
Submitted:
06 March 2024
Posted:
07 March 2024
You are already at the latest version
Abstract
Diffuse large B-cell lymphoma (DLBCL) requires a complete staging at diagnosis that may have prognostic and therapeutic implications. The role of bone marrow (BM) biopsy (BMB) is contro-versial in the era of nuclear-imaging techniques. We performed a comparative review of 25 studies focused on BM evaluation at DLBCL diagnosis, including at least two of the following techniques: BMB, flow cytometry, and positron emission tomography (PET-FDG). The report about BM involvement (BMi), diagnostic accuracy and prognostic significance was collected and compared among techniques. A concordance analysis between BMB, FCM and PET was also per-formed, and we deeply evaluated the implications of the different types of BMi: concordant by LBCL or discordant by low-grade B-cell lymphoma for both BMB and FCM, and focal or diffuse uptake pattern for PET. As main conclusion, BMB, FCM and PET are complementary tools which provide different and clinically relevant information in the assessment of BMi in newly DLBCL.
Keywords:
Bone marrow
; Large B cell lymphoma
; Lymphoma
; Histology
; Flow cytometry
; PET
1. Introduction
Diffuse large B cell lymphoma (DLBCL) is the most common lymphoma [1]. It is a biologically heterogeneous disease with an aggressive behavior that requires prompt chemoimmunotherapy administration after diagnosis. Prior to treatment initiation a complete staging assessment must be performed to evaluate the disease extension [2], which is also an important aspect necessary to calculate the patient risk, and which may be a key for designing the therapeutic approach. Thus, in most patients with localized stage a frontline approach with a reduced number of chemoimmunotherapy cycles with or without radiotherapy is enough to achieve a complete remission [3,4], and cases with advanced stage and intermediate to high-risk probably benefit for receiving Pola-R-CHP (polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, and prednisone) as first-line therapy rather than R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone) [5].
When it comes to addressing DLBCL extension, a whole-body positron emission tomography with 18-fluorodeoxiglucose along with a computerized tomography (PET-FDG/CT) is the key technique to perform the staging evaluation [2]. The examination of central nervous system by imaging (magnetic resonance) or cerebrospinal fluid analysis (flow cytometry and cytomorphological assessment) is recommended in cases considered with high-risk of neurologic invasion [6], such as those with high CNS-IPI or patients with extranodal involvement of certain sites such as testes or kidneys. In reference to bone marrow (BM) evaluation, according to the last Lugano criteria [2] a morphologic and immunohistochemical examination of the BM trephine biopsy (BMB) in patients with DLBCL is only needed when BM infiltration (BMi) is negative by positron emission tomography (PET) and the identification of occult discordant histology is clinically important.
BMi assessment can be performed by different techniques. BMB has been historically considered the gold-standard for detecting BMi in DLBCL [7] until the development of nuclear-imaging assays, but still nowadays there is a hot debate about the diagnostic accuracy and prognostic role of both techniques. BMB is an invasive procedure which may bring complications such as pain, anxiety, or bleeding [8,9]. In some cases, the BM sample obtained from the iliac crest is not sufficient for morphological assessment, and in others the BMB analysis yields a false negative result due to focal marrow infiltration in a location different from the punctured one [10]. The characterization of BMi by BMB in DLBCL includes two types of morphological invasion: concordant (BMi by LBCL) and discordant (BMi by small cell low-grade B-cell histology). PET with computed tomography (PET-CT) is a non-invasive metabolic and imaging technique which has demonstrated a high sensitivity in detecting BMi in the setting of aggressive lymphomas [11], nevertheless, some authors find it controversial avoiding BMB in most DLBCL cases as the 2014 Lugano criteria suggests [12,13,14]. When it comes to evaluating BM characterization by PET, different uptake patterns have been studied, being the focal and the diffuse ones the most widely described [15]. A focal uptake is usually defined as one or more circumscribed areas of high fluorodeoxyglucose (FDG) uptake within the skeleton or marrow space, and diffuse uptake is considered as the uniformly increased FDG uptake throughout the marrow space. In patients with DLBCL, a focal FDG uptake in the BM has been described as a pattern of tumor infiltration in most cases, however, the significance of a diffuse uptake is controversial, being related with reactive, inflammatory, or non-malignant conditions in some cases [16,17,18]. Furthermore, it has been shown that PET is less sensitive in detecting BMi by low-grade B-cell lymphoma and concordant LBCL BMi of low-quantity [19,20]. Even though, the role of some other technologies with higher methodological sensitivity rates have been evaluated in the setting of assessing BMi in DLBCL, such as flow cytometry (FCM) or molecular assays. Prior recommendations in response criteria for malignant lymphoma proposed that for routine practice clinical decision making only BMi greater than 2% by FCM or genetics should be taken into account if BMB is negative [21]. FCM assessment has been suggested to be complementary to BMB in detecting BMi at DLBCL diagnosis [22], although it is not exempt of technical difficulties for detecting concordant involment, such as hemodilution of the BM aspirate or cellular adhesion in bone trabeculae [23,24]. Nonetheless, FCM has demonstrated an important role in detecting discordant low-grade BMi in DLBCL [25,26].
When it comes to defining the prognostic significance of BMi at DLBCL diagnosis, both the technique and the infiltration pattern seem to be relevant. BMB has demonstrated being an adverse prognostic factor, even independently from International Prognostic Index (IPI), performance status, or age [27,28,29]. The concordant infiltration of the BM has clearly showed a prediction of worse prognosis when compared to the discordant BMi [30,31], but there is no agreement if the discordant pattern implies an intermediate prognosis between the concordant one and the absence of BMi [27,28,32] or if discordant cases have a similar outcome that patients without BMi [29,31,33]. The role of PET for defining prognosis in DLBCL according to BMi is controversial. Some studies suggest that BMi by PET is associated with worse outcomes [16,34], while other studies indicate that it has no prognostic relevance [35,36]. In the setting of BM evaluation by PET, it is described that the focal uptake pattern implies a worse prognosis than the diffuse pattern [16], whose outcome could be equivalent to patients with negative BMi by PET. The prognostic impact of FCM or molecular assays has scarcely been reported.
On many occasions, discrepancies between the different techniques occur when assessing BMi in DLBCL, and the the diagnostic accuracy and definition of a true positive BMi is still controversial. Furthermore, the surveillance implication of BMi is still not clear and some studies have combined and compared the results of different techniques in an attempt to solve this topic. Our aim is to perform a comparative review of the three techniques most widely performed when evaluating BMi at DLBCL diagnosis (BMB, PET, and FCM) to analyze the diagnostic accuracy, the concordance and discordance rate, and the prognostic role of each of them when compared or combined with other techniques. When appropriate and available, data about each type of result was also collected, thus, concordant or discordant BMi by BMB and FCM, and focal or diffuse pattern of BMi by PET-FDG.
2. Materials and Methods
2.1. Population:
The considered study population is patients with histological diagnosis of DLBCL with a BM assessment at diagnosis including a direct BM evaluation (BMB and/or FCM) with or without a nuclear-imaging assessment (PET-FDG), and prior to treatment initiation. Only adult patients (aged 18 or greater) and those treated in the rituximab era (mainly with R-CHOP) were considered.
2.2. Bibliographic Search Strategy and Selection:
MEDLINE and Embase were used for the study search. The search strategy was (marrow[Title] OR BM[Title]) AND (DLBCL[Title] OR LBCL[Title] OR diffuse large[Title] OR large B-cell[Title] OR large B cell[Title]) for MEDLINE and 'marrow':ti AND ('dlbcl':ti OR 'large b cell:ti' OR 'large b-cell':ti OR 'lbcl':ti) AND [embase]/lim AND [humans]/lim AND [2000-2024]/py for Embase. Other sources such as article citations were also used. The study period was from January 2000 to December 2023.
After eliminating duplicates, two authors (F.M-M. and JA.G-V.) screened the records by title and abstract, removing reports due to article type (reviews, case reports, case series, commentaries, responses and conference abstracts) or because studies did not involve human samples, full-text was not available, histologies included were different than DLBCL, or research was not focused on BMi assessment or prognosis. Then, the same authors evaluated full-text articles for their eligibility, eliminating those because of research not performed at diagnosis, small sample (less than 75 patients), pre-rituximab era, imaging or genetics-based studies, or insufficient reporting. One important point is that only articles were considered suitable for performing comparisons – and therefore to be included in this review – if at least results from two of the three chosen techniques (BMB, FCM, and PET) were reported. Articles based on magnetic resonance imaging (MRI), or genetic assays were excluded due to scarce presence of comparative studies with other techniques in literature (less than five of each of them).
2.3. Statistical Analysis:
A flow chart was created to illustrate the process of bibliographic search and articles selection. A description of each included study and their population characteristics was performed including region, study type, recruitment period, sample size (N), male/female ratio, age, cell-of-origin (COO) classification according to Hans algorithm, stage, IPI, frontline approach, and follow-up time. The BM assessment according to BMB, FCM, and/or PET was included according to the reports of each report, describing separately the type of BMi (concordant or discordant for BMB and FCM, and focal or diffuse patterns for PET) if available. A complete report was considered if information about both concordant and discordant BMi by BMB or FCM was available, and if information about both focal and diffuse BM uptake patterns by PET was available. Proportions of complete and incomplete reports among each technique were compared by chi-square test or Fisher’s test when appropriate. A complete record of the number of patients with BMi by each technique and type of infiltration was calculated to assess the proportion of involvement among the global cohort, making comparisons between techniques and infiltration patterns by chi-square test. Statistical significance was considered when p values were lower than 0.05.
An analysis of concordance and discordance between the different reported techniques was performed. Cohen’s kappa index was obtained from records or calculated if not reported to measure the statistical concordance among techniques to evaluate BMi at DLBCL diagnosis. Results were interpreted as follows: values ≤ 0 as indicating no agreement, 0.01 to 0.2 as none to slight agreement, 0.21 to 0.4 as fair, 0.41 to 0.6 as moderate, 0.61 to 0.8 as substantial, and 0.81 to 1 as almost perfect agreement.
If information about sensitivity, specificity, positive predictive value, negative predictive value, Youden’s index, or diagnostic accuracy was reported by any of the included articles it was also recorded. As the definition of a true positive BMi may change among studies, it was also described for each report.
Direct or indirect prognostic comparisons were described according to the information available from studies reporting outcome significance of BMi at DLBCL diagnosis by at least two techniques. If the prognostic evaluation was performed in a subcohort of patients of patients in each study, it was specified. Survival endpoints included progression-free survival (PFS, time from diagnosis to first disease progression or relapse) or event-free survival (EFS, time from diagnosis to first disease progression or relapse or death by any cause) as reported by each study, and overall survival (OS, time from diagnosis to death by any cause). It was described the available information about prognosis and univariate/multivariate hazard ratio analysis (Cox regression model) of each technique and/or type of BMi. The other variables studied in each reported multivariate analysis which included BM assessment were also recorded.
3. Results
3.1. Description of the Included Studies, Charancteristics of the DLBCL Populations and BM Evaluation:
A total of 369 unique citations were identified from the electronic database and other sources search. Of these, 291 records were excluded based on title and abstract screening and 53 were excluded after full-text evaluation. In the end, 25 studies were included in the comparative review (Figure 1), accounting for 4,849 newly DLBCL patients. Study characteristics are presented in Table 1. Almost all records were retrospective studies (22/25, 88%), 2/25 were prospective (8%) and 1/25 did not report the type of study (4%). All studies provided information about BMB, while 6/25 (24%) included FCM (accounting for 814 patients) and 21/25 (84%) provided PET data (accounting for 4,175 patients). Only 2/25 (8%) combined BMB, FCM and PET, 4/25 (16%) included BMB and FCM, and 19/25 (76%) reported BMB and PET. No article combining solely FCM and PET was found. PET reports were complete of BM characterization at a higher rate than BMB (71% vs 40%, p=0.033) and FCM (71% vs 17%, p=0.027) ones (Figure 2). Although proportional differences were seen in the rate of complete reports between BMB and FCM, statistical significance was not reached (40% vs 17%, p=0.38).
BM direct assessment was performed in 20/25 studies (80%) after unilateral iliac crest punction, in 4/25 (16%) it was performed bilateral, and 1/25 (4%) reported both results after unilateral and bilateral procedures; this study [37] accounted twice to calculate the rate of BMi by BMB and FCM, separating the results from unilateral and bilateral iliac crest punctions. In the global cohort, BMB detected BMi in 15% of DLBCL patients (744/4,951), with a slightly higher rate of BMi detected by bilateral punction (17.1%, 244/1,425) than by unilateral punction (14.8%, 480/3,255) (p=0.039). A concordant and discordant BMi by BMB was seen in 11.5% (238/2,062) and 4.7% (88/1,978) of patients, respectively. FCM showed BMi in 24.5% cases, a higher rate when compared with BMB (p <0.001). Only one study [47] provided sufficient information about the type of BMi by FCM, detecting a concordant involvement in 10.3% cases (24/232) and discordant in 15.1% (35/232). There was no difference between BMB and FCM in detecting a concordant invasion of the BM (p=0.59), but it was found when assessing a discordant infiltration favoring the FCM analysis (p <0.001). BM uptake by PET-FDG was globally described in 21.9% of DLBCL cases (749/4,175 included in 18 studies); a focal and diffuse pattern of BM uptake was seen in 18.1% (714/3,949 included in 18 studies) and 5.5% (174/3,191 included in 15 studies) of patients, respectively.
3.2. Concordance Analysis Among BMB, FCM and PET When Assessing BMi at DLBCL Diagnosis:
All 25 studies were suitable for concordance comparisons between assessed techniques (Table 2).
3.2.1. Concordance between BMB and FCM in the Setting of DLBCL BMi Assessment:
Five studies evaluated the concordance between BMB and FCM. The median Cohen’s kappa index of the studies was 0.65 (range 0.25-0.66), which is defined as a substantial agreement between techniques. The proportion of concordant positive (+) and negative (-) cases for both BMB/FCM ranged 3-26% and 37-83%, respectively. The most common discordant rates were seen favoring BMi by FCM, thus, BMB-/FCM+ group accounted for 7-37% of cases, while only 0-6% of cases were classified as BMB+/FCM-. Interestingly, one study [49] reported that among FCM+ patients, the percentage of pathological cells infiltrating the BM detected by FCM was higher among BMB+ cases compared with the BMB- ones (15% vs 2.1%, p < 0.001).
3.2.2. Concordance between BMB and PET in the Setting of DLBCL BMi Assessment:
Twenty-one studies evaluated the concordance between BMB and PET. The median Cohen’s kappa index of the studies was 0.36 (range 0.19-0.68), which is defined as a fair agreement between techniques. Concordant BMB+/PET+ and BMB-/PET- cases accounted for 5-21% and 50-83%, respectively. Discordant results were seen in both ways, thus in up to 17% cases BMi is detected only by BMB (BMB+/PET-) and in up to 29% only by PET (BMB-/PET+). In one study [37], the agreement among techniques changed from moderate (Cohen’s kappa index 0.59) to substantial (Cohen’s kappa index 0.8) after performing a second BMB in cases BMB-/PET+. Another study [10] showed that the agreement raised from none-slight (Cohen’s kappa index 0.19) to fair (Cohen’s kappa index 0.23) when considering only PET+ cases with focal uptake pattern. As described in different studies, a cause of BMB-/PET+ discrepancy is due to focal involvement far from iliac crest location [10], in fact, the focal pattern is described as the most common in BMB-/PET+ cases [35,36]. In contrast, there is no agreement among articles in defining the most common uptake pattern in BMB+/PET+ cases, being mainly focal in some studies [20], while diffuse in others [36]. When it comes to define de type of infiltration by BMB, different studies agree that the concordant involvement is mostly found in BMB+/PET+ cases, while patients from the BMB+/PET- group usually have a discordant invasion or a low-quantity concordant one [20,33,36]. One study [38] suggests higher rates of BMB/PET discrepancies among elderly patients and those with high grade B cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements.
3.2.3. Concordance between FCM and PET in the Setting of DLBCL BMi Assessment:
Only two studies evaluated the concordance between FCM and PET. As described in the BMB/PET analysis, in one study [37] the agreement among FCM and PET rose from moderate (Cohen’s kappa index 0.54) to substantial (Cohen’s kappa index 0.74) after performing a second BM punction in patients BMB-/PET+. The other study [43] reported a fair agreement between techniques (Cohen’s kappa index 0.3). Both articles agree in describing that approximately 70% of cases are both FCM/PET negative, while 8-14% are FCM+/PET+. Discrepant cases accounted for 4-13% for FCM+/PET- and 8-12% for FCM-/PET+.
3.3. Diagnostic Accuracy of BMB and PET for Detecting BMi at DLBCL Diagnosis:
Few studies reported sufficient information about sensitivity, specificity, positive predictive value, negative predictive value, Youden’s index, or diagnostic accuracy (Table 3). Furthermore, the definition of a true positive BMi strongly varies among studies. It seems that PET sensitivity is higher when BM is focal rather than diffuse [10], which carried that some studies considered as true positive cases for BMi those with PET+ by a focal pattern [16,33,44]. Studies that used a true positive BMi defined by BMB+, or by PET+ if accompanied with targeted/morphologic imaging changes or FDG disappearance with response after treatment or concordant FDG progression on follow-up [10,44,46], reported a higher PET sensitivity and diagnostic accuracy, while a higher BMB specificity. Equivalent findings were seen in one study that considered BMB+ or PET+ focal as true positive BMi [16]. As expected, when BMB+ was considered solely as true positive BMi the sensitivity, specificity, predictive value, and diagnostic accuracy of PET is reduced [33,37,41,42,45,51], as it also happened to BMB when true positive BMi is only defined by PET+ [33]. No studies reported data about sensitivity or specificity regarding BMi by FCM.
The upstagement to a higher stage by BMB or PET has been evaluated in many studies. Discrepant results were seen about the role of BMB in this setting, thus, some studies described that BMB upstaged to Ann Arbor IV 2-15% of cases in their global cohorts that were grouped as PET- for BMi [33,42,50], while others reported that BMB did not upstage any BMB+/PET- case to Ann Arbor IV [20,35,44]. Four studies agreed in reporting that up to 5-8% patients in their global series were upstaged to Ann Arbor IV due to BMi by PET (particularly the focal pattern) not detected by BMB [10,20,35,50].
3.4. Prognostic Impact of BMi at DLBCL Diagnosis According to BMB, FCM and PET in Comparative Studies:
Eighteen studies accounting for 3,649 patients evaluated the prognostic impact of BMB, FCM or PET by the comparation or combination of at least two techniques (Table 4). There were no studies comparing PET and FCM findings.
3.4.1. BMB and FCM Outcomes According to BMi in Newly DLBCL:
Four studies (536 patients) described outcomes according to BMB and FCM. Despite the low number of reports, it seems that BMi by FCM is associated with worse prognosis when compared with FCM- cases, even in patients with BMB+. Two studies [43,49] that analyzed outcomes after combining BMB/FCM findings described discrepancies about the worse prognosis of BMB+/FCM+ cases compared with BMB-/FCM+ ones. On the one hand, M Moro et al. reported that the BMB-/FCM+ group presented an adverse outcome, equivalent to the BMB+/FCM+ population; similar findings were described in another study not included in the comparative review due to insufficient data [56]. On the other hand, Greenbaum et al. described that the prognosis of BMB-/FCM+ cases were intermediate between the BMB-/FCM- and the BMB+/FCM+ groups. As a third study points out [40], both BMB and FCM analyzed separately are related to worse prognosis, with a trend to worse outcome when BMi is detected by BMB.
Two studies that not met criteria to be included in the comparative review [32,57] and one more recent study that was included [47] analyzed the prognostic role of BMi detected by direct BM assessment when combined with the cell-of-origin classification according to Hans algorithm. The first study reported that BMB+ cases presented an equivalent worse prognosis regardless of being classified as germinal center B (GCB) or non-GCG [32], while in the second study non-GCB BMB+ cases presented a worse outcome than the GCB BMB+ group [57]. Interestingly, the third study suggested that BMB+/FCM+ with a concordant BMi presented a worse outcome regardless of cell-of-origin classification, in contrast with BMB+/FCM+ cases with a discordant type of BMi, in which non-GCB patients presented a worse prognosis when compared with GCB cases [47].
3.4.2. BMB and PET Outcomes According to BMi in Newly DLBCL:
Fourteen studies (3,113 patients) reported surveillance information according to BMB and PET.
Most reports (9/14) described a worse prognosis when BMi was detected by BMB than by PET. Seven studies [10,35,36,45,50,51,53] reported worse outcome (PFS/EFS and/or OS) in BMB+ DLBCL patients than in PET+ ones, and similar results were seen in another article analyzing PET+ focal cases [46]. Another group [48], ranked patients according to their BMi by BMB/PET from worse to better prognosis as follows: BMB+/PET+, BMB+/PET-, and BMB-/PET+; the BMB-/PET+ group presented an equivalent prognosis than BMB-/PET- cases. In contrast, Hong et al. reported similar outcomes between the BMB+/PET+ and the BMB+/PET- groups, while the surveillance was still equivalent between BMB-/PET+ and BMB-/PET-. Four studies out of 14 showed no differences between BMB and PET in predicting prognosis by BMi [20,41,48,52]: Liam et al. and Liang et al. reported equivalent prognosis between BMB+ and PET+, and Wang et al. described similar findings between BMB+ and PET+ focal; Cerci et al. saw that BMB+/PET+ focal patients associated a worse outcome when compared with BMB+/PET-, BMB-/PET+ and BMB-/PET+ focal, without differences between these three groups. Only 1/14 reports showed worse outcome in PET+ focal cases than in BMB+, although it was only described for PFS and not for OS [16]. Additionally, one analysis including only stage IV DLBCL patients showed no differences in EFS or OS between the BMB+ or PET+ group and the PET+ group [33].
Regarding BM uptake pattern by PET, three studies reported the prognostic significance of PET+ focal [20,46,48]. Chen et al. presented data about prognosis according to focal and diffuse PET+ patterns, showing PET+ focal cases a worse impact in both EFS and OS, while PET+ diffuse did not relate with worse outcome. Only one study described a slight trend of a worse lymphoma specific survival in PET+ diffuse patients than in PET+ focal ones [41].
No report studied the prognostic significance of BMB according to concordant or discordant types of infiltration in the setting of a comparative study with BMi by PET.
4. Discussion
Here is reported the first comparative review evaluating the diagnostic accuracy and prognostic implications of three different techniques (BMB, FCM and PET) regarding BMi at DLBCL diagnosis. This review included twenty-five studies with a total sample size of 4,849 patients with newly diagnosed DLBCL. Although BMB data was available in all studies, complete information about BMi (defined as a description of the different types of BMi according to each technique) by PET was available in a higher proportion of reports; it is probably due to the growing interest on nuclear-imaging techniques to evaluate BMi in an attempt to abandon the direct assessment of BM by trephine biopsy and aspiration in DLBCL patients. The global rate of BMi was 15% for BMB, 24.5% by FCM, and 21.9% by PET. This review also supports the fact that a unilateral punction of the iliac crest is sufficient for assessing BMi in DLBCL, being the difference of performing a bilateral BMB not clinically relevant. The BMB detected concordant infiltration more frequently than the discordant one, while the solely study that reported information about de type of BMi by FCM observed a higher rate of discordant invasion [47], in line with previous reports that highlighted the role of FCM in detecting BMi by low-grade small B-cell populations in DLBCL [25,26]. In a concordance comparison between techniques regarding their role to detect BMi at DLBCL diagnosis, the agreement between BMB and FCM was higher than between BMB and PET. Most discrepancies between BMB and FCM occur due to discordant or minor BMi detected by FCM and not detected by BMB, probably explained by the higher sensitivity of the FCM technique. In this setting, future studies based on FCM may provide interesting information about the biological implications of detecting discordant BMi by a low-grade B-cell entity in DLBCL patients; in fact, although the possible clonal relationship between the DLBCL and their BM discordant clones has barely been studied it is a topic of high interest which may have diagnostic and therapeutic implications in future. The high incidence of clonal identity in DLBCL cases with discordant BMi could suggest that in those cases the DLBCL develops from a previous indolent B-cell lymphoma [47,58] and, in this setting, a BM detection and complete phenotypic characterization of the low-grade population by FCM may provide a first step in the suspicion of a histological transformation. In fact, some patients with DLBCL are concomitantly diagnosed with indolent lymphoma, but their outcome do not differ from those diagnosed with DLBCL alone [59].
When BMB and PET were compared, both BMB+/PET- and BMB-/PET+ discrepant cases were seen among studies, suggesting that both techniques are complementary in assessing BMi in newly DLBCL. BMB is probably a better tool for detecting concordant BMi of low quantity or discordant infiltration than PET, and PET-FDG is easily able to determine focal involvement that BMB cannot recognize without a guided punction. In fact, a focal pattern BM uptake detected by PET is highly suggestive of BMi and a guided BM assessment is not necessary to confirm the invasion of BM in these cases, but even nowadays there is not a stablished definition of true positive BMi by PET in DLBCL. Some studies included as part of the definition of true BMi by PET the concept of following-up the uptake patterns of the BM, making comparisons with the response or progression of the DLBCL in later explorations, stablishing the BMi if concordance between determinations is found, thus, disappearance of BM FDG uptake after treatment or BM FDG increasing with disease progression. Apart from the fact that a retrospective evaluation of BMi is not operative for providing this information at DLBCL diagnosis, evaluating the BM PET may be even more challenging during follow-up due to the high frequency of reactive uptake pattern, such as in the context of the systemic therapies administered (such as steroids, immunochemotherapy, or supportive treatment with granulocyte colony stimulating factor), driving into false positive results. Nonetheless, as previously reported, PET-FDG is highly accurate for detecting BMi in newly diagnosed DLBCL and BMB may be avoided in cases with positive PET BM uptake [15], but it is a fact that in some cases with negative PET an occult BMi may be present, and a direct BM assessment may be performed to rule it out. Another controversial topic is the fact that avoiding BMB may have or not staging implications and, consequently, a possible effect on the therapeutic approach. Since there are both studies that defend the role of BMB in upstaging to advanced disease DLBCL cases with negative PET for BMi [33,42,50], and others that report the null effect of BMB in upstaging PET negative cases [20,35,44], from the point of view of the authors there is not strongly enough evidence to affirm that abandoning BMB would not have clinically relevant consequences.
Studies describing DLBCL outcomes according to BMi when comparing different techniques mostly report data facing BMB and PET results. Although BMi by BMB has clearly demonstrated being an adverse prognostic factor in DLBCL, there is not sufficient evidence to determine if BM uptake by PET is associated with a worse prognosis in DLBCL patients with positive BMB. Even though, some studies did not find correlation between BMi by PET and worse prognosis; this could be explained due to the different prognosis significance among the pattern of BM uptake (focal or diffuse). Two studies [41,50] described higher median SUVmax in DLBCL cases with BM focal pattern compared with those with BM diffuse pattern. Some groups are investigating the prognostic implication of metabolic measures in DLBCL patients including parameters related to BM, such as the BM retention index and the BM-to-liver ratio of baseline PET-FDG, both described as predictors of PFS and OS [60]. Few studies have analyzed the prognostic impact of BMi by FCM in DLBCL, showing that a positive BMi detected by FCM associates a worse outcome, even without considering BMB findings. The fact that DLBCL patients with BMi demonstrated by FCM but not by BMB have a worse prognosis when compared with cases both negative for BMB and FCM is very relevant, as it may suggest that BMB is not able to screen a group of patients with worse outcome in which a direct BM is performed. The combination of the type of BMi by BMB/FCM (concordant or discordant) and the immunohistochemical cell-of-origin classification is an interesting topic that should be evaluated in future studies, as it seems that non-GCB patients associates a worse prognosis if BMi is detected by direct BM assessment, while the prognostic of GCB group depends on the type of BMi.
Some other tools have been explored to assess BMi at DLBCL diagnosis. The examination of pelvic [61] or whole-body [62] magnetic resonance imaging (MRI) focusing on DLBCL BMi has been evaluated as a complementary tool for BMB and PET, and even a prognostic implication of positive MRI has been suggested. Different genetic assays have been studied to detect BMi in de novo DLBCL. The molecular analysis of immunoglobulin heavy chain (IgH) gene rearrangement has been evaluated in some studies, combining their results with BMB [63] or PET-FDG [39] for a better diagnostic accuracy and a greater prognostic stratification in newly DLBCL cases. Furthermore, the finding of cytogenetic alterations [64] or occult involvement by polymerase chain reaction [54] in BM assessment of DLBCL patients has been related with worse outcomes independently from BMB results.
5. Conclusions
BM assessment in newly DLBCL is still a controversial and interesting topic with discrepant results in literature regarding the diagnostic accuracy and prognostic implications of the different available techniques for its evaluation. Both the BMB, the FCM, and the PET-FDG are complementary tools that provide different and clinically relevant information. There is still not enough evidence to recommend avoiding the direct BM assessment at baseline evaluation of DLBCL. In fact, it is necessary to increase knowledge in this regard by performing prospective studies and deeply analyzing the role of novel technologies such as multiparametric FCM and molecular assays.
Author Contributions
All authors performed conceptualization, methodology and formal analysis. F.M-M. and JA.G-V. wrote the original manuscript, and J.L-J. and JA.G-M. reviewed it. The final version of the manuscript has been read and approved by all authors.
Funding
This research received no external funding.
Data Availability Statement
All the studies used in this study are published in the literature.
Conflicts of Interest
The authors declare no conflict of interest related to this work.
References
- Bastos-Oreiro, M.; Muntañola, A.; Panizo, C.; Gonzalez-Barca, E.; de Villambrosia, S.G.; Córdoba, R.; López, J.L.B.; González-Sierra, P.; Terol, M.J.; Gutierrez, A.; Grande, C.; Ramirez, M.J.; Iserte, L.; Perez, E.; Navarro, B.; Gomez, P.; Salar, A.; Luzardo, H.; López, A.; Del Campo, R.; García-Belmonte, D.; Vida, M.J.; Infante, M.; Queizan-Hernandez, J.A.; Novelli, S.; Moreno, M.; Penarrubia, M.; Gómez, J.; Domingo, A.; Donato, E.; Viguria, M.C.; López, F.; Rodriguez, M.J.; Pardal, E.; Noriega, V.; Andreu, R.; Peñalver, J.; Martín, A.; Caballero, D.; López-Guillermo, A. RELINF: Prospective Epidemiological Registry of Lymphoid Neoplasms in Spain. A Project from the GELTAMO Group. Ann Hematol 2020, 99, 799–808. [Google Scholar] [CrossRef]
- Sehn, L.H.; Salles, G. Diffuse Large B-Cell Lymphoma. New England Journal of Medicine 2021, 384, 842–858. [Google Scholar] [CrossRef]
- Lamy, T.; Damaj, G.; Soubeyran, P.; Gyan, E.; Cartron, G.; Bouabdallah, K.; Gressin, R.; Cornillon, J.; Banos, A.; Le Du, K.; Benchalal, M.; Moles, M.-P.; Le Gouill, S.; Fleury, J.; Godmer, P.; Maisonneuve, H.; Deconinck, E.; Houot, R.; Laribi, K.; Marolleau, J.P.; Tournilhac, O.; Branger, B.; Devillers, A.; Vuillez, J.P.; Fest, T.; Colombat, P.; Costes, V.; Szablewski, V.; Béné, M.C.; Delwail, V.; LYSA Group. R-CHOP 14 with or without Radiotherapy in Nonbulky Limited-Stage Diffuse Large B-Cell Lymphoma. Blood 2018, 131, 174–181. [Google Scholar] [CrossRef]
- Poeschel, V.; Held, G.; Ziepert, M.; Witzens-Harig, M.; Holte, H.; Thurner, L.; Borchmann, P.; Viardot, A.; Soekler, M.; Keller, U.; Schmidt, C.; Truemper, L.; Mahlberg, R.; Marks, R.; Hoeffkes, H.-G.; Metzner, B.; Dierlamm, J.; Frickhofen, N.; Haenel, M.; Neubauer, A.; Kneba, M.; Merli, F.; Tucci, A.; de Nully Brown, P.; Federico, M.; Lengfelder, E.; di Rocco, A.; Trappe, R.; Rosenwald, A.; Berdel, C.; Maisenhoelder, M.; Shpilberg, O.; Amam, J.; Christofyllakis, K.; Hartmann, F.; Murawski, N.; Stilgenbauer, S.; Nickelsen, M.; Wulf, G.; Glass, B.; Schmitz, N.; Altmann, B.; Loeffler, M.; Pfreundschuh, M.; FLYER Trial Investigators; German Lymphoma Alliance. Four versus Six Cycles of CHOP Chemotherapy in Combination with Six Applications of Rituximab in Patients with Aggressive B-Cell Lymphoma with Favourable Prognosis (FLYER): A Randomised, Phase 3, Non-Inferiority Trial. Lancet 2019, 394, 2271–2281. [Google Scholar] [CrossRef]
- Tilly, H.; Morschhauser, F.; Sehn, L.H.; Friedberg, J.W.; Trněný, M.; Sharman, J.P.; Herbaux, C.; Burke, J.M.; Matasar, M.; Rai, S.; Izutsu, K.; Mehta-Shah, N.; Oberic, L.; Chauchet, A.; Jurczak, W.; Song, Y.; Greil, R.; Mykhalska, L.; Bergua-Burgués, J.M.; Cheung, M.C.; Pinto, A.; Shin, H.-J.; Hapgood, G.; Munhoz, E.; Abrisqueta, P.; Gau, J.-P.; Hirata, J.; Jiang, Y.; Yan, M.; Lee, C.; Flowers, C.R.; Salles, G. Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma. New England Journal of Medicine 2022, 386, 351–363. [Google Scholar] [CrossRef]
- Bobillo, S.; Khwaja, J.; Ferreri, A.J.M.; Cwynarski, K. Prevention and Management of Secondary Central Nervous System Lymphoma. Haematologica 2023, 108, 673–689. [Google Scholar] [CrossRef]
- Tilly, H.; Gomes da Silva, M.; Vitolo, U.; Jack, A.; Meignan, M.; Lopez-Guillermo, A.; Walewski, J.; André, M.; Johnson, P.W.; Pfreundschuh, M.; Ladetto, M.; ESMO Guidelines Committee. Diffuse Large B-Cell Lymphoma (DLBCL): ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann Oncol 2015, 26 (Suppl. 5), v116–v125. [Google Scholar] [CrossRef]
- Bain, B.J. Morbidity Associated with Bone Marrow Aspiration and Trephine Biopsy - a Review of UK Data for 2004. Haematologica 2006, 91, 1293–1294. [Google Scholar]
- Brunetti, G.A.; Tendas, A.; Meloni, E.; Mancini, D.; Maggiore, P.; Scaramucci, L.; Giovannini, M.; Niscola, P.; Cartoni, C.; Alimena, G. Pain and Anxiety Associated with Bone Marrow Aspiration and Biopsy: A Prospective Study on 152 Italian Patients with Hematological Malignancies. Ann Hematol 2011, 90, 1233–1235. [Google Scholar] [CrossRef]
- Berthet, L.; Cochet, A.; Kanoun, S.; Berriolo-Riedinger, A.; Humbert, O.; Toubeau, M.; Dygai-Cochet, I.; Legouge, C.; Casasnovas, O.; Brunotte, F. In Newly Diagnosed Diffuse Large B-Cell Lymphoma, Determination of Bone Marrow Involvement with 18 F-FDG PET/CT Provides Better Diagnostic Performance and Prognostic Stratification Than Does Biopsy. J Nucl Med 2013, 54, 1244–1250. [Google Scholar] [CrossRef]
- El-Galaly, T.C.; Gormsen, L.C.; Hutchings, M. PET/CT for Staging; Past, Present, and Future. Semin Nucl Med 2018, 48, 4–16. [Google Scholar] [CrossRef]
- Adams, H.J.A.; Kwee, T.C. Do Not Abandon the Bone Marrow Biopsy yet in Diffuse Large B-Cell Lymphoma. J Clin Oncol 2015, 33, 1217. [Google Scholar] [CrossRef]
- Adams, H.J.A.; Kwee, T.C. Increased Bone Marrow FDG Uptake at PET/CT Is Not a Sufficient Proof of Bone Marrow Involvement in Diffuse Large B-Cell Lymphoma. Am J Hematol 2015, 90, E182–E183. [Google Scholar] [CrossRef]
- Avigdor, A. Staging DLBCL: Bone Marrow Biopsy or PET-CT? Blood 2013, 122, 4–5. [Google Scholar] [CrossRef]
- Adams, H.J.A.; Kwee, T.C.; de Keizer, B.; Fijnheer, R.; de Klerk, J.M.H.; Nievelstein, R.A.J. FDG PET/CT for the Detection of Bone Marrow Involvement in Diffuse Large B-Cell Lymphoma: Systematic Review and Meta-Analysis. Eur J Nucl Med Mol Imaging 2014, 41, 565–574. [Google Scholar] [CrossRef]
- Chen, Y.; Zhou, M.; Liu, J.; Huang, G. Prognostic Value of Bone Marrow FDG Uptake Pattern of PET/CT in Newly Diagnosed Diffuse Large B-Cell Lymphoma. J. Cancer 2018, 9, 1231–1238. [Google Scholar] [CrossRef]
- Elstrom, R.L.; Tsai, D.E.; Vergilio, J.-A.; Downs, L.H.; Alavi, A.; Schuster, S.J. Enhanced Marrow [18F]Fluorodeoxyglucose Uptake Related to Myeloid Hyperplasia in Hodgkin’s Lymphoma Can Simulate Lymphoma Involvement in Marrow. Clin Lymphoma 2004, 5, 62–64. [Google Scholar] [CrossRef]
- Akin, O.; Brennan, S.B.; Dershaw, D.D.; Ginsberg, M.S.; Gollub, M.J.; Schöder, H.; Panicek, D.M.; Hricak, H. Advances in Oncologic Imaging: Update on 5 Common Cancers. CA Cancer J Clin 2012, 62, 364–393. [Google Scholar] [CrossRef]
- Jerusalem, G.; Beguin, Y.; Najjar, F.; Hustinx, R.; Fassotte, M.F.; Rigo, P.; Fillet, G. Positron Emission Tomography (PET) with 18F-Fluorodeoxyglucose (18F-FDG) for the Staging of Low-Grade Non-Hodgkin’s Lymphoma (NHL). Ann Oncol 2001, 12, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Cerci, J.J.; Györke, T.; Fanti, S.; Paez, D.; Meneghetti, J.C.; Redondo, F.; Celli, M.; Auewarakul, C.; Rangarajan, V.; Gujral, S.; Gorospe, C.; Campo, M.V.; Chung, J.-K.; Morris, T.P.; Dondi, M.; Carr, R. Combined PET and Biopsy Evidence of Marrow Involvement Improves Prognostic Prediction in Diffuse Large B-Cell Lymphoma. J Nucl Med 2014, 55, 1591–1597. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Pfistner, B.; Juweid, M.E.; Gascoyne, R.D.; Specht, L.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Hagenbeek, A.; Zucca, E.; Rosen, S.T.; Stroobants, S.; Lister, T.A.; Hoppe, R.T.; Dreyling, M.; Tobinai, K.; Vose, J.M.; Connors, J.M.; Federico, M.; Diehl, V.; International Harmonization Project on Lymphoma. Revised Response Criteria for Malignant Lymphoma. J Clin Oncol 2007, 25, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Cabezas-Quintario, M.A.; Gomez, P.; Yuste-Del Pozo, V.; Valencia-Mesa, A.L.; Sosa, G.; Ricard, P.; Hijas-Gómez, A.I.; Pinedo, F.; Arguelles, M. Bone Marrow Trephine Biopsy Involvement by Lymphoma: Pattern of Involvement and Concordance with Flow Cytometry, in 10 Years from a Single Institution. Clin Transl Oncol 2016, 18, 537–540. [Google Scholar] [CrossRef] [PubMed]
- Talaulikar, D.; Dahlstrom, J.E. Staging Bone Marrow in Diffuse Large B-Cell Lymphoma: The Role of Ancillary Investigations. Pathology 2009, 41, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Pittaluga, S.; Tierens, A.; Dodoo, Y.L.; Delabie, J.; De Wolf-Peeters, C. How Reliable Is Histologic Examination of Bone Marrow Trephine Biopsy Specimens for the Staging of Non-Hodgkin Lymphoma? A Study of Hairy Cell Leukemia and Mantle Cell Lymphoma Involvement of the Bone Marrow Trephine Specimen by Histologic, Immunohistochemical, and Polymerase Chain Reaction Techniques. Am J Clin Pathol 1999, 111, 179–184. [Google Scholar] [CrossRef]
- Tierens, A.M.; Holte, H.; Warsame, A.; Ikonomou, I.M.; Wang, J.; Chan, W.C.; Delabie, J. Low Levels of Monoclonal Small B Cells in the Bone Marrow of Patients with Diffuse Large B-Cell Lymphoma of Activated B-Cell Type but Not of Germinal Center B-Cell Type. Haematologica 2010, 95, 1334–1341. [Google Scholar] [CrossRef] [PubMed]
- Stacchini, A.; Demurtas, A.; Godio, L.; Martini, G.; Antinoro, V.; Palestro, G. Flow Cytometry in the Bone Marrow Staging of Mature B-Cell Neoplasms. Cytometry B Clin Cytom 2003, 54, 10–18. [Google Scholar] [CrossRef]
- Shim, H.; Oh, J.-I.; Park, S.H.; Jang, S.; Park, C.-J.; Huh, J.; Suh, C.; Chi, H.-S. Prognostic Impact of Concordant and Discordant Cytomorphology of Bone Marrow Involvement in Patients with Diffuse, Large, B-Cell Lymphoma Treated with R-CHOP. J Clin Pathol 2013, 66, 420–425. [Google Scholar] [CrossRef]
- Sehn, L.H.; Scott, D.W.; Chhanabhai, M.; Berry, B.; Ruskova, A.; Berkahn, L.; Connors, J.M.; Gascoyne, R.D. Impact of Concordant and Discordant Bone Marrow Involvement on Outcome in Diffuse Large B-Cell Lymphoma Treated With R-CHOP. JCO 2011, 29, 1452–1457. [Google Scholar] [CrossRef]
- Chung, R.; Lai, R.; Wei, P.; Lee, J.; Hanson, J.; Belch, A.R.; Turner, A.R.; Reiman, T. Concordant but Not Discordant Bone Marrow Involvement in Diffuse Large B-Cell Lymphoma Predicts a Poor Clinical Outcome Independent of the International Prognostic Index. Blood 2007, 110, 1278–1282. [Google Scholar] [CrossRef]
- Yao, Z.; Deng, L.; Xu-Monette, Z.Y.; Manyam, G.C.; Jain, P.; Tzankov, A.; Visco, C.; Bhagat, G.; Wang, J.; Dybkaer, K.; Tam, W.; Hsi, E.D.; Van Krieken, J.H.; Ponzoni, M.; Ferreri, A.J.M.; Møller, M.B.; Winter, J.N.; Piris, M.A.; Fayad, L.; Liu, Y.; Song, Y.; Orlowski, R.Z.; Kantarjian, H.; Medeiros, L.J.; Li, Y.; Cortes, J.; Young, K.H. Concordant Bone Marrow Involvement of Diffuse Large B-Cell Lymphoma Represents a Distinct Clinical and Biological Entity in the Era of Immunotherapy. Leukemia 2018, 32, 353–363. [Google Scholar] [CrossRef]
- Chigrinova, E.; Mian, M.; Scandurra, M.; Greiner, T.C.; Chan, W.C.; Vose, J.M.; Inghirami, G.; Chiappella, A.; Baldini, L.; Ponzoni, M.; Ferreri, A.J.M.; Franceschetti, S.; Gaidano, G.; Tucci, A.; Facchetti, F.; Lazure, T.; Lambotte, O.; Montes-Moreno, S.; Piris, M.A.; Nomdedeu, J. Fr.; Uccella, S.; Rancoita, P.M.V.; Kwee, I.; Zucca, E.; Bertoni, F. Diffuse Large B-cell Lymphoma with Concordant Bone Marrow Involvement Has Peculiar Genomic Profile and Poor Clinical Outcome. Hematological Oncology 2011, 29, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Park, M.-J.; Park, S.-H.; Park, P.-W.; Seo, Y.-H.; Kim, K.-H.; Seo, J.-Y.; Jeong, J.-H.; Kim, M.J.; Ahn, J.-Y.; Hong, J. Prognostic Impact of Concordant and Discordant Bone Marrow Involvement and Cell-of-Origin in Korean Patients with Diffuse Large B-Cell Lymphoma Treated with R-CHOP. J Clin Pathol 2015, 68, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, M.; El-Galaly, T.C.; Hutchings, M.; Hansen, J.W.; Loft, A.; Johnsen, H.E.; Iyer, V.; Wilson, D.; Sehn, L.H.; Savage, K.J.; Connors, J.M.; Gascoyne, R.D.; Johansen, P.; Clasen-Linde, E.; Brown, P.; Villa, D. The Value of Routine Bone Marrow Biopsy in Patients with Diffuse Large B-Cell Lymphoma Staged with PET/CT: A Danish-Canadian Study. Annals of Oncology 2016, 27, 1095–1099. [Google Scholar] [CrossRef] [PubMed]
- Soydal, C.; Koksoy, E.B.; Yasar, A.; Turgal, E.; Erdogan, B.D.; Akbulut, H.; Kucuk, N.O. Prognostic Importance of Bone Marrow Uptake on Baseline 18F-FDG Positron Emission Tomography in Diffuse Large B Cell Lymphoma. Cancer Biother Radiopharm 2016, 31, 361–365. [Google Scholar] [CrossRef]
- Khan, A.B.; Barrington, S.F.; Mikhaeel, N.G.; Hunt, A.A.; Cameron, L.; Morris, T.; Carr, R. PET-CT Staging of DLBCL Accurately Identifies and Provides New Insight into the Clinical Significance of Bone Marrow Involvement. Blood 2013, 122, 61–67. [Google Scholar] [CrossRef]
- Hong, J.; Lee, Y.; Park, Y.; Kim, S.G.; Hwang, K.H.; Park, S.H.; Jeong, J.; Kim, K.-H.; Ahn, J.Y.; Park, S.; Park, J.; Lee, J.H. Role of FDG-PET/CT in Detecting Lymphomatous Bone Marrow Involvement in Patients with Newly Diagnosed Diffuse Large B-Cell Lymphoma. Ann Hematol 2012, 91, 687–695. [Google Scholar] [CrossRef]
- Bo, G.; Ran, Q.; Yang, G.Z.; Fen, L.Y.; Lei, G.; Rong, H.W. Diagnostic Efficacy of 18F-FDG PET/CT in Detecting Bone Marrow Infiltration in Patients with Newly Diagnosed Diffuse Large B-Cell Lymphoma. Biomed Environ Sci 2023, 36, 510–516. [Google Scholar] [CrossRef]
- Han, E.J.; O, J.H.; Yoon, H.; Ha, S.; Yoo, I.R.; Min, J.W.; Choi, J.-I.; Choi, B.-O.; Park, G.; Lee, H.H.; Jeon, Y.-W.; Min, G.-J.; Cho, S.-G. Comparison of FDG PET/CT and Bone Marrow Biopsy Results in Patients with Diffuse Large B Cell Lymphoma with Subgroup Analysis of PET Radiomics. Diagnostics 2022, 12, 222. [Google Scholar] [CrossRef]
- Kim, M.; Ahn, S.-Y.; Ahn, J.-S.; Song, G.-Y.; Jung, S.-H.; Lee, J.-J.; Kim, H.-J.; Lee, J.H.; Shin, M.-G.; Song, S.Y.; Yang, D.-H. Diagnostic Accuracy and Prognostic Relevance of Immunoglobulin Heavy Chain Rearrangement and 18F-FDG-PET/CT Compared With Unilateral Bone Marrow Trephination for Detecting Bone Marrow Involvement in Patients With Diffuse Large B-Cell Lymphoma. J Korean Med Sci 2022, 37, e2. [Google Scholar] [CrossRef]
- Okamoto, H.; Uoshima, N.; Muramatsu, A.; Isa, R.; Fujino, T.; Matsumura-Kimoto, Y.; Tsukamoto, T.; Mizutani, S.; Shimura, Y.; Kobayashi, T.; Kawata, E.; Uchiyama, H.; Kuroda, J.; Kyoto Clinical Hematology Study Group Investigators. Combination of Bone Marrow Biopsy and Flow Cytometric Analysis: The Prognostically Relevant Central Approach for Detecting Bone Marrow Invasion in Diffuse Large B-Cell Lymphoma. Diagnostics 2021, 11, 1724. [Google Scholar] [CrossRef]
- Lim, C.H.; Hyun, S.H.; Cho, Y.S.; Choi, J.Y.; Lee, K.-H. Prognostic Significance of Bone Marrow 2-[18F]-Fluoro-2-Deoxy-d-Glucose Uptake in Diffuse Large B-Cell Lymphoma: Relation to Iliac Crest Biopsy Results. Clinical Radiology 2021, 76, 550.e19–550.e28. [Google Scholar] [CrossRef]
- Saiki, Y.; Tomita, N.; Uchida, A.; Uemura, Y.; Suzuki, Y.; Hirakawa, T.; Kato, M.; Hoshikawa, M.; Kawano, T.; Nakamura, N.; Miura, I.; Arai, A. Biopsy Remains Indispensable for Evaluating Bone Marrow Involvement in DLBCL Patients despite the Use of Positron Emission Tomography. Int J Hematol 2021, 113, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Martín-Moro, F.; Piris-Villaespesa, M.; Marquet-Palomanes, J.; García-Cosío, M.; Villarrubia, J.; Lario, A.; García, I.; Michael, B.; Roldán, E.; García-Vela, J.A.; Lopez-Jiménez, J. Bone Marrow Infiltration by Flow Cytometry at Diffuse Large B-cell Lymphoma NOS Diagnosis Implies Worse Prognosis without Considering Bone Marrow Histology. Cytometry Part B Clinical 2020, 98, 525–528. [Google Scholar] [CrossRef] [PubMed]
- Al-Sabbagh, A.; Ibrahim, F.; Szabados, L.; Soliman, D.S.; Taha, R.Y.; Fernyhough, L.J. The Role of Integrated Positron Emission Tomography/Computed Tomography (PET/CT) and Bone Marrow Examination in Staging Large B-Cell Lymphoma. Clin Med Insights Oncol 2020, 14, 117955492095309. [Google Scholar] [CrossRef] [PubMed]
- Min, G.-J.; Jeon, Y.-W.; Park, S.-S.; Shin, S.-H.; Yahng, S.-A.; Yoon, J.-H.; Lee, S.-E.; Cho, B.-S.; Eom, K.-S.; Kim, Y.-J.; Lee, S.; Kim, H.-J.; Min, C.-K.; Kim, D.-W.; Lee, J.-W.; Cho, S.-G. Poor Prognosis in Patients with Diffuse Large B Cell Lymphomas with Bone Marrow Involvement Possessing Chromosomal Abnormalities, despite Aggressive Treatment. Ann Hematol 2020, 99, 557–570. [Google Scholar] [CrossRef]
- Kandeel, A.A.; Hussein, M.; Zidan, L.; Younis, J.; Edesa, W.; Alsayed, Y. Diagnostic Performance of 18F-2-Fluoro-2-Deoxy-D-Glucose PET/Computerized Tomography in Identifying Bone Marrow Infiltration in New Patients with Diffuse Large B-Cell Lymphoma and Hodgkin Lymphoma. Nuclear Medicine Communications 2020, 41, 269–279. [Google Scholar] [CrossRef]
- Alonso-Álvarez, S.; Alcoceba, M.; García-Álvarez, M.; Blanco, O.; Rodríguez, M.; Baile, M.; Caballero, J.C.; Dávila, J.; Vidriales, M.B.; Esteban, C.; Arias, P.; Díaz, L.G.; Tamayo, P.; Caballero, M.D.; Gutiérrez, N.C.; González, M.; Martín, A. Biological Features and Prognostic Impact of Bone Marrow Infiltration in Patients with Diffuse Large B-Cell Lymphoma. Cancers 2020, 12, 474. [Google Scholar] [CrossRef]
- Wang, J.; Kim, D.; Kang, W.J.; Cho, H. Prognostic Value of Bone Marrow F-18 FDG Uptake in Patients with Advanced-Stage Diffuse Large B-Cell Lymphoma. Nucl Med Mol Imaging 2020, 54, 28–34. [Google Scholar] [CrossRef]
- Greenbaum, U.; Levi, I.; Madmoni, O.; Lior, Y.; Al-Athamen, K.; Perry, Z.H.; Hatzkelzon, L.; Shubinsky, G. The Prognostic Significance of Bone Marrow Involvement in Diffuse Large B Cell Lymphoma According to the Flow Cytometry. Leukemia & Lymphoma 2019, 60, 2477–2482. [Google Scholar] [CrossRef]
- Chen-Liang, T.; Martín-Santos, T.; Jerez, A.; Rodríguez-García, G.; Senent, L.; Martínez-Millán, C.; Muiña, B.; Orero, M.; Teruel, A.; Martín, A.; Gómez-Espuch, J.; Kennedy, K.; Benet, C.; Raya, J.M.; Fernández-González, M.; De La Cruz, F.; Guinot, M.; Villegas, C.; Ballester, I.; Baile, M.; Moya, M.; López-Jiménez, J.; Frutos, L.; Navarro, J.L.; Uña, J.; Fernández-López, R.; Igua, C.; Contreras, J.; Sánchez-Vañó, R.; Cozar, M.D.P.; Tamayo, P.; Mucientes, J.; Sánchez-Blanco, J.J.; Pérez-Ceballos, E.; Ortuño, F.J. Bone Marrow Biopsy Superiority over PET / CT in Predicting Progression-free Survival in a Homogeneously-treated Cohort of Diffuse Large B-cell Lymphoma. Cancer Medicine 2017, 6, 2507–2514. [Google Scholar] [CrossRef]
- Vishnu, P.; Wingerson, A.; Lee, M.; Mandelson, M.T.; Aboulafia, D.M. Utility of Bone Marrow Biopsy and Aspirate for Staging of Diffuse Large B Cell Lymphoma in the Era of Positron Emission Tomography With 2-Deoxy-2-[Fluorine-18]Fluoro-Deoxyglucose Integrated With Computed Tomography. Clinical Lymphoma Myeloma and Leukemia 2017, 17, 631–636. [Google Scholar] [CrossRef] [PubMed]
- Liang, J.-H.; Sun, J.; Wang, L.; Fan, L.; Chen, Y.-Y.; Qu, X.-Y.; Li, T.-N.; Li, J.-Y.; Xu, W. Prognostic Significance of Bone Marrow Infiltration Detected by PET-CT in Newly Diagnosed Diffuse Large B Cell Lymphoma. Oncotarget 2016, 7, 19072–19080. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.J.A.; Kwee, T.C.; Fijnheer, R.; Dubois, S.V.; Nievelstein, R.A.J.; De Klerk, J.M.H. Bone Marrow 18 F-fluoro-2-deoxy- d -glucose Positron Emission Tomography/Computed Tomography Cannot Replace Bone Marrow Biopsy in Diffuse Large B-cell Lymphoma. American J Hematol 2014, 89, 726–731. [Google Scholar] [CrossRef] [PubMed]
- Arima, H.; Maruoka, H.; Nasu, K.; Tabata, S.; Kurata, M.; Matsushita, A.; Imai, Y.; Takahashi, T.; Ishikawa, T. Impact of Occult Bone Marrow Involvement on the Outcome of Rituximab plus Cyclophosphamide, Doxorubicin, Vincristine and Prednisone Therapy for Diffuse Large B-Cell Lymphoma. Leukemia & Lymphoma 2013, 54, 2645–2653. [Google Scholar] [CrossRef]
- Cortés-Romera, M.; Sabaté-Llobera, A.; Mercadal-Vilchez, S.; Climent-Esteller, F.; Serrano-Maestro, A.; Gámez-Cenzano, C.; González-Barca, E. Bone Marrow Evaluation in Initial Staging of Lymphoma: 18F-FDG PET/CT Versus Bone Marrow Biopsy. Clinical Nuclear Medicine 2014, 39, e46–e52. [Google Scholar] [CrossRef] [PubMed]
- Wolach, O.; Fraser, A.; Luchiansky, M.; Shapiro, C.; Radnay, J.; Shpilberg, O.; Lishner, M.; Lahav, M. Can Flow Cytometry of Bone Marrow Aspirate Predict Outcome of Patients with Diffuse Large B Cell Lymphoma? A Retrospective Single Centre Study. Hematological Oncology 2015, 33, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Cho, M.-C.; Chung, Y.; Jang, S.; Park, C.-J.; Chi, H.-S.; Huh, J.; Suh, C.; Shim, H. Prognostic Impact of Germinal Center B-Cell-like and Non-Germinal Center B-Cell-like Subtypes of Bone Marrow Involvement in Patients with Diffuse Large B-Cell Lymphoma Treated with R-CHOP. Medicine 2018, 97, e13046. [Google Scholar] [CrossRef]
- Kremer, M.; Spitzer, M.; Mandl-Weber, S.; Stecker, K.; Schmidt, B.; Höfler, H.; Quintanilla-Martínez, L.; Fend, F. Discordant Bone Marrow Involvement in Diffuse Large B-Cell Lymphoma: Comparative Molecular Analysis Reveals a Heterogeneous Group of Disorders. Lab Invest 2003, 83, 107–114. [Google Scholar] [CrossRef]
- Wang, Y.; Link, B.K.; Witzig, T.E.; Maurer, M.J.; Allmer, C.; King, R.L.; Feldman, A.L.; Habermann, T.M.; Ansell, S.M.; Slager, S.L.; Cerhan, J.R.; Nowakowski, G.S. Impact of Concurrent Indolent Lymphoma on the Clinical Outcome of Newly Diagnosed Diffuse Large B-Cell Lymphoma. Blood 2019, 134, 1289–1297. [Google Scholar] [CrossRef]
- El-Azony, A.; Basha, M.A.A.; Almalki, Y.E.; Abdelmaksoud, B.; Hefzi, N.; Alnagar, A.A.; Mahdey, S.; Ali, I.M.; Nasr, I.; Abdalla, A.A.E.-H. M.; Yousef, H.Y.; Zaitoun, M.M.A.; Elsayed, S.B.; Nada, M.G.; Amin, M.I.; Hassan, R.M.; Ali, S.A.; Dawoud, T.M.; Aly, S.A.; Algazzar, Y.H.; Abdelhamed, H. The Prognostic Value of Bone Marrow Retention Index and Bone Marrow-to-Liver Ratio of Baseline 18F-FDG PET/CT in Diffuse Large B-Cell Lymphoma. Eur Radiol 2023. [Google Scholar] [CrossRef]
- Ke, Q.; Liao, C.-C.; Tan, X.-H.; Guo, B.-P.; Cen, H.; Li, L.-Q. Diagnostic Accuracy of Pelvic Magnetic Resonance Imaging for the Assessment of Bone Marrow Involvement in Diffuse Large B-Cell Lymphoma. PLoS One 2021, 16, e0252226. [Google Scholar] [CrossRef]
- Adams, H.J.A.; Kwee, T.C.; Lokhorst, H.M.; Westerweel, P.E.; Fijnheer, R.; Kersten, M.J.; Verkooijen, H.M.; Stoker, J.; Nievelstein, R.A.J. Potential Prognostic Implications of Whole-Body Bone Marrow MRI in Diffuse Large B-Cell Lymphoma Patients with a Negative Blind Bone Marrow Biopsy. J Magn Reson Imaging 2014, 39, 1394–1400. [Google Scholar] [CrossRef]
- Cho, Y.A.; Yang, W.I.; Song, J.; Min, Y.H.; Yoon, S.O. The Prognostic Significance of Monoclonal Immunoglobulin Gene Rearrangement in Conjunction with Histologic B-cell Aggregates in the Bone Marrow of Patients with Diffuse Large B-cell Lymphoma. Cancer Medicine 2016, 5, 1066–1073. [Google Scholar] [CrossRef]
- Kim, S.Y.; Kim, H.J.; Kang, H.J.; Kim, J.S.; Eom, H.S.; Kim, T.M.; Yoon, S.-S.; Suh, C.; Lee, D.S.; Korean Society of Hematology Lymphoma Working Party. Clinical Significance of Cytogenetic Aberrations in Bone Marrow of Patients with Diffuse Large B-Cell Lymphoma: Prognostic Significance and Relevance to Histologic Involvement. J Hematol Oncol 2013, 6, 76. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of the study selection process.
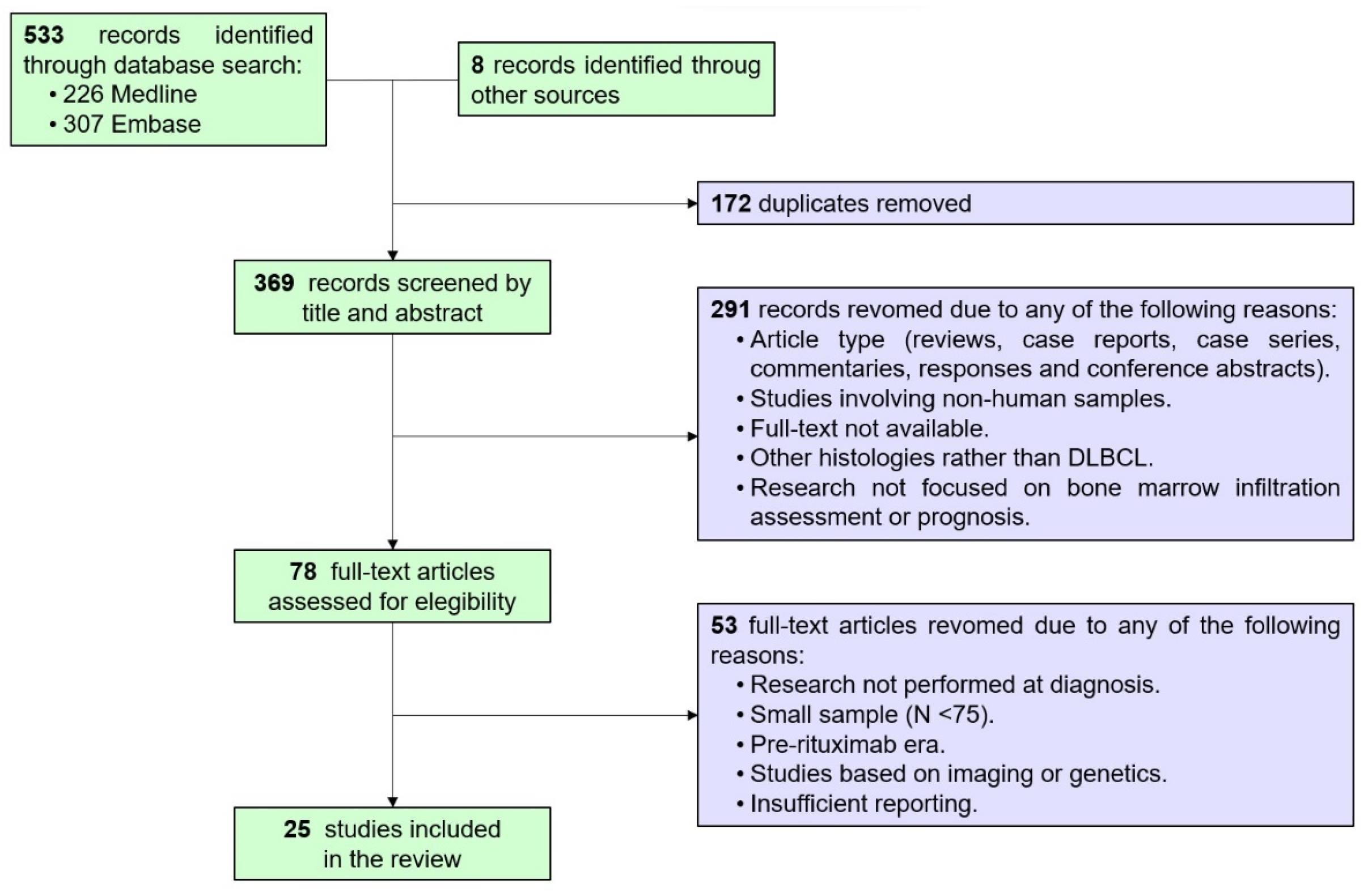
Figure 2.
Correlation between techniques (PET/BMB and BMB/FCM) according to available data reported in the twenty-five studies included in the review.
Figure 2.
Correlation between techniques (PET/BMB and BMB/FCM) according to available data reported in the twenty-five studies included in the review.
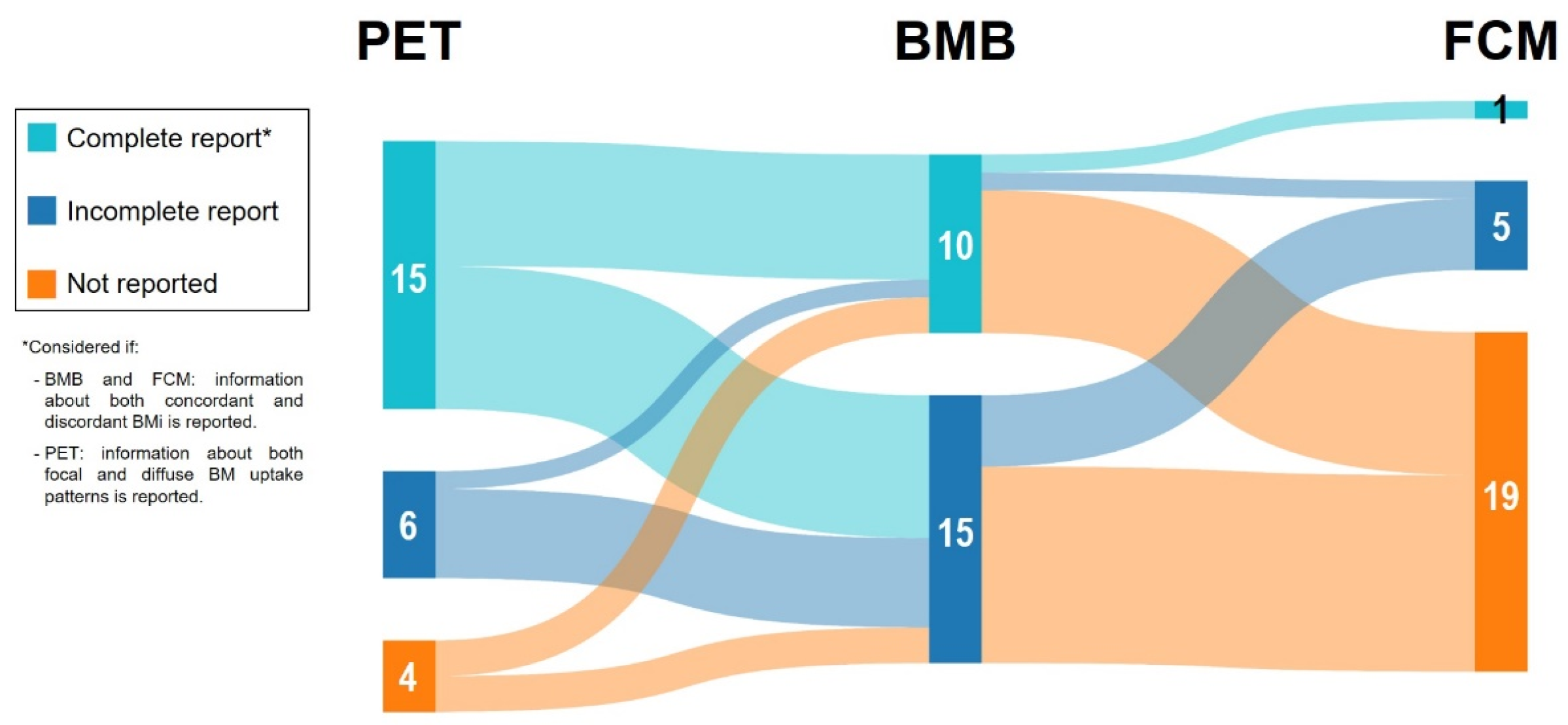

Table 1.
Newly DLBCL population characteristics and pretreatment bone marrow evaluation.
| Ref.* | Region | Study type | Period | N | DLBCL population characteristics | Bone marrow assessment | |||||||||||||||
| Male/female ratio | Median age (range) | COO† | Ann Arbor | IPI | Frontline | Follow-up (months) | Histology | Flow cytometry | PET-FDG | ||||||||||||
| Not specified or global | Concordant | Discordant | Not specified or global | Concordant | Discordant | Not specified or global | Focal | Diffuse | |||||||||||||
| Bo et al. [37] | China | Retrospective | 2019-2022 | 102 | 1.2 | 29.4% ≥60yo | GCB: 35%Non-GCB: 65% | I-II: 14%III: 0%IV: 86% | 3-5: 28% | - | - | 21% (28% after second punction) | - | - | 18% (24% after second punction) | - | - | 26% | 23% | 3% | |
| Han et al. [38] | South Korea | Retrospective | 2014-2020 | 328 | 1.3 | 59 (44-74) | - | I-II: 52%III-IV: 48% | 3-5: 41% | - | - | 14% | - | - | - | - | - | 18% | 11% | 7% | |
| Kim et al. [39] | South Korea | Prospective | 2017-2018 | 94 | 1.8 | 66 (24-85) | - | I-II: 47%III-IV: 53% | 3-5: 61% | R-CHOP | 35 (23-47) | 10% | 6% | 3% | - | - | - | 17% | 12% | 5% | |
| Okamoto et al. [40] | Japan | Retrospective | 2012-2018 | 221 | 1.6 | 72 (26-97) | - | I-II: 42%III-IV: 58% | Poor R-IPI 53% | R-CHOP or R-CHOP-like 83% | 31 (N=184 subcohort R-CHOP or R-CHOP-like) | 8% | - | - | 12% | - | - | - | - | - | |
| Lim et al. [41] | South Korea | Retrospective | 2009-2014 | 512 | 1.2 | 57 (47-67) | - | I-II: 56%III-IV: 44% | 3-5: 32% | R-CHOP | 52 (1-127) | 12% (bilateral) | 11% | 1% | - | - | - | 13% | 8% | 2% | |
| 2% heterogeneous | |||||||||||||||||||||
| Saiki et al. [42] | Japan | Retrospective | 2008-2017 | 84 | 1.2 | 70 (19-86) | - | I-II: 47%III-IV: 53% | - | Mostly R-CHOP | - | 26% | 19% | 7% | - | - | - | 19% | 8% | 11% | |
| Martin-Moro et al. [43] | Spain | Retrospective | 2013-2017 | 82 (38 PET data) | 1.2 | 63 (33-85) | GCB: 49%Non-GCB: 51% | I-II: 50%III-IV: 50% | aaIPI 2-3: 41% | R-CHOP or R-CHOP-like | 33 (NR) | 13% | - | - | 24% | - | - | 16% | - | - | |
| Al-Sabbagh et al. [44] | Qatar | Retrospective | 2013-2017 | 89 | 2.6 | 48 (18-77) | - | I-II: 39%III-IV: 61% | - | - | - | 13% | - | - | - | - | - | 26% (focal and heterogeneous) | - | - | |
| Min et al. [45] | South Korea | Retrospective | 2009-2016 | 600 | 1.4 | 59 (17-88) | GCB: 36%Non-GCB: 64% | I-II: 44%III-IV: 56% | 3-5: 50% | R-CHOP | 50 (0.2-123) | 15%(bilateral) | - | - | - | - | - | 16% | 10% | 3% | |
| Both 3% | |||||||||||||||||||||
| Kandeel et al. [46] | Egypt | Retrospective | 2015-2018 | 88 | 0.7 | 50 (21-70) | GCB: 43%Non-GCB: 57% | I-II: 14%III-IV: 86% | - | Mostly R-CHOP | 11 (2-20) | 25% | - | - | - | - | - | - | 30% | - | |
| Alonso-Alvarez et al. [47] | Spain | Retrospective | 1999-2014 | 232 | 1 | 66% >60yo | GCB: 37%Non-GCB: 63% | I-II: 29%III-IV: 71% | Poor R-IPI: 41% | 81% R-CHOP or R-CHOP-like | 58 (1-152) | 25% | 16% | 9% | 25% | 10% | 15% | - | - | - | |
| Wang et al. [48] | South Korea | Retrospective | 2011-2017 | 140 | 1.4 | 65 (22-86) | GCB: 9%Non-GCB: 91% | I-II: 0%III-IV: 100% | >3: 45% | R-CHOP | 49 (1-98) | 36%(bilateral) | - | - | - | - | - | - | 31% | - | |
| Greenbaum et al. [49] | Israel | Retrospective | 2005-2014 | 81 | 1.5 | 65 (23-87) | - | I-II: 38%III-IV: 62% | Median 3 | 91% R-CHOP | - | 26% | - | - | 63% | - | - | - | - | - | |
| Chen et al. [16] | China | Retrospective | 2007-2016 | 193 | 0.9 | 58 (14-87) | GCB: 32%Non-GCB:68% | I-II: 44%III-IV: 56% | 3-5: 43% | R-CHOP | 30 (12-124) | 7% | - | - | - | - | - | 24% | 15% | 9% | |
| Chen-Liang et al. [50] | Spain | Retrospective | 2007-2015 | 268 | 1 | 61 (18-85) | - | I-II: 25%III-IV: 75% | 3-5: 42% | 76% R-CHOP | 25 (1-91) | 13% | - | - | - | - | - | 22% | 17% | 6% | |
| Vishnu et al. [51] | USA | Retrospective | 2004-2013 | 99 | 1.7 | 62 (24-88) | - | - | Poor R-IPI: 24% | - | 91 (28-140) | 14% | - | - | - | - | - | 24% | - | - | |
| Alzahrani et al. [33] | Canada and Denmak | Retrospective | 2007-2013 | 530 | 1.2 | 65 (16-90) | - | I-II: 37%III-IV: 63% | 3-5: 43% | - | 24 (3-78) | 16% | 10% | 7% | - | - | - | - | 28% | - | |
| Liang et al. [52] | China | Retrospective | 2005-2014 | 169 | 1.3 | 55 (18-85) | GCB: 40%Non-GCB: 60% | I-II: 36%III-IV: 64% | 4-5: 17% | R-CHOP (60%) or DA-EPOCH-R (40%) | 38 (12-113) | 12% (some bilateral) | - | - | - | - | - | 21% | 20% | 2% | |
| Cerci et al. [20] | Brazil, Chile, Hungary, India, Italy, South Korea, Philippines, and Thailand | Prospetive | 2008-2011 | 327 | 1.1 | 55 (IQR 44-63) | - | I-II: 36%III-IV: 64% | 3-5: 34% | R-CHOP recommended | 35 (NR) | 11% | - | - | - | - | - | 26% | 21% | 6% | |
| Adams et al. [53] | The Netherlands | Retrospective | 2007-2013 | 78 | 1.2 | 69 (33-88) | - | I-II: 23%III-IV: 77% | NCCN-IPI >3: 71% | 91% R-CHOP | 28 (5-74) | 21% (3% undetermined) | 14% | 4% | - | - | - | 44% | 39% | 5% | |
| Arima et al. [54] | Japan | Retrospective | 2006-2011 | 96‡ | 1.5 | 69 (22-89) | - | I-II: 39%III-IV: 61% | 3-5: 52% | R-CHOP | 36 (1-72) | 20% | 15% | 5% | 28% | - | - | - | - | - | |
| Berthet et al. [10] | France | Retrospective | 2006-2011 | 133 | 1 | 57 (18-87) | - | I-II: 26%III-IV: 74% | 3-5: 40% | R-CHOP or R-CHOP-like | 24 (1-67) | 6% | 4% | 2% | - | - | - | 32% | 24% | 8% | |
| Khan et al. [35] | United Kingdom | Retrospective | 2005-2012 | 130 | 1.5 | 59 (22-87) | - | I-II: 45%III-IV: 55% | 3-5: 40% | 95% R-CHOP | - | 11% | 11% | 0% | - | - | - | 25% | 21.5% | 1.5% | |
| Both 2% | |||||||||||||||||||||
| Hong et al. [36] | South Korea | Retrospective | 2007-2011 | 89 | 0.8 | 59 (26-83) | GCB: 49%Non-GCB: 51% | I-II: 47%III-IV: 52% | Poor R-IPI: 35% | R-CHOP | 16 (NR) | 16%(bilateral) | 10% | 6% | - | - | - | 19% | 11% | 8% | |
| Cortes Romera et al. [55] | Spain | - | 2004-2010 | 84 | 1 | 63 (19-78) | - | I-II: 50%III-IV: 50% | - | R-CHOP | NR (9-34) | - | 19% | - | - | - | - | 29% | 23% | 6% | |
aa: age-adjusted; COO: cell-of-origin; DLBCL: diffuse large B-cell lymphoma; GCB: germinal center B; IPI: International Prognostic Index; IQR: interquartile range; NCCN: National Comprehensive Cancer Network; PET-FDG: positron emission tomography-fluorodeoxyglucose; R-IPI: revised IPI; Ref.: reference; yo: years old. * References are ordered according to the sequence obtained from the bibliographic search. †Taking into account cases with available data to calculate the percentages. ‡After excluding 21 cases with FCM not done.
Table 2.
Concordance analysis in DLBCL among BMB, FCM and PET in the assessment of BMi at diagnosis.
Table 2.
Concordance analysis in DLBCL among BMB, FCM and PET in the assessment of BMi at diagnosis.
| Ref. | Concordant results | Discordant results | Cohen’s kappa index | ||||||||||||
| BMB+/FCM+ | BMB+/PET+ | FCM+/PET+ | BMB-/FCM- | BMB-/PET- | FCM-/PET- | BMB+/FCM- | BMB+/PET- | BMB-/FCM+ | BMB-/PET+ | FCM+/PET- | FCM-/PET+ | BMB/FCM | BMB/PET | FCM/PET | |
| Bo et al. [37] | - | 16% (23% after second punction) | 14% (20% after second punction) | - | 71% | 72% | - | 5% | - | 10% (3% after second punction) | 4% | 12% (6% after second punction) | - | 0.59 (0.8 after second punction) | 0.54 (0.74 after second punction) |
| Han et al. [38] | - | 7% | - | - | 76% | - | - | 6% | - | 11% | - | - | - | 0.36* | - |
| Kim et al. [39] | - | 5% | - | - | 79% | - | - | 4% | - | 12% | - | - | - | 0.32* | - |
| Okamoto et al. [40] | 3% | - | - | 83% | - | - | 5% | - | 9% | - | - | - | 0.25 | - | - |
| Lim et al. [41] | - | 7% | - | - | 83% | - | - | 5% | - | 6% | - | - | - | 0.51* | - |
| Saiki et al. [42] | - | 10% | - | - | 64% | - | - | 17% | - | 10% | - | - | - | 0.26* | - |
| Martín-Moro et al. [43] | 13% | 5% | 8% | 76% | 79% | 71% | 0% | 5% | 15% | 11% | 13% | 8% | 0.65* | 0.31* | 0.30* |
| Al-Sabbagh et al. [44] | - | 12% | - | - | 73% | - | - | 1% | - | 13% | - | - | - | 0.55* | - |
| Min et al. [45] | - | 9% | - | - | 76% | - | - | 7% | - | 8% | - | - | - | 0.43* | - |
| Kandeel et al. [46] | - | 14% | - | - | 59% | - | - | 11% | - | 16% | - | - | - | 0.31* | - |
| Alonso-Alvarez et al. [47] | 18% | - | - | 69% | - | - | 6% | - | 7% | - | - | - | 0.65* | - | - |
| Wang et al. [48] | - | 21% | - | - | 54% | - | - | 14%† | - | 10% | - | - | - | 0.46* | - |
| Greenbaum et al. [49] | 26% | - | - | 37% | - | - | 0% | - | 37% | - | - | - | 0.4* | - | - |
| Chen et al. [16] | - | 7% | - | - | 76% | - | - | 1% | - | 17% | - | - | - | 0.36* | - |
| Chen-Liang et al. [50] | - | 9% | - | - | 74% | - | - | 4% | - | 13% | - | - | - | 0.41* | - |
| Vishnu et al. [51] | - | 12% | - | - | 74% | - | - | 2% | - | 12% | - | - | - | 0.55* | - |
| Alzahrani et al. [33] | - | 9% | - | - | 66% | - | - | 7% | - | 18% | - | - | - | 0.30* | - |
| Liang et al. [52] | - | 11% | - | - | 78% | - | - | 1% | - | 10% | - | - | - | 0.59* | - |
| Cerci et al. [20] | - | 8% | - | - | 71% | - | - | 3% | - | 19% | - | - | - | 0.31* | - |
| Adams et al. [53] | - | 14% | - | - | 50% | - | - | 6% | - | 29% | - | - | - | 0.22* | - |
| Arima et al. [54] | 18% | - | - | 70% | - | - | 2% | - | 10% | - | - | - | 0.66* | - | - |
| Berthet et al. [10] | - | 5% (4% subcohort PET focal) | - | - | 67% (74% subcohort PET focal) | - | - | 1% (2% subcohort PET focal) | - | 27% (20% subcohort PET focal) | - | - | - | 0.19* (0.23* subcohort PET focal) | - |
| Khan et al. [35] | - | 9% | - | - | 73% | - | - | 2% | - | 16% | - | - | - | 0.42* | - |
| Hong et al. [36] | - | 8% | - | - | 73% | - | - | 8% | - | 11% | - | - | - | 0.34* | - |
| Cortes Romera et al. [55] | - | 18% | - | - | 70% | - | - | 1% | - | 11% | - | - | - | 0.68* | - |
BMB: bone marrow biopsy; FCM: flow cytometry; PET: positron emission tomography; Ref.: reference. *Not reported, calculated according to data extracted from each study. †All cases presented a diffuse BM pattern by PET, considered as negative BMi by the authors.
Table 3.
Diagnostic accuracy of BMB and PET for detecting BMi at DLBCL diagnosis.
| Ref. | Definition of true positive BMi | Sensitivity (CI 95%) | Specificity (CI 95%) | Positive/Negative predictive value | Youden’s index / Diagnostic Accuracy | ||||||||
| BMB | PET | PET focal | BMB | PET | PET focal | BMB | PET | PET focal | BMB | PET | PET focal | ||
| Bo et al. [37] | After first direct BM study (BMB and FCM) | - | 62% (43-78) | - | - | 93% (86-97) | - | - | - | - | - | 0.55% (YI) | - |
| After second direct BM study (BMB and FCM) | - | 92% (76-98) | - | - | - | - | - | - | - | 0.86% (YI) | - | ||
| Lim et al. [41] | Billateral BMB | - | 59% (NR) | - | - | 94% | - | - | 55%/95% | - | - | 90% (DA) | - |
| Saiki et al. [42] | BMB | - | 36% (NR) | - | - | 87% (NR) | - | - | 50%/79% | - | - | - | - |
| Al-Sabbagh et al. [44] | BMBorPET + any of guided biopsy confirmation / MRI / focal uptake / FDG disappearance with treatment | 50% (29-71) | 96% (79-100) | - | 100% (94-100) | 100% (95-100) | - | 100%/84% | 100%/98% | - | 87% (DA) | 99% (DA) | - |
| Min et al. [45] | Billateral BMB | - | 52% | - | - | 91% | - | - | - | - | - | - | - |
| Kandeel et al. [46] | BMBorPET + any of concordant morphologic changes by CT / FDG disappearance with treatment / concordant FDG progression on follow-up | 69% (NR) | - | 67% (NR) | 100% (NR) | - | 90% (NR) | 100%/85% | - | 77%/84% | 89% (DA) | - | 82% (DA) |
| Chen et al. [16] | BMB or PET focal | 44% (NR) | 88% (NR) | - | - | - | - | NR/90% | NR/98% | - | 91% (DA) | 98% (DA) | - |
| Chen-Liang et al. [50] | BMB or PET | 40% (27-53) | 69% (52-85) | - | 95% (91-98) | 85% (80-89) | - | NR/85% | NR/95% | - | 83% (DA) / 0.4 (YI) | 83% (DA) / 0.5 (YI) | |
| Vishnu et al. [51] | BM aspirate and trephine biopsy | - | 86% (56-97) | - | - | 86% (76-92) | - | - | 50%/98% | - | - | 86% (DA) | |
| Alzahrani et al. [33] | BMB or PET | 48% (41-56) | - | 81% (74-86) | - | - | - | NR/79% | - | NR/91% | - | - | - |
| BMB | - | - | 60% (49-70) | - | - | 79% (75-83) | - | - | 36%/91% | - | - | - | |
| BMB concordant | - | - | 77% (63-87) | - | - | 79% (75-83) | - | - | 29%/97% | - | - | - | |
| PET focal | 36% (28-44) | - | - | 91% (88-94) | - | - | 60%/79% | - | - | - | - | - | |
| Berthet et al. [10] | BMBorPET focal + confirmed byguided biopsy / targeted MRI / after chemotherapy by concomitant disappearance of uptake | 24% (9-39) | - | 94% (86-100) | 100% (100-100) | - | 99% (97-100) | 100%/80% | - | 97%/98% | 81% (DA) | - | 98% (DA) |
| Khan et al. [35] | BMB or PET | 40% (NR) | 94% (NR) | - | 100% (NR) | 100% (NR) | - | NR | NR | - | 84% (DA) | 99% (DA) | - |
| Cortes Romera et al. [55] | BMB | - | 95% | - | - | 86% | - | - | 54%/99% | - | - | 87% (DA) | |
BM: bone marrow; BMB: bone marrow biopsy; CI: confidence interval; DA: Diagnostic Accuracy; FCM: flow cytometry; MRI: magnetic resonance imaging; NR: not reported; PET: positron emission tomography; Ref.: reference; YI: Youden’s index.
Table 4.
Prognostic impact of BMi at DLBCL diagnosis according to BMB, FCM and PET in comparative studies.
Table 4.
Prognostic impact of BMi at DLBCL diagnosis according to BMB, FCM and PET in comparative studies.
| Ref. | N | Adverse factor related to BM assessment (compared with its complementary good prognosis reference in each case) | Survival endpoints | ||||||
| Event-free survival or progression-free survival | Overall survival | ||||||||
| Prognosis | UV HR (CI 95%) | MV HR (CI 95%) | Prognosis | UV HR (CI 95%) | MV HR (CI 95%) | ||||
| Okamoto et al.* [40] | 184 (subcohort R-CHOP or R-CHOP-like) | BMB+ | 20% (2-year)C-index 0.68 | 4.3 (2.1-8.8) | 2.3 (1.3-6.5)1 | 24% (2-year)C-index 0.74 | 5.2 (2.6-10.5) | 3 (1.3-6.8)1 | |
| FCM+ | C-index 0.70 | 3.1 (1.6-5.8) | 2.8 (1.4-5.2)1 | C-index 0.74 | 2.2 (1.1-4.5) | 1.9 (0.9-3.7)1 | |||
| Lim et al.‡ [41] | 512 | BMB+ | - | 3.1 (1.8-5.4) | 1.7 (1.1-2.6)2 | 52% (2-year)37% (5-year) | - | - | |
| PET | PET+ | 29% (2-year) | 2.8 (1.6-4.7) | 1.7 (1.1-2.6)2 | - | - | - | ||
| PET+ focal | - | 2.1 (1.1-3.9) | - | - | - | - | |||
| PET+ diffuse | - | 3.1 (0.8-11) | - | - | - | - | |||
| PET+ heterogeneous | - | 4.2 (1-16.9) | - | - | - | - | |||
| Martin-Moro et al.* [43] | 82 | BMB+/FCM+ | 27% (18-month) | 2.2 (1.4-3.3) | - | 55% (18-month) | 1.9 (1.2-3) | - | |
| BMB-/FCM+ | 23% (18-month) | 4.9 (1.7-14.2) | - | 46% (18-month) | 4.4 (1.5-12.4) | - | |||
| FCM+ | - | 4.8 (2.3-10) | 1.9 (1.3-2.9)32 (1.3-3.1)4 | - | 3.8 (1.8-8.3) | 1.7 (1.1-2.7)31.7 (1.1-2.7)4 | |||
| Min et al.* [45] | 600 | BMB+ | - | - | - | 56% (4-year) | - | 1 (0.8-1.3)5 | |
| PET+ | 43% (4-year) | - | - | 65% (4-year) | - | - | |||
| Kandeel et al.• [46] | 88 | BMB+ | 64% (18-month) | 1.4 (0.5-3.5) | - | - | - | - | |
| PET+ focal | 73% (18-month) | 1 (0.4-2.5) | - | - | - | - | |||
| Alonso-Alvarez et al.* [47] | 189 (subcohort R-CHOP or R-CHOP-like) | Concordant | BMB+ concordant | 32% (5-year) | - | 2.2 (1.1-4.3)6 | 51% (5-year) | - | 1.6 (0.7-3.4)6 |
| BMB+ concordant GCB | 25% (5-year) | - | 2.9 (1-8.7)7 | 38% (5-year) | - | 1.2 (0.3-4.4)7 | |||
| BMB+ concordant non-GCB | 33% (5-year) | - | 3 (1.4-6.4)7 | 49% (5-year) | - | 1.6 (0.7-3.9)7 | |||
| Discordant | BMB/FCM+ discordant | 62% (5-year) | - | 1.5 (0.7-3)6 | 73% (5-year) | - | 1.5 (0.7-3.2)6 | ||
| BMB/FCM+ discordant GCB | 76% (5-year) | - | 0.7 (0.1-3)7 | 76% (5-year) | - | 0.7 (0.1-3.4)7 | |||
| BMB/FCM+ discordant non-GCB | 46% (5-year) | - | 1.9 (0.9-4.2)7 | 63% (5-year) | - | 1.6 (0.6-3.7)7 | |||
| Wang et al.† [48] | 140 (all cases advanced stage) | BMB+ | - | 2.3 (1.4-3.9) | 2.3 (1.4-3.9)8 | - | 1.7 (1-2.8) | Not significant8 | |
| PET+ focal | - | 2.1 (1.3-3.6) | Not significant8 | - | 1.8 (1.1-3) | 1.9 (1.1-3.1)8 | |||
| BMB+/PET+ | 7 months (median) | - | - | 12 months (median) | - | - | |||
| BMB+/PET- | 14 months (median) | - | - | 27 months (median) | - | - | |||
| BMB-/PET+ | 26 months (median) | - | - | 31 months (median) | - | - | |||
| Greenbaum et al.† [49] | 81 | BMB+/FCM+ | 67 months (median)47% (1-year)36% (5-year)24% (7-year) | - | - | 54 months (median)43% (1-year)32% (5-year)32% (7-year) | - | - | |
| BMB-/FCM+ | 77 months (median)61% (1-year)56% (5-year)49% (7-year) | - | - | 77 months (median)60% (1-year)55% (5-year)54% (7-year) | - | - | |||
| FCM+ | - | - | 2.6 (1-6.8)9 | - | - | 1.4 (0.7-3)9 | |||
| Chen et al.† [16] | 193 | BMB+ | 61% (3-year) | 1.8 (0.7-4.6) | - | 61% (3-year) | 4 (1.3-11.9) | - | |
| PET+ focal | 33% (3-year) | 4.4 (2.4-8.2) | 2.3 (1.1-4.7)10 | 69% (3-year) | 3.7 (1.5-9.3) | Not significant10 | |||
| PET+ diffuse | 81% (3-year) | 0.9 (0.3-2.4) | - | 94% (3-year) | 0.6 (0.1-4.3) | - | |||
| BMB-/PET+ focal | 0% (3-year) | - | - | 77% (3-year) | - | - | |||
| BMB-/PET+ diffuse | 90% (3-year) | - | - | 100% (3-year) | - | - | |||
| Chen-Liang et al.* [50] | 203 (subcohort R-CHOP) | BMB+ | - | P <0.001 | 3.6 (1.7-7.6)11 | - | P = 0.326 | ||
| PET+ | - | P = 0.121 | P >0.1511 | - | P = 0.018 | P >0.1511 | |||
| Vishnu et al. [51] | 99 (not reported treatment approach) | BMB+ | - | - | - | 65 months (median)80% (2-year)66% (5-year) | - | - | |
| PET+ | - | - | - | 67 months (median)83% (2-year)79% (5-year) | - | - | |||
| Alzahrani et al.* [33] | 256 (subcohort Ann Arbor IV) | BMB+ or PET+ | 57% (2-year) | - | - | 65% (2-year) | - | - | |
| PET+ | 53% (2-year) | - | - | 63% (2-year) | - | - | |||
| Liang et al.† [52] | 169 | BMB+ | - | 4.5 (2.5-8) | NS12 | - | 6.2 (3.1-12.7) | NS12 | |
| PET+ | - | 4 (2.3-6.6) | NS12 | - | 6.7 (3.4-13.3) | 2.9 (1.2-7)12 | |||
| 68 (subcohort Ann Arbor IV) | PET+ | 29% (3-year) | - | - | 44% (3-year) | - | - | ||
| Cerci et al.• [20] | 327 | BMB+ | 56% (2-year) | 2.2 (1.3-3.3) | - | 68% (2-year) | - | - | |
| BMB+/PET+ | 45% (2-year) | 2.7 (1.5-4.8) | 1.6 (0.8-3.1)13 | 55% (2-year) | 3.9 (1.9-8.1) | 2.3 (1-5)13 | |||
| BMB+/PET+ focal | 46% (2-year) | 2.5 (1.1-5.5) | - | 57% (2-year) | 3 (1.1-8.4) | - | |||
| BMB+/PET- | 80% (2-year) | - | 1.1 (0.4-3.2)13 | 100% (2-year) | - | 0.5 (0.1-3.7)13 | |||
| BMB-/PET+ | 81% (2-year) | - | 0.7 (0.4-1.3)13 | 88% (2-year) | - | 0.7 (0.3-1.7)13 | |||
| BMB-/PET+ focal | 78% (2-year) | - | - | 87% (2-year) | - | ||||
| Adams et al.* [53] | 71 (subcohort R-CHOP) | BMB+ | - | 3.2 (1.3-7.6) | 3.3 (1.3-8.6)14 | - | 3.5 (1.3-9.3) | 4.5 (1.6-12.4)14 | |
| PET+ | - | 0.9 (0.4-2.1) | - | - | 0.7 (0.3-2.2) | - | |||
| Berthet et al.* [10] | 133 | BMB+ | 38% (2-year) | 4.9 (1.6-14.6) | 2..2 (0.8-6)15 | 63% (2-year) | 4.1 (1.4-12.4) | 2.7 (0.9-8.2)15 | |
| PET+ | 63% (2-year) | 2.9 (1.2-7) | 2.5 (1.2-5.3)15 | 76% (2-year) | 2.8 (1.2-6.8) | 2.2 (0.9-5.3)15 | |||
| Khan et al.† [35] | 44 (subcohort Ann Arbor IV) | BMB+ | - | 3.7 (1.6-8.8) | - | - | 3.9 (1.5-10) | - | |
| PET+ | - | 0.8 (0.3-2) | - | - | 0.9 (0.3-2.5) | - | |||
| PET+/BMB- | - | 0.4 (0.1-1.2) | - | - | 0.4 (0.1-1.6) | - | |||
| Hong et al.* [36] | 89 | BMB+ | 37% (2-year) | - | - | 36% (2-year) | 7.9 (3.2-19.6) | 8.7 (3.2-23.5)16 | |
| PET+ | 63% (2-year) | - | - | 59% (2-year) | 2 (0.8-5.3) | - | |||
| BMB+/PET+ | 38% (2-year) | - | - | 38% (2-year) | - | - | |||
| BMB+/PET- | 36% (2-year) | - | - | 36% (2-year) | - | - | |||
| BMB-/PET+ | 79% (2-year) | - | - | 73% (2-year) | - | - | |||
BMB: bone marrow biopsy; BMi: bone marrow involvement; CI: confidence interval; COO: cell-of-origin; ECOG: Eastern Cooperative Oncology Group; FCM: flow cytometry; FDG: fluorodeoxyglucose; HR: hazard ratio; LDH: lactate dehydrogenase; NCCN: National Comprehensive Cancer Network; IPI: International Prognostic Index; MV: multivariate; PET: positron emission tomography; R-IPI: revised IPI; Ref.: reference; UV: univariate. Survival endpoint: *Event-free survival (EFS): time from diagnosis to first disease progression or relapse or death by any cause. †Progression-free survival (PFS): time from diagnosis to first disease progression or relapse. ‡Lymphoma specific survival (LSS): time from diagnosis to death caused by relapse/refractory disease or treatment-related complication of lymphoma. •Not reported de definition of EFS/PFS. Overall survival was defined as the time from diagnosis to death by any cause in all studies. Adverse variables reported as included in each multivariate analysis: 1 Adjusting for IPI factors: age, LDH, PS > 1, stage >II, and extranodal site. 2 Including: age >60, IPI 4-5, bulky, biopsy-confirmed BMI, and any pattern of FDG+ BM. 3 Including: FCM BMi, COO Hans, and IPI. 4 Including: FCM BMi, and IPI. 5 Including: age ≥60 years, Ann Arbor III-IV or II bulky, high LDH, ≥2 extranodal sites, ECOG 2-4, BMi by BMBx, COO Hans, and complex karyotype. 6 Including: R-IPI and concordant/discordant BMi. 7 Including: R-IPI and concordant/discordant BMi with COO. 8 Including: male sex, age, BMi by BMB, BMi by PET focal, Ann Arbor IV (vs III), IPI >3, and B symptoms. 9 Including: IPI, BMi by FCM, sex male, and hemoglobin. 10 Including: advanced stage and PET+ focal. 11 Including: male sex, age >60, ECOG >1, elevated beta-2 microglobulin, elevated LDH, BMi by PET, and BMi by BMB. 12 Including: BMi by BMB, BMi by PET, IPI >2, Ann Arbor III-IV, ECOG >1, elevated LDH, and extranodal >1. 13 Including: BMi by a combination of BMB and PET (BMB+/PET+, BMB+/PET- or BMB-/PET+, respectively), age >60 years, Ann Arbor III-IV, high LDH, ≥2 extranodal sites, ECOG 2-4, and omission of rituximab therapy. 14 Including: BMi by BMB, BMi by PET, metabolic parameters by PET, and high-risk NCCN-IPI. 15 Including: BMi by BMB and PET, age >60 years, Ann Arbor III-IV, high LDH, ≥2 extranodal sites, ECOG 2-4, and IPI >2. 16 Including: BMi by BMB, elevated LDH, Ann Arbor III-IV, ECOG >1, and extranodal >1.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



