
Submitted:
28 May 2024
Posted:
28 May 2024
You are already at the latest version
Abstract
Entropion is a condition characterized by the total or partial inversion of the eyelid margin, resulting in contact between the outer skin and the corneal or conjunctival surface, and sometimes both. This condition can affect various animals, including horses, pigs, goats, sheep, rabbits, felines, and particularly canines. It typically manifests in the lower lid's lateral portion but can affect any part of the lid. This contact between eyelashes or facial hair and the cornea or conjunctiva leads to severe irritation, causing self-inflicted trauma, as evidenced by clinical signs of pain, irritation, ulcerations, and vision loss. Entropion can be classified as primary (congenital or developmental) or secondary (spastic and scarring). Diagnosis relies on clinical signs, the animal's history, and its breed. It's essential to assess the degree of entropion in the dog without applying topical anesthesia. This study conducts a literature review on surgical techniques for correcting various types of entropion in canines.
Keywords:
canine
; surgical
; Hotz-Celsus technique
; eyelids
; entropion
1. Introduction
Entropion is an ophthalmic condition characterized by the partial or complete inversion of the eyelid margin, being highly prevalent in certain canine breeds, especially among brachycephalics [1,2]. A study conducted by O'Neill et al. [3], revealed that, in a population of 455,557 Shar Pei patients (brachycephalics), the prevalence of entropion reached 17.88%. Continuing this trend, Costa et al. [4] reported a prevalence of 22% out of a sample of 98 brachycephalic canines. It is important to note that the prevalence of entropion can vary in other dog breeds. Among the breeds most susceptible to this condition are: Cocker spaniel, Shar-pei, English Springer Spaniel, Labrador Retriever, American Bulldog, Rottweiler, Chow Chow [5], Pug [6], among others.
The causes of entropion can be either hereditary or acquired., resulting from chronic injuries or inflammation, and is typically associated with irritation to the conjunctiva, cornea, and sclera [7].
2. Entropion Definition and Types
The most common diseases affecting the eyelids are abnormalities in palpebral position [10]. One such condition is entropion, characterized by the inward rolling of the margin of a part or the entire eyelid (Figure 1). This anomaly appears to result from the difference in tension between the orbicularis oculi muscle and the malaris muscle [11]. Entropion predisposes the cornea and/or conjunctiva to irritation, ulceration, and, in severe cases, perforation [12].
Entropion is a prevalent pathology in dogs, with purebred canines being more affected than mongrels. In many cases, it can be attributed to hereditary factors, although the genetic basis is not yet fully understood. It is evident that certain breeds, are more susceptible to primary entropion [13]. Brachycephalic dogs often exhibit ocular issues, including entropion, which can be exacerbated by their prominent nasal folds and the anatomical characteristics of their breeds [14].
Entropion can manifest as lateral, medial, angular, or total, affecting either the lower or upper eyelid [15]. This condition is categorized as either primary (conformational or congenital) or secondary (spastic or cicatricial) [16].
2.1. Clinical Signs and Diagnosis
Diagnosis is clinical and sometimes accompanied by a combination of conditions, such as ectropion with entropion where the patient presents a macropalpebral fissure; additionally, a 'diamond eye' is observed in the affected eye(s) [17,18,19]. Entropion presents a spectrum of clinical signs, with the severity of symptoms varying from mild to severe. In mild cases, patients may exhibit increased tearing (wetting) and subsequently, epiphora. When entropion is moderate, inflammation becomes the prominent sign, accompanied by conjunctivitis featuring pronounced ocular discharge and noticeable eyelid twisting. In more severe instances, patients experience blepharospasm, marked conjunctivitis with copious purulent or mucopurulent discharge, photophobia, depigmentation of the palpebral margin, and neovascularization of the cornea. Severe cases even carry the risk of ulcerative keratitis and potential corneal perforation, with a consequent increased risk of eye loss [20].
Diagnosing entropion involves considering the patient's history, clinical signs, and breed predisposition. An essential step is the direct observation of eyelid positioning. Prior to any detailed examination or manipulation, it is crucial to evaluate the eyes from a distance to gauge the degree of blepharospasm and discomfort, as these symptoms may worsen during closer examination [21].
Upon closer examination, care should be taken to avoid excessive manipulation of the facial skin, which can significantly alter the palpebral position, particularly in breeds with pronounced facial skin laxity [10]. It's also essential to assess the eyelids for their position, presence of swellings, and any abnormalities of the eyelashes. Additionally, the position and size of the lacrimal points should be carefully examined [10]. Observing the animal freely is instrumental in determining the extent of the condition.
In order to indicate solutions or treatments, the condition must be classified according to its primary or secondary cause, its degree of severity (mild, moderate, or severe), and whether it affects one or both eyelids.
2.2. Primary Entropion
According to [19] The primary entropion can occur in two ways: congenital or acquired. This means that the patient could develop this condition in their early months of life or later in adulthood, often because of a combination of factors that trigger this condition. Read and Braun [17] indicate that these can be: Orbital anatomy, cranial conformation, large skin folds, eyelid fissure length, and skin laxity. Within primary entropion, the highest prevalence is in purebred breeds, which could indicate a hereditary basis (Figure 2). This type of entropion can vary in terms of the degree of eyelid involvement. Depending on the extent of the rotation of the palpebral margin, it can be classified as mild (45°), moderate (90°), or severe (180°) [22]. It may also be present in different positions, such as medial, angular, or total, affecting either the upper or lower eyelid [23].
Developmental entropion is considered a non-congenital hereditary condition [24]. Breeds like Chow-Chow and Shar-Pei often develop entropion shortly after opening their eyelids, affecting both upper and lower eyelids. In most cases, it is believed to result from an inherited defect, possibly a polygenic condition [24]. Another potential cause of primary entropion is the difference in tension between the orbicularis and malar muscles [23].
In cases of entropion affecting puppies and young dogs, the most common treatments involve the temporary fixation of the affected eyelid with sutures (tacking) or the permanent eversion of the affected eyelids using the modified Hotz-Celsus technique [24].
2.3. Secondary Entropion
Secondary entropion can be categorized as either spastic or cicatricial and is less common. This type of entropion typically arises because of other factors, such as trauma, disease, or scarring (Figure 3). It's crucial to address the primary underlying cause, as simply correcting the entropion without addressing the root issue may lead to recurrence [25].
2.3.1. Spastic Entropion
Spastic entropion is characterized by the pronounced contraction of the orbicularis oculi muscle, which is often triggered by painful ocular conditions such as ulcerative and non-ulcerative keratitis, conjunctivitis, tear film instabilities. It can also be induced by painful condition leads to blepharospasm and enophthalmos, causing the eyelid inversion [26].
In many cases of secondary spastic entropion, effective pain management for the underlying ocular condition causing blepharospasm may be sufficient for resolution. However, once entropion has developed, the irritation it causes can further worsen blepharospasm, exacerbating the entropion. In such cases, a procedure to evert the eyelid, even if only temporarily, is often necessary to relieve blepharospasm and correct the entropion [24].
2.3.2. Cicatricial Entropion
Cicatricial entropion is related to fibrosis caused by severe inflammation of the eyelid or conjunctiva, or by a previous injury or surgical trauma [26].
3. Treatments for Entropion Correction
3.1. Non-Traumatic Procedures
3.1.1. Tacking Procedure
The temporary or "Tacking" method is often preferred over permanent surgical procedures in certain cases. First, it is used when a patient is suffering from spastic entropion due to pain. The "Tacking" method can provide relief while addressing the underlying cause. Second, for young patients, permanent eyelid correction is typically postponed until they reach 5 to 12 months of age, when their facial development is more complete. During this period, the "Tacking" method is employed to prevent ocular irritation and reduce the risk of severe corneal damage in these patients [16].
In the "Tacking" procedure (Figure S1), two to four nonabsorbable vertical or interrupted simple mattress sutures, typically 4-0 to 5-0 in size, are placed alongside the affected eyelid margin. These sutures, approximately 5 mm in length, ensure proper retraction and tissue attachment. Often, the sutures are left longer to allow for multiple adjustments. They can be removed within 2 to 4 weeks, leaving behind a "scar tunnel" that provides corrective traction at the lid margin. Following "tacking," entropion often does not require further correction. If entropion persists, surgical intervention may become necessary [21].
The "Tacking" procedure is also recommended for adult dogs to address spastic etropion or to prevent secondary trichiasis-entropion from the upper lid to the lower lid following lower lid entropion correction [27].
3.1.2. Quickert-Rathbun Procedure
The Quickert-Rathbun procedure involves the use of sutures at the base of the eyelid fornix in puppies, young dogs, and older dogs with lower lid entropion. It can also serve as an alternative procedure to the Tacking method, especially in puppies, particularly when entropion reoccurs after Tacking. In this procedure, a 4-0 two-pronged resorbable suture is inserted from the bottom of the fornix to emerge externally 1-2 mm from the palpebral margin, causing an immediate eversion of the palpebral margin and correction of the entropion. Suture tension can be adjusted to achieve normal or slight ectropion [21]. This technique typically delivers acceptable results in most cases without the necessity for incisional surgery [28].
3.1.3. Lateral Temporal Tarsorrhaphy Procedure
It is a non-invasive technique that is also used to prevent keratitis and trichiasis. The technique consists of a non-absorbable mattress suture with a caliber 3-0, from the lower lateral eyelid to the upper eyelid. The idea is to prevent eversion of the lower eyelid, therefore, it should be left with a slight tension and maintained for a few weeks. This technique was used in 14 patients and yielded positive results in 8 of them [29].
3.1.4. Hyaluronic Acid
Hyaluronic acid (HA) is a substance that has been used in injections in humans for the last 15 years with few adverse reactions. In dogs, it is used for subdermal eyelid filling, especially in puppies [30]. Injections can be administered either on the upper or lower eyelid, based on the veterinarian's discretion. Additionally, multiple inoculations at different points or a linear injection can be performed, which have proven to be effective in maintaining the proper position of the eyelids for approximately 6-8 months post-procedure [5]. While HA can swiftly and effectively alleviate clinical signs, it offers temporary relief [30].
3.1.5. CO2 Laser
Similar tissue sectioning, conventional incisions, and resections procedures are conducted, albeit utilizing a CO2 laser instead of a scalpel. This approach offers comparative advantages, such as reduced risks, lesser bleeding and inflammation, shorter procedures, consequently leading to decreased patient discomfort, coupled with expedited recovery [11].
3.2. Traumatic o Surgical Procedures
While several methods have been proposed for treating entropion, it's crucial to recognize that surgical intervention remains the definitive solution. Several techniques, including the Hotz-Celsus procedure, lateral canthoplasty, Y to V plasty, Stades procedure, or a combination of these methods, are available [15]. The choice of technique depends on factors like the patient's breed, age, the degree of entropion, and its underlying cause [16].
It's essential to note that each surgical procedure has specific indications, success rates, and potential complications (Table 1). In severe cases involving multiple forms of entropion, such as lower and upper lid entropion, medial entropion, and lateral canthal entropion, a combination of surgical procedures or even multiple surgeries may be required for effective correction [15].
3.2.1. Hotz-Celsus Procedure
The Hotz-Celsus procedure was created by Celsus in antiquity and improved by Hotz in the 19th century. The procedure indicated in cases of conformational entropion in adult dogs is the Hotz-Celsus technique [31]. To perform the technique, the affected eyelid is kept stretched and the eye is protected by a Jaeger plate, or by the palmar surface of the eye or by the palmar surface of the surgeon's index finger [31,35]. An incision is made at 2 - 2.5 mm from the palpebral margin, parallel to it, with a #15 scalpel blade extending at least 1 mm medial and lateral to the entropion area [23] as shown in Figure S2.
Overcorrection can cause ectropion, which may result in additional surgery, so correctly estimating the amount of tissue to be removed is critical to the success of this blepharoplasty [35].
3.2.2. Modified Hotz-Celsus
As its name indicates, this technique, based on the original Hotz-Celsus surgical technique (Figure S3), in addition to the semilunar incision in the affected eyelid, includes another wedge-shaped incision on the outer edge of the eye. This modification of the technique has brought lasting results in patients and few postoperative complications [12].
3.2.3. Y-V Procedure
The Y-V procedure is recommended for correcting moderate medial entropion of both the upper and lower eyelids. The procedure commences with an incision, resembling a Y-shape, made through the palpebral skin layers and orbicularis muscle. This incision starts approximately 1-2 mm from the lid margin. The lower part of the Y-shaped incision, often referred to as the Y-leg, overlaps with the V-shaped area to achieve eversion of the lid margin. This is accomplished using a simple suture pattern and a 5-0 to 6-0 nonabsorbable thread [32].
On the other hand, this procedure is indicated for cicatricial entropion, where a Y-shaped incision is created by extending its arms just below the affected palpebral segment. Tension is applied to the skin flap until the eyelid margins return to their normal position, determining the length of the Y-shaped incision's body. The flap is then dissected to remove scar tissue. Finally, the apex of the flap is sutured to the most distal part of the incision, and the remaining edges of the incision are closed [34].
3.2.4. Wyman Procedure
The Wyman procedure and its modifications are employed to address the issue of palpebral instability, particularly in large and giant breeds of dogs [33]. This procedure, often combined with the Hotz-Celsus technique, is utilized to treat lower lid entropion. It involves the construction of a pedicle that is anchored in the subcutaneous tissue to evert the eyelid margin. This procedure is also employed in patients who have previously undergone other surgical interventions [32].
The process begins with a skin incision made approximately 1 to 2 mm from the palpebral margin. Subsequently, a tarsal pedicle is constructed along the palpebral margin in the widest part of the entropion using a scalpel. A 5-0 nonabsorbable suture is then passed through a subcutaneous tunnel created with scissors and attached to the tarsal pedicle below the surgical wound to prevent skin laceration. Another incision is made, following the Hotz-Celsus technique, in the skin, and an elliptical-shaped portion is removed. The remaining wound is closed with a simple suture pattern using 5-0 to 6-0 nonabsorbable suture [32,36].
3.2.5. Arrowhead Procedure
The Arrowhead procedure is employed when the primary component of entropion involves the inversion of the lateral canthus. In such cases, a modification to the Hotz-Celsus technique, known as the arrowhead modification, is carried out [34].
In this procedure, instead of creating an elliptical incision over the lateral canthus, an arrowhead resection is performed. Additionally, a tension suture is placed in the subcutaneous tissue at the lateral canthus to anchor and stabilize it. A horizontal mattress suture is positioned below the skin incision and the fascia covering the orbital ligament [34].
3.2.6. Stades Procedure
The Stades procedure, described by Stades [23], is employed to correct upper lid entropion while simultaneously preventing its recurrence by creating a band of hairless skin parallel to the palpebral margin (Figure S4) [24].
The procedure involves the removal of 15 to 25 mm of eyelid skin. A skin incision is made along the upper lid margin, positioned 0.5 to 1.0 mm dorsally to the Meibomian gland openings and inferiorly to the first cilia of the eyelid. This incision begins about 2 to 4 mm from the inner canthus and extends 5 to 10 mm beyond the lateral canthus. A second incision is made in an arched fashion, approximately following the sulcus parallel to the dorsal orbital rim, at a maximum distance of 15 to 25 mm from the palpebral rim. The wound edge is then dissected and trimmed, and the skin is sutured with absorbable material to the subcutaneous cellular tissue, maintaining 4 to 5 mm from the palpebral edge [37].
In a study conducted by Kim et al. [16], the Stades forced granulation technique was employed for the correction of upper lid entropion, in combination with the Hotz-Celsus procedure for lower lid entropion. This modification was shown to be effective in preventing recurrence.
3.2.7. Robertson Procedure
The Robertson procedure is especially suited for addressing lateral lower lid entropion and canthal entropion, particularly in large and giant dog breeds. Many giant breeds encounter intricate cases of entropion, primarily attributed to the combination of having long eyelids, sunken eyes, and a lax lateral canthus, which creates a palpebral macro-slit [10].
4. Postoperative Management
Postoperative management involves the administration of ocular antibiotic ointment and systemic nonsteroidal anti-inflammatory drugs (NSAIDs) for reducing inflammation and providing analgesia. Sutures are typically removed approximately 10 to 14 days following the surgery. It's worth noting that the eyelids have an excellent blood supply, making them prone to significant bleeding and susceptibility to severe edema and distortion even after minor injuries. Therefore, the use of an Elizabethan collar is essential to prevent self-inflicted trauma
5. Prognosis and Prevention
With a well-performed surgical procedure, entropion generally carries a favorable prognosis, even in complex cases involving ulceration. In instances of deep corneal damage, some corneal scars may persist. It's not uncommon for animals from the same family to be affected, making it advisable that animals with primary entropion do not reproduce. Given the strong breed predisposition, it is recommended not to breed animals with this condition, and breed societies should actively work to reduce the incidence of entropion within their specific breed [10].
6. Conclusions
Entropion is a common condition in dogs, and certain breeds are more susceptible to it. Understanding the different types of entropion and the appropriate surgical treatments is crucial. The most widely used surgical procedure is the modified Hotz-Celsus, often combined with other techniques. The variety of available techniques underscores the importance of staying updated on surgical methods, whether permanent or temporary.
Future research should continue to investigate the use of CO2 lasers and hyaluronic acid in treating entropion and explore their broader applications in veterinary ophthalmology, given their potential benefits in various aspects.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Investigation, J.M.-G. and A.E.A.; resources, J.M.-G.; writing—original draft preparation, A.E.A. and F.F.; writing—review and editing J.M.-G., C.C-C, C.E.-J. and C.G-V.; supervision, J.M.-G.; funding acquisition, C.E.-J. and J.M.-G.
Funding
The APC was funded by the Dirección General de Investigación e Innovación, Universidad del Alba, Chile.
Institutional Review Board Statement
This study did not require ethical approval.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We are grateful to the University of Alba for their generous support in funding the APC, and extend our thanks to Dr. Wendy Parra for her contribution of Figure 2 to this review.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Andrews ALMM, Youngman KL, Packer RMA, O’Neill DG, Kafarnik C. A Review of Clinical Outcomes, Owner Understanding and Satisfaction following Medial Canthoplasty in Brachycephalic Dogs in a UK Referral Setting (2016–2021). Animals 2023, 13, 2032. [Google Scholar] [CrossRef]
- Sebbag L, Sanchez RF. The pandemic of ocular surface disease in brachycephalic dogs: The brachycephalic ocular syndrome. Vet Ophthalmol 2023, 26 (Suppl 1), 31–46. [Google Scholar] [CrossRef]
- O’Neill DG, Engdahl KS, Leach A, Packer RMA, Church DB, Brodbelt DC. Is it now time to iron out the wrinkles? Health of Shar Pei dogs under primary veterinary care in the UK. Canine Med Genet 2023, 10, 11. [Google Scholar] [CrossRef]
- Costa J, Steinmetz A, Delgado E. Clinical signs of brachycephalic ocular syndrome in 93 dogs. Ir Vet J 2021, 74, 3. [Google Scholar] [CrossRef] [PubMed]
- McDonald JE, Knollinger AM. The use of hyaluronic acid subdermal filler for entropion in canines and felines: 40 cases. Vet Ophthalmol 2019, 22, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Krecny M, Tichy A, Rushton J, Nell B. A retrospective survey of ocular abnormalities in pugs: 130 cases. J Small Anim Pract 2015, 56, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Bergstrom R, Czyz CN. Entropion. Treasure Island (FL): StatPearls Publishing; 2024.
- Maman DY, Taub PJ. Congenital entropion. Ann Plast Surg 2011, 66, 351–353. [Google Scholar] [CrossRef] [PubMed]
- Angulo, A. Oftalmología veterinaria en especies menores con énfasis en trastornos oculares externos en caninos. Licenciatura en Medicina Veterinaria. Universidad Nacional, 2013.
- Turner, SM. Oftalmología de pequeños animales. 1era ed. España: Elsevier España; 2010.
- Serrano C, Rodríguez J. Nonsutured Hotz-Celsus technique performed by CO2 laser in two dogs and two cats. Vet Ophthalmol 2014, 17, 228–232. [Google Scholar] [CrossRef]
- Walter H, Bilotta T, Goncalves C, Busse C. A combination of modified Kuhnt–Szymanowski and Celsus–Hotz techniques for correction of entropion and overlong lower eyelids in dogs (40 eyes). Vet Ophthalmol 2023:1–10. [CrossRef]
- Gelatt KN, Gilger B, Kern T. Essentials of Veterinary Ophthalmology. vol. 2. 5ta ed. EEUU: Wiley-Blackwell; 2013.
- Silva ABS. Dermoplastia da prega cutânea nasal para correção de entrópio em cão da raça pug: relato de caso. Res Soc Dev 2022, 11, 17. [Google Scholar] [CrossRef]
- Gelatt K, Ben-Sholmo G, Gilger B, Hendrix D, Kern C, Plumer C. Veterinary Ophthalmology. vol. 2. 6th Edition. EEUU: Wiley-Blackwell; 2021.
- Kim Y, Kang S, Seo K. Combination of Stades Forced Granulation Method and Hotz-Celsus Procedure for Treatment of Upper and Lower Eyelid Entropion-Trichiasis in Three Dogs. J Vet Clin 2021, 38, 32–35. [Google Scholar] [CrossRef]
- Read RA, Broun HC. Entropion correction in dogs and cats using a combination Hotz–Celsus and lateral eyelid wedge resection: results in 311 eyes. Vet Ophthalmol 2007, 10, 6–11. [Google Scholar] [CrossRef]
- Steinmetz, A. Shared rhytidectomy continued to lateral canthoplasty in a Mastiff with excessive facial folding and macroblepharon. Tierarztl Prax Ausg K Klientiere Heimtiere 2015, 43, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Carrozza R, Lenihan E, Hamzianpour N, Linn-Pearl R, Heinrich C, Walsh K, et al. Lower lid entropion in dogs: A modified technique of the combined Hotz–Celsus and wedge resection procedure. Vet Rec 2022, 190, e1383. [Google Scholar] [CrossRef] [PubMed]
- Hadzimilic, M. Entropium in dogs and its correction. Vet Glas 2003, 57, 51–62. [Google Scholar] [CrossRef]
- Gelatt, K. Essentials of Veterinary Ophthalmology. 3era ed. EEUU: 2014.
- Delgado E, Borrego S, Sales J. Entrópion em canídeos e felídeos – 71 casos clínic. Rev Port Cienc Vet 2005, 100, 211–217. [Google Scholar]
- Stades F, Boevé M, Neumann W, Wyman M. Oftalmología para el veterinario práctico. 1era ed. Argentina: Inter-Médica; 1999.
- Petersen S, Crispin S. Manual de Oftalmologia en Pequeños Animales. 1era ed. España: Lexus; 2012.
- Konig H, Liebich H. Anatomia de los animales Domesticos. 2nd ed. Madrid: Médica Panamericana; 2004.
- Sandmeyer LS, Osinchuk S. Diagnostic Ophthalmology. Can Vet J 2022, 63, 89–90. [Google Scholar]
- Gelatt, K. Fundamentos de oftalmología veterinaria. 1era ed. EEUU: Elsevier; 2003.
- Williams, DL. Entropion correction by fornix-based suture placement: use of the Quickert-Rathbun technique in ten dogs. Vet Ophthalmol 2004, 7, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Lewin, GA. Temporary lateral tarsorrhaphy for the treatment of lower lateral eyelid entropion in juvenile dogs. Vet Rec 2000, 146, 439–440. [Google Scholar] [CrossRef] [PubMed]
- Lee H-E. Hyaluronic Acid Filler Injection as an Alternative to Surgery for the Correction of Canine Entropion. Pak Vet J 2021, 41, 173–175. [Google Scholar] [CrossRef]
- Moore CP, Constantinescu GM. Surgery of the adnexa. Vet Clin North Am Small Anim Pract 1997, 27, 1011–1066. [Google Scholar] [CrossRef]
- Silveira TJ da, S. Principais abordagens cirúrgicas das afecções de pálpebras e cílios de cães e gatos: revisão bibliográfica. Licenciatura en Medicina Veterinaria. Universidade Federal da Paraíbada, 2021.
- Cardoso KM, Navega P, Esteves P, Coutinho C, Monteiro J, Vaz R, et al. Técnica de cantoplastia lateral para correção de “olho de diamante” em cão: Relato de caso. Pubvet 2021, 15, 1–5. [Google Scholar] [CrossRef]
- Fossum, TW. Small Animal Surgery. 5ta ed. EEUU: Elsevier Health Sciences; 2018.
- Van der Woerdt, A. Adnexal surgery in dogs and cats. Vet Ophthalmol 2004, 7, 284–290. [Google Scholar] [CrossRef] [PubMed]
- 36. Gould D, McLellan G. BSAVA Manual of Canine and Feline Ophthalmology. Quedgeley:.
- Laus JL, Vicenti FAM, Bolzan AA, Galera PD, Sanches RC. Stades method for surgical correction of upper eyelid trichiasis-entropion: results and follow-up in 21 cases. Ciênc Rural 2000, 30, 651–654. [Google Scholar] [CrossRef]
Figure 1.
Canine patient, 6-year-old Boxer, with untreated entropion.
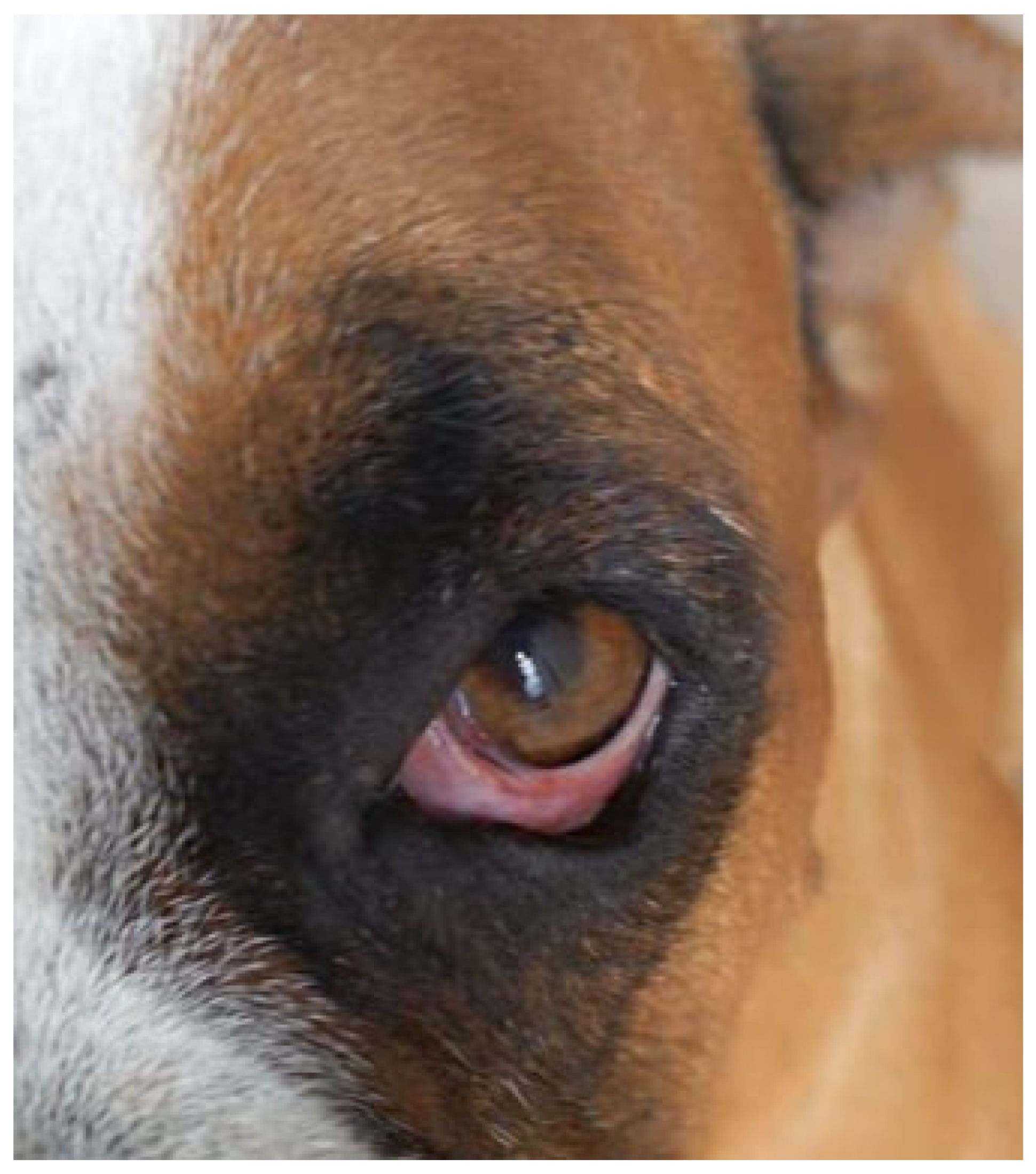
Figure 2.
A canine patient, 2.5-month-old boxer diagnosed with primary entropion.
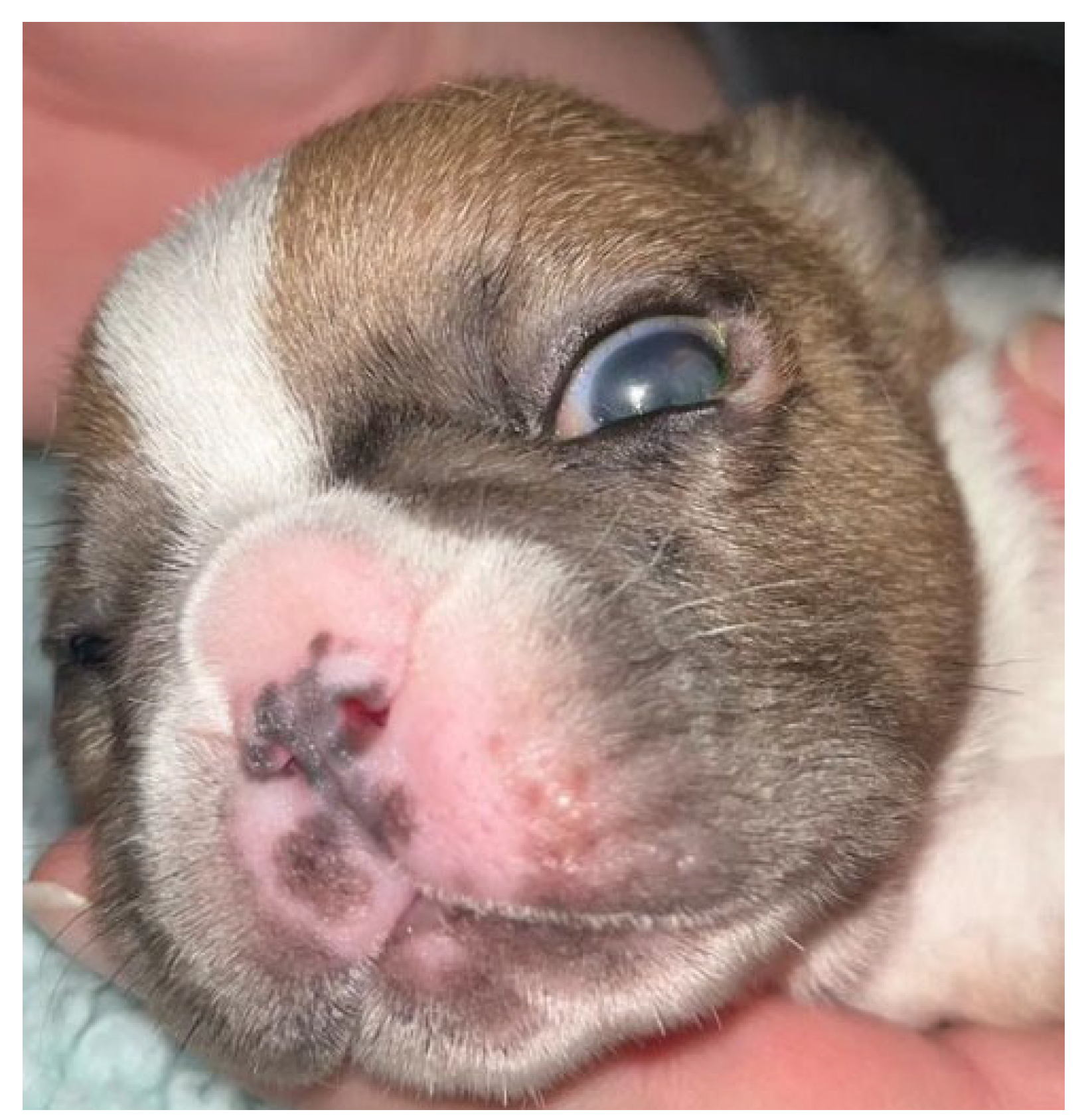
Figure 3.
9-year-old canine patient, Boxer diagnosed with secondary entropion.


Table 1.
Overview: Types of Entropion, Surgical Procedures, and Recommendations.
| Entropion Type | Surgical Procedure | Indications of Entropion Type | Success Rates | Potential Complications | Recommended Age* | Ref. |
|---|---|---|---|---|---|---|
| Lower and medial eyelid. | “Tacking” temporary retraction | Temporary relief of entropion. Avoid contact with conjunctiva and/or cornea (pain). | Temporary relief | - | All ages, preferably puppies dogs | [16] |
| Upper, Lower, Medial, and lateral canthal eyelid | Hotz-Celsus procedure | Mild to moderate entropion | High | Minimal complications | All ages | [31] |
| Upper and lower eyelid | Y to V plasty | Moderate entropion | Moderate | Suture granulomas, eyelid malposition | Usually in adult canines | [32] |
| Lower eyelid | Quikert-Rathbun | Moderate to severe entropion | Variable | Scarring, eyelid malposition, suture issues | Puppies and young dogs | [21] |
| Lateral entropion of the lower eyelid | Temporal lateral tarsorrhaphy | Moderate to severe entropion | Variable | Scarring, suture issues | Usually in adult canines | [29] |
| Central inferior entropion | Wyman | Moderate to severe entropion | Variable | Scarring, suture issues | Usually in adult canines | [32,33] |
| Lateral canthal entropion | Arrowhead (Hotz-Celsus modification) | Moderate to severe entropion | Variable | Scarring, suture issues | Usually in adult canines | [34] |
| Upper eyelid | Stades procedure | Severe entropion (shar pei breed) | Moderate | Potential for scarring, eyelid malposition | Usually in adult canines | [24] |
| Lateral lower and canthal eyelid. | Robertson | Severe entropion (large and giant breeds) | Variable | Scarring, suture issues | Usually in adult canines | [10] |
| Upper, Lower, and medial eyelid. | Combination of methods | Complex cases, multiple types | Variable | Varied complications | Varies depending on case | [11] |
* The column indicates whether the procedure is typically recommended for puppies, juveniles, or adults, but keep in mind that these recommendations may vary depending on the individual evaluation of the case by a professional.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



