
Submitted:
03 March 2024
Posted:
05 March 2024
You are already at the latest version
Abstract
To study the spatial accessibility of healthcare services in cities on the Tibetan Plateau, this paper proposes an improved 3SFCA method in the main urban area of Xining City. The improved 3SFCA method incorporates both selection weights from the Huff model and the M2SFCA approach to addressing suboptimal allocation of supply resources. Results show that the accessibility of healthcare for the main urban area of Xining City decreases in a circle to four axes, with good accessibility in the east and center but poor accessibility in the north. And there is a positive spatial relationship between population and accessibility. Besides, this paper proposes a framework for studying the spatial accessibility of healthcare on the Tibetan Plateau.
Keywords:
Tibetan Plateau
; Spatial accessibility
; 3SFCA
; healthcare service
; Xining city
1. Introduction
Healthcare services are an important part of basic public services in China and the basis for improving the health level of urban residents [12-3]. Key to residents’ fair enjoyment of medical services is the reasonable allocation of medical resources and improved utilization efficiency [4]. Spatial accessibility is an important indicator of whether scarce medical facilities and resources are allocated efficiently and distributed fairly [3,5-7]. In recent years, China’s public healthcare service capacity has been continuously improved but the gap between the east and west is still significant. The Tibetan Plateau (TP) is the most unique geographical, ecological, population-transportation unit in the world. It is characterized by high altitude, low temperature, widespread permafrost, active neotectonics, and diverse geomorphic types. Most of its cities are valley-type cities distributed in the Hehuang Valley and in the “One River and Two Streams” region of Tibet. On the TP, urban morphology is closely related to the spatial pattern of topography and geomorphology.
Healthcare services are particularly important in the development and construction of cities in the high-altitude life exclusion zone, and are also fundamental to the sustainable development of cities in high and cold regions [3,8,9]. However, due to the poor healthcare special geographical environment, and complex social factors, cities on the TP face ongoing problems regarding healthcare resources, such as low quality, unreasonable layout, low service efficiency, and a mismatch between fairness and efficiency. Therefore, scientific measurement of the accessibility of urban public healthcare services on the TP is essential to the rational allocation of medical resources in plateau cities, the improvement of urban residents’ health, the revitalization of the western region, and the high-quality development of all society.
To address shortcomings in the original 3SFCA model, this paper proposes an improved 3SFCA incorporating both selection weights from the Huff model and the M2SFCA approach to addressing suboptimal allocation of supply resources. Most of the studies cited above focus on large and medium-sized cities located on plains; few have researched plateau cities. Therefore, this paper takes Xining City on the TP as an example, and comprehensively considers its special terrain and traffic conditions, population distribution characteristics, and healthcare service capacity. We also optimize the original accessibility calculation model and basic data, and analyze the spatial accessibility of healthcare facilities in a representative plateau city. First, the population data in the study area are gridded to improve accuracy. Second, the online Amap is used to obtain travel times based on real-time road conditions for driving and public transportation. We also determine the Gaussian function as the distance attenuation function and use frequency histograms of travel time to set the search threshold, thereby improving the reliability of travel time. Third, we improve the 3SFCA model by incorporating selection weight from the Huff model and the M2SFCA approach to addressing the suboptimal allocation of supply resources of the M2SFCA model. The improved model is used to analyze the spatial accessibility of medical services in the main urban area of Xining City for people driving or taking public transportation. Finally, the spatial distribution characteristics of hospital accessibility are further evaluated by the Moran autocorrelation index. The study’s findings should inform reasonable policy suggestions for the rational layout of urban hospitals on the TP, thereby helping to improve the fairness of medical service provision for urban residents.
2. Overview of the Study Area
The Tibetan Plateau, known as the “Earth’s third pole” is a sparsely populated area in China and even the world because of its unique alpine natural environment. Healthcare services on the plateau are in a state of long-term backwardness, and the layout of medical facilities is seriously uneven [10]. Therefore, it is important to research the spatial accessibility of urban hospitals on the TP [11]. In terms of spatial scope, the TP covers six provinces and regions: Qinghai, Tibet, Gansu, Sichuan, Xinjiang and Yunnan. The central city nodes include two provincial capitals (Xining and Lhasa), five prefecture-level cities (Haidong, Changdu, Nyingchi, Shannan, and Xigaze), and seven county-level cities (Delingha, Golmud, Yushu, Hezuo, Malkang, Kangding, and Shangri-La) (Figure 1).
As a special geographical division of China, the TP is an alpine region [12]. Affected by the alpine climate, topography, and other conditions, its urban spatial form, traffic network layout, population, and medical facilities and service capacity all show unique characteristics of plateau cities (Table 1), which obviously differ from those of coastal cities [13,14]. As a typical plateau city, Xining is the only central city on the TP with a population exceeding one million.
3. Data and Method
3.1. Data
This study uses three main types of data. First is information on public healthcare l service facilities in the main urban area of Xining City. In total, there are twenty-four medical service institutions at or above the second tier, comprising fifteen comprehensive and specialized 3A-Grade hospitals, four 3B-Grade hospitals, and five 2A/B-Grade hospitals. Relevant information includes hospital locations, the building area of each hospital, the number of beds, and the number of health technicians. All data are sourced from each hospital’s official website of each hospital. Second, we use street-level population data for Chengdong, Chengzhong, Chengxi, and Chengbei districts, sourced from the Seventh National Population: these data are available on the official website of Xining Municipal People's Government. Third, this study employs multi-source street division data, including the 2021 version of a 1:250,000 topographic map of Xining City (from which residential areas were extracted), vector data of the street administrative division of main urban area, Xining City’s urban administrative division map, and hospital locations. We sourced the topographic map from the National Basic Geographic Information Center, the street administrative division data from the Qinghai Provincial Disaster Prevention Center, and the hospital location data from AmapGeocode.
3.2. Method
The overall research framework is shown (Figure 2) and comprises six main steps. The first step is data preparation and accuracy optimization. Residential areas extracted from the topographic map are gridded, then population data are distributed to each grid according to the area of street residential areas, thereby effectively improving the accuracy of population data. The second step is factor analysis to comprehensively characterize the service capacity of medical facilities. The three indicators of hospital grade, number of health technicians, and number of beds are reduced by factor analysis to calculate the comprehensive score index of each healthcare facility. In the third step, the travel time and distance between the hospital and residential area are measured for driving and taking public transportation using the AMAP API. We construct a travel-time frequency histogram to determine the search radius range. The fourth step is performing trend surface analysis of the spatial distribution pattern of population and hospital facilities in the main urban area of Xining City. In the fifth step, we calculate the accessibility of healthcare services. The basic form of the 3SFCA is first explained, then we improve it based on the Huff model, detailing the calculation process of the improved 3SFCA model with a diagram. The improved 3SFCA model is used to calculate the accessibility of each residential area. The final step is to calculate the spatial autocorrelation between hospital accessibility and the population of residential areas using the bivariate Moran autocorrelation index. We also analyze the reasons of autocorrelation.
3.2.1. Data Optimization
3.2.1.1. Population Data
Since streets are often the smallest unit in public population data, previous studies use the administrative or geometric center of a street as the demand point. For example, Liu et al. (2017) treated the village committee as the demand point of administrative villages [22], while Deng et al. (2015) treated the village administrative center as the center of residential areas and assumed the population to be evenly distributed to the street area [23]. These studies’ approaches are more applicable to eastern cities with dense and uniform population. With great restrictions imposed by the terrain, cities on the TP have small populations with a relatively scattered distribution, and there are many non-habitable areas such as mountains in the street area, leading to exaggerated regional scope. If the administrative or geometric center of a street were taken as the demand point in these cities, the potential demand center may be shifted or the demand point may be outside the search radius of healthcare facilities, leading to inaccurate accessibility calculations [24]. Both Zhang et al. (2022) and Luo (2004) show that expressing demand and supply points on a finer spatial scale can improve the accuracy of accessibility calculations [25,26]. In particular, Zhang et al. (2022) reported that 500m is suitable for expressing the difference in population distribution in local areas as grid scale [25]. Therefore, being to improve the accuracy of population data and the spatial distribution of urban population on the plateau, we take the residential area in the 1:250,000 topographic map as the population distribution range in the street, then grid residential areas, allocate street population proportionately by grid area, and take each grid’s geometric center as the demand point.
3.2.1.2. Factor Analysis of Healthcare Service Capacity
Factor analysis is a multivariate statistical method. It has been successfully applied in health sciences, psychology, sociology, economics, demography, geology, and education [27,28]. Therefore, this study uses factor analysis in SPSS 24 to calculate the comprehensive score of hospital service capacity. Three indicators are selected to measure a hospital’s healthcare service capacity: hospital grade, number of health technicians, and number of beds. Following China’s hospital grading management standards for the ratio of health technicians to beds, we assign 1.03 to 3A-Grade hospitals, 0.88 to 3B-Grade hospitals, and 0.7 to 2A/B-Grade hospitals in the standardization process. Since the final comprehensive score ranges from −4 to 5, we carry out forward processing to more intuitively represent each hospital’s service capacity and facilitate the follow-up accessibility calculation. The basic idea is to limit the comprehensive score of each hospital between 0 and 1, with higher scores denoting higher service capacity. The formula is as follows:
where, Sj is the service capacity of a healthcare facility after forward processing, Xn is the comprehensive service score of a healthcare, Xmin is the minimum comprehensive score of the 24 hospitals, and Xmax is the maximum comprehensive score of the 24 hospitals.
3.2.1.3. Calculation of Catchment Size (Search Radius)
Due to the large topographic relief and high mountains on the TP, the actual travel time between two nearby places can be very long, and the AMAP navigation system provides the best route according to road conditions, detouring where necessary. Therefore, it is in line with the actual situation to use the AMAP API real-time travel time by car and bus time as the travel cost. The specific operation is as follows: after obtaining permission in the AMAP API, we use the platform’s online map to calculate the driving travel time and distance and the bus travel time and distance between the hospital and residential area. We then generate travel-time frequency histograms (including cumulative percentage) for the two travel modes, with time intervals of 5 min for car and 30 min for bus. As shows in Figure 3, the travel time difference between driving and public transport is very large, so it is necessary to explore the accessibility difference between the two travel modes. In addition, the maximum travel time by car is not more than 60min, while the travel time by bus is less than 150 min in 90% of the main urban areas of Xining City. Considering the dispersed population distribution on the TP and the large distance between the urban edge and the urban center road network, we define the maximum travel time, and thus the search range thresholds, for car and bus as 60 min and 150 min respectively [28]. This ensures that value of 90% travel time in the region is within the threshold range.
3.2.2. Spatial Trend Surface Analysis
This paper uses trend surface analysis in GIS to intuitively express the spatial distribution of residential areas and medical resources and facilities in the main urban area of Xining City (Figure 4). The population is mainly concentrated in the east of the old urban area. For hospitals, comprehensive service capacity is also high in the east and middle but low in the west, north, and south. Hospitals with strong medical service capacity are mainly distributed the middle of Chengdong District, and there are almost no 2-Grade and upgrad hospitals in the middle and north of the city.
3.2.3. Accessibility Model of Healthcare Services
3.2.3.1. 3SFCA Algorithm
The original 3SFCA was proposed by Wan et al. (2012) to minimize the overestimation of medical needs in the 2SFCA and extended 2SFCA model [29]. When multiple supply points are located within the search radius of a demand point, there is a competitive effect between supply points. Wan et al. (2012) quantitatively expressed the competitive effect as a competitive selection of supply points within the search range based on the spatial impedance function of travel cost (travel time) [29], and assigned a competitive weight (or selection weight) to each healthcare according to its spatial impedance with the demand point. The 3SFCA thus accounts for the fact that people’s demand for those particular healthcare facilities are influenced by nearby one based on the travel cost spatial impedance. Then we can calculate the demand for a healthcare facility t according to the selection weight. For this study’s purposes, the 3SFCA model is formulated in three steps.
The first step is to calculate the selection weight Cij. The search radius of the demand point is 60 min for driving, and it is divided into four sub-areas including 30 min, 20 min, and 10 min. We search for all supply points within 60 min, calculate the Gauss value of the sub-area by Gauss function in its division time range, and assign the Gauss value of the sub-area to each supply point it contains. The ratio of the Gauss value of a supply point in the search range to the sum of the Gauss values of all supply points is the selection weight between the demand point and supply point. The specific formula is as follows:
where Cij is the selection weight between demand point i and supply point j; Tij is the Gauss value of the supply point (substituting travel time for travel cost in the Gaussian distance impedance function); Tik is the Gauss value of supply point k; d0 is the driving time of 60 min; and dik is the distance between demand point i and supply point k.
The Gaussian attenuation function is as follows:
The meaning of each variable in the formula is the same as above.
The second step is to calculate the supply–demand ratio R. For driving, 60 min is the search radius of the supply point. Similarly, the search radius of 60 min is divided into four sub-areas including 30 min, 20 min, and 10 min. The search radius of the four sub-areas is taken as the time cost of the distance attenuation function, and the supply–demand ratio R between a supply point and each demand point within its search range is calculated using the following formula:
where Sj is the healthcare service capacity of the supply point j; Wr is the impedance obtained by the attenuation function of the r-th sub-areaDr; Gkj is the selection weight of the supply point; and Pk is the population of the demand point k.
The third step is to calculate the accessibility A of the demand point:
The meaning of each variable in the formula is the same as above.
3.2.3.2. Improved 3SFCA Model Based on the Huff Model
In the selection weight of supply points in formula (2), the 3SFCA model assumes that residents’ demand for a healthcare facility is affected by the travel cost from the demand point to facility or nearby healthcare facilities within the search radius. However, people consider not only the travel cost but also the service capacity of healthcare facilities will affect the residents’ demand. Therefore, Luo et al. (2014) introduced the selecting the weight of Huff model that defined as H2SFCA [30], it taking into account both travel cost and service capacity of healthcare facilities. On this basis, formula (2) can be improved as follows:
where HGij is the selection weight between demand point i and supply point j; Sj is the healthcare service capacity of supply point j; Gij is the impedance value of supply point j based on the Gaussian function (substituting travel time for travel cost); Gik is the Gaussian impedance of supply point k; d0 is the driving time of 60min; and dik is the distance between demand point i and supply point k.
The initial 3SFCA and its previous extended form assume in advance that all medical facilities have been optimally configured and reached optimal availability. In this assumed situation, the supply and demand points need to coincide. This assumption is obviously far from the actual situation, in which some healthcare services are not effectively utilized by potential demand points. Therefore, adopting from M2SFCA the approach to addressing suboptimal configuration of service supply points, a distance attenuation function is added to the accessibility calculation to make the model closer to the actual situation in the region. Formula (5) can thus be improved as follows:
Figure 5 illustrates the improved 3SFCA.
The improved 3SFCA model is used to calculate the accessibility of medical facilities for each residential area by car and bus. First, the selection weight for each facility is calculated according to the search area radius of the two travel modes (60 min for car, 150 min for bus). Next, the supply–demand ratio of medical facilities is calculated. Finally, we calculate the accessibility of medical facilities for residential areas. The calculation process was completed in Excel 2016, and mapping was performed using ArcGIS 10.7.
3.2.4. Bivariate Moran Spatial Autocorrelation Analysis
This paper uses bivariate Moran spatial autocorrelation analysis to study the spatial correlation characteristics of two variables—population number and hospital spatial accessibility—in each residential area. The global Moran index represents whether there is an overall spatial distribution correlation between population number and hospital spatial accessibility [32]. The specific formula is as follows:
where Iap is the global spatial correlation index, N is the number of spatial entities (the total number of residential areas in this paper), Wbc is the spatial weight matrix, in this paper, the population is used as the basis for weight distribution, is the standardized value for the accessibility of the b-th residential area, and is the standardized value for the population of the c-th residential area., is the accessibility of the b-th residential area, is the population of the c-th residential area, is the average accessibility of healthcare in all residential areas, is the average of population value of all residential area. The value range of global Moran index is [−1,1]. A value greater than 0 indicates that there is a positive correlation between the hospital accessibility and population density of the residential area. A larger value indicates that the clustering degree is higher and the correlation is stronger.
If the global autocorrelation index is greater than 0, then the local Moran index is used to analyze the local spatial correlation among geographical units in the region. The relationship between population and average hospital accessibility for a given location can be intuitively expressed by a Lisa cluster diagram, which can be divided into four different cluster relationships: high–high, low–low, high–low, and low–high cluster. Statistical significance indicates whether the directional relationship is obvious. In this paper, the explanatory (independent) variable is population and the explained (dependent) variable is hospital accessibility.
4. Results
4.1. Factor Analysis Results for Healthcare Service Capacity
The KMO value of 0.607 (> 0.5) indicates that there is no significant difference in the degree of correlation between variables, and that the data are suitable for factor analysis. This is reinforced by the p-value of Bartlett’s spherical test being less than 0.05, which indicates that the spherical hypothesis is rejected and there is correlation between the original variables (hospital grade, number of health technicians, and number of beds). Factor analysis results show that the cumulative variance interpretation rate of the first common factor exceeds 70%, so that factor is extracted for subsequent analysis. Next, that factor’s score is calculated by regression analysis based on the component score coefficient matrix of the first common factor in the component matrix table. The comprehensive score is then obtained according to the variance interpretation rate of the first common factor. Finally, we calculate the hospital service capacity value Sj using the forward processing formula.
4.2. Spatial Accessibility Results
The results of analysis using the improved 3SFCA model (Figure 6) show that the healthcare accessibility of in the main urban area of Xining City is distributed in a circular manner and decreases with increasing distance from the urban center in an “X” shape to a four axis direction. Affected by the special valley topography of the TP, the spatial distribution pattern of healthcare accessibility differs greatly across the main urban area of Xining City, On the whole, it spreads from the central street of the urban area with a wide river valley to the four axes with a narrow river valley in an “X” shape. Accessibility is high in the urban center and in nearby streets to the east, but low at the edge of the city including (the western edge, the northern edge and other peripheral areas of the HR Valley); it is also generally low in the north of the city.
Among the four urban areas, Chengbei District has generally lower accessibility than the other three, Xiaoqiao Street being an exception given its proximity to the central circle of the urban area. There are two main reasons for low hospital accessibility in the north and west of Chengbei District. First, the district has only two 2-Grade and upward hospitals, representing a lack of medical resources. Second, in the narrow valley where the north of the city is located, the north–south road network is sparse and traffic is congested. Whether by car or bus, residents’ travel time to the Central Hospital is long, resulting in uneven distribution of hospital accessibility in the north of Xining City.
Focusing on the two travel modes, the high-value areas of accessibility for driving and bus travel are both distributed around the central circle of the city’s east district, with accessibility declining the further out the demand point. Differences in hospital accessibility between the two travel modes are mainly explained by the traffic network. The high-value area of hospital accessibility for driving is obviously larger than that for bus travel, encompassing the central circle to the outer circle. By contrast, the high-value area for bus travel is scattered across Xiaoqiao Subdistrict in Chengbei District, the east of Chengdong District, Wenhui Road Subdistrict in Chengxi District, andZongzhai Town in Chengzhong District. These characteristics may be related to the distribution of bus rapid transit stations and bus stops, and by bus and bus rapid transit routes. Within Chengbei District, the accessibility of Chaoyang Subdistrict is low by bus but high by car, whereas theaccessibility of Xiaoqiao Subdistrict is high by bus but low by car. One plausible explanation is that the bus route from Chaoyang Subdistrict to Chengdong District generally stops around the city center instead of going eastward, whereas driving follows a shorter route.
4.3. Spatial Autocorrelation Analysis
Based on the accessibility results, we next use bivariate Moran spatial autocorrelation analysis to explore the correlation between population and hospital accessibility for each street in the main urban area of Xining City, considering both driving and public transport. According to the autocorrelation calculation, the global bivariate Moran index is 0.281 for driving and 0.282 for bus travel. These values indicate a positive spatial relationship between population and hospital accessibility at street level. The Lisa cluster diagram (Figure 7) shows that high–high cluster residential areas have the largest area, expanding outward in a circular manner from the central circle of the east district. These residential areas have a large population but also high hospital accessibility, ensuring that residents’ medical needs can be fully met. Low–low cluster residential areas—those with small populations and limited hospital accessibility—are mostly distributed at the urban edge. These areas need improvements to healthcare service capacity and the road network. Low–high clustering is distributed in Mafang Subdistrict of Chengbei District, Tonghai Road Subdistrict of Chengxi District, and near the north side of Xiaoqiao Subdistrict. These residential areas are characterized by a mismatch of low hospital accessibility and large population, resulting in excessive pressure on medical facilities. To address unmet demand, these areas need more medical facilities or upgrades to the service capacity of existing facilities. The high–low cluster areas are mostly located in Lejiawan Town in Chengdong District, Nanchuan East Road Subdistrict in Chengzhong District, and the north of Zongzhai Town near the urban center. These residential areas have small populations of predominantly older residents and are located close to the third tier hospital in Chengdong District and the center of Chengzhong District. For bus travel, the high–low cluster streets in Chengdong District are Bayi Road Subdistrict and the southern residential area of Lejiawan Town; only the latter is included in the cluster area for driving.
Overall, high–high clustering is mostly distributed in the central circle of Chengdong District, whereas low–high clustering is entirely distributed in the city’s northern district, where healthcare service capacity is in short supply in areas with high populations.
5. Discussion and Conclusion
5.1. Main Findings
To better understand the spatial distribution of healthcare services in cities on the TP, this paper proposes an improved 3SFCA method. We take Xining City as a representative example to analyze and evaluate the spatial accessibility of medical services. Our approach takes into account terrain and traffic conditions on the TP, the accuracy of population data, the service capacity of medical facilities, different travel modes, the competitive effect of nearby medical facilities, and the suboptimal allocation of supply points. Moreover, we analyze the spatial autocorrelation between hospital accessibility and population size for residential areas using the bivariate Moran index, further revealing the distribution characteristics of hospital accessibility in plateau cities. The studies main findings are as follows.
First, the TP has a special natural environment, with terrain that greatly restricts the traffic network and population distribution, are greatly restricted by the terrain. By gridding population demand points based on multi-source data and using online real-time route planning to calculate travel time by different modes, we effectively improved the accuracy of data for the urban population distribution and travel status. The improved 3SFCA method, incorporating selection weights and the suboptimal allocation of supply points, better reflects the reality of urban areas on the TP.
Second, the accessibility of healthcare in the main urban area of Xining City is distributed in a circular manner in space, and decreases in an “X” shape to four axes with the urban center as the axis. This is closely related to the urban distribution pattern. In general, the accessibility of healthcare is affected by the topography of the two river valleys and shows great differences in spatial distribution: it gradually decreases from the central part of Hehuang Valley to the valley edge, with the urban center as the axis of the circle and ring-shaped diffusion. At street level, the accessibility is high in the central urban area and the nearby central part of Chengdong District. However, the accessibility is low at the southern edge of Chengzhong District, the western edge of Chengxi District, and the northern edge of Chengbei District, and is generally low in Chengbei District. Streets with the highest hospital accessibility are mainly distributed in the east and middle, with few in the west and north. For both driving and bus trips, high hospital accessibility is found in the central circle of the city’s east district and gradually weakens moving outward. Accessibility by bus is affected by the distribution of stops and the routes for buses and bus rapid transit.
Third, there is a positive spatial relationship between population and accessibility in the main urban area of Xining City. In the areas with significant clustering, high–high clusters are mostly distributed in the central circle of the east district, whereas low–high clusters are mostly distributed in the Chengbei District, where healthcare is in short supply relative to the high population. The obvious streets in low-high cluster are near the north side of Mafang Subdistrict and Xiaoqiao Subdistrict in the north district.
5.2. Theoretical and Practical Implications
Our proposed framework for studying the spatial accessibility of healthcare facilities in plateau cities addresses a clear gap in the literature. The research framework is mainly applicable to terrain-restricted urban areas on the TP. It could also be adapted for studying rural and county areas with scattered population distribution and obvious differences between urban and rural areas. In general, hospital accessibility of the main urban area of Xining City decreases in a circle to four axes, with good accessibility in the east and center but poor accessibility in the north, consistent with previous research conclusions. Differences in hospital accessibility between travel by car and by bus are mainly explained by the traffic network, with public transportation affected by stops and routes for buses and bus rapid transit, again basically consistent with findings from studies of larger regions [11].
Based on our findings for the spatial autocorrelation between hospital accessibility and resident population in the main urban area of Xining City, we make the following suggestions. First, the total amount of urban medical and healthcare resources on the TP is seriously insufficient, especially in comparison to China’s eastern developed region. The country should continue implementing the policies of counterpart support and assistance from the east, revitalization of the western region, and high-quality development of the whole society. Second, to ensure that residents’ basic medical needs are met, it is necessary to increase the number of 2-Grade and upward hospitals in the middle and west of Chengbei District, the middle of Chengzhong District, and the middle of Chengxi District, especially in densely populated areas such as Mafang Subdistrict, Tonghai Road Subdistrict near the bank of the HR and the north side of Xiaoqiao Subdistrict. Third, the 3A-Grade hospital in Chengdong District should be relocated (transfer high-quality medical teams) to supplement the areas with serious shortages of healthcare. Specifically, hospitals located in areas with relatively small populations and dense medical resources (including areas near the west of Lejiawan Town, Nanchuan East Road Street in Chengdong District, and the north of Zongzhai Town near the city center) will be relocated to those areas (including the south of Chengzhong District, the north and west of Chengbei District, and the west of Chengxi District). Besides counterpart support and assistance from the east, rational coordination of regional hospital resources is needed to effectively improve the spatial fairness of public medical resource allocation, to guarantee the fulfillment of residents’ basic medical needs, and to gradually narrow the gap in medical service levels between China’s eastern and western regions.
5.3. Limitations and Future Research Avenues
Our research framework and the improved 3SFCA model have several shortcomings that future studies should aim to address. The first limitation is uneven population distribution: although we extracted residential areas from a topographic map, thus excluding parks, mountains, and other non-residential areas, we calculated the population of each grid assuming even distribution according to the total street population and size of the residential area. Therefore, our approach ignored the uneven population distribution in residential areas. Second, in calculating hospital accessibility, we did not consider different demand groups: the study’s population data comprised numbers of permanent residents in the streets of Xining City’s main urban area. In actual life, the elderly and children may have higher medical needs. Third, since the TP is a gathering place of ethnic minorities with different languages and medical habits, resulting differences in supply and demand relations regarding healthcare need to be considered. Fourth, our method includes just three indicators of service capacity (hospital grade, number of health technicians, and number of beds) for factor analysis. Follow-up studies should consider more indicators of hospital service capacity, such as the number of inpatients, outpatient volume, hospital area, and annual number of operations. Finally, we set more than 90% travel time as the search threshold for hospitals, based on frequency histograms of residents’ travel time to hospital by car or bus. Future studies should conduct sensitivity analysis for medical service facilities of different tiers/levels to reasonably determine the search threshold range.
Author Contributions
All authors contributed to the study conception and design. Data collection and analysis were performed by Hongkui Yang, Wanqiang Qi, Shilin Wang, Mingxin Yang, Zhen Zhang, Maqiang Xu, Wenlong Pang, Guangchao Cao and Yanhe Wang. The first draft of the manuscript was written by Yousan Li and all authors commented on previous versions of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Geological survey project of China Geological Survey [DD20191016、ZD20220409、ZD20220125、DD20211570].
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Acknowledgments
This work was supported by the Geological survey project of China Geological Survey. The authors are grateful to insightful comments suggested by the editor and the anonymous reviewers.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Kim, K., Ghorbanzadeh, M., Horner, M. W., Ozguven, E. E., 2021. Identifying areas of potential critical healthcare shortages: A case study of spatial accessibility to ICU beds during the COVID-19 pandemic in Florida. Transport Policy, 110, 478–486. [CrossRef]
- Jia, P., Wang, Y. F., Yang, M., Yang, X. C., Shi, X. Y., Yang, L. J., Wen, J., Liu, Y., Yang, M. K., Xin, J. G., Zhang, F. Y., Jiang, L. H., Chi, C. H., Zhang, L. X., Ma, X. D., Ma, X., Zhao, L., Li, W. M., 2022. Inequalities of spatial primary healthcare accessibility in China. Social Science Medicine, 314,115458. [CrossRef]
- Yin, C., He, Q., Liu, Y., Chen, W., Gao, Y., 2018. Inequality of public health and its role in spatial accessibility to medical facilities in China. Applied Geography, 92, 50–62. [CrossRef]
- Gómez, J. N., Loures, L., Castanho, R., Cabezas, J., Panagopoulos, T., 2018. Assessing the feasibility of GIS multimethod approach to ascertain territorial accessibility to hemodynamics rooms in Spain mainland. Habitat International, 71, 22–28. [CrossRef]
- Rekha, R. S., Wajid, S., Radhakrishnan, N., Mathew, S., 2017. Accessibility analysis of health care facility using geospatial techniques. Transportation Research Procedia, 27, 1163–1170. [CrossRef]
- Ben-Elia, E., Benenson, I., 2019. A spatially-explicit method for analyzing the equity of transit commuters’ accessibility’. Transportation Research Part A: Policy and Practice, 120, 31–42. [CrossRef]
- Wang, X., Yang, H., Duan, Z., Pan, J., 2018. Spatial accessibility of primary health care in China: A case study in Sichuan Province. Social Science & Medicine, 209, 14–24. [CrossRef]
- Shin, K., Lee, T., 2018. Improving the measurement of the Korean emergency medical system’s spatial accessibility. Applied Geography, 100, 30–38. [CrossRef]
- Hu, S. Y., Lu, Y. Q., Hu, G. J., 2021. Measuring accessibility and equity of medical resources in Shenzhen based on multi-source big data. Economic Geography, 41(11), 87–90.
- Gao, X. C., Wang, B., 2022. Do railways improve territorial cohesion of the Tibetan Plateau? A case study of the Qinghai-Tibet Railway. Applied Geography, 144, 102720. [CrossRef]
- Gao, X. C., Cao, X. S., Li, T., Lv, M. J., 2019. Evolution of accessibility spatial pattern of the Qinghai-Tibet Plateau in 1976–2016. Acta Geographica Sinica, 74(6), 1190–1204. [CrossRef]
- Lu, X. C., Cao, L., Ding, H. Y., Gao, M. M., Meng, X. H., 2022. The relationship between the altitude and the simulations of ozone and NO2 by WRF-Chem for the Tibetan Plateau. Atmospheric Environment, 274, 118981. [CrossRef]
- Nie, Y., Zhang, X., Yang, Y., Liu, Z., He, C., Chen, X., Lu, T., 2023. Assessing the impacts of historical and future land-use/cover change on habitat quality in the urbanizing Lhasa River Basin on the Tibetan Plateau. Ecological Indicators, 148, 110147. [CrossRef]
- Wang, Z., Li, J., Liang, L., 2022. Ecological risk in the Tibetan Plateau and influencing urbanization factors. Environmental Challenges, 6, 100445. [CrossRef]
- Yang, Y. C., Sun, Y., Wang, W. W., 2019. The scale logic of Shigatse City’s development and urban spatial evolution since the year of 1959. Economic Geography, 39(12), 48–61.
- Dai, K. X., Shen, S., Chen, C. X., Geng, J. C., Zhang, T. Y., 2022. Assessment of urban flood mitigation capacity on the Qinghai-Tibet Plateau: The case of Lhasa City. Journal of Beijing Normal University (Natural Science), 58(2), 318–327. [CrossRef]
- Sun, J. P., 2016. Dynamic analysis of ecological footprint and ecological capacity in Yushu City. Journal of Neijiang Normal University, 32(2), 21–22. [CrossRef]
- Cao, Y. P., et al., 2022. Study on dynamic change of land use in Changdu City based on GIS. Journal of Anhui Agricultural Sciences, 50(2), 86–88.
- Wang, J. Z., Gao, Y. C., Tie, Y. B., Xu, W., Bai, Y. J., 2021. Evaluation of the susceptibility to landslide in mountainous towns based on slope unit: Taking Kangding as an example. Sedimentary Geology and Tethyan Geology. [CrossRef]
- Pan, J. Y., Wang, J. L., Gao, F., 2022. Research of land use change and ecological security of typical area of alpine canyon in Northwest Yunnan. Ecological Science, 41(2), 29–40. [CrossRef]
- Tao, X. Y., Liu, J. B., Huang, Z. G., Ba, S., 2022. Zoning of highway geological hazard susceptibility and meteorological forecast model in Linzhi City. Bulletin of Soil and Water Conservation, 42(2), 195–209.
- Liu, Z., Yang, H. Y., Xiong, W. K., Chen, G. H., 2017. Spatial accessibilities of medical services at county level based on optimized two-step floating catchment area method. Scientia Geographica Sinica, 37(5), 728–737. [CrossRef]
- Deng, L., Shao, J. A., Guo Y., Xu, X. L., 2015. Spatial accessibility of medical services in mountainous regions based on modified two-step floating catchment area method: A case study of Shizhu County, Chongqing. Progress in Geography, 34(6), 716–725. [CrossRef]
- Tong, D., Sun, Y., Xie, M., 2021. Evaluation of green space accessibility based on improved Gaussian two-step floating catchment area method: A case study of Shenzhen City, China. Progress in Geography, 40(7), 1113–1126. [CrossRef]
- Zhang, J., Lin, D., Zhou, X., Li, F., Zhou, Y., Cheng, Y., Wang, P., 2022. Spatial accessibility and equality of public medical facilities in rural areas based on the improved 3SFCA: A case of Haikou City. Progress in Geography, 41(4), 636–647. [CrossRef]
- Luo, W. 2004. Using a GIS-based floating catchment method to assess areas with shortage of physicians. Health Place, 10(1), 1–11. [CrossRef]
- Ma, X., Ren, F., Du, Q., Liu, P., Li, L., Xi, Y., Jia, P., 2019. Incorporating multiple travel modes into a floating catchment area framework to analyse patterns of accessibility to hierarchical healthcare facilities. Journal of Transport Health, 15,100675. [CrossRef]
- Xing, J., Ng, S. T., 2022. Analyzing spatiotemporal accessibility patterns to tertiary healthcare services by integrating total travel cost into an improved E3SFCA method in Changsha, China. Cities, 122, 103541. [CrossRef]
- Wan, N., Zou, B., Sternberg, T., 2012. A three-step floating catchment area method for analyzing spatial access to health services. International Journal of Geographical Information Science, 26(6), 1073–1089. [CrossRef]
- Luo, J., 2014. Integrating the Huff Model and floating catchment area methods to analyze spatial access to healthcare services. Transactions in GIS, 18(3), 436–448. [CrossRef]
- Subal, J., Paal, P., Krisp, J. M., 2021. Quantifying spatial accessibility of general practitioners by applying a modified Huff three-step floating catchment area (MH3SFCA) method. International Journal of Health Geographics, 20(1), 9. [CrossRef]
- Wang, Z., Li, Z., Cheng, H., 2022. The equity of urban park green space accessibility in large Chinese cities: A case study of Wuhan City. Progress in Geography, 41(4), 621–635. [CrossRef]
- Chen, X., 2019. Enhancing the two-step floating catchment area model for community food access mapping: Case of the Supplemental Nutrition Assistance Program. The Professional Geographer, 71(4), 668–680. [CrossRef]
- Kiran, K. C., Corcoran, J., Chhetri, P., 2020. Measuring the spatial accessibility to fire stations using enhanced floating catchment method. Socio-Economic Planning Sciences, 69. [CrossRef]
- Liu, H., Duan, H. M., Fan, X. W., Xie, Y. L., 2009. Research on the evolution of urban spatial form in Xining. Areal Research and Development, 28(5), 56–61.
- Tao, Z. L., Cheng, Y., 2016. Research progress of the two-step floating catchment area method and extensions. Progress in Geography, 35(5), 589–599. [CrossRef]
- Luo, W., Whippo, T., 2012. Variable catchment sizes for the two-step floating catchment area (2SFCA) method. Health Place, 18(4), 789–795. [CrossRef]
- Zhao, Z., Li, X., Xu, Y., Yang, S., Jiang, Y., Wang, S., 2022. Evaluating spatial accessibility of cultural urban land use by using improved 2SFCA method in Xi’an, China. Heliyon, 8(12), e11993. [CrossRef]
- Rauch, S., Stangl, S., Haas, T., Rauh, J., Heuschmann, P. U., 2023. Spatial inequalities in preventive breast cancer care: A comparison of different accessibility approaches for prevention facilities in Bavaria, Germany. Journal of Transport & Health, 29, 101567. [CrossRef]
- McGrail, M. R., Humphreys, J. S., 2009. Measuring spatial accessibility to primary care in rural areas: Improving the effectiveness of the two-step floating catchment area method. Applied Geography, 29(4), 533–541. [CrossRef]
- Yang, Y. C., Zhao, M. Y., Jia, Z., Cheng, S. H., 2022. Study on green development planning of Plateau Xining metropolitan area. Areal Research and Development, 41(5), 56–62.
- Knap, E., Ulak, M. B., Geurs, K. T., Mulders, A., van der Drift, S., 2023. A composite X-minute city cycling accessibility metric and its role in assessing spatial and socioeconomic inequalities – A case study in Utrecht, the Netherlands. Journal of Urban Mobility, 3, 100043. [CrossRef]
- Xing, L., Liu, Y., Wang, B., Wang, Y., Liu, H., 2020. An environmental justice study on spatial access to parks for youth by using an improved 2SFCA method in Wuhan, China. Cities, 96, 102405. [CrossRef]
- Chen, Y., Yang, M., Tao, Z. L., Kong, J. S., Liu, Z., 2023. Access and cost of primary educational services in plateau areas: A case study in Tibet, China. Applied Geography, 152,102874. [CrossRef]
- Kelobonye, K., Zhou, H., McCarney, G., Xia, J., 2020. Measuring the accessibility and spatial equity of urban services under competition using the cumulative opportunities measure. Journal of Transport Geography, 85, 102706. [CrossRef]
- Wang, J., Kwan, M. P., Liu, D., Peng, X., 2023. Assessing the spatial distribution of and inequality in 15-minute PCR test site accessibility in Beijing and Guangzhou, China. Applied Geography, 154, 102925. [CrossRef]
- Delamater, P. L., 2013. Spatial accessibility in suboptimally configured health care systems: A modified two-step floating catchment area (M2SFCA) metric. Health Place, 24, 30–43. [CrossRef]
- Salih, S. M., Lee, J. (B)., 2022. Measuring transit accessibility: A dispersion factor to recognise the spatial distribution of accessible opportunities. Journal of Transport Geography, 98, 103238. [CrossRef]
- Liu, L., Lyu, H., Zhao, Y., Zhou, D., 2022. An improved two-step floating catchment area (2SFCA) method for measuring spatial accessibility to elderly care facilities in Xi’an, China. International Journal of Environmental Research and Public Health, 19(18), 11465. [CrossRef]
- Radke, J., Mu, L., 2000. Spatial decompositions, modeling and mapping service regions to predict access to social programs. Annals of GIS, 6(2), 105–112. [CrossRef]
- Chen, X., Jia, P., 2019. A comparative analysis of accessibility measures by the two-step floating catchment area (2SFCA) method. International Journal of Geographical Information Science, 33(9), 1739–1758. [CrossRef]
- Cheng, L., Yang, M., De Vos, J., Witlox, F., 2020. Examining geographical accessibility to multi-tier hospital care services for the elderly: A focus on spatial equity. Journal of Transport Health, 19, 100926. [CrossRef]
- Jorg, R., Haldimann, L., 2023. MHV3SFCA: A new measure to capture the spatial accessibility of health care systems. Health Place, 79, 102974. [CrossRef]
- McGrail, M. R., Humphreys, J. S., 2014. Measuring spatial accessibility to primary health care services: Utilising dynamic catchment sizes. Applied Geography, 54, 182–188. [CrossRef]
- Pei, X. R., Guo, P., Chen, Q. Y., Li, J. R., Liu, Z. F., Sun, Y. L., Zhang, X. K., 2022. An improved multi-mode two-step floating catchment area method for measuring accessibility of urban park in Tianjin, China. Sustainability, 14(18), 11592. [CrossRef]
- Chen, B. Y., Cheng, X. P., Kwan, M. P., Schwanen, T., 2020. Evaluating spatial accessibility to healthcare services under travel time uncertainty: A reliability-based floating catchment area approach. Journal of Transport Geography, 87, 102794. [CrossRef]
Figure 1.
Overview of the study area’s geographical location. Left: Enhanced Thematic Mapper image of the TP; Right: Google image of the main urban area of Xining City.
Figure 1.
Overview of the study area’s geographical location. Left: Enhanced Thematic Mapper image of the TP; Right: Google image of the main urban area of Xining City.
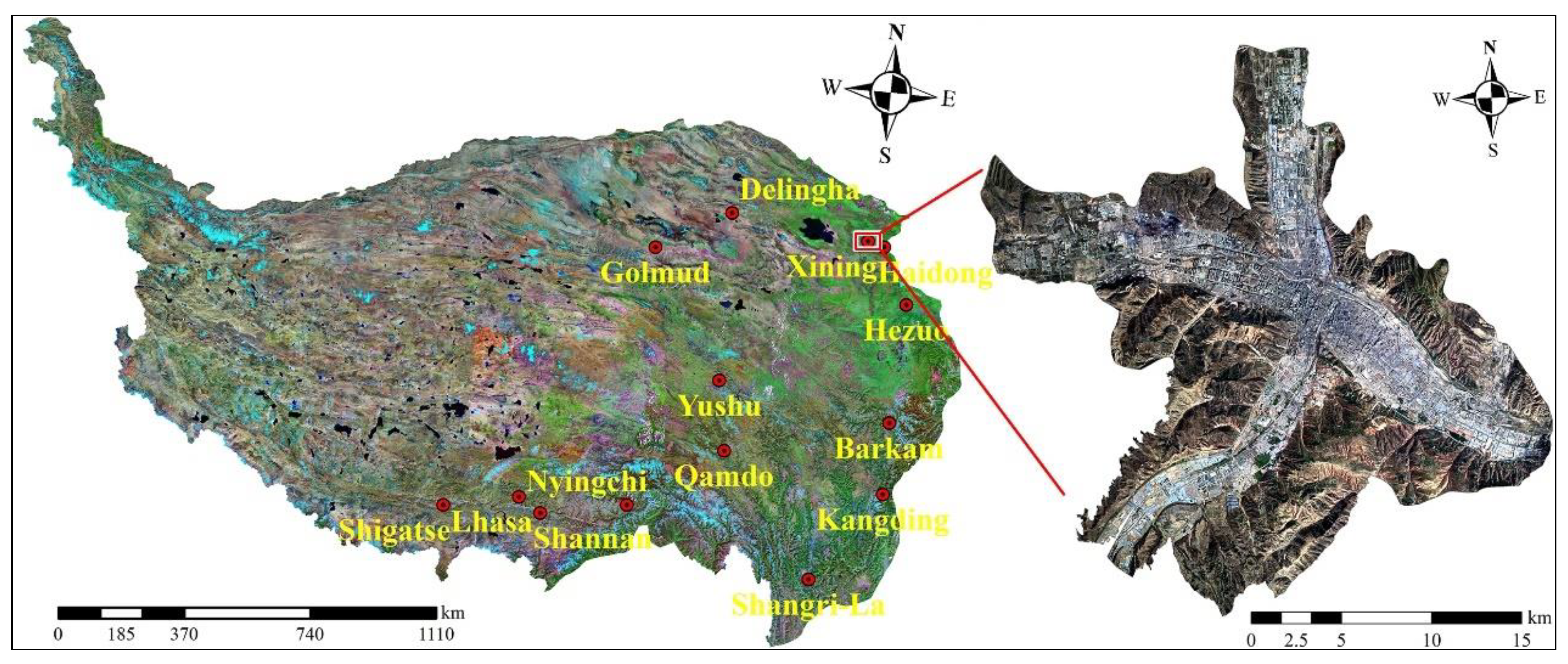
Figure 2.
Research framework.
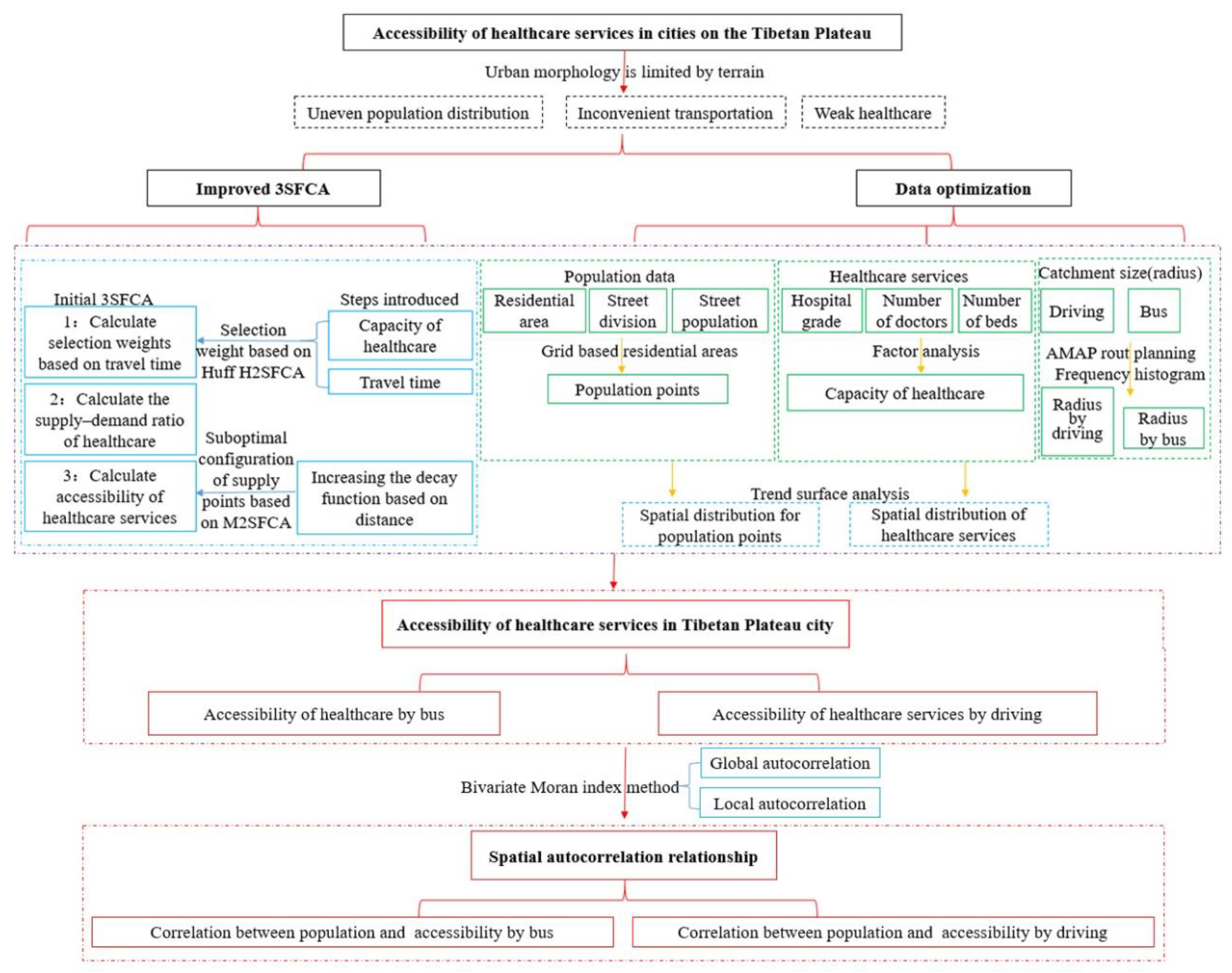
Figure 3.
Travel-time frequency histograms (including cumulative percentage) for driving and bus travel.
Figure 3.
Travel-time frequency histograms (including cumulative percentage) for driving and bus travel.
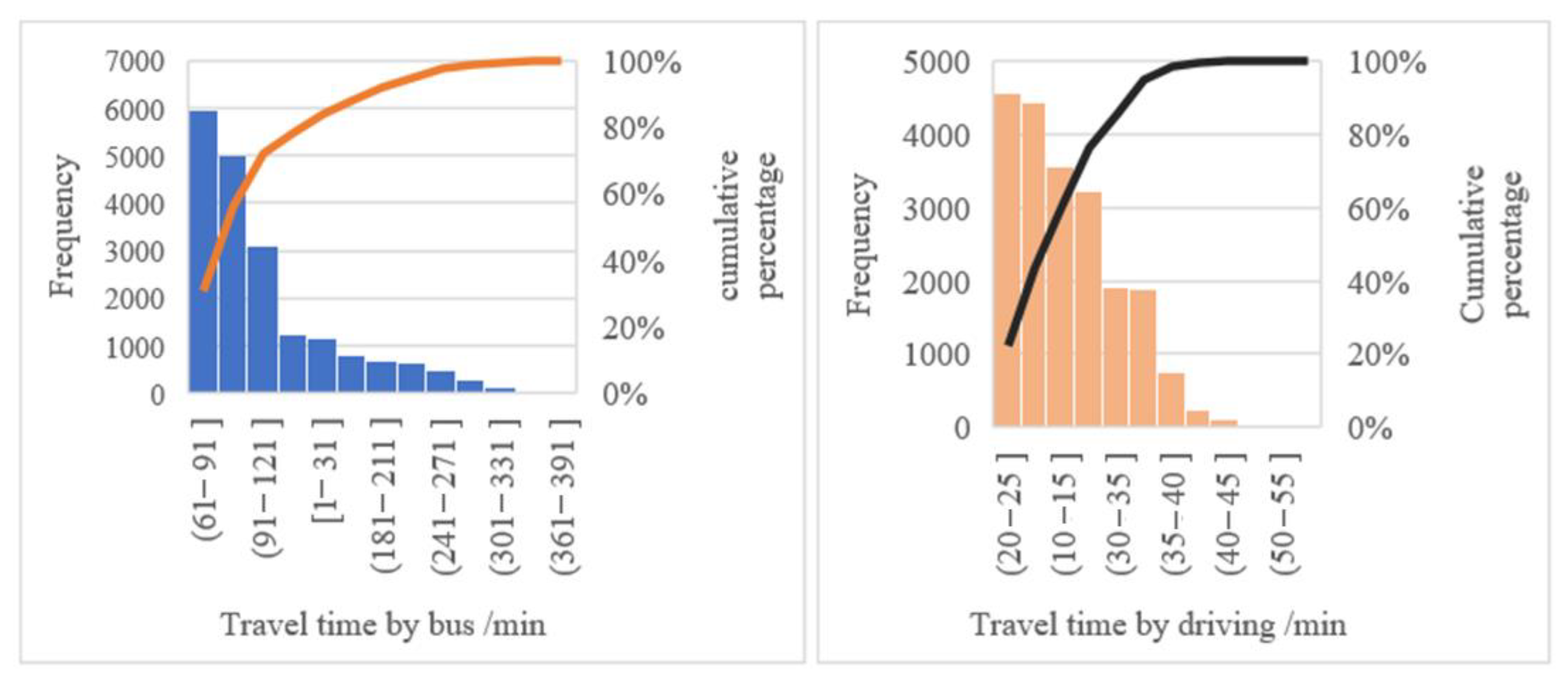
Figure 4.
Spatial trend surface analysis of residential area population (left) and hospitals (right).
Figure 4.
Spatial trend surface analysis of residential area population (left) and hospitals (right).
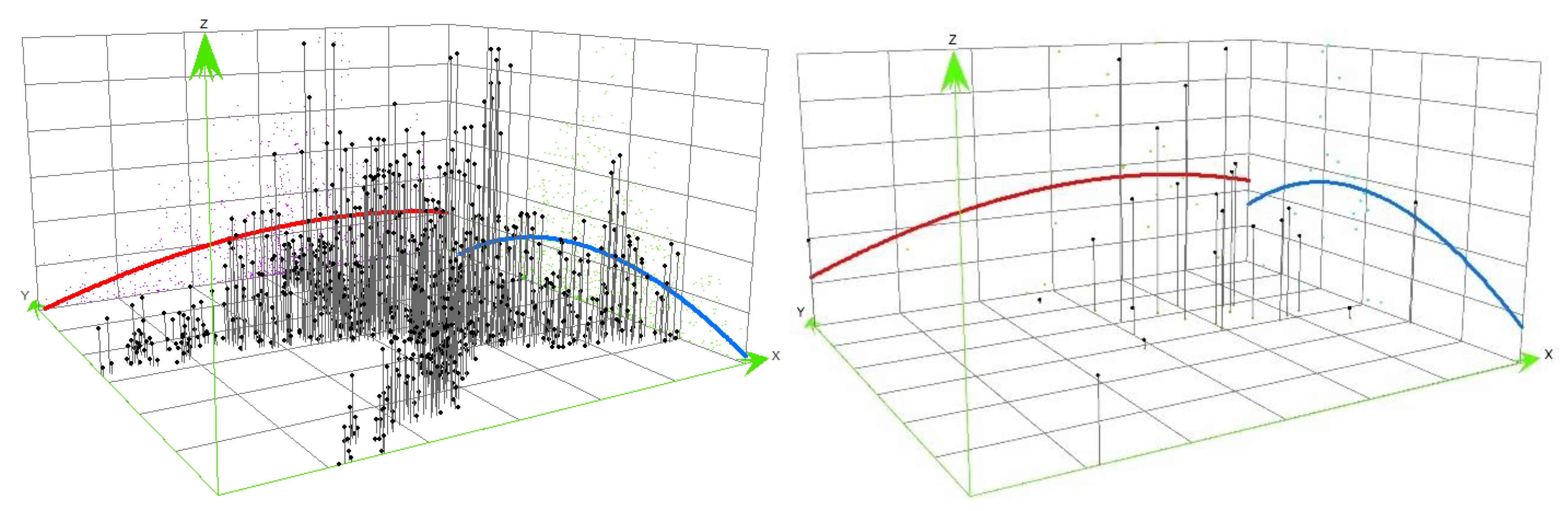
Figure 5.
Calculation steps of the improved 3SFCA model (adapted from Subal et al., 2021) [31].
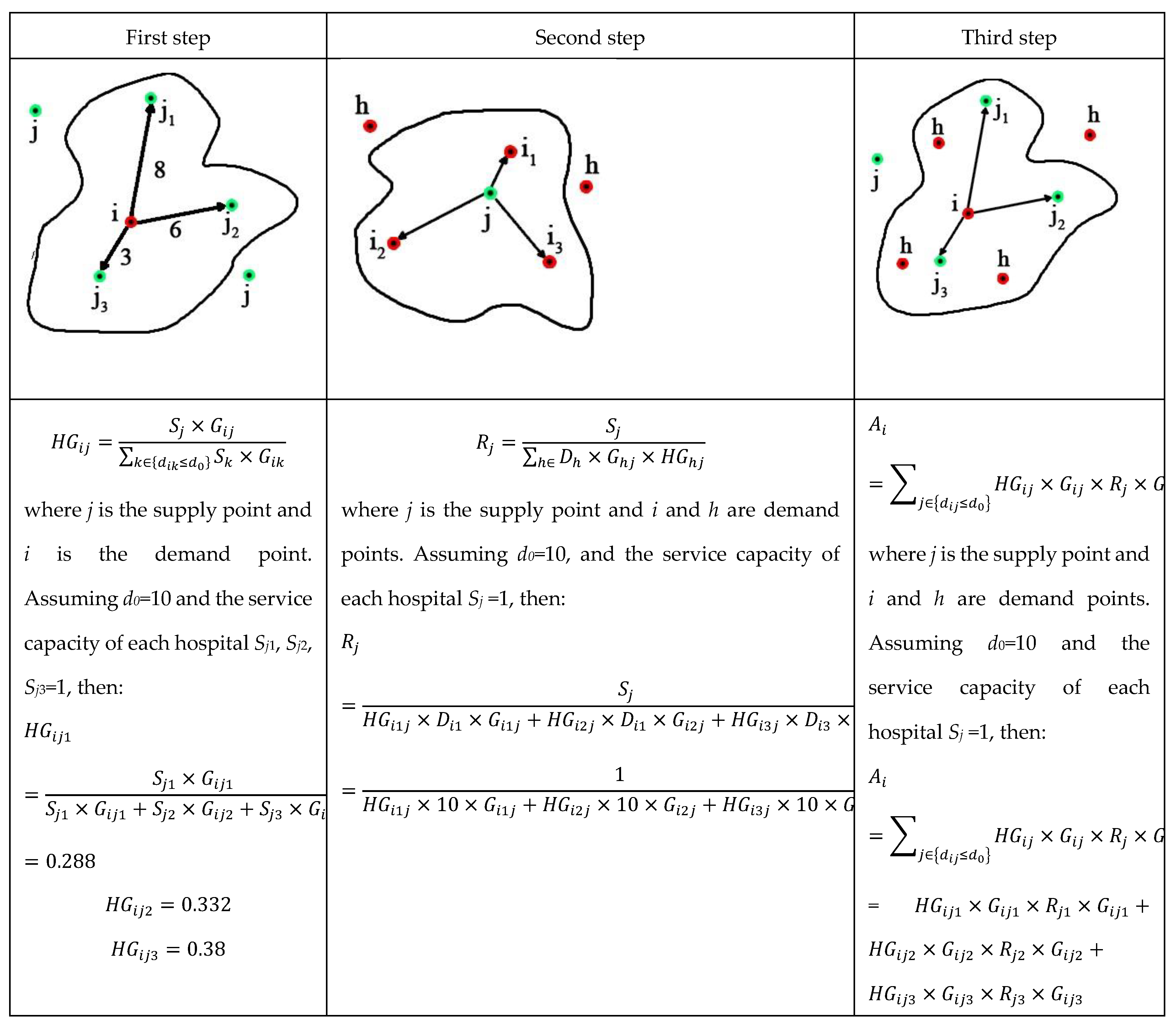
Figure 6.
Hospital accessibility distribution in the main urban area of Xining City for car (left) and bus travel (right).
Figure 6.
Hospital accessibility distribution in the main urban area of Xining City for car (left) and bus travel (right).
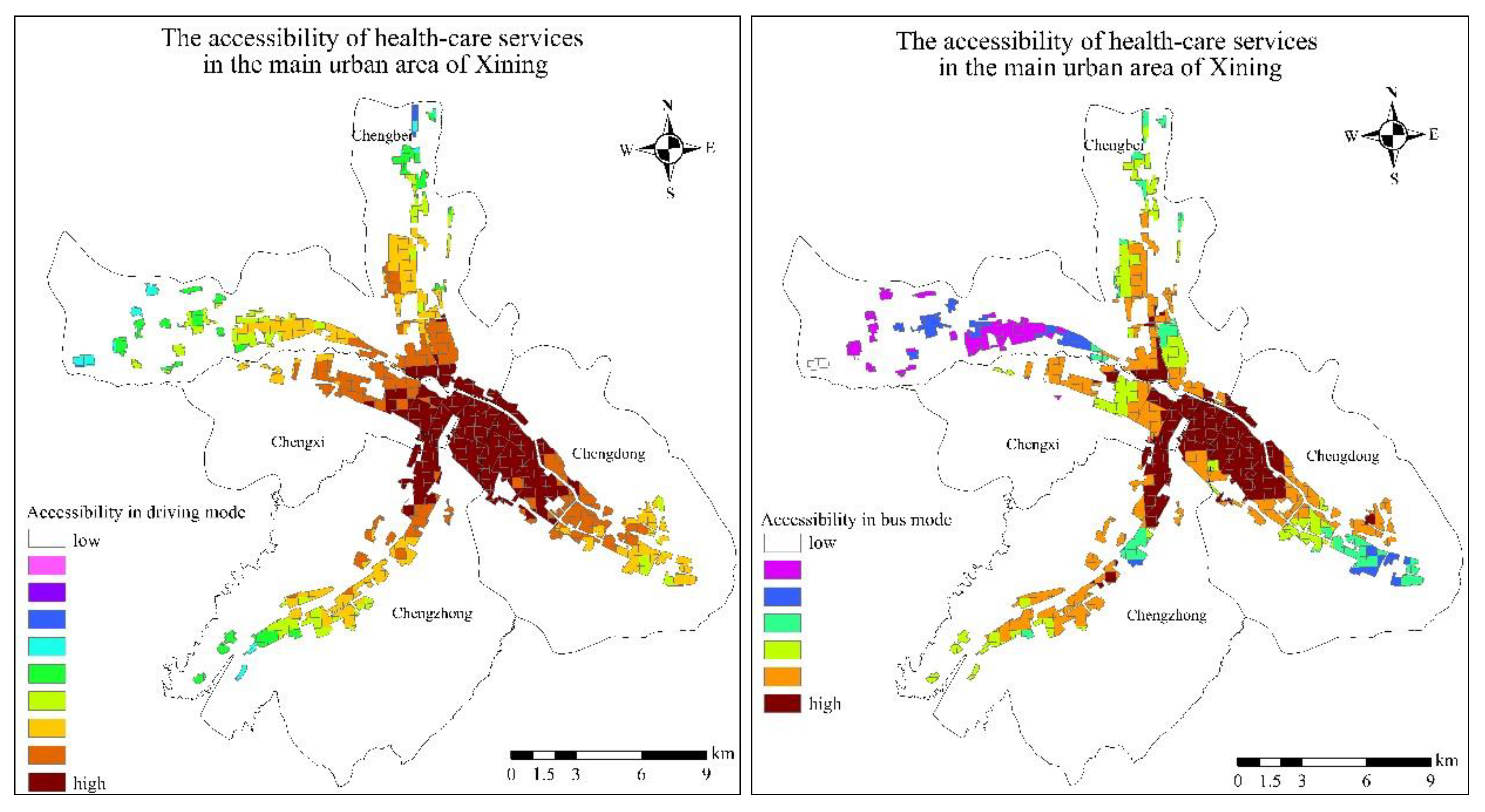
Figure 7.
Autocorrelation diagram of population and accessibility under driving and bus travel modes (left is driving mode, right is bus mode).
Figure 7.
Autocorrelation diagram of population and accessibility under driving and bus travel modes (left is driving mode, right is bus mode).
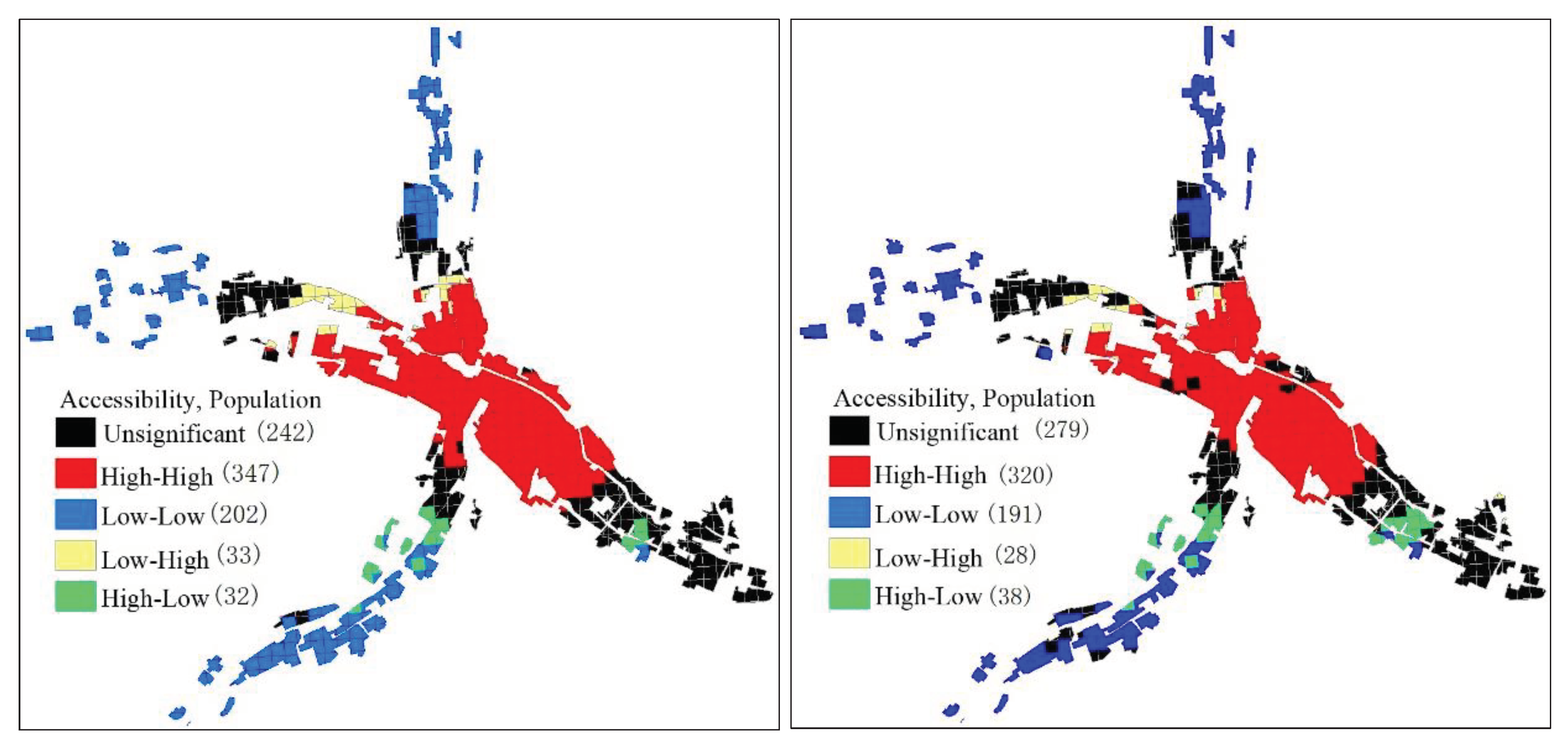

Table 1.
Urban characteristics of the TP.
| City | Spatial distribution | Traffic network | Population (10,000) |
| Xining | X-shaped Huangshui River(HR) Valley [15] | Distributed along the valley | 246.8 |
| Lhasa | Narrow strip valley [16] | Distributed along the valley | 86.8 |
| Golmud | Strip alluvial-proluvial wide valley | Distributed along the valley | 22.2 |
| Haidong | Banded, Huangshui Valley | Distributed along the valley | 135.8 |
| Delingha | Alluvial-lacustrine Piedmont plain | Distributed in the middle of the plain | 8.8 |
| Hezuo | λ-shaped Tiaohe River and Daxia Valley | Distributed along the valley | 11.2 |
| Yushu | Banded Tongtian River Valley [17] | Distributed along the valley | 14.1 |
| Qamdo | Narrow-long Sanjiang River Valley [18] | Distributed along the valley | 76.1 |
| Barkam | Banded, Dadu River Canyon | Distributed along the canyon | 5.8 |
| Kangding | Y-shaped Yarra River Valley [19] | Distributed along the valley | 12.7 |
| Shangri-La | Willow-leaf-shaped Sanjiang River Valley [20] | Distributed along the valley | 18.6 |
| Shigatse | Banded, Nianchu River Valley [15] | Distributed along the valley | 79.8 |
| Nyingchi | Banded, Yarlung Zangbo River Valley 21 | Distributed along both sides of the canyon | 23.9 |
| Shannan | T-shaped, Yajiang Valley | Distributed along the valley | 35.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



