
Submitted:
08 March 2024
Posted:
08 March 2024
You are already at the latest version
Abstract
Severe malaria is a major public health concern in Angola, particularly among adults, with limited data on clinical outcomes and manifestations. The study therefore assessed the clinical manifestations and outcome of severe Plasmodium falciparum malaria in adult patients admitted to Hospital Central Dr. António Agostinho Neto of Lubango, Angola. The study retrospectively reviewed the individual records of patients over 14 years old, admitted for severe malaria during the first trimester of 2021 and 2022. World Health Organization (WHO) criteria were used to define severity. A total of 640 patients were recorded into the study, 167 in 2021 and 473 in 2022, distributed across the departments; Intensive Care Unit (ICU; n=81), Medicine (MED; n=458) and Infectiology (INF; n=101). The median age was 26 years and 59.4% were males. The most common manifestation of severe malaria was renal impairment (37.4%). The overall mortality rate was 7% and decreased considerably from 10.2% in 2021 to 5.9% in 2022. The increase in malaria cases during 2022 with increased in prevalence of life-threatening signs like renal impairment, jaundice and impaired conscience, underscores the urgent need for enhanced malaria control and surveillance strategies to mitigate morbidity and mortality, highlighting the potential for antimalarial drug resistance.
Keywords:
Severe malaria
; Angola
; Plasmodium falciparum
; Renal impairment
; Impaired conscience
1. Introduction
In 2022, nearly half of the world’s population was still at risk of malaria. An estimated 249 million cases occurred and 608000 people died of malaria, 95% of the disease cases and 96% of deaths occur in WHO African Region [1]. Angola ranked fifth and seventh among African countries in malaria cases and deaths, respectively [1]. There are significant differences in the disease incidence across Angola provinces [2]. In the country malaria burden is divided into three distinct zones: high transmission year-round in the north, mesoendemic in the center, and seasonal malaria (unstable) in the south [3]. Malaria symptoms are non-specific, and clinical diagnostic relies mostly on the basis of fever or a history of fever. Severe malaria is defined as malaria with a significantly increased risk of death compared to others in the community with the illness (uncomplicated malaria) [4,5]. More than 90% of severe malaria cases are caused by Plasmodium falciparum [4]. The definition of severe malaria is based on clinical and laboratory findings, with some criteria including: impaired consciousness, prostration, acidosis, hypoglycaemia, severe anemia, renal impairment, jaundice, pulmonary oedema, significant bleeding, shock, and hyperparasitaemia [4,5].
In low endemic regions, such as Huíla province (capital city Lubango) [2,3], severe malaria is common in young adults. Lower exposure to the disease leads to a lower immunity, possibly making them more susceptible to sever malaria [6,7]. Despite the severity and impact of the disease, there are few published case studies of severe malaria in adults, particularly in lower endemic areas [8,9].
The purpose of this study was to describe the clinical aspects on admission and clinical outcome, of severe malaria patients admitted to Hospital Central Dr. António Agostinho Neto of Lubango (hereafter designated HCL), Angola at the departments of Intensive Care Unit (ICU), Infectiology (INF) and Internal Medicine (MED).
2. Materials and Methods
2.1. Study Site
In order to capture the peak of malaria transmission in the Province of Huíla, Angola, a retrospective descriptive hospital-based study was carried out at HCL, located in Lubango, the capital of the Huíla province (Figure 1). HCL is a level 3 health care unit and one of the largest hospitals in southern Angola. It serves the population of entire Huíla province, as well as the population of the neighboring provinces of Namibe and Cunene. The hospital provides over 70000 medical consultations/year (including external consultations).
2.2. Patients
This study was based on individual patient records (including socio-demographic information, presenting signs and symptoms, laboratory examinations, and outcome), admitted to HCL from January to March 2021 and 2022 at the departments of Internal Medicine (MED), Infectiology (INF) and Intensive Care Unit (ICU). The following criteria were used for inclusion in the study: patients of all genders, with at least 14 years of age; laboratory confirmed diagnosis of P. falciparum infection through a rapid diagnostic test (RDT) or a positive blood smear. For epidemiological purposes, severe malaria was defined according to World Health Organization [4], by the following criteria: impaired consciousness, prostration, multiple convulsions, hypoglycaemia, anemia, renal impairment, jaundice, pulmonary oedema, significant bleeding, shock, hyperparasitaemia, metabolic acidosis (criteria detailed in Supplementary Material) [4].
2.3. Statistical Analysis
Data collection and construction of the study database were conducted by a medical doctor and a nurse (both with professional clarence to consult individual patient records), registered in a Microsoft Excel Database and analyzed using GraphPad Prism Software version 8 for Windows (GraphPad Software). The comparison of categorical variables was carried out through the application of the Chi-square test and linear relationship between two variables measured using Pearson correlation.
2.4. Research Ethics
The study was approved by the Hospital Central Dr. António Agostinho Neto (HCL) institutional ethics review committee (Proc. nº 02/2023).
3. Results
3.1. Characteristics of patients
This is retrospective study performed in adult patients with severe malaria hospitalized at HCL between January and March 2021 and the same period in 2022. Nevertheless, regardless of whether they meet the severe malaria criteria (Supplementary Material), the attending clinician should provide the best care possible to patients identified as having an elevated risk to progress to severe malaria.
Of the 640 patients admitted to this study, 93.3% were confirmed infected with P. falciparum on thick blood film and 6.7% positive rapid diagnostic test (RDT) alone. Eighty-one 81/640 (12.7%) were admitted to the ICU, 101/640 (15.8%) to INF and 458/640 (71.5%) admitted to MED. January was the month with the highest number of hospitalizations both in 2021 and 2022 (Table S1 of Supplementary Material).
The ratio of female:male for ICU for both years was 1:4 and infectiology (INF) in 2022 where the ratio was 3:7 (Table 1). Recognizing the potential impact of age on malaria-related mortality [10], the patients were divided into three different groups 14-18 (young), 18-60 (adults) and 60 years (seniors) [8,10]. This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
The median age of the patients was 26 years (mean 30.3± 14.7), and the population ranged from 14 to 88 years. The majority of the patients, 81%, were between the ages of 18 and 59, patients <18 years accounting for 13% of the study population and seniors (60 years) accounting for 6% (Table 1). On average, patients were admitted to HCL, 4.4 days (± 2.1 days) after the onset of symptoms (as reported by the patient). Following HCL established guidelines (in accordance WHO), the predominant therapeutic approach chosen for the majority of patients was intravenously administration of artesunate [4].
3.2. Clinical manifestations of severe malaria patients
Table 640. patients admitted to this study tested positive for P. falciparum and meet one or more of the severe malaria criteria [4]. Pulmonary oedema was not observed in any of the enrolled patients. The absence of patients presenting multiple convulsions, active bleeding, impaired conscientiousness, or shock admitted to INF during 2021, is probably due to the fact that fewer patients were admitted to this department as compared to 2022. Acidosis was observed in 28.6% of patients admitted to MED in 2021 on the other hand in 2022 none of the patients observed at MED presented with acidosis. At INF none of the observed patients presented acidosis. Overall, manifestations of severe malaria were, as expected, less frequent in patients admitted to MED and INF than in ICU. Nevertheless, some of the patients admitted to MED and INF, presented critical signs such as impaired conscience or active bleeding (Figure 2). The most prevalent sign of severe malaria was renal impairment, registered in 37.4% of patients. During 2021, more than 56% of the patients at ICU suffered from renal impairment. In 2022, despite the rise in the total number of patients, the incidence of renal impairment further increased to 78.2%. Renal impairment was also notably high (>20%) among those admitted to MED and INF during both years (Figure 2). Jaundice was the second most prevalent (28.9%) manifestation overall.
Amongst ICU patients, the most common clinical features at presentation were acidosis and impaired consciousness (median GCS = 10, min. 4 and 25% of the patients had GCS 8; Figure 3). We used the Sequential Organ Failure Assessment (SOFA) as a measure of severity of disease amongst patients admitted to the ICU, the median SOFA was 11 (min. 4; max. 21). The median SOFA score was higher in 2022 (11.0, min. 6; max. 21) than 2021 (10.5, min. 4 max. 18), though the difference did not reach statistical significance (t test p=0.8325; Figure 3). SOFA scores were not significantly different between patients that had a positive (survival) or negative outcome (died due to severe malaria), however the median SOFA of those with negative outcome was higher (median = 12, min. 7 max. 21; p=0.3175) than those with positive outcome (median = 10.5, min. 4 max. 15; Figure 3). Severity of the disease, as measured by SOFA, does not seem to impact the length of hospital stay (LOS), SOFA values do not correlate with LOS (LOS; Pearson correlation p=0.7681).
3.3. Clinical manifestations of severe malaria and outcome
During the period of this study 45 patients died from complications of severe malaria, 10.2% (17/167) in 2021 and 5.9% (28/473) in 2022. Of these, 44.4% of patients were female and 55.6% male and the average age was 28.9 ± 14.1 years (range from 14 to 85 years). We did not observed association between age and mortality rate in any of the age group. Detailed description of the clinical features of patients that died during the study period, is presented in Table S2 (Supplementary Material). The median LOS was 7 days in 2021 (min. 1, max. 52) and 8 days in 2022 (min. 1, max. 55). ICU had the highest mortality rate in both 2021 (38.5%) and 2022 (27.3%; Figure 4). None of the patients admitted to INF had a negative outcome during 2021 (2021 numbers are probably biased due to fewer patients had been admitted to INF during 2021 as compared to 2022; Figure 4). The ICU was the department with the majority of the fatalities in both years. There was an overall decrease in the mortality rate from 2021 (10.2%) to 2022 (5.9%) (Figure 4), though this difference did not reach significance (ICU p = 0.1308 and MED p > 0.9999).
Overall, 52.6% of the patients that died, had acidosis at admission and 76.7% presented renal impairment (Supplementary Table S2) and impaired consciousness came as the third most common (42%) sign. Renal impairment, impaired consciousness and jaundice emerged as the most commonly observed clinical features amongst patients that died, and prevalence increased from one year to the next (Figure 5A). Overall, the median parasite density was below 500,000 parasites/µL (Figure 5B).
Patients with negative outcome, presented higher values of creatinine and bilirubin in 2022 (median 2.62, min. 0.86 max. 20.00 and median 3.04 min. 0.40 max. 31.46 respectively) than in 2021 (median 1.63 min.0.66 max. 20.00 and median 2.14 min. 0.56 max. 11.79 respectively) (Figure 5C/6D). Impaired conscience (cerebral malaria, unarousable coma with GCS <11) [11] was registered in 29.4% of patients admitted during 2021 (median GCS = 11, min. 4) and in 50% during 2022 (median GCS = 10, min.4; Figure 5E). All patients admitted to the MED with a negative outcome, presented a GSC >11 (ranging from 12-15) at admission. At INF the two patients that died (during 2022) presented GCS of 6 and 15 on admission. There was no significant relationship between death and cerebral malaria (impaired consciousness with GSC<11) at admission. Nevertheless 42.2% of the patients who died presented GCS<11 on admission.
4. Discussion
This study provides an overview of the clinical characteristics observed in severe malaria patients at HCL (Lubango, Huíla province, Angola) during the peak months of January, February, and March in 2021 and 2022.
For the purpose of context, at that the Emergency Room (ER) of HCL mortality rate due to malaria rose 12.3% in 2022 as compared to the same period in the year 2021 (data relative to the first semester, according to HCL internal Official Report). These patients arrived at HCL ER in critical condition, exhibiting multiorgan failure and some of them requiring live saving hemodialysis. This surge in mortality has positioned malaria as the leading cause of death at the ER of HCL during the first half of 2022, surpassed only by stroke and pneumonia. Our study was conducted in order to shine some light to the profile of the patients arriving at the hospital and represents the first study of severe malaria systematic characterization in Angola (apart from one study with 101 patients; Antunes et al, 2020) [12].
From 2020 to 2021, amidst the coronavirus 19 (COVID-19) pandemic, malaria emerged as the sixth leading cause of mortality among the hospitalized patients admitted to HCL. Furthermore, in 2021, it remains the primary cause for medical consultations, indicating a notable rise in the fatality rate compared to 2020 (increasing from 2% to 4%). According to HCL internal Official Report, the number of cases of malaria had a notable surge, rising from 1640 in 2021 to 2273 in 2022. This might be due to the constrained availability of healthcare services and the heightened level of fear within the population regarding seeking medical help [13]. Also decreased income of the families, due to COVID-19 pandemic restrictions most probably led to increased challenges in covering health related costs [14].
At HCL, the total number of severe malaria patients in 2022 almost tripled in comparison to 2021, a trend also registered in other studies from Africa [15]. However at HCL, the mortality rate decreased substantially from 10.2% to 5.9% in 2022. Severe malaria usually has a mortality well over 5%, and therefore represents a > 50-fold increase in the risk of death [5]. Many factors affecting the prognosis of P. falciparum malaria have been identified [16]. The SOFA a score that describes quantitively the degree of organ dysfunction/failure over time in patients, has become a common feature for the assessment of morbidity in critical illness [17] including severe malaria [12]. Increasing SOFA reflects severity of illness [12,18]. At ICU, as expected, most patients had multiorgan dysfunction, with a median SOFA of 11 (min. 4, max. 21) though in our study SOFA was not a predictor of mortality, corroborating what was previously reported from Luanda, Angola [12]. We could not corroborate that SOFA is a good predictor of mortality at ICU [19]. This cloud be due to low number of patients with negative outcome at the ICU and also the fact that 68% died within the first 48h after admission. Hence, we could not detect the predictive value of SOFA for 28-day mortality [18,19].
Mortality due to severe malaria varies substantially, as it depends on (among others) the host immunity, [5]. P. falciparum malaria positivity rate tends to be higher during productive age [10,20] although the severity of the disease tends to be lower, due to higher antimalarial immunity [6]. In our study the majority of the individuals afflicted by severe malaria were young adults (mean of 29.5 ± 13.6 years) closely mirroring that of the patients who died during the study period (28.9 ± 14.1 years). Recent literature suggests that severe and complicated malaria can occur in this population more frequently than previously thought [8,21]. These findings highlight the importance of a focused approach to studying the underlying causes behind this pattern. Although hyperparasitaemia (parasites/µL) is poor predictor of outcome [5], it is established that high parasitaemia has a negative impact on the overall severity of illness particularly because of increased risk of severe anemia, as the disease progresses [22]. After renal impairment, impaired consciousness, and jaundice, emerged in our study, as the most commonly observed clinical features overall. These findings align with other studies from sub-Saharan Africa [8,9,21], demonstrating similarities in clinical presentations, with the exception of jaundice, which was notably common in our study.
Our overall findings indicate that in spit the number of fatalities decreased from 2021 to 2022, life threatening signs like renal impairment, jaundice and impaired conscience increased considerably (particularly among patients with a negative outcome). Several other studies have also identified these as prevailing clinical feature among patients with severe malaria [23].
Among patients with renal impairment, jaundice was the second most common other complication seen in both years (27.3% in 2021 and 47.6% in 2022). Although jaundice has been associated with renal impartment in other studies [8], the increased occurrence at HCL is nevertheless worrisome. The most common other complication among patients with renal impairment, was impaired conscience. Long-term effects, attributed to cerebral malaria (impaired conscience), are extensively studied in pediatric patients [11,24] and thought to be more frequent in children than in adults [25,26]. In fact in African children, severe malaria is the leading cause of acquired neurodisability [27]. In adults studies of neurological sequelae with serial follow-up assessments are currently lacking. Our study was not designed to identify the cause of the increased number of patients presenting renal impairment and impaired conscience from 2021 to 2022, but it highlighted the need to understand the reason behind this increase in order to enable mitigation measures to be implemented at HCL. More so because an emerging link between acute renal impairment and the brain (neurologic deficits and neurocognitive sequelae) in severe malaria patients is gaining momentum [28,29,30,31,32,33]. Rapid diagnosis with timely blood transfusion, renal replacement therapy, and restrictive fluid therapy can improve survival in severe malaria [34].
Thrombocytopenia is a common finding in adults with severe P. falciparum malaria and has been presented as a potential predictor of poor outcome in P. falciparum malaria [35,36]. In our study 82.2% of patients that survive and 75.6% of the ones that died, presented thrombocytopenia at addition. In both, the survival group and the diseased, platelets counts decreased as parasitaemia increased (p<0,0001 and p=0,0417 respectively), corroborating other findings [35,36,37,38]. Hence we agree that thrombocytopenia is a marker of disease severity in adults with P. falciparum malaria, but has limited utility in prognostication, triage and management [37].
The time-lapse from symptoms-onset to hospital admission (this data was self-reported and may not entirely reliable), showed an insignificant difference between 2021 (4.6±2.2 days) and 2022 (4.5±2.1 days). By itself, it seems insufficient to account for, or substantiate the increased severity of patients severity of illness, registered in 2022 when compared to 2021. For the same admission severity, outcomes in well-equipped intensive care units (ICUs) with well-trained staff, are better than in peripheral health centers [39,40]. Hence, we are inclined to attribute the reduction in mortality by half, during 2022, to a general improvement of the ICU conditions due to the recent hospital (HCL) infrastructure intervention.
This retrospective study is subject to limitations as it is a single-center study and as a result, the generalizability of our findings to other settings may be limited. Nevertheless, this study provides both a baseline and valuable (up to date) data on severe malaria in adult patients in a low transmission region. A well-designed cohort study with adult patients with serial follow-up assessments is needed.
5. Conclusions
Although the total number of severe malaria patients in 2022 almost tripled in comparison to 2021, the mortality rate was reduced by half. The increase in malaria cases during 2022, requires greater monitoring of the disease in subsequent years, in order to evaluate the impact of the reduction of preventive actions against malaria, in the context of the Covid19 pandemic as well as the possible presence of antimalarial drug resistance. A significant increase in the prevalence of renal impairment occurred from 2011 to 2022. This study establishes a valuable foundation for future research in this field, serving as a reference point for subsequent studies in low transmission regions and other areas within Angola.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org., Table S1 – Severe malaria profile of patients (regarding severe malaria manifestations) admitted to HCL during 2021 and 2022. The first line displays the number of patients for each department and year. If data was missing for some patients, the percentage of patients meeting the specific severe malaria criteria was calculated based on the available patient count mentioned in the corresponding table cell.; Table S2 – Profile of patients (regarding severe malaria manifestations) who died during the study period at the Hospital Central Dr. António Agostinho Neto of Lubango. The first line displays the number of patients for each department and year. If data was missing for some patients, the percentage of patients meeting the specific severe malaria criteria was calculated based on the available patient count mentioned in the corresponding table cell.
Author Contributions
I.M. analyzed data and prepared the original draft of the text; S.R., A.M., S.E. and A.B. data collection; F.N. designed the research study, curated the data, edited the final text; M.A. designed the research study, reviewing and edited the final text.
Funding
This work was partially supported by Fundação para a Ciência e a Tecnologia GHTM UID/04413/2020 and LA-REAL - LA/P/0117/2020.
Institutional Review Board Statement
The study was approved by the Hospital Central Dr. António Agostinho Neto (HCL) institutional ethics review committee (Proc. nº 02/2023). The need for consent approval was waive.
Acknowledgments
The authors thank the Hospital Central de Lubango Dr. António Agostinho Neto (Lubango, Angola) for providing the conditions to conduct the present study.
Conflicts of Interest
All the authors have no conflicting interests (financial or non-financial) to disclose.
Appendix A
A retrospective study was performed in adult patients with severe malaria hospitalized in the departments of Internal Medicine (MED), Infectiology (INF) and Intensive Care Unit (ICU). This study was based on individual patient records, admitted to HCL from January to March 2021 and 2022. The following criteria were used for inclusion in the study: patients of all genders, with at least 14 years of age and without an upper age limit; laboratory confirmed diagnosis of P. falciparum infection through a rapid diagnostic test (RDT) or a positive blood smear. For epidemiological purposes, severe malaria was defined according to WHO following criteria for Severe Malaria [1].
For epidemiological purposes, severe malaria was defined according to World Health Organization [1], indicating the presence of P. falciparum infection and one or more of the following criteria:
- impaired consciousness (Glasgow score, GCS < 11), prostration (generalized weakness so that the person is unable to sit, stand or walk without assistance);
- multiple convulsions (more than two episodes within 24h);
- hypoglycaemia (blood or plasma glucose < 40 mg/dL);
- anemia (hemoglobin concentration < 7 g/dL or a haematocrit of < 20% in adults, with a parasites count > 10000/µl of blood);
- renal impairment (plasma or serum creatinine > 3 mg/dL or blood urea > 20 mmol/L);
- jaundice (plasma or serum bilirubin > 3 mg/dL, with a parasites count > 10000/µl);
- pulmonary oedema (radiologically confirmed or oxygen saturation < 92% on room air with a respiratory rate > 30/min, often with chest indrawing and crepitations on auscultation);
- significant bleeding (recurrent or prolonged bleeding from the nose, gums or venipuncture sites, hematemesis or melaena);
- shock (compensated shock: capillary refill ≥ 3 seconds or temperature gradient on leg (mid to proximal limb), no hypotension;
- decompensated shock (systolic blood pressure < 80 mmHg in adults, with evidence of impaired perfusion);
- hyperparasitaemia (10% or > 500,000 parasites/μl). Metabolic acidosis (a base deficit of > 8 mEq/L or, if not available, a plasma bicarbonate level of < 15 mmol/L or venous plasma lactate ≥ 5 mmol/l).
References
- World Health Organization. World malaria report 2023. In: World malaria report 2023. 2023. https://www.who.int/publications/i/item/9789240086173 Accessed 4 December 2023.
- Huntley BJ. Angola in Outline: Physiography, Climate and Patterns of Biodiversity [Internet]. In: Huntley BJ, Russo V, Lages F, Ferrand N, editors. Biodiversity of Angola: Science & Conservation: A Modern Synthesis. Cham: Springer International Publishing; 2019 [cited 2023 10]. p. 15–42. [CrossRef]
- Tavares, W.; Morais, J.; Martins, J.F.; Scalsky, R.J.; Stabler, T.C.; Medeiros, M.M.; Fortes, F.J.; Arez, A.P.; Silva, J.C. Malaria in Angola: recent progress, challenges and future opportunities using parasite demography studies. Malar. J. 2022, 21, 1–13. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO guidelines for malaria, 16 October 2023. World Health Organization; 2023. https://iris.who.int/bitstream/handle/10665/373339/WHO-UCN-GMP-2023.01-Rev.1-eng.pdf?sequence=1 Accessed 4 December 2023.
- White, N.J. Severe malaria. Malar. J. 2022, 21, 1–17. [Google Scholar] [CrossRef]
- Griffin, J.T.; Hollingsworth, T.D.; Reyburn, H.; Drakeley, C.J.; Riley, E.M.; Ghani, A.C. Gradual acquisition of immunity to severe malaria with increasing exposure. Proc. R. Soc. B: Biol. Sci. 2015, 282, 20142657–20142657. [Google Scholar] [CrossRef] [PubMed]
- Reyburn, H.; Mbatia, R.; Drakeley, C.; Bruce, J.; Carneiro, I.; Olomi, R.; Cox, J.; Nkya, W.M.M.M.; Lemnge, M.; Greenwood, B.M.; et al. Association of Transmission Intensity and Age With Clinical Manifestations and Case Fatality of Severe Plasmodium falciparum Malaria. JAMA 2005, 293, 1461–1470. [Google Scholar] [CrossRef] [PubMed]
- Bittaye, S.O.; Jagne, A.; Jaiteh, L.E.; Nadjm, B.; Amambua-Ngwa, A.; Sesay, A.K.; Singhateh, Y.; Effa, E.; Nyan, O.; Njie, R. Clinical manifestations and outcomes of severe malaria in adult patients admitted to a tertiary hospital in the Gambia. Malar. J. 2022, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Yusuph, R.; Sawe, H.R.; Nkondora, P.N.; Mfinanga, J.A. Profile and outcomes of patients with acute complications of malaria presenting to an urban emergency department of a tertiary hospital in Tanzania. BMC Res. Notes 2019, 12, 1–5. [Google Scholar] [CrossRef]
- Debash, H.; Bisetegn, H.; Ebrahim, H.; Tilahun, M.; Dejazmach, Z.; Getu, N.; Feleke, D.G. Burden and seasonal distribution of malaria in Ziquala district, Northeast Ethiopia: a 5-year multi-centre retrospective study. BMJ Open 2023, 13, e067103. [Google Scholar] [CrossRef]
- Storm, J.; Jespersen, J.S.; Seydel, K.B.; Szestak, T.; Mbewe, M.; Chisala, N.V.; Phula, P.; Wang, C.W.; E Taylor, T.; A Moxon, C.; et al. Cerebral malaria is associated with differential cytoadherence to brain endothelial cells. EMBO Mol. Med. 2019, 11. [Google Scholar] [CrossRef]
- Antunes, M.L.; Seixas, J.; Ferreira, H.E.; Silva, M.S. Adequacy of Severe Malaria Markers and Prognostic Scores in an Intensive Care Unit in Luanda, Angola: A Clinical Study. J. Clin. Med. 2020, 9, 3862. [Google Scholar] [CrossRef]
- UNITED NATIONS CONFERENCE ON TRADE AND DEVELOPMENT. Economic and social impact of COVID-19 in Angola 2021. 2022; https://unctad.org/system/files/official-document/aldcinf2021d6_en.pdf. Accessed 5 December 2023.
- Awucha, N.E.; Janefrances, O.C.; Meshach, A.C.; Henrietta, J.C.; Daniel, A.I.; Chidiebere, N.E. Impact of the COVID-19 Pandemic on Consumers’ Access to Essential Medicines in Nigeria. Am. J. Trop. Med. Hyg. 2020, 103, 1630–1634. [Google Scholar] [CrossRef]
- Bittaye, S.O.; Jagne, A.; Jaiteh, L.E.S.; Amambua-Ngwa, A.; Sesay, A.K.; Ekeh, B.; Nadjm, B.; Ramirez, W.E.; Ramos, A.; Okeahialam, B.; et al. Malaria in adults after the start of Covid-19 pandemic: an analysis of admission trends, demographics, and outcomes in a tertiary hospital in the Gambia. Malar. J. 2023, 22, 1–9. [Google Scholar] [CrossRef]
- Srinamon, K.; Watson, J.A.; Silamut, K.; Intharabut, B.; Phu, N.H.; Diep, P.T.; Lyke, K.E.; Fanello, C.; von Seidlein, L.; Chotivanich, K.; et al. The prognostic and diagnostic value of intraleukocytic malaria pigment in patients with severe falciparum malaria. Nat. Commun. 2022, 13, 1–12. [Google Scholar] [CrossRef]
- Lie, K.C.; for Southeast Asia Infectious Disease Clinical Research Network; Lau, C.-Y.; Chau, N.V.V.; West, T.E.; Limmathurotsakul, D. Utility of SOFA score, management and outcomes of sepsis in Southeast Asia: a multinational multicenter prospective observational study. J. Intensiv. Care 2018, 6, 1–8. [CrossRef]
- Teparrukkul, P.; Hantrakun, V.; Imwong, M.; Teerawattanasook, N.; Wongsuvan, G.; Day, N.P.; Dondorp, A.M.; West, T.E.; Limmathurotsakul, D. Utility of qSOFA and modified SOFA in severe malaria presenting as sepsis. PLOS ONE 2019, 14, e0223457. [Google Scholar] [CrossRef]
- Rudd, K.E.; Seymour, C.W.; Aluisio, A.R.; Augustin, M.E.; Bagenda, D.S.; Beane, A.; Byiringiro, J.C.; Chang, C.-C.H.; Colas, L.N.; Day, N.P.J.; et al. Association of the Quick Sequential (Sepsis-Related) Organ Failure Assessment (qSOFA) Score With Excess Hospital Mortality in Adults With Suspected Infection in Low- and Middle-Income Countries. JAMA 2018, 319, 2202–2211. [Google Scholar] [CrossRef] [PubMed]
- Nkumama, I.N.; O’meara, W.P.; Osier, F.H. Changes in Malaria Epidemiology in Africa and New Challenges for Elimination. Trends Parasitol. 2016, 33, 128–140. [Google Scholar] [CrossRef] [PubMed]
- Boushab, B.M.; Salem, M.S.O.A.; Boukhary, A.O.M.S.; Parola, P.; Basco, L. Clinical Features and Mortality Associated with Severe Malaria in Adults in Southern Mauritania. Trop. Med. Infect. Dis. 2020, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Poespoprodjo, J.R.; Douglas, N.M.; Ansong, D.; Kho, S.; Anstey, N.M. Malaria. Lancet 2023, 402, 2328–2345. [Google Scholar] [CrossRef] [PubMed]
- Plucinski, M.M.; Ferreira, M.; Ferreira, C.M.; Burns, J.; Gaparayi, P.; João, L.; da Costa, O.; Gill, P.; Samutondo, C.; Quivinja, J.; et al. Evaluating malaria case management at public health facilities in two provinces in Angola. Malar. J. 2017, 16, 1–10. [Google Scholar] [CrossRef]
- Kariuki, S.M.; Abubakar, A.; Newton, C.R.; Kihara, M. Impairment of executive function in Kenyan children exposed to severe falciparum malaria with neurological involvement. Malar. J. 2014, 13, 1–9. [Google Scholar] [CrossRef]
- Boivin, M.J.; Bangirana, P.; Byarugaba, J.; Opoka, R.O.; Idro, R.; Jurek, A.M.; John, C.C. Cognitive Impairment After Cerebral Malaria in Children: A Prospective Study. PEDIATRICS 2007, 119, e360–e366. [Google Scholar] [CrossRef]
- Birbeck, G.L.; Glover, S.J.; Beare, N.; Taylor, T.E.; Molyneux, M.E.; Kaplan, P.W.; Lewallen, S. Identification of Malaria Retinopathy Improves the Specificity of the Clinical Diagnosis of Cerebral Malaria: Findings from a Prospective Cohort Study. Am. J. Trop. Med. Hyg. 2010, 82, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Idro, R.; Marsh, K.; John, C.C.; Newton, C.R.J. Cerebral Malaria: Mechanisms of Brain Injury and Strategies for Improved Neurocognitive Outcome. Pediatr. Res. 2010, 68, 267–274. [Google Scholar] [CrossRef]
- Conroy, A.L.; Opoka, R.O.; Bangirana, P.; Idro, R.; Ssenkusu, J.M.; Datta, D.; Hodges, J.S.; Morgan, C.; John, C.C. Acute kidney injury is associated with impaired cognition and chronic kidney disease in a prospective cohort of children with severe malaria. BMC Med. 2019, 17, 98. [Google Scholar] [CrossRef]
- Namazzi, R.; Opoka, R.; Datta, D.; Bangirana, P.; Batte, A.; Berrens, Z.; Goings, M.J.; Schwaderer, A.L.; Conroy, A.L.; John, C.C. Acute Kidney Injury Interacts With Coma, Acidosis, and Impaired Perfusion to Significantly Increase Risk of Death in Children With Severe Malaria. Clin. Infect. Dis. 2022, 75, 1511–1519. [Google Scholar] [CrossRef] [PubMed]
- Namazzi, R.; Batte, A.; Opoka, R.O.; Bangirana, P.; Schwaderer, A.L.; Berrens, Z.; Datta, D.; Goings, M.; Ssenkusu, J.M.; Goldstein, S.L.; et al. Acute kidney injury, persistent kidney disease, and post-discharge morbidity and mortality in severe malaria in children: A prospective cohort study. EClinicalMedicine 2022, 44, 101292. [Google Scholar] [CrossRef]
- Conroy, A.L.; Datta, D.; Hoffmann, A.; Wassmer, S.C. The kidney–brain pathogenic axis in severe falciparum malaria. Trends Parasitol. 2023, 39, 191–199. [Google Scholar] [CrossRef]
- Hickson, M.R.; Conroy, A.L.; Bangirana, P.; Opoka, R.O.; Idro, R.; Ssenkusu, J.M.; John, C.C. Acute kidney injury in Ugandan children with severe malaria is associated with long-term behavioral problems. PLOS ONE 2019, 14, e0226405. [Google Scholar] [CrossRef]
- Bangirana, P.; Conroy, A.L.; Opoka, R.O.; Hawkes, M.T.; Hermann, L.; Miller, C.; Namasopo, S.; Liles, W.C.; John, C.C.; Kain, K.C. Inhaled nitric oxide and cognition in pediatric severe malaria: A randomized double-blind placebo controlled trial. PLOS ONE 2018, 13, e0191550. [Google Scholar] [CrossRef]
- Xu, J.-W.; Deng, D.-W.; Wei, C.; Zhou, X.-W.; Li, J.-X. Treatment-seeking behaviours of malaria patients versus non-malaria febrile patients along China-Myanmar border. Malar. J. 2023, 22, 1–13. [Google Scholar] [CrossRef]
- Sirak, S.; Fola, A.A.; Worku, L.; Biadgo, B. Malaria parasitemia and its association with lipid and hematological parameters among malaria-infected patients attending at Metema Hospital, Northwest Ethiopia. Pathol. Lab. Med. Int. 2016, ume 8, 43–50. [Google Scholar] [CrossRef]
- Lampah, D.A.; Yeo, T.W.; Malloy, M.; Kenangalem, E.; Douglas, N.M.; Ronaldo, D.; Sugiarto, P.; Simpson, J.A.; Poespoprodjo, J.R.; Anstey, N.M.; et al. Severe Malarial Thrombocytopenia: A Risk Factor for Mortality in Papua, Indonesia. J. Infect. Dis. 2014, 211, 623–634. [Google Scholar] [CrossRef] [PubMed]
- Hanson, J.; Phu, N.H.; Hasan, M.U.; Charunwatthana, P.; Plewes, K.; Maude, R.J.; Prapansilp, P.; Kingston, H.W.; Mishra, S.K.; Mohanty, S.; et al. The clinical implications of thrombocytopenia in adults with severe falciparum malaria: a retrospective analysis. BMC Med. 2015, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Tiiba, J.-D.I.; Ahmadu, P.U.; Naamawu, A.; Fuseini, M.; Raymond, A.; Osei-Amoah, E.; Bobrtaa, P.C.; Bacheyie, P.P.; Abdulai, M.A.; Alidu, I.; et al. Thrombocytopenia a predictor of malaria: how far? J. Parasit. Dis. 2022, 47, 1–11. [Google Scholar] [CrossRef]
- Legros, F.; Bouchaud, O.; Ancelle, T.; Arnaud, A.; Cojean, S.; Le Bras, J.; Danis, M.; Fontanet, A.; Durand, R.; Epidemiology, A.M.; et al. Risk Factors for Imported FatalPlasmodium falciparumMalaria, France, 1996–2003. Emerg. Infect. Dis. 2007, 13, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Njuguna, P.; Newton, C. Management of severe falciparum malaria. . 2004, 50, 45–50. [Google Scholar] [PubMed]
Figure 1.
Map of Angola provinces highlighting the study site. Dark blue, Angola; light blue Huíla province; star Lubango city; HCL, Hospital Central do Lubango Hospital Central Dr. António Agostinho Neto. Figure was created using Inkscape version 1.2.
Figure 1.
Map of Angola provinces highlighting the study site. Dark blue, Angola; light blue Huíla province; star Lubango city; HCL, Hospital Central do Lubango Hospital Central Dr. António Agostinho Neto. Figure was created using Inkscape version 1.2.
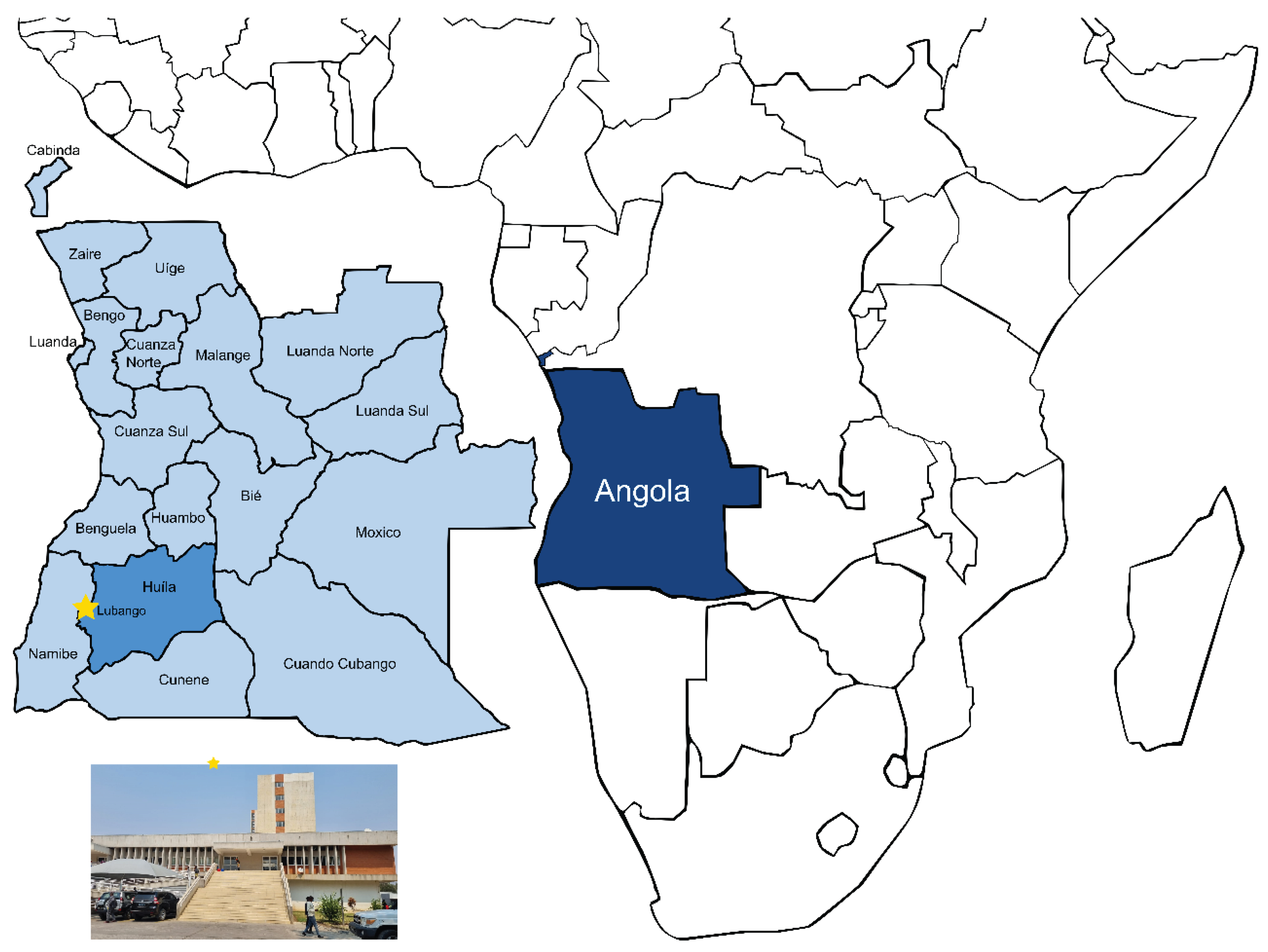
Figure 2.
Severe malaria profile of patients admitted to HCL during 2021 and 2022. Numbers inside boxes represent the % of patients that presented the correspondent severe malaria criteria, admitted to each department; ICU, Intensive Care Unit; INF, Infectiology; MED, Internal Medicine; Pulmonary oedema was not recorded in any of the patients.
Figure 2.
Severe malaria profile of patients admitted to HCL during 2021 and 2022. Numbers inside boxes represent the % of patients that presented the correspondent severe malaria criteria, admitted to each department; ICU, Intensive Care Unit; INF, Infectiology; MED, Internal Medicine; Pulmonary oedema was not recorded in any of the patients.
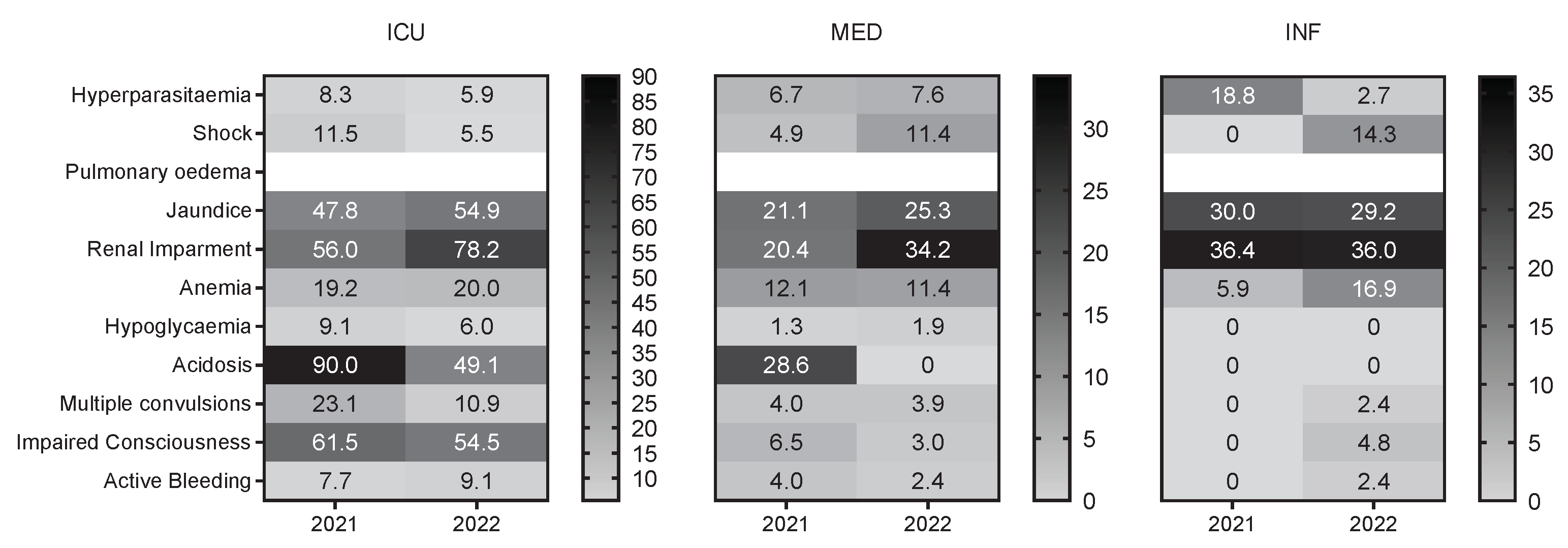
Figure 3.
Sequential Organ Failure Assessment (SOFA) score according to date of admission and outcome. – negative outcome (death due to severe malaria); + positive outcome (survive).
Figure 3.
Sequential Organ Failure Assessment (SOFA) score according to date of admission and outcome. – negative outcome (death due to severe malaria); + positive outcome (survive).
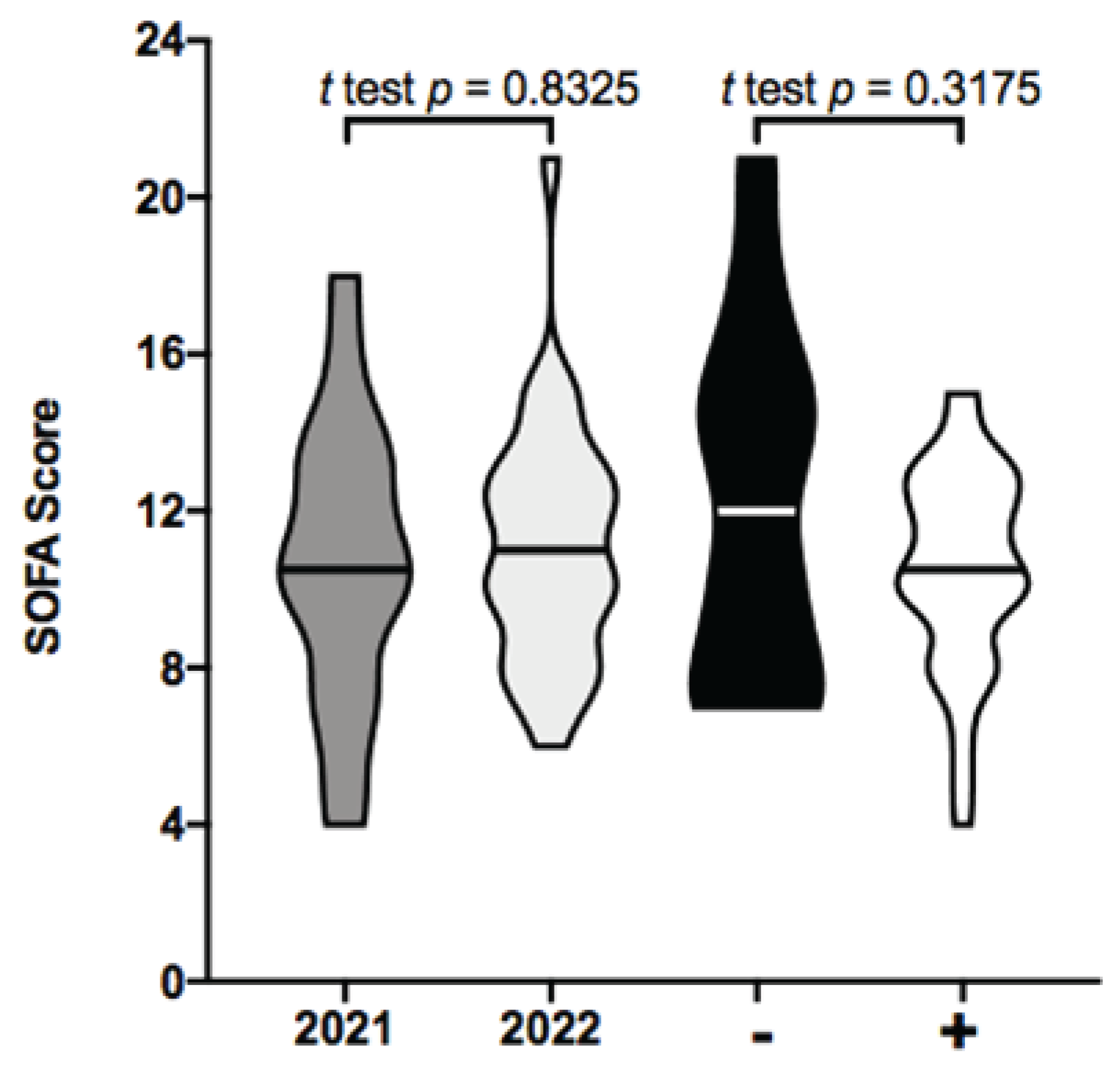
Figure 4.
Clinical outcome of severe malaria patients. *Three (3) patients admitted to MED during 2021, abandoned the hospital before receiving medical discharge.
Figure 4.
Clinical outcome of severe malaria patients. *Three (3) patients admitted to MED during 2021, abandoned the hospital before receiving medical discharge.
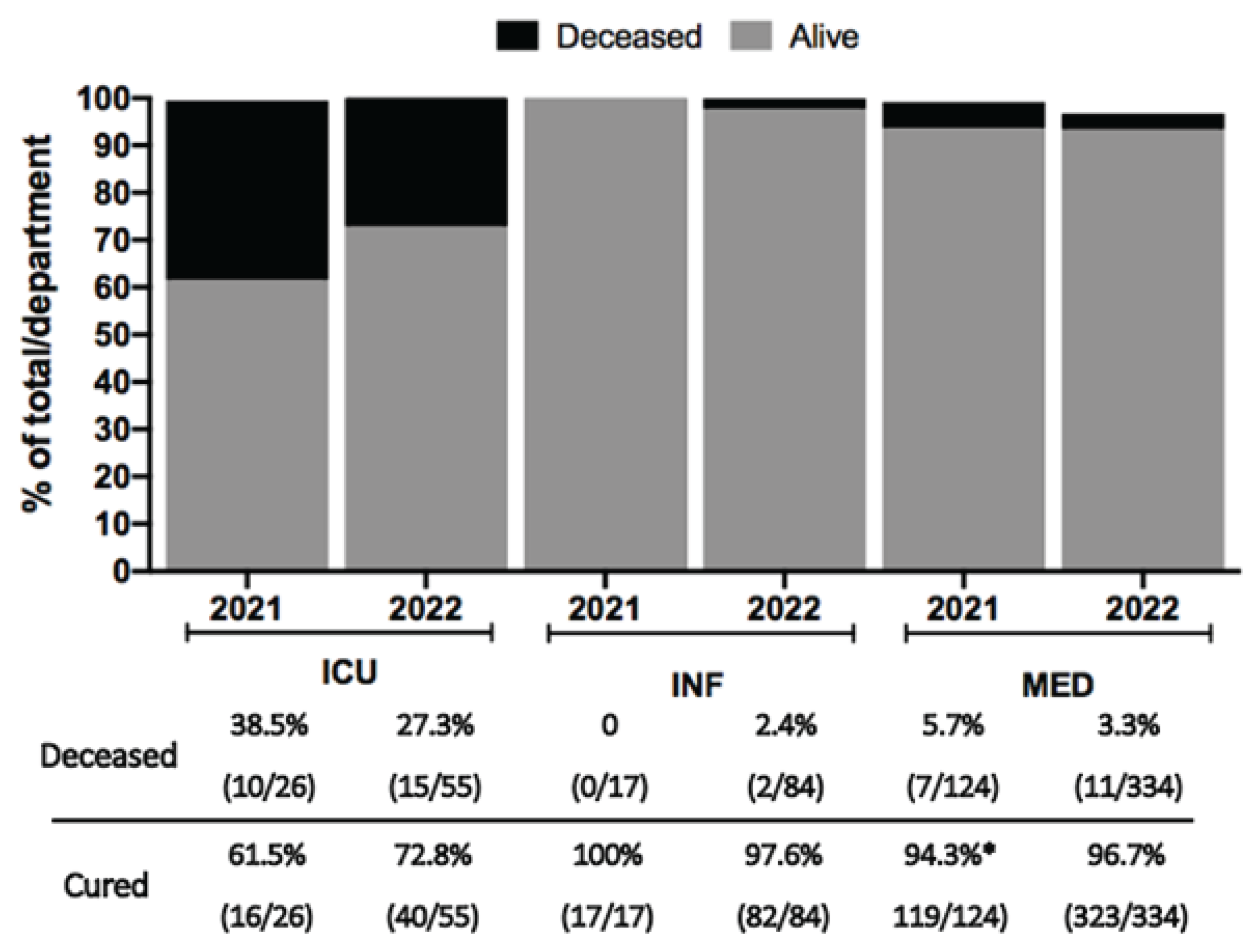
Figure 5.
Severe malaria features on admittance amongst patients with fatal outcome. A Numbers represent the % of patients admitted to each department; ICU, Intensive Care Unit; INF, Infectiology; MED, Internal Medicine. Pulmonary oedema was not recorded in any of the patients. There were no fatalities in INF during 2021; B Parasitaemia at admission distributed by department and outcome. Black bars, negative outcome (death due to severe malaria), white bars, positive outcome (survive); C, D creatinine and bilirubin levels and E Glasgow coma score (GCS). Dotted line indicates cut-off values for each parameter.
Figure 5.
Severe malaria features on admittance amongst patients with fatal outcome. A Numbers represent the % of patients admitted to each department; ICU, Intensive Care Unit; INF, Infectiology; MED, Internal Medicine. Pulmonary oedema was not recorded in any of the patients. There were no fatalities in INF during 2021; B Parasitaemia at admission distributed by department and outcome. Black bars, negative outcome (death due to severe malaria), white bars, positive outcome (survive); C, D creatinine and bilirubin levels and E Glasgow coma score (GCS). Dotted line indicates cut-off values for each parameter.
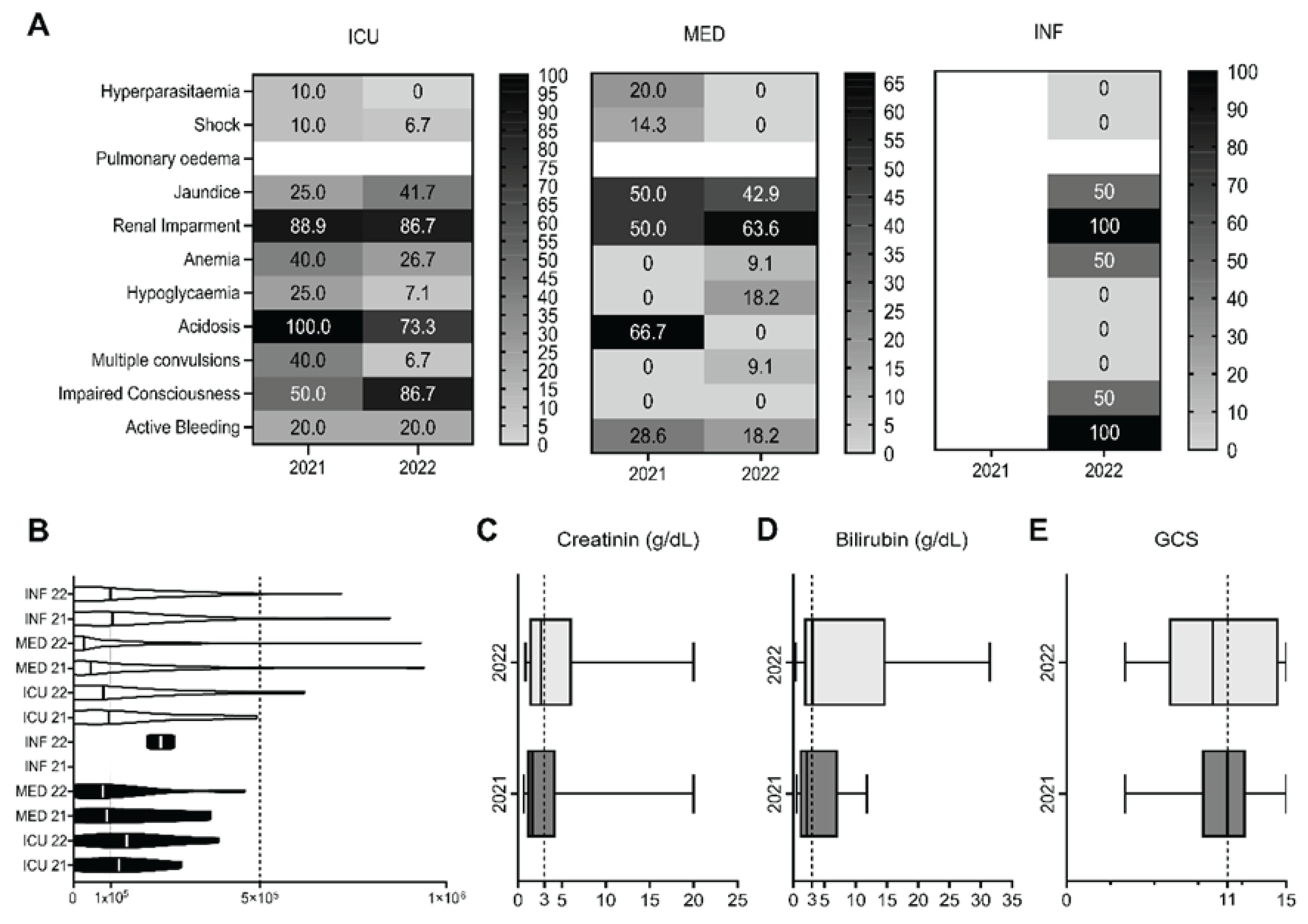

Table 1.
Demographics of the patients admitted to HCL in 2021 and 2022, during the peak months of malaria transmission. MED, Internal Medicine; INF, Infectiology; ICU, Intensive Care Unit.
Table 1.
Demographics of the patients admitted to HCL in 2021 and 2022, during the peak months of malaria transmission. MED, Internal Medicine; INF, Infectiology; ICU, Intensive Care Unit.
| 2021 | 2022 | ||||||
|
ICU % |
MED % |
INF % |
ICU % |
MED % |
INF % |
||
| Sex | Female | 19.2 (5/26) | 47.6 (59/124) | 52.9 (9/17) | 21.8 (12/55) | 44.9 (150/334) | 29.8 (25/84) |
| Male | 80.8 (21/26) | 52.4 (65/124) | 47.1 (8/17) | 78.2 (43/55) | 55.1 (184/334) | 70.2 (59/84) | |
| Age group | 14 - 18 | 7.7 (2/26) | 15.3 (19/124) | 5.9 (1/17) | 12.7 (7/55) | 11.4 (38/334) | 19.0 (16/84) |
| 18 - 60 | 84.6 (22/26) | 78.2 (97/124) | 88.2 (15/17) | 83.7 (46/55) | 82.0 (274/334) | 75.0 (63/84) | |
| ≥ 60 | 7.7 (2/26) | 6.5 (8/124) | 5.9 (1/17) | 3.6 (2/55) | 6.6 (22/334) | 6.0 (5/84) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



