
Submitted:
06 March 2024
Posted:
07 March 2024
You are already at the latest version
Abstract
Fetal growth restriction (FGR) is a major concern in perinatal care. Various medications have been proposed as potential treatments for this serious condition. Nonetheless, there is still no definitive treatment. We studied tadalafil, a phosphodiesterase-5 inhibitor, as a therapeutic agent for FGR in clinical studies and animal experiments. In this review, we summarize our preclinical and clinical data on the use of tadalafil for FGR. Our studies in mouse models indicated that tadalafil improved FGR and hypertensive disorders of pregnancy. In addition, tadalafil protected cerebral nerve development in FGR offspring. The clinical trials we have conducted to date, including a case–control study, a phase I trial, and a phase II trial, have indicated the efficacy of tadalafil in prolonging pregnancy, as well as a good safety profile for fetuses and neonates. The number of fetal, neonatal, and infant deaths was significantly lower in those receiving tadalafil treatment group than that in controls, and no severe adverse maternal events associated with tadalafil were observed. Although further studies are needed to establish the usefulness of tadalafil in FGR treatment, our research indicates that the use of tadalafil in FGR treatment may be a paradigm shift in perinatal care.
Keywords:
Phosphodiesterase 5 inhibitor
; Tadalafil
; Fetal growth restriction
1. Introduction
Fetal growth restriction (FGR) is associated with perinatal mortality and morbidity [1,2,3,4] and can cause neurological sequelae in infants, such as cerebral palsy and pervasive developmental disorders [5,6]. Intrauterine hypoxia and malnutrition during fetal development may lead to cardiovascular disease and diabetes mellitus [7]. Furthermore, survival rates for babies born with severe FGR are low depending on the gestational age and severity [8,9], and the only way to manage this condition successfully is to deliver the fetus at the appropriate time.
Placental insufficiency is one of the causes of FGR. The placenta requires increased access to the maternal blood supply for fetal growth, which is achieved through extensive remodeling of the maternal spiral arteries, delivering blood directly into the placental intervillous space. Remodeling depends on the extravillous cytotrophoblasts, which invade the lining of the pregnant uterus at 18 weeks of gestation. In conditions of FGR, trophoblast invasion is inhibited, arteries are poorly remodeled, and the uteroplacental circulation capacity is extremely low [10]. As a result, fetal growth is suppressed. In cases of FGR associated with placental insufficiency, perinatologists have no definitive treatment options. The only strategy is to determine the optimal delivery time for the fetus.
Recently, phosphodiesterase 5 (PDE5) inhibitors have been investigated as promising medications for the treatment of FGR associated with placental insufficiency [11]. We studied tadalafil, a PDE5 inhibitor with a long half-life and high selectivity for PDE5, as a treatment option for FGR.
In this review, we summarize the results of our clinical and basic research on the use of tadalafil for the treatment of FGR.
2. Why Did We Select to Study Tadalafil as an Agent for the Treatment of FGR?
2.1. PDE5 Inhibitors
Inhibition of the enzymatic activity of PDE5 prevents inactivation of the intracellular second messenger cyclic guanosine monophosphate (cGMP) within vascular smooth muscle cells, which potentiates the activity of nitric oxide, leading to vasodilatation and increased blood flow. Since PDE5 inhibitors are also said to have anti-inflammatory effects [12,13,14], and inflammation in the placenta is known to be a factor in the occurrence of placental insufficiency, the PDE5 inhibitor could be effective for placental insufficiency, including FGR [15].
2.2. Sildenafil
Sildenafil is a PDE5 inhibitor that was first used in 1989 for erectile dysfunction [16]. Research on sildenafil citrate for the treatment of FGR has been ongoing, and the vasodilatory and vascular endothelial-improving effects of sildenafil have been established in several studies [17,18,19,20,21,22]. Zoma et al. reported improved uterine blood flow via cGMP-mediated endothelial relaxation of ovine uterine vessels in 2004, providing evidence suggesting its efficacy in improving fetoplacental perfusion in FGR [23]. Evidence from ex-vivo and animal models of FGR indicate that sildenafil citrate increases birth weight and improves the uteroplacental blood flow [24,25,26].
In an ex-vivo study using human specimens, Maharaj et al. demonstrated that sildenafil citrate acts as a vasodilator in human chorionic plate arteries [27]. In addition, it reportedly improves uterine blood flow via cGMP-mediated endothelial relaxation of uterine vessels and causes relaxation of the human myometrium [23,28,29].
Several clinical studies have been conducted to treat FGR and pre-eclampsia (PE). Lin et al. reported that administering sildenafil citrate decreased the uterine pulsatility index and notching in FGR [30]. A randomized controlled trial reported the safe use of sildenafil during pregnancy and increased birth weights of neonates [31]. Additionally, it was reported that sildenafil was associated with increased fetal abdominal circumference growth velocity in severe early-onset FGR [32]. Based on the findings from these small clinical studies, the Sildenafil TheRapy in Dismal prognosis Early-onset intrauterine growth Restriction (STRIDER) consortium was launched. The study group evaluated sildenafil for the treatment of FGR with a prospective Individual Participant Data (IPD) and aggregate data systematic review with meta-analysis and trial sequential analysis [33,34,35,36,37,38,39]. The STRIDER consortium including the United Kingdom (UK), the Netherlands, New Zealand/Australia, and Canada had conducted randomized controlled trials examining the effects of sildenafil for the treatment of FGR [33]. Although these results were first reported in the UK, the primary outcome, the time from randomization to delivery, was not prolonged by sildenafil treatment for FGR [34]. Furthermore, in a randomized control trial (RCT) performed in New Zealand and Australia, the fetal growth velocity as a primary outcome was not increased by sildenafil [35]. The Dutch STRIDER group reported an increased risk of neonatal persistent pulmonary hypertension (PPHN) due to maternal sildenafil administration, which generated global media interest [36]. Based on the above, the benefits of sildenafil for the treatment of FGR is considered negative, and even harmful [11,40]. Subsequent data from neonates born to the Dutch STRIDER participants have been evaluated for causes of PPHN [39]. In that study, the authors speculated that sildenafil may have had a “rebound effect” on neonates due to sudden withdrawal of the drug at birth. Generally, sildenafil lowers blood pressure without directly affecting heart rate, but the analysis showed increased blood pressure in neonates. A similar phenomenon has been reported in human adults diagnosed with PPHN [41], classified as a “Type E” adverse drug reaction [42].
2.3. The Characteristics of Tadalafil
Tadalafil is a PDE5 inhibitor that acts as a vasodilator through the NO-cGMP pathway and is prescribed for erectile dysfunction and PPHN [43,44]. Tadalafil reportedly improves vascular endothelial dysfunction and suppresses inflammation [45]. It is widely known that placental inflammation and endothelial dysfunction trigger PE; therefore, we can hypothesize that tadalafil would be effective against placental insufficiency [46,47]. Figure 1 summarizes the expected hypothetical properties of tadalafil.
Tadalafil is a PDE5 inhibitor with several promising features: (1) it has a longer half-life and shows a more rapid onset of action than does sildenafil [48]; (2) food intake has negligible effects on its bioavailability [49], and (3) it is particularly selective for the PDE5 enzyme and shows fewer side effects than sildenafil [50,51]. Tadalafil was administered to vasodilate the pulmonary artery and improve pulmonary arterial hypertension (PAH). Eleven PDE isoforms (1–11) are found throughout the body. PDE5 is mainly expressed in the lungs and reproductive organs, including the placenta. A study on sheep reported that PDE5 is particularly highly expressed in the uterine artery during pregnancy and in the placenta and myometrium [52]. Therefore, it seems logical to attempt to improve fetoplacental circulation in cases of FGR using tadalafil, which is highly selective for PDE5. In our recent research, we demonstrated enhanced uterine blood flow with the use of tadalafil [53].
Our research on the use of tadalafil for the treatment of FGR was based on clinical experience. Women with severe PAH show high rates of small-for-gestational-age infants (SGA) [54]. However, it has been reported that when these women are treated with tadalafil, their infants were no longer SGA and were appropriate for gestational age [55].
The placental transport of tadalafil differs from that of sildenafil. Walton et al. [56] reported that sildenafil dilated the fetoplacental arteries and reduced fetal arterial pressure, whereas tadalafil had no effect on the fetus. One possible reason for this is that tadalafil does not cross the human placental barrier nor has active metabolites. In our study, using an L-NAME-induced mouse model, tadalafil dilated the maternal placental blood sinuses, while no fetal capillary dilation was observed [57], which is believed to be due to the low placental transportability of tadalafil. From a pharmacological perspective, Nishimura et al. reported that in pregnant mice, fetal transfer of tadalafil is limited due in part to a difference in the contribution of breast cancer resistance protein (BCRP) to fetus-to-mother transport across the placenta [58]. These results also indicate that tadalafil might act less on the fetal side.
Our previous report suggested that tadalafil restored the levels of HIF-2, phospho-rps6, and eIF-4E in the placenta of FGR, which act downstream of the mammalian target of rapamycin (mTOR) signaling that regulates oxygen and nutrition [59]. mTOR signaling is important for the growth of fetal organs. Therefore, tadalafil may treat FGR by improving oxygenation and nutrition rather than by directly increasing blood flow of the fetus. Tadalafil has the potential to improve FGR not through direct effects on the fetus, but through improvements in feto-placental perfusion and nutritional exchange at the placental barrier.
2.4. Case Report
This case study was initiated in 2014 after obtaining permission from the Institutional Review Board [60]. Our first experience treating FGR with tadalafil was that of a 41-year-old primigravida Japanese woman who became pregnant after in vitro fertilization pre-embryo transfer. At 22 weeks and 4 days of gestation, the estimated fetal weight (EFW) was 309 g [–2.6 standard deviation [SD]), and severe oligohydramnios was observed. After informed consent for this treatment was obtained from the patient and her husband, she was administered a 20 mg/day tablet of tadalafil. The fetal bladder started to dilate 4 days after starting tadalafil and the volume of amniotic fluid increased at 10 days. The weight of the fetus increased by approximately 50–100 g per week. The patient did not experience adverse events. Because the amount of amniotic fluid had decreased and the fetal heart rate monitoring showed many variable decelerations at 32 weeks of gestation, we performed a cesarean section. A 1024 g baby was delivered with Apgar scores of 5 and 7 at 1 and 5 min after birth, respectively. At 5 years of age, the baby boy had no neurodevelopmental abnormalities, and his height and weight reached the reference range.
2.5. Case-Control Study
We also conducted a case–control study to assess maternal and perinatal outcomes of tadalafil treatment in pregnant women with FGR [61]. Eleven pregnant women treated with tadalafil with FGR were compared with 14 pregnant women matched for maternal age, parity, gestational age, and estimated fetal weight at enrollment and treated with conventional treatment according to the existing guidelines for obstetric practice in Japan [62]. The fetal growth velocity (FGV) from enrollment to delivery was significantly higher in the tadalafil group (median: 17.7 g/day; interquartile range (IQR): 10.6–23.0 g/day) than in the conventional management group (median: 12.8 g/day; IQR: 0–17.2 g/day). Based on these results, we considered FGV to be the most important outcome and decided to use it as the primary outcome in subsequent clinical trials.
2.6. Phase I Trial
A phase I trial was conducted to investigate the safety of tadalafil administration to the mother for FGR [63]. According to the case cohort method, the dose was started at 10 mg/day and sequentially increased to 20 and 40 mg/day while evaluating the onset of adverse events. Adverse events were evaluated according to the National Cancer Institute Common Terminology Criteria for Adverse Events [64]. No serious adverse events were causally related to maternal administration of tadalafil. The only fatal adverse event was intrauterine death, which was believed to be caused by velamentous insertion of the umbilical cord and was determined by the Safety Evaluation Committee to have no causal relationship with tadalafil. No adverse neonatal events related to tadalafil administration were observed.
2.7. Phase II Trial
Next, a phase II multicenter, randomized, controlled trial (TADAlafil treatment for fetuses with early onset growth restriction: TADAFER II) was conducted at a major medical center in Japan in September 2016 [65]. This study investigated the efficacy and safety of tadalafil in the treatment of FGR using an open-label design. Singleton pregnant women with FGR, with a gestation period ranging from 22 weeks and 0 days to 33 weeks and 6 days, were randomized into two groups, and the primary outcome was FGV. One group received only conventional treatment for FGR according to the guidelines for obstetric practice in Japan [62] (conventional treatment group), and the other group received 20 mg/day of tadalafil in conjunction with conventional treatment (tadalafil treatment group).
Following the results of STRIDER UK, which reported no benefits of sildenafil in pregnancy prolongation [34], the Japan Agency for Medical Research and Development concluded that all PDE5 inhibitors were ineffective against FGR due to the results and recommended that we stop recruiting new candidates for the TADAFER II trial at the end of March 2018. Eighty-nine patients (tadalafil treatment group, 45 patients; conventional treatment group, 44 patients) who participated at that time were analyzed in this study. For safety assessment, fetal, neonatal, and infant deaths were compared between the tadalafil and conventional treatment groups. There were seven cases (four fetal deaths, one neonatal death, and two infant deaths) in the conventional treatment group and only one case (neonatal death) in the tadalafil treatment group (Figure 2).
All patients had early onset severe FGR, suggesting placental insufficiency; there were 3 cases of showing reversed end-diastolic velocity (REDV) or absent end-diastolic velocity (AEDV) in the Doppler study in the conventional group, whereas there were no cases in the tadalafil treatment group (Table 1). Two cases of REDV and AEDV improved. This finding is reasonable because tadalafil ameliorates placental dysfunction.
The rate of neonatal adverse events did not differ between the two groups, with two cases of persistent pulmonary hypertension (PPHN) occurring in each group [65]. This is an important finding in the aspect of fetal safety because PPHN has been reported worldwide in the STRIDER trial [40]. Among the adverse maternal events, headache and facial flushing were more common in the tadalafil group; however, no severe adverse events associated with tadalafil were observed. In particular, while no significant differences were found in FGV, which is the primary outcome, prolongation of pregnancy was observed in the tadalafil treatment group in early-onset FGR (Figure 3).
Additional analysis of the TADAFER II data showed that tadalafil decreased the umbilical artery pulsatility index when the EFW was less than -2.0 SD (unpublished data). This indicates that vascular resistance to blood flow in the uteroplacental and fetoplacental circulations is reduced, which was also reported on the study of sildenafil [66,67].
TADAFER II was an incomplete study; therefore, we were unable to prove the efficacy of tadalafil and further studies are required.
2.8. Basic Research
We investigated the efficacy of tadalafil in an l-NG-nitroarginine methyl ester (l-NAME)-induced mouse model of PE with FGR [57]. Pregnant C57BL/6 mice divided into two groups: a control group of dams received 0.5% carboxymethylcellulose (CMC) dissolved in drinking water (C-dams), and the L-NAME group received 1 mg/mL L-NAME dissolved in 0.5% CMC, which was further divided into the tadalafil-treated group (TL-dam) and L-NAME only group (L-dam). Blood pressure, proteinuria, and fetal weight of PE and FGR mice were improved by TL-dam compared to L-dam. In TL dams, placental maternal blood sinuses were significantly narrower than those in C dams, and the placental growth factor (PLGF) concentration was increased. Interestingly, fetal capillaries did not show a change in TL dams in contrast to dilated maternal blood sinuses, which means that tadalafil has less transportability in the placenta.
Several reports have verified the efficacy of tadalafil [68,69]. Li et al. reported that prophylactic administration of tadalafil reduced hypertension, proteinuria, FGR, and flow-mediated dilatation; balanced endothelial-relative factors; and prevented activation of inflammation in the placenta and kidney tissues in rat models with induced PE [68]. Lambert et at. reported that administering tadalafil lowered tumor necrosis factor (TNF)-α, interleukin (IL)-6, and keratinocyte-derived chemokine/growth-related oncogene (KC/GRO) levels in plasma; additionally, it reduced TNF-α expression in the placenta of halogen inhalation-induced pulmonary and systemic injuries in pregnant mice [69]. A report suggests that tadalafil suppresses inflammatory cytokines [70], which highlights its potential efficacy in treating placental insufficiency.
Subsequently, we studied the neuroprotective action of tadalafil in an L-NAME-induced mouse model [71]. The number of HIF-2α-positive cells in the white matter and dentate gyrus regions of the fetal hippocampal hippocampus was higher for the L-dams than for the C-dams but was significantly lower for the TL-dams than for the L-dams. In the labyrinth zone of the placenta, the number of HIF-2α+ cells were also significantly lower in the TL-dams than in the L-dams. The number of cells positive for glial fibrillary acid protein (GFAP) in corpus callosum was significantly lower in the offspring than in the L offspring. The area positive for myelin basic protein (MBP) in the cingulum was significantly improved in the offspring compared to that in the offspring L. Since poor neurodevelopment is a serious problem in FGR [72], this result may shed light on improving neurologic prognosis in humans.
We also investigated the efficacy of tadalafil in another mouse model of FGR: the reduced uterine perfusion pressure (RUPP) model. To establish the RUPP model, bilateral uterine and ovarian vessels were ligated with a nylon thread (0.75 mm in diameter), and the thread was immediately removed, leaving a small space [73]. In the RUPP model, elevated maternal sBP and FGR levels also improved. The sFlt-1 concentration was significantly decreased in the placenta of the RUPP group treated with tadalafil. Furthermore, tadalafil treatment improves renal pathologies such as endotheliosis and increases the mesangial area [74].
2.9. Developmental Prognosis of Children Treated with Tadalafil
We also evaluated the development prognosis of children in the long term [75]. The developmental quotient (DQ) was evaluated using the Kyoto Scale of Psychological Development (KSPD) test at 1.5 years of corrected age, of 3 years old. The median score of each area (postural–motor functions, P–M; cognitive–adaptive functions, C–A; and language–social functions, L–S) in the tadalafil treatment group exceeded 85 (normal range), and the proportion of cases that had a DQ≤70 was less than 20%, which was considered favorable. Although this study was conducted in a single institution and evaluated a single group of children treated with tadalafil, it provides valuable data for further research.
2.10. TADAFER IIb
A multicenter, placebo-controlled, randomized controlled trial (TADAFER IIb), which started in 2018, is currently ongoing [76]. Since TADAFER II was an incomplete study and had an open-label design that did not use a placebo, further trials are necessary to establish a higher level of evidence.
The study population is as follows: (1) pregnant women aged ≥20 and <45 years; (2) EFW of −1.5 SD or less of the mean EFW for gestational age (GA) according to the Japanese standard curve [77]; (3) GA between 20+0 and 31+6 weeks; (4) expected date of confinement determined using the criteria of the guidelines for obstetrical practice in Japan (2017) [78]; (5) singleton pregnant women, and (6) provision of signed written informed consent from the pregnant women.
The patient will be randomly assigned to the following three arms.
Arm A: Patients will receive a placebo twice daily along with conventional treatment until delivery.
Arm B: Patients will receive 20 mg of tadalafil once per day and placebo once per day (morning: tadalafil, evening: placebo) in conjunction with conventional treatment until delivery.
Arm C: Patients will receive 20 mg of tadalafil twice daily (total 40 mg) along with conventional management until delivery.
Since the previous study (TADAFER II) was terminated midway, and the TADAFER IIb protocol includes the verification of the effects of a dose of 40 mg/day (20 mg x 2) in addition to the dose of 20 mg/day of tadalafil, this study was designated as an ‘exploratory study’ phase II. The blood concentration of tadalafil decreases over time, as the time to maximum concentration is 4 hours [79] (Figure 4). Considering that maintaining blood concentration throughout the day is necessary to maintain blood flow, we designed an arm for oral administration twice daily.
The primary endpoint was the prolongation of GA, defined as the days from the first day of protocol-defined treatment to birth, which was significantly prolonged in the tadalafil treatment group in the TADAFER II study [65]. The case registration period was originally set to end in May 2022. However, as the planned number of cases had not been achieved, it has been extended to May 2024.
3. Conclusions and Future Aspects
Tadalafil is a promising therapeutic agent for FGR that can improve placental function in terms of fetoplacental perfusion and nutritional exchange.
A systematic review of the maternal and perinatal safety and clinical outcomes of PDE5 inhibitors was published in 2022 [80]. The article reported that tadalafil was safe for pregnant women, fetuses, and neonates. Lim et al. reported the analysis of new candidates for the prevention and treatment of FGR [11]. Tadalafil is ranked as a “medium potential” drug for the treatment of FGR. Given that sildenafil has been associated with increased neonatal PPHN, caution regarding the safety of tadalafil was included in the article. The safety profile and distinctions from sildenafil have been outlined as described earlier.
In 2023, Pels et al. published a systematic review of FGR treatments via the nitric oxide pathway [81]. The review reported that interventions affecting the nitric oxide pathway do not influence fetal and neonatal mortality in pregnant women with FGR. However, there is limited data available on tadalafil, and its evidential support is classified as “low.” As mentioned earlier, tadalafil and sildenafil exhibit distinct effects, suggesting potential variations in the effectiveness of tadalafil. Additional data accumulation is required for a comprehensive understanding.
Clinical trials investigating the efficacy of tadalafil for FGR have been progressing through Phase I and Phase II trials, and, currently, a multicenter, placebo-controlled, randomized controlled trial, TADAFER Iib, is being conducted. Case registration is ongoing, and we await the results.
Author Contributions
Conceptualization, S.M. (Shintaro Maki), S.T., T.I.; methodology, S.M. (Shintaro Maki), S.T., T.I.; investigation, S.M. (Shintaro Maki), S.T., M.T., S.M. (Shoichi Magawa), Y.T., N.M., M.K., K.Y., and K.T.; writing—original draft preparation, S.M. (Shintaro Maki), S.T.; writing—review and editing, E.K., T.I.; supervision, E.K., T.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Temming, L.A.; Dicke, J.M.; Stout, M.J.; Rampersad, R.M.; Macones, G.A.; Tuuli, M.G.; Cahill, A.G. Early second-trimester fetal growth restriction and adverse perinatal outcomes. Obstet Gynecol 2017, 130, 865–869. [Google Scholar] [CrossRef]
- Lees, C.; Marlow, N.; Arabin, B.; Bilardo, C.M.; Brezinka, C.; Derks, J.B.; Duvekot, J.; Frusca, T.; Diemert, A.; Ferrazzi, E.; et al. Perinatal morbidity and mortality in early-onset fetal growth restriction: cohort outcomes of the trial of randomized umbilical and fetal flow in Europe (TRUFFLE). Ultrasound Obstet Gynecol 2013, 42, 400–408. [Google Scholar] [CrossRef]
- Levine, T.A.; Grunau, R.E.; McAuliffe, F.M.; Pinnamaneni, R.; Foran, A.; Alderdice, F.A. Early childhood neurodevelopment after intrauterine growth restriction: a systematic review. Pediatrics 2015, 135, 126–141. [Google Scholar] [CrossRef] [PubMed]
- Hui, L.; Challis, D. Diagnosis and management of fetal growth restriction: the role of fetal therapy. Best Pract Res Clin Obstet Gynaecol 2008, 22, 139–158. [Google Scholar] [CrossRef]
- Maeyama, K.; Morioka, I.; Iwatani, S.; Fukushima, S.; Kurokawa, D.; Yamana, K.; Nishida, K.; Ohyama, S.; Fujioka, K.; Awano, H.; et al. Gestational age-dependency of height and body mass index trajectories during the first 3 years in Japanese small-for-gestational age children. Sci Rep 2016, 6, 38659. [Google Scholar] [CrossRef]
- Baschat, A.A. Neurodevelopment after fetal growth restriction. Fetal Diagn Ther 2014, 36, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Gluckman, P.D.; Hanson, M.A. Living with the past: evolution, development, and patterns of disease. Science 2004, 305, 1733–1736. [Google Scholar] [CrossRef] [PubMed]
- Flenady, V.; Koopmans, L.; Middleton, P.; Frøen, J.F.; Smith, G.C.; Gibbons, K.; Coory, M.; Gordon, A.; Ellwood, D.; McIntyre, H.D.; et al. Major risk factors for stillbirth in high-income countries: a systematic review and meta-analysis. Lancet 2011, 377, 1331–1340. [Google Scholar] [CrossRef]
- Iliodromiti, S.; Mackay, D.F.; Smith, G.C.; Pell, J.P.; Sattar, N.; Lawlor, D.A.; Nelson, S.M. Customised and noncustomised birth weight centiles and prediction of stillbirth and infant mortality and morbidity: a cohort study of 979,912 term singleton pregnancies in Scotland. PLOS Med 2017, 14, e1002228. [Google Scholar] [CrossRef]
- Redman, C.W.; Sargent, I.L. Latest advances in understanding preeclampsia. Science 2005, 308, 1592–1594. [Google Scholar] [CrossRef]
- Lim, S.; McDougall, A.R.A.; Goldstein, M.; Tuttle, A.; Hastie, R.; Tong, S.; Ammerdorffer, A.; Rushwan, S.; Ricci, C.; Gülmezoglu, A.M.; et al. Analysis of a maternal health medicines pipeline database 2000–2021: new candidates for the prevention and treatment of fetal growth restriction. BJOG 2023, 130, 653–663. [Google Scholar] [CrossRef]
- Raposo, C.; Nunes, A.K.; Luna, R.L.; Araújo, S.M.; da Cruz-Höfling, M.A.; Peixoto, C.A. Sildenafil (Viagra) protective effects on neuroinflammation: the role of iNOS/NO system in an inflammatory demyelination model. Mediators Inflamm 2013, 2013, 321460. [Google Scholar] [CrossRef]
- Zhang, J.; Guo, J.; Zhao, X.; Chen, Z.; Wang, G.; Liu, A.; Wang, Q.; Zhou, W.; Xu, Y.; Wang, C. Phosphodiesterase-5 inhibitor sildenafil prevents neuroinflammation, lowers beta-amyloid levels and improves cognitive performance in APP/PS1 transgenic mice. Behav Brain Res 2013, 250, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Bogdan, S.; Seferian, A.; Totoescu, A.; Dumitrache-Rujinski, S.; Ceausu, M.; Coman, C.; Ardelean, C.M.; Dorobantu, M.; Bogdan, M. Sildenafil reduces inflammation and prevents pulmonary arterial remodeling of the monocrotaline - induced disease in the Wistar rats. Maedica (Bucur) 2012, 7, 109–116. [Google Scholar] [PubMed]
- Cheng, S.B.; Nakashima, A.; Huber, W.J.; Davis, S.; Banerjee, S.; Huang, Z.; Saito, S.; Sadovsky, Y.; Sharma, S. Pyroptosis is a critical inflammatory pathway in the placenta from early onset preeclampsia and in human trophoblasts exposed to hypoxia and endoplasmic reticulum stressors. Cell Death Dis 2019, 10, 927. [Google Scholar] [CrossRef]
- Ravipati, G.; McClung, J.A.; Aronow, W.S.; Peterson, S.J.; Frishman, W.H. Type 5 phosphodiesterase inhibitors in the treatment of erectile dysfunction and cardiovascular disease. Cardiol Rev 2007, 15, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Khaodhiar, L.; Veves, A. Acute and prolonged effects of sildenafil on brachial artery flow-mediated dilatation in type 2 diabetes. Diabetes Care 2003, 26, 962–963, author reply 963. [Google Scholar] [CrossRef]
- Halcox, J.P.; Nour, K.R.; Zalos, G.; Mincemoyer, R.A.; Waclawiw, M.; Rivera, C.E.; Willie, G.; Ellahham, S.; Quyyumi, A.A. The effect of sildenafil on human vascular function, platelet activation, and myocardial ischemia. J Am Coll Cardiol 2002, 40, 1232–1240. [Google Scholar] [CrossRef]
- Herrmann, H.C.; Chang, G.; Klugherz, B.D.; Mahoney, P.D. Hemodynamic effects of sildenafil in men with severe coronary artery disease. N Engl J Med 2000, 342, 1622–1626. [Google Scholar] [CrossRef]
- Katz, S.D.; Balidemaj, K.; Homma, S.; Wu, H.; Wang, J.; Maybaum, S. Acute type 5 phosphodiesterase inhibition with sildenafil enhances flow-mediated vasodilation in patients with chronic heart failure. J Am Coll Cardiol 2000, 36, 845–851. [Google Scholar] [CrossRef]
- Mahmud, A.; Hennessy, M.; Feely, J. Effect of sildenafil on blood pressure and arterial wave reflection in treated hypertensive men. J Hum Hypertens 2001, 15, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Schofield, R.S.; Edwards, D.G.; Schuler, B.T.; Estrada, J.; Aranda, J.M.; Pauly, D.F.; Hill, J.A.; Aggarwal, R.; Nichols, W.W. Vascular effects of sildenafil in hypertensive cardiac transplant recipients. Am J Hypertens 2003, 16, 874–877. [Google Scholar] [CrossRef] [PubMed]
- Zoma, W.D.; Baker, R.S.; Clark, K.E. Effects of combined use of sildenafil citrate (Viagra) and 17beta-estradiol on ovine coronary and uterine hemodynamics. Am J Obstet Gynecol 2004, 190, 1291–1297. [Google Scholar] [CrossRef]
- Stanley, J.L.; Andersson, I.J.; Poudel, R.; Rueda-Clausen, C.F.; Sibley, C.P.; Davidge, S.T.; Baker, P.N. Sildenafil citrate rescues fetal growth in the catechol-O-methyl transferase knockout mouse model. Hypertension 2012, 59, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Wareing, M.; Myers, J.E.; O’Hara, M.; Baker, P.N. Sildenafil citrate (Viagra) enhances vasodilatation in fetal growth restriction. J Clin Endocrinol Metab 2005, 90, 2550–2555. [Google Scholar] [CrossRef]
- Herraiz, S.; Pellicer, B.; Serra, V.; Cauli, O.; Cortijo, J.; Felipo, V.; Pellicer, A. Sildenafil citrate improves perinatal outcome in fetuses from pre-eclamptic rats. BJOG 2012, 119, 1394–1402. [Google Scholar] [CrossRef]
- Maharaj, C.H.; O’Toole, D.; Lynch, T.; Carney, J.; Jarman, J.; Higgins, B.D.; Morrison, J.J.; Laffey, J.G. Effects and mechanisms of action of sildenafil citrate in human chorionic arteries. Reprod Biol Endocrinol 2009, 7, 34. [Google Scholar] [CrossRef]
- Khan, R.N.; Hamoud, H.; Warren, A.; Wong, L.F.; Arulkumaran, S. Relaxant action of sildenafil citrate (Viagra) on human myometrium of pregnancy. Am J Obstet Gynecol 2004, 191, 315–321. [Google Scholar] [CrossRef]
- Méhats, C.; Schmitz, T.; Breuiller-Fouché, M.; Leroy, M.J.; Cabrol, D. Should phosphodiesterase 5 selective inhibitors be used for uterine relaxation? Am J Obstet Gynecol 2006, 195, 184–185. [Google Scholar] [CrossRef]
- Lin, T.H.; Su, Y.N.; Shih, J.C.; Hsu, H.C.; Lee, C.N. Resolution of high uterine artery pulsatility index and notching following sildenafil citrate treatment in a growth-restricted pregnancy. Ultrasound Obstet Gynecol 2012, 40, 609–610. [Google Scholar] [CrossRef]
- Samangaya, R.A.; Mires, G.; Shennan, A.; Skillern, L.; Howe, D.; McLeod, A.; Baker, P.N. A randomised, double-blinded, placebo-controlled study of the phosphodiesterase type 5 inhibitor sildenafil for the treatment of preeclampsia. Hypertens Pregnancy 2009, 28, 369–382. [Google Scholar] [CrossRef] [PubMed]
- von Dadelszen, P.; Dwinnell, S.; Magee, L.A.; Carleton, B.C.; Gruslin, A.; Lee, B.; Lim, K.I.; Liston, R.M.; Miller, S.P.; Rurak, D.; et al. Sildenafil citrate therapy for severe early-onset intrauterine growth restriction. BJOG 2011, 118, 624–628. [Google Scholar] [CrossRef] [PubMed]
- Ganzevoort, W.; Alfirevic, Z.; von Dadelszen, P.; Kenny, L.; Papageorghiou, A.; van Wassenaer-Leemhuis, A.; Gluud, C.; Mol, B.W.; Baker, P.N. STRIDER: sildenafil Therapy in Dismal prognosis Early-onset intrauterine growth restriction--a protocol for a systematic review with individual participant data and aggregate data meta-analysis and trial sequential analysis. Syst Rev 2014, 3, 23. [Google Scholar] [CrossRef]
- Sharp, A.; Cornforth, C.; Jackson, R.; Harrold, J.; Turner, M.A.; Kenny, L.C.; Baker, P.N.; Johnstone, E.D.; Khalil, A.; von Dadelszen, P.; et al. Maternal sildenafil for severe fetal growth restriction (STRIDER): a multicentre, randomised, placebo-controlled, double-blind trial. Lancet Child Adolesc Health 2018, 2, 93–102. [Google Scholar] [CrossRef]
- Groom, K.M.; McCowan, L.M.; Mackay, L.K.; Lee, A.C.; Gardener, G.; Unterscheider, J.; Sekar, R.; Dickinson, J.E.; Muller, P.; Reid, R.A.; et al. STRIDER NZAus: a multicentre randomised controlled trial of sildenafil therapy in early-onset fetal growth restriction. BJOG 2019, 126, 997–1006. [Google Scholar] [CrossRef]
- Pels, A.; Derks, J.; Elvan-Taspinar, A.; van Drongelen, J.; de Boer, M.; Duvekot, H.; van Laar, J.; van Eyck, J.; Al-Nasiry, S.; Sueters, M.; et al. Maternal sildenafil vs placebo in pregnant women with severe early-onset fetal growth restriction: a randomized clinical trial. JAMA Netw Open 2020, 3, e205323. [Google Scholar] [CrossRef] [PubMed]
- Sharp, A.; Jackson, R.; Cornforth, C.; Harrold, J.; Turner, M.A.; Kenny, L.; Baker, P.N.; Johnstone, E.D.; Khalil, A.; von Dadelszen, P.; et al. A prediction model for short-term neonatal outcomes in severe early-onset fetal growth restriction. Eur J Obstet Gynecol Reprod Biol 2019, 241, 109–118. [Google Scholar] [CrossRef]
- Khalil, A.; Sharp, A.; Cornforth, C.; Jackson, R.; Mousa, H.; Stock, S.; Harrold, J.; Turner, M.A.; Kenny, L.C.; Baker, P.N.; et al. Effect of sildenafil on maternal hemodynamics in pregnancies complicated by severe early-onset fetal growth restriction: planned subgroup analysis from a multicenter randomized placebo-controlled double-blind trial. Ultrasound Obstet Gynecol 2020, 55, 198–209. [Google Scholar] [CrossRef]
- Terstappen, F.; Richter, A.E.; Lely, A.T.; Hoebeek, F.E.; Elvan-Taspinar, A.; Bos, A.F.; Ganzevoort, W.; Pels, A.; Lemmers, P.M.; Kooi, E.M.W. Prenatal use of sildenafil in fetal growth restriction and its effect on neonatal tissue oxygenation-A retrospective analysis of hemodynamic data from participants of the Dutch STRIDER trial. Front Pediatr 2020, 8, 595693. [Google Scholar] [CrossRef]
- Groom, K.M.; Ganzevoort, W.; Alfirevic, Z.; Lim, K.; Papageorghiou, A.T.; STRIDER Consortium. Clinicians should stop prescribing sildenafil for fetal growth restriction (FGR): comment from the STRIDER Consortium. Ultrasound Obstet Gynecol 2018, 52, 295–296. [Google Scholar] [CrossRef]
- Keogh, A.M.; Jabbour, A.; Hayward, C.S.; Macdonald, P.S. Clinical deterioration after sildenafil cessation in patients with pulmonary hypertension. Vasc Health Risk Manag 2008, 4, 1111–1113. [Google Scholar] [CrossRef]
- Edwards, I.R.; Aronson, J.K. Adverse drug reactions: definitions, diagnosis, and management. Lancet 2000, 356, 1255–1259. [Google Scholar] [CrossRef]
- Gacci, M.; Andersson, K.E.; Chapple, C.; Maggi, M.; Mirone, V.; Oelke, M.; Porst, H.; Roehrborn, C.; Stief, C.; Giuliano, F. Latest evidence on the use of phosphodiesterase type 5 inhibitors for the treatment of lower urinary tract symptoms secondary to benign prostatic hyperplasia. Eur Urol 2016, 70, 124–133. [Google Scholar] [CrossRef]
- Galiè, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: the Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J 2016, 37, 67–119. [Google Scholar] [CrossRef]
- Aversa, A.; Fittipaldi, S.; Francomano, D.; Bimonte, V.M.; Greco, E.A.; Crescioli, C.; Di Luigi, L.; Lenzi, A.; Migliaccio, S. Tadalafil improves lean mass and endothelial function in nonobese men with mild ED/LUTS: in vivo and in vitro characterization. Endocrine 2017, 56, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Tenório, M.B.; Ferreira, R.C.; Moura, F.A.; Bueno, N.B.; de Oliveira, A.C.M.; Goulart, M.O.F. Cross-talk between oxidative stress and inflammation in preeclampsia. Oxid Med Cell Longev 2019, 2019, 8238727. [Google Scholar] [CrossRef] [PubMed]
- Lip, S.V.; Boekschoten, M.V.; Hooiveld, G.J.; van Pampus, M.G.; Scherjon, S.A.; Plösch, T.; Faas, M.M. Early-onset preeclampsia, plasma microRNAs, and endothelial cell function. Am J Obstet Gynecol 2020, 222, 497.e1–497.e12. [Google Scholar] [CrossRef] [PubMed]
- Rotella, D.P. Phosphodiesterase 5 inhibitors: current status and potential applications. Nat Rev Drug Discov 2002, 1, 674–682. [Google Scholar] [CrossRef] [PubMed]
- Forgue, S.T.; Patterson, B.E.; Bedding, A.W.; Payne, C.D.; Phillips, D.L.; Wrishko, R.E.; Mitchell, M.I. Tadalafil pharmacokinetics in healthy subjects. Br J Clin Pharmacol 2006, 61, 280–288. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. Scientific Discussion. Available online: https://www.ema.europa.eu/en/documents/scientific-discussion/viagra-epar-scientific-discussion_en.pdf (accessed on 13 October 2023).
- European Medicines Agency. Annex I: Summary of Product Characteristics: ADCIRCA. Available online: https://www.ema.europa.eu/en/documents/product-information/adcirca-epar-product-information_en.pdf (accessed on 13 October 2023).
- Coppage, K.H.; Sun, X.; Baker, R.S.; Clark, K.E. Expression of phosphodiesterase 5 in maternal and fetal sheep. Am J Obstet Gynecol 2005, 193, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Nii, M.; Enomoto, N.; Ishida, M.; Magawa, S.; Takakura, S.; Maki, S.; Tanaka, K.; Toriyabe, K.; Tanaka, H.; Kondo, E.; et al. Two-dimensional phase-contrast MRI reveals changes in uterine arterial blood flow in pregnant women administered tadalafil for fetal growth restriction. Placenta 2024, 146, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Katsuragi, S.; Yamanaka, K.; Neki, R.; Kamiya, C.; Sasaki, Y.; Osato, K.; Miyoshi, T.; Kawasaki, K.; Horiuchi, C.; Kobayashi, Y.; et al. Maternal outcome in pregnancy complicated with pulmonary arterial hypertension. Circ J 2012, 76, 2249–2254. [Google Scholar] [CrossRef] [PubMed]
- Daimon, A.; Kamiya, C.A.; Iwanaga, N.; Ikeda, T.; Nakanishi, N.; Yoshimatsu, J. Management of pulmonary vasodilator therapy in three pregnancies with pulmonary arterial hypertension. J Obstet Gynaecol Res 2017, 43, 935–938. [Google Scholar] [CrossRef] [PubMed]
- Walton, R.B.; Reed, L.C.; Estrada, S.M.; Schmiedecke, S.S.; Villazana-Kretzer, D.L.; Napolitano, P.G.; Ieronimakis, N. Evaluation of sildenafil and tadalafil for reversing constriction of fetal arteries in a human placenta perfusion model. Hypertension 2018, 72, 167–176. [Google Scholar] [CrossRef]
- Yoshikawa, K.; Umekawa, T.; Maki, S.; Kubo, M.; Nii, M.; Tanaka, K.; Tanaka, H.; Osato, K.; Kamimoto, Y.; Kondo, E.; et al. Tadalafil improves L-NG-nitroarginine methyl ester-induced preeclampsia with fetal growth restriction-like symptoms in pregnant mice. Am J Hypertens 2017, 31, 89–96. [Google Scholar] [CrossRef]
- Nishimura, T.; Ishii, M.; Tanaka, H.; Noguchi, S.; Ikeda, T.; Tomi, M. Breast cancer resistance protein limits fetal transfer of tadalafil in mice. J Pharm Sci 2024, 113, 486–492. [Google Scholar] [CrossRef]
- Tsuchiya, K.; Tanaka, K.; Tanaka, H.; Maki, S.; Enomoto, N.; Takakura, S.; Nii, M.; Toriyabe, K.; Katsuragi, S.; Ikeda, T. Tadalafil treatment ameliorates hypoxia and alters placental expression of proteins downstream of mTOR signaling in fetal growth restriction. Medicina (Kaunas) 2020, 56, 722. [Google Scholar] [CrossRef]
- Sakamoto, M.; Osato, K.; Kubo, M.; Nii, M.; Tanaka, H.; Murabayashi, N.; Umekawa, T.; Kamimoto, Y.; Ikeda, T. Early-onset fetal growth restriction treated with the long-acting phosphodiesterase-5 inhibitor tadalafil: a case report. J Med Case Rep 2016, 10, 317. [Google Scholar] [CrossRef]
- Kubo, M.; Umekawa, T.; Maekawa, Y.; Tanaka, H.; Nii, M.; Murabayashi, N.; Osato, K.; Kamimoto, Y.; Ikeda, T. Retrospective study of tadalafil for fetal growth restriction: impact on maternal and perinatal outcomes. J Obstet Gynaecol Res 2017, 43, 291–297. [Google Scholar] [CrossRef]
- Minakami, H.; Maeda, T.; Fujii, T.; Hamada, H.; Iitsuka, Y.; Itakura, A.; Itoh, H.; Iwashita, M.; Kanagawa, T.; Kanai, M.; et al. Guidelines for obstetrical practice in Japan: Japan Society of Obstetrics and Gynecology (JSOG) and Japan Association of Obstetricians and Gynecologists (JAOG) 2014 edition. J Obstet Gynaecol Res 2014, 40, 1469–1499. [Google Scholar] [CrossRef] [PubMed]
- Kubo, M.; Tanaka, H.; Maki, S.; Nii, M.; Murabayashi, N.; Osato, K.; Kamimoto, Y.; Umekawa, T.; Kondo, E.; Ikeda, T. Safety and dose-finding trial of tadalafil administered for fetal growth restriction: a phase-1 clinical study. J Obstet Gynaecol Res 2017, 43, 1159–1168. [Google Scholar] [CrossRef]
- NCI Division of Cancer Treatment and Diagnosis. Common terminology criteria for adverse events v4.0. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm#ctc_40 (accessed on 14 June 2014).
- Maki, S.; Tanaka, H.; Tsuji, M.; Furuhashi, F.; Magawa, S.; Kaneda, M.K.; Nii, M.; Tanaka, K.; Kondo, E.; Tamaru, S.; et al. Safety evaluation of tadalafil treatment for fetuses with early-onset growth restriction (TADAFER): results from the Phase II trial. J Clin Med 2019, 8, 856. [Google Scholar] [CrossRef]
- Trapani, A.; Gonçalves, L.F.; Trapani, T.F.; Vieira, S.; Pires, M.; Pires, M.M.S. Perinatal and hemodynamic evaluation of sildenafil citrate for preeclampsia treatment: a randomized controlled trial. Obstet Gynecol 2016, 128, 253–259. [Google Scholar] [CrossRef]
- Panda, S.; Das, A.; Md Nowroz, H. Sildenafil citrate in fetal growth restriction. J Reprod Infertil 2014, 15, 168–169. [Google Scholar]
- Li, Y.; Yang, N.; Wang, B.; Niu, X.; Cai, W.; Li, Y.; Li, Y.; Chen, S. Effect and mechanism of prophylactic use of tadalafil during pregnancy on l-NAME-induced preeclampsia-like rats. Placenta 2020, 99, 35–44. [Google Scholar] [CrossRef]
- Lambert, J.A.; Carlisle, M.A.; Lam, A.; Aggarwal, S.; Doran, S.; Ren, C.; Bradley, W.E.; Dell’Italia, L.; Ambalavanan, N.; Ford, D.A.; et al. Mechanisms and treatment of halogen inhalation-induced pulmonary and systemic injuries in pregnant mice. Hypertension 2017, 70, 390–400. [Google Scholar] [CrossRef] [PubMed]
- Laxmi, V.; Gupta, R.; Bhattacharya, S.K.; Ray, A.; Gulati, K. Inhibitory effects of sildenafil and tadalafil on inflammation, oxidative stress and nitrosative stress in animal model of bronchial asthma. Pharmacol Rep 2019, 71, 517–521. [Google Scholar] [CrossRef] [PubMed]
- Tachibana, R.; Umekawa, T.; Yoshikawa, K.; Owa, T.; Magawa, S.; Furuhashi, F.; Tsuji, M.; Maki, S.; Shimada, K.; Kaneda, M.K.; et al. Tadalafil treatment in mice for preeclampsia with fetal growth restriction has neuro-benefic effects in offspring through modulating prenatal hypoxic conditions. Sci Rep 2019, 9, 234. [Google Scholar] [CrossRef] [PubMed]
- Korkalainen, N.; Räsänen, J.; Kaukola, T.; Kallankari, H.; Hallman, M.; Mäkikallio, K. Fetal hemodynamics and adverse outcome in primary school-aged children with fetal growth restriction: a prospective longitudinal study. Acta Obstet Gynecol Scand 2017, 96, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Fushima, T.; Sekimoto, A.; Minato, T.; Ito, T.; Oe, Y.; Kisu, K.; Sato, E.; Funamoto, K.; Hayase, T.; Kimura, Y.; et al. Reduced uterine perfusion pressure (RUPP) model of preeclampsia in mice. PLOS ONE 2016, 11, e0155426. [Google Scholar] [CrossRef] [PubMed]
- Sekimoto, A.; Tanaka, K.; Hashizume, Y.; Sato, E.; Sato, H.; Ikeda, T.; Takahashi, N. Tadalafil alleviates preeclampsia and fetal growth restriction in RUPP model of preeclampsia in mice. Biochem Biophys Res Commun 2020, 521, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, M.; Maki, S.; Enomoto, N.; Okamoto, K.; Kitamura, A.; Magawa, S.; Takakura, S.; Nii, M.; Tanaka, K.; Yodoya, N.; et al. Fetal biometric assessment and infant developmental prognosis of the tadalafil treatment for fetal growth restriction. Medicina (Kaunas) 2023, 59, 900. [Google Scholar] [CrossRef] [PubMed]
- Maki, S.; Tanaka, H.; Takakura, S.; Nii, M.; Tanaka, K.; Ogura, T.; Kotera, M.; Nishimura, Y.; Tamaru, S.; Ushida, T.; et al. Tadalafil treatment for fetuses with early-onset growth restriction: a protocol for a multicentre, randomised, placebo-controlled, double-blind phase II trial (TADAFER IIb). BMJ (Open) 2022, 12, e054925. [Google Scholar] [CrossRef] [PubMed]
- Japan Society of Ultrasound in Medicine. Ultrasound fetal measurement standardization and Japanese standard. J Med Ultrason 2003, 30, 416–440. [Google Scholar]
- Japan Society of Obstetrics and Gynecology. Sanfujinka Shinryou Gaidorain-Sankahen 2017; Japan society of Obstetrics and Gynecology: Tokyo, Japan, 2017. (In Japanese) [Google Scholar]
- Tanaka, H.; Maki, S.; Magawa, S.; Nii, M.; Tanaka, K.; Ikemura, K.; Toriyabe, K.; Ikeda, T. Maternal blood concentration of tadalafil and uterine blood flow in pregnancy. Medicina (Kaunas) 2019, 55, 708. [Google Scholar] [CrossRef]
- Turner, J.M.; Russo, F.; Deprest, J.; Mol, B.W.; Kumar, S. Phosphodiesterase-5 inhibitors in pregnancy: systematic review and meta-analysis of maternal and perinatal safety and clinical outcomes. BJOG 2022, 129, 1817–1831. [Google Scholar] [CrossRef]
- Pels, A.; Ganzevoort, W.; Kenny, L.C.; Baker, P.N.; von Dadelszen, P.; Gluud, C.; Kariya, C.T.; Leemhuis, A.G.; Groom, K.M.; Sharp, A.N.; et al. Interventions affecting the nitric oxide pathway versus placebo or no therapy for fetal growth restriction in pregnancy. Cochrane Database Syst Rev 2023, 7, CD014498. [Google Scholar] [CrossRef]
Figure 1.
Summary of hypotheses and characteristics regarding the effects of tadalafil. FGR: fetal growth restriction, PDE5: phosphodiesterase 5.
Figure 1.
Summary of hypotheses and characteristics regarding the effects of tadalafil. FGR: fetal growth restriction, PDE5: phosphodiesterase 5.
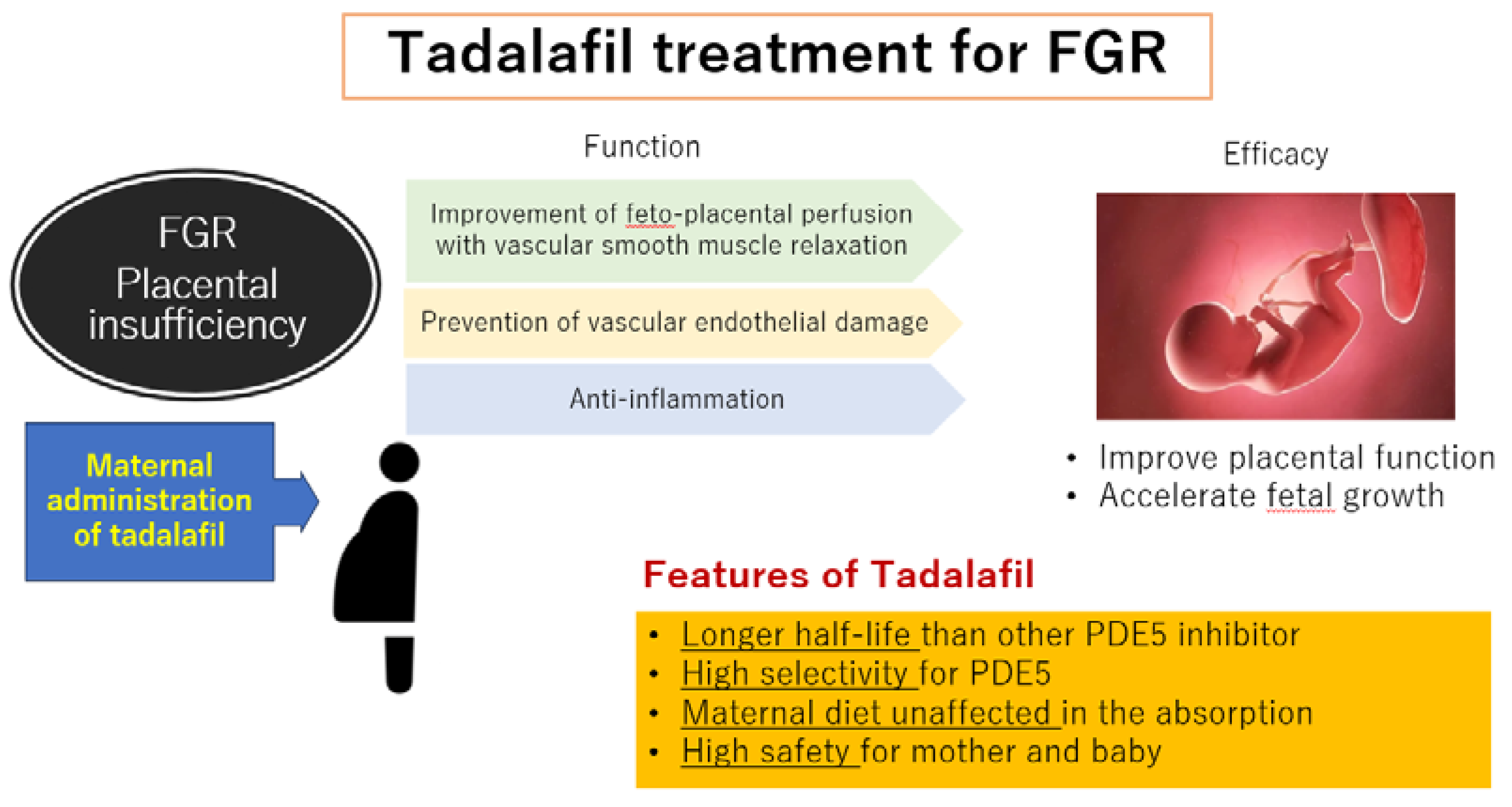
Figure 2.
Total number of fetal, neonatal, infant death cases in TADAFER II study.
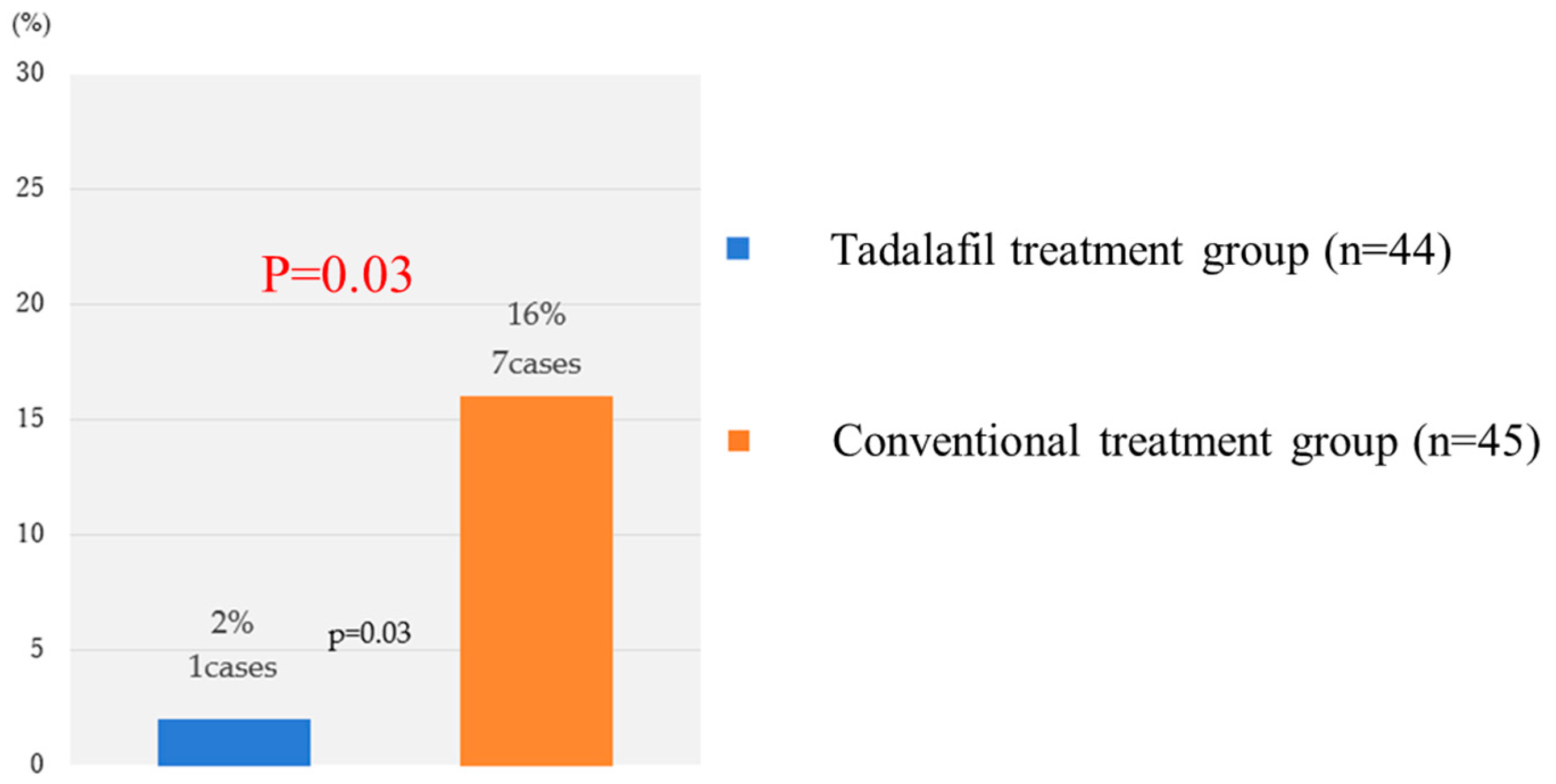
Figure 3.
Prolongation of gestational weeks. Prolongation of GA was defined as days from the first day of protocol-defined treatment to birth. The figure above shows the prolongation of GA in Kaplan–Meier curves for each GA at treatment initiation (<32 weeks, <30 weeks), comparing binary data across two groups using the generalized Wilcoxon test.
Figure 3.
Prolongation of gestational weeks. Prolongation of GA was defined as days from the first day of protocol-defined treatment to birth. The figure above shows the prolongation of GA in Kaplan–Meier curves for each GA at treatment initiation (<32 weeks, <30 weeks), comparing binary data across two groups using the generalized Wilcoxon test.
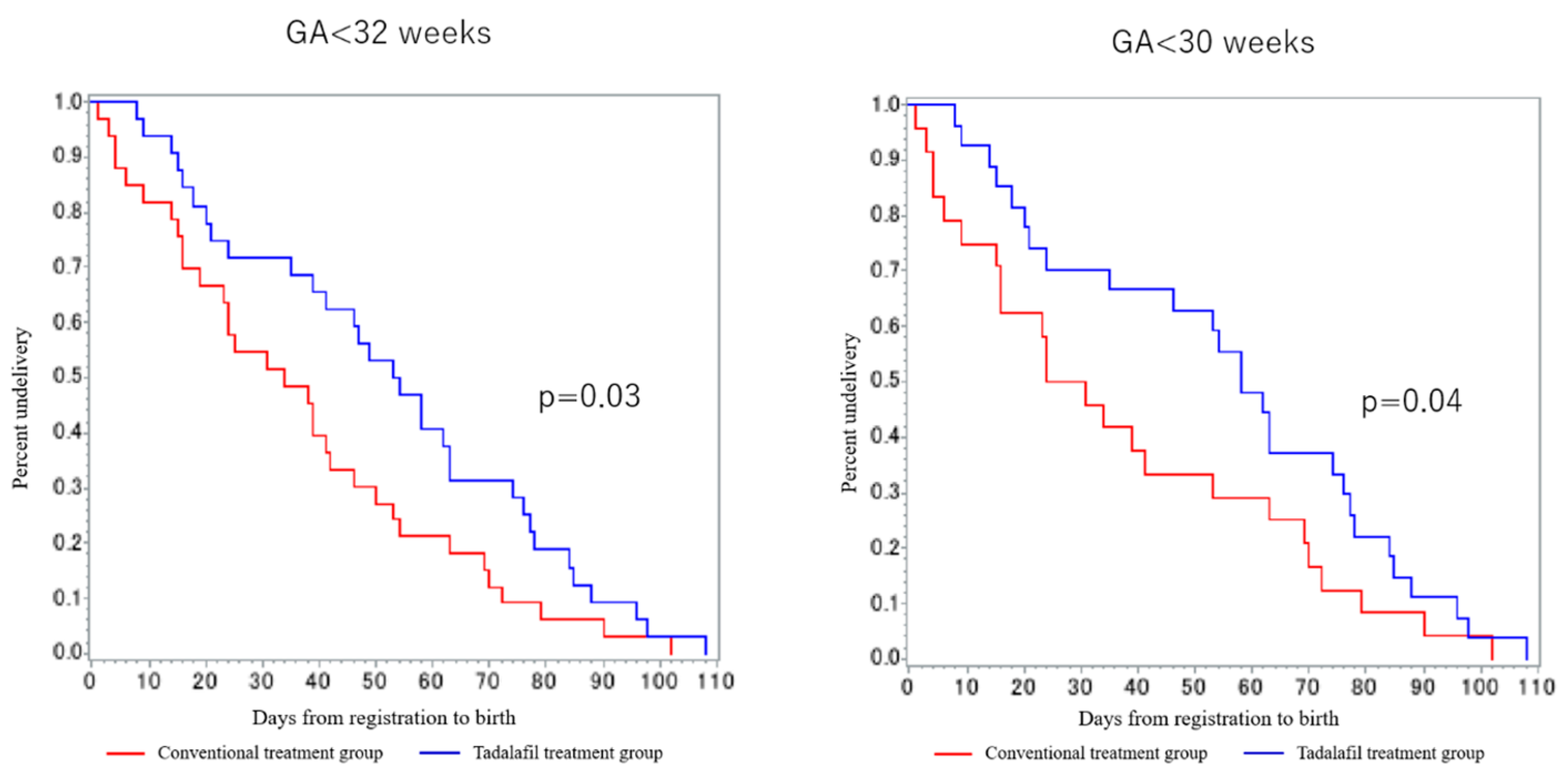
Figure 4.
Serum concentration of tadalafil in pregnancy.
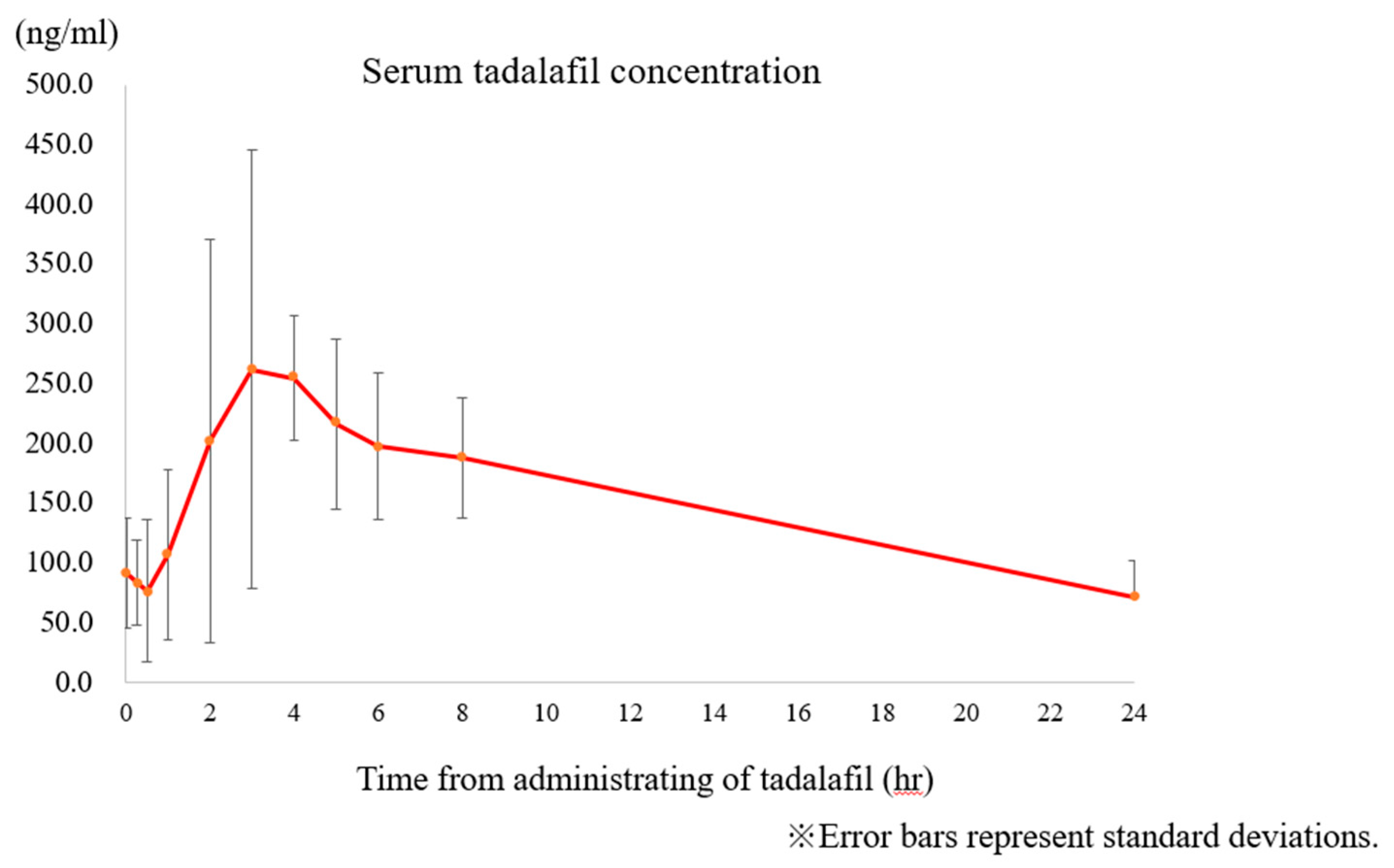

Table 1.
Details of death cases (TADAFER II).
| Case | Allocation | GW at registration (week) | BW (g) | UA REDV or AEDV | |
|---|---|---|---|---|---|
| Fetal death | Conventional treatment group | 23 | 328 | + | |
| Fetal death | Conventional treatment group | 20 | <300 | + | |
| Fetal death | Conventional treatment group | 25 | 440 | + | |
| Fetal death | Conventional treatment group | 21 | 484 | − | |
| Neonatal death | Tadalafil treatment group | 21 | 317 | − | |
| Neonatal death | Conventional treatment group | 24 | 440 | − | |
| Infant death | Conventional treatment group | 27 | 704 | − | |
| Infant death | Conventional treatment group | 28 | 730 | − |
GW: Gestational weeks. BW: Birth weight. UA: Umbilical artery. REDV: Reversed end-diastolic velocity. AEDV: Absent end-diastolic velocity.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



