
Submitted:
05 March 2024
Posted:
06 March 2024
You are already at the latest version
Abstract
There is a considerable increase in the use of substances and medical procedures aimed at changing the esthetics of the face, particularly the appearance of the lips. Permanent fillers such as polydimethylsiloxane, also called liquid silicone, are widely used, but their application for facial esthetics is currently obsolete. However, the long-term complications remain a reality, as they can occur decades after the application. Thus, the goal of this case report was to present a complication after 16 years of treatment using liquid silicone. This case report involved a 52-year-old male with a complication of bilateral permanent filler in the upper lip performed 16 years ago, its surgical removal, and histological analysis. Histologically, it was possible to identify a chronic inflammatory, lymphoplasmacytic, and granulomatous reaction, with foreign body giant cells’ reaction, in relation to non-polarizable exogenous material due to the reaction to silicone. The most common complications are granulomas' appearance and material displacement. The case report shows these granulomas are characterized as chronic low-caliber inflammation around the silicone. They have an unknown etiology but are probably multifactorial, from continuous trauma, friction or irritation, iatrogenic factors, infection, immunological mechanisms, and genetic and molecular variations, and can be highly related to the impurity of the injected material.
Keywords:
Filler
; complication
; silicone
; polymethylsiloxane
; lip augmentation
; facial esthetics
1. Introduction
Since the 1990s, there has been a considerable increase in the use of substances and medical procedures aimed at changing the esthetics of the face, particularly the appearance of the lips. This is probably due to the impact of beauty standards, which are increasingly rooted today and motivate the population to pursue an idea of beauty present in the media or cinema industry. For this reason, several procedures and surgical techniques have been developed to enhance lip and perioral rejuvenation [1,2]. Then, minimally invasive procedures for lip augmentation have been performed.
Lip enhancement has become a popular procedure mainly because of the application of nonsurgical techniques. Even though the safest material is the hyaluronic acid-based fillers, it is a non-permanent solution, requiring repeated injections [3]. Over the years, numerous products have been used for these aesthetic purposes, from autogenous to alloplastic materials [4]. The natural/biologic injection fillers are ultimately resorbable (temporary), requiring repeated treatments to maintain desired esthetic results, such as collagen, hyaluronic acid, poly-L-lactic acid, calcium hydroxyapatite microspheres, polyacrylamide, and polymethylmethacrylate, whereas others are permanent, such as bioalcamide and silicone. Many synthetic polymers are not easily phagocytized, remaining in situ with minimal resorption for years, and are therefore considered permanent [5,6]. On this hand, inert injectable polymers can be placed precisely in the dermis to increase soft tissue bulk, creating an esthetic contour and flattening wrinkles. Moreover, there is a report in the literature on the off-label use of permanent fillers (silicon oil, polyacrylamide hydrogel, and polymethylmethacrylate microspheres) [7,8].
Silicone belongs to this polymer family. Its viscosity is determined by its degree of polymerization. Liquid injectable silicone is odorless, colorless, non-volatile, and oily to the touch. The substance is not altered by storage at room temperature and is not carcinogenic or teratogenic [1,9]. These dermal fillers must be tested in animal models before being followed for clinical studies and then released and marketed to ensure biocompatibility [5,10]. Moreover, subcutaneous injection with histopathologic evaluation among human subjects has also been undertaken [4,11]. Most patients tolerate those biomaterials without complications. Otherwise, some develop prominent, unexpected lesions with clinical/histologic evidence of inflammation and foreign body reaction. Then, patients may not associate any esthetic procedure with fillers with the development of a nodular mass a period later [12,13].
Natural and synthetic polymers serve as gelatinous matrices with suspended particulate or spherical filler substances measuring 2–100 µm. Polydimethylsiloxane, also called liquid silicone, is widely used in medicine, especially in facial aesthetic medicine, namely in disguising scars, earlobe enlargement, and nose, chin, and lips remodeling [14]. Its use for lip augmentation was first described about 30 years ago, with numerous authors reporting more than 17,000 cases. Currently, this material is considered obsolete for cosmetic applications [15].
Even though some studies consider the permanent lip filler a safe option, others describe possible early- and late-onset complications [16,17,18,19,20]. Those are usually related to overfilling or improper injection technique, whereas late-onset complications are generally caused by foreign body reactions or dehydration of the filler, leading to unfavorable results. It is important to report that many fillers comprise 2.5% to 5% of a permanent agent, and the remaining portion is sterile water [21,22,23]. Thus, the goal of this case report was to present a complication after 16 years of treatment using liquid silicone. To the best of our knowledge, this is a unique case report in the long term (16 years) showing lip complications and clinical solutions associated with fillers in the lip.
2. Case Report
Prior to collecting any information and developing any procedure, the patient filled out the informed consent. The study was conducted in accordance with the Declaration of Helsinki (1975, revised 2013). Moreover, this case report followed the CARE (Case Report) guidelines. A 52-year-old Caucasian male patient presented for the first time at the University Dental Clinic - Universidade Católica Portuguesa (Viseu, Portugal) in April 2022, dissatisfied with his upper lip's aesthetic appearance and shape (Figure 1). No smoker or diabetic; the patient had hypertension and hypercholesterolemia and was medicated with Losartan, Hydrochlorothiazide, and Pitavastatin. There were no relevant findings in the extraoral examination. The intraoral examination presented bruxism and a good periodontal condition.
The patient had an asymptomatic bilateral mass, hard to palpation, located on the upper lip due to permanent lip filling done to increase its volume in 2006 associated with non-related generalized granules of Fordyce.
The treatment options presented were: 1. just observation or 2. complete filling material removal in two surgical steps, which was the patient's choice. In the written consent provided and signed, the patient agreed to the use/analysis of the data.
Then, the first surgical procedure was performed under local anesthesia on the right side of the lip, one carpule of Lidocaine 2% with adrenaline 1:100,000, with a chalazion clamp, a diode laser for hemorrhagic control, and a simple suture with 6-0 Vycril resorbable thread, suturing by layers (Figure 2).
In this procedure, three fragments were biopsied: a cuboid measuring 1 x 1 x 0.8 cm and an irregular one consisting of two fragments that at one end of the piece are in continuity with each other, one measuring 1.6 x 0.5 x 0.4 cm and the other 2.5 x 0.6 x 0.5 cm (Figure 3). A similar macroscopic appearance in all the material, white in color, irregular surface, elastic, white section surface, or slightly fasciculate. The patient was medicated with Tylenol 500 mg thrice a day for two days.
After 20 days, the sutures from the first surgery were removed, as well as the foreign body from the upper lip on the left side, following the same surgical technique and medication. Histologically, all the slides were similar to each other, in which a chronic inflammatory, lymphoplasmacytic, and granulomatous reaction was observed, with foreign body giant cells’ reaction, in relation to non-polarizable exogenous material, in a “Swiss cheese” pattern, with circular empty spaces of variable size. These features suggest a reaction to silicone (Figure 4).
The patient did not intend to have more lip fillings, so he is satisfied with the aesthetics achieved after the surgery. The surgical wound was well healed and almost imperceptible on visual examination and palpation (Figure 5).
3. Discussion
The use of facial fillers to improve aesthetics, such as filling the subcutaneous area, is one of the most frequently nonsurgical procedures performed in the U.S.A. [24]. According to their degradability, they can be bioresorbable or non-bioresorbable [25]. The number of performed filler procedures increases, and the chance of adverse events also increases [26]. These occurrences can be divided into acute and delayed adverse events [27,28]. Early events include edema, erythema, redness, swelling, ecchymosis, bruising, pain, discoloration, infection, embolism, blindness, and skin necrosis (glabella and nasolabial folds). In contrast, late effects include chronic inflammation, late allergic reaction, asymmetry, discoloration, migration, granulomatous nodules, lipoatrophy, and telangiectasia.
Thus, knowing the ideal soft-tissue filler can be relevant to performing esthetic treatment. The ideal biomaterial should be safe and stable after application, compatible with the local tissues, phagocytosis resistant, without migration from the implantation site, pliable‚ and able to maintain the volume without absorption. Moreover, it should induce minimal foreign body reaction and must be non-teratogenic, non-immunogenic, non-carcinogenic, and non-infectious. Even though far from achieving it, the treatments have led to multiple injections and complications, with the presence of nodules and granulomas [29].
The most common causes of post-filler injections are inflammatory reactions, inadequate training, and technical injection faults. To avoid or treat this problem, the professional must know the composition of the filler biomaterial, possible tissue reaction, absorption capability, and filler persistence [27]. In the 2000s, the first evidence of the adverse effects inherent to this material appeared, namely in the form of foreign body granulomas [30,31]. These complications are due to the operator's lack of experience, inadequate technique, material impurities, and material displacement when dealing with large volumes injected [32]. The most common complications are granulomas' appearance and material displacement. As reported in our case, these granulomas are characterized as chronic low-caliber inflammation around the silicone. They have an unknown etiology but are probably multifactorial, from continuous trauma, friction or irritation, iatrogenic factors, infection, immunological mechanisms, or genetic and molecular variations. However, some authors believe there is also a strong possibility that it is highly related to the impurity of the injected material, and others believe that another possible explanation is the presence of a systemic infection that can trigger a local immune reaction. The displacement of the material may be due to the absence of the formation of a fibrous capsule, which allows its migration, especially due to gravity [9,15,30,31,32].
Inflammatory nodules and granulomas are the most claimed and disfiguring complications. Post-filler injection problems happen due to infection (probably caused by biofilm), granuloma as a response to body foreign material, inflammatory nodule due to immune system activation without granuloma formation (sterile abscess), and Tyndall effect (misapplication of the filler) [28]. Then, the result from the body’s response to foreign material or due to phagocytosis of the material is granulomatous inflammations, mostly found between 6–24 months post-filler treatment [27,28,33]. The material in the defense cells (macrophages and monocytes) stimulates cytokines and inflammatory mediators in order to attract more defense cells to form multinucleated foreign body giant cells, which is visibly and mainly observed in the histopathological images of granuloma. Infection of the injected material or local inflammation without microorganism involvement (sterile abscess) triggers the granulomatous reaction [34,35]. The diagnosis of this pathology is sometimes facilitated since patients, in most cases, do not associate it with the filler treatment carried out weeks, months, or years before. Therefore, regarding differential diagnoses, we can have numerous occurrences ranging from abscesses, sialadenitis, mucocele, or benign salivary gland neoplasia. It can also occur early or late in the clinical course and are most commonly single nodules. If multiple sites are involved, this suggests a granulomatous foreign body response [36]. Although rare, it is worth reporting that vascular compromise can be found, and it causes serious complications. It is a result of intravascular injection into an artery; this fact impedes normal blood flow or causes compression blockage close to the vessel. Pain and blanching followed by a livedoid discoloration can be clinically observed in the case of arterial occlusion, which has immediate onset; it can be considered the most serious and dangerous complication when using dermal fillers, mainly if it occurs within the retinal artery region [34].
Comparing silicone material with hyaluronic acid or poly-l-lactic acid fillers, rare cases of granulomatous reaction are found [28,35,37]. Then, the use of nonbiodegradable fillers, mass bolus filler injection, and infection at the injection site are factors that increase the granulomatous body reaction rate [28,34,35].
In our case report, it should be noted that initially, when the filling took place (2006), the patient was satisfied with the appearance of the lips; however, after a few years, deformation began to exist due to the appearance of these granulomas. This leads us to conclude that this mixed inflammatory infiltrate with multinucleated giant cells led to its distortion. Therefore, the complication of the present case is related to the unsatisfactory aesthetics of the lip due to this late inflammatory reaction. The literature is in line with our histological results and other case reports. At the histological level, there are typical histological features of granulomas formed due to foreign body reactions, such as the presence of multinucleated giant cells and chronic inflammatory infiltration. These granulomas can develop several decades after the injections [2,9,15,30,31,32,38,39].
Identification of the filler materials microscopically is important because granuloma formation to foreign materials may simulate a chronic inflammatory reaction. The literature reported that hydroxyethylmethacrylate induced a foreign body reaction, with vacuoles containing ‘‘broken glass"-like particles, which failed to exhibit birefringence. Less commonly used fillers have also been reported to induce foreign body reactions [40,41,42,43].
Treatments for nodules and granulomatous masses causing facial deformities have been cited in the literature and involve either dealt with by nonsurgical therapeutic approaches (systemic antibiotics, intralesional steroids, 5-fluorouracil injection, and needle aspiration) or surgical procedures‚ such as drainage and excision [44]. Surgical removal is reported to be the first line of action whenever possible due to its greater effectiveness, which is why we opted for this line of treatment; however, other techniques can be used when it is not possible. In our case report, there were some treatment options, such as surgical excision, allopurinol, oral or intralesional steroids, minocycline or etanercept, and imiquimod cream or immunomodulatory drugs known to increase interferon levels. Intralesional steroids are applied locally or orally, in monotherapy, or association with antibiotics or non-steroidal anti-inflammatory drugs, however, with little associated efficacy. In the case of the application of Allopurinol, an immune response modifier, a curative effect of these granulomas was verified. Minocycline applied in monotherapy has the same efficacy as oral prednisolone or a combination of the above. However, the latter has some associated side effects, such as pigmentation, although minimal and well tolerated. This therapy also requires a longer treatment time. Other studies suggest that a possible alternative to minocycline is etanercept, which is applied subcutaneously and acts on the pain component if present. Finally, Imiquimod, although not described in the literature as a treatment for foreign body type reactions, has been reported as having positive results in some clinical cases [38,39,45,46].
Some surgical procedures have been reported in the literature. Kastner et al. [47] described an 8-year experience in polyacrylamide gel removal from 18 lips. They operated 11 patients using the surgical lip reduction named “bikini technique” [48]; the gel and the local scar tissue were removed by sharp scissor dissection. Rauso et al. [49] showed their retrospectively experience in surgical lip for esthetic remodeling after permanent filler injection; 38 patients were operated (a total of 69 lips). They presented an incision following the dry-wet mucosa margin, marking the lip mucosa excess with calipers; then, a V-shaped marking was performed on the midline along with perpendicular markings; the mucosal flap was harvested (3 mm on the vestibular and around 7 mm on the labial side) to removal of the foreign body. In our study, we performed a different surgical approach, with a chalazion clamp and diode laser for hemorrhagic control, and then, a simple suture.
Therefore, as the case was 16 years after lip filling, it can be considered above the range compared to other studies done [50]. Moreover, the literature has recommended local post-operative massage, if possible, which showed very helpful in reducing edema and indurations after surgical procedures.
4. Conclusions
The population's growing demand for facial esthetics, particularly the lip and perioral region. This fact requires health professionals to grow awareness of the short and long-term adverse effects of each type of material used to make their application technique more predictable and conscious.
Author Contributions
Conceptualization, TM, IP, NV, PC; methodology, SF, TM, IP, MTC, NV, JCHF, GVOF, PC; software, SF, TM, PC; validation, TM, GVOF, PC; formal analysis, SF, TM, IP, MTC, NV, JCHF, GVOF, PC; investigation, SF, TM, IP, MTC, NV, JCHF, GVOF, PC; resources, SF, TM, IP, MTC, NV, JCHF, GVOF, PC; data curation, SF, TM, IP, MTC, NV, JCHF, GVOF, PC; writing—original draft preparation, SF, TM, IP, MTC, NV, JCHF, GVOF, PC; writing—review and editing, NV, JCHF, GVOF, PC; visualization, X.X.; supervision, TM, NV, GVOF, PC; project administration, TM, IP, GVOF, PC; funding acquisition, NV, PC. All authors have read and agreed to the published version of the manuscript.
Funding
This work is financially supported by National Funds through FCT – Fundação para a Ciência e a Tecnologia, I.P., under the project UIDB/04279/2020.
Informed Consent Statement
Informed consent was obtained from the patient involved in the case report.
Data Availability Statement
All data were inserted in the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Schmidt-Westhausen, A.; Frege, J.; Reichart, P. Abscess formation after lip augmentation with silicone: case report. Int J Oral Maxillofac Surg 2004, 33(2), 198–200. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Miller, P.J. Management of lip complications. Facial Plast Surg Clin North Am 2019, 27(4), 565–570. [Google Scholar] [CrossRef] [PubMed]
- Rivkin, A.; Weinkle, S.H.; Hardas, B.; et al. Safety and effectiveness of repeat treatment with VYC-15L for lip and perioral enhancement: results from a prospective multicenter study. Aesthet Surg J 2019, 39, 413–422. [Google Scholar] [CrossRef] [PubMed]
- Ajuz, D.; Oliveira, M.D.; Fernandes, J.C.H.; Fernandes, G.V.d.O. Facial Hemiplegia Treated with Botulinum Toxin: A Case Report. Diseases 2022, 10, 67. [Google Scholar] [CrossRef] [PubMed]
- Lemperle, G.; Morhenn, V.; Charrier, U. Human histology and persistence of various injectable filler substances for soft tissue augmentation. Aesthetic Plast Surg 2003, 27(5), 354–367. [Google Scholar] [CrossRef]
- Johl, S.S.; Burgett, R.A. Dermal filler agents: a practical review. Curr Opin Ophthalmol 2006, 17, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Clymer, M.A. Evolution in techniques: lip augmentation. Facial Plast Surg 2007, 23, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Rauso, R. 5-year study of a polyacrylamide hydrogel-based filler for rehabilitation of HIV-related facial lipoatrophy. Aesthet Surg J 2015, 35, 1021–1029. [Google Scholar] [CrossRef]
- Moscona, R.A. , Fodor, L. A retrospective study on liquid injectable silicone for lip augmentation: long -term results and patient satisfaction. J Plast Reconstr Aesthet Surg; 2010; 63, pp. 1694–1698. [Google Scholar] [CrossRef]
- Alster, T.S.; West, T.B. Human-derived and new synthetic injectable materials for soft-tissue augmentation: current status and role in cosmetic surgery. Plast Reconstr Surg 2000, 105, 2515. [Google Scholar] [CrossRef]
- Smith, K.C. Reversible versus nonreversible fillers in facial aesthetics: concerns and considerations. Dermatol Online J 2008, 14, 3. [Google Scholar] [CrossRef]
- Hirsch, R.J.; Stier, M. Complications of soft tissue augmentation. J Drugs Dermatol 2008, 7, 841–845. [Google Scholar] [PubMed]
- Salles, A.G.; Lotierzo, P.H.; Gemperli, R.; Besteiro, J.M.; Ishida, L.C.; Gimenez, R.P.; Menezes, J.; Ferreira, M.C. Complications after polymethylmethacrylate injections: report of 32 cases. Plast Reconstr Surg 2008, 121, 1811–1820. [Google Scholar] [CrossRef] [PubMed]
- Abtahinaeini, B.; Faghihi, G.; Shahmoradi, Z.; Saffaei, A. Filler migration and extensive lesions after lip augmentation: Adverse effects of polydimethylsiloxane filler. J Cosmet Dermatol 2018, 17(6), 996–999. [Google Scholar] [CrossRef] [PubMed]
- Fulton Jr, J.E.; Porumb, S.; Caruso, J.C.; Shitabata, P.K. Lip augmentation with liquid silicone. J Dermatol Surg 2005, 31, 1577–1586. [Google Scholar] [CrossRef] [PubMed]
- Pallua, N.; Wolter, T.P. A 5-year assessment of safety and aesthetic results after facial soft-tissue augmentation with polyacrylamide hydrogel (Aquamid): a prospective multicenter study of 251 patients. Plast Reconstr Surg 2010, 125, 1797–1804. [Google Scholar] [CrossRef] [PubMed]
- Hevia, O. Six-year experience using 1,000-centistoke silicone oil in 916 patients for soft-tissue augmentation in a private practice setting. Dermatol Surg 2009, 35 (Suppl 2), 1646–1652. [Google Scholar] [CrossRef] [PubMed]
- Kavoussi, H.; Ebrahimi, A. Delayed gel indurations as an adverse effect of polyacrylamide filler and its easy treatment. Dermatol Res Pract 2012, 2012, 4. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.R.; Holmes, R.E. Artecoll: a long-lasting injectable wrinkle filler material: report of a controlled, randomized, multicenter clinical trial of 251 subjects. Plast Reconstr Surg 2004, 114, 964–976. [Google Scholar] [CrossRef]
- Rauso, R.; Califano, L.; Rugge, L.; et al. Late onset complications secondary to polyacrylamide hydrogel-based filler for rehabilitation of HIV-related facial lipoatropy. Aesthet Surg J 2018, 38, N170–N174. [Google Scholar] [CrossRef]
- Salles, A.G.; Lotierzo, P.H.; Gemperli, R.; et al. Complications after polymethylmethacrylate injections: report of 32 cases. Plast Reconstr Surg 2008, 121, 1811–1820. [Google Scholar] [CrossRef]
- Park, T.H.; Seo, S.W.; Kim, J.K.; et al. Clinical experience with polymethylmethacrylate microsphere filler complications. Aesthetic Plast Surg 2012, 36, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Rauso, R.; Curinga, G.; Rusciani, A.; et al. Safety and efficacy of one-step rehabilitation of human immunodeficiency virus-related facial lipoatrophy using an injectable calcium hydroxyapatite dermal filler. Dermatol Surg 2013, 39, 1887–1894. [Google Scholar] [CrossRef] [PubMed]
- Rohrich, R.J. Advances in facial rejuvenation: botulinum toxin A, hyaluronic acid dermal fillers, and combination therapies-consensus recommendations. Plast Reconstr Surg 2008, 121, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Bergeret-Galley, C.; Latouche, X.; Illouz, Y.G. The value of a new filler material in corrective and cosmetic surgery: DermaLive and DermaDeep. Aesthetic Plast Surg 2001, 25, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Requena, C.; Izquierdo, M.J.; Navarro, M.; et al. Adverse reactions to injectable aesthetic microimplants. Am J Dermatopathol 2001, 23, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Lemperle, G.; Rullan, P.P.; Gauthier-Hazan, N. Avoiding and treating dermal filler complications. Plast Reconstr Surg 2006, 118 (Suppl. S3), 92S–107S. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, H.B.; Cohen, J.L. Adverse effects when injecting facial fillers. Semin Cutan Med Surg 2007, 26, 34–39. [Google Scholar] [CrossRef]
- Broder, K.W.; Cohen, S.R. An overview of permanent and semipermanent fillers. Plast Reconstr Surg 2006, 118(3 Suppl), 7S–14S. [Google Scholar] [CrossRef]
- Sanchis-Bielsa, J.M.; Bagán, J.V.; Poveda, R.; Salvador, I. Foreign body granulomatous reactions to cosmetic fillers: a clinical study of 15 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009, 108(2), 237–241. [Google Scholar] [CrossRef]
- Lombardi, T.; Samson, J.; Plantier, F.; Husson, C.; Küffer, R. Orofacial granulomas after injection of cosmetic fillers. Histopathologic and clinical study of 11 cases. J Oral Pathol Med 2004, 33, 115–120. [Google Scholar] [CrossRef]
- Jham, B.C.; Nikitakis, N.G.; Scheper, M.A.; Papadimitriou, J.C.; Levy, B.A.; Rivera, H. Granulomatous foreign-body reaction involving oral and perioral tissues after injection of biomaterials: a series of 7 cases and review of the literature. J Oral Maxillofac Surg 2009, 67(2), 280–285. [Google Scholar] [CrossRef]
- Stolman, L.P. Human collagen reactions. Dermatol Surg 2005, 31(11Pt 2) Pt 2, 1634. [Google Scholar] [CrossRef]
- Funt, D.; Pavicic, T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol 2013, 6, 295–316. [Google Scholar] [CrossRef] [PubMed]
- Monheit, G.D.; Rohrich, R.J. The nature of long-term fillers and the risk of complications. Dermatol Surg 2009, 35 (Suppl 2), 1598–1604. [Google Scholar] [CrossRef]
- Trinh, L.N.; McGuigan, K.C.; Gupta, A. Delayed Granulomas as a Complication Secondary to Lip Augmentation with Dermal Fillers: A Systematic Review. Surg J (N Y) 2022, 8, e69–e79. [Google Scholar] [CrossRef] [PubMed]
- Sage, R.J.; Chaffins, M.L.; Jouba, D.J. Granulomatous foreign body reaction to hyaluronic acid: report of a case after nasolabial fold augmentation and review of management. Derm Surg 2009, 35, 1696–1700. [Google Scholar] [CrossRef] [PubMed]
- Arin, M.J.; Bäte, J.; Krieg, T.; Hunzelmann, N. Silicone granuloma of the face treated with minocycline. J Am Acad Dermatol 2005, 52(2), S53–S56. [Google Scholar] [CrossRef]
- Baumann, L.S.; Halem, M.L. Lip silicone granulomatous foreign body reaction treated with aldara (imiquimod 5%). Dermatol Surg 2003, 29(4), 429–432. [Google Scholar] [CrossRef]
- Akrish, S.; Dayan, D.; Taicher, S.; Adam, I.; Nagler, R.M. Foreign body granulomas after injection of bio-alcamid for lip augmentation. Am J Otolaryngol 2009, 30, 356–359. [Google Scholar] [CrossRef]
- Hubmer, M.G.; Hoffmann, C.; Popper, H.; Scharnagl, E. Expanded polytetrafluoroethylene threads for lip augmentation induce foreign body granulomatous reaction. Plast Reconstr Surg 1999, 103(4), 1277–1279. [Google Scholar] [CrossRef]
- Mercer, S.E.; Kleinerman, R.; Goldenberg, G.; Emanuel, P.O. Histopathologic identification of dermal filler agents. J Drugs Dermatol 2010, 9, 1072–1078. [Google Scholar] [PubMed]
- Requena, L.; Requena, C.; Christensen, L.; Zimmermann, U.S.; Kutzner, H.; Cerroni, L. Adverse reactions to injectable soft tissue fillers. J Am Acad Dermatol 2011, 64, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Conejo-Mir, J.S.; Sanz Guirado, S.; Angel Muñoz, M. Adverse granulomatous reaction to Artecoll treated by intralesional 5-fluorouracil and triamcinolone injections. Dermatol Surg 2006, 32, 1079–1082. [Google Scholar]
- Christensen, L.; Breiting, V.; Janssen, M.; Vuust, J.; Hogdall, E. Adverse reactions to injectable soft tissue permanent fillers. Aesthetic Plast Surg 2005, 29, 34–48. [Google Scholar] [CrossRef] [PubMed]
- Pasternack, F.R.; Fox, L.P.; Engler, D.E. Silicone granulomas treated with etanercept. Arch Dermatol 2005, 141(1), 13–15. [Google Scholar] [CrossRef] [PubMed]
- Kastner, S.; Gonser, P.; Paprottka, F.; et al. Removal of polyacrylamide gel (Aquamid) from the lip as a solution for late-onset complications: our 8-year experience. Aesthetic Plast Surg 2018, 42, 791–797. [Google Scholar] [CrossRef] [PubMed]
- Fanous, N.; Brousseau, V.J.; Yoskovitch, A. The ’bikini lip reduction’: a detailed approach to hypertrophic lips. Can J Plast Surg Winter 2007, 15, 205–210. [Google Scholar] [CrossRef]
- Rauso, R.; Califano, L.; Rugge, L.; et al. Surgical lip remodeling after injection of permanent filler. Aesthet Surg J 2019, 39, 565–571. [Google Scholar] [CrossRef]
- El-Nahas, M.A.; Ghareeb, F.M. Complicated facial filler management by facelift. Menoufia Med J 2021, 33, 1347–1351. [Google Scholar]
Figure 1.
The upper lip’s aesthetic is shaped after 16 years of treatment using a liquid silicone filling (Frontal view and upper lip vermilion).
Figure 1.
The upper lip’s aesthetic is shaped after 16 years of treatment using a liquid silicone filling (Frontal view and upper lip vermilion).

Figure 2.
The first surgical procedure used a chalazion clamp that was placed (left) to help with the linear incision.
Figure 2.
The first surgical procedure used a chalazion clamp that was placed (left) to help with the linear incision.
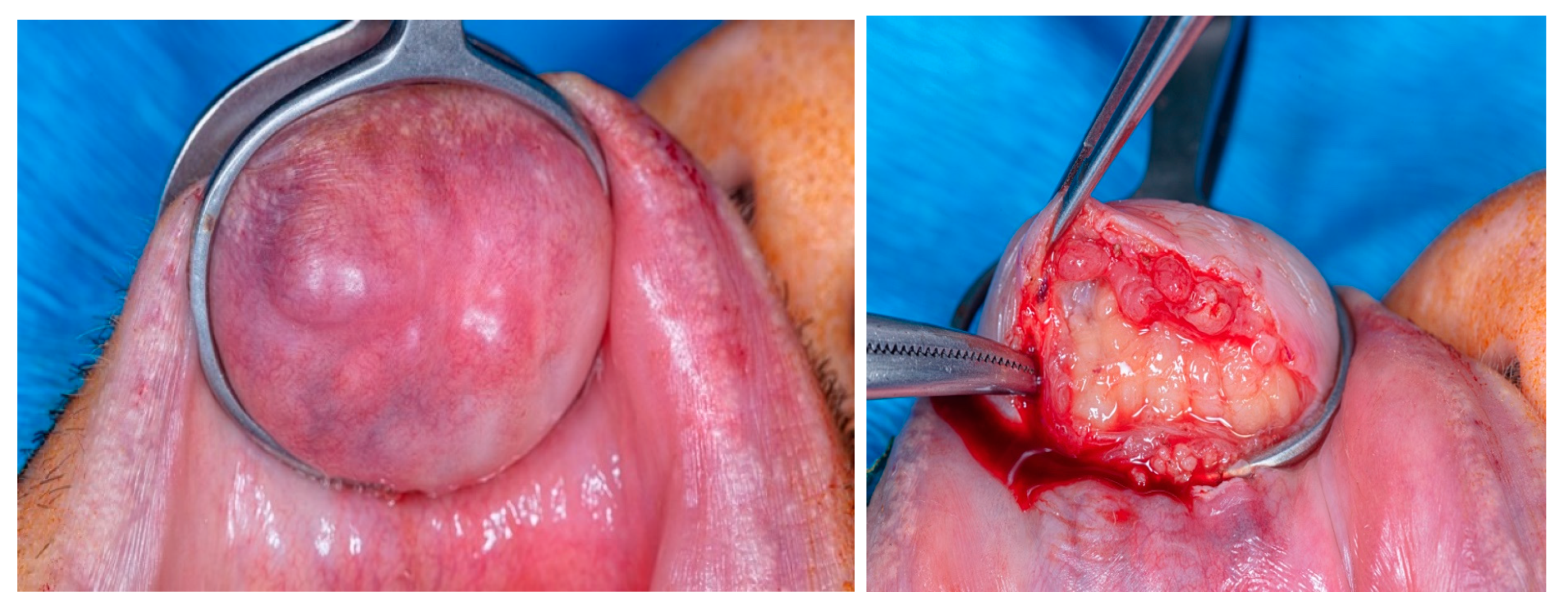
Figure 3.
A portion of the biopsied material.
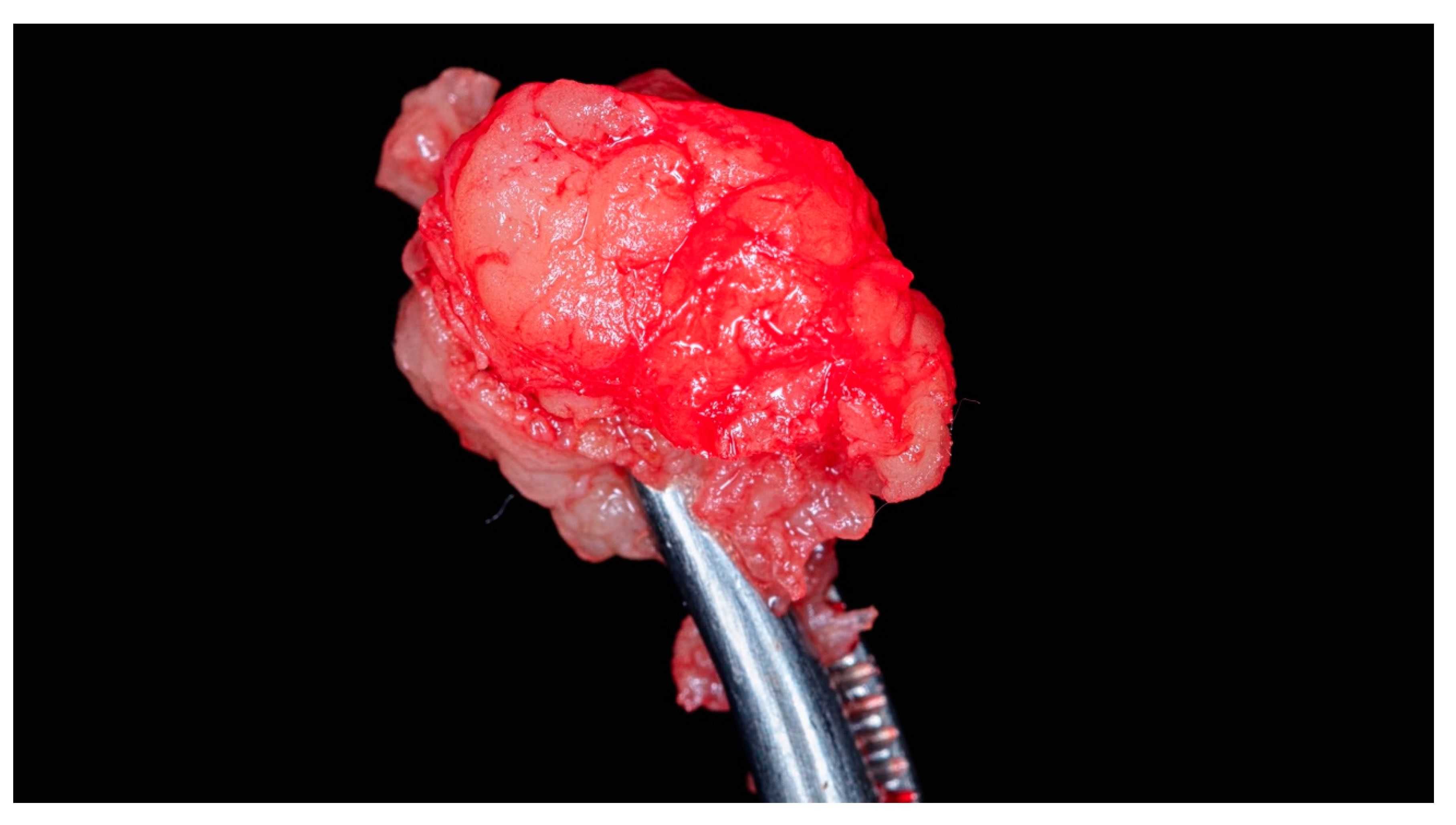
Figure 4.
Left side: Histological analysis with Hematoxylin and eosin stain (HE), 40x, showing a fibroadipose tissue, mixed inflammatory infiltrate, and multinucleated giant foreign body-type cells in relation to eosinophilic material; Right side: 100x mixed mononuclear and polymorphonuclear inflammatory infiltrate including foreign body multinucleated giant infectious cells.
Figure 4.
Left side: Histological analysis with Hematoxylin and eosin stain (HE), 40x, showing a fibroadipose tissue, mixed inflammatory infiltrate, and multinucleated giant foreign body-type cells in relation to eosinophilic material; Right side: 100x mixed mononuclear and polymorphonuclear inflammatory infiltrate including foreign body multinucleated giant infectious cells.
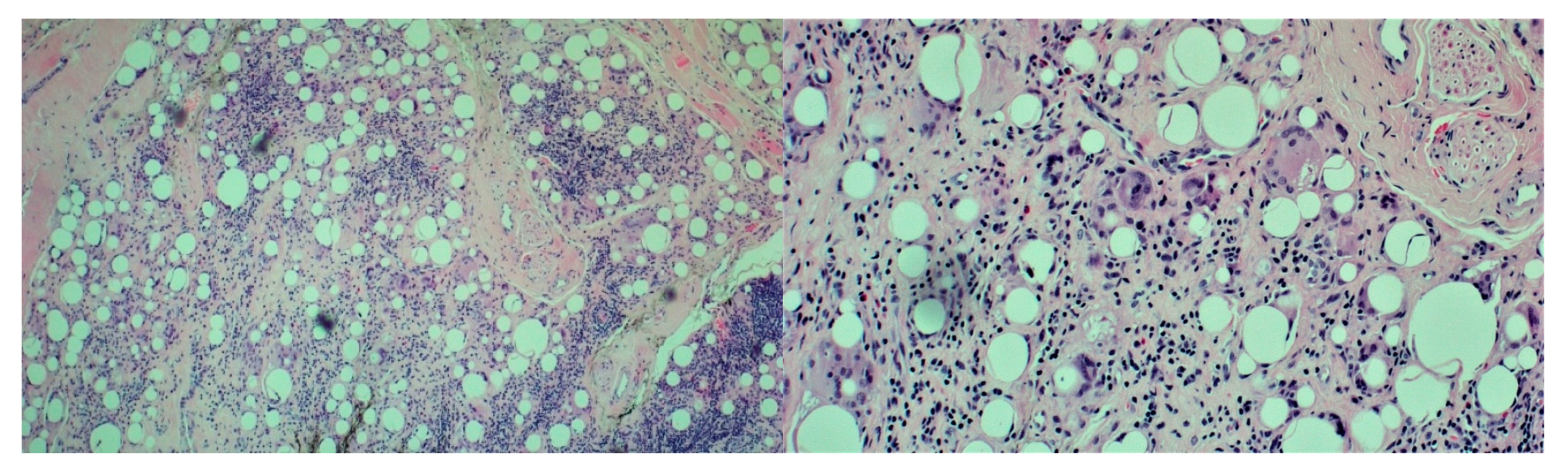
Figure 5.
Four months postoperative. Left side: Frontal view; Right side: Upper lip vermilion.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



