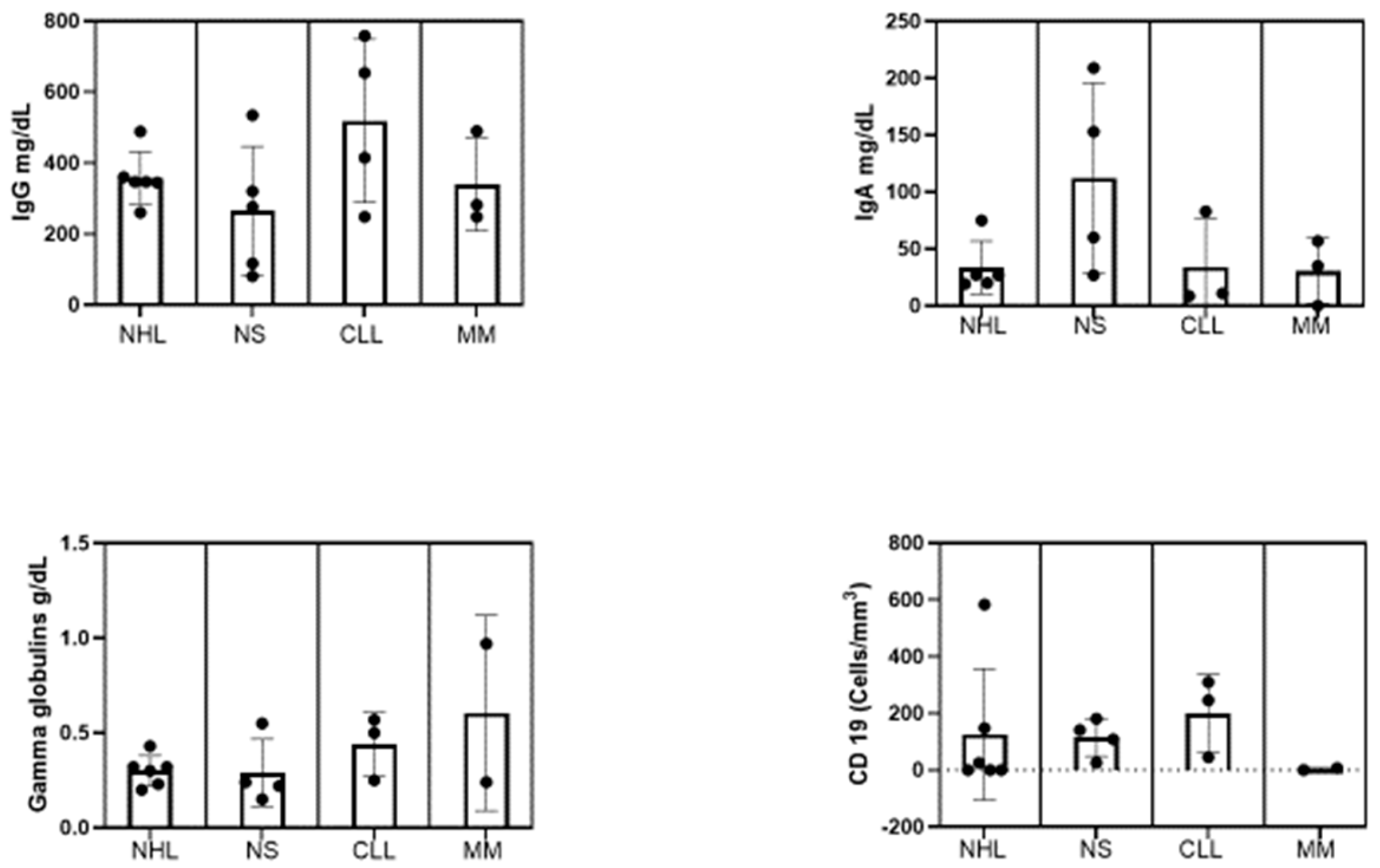
Figure 3.
Distribution of infections by organs.
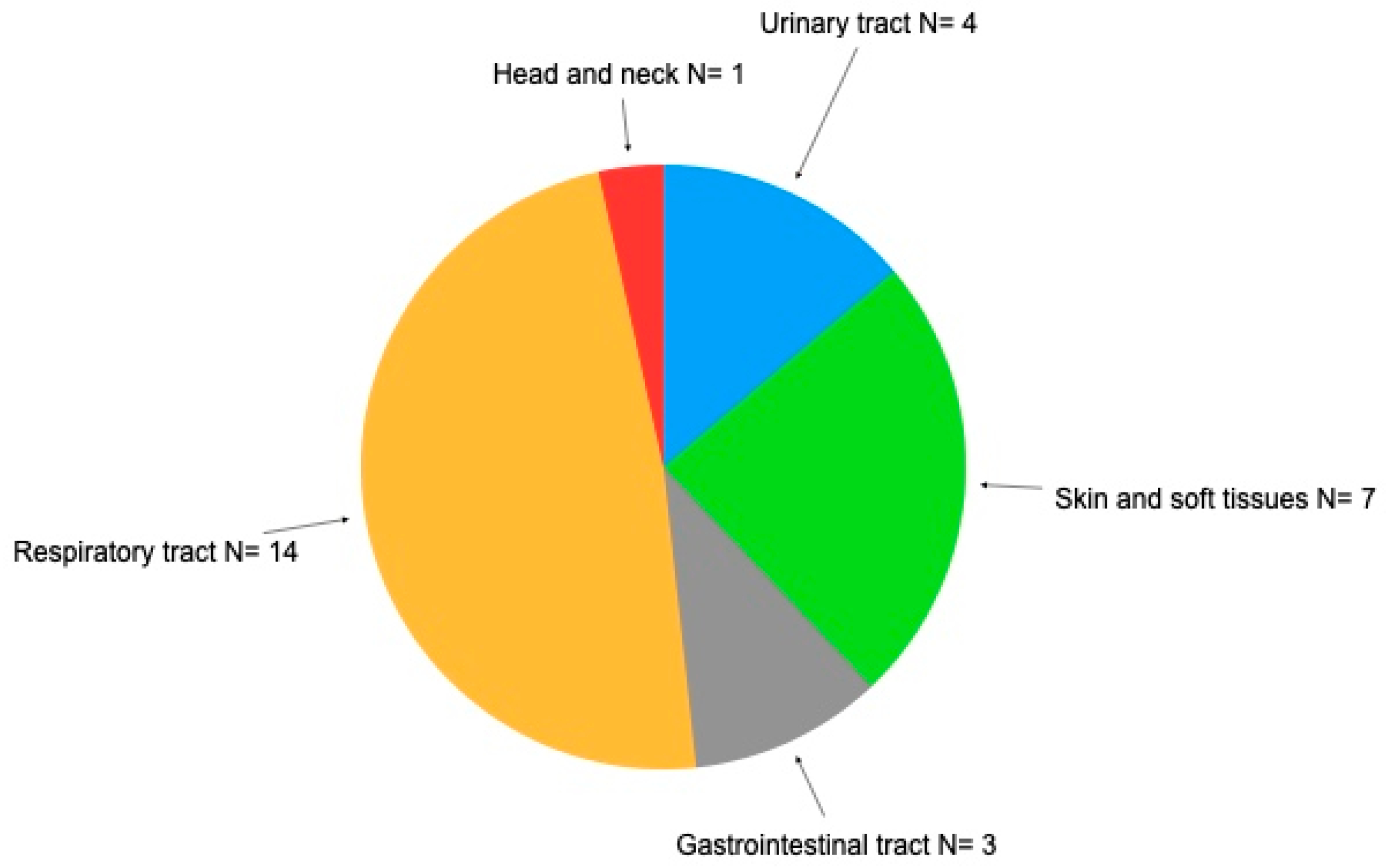

Table 1.
Immunologic markers, pathology, cell target therapy, and drug used.
| No. | IgG (mg/dL) | IgA (mg/dL) | γ-Globulins (g/dL) | CD19 (cells/mm3) | Pathology | Target | Drug use |
|---|---|---|---|---|---|---|---|
| 1 | 360 | 27 | 0.30 | 0 | NHL | Anti-CD-20 | Rituximab |
| 2 | 489 | 75 | 0.43 | 584 | NHL | Anti-CD-20 | Rituximab |
| 3 | 260 | 27.2 | 0.23 | 25 | NHL | Anti-CD-20 | Rituximab |
| 4 | 345 | 19.2 | 0.32 | 0 | NHL | Anti-CD-20 | Rituximab |
| 5 | 347 | 20 | 0.32 | 148 | NHL | BTK | Ibrutinib |
| 6 | 347 | 2210 | 0.20 | 00 | NHL | BTK | Ibrutinib |
| 7 | 117 | 153 | 0.22 | 141 | NS | Anti-CD-20 | Prednisone |
| 8 | 320 | NA | NA | NA | NS | Anti-CD-20 | Prednisone |
| 9 | 535 | 209 | 0.55 | 26 | NS | IMPDH | Prednisone;/mycophenolate |
| 10 | 276 | 27 | 0.24 | 109 | NS | Anti-CD-20 | Prednisone |
| 11 | 81 | 60 | 0.15 | 181 | NS | Anti-CD-20 | Prednisone |
| 12 | 248 | 10.9 | 0.24 | 246 | CLL | Anti-CD-20 | Rituximab |
| 13 | 654 | 8.73 | 0.70 | 45 | CLL | Anti-CD-20 | Rituximab |
| 14 | 759 | 83 | 0.97 | 310 | CLL | Anti-CD-20 | Rituximab |
| 15 | 415 | NA | NA | NA | CLL | Anti-CD-20 | Rituximab; ibrutinib |
| 16 | 490 | 35 | 0.50 | NA | MM | DNA | Cyclophosphamide;talidomid |
| 17 | 248 | 57 | 0.57 | 7 | MM | Anti-CD-20 | Rituximab |
| 18 | 282 | 0 | 0.25 | 0 | MM | BCMA/CD3 | Teclistamab |
| 19 | 76 | 33 | 0.11 | 218 | PD | 0 | No imunossupressor |
| 20 | 460 | 39.7 | 0.35 | 0 | ITP | Anti-CD-20 | Rituximab |
NHL, non-Hodgkin lymphoma; BTK, Bruton tyrosine kinase; NS, nephrotic syndrome; IMPDH, inosine monophosphate dehydrogenase; CLL, chronic lymphocytic leukemia; MM, multiple myeloma; BCMA, B cell maturation antigen; PLE, Protein-losing enterophaty; ITP, immune thrombocytopenia; NA, not available.
Table 2.
Patient demographics, clinical and laboratory characteristics.
| Participants (N=20) | n (%) | Mean±SD | 95% Confidence interval | |
|---|---|---|---|---|
| Age (years) | <18 | 7 (35) | 10.80±7.29 | 4.05–17.54 |
| 18–60 | 7 (35) | 49.29±12.74 | 37.51–61.07 | |
| ≥60 | 6 (30) | 70.83±8.25 | 62.17–79.50 | |
| Gender | Female | 8 (40) | ||
| Male | 12 (60) | |||
| Race | European | 10 (50) | ||
| South American | 6 (30) | |||
| African | 2 (10) | |||
| Asian | 2 (10) | |||
| SID type | Non-Hodgkin lymphoma | 6 (30) | ||
| Nephrotic Syndrome | 5 (25) | |||
| Chronic lymphocyte leukemia | 4 (25) | |||
| Multiple myeloma | 3 (15) | |||
| Protein-losing enteropathy | 1 (5) | |||
| Immune thrombocytopenia | 1 (5) | |||
| Baseline immunoglobulin (mg/dL) | IgG<400 | 12 (60) | 269.3±89.67 | 212.3–326.2 |
| IgG≥400 | 8 (40) | 570.1±135.7 | 456.7–683.5 | |
| IgA<6.0 | 1(5) | – | – | |
| IgA>6.1<40 | 10 (50) | 24.77±10.08 | 17.56–31.98 | |
| >41 | 7 (35) | 406.7±797.1 | -1474.5 | |
| γ-Globulins (g/dL) | <0.70 | 19 (95) | 0.31±0.12 | 0.25–0.38 |
| >0.70 | 1 (5) | 0.97 | ||
| CD19+ B cell count (cells/mm3) | >20 | 11 (55) | 1.16±2.85 | 1.83–4.06 |
| ≤20 | 6 (30) | 184.8±161.0 | 76.66–293 | |
| NA | 3 (15) | |||
| Origen of the service | Public | 10 (50) | ||
| Private | 10 (50) | |||
| IgG replacement | Endovenous | 12 (60) | ||
| Subcutaneous | 4 (25) | |||
| Not indicated | 4 (25) |
SD, standard deviation; SID, secondary immunodeficiency.
Table 3.
Infections in different sites in patients diagnosed with secondary immunodeficiency (2014–2023).
Table 3.
Infections in different sites in patients diagnosed with secondary immunodeficiency (2014–2023).
| Patient number | ||||||||||||||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | |
| Infection sites | ||||||||||||||||||||
| Respiratory | + | +++ | + | ++ | + | |||||||||||||||
| Amigdalitis | ++++ | + | +++ | ++ | ++ | ++ | + | |||||||||||||
| Sinusitis | ++ | |||||||||||||||||||
| Otitis | + | +++ | ++ | + | +++ | + | +++ | +++ | ||||||||||||
| Pneumonia | + | |||||||||||||||||||
| Skin diseases and soft tissues | ||||||||||||||||||||
| Herpes simplex | ++ | +++ | +++ | |||||||||||||||||
| Herpes zoster | ++ | + | + | +++ | ||||||||||||||||
| Skin mycosis | +++ | +++ | ||||||||||||||||||
| Head and neck | ||||||||||||||||||||
| Tongue lesion | ++ | |||||||||||||||||||
| Other | ||||||||||||||||||||
| Gastroenteritis | - | +++ | +++ | + | ||||||||||||||||
| Urinary tract infection | +++ | + | +++ | ++ | ||||||||||||||||
| Dengue infection (number) | + | + | + | |||||||||||||||||
| Covid-19 infection (number) | ++ | + | + | + | ++ | |||||||||||||||
| Sepsis | + | + | + | ++ | ++ | +++ | ||||||||||||||
| Severity of infections | ||||||||||||||||||||
| Mild | + | + | + | + | + | + | + | |||||||||||||
| Moderate | + | |||||||||||||||||||
| Life-threatening | + | + | + | + | + | + | + | + | ||||||||||||
| Fatal | + | + | ||||||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



