
Submitted:
08 March 2024
Posted:
11 March 2024
You are already at the latest version
Abstract
The late diagnosis of Type 2 Diabetes Mellitus can occur due to lack of access to the primary health care system and the non-manifestation of symptoms. Faced with this problem, this work presents the creation of a mobile application, called DiabetesCheck, for predicting the risk of Type 2 Diabetes Mellitus. A mathematical model is used, which classifies the risk of Type 2 Diabetes Mellitus for a group of patients with intervention and for a comparative group, using Fuzzy Classification and Decision Trees. The proposed application allows the health professional to monitor patients through the history stored in a database, allowing a representation of the evolution of patients and indication of medications. Therefore, this proposal aims to carry out the diagnosis in the initial phase of the disease and help in the prescription of more effective treatments and in the proposition of public policy strategies in epidemiology and screening.
Keywords:
Type 2 Diabetes Mellitus
; mobile application
; primary health care
; evolution of patients
1. Introduction
According to Whiting [1], Diabetes Mellitus is one of the most common chronic diseases in almost all countries and continues to increase in number of occurrences and significance. Economic development and urbanization drive changes in lifestyle, which causes a reduction in physical activity and an increase in obesity, which impacts the development of the disease.
The World Health Organization [2] estimates that the number of people with diabetes increased from 108 million in 1980 to 422 million in 2014, in terms of prevalence. Low- and middle-income countries have a higher proportion of cases than high-income countries. Regarding mortality, between 2000 and 2019, there was a 3% increase in mortality rates, in addition, diabetes and kidney disease caused by diabetes promoted around 2 million deaths in this period [2].
Diabetes Mellitus is a common disease in glucose metabolism, resulting from inefficient production or poor absorption of insulin in the body [3]. Diabetes Mellitus describes a group of metabolic disorders characterized by increased blood glucose concentration. People living with diabetes are at higher risk of morbidity and mortality than the general population. The global prevalence of diabetes in adults has increased in recent decades [4].
Insulin is a hormone produced by the pancreas, whose function is to break down glucose molecules and transform them into energy to maintain the body’s cells. Therefore, when these molecules are not broken down and used as they should, there is an accumulation of glucose in the blood (hyperglycemia), causing several problems for the patient [3].
Most of the time, the disease does not present characteristic symptoms (asymptomatic) and, as routine exams are not performed, mainly due to the difficulty of accessing primary care in the health area of the region where they live, most patients receive a late diagnosis, with several complications, such as slow wound healing, loss of vision (blindness), problems with the kidneys (kidney failure) and heart (heart attacks and stroke), amputation of lower limbs and even death [2].
On the other hand, there is increasing evolution in the area of technology with the development of software systems (for example, mobile applications) for the most diverse uses and devices. In the work of Vêsvoci [5], a mobile application is presented for evaluating the feet of people with Diabetes Mellitus, validated by nurses regarding aspects of functionality, reliability, usability and efficiency. A narrative review was carried out in [6], whose objective was to identify and characterize the mobile applications available on Google PlayStore related to Diabetes Mellitus. Most applications can improve the management of this chronic condition and promote self-care, proving to be a promising tool.
Regarding this scenario, considering that public health is faced with a serious problem in relation to Diabetes Mellitus and that technology can assist in early diagnosis and prescription of more effective treatments, the objective of this work is to present the development of a mobile application, the DiabetesCheck, for predicting the risk of Type 2 Diabetes Mellitus, aiming to assist health professionals and public health managers in diagnosing the disease in patients and providing assistance to prescribe appropriate treatments, with greater chances of success.
The main contribution of the DiabetesCheck is to allow healthcare professionals to monitor the evolution of their patients through the history stored in a database, which is presented graphically, allowing a representation of the patients’ evolution and enabling better decision-making. decisions regarding medication maintenance.
It is worth mentioning that Type 2 Diabetes Mellitus can be treated and its consequences avoided or delayed with a healthy diet, regular physical activity, medication, maintaining normal body weight, avoiding tobacco use, regular screening in the primary healthcare system and treatment of complications [2,7]. The mathematical model proposed in [8] was used to guide the development of the application. This model classifies the risk of type 2 Diabetes Mellitus for the group of patients with intervention and for the comparative group using Fuzzy Logic and Decision Trees. The intervention is based on the use of the nursing case management method, with multidisciplinary care, educational actions in groups, home care and telephone approach [9]. The comparative group consists of conventional treatment of the disease, using medication.
According to the cross-validation process, this model presented 73.68% accuracy for the intervention group and 69.23% accuracy for the comparative group. In this way, the results obtained in [8] were satisfactory and could contribute to controlling and predicting the development of patients with type 2 Diabetes Mellitus. Complementing this mathematical study, the development of the DiabetesCheck application contributes to make the results more accessible and applicable in the practice of health professionals, providing better data visibility for more assertive prescription.
2. Materials and Methods
2.1. Mathematical Models
Introduced in 1965 by Zadeh [10], Fuzzy Logic makes it possible to represent models with a level of imprecision and express them as a set of linguistic rules. This ability to work with uncertainties and overlaps between the edges of class intervals makes the model more consistent and mathematically easier to interpret.
In this work, considering the development of the proposed application, some features of patients with diabetes were considered as input variables for the classification of the glycemic index, namely: age, triglycerides, evolutionary time, Body Mass Index (BMI), abdominal circumference, income and education. Each attribute has a defined range for the linguistic fuzzy variables “low, medium and high”, both for the intervention group (Table 1) and for the comparative group (Table 2) [8]. All patients are diabetic and follow conventional medication treatment. However, as described previously, the intervention group receives a personal monitoring by professionals, while the comparative group does not. Each trio of values [A, B, C] represents the so-called “membership functions” (Figure 1), for example, for the input variable “age”.
For each group, a base of “if-then” linguistic rules was developed, combining the values of the inputs. A total of 11 rules were created for the Intervention group and 11 rules for the Comparative group, which are expressed and determined using Decision Trees, as shown in Figure 2 and Figure 3, respectively. The output classes, related to the task of classifying the glycemic index of diabetic patients, are: I = Increased, D = Decreased, S = Stable and DL = Decreased a lot. Using the data presented in Table 1 and Table 2, the Fuzzy classification steps were carried out, using the JFuzzyLogic [11] library, loading the rules for each group.
2.2. Application Development
The DiabetesCheck app was developed using current technologies (Ionic - https://ionicframework.com e Spring - https://spring.io). Ionic is a technology for developing hybrid mobile applications, that is, they can be used on different operating systems and devices. Spring is a framework whose objective is to facilitate the development of business logic and access to application data.
Regarding data storage, a relational database management system called MySQL (https://www.mysql.com/) was used. In this way, the application structure was organized into three parts: frontend (Ionic), backend (Spring) and database (MySQL). The user interacts with the application through the frontend, using their mobile device, which, in turn, accesses the backend, which stores and retrieves data from the database (Figure 4).
Figure 5A–C show the application’s home screen, the login screen and the account creation screen, respectively. Regarding functionality (Figure 6A), the healthcare professional has the following options available:
- Patients: allows nurses to view patients registered in the system, edit or delete data for a specific patient and add new patients (Figure 6B);
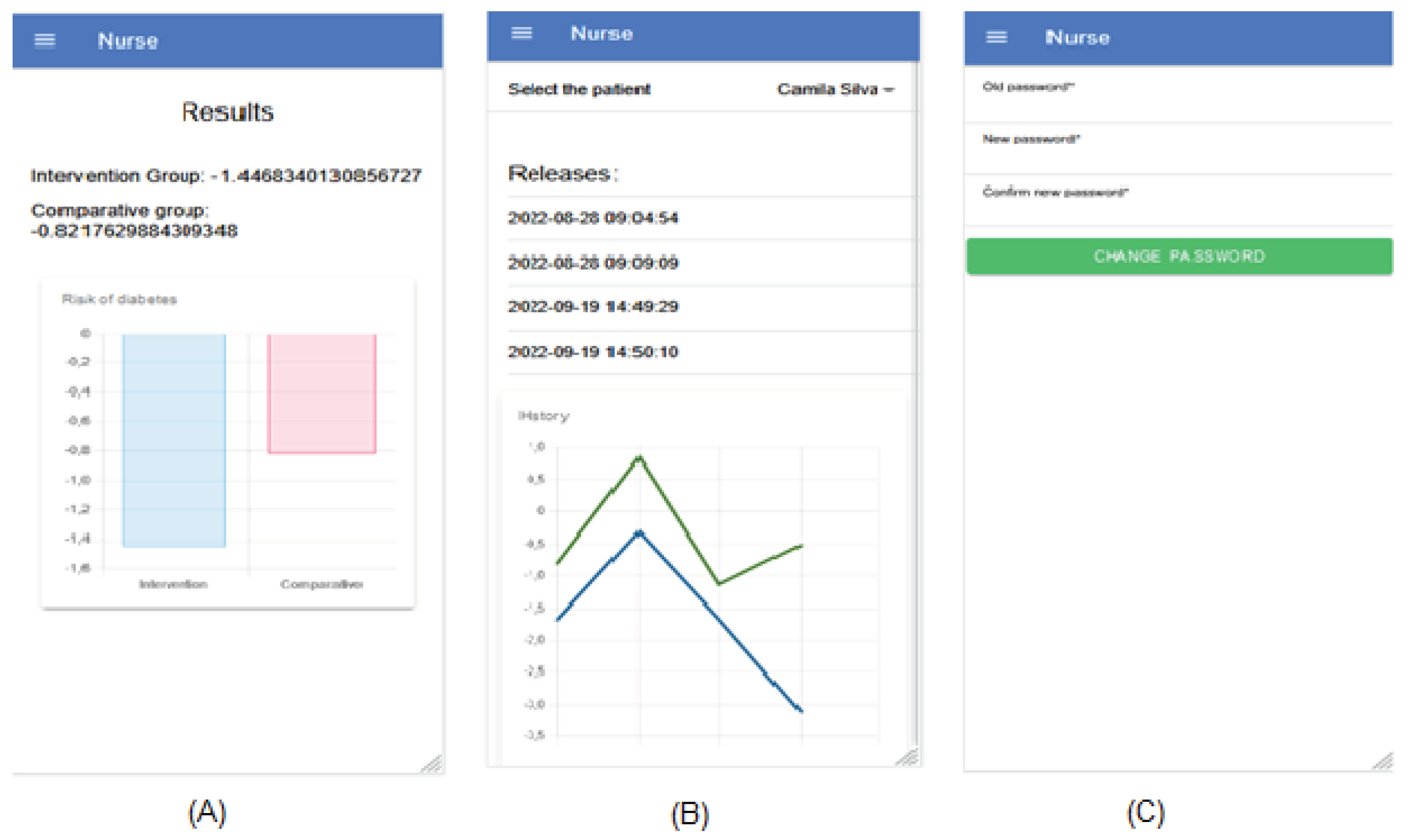
- Launch: when selecting a patient, new entries can be made (Figure 6C). To do this, data from the last entry performed for that patient is shown, providing the nurse with a view of whether the current values are higher or lower than the last time they were entered. At the end of the launch, the results obtained for the two groups are shown numerically and graphically (Figure 7A);
- View history: when selecting a patient, all entries made for him and their respective dates and times are listed (Figure 7B). Also, a line graph is presented, where each point refers to the result found in a launch, with two lines, with the blue line indicating the Intervention group and the green line the Comparative group. This enables future analyzes of the variation in results obtained that can lead to good or bad consequences for the patient’s condition;
- Update password: allows the user to change their access password whenever necessary (Figure 7C). If the user forgets their password and uses the option in Figure 5B to recover it, they will receive an email with a randomly generated password with which they can log in. Thus, with the option to update password, he can change it to a password he deems more appropriate, maintaining the security of his account.
Figure 7.
Other DiabetesCheck functionality for healthcare professionals.
For the administrator, the following options are available (Figure 8A):
- Report: allows the administrator to view a report on which patients were seen by a specific nurse in a specified date range (Figure 8B). To do this, he selects the name of the nurse who wants to perform the search and the date range. The list of patients will then be shown. This report is useful in several analyses, such as knowing who served the most patients;
- Activate users: allows the administrator to authorize new users to access the application (Figure 8C). To do this, a list of users who have recently registered and are awaiting approval is shown. Whenever a user registers on the application, their access is not granted. It is the administrator’s role to do this, being able to control who has access to patient data and providing greater security.
3. Results and Discussion
In this section, a comparison of DiabetesCheck app with related applications [12] is discussed in Subsection 3.1. Next, a self-assessment on user experience and usability is presented in section 3.2, considering the guidelines proposed by [13].
3.1. Discussion
In the literature, some works that address the development of a mobile application that considers Diabetes Mellitus can be found. In [12], the authors considered the high incidence of Diabetes Mellitus in the world population and the growing trend of using mobile applications to survey and characterize applications available on the Google Play Store platform related to Diabetes Mellitus. To achieve this, the authors developed a narrative review of the applications, using the search string: “Diabetes Mellitus”.
Some data was collected, such as the name of the application, whether it is free or not, the description of the application, target audience, category, number of downloads, developer, last update and the first ten user reviews. As a result, 222 applications were found, with a predominance in the Medicine category (87 applications) and Health and Fitness (77 applications) that work as data storage, carbohydrate counting, medication reminders and others. Finally, they concluded that most applications can improve the management of Diabetes Mellitus and promote self-care [12].
A mapping of scientific production on mobile applications for self-management of care aimed at the elderly was developed in [14]. As a result, 14 articles were mapped, categorized into three management aspects: medications, comorbidities and healthy practices. In most studies, the applications were aimed at self-management of medications, followed by care for chronic conditions and, finally, self-assessment of the risk of falls and non-pharmacological pain treatments. Of these works, 4 were dedicated to the topic of diabetes. Also aimed at seniors, [15] conducted a study on how seniors with type 2 diabetes and hypertension use an online app designed to help manage these conditions. Usability testing was performed on the TAPESTRY-CM Healthy Lifestyle App, an online self-management application. This included an online session, using a cognitive interview approach and semi-structured interviews at various points in time.
Zheng et al. [16] examined actual use of various health monitors for lifestyle changes over 3 months among elderly with Diabetes Mellitus. Additionally, they explored changes in caloric intake and physical activity (PA) over 3 months. This was a single-group study lasting 3 months. The study sample included participants aged years diagnosed with Diabetes Mellitus. The results suggest the need for a larger study to confirm them.
In [17], the authors developed an app called GlucoNote that uses Apple’s ResearchKit to support self-management for patients with type 2 diabetes and prediabetes. This app does not require a prescription or intervention from medical professionals. Their usage patterns were assessed through a remotely conducted study. As a result, GlucoNote provided an opportunity to evaluate application usage patterns. In [18], the authors understood users’ acceptability of a mobile app for diabetes self-management and explored their communication with healthcare personnel about the app. It is interesting to note that if users found the app’s usefulness acceptable, they might tolerate some lack of usability.
Table 3 presents the comparison between the related works and the DiabetesCheck app, proposed in this paper. The first column presents the reference for the works in question and the subsequent ones present the comparison criteria between them.
Therefore, observing Table 3, most of the applications developed are aimed at the elderly and for monitoring medications, reminders and healthy practices. Unlike the articles presented previously, the DiabetesCheck app consists of allowing healthcare professionals, duly registered in the DiabetesCheck application, to monitor and predict the risk of diabetes in relation to the evolution of their patients. This way, the healthcare professional has the history of their patients stored in a database. This history is presented graphically, which allows healthcare professionals to have a representation of the evolution of their patients and make decisions regarding the maintenance of medications.
3.2. Self-Assessment on User Experience and Usability
In [13], the authors propose the “User Experience and Usability Guidelines for Agile Project (UXUG-AP)” technique, composed of a set of guidelines that support the design and evaluation of software system prototypes, in terms of the user experience and usability. In Table 4, technique guidelines are presented, grouped by categories, as well as the result of the self-assessment for the DiabetesCheck application. The self-assessment was conducted by two system developers and two health professionals.
As can be seen in Table 4, 11 of the 15 guidelines (74%) proposed by the UXUG-AP technique are implemented in the DiabetesCheck application.
4. Conclusions
DiabetesCheck is a mobile application that provides several functions designed to predict diabetes risk. It can be used by various health professionals (nurses, nursing technicians, doctors, health managers, residents), with the aim of assisting in the diagnosis and treatment of diabetes, a disease that, although common, in most cases, is only detected when it is in an advanced stage, causing serious consequences for the patient, as it is asymptomatic in specific age groups.
In this way, DiabetesCheck aims to provide health professionals with a tool that helps them predict the risk of diabetes in their patients, to serve those who have difficulty accessing specialized doctors in the region where they live, that is, a support tool in terms of primary health care. Based on the results obtained, they can prescribe the treatment they deem most appropriate, which can range from dietary changes and physical exercise to medications and synthetic insulin injections. This increases the chances of treatment success and gives patients more confidence, in addition to enabling elements of clinical epidemiology applied to the development of public health actions in a specific population.
As perspectives for continuing this work, it is proposed to develop an evaluation of the application by users, based on an application evaluation questionnaire that must be developed based on the indicators and sentences of the TAM model (Technology Acceptance Model). Furthermore, efforts will be invested to address the limitations highlighted with the application of the UXUG-AP technique.
Author Contributions
Conceptualization, G.M.B., P.A.P.J. and E.A.S.L.; methodology, G.M.B., P.A.P.J., H.C. and E.A.S.L.; software, P.A.P.J., H.C. and I.C.J.; validation, G.M.B., P.A.P.J., H.C. and E.A.S.L.; formal analysis, G.M.B., P.A.P.J. and E.A.S.L.; investigation, G.M.B., P.A.P.J. and E.A.S.L.; data curation, G.M.B., P.A.P.J. and I.C.J.; writing—original draft preparation, G.M.B., P.A.P.J., H.C. and I.C.J.; writing—review and editing, G.M.B., P.A.P.J. and E.A.S.L.; visualization, G.M.B., P.A.P.J. and E.A.S.L.; supervision, G.M.B., P.A.P.J., H.C. and E.A.S.L.; project administration, G.M.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Whiting, D.R.; Guariguata, L.; Weil, C.; Shaw, J. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res Clin Pract. 2011, 94, 311–321. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization - WHO. Diabetes. [Internet]. 2023. Available in: https://www.who.int/news-room/fact-sheets/detail/diabetes.
- American Diabetes Association - ADA. Standards of medical care in diabetes—2015 abridged for primary care providers. Clin Diabetes 2015, 33, 97. [Google Scholar] [CrossRef] [PubMed]
- Ogurtsova, K.; da Rocha Fernandes, J.D.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; et al. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Vêscovi, S.D.J.B.; Primo, C.C.; Sant’Anna, H.C.; Bringuete, M.E.D.O.; Rohr, R.V.; Prado, T.N.D.; et al. Aplicativo móvel para avaliação dos pés de pessoas com diabetes mellitus. Acta Paul Enferm. 2017, 30, 607–613. [Google Scholar] [CrossRef]
- Marcelo, C.A.S.; Coutinho, M.A.P.; Lara, C.R.; Paraizo, C.M.S.; Fava, S.M.C. Aplicativos móveis sobre diabetes mellitus - Revisão Narrativa. J Health Inform. 2020, 12. [Google Scholar]
- McLellan, K.C.P.; Barbalho, S.M.; Cattalini, M.; Lerario, A.C. Diabetes mellitus do tipo 2, síndrome metabólica e modificação no estilo de vida. Rev Nutr. 2007, 20, 515–524. [Google Scholar] [CrossRef]
- Bressan, G.M.; de Azevedo, B.C.F.; Souza, R.M. A Fuzzy Approach for Diabetes Mellitus Type 2 Classification. Braz Arch Biol Technol. 2020, 63, 1–11. [Google Scholar] [CrossRef]
- Castanho, R.M.. Efeito do uso do método de gerenciamento de caso sobre o controle glicêmico de pessoas com diabetes mellitus tipo 2. [Dissertação de Doutorado]. Curitiba PR: Universidade Federal do Paraná; 2013.
- Zadeh, L.A. . Conjuntos difusos. Inf Ao Controle. 1965, 8, 338–353. [Google Scholar] [CrossRef]
- Cingolani, P.; Alcala-Fdez, J. jFuzzyLogic: a robust and flexible Fuzzy-Logic inference system language implementation. In: 2012 IEEE International Conference on Fuzzy Systems. IEEE; 2012. p. 1-8.
- Marcelo, C.A.S.; Pereira Coutinho, M.A.; Lara, C.R.; Silva Paraizo, C.M.; Coelho Leite Fava, S.M. Aplicativos Móveis sobre Diabetes Mellitus - Revisão Narrativa. J Health Inform. Disponível em: https://jhi.sbis.org.br/index.php/jhi-sbis/article/view/726.. 2020, 12. [Google Scholar]
- Sousa, A.; Malveira, N.. Designing Usability and UX with UXUG-AP: Na Observational Study and an Interview with Experts. In: XVII Brazilian Symposium on Information Systems, SBSI. New York, USA: Association for Computing Machinery; 2021.
- Gomes, M.L.F.; Linhares, M.I.F.; Ferreira, C.F.; Fernandes, C.I.; Silva, M.S.; Sousa, M.A.; et al. Aplicativos móveis direcionados aos idosos para autogerenciamento do cuidado: revisão de escopo. Rev Cuidarte. 2023, 14, e2594. [Google Scholar]
- Smith-Turchyn, J.; Gravesande, J.; Agarwal, G.; Mangin, D.; Javadi, D.; Peter, J.; et al. A Healthy Lifestyle App for Older Adults with Diabetes and Hypertension: Usability Assessment. Int J Healthc Technol Manag. 2017, 16, 250–270. [Google Scholar] [CrossRef]
- Zheng, Y.; Weinger, K.; Greenberg, J.; Burke, L.E.; Sereika, S.M.; Patience, N.; et al. Actual Use of Multiple Health Monitors Among Older Adults With Diabetes: Pilot Study. JMIR Aging 2020, 3, e15995. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, S.; Waki, K.; Nannya, Y.; Nangaku, M.; Kadowaki, T.; Ohe, K. Usage Patterns of GlucoNote, a Self-Management Smartphone App, Based on ResearchKit for Patients With Type 2 Diabetes and Prediabetes. JMIR Mhealth Uhealth. 2019, 7. [Google Scholar] [CrossRef] [PubMed]
- Torbjørnsen, A.; Ribu, L.; Rønnevig, M.; Grøttl, A.; Helseth, S. Users’ Acceptability of a Mobile Application for Persons with Type 2 Diabetes: A Qualitative Study. BMC Health Serv Res. 2019, 19, 641. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Triangular membership function for the age variable.
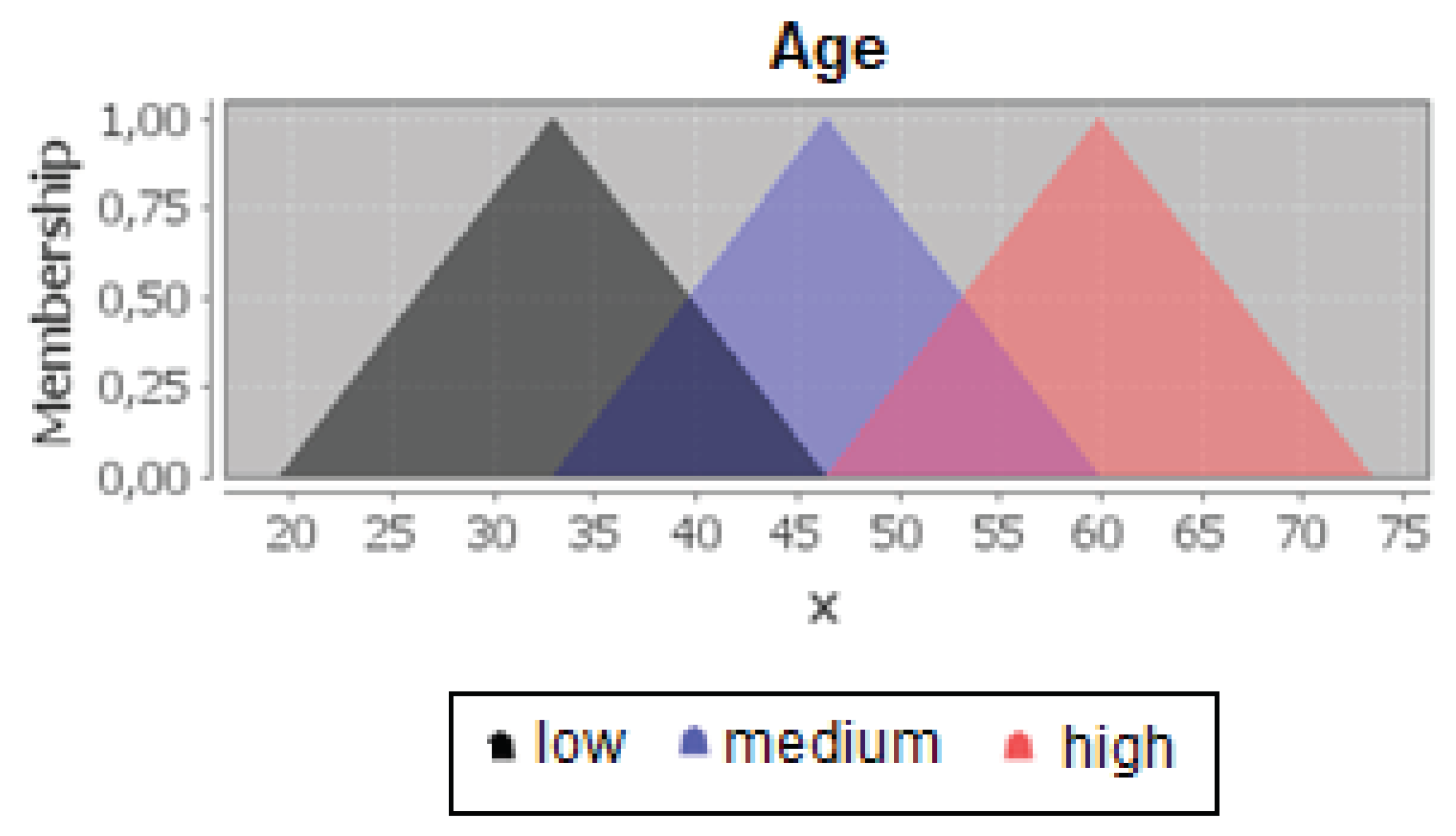
Figure 2.
Decision Tree for the Intervention Group [8].
Figure 2.
Decision Tree for the Intervention Group [8].
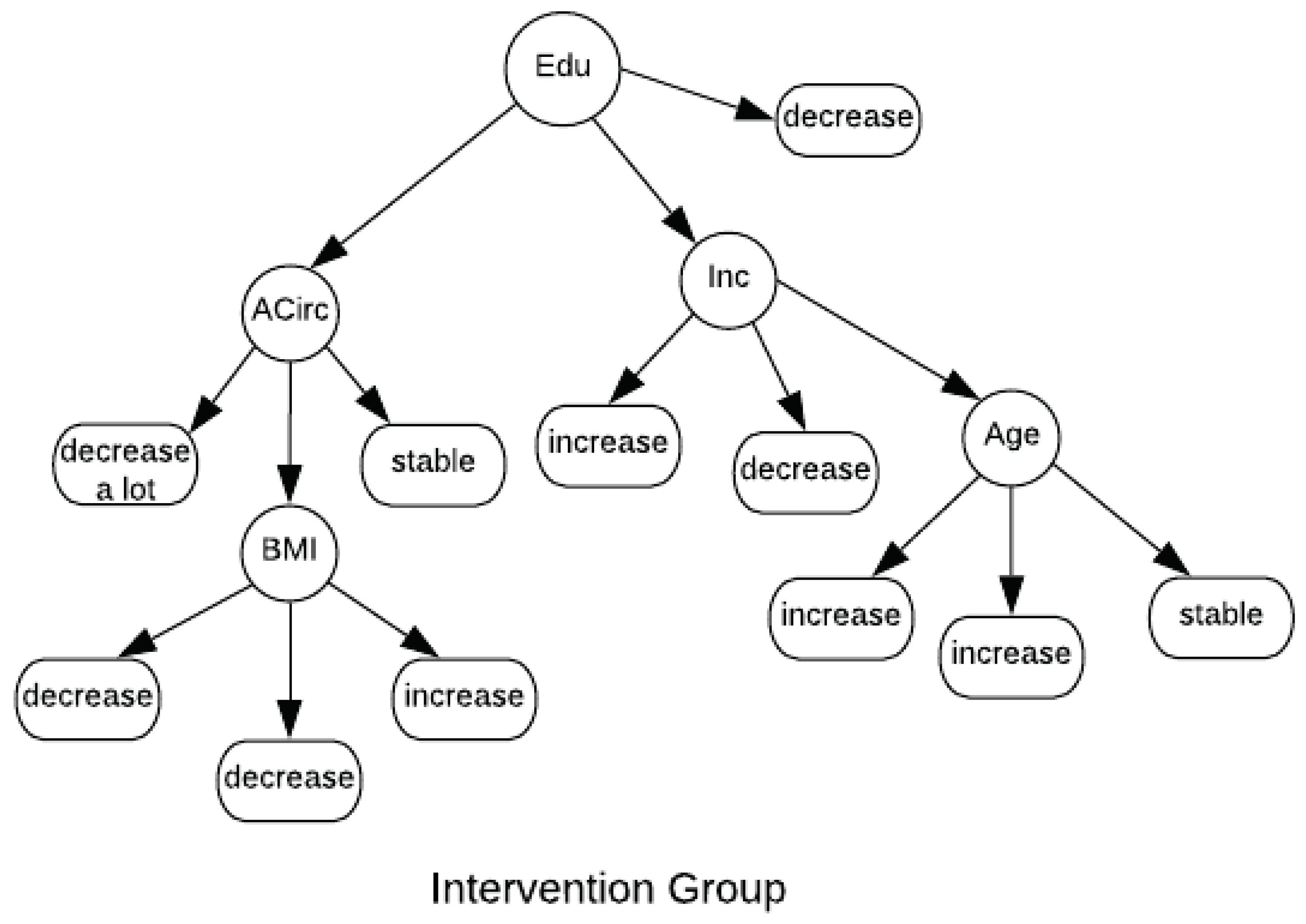
Figure 3.
Decision Tree for the Comparative Group [8].
Figure 3.
Decision Tree for the Comparative Group [8].
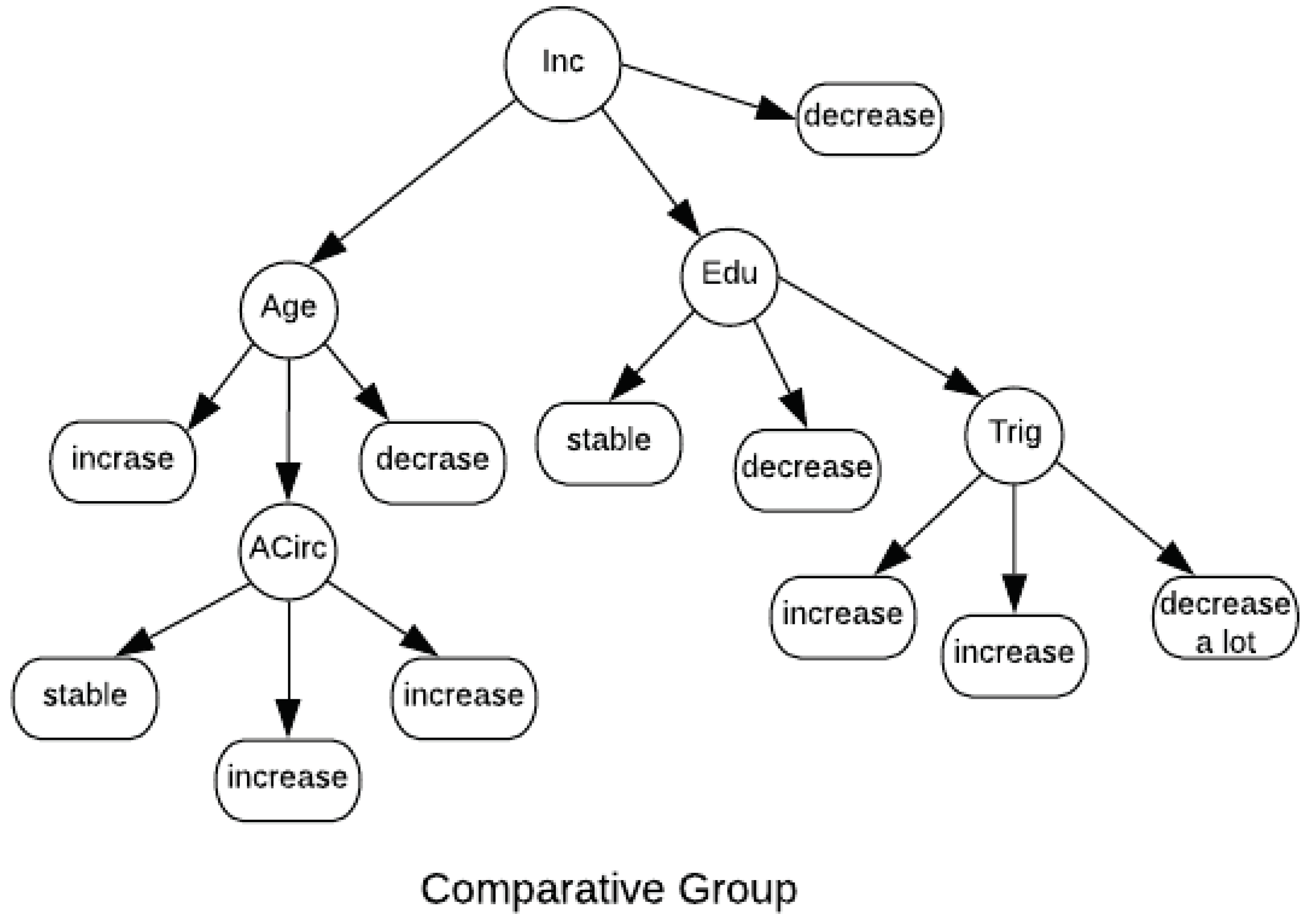
Figure 4.
DiabetesCheck application architecture.
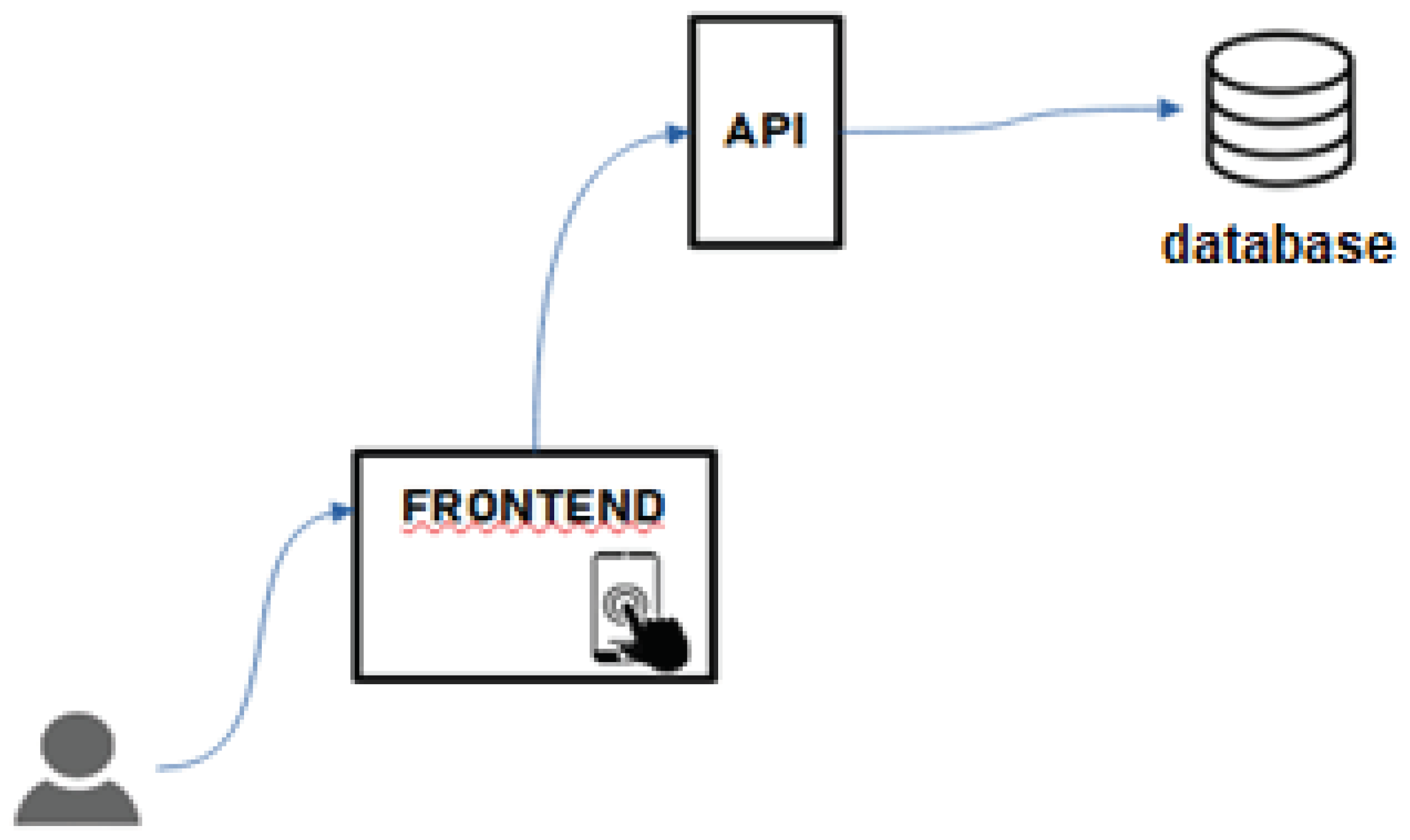
Figure 5.
DiabetesCheck application screens for creating a user account.
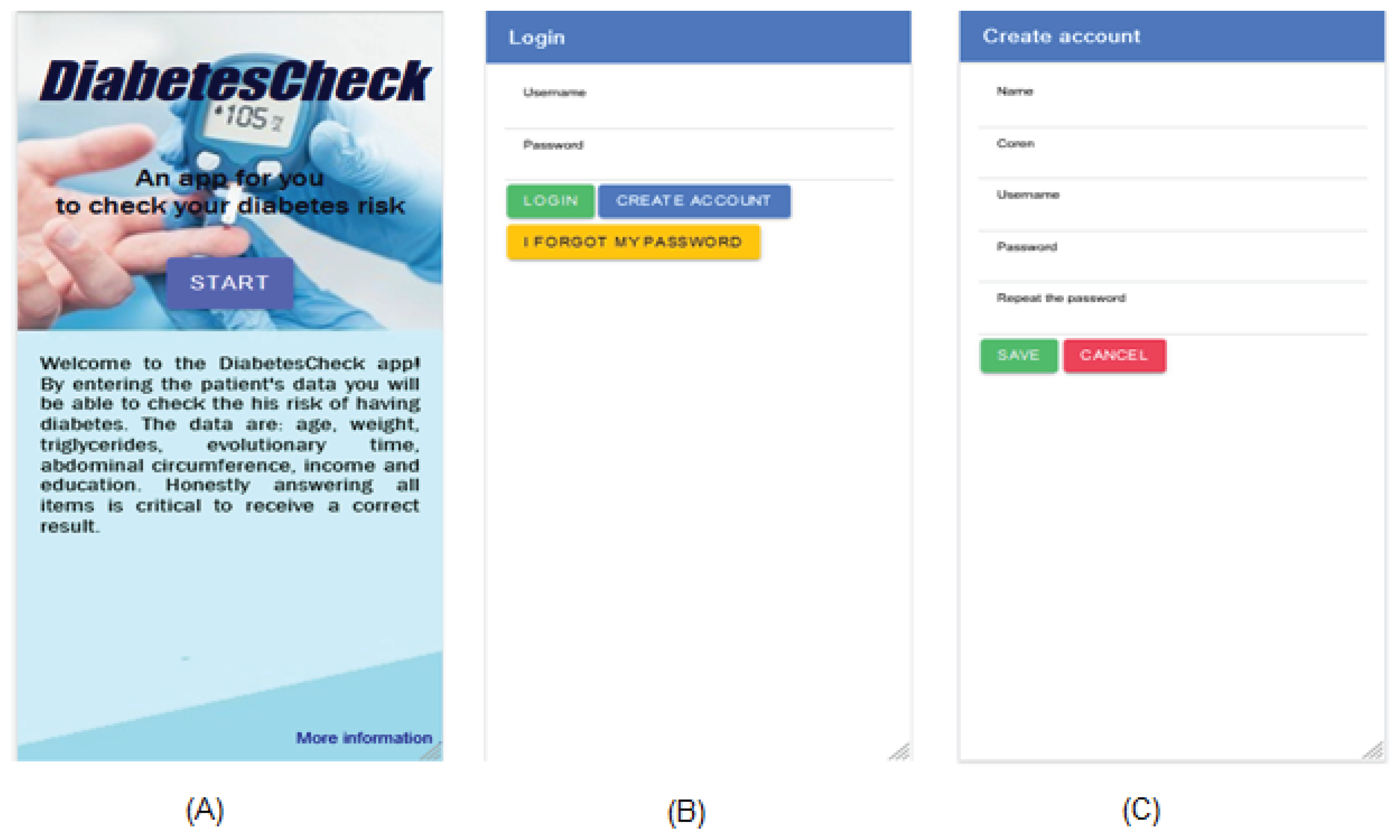
Figure 6.
DiabetesCheck functionality for healthcare professionals.
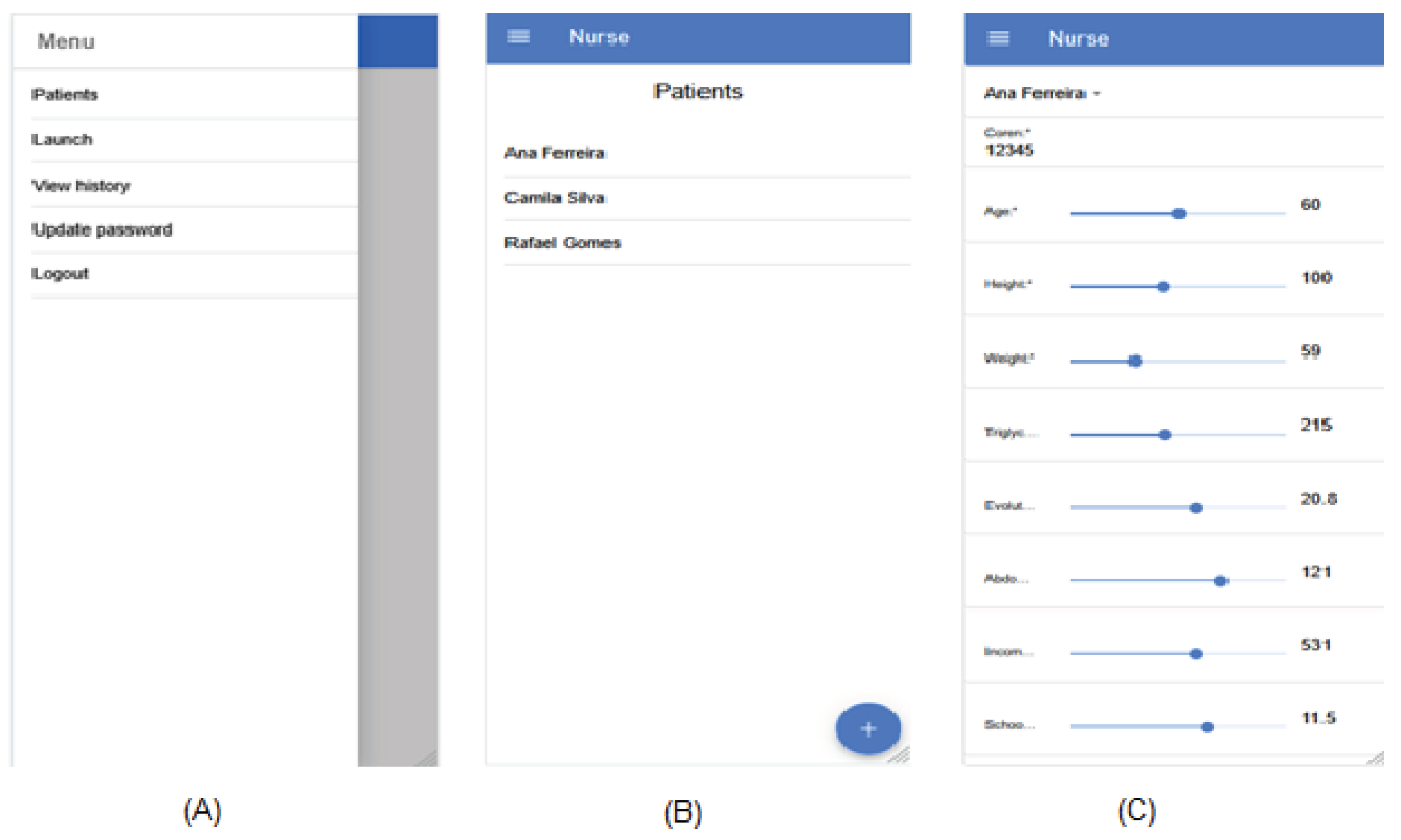
Figure 8.
DiabetesCheck functionality for administrators.
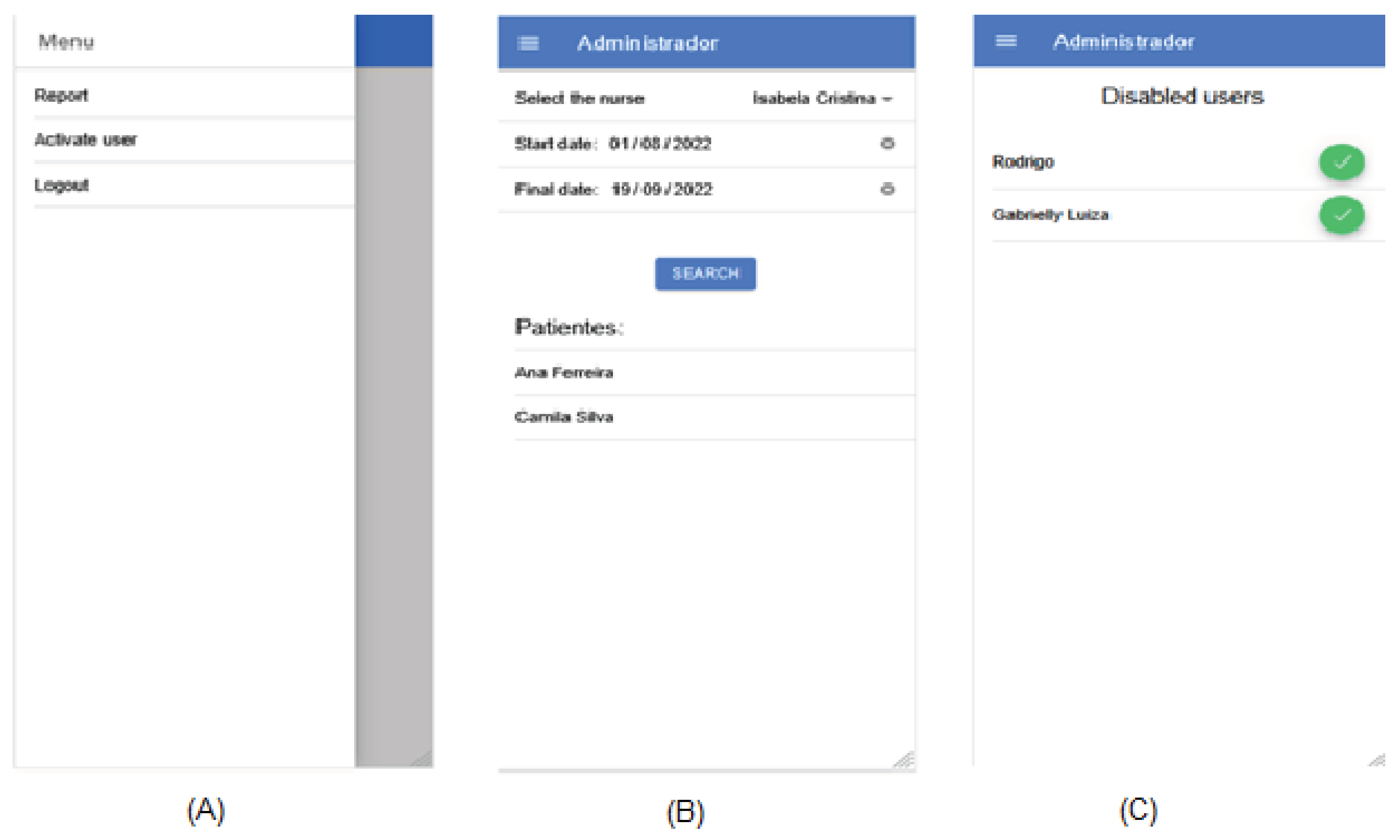

Table 1.
Intervention group features
| Attribute | Low value | Medium value | High value |
|---|---|---|---|
| Age | [19,5; 33; 46,5] | [33; 46,5; 60] | [46,5; 60; 73,5] |
| Triglycerides | [-174; 47; 268,5] | [47; 268,5; 490] | [268,5; 490; 711] |
| Evolutionary Time | [-15,2; 0,20; 15,6] | [0,2; 15,6; 31] | [15,6; 31; 46,4] |
| Body Mass Index (BMI) | [3,7; 16,06; 28,4] | [16,1; 28,41; 40,8] | [28,1; 40,8; 53,1] |
| Abdominal Circumference | [45; 72; 99] | [72; 99; 126] | [99; 126; 153] |
| Income | [-400; 4.48e-05; 400] | [6,1e-05; 400; 800] | [400 ;800; 1.200] |
| Education | [-7,5; -1e-03; 7,5] | [1,1e-03; 7,5; 15] | [7,5; 15; 22,5] |
Table 2.
Comparative group features
| Attribute | Low value | Medium value | High value |
|---|---|---|---|
| Age | [3; 22; 41] | [22; 41; 59,9] | [41; 60; 79] |
| Triglycerides | [-135; 45; 225] | [45; 225; 405] | [225; 405; 585] |
| Evolutionary Time | [-11.63; 0,25; 12,1] | [0,27; 12,1; 24] | [12,1; 24; 35,9] |
| Body Mass Index (BMI) | [2,2; 21,7; 41,2] | [21,7; 41,2; 60,7] | [41,2; 60,7; 80,2] |
| Abdominal Circumference | [52,8; 81; 109,2] | [81; 109,2; 137,5] | [500; 1.000; 1.500] |
| Income | [-500; -9,2e-05; 500] | [8,4e-05; 500; 1.000] | [400 ;800; 1.200] |
| Education | [-7,5; -2,6e-05; 7,5] | [6,4e-03; 7,5; 14,9] | [7,5; 15; 22,5] |
Table 3.
Comparison of related works
| Work | Target audience | Main goal of the application | Does it interact with healthcare professionals? |
|---|---|---|---|
| Jenna et al. (2017) | Elderly | Promote self-care and disease management | Not specified |
| Zheng et al. (2020) | Elderly | Promote self-care and disease management | Not specified |
| Yamaguchi et al. (2019) | Not specified | Promote self-care and disease management | Not specified |
| Torbjørnsen (2019) | Not specified | Promote self-care and disease management | Yes |
| DiabetesCheck | General population | Perform monitoring and prediction of diabetes risk | Yes |
Table 4.
Guidelines proposed by the UXUG-AP technique for application self-assessment
| Category | Guidelines | Self-assessment |
|---|---|---|
| Requirements | Was there an exchange of information between the team and the client through interviews and/or workshops to identify key prototype requirements? | Yes. The development team, in addition to the knowledge obtained, had access to meetings with the authors of the work to identify the requirements of the application. |
| Understanding user needs | Does the prototype interface have language accessible to different user profiles: children, youth, academics, professionals, etc.? | Yes. During development, there was a concern to use vocabulary relevant to healthcare professionals impacted by the system, namely doctors and nurses. |
| Accessibility | Does the prototype allow customization of the interface to suit users with visual impairments (increased color contrast, font size)? | No. However, it is an important demand and will be incorporated into the list of requirements to be implemented in the future. |
| Ease of use | Are there standardization of elements in the prototype interface, such as buttons, icons, etc., in relation to their location? | Yes. The organization of the elements of the application interface was designed to minimize the user’s cognitive effort to find what they need. |
| Informative feedback | Are there informative feedback for the user, such as alert and error messages, loading and progress indicators, among others? | Yes. Any activity that requires extended time (such as data retrieval from the backend) is highlighted to the user through informative feedback. |
| Are the feedback informative enough for the user to understand what is happening and why? | Yes. Error and alert messages were created to use the vocabulary of the end user. | |
| Information | Are the information modularized and independent, so that the user does not need to remember other screens while performing an activity? | Yes. All the information necessary for the user to perform an activity in the application is available on the current screen. |
| Error prevention | Does the prototype protect the user from errors they might make (e.g., forgetting a required field, entering more or fewer characters than required)? | Yes. Mandatory fields are properly highlighted in the application interface. We sought to use appropriate components for each type of field. For values on a scale of 0 to 5, a selector component was used instead of requiring the user to enter the value. |
| Does the prototype use icons that suggest the action taken and hints that explain the icon and the action? | No. This is an improvement that the application interface needs to enhance user experience and usability. |
|
| Sequence of actions | Are the prototype actions reversible? | No. The current version of the application does not have the option to undo actions. However, in the case of destructive actions, the application requests user confirmation before proceeding with the action. |
| Are the action sequences organized into groups with a beginning, middle, and end? | Yes. | |
| Sense of belonging | Do the colors, icons, and styles represent the user in a way that allows the user to feel that the software was made with them in mind? | Yes. The choice of colors, icons, and other visual elements was made considering the context of the healthcare field. |
| Degree of importance | Are elements of higher importance highlighted in the prototype interface? | Yes. An example is the page titles, which are prominently positioned on the application screen (centered and with larger font size). |
| Privacy | Is it possible to control who can access certain information and when? | Yes. The application implements user authentication through profiles, so that each type of user has access to certain functions. |
| Is there an option for password recovery in the prototype, ensuring user control? | No. This functionality will be implemented in a future version of the application. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



