
Submitted:
08 March 2024
Posted:
12 March 2024
You are already at the latest version
Abstract
Precision medicine (PM), also termed stratified, individualised, targeted or personalised medicine, embraces a rapidly expanding area of research, knowledge, and practice. It brings together two emerging health technologies to deliver better individualised care: the many “-omics” arising from increased capacity to understand the human genome; and “big data” and data analytics including Artificial Intelligence (AI). PM has the potential to transform an individual’s health, moving from population-based disease prevention to more personalised management. There is however a tension between the two, with a real risk that this will exacerbate health inequalities and divert funds and attention from basic healthcare requirements leading to worse health outcomes for many. All areas of medicine should consider how this will affect their practice, with PM now strongly encouraged and supported by government initiatives and research funding. In this review we discuss examples of PM in current practice and its emerging applications in primary care, such as clinical prediction tools that incorporate genomic markers and pharmacogenomic testing. We look towards potential future applications and consider some key questions for PM including evidence of real-world impact, its affordability, the risk of exacerbating health inequalities, and the computational and storage challenges of applying PM technologies at scale.
Keywords:
Precision medicine
; personalised medicine
; primary care
; genomics
; pharmacogenoics
; prediction modelling
; artificial intelligence
1. Take-Home Points
Precision medicine (PM), a term often used interchangeably with targeted, stratified, individualised, and personalised medicine, is a rapidly developing area of research and practice.
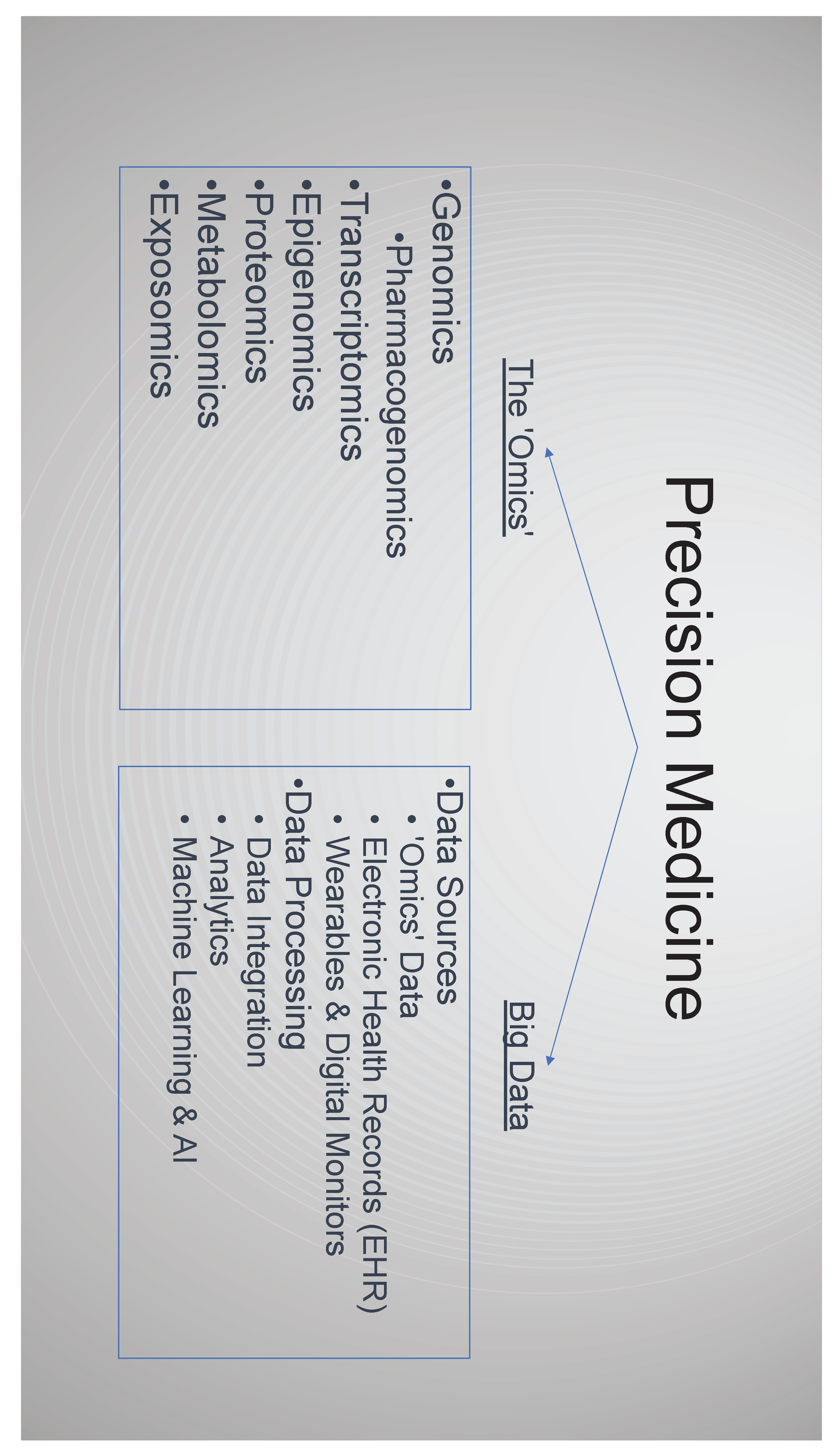
PM can be considered to involve two broad areas each with its own sub-domains.1) The “–omics” with a whole array of prefixes including but not limited to: Genomics, Pharmacogenomics, Transcriptomics, Epigenomics, Proteomics, Metabolomics & Exposomics. 2) Big data, data analytics and artificial intelligence (AI).
PM is data-science driven and is built upon large volumes of biomedical data. AI is a key tool to manage, analyse and communicate the insights from the multiple big data health care sources.
The three -omics likely to impact primary care are: polygenic risk scores to optimise patient risk stratification, pharmacogenomics to tailor treatment, and molecular genetic diagnostic testing. The impact of all will be optimised when integrated with the primary care electronic health record (EHR), which forms the key data resource for PM development and implementation in this setting.
The evidence base for PM is still emerging. Pressures and incentives for early adoption of PM technologies are multifactorial and complex. There is a need for PM initiatives that have real world evidence of clinical utility in the context they are to be deployed. Particular attention to demonstrating cost effectiveness and effect on health inequalities is required.
2. Introduction
‘ Variability is the law of life, and as no two faces are the same, so no two bodies are alike, and no two individuals react alike and behave alike under the abnormal conditions which we know as disease ’[1].
Precision medicine (PM) is a popular though poorly defined term in the academic and general health literature [2]. It is often used interchangeably with targeted; stratified; individualised; and personalised medicine. Personalised medicine is perhaps the most ambiguous of these terms, sometimes used to describe holistic or integrative medicine [3], or when used to describe PM to also capture concepts related to an individual’s beliefs, attitudes and preferences towards health care [4], concepts central to providing holistic patient care. To avoid semantic ambiguity, we will use the term precision medicine (PM) in this review, as defined by the US National Academy of Sciences:
“the use of genomic, epigenomic, exposure and other data to define individual patterns of disease, potentially leading to better individual treatment” (National Research Council Committee, 2011).
The promise of PM is the optimisation of the care of patients. By screening and surveillance based on better risk stratification, earlier recognition of disease, a molecularly defined diagnosis and a more accurate diagnosis, the most effective treatment for that individual can be delivered at the best time for the most optimum outcome [4].
The growth and diversity of PM publications and initiatives in recent years has been largely driven by the advances in two technologies: molecular biology, especially the reduction in cost and expansion of use of genomic sequencing; and advances in computational approaches for big data analysis. So-called -omic technologies such as whole genome sequencing (WGS) generate vast amounts of data, and the use of electronic health records (EHR) as well as wearable monitoring devices, provide a further source of rich biomedical data [4,6,7].
These advances have given momentum to many PM developments, and the much heralded promise that PM will lead to a paradigm shift in health across one’s lifetime [4,8,9]. This enthusiasm is tempered by a healthy degree of scepticism, sometimes expressed by the same authors. Some comment that PM is over-hyped [10,11], and that this focus of attention and resource on the individual presents a tension with delivering affordable and equitable population medicine, exacerbating health inequality.
In this review we focus on primary care and the non-specialist setting. We examine current examples of PM and its emerging applications, and the opportunities and challenges PM presents with an eye on the future, the review considers PM in the context of -omics and big data. We have included electronic health records (EHR) and wearable technologies within Big Data as both are highly relevant to primary care and crucial to capturing the data that enables PM.
Figure 1.
3. The Emergence of -Omics
3.1. Genomics
Genomic medicine, distinct from traditional genetics, is the study of the function and interaction of the entire genome [12]. Until recently, the clinical application of genomics has been largely restricted to cancer, rare inherited diseases and pharmacogenomics testing for oncology [13]. However, as genomic knowledge increases and the cost of sequencing falls, the frequency of use and breadth of applications has increased. A wide range of projects to mainstream genomic technologies have emerged with countries competing to lead the way in incorporating these technologies into routine care [4,8,14,15].
There are three PM genomic applications that may impact primary care: 1) refined molecular diagnoses, 2) polygenic risk scores and 3) pharmacogenomics.
3.1.1. Molecular Disease Definition
Genomic and other molecular technological advances has led to a new and evolving molecular taxonomy of disease [4]. This taxonomy reflects a greater recognition of the molecular basis of disease with the identification that many diseases that were previously considered a single entity are in fact made of multiple ‘subtypes’, a product of both the complexity of the disease pathology and the physiology of the individuals affected[15]. Defining diseases into subtypes by genomic and other biomarkers is now standard practice in oncology enabling targeted treatments with a significant impact on outcomes[16]. Applications in other clinical areas are more limited, although emerging examples exist in cardiovascular disease, neurology, diabetes, autoimmune and respiratory diseases [17]. For example, asthma is now viewed as a syndrome encompassing several distinct yet inter-related diseases, each driven by a unique set of genetic and non-genetic risk factors [18,19]. As the understanding of the molecular basis of each asthma subtype is enhanced so the clinical models will improve and with this the interventions to prevent asthma, predict the disease course and manage the disease [20].
3.1.2. Polygenic Risk Scores
Genome wide association studies (GWAS) have led to the development of polygenic risk scores (PRS), based on the aggregate effect of multiple, even thousands of variants across a person’s genome. Unlike monogenic disease risk, such as BRCA1, gene variants for breast and ovarian cancer or familial hypercholesterolemia for cardiovascular disease, these variants may only confer a modest effect, but when combined lead to a clinically meaningful and actionable level of risk. For example, the eMERGE study is generating genome informed risk assessments (GIRA) for 11 conditions. The GIRA incorporates PRS, monogenic risk where applicable, family history and other clinical factors to generate a summary risk report [21].
Although disease areas with PRS development is growing, examples in routine practice are limited. Risk stratification for cancer screening is the most active area. Currently, cancer screening is typically one-size-fits-all, with screening dictated solely by age thresholds. Breast cancer screening is an exception, with family history informing the age and frequency of mammography and testing for the oncogenes BRCA1 and BRCA2 [22]. The PROCAS study, a large UK based cohort, is exploring the role of PRS to further refine breast cancer screening [23], and the BARCODE1 study, uses a prostate cancer PRS in primary care to identify men at risk and then offer further testing [24]. In cardiovascular disease there has been a recent UK pilot incorporating a PRS with the standard risk prediction tool QRISK2 to refine CV risk [25].
There are several important considerations regarding PRS.
Firstly, what level of refinement they offer beyond existing methods of risk assessment. For example, previous work in cardiovascular disease showed adding PRS made only a slight increase in (discriminatory) predictive power[26]. In cancer, especially rare cancers, PRS often have a modest effect on absolute disease risk. A polygenic risk score for ovarian cancer gives a lifetime risk of 2.1% for those in the top 5% of risk, compared to 1.6% in the general population [27,28].
Secondly ,where will the PRS fit in the clinical pathway a decision critical for both clinical utility and cost-effectiveness. For example, in cardiovascular risk prediction the cost-effectiveness of PRS to guide statin prescribing is unclear [29]. However combining PRS with clinical data captured from the patient’s EHR, to prioritise those who should have a formal cardiovascular risk assessment may be the optimum approach [30].
Thirdly, PRS may risk exacerbating health inequality. PRS performance is not always maintained across genders and those of non-European ancestry, reflecting a lack of diversity in dataset development [21,31,32]. Implementing these biased PRS into clinical practice risks worsening inequality. Initiatives to diversify the patient cohorts used for PRS development, such as the Global Biobank Meta-analysis Initiative (GBMI) [33], will help the broader applicability of PRS.
Fourthly, no matter how well optimised the PRS is there will always be a ceiling to its accuracy, as they do not capture lifestyle risk factors nor other poorly understood non-genetic factors [27,34]. Therefore, to maximise clinical utility, PRS results will need to be combined with risk data from other sources. Examples of this approach include eMERGE [21] and BOADICEA, a breast cancer risk prediction model, that combines PRS with monogenic risk factors, lifestyle/ hormonal and reproductive risk factors and mammography breast density measurements [35].
Even when optimised to maximize clinical utility, a central ethical consideration exists, what happens when you inform a person of their risk? Is there something fundamentally different in response to a PRS informed risk rather than a risk derived from other methodologies? Concepts of genetic determinism are often poorly understood, with a tendency to exaggerate the anticipated magnitude of impact of genetic findings [36]. This may affect individuals differently, with some feeling overly reassured by a low PRS and therefore not engaging in routine screening which may be easy to do, cheap and effective [34]. In contrast, those with a high PRS may then adopt a fatalistic view, thinking there is no point making the lifestyle changes as their outcome is predetermined [37]. These questions remain unanswered [34,38].
3.1.3. Pharmacogenomics
Emerging from the convergence of pharmacology and genomics, pharmacogenomics (PGx), is the study of the variations in DNA and RNA, that relate to drug response [39]. PGx aims to individualise drug therapy, to ensure that prescriptions are: ‘The right drug, for the right patient at the right dose’ [40]
Adverse drug reactions (ADRs), are common and cause significant iatrogenic harm with ADRs estimated to affect 10% of inpatients [41], and the annual cost of avoidable ADRs in the UK estimated at £530 million [42], and more than $30 billion in the US [43].
Emerging examples of PGx use in primary (and other non-specialist) settings include:
- Improving drug efficacy. Variation in the cytochrome P450 gene CYP2D6 affects the metabolism and elimination of more than 100 drugs [46]. One of these drugs is the analgesic codeine which is metabolised to the bioactive form morphine. Patients can be classified by their rate of metabolism, with clinical implications for the ultra-rapid metabolisers (UMs) and poor-metabolisers [47], and pharmacogenomic guidance in the summary of product characteristics (SmPC) [48]. Variants for another cytochrome P450 gene, CYP2C19, can also significantly impact clopidogrel metabolism and efficacy with an FDA ‘black box warning’ for those carrying these variants [49].
With a range of further uses in specialist settings including gene variant specific drug treatments [39], and PGx testing to inform drug dosing [50].
There are now actionable drug-gene interactions for many commonly prescribed drugs in primary care, including codeine, clopidogrel, antidepressants and statins. The PharmGKB database lists 428 drugs with a pharmacogenomic FDA label annotation,137 of which have a requirement for genomic testing [51].
Currently PGx has not been widely implemented into any health care system [52], but with a growing number of indications there are initiatives to incorporate testing into routine practice. Primary care is perhaps the most suitable setting for implementing PGx clinical decision support. Most prescribing decisions are performed in primary care and there is already the widespread use of primary care EHR systems that are integrated with prescribing software [52].
Implementing a PGx test include considering not just what should be tested for, but also where, when and how the test is performed, and then how the result can be easily retrieved when needed. There are broadly two approaches to PGx testing:
- Testing at the time of prescribing. Typically, this is a single drug-gene test performed in advance of the prescription decision about to made. For example, in oncology DPYD testing in advance of initiating 5-FU, or in neonatal sepsis testing the RNR1 gene for variants associated with aminoglycoside induced hearing loss[53]. Opportunities for this approach, rapid testing for a single and significant gene-drug interaction, will broaden as molecular diagnostics continue to advance [54]. Although point of care testing (POCT) is already utilised in primary care [55], it is hard to see PGx POCT expand beyond a relatively limited number of indications. In primary care given the range of clinical presentations and prescribing decisions, the feasibility of POCT and the effect of even a modest delay on patient flow, an alternative approach is likely to be better suited.
- Testing patients in advance of prescribing decisions. This is a more distant prospect for primary care but would involve pre-emptively performing a PGx gene panel test for several key drug-gene interactions with the results captured to inform future prescribing decisions. This may involve testing at a separate time to the prescribing decision or triggered by prescribing a single drug on the panel, the specific drug information available to guide that treatment, and the other PGx information available for future reference. An attractive approach is to use existing sequencing data, captured for another indication to identify PGx variants, feasible given as an increasing proportion of the population has had genome or exome sequencing [52].
Whichever approach is used capturing PGx data is only worth doing if it is available and easily interpretable at the point of future prescribing decisions. Currently in primary care this is likely to mean targeted pre-emptive testing in those patients who are more likely to be prescribed specific medications, with the result recorded in the EHR and integrated with prescribing software to give actionable prompts at the point of prescribing.
3.2. Transcriptomics, Epigenomics, Proteomics, Metabolomics & Exposomics
As technology has improved so too has the capacity to study not only the genome but also the multiple steps for modification between this genetic code and the final product, the protein. The–omics describe elements of these steps and their outcomes. Exposomics, however is different, an emerging field in PM that attempts to capture the totality of chemical and non-chemical exposures (e.g., physical activity, diet, psychosocial stressors and toxins), that occur across an individual’s lifetime [56].
Transcriptomics describes the sum of all of the RNA transcripts, the different readings of the genome [57]. This captures the dynamic state of the cell, identifying gene fusions, posttranscriptional changes and other RNAs (e.g., microRNA, ribosomal RNA, transfer RNA) that play key roles in fine-tuning how the RNA transcript is read and how the protein is made. It enables a far greater insight into what is happening at a functional level than genomics. For example, an emerging area of transcriptomics research is the impact of environmental exposures on how RNA transcripts are processed and modified [58].
Epigenomic factors, meaning on top of the genome, influence what parts of the genome are read and how thoroughly. They play an important role in cancer and the predisposition and risk of complication in common diseases [57,59].
Proteomics is the measurement of the final product (proteins), how they vary from cell to cell and under different influences, with metabolomics the term used when the protein affects a metabolic pathway. Proteomics show promise in asthma patient stratification. Asthma is the consequence of a pathogenic process that involves both environmental and genetic risk factors. Proteomic analysis of body fluids, (eg serum, sputum or bronchiolar lavage) gives an insight into the consequences of both these risk factors, and a better understanding of the biological mechanism driving the patient’s asthma with the potential for precision therapeutic targets [60].
These -omic technologies generate vast amounts of data, the processing and interpretation of which is a substantial undertaking requiring the input of expert bioinformaticians [57]. This is true with a single -omic technology, but even more so when several technologies are incorporated into the analysis, sometimes referred to as the “multi-ome” or “panor-ome” [57]. AI is increasingly being deployed to manage and interpret this multi-omic “Big data” [61]. In primary care, the closest multi-omic application is in cardiovascular disease prevention and management, combining proteomic and genomic markers [62].
4. Big Data, Data Analytics and AI
4.1. Electronic Health Records
In the UK and increasingly other countries, primary care is almost entirely paperless. The widespread use of electronic health records (EHR), driven by the need to capture healthcare utilisation for the purpose of reimbursement, and to improve the recall of information to optimise patient care. EHR systems also provide a resource of data that can be interrogated at a population level.
Many advances in PM have utilised primary care EHRs research datasets, in their development, with patient level data used to stratify patients into subgroups for targeted clinical care and treatments [13,15]. The EHR can also act as a platform for implementation of PM in primary care, integrating clinical decision support tools. However there remain challenges to address.
Incorporating non-structured data. EHR data is typically held in multiple different formats: coded data, numerical values, images, and free text. Non-structured formats of data, such as free text are of limited use, they are often excluded from anonymised research data sets to preserve participants’ anonymity [63], and natural language processing (NLP) software historically has been of limited use. The situation is changing with significant advances in NLP [64], although many of the information governance concerns remain.
Data needs to be standardised, so it is comparable and consistent. A coded term for a diagnosis or intervention in one setting should mean the same in another setting, for example a diagnosis of type 2 diabetes is the same in all setting in one primary care practice to another and in secondary care. This is a necessity for efficient data integration and interoperability, and the focus of initiatives across the world [61,65].
EHR linkage. PM can be further refined by linking to other sources of patient data including other health care settings: secondary care records, radiology/pathology results and images; and non-healthcare settings: education, social care, and national statistics data such as levels of deprivation [4].
Information governance concerns. When using healthcare data there are sensitivities and legal restrictions on how it used and shared. In the UK there is broad, but not universal, consensus for sharing data for clinical care and sharing anonymised data for research. There is far less agreement when anonymised data is shared with private companies [66], who are often at the vanguard of PM projects. For example there have been major concerns in the UK about awarding the contract for the NHS federated data platform to the US company Palantir [67]. A further complicator is the role of the primary care physician or general practitioner as data controller for UK primary care EHR data. Although the data is held by a few EHR providers, the responsibility for this data sits with thousands of practice level decision makers. Consequently decisions about what can and can’t be done vary significantly with different interpretations of their position and responsibilities, as demonstrated by a reluctance to release records for key PM research initiatives such as the UK Biobank [68].
4.2. Digital Technologies Including Wearables
A further rich source of data is now captured by the patient both through intermittent home measurements and wearable technologies. These wearable technologies can capture location, activity and physiological parameters, such as blood pressure, pulse, oxygen saturation, respiratory rate and temperature in a near continuous manner. This enables a deeper understanding of disease, including intra- and inter-patient variability beyond what is possible with intermittent clinic based measurements [69]. The information can be used to both diagnose disease, for example capturing heart arrhythmias (e.g., atrial fibrillation) , and to monitor and help manage disease [70].
Wearable technologies also open the possibility to capture data on the major determinants of health, not normally captured in health data, with measurements related to lifestyle, nutrition and the environment. Such data will be crucial if PM interventions are to make a significant impact upon broader societal health [71,72]. The storage, processing and interpretation of this data poses a further big data challenge.
4.3. Prediction Modelling
Clinical prediction tools are the most widely used PM application in primary care. They involve modelling the relationship between future or unknown outcomes (endpoints) and baseline health states (starting points) [73]. They are well established, used across medicine for more than 40 years [74,75], with widely adopted examples in primary care to stratify patients’ risk of cardiovascular disease, osteoporosis, emergency admission and degree of frailty [76,77,78,79]. Artificial intelligence (AI) is increasingly being used to enhance modelling, enabling a broader range of models to be developed at greater speed [80]. AI derived models have been shown to be superior, in some but not all examples, to those developed using standard epidemiological methods for predicting disease [81,82], estimating prognosis [83] and predicting all-cause mortality [84]. As discussed previously, the inclusion of PRS may further enhance the precision of these tools.
4.4. Artificial Intelligence (AI)
Much of the promised potential and enthusiasm for PM is due to the acceleration in advances in AI. AI is a term used to describe technologies and methods that allow machines to exhibit intelligent behaviour, an area of research and development that has grown from the convergence of advances in computing power and the availability of vast amounts of data [85]. Significant amounts of AI research efforts have focussed on health care, in particular PM, with a growing number of partnerships announced between AI developers and the EHR providers who hold large repositories of healthcare data [86].
To date many of the AI healthcare uses have used a single data type or mode, with image-based applications, such as the assessment of radiology, dermatology, pathology and retinal images, the most widely researched and utilised applications. In ophthalmology retinal image analysis includes clinical applications such as identifying diabetic retinopathy [87], and research to identify retinal changes as early markers for a range of conditions [88,89,90,91]. These image applications are already impacting their respective specialties and likely to affect workforce requirements in the next 5-10 years [92]. These AI applications, have largely utilised supervising learning, requiring inputs annotated with the correct information for the AI algorithm to learn.
Examples in primary care are limited with early examples of skin lesion analysis, [93,94], including eczema assessment [95], supporting clinical documentation and coding [96], and automating some administrative tasks [97].
The goal of AI in PM is to incorporate and analyse the multi-modal data of PM, -omic, EHR and wearable data, to generate personalised actionable and timely patient insights delivered in a manner optimised for the individual patient and their clinician. The prospect of achieving this has recently been made more realistic by progress in generative AI, in particular Large Language Models (LLMs), such as ChatGPT [98] & BARD[99]. By using unsupervised learning, without the need to prior annotate data, LLMs can both significantly increase the amount of data used and the speed with which they learn, enabling a move from narrow-AI, developed and retrained for each use case, to general AI transferrable across applications. Early examples of LLMs utilised language data only, but later versions now incorporate other modes of data and are sometimes referred to as large multimodal models (LMMs), with an early medical example the use of ChatGPT-4V(ision) to both interpret the radiology image and generate the radiology report [100].
The promise of LMM is that one will be able to move beyond current multi-modal PM applications, involving the analysis of genomic and EHR data [72,101], to the ability to analyse several data inputs: past medical history, biological, physiological, environmental and socio-economic data. This data could be used to create a ‘digital twin’, upon which health care interventions could be modelled, the output delivered via a virtual health assistant working alongside the clinician to give patient specific guidance on disease prevention and management, including personalised lifestyle interventions [85]. (see Figure 2)
Similarly in pandemic surveillance real-time precision risk assessments could be made based on patient specific information: comorbidities vaccination status, location data and physiological measurements from wearable sensors, combined with data such as wastewater analysis to understand levels of the pathogen in their community [102].
These potential applications may seem a long way off, but the hyper-evolution of AI technologies and the reduction in the proposed timescales for general AI to reach human levels of performance suggest it may arrive sooner than we would expect [103].
The promise of AI is mirrored by significant concerns about the societal impact of advanced generative AI [104]. Some of the broad questions to consider before implementing AI tools are also captured in existing frameworks such as the ACCE model process for evaluating genetic testing (see Figure 3) [105,106]
There are some AI specific considerations, with regulatory and ethical frameworks developed for the implementation of AI in health care [107,108]. Firstly, the financial and ecological cost of AI applications may be higher, with an LLM search estimated to be 10 times the cost and energy consumption of a conventional text based google search [109]. Secondly the erosion of trust in healthcare, which may be worsened by a so-called ‘Black Box result’, with health care decisions made by an AI system we can’t fully interrogate [110,111]. Trust is not only necessary for AI system adoption, but also to maximise compliance with any recommendations made. Thirdly, like many “big data” derived tools, its effectiveness is dependent upon the learning dataset used to create it, “the output is only as good as the input”. If the learning dataset doesn’t reflect the real world, e.g., by under-representing certain groups in society or biased in some other way, the AI output will be less effective and possibly inaccurate and unsafe. The term ‘Health Data Poverty’ describes this phenomena, where underrepresented groups will least benefit from the innovations derived from these datasets [112]. This is especially concerning when many of the multimodal data repositories are voluntary natural history studies and genomic data sets, both of which are underrepresented with people from minority or diverse social and economic backgrounds [110,113]. Even when the dataset is representative, in that it reflects national census data for age and other demographic measures, if a certain group has, for example, a higher rate of misdiagnoses, then the insights derived from the data will still be biased [114].
5. Discussion
Precision medicine sits at the interface of two significant technological advances, molecular biology and big-data analysis. The effect on healthcare is already substantial, and likely to be increasingly so. Some predict a disruptive paradigm shift in clinical practice. However precision medicine might best be regarded more as a continuation of what is currently done, and thus a natural evolution of evidence based medicine, reducing errors and optimising care [115].
If we consider the current and near future applications of PM in primary care, there are three key areas: pharmacogenomics, with results seamlessly integrating with electronic health record prescribing software; the greater use of patient stratification and prediction tools that incorporate polygenic risk scores; and more precise molecular diagnoses. These are evolutions of what is done already, with prescribing support software and risk prediction tools already utilised widely. Therefore, the potential for disruption of primary care and the doctor-patient relationship, can be minimised by building on these current skills and processes.
Looking further ahead the path is less clear. Many of the PM applications are largely aspirational with the route to implementation unclear. The two key technologies, AI and -omics, will lead to more and more sophisticated PM technologies. If they are to impact patient care at scale, they will need to be implemented in primary care. There will be technology specific questions but many of the challenges and considerations are shared across technologies: ensuring the technology meets the needs of primary care; that the evidence base is robust and from its intended clinical setting; that the datasets upon which the PM are derived are representative; that the technology is affordable; that it doesn’t increase health inequalities; and minimising the erosion of trust and holistic care. There are key gaps in what we know regarding these challenges, to capture this evidence before implementing PM in primary care it is important to consider the following:
- Co-development of technologies. To date, healthcare AI tools have often been driven by a focus on the technology and commercial need to find a marker rather than patient and clinician need [97]. Co-development of PM technologies with primary care clinicians, patients and the public, is key to ensure they address the needs and meet the standards and values of society and primary care. With a specific focus on ensuring an evidence base in the primary care setting they are to be deployed, consideration of their impact on continuity of care and how they fit into the consultation, how they will avoid overmedicalisation and increasing health anxiety [97]. It will also be important to ensure that the outputs of PM technologies are delivered in such a way to have optimal impact, effectively inform clinical decision making and create meaningful change in people’s behaviour.
- Real world evidence in the population and setting it is to be deployed. Unrepresentative and biased datasets lead to PM tools that may exacerbate health inequalities. Before implementing PM at scale, health strategies need to ensure that the foundations upon which PM is built: datasets, genetic databases, cohort studies and EHR datasets are appropriately diverse and representative of their intended use population. Endeavours such as the STANDING Together initiative, will be key to encourage representativeness in datasets and ensure transparency in how diversity is reported [116].
Fundamentally, evidence needs to be gathered on PM technology in the setting that it is intended to be deployed. Environmental factors and where the technology is placed in the current workflow can significantly impact its performance and utility [72,117]. Before widespread adoption of PM, implementation models need to be used suitable for these new technologies [118], and appropriate evaluation frameworks applied to ensure robust real world evidence [105,119].
- Demonstrating the cost-effectiveness of PM. There is still much uncertainty about the affordability and health economic profile across the range of PM interventions [120]. PM enthusiasts, and frequently policy makers, highlight the potential cost savings of PM: avoiding ill health; promoting health prevention; streamlining diagnostic pathways with earlier diagnoses and making better therapeutic decisions, with less associated waste and adverse events and decreasing the disease burden for the public at large [72,121,122]. However, the evidence for these health system efficiencies is hard to capture, the PM interventions adding an upfront cost with the later benefit harder to measure. For example, currently drugs are prescribed without pharmacogenomic information. Will a net reduction in adverse events and inappropriate prescribing, and thus in health impact and cost, justify the expenditure of pharmacogenomic testing at a population level?
Whilst PM does not in itself seek to establish novel medications it does stratify patients into subgroups who will respond to specific treatments regimes. Molecular disease definitions divide common conditions into multiple distinct subgroups, many of which will have its own treatment. In cancer this has led to the development of drugs that have in many settings been prohibitively expensive [123]. Repositioning affordable licensed drugs based on specific molecular targets is an attractive proposition to reduce drug costs whilst maximising efficacy [121]. Although, this has not been widely utilised to date, pharmaceutical companies and government research funders could use this opportunity to revisit “old drugs” for targeted personalised therapy in specific subgroups [124].
- Data collection sharing and transfer. Much of the potential of PM is dependent upon processing and analysing large amounts of data. Genomic sequencing has advanced at pace, however the availability of information on diverse well-phenotyped individuals has not kept pace, hampering the ability to establish connections between disease and genomics [125]. Optimising the quality of data recorded is key. To achieve this establishing standards for data recording, including clinical vocabulary that is used across care settings, and frameworks to share data, compliant with legal restrictions, that maintain patient privacy and incorporating individual preferences for their data use need to be prioritised.
In UK primary care, for example, better guidance regarding data sharing is needed to ensure practice is more uniform, with recent proposals that data controller responsibilities could be shared with national bodies [126]. In addition to ensuring the quality of data recorded and standards for sharing, significant attention should be focussed on the storage and processing of the vast quantity of data that PM needs and will generate. This risks overwhelming an already stretched health system and workforce. Although plans are in place to advance NHS digital systems [127], this needs to be prioritised with suitable cautions given that previous large scale IT infrastructure projects across the NHS have failed [128].
- Impact upon holistic care. There is concern that the advance of PM interventions may reduce the need for human interaction, with the virtual clinical assistant taking a greater role and affecting the patient doctor relationship. As health care interventions become more personalised, derived from increasingly complex methodologies, the rational for the intervention may become more opaque [110,111]. Will this lack of transparency erode trust and further impact the doctor-patient relationship? Advocates of PM suggest that it will enable better use or resources, bringing together disparate information to support the clinician to make the best decision, thus freeing time for human intelligence and restoring empathy [129]. However, evidence for or against this position needs to be established, with robust primary care based qualitative research incorporating the views of clinicians and patients.
Advances in PM will undoubtedly impact primary care. The opportunities are plentiful but there are significant challenges. Primary care-based research should be at the centre of these advances to establish a robust evidence base that demonstrates if PM improves health outcomes, is cost effective and acceptable to society. If these challenges are not addressed, PM risks becoming a shiny new initiative, available only to the wealthy minority, exacerbating health inequality and diverting valuable funds from core services, with little health gain.
Funding
“William Evans is funded by a National Institute for Health Research (NIHR), School for primary care (SPCR) GP career progression fellowship. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.”.
References
- Osler, W. On the educational value of the medical society. In: equanimitas with Other Addresses to Medical Students, Nurses and Practitioners of Medicine [Internet]. Philadelphia: Blakiston; 1904. p. 343–62. Available online: https://onlinelibrary.wiley.com/doi/full/10.1046/j.1365-2141.2003.04615.x.
- Schleidgen, S.; Klingler, C.; Bertram, T.; Rogowski, W.H.; Marckmann, G. What is personalized medicine: sharpening a vague term based on a systematic literature review. BMC Med Ethics. 2013, 14, 55. [Google Scholar] [CrossRef] [PubMed]
- Boyer, M.S.; Widmer, D.; Cohidon, C.; Desvergne, B.; Cornuz, J.; Guessous, I. , et al. Representations of personalised medicine in family medicine: a qualitative analysis. BMC Prim Care. 2022, 23, 37. [Google Scholar] [CrossRef]
- Ginsburg, G.S.; Phillips, K.A. Precision Medicine: From Science To Value. Health Aff Proj Hope. 2018, 37, 694–701. [Google Scholar] [CrossRef] [PubMed]
- National Research Council Committee on AF for D a NT of D. The National Academies Collection: Reports funded by National Institutes of Health. In Toward Precision Medicine: Building a Knowledge Network for Biomedical Research and a New Taxonomy of Disease; National Academies Press (US) National Academy of Sciences: Washington (DC), 2011. [Google Scholar]
- Evans, R.S. Electronic Health Records: Then, Now, and in the Future. Yearb Med Inform. 2016, (Suppl 1) (Suppl 1), S48–61. [Google Scholar] [CrossRef]
- Abdelhalim, H.; Berber, A.; Lodi, M.; Jain, R.; Nair, A.; Pappu, A. , et al. Artificial Intelligence, Healthcare, Clinical Genomics, and Pharmacogenomics Approaches in Precision Medicine. Front Genet. 2022, 13, 929736. [Google Scholar] [CrossRef] [PubMed]
- Collins, F.S.; Varmus, H. A New Initiative on Precision Medicine. N Engl J Med. 2015, 372, 793–5. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health (NIH) All of Us [Internet]. 2019 [cited 2019 Jun 13]. Available online: https://allofus.nih.gov/.
- Joyner, M.J.; Paneth, N. Promises, promises, and precision medicine. J Clin Invest. 3AD, 129, 946–8. [Google Scholar] [CrossRef]
- Evans, J.P.; Meslin, E.M.; Marteau, T.M.; Caulfield, T. Genomics. Deflating the genomic bubble. Science 2011, 331, 861–2. [Google Scholar]
- Guttmacher, A.E.; Collins, F.S. Genomic Medicine — A Primer. Guttmacher AE, Collins FS, editors. N Engl J Med. 2002, 347, 1512–20. [Google Scholar] [CrossRef]
- Qureshi, N.; Humphries, S.E.; Gray, H. Personalised medicine in general practice: the example of raised cholesterol. 2018 Feb 1. Available online: https://bjgp.org/content/68/667/68.
- Davies, S.C. Annual Report of the Chief Medical Officer 2016, Generation Genome, 2016 [Internet]. London KW -:-: Department of Health (2017); 2017. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/631043/CMO_annual_report_generation_genome.
- NHS England » Improving Outcomes through Personalised Medicine [Internet]. [cited 2023 Sep 18]. Available from: https://www.england.nhs.uk/publication/improving-outcomes-through-personalised-medicine/.
- Orrantia-Borunda, E.; Anchondo-Nuñez, P.; Acuña-Aguilar, L.E.; Gómez-Valles, F.O.; Ramírez-Valdespino, C.A. Subtypes of Breast Cancer. In: Mayrovitz HN, editor. Breast Cancer [Internet]. Brisbane (AU): Exon Publications; 2022 [cited 2023 Oct 13]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK583808/.
- Wang, R.C.; Wang, Z. Precision Medicine: Disease Subtyping and Tailored Treatment. Cancers. 2023, 15, 3837. [Google Scholar] [CrossRef]
- Borish, L.; Culp, J.A. Asthma: a syndrome composed of heterogeneous diseases. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol. 2008, 101, 1–8, quiz 8–11, 50. [Google Scholar] [CrossRef] [PubMed]
- Tsuo, K.; Zhou, W.; Wang, Y.; Kanai, M.; Namba, S.; Gupta, R. , et al. Multi-ancestry meta-analysis of asthma identifies novel associations and highlights the value of increased power and diversity. Cell Genomics. 2022, 2, 100212. [Google Scholar] [CrossRef] [PubMed]
- Colicino, S.; Munblit, D.; Minelli, C.; Custovic, A.; Cullinan, P. Validation of childhood asthma predictive tools: A systematic review. Clin Exp Allergy. 2019, 49, 410–8. [Google Scholar] [CrossRef] [PubMed]
- Linder, J.E.; Allworth, A.; Bland, H.T.; Caraballo, P.J.; Chisholm, R.L.; Clayton, E.W. , et al. Returning integrated genomic risk and clinical recommendations: The eMERGE study. Genet Med Off J Am Coll Med Genet. 2023, 25, 100006. [Google Scholar]
- NICE. Overview | Familial breast cancer: classification, care and managing breast cancer and related risks in people with a family history of breast cancer | Guidance | NICE [Internet]. NICE; 2017 [cited 2019 May 23]. Available from: https://www.nice.org.uk/guidance/cg164. 23 May.
- Evans, D.G.; Astley, S.; Stavrinos, P.; Harkness, E.; Donnelly, L.S.; Dawe, S. , et al. Improvement in risk prediction, early detection and prevention of breast cancer in the NHS Breast Screening Programme and family history clinics: a dual cohort study [Internet]. Southampton (UK): NIHR Journals Library; 2016 [cited 2023 Sep 24]. (Programme Grants for Applied Research). Available from: http://www.ncbi.nlm.nih.gov/books/NBK379488/.
- McHugh, J.K.; ni Raghallaigh, H.; Bancroft, E.; Kote-Jarai, Z.; Benafif, S.; Eeles, R.A. The BARCODE1 study in primary care: Early results targeting men with increased genetic risk of developing prostate cancer—Examining the interim data from a community-based screening program using polygenic risk score to target screening. J Clin Oncol. 2022, 40, (6_suppl). 231–231. [Google Scholar] [CrossRef]
- Genomics E, unchanged E field is for validation purposes and should be left, Oxford U contacts, Cambridge U contacts, Cambridge M contacts, Use T of, et al. Genomics plc. 2022 [cited 2023 Sep 24]. Genomics plc announces successful world-first pilot using improved genomic risk assessment in cardiovascular disease prevention in the NHS. Available from: https://www.genomicsplc.com/news/successful-world-first-pilot-using-improved-genomic-risk-assessment-in-cardiovascular-disease-prevention-in-the-nhs/.
- Elliott, J.; Bodinier, B.; Bond, T.A.; Chadeau-Hyam, M.; Evangelou, E.; Moons, K.G.M. , et al. Predictive Accuracy of a Polygenic Risk Score-Enhanced Prediction Model vs a Clinical Risk Score for Coronary Artery Disease. JAMA. 2020, 323, 636–45. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.D.; Hurson, A.N.; Zhang, H.; Choudhury, P.P.; Easton, D.F.; Milne, R.L. , et al. Assessment of polygenic architecture and risk prediction based on common variants across fourteen cancers. Nat Commun. 2020, 11, 3353. [Google Scholar] [CrossRef]
- Hingorani, A.; Gratton, J.; Finan, C.; Schmidt, A.; Patel, R.; Sofat, R. , et al. Performance of polygenic risk scores in screening, prediction, and risk stratification [Internet]. medRxiv; 2022 [cited 2023 Aug 28]. p. 2022.02.18.22271049. Available from: https://www.medrxiv.org/content/10.1101/2022.02.18.22271049v2.
- Kiflen, M.; Le, A.; Mao, S.; Lali, R.; Narula, S.; Xie, F. , et al. Cost-Effectiveness of Polygenic Risk Scores to Guide Statin Therapy for Cardiovascular Disease Prevention. Circ Genomic Precis Med. 2022, 15, e003423. [Google Scholar] [CrossRef]
- Chung, R.; Xu, Z.; Arnold, M.; Ip, S.; Harrison, H.; Barrett, J. , et al. Using Polygenic Risk Scores for Prioritizing Individuals at Greatest Need of a Cardiovascular Disease Risk Assessment. J Am Heart Assoc. 2023, 12, e029296. [Google Scholar] [CrossRef]
- GWAS to the people. Nat Med. 2018, 24, 1483–1483. [CrossRef]
- Martin, A.R.; Kanai, M.; Kamatani, Y.; Okada, Y.; Neale, B.M.; Daly, M.J. Current clinical use of polygenic scores will risk exacerbating health disparities. Nat Genet. 2019, 51, 584–91. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Namba, S.; Lopera, E.; Kerminen, S.; Tsuo, K.; Läll, K. , et al. Global Biobank analyses provide lessons for developing polygenic risk scores across diverse cohorts. Cell Genomics. 2023, 3, 100241. [Google Scholar] [CrossRef] [PubMed]
- Sud, A.; Horton, R.H.; Hingorani, A.D.; Tzoulaki, I.; Turnbull, C.; Houlston, R.S. , et al. Realistic expectations are key to realising the benefits of polygenic scores. The BMJ. 2023, 380, e073149. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Mavaddat, N.; Wilcox, A.N.; Cunningham, A.P.; Carver, T.; Hartley, S. , et al. BOADICEA: a comprehensive breast cancer risk prediction model incorporating genetic and nongenetic risk factors. Genet Med Off J Am Coll Med Genet. 2019, 21, 1708–18. [Google Scholar]
- Resnik, D.B.; Vorhaus, D.B. Genetic modification and genetic determinism. Philos Ethics Humanit Med. 2006, 1, 9. [Google Scholar] [CrossRef] [PubMed]
- Middlemass, J.B.; Yazdani, M.F.; Kai, J.; Standen, P.J.; Qureshi, N. Introducing genetic testing for cardiovascular disease in primary care: a qualitative study. Br J Gen Pract J R Coll Gen Pract. 2014, 64, e282–289. [Google Scholar] [CrossRef] [PubMed]
- Hollands, G.J.; French, D.P.; Griffin, S.J.; Prevost, A.T.; Sutton, S.; King, S. , et al. The impact of communicating genetic risks of disease on risk-reducing health behaviour: systematic review with meta-analysis. Bmj. i1102–i1102.
- Adminstration UF and DK: Paving the Way for Personalized Medicine: FDA’s ROle in a New Era of Medical product development [Internet]. 2013. Available online: https://www.fdanews.com/ext/resources/files/10/10-28-13-Personalized-Medicine.
- Sadee, W.; Dai, Z. Pharmacogenetics/genomics and personalized medicine. Hum Mol Genet. 2005, 14 Spec No. 2, R207–14. [Google Scholar] [CrossRef]
- Donaldson, L. An organisation with a memory. Clin Med [Internet]. 2002;2(5 KW-:-). Available online: https://pdfs.semanticscholar.org/a675/29ad58dbc031e82f33555d071a568a4e5c6c.pdf.
- Overview | Medicines optimisation: the safe and effective use of medicines to enable the best possible outcomes | Guidance | NICE [Internet]. NICE; 2015 [cited 2023 Sep 25]. Available online: https://www.nice.org.uk/guidance/ng5.
- Sultana, J.; Cutroneo, P.; Trifirò, G. Clinical and economic burden of adverse drug reactions. J Pharmacol Pharmacother. 2013, 4 (Suppl1), S73–7. [Google Scholar] [CrossRef]
- Tangamornsuksan, W.; Chaiyakunapruk, N.; Somkrua, R.; Lohitnavy, M.; Tassaneeyakul, W. Relationship between the HLA-B*1502 allele and carbamazepine-induced Stevens-Johnson syndrome and toxic epidermal necrolysis: a systematic review and meta-analysis. JAMA Dermatol. 2013, 149, 1025–32. [Google Scholar] [CrossRef]
- BNF content published by NICE [Internet]. 2023 [cited 2023 Oct 20]. https://bnf.nice.org.uk.
- Bertilsson, L.; Dahl, M.L.; Dalén, P.; Al-Shurbaji, A. Molecular genetics of CYP2D6: Clinical relevance with focus on psychotropic drugs. Br J Clin Pharmacol. 2002, 53, 111–22. [Google Scholar] [CrossRef] [PubMed]
- Crews, K.R.; Gaedigk, A.; Dunnenberger, H.M.; Leeder, J.S.; Klein, T.E.; Caudle, K.E. , et al. Clinical Pharmacogenetics Implementation Consortium guidelines for cytochrome P450 2D6 genotype and codeine therapy: 2014 update. Clin Pharmacol Ther. 2014/01/25 ed. 2014, 95, 376–82. [Google Scholar] [CrossRef] [PubMed]
- Codeine Phosphate 30mg Tablets - Summary of Product Characteristics (SmPC) - (emc) [Internet]. [cited 2023 Sep 26]. 2375. Available online: https://www.medicines.org.uk/emc/product/2375/smpc#gref.
- Administration UF and, D. FDA Drug Safety Communication: Reduced effectiveness of Plavix (clopidogrel) in patients who are poor metabolizers of the drug | FDA [Internet]. US_FDA; 2010. Available online: https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/fda-drug-safety-communication-reduced-effectiveness-plavix-clopidogrel-patients-who-are-poor.
- Henricks, L.M.; Lunenburg, C.A.T.C.; Cats, A.; Mathijssen, R.H.J.; Guchelaar, H.J.; Schellens, J.H.M. DPYD genotype-guided dose individualisation of fluoropyrimidine therapy: who and how? – Authors’ reply. Lancet Oncol. 2019, 20, e67. [Google Scholar] [CrossRef] [PubMed]
- PharmGKB [Internet]. [cited 2023 Sep 26]. PharmGKB. Available online: https://www.pharmgkb.org/.
- RCP London [Internet]. 2022 [cited 2023 Sep 25]. Personalised prescribing: using pharmacogenomics to improve patient outcomes. Available online: https://www.rcp.ac.uk/projects/outputs/personalised-prescribing-using-pharmacogenomics-improve-patient-outcomes.
- McDermott, J.H.; Mahaveer, A.; James, R.A.; Booth, N.; Turner, M.; Harvey, K.E. , et al. Rapid Point-of-Care Genotyping to Avoid Aminoglycoside-Induced Ototoxicity in Neonatal Intensive Care. JAMA Pediatr. 2022, 176, 486–92. [Google Scholar] [CrossRef] [PubMed]
- McDermott, J.H.; Burn, J.; Donnai, D.; Newman, W.G. The rise of point-of-care genetics: how the SARS-CoV-2 pandemic will accelerate adoption of genetic testing in the acute setting. Eur J Hum Genet. 2021, 29, 891–3. [Google Scholar] [CrossRef] [PubMed]
- Lingervelder, D.; Koffijberg, H.; Kusters, R.; IJzerman, M.J. Point-of-care testing in primary care: A systematic review on implementation aspects addressed in test evaluations. Int J Clin Pract. 2019, 73, e13392. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, R.; Schymanski, E.L.; Barabási, A.L.; Miller, G.W. The exposome and health: Where chemistry meets biology. Science. 2020, 367, 392–6. [Google Scholar] [CrossRef] [PubMed]
- Topol, E.J. Individualized Medicine from Prewomb to Tomb. Cell. 2014, 157, 241–53. [Google Scholar] [CrossRef]
- Baccarelli, A.; Dolinoy, D.C.; Walker, C.L. A precision environmental health approach to prevention of human disease. Nat Commun. 2023, 14, 2449. [Google Scholar] [CrossRef]
- Pirola, L.; Balcerczyk, A.; Okabe, J.; El-Osta, A. Epigenetic phenomena linked to diabetic complications. Nat Rev Endocrinol. 2010/11/04 ed. 2010, 6, 665–75. [Google Scholar] [CrossRef]
- Xu, P.; Wang, L.; Chen, D.; Feng, M.; Lu, Y.; Chen, R. , et al. The application of proteomics in the diagnosis and treatment of bronchial asthma. Ann Transl Med. 2020, 8, 132. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, Z.; Mohamed, K.; Zeeshan, S.; Dong, X. Artificial intelligence with multi-functional machine learning platform development for better healthcare and precision medicine. Database J Biol Databases Curation. 2020, 2020, baaa010. [Google Scholar] [CrossRef] [PubMed]
- Leon-Mimila, P.; Wang, J.; Huertas-Vazquez, A. Relevance of Multi-Omics Studies in Cardiovascular Diseases. Front Cardiovasc Med [Internet]. 2019 [cited 2023 Dec 8];6. Available online: https://www.frontiersin.org/articles/10.3389/fcvm.2019.00091.
- Wolf, A.; Dedman, D.; Campbell, J.; Booth, H.; Lunn, D.; Chapman, J. , et al. Data resource profile: Clinical Practice Research Datalink (CPRD) Aurum. Int J Epidemiol. 2019, 48, 1740–1740g. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Yang, X.; Chen, A.; Smith, K.E.; PourNejatian, N.; Costa, A.B. A Study of Generative Large Language Model for Medical Research and Healthcare [Internet]. arXiv; 2023 [cited 2023 Oct 25]. Available online: http://arxiv.org/abs/2305.13523.
- Dzau, V.J.; Ginsburg, G.S. Realizing the Full Potential of Precision Medicine in Health and Health CarePotential of Precision Medicine in Health and Health CarePotential of Precision Medicine in Health and Health Care. JAMA. 2016, 316, 1659–60. [Google Scholar] [CrossRef] [PubMed]
- Jones, L.A.; Nelder, J.R.; Fryer, J.M.; Alsop, P.H.; Geary, M.R.; Prince, M. , et al. Public opinion on sharing data from health services for clinical and research purposes without explicit consent: an anonymous online survey in the UK. BMJ Open. 2022, 12, e057579. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, S. Pause plans for data sharing contract to ensure trust and patient consent, plead doctors’ leaders. BMJ. 2023, 383, p2674. [Google Scholar] [CrossRef] [PubMed]
- Parr, E. UK Biobank writes to all GP practices requesting they share patient data [Internet]. Pulse Today. 2023 [cited 2023 Oct 17]. 2023. Available online: https://www.pulsetoday.co.uk/news/technology/uk-biobank-writes-to-all-gp-practices-requesting-they-share-patient-data/.
- Izmailova, E.S.; Wagner, J.A.; Perakslis, E.D. Wearable Devices in Clinical Trials: Hype and Hypothesis. Clin Pharmacol Ther. 2018, 104, 42–52. [Google Scholar] [CrossRef]
- The Topol Review [Internet]. [cited 2023 Sep 18]. Available online: https://topol.hee.nhs.uk/the-topol-review/.
- McGinnis, J.M.; Williams-Russo, P.; Knickman, J.R. The Case For More Active Policy Attention To Health Promotion. Health Aff (Millwood). 2002, 21, 78–93. [Google Scholar] [CrossRef]
- Johnson, K.B.; Wei, W.; Weeraratne, D.; Frisse, M.E.; Misulis, K.; Rhee, K. , et al. Precision Medicine, AI, and the Future of Personalized Health Care. Clin Transl Sci. 2021, 14, 86–93. [Google Scholar] [CrossRef]
- Hemingway, H.; Croft, P.; Perel, P.; Hayden, J.A.; Abrams, K.; Timmis, A. , et al. Prognosis research strategy (PROGRESS) 1: a framework for researching clinical outcomes. Bmj. 2013, 346, e5595. [Google Scholar] [CrossRef]
- Cox, D.R. Regression Models and Life-Tables. J R Stat Soc Ser B Methodol. 1972, 34, 187–220. [Google Scholar] [CrossRef]
- Vasan, R.S.; Beiser, A.; Seshadri, S.; Larson, M.G.; Kannel, W.B.; D’Agostino, R.B. , et al. Residual Lifetime Risk for Developing Hypertension in Middle-aged Women and MenThe Framingham Heart Study. JAMA. 2002, 287, 1003–10. [Google Scholar] [CrossRef]
- Kanis, J.A.; Johnell, O.; Oden, A.; Johansson, H.; McCloskey, E. FRAX and the assessment of fracture probability in men and women from the UK. Osteoporos Int J Establ Result Coop Eur Found Osteoporos Natl Osteoporos Found USA. 2008, 19, 385–97. [Google Scholar] [CrossRef] [PubMed]
- Dent, E.; Kowal, P.; Hoogendijk, E.O. Frailty measurement in research and clinical practice: A review. Eur J Intern Med. 2016, 31, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Hippisley-Cox, J.; Coupland, C.; Brindle, P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: prospective cohort study. BMJ. 2017, 357, j2099. [Google Scholar] [CrossRef] [PubMed]
- Kingston, M.; Griffiths, R.; Hutchings, H.; Porter, A.; Russell, I.; Snooks, H. Emergency admission risk stratification tools in UK primary care: a cross-sectional survey of availability and use. Br J Gen Pract. 2020, 70, e740–8. [Google Scholar] [CrossRef]
- Papadakis, G.Z.; Karantanas, A.H.; Tsiknakis, M.; Tsatsakis, A.; Spandidos, D.A.; Marias, K. Deep learning opens new horizons in personalized medicine. Biomed Rep. 2019, 10, 215–7. [Google Scholar] [CrossRef]
- Weng, S.F.; Reps, J.; Kai, J.; Garibaldi, J.M.; Qureshi, N. Can machine-learning improve cardiovascular risk prediction using routine clinical data? PLOS ONE. 2017, 2017. 12, e0174944. [Google Scholar] [CrossRef]
- Callender, T.; Imrie, F.; Cebere, B.; Pashayan, N.; Navani, N.; Schaar M van, d.e.r. , et al. Assessing eligibility for lung cancer screening using parsimonious ensemble machine learning models: A development and validation study. PLOS Med. 2023, 20, e1004287. [Google Scholar] [CrossRef]
- Montazeri, M.; Montazeri, M.; Bahaadinbeigy, K.; Montazeri, M.; Afraz, A. Application of machine learning methods in predicting schizophrenia and bipolar disorders: A systematic review. Health Sci Rep. 2022, 6, e962. [Google Scholar] [CrossRef]
- Weng, S.F.; Vaz, L.; Qureshi, N.; Kai, J. Prediction of premature all-cause mortality: A prospective general population cohort study comparing machine-learning and standard epidemiological approaches. PloS One. 2019, 14, e0214365. [Google Scholar] [CrossRef] [PubMed]
- Topol, E.J. As artificial intelligence goes multimodal, medical applications multiply. Science. 2023, 381, adk6139. [Google Scholar] [CrossRef]
- Archer-Williams, A. Microsoft and Epic expand AI collaboration to tackle current healthcare needs [Internet]. htn. 2023 [cited 2023 Aug 29]. Available from: Available from: https://htn.co.uk/2023/08/23/microsoft-and-epic-expand-ai-collaboration-to-tackle-current-healthcare-needs/.
- Lim, J.I.; Regillo, C.D.; Sadda, S.R.; Ipp, E.; Bhaskaranand, M.; Ramachandra, C. , et al. Artificial Intelligence Detection of Diabetic Retinopathy. Ophthalmol Sci. 2022, 3, 100228. [Google Scholar] [CrossRef] [PubMed]
- Poplin, R.; Varadarajan, A.V.; Blumer, K.; Liu, Y.; McConnell, M.V.; Corrado, G.S. , et al. Prediction of cardiovascular risk factors from retinal fundus photographs via deep learning. Nat Biomed Eng. 2018, 2, 158–64. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.Y.; Ran, A.R.; Wang, S.; Chan, V.T.T.; Sham, K.; Hilal, S. , et al. A deep learning model for detection of Alzheimer’s disease based on retinal photographs: a retrospective, multicentre case-control study. Lancet Digit Health. 2022, 4, e806–15. [Google Scholar] [CrossRef]
- Diaz-Pinto, A.; Ravikumar, N.; Attar, R.; Suinesiaputra, A.; Zhao, Y.; Levelt, E.; et al. Predicting myocardial infarction through retinal scans and minimal personal information. Nat Mach Intell. 2022, 4, 55–61. [Google Scholar] [CrossRef]
- Wagner, S.K.; Romero-Bascones, D.; Cortina-Borja, M.; Williamson, D.J.; Struyven, R.R.; Zhou, Y. Retinal Optical Coherence Tomography Features Associated With Incident and Prevalent Parkinson Disease. Neurology [Internet]. 2023 Aug 21 [cited 2023 Aug 31]; Available from: https://n.neurology.org/content/early/2023/08/21/WNL.0000000000207727.
- Scheetz, J.; Rothschild, P.; McGuinness, M.; Hadoux, X.; Soyer, H.P.; Janda, M. , et al. A survey of clinicians on the use of artificial intelligence in ophthalmology, dermatology, radiology and radiation oncology. Sci Rep. 2021, 11, 5193. [Google Scholar] [CrossRef]
- Du-Harpur, X.; Watt, F.M.; Luscombe, N.M.; Lynch, M.D. What is AI? Applications of artificial intelligence to dermatology. Br J Dermatol. 2020, 183, 423–30. [Google Scholar] [CrossRef]
- Escalé-Besa, A.; Yélamos, O.; Vidal-Alaball, J.; Fuster-Casanovas, A.; Miró Catalina, Q.; Börve, A. , et al. Exploring the potential of artificial intelligence in improving skin lesion diagnosis in primary care. Sci Rep. 2023, 13, 4293. [Google Scholar] [CrossRef]
- Pan, K.; Hurault, G.; Arulkumaran, K.; Williams, H.C.; Tanaka, R.J. EczemaNet: Automating Detection and Severity Assessment of Atopic Dermatitis. In: Liu M, Yan P, Lian C, Cao X, editors. Machine Learning in Medical Imaging. Cham: Springer International Publishing; 2020. p. 220–30. (Lecture Notes in Computer Science).
- Ambient Clinical Intelligence | Automatically Document Care | Nuance [Internet]. [cited 2023 Oct 4]. Available online: https://www.nuance.com/healthcare/ambient-clinical-intelligence.html.
- Mistry, P. Artificial intelligence in primary care. Br J Gen Pract. 2019, 69, 422–3. [Google Scholar] [CrossRef]
- ChatGPT [Internet]. [cited 2023 Oct 5]. Available from: https://chat.openai.com.
- Bard - Chat Based AI Tool from Google, Powered by PaLM 2 [Internet]. [cited 2023 Oct 20]. Available from: https://bard.google.com.
- Yang, Z.; Li, L.; Lin, K.; Wang, J.; Lin, C.C.; Liu, Z. The Dawn of LMMs: Preliminary Explorations with GPT-4V(ision) [Internet]. arXiv; 2023 [cited 2023 Oct 16]. Available from: http://arxiv.org/abs/2309.17421.
- Magavern, E.F.; Smedley, D.; Caulfield, M.J. Factor V Leiden, oestrogen and multimorbidity association with venous thromboembolism in a British-South Asian Cohort. iScience [Internet]. 2023 Aug 31 [cited 2023 Sep 20];0(0). Available from: https://www.cell.com/iscience/abstract/S2589-0042(23)01872-2.
- Pandit, J.A.; Radin, J.M.; Quer, G.; Topol, E.J. Smartphone apps in the COVID-19 pandemic. Nat Biotechnol. 2022, 40, 1013–22. [Google Scholar] [CrossRef] [PubMed]
- Generative AI Country Automation [Internet]. [cited 2023 Oct 5]. Available from: http://ceros.mckinsey.com/generative-ai-country-automation.
- Pause Giant AI Experiments: An Open Letter [Internet]. Future of Life Institute. [cited 2023 Oct 20]. Available from: https://futureoflife.org/open-letter/pause-giant-ai-experiments/.
- Sanderson, S.; Zimmern, R.; Kroese, M.; Higgins, J.; Patch, C.; Emery, J. How can the evaluation of genetic tests be enhanced? Lessons learned from the ACCE framework and evaluating genetic tests in the United Kingdom. Genet Med Off J Am Coll Med Genet. 2005, 7, 495–500. [Google Scholar] [CrossRef]
- ACCE Model Process for Evaluating Genetic Tests | CDC [Internet]. 2022 [cited 2023 Oct 20]. Available online: https://www.cdc.gov/genomics/gtesting/acce/index.htm.
- WHO outlines considerations for regulation of artificial intelligence for health [Internet]. [cited 2023 Oct 25]. 2023. Available online: https://www.who.int/news/item/19-10-2023-who-outlines-considerations-for-regulation-of-artificial-intelligence-for-health.
- About the AI and Digital Regulations Service - AI regulation service - NHS [Internet]. [cited 2023 Oct 25]. Available online: https://www.digitalregulations.innovation.nhs.uk/about-this-service/.
- Vries A, d.e. The growing energy footprint of artificial intelligence. Joule [Internet]. 2023 Oct 10 [cited 2023 Oct 12];0(0). 2023. Available online: https://www.cell.com/joule/abstract/S2542-4351(23)00365-3.
- Topol, E.J. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019, 25, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, D.A.; Witkowski, E.; Gao, L.; Meireles, O.; Rosman, G. Artificial Intelligence in Anesthesiology: Current Techniques, Clinical Applications, and Limitations. Anesthesiology. 2020, 132, 379–94. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, H.; Liu, X.; Zariffa, N.; Morris, A.D.; Denniston, A.K. Health data poverty: an assailable barrier to equitable digital health care. Lancet Digit Health. 2021, 3, e260–5. [Google Scholar] [CrossRef] [PubMed]
- Fry, A.; Littlejohns, T.J.; Sudlow, C.; Doherty, N.; Adamska, L.; Sprosen, T. , et al. Comparison of Sociodemographic and Health-Related Characteristics of UK Biobank Participants With Those of the General Population. Am J Epidemiol. 2017/06/24 ed. 2017, 186, 1026–34. [Google Scholar] [CrossRef] [PubMed]
- Arora, A.; Alderman, J.E.; Palmer, J.; Ganapathi, S.; Laws, E.; McCradden, M.D. , et al. The value of standards for health datasets in artificial intelligence-based applications. Nat Med. 2023, 1–10. [Google Scholar]
- Tobias, D.K.; Merino, J.; Ahmad, A.; Aiken, C.; Benham, J.L.; Bodhini, D. , et al. Second international consensus report on gaps and opportunities for the clinical translation of precision diabetes medicine. Nat Med. 2023, 1–20. [Google Scholar]
- Ganapathi, S.; Palmer, J.; Alderman, J.E.; Calvert, M.; Espinoza, C.; Gath, J. , et al. Tackling bias in AI health datasets through the STANDING Together initiative. Nat Med. 2022, 28, 2232–3. [Google Scholar] [CrossRef]
- Jorgensen, A.L.; Prince, C.; Fitzgerald, G.; Hanson, A.; Downing, J.; Reynolds, J. , et al. Implementation of genotype-guided dosing of warfarin with point-of-care genetic testing in three UK clinics: a matched cohort study. BMC Med. 2019, 17, 1–11. [Google Scholar] [CrossRef]
- Mogaka, J.J.O.; James, S.E.; Chimbari, M.J. Leveraging implementation science to improve implementation outcomes in precision medicine. Am J Transl Res. 2020, 12, 4853–72. [Google Scholar] [PubMed]
- Khoury, MJ. No Shortcuts on the Long Road to Evidence-Based Genomic Medicine. JAMA. 2017, 318, 27–8. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Anothaisintawee, T.; Butani, D.; Wang, Y.; Zemlyanska, Y.; Wong, C.B.N. Assessing the cost-effectiveness of precision medicine: protocol for a systematic review and meta-analysis. BMJ Open. 2022, 12, e057537. [Google Scholar] [CrossRef] [PubMed]
- Mathur, S.; Sutton, J. Personalized medicine could transform healthcare. Biomed Rep. 2017, 7, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Evans, B.J.; Flockhart, D.A.; Meslin, E.M. Creating incentives for genomic research to improve targeting of therapies. Nat Med. 2020, 10, 1289–91. [Google Scholar] [CrossRef] [PubMed]
- Prasad, V.; De Jesús, K.; Mailankody, S. The high price of anticancer drugs: origins, implications, barriers, solutions. Nat Rev Clin Oncol. 2017, 14, 381–90. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.L.; Ziesche, S.; Yancy, C.; Carson, P.; D’Agostino, R.; Ferdinand, K. , et al. Combination of Isosorbide Dinitrate and Hydralazine in Blacks with Heart Failure. N Engl J Med. 2004, 351, 2049–57. [Google Scholar] [CrossRef]
- Linder, J.E.; Bastarache, L.; Hughey, J.J.; Peterson, J.F. The Role of Electronic Health Records in Advancing Genomic Medicine. Annu Rev Genomics Hum Genet. 2021, 22, 219–38. [Google Scholar] [CrossRef]
- Lind, S. NHS England could take co-data controller responsibility for GP patient records [Internet]. Pulse Today. 2023 [cited 2023 Oct 17]. https://www.pulsetoday.co.uk/news/breaking-news/nhs-england-could-take-co-data-controller-responsibility-for-gp-patient-records/.
- NHS Long Term Plan » Overview and summary [Internet]. [cited 2023 Nov 3]. Available online: https://www.longtermplan.nhs.uk/online-version/overview-and-summary/.
- Syal, R. Abandoned NHS IT system has cost £10bn so far. The Guardian [Internet]. 2013 Sep 17 [cited 2023 Nov 3]; Available from: https://www.theguardian.com/society/2013/sep/18/nhs-records-system-10bn.
- Topol, E.J. Machines and empathy in medicine. The Lancet. 2023, 402, 1411. [Google Scholar] [CrossRef]
Figure 2.
Figure 3.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



