
Submitted:
04 March 2024
Posted:
05 March 2024
You are already at the latest version
Abstract
This study aimed to review the dietary risk factors for root caries prevalence in older adults, from socially active people to frail patients. A comprehensive search strategy was used to select studies from PubMed and Scopus databases. Two evalua-tors performed data extraction, screening, and quality assessment independently. Only studies written in English were included. Caries is very common in the elderly, as there are several aggravating factors such as the decrease of the ability to self-care and, by extension, insufficient oral hygiene, a carious diet, limited exposure to fluoride, xero-stomia, gingival recession, limited access to dental care. Root caries is prevalent in the elderly due to gingival recession and root exposure to the oral environment. Dietary risk factors significantly affect root caries prevalence in older adults, including high intake of sugars and an alteration of their composition preference in this age group. Caries risk appears more significant in frail, standardized patients who feed with even softer food or supplements.
Keywords:
diet
; elderly
; carries
; root caries
1. Introduction
The older population is significantly increasing worldwide, facing multiple socio-medical and dental needs. Aging is associated with physiological changes that can affect nutrient absorption, metabolism, and overall health status. Therefore, maintaining a healthy diet becomes paramount for promoting longevity and reducing the risk of chronic diseases among older adults.
Even though caries prevalence in the Western world seems to decrease, two age groups continue to record a high prevalence of caries: children and older adults. These two groups are similar in that they depend on carers for their oral health and diet habits. Despite progress in oral health prevention, oral disease is still common in older people due to multiple barriers and risk factors. The prevalence and severity of dental caries vary among different age groups, with older adults often exhibiting a higher burden of untreated caries compared to younger populations (1). Several factors contribute to this disparity, including cumulative exposure to cariogenic risk factors over a lifetime, compromised oral hygiene due to physical or cognitive impairments, and barriers to accessing dental care services (2). Epidemiological studies have consistently demonstrated a high prevalence of dental caries among elderly individuals, particularly those residing in long-term care facilities or experiencing socioeconomic disadvantage (1,2).
Nevertheless, the older adults are known to be a mixed group of three subgroups. Firstly, there are the younger, active people living in the community and taking care of themselves. They are genuinely of good general health, and medical practitioners do not treat them differently than any other adult. Secondly, there is a partially dependent group -they could receive support, but they mainly choose their lifestyle (including diet and oral hygiene). Finally, the third group (older old) can also be frail and depend on carers who dictate their food choices and provide oral care. It is mainly the third group and then the second group that faces the problem of dental caries [1,2].
Caries is prevalent amongst older adults, as there are several aggravating factors such as the decrease of the ability to self-care and, by extension, insufficient oral hygiene, a carious diet, limited exposure to fluoride, xerostomia, receding gums, limited access to dental care, etc. Dietary factors, particularly the consumption of fermentable carbohydrates and sugars, are primary contributors to the development of dental caries. Fermentable carbohydrates in various foods, including bread, cereals, fruits, and starchy vegetables, serve as substrates for acid-producing bacteria in dental plaque, leading to localized demineralization of enamel and subsequent cavity formation. Likewise, sugars, such as sucrose, glucose, and fructose, are metabolized by cariogenic bacteria, producing acidic by-products that promote enamel erosion and caries progression. In addition, removable prosthetic works, which are not carefully cleaned, increase the concentration of dental microbial plaque and create conditions for caries. Root caries is prevalent in the elderly due to gingival recession and root exposure to the oral environment [3,4]. Older adults today tend to retain more of their natural teeth, with edentulism decreasing [5,6]. This means that caregivers (dentists and nursing personnel) of old individuals will have to be trained for treatment in old age and oral hygiene since there is an increasing risk of oral diseases, including dental caries.
The aim of this study was to identify any dietary habits that influence the prevalence of caries (either root caries or coronal caries) and the way that these dietary habits could be different amongst the different groups of the elderly.
2. Methodology
Design and eligibility criteria
To identify the role of the diet of the elderly in the caries process, a scoring review was performed. A scoping review approach was chosen because it allowed the synthesis of information from diverse sources, including theoretical reviews and qualitative and quantitative research. We included scientific papers in English reporting information that answers our question. Reviews, systematic reviews, clinical studies, in vitro studies, and studies in animals were included.
Sources of information and search strategy
Systematic research of the literature was conducted using the following electronic databases, MEDLINE and Scopus, from inception to February 2024. Keywords used for the search included “elderly,” “old people,” “diet,” “caries,” “root caries,” and “older adults” (for example, “elderly AND diet AND caries”). Reference listings of selected articles were hand-searched to identify other possible studies to be included. Two reviewers (GG and CR) independently selected the studies by title and abstract and then by full text according to the eligibility criteria. If there was a discrepancy, a consensus was reached.
Data charting process
One reviewer (GG) extracted relevant data from eligible studies, and an additional reviewer (CR) checked the information for accuracy. An Excel form was then created with information extracted from each article, including authors and journal, year, study objectives, type of the study, and conclusions of the study.
3. Results
The search identified a total of 664 articles, and after they were screened by title and abstract and 56 abstracts because the original article was not in English, more than 575 were removed because of lacking relevance (Figure 1). A total of 33 articles were retrieved and assessed for eligibility. 3 of them were removed because we could not permit the full text, and out of the 30 remaining, 11 were excluded after reading the full text because they were irrelevant to the topic of the search.
3. Discussion
Dental caries
Dental caries is the localized destruction of dental hard tissues (enamel and dentine). It is a dynamic process with repeated circles of demineralization and remineralization of dental hard tissues related to pH alterations of the biofilm. The process is defined as a chemical dissolution caused by acid production by biofilm, frequently exposed to sugars. Literature links the quality of saliva to its increased viscosity, with reduced salivary clearance and, therefore, a more significant time interval in which pH stays below 6.7, which is the critical point for dentine demineralization [7,8]. Dental caries might be the result of lifelong exposure to a dietary risk factor (i.e., free sugars), which means that the influence of carbohydrates is cumulative; we expect people of old age to be more affected because the teeth are exposed for a much more extended period in the dietary risk factors.
Xerostomia
One of the first common symptoms of deterioration in the oral health of older people is xerostomia [9,10,11,12]. Xerostomia or dry mouth is a common symptom, with a wide prevalence range with increasing age [13,14]. The proportion of individuals experiencing xerostomia will continue to rise as the older population grows. The symptom is multicausal and is mainly related to salivary gland disorders, medication use, and various medical conditions [13,15,16,17].
Women seem to have high xerostomia prevalence in comparison to men, mainly after the age of 50 [18]. Also, there is a large amount of literature on the relationship between diabetes and xerostomia [19,20,21]. Medication use is the most common cause of xerostomia [22,23,24,25,26]. As xerostomia is an increasing caries risk, dentists should encourage their patients to increase their water consumption [3]. Also, it is widespread for older people to suck candies or sweets for the relief of the symptoms of dry mouth. This has deteriorating outcomes for teeth, causing caries due to the sugar added in the candies and the frequency of the intake [27].
Diet
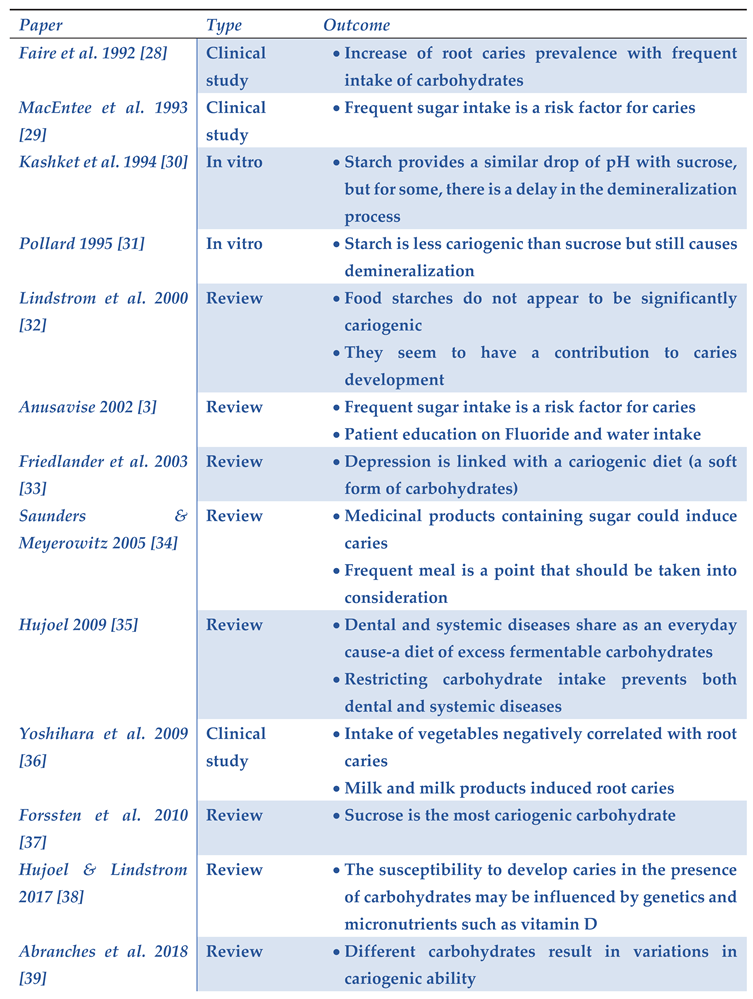
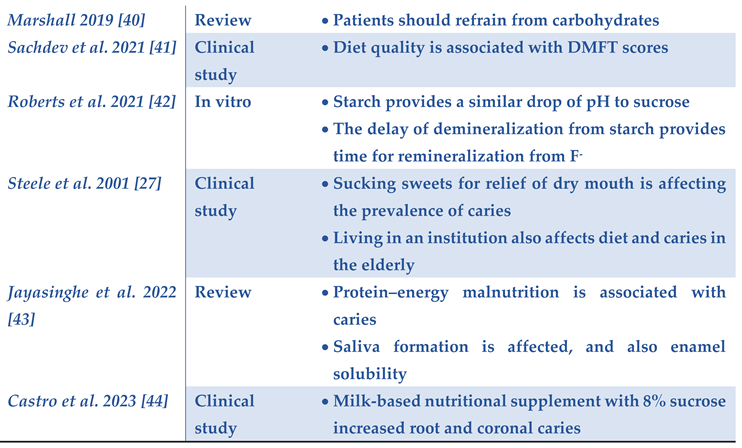
The prevalence of coronal and root caries in the older population varies between different studies but is relatively high in the Western world (Table 1).
The increased use of sugar intake that started in the 1970s in these countries determined the prevalence of dental caries. Studies show that risk factors for root caries in older adults include a high intake of sugars (both in a liquid or a solid form), an alteration of their composition preference in this age group, and lower consumption of vegetables and dairy products [31,37,42]. Older people tend to prefer a softer diet, which means that softer food could get stuck more easily in the root areas of the teeth. This preference is because they lose the ability to chew due to lack of teeth but also due to masticatory muscle weakness caused by old age or comorbidities. Any sugars that dental plaque bacteria can utilize as an energy source contribute more or less to the virulence of the microbiota and thus have a cariogenic potential. Sucrose is not only rapidly fermented to acidic end products, but it is also the only dietary carbohydrate that can be transformed into polysaccharides in the plaque. Thus, it is considered the most cariogenic carbohydrate in the human diet [37]. The frequency of carbohydrate intake also plays a crucial part in caries risk in the elderly [34]. It seems that as the frequency increases (regardless of whether they are in a beverage or food), the risk of caries increases with an extreme cariogenic risk when it is above six consumptions per day [28].
Restricting sugar intake is highly recommended by the American Heart Association and the World Health Organization [45]. The American Diabetes Association agreed on a low-carbohydrate diet in 2008 [46]. Similar dietary restrictions are recommended in some European countries, such as Sweden. The Nordic Nutrition Recommendations warn that added sugar intake should be limited from sugar-sweetened beverages and sugar-rich foods to reduce the risk of diabetes, weight gain, and dental caries. These guidelines also clarify that a limitation of such products is necessary to ensure an adequate intake of essential nutrients and dietary fiber [47]. Those dietary recommendations provide a starting point for an optimum diet for preventing dental caries and improving periodontal health.
The primary impact of nutrition on dental caries is understanding that refraining from carbohydrates consumed in solid or liquid form translates into an absence of dental caries [35,41]. The literature shows us that populations living on a diet low in carbohydrates develop dental caries to a shallow extent [48]. Caries process is a consequence of the intake of monosaccharides and disaccharides, including sucrose, glucose, fructose, lactose, maltose, and starch, that are broken down by microorganisms of dental biofilm, which then release acidic end products, with lactate and acetate playing a significant role. Among the different carbohydrates, there is only a tiny variation in acid production ability [39]. This means the local dietary effects depend on what is consumed at a specific time. Many factors influence the intra-oral environment, such as dietary habits, biofilm composition, saliva, and fluoride. Thus, the effect of diet on caries can vary from one individual to another but also from one tooth to another. The enamel will start demineralizing if the pH is lowered below the critical pH level of 5.5– 5.7. Still, when not covered by enamel, a tooth’s dentine or root surfaces have a higher critical pH (around pH 6.2) due to their lower organic content. This occurs after consuming most of the sugars found in candy, soft drinks, fruit juices, or the sugars added to coffee or tea. Complex carbohydrates found in whole foods such as potatoes, rice, cereals, and bread contribute to the caries of the dentine [31,49]. In studies mainly made in animals and in vitro, it is reported that such carbohydrates do not appear significantly cariogenic. However, depending on the frequency of the meals and if sucrose is also present in some form in the diet, they become cariogenic [30,31]. In the in vitro studies, there seems to be a similar pH drop after sucrose or starch solutions, but there is a substantial delay in the demineralization process [29]. When the pH drops slowly, the fluoride ions in the saliva find time to remineralize the tooth structure [40]. The latter could be beneficial when addressing older people because we know that with age, the ion exchange between saliva and tooth is reduced [50,51]. Thus, even these types of carbohydrates could contribute to caries development.
Therefore, the relationship between carbohydrates and dental caries may change during a lifetime as the root surface becomes exposed with age, as periodontitis occurs. This is why older people must get diet recommendations different from those for children and adolescents [38].
The acid-producing Streptococcus species form extracellular polysaccharides in the presence of sucrose but also from fructose and glucose. The energy-rich glycosidic bond between the glucose and fructose parts supplies the energy needed to synthesize polysaccharides. Glucose homopolysaccharides are called glucans, while fructose homopolysaccharides are called fructans. Glucosyltransferases produce glucans, while fructosyltransferases produce fructans. Producing large quantities of polysaccharides from sucrose is essential to S. mutan’s cariogenicity [37].
Dental caries, which is known to be linked to social and behavioral factors, is described as a significant public health problem among older people. Depression is a psychiatric disorder in which appetite and hygiene habits could be affected, often for an extended period, and is particularly common in older, especially those living in nursing homes (late-life depression) [52,53]. In a review held in 2003, it is stated that depression is linked with a more cariogenic diet, containing more carbohydrates than usual and in a softer form that could be stuck into areas of roots, inducing root caries [33]. In addition, oral hygiene and hygiene in general is commonly low on these patients; the risk of root caries is increased [33].
Older people today retain more teeth than earlier generations, often maintaining a so-called “functional dentition,” defined as the presence of at least 20 natural teeth, many of which may be heavily restored with fillings, crowns, and bridges [54,55]. As more teeth are present in the mouth, they are susceptible to oral disease at a more severe and high rate. Root recession, caused either by periodontitis or by wear and is more common in old age, dramatically increases the risk of developing root caries since it is a biological factor necessary for the onset of the disease [55,56,57,58]. Coronal and root surface caries are highly prevalent among old-age populations worldwide, and severe dental caries and periodontal disease are the primary reasons for tooth extractions [54].
Concerning all these, caries risk assessment is an integral part of modern dentistry since more and more people suffer from a disease that could be potentially preventable and manageable. Therefore, early identification of relevant factors affecting older people that could increase caries risk is essential [52]. Higher morbidity associated with chronic disease, the use of medications with xerostomic side effects, frequent carbohydrate intake, and heavy restoration of dentition are additional risk factors that challenge older people. Because of the heterogeneity of the elderly population and the broad spectrum of factors that affect this chronic disease, those at risk can benefit from individually designed preventive programs. Recent dental research in risk assessment has examined new and advanced methods for diagnosing and early predicting caries [60].
A longitudinal study in 2020 revealed no increase in the prevalence of dental caries lesions in older people, indicating that good oral health can be preserved among older adults, resulting in altering the effects of carbohydrate intake [61]. The highest risk for dental caries lesions was among participants with inadequate oral hygiene routines (toothbrushing once a day or less and seldom using interproximal devices) and in need of help in daily living, emphasizing the importance of oral hygiene and collaboration between dental services and community-based health care [61]. Oral diseases, especially dental caries, periodontal disease, and tooth loss, affect general health and can impair quality of life [62].
Alongside the reduction of consumption of sugary foods and drinks, it is also necessary to reduce the consumption of any medicinal products containing sugar that could be prescripted or delivered over the counter to older people and replace them with other, less cariogenic ones [32,34,63]. For example, a very recent clinical study shows that a milk–based nutritional supplement with 8% sucrose used for cases of malnutrition in the elderly increases the risk of coronal and root caries [44]. Also, there are a lot of energy-inducing medicinal products containing carbohydrates [63]. Diet modification may be more difficult in medically burdened elderly whose underlying diseases require frequent meals, i.e., type 2 diabetes, or medicine that should be taken frequently during the day with a full stomach [34,63]. Also, in a recent review, it was concluded that malnutrition affects oral diseases in various ways [43]. It seems that malnutrition, which can be easily reached in the elderly with a low intake of proteins, can induce caries by affecting the saliva glands and, therefore, saliva consistency and quantity [43]. Another way that protein-energy malnutrition can affect caries risk is by increasing enamel solubility [43]. Thus, it is safe to say that maintaining a healthy diet can be beneficial in older people for more than one reason.
In a 2021 study of a Japanese elderly population, it was found that an increase in sugar in beverages and a lower milk consumption led to an increase in the prevalence of caries [64]. The authors attributed this alteration in the diet of older people to taste alterations of old age [64]. In some other studies, it is attributed to economic boundaries, but they all increase caries prevalence [65]. In another study of an Indian population, there was a similar finding that diet alterations with high added sugars lead to more carious lesions [66]. Also, a study in 1995 specifies that coronal caries and root caries have a similar etiology: an increase in sucrose consumption [67].
Root caries
As previously stated, when root surfaces are exposed to the oral cavity due to periodontitis, they become prone to becoming demineralized because the roots are dentine, and exposed organic materials can be degraded by host-derived proteases contained in saliva [68]. We ought to identify root caries risks to set prevention strategies, a field studied in a large part of the literature.
Socioeconomic factors
As a vulnerable group, the elderly population’s oral health status seems to be worsening because of social and economic inequalities [69,70].
Schwendicke et al. reviewed that those with lower educational levels, occupational backgrounds, or incomes were more likely to have a higher risk of caries lesions or experience [71]. Many studies describe the influence of low socioeconomic status and dental caries [72,73,74]. Hobdell et al. (2003) strongly associate oral diseases with socioeconomic status [75]. Studies have shown that people with a low socioeconomic status have poorer oral health status than those with a higher socioeconomic status [76,77]. A study in 2017 in China in a population of elderly also showed a caries prevalence increase with low socioeconomic status, with household income playing a more critical role than education [74]. It could be safe to assume that income alterations can bring barriers to medical and dental care access. Still, some authors also assume that there are alterations in the diet, with a differentiation in the carbohydrates used and a reduction of fibers, proteins, and dairy products due to economic reasons [70].
Household income and educational level are significantly associated with periodontitis and edentate status in older people [77]. It is stated that social status could influence diet due to a total change in oral health perception [66].
Institutionalized patients and frailty
Institutionalized patients could depend on caregivers for their diet and oral hygiene depending on the facility, which also correlates with the patient’s socioeconomic status. This could be why, in some studies, the prevalence of dental caries is increased in institutionalized patients, mainly in cases where they depend on caregivers [78,79]. In other studies, in which the patients are standardized but not frail, there is no increase [4].
Frailty and the physical and mental decline associated with aging significantly impact personal oral hygiene practices [52]. Older people and their caregivers should be informed that the need for caries preventive measures increases with age and get a complete analysis of those.
Caries risk appears to be greater in frail and standardized patients, who tend to feed with even softer food or even supplements. A study from 2014 showed that caries prevalence was higher in patients with oropharyngeal dysphagia, which should be recognized as a significant geriatric syndrome as its prevalence is very high in elderly patients and leads to multiple diseases and risk factors [80].
In extreme frailty conditions, patients could be fed with nursing bottles and medicinal products that would provide proteins and energy to the suffering patient. This means that, more often than not, these products are full of carbohydrates. The method of delivering this product – through nursing bottles is also known to contribute to the increase of dental caries by studies conducted by children [2].
4. Conclusions
Even though diet is a very well-known risk factor for caries (both coronal and root caries), there are very few studies to understand the specific alterations that could prevent the burden of this disease.
Because people live longer and retain more natural teeth than previous generations, oral health care providers must remain attentive to caries risk factors and effectively manage caries throughout the lifespan.
As older adults often refrain from dental care due to various socioeconomic reasons, the role of primary health care professionals in identifying elders needing dental care is crucial.
Dental caries is closely linked to socioeconomic status and, hence, disproportionally affects the poorer and more marginalized groups in society.
It is safe to say that population-wide strategies to reduce free sugar consumption are a critical public health approach that should be a high and urgent priority. Because dental caries results from lifelong exposure to a dietary risk factor (i.e., free sugars), even a slight reduction in the risk of dental caries in the early years is significant in later life. Therefore, to minimize the lifelong risk of dental caries, free sugar intake should be as low as possible from as early as possible.
Population-wide prevention interventions must be universally available and accessible. Such interventions include the use of fluoride and comprehensive patient-centered essential oral health care.
Author Contributions
“Conceptualization, G.G. and C.R.; methodology, G.G.; software, G.G.; validation, G.G., and E.P.; formal analysis, G.G.; investigation, G.G.; resources, P.M.; data curation, G.G.; writing—original draft preparation, G.G.; writing—review and editing, all.; visualization, G.G.; supervision, C.R.; project administration, P.M. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Marchini L, Ettinger R, Hartshorn J. Personalized Dental Caries Management for Frail Older Adults and Persons with Special Needs. Dent Clin North Am 2019, Oct;63(4), 631-651. [CrossRef]
- Curzon ME, Preston AJ. Risk groups: nursing bottle caries/caries in the elderly. Caries Res 2004, 38 Suppl 1, 24-33. [CrossRef]
- Anusavice KJ. Dental caries: risk assessment and treatment solutions for an elderly population. Compend Contin Educ Dent 2002, Oct;23(10 Suppl),12-20.
- Tan HP, Lo EC. Risk indicators for root caries in institutionalized elders. Community Dent Oral Epidemiol 2014, Oct;42(5), 435-40. [CrossRef]
- Edman K, Öhrn K, Nordström B, Holmlund A, Hellberg D Trends over 30 years in the prevalence and severity of alveolar bone loss and the influence of smoking and socio-economic factors – based on epidemiological surveys in Sweden 1983–2013. Int J Dent Hyg 2015, 13, 283-291. [CrossRef]
- Wahlin Å, Papias A, Jansson H, Norderyd O. Secular trends over 40 years of periodontal health and disease in individuals aged 20–80 years in Jonkoping, Sweden: repeated cross-sectional studies. J Clin Periodontol 2018, 45, 1016-1024. [CrossRef]
- Featherstone JD. The continuum of dental caries--evidence for a dynamic disease process. J Dent Res 2004, 83(Spec No C:C39-42). [CrossRef]
- Kidd EA, Fejerskov O What constitutes dental caries? Histopathology of carious enamel and dentin related to the action of cariogenic biofilms. J Dent Res 2004, 83(Spec Iss C), C35-C38. [CrossRef]
- Locker D. Dental status, xerostomia and the oral health-related quality of life of an elderly institutionalized population. Spec Care Dentist 2003, 23(3), 86-93. [CrossRef]
- Ikebe K, Matsuda K, Morii K, Wada M, Hazeyama T, Nokubi T, Ettinger RL. Impact of dry mouth and hyposalivation on oral health-related quality of life of elderly Japanese. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007, Feb;103(2), 216-22. [CrossRef]
- Hahnel S, Schwarz S, Zeman F, Schafer L, Behr M, Prevalence of xerostomia and hyposalivation and their association with quality of life in elderly patients in dependence on dental status and prosthetic rehabilitation. A pilot study. Journal of Dentistry 2014, 42(6), 664-670. [CrossRef]
- Thomson WM, Lawrence HP, Broadbent JM, Poulton R. The impact of xerostomia on oral-health related quality of life among younger adults. Health Qual Life Outcomes 2006, 8(4), 86. [CrossRef]
- Ohara Y, Hirano H, Yoshida H, Obuchi S, Ihara K, Fujiwara Y, Mataki S. Prevalence and factors associated with xerostomia and hyposalivation among community-dwelling older people in Japan. Gerodontology 2016, Mar;33(1), 20-7. [CrossRef]
- Johansson AK, Johansson A, Unell L, Ekback G, Ordell S Carsson GE, Self-reported dry mouth in Swedish population samples aged 50, 65 and 75 years. Gerodontology, 2012, 29, e107-115. [CrossRef]
- Turner MD, Ship JA. Dry mouth and its effects on the oral health of elderly people. JADA 2007, 138(Suppl), P15S-20S. [CrossRef]
- Napenas JJ, Brennan MT, Fox PC. Diagnosis and treatment of xerostomia (dry mouth). Odontology 2009, 97(2), 76-83. [CrossRef]
- Mignogna MD, Fedele S, Lo Russo L, Lo Muzio L, Wolff A. Sjogren ‘s Syndrome: The diagnostic potential of early oral manifestations precenting hyposalivation/xerostomia. J Oral Pathol Med 2005, 34(1), 1-6. [CrossRef]
- Billings RJ, Proskin HM, Moss ME. Xerostomia and associated factors in a community-dwelling adult population. Community Dent Oral Epidemiol 1996, Oct;24(5),312-6. [CrossRef] [PubMed]
- Sandberg GE, Sundberg HE, Fjellstrom CA, Wikblad KF. Type 2 diabetes and oral health: a comparison between diabetic and non-diabetic subjects. Diabetes Res Clin Pract 2000, 50(1), 27-34. [CrossRef]
- Soell M, Hassan M, Miliauskaite A, Haïkel Y, Selimovic D. The oral cavity of elderly patients in diabetes. Diabetes Metab 2007, 33 Suppl 1, S10-8. [CrossRef]
- Vasconcelos AC, Soares MS, Almeida PC, Soares TC. Comparative study of the concentration of salivary and blood glucose in type 2 diabetic patients. J Oral Sci, 2010, 52(2), 293-8. [CrossRef]
- Sreebny LM, Schwartz SS. A reference guide to drugs and dry mouthQ2nd edition. Gerodontology 1997, 14(1), 33-47. [CrossRef]
- Thomson WH, Chalmers JM, Spencer AJ, Slade ED. Medication and dry mouth: findings from a cohort study of older people. J Public Health Den 2000, 60(1), 12-20. [CrossRef]
- Scully C. Drug effects on salivary glands: dry mouth. Oral Diseases 2003, 9, 165-76. [CrossRef]
- Atkinson JC, Grisius M, Massey W. Salivary hypofunction and xerostomia: diagnosis and treatment. Dent Clin North Am 2005, 49(2),309-26. [CrossRef]
- McCann TV, Clark E, Lu S. Subjective side effects of antipsychotics and medication adherence in people with schizophrenia. J Adv Nursing 2009,534-43. [CrossRef]
- Steele JG, Sheiham A, Marcenes W, Fay N, Walls AW. Clinical and behavioural risk indicators for root caries in older people. Gerodontology. 2001 Dec;18(2):95-101. [CrossRef] [PubMed]
- Faine MP, Allender D, Baab D, Persson R, Lamont RJ. Dietary and salivary factors associated with root caries. Spec Care Dentist. 1992 Jul-Aug;12(4):177-82. [CrossRef] [PubMed]
- MacEntee MI, Clark DC, Glick N. Predictors of caries in old age. Gerodontology 1993, Dec;10(2), 90-7. [CrossRef] [PubMed]
- Kashket S, Yaskell T, Murphy JE. Delayed effect of wheat starch in foods on the intraoral demineralization of enamel. Caries Res 1994, 28(4), 291-6. doi: 10.1159/000261988. PMID: 8069887. [CrossRef] [PubMed]
- Pollard MA. Potential cariogenicity of starches and fruits as assessed by the plaque-sampling method and an intraoral cariogenicity test. Caries Res 1995, 29(1), 68-74. [CrossRef] [PubMed]
- Lingström P, Liljeberg H, Björck I, Birkhed D. The relationship between plaque pH and glycemic index of various breads. Caries Res 2000 Jan-Feb;34(1), 75-81. [CrossRef] [PubMed]
- Friedlander AH, Friedlander IK, Gallas M, Velasco E. Late-life depression: its oral health significance. Int Dent J. 2003 Feb;53(1):41-50. [CrossRef] [PubMed]
- Saunders RH, Meyerowitz C. Dental caries in older adults. Dental Clinics of North America 2005, 49(2), 293–308. [CrossRef]
- Hujoel, P. Dietary carbohydrates and dental-systemic diseases. Journal of Dental Research 2009, 88, 490–502. [CrossRef]
- Yoshihara A, Watanabe R, Hanada N, Miyazaki H. A longitudinal study of the relationship between diet intake and dental caries and periodontal disease in elderly Japanese subjects. Gerodontology 2009, Jun;26(2), 130-6. [CrossRef] [PubMed]
- Forssten SD, Björklund M, Ouwehand AC. Streptococcus mutans, caries and simulation models. Nutrients 2010, Mar;2(3), 290-8. [CrossRef]
- Hujoel PP, Lingström P. Nutrition, dental caries and periodontal disease: a narrative review. J Clin Periodontol 2017, Mar;44 Suppl 18, S79-S84. [CrossRef] [PubMed]
- Abranches J, Zeng L, Kajfasz JK, Palmer SR, Chakraborty B, Wen ZT, Richards VP, Brady LJ, Lemos JA. Biology of Oral Streptococci. Microbiol Spectr 2018, Oct;6(5),10.1128/microbiolspec.GPP3-0042-2018. [CrossRef]
- Marshall TA. Dietary Implications for Dental Caries: A Practical Approach on Dietary Counseling. Dent Clin North Am 2019, Oct;63(4), 595-605. [CrossRef] [PubMed]
- Sachdev PK, Freeland-Graves J, Babaei M, Sanjeevi N, Zamora AB, Wright GJ. Associations Between Diet Quality and Dental Caries in Low-Income Women. J Acad Nutr Diet 2021, Nov;121(11), 2251-2259. [CrossRef] [PubMed]
- Roberts JM, Bradshaw DJ, Lynch RJM, Higham SM, Valappil SP. The cariogenic effect of starch on oral microcosm grown within the dual constant depth film fermenter. PLoS ONE 2021, 16(10), e0258881. [CrossRef]
- Jayasinghe TN, Harrass S, Erdrich S, King S, Eberhard J. Protein Intake and Oral Health in Older Adults-A Narrative Review. Nutrients 2022, Oct 25;14(21):4478. [CrossRef]
- Castro RJ, Gambetta-Tessini K, Clavijo I, Arthur RA, Maltz M, Giacaman RA. Caries Experience in Elderly People Consuming a Milk-Based Drink Nutritional Supplement: A Cross-Sectional Study. Caries Res. 2023;57(3):211-219. [CrossRef] [PubMed]
- Guideline: Sugars Intake for Adults and Children. Geneva: World Health Organization; 2015. [PubMed]
- American Diabetes Association. Standards of medical care in diabetes--2008. Diabetes Care 2008, Jan;31 Suppl 1,S12-54. [CrossRef] [PubMed]
- NNR. Nordic Nutrition Recommendations 2012. Nordic Council of Ministers 2014, Narayana Press. ISBN 978-92-893-2.
- Lingström P, van Houte J, Kashket S. Food starches and dental caries. Crit Rev Oral Biol Med 2000, 11(3), 366-80. [CrossRef] [PubMed]
- Zussman E, Yarin AL, Nagler RM. Age- and flow-dependency of salivary viscoelasticity. J Dent Res 2007, Mar;86(3,:281-5. [CrossRef] [PubMed]
- Carvalho TS, Lussi A. Age-related morphological, histological and functional changes in teeth. J Oral Rehabil 2017, Apr;44(4),291-298. [CrossRef] [PubMed]
- Ettinger RL. The unique oral health needs of an aging population. Dent Clin North Am 1997, Oct;41(4), 633-49. [CrossRef] [PubMed]
- Quirk SE, Williams LJ, O’Neil A, Pasco JA, Jacka FN, Housden S, Berk M, Brennan SL. The association between diet quality, dietary patterns and depression in adults: a systematic review. BMC Psychiatry 2013, Jun 27;1, 175. [CrossRef]
- Petersen PE Sociobehavioural risk factors in dental caries – international perspectives. Community Dent Oral Epidemiol 2005, 33(4), 274-279. [CrossRef]
- Ritter AV, Shugars DA, Bader JD. Root caries risk indicators: a systematic review of risk models. Community Dent Oral Epidemiol 2010, Oct;38(5), 383-97. [CrossRef]
- Locker D. Incidence of root caries in an older Canadian population. Community Dent Oral Epidemiol 1996, 24, 403–7. [CrossRef]
- Lawrence HP, Hunt RJ, Beck JD. Three-year root caries incidence and risk modeling in older adults in North Carolina. J Public Health Dent 1995, 55, 69–78. [CrossRef]
- Powell LV, Mancl LA, Senft GD. Exploration of prediction models for caries risk assessment of the geriatric population. Community Dent Oral Epidemiol 1991, 19, 291–5. [CrossRef]
- Gati D, Vieira AR. Elderly at greater risk for root caries: a look at the multifactorial risks with emphasis on genetics susceptibility. Int J Dent 2011, 2011:647168. [CrossRef]
- Johnson MF. The role of risk factors in the identification of appropriate subjects for caries clinical trials: design considerations. J Dent Res 2004, 83(Spec No C), C116–8.
- Edman K, Holmlund A, Norderyd O. ‘Caries disease among an elderly population-A 10-year longitudinal study’. Int J Dent Hyg 2021, May;19(2),166-175. [CrossRef] [PubMed]
- White DA, Tsakos G, Pitts NB, Fuller E, Douglas GV, Murray JJ, Steele JG. Adult Dental Health Survey 2009: common oral health conditions and their impact on the population. Br Dent J 2012, Dec;213(11), 567-72. [CrossRef] [PubMed]
- Chalmers JM. Minimal intervention dentistry: part 1. Strategies for addressing the new caries challenge in older patients. J Can Dent Assoc 2006, Jun;72(5), 427-33.
- Yoshihara A, Suwama K, Miyamoto A, Watanabe R, Ogawa H. Diet and root surface caries in a cohort of older Japanese. Community Dent Oral Epidemiol 2021, Jun;49(3), 301-308. [CrossRef] [PubMed]
- Liu L, Zhang Y, Wu W, Cheng M, Li Y, Cheng R. Prevalence and correlates of dental caries in an elderly population in northeast China. PLoS One 2013, Nov 19;8(11), e78723. [CrossRef]
- Shah N, Sundaram KR. Impact of socio-demographic variables, oral hygiene practices, oral habits and diet on dental caries experience of Indian elderly: a community-based study. Gerodontology 2004, Mar;21(1), 43-50. [CrossRef] [PubMed]
- Papas AS, Joshi A, Palmer CA, Giunta JL, Dwyer JT. Relationship of diet to root caries. Am J Clin Nutr 1995, Feb;61(2), 423S-429S. [CrossRef] [PubMed]
- Takahashi N, Nyvad B. Ecological Hypothesis of Dentin and Root Caries. Caries Res 2016,50(4),422-31. [CrossRef] [PubMed]
- Duke A, MacInnes A. What are the main factors associated with root caries? Evid Based Dent 2021, Jan;22(1),16-17. [CrossRef] [PubMed]
- Costa SM, Martins CC, Bonfim Mde L, Zina LG, Paiva SM, Pordeus IA, Abreu MH. A systematic review of socioeconomic indicators and dental caries in adults. Int J Environ Res Public Health 2012, Oct 10,9(10), 3540-74. [CrossRef]
- Schwendicke F, Dörfer CE, Schlattmann P, Foster Page L, Thomson WM, Paris S. Socioeconomic inequality and caries: a systematic review and meta-analysis. J Dent Res 2015, Jan;94(1), 10-8. [CrossRef] [PubMed]
- Listl S. Income-related inequalities in dental service utilization by Europeans aged 50+. J Dent Res 2011, 90, 717–23. [CrossRef]
- Han DH, Khang YH, Choi HJ. Association of parental education with tooth loss among Korean Elders. Community Dent Oral Epidemiol 2015, 43, 489–99. [CrossRef]
- Wang L, Cheng L, Yuan B, Hong X, Hu T. Association between socio-economic status and dental caries in elderly people in Sichuan Province, China: a cross-sectional study. BMJ Open 2017, Sep 24;7(9, :e016557. [CrossRef]
- Hobdell MH, Oliveira ER, Bautista R, et al. Oral diseases and socioeconomic status (SES). Br Dent J 2003, 194, 91–6. discussion 88. [CrossRef] [PubMed]
- Steele J, Shen J, Tsakos G, Fuller E, Morris S, Watt R, Guarnizo-Herreño C, Wildman J. The Interplay between socioeconomic inequalities and clinical oral health. J Dent Res 2015, Jan;94(1), 19-26. [CrossRef] [PubMed]
- Kim DW, Park JC, Rim TT, Jung UW, Kim CS, Donos N, Cha IH, Choi SH. Socioeconomic disparities of periodontitis in Koreans based on the KNHANES IV. Oral Dis 2014, Sep;20(6), 551-9. [CrossRef] [PubMed]
- Shimazaki Y, Soh I, Koga T, Miyazaki H, Takehara T. Risk factors for tooth loss in the institutionalised elderly; a six-year cohort study. Community Dent Health 2003, Jun;20(2), 123-7. [PubMed]
- Ellefsen B, Holm-Pedersen P, Morse DE, Schroll M, Andersen BB, Waldemar G. Assessing caries increments in elderly patients with and without dementia: a one-year follow-up study. J Am Dent Assoc 2009, Nov;140(11), 1392-400. [CrossRef] [PubMed]
- Ortega O, Parra C, Zarcero S, Nart J, Sakwinska O, Clavé P. Oral health in older patients with oropharyngeal dysphagia. Age Ageing 2014, Jan;43(1), 132-7. [CrossRef]
Figure 1.
Flow chart of the study showing the number of studies during identification and screening.
Figure 1.
Flow chart of the study showing the number of studies during identification and screening.
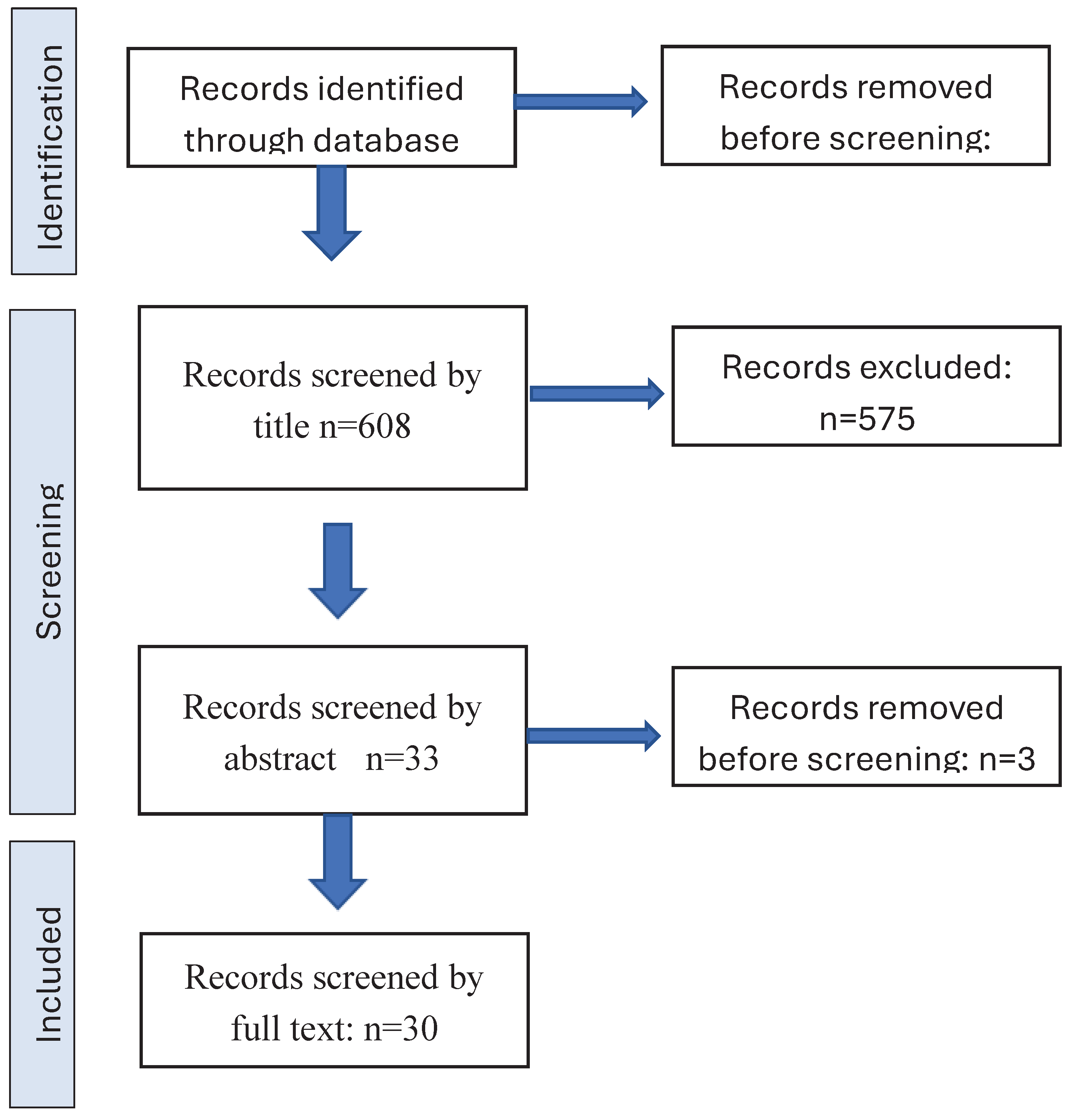

Table 1.
Literature on caries and diet.
 |
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



