
Submitted:
08 March 2024
Posted:
08 March 2024
You are already at the latest version
Abstract
Pseudomonas aeruginosa infections are the focus of new treatment alternatives due to their frequent development of resistance to antibiotics and formation of biofilms. Recently, emphasis has been placed on combinations of antibiotics with drugs used for different indications. In this study the combined effects of metformin with imipenem, ceftazidime, cefepime, ciprofloxacin and levofloxacin has been investigated. 50 P. aeruginosa isolates isolated from patients with cystic fibrosis come to Gaziantep University Microbiology Laboratory were included in the study. The susceptibilities of the isolates to antibiotics were investigated by the liquid microdilution method and the combined effect of metformin and antibiotics by the chequerboard synergy test. In our study, as a result of the chequerboard synergy test; synergy between ceftazidime and metformin 6%, partial synergistic 22% isolates; while no synergistic effect was detected between cefepime and metformin in any isolate, partially synergy 46%; synergy between imipenem and metformin 4%, partial synergy 10%; synergy between ciprofloxacin and metformin 6%, partial synergy 6%, antagonist effect 2%; synergy was detected between levofloxacin and metformin 2% and a partial synergy was detected 12%. This study shows that metformin could be a potential antibiotic in its current form or in different chemical forms to be produced synthetically.
Keywords:
antibiotic resistance
; chequerboard
; metformin
; pseudomonas aeruginosa
; synergy
1. Introduction
Pseudomonas aeruginosa is a gram-negative, rod-shaped, mobility bacterium that reproduces at temperatures between 37 and 42 °C. The cytochrome-oxydase enzyme is present and does not ferment lactose. It produces a blue-green-coloured pigment, pyocyanin, and a black and green pigment, pyoverdin. It is an opportunistic pathogen that can lead to blood-circulation infections, respiratory, urinary, bone and joint infections and skin and subcutaneous tissue infections [1,2,3]. P. aeruginosa is a common pathogen in environmental areas, but rarely colonizes in healthy people [4].
In the treatment of P. aeruginosa, penicillins such as piperasiline and tikarsiline, cephalosporins such as seftaidim and sefepim, aztreonam in the monobactam group, and carbapenems, imipenem (often used in conjunction with silastatin), meropenem and doripeneem are used [5]. Another group used in antipsedomonal therapy are fluoroquinolones, the most commonly used being ciprofloxacin and levofloxacine [6]. Amikacin, gentamicin, and tobramicin are aminoglycosites with antipsedomonal effects [7]. In the treatment of P. aeruginosa, which is resistant to commonly used antipsedomonal drugs, new antibiotics are used, such as seftalosan-tasobactam, seftasidim-avibaktam, imipenem-silastatin-relebactam and sefiderokol [8].
In P. aeruginosa infections, the main mechanisms that play a role in developing resistance (chromosomal) resistance to antimicrobials are acquired, including the production of enzymes that break down antibiotics such as beta-lactamase, including hyperexpressed exhaust pump and reduced external membrane permeability. As several of these resistance mechanisms often occur simultaneously, treatment options in drug-resistant P. aeruginosa isolates are very limited [3]. The most common mechanisms inducing intrinsic resistance in P. aeruginosa isolates are inducable AmpC (cephalosporinase) expression, exhaust pump hyperexpression, and low level external membrane permeability. The production of injectable beta-lactamase, along with cephalosporins, has resulted in reduced sensitivity to aminopenicillins and imipename [9]. The most commonly observed mutation-induced beta-lactam resistance mechanism in P. aeruginosa isolates is the overexpression of AmpC cephalosporinase [10]. Another common resistance mechanism is the excess expression of the exhaust pump. The expression of the MexAB-OprM exhaust pump leads to resistance to all beta-lactams, fluoroquinolones, tetracyclines, macrolytes, chloramphenicol and novobiosis, with the exception of imipenem, including aztreonam. MexXY-OprM and MexCD-OperJ exhaust pumps also show substrat specificity to other beta-lactam antibiotics, with the exception of beta-lactam antibodies such as aztreonam, imipenem and saftazidim [11,12].
To prevent increased antibiotic resistance, studies have been conducted showing synergies between metformin, antihistamines, anti-inflammatory drugs or neuroleptics and antibiotics [13,14,15]. Patients taking metformin due to diabetes have been shown to have fewer cases of infection [16]. Studies on the combination of metformin and different antibiotics have shown synergies between metformine and antibiotics [13,17].
P. aeruginosa can lead to serious infections and develop resistance to antibiotics used to treat the infections it causes, using different mechanisms. In this study, P. aeruginosa isolates were investigated using a chequerboard test for synergy between metformin and ceftazidime, cefepime, imipenem, ciprofloxacin and levofloxasin.
2. Results
The results of the liquid microdilution test of P. aeruginosa isolates included in our study showed that 31 isolates (62%) were resistant to ceftazidime, 37 isolates (74%), were resistant to cefepime, 48 isolates (96%) were resistant to imipenem, 30 isolates (60%) were resistant to ciprofloxacin, and 23 isolates (46%) were resistant to levofloxacin. No antibacterial effect of metformin alone has been detected in any of the tested dosage ranges.
The results of the chequerboard synergy test between ceftazidime and metformin showed a synergistic effect in three isolates (6%), a partial synergetic effect in 11 isolates (22%) and an indifferential effect in 36 isolates (72%) (Table 2) (Supplementary Table S1). Prior to combination with metformin, 19 isolates (38%) were sensitive to high doses of ceftazidine, while 26 isolates (52%) were highly sensitive after combination. (Table 3).
The results of the chequerboard synergy test between cefepime and metformin showed no synergistic effect on any isolate, partial synergic effect in 23 isolates (46%) and indifferential effect in 27 isolates (54%) (Table 2) (Supplementary Table S2). Prior to combination with metformin, 13 isolates (26%) were sensitive to high doses of cefepime; after combination, 23 isolates (46%) were susceptible to higher doses. (Table 3).
The results of the chequerboard synergy test between imipenem and metformin showed a synergistic effect in two isolates (%4), a partial synergetic effect in five (%10) and an indifferential effect in 43 isolates (%86) (Table 2)(Supplementary Table S3). Before combination with metformin, two isolates (%4) were sensitive to imipening at high doses; after combination, three (%6) isolates were found to be susceptible to imiphening at higher doses. (Table 3).
The results of the chequerboard synergy test between ciprofloxacin and metformin showed synergistic effect in three isolates (%6), partial synergies in three isolates (%6) and indifferential effect in 43 isolates (%84) and antagonism in one isolate (%2) (Table 2)(Supplementary Table S4). The only isolates with antagonist effect have been found to have a partial synergistic effect with cefepime and levofloxacin. Prior to combination with metformin, 20 isolates (40%) were sensitive to high doses of ciprofloxacin, while 23 isolates (46%) were highly sensitive after combination. (Table 3).
Based on the results of the dama board synergy test between levofloxacin and metformin, a synergistic effect was observed in one isolate (%2), a partial synergetic effect in six isolates (%12) and an indifferential effect in 43 isolates (%86) (Table 2) (Supplementary Table S5). Prior to combination with metformin, 27 isolates (54%) were sensitive to high doses of levofloxacin, while after combination, 29 isolates (58%) were susceptible to higher doses. (Table 3).
In our study, the value of MBC for antibiotics and metformin has also been investigated. The MBC value for metformin has not been studied since reproduction occurred in all stacks containing only metformine. After microdilution and chequerboard synergy testing for antibiotics and combinations of antibiotic and metformin, transition from non-microplate-reproducing pins to SBA, no reproduction was observed. Therefore, the MIC values determined by the microdilution method were also found to be equal to the MBC value.
3. Discussion
One of the most important health problems today is that microorganisms develop short-term resistance to the used antimicrobials [20]. Microorganisms that are resistant to antimicrobials have a high mortality and morbidity rate because of the very severe infections they cause [21]. The study investigated the presence of synergies between sephtazidim, sefepim, imipenem, ciprofloxacin and levofloxasin, commonly used in the treatment of P. aeruginosa infections, and metformin, a pathogen that can develop short-term resistance to antimicrobials.
In our study, no antibacterial effect was shown on any isolates in the tested dose ranges for metformin (512-8 μg/ml). In a study by Masadeh and ark.[11], the antibacterial effect of metformin was studied on strains of P. aeruginosa ATCC BAA-2114 and Staphylococcus aureus ATSC 33591 at concentrations of 500 μM or less, but no antibacteric effect was found on metformine alone. A study conducted by Zuo and ark.[23] with Streptococcus suis isolates found no inhibitory or bactericidal effect on metformin isolates.
In our study, the presence of synergies between metformin and septazidim, sefepim, imipenem, ciprofloxacin, and levofloxasin was studied on 50 P. aeruginosa isolates. A synergistic effect in three isolates for ceftazidime, a partial synergetic effect in 11 isolates; a synergic effect in zero isolate for cefepime, and a partial synergistic effect in 23 isolats; a synergic effect for imipenem in two isolates, a partial synergetic effect of five isolations; a synergic effect for ciprofloxacin in three isolates, a synergic effect on three izolates; and a synergic effect for levofloxase in one isolate and a partial synergic effect at six isolates were observed. There are studies in the literature that investigate the antibacterial synergic effects of metformin and various chemicals. The presence of synergies between metformin and levofloxacin, chloramphenicol, ampicillin, rifampicine and doxycycline was investigated by Masadeh and ark.[11] on the multi-drug-resistant P. aeruginosa ATCC BAA-2114 isolate and the methiciline-resistent S. aureus ATCC 33591 isolate. The study showed a synergistic effect on P. aeruginosa between metformin and all medicines. On S. aureus, all drugs except rifampicin have been found to have a synergistic effect with metformin. However, although synergies were found in this study, the antibiotic's MIC values were not resistant to high doses, a subcategory of the resistant category. In a study conducted by Wu and ark. [15] using metformin and silver ions (Ag+) on Enterococcus faecalis isolates, colonies were found to be fewer than when used alone. He and ark. [17] investigated synergies between metformin and Triton X-100 in the antibacterial effects of E. faecalis isolates. When metformin and Triton X-100 were combined, they were found to be well below the MIC values detected when used alone. Another study by Liu and ark. [16] investigated the synergic effects of metformin and tetracyclines on isolates of Escherichia coli that are resistant to tetracicline. When used in combination with metformin and doxycycline, the MIC values of doxycyline were found to decrease.
Studies in the literature have shown that metformin increases the antibacterial effectiveness of various antibiotics. And in our study, there are isolates that have detected synergy and partial synergy when metformin is combined with antibiotics. In the light of this information, metformin still retains its potential antibacterial properties. However, it is believed that different chemical modifications may be required to reveal the potential antibacterial effect of metformin. In addition, unlike other studies in the literature in our study, when antibiotics are combined with metformin, the number of isolates passing through high-dose sensitive profiles from resistant profiles has been investigated. Seven for ceftazidime (14%), 10 for cefepime (20%), one for imipenem (2%), three for ciprofloxacin (6%), and two for levofloxasin (4%), while the isolate was resistant before combination with metformin; it passed a high-dose sensitive profile when combined with antibiotics.
In our study, metformin has not been investigated by what mechanism or mechanisms it increases the effect of antibiotics. In the literature, studies investigating the antibacterial effectiveness of metformin have shown synergistic effects with antibiotics through similar mechanisms. A study that investigated the synergistic effect of metformin and tetracyclines on E. coli found that the dose of doxycycline in the bacterium increased after metformine was administered. The study showed that metformin interacts with the hydrophobic part of the phospholipid double layer of the bacterial cell membrane, increasing the permeability of the external membrane to antibiotics [16]. A study that measured the effectiveness of metformin and Ag+ ions on E. faecalis isolates also showed that metformine increases cell membrane permeability, leading to the accumulation of Ag+ ion in the cell [15]. Although it is unclear exactly by what mechanism or mechanisms metformin increases the effectiveness of antibiotics, it is generally accepted that it increases intra-cellular antibacterial concentration by disrupting the external membrane of the bacterium [11].
The most important mechanisms that contribute to antibiotic resistance on P. aeruginosa isolates, primarily the beta-lactam group antibiotics and fluoroquinolones, are the inhibition of antibiotic penetration into the bacteria, causing changes in the structure of the outer membrane, and the exhaust pump that the bacterium has [6,9,23]. In the light of this information, the synergy test with metformin and various antibiotics on the P. aeruginosa isolates included in our study suggests that the isolates have different characteristic structures, such as synergistic, partial synergetic or indifferential effects. In isolates with a synergistic effect with metformin, the outer membrane of the bacterium was degraded on the metformine side, allowing the antibiotic to pass into the bacteria at sufficient concentrations; in isolates without a synergies effect, the antibiotic concentration in the bacteries did not increase even after the application of the external membrane.
It is also noted that the contribution of the exhaust pump to imipenem resistance at the head of the mechanisms that most commonly play a role in the resistance of beta-lactam antibiotics on P. aeruginosa isolates is very limited [10]. Our study also found that the antibiotic with the least synergy between metformin and beta-lactam antibiotics is imipenem (two synergies, five partial synergies). This suggests that the passage of imipenem bacteria through the outer membrane will not make a major contribution to immunodeficiency. This finding is also consistent with studies in the literature where the mechanism of action of metformin increases bacterial external membrane permeability.
In our study, the cytotoxic effect of metformin alone or in combination with antibiotics has not been investigated. In one study, the reliability of metformin was measured by treating it with mammary VERO cells. As a result of the study, even cells treated with high doses of metformin retained their vitality and were found to be quite safe for mammal cells [11]. Another study investigated the cytotoxic effect of metformin on cells, but no significant cytotoxin effect was observed. Another study, in which the synergy between metformin and Triton X-100 was investigated, investigated the cytotoxicity of metformine, and found no significant cytotoxin in the control group [17]. Another study using Ag+ and metformin on E. faecalis isolates found no significant difference in cell proliferation from the control group to the metformine-treated group [15]. Although the toxicity of metformin has not been investigated in our study, studies in the literature have not found a significant cytotoxic effect of metformine. These findings suggest that if metformin has a synergistic effect with antibiotics, it can be used safely.
In this study, various studies have investigated the synergic effect of metformin, which is described as a potential antibiotic, with various antibiotics. Electron microscopic examination or molecular tests to clarify the mechanism of action of metformin have not been carried out. The lack of research into the cytotoxic effect of metformin alone or in combination with the tested antibiotics is also a shortcoming of our study.
As a result, in our study, synergy and partial synergy between metformin and antibiotics have been observed on some isolates. It is believed that chemical modifications on metformin, even if not in its present form, could increase its antibacterial activity. Therefore, further research is needed to investigate the antibacterial effectiveness of metformin, with its present form and various chemical modifications to be produced synthetically. Furthermore, more extensive studies need to be undertaken to clarify the genotypic and phenotypic differences between the mechanism or mechanisms by which metphromine increases the effectiveness of antibiotics, the isolations that are effective, and the isolates that are not, the issues of whether it produces a cytotoxic effect when used in conjunction with antibiotics and the pharmacokinetic and pharmacodynamic effects that we will encounter if used in animals.
4. Materials and Methods
4.1. Selection and Revitalization of Isolates
The study included 50 P. aeruginosa isolates from clinical samples stored in skim milk feed at -20°C as archival material. The isolates were incubated at 37°C for 16-24 hours by planting 5% sheep blood agara (SBA) (BD, United States).
4.2. Determining the MIC Value for Metformin and Antibiotics and Investigating the Existence of Synergy Between Metformin and Antibiotics
Stock solutions have been prepared for the manufacturers' recommendations of metformin (Biosynth, United States) and sefepim (Biosynth, United States), seftazidim (BioSyneth, United State), imipenem (Biosynth, United States), ciprofloxacin (Biosynth, United States) and levofloxacin (Biosynth, United States), as the lyofilized forms are supplied. Because the antibiotics will be twice diluted, the antibiotic stock solution will be prepared to double the maximum concentration to be tested; and because metformin will be diluted four times, the metformine stock solution has been prepared in a way that will be four times the highest concentration tested. The drug concentrations and studied dosage ranges of antibiotics and metformin stock solutions are shown in Table 1. For the liquid microdistribution test, the cation-adjustable Müller-Hinton Broth (MHB) (BD, United States) dehydrate diet was prepared in accordance with the manufacturer's recommendations.
A chequerboard synergy test was performed to determine the presence of synergies between metformin and antibiotics. 100 μL of MHB was added to all ponds in a sterile U-based microplate. Subsequently, 100 μL metformin was added to all hives in the first order in the horizontal direction of the microplate, and the other hives were diluted in the vertical direction to exclude the last hive. A 100 μL antibiotic solution was then added to the first row of the microplate in the vertical direction, and a series dilution was done in the horizontal direction to exclude the last rows. The schematic representation of the study is shown in Figure 1.
A bacterial suspension of 0.5 McFarland (108 bacteria/ml) was then prepared from pre-animated P. aeruginosa isolates. The prepared suspension was diluted by 1/10 and added to all pins in the suspension microplate at a volume of 5 μl. The final bacterial concentration in the hooks was 5x105 bacteria/ml. The prepared microplate was incubated for 16 to 24 hours. The incubation resulted in bacterial reproduction of clums that were blurred, while non-blurred clums showed no reproduction. The MIC values obtained were interpreted according to the EUCAST table of clinical limit values [18].
In order to interpret the results of the Chequerboard synergy test, Index of fractional inhibitor concentration (FICI) was calculated using the following formula:
FICI= [MIC value of the combined antibiotic/MIC values of the antibiotic]+[MIC value of combined metformin/ MIC values of the metformine]
The FICI values were also interpreted according to the following equations:
- FICI ≤ 0,5 is a synergistic effect,
- FICI > 0.5 to ≤ 1 is a partial synergetic effect, ·
- FICI 1 > to ≥ 4 is an additive or indifferential effect, and
- FICI > 4 an antagonistic effect [19].
The calculations determined the potency of the potential synergistic effect between antibiotics and metformin.
4.3. Determination of the Minimum Bactericidal Concentration Value for Metformin and Antibiotics
For the determination of minimum bactericidal concentration (MBC) for metformin and antibiotics, samples taken with a sterile sample from stacks that were not present in the microplectal reproduction assessed during the synergy test were passed to 5% SBA. It was assessed whether a colony was formed during the incubation period of 16-24 hours.
5. Conclusions
In conclusion, metformin still maintains its potential antibacterial effect. In order to reveal this effect, it may be appropriate to synthesize synthetic derivatives by making appropriate modifications on the molecule. Although metformin maintains its potential antibacterial effect, further studies and animal experiments are required to clearly demonstrate the pharmacodynamic and pharmacokinetic effects of its use for antibacterial purposes, alone or in combination.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, K.Ç. and Y.Z.; methodology, K.Ç. and Y.Z.; software, K.Ç.; validation, K.Ç. and Y.Z.; formal analysis, K.Ç.; investigation, Y.Z.; resources, K.Ç., G.K.Ö. and E.K.K.; data curation, G.K.Ö.; writing—original draft preparation, K.Ç. and E.K.K.; writing—review and editing, K.Ç. and G.K.Ö.; visualization, K.Ç.; supervision, Y.Z.; project administration, K.Ç., Y.Z., G.K.Ö. and E.K.K.; funding acquisition, Y.Z. All authors have read and agreed to the published version of the manuscript.
Funding
The study was carried out with the support of Gaziantep University Scientific Research Projects No. TF.UT.22.79.
Institutional Review Board Statement
This study is conducted in accordance with the Declaration of Helsinki. Before the study, ethics committee approval was received from Gaziantep University Clinical Research Ethics Committee unit with the date 28/09/2022 and decision number 2022/324.
Informed Consent Statement
Since this study was conducted in-vitro, volunteer participation and consent are not required.
Data Availability Statement
The data obtained in this study are presented in supplementary tables. No ready-made data was used.
Acknowledgments
We would like to thank Dr Deniz Gazel and Mustafa Işık for their technical support during the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Brindhadevi K, LewisOscar F, Mylonakis E, Shanmugam S, Verma TN, Pugazhendhi A. Biofilm and Quorum sensing mediated pathogenicity in Pseudomonas aeruginosa. Process Biochem. 2020;96:49-57.
- Chadha J, Harjai K, Chhibber S. Revisiting the virulence hallmarks of Pseudomonas aeruginosa: a chronicle through the perspective of quorum sensing. Environ. Microbiol.. 2022;24(6):2630-56.
- Pachori P, Gothalwal R, Gandhi P. Emergence of antibiotic resistance Pseudomonas aeruginosa in intensive care unit; a critical review. Genes Dis. 2019;6(2):109-19.
- Pang Z, Raudonis R, Glick BR, Lin T-J, Cheng Z. Antibiotic resistance in Pseudomonas aeruginosa: mechanisms and alternative therapeutic strategies. Biotechnol. Adv.. 2019;37(1):177-92.
- Glen, K. A. , & Lamont, I. L. (2021). β-lactam resistance in Pseudomonas aeruginosa: Current status, future prospects. Pathogens, 10(12), 1638.
- Zhao L, Wang S, Li X, He X, Jian L. Development of in vitro resistance to fluoroquinolones in Pseudomonas aeruginosa. Antimicrob Resist Infect Control. 2020;9(1):1-8.
- Thacharodi, A. , & Lamont, I. L. (2022). Aminoglycoside-modifying enzymes are sufficient to make Pseudomonas aeruginosa clinically resistant to key antibiotics. Antibiotics, 11(7), 884.
- Reynolds D, Kollef M. The epidemiology and pathogenesis and treatment of Pseudomonas aeruginosa infections: an update. Drugs. 2021;81(18):2117-31.
- Horcajada JP, Montero M, Oliver A, Sorlí L, Luque S, Gómez-Zorrilla S, et al. Epidemiology and treatment of multidrug-resistant and extensively drug-resistant Pseudomonas aeruginosa infections. Clin. Microbiol. Rev.. 2019;32(4):e00031-19.
- Moya B, Dötsch A, Juan C, Blázquez J, Zamorano L, Haussler S, et al. β-Lactam resistance response triggered by inactivation of a nonessential penicillin-binding protein. PLoS pathogens. 2009;5(3):e1000353.
- Masadeh MM, Alzoubi KH, Masadeh MM, Aburashed ZO. Metformin as a potential adjuvant antimicrobial agent against multidrug resistant bacteria. Clin. Pharmacol.: Adv. Appl. 2021:83-90.
- Opal, SM. Non-antibiotic treatments for bacterial diseases in an era of progressive antibiotic resistance. Springer; 2016. p. 1-3.
- Dastidar SG, Saha P, Sanyamat B, Chakrabarty A. Antibacterial activity of ambodryl and benadryl. J. appl. bacteriol. 1976;41(2):209-14.
- Duncan AI, Koch CG, Xu M, Manlapaz M, Batdorf B, Pitas G, et al. Recent metformin ingestion does not increase in-hospital morbidity or mortality after cardiac surgery. Anesth. Analg. 2007;104(1):42-50.
- Wu X, Fan W, Fan B. Synergistic effects of silver ions and metformin against Enterococcus faecalis under high-glucose conditions in vitro. BMC Microbiol. 2021;21(1):1-9.
- Liu Y, Jia Y, Yang K, Li R, Xiao X, Zhu K, et al. Metformin restores tetracyclines susceptibility against multidrug resistant bacteria. Adv. Sci. 2020;7(12):1902227.
- He X, Jin S, Fan W, Fan B. Synergistic In vitro Antimicrobial Activity of Triton X-100 and Metformin against Enterococcus faecalis in Normal and High-Glucose Conditions. Microorganisms. 2022;10(1):124.
- "The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 13.1, 2023. http://www.eucast.org.
- Adaleti R, Nakipoğlu Y, Arıcı N, Kansak N, Çalık Ş, Şenbayrak S, et al. Evaluation of In vitro Efficacy of Meropenem/Colistin and Meropenem/Fosfomycin Combinations on Multidrug Resistant Gram-Negative Bacilli. Mikrobiyol Bul. 2023;57(3):365-77.
- Defoirdt, T. Quorum-sensing systems as targets for antivirulence therapy. Trends Microbiol. 2018;26(4):313-28.
- Prestinaci F, Pezzotti P, Pantosti A. Antimicrobial resistance: a global multifaceted phenomenon. Pathog Glob Health. 2015;109(7):309-18.
- Opal, SM. Non-antibiotic treatments for bacterial diseases in an era of progressive antibiotic resistance. Springer; 2016. p. 1-3.
- Zuo J, Shen Y, Wang H, Gao S, Yuan S, Song D, et al. Effects of metformin on Streptococcus suis LuxS/AI-2 quorum sensing system and biofilm formation. Microb. Pathog. 2023:106183.
- López-Causapé C, Sommer LM, Cabot G, Rubio R, Ocampo-Sosa AA, Johansen HK, et al. Evolution of the Pseudomonas aeruginosa mutational resistome in an international cystic fibrosis clone. Sci. Rep. 2017;7(1):5555.
Figure 1.
Schematic representation of checkerboard synergy testing application.
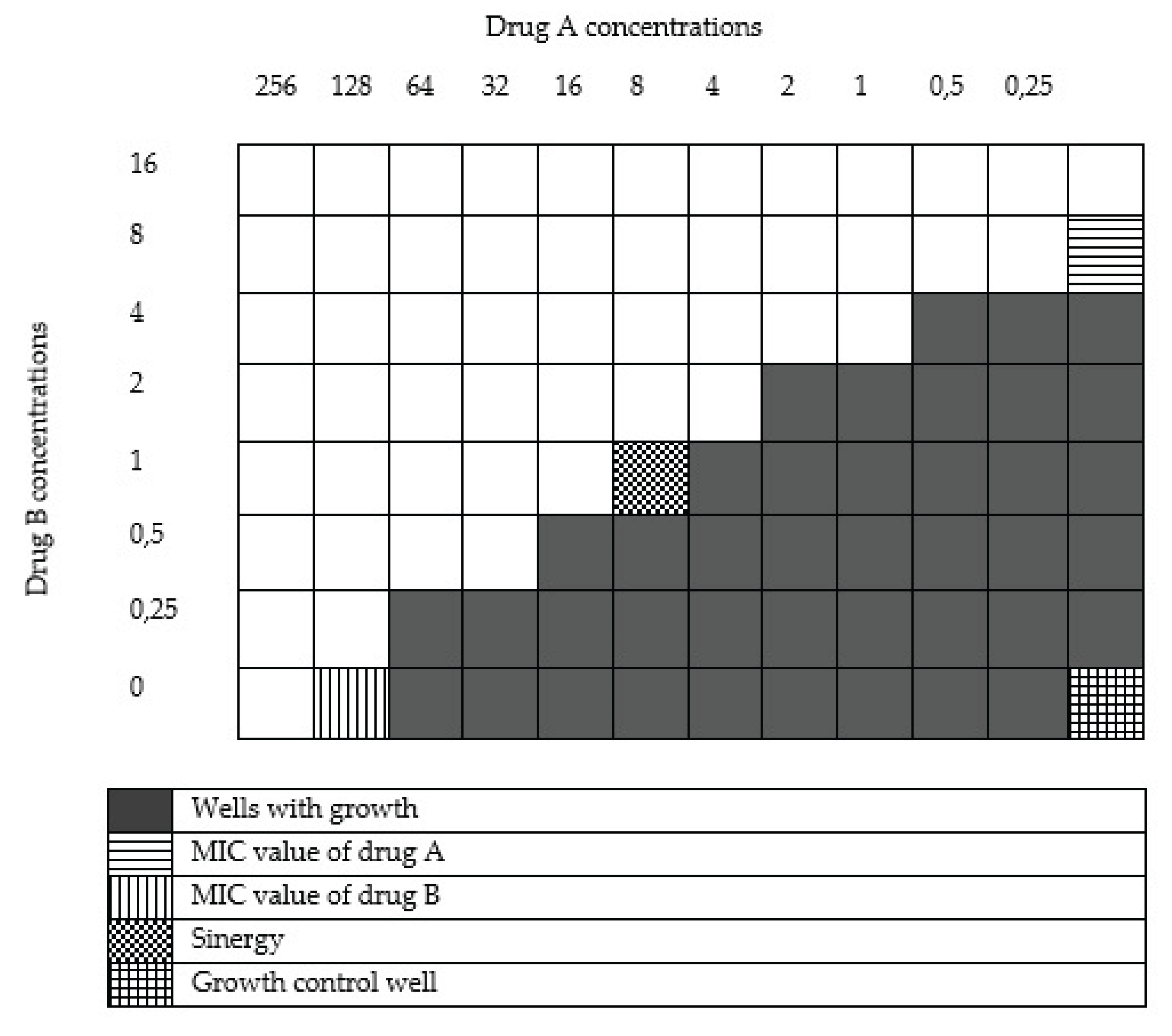

Table 2.
Synergistic effects of metformin and antibiotics against isolates.
| Antibiyotik | Sinergy N (%) | Partial sinergy N (%) | Undifferentiated N (%) | Antagonist N (%) |
|---|---|---|---|---|
| Ceftazidime | 3/50 (% 6) | 11/50 (% 22) | 36/50 (% 72) | 0/50 (% 0) |
| Cefepime | 0/50 (% 0) | 23/50 (% 46) | 27/50 (% 54) | 0/50 (% 0) |
| İmipenem | 2/50 (% 4) | 5/50 (% 10) | 43/50 (% 86) | 0/50 (% 0) |
| Ciprofloxacin | 3/50 (% 6) | 3/50 (% 6) | 43/50 (% 86) | 1/50 (% 2) |
| Levofloxacin | 1/50 (% 2) | 6/50 (% 12) | 43/50 (% 86) | 0/50 (% 0) |
Table 3.
Change in antibiotic susceptibility profiles of isolates when antibiotics alone were used and when metformin and antibiotics were combined.
Table 3.
Change in antibiotic susceptibility profiles of isolates when antibiotics alone were used and when metformin and antibiotics were combined.
| Antibiotic | Isolates found to be sensitive to high doses only when antibiotics were administered N (%) | Isolates found to be sensitive to high doses when antibiotics and metformin are combined N (%) | Isolates whose resistance profile changed positively when combined with the antibiotic metformin N (%) |
|---|---|---|---|
| Ceftazidime | 19/50 (% 38) | 26/50 (% 52) | 7 (% 14) |
| Cefepime | 13/50 (% 26) | 23/50 (% 46) | 10 (%20) |
| İmipenem | 2/50 (% 4) | 3/50 (% 6) | 1 (% 2) |
| Ciprofloxacin | 20/50 (% 40) | 23/50 (% 46) | 3 (% 6) |
| Levofloxasin | 27/50 (% 54) | 29/50 (% 58) | 2 (% 4) |
MİC: minimum inhibitory concentration.
Table 1.
Stock solution concentrations of metformin and antibiotics to be prepared and dose ranges to be studied in sensitivity testing and checkerboard synergy testing.
Table 1.
Stock solution concentrations of metformin and antibiotics to be prepared and dose ranges to be studied in sensitivity testing and checkerboard synergy testing.
| Antibiotic name | Stock solution concentration (µg/mL) | Dose ranges to be tested (µg/mL) |
|---|---|---|
| Cefepime | 640 | 320-0.3 |
| Ceftasidime | 640 | 320-0,3 |
| İmipenem | 320 | 160-0.15 |
| Ciprofloxacin | 32 | 16-0.015 |
| Levofloxacin | 32 | 16-0,015 |
| Metformin | 2048 | 512-8 |
µg/ml: microgram/milliliter.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



