
Submitted:
06 March 2024
Posted:
07 March 2024
You are already at the latest version
Abstract
Shoulder tendinopathies produce pain and reduce functionality. The aim of this randomized clinical trial was to analyze the effects of Percutaneous electrolysis (PE), Percutaneous peripheral Nerve Stimulation (PNS) and eccentric exercise (EE), on pain (NPRS), strength, electromyographic activity, ultrasound characteristics of the tendon (echogenicity, thickness and hypervascularization) and functionality (DASH and SPADI) on individuals with supraspinatus tendinopathy. Participants (n=50) were divided into two groups, they received 4 treatment sessions, one per week, of PE and PNS (n=25) or 10 treatment sessions of TENS and US (n=25). Both groups performed EE program consisted of 3 sets of 10 repetitions of each of the 3 exercises, twice a day, during the 4 weeks. Follow-up was carried out at 4, 12 and 24 weeks after the start of the intervention. There are statistically significant differences in the analysis between groups (p<0.001) in the post-treatment and follow-up measurements favorable to the PE+PNS+EE treatment on pain (NPRS), strength, supraspinatus electromyographic amplitude, ultrasound characteristics of the tendon (echogenicity, thickness and hypervascularization) and DASH and SPADI questionnaires. The combined treatment PE, PNS and EE is an effective option in the clinical management of tendinopathies, with positive results in the short and long term on the variables studied.
Keywords:
percutaneous electrolysis
; peripheral nerve stimulation
; physical therapy
; shoulder pain
; supraspinatus tendinopathy
; ultrasonography.
1. Introduction
Tendinopathies are pathological situations of the tendon characterized by a degradation process of collagen fibers [1,2,3]. The disease causes pain, reduced range of motion, and decreased function and exercise tolerance [4]. Tendon injuries stand out in the shoulder [5,6,7], especially in the rotator cuff [8,9,10], with a prevalence of 4.5% in men and 6.1% in women [11] and high socioeconomic costs.
Injury to the supraspinatus affects joint stability, especially abduction and rotation movements. This greatly impairs the ability to carry out daily living activities, for example combing one’s hair or reaching for objects located on high shelves [9,12].
It is necessary to search for new treatment methodologies in the face of dissatisfaction with traditional medical and physiotherapeutic care protocols (rest, non-steroidal anti-inflammatory drugs and passives therapies) and the lack of consensus between them [7].
Nowadays, there are a few studies that support the effectiveness of invasive techniques such as Percutaneous Electrolysis (PE) directly at the point of injury [13] and Percutaneous peripheral Nerve Stimulation (PNS) to stimulate supraescapular nerve causing motor and sensory changes [14]. Both therapies are based on the application of direct current through needles, thanks to the ultrasound-guided development of the puncture [13]. This treatment causes an electrochemical reaction in the degenerated region of the tendon that facilitates collagen synthesis [15] and soft tissue regeneration [16,17,18], and reduce pain, and enhance movement, flexibility, strength and the development of tendon resistance over time [11,13].
Furthermore, updated interventions include Eccentric exercise (EE) to improve the resistance of non-contractile tissue thanks to the stimulation of fibroblasts, increasing collagen synthesis to reverse the pathological cycle [19,20,21,22].
The objective of this trial was to compare the effects of PE, PNS and EE with those of a well-established technique such as Transcutaneous Electrical Nerve Stimulation (TENS) and Therapeutic Ultrasound (US) for the management of supraspinatus tendinopathy. The hypothesis of our work was that treatment by PE and PNS is better than TENS and US in relieving pain (NPRS), increasing strength, and improving electromyographic activity, ultrasound characteristics of the tendon (echogenicity, thickness and hypervascularization) and functionality (DASH and SPADI) of patients with supraspinatus tendinopathy who simultaneously perform EE.
2. Materials and Methods
2.1. Study Design
Randomized clinical trial with blinded evaluation by third parties, longitudinal and prospective. The research was developed following the Declaration of Helsinki and the CONSORT guidelines for clinical research. Approval was received from the Cádiz Research Ethics Committee (registration code 1681-N-21) and the protocol was registered at ClicialTrials.gov (NCT05627102). The intervention lasted 4 weeks, the study variables were evaluated pre-intervention and with follow-up in the post-treatment (4 weeks) and at 12 and 24 weeks.
2.2. Participants
Individuals of both sexes between 18 and 65 years of age with painful symptoms associated with the supraspinatus tendon [10]: Shoulder pain in the insertion area of the supraspinatus tendon, which increases on palpation and is not associated with signs of root irritation. Structural changes in the tendon on ultrasound examination [23,24,25]. Reproducible pain in shoulder movements against resistance [10,26]. Positive result to Jobe, Neer and Hawkins-Kennedy tests [26].
Patients with any of the following conditions were excluded: bilateral involvement; previous treatment with PE or PNS in myotendinous pathology of the shoulder; recent severe trauma, surgery, previous shoulder fractures or dislocations; regular drug treatment; contraindicated invasive physiotherapy treatment (pregnant women, fibromyalgia, pacemaker patients, cancer patients, infectious processes or lymphedema).
All potential participants received the study information and signed the informed consent.
2.3. Sample Size Calculation, Randomization and Blinding
Epidat software version 3.1 (Servicio de Epidemiología de la Dirección Xeral de Saúde Pública da Consellería de Sanidade, Xunta de Galicia, Santiago de Compostela) is used. The calculation of the sample size is based on statistically significant differences of two units on the Numerical Pain Rate Scale (NPRS) [12], with a statistical power of 80% and setting a confidence level of 95%. Thus, it is determined that to carry out a study of these characteristics the sample size must be at least of 18 individuals per group (36 in total), however, when carrying out long-term follow-up and in view of possible losses, the sample was expanded to 25 subjects per group (making a total of 50 participants).
Recruitment took place at the Policlínica Santa María Clinic (Cádiz, Spain). The participants were randomly divided into two equal groups with the AleatorMetod program, with an equal distribution (1:1). The initial assessment and follow-up measurements were made by a blinded evaluator without access to the distribution of the groups.
2.4. Statistical Analysis
The statistical application was the SPSS® 23.0 (Statistical Package for the Social Sciences, Chicago, IL, USA) to MS Windows10®. Statistically significant differences between the quantitative variables of the groups are sought by studying the change with a Student’s t test for independent measures between the differences in means in the case of normal distributions. The measure of association between two categorical variables is carried out using χ2. A value of p≤0.05 and a 95% confidence interval were considered the degree of statistical significance.
2.5. Outcomes Measurements
NPRS allows pain to be assessed through eleven levels, from 0 (absence of pain) to 10 (maximum pain), it is a validated instrument for pain assessment and shows excellent test-retest reliability [12,27,28].
Assessment of rotator cuff muscle strength may be related to the integrity of the rotator cuff [29,30,31]. Strength in abduction movements and internal and external rotations was assessed with a portable handheld dynamometer held by the evaluator [26].
Surface electromyography (EMG) involves the quantitative recording and graphic representation of the electrical signal produced in muscle contraction [32]. The electromyographic amplitude of the supraspinatus and upper trapezius is assessed during the maximum voluntary isometric contraction in the abduction movement against resistance [33]. mDurance® device (MDurance Solutions S.L., España) was used.
Ultrasound assessment analyzed changes in echogenicity, thickening, and vascularization of the supraspinatus tendon [23,34]. The findings were compared with the unaffected contralateral shoulder. For each variable, the condition of positive or negative was registered. The ultrasound Mindray® DP30 was used with a high-frequency linear probe, carrying out a transverse and longitudinal scan [23,24,25,34,35,36,37].
Disabilities of the Arm, Shoulder and Hand (DASH) is a specific tool for assessing functionality and quality of life related to upper limb pathologies [38]. Shoulder Pain and Disability Index (SPADI) evaluates the patient’s perception regarding pain and disability associated with shoulder problems in their daily living activities [6,26,39].
2.6. Interventions
Two intervention groups are established, one with invasive physiotherapy treatment (PE+PNS) and the other with conventional electrotherapy treatment (TENS+US). Patients in both groups complete an EE program.
PE application (Figure 1) was carried out once a week for four weeks. The intensity was 350µA, for 72 seconds [11,12]. EPTE® Bipolar System device (Ionclinics & Deionics S.L., Valencia, Spain) was used for treatment and the Mindray® DP30 ultrasound machine was used for Ultrasound-Guided localization of the target tissue [40]. The patient should be supine, with the shoulder in internal rotation, elbow semi flexed, and forearm pronated on his abdomen [11,12,40,41]. With the probe over the supraspinatus tendon, the needle (negative electrode) is inserted at an angle of between 30º and 45º with the axis of the tendon [11,41] and the surface positive electrode is placed proximally over the upper trapezius muscle. 0.30x40mm acupuncture needles are used [11,40,42].
PNS is carried out after the application of PE, with the same treatment frequency, EPTE® Bipolar System device (Ionclinics & Deionics S.L., Valencia, Spain) and the Mindray® DP30 ultrasound machine were used. The needles are placed adjacent to the suprascapular nerve, deep to the upper trapezius and supraspinatus, the patient must be placed in lateral decubitus. A low frequency current (10Hz) is applied seeking a sensory or motor response (at an intensity tolerable for the patient) for 90 seconds [14]. 0.30x40mm acupuncture needles are used [40] (Figure 2).
Patients in the conventional electrotherapy treatment group receive 10 sessions of TENS and US, five days per week. TENS was applied with the Megasonic 313 P4 device (Electromedicarin®), for 20 minutes, frequency of 150Hz, pulse duration of 100µs [43] and tolerable intensity [44,45]. Positive electrode was placed on the supraspinatus muscle and negative electrode on the tendon [43] (conventional 5x9cm electrodes were used). Megasonic 212 K device (Electromedicarin®) was used to US treatment: 1MHz frequency, 1,5 W/cm2 power, in continuous mode over the painful area for 5 minutes [45,46,47,48].
The EE protocol includes 3 exercises, with 3 sets of 10 repetitions of each exercise, twice a day, for four weeks [11,19]. The first exercise focuses on the supraspinatus, the patient is standing and must perform shoulder abduction (concentric phase) followed by adduction of the same slowly (eccentric phase), with resistance from an elastic band [11,12,42]. The focus of the second exercise is the infraspinatus, from the seating position, the concentric phase will depend on external rotation, slowly returning to the initial position towards internal rotation [11,12,42]. The last one of the exercises focuses on global shoulder stability, the subject is placed on quadruped position, concentric phase in shoulder flexion and eccentric phase in the return movement [11,12,42] (Figure 3).
3. Results
A total of 50 patients completed all the tests and evaluations programmed in the study and were randomly assigned to 2 groups of 25 subjects (Figure 4). Men represented the 72% of the sample with a mean age of the total sample of 44.24 years old (SD=11.80). During ultrasound exploration, it has been possible to observe hypo-echogenicity, thickness and hypervascularization signs in more than 86% of the sample, finding statistically significant correlations between echogenicity and thickness (r=0.626; p<0.001), echogenicity and hypervascularization (r=0.626; p<0.001), as well as between thickness and hypervascularization (r=0.291; p=0.040). Conversely, although patients presented higher prevalence of right hand as dominant hand, as well as a greater prevalence of right hand as affected arm, the analysis has not revealed statistically significant correlations between the dominant hand and the affected arm (r=0.007; p=0.960). All morphologic and baseline data are exposed in Table 1.
In ultrasound scan evaluation at immediate post-treatment statistically significant differences have been only observed in hypervascularization (Echogenicity χ2=1.495; p=0.221 / Thickness χ2=0.355; p=0.552 / Hypervascularization χ2=9.921; p=0.002), being able to observe a reduction of positive cases in PE+PNS+EE group ranged between 8 and 40 percentage points in ultrasound scan evaluation (Table 2).
The results of the analysis of the variance performed, to evaluate the effect of the experimental therapy through time, showed statistically significant improvements in favor of the PE+PNS+EE group in all study variables, with effect sizes between medium and large and power values between 0.777 and 1.000 (Table 3).
Moreover, although the analysis of repeated measurements to evaluate within-groups differences revealed statistically significant improvements in both groups for all study variables (Table 4), the between-groups analysis thrown greater statistically significant enhancements in favor of the PE+PNS+EE group for all study variables. Furthermore, all significant variables, except internal rotation strength (d=0.691) and trapezius muscular recruitment (d=0.710) that showed medium effect size values, showed large effect size values ranged between 0.879 and 2.117 (Table 4). Attending the stablished clinical success criteria, PE+PNS+EE group showed a clinical success of 80% (20 patients), meanwhile TENS+US+EE group showed a clinical success of 32% (8 patients) at immediate post-treatment. Thus, in case of the PE+PNS+EE treatment, probability of success increases by 48% (Absolute risk reduction (ARR)=0.48; 95%IC=0.24 to 0.72). In other words, 2.083 subjects are needed to get at least one favorable outcome compared to the TENS+US+EE group (Number needed to treat (NNT)=2.083; 95%IC=1.39 to 4.18) at immediate post-treatment.
At 12 weeks follow-up, statistically significant differences are appreciated between PE+PNS+EE and TENS+US+EE groups percentages for all ultrasound scan evaluations (Echogenicity χ2=3.947; p=0.047 / Thickness χ2=12.000; p=0.001 / Hypervascularization χ2=11.688; p=0.001), being able to observe a reduction of positive cases in PE+PNS+EE group ranged between 24 and 60 percentage points in ultrasound scan evaluation (Table 2). In the same way that immediate post-treatment analysis, the between-groups analysis thrown greater statistically significant enhancements in favor of the PE+PNS+EE group for all study variables (Table 4).
All significant variables showed large effect size values ranged between -0.883 and -2.358 (Table 4). Attending the stablished clinical success criteria, PE+PNS+EE group showed a clinical success of 92% (23 subjects), meanwhile TENS+US+EE group showed a clinical success of 68% (17 subjects) at the 12 weeks follow-up.
Therefore, in case of the PE+PNS+EE treatment, probability of success increases by 24% (ARR=0.24; 95%IC=0.03 to 0.45). In other words, 4.167 patients are needed to get at least one favorable outcome compared to the TENS+US+EE group (NNT=4.167; 95%IC=2.21 to 35.13) at the 12 weeks follow-up.
At 24 weeks follow-up, statistically significant differences are appreciated between PE+PNS+EE and TENS+US+EE groups percentages for all ultrasound scan evaluations (Echogenicity χ2=8.117; p=0.004 / Thickness χ2=14.346; p<0.001 / Hypervascularization χ2=13.235; p<0.001), being able to observe a reduction of positive cases in PE+PNS+EE group ranged between 52 and 84 percentage points in ultrasound scan evaluation (Table 2). Table 4 shows statistically significant improvements in both groups for all study variables. PE+PNS+EE group showed a clinical success of 92% (23 subjects), meanwhile TENS+US+EE group showed a clinical success of 72% (18 subjects). Therefore, in case of the PE+PNS+EE treatment, probability of success increases by 20% (ARR=0.20; 95%IC=-0.01 to 0.41). In other words, 5 people are needed to get at least one favorable outcome compared to the TENS+US+EE group (NNT=5; 95%IC=2.47 to-177.26).
4. Discussion
The effects achieved with the treatment of PE+PNS+EE offer statistically significant improvements superior to the treatment protocol of TENS+US+EE on variables analyzed, both in the direct post-intervention assessment and in the follow-up measurements.
The combination of PE, PNS and EE has superior clinical success (pain reduction and structural changes), the effect occurs in the shorter term (at the end of the treatment) and is maintained over time. Therefore, it would be possible to consider that these treatments favor the repair of the injured structure and control the nociceptive stimulus of local origin [49,50,51].
PE produces a localized inflammatory response on the injured tendon, thus initiating the repair mechanisms [52] thanks to the mechanical stimulus, the modification of the pH [53] and the activation of the NLRP3 inflammasome that promotes collagen synthesis [54,55] and matrix remodeling [56]. In addition, PNS causes stimulation of Aβ nerve fibers, which blocks nociceptive information from the Aδ and C fibers [14,57]. This may be linked to the control of pain perception and also to the optimization of muscle function [14,57,58] taking into account the relationship between the suprascapular nerve and rotator cuff tendinopathy [59,60,61].
On the other hand, exercise makes possible to achieve changes in pain perception [51] and provides mechanical loading stimulus, this enables tendon development and longitudinal collagen alignment [62], increases the cross section, muscle strengthening and greater resistance capacity of the tendon [19,63]. The EE program represents the common point between the treatments and intra-group improvements were found in both groups at follow-up. The changes in the TENS+US+EE group appear in the longer term and could be related to the effects derived from the EE.
In both treatment groups, higher strength levels were achieved in the post-intervention follow-up evaluations compared to baseline strength. These changes are statistically significant and attributable to the EE in the protocols. Loss of strength could be a predisposing factor for shoulder injuries [64], Through EE, muscle strengthening is achieved and the capacity of the tendon increases [65].
Along the same lines, the increase in strength levels is also reflected in electromyographic activity. In the analysis of the basal condition, it is observed that in the subjects of both groups there are average levels of activation of the upper trapezius above the supraspinatus in the abduction movement, taking into account that pain and dysfunction modify glenohumeral and scapulothoracic neuromuscular recruitment patterns [32].
The intragroup analysis indicates that in both groups there is progress towards greater activation of the supraspinatus and a stabilization of the signal amplitude of the upper trapezius. With PE+PNS+EE treatment there is a greater increase in the electromyographic activity of the supraspinatus. This could indicate that better biomechanical performance is achieved when the treatment produces analgesia and reversal of the pathological cycle.
In the ultrasound evaluation, focal hypoechoic areas [34], thickening as part of the degenerative process [34] (there is no classic prostaglandin inflammation [66]), neovascularization and neoinnervation as a result of a failed repair process [34] are observed. There is a statistically significant correlation between echogenicity and thickening, echogenicity and vascularization, and thickening and vascularization.
In the post-intervention results, a greater reduction in positive cases was found in the PE+PNS+US group than in the TENS+US+EE group. Therefore, the combination of PE+PNS+US could be associated with greater structural changes in the tissue and in symptomatology.
DASH [38] and SPADI [6,39] questionnaires express the degree of disability of the patient, which could be explained as the result of the combination of painful perception and limitation of movement. In the intragroup analysis of the pre- and post-intervention differences, changes appear in both treatment groups.
However, The comparison between groups offers statistically significant differences favorable to the PE+PNS+EE group, same results as in research that includes PE+EE [11,42] or different types of exercise [67].
The strong point of this study is the inclusion of two invasive physiotherapy techniques at the forefront in the clinical field, long-term monitoring of study variables, and the inclusion of ultrasound analysis, electromyographic activity of the supraspinatus muscle, and muscle strength in rotator cuff movements.
There are limitations because the invasive physiotherapy treatments applied depend on the physiotherapist and performing EE daily depends on the patient. Likewise, the ultrasound study of the tendon has been evaluated qualitatively and is dependent on the evaluator.
A more in-depth analysis of EMG could be included in future studies: contralateral comparison; assessment of more muscle groups and in different movements or types of contraction; evaluation of the muscle activation sequence; and the assessment combined with other variables (electromyographic activity and dynamometry). Equally, in future research it would be advisable to separately analyze the effects of each proposed intervention, to include greater blinding conditions (sham invasive treatment), different dosages of the treatments and analyze the effects on tendons in other areas of the body.
5. Conclusions
The combined treatment of PE, PNS and EE is an effective option in the clinical management of tendinopathies, with positive results in the short and long term. Statistically significant improvements appear in pain (NPRS), strength in abduction movements and internal and external rotations, electromyographic activity of the supraspinatus in shoulder abduction, ultrasound characteristics of the tendon (thickening, echogenicity and hypervascularization) and functionality shoulder (DASH and SPADI) with the intervention parameters proposed in this study.
Author Contributions
Conceptualization, J.G.-R. and M.R.-H.; methodology, J.G.-R M.R.-H. and P.G.-R.; software, D.R.-A. and P.G.-R.; validation, J.G.-R.; formal analysis, D.R.-A.; R.M.-V. and M.A.R.-R.; investigation, J.G.-R. and M.R.-H.; resources, M.R.-H. and M.A.R.-R.; data curation, J.G.-R and D.R.-A.; writing—original draft preparation, J.G.-R. and P.G.-R.; writing—review and editing, M.R.-H.; M.A.R.-R. and R.M.-V.; visualization, R.M.-V. and J.G.-R.; supervision, M.R.-H. and M.A.R.-R.; project administration, J.G.-R.; M.R.-H; and M.A.R.-R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by Cádiz Research Ethics Committee (registration code 1681-N-21).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
Jorge Góngora-Rodríguez received Aid Program for Researchers in Training of the Ilustre Colegio Profesional de Fisioterapeutas de Andalucía (Professional College).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lipman, K.; Wang, C.; Ting, K.; Soo, C.; Zheng, Z. Tendinopathy: injury, repair, and current exploration. Drug Des. Devel. Ther. 2018, 12, 591–603. [Google Scholar] [CrossRef]
- Millar, N.L.; Silbernagel, K.G.; Thorborg, K.; Kirwan, P.D.; Galatz, L.M.; Abrams, G.D.; Murrell, G.A.C.; McInnes, I.B.; Rodeo, S.A. Tendinopathy. Nat. Rev. Dis. Prim. 2021, 7. [Google Scholar] [CrossRef]
- Andarawis-Puri, N.; Flatow, E.L. Promoting effective tendon healing and remodeling. J. Orthop. Res. 2018, 36, 3115–3124. [Google Scholar] [CrossRef]
- Joyce, D.; Robinson, K. Sport Science of Injury. In NSCA’s Essentials of Sport Science; French, D., Torres Ronda, L., Eds.; Human Kinetics Publishers Inc.: Champaign, 2022; ISBN 978-1-4925-9335-5. [Google Scholar]
- Chianca, V.; Albano, D.; Messina, C.; Midiri, F.; Mauri, G.; Aliprandi, A.; Catapano, M.; Pescatori, L.C.; Monaco, C.G.; Gitto, S.; et al. Rotator cuff calcific tendinopathy: from diagnosis to treatment. Acta Biomed. 2018, 89, 186–196. [Google Scholar] [CrossRef]
- Engebretsen, K.; Grotle, M.; Bautz-Holter, E.; Ekeberg, O.M.; Brox, J.I. Determinants of the Shoulder Pain and Disability Index in patients with subacromial shoulder pain. J. Rehabil. Med. 2010, 42, 499–505. [Google Scholar] [CrossRef]
- Doiron-Cadrin, P.; Lafrance, S.; Saulnier, M.; Cournoyer, É.; Roy, J.S.; Dyer, J.O.; Frémont, P.; Dionne, C.; MacDermid, J.C.; Tousignant, M.; et al. Shoulder Rotator Cuff Disorders: A Systematic Review of Clinical Practice Guidelines and Semantic Analyses of Recommendations. Arch. Phys. Med. Rehabil. 2020, 101, 1233–1242. [Google Scholar] [CrossRef]
- Lewis, J.S. Rotator cuff tendinopathy. Br. J. Sports Med. 2009, 43, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Osborne, J.D.; Gowda, A.L.; Wiater, B.; Wiater, J.M. Rotator cuff rehabilitation: Current theories and practice. Phys. Sportsmed. 2016, 44, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Littlewood, C.; Bateman, M.; Connor, C.; Gibson, J.; Horsley, I.; Jaggi, A.; Jones, V.; Meakins, A.; Scott, M. Physiotherapists’ recommendations for examination and treatment of rotator cuff related shoulder pain: A consensus exercise. Physiother. Pract. Res. 2019, 40, 87–94. [Google Scholar] [CrossRef]
- Arias-Buría, J.L.; Truyols-Domínguez, S.; Valero-Alcaide, R.; Salom-Moreno, J.; Atín-Arratibel, M.A.; Fernández-De-Las-Peñas, C. Ultrasound-Guided Percutaneous Electrolysis and Eccentric Exercises for Subacromial Pain Syndrome: A Randomized Clinical Trial. Evidence-based Complement. Altern. Med. 2015, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Huguet, M.; Góngora-Rodríguez, J.; Rodríguez-Huguet, P.; Ibañez-Vera, A.J.; Rodríguez-Almagro, D.; Martín-Valero, R.; Díaz-Fernández, Á.; Lomas-Vega, R. Effectiveness of Percutaneous Electrolysis in Supraspinatus Tendinopathy: A Single-Blinded Randomized Controlled Trial. J. Clin. Med. 2020, 9, 1837. [Google Scholar] [CrossRef] [PubMed]
- Valera-Garrido, F.; Minaya-Muñoz, F. Concepto y fundamentos de la electrolisis percutánea musculoesquelética (EPM). In Electrolisis percutánea musculoesquelética. Tendón y bursa; Valera-Garrido, F., Minaya-Muñoz, F., Eds.; Elsevier: Barcelona, 2021; pp. 3–24. ISBN 978-84-9113-016-1. [Google Scholar]
- Minaya-Muñoz, F.; Valera-Garrido, F. Neuromodulación percutánea ecoguiada. In Fisioterapia invasiva; Valera-Garrido, F., Minaya-Muñoz, F., Eds.; Elsevier: Barcelona, 2017; pp. 283–294. [Google Scholar]
- Sánchez-Ibáñez, J.; Colmena, C.; Benabent, J.; García-Herreros, S.; Valles, S.-L. New Technique in Tendon Sport Recovery. Percutaneous Electrolysis Intratissue (EPI®). Int. J. Phys. Med. Rehabil. 2013, 1, 1000113, http://dx.doi.org/10.4172/jpmr.1000113. [Google Scholar]
- Valera-Garrido, F.; Minaya-Muñoz, F.; Sánchez-Ibáñez, J.M.; García-Palencia, P.; Valderrama-Canales, F.; Medina-Mirapeix, F.; Polidori, F. Comparison of the Acute Inflammatory Response and Proliferation of Dry Needling and Electrolysis Percutaneous Intratissue (EPI®) in Healthy Rat Achilles Tendons. Br. J. Sports Med. 2013, 47, 29–30. [Google Scholar] [CrossRef]
- García-Bermejo, P.; De-La-Cruz-Torres, B.; Naranjo-Orellana, J.; Albornoz-Cabello, M. Autonomic Responses to Ultrasound-Guided Percutaneous Needle Electrolysis: Effect of Needle Puncture or Electrical Current? J. Altern. Complement. Med. 2018, 24, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Huguet, M.; Góngora-Rodríguez, J.; Lomas-Vega, R.; Martín-Valero, R.; Díaz-Fernández, Á.; Obrero-Gaitán, E.; Ibáñez-Vera, A.J.; Rodríguez-Almagro, D. Percutaneous Electrolysis in the Treatment of Lateral Epicondylalgia: A Single-Blind Randomized Controlled Trial. J. Clin. Med. 2020, 9, 2068. [Google Scholar] [CrossRef]
- Macías-Hernández, S.I.; Pérez-Ramírez, L.E. Fortalecimiento excéntrico en tendinopatías del manguito de los rotadores asociadas a pinzamiento subacromial. Evidencia actual. Cir. Cir. 2015, 83, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Dejaco, B.; Habets, B.; van Loon, C.; van Grinsven, S.; van Cingel, R. Eccentric versus conventional exercise therapy in patients with rotator cuff tendinopathy: a randomized, single blinded, clinical trial. Knee Surgery, Sport. Traumatol. Arthrosc. 2017, 25, 2051–2059. [Google Scholar] [CrossRef]
- Malliaras, P.; Johnston, R.; Street, G.; Littlewood, C.; Bennell, K.; Haines, T.; Buchbinder, R. The Efficacy of Higher Versus Lower Dose Exercise in Rotator Cuff Tendinopathy: A Systematic Review of Randomized Controlled Trials. Arch. Phys. Med. Rehabil. 2020, 101, 1822–1834. [Google Scholar] [CrossRef]
- Heron, S.; Woby, S.; Thompson, D. Comparison of three types of exercise in the treatment of rotator cuff tendinopathy/shoulder impingement syndrome: A randomized controlled trial. Physiotherapy 2017, 103. [Google Scholar] [CrossRef]
- Martinoli, C.; Beggs, I.; Bianchi, S.; Bueno, A.; Cohen, M.; Court-payen, M.; Grainger, A.; Kainberger, F.; Klauser, A.; Mcnally, E.; et al. Musculoskeletal ultrasound: technical guidelines. Insights Imaging 2010, 1, 99–141. [Google Scholar] [CrossRef]
- Jacobson, J.A. Shoulder US: anatomy, technique, and scanning pitfalls. Radiology 2011, 260, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.H.; Sheehan, S.E.; Orwin, J.F.; Lee, K.S. Comprehensive Shoulder US Examination: A Standardized Approach with Multimodality Correlation for Common Shoulder Disease. Radiogr. a Rev. Publ. Radiol. Soc. North Am. Inc 2016, 36, 1606–1627. [Google Scholar] [CrossRef] [PubMed]
- Kinsella, R.; Cowan, S.M.; Watson, L.; Pizzari, T. A comparison of isometric, isotonic concentric and isotonic eccentric exercises in the physiotherapy management of subacromial pain syndrome/rotator cuff tendinopathy: Study protocol for a pilot randomised controlled trial. Pilot Feasibility Stud. 2017, 3. [Google Scholar] [CrossRef] [PubMed]
- Thong, I.S.K.; Jensen, M.P.; Miró, J.; Tan, G. The validity of pain intensity measures: What do the NRS, VAS, VRS, and FPS-R measure? Scand. J. Pain 2018, 18, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Alghadir, A.; Anwer, S.; Iqbal, A.; Iqbal, Z. Test-retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J Pain Res 2018, 11, 851–856. [Google Scholar] [CrossRef]
- Beshay, N.; Lam, P.H.; Murrell, G.A.C. Assessing the Reliability of Shoulder Strength Measurement: Hand-Held versus Fixed Dynamometry. Shoulder Elb. 2011, 3, 244–251. [Google Scholar] [CrossRef]
- Holt, K.L.; Raper, D.P.; Boettcher, C.E.; Waddington, G.S.; Drew, M.K. Hand-held dynamometry strength measures for internal and external rotation demonstrate superior reliability, lower minimal detectable change and higher correlation to isokinetic dynamometry than externally-fixed dynamometry of the shoulder. Phys. Ther. Sport 2016, 21, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, L.; Oestergaard, L.G.; van Tulder, M.; Petersen, A.K. Measurement Properties of Isokinetic Dynamometry for Assessment of Shoulder Muscle Strength: A Systematic Review. Arch. Phys. Med. Rehabil. 2021, 102, 510–520. [Google Scholar] [CrossRef]
- Guzmán-Muñoz, E.; Méndez-Rebolledo, G. Electromiografía en las Ciencias de la Rehabilitación. Salud Uninorte 2018, 34, 753–765. [Google Scholar] [CrossRef]
- Sethi, K.; Noohu, M.M. Scapular muscles strengthening on pain, functional outcome and muscle activity in chronic lateral epicondylalgia. J. Orthop. Sci. 2018, 23, 777–782. [Google Scholar] [CrossRef]
- Valera-Garrido, F.; Minaya-Muñoz, F. Evaluación, descripción y guía ecográfica en la aplicación de la electrolisis percutánea en las tendinopatías y lesiones bursales. In Electrolisis percutánea musculoesquelética. Tendón y bursa; Valera-Garrido, F., Minaya-Muñoz, F., Eds.; Elsevier: Barcelona, 2021; pp. 71–88. [Google Scholar]
- Valera-Garrido, F.; Minaya-Muñoz, F. Procedimientos invasivos ecoguiados en fisioterapia. In Fisioterapia invasiva; Valera-Garrido, F., Minaya-Muñoz, F., Eds.; Elsevier: Barcelona, 2017; pp. 215–246. [Google Scholar]
- Papatheodorou, A.; Ellinas, P.; Takis, F.; Tsanis, A.; Maris, I.; Batakis, N. US of the shoulder: Rotator cuff and non-rotator cuff disorders. Radiographics 2006, 26. [Google Scholar] [CrossRef] [PubMed]
- Del-Castillo-González, F. Diagnóstico ecográfico. In Lesiones músculo-tendinosas en el medio deportivo; Del-Castillo-Campos, M.J., Ramos-Álvarez, J.J., Polo-Portes, C., Eds.; Dirección General de Juventud y Deportes. Consejería de Educación, Juventud y Deporte. Comunidad de Madrid: Madrid, 2017; pp. 74–82. [Google Scholar]
- Hervás, M.T.; Navarro Collado, M.J.; Peiró, S.; Rodrigo Pérez, J.L.; López Matéu, P.; Martínez Tello, I. Versión Española del cuestionario DASH. Adaptación transcultural, fiabilidad, validez y sensibilidad a los cambios. Med. Clin. (Barc). 2006, 127, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Torres-Lacomba, M.; Sánchez-Sánchez, B.; Prieto-Gómez, V.; Pacheco-da-Costa, S.; Yuste-Sánchez, M.J.; Navarro-Brazález, B.; Gutiérrez-Ortega, C. Spanish cultural adaptation and validation of the shoulder pain and disability index, and the oxford shoulder score after breast cancer surgery. Health Qual. Life Outcomes 2015, 13. [Google Scholar] [CrossRef]
- Valera-Garrido, F.; Minaya-Muñoz, F. Electrolisis percutánea en tendón y bursa. Metodología de aplicación. In Electrolisis percutánea musculoesquelética. Tendón y bursa; Valera-Garrido, F., Minaya-Muñoz, F., Eds.; Elsevier: Barcelona, 2021; pp. 45–70. ISBN 978-84-9113-016-1. [Google Scholar]
- Valera-Garrido, F.; Minaya-Muñoz, F.; Pereira-Barbosa, M. Electrolisis percutánea ecoguiada en el manguito rotador. In Electrolisis percutánea musculoesquelética. Tendón y bursa; Valera-Garrido, F., Minaya-Muñoz, F., Eds.; Elsevier: Barcelona, 2021; pp. 107–130. [Google Scholar]
- De-Miguel-Valtierra, L.; Salom-Moreno, J.; Fernández-de-las-Peñas, C.; Cleland, J.A.; Arias-Buría, J.L. Ultrasound-Guided Application of Percutaneous Electrolysis as an Adjunct to Exercise and Manual Therapy for Subacromial Pain Syndrome: A Randomized Clinical Trial. J. Pain 2018, 19, 1201–1210. [Google Scholar] [CrossRef]
- Maya-Martín, J.; Albornoz-Cabello, M. Estimulación eléctrica transcutánea. In Electroestimulación transcutánea y neuromuscular, y neuromodulación; Albornoz-Cabello, M., Maya-Martín, J., Eds.; Elsevier: Barcelona, 2021; pp. 1–76. ISBN 978-84-9113-606-4. [Google Scholar]
- Lin, M.L.; Chiu, H.W.; Shih, Z.M.; Lee, P.Y.; Li, P.Z.; Guo, C.H.; Luo, Y.J.; Lin, S.C.; Lin, K.Y.; Hsu, Y.M.; et al. Two transcutaneous stimulation techniques in shoulder pain: Transcutaneous Pulsed Radiofrequency (TPRF) versus transcutaneous electrical nerve stimulation (TENS): A comparative pilot study. Pain Res. Manag. 2019, 2019. [Google Scholar] [CrossRef]
- Gunay Ucurum, S.; Kaya, D.O.; Kayali, Y.; Askin, A.; Tekindal, M.A. Comparison of different electrotherapy methods and exercise therapy in shoulder impingement syndrome: A prospective randomized controlled trial. Acta Orthop. Traumatol. Turc. 2018, 52, 249–255. [Google Scholar] [CrossRef]
- Desmeules, F.; Boudreault, J.; Dionne, C.E.; Frémont, P.; Lowry, V.; MacDermid, J.C.; Roy, J.-S. Efficacy of exercise therapy in workers with rotator cuff tendinopathy: a systematic review. J. Occup. Health 2016, 58, 15-0103-RA. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Green, S.; Mrocki, M.A.; Surace, S.J.; Deitch, J.; Mcbain, B.; Lyttle, N.; Buchbinder, R. Electrotherapy modalities for rotator cuff disease. Cochrane Database Syst. Rev. 2016, 2016. [Google Scholar] [CrossRef]
- Balci, T.O.; Turk, A.C.; Sahin, F.; Kotevoglu, N.; Kuran, B. Efficacy of therapeutic ultrasound in treatment of adhesive capsulitis: A prospective double blind placebo-controlled randomized trial. J. Back Musculoskelet. Rehabil. 2018, 31, 955–961. [Google Scholar] [CrossRef]
- Cook, J.L.; Purdam, C.R. Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br. J. Sports Med. 2009, 43, 409–416. [Google Scholar] [CrossRef]
- Rio, E.; Moseley, L.; Purdam, C.; Samiric, T.; Kidgell, D.; Pearce, A.J.; Jaberzadeh, S.; Cook, J. The pain of tendinopathy: physiological or pathophysiological? Sports Med. 2014, 44, 9–23. [Google Scholar] [CrossRef] [PubMed]
- Rio, E.; Kidgell, D.; Lorimer Moseley, G.; Gaida, J.; Docking, S.; Purdam, C.; Cook, J. Tendon neuroplastic training: changing the way we think about tendon rehabilitation: a narrative review. Br. J. Sports Med. 2016, 50, 209–215. [Google Scholar] [CrossRef]
- Calderón-Díez, L.; Sánchez-Sánchez, J.L.; Sánchez-Ibáñez, J.M.; Belón-Pérez, P. Percutaneous Electrolysis (EPI®), a Promising Technology in the Treatment of Insertional Patellar Tendinopathy in Soccer Players. 2023, 24–31, https://doi.org/10.1007/978-3-031-22356-3_3/COVER. [Google Scholar]
- Margalef, R.; Minaya-Muñoz, F.; Valera-Garrido, F.; Bosque, M.; Santafé, M.M. Changes in pH as a result of galvanic currents used in percutaneous needle electrolysis. Rev. Fisioter. Invasiva / J. Invasive Tech. Phys. Ther. 2020, 03, 006–006. [Google Scholar] [CrossRef]
- Peñín-Franch, A.; García-Vidal, J.A.; Martínez, C.M.; Escolar-Reina, P.; Martínez-Ojeda, R.M.; Gómez, A.I.; Bueno, J.M.; Minaya-Muñoz, F.; Valera-Garrido, F.; Medina-Mirapeix, F.; et al. Galvanic current activates the NLRP3 inflammasome to promote Type I collagen production in tendon. Elife 2022, 11, e73675. [Google Scholar] [CrossRef] [PubMed]
- Peñín-Franch, A.; García-Vidal, J.A.; Escolar-Reina, P.; Medina-Mirapeix, F.; Pelegrín-Vivancos, P. Electrolisis e inflamación. Bases biológicas de la electrolisis percutánea. In Electrolisis percutánea musculoesquelética. Tendón y bursa; Valera-Garrido, F., Minaya-Muñoz, F., Eds.; Elsevier: Barcelona, 2021; pp. 25–32. ISBN 978-84-9113-016-1. [Google Scholar]
- Sánchez-Sánchez, J.L.; Calderón-Díez, L.; Herrero-Turrión, J.; Méndez-Sánchez, R.; Arias-Buría, J.L.; Fernández-De-Las-Peñas, C. Changes in Gene Expression Associated with Collagen Regeneration and Remodeling of Extracellular Matrix after Percutaneous Electrolysis on Collagenase-Induced Achilles Tendinopathy in an Experimental Animal Model: A Pilot Study. J. Clin. Med. 2020, 9, 3316. [Google Scholar] [CrossRef]
- Albornoz-Cabello, M.; Castro-Sánchez, A.M. Neuromodulación periférica transcutánea. In Electroestimulación transcutánea y neuromuscular, y neuromodulación; Albornoz-Cabello, M., Maya-Martín, J., Eds.; Elsevier: Barcelona, 2021; pp. 171–196. ISBN 978-84-9113-606-4. [Google Scholar]
- Wilson, R.D.; Harris, M.A.; Gunzler, D.D.; Bennett, M.E.; Chae, J. Percutaneous peripheral nerve stimulation for chronic pain in subacromial impingement syndrome: A case series. Neuromodulation 2014, 17, 771–776. [Google Scholar] [CrossRef]
- Shi, L.L.; Freehill, M.T.; Yannopoulos, P.; Warner, J.J.P. Suprascapular nerve: is it important in cuff pathology? Adv. Orthop. 2012, 2012, 1–6. [Google Scholar] [CrossRef]
- Wu, W.T.; Chen, L.R.; Chang, H.C.; Chang, K.V.; Özçakar, L. Quantitative Ultrasonographic Analysis of Changes of the Suprascapular Nerve in the Aging Population With Shoulder Pain. Front. Bioeng. Biotechnol. 2021, 9, 640747. [Google Scholar] [CrossRef]
- Sun, Y.; Wang, C.; Kwak, J.M.; Jung, H. won; Kholinne, E.; Jeon, I.H. Suprascapular nerve neuropathy leads to supraspinatus tendon degeneration. J. Orthop. Sci. 2020, 25, 588–594. [Google Scholar] [CrossRef]
- Nakanishi, Y.; Okada, T.; Takeuchi, N.; Kozono, N.; Senju, T.; Nakayama, K.; Nakashima, Y. Histological evaluation of tendon formation using a scaffold-free three-dimensional-bioprinted construct of human dermal fibroblasts under in vitro static tensile culture. Regen. Ther. 2019, 11, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Alfredson, H.; Ljung, B.O.; Thorsen, K.; Lorentzon, R. In vivo investigation of ECRB tendons with microdialysis technique--no signs of inflammation but high amounts of glutamate in tennis elbow. Acta Orthop. Scand. 2000, 71, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Croteau, F.; Robbins, S.M.; Pearsall, D. Hand-Held Shoulder Strength Measures Correlate With Isokinetic Dynamometry in Elite Water Polo Players. J. Sport Rehabil. 2021, 30, 1233–1236. [Google Scholar] [CrossRef] [PubMed]
- Boudreau, N.; Gaudreault, N.; Roy, J.S.; Bédard, S.; Balg, F. The addition of glenohumeral adductor coactivation to a rotator Cuff exercise program for rotator Cuff tendinopathy: A single-blind randomized controlled trial. J. Orthop. Sports Phys. Ther. 2019, 49, 126–135. [Google Scholar] [CrossRef] [PubMed]
- Cook, J.L.; Khan, K.M.; Maffulli, N.; Purdam, C. Overuse tendinosis, not tendinitis part 2: applying the new approach to patellar tendinopathy. Phys. Sportsmed. 2000, 28, 31–46. [Google Scholar] [CrossRef]
- Maenhout, A.G.; Mahieu, N.N.; De Muynck, M.; De Wilde, L.F.; Cools, A.M. Does adding heavy load eccentric training to rehabilitation of patients with unilateral subacromial impingement result in better outcome? A randomized, clinical trial. Knee Surg Sport. Traumatol Arthrosc 2013, 21, 1158–1167. [Google Scholar] [CrossRef]
Figure 1.
PE application in supraspinatus tendon.

Figure 2.
PNS application to suprascapular nerve.
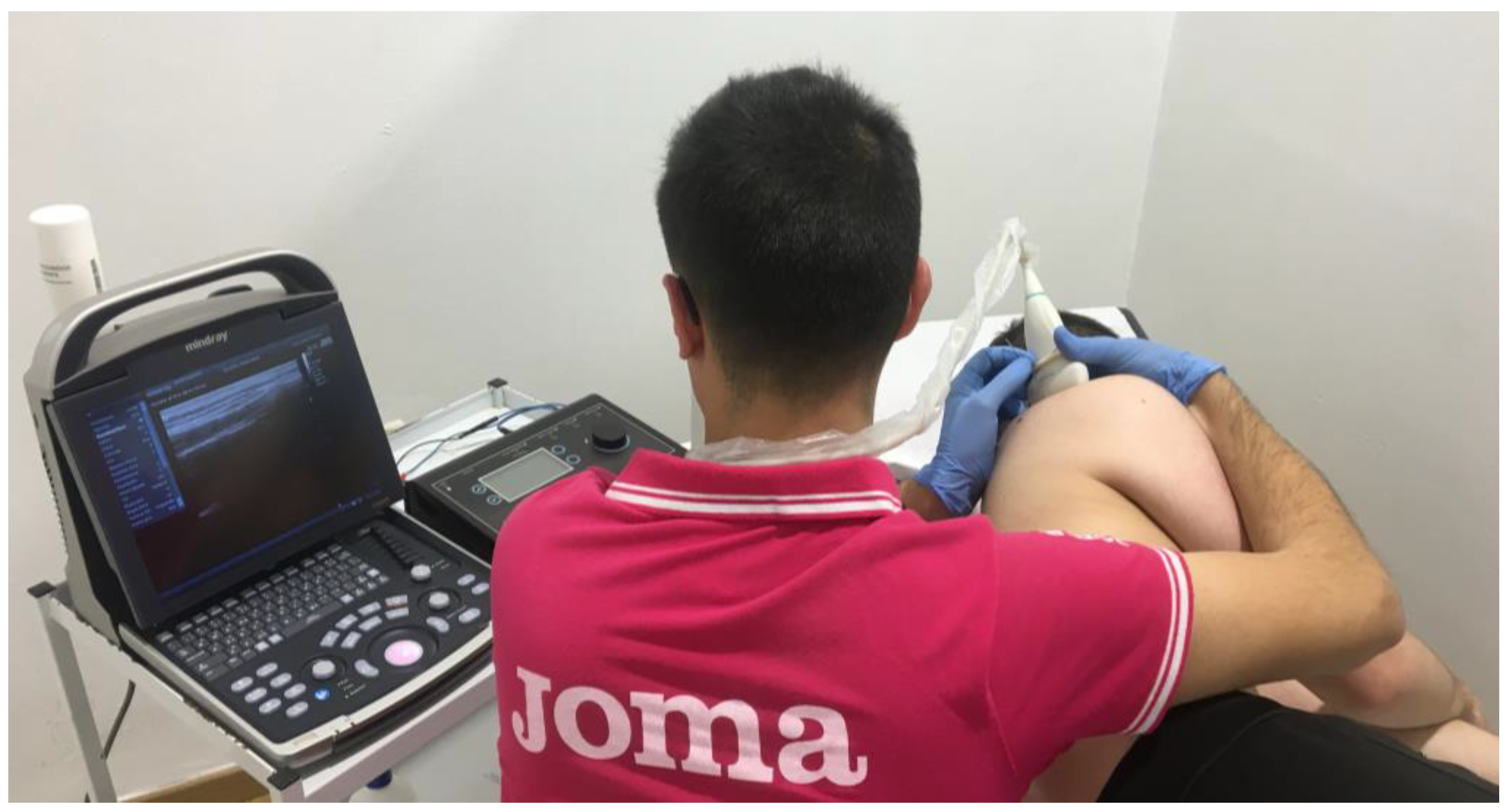
Figure 3.
EE protocol.

Figure 4.
CONSORT Flow diagram.
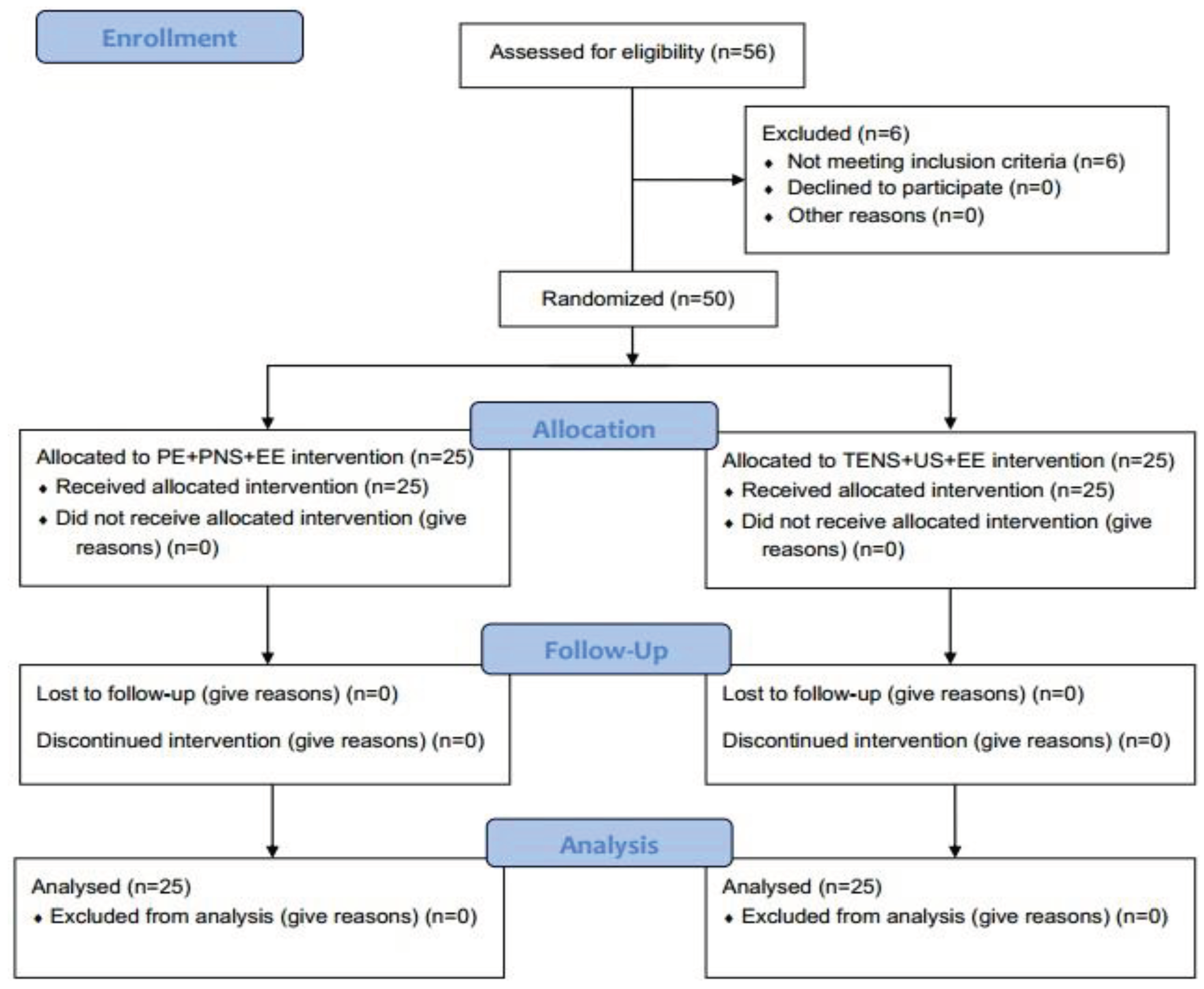

Table 1.
Morphological and clinical characteristics of the sample.
| ALL (50) | PE+PNS+EE (16) | TENS+US+EE (16) | ||||||
|---|---|---|---|---|---|---|---|---|
| CATEGORICAL | Frequency | % | Frequency | % | Frequency | % | p | |
| Sex | Male | 36 | 72.0 | 19 | 76.0 | 17 | 68.0 | 0.529 |
| Female | 14 | 28.0 | 6 | 24.0 | 8 | 32.0 | ||
| Hipo-echogenicity | Yes | 43 | 86.0 | 22 | 88.0 | 21 | 84.0 | 0.684 |
| No | 7 | 14.0 | 3 | 12.0 | 4 | 16.0 | ||
| Thickness | Yes | 47 | 94.0 | 24 | 96.0 | 23 | 92.0 | 0.552 |
| No | 3 | 6.0 | 1 | 4.0 | 2 | 8.0 | ||
| Hypervascularization | Yes | 47 | 94.0 | 23 | 92.0 | 24 | 96.0 | 0.552 |
| No | 3 | 6.0 | 2 | 8.0 | 1 | 4.0 | ||
| Affected side | Right | 34 | 68.0 | 16 | 64.0 | 18 | 72.0 | 0.544 |
| Left | 16 | 32.0 | 9 | 36.0 | 7 | 28.0 | ||
| Dominant hand | Right | 47 | 94.0 | 24 | 96.0 | 23 | 92.0 | 0.552 |
| Left | 3 | 6.0 | 1 | 4.0 | 2 | 8.0 | ||
| CONTINUOUS | Mean | SD | Mean | SD | Mean | SD | p | |
| Age | 44.24 | 11.80 | 44.36 | 13.36 | 44.12 | 10.29 | 0.944 | |
| Weight | 82.08 | 11.44 | 83.88 | 7.50 | 80.28 | 14.28 | 0.270 | |
| Height | 1.74 | 0.07 | 1.74 | 0.07 | 1.74 | 0.07 | 0.752 | |
| BMI | 27.17 | 4.10 | 27.66 | 2.81 | 26.68 | 5.09 | 0.402 | |
| NPRS | 7.24 | 1.36 | 7.56 | 1.26 | 6.92 | 1.41 | 0.097 | |
| DASH | 54.50 | 19.40 | 62.16 | 15.86 | 46.84 | 19.86 | 0.004 | |
| % DASH | 45.42 | 16.16 | 51.80 | 13.22 | 39.03 | 16.55 | 0.004 | |
| SPADI | 69.32 | 18.75 | 71.24 | 17.50 | 67.40 | 20.09 | 0.475 | |
| % SPADI | 53.32 | 14.42 | 54.80 | 13.46 | 51.85 | 15.46 | 0.475 | |
| Abduction strength | 8.45 | 1.42 | 8.56 | 1.74 | 8.34 | 1.03 | 0.590 | |
| Internal rotation strength | 8.55 | 1.42 | 8.70 | 1.68 | 8.41 | 1.12 | 0.480 | |
| External rotation strength | 8.40 | 1.39 | 8.42 | 1.54 | 8.38 | 1.26 | 0.920 | |
| Supraspinatus EMS | 168.31 | 89.32 | 162.73 | 104.37 | 173.88 | 73.01 | 0.663 | |
| Upper trapezius EMS | 391.98 | 165.12 | 400.94 | 173.91 | 383.02 | 158.92 | 0.705 | |
Abbreviatures. %: Percentage; p: p-value; BMI: Body Mass Index; DASH: Disabilities of the Arm, Shoulder and Hand; EE: Eccentric exercise; EMS: Surface Electromyography; NPRS: Numerical Pain Rate Scale; PE: Percutaneous Electrolysis; PNS: Percutaneous peripheral Nerve Stimulation; SD: Standard Deviation; SPADI: Shoulder Pain and Disability Index; TENS: Transcutaneous Electrical Nerve Stimulation; US: Therapeutic Ultrasound.
Table 2.
Frequencies and percentages of categorical variables at post-treatment, 12 weeks follow-up and 24 weeks follow-up.
Table 2.
Frequencies and percentages of categorical variables at post-treatment, 12 weeks follow-up and 24 weeks follow-up.
| VARIABLE | Post-treatment | 12 weeks follow-up | 24 weeks follow-up | |||||
|---|---|---|---|---|---|---|---|---|
| Frequency | % | Frequency | % | Frequency | % | |||
| Hipo-echogenicity | PE+PNS+EE | Yes | 20 | 80.0 | 16 | 64.0 | 9 | 36.0 |
| No | 5 | 20.0 | 9 | 36.0 | 16 | 64.0 | ||
| TENS+US+EE | Yes | 23 | 92.0 | 22 | 88.0 | 19 | 76.0 | |
| No | 2 | 8.0 | 3 | 12.0 | 6 | 24.0 | ||
| Thickness | PE+PNS+EE | Yes | 19 | 76.0 | 9 | 36.0 | 3 | 12.0 |
| No | 6 | 24.0 | 16 | 64.0 | 22 | 88.0 | ||
| TENS+US+EE | No | 23 | 92.0 | 21 | 84.0 | 16 | 64.0 | |
| No | 2 | 8.0 | 4 | 16.0 | 9 | 36.0 | ||
| Hypervascularization | PE+PNS+EE | Yes | 13 | 52.0 | 8 | 32.0 | 2 | 8.0 |
| No | 12 | 48.0 | 17 | 68.0 | 23 | 92.0 | ||
| TENS+US+EE | Yes | 23 | 92.0 | 20 | 80.0 | 14 | 56.0 | |
| No | 2 | 8.0 | 5 | 20.0 | 11 | 44.0 | ||
Abbreviatures. %: Percentage; p: p-value; EE: Eccentric exercise; PE: Percutaneous Electrolysis; PNS: Percutaneous peripheral Nerve Stimulation; TENS: Transcutaneous Electrical Nerve Stimulation; US: Therapeutic Ultrasound.
Table 3.
Statistical significance, effect size and power of time-by-group interaction form the analysis of variance.
Table 3.
Statistical significance, effect size and power of time-by-group interaction form the analysis of variance.
| VARIABLE | F | p | η2 | POTENCIA |
|---|---|---|---|---|
| NPRS | 17.684** | 0.000 | 0.536 | 1.000 |
| DASH | 22.962** | 0.000 | 0.600 | 1.000 |
| % DASH | 22.962** | 0.000 | 0.600 | 1.000 |
| SPADI | 21.328** | 0.000 | 0.582 | 1.000 |
| % SPADI | 21.328** | 0.000 | 0.582 | 1.000 |
| Abduction strength | 6.086* | 0.001 | 0.284 | 0.945 |
| Internal rotation strength | 3.754* | 0.017 | 0.197 | 0.777 |
| External rotation strength | 8.340** | 0.000 | 0.352 | 0.988 |
| Supraspinatus EMS | 17.443** | 0.000 | 0.532 | 1.000 |
| Upper trapezius EMS | 5.703* | 0.002 | 0.271 | 0.929 |
Abbreviatures. η2: Eta-squared; p: p-value; DASH: Disabilities of the Arm, Shoulder and Hand; EMS: Surface Electromyography; SPADI: Shoulder Pain and Disability Index. *: p < 0.05 **: p < 0.001.
Table 4.
Within-groups and between-groups differences in post-treatment, 12 weeks follow-up and 24 weeks follow-up.
Table 4.
Within-groups and between-groups differences in post-treatment, 12 weeks follow-up and 24 weeks follow-up.
| Post-treatment | 12 weeks follow-up | 24 weeks follow-up | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| VARIABLE | Within-Group Change Score |
Between-Groups Change Score | Effect Size |
Within-Group Change Score | Between-Groups Change Score | Effect Size | Within-Group Change Score | Between-Groups Change Score | Effect Size | |||||||
| Mean dif. |
p | Mean dif. |
p | d | Mean dif. |
p | Mean dif. |
p | d | Mean dif. |
p | Mean dif. |
p | d | ||
| NPRS | PE+PNS+EE | -5.48 | 0.000** | -2.96 | 0.000** | 1.527 | -6.22 | 0.000** | -2.74 | 0.000** | -1.39 | -6.60 | 0.000** | -3.08 | 0.000** | -1.857 |
| TENS+US+EE | -2.52 | 0.000** | -3.48 | 0.000** | -3.52 | 0.000** | ||||||||||
| DASH | PE+PNS+EE | -48.16 | 0.000** | -33.16 | 0.000** | 2.117 | -55.12 | 0.000** | -36.56 | 0.000** | -2.358 | -57.20 | 0.000** | -37.44 | 0.000** | -2.374 |
| TENS+US+EE | -15.00 | 0.000** | -18.56 | 0.000** | -19.76 | 0.000** | ||||||||||
| % DASH | PE+PNS+EE | -40.13 | 0.000** | -27.63 | 0.000** | 2.116 | -45.93 | 0.000** | -30.47 | 0.000** | -2.357 | -47.67 | 0.000** | -31.20 | 0.000** | -2.348 |
| TENS+US+EE | -12.50 | 0.000** | -15.47 | 0.000** | -16.47 | 0.000** | ||||||||||
| SPADI | PE+PNS+EE | -52.84 | 0.000** | -30.96 | 0.000** | 2.016 | -61.04 | 0.000** | -33.64 | 0.000** | -2.02 | -63.96 | 0.000** | -35.36 | 0.000** | -2.133 |
| TENS+US+EE | -21.88 | 0.000** | -27.40 | 0.000** | -28.60 | 0.000** | ||||||||||
| % SPADI | PE+PNS+EE | 40.65 | 0.000** | -23.82 | 0.000** | 2.016 | -46.95 | 0.000** | -25.88 | 0.000** | -2.02 | -49.20 | 0.000** | -27.20 | 0.000** | -2.132 |
| TENS+US+EE | 16.83 | 0.000** | -21.08 | 0.000** | -22.00 | 0.000** | ||||||||||
| Abduction strength | PE+PNS+EE | 1.42 | 0.000** | 0.74 | 0.000** | 1.132 | 1.81 | 0.000** | 0.83 | 0.000** | 1.169 | 2.18 | 0.000** | 1.10 | 0.000** | 1.178 |
| TENS+US+EE | 0.68 | 0.000** | 0.98 | 0.000** | 1.09 | 0.000** | ||||||||||
| Internal rotation strength | PE+PNS+EE | 1.10 | 0.000** | 0.32 | 0.030* | 0.637 | 1.60 | 0.000** | 0.56 | 0.002** | 0.911 | 1.82 | 0.000** | 0.66 | 0.004** | 0.868 |
| TENS+US+EE | 0.78 | 0.000** | 1.04 | 0.000** | 1.16 | 0.000** | ||||||||||
| External rotation strength | PE+PNS+EE | 1.40 | 0.000** | 0.58 | 0.000** | 1.065 | 1.87 | 0.000** | 0.81 | 0.000** | 1.193 | 2.22 | 0.000** | 1.02 | 0.000** | 1.408 |
| TENS+US+EE | 0.82 | 0.000** | 1.06 | 0.000** | 1.20 | 0.000** | ||||||||||
| Supraspinatus EMS | PE+PNS+EE | 85.36 | 0.000** | 67.82 | 0.000** | 1.890 | 127.57 | 0.000** | 96.16 | 0.000** | 1.958 | 155.67 | 0.000** | 122.21 | 0.000** | 1.881 |
| TENS+US+EE | 17.54 | 0.000** | 31.40 | 0.000** | 33.46 | 0.000** | ||||||||||
| Upper trapezius EMS |
PE+PNS+EE | -136.96 | 0.000** | -71.05 | 0.016* | 0.710 | -167.15 | 0.000** | -95.92 | 0.003** | -0.883 | 155.67 | 0.000** | -78.50 | 0.015* | -1.719 |
| TENS+US+EE | -65.91 | 0.000** | -71.23 | 0.000** | -88.81 | 0.000** | ||||||||||
Abbreviatures. d: Cohen´s d; p: p-value; DASH: Disabilities of the Arm, Shoulder and Hand; EE: Eccentric exercise; EMS: Surface Electromyography; Mean dif.: Mean difference; NPRS: Numerical Pain Rate Scale; PE: Percutaneous Electrolysis; PNS: Percutaneous peripheral Nerve Stimulation; SPADI: Shoulder Pain and Disability Index; TENS: Transcutaneous Electrical Nerve Stimulation; US: Therapeutic Ultrasound. *: p-value < 0.05. **: p-value < 0.01.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



