
Submitted:
04 March 2024
Posted:
05 March 2024
Read the latest preprint version here
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: Here, we investigated the inflammaging and physical performance in older adults before and after the COVID-19 pandemic. Methods: Women(n=18) and men(n=7) older were evaluated before the COVID-19 pandemic(PRE), 12 months after the lockdown(POST), and 10 months after resuming exercise training(POS-TR). Physical tests [gait speed(GS) and timed-up-and-go(TUG)]; muscle strength (handgrip-HG), and serum cytokine levels were assessed. Results: The older women showed higher GS and TUG at POST than PRE and POST-TR, besides lower HG at POST-TR than PRE, whereas older men exhibited lower HG at POST and POST-TR than PRE. Both groups presented (1)lower IL-10 and IL-12p70 values in contrast to higher IL-6/IL-10 and IL-8/IL-10 ratios at POST than PRE; (2)higher IL-10 values and lower IL-8/IL-10 ratio at POST-TR than POST; (3)higher IL-12p70/IL-10 ratio at POST-TR than PRE and POST. Particularly older women showed: (4)lower IL-6 values at POST and POST-TR than PRE; (5)lower IL-8 and IL-10 values at POST-TR than POST; (6)and higher TNF-α/IL-10 and IFN-γ/IL-10 ratios at POST than PRE and POST-TR. Significant correlations between the variables were found in both groups. Conclusion: During the COVID-19 pandemic, detraining and resumption of exercise training promoted distinct alterations in physical capacity and inflammaging among older women and older men population.
Keywords:
aging
; older people
; citokines
; gait speed
; TUGT
; handgrip
INTRODUCTION
Among the most remarkable achievements by humanity
over the last two centuries is the increase in human lifespan, which was extended mainly due to the improvement of worldwide public health policy and modern medicine [1,2]. As a consequence of this triumph, the population over 65 years, which was around 8,5-9% in 2019, in accordance with the global estimate will increase to 12% in 2030 and 17% in 2050 [3]. Although the recent COVID-19 pandemic, unfortunately, caused a higher number of deaths, particularly of older adults, the estimates concerning the pace of population aging is still accelerated [4]. However, it is paramount to mention that living longer is not closely associated with living with health since it is evidenced that the expansion in lifespan is accompanied by the high prevalence of several chronic diseases and comorbidities, such as cancer, diabetes, cardiovascular, renal, lung, liver, neurological diseases, sarcopenia, frailty, and also an increased susceptibility to infectious diseases, which directly impacts the survival and well-being of older people [5,6]. Therefore, in order to minimize the burden on health systems and maintain quality of life in the aging process, the World Health Organization (WHO) has worked to stimulate public policies aimed at promoting healthy aging [7].
Regarding aging, it is a natural, dynamic, and multifactorial process characterized by a progressive decline of the majority of physiological systems [2,8]. Among these systems, the immunological is one of the most affected by aging and leads to the development of the phenomenon named immunosenescence, which affects both innate and adaptive immunity [9,10,11]. From 2000, when Prof. Francheschi and collaborators published the article entitled “Inflammaging: an evolutionary perspective on immunosenescence” [12], the literature has highlighted that one of the main players involved in the development and progression of immunosenescence is the phenomenon inflammaging, which translate a chronic, sterile, low-grade inflammation associated with aging. It has been reported that the increased systemic levels of some pro-inflammatory mediators, particularly the C-reactive protein (CRP), interleukins (ILs) such as IL-1, IL-6, IL-8, IL-12, the tumor necrosis factor-alpha (TNF-α), and the interferon-gamma (IFN-γ), in association with the decreased levels of IL-1Ra and IL-10, two well-known anti-inflammatory cytokines, characterizes the inflammaging [13,14]. Furthermore, it is worth mentioning that these both phenomena (immunosenescence and inflammaging) presented a virtuous circle since one can fuel the other [15] and also can be pillars to the increased risk of the occurrence of chronic and infectious diseases in older adults [16].
In order to mitigate the deleterious effect of aging, especially in the older adult population, it is consensus that some
approaches related to achieving an adequate nutritional status and regular physical exercise practice are considered powerful strategies in this context [17,18]. It is broadly accepted that the adoption
and maintenance of an active lifestyle, through lifelong training, can maintain
performance related to endurance and strength, as also muscle mass, favoring
healthy aging in different ways, which includes the regulation of systemic
inflammatory status by increasing the IL-10 and decrease IL-6, IL-8, TNF-α, and
CRP [15,19,20].
In opposite to the benefits of regular physical
exercises in aging, a sedentary lifestyle and a decrease of strength and
skeletal muscle are related to an increased risk to develop chronic diseases,
comorbidities and premature mortality [21,22].
At this point, it is of utmost importance to highlight that, regarding the
literature, during the confinement imposed by COVID-19 there was a significant
elevation in sedentary behavior [23,24].
Although the WHO declared the end of the COVID-19
pandemic in May 2023, the consequences of the alteration in lifestyle imposed
by the pandemic, particularly associated with the interruption of the regular
practice of physical exercises on the inflammaging phenomenon in the older
adult population, is until unclear. Therefore, in the present study, we
investigated the effect of the interruption of the regular physical exercise
imposed by the COVID-19 pandemic and the consequences of the return to this
exercise training program on the inflammaging in a group of older adults.
MATERIAL AND METHODS
Participants and Study Design
This study is an interventional, multifactorial,
and retrospective and prospective study, involving 25 older adults of both
sexes (7 men and 18 women), aged 65-85, who had been engaged in combined
exercise training for, at least, 24 months before COVID-19. Data were collected
at three time points: pre-pandemic (April-May 2019), post 12-month pandemic
hiatus (February-March 2021), and post 10-months of resumed exercise training
(November-December 2022).
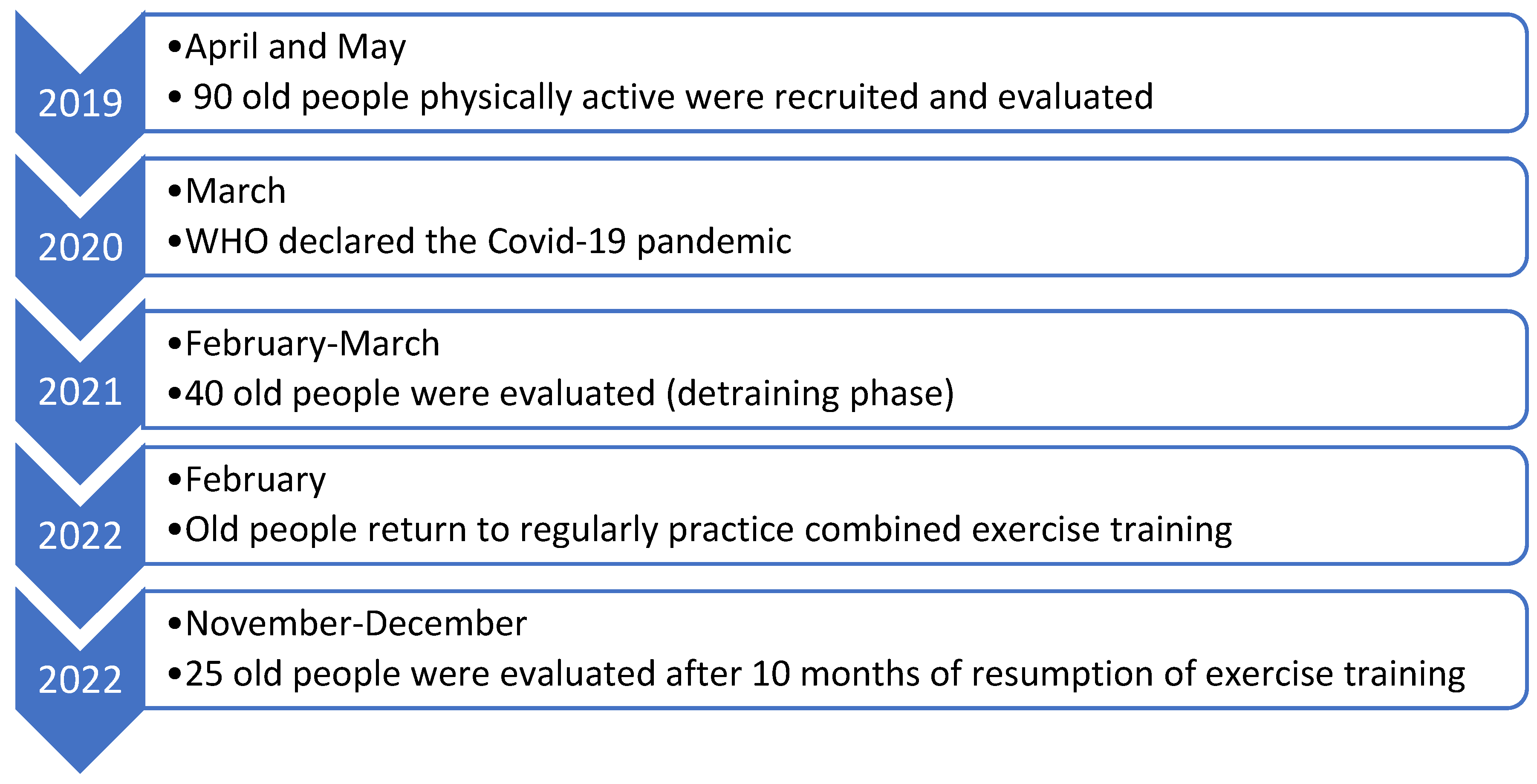
All volunteers took part in both a Primary Health
Care Program for Older Adults at the Federal University of São Paulo (UNIFESP),
Brazil, and the "Mané Garrincha" Sports and Education Center. As
presented in Figure 1, in 2019, a pool of
over 90 volunteers was enrolled to participate in a previous study. In 2021,
during the COVID-19 pandemic, only 40 volunteers accepted to participate in the
present study and this number dropped again to 25 older adults in 2022 due to
various pandemic-related factors. The study adhered to the Transparent
Reporting of Evaluations with Nonrandomized Designs (TREND) guidelines [25].
All study procedures were thoroughly explained to
the participants, who then provided informed consent, previously reviewed and
approved by the Research Ethics Committees at UNIFESP (number 3,623,247) and
the University of Santo Amaro - UNISA (numbers 4,350,476 and 5,318,499),
ensuring compliance with Brazilian Resolution (196/96) on research ethics with
human subjects [26] and the Helsinki
Declaration [27]. The study also followed
international guidelines for ethics in physical exercise science research [28].
Inclusion and exclusion criteria were carefully
designed and evaluate by a single physician to ensure the safety and relevance
of the participant pool. The inclusion criteria were: (i) to be older than 60
years, (ii) have the autonomy to move to the exercise training center, (iii)
receive medical clearance to engage in the exercise program, and (iv) perform
the same exercise program and be supervised by the same physical education
professional. The exclusion criteria were: (i) present diagnosis of mental and
physical illness, neoplasm, renal and liver diseases, Type-1 Diabetes Mellitus,
chronic infections or out-of-control cardiovascular and metabolic disease, (ii)
present symptoms or diagnosis of respiratory infections, (iii) use of
anti-inflammatory drugs or multivitamin/antioxidant supplements until the last
2 months before the evaluations.
Figure 1.
Timeline of study design.
Combined Exercise Training Program
The combined exercise training program, formerly
described [9], was composed of aerobic and
resistance exercises and was performed three times per week, lasting 60–75
minutes, for, at least, 24 months pre-pandemic, and for 10 months in 2022,
during COVID-19 pandemic.
Anthropometric Data and Physical Tests
The Body Mass Index (BMI) of each volunteer was
calculated by measuring height and body weight measured on digital scale and
stadiometer (Personal® scale, Filizzola, São Paulo, Brazil). Physical tests
were assessed through the tests Time-Up-Go (TUG) and Gait Speed (GS), and the
muscle strength was evaluated through handgrip strength (HG) using an analog
dynamometer (Jamar Hydraulic Hand Dynamometer®, Sammons Preston Rolyan,
Bollingbrook, IL, USA). We used protocols previously described in our study [29].
Blood Sample Collection and Analysis
Blood samples were collected at three different
occasions: pre-pandemic (PRE, in 2019), post-pandemic (POST, in 2021), and
post-training resumption (POST-TR, in 2022). Serum levels of pro- and
anti-inflammatory cytokines (IL-6, IL-8, IL-10, IL-12p70, TNF-α, and IFN-γ)
were determined using multiplex assay (LEGENDplex™ bead-based multiplex assays,
Biolegend, San Diego, CA, USA) and analyzed with a BD Accuri™C6 Plus Flow
Cytometer (BD Biosciences San Jose. CA. USA), following the data analysis with
LEGENDPlex™ V8.0 software (Biolegend).
Statistical Analysis
Data normality and variance homogeneity were
assessed using Shapiro-Wilk and Levene’s tests. Differences between parametric
(anthropometrics and physical function) and non-parametric variables
(cytokines) were analyzed using one-way ANOVA with Tukey´s posthoc test and the
Friedman test with Bonferoni´s posthoc test, respectively. Spearman´s rank
correlation coefficient evaluated associations between variables. A
significance level of 5% (p<0.05) was set. Analyses were performed using
GraphPad Prism version 10.1.1 (GraphPad Software, Boston, Massachusetts USA).
RESULTS
Table 1 shows
the data concerning anthropometric (age, weight, height, and BMI), physical
tests (GS, TUG), and muscle strength (HG) of the older groups (women and men)
participants in this study. In addition to the significant chronological ageing
of the all volunteers, notably the older women presented a significant worst
performance not only in GS at POST compared to PRE and POST-TR but also in TUG
test at POST in comparison to PRE, as well as lower HG values at POST-TR than
at PRE. Older men exhibited a significant decrease in HG values at POST and
POST-TR compared to PRE.
As presented in the up panel of Figure 2, lower levels of IL-10 (2C) and IL-12p70 (2D) were found in both groups at POST than at PRE. A significant reduction in IL-6 (2A) was verified both at POST and POST-TR compared to PRE, particularly in older women. Reduced levels of IL-8 (2B), in contrast to increased IL-10 (2C), were found in older women at POST compared to POST-TR. Lastly, IL-10 (2C) levels were significantly higher in both groups at POST-TR than at POST. Levels of TNF-α (2E) and IFN-γ (2F) were unchanged.
The lower panel at Figure 2 shows the ratios between pro-inflammatory cytokines and IL-10. At POST, whereas both groups presented a significant increase in the ratios of IL-6/IL-10 (2G) and IL-8/IL-10 (2H), a higher TNF-α /IL-10 ratio (2K) was observed in the older women than at PRE. In contrast, at POST-TR, not only did the older women present a lower TNF-α /IL-10 ratio (2K) but also both groups showed a reduced IL-8/IL-10 ratio (2H) compared to POST. Interestingly, the IL-12p70/IL-10 ratio (2I) was higher at POST-TR than at PRE and POST, in both groups. Table S1 shows the values of cytokines and the ratios between IL-10 and the inflammatory cytokines.
Data obtained in Spearman's correlation analysis, particularly in the older women's group (Table 2), revealed positive associations between BMI and TUG, and also between IL-6, IL-10 or IL-12p70 in all time points assessed. Age correlated positively with the IL-12p70/IL-10 ratio at PRE and POST-TR, whilst GS correlated positively with IL-10 at PRE. Several other positive correlations between anthropometrics, physical function tests, and cytokines were evidenced at PRE, POST, and POST-TR, whereas negative correlations between GS and TUG at POS and POST-TR, GS and Age or IL-12p70/IL-10 ratio at PRE, GS and IL-8/IL-10 ratio at POST. And exclusively at POST, the muscle strength, assessed by HG, and IL-12p70, or the ratios IL-12p70/IL-10 and IL-8/IL-10 were found.
Concerning the older men group, as shown the Table 3, positive correlations between IL-10 and IL-6 or IL-8, and a negative correlation between TUG and IL-10 were found at PRE and POST-TR. The GS and IFN-γ were negatively correlated in PRE. The HG negatively correlated with the TNF-α/IL-10 ratio at POST and with TNF-α, IFN-γ, and IFN-γ/IL-10 ratio at POST-TR, in contrast to positive correlation with IL-10 at POST-TR. Other positive and negative correlations were found between anthropometrics, physical function tests, and cytokines on all occasions assessed here. Table S1 shows the values of cytokines and the ratios between IL-10 and the inflammatory cytokines.
DISCUSSION
In general, our results showed that: (i) the interruption of regular physical exercise for a year negatively impacted both the performance of physical tests, which could supposedly impair the ability to perform some daily activities, and the control of the systemic inflammatory state, since deregulation of inflammation was mainly evidenced during this period; (ii) ten months of regular involvement in combined exercise training was able to reverse or even mitigate the inflammatory disturbance, although the performance of some physical tests was not improved; and (iii) the interruption and resuming of exercise training impacted differently older women and older men.
Although we were able to show interesting findings, some aspects need to be mentioned, such as, unfortunately, due to issues related to the COVID-19 pandemic (for example, change of address to distant locations and the fear of contamination), it was impossible to complete the study with the initially eligible volunteers. Since the aging process of skeletal muscle, immune, and inflammation occurs differently in men and women [8,30], the aged people were assessed separately. Besides, our volunteers were robust [31] and very active pre-pandemic, including performing 600 minutes of moderate-intensity activities per week, presented positive adaptations in physical and inflammatory aspects, as we have shown in previous studies [32], thus, even with the decrease in physical performance during the COVID-19 pandemic, the evaluations of some physical determinants of intrinsic capacity suggest a successful aging process by these volunteers [33].
It was reported that lockdown related to the COVID-19 pandemic increased sedentary behavior and detraining [23,24] which could putatively justify the reduction in physical performance found here. Additionally, some results of this study can reinforce already-known associations, such as the influence of age and BMI in physical tests involving body movement, and the fact that GS and TUG tests can evaluate similar muscle functions [29]. In this sense, studies performed during the COVID-19 pandemic revealed the nullification of physical and metabolic benefits of exercise training after detraining. For instance, a reduction of 5%, 15%, and 17% in muscle strength and power and type II thigh muscle fibers after 12 weeks of social isolation [34], as well as a decrease in muscle functions, type II fibers, and satellite cells post-12 months of sedentary behavior were reported [35]. As expected, our results showed differences between the groups, since after twelve months of detraining the older women’s group showed reductions of 37% and 7%, in GS and TUG tests, respectively, and the older men group showed a decrease around of 10% in HG. Thus, specifically during this period, whereas women lost lower limb physical performance, the men's upper limb performance. Some possible explanations for these discrepant observations could be associated with the fact that: (i) although the literature mentions that women lose muscle strength earlier than men [36] during aging, the absence of significant HG strength loss in the women’s group, in the detraining phase, could be related to cultural reasons, since during the confinement period these women were possibly involved with domestic tasks, which could supposedly attenuate the reduction of muscle strength in this group [37]; besides (ii) by generally being stronger [36], the ceiling effect [38] could have occurred in the application of the physical tests in the older men, as the GS and TUG, have low correlation with classic strength tests [29].
Another remarkable observation found here was associated with the fact that the return to physical training did not "reverse" or mitigate the effect of detraining in this strength parameter on both groups. Studies demonstrated that twelve weeks of regular physical training, after eight weeks of detraining, should be sufficient to recover the architecture, strength, and muscle power [34]. Likewise, notable neuromuscular adaptations could be achieved, in these volunteers, after ten months of regular physical training practice [39]. Despite the physical aspects of 'muscle memory' [40] were not evaluated here, the fact is that none of the volunteer groups, after 10 months of training, reached pre-pandemic HG results, even if it could be expected [41]. Regarding muscle plasticity after a long period of detraining, it is known that epigenetic factors are fundamental [42], so the significant reduction in muscle strength assessed by the HG, an average of 10% in both groups, could be supposedly associated not only with the aging process but also with behavioral, dietary, and nutritional issues related to the pandemic, recalling that none of the volunteers presented clinical symptoms related to COVID-19 during the study.
Each day, studies present different biomarkers that can be useful to determine both successful aging and vulnerabilities to frailty, as well as the physical performance and inflammaging phenomenon [2]. In this respect, it is known that cytokines present a myriad of actions and older adults who regularly practice physical exercises presented an exemplary phenotype of the best regulations of inflammaging [19]. Although the systemic levels of IL-6, IL-8, IL-12p70, and IL-10 were higher at PRE, and these findings putatively suggested that long-standing physical exercise would drive the systemic state toward a pro-inflammatory direction, the data obtained in the ratios between pro- and anti-inflammatory cytokines, in general, demonstrated an inflammatory status regulated pre-pandemic [32], a significant deregulation during detraining phase [43,44], and a "return" of regulated status with the resumption of exercise training [19].
Based on our results, these variations in inflammatory status found in both groups can closely be related to the anti-inflammatory properties of IL-10 [13], which were reduced in the detraining phase and increased with the resumption of exercise training. It is known that exercise training can improve the circulating IL-10 levels, which strengthens its role in the regulation of inflammaging [19]. During physical exercise, muscle contraction activates the transcription of several genes, mainly IL-6 that, among some actions, promote IL-10 releases, which lead to the control of inflammation in this context [17]. Particularly, our data concerning the ratios between the pro-inflammatory cytokines IL-6, IL-8, TNF-α, and IFN-γ, with IL-10, reinforces this remarkable capacity of exercise training in improving IL-10 levels, which, consequently, can favor the regulation of the systemic inflammatory state, including in older population. Likewise, the increase in the IL-12p70/IL-10 ratio in 2022 (at POST-TR), not only is interesting but also could represent a lack of systemic inflammatory control. However, the literature claims that IL-12p70 is pivotal both in increasing the immune cells' activity, especially Natural Killer (NK) cells, and its increase have been associated with successful aging [45].
Taking together, our data allows us to suppose that the interruption of regular physical exercise during the COVID-19 pandemic, in this physically active older population, led to a prominent imbalance in systemic cytokine levels that favored the progression of the inflammatory phenomenon, as previously reported in sedentary older people [20,46] and detrained individuals, also related to COVID-19 [44].
Regarding the correlations between physical function tests and cytokines, during the detraining period, it was found that better physical performance was associated with the best regulation of the systemic inflammatory state. Despite the older women group did not present significant alterations in the HG results, between pre-pandemic and during the detraining period, the correlations found illustrated that the stronger and faster volunteer presented advantages in the systemic inflammatory profile. Specifically to the older men group, the HG test was the most important evaluation both in the perception of strength loss during the detraining period and in the interpretation that greater muscle strength was associated with a balanced systemic inflammatory status. Indeed, the association between muscle strength and positive health outcomes has been the subject of investigation for a long time and seems to be a 'two-way street’ [17]. Based on these aspects and our results, we can suggest that not only the lifestyle alterations associated with the COVID-19 pandemic could negatively influence the benefits of years of regular physical training practice, but also those physically fitter older adults might be less affected, as previously described in the literature [19,22].
Interestingly, the associations between physical performance tests and the inflammatory phenomenon found after resuming training in the group of older men can reinforce the previous suggestion that stronger and faster volunteers might generate better conditions to mitigate the development and progression of inflammaging [22]. However, the lack of associations between these parameters in older women can suggest that ten months of resuming physical training is not enough to promote the same regulatory effect found in older men, although it was sufficient for the ratios between pro-inflammatory (IL-6, IL-8, TNF-α) and anti-inflammatory (IL-10) cytokines to become similar to the pre-pandemic period. These results strengthen the differences between genders during aging, although the increase in BMI and age can supposedly affect this balance [32]. Therefore, these differences between the groups of volunteers during detraining and the resumption of supervised physical training, during the COVID-19 pandemic, are unprecedented and can corroborate the literature, as both in vitro and/or in vivo studies have shown that men and women are differently affected by pro-inflammatory cytokines [30,47].
It is worth mentioning that our results reinforce the perception that multiple factors are involved in the inflammaging both in men and women. For instance, it has been reported that hormonal, genetic, and epigenetic factors could favor the generation of robust anti-inflammatory responses in women [30]. Furthermore, there is an understanding that the cytokine network is pleiotropic, as it presents redundant and overlapping activities associated with chemotaxis, proliferation, development, activation, and migration of different types of cells (immune, neuronal, muscular, and vascular endothelial, among others), in addition to demonstrating positive or negative actions, particularly related to their levels and chronicity [48].
As for the limitations of the study, they include: (a) the discrepant number of participants in each volunteer group; (b) the absence of a comparison group comprising sedentary older individuals, encompassing both women and men; (c) insufficient information regarding the participants' nutritional habits and levels of physical exercise; (d) a lack of data from other physical function tests; and (e) the absence of data collected immediately upon the resumption of supervised physical training.
CONCLUSION
The findings of this study lead us to propose that: (a) the regular practice of combined exercise training can benefit and help in regulating systemic inflammatory status; (b) the period of detraining significantly impacted physical functional capacity and contributed to the progression of the inflammaging process; and also (c) older individuals, both women and men, were differently influenced by both the detraining and the resumption of exercise training.
References
- Conway, J.; Certo, M.; Lord, J.M.; Mauro, C.; Duggal, N.A. Understanding the role of host metabolites in the induction of immune senescence: Future strategies for keeping the ageing population healthy. Br J Pharmacol 2022, 179, 1808–1824. [Google Scholar] [CrossRef]
- Moqri, M.; Herzog, C.; Poganik, J.R.; Biomarkers of Aging, C.; Justice, J.; Belsky, D.W.; Higgins-Chen, A.; Moskalev, A.; Fuellen, G.; Cohen, A.A.; et al. Biomarkers of aging for the identification and evaluation of longevity interventions. Cell 2023, 186, 3758–3775. [Google Scholar] [CrossRef] [PubMed]
- Almohaisen, N.; Gittins, M.; Todd, C.; Sremanakova, J.; Sowerbutts, A.M.; Aldossari, A.; Almutairi, A.; Jones, D.; Burden, S. Prevalence of Undernutrition, Frailty and Sarcopenia in Community-Dwelling People Aged 50 Years and Above: Systematic Review and Meta-Analysis. Nutrients 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Msemburi, W.; Karlinsky, A.; Knutson, V.; Aleshin-Guendel, S.; Chatterji, S.; Wakefield, J. The WHO estimates of excess mortality associated with the COVID-19 pandemic. Nature 2023, 613, 130–137. [Google Scholar] [CrossRef] [PubMed]
- MacNee, W.; Rabinovich, R.A.; Choudhury, G. Ageing and the border between health and disease. Eur Respir J 2014, 44, 1332–1352. [Google Scholar] [CrossRef] [PubMed]
- Soegiarto, G.; Purnomosari, D. Challenges in the Vaccination of the Elderly and Strategies for Improvement. Pathophysiology 2023, 30, 155–173. [Google Scholar] [CrossRef] [PubMed]
- Rudnicka, E.; Napierala, P.; Podfigurna, A.; Meczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, Q.D.; Moodie, E.M.; Forget, M.F.; Desmarais, P.; Keezer, M.R.; Wolfson, C. Health Heterogeneity in Older Adults: Exploration in the Canadian Longitudinal Study on Aging. J Am Geriatr Soc 2021, 69, 678–687. [Google Scholar] [CrossRef] [PubMed]
- Amirato, G.R.; Borges, J.O.; Marques, D.L.; Santos, J.M.B.; Santos, C.A.F.; Andrade, M.S.; Furtado, G.E.; Rossi, M.; Luis, L.N.; Zambonatto, R.F.; et al. L-Glutamine Supplementation Enhances Strength and Power of Knee Muscles and Improves Glycemia Control and Plasma Redox Balance in Exercising Elderly Women. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Kovaiou, R.D.; Herndler-Brandstetter, D.; Grubeck-Loebenstein, B. Age-related changes in immunity: implications for vaccination in the elderly. Expert Rev Mol Med 2007, 9, 1–17. [Google Scholar] [CrossRef]
- Fulop, T.; Larbi, A. Biology of aging: Paving the way for healthy aging. Exp Gerontol 2018, 107, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, C.; Bonafe, M.; Valensin, S.; Olivieri, F.; De Luca, M.; Ottaviani, E.; De Benedictis, G. Inflamm-aging. An evolutionary perspective on immunosenescence. Ann N Y Acad Sci 2000, 908, 244–254. [Google Scholar] [CrossRef] [PubMed]
- Minciullo, P.L.; Catalano, A.; Mandraffino, G.; Casciaro, M.; Crucitti, A.; Maltese, G.; Morabito, N.; Lasco, A.; Gangemi, S.; Basile, G. Inflammaging and Anti-Inflammaging: The Role of Cytokines in Extreme Longevity. Arch Immunol Ther Exp (Warsz) 2016, 64, 111–126. [Google Scholar] [CrossRef] [PubMed]
- Felismino, E.S.; Santos, J.M.B.; Rossi, M.; Santos, C.A.F.; Durigon, E.L.; Oliveira, D.B.L.; Thomazelli, L.M.; Monteiro, F.R.; Sperandio, A.; Apostolico, J.S.; et al. Better Response to Influenza Virus Vaccination in Physically Trained Older Adults Is Associated With Reductions of Cytomegalovirus-Specific Immunoglobulins as Well as Improvements in the Inflammatory and CD8(+) T-Cell Profiles. Front Immunol 2021, 12, 713763. [Google Scholar] [CrossRef] [PubMed]
- Fulop, T.; Larbi, A.; Dupuis, G.; Le Page, A.; Frost, E.H.; Cohen, A.A.; Witkowski, J.M.; Franceschi, C. Immunosenescence and Inflamm-Aging As Two Sides of the Same Coin: Friends or Foes? Front Immunol 2017, 8, 1960. [Google Scholar] [CrossRef]
- Fulop, T.; Dupuis, G.; Witkowski, J.M.; Larbi, A. The Role of Immunosenescence in the Development of Age-Related Diseases. Rev Invest Clin 2016, 68, 84–91. [Google Scholar]
- Severinsen, M.C.K.; Pedersen, B.K. Muscle-Organ Crosstalk: The Emerging Roles of Myokines. Endocr Rev 2020, 41, 594–609. [Google Scholar] [CrossRef]
- Coelho-Junior, H.J.; Calvani, R.; Tosato, M.; Landi, F.; Picca, A.; Marzetti, E. Protein intake and physical function in older adults: A systematic review and meta-analysis. Ageing Res Rev 2022, 81, 101731. [Google Scholar] [CrossRef] [PubMed]
- Minuzzi, L.G.; Rama, L.; Bishop, N.C.; Rosado, F.; Martinho, A.; Paiva, A.; Teixeira, A.M. Lifelong training improves anti-inflammatory environment and maintains the number of regulatory T cells in masters athletes. Eur J Appl Physiol 2017, 117, 1131–1140. [Google Scholar] [CrossRef]
- Lavin, K.M.; Perkins, R.K.; Jemiolo, B.; Raue, U.; Trappe, S.W.; Trappe, T.A. Effects of aging and lifelong aerobic exercise on basal and exercise-induced inflammation. J Appl Physiol (1985) 2020, 128, 87–99. [Google Scholar] [CrossRef]
- Martins, G.S.; Galvao, L.L.; Tribess, S.; Meneguci, J.; Virtuoso Junior, J.S. Isotemporal substitution of sleep or sedentary behavior with physical activity in the context of frailty among older adults: a cross-sectional study. Sao Paulo Med J 2023, 141, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, C.S.L.; Thang, L.A.N.; Maier, A.B. Markers of inflammation and their association with muscle strength and mass: A systematic review and meta-analysis. Ageing Res Rev 2020, 64, 101185. [Google Scholar] [CrossRef] [PubMed]
- Furtado, G.E.; Letieri, R.V.; Caldo-Silva, A.; Sardao, V.A.; Teixeira, A.M.; de Barros, M.P.; Vieira, R.P.; Bachi, A.L.L. Sustaining efficient immune functions with regular physical exercise in the COVID-19 era and beyond. Eur J Clin Invest 2021, 51, e13485. [Google Scholar] [CrossRef] [PubMed]
- Alomari, M.A.; Khabour, O.F.; Alzoubi, K.H. Changes in Physical Activity and Sedentary Behavior Amid Confinement: The BKSQ-COVID-19 Project. Risk Manag Healthc Policy 2020, 13, 1757–1764. [Google Scholar] [CrossRef] [PubMed]
- Des Jarlais, D.C.; Lyles, C.; Crepaz, N.; Group, T. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: the TREND statement. Am J Public Health 2004, 94, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Lima, S.G.; Lima, T.A.; Macedo, L.A.; Sa, M.P.; Vidal Mde, L.; Gomes, A.F.; Oliveira, L.C.; Santos, A.M. Ethics in research with human beings: from knowledge to practice. Arq Bras Cardiol 2010, 95, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Petrini, C. Helsinki 50 years on. Clin Ter 2014, 165, 179–181. [Google Scholar] [CrossRef]
- Shephard, R.J. Ethics in exercise science research. Sports Med 2002, 32, 169–183. [Google Scholar] [CrossRef] [PubMed]
- Santos, C.A.F.; Amirato, G.R.; Jacinto, A.F.; Pedrosa, A.V.; Caldo-Silva, A.; Sampaio, A.R.; Pimenta, N.; Santos, J.M.B.; Pochini, A.; Bachi, A.L.L. Vertical Jump Tests: A Safe Instrument to Improve the Accuracy of the Functional Capacity Assessment in Robust Older Women. Healthcare (Basel) 2022, 10. [Google Scholar] [CrossRef]
- Mauvais-Jarvis, F.; Bairey Merz, N.; Barnes, P.J.; Brinton, R.D.; Carrero, J.J.; DeMeo, D.L.; De Vries, G.J.; Epperson, C.N.; Govindan, R.; Klein, S.L.; et al. Sex and gender: modifiers of health, disease, and medicine. Lancet 2020, 396, 565–582. [Google Scholar] [CrossRef]
- Garfein, A.J.; Herzog, A.R. Robust aging among the young-old, old-old, and oldest-old. J Gerontol B Psychol Sci Soc Sci 1995, 50, S77–87. [Google Scholar] [CrossRef] [PubMed]
- Santos, C.A.F.; Amirato, G.R.; Paixão, V.; Almeida, E.B.; Do Amaral, J.B.; Monteiro, F.R.; Roseira, T.; Juliano, Y.; Novo, N.F.; Rossi, M.; et al. Association among inflammaging, body composition, physical activity, and physical function tests in physically active women. Frontiers in Medicine 2023, 10. [Google Scholar] [CrossRef] [PubMed]
- Aliberti, M.J.R.; Bertola, L.; Szlejf, C.; Oliveira, D.; Piovezan, R.D.; Cesari, M.; de Andrade, F.B.; Lima-Costa, M.F.; Perracini, M.R.; Ferri, C.P.; et al. Validating intrinsic capacity to measure healthy aging in an upper middle-income country: Findings from the ELSI-Brazil. Lancet Reg Health Am 2022, 12, 100284. [Google Scholar] [CrossRef] [PubMed]
- Blocquiaux, S.; Gorski, T.; Van Roie, E.; Ramaekers, M.; Van Thienen, R.; Nielens, H.; Delecluse, C.; De Bock, K.; Thomis, M. The effect of resistance training, detraining and retraining on muscle strength and power, myofibre size, satellite cells and myonuclei in older men. Exp Gerontol 2020, 133, 110860. [Google Scholar] [CrossRef] [PubMed]
- Snijders, T.; Leenders, M.; de Groot, L.; van Loon, L.J.C.; Verdijk, L.B. Muscle mass and strength gains following 6 months of resistance type exercise training are only partly preserved within one year with autonomous exercise continuation in older adults. Exp Gerontol 2019, 121, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Lauretani, F.; Russo, C.R.; Bandinelli, S.; Bartali, B.; Cavazzini, C.; Di Iorio, A.; Corsi, A.M.; Rantanen, T.; Guralnik, J.M.; Ferrucci, L. Age-associated changes in skeletal muscles and their effect on mobility: an operational diagnosis of sarcopenia. J Appl Physiol (1985) 2003, 95, 1851–1860. [Google Scholar] [CrossRef]
- McGee, C.; Mathiowetz, V. Reliability and validity of a novel instrument for the quantification of hand forces during a jar opening task. J Hand Ther 2022, 35, 488–500. [Google Scholar] [CrossRef]
- Santana, M.G.; de Lira, C.A.; Passos, G.S.; Santos, C.A.; Silva, A.H.; Yoshida, C.H.; Tufik, S.; de Mello, M.T. Is the six-minute walk test appropriate for detecting changes in cardiorespiratory fitness in healthy elderly men? J Sci Med Sport 2012, 15, 259–265. [Google Scholar] [CrossRef]
- Kirkendall, D.T.; Garrett, W.E., Jr. The effects of aging and training on skeletal muscle. Am J Sports Med 1998, 26, 598–602. [Google Scholar] [CrossRef]
- Snijders, T.; Aussieker, T.; Holwerda, A.; Parise, G.; van Loon, L.J.C.; Verdijk, L.B. The concept of skeletal muscle memory: Evidence from animal and human studies. Acta Physiol (Oxf) 2020, 229, e13465. [Google Scholar] [CrossRef]
- Peterson, M.D.; Rhea, M.R.; Sen, A.; Gordon, P.M. Resistance exercise for muscular strength in older adults: a meta-analysis. Ageing Res Rev 2010, 9, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Rahmati, M.; McCarthy, J.J.; Malakoutinia, F. Myonuclear permanence in skeletal muscle memory: a systematic review and meta-analysis of human and animal studies. J Cachexia Sarcopenia Muscle 2022, 13, 2276–2297. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, C.V.; Ribeiro, I.S.; Galantini, M.P.L.; Muniz, I.P.R.; Lima, P.H.B.; Santos, G.S.; da Silva, R.A.A. Inflammaging and body composition: New insights in diabetic and hypertensive elderly men. Exp Gerontol 2022, 170, 112005. [Google Scholar] [CrossRef] [PubMed]
- Heo, S.J.; Park, S.K.; Jee, Y.S. Detraining Effects of COVID-19 Pandemic on Physical Fitness, Cytokines, C-Reactive Protein and Immunocytes in Men of Various Age Groups. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Singh, H.; Kwon, K.; Tsitrin, T.; Petrini, J.; Nelson, K.E.; Pieper, R. Protein signatures from blood plasma and urine suggest changes in vascular function and IL-12 signaling in elderly with a history of chronic diseases compared with an age-matched healthy cohort. Geroscience 2021, 43, 593–606. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K. Chronic Inflammation as an Immunological Abnormality and Effectiveness of Exercise. Biomolecules 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Della Peruta, C.; Lozanoska-Ochser, B.; Renzini, A.; Moresi, V.; Sanchez Riera, C.; Bouche, M.; Coletti, D. Sex Differences in Inflammation and Muscle Wasting in Aging and Disease. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Fulop, T.; Larbi, A.; Pawelec, G.; Khalil, A.; Cohen, A.A.; Hirokawa, K.; Witkowski, J.M.; Franceschi, C. Immunology of Aging: the Birth of Inflammaging. Clin Rev Allergy Immunol 2023, 64, 109–122. [Google Scholar] [CrossRef]
Figure 2.
In the up panel is shown the comparison of the serum cytokines levels, in median and interquartile range, of IL-6 (A), IL-8 (B), IL-10 (C), IL-12p70 (D), IFN-γ (E), and TNF-α (F), as well as in the down panel the ratio, in median and standard deviation, between IL-6/IL-10 (G), IL-8/IL-10 (H), IL-12p70/IL-10 (I), IFN-γ/IL-10 (J), and TNF-α/IL-10 (K), in the volunteer groups (older women and older men) before COVID-19 pandemic (PRE), after 12 months of interruption (POST, detraining phase), and also after 10 months of resuming of regular practice of combined exercise training program (POST-TR).
Figure 2.
In the up panel is shown the comparison of the serum cytokines levels, in median and interquartile range, of IL-6 (A), IL-8 (B), IL-10 (C), IL-12p70 (D), IFN-γ (E), and TNF-α (F), as well as in the down panel the ratio, in median and standard deviation, between IL-6/IL-10 (G), IL-8/IL-10 (H), IL-12p70/IL-10 (I), IFN-γ/IL-10 (J), and TNF-α/IL-10 (K), in the volunteer groups (older women and older men) before COVID-19 pandemic (PRE), after 12 months of interruption (POST, detraining phase), and also after 10 months of resuming of regular practice of combined exercise training program (POST-TR).
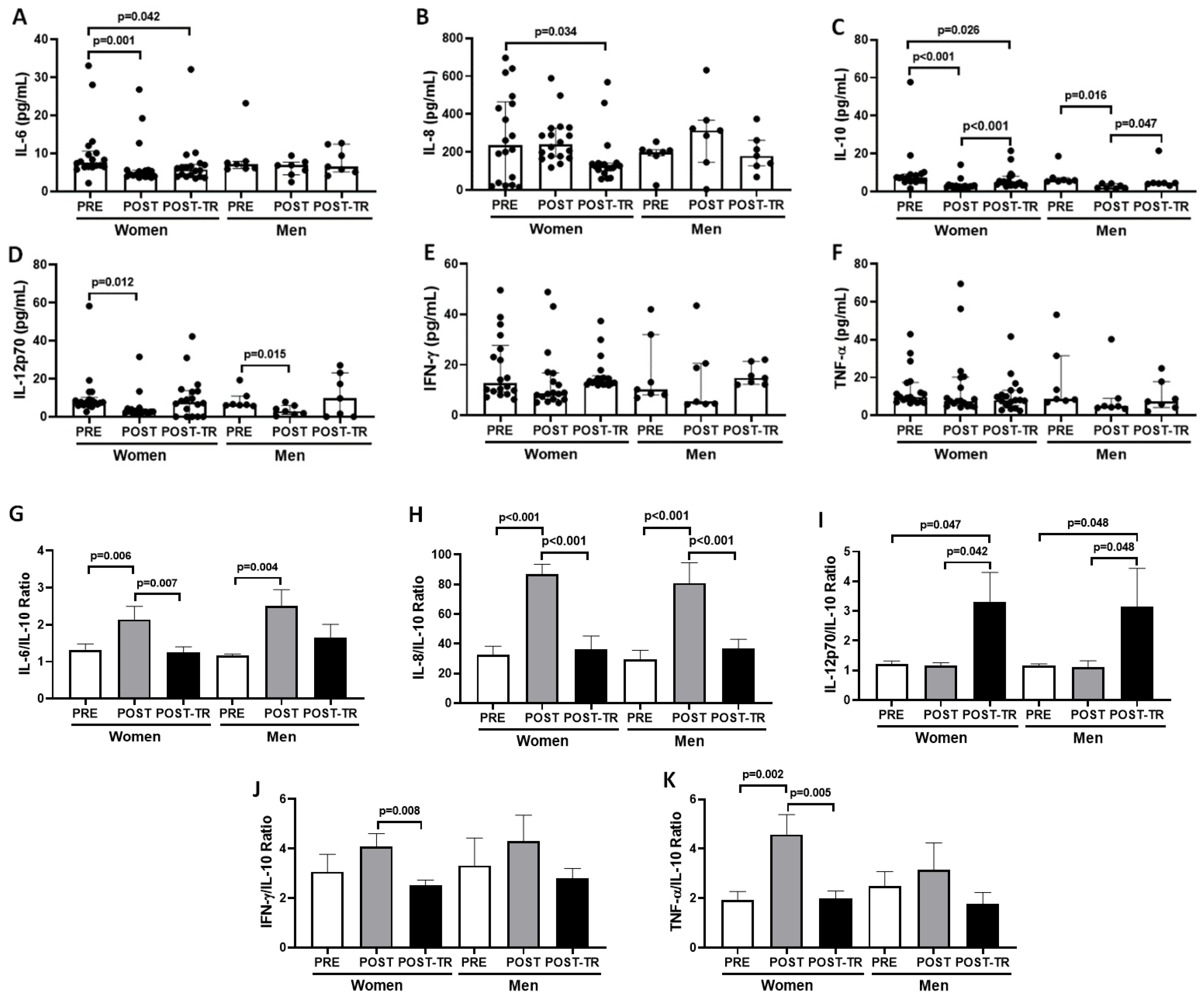

Table 1.
Data (mean and standard deviation) concerning demographic and anthropometric characteristics, as well as physical function tests [assessed by gait speed – (GS) and Timed-up-go (TUG)] and muscle strength (assessed by handgrip - HG) of the older women and older men groups in the different occasions: before COVID-19 pandemic (PRE), after 12 months of interruption (POST, detraining phase), and also after 10 months of resuming of regular practice of combined exercise training program (POST-TR). The level of significance was established at 5% (p<0.05).
Table 1.
Data (mean and standard deviation) concerning demographic and anthropometric characteristics, as well as physical function tests [assessed by gait speed – (GS) and Timed-up-go (TUG)] and muscle strength (assessed by handgrip - HG) of the older women and older men groups in the different occasions: before COVID-19 pandemic (PRE), after 12 months of interruption (POST, detraining phase), and also after 10 months of resuming of regular practice of combined exercise training program (POST-TR). The level of significance was established at 5% (p<0.05).
| Variables | Volunteer Groups | |||||||
| Older women (n=18) | p-values | Older men (n=7) | p-values | |||||
| PRE | POST | POST-TR | PRE | POST | POST-TR | |||
| Age (years) | 75.2±7.0* | 76.2±7.0 | 77.1±7.1† | *†<0.001 | 72.4±7.1* | 73.4±7.1 | 75.1±7.1† | *†<0.001 |
| Weight (kg) | 60.32±14.5 | 59.78±14.23 | 59.58±14.11 | 0.534 | 70.69±9.14 | 67.61±10.79 | 70.96±8.71 | 0.312 |
| Height (m) | 1.53±0.07 | 1.53±0.07 | 1.53±0.07 | 0.955 | 1.68±0.08 | 1.68±0.08 | 1.68±0.08 | 0.915 |
| BMI (kg/m2) | 24.32±4.21 | 24.14±4.46 | 24.29±4.16 | 0.694 | 24.82±3.29 | 23.59±2.05 | 25.30±2.98 | 0.401 |
| GS (m/s) | 0.97±0.21* | 0.81±0.25 | 0.99±0.18† | *0.009†0.015 | 1.03±0.15 | 1.06±0.18 | 1.02±0.19 | 0.914 |
| TUG (s) | 6.8±1.0* | 7.3±1.2 | 7.1±0.8 | *0.033 | 6.0±0.5 | 6.1±0.4 | 6.3±0.6 | 0.707 |
| HG (kgf) | 23.1±3.7# | 21.3±4.5 | 20.7±3.6 | #0.005 | 37.6±5.9*,# | 33.6±7.5 | 33.8±7.4 | *0.008#0.019 |
Note: *significant difference between the values obtained in PRE and POS. #significant difference between the values obtained in PRE and POS-TR. †significant difference between the values obtained in POS and POS-TR.
Table 2.
In the older women group, significant associations found by using Spearman’s correlation coefficient analysis between the data concerning physical function tests [(assessed by gait speed – (GS) and Timed-up-go (TUG)] and muscle strength (assessed by handgrip - HG), systemic cytokine levels, and the ratio between pro- and anti-inflammatory cytokines obtained in the different occasions: before COVID-19 pandemic (PRE), after 12 months of interruption (POST, detraining phase), and also after 10 months of resuming of regular practice of combined exercise training program (POST-TR). The level of significance was established at 5% (p<0.05).
Table 2.
In the older women group, significant associations found by using Spearman’s correlation coefficient analysis between the data concerning physical function tests [(assessed by gait speed – (GS) and Timed-up-go (TUG)] and muscle strength (assessed by handgrip - HG), systemic cytokine levels, and the ratio between pro- and anti-inflammatory cytokines obtained in the different occasions: before COVID-19 pandemic (PRE), after 12 months of interruption (POST, detraining phase), and also after 10 months of resuming of regular practice of combined exercise training program (POST-TR). The level of significance was established at 5% (p<0.05).
| Older women group (n=18) | ||||||||
| Parameters | 2019 (PRE) | Parameters | 2021 (POST) | Parameters | 2022 (POST-TR) | |||
| rho-value | p-value | rho-value | p-value | rho-value | p-value | |||
| BMI X TUG | 0.60 | 0.009 | BMI X TUG | 0.65 | 0.009 | BMI X TUG | 0.53 | 0.025 |
| Age X GS | - 0.56 | 0.016 | GS X TUG | - 0.63 | 0.012 | GS X TUG | - 0.54 | 0.020 |
| Age X IL-12p70/IL-10 | 0.58 | 0.012 | GS X IL-8/IL-10 | - 0.51 | 0.044 | BMI X TNF-α | 0.48 | 0.045 |
| GS X IL-12p70/IL-10 | - 0.57 | 0.014 | TUG X IL-8 | 0.55 | 0.034 | Age X IL-6 | 0.53 | 0.023 |
| GS X IL-10 | 0.50 | 0.036 | HG X IL-10 | 0.49 | 0.041 | Age X IL-12p70 | 0.49 | 0.038 |
| IL-6 X IL-10 | 0.99 | <0.001 | HG X IL-12p70 | - 0.51 | 0.030 | Age X IL-12p70/IL-10 | 0.48 | 0.044 |
| IL-6 X IL-12p70 | 0.99 | <0.001 | HG X IL-12p70/IL-10 | - 0.51 | 0.032 | IL-6 X IL-10 | 0.77 | <0.001 |
| IL-6 X TNF-α | 0.99 | <0.001 | HG X IL-8/IL-10 | - 0.56 | 0.016 | IL-6 X IL-12p70 | 0.58 | 0.011 |
| IL-6 X IFN-γ | 0.91 | <0.001 | IL-6 X IL-10 | 0.81 | <0.001 | IL-10 X IL-12p70 | 0.70 | 0.001 |
| IL-10 X IL-12p70 | 0.99 | <0.001 | IL-6 X IL-12p70 | 0.82 | <0.001 | |||
| IL-10 X TNF-α | 0.99 | <0.001 | IL-10 X IL-12p70 | 0.99 | <0.001 | |||
| IL-10 X IFN-γ | 0.91 | <0.001 | IL-8 X TNF-α | 0.64 | 0.004 | |||
| IL-12p70 X TNF-α | 0.99 | <0.001 | IL-8 X IFN-γ | 0.59 | 0.011 | |||
| IL-12p70 X IFN-γ | 0.90 | <0.001 | TNF-α X IFN-γ | 0.86 | <0.001 | |||
Table 3.
In the older men group, significant associations found by using Spearman’s correlation coefficient analysis between the data concerning physical function tests [(assessed by gait speed – (GS) and Timed-up-go (TUG)] and muscle strength (assessed by handgrip - HG), systemic cytokine levels, and the ratio between pro- and anti-inflammatory cytokines obtained in the different occasions: before COVID-19 pandemic (PRE), after 12 months of interruption (POST, detraining phase), and also after 10 months of resuming of regular practice of combined exercise training program (POST-TR). The level of significance was established at 5% (p<0.05).
Table 3.
In the older men group, significant associations found by using Spearman’s correlation coefficient analysis between the data concerning physical function tests [(assessed by gait speed – (GS) and Timed-up-go (TUG)] and muscle strength (assessed by handgrip - HG), systemic cytokine levels, and the ratio between pro- and anti-inflammatory cytokines obtained in the different occasions: before COVID-19 pandemic (PRE), after 12 months of interruption (POST, detraining phase), and also after 10 months of resuming of regular practice of combined exercise training program (POST-TR). The level of significance was established at 5% (p<0.05).
| Older men group (n=7) | ||||||||
| Parameters | 2019 (PRE) | Parameters | 2021 (POST) | Parameters | 2022 (POST-TR) | |||
| rho-value | p-value | rho-value | p-value | rho-value | p-value | |||
| GS X IFN-γ | - 0.78 | 0.049 | Age X TUG | 0.81 | 0.029 | BMI X IL-6 | 0.76 | 0.049 |
| TUG X IL-10 | - 0.79 | 0.048 | HG X TNF- α | - 0.79 | 0.048 | TUG X IL-10 | - 0.87 | 0.010 |
| IL-6 X IL-10 | 0.96 | 0.003 | IL-10 X IL-12p70 | 0.95 | <0.001 | TUG X IL-8 | 0.81 | 0.027 |
| IL-6 X IL-12p70 | 0.86 | 0.024 | IL-10 X IFN-γ | 0.90 | 0.006 | HG X TNF-α | - 0.79 | 0.033 |
| IL-8 X IL-10 | 0.79 | 0.048 | IL-12p70 X IFN-γ | 0.93 | 0.002 | HG X IFN-γ | - 0.83 | 0.022 |
| IL-10 X TNF-α | 0.86 | 0.024 | TNF-α X IFN-γ | 0.85 | 0.016 | IL-8 X IL-10 | 0.80 | 0.032 |
| IL-8 X TNF-α | 0.77 | 0.041 | ||||||
| IL-10 X TNF-α | 0.79 | 0.035 | ||||||
| TNF-α X IFN-γ | 0.85 | 0.015 | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



