
Submitted:
09 March 2024
Posted:
11 March 2024
You are already at the latest version
Abstract
The impact of systemic vascular resistance (SVR) in hypertrophic (HCM) and amyloid cardio-myopathies has been seldom investigated. We studied pressure-strain loop derived myocardial work (MW) indices and SVR in patients with either sarcomere HCM or wild type transthyretin cardiac amyloidosis (ATTR), presented with heart failure and preserved left ventricular ejection fraction (HFpEF) at the outpatient cardiology units at Messina and Catania University Hospitals (Italy). Patients were in sinus rhythm and needed to have good transthoracic ultrasound imaging quality to undergo transthoracic strain-echocardiography. Other than conventional parameters, SVR and GWI (global work index) were measured. Based on cross-tabulation (a way to assess the ventricular-arterial coupling), the patients were then classified in 4 classes according to the cut-off values suggested by previous studies of 1,440 dyne/s/cm-5 for SVR (Stefadouros et al., 1973) and 1576 mm Hg% for GWI (Olsen et al., 2022). Sixty patients, 30 in each group, aged 61±16 years, 78% males, were studied. HCM were younger than ATTR patients and in a better clinical status (23% HCM vs 77% ATTR were NYHA class 3, p<0.001). Overall, 51 patients (85%) showed high SVR, of whom 21 were HCM (70%) and 30 ATTR (100%) (p<0.005). Both, SVR and GWI were impaired (the poorest class C) in 43% HCM patients (with greater left ventricular concentric hypertrophy) vs 93% of ATTR patients (in advanced NYHA class) (p<0.001). In conclusion, assessing SVR and GWI in HFpEF patients with HCM or ATTR can help clinicians to interpret the pathophysiological and clinical features of such complex diseases.
Keywords:
Cardiac Amyloidosis
; Hypertrophic Cardiomyopathy
; Preserved Left Ventricular Ejection Fraction
; Systemic Vascular Resistance
; Strain Echocardiography
; Ventricular-Arterial Coupling.
1. Introduction
Although the concept of systemic vascular resistance (SVR) has long been recognized through experimental and human studies on hypertensive and cerebrovascular patients [1,2,3,4], it is only recently that gained popularity also in chronic heart failure (HF) settings [5,6]. SVR can be calculated by ultrasound-derived parameters, noninvasively, and it is considered a marker of left ventricular (LV) afterload, aortic arterial elastance, and distal vascular resistance to blood flow [1,2,5,6]. Patients with chronic HF may demonstrate changes in SVR related to higher arteriolar and microvascular tone, sympathetic drive, hyperactivity of the renin-angiotensin-aldosterone system (SRAA) and/or blood viscosity [3,4,5,6,7]. Hemodynamic studies have provided a normal SVR range varying from 900 to 1440 dynes/s/cm−5 [8], while its calculation can contribute to differentiate underlying pathophysiologic mechanisms and guide therapy even in the acute HF settings. In fact, hypotensive patients due to sepsis can reveal low SVR, while hypotension resulting from cardiogenic shock may be linked to elevated SVR [9]. From this perspective, the evaluation of SVR and LV function underlies the concept of ventricular-arterial coupling (VAC), the interplay between the heart and the arterial system, that is quite hard to be reproduced noninvasively. VAC offers a unique chance of analyzing the cardiovascular system adaptation to various clinical settings, including hypertrophic phenotypes, whose studies are lacking [10]. Recent European documents indicate that global longitudinal strain (GLS) by speckle-tracking echocardiography and pressure-strain loop-derived myocardial work (MW) analyses (especially global work index [GWI]) can be reliable surrogates of VAC [11].
At present time, hypertrophic cardiomyopathy (HCM) and transthyretin cardiac amyloidosis (ATTR) are common hypertrophic phenotypes in clinical practice. We recently demonstrated that, despite similar echocardiographic presentation, MW parameters are more impaired in ATTR than in HCM patients, correlated to their reduced ejection fraction (EF) [12,13]. The present study aimed to investigate whether the combined use of MW and SVR can be helpful to interpret these cardiovascular conditions in the same hypertrophic settings with preserved LVEF.
2. Materials and Methods
This was an observational study in consecutive adult patients admitted to the outpatient HF units at Cardiology Departments of G. Martino University Hospital (Messina, Italy) and G. Rodolico University Hospital (Catania, Italy) from October 2022 to October 2023, scheduled to a clinical follow-up or screening for HCM or ATTR.
Admission criteria were as follows: a) age >18 years; b) HCM and wild-type ATTR according to current diagnostic criteria [14,15]; c) good technical quality of the transthoracic echocardiogram; d) preserved LV ejection fraction (>50% on two-dimensional imaging); e) sinus rhythm. Exclusion criteria were active (or previous) ischemic heart disease, systemic conditions with potential interference on cardiac function, severe heart valve disease, permanent atrial fibrillation, cancer, light chain (AL) amyloidosis and mutated ATTR.
A careful patient’s screening was mandatory on enrolment via clinical history, physical examination, resting electrocardiogram (ECG), basic echocardiographic examination, advanced diagnostic techniques and genetic testing, according to current guidelines on cardiomyopathies [16]. Primary nonobstructive HCM was confirmed in patents presenting with all the following criteria [14]: 1) LV wall thickness ≥15 mm in any myocardial wall segment, in a nondilated chamber and in the absence of relevant causes leading to LV hypertrophy; 2) typical ECG pattern; 3) family history of HCM, except in case of an individual suspected to be the proband; 4) LV outflow tract gradient ≤ 30 mmHg at rest, exercise and/or Valsalva maneuver; 5) genetic testing, if available.
Diagnosis of wild-type ATTR was made according to all the following criteria [15]: 1) clinical history; 2) LV hypertrophy (wall thickness >12 mm in any myocardial wall segment) on echocardiography or cardiac magnetic resonance, checking for extra-ventricular features of ATTR as well (18); 3) discrepancy between ECG signs and echo criteria for LV hypertrophy; 4) genetic testing to rule out mutative forms; 5) total body 99mTechnetium-Pyrophosphate bone scintigraphy, showing Perugini score 2 or 3.
The observational design was approved by the local Cardiology Research Board, ensuring the patient’s data privacy.
Transthoracic Echocardiography and Formulas
Ultrasound studies were all performed with the same vendor machine (Vivid E95; GE Vingmed Ultrasound, Horten, Norway). Conventional mono- and two-dimensional measurements, color-Doppler sampling and advanced analyses (global longitudinal strain, myocardial work assessment) were performed in each patient and stored in a digital system, whereas post-processing analysis required a skilled examiner (physician). Transthoracic echocardiographic study comprised imaging from the parasternal long-axis, short-axis, and 2-, 3-, and 4-chamber apical views and the measurements were performed according to the current European/American guidelines [17].
As above mentioned, the hypertrophic phenotype was assessed by measuring the greatest wall thickness in the LV chamber. LV end-diastolic/systolic volumes were achieved by all apical views using the Simpson rule triplane method. Atrial chamber volumes were measured by the biplane method. Cardiac chamber volumes were then indexed to the body surface area (BSA). LV ejection fraction was measured automatically by the software, after checking for correctness of the border detection by the examiners. LV mass was calculated according to the American Society of Echocardiography method from the parasternal long-axis view. Diastolic function was assessed with pulsed-wave Doppler at the mitral inflow (peak early velocity = E wave) divided by the early diastolic tissue velocity (e’ wave) measured as the average value between the basal septum and the lateral mitral annulus (E/e’ ratio). Dynamic obstructive physiology was ruled out by measuring the LV outflow tract peak systolic gradient with color-Doppler guided continuous-wave Doppler sampling under resting or/and Valsalva maneuver or stress condition. Speckle-tracking analysis was performed with an ultrasound frame rate of 50-60 frames/s. Adjustments of the region of interest were manually achieved by the two experienced examiners, and strain measurements taken from the apical 2- 3- and 4-chamber views of the LV. GLS and MW were calculated using digitally stored videoclips from each patient, using a dedicate analytic software (EchoPAC, GE Vingmed Ultrasound, Horten, Norway). Analysis of MW required the LV pressure/strain loop digital construction starting from the measurement of systolic blood pressure (BP) in the sitting position, just before ultrasound imaging acquisition, after the patient had rested for 15 minutes by using an appropriate brachial cuff. MW indices were the average measurement of the respective 17-segment model analyses. Based on our recent study, we evaluated the 2 most significant MW markers, the global work index (GWI), which is consistent of the total work performed from the mitral valve closure until its opening, plus isovolumetric contraction and relaxation, and the global constructive work (GCW), which is the myocardial work performed during all the LV shortening [13].
Total SVR was calculated using the original formula (SVRecho) by Stefadouros et al. [3], with the correction (SVRc) proposed to attain the value as closest as possible to the invasive hemodynamic determination, as follows:
where mBP was the mean blood pressure (mm Hg) calculated by the formula [(systolic BP-diastolic BP)/3] + diastolic BP, and CO (L/m) was the product of LV stroke volume (SV) x heart rate (bpm).
SVRc = [(mBP/CO) x 80 x 0.865] + 216 dyne/s/cm-5
In order to better investigate the underlying cardiovascular status, the patient population was divided into 4 classes, according to cut-off values of 1,440 dyne/s/cm-5 representing the normal limit for SVRc, as suggested by previous studies [3,8], and of 1576 mm Hg% for GWI index. This latter value constituted the lowest range value from 1827 healthy participants, median aged 45 years, in the recent Copenhagen City Heart Study [18]. Secondary clinical cut-off points were also considered in the scatter plot diagram.
Statistics
Shapiro-Wilk test was applied to evaluate whether the data set was normally distributed or not. Continuous variables are expressed in the form of mean ± standard deviation (SD), if normally distributed, or median and interquartile range [IQR], if not. Categorical variables are represented by the absolute number and their respective percentages (%). Between-group and in-group differences of clinical and echocardiographic characteristics were compared through Student’s t test or Mann–Whitney U test, as appropriate. Categorical variables were analyzed by the χ2 test for the overall assessment, and by the Fisher's exact test for pairwise group comparisons.
Correlation coefficients were determined for establishing the intra-observer agreement in 10 randomly selected patients to evaluate reproducibility. The null hypothesis was considered rejected for p-values <0.05 at two-tailed significance level. Statistical analysis was conducted using SPSS (IBM SPSS Statistics) version 26.
3. Results
From an initial cohort of 87 patients referred to both clinical Centers, 27 (31%) were excluded, because of obstructive HCM (n=8, 9%), familiar ATTR (n=8, 9%), AL amyloid variant (n=6, 7%), permanent atrial fibrillation (n=3; 3%), and inadequate acoustic imaging for strain and myocardial work assessments (n=2, 2%). A total of 60 patients, mean aged 61±16 years, 30 in each group, 47 males (78%), were finally enrolled. Demographic and clinical characteristics of the respective patients are displayed in Table 1.
There was no difference regarding the proportion of male patients between the groups, but those with HCM were younger than those with ATTR. An advanced New York Heart Association (NYHA) functional class was evident in this latter group, although none of individuals were class IV. Accordingly, 77% of ATTR patients complained with mild to moderate dyspnea on effort, compared to 23% of HCM patients (p<0.001). Office BP measurements were similar between the groups, facilitating interpretation of the target markers of LV dysfunction, MW and SVR. ATTR patients were all on treatment with Tafamidis at the dose of 61 mg daily. Every patient provided a written consent for the echocardiographic study.
3.1. Conventional Echocardiography Findings
Main echocardiographic measurements are exposed in Table 2. There were no significant between-group differences regarding LV end-diastolic volume index, ventricular septum thickness, and LV mass index (weakly higher in ATTR patients). Although the LVEF was lower in this group, largely due to higher end-systolic volumes and ensuing lower CO, the whole participants were fulfilled the HFpEF criteria, according to current guidelines [19]. Both groups revealed the same degree of left atrial chamber enlargement, but ATTR patients demonstrated greater LV diastolic dysfunction and lower GLS values than HCM patients.
3.2. Systemic Vascular Resistance and Myocardial Work Indices
SVRc, GWI and GCW were calculated in each patient (Table 2). Overall, 51 patients showed high SVRc (85%), 21 were from the HCM (70%) and 30 from the ATTR group (100%) (p<0.005). Moreover, SVRc was reversely correlated to GWI and GCW (Figure 1). There was no linear correlation between mean blood pressure values and SVRc (additional online material).
ATTR patients presented much lower GWI and GCW values than HCM patients, that were consistent with our recent study results [13].
The novel functional classification was performed according to SVRc and GWI value cross-tabulation (Figure 2, Table 3). Only 9 patients out of HCM group (15%) showed normal SVRc (classes A or B), whereas 43% entered the poorest class C and 27% the intermediate class D. Except from 2 cases, almost all ATTR patients (93%) were in class C.
Patients who had GWI<1576 mm Hg% also included those with GCW<1730 mm Hg%, which was suggested to be another prognostic factor in patients with nonobstructive HCM [20].
Figure 2.
- Scatter plot diagram showing 4 classes categorized according to SVRc (cut-off 1440 dyne/cm/s-5) [3,8] and GWI (cut-off 1576 mm Hg%) [18]. Therefore, Class A included patients with low/normal SVRc and preserved GWI, then interpreted as the best functional class. Class B included patients with lower GWI and normal SVRc, taken as intermediate risk class. Class C included patients with higher SVRc and impaired GWI, then considered as the worst one. Class D, another intermediate class due to high SVRc. Vertical dashed lines indicate the cut-off values by previous studies for impaired myocardial perfusion and late gadolinium enhancement (LGE) in HCM patients [21], and major cardiovascular events (MACE) in ATTR patients [22]. Tabulation below the graphics refers to some clinical findings from the patients belonging to different Classes (see also Table 3). ATTRwt, wild-type transthyretin cardiac amyloidosis; HCM, nonobstructive hypertrophic cardiomyopathy; NYHA, New York Heart Association functional class; NSVT, nonsustained ventricular tachycardia on 24-hour ECG Holter monitoring; PAF, paroxysmal atrial fibrillation.
Figure 2.
- Scatter plot diagram showing 4 classes categorized according to SVRc (cut-off 1440 dyne/cm/s-5) [3,8] and GWI (cut-off 1576 mm Hg%) [18]. Therefore, Class A included patients with low/normal SVRc and preserved GWI, then interpreted as the best functional class. Class B included patients with lower GWI and normal SVRc, taken as intermediate risk class. Class C included patients with higher SVRc and impaired GWI, then considered as the worst one. Class D, another intermediate class due to high SVRc. Vertical dashed lines indicate the cut-off values by previous studies for impaired myocardial perfusion and late gadolinium enhancement (LGE) in HCM patients [21], and major cardiovascular events (MACE) in ATTR patients [22]. Tabulation below the graphics refers to some clinical findings from the patients belonging to different Classes (see also Table 3). ATTRwt, wild-type transthyretin cardiac amyloidosis; HCM, nonobstructive hypertrophic cardiomyopathy; NYHA, New York Heart Association functional class; NSVT, nonsustained ventricular tachycardia on 24-hour ECG Holter monitoring; PAF, paroxysmal atrial fibrillation.
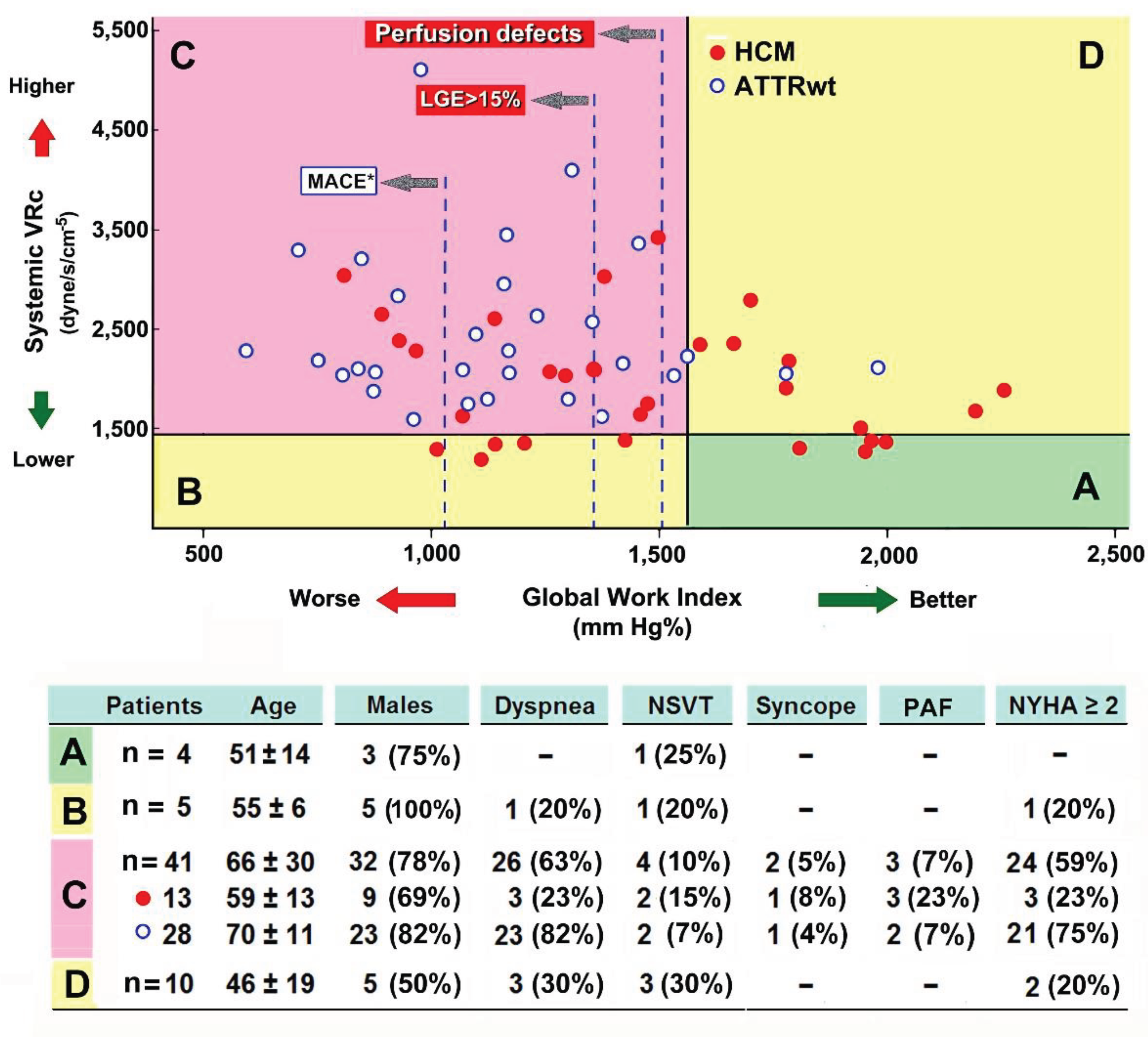
In Figure 2, three more cut-off values for GWI are represented in the diagram according to other studies. The value of GWI <1517 mm Hg% was found in HCM patients with myocardial perfusion defects at stress-perfusion cardiac magnetic resonance, and the value of <1363 mm Hg% also discriminated the presence of late gadolinium enhancement >15% of myocardial mass at cardiac magnetic resonance imaging [21]. The interrupted line indicating the risk of “MACE” at the cut-off value of GWI <1043 mm Hg% was previously found as all-cause mortality risk factor in amyloid patients (61% wildtype ATTR) [22].
Paired ingroup HCM analysis demonstrated that patients in class C had smaller LV chambers and higher septum thickness, as well as lower GLS than those in the other classes. Those were rather older, with a tendency towards lower LVEF and LAVi, but the subgroup consistency hindered reaching a statistical significance.
On the other hand, all ATTR patients showed higher SVRc and only 2 out of these had normal GWI. Therefore, the large numerically discrepancy did not allow a between-class comparison (Table 3, bottom panel).
3.3. Intra-Observer Variability in MW and SVR Measurements
Intra-observer variability for the MW parameters and GLS was recently tested in our echo laboratories. Myocardial work index variability approximately was ±1.0% for GWI (bias 21 mm Hg%), ±4.5% for GCW (bias 62 mm Hg%) and 4.7% (bias -0.5%) for GLS. Variability of SVRc measurement was mainly related to LV chamber volume assessment, then to the automated software recognition and operator adjustments, as required. Thus, inter- and intra-observed variability were in the order of ±5.5-6.0% (bias 0.2-0.3 L/min) for CO.
4. Discussion
Currently, the precise assessment of cardiovascular function in patients with cardiac hypertrophy is abridged by multitasking imaging technology that contributes to diagnosis and better management compared to previous years. Echocardiography and cardiac magnetic resonance remain the gold standards for the assessment of hypertrophic phenotypes at risk for HF [23,24].
Main findings from the present study indicate that combined evaluation of SVRc and GWI can be useful to assign different functional (VAC) class to HFpEF patients with either HCM or ATTR. For the first time to our knowledge, we disclosed SVRc >1440 dyne/m/sec-5 in 85% of study population, but mostly in ATTR patients. Despite the lack of univocal cut-off values, an impairment in GWI resulted in 73% of patients, according to the lowest normal value reported by the CCHS study [18]. Taken these together, both study markers were impaired in 43% of HCM vs 93% of ATTR patients, all classified in the poorest class C. Of interest, the HCM individuals in class C were quite older than in other classes, demonstrating a high degree of concentric LV hypertrophy, which usually constitutes a predictor of obstructive physiology [14].
According to Garcia Brás at al. [21], 18 patients out of the HCM group (60%) also presented GWI values suggestive of impaired myocardial perfusion, in 13 cases (43%) with possible late gadolinium enhancement >15%.
However, only 13/18 (72%) and 8/13 patients (61%), respectively, also had higher SVRc, evidence that could further identify their risk for microvascular disease.
In amyloid patients, GWI <1043 mm Hg% was linked to unfavorable outcomes in the study of Clemmersen et al. [22]. Although most ATTR patients in our series showed impaired GWI, only in 10 cases (33%) it was <1043 mm Hg%. Of note, in the ATTR population, SVRc lost significance in discriminating these latter from other individuals.
The assessment of SVRc is a long-standing methodological problem in cardiovascular diseases, due to such a problematic reproduction of measurements across studies. However, early data by Wiggers in 1951 demonstrated that vascular reactivity, arterial elastance, and peripheral resistance do affect the LV function by imposing a rising afterload, at times, disproportionately to the basic cardiac condition [1].
Today, the cardiovascular interplay consists with the ultimate concept of ventricular-arterial coupling (VAC), which is a central target in various clinical and experimental studies [3,6,10,11]. Characterization of VAC should also include SVR, as the cardio-vascular functional interplay is the pivotal feature of systemic workload, also addressing potential therapeutic interventions in HF patients [9,11].
As suggested by Suga and Sagawa [25] and then confirmed by Sunagawa et al. [6], VAC belongs to the ratio of effective arterial elastance over end-systolic elastance. More recently, experts’ consensus documents suggested the VAC to be attained by advanced ultrasound-derived indices such as MW, and GWI has been proposed as a valid surrogate in various clinical settings [10,11,26]. By adopting the simple speckle-tracking modality over a single cardiac cycle, pressure-strain loop derived MW computation likely outperforms the old methods for VAC. This is a breakthrough in the functional measurement as closest as possible to traditional LV pressure-volume curves [11,18]. Accordingly, GWI and GCW were demonstrated to be prognostic factors in various clinical settings, including acute and chronic coronary syndromes, cardiomyopathies, and cardio-oncology [11,12,13,27,28]. Compared to conventional echocardiographic and Doppler techniques, the analysis of MW provides an amelioration in the study of VAC, also because imaging procession is load- and angle-independent. The use of a pressure-strain loop derived analysis also allows a comprehensive assessment of the LV mechanics, with low inter- and intra-observer variability that ensures consistent results across different examiners.
However, further studies are still needed to better interpret the prognostic impact of MW indices and its qualified cut-off values in hypertrophic phenotypes [29]. A very low GWI value (<937 mm Hg%) was suggested as a predictor of cardiovascular mortality in 118 patients with cardiac amyloidosis, but such value suffered from low sensitivity and specificity [30].
Interestingly, Hiemstra et al. demonstrated a correlation between GCW and maximal LV wall thickness and diastolic function, suggesting the value <1730 mm Hg% as a long-term outcome discriminator in HCM patients [20]. In our study, all HCM patients with GWI<1576 mm Hg% also had GCW <1730 mm Hg%, but only a proportion of them also showed high SVRc.
On the other hand, MW only in part reflects the aortic compliance and SVR, which represent important factors of the CO and systemic perfusion. For these reasons, in the present study we aimed at combining both GWI and SVRc parameters to better interpret the cardiovascular function in such hypertrophic phenotypes. In non-obstructive HCM, adding SVRc information to low GWI may indicate a subset of patients more inclined to microvascular and/or small coronary artery disease, both potential forecasters of tissue fibrosis even in the absence of epicardial vessel stenosis [21,31]. According to clinical characteristics of class C patients, the combined score of GWI and SVR might be more predictive of weak clinical conditions in ATTR patients, while linked to greater concentric hypertrophy in HCM patients, anticipating their potential obstructive physiology.
Even though all ATTR patients in this study were classified as HFpEF, present results reinforce the pathophysiological theory that amyloidosis is a systemic illness in which the vascular compartment progressively deteriorates alongside the heart, somehow consistent with their clinical status. On the other hand, most ATTR patients present with autonomic dysfunction and BP variability, with a challenging vascular reactivity that affects their quality of life and prognosis [16,32,33]. This further confirms their cardiovascular system impairment is differently influenced by interstitial amyloid fibril accumulation than by genetic disorders featuring primary HCM [15,16,21,24,33,34]. Conversely, preserved MW indices and weakly higher (or normal) SVRc, as in 2 ATTR patients in our class D, may suggest a less compromised systemic condition or early stage of disease, more likely to get benefit from specific therapy [23,24,28,32,35].
4.1. Study Limitations
This study has important limitations. The number of patients was modest, due to the low incidence of the ATTR among HF patients. Also, we needed to include only those with HFpEF, which is an even rare condition in such clinical setting.
The method used for SVR computation by ultrasound may be imprecise, and no large studies have been conducted for the clinical validation of the formula proposed by Stefadouros et al. in hypertrophic phenotypes. It should also be considered the role for the RA mean pressure in the native formula, although this likely was more helpful for pulmonary capillary resistance rather SVR [10,12,35].
Calculation of MW needs multiple parameters and optimal acoustic window from all echocardiographic sections, not always excellent in such patients, and this may affect reproducibility [33]. Also, the fluctuation in BP measurements, especially in ATTR patients, hypertensives or in the context of anxiety, can lead to relevant methodological errors and then impact onto statistics and conclusions.
Also, we missed performing any comparison between SVRc, MW and LV mass, because conventional echocardiographic methods likely fail to assess myocardial mass in a reliable way, compared with cardiac MRI. Four-dimensional echocardiography will surely address a better recognition of such interplay in both clinical settings [XX}.
Finally, we were unable to assess the correlations between tested markers and the history of cardiovascular events, as well as tissue information from cardiac magnetic resonance imaging, because those findings were unattainable by some patients.
5. Conclusions
A significant proportion of present study population was shown to get impaired SVRc and/or GWI, despite preserved LVEF. These markers are expressions of detrimental VAC that affects a sizable majority of ATTR (in advanced NYHA class) and over half of those with HCM (showing greater LV concentric hypertrophy).
The suggested classification may shed further lights on different patient subsets and facilitate physicians to interpret their composite pathophysiological and clinical characteristics. Larger studies are required to validate present results and establish a potential prognostic impact.
Funding
This research received no funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. Ethical review and approval were waived due to the observational retrospective nature of the study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study at the time of first visit.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data underlying this article will be shared on reasonable request to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Wiggers, C.J. Determinants of Cardiac Performance. Circulation 1951, 4, 485–495. [Google Scholar] [CrossRef]
- Ilebekk, A. Determinants of Cardiac Performance. J Oslo City Hosp 1979, 29, 91–102. [Google Scholar]
- Stefadouros, M.A.; Dougherty, M.J.; Grossman, W.; Craige, E. Determination of Systemic Vascular Resistance by a Noninvasive Technic. Circulation 1973, 47, 101–107. [Google Scholar] [CrossRef]
- Schiffrin, E.L. Remodeling of Resistance Arteries in Essential Hypertension and Effects of Antihypertensive Treatment. Am J Hypertens 2004, 17, 1192–1200. [Google Scholar] [CrossRef]
- Trammel, J.E.; Sapra, A. Physiology, Systemic Vascular Resistance. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2023. [Google Scholar]
- Sunagawa, K.; Maughan, W.L.; Burkhoff, D.; Sagawa, K. Left Ventricular Interaction with Arterial Load Studied in Isolated Canine Ventricle. Am J Physiol 1983, 245, H773–780. [Google Scholar] [CrossRef] [PubMed]
- Forrester, S.J.; Booz, G.W.; Sigmund, C.D.; Coffman, T.M.; Kawai, T.; Rizzo, V.; Scalia, R.; Eguchi, S. Angiotensin II Signal Transduction: An Update on Mechanisms of Physiology and Pathophysiology. Physiol Rev 2018, 98, 1627–1738. [Google Scholar] [CrossRef] [PubMed]
- Naderi, N. Chapter 11 - Hemodynamic Study. In Practical Cardiology (Second Edition); Maleki, M., Alizadehasl, A., Haghjoo, M., Eds.; Elsevier, 2022; pp. 201–216 ISBN 978-0-323-80915-3.
- Cotter, G.; Moshkovitz, Y.; Kaluski, E.; Milo, O.; Nobikov, Y.; Schneeweiss, A.; Krakover, R.; Vered, Z. The Role of Cardiac Power and Systemic Vascular Resistance in the Pathophysiology and Diagnosis of Patients with Acute Congestive Heart Failure. Eur J Heart Fail 2003, 5, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Vriz, O.; Fadl Elmula, F.M.; Antonini-Canterin, F. Noninvasive Assessment of Ventricular-Arterial Coupling in Heart Failure. Heart Fail Clin 2021, 17(2), 245–254. [Google Scholar] [CrossRef]
- Ikonomidis, I.; Aboyans, V.; Blacher, J.; Brodmann, M.; Brutsaert, D.L.; Chirinos, J.A.; De Carlo, M.; Delgado, V.; Lancellotti, P.; Lekakis, J.; et al. The Role of Ventricular–Arterial Coupling in Cardiac Disease and Heart Failure: Assessment, Clinical Implications and Therapeutic Interventions. A Consensus Document of the European Society of Cardiology Working Group on Aorta & Peripheral Vascular Diseases, European Association of Cardiovascular Imaging, and Heart Failure Association. European Journal of Heart Failure 2019, 21, 402–424. [Google Scholar] [CrossRef]
- Monte, I.P.; Faro, D.C.; Trimarchi, G.; de Gaetano, F.; Campisi, M.; Losi, V.; Teresi, L.; Di Bella, G.; Tamburino, C.; de Gregorio, C. Left Atrial Strain Imaging by Speckle Tracking Echocardiography: The Supportive Diagnostic Value in Cardiac Amyloidosis and Hypertrophic Cardiomyopathy. J Cardiovasc Dev Dis 2023, 10, 261. [Google Scholar] [CrossRef]
- de Gregorio, C.; Trimarchi, G.; Faro, D.C.; De Gaetano, F.; Campisi, M.; Losi, V.; Zito, C.; Tamburino, C.; Di Bella, G.; Monte, I.P. Myocardial Work Appraisal in Transthyretin Cardiac Amyloidosis and Nonobstructive Hypertrophic Cardiomyopathy. Am J Cardiol 2023, 208, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Ommen, S.R.; Mital, S.; Burke, M.A.; Day, S.M.; Deswal, A.; Elliott, P.; Evanovich, L.L.; Hung, J.; Joglar, J.A.; Kantor, P.; et al. 2020 AHA/ACC Guideline for the Diagnosis and Treatment of Patients With Hypertrophic Cardiomyopathy: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2020, 142, e558–e631. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Pavia, P.; Rapezzi, C.; Adler, Y.; Arad, M.; Basso, C.; Brucato, A.; Burazor, I.; Caforio, A.L.P.; Damy, T.; Eriksson, U.; et al. Diagnosis and Treatment of Cardiac Amyloidosis. A Position Statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur J Heart Fail 2021, 23, 512–526. [Google Scholar] [CrossRef]
- Arbelo, E.; Protonotarios, A.; Gimeno, J.R.; Arbustini, E.; Barriales-Villa, R.; Basso, C.; Bezzina, C.R.; Biagini, E.; Blom, N.A.; De Boer, R.A.; et al. 2023 ESC Guidelines for the Management of Cardiomyopathies. European Heart Journal 2023, 44, 3503–3626. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2015, 28, 1–39. [Google Scholar] [CrossRef]
- Olsen, F.J.; Skaarup, K.G.; Lassen, M.C.H.; Johansen, N.D.; Sengeløv, M.; Jensen, G.B.; Schnohr, P.; Marott, J.L.; Søgaard, P.; Gislason, G.; et al. Normal Values for Myocardial Work Indices Derived From Pressure-Strain Loop Analyses: From the CCHS. Circ Cardiovasc Imaging 2022, 15, e013712. [Google Scholar] [CrossRef]
- Authors/Task Force Members; McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; et al. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure: Developed by the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure of the European Society of Cardiology (ESC). With the Special Contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2022, 24, 4–131. [Google Scholar] [CrossRef]
- Hiemstra, Y.L.; Bijl, P. van der; Mahdiui, M. el; Bax, J.J.; Delgado, V.; Marsan, N.A. Myocardial Work in Nonobstructive Hypertrophic Cardiomyopathy: Implications for Outcome. J Am Soc Echocardiogr 2020, 33, 1201–1208. [Google Scholar] [CrossRef]
- Garcia Brás, P.; Rosa, S.A.; Cardoso, I.; Branco, L.M.; Galrinho, A.; Gonçalves, A.V.; Thomas, B.; Viegas, J.M.; Fiarresga, A.; Branco, G.; et al. Microvascular Dysfunction Is Associated With Impaired Myocardial Work in Obstructive and Nonobstructive Hypertrophic Cardiomyopathy: A Multimodality Study. J Am Heart Assoc 2023, 12, e028857. [Google Scholar] [CrossRef]
- Clemmensen, T.S.; Eiskjær, H.; Ladefoged, B.; Mikkelsen, F.; Sørensen, J.; Granstam, S.-O.; Rosengren, S.; Flachskampf, F.A.; Poulsen, S.H. Prognostic Implications of Left Ventricular Myocardial Work Indices in Cardiac Amyloidosis. European Heart Journal - Cardiovascular Imaging 2021, 22, 695–704. [Google Scholar] [CrossRef]
- Licordari, R.; Trimarchi, G.; Teresi, L.; Restelli, D.; Lofrumento, F.; Perna, A.; Campisi, M.; de Gregorio, C.; Grimaldi, P.; Calabrò, D.; et al. Cardiac Magnetic Resonance in HCM Phenocopies: From Diagnosis to Risk Stratification and Therapeutic Management. J Clin Med 2023, 12, 3481. [Google Scholar] [CrossRef] [PubMed]
- Moura, B.; Aimo, A.; Al-Mohammad, A.; Keramida, K.; Ben Gal, T.; Dorbala, S.; Todiere, G.; Cameli, M.; Barison, A.; Bayes-Genis, A.; et al. Diagnosis and Management of Patients with Left Ventricular Hypertrophy: Role of Multimodality Cardiac Imaging. A Scientific Statement of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2023, 25, 1493–1506. [Google Scholar] [CrossRef] [PubMed]
- Suga, H.; Sagawa, K. Instantaneous Pressure-Volume Relationships and Their Ratio in the Excised, Supported Canine Left Ventricle. Circ Res 1974, 35, 117–126. [Google Scholar] [CrossRef]
- Duan, Q.; Tao, H.; Dong, Q.; Liao, K.; Yang, Y.; Cheng, X.; Ge, P. Non-Invasive Global Myocardial Work Index as a New Surrogate of Ventricular-Arterial Coupling in Hypertensive Patients with Preserved Left Ventricular Ejection Fraction. Front Cardiovasc Med 2022, 9, 958426. [Google Scholar] [CrossRef] [PubMed]
- Mihalcea, D.; Memis, H.; Balinisteanu, A.; Vladareanu, A.-M.; Mihaila, S.; Vinereanu, D. Myocardial Work-A New Tool for Early Detection of Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, Prednisone Chemotherapy Induced-Cardiotoxicity in Hematological Patients. J Clin Ultrasound 2023, 51, 377–384. [Google Scholar] [CrossRef]
- Palmiero, G.; Vetrano, E.; Rubino, M.; Monda, E.; Dongiglio, F.; Lioncino, M.; Di Fraia, F.; Caiazza, M.; Verrillo, F.; Capodicasa, L.; et al. The Role of New Imaging Technologies in the Diagnosis of Cardiac Amyloidosis. Heart Fail Clin 2022, 18, 61–72. [Google Scholar] [CrossRef]
- Henein, M.Y.; Lindqvist, P. Myocardial Work Does Not Have Additional Diagnostic Value in the Assessment of ATTR Cardiac Amyloidosis. J Clin Med 2021, 10, 4555. [Google Scholar] [CrossRef]
- Roger-Rollé, A.; Cariou, E.; Rguez, K.; Fournier, P.; Lavie-Badie, Y.; Blanchard, V.; Roncalli, J.; Galinier, M.; Carrié, D.; Lairez, O.; et al. Can Myocardial Work Indices Contribute to the Exploration of Patients with Cardiac Amyloidosis? Open Heart 2020, 7, e001346. [Google Scholar] [CrossRef]
- de Gregorio, C. , Micari, A., Di Bella, G., Carerj, S., Coglitore, S. Systolic wall stress may affect the intramural coronary blood flow velocity in myocardial hypertrophy, independently on the left ventricular mass. Echocardiography. [CrossRef]
- Briasoulis, A.; Bampatsias, D.; Petropoulos, I.; Rempakos, A.; Patras, R.; Theodorakakou, F.; Makris, N.; Dimopoulos, M.A.; Stamatelopoulos, K.; Kastritis, E. Left Ventricular Myocardial Work Improves in Response to Treatment and Is Associated with Survival Among Patients with Light-Chain Cardiac Amyloidosis. Eur Heart J Cardiovasc Imaging 2023, jead351. [Google Scholar] [CrossRef]
- Barroso, F.A.; Coelho, T.; Dispenzieri, A.; Conceição, I.; Waddington-Cruz, M.; Wixner, J.; Maurer, M.S.; Rapezzi, C.; Planté-Bordeneuve, V.; Kristen, A.V.; et al. Characteristics of Patients with Autonomic Dysfunction in the Transthyretin Amyloidosis Outcomes Survey (THAOS). Amyloid 2022, 29, 175–183. [Google Scholar] [CrossRef]
- Di Bella, G.; Cappelli, F.; Licordari, R.; Piaggi, P.; Campisi, M.; Bellavia, D.; Minutoli, F.; Gentile, L.; Russo, M.; de Gregorio, C.; et al. Prevalence and Diagnostic Value of Extra-Left Ventricle Echocardiographic Findings in Transthyretin-Related Cardiac Amyloidosis. Amyloid 2022, 29, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Holm, H.; Magnusson, M.; Jujić, A.; Bozec, E.; Girerd, N. How to Calculate Ventricular-Arterial Coupling? Eur J Heart Fail 2022, 24(4), 600–602. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Median values of global myocardial constructive work (GCW), global work index (GWI) and systemic vascular resistance (SVRc) in the study population. ATTR, wild-type transthyetin amyloid cardiomyopathy HCM, hypertrophic cardiomyopathy; SVRc, systemic vascular resistance, corrected (see methods). HCM vs ATTR: *p=0.008; #p=0.001. Differences in SVRc between the groups were significant (p=0.008).
Figure 1.
Median values of global myocardial constructive work (GCW), global work index (GWI) and systemic vascular resistance (SVRc) in the study population. ATTR, wild-type transthyetin amyloid cardiomyopathy HCM, hypertrophic cardiomyopathy; SVRc, systemic vascular resistance, corrected (see methods). HCM vs ATTR: *p=0.008; #p=0.001. Differences in SVRc between the groups were significant (p=0.008).
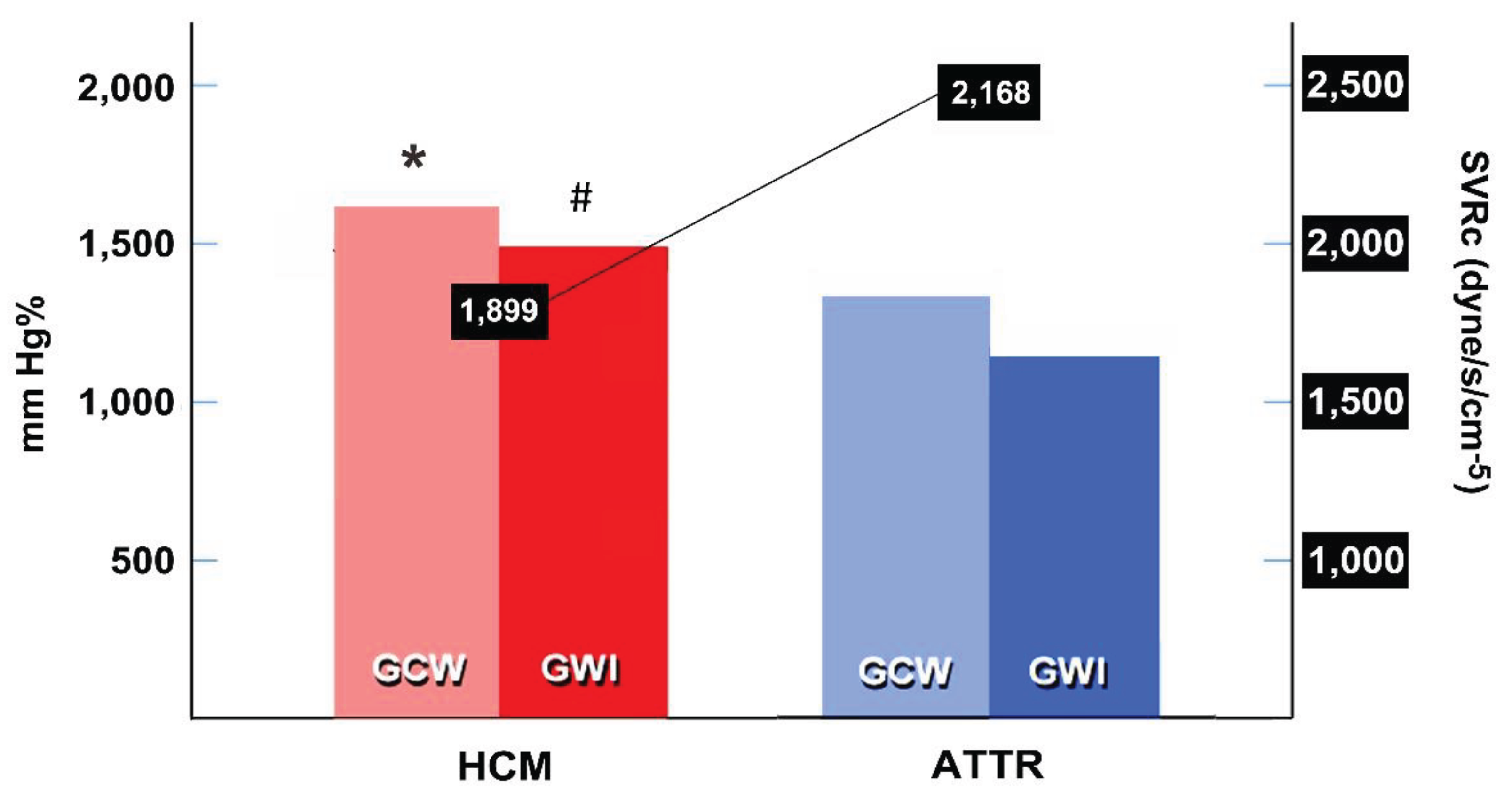

Table 1.
Demographic and clinical characteristics of study population.
| HCM (n=30) | ATTR (n=30) | P value | |
|---|---|---|---|
| Age, years | 58 [54 – 73] | 69 [62 – 78] | <0.001 |
| Males | 24 (80%) | 23 (77%) | 0.754 |
| Body surface area, m2.7 | 1.9 [1.7 – 2.0] | 1.7 [1.6 – 1.9] | <0.001 |
| Systolic BP, mm Hg | 128.8 ± 11.9 | 128.5 ± 12.7 | 0.925 |
| Diastolic BP, mm Hg | 77.4 ± 12.3 | 80.7 ± 7.9 | 0.226 |
| Mean BP, mm Hg | 94.5 ± 10.3 | 96.6 ± 7.4 | 0.375 |
| Pulse pressure, mm Hg | 51.4 ± 13.5 | 47.9 ±13.5 | 0.311 |
| Heart rate, bpm | 67.2 ± 11.3 | 68.4 ± 11.2 | 0.690 |
| NYHA class I-III | 1.4 ± 0.56 | 1.9 ± 0.46 | <0.001 |
| Dyspnea | 7 (23%) | 23 (77%) | <0.001 |
| Family history of SD | 7 (23%) | 3 (10%) | 0.166 |
| Implantable cardioverter defibrillator | 3 (10%) | 1 (3%) | NA |
| Therapy | |||
| Beta-blockers | 25 (83%) | 10 (33%) | <0.001 |
| Calcium antagonists | 11 (37%) | 5 (17%) | 0.080 |
| ACE-inhibitors | 8 (27%) | 2 (7%) | 0.07 |
| ARB | 1 (3%) | 7 (23%) | 0.023 |
| Statins | 6 (20%) | 15 (50%) | 0.015 |
| Anti-coagulants | 6 (20%) | 6 (20%) | 1.000 |
| Anti-platelet drugs | 5 (17%) | 9 (30%) | 0.222 |
| Diuretics | 4 (13%) | 17 (57%) | <0.001 |
| Tafamidis 65 mg | - | 30 (100%) | NA |
| Values are numbers (%), mean ± SD, or median values [IQR], as appropriate. ACE, angiotensin-converting enzyme; ARB, angiotensin receptor antagonists; ATTR, wild-type transthyretin cardiac amyloidosis; BP, blood pressure; HCM, nonobstructive hypertrophic cardiomyopathy; NA, not available/performed; SCD, sudden cardiac death. | |||
Table 2.
Main echocardiographic measurements in both study groups.
| HCM (n=30) | ATTR (n=30) | P value | |
|---|---|---|---|
| Left ventricular end-diastolic volume index, mL/m2.7 | 51.4 [37.9 – 59.8] | 49.7 [38.7 – 60.0] | 0.831 |
| Left ventricular end-systolic volume index, mL/m2.7 | 18.8 [15.0 – 25.9] | 23.2 [17.2 – 27.1] | 0.020 |
| Left ventricular ejection fraction, % | 63.4 [54.4 – 63.8] | 55.0 [52.3 – 57.2] | <0.001 |
| Stroke volume index, mL/m2.7 | 32.5 [23.2 – 36.3] | 27.8 [21.5 – 31.8] | 0.444 |
| Cardiac output, L/min | 3.9 [2.8 – 4.4] | 3.4 [2.4 – 3.7] | 0.004 |
| Ventricular septum thickness, mm | 15.2 [14.6 – 18.0] | 15.5 [14.0 – 21.0] | 0.688 |
| Mitral E / tissue E' velocity ratio | 11.7 ± 5.0 | 16.8 ± 5.9 | 0.001 |
| Global longitudinal strain, -% | 15.0 [16.0 – 10.3] | 12.5 [14.5 – 10.0] | 0.022 |
| Global myocardial work index, mm Hg% | 1468.5 ± 403.5 | 1149.7 ± 319.3 | 0.001 |
| Global constructive work, mm Hg% | 1442 [989 – 1554] | 1141 [874 - 1356] | 0.008 |
| Left atrial volume index, ml/m2.7 | 43.7 ± 16.2 | 44.6 ± 15.5 | 0.991 |
| Systemic vascular resistance (corrected), dyne/s/cm-5 | 1899 [1693 – 2600] | 2168 [2051 – 2860] | 0.008 |
| Measurements are expressed as mean values ± SD or median values [IQR], as appropriate. | |||
Table 3.
Classification of study population based on SVRc and GWI (see also Figure 2).
Table 3.
Classification of study population based on SVRc and GWI (see also Figure 2).
| HCM (n=30) | ATTR (n=30) | Total (n=60) | |
|---|---|---|---|
| Class A (best class) | 4 (13%) | - | 4 (7%) |
| Class B (impaired GWI) | 5 (17%) | - | 5 (8%) |
| Class C (poorest class) | 13 (43%) | 28 (93%) | 41 (68%) |
| Class D (higher SVRc) | 8 (27%) | 2 (7%) | 10 (17%) |
| Differential characteristics in subclass patients with HCM | |||
| Class C (n=13) | Other Classes (n=17) | p-value | |
| Stroke volume index, ml/ m2.7 | 26.7 ± 8.7 | 37.5 ± 10.8 | 0.005 |
| LV end-diastolic volume index, ml/ m2.7 | 43.7 ± 12.8 | 57.5 ± 16.1 | 0.015 |
| GLS, -% | 13.0 ± 3.4 | 16.0 ± 4.3 | 0.043 |
| IVS thickness, mm | 18.2 ± 3.4 | 15.6 ± 2.8 | 0.029 |
| LV ejection fraction, % | 60.6 ± 6.1 | 64.8 ± 5.1 | 0.055 |
| Age, years | 58.7 ± 13.0 | 48.9 ± 16.2 | 0.076 |
| Left atrial volume index, ml/ m2.7 | 47.1 ± 20.8 | 41.14 ± 11.6 | 0.368 |
| Measurements are expressed as mean values ± SD. HCM, hypertrophic cardiomyopathy; GLS, global longitudinal strain; IVS, interventricular septum; LV, left ventricle/ventricular. | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



