
Submitted:
12 March 2024
Posted:
13 March 2024
You are already at the latest version
Abstract
Background:
Asthma is a widespread chronic respiratory disease that poses a significant public health challenge. The current study investigated the associations between air pollution and asthma severity among individuals residing near the Sohar industrial port (SIP) in Oman. Despite the presence of multiple major industrial complexes in Oman, limited knowledge regarding their impact on respiratory health is accredited. Hence, the primary objective of this study is to offer valuable insights into the respiratory health consequences of industrial air pollution in Al Batinah North.
Methods:
The state health clinics' records for patient visits related to asthma were collected for the timeframe spanning 2014 to 2022. Exposure was defined as the distance from SIP, Majan Industerial Area (MIA) and Sohar Industerial Zone (SIZ) to determine high, intermediate, and low exposure zones (12 km, respectively). Exposure effect modifications by age, gender, and smoking status were also examined.
Results:
The conducted cross-sectional study of 410 patients (46.1% males and 53.9% females) living in over 17 areas around SIP revealed that 73.2% of asthmatics were under 50 years old, with severity significantly associated with closeness to the port. Risk ratios were estimated to be (RR:2.42; CI95%: 1.01–5.78), (RR:1.91; CI95%: 1.01–3.6), and (RR:1.68; CI95%: 0.92–3.09) for SIP, MIP and SIZ areas, respectively, compared to the control area. Falaj Al Qabail (6.4 km) and Majees (6 km) had the highest number of asthma patients (N. 69 and N. 72), and highest percentages of severe asthma cases among these patients (28% and 24%) with significant risk ratios (RR:2.97; CI95%: 1.19–7.45 and RR:2.55; CI95%: 1.00–6.48), correspondingly. Moreover, severe asthma prevalence peaked in the 25-50 age group (RR:2.05; CI95%: 1.26–3.33), and this linkage between asthma and age was much more pronounced in males than females. Smoking and exposure to certain contaminant (dust and smoke) increased also the risk of severe asthma symptoms, but their effects were less important in the high risk zone, suggesting much more important risk factor. A neural network model accurately predicted asthma risk (94.8% accuracy), with proximity to Sohar Industrial Port as the most influential predictor.
Conclusion:
The study highlights the High asthma burden near Sohar Industrial Port, linked to port proximity and smoking and wind direction as major risk factors. These findings inform vital public health policies to reduce air pollution and improve respiratory health in the region, prompting national policy review.
Keywords:
Asthma
; Industrial Pollution
; Air Pollution
; Lung Diseases
; Health survey
; Oman
1. Introduction
Air pollution is a substantial environmental issue with profound implications for public wellbeing, particularly respiratory health. Industrial air pollution is a significant concern, with numerous studies highlighting its adverse effects on respiratory health [1,2,3]. Industrial activities, such as the combustion of fossil fuels, emit a wide range of pollutants, among which fine particulate matter (PM2.5) is prominent. These pollutants have been found to possess detrimental effects on respiratory health, contributing to the development of symptoms, exacerbating asthma, and increasing the risk of chronic respiratory diseases [4,5]. Moreover, long-term exposure to air pollution increases the risk of respiratory infections, cardiovascular diseases, and premature mortality [6,7,8]. It is noteworthy that living near industrial complexes auguments exposure to air pollutants, elevating the risk of respiratory diseases such as asthma, chronic obstructive pulmonary disease (COPD), and lung cancer [9,10].
Asthma is a chronic respiratory condition globally affecting individuals of all ages. It is characterized by an airway inflammation, bronchial hyperresponsiveness, and recurring episodes of airflow obstruction [11]. Worldwide, asthma affects 339 million people with approximately 5-10% experiencing severe symptoms that corresponds to around 17-34 million individuals. More than half of those face the challenges of an uncontrolled disease [12,13]. Severe asthma poses a significant burden due to its unpredictable symptoms and potential for life-threatening exacerbations [14]. It leads to substantial morbidity and mortality, resulting in a premature death and a reduced quality of life [15]. Lately, in 2019 asthma claimed over 461,000 lives, predominantly in low- and middle-income countries (LMIC) [16,17]. The challenges of timely diagnosis and effective treatment in these regions highlight the urgent need for exceptional management and prevention strategies. Oman ranks intermediate in asthma prevalence, with a 2009 study revealing high hospitalization rates, low use of preventive medications 5%, and a significant reliance on rescue medications 92% [18,19]. In Oman, asthma prevalence is 7.3% among adults and 12.7% among children [20]. 95% of asthma patients rely on government healthcare services. Inpatient visits account for 55% of direct costs, followed by emergency room and outpatient visits, 25% and 20%, respectively [20]. Older children have higher prevalence rates of asthma, allergic rhinitis, and eczema compared to younger children (20.7%, 10.5%, and 14.4% vs. 10.5%, 7.4%, and 7.5% respectively) [21]. Asthma control in Oman falls below the standard and falls short of the Global Initiative for Asthma (GINA) guidelines for long-term management [18]. Asthma management in Oman is poor, with high dependence on rescue medications and low utilization of preventive medications. Additionally, there is a lack of awareness about asthma severity, limited education, and low rates of lung function testing [18]. In 2009, the total direct cost of managing asthma in the country was estimated to exceed Omani rial 61,500,294, which is equivalent to approximately 160 million United States dollars [20]. This substantial economic impact underscores the need for effective strategies to manage asthma and reduce its associated costs.
Asthma is a multifactorial disorder influenced by both genetic and environmental factors which drastically contribute to its development and progression [22]. Even though genetic susceptibility plays a crucial role, the development and the progression of asthma also depend profoundly on numerous interactions with various environmental triggers [23]. Several issues including, family history of asthma, specific genetic variants related to the immune system function and airway responsiveness have been identified as risk factors [24]. In the same vein, epigenetic factors such as DNA methylation, histone modifications, and non-coding RNAs are also important contributors to the development and progression of asthma [25,26]. However, the increasing prevalence of asthma is primarily attributed to environmental changes as genetic and epigenetic factors alone are unlikely to undergo significant alterations within a short timeframe [27,28]. Extensive epidemiological and clinical experimental investigations consistently demonstrate a compelling association between air pollution exposure and the increased risk of exacerbating asthma symptoms. These studies have consistently shown a clear link between poor air quality and increased asthma incidence in both children and adults [29,30,31]. Furthermore, long-term exposure to various types of ambient air pollution, such as Traffic-related air pollution (TRAP) and indoor pollutants, has been identified as a significant factor in asthma development [32,33]. Furthermore, growing evidence suggests that air pollution not only triggers asthma exacerbations but also contributes to the development of new-onset asthma cases [10,34].
Several previous studies have emphasized the growing prevalence of asthma in low- and middle-income countries experiencing transitions, notably China, India, Brazil, and Oman. These studies highlight the importance of multiple factors, including rapid urbanization, changing lifestyle habits, and increased exposure to environmental allergens, as key contributors to the escalating burden of asthma in these regions [35,36,37,38].
The rapid industrialization and urbanization in Oman have led to a significant escalation in air pollution levels, primarily driven by industries such as oil refineries and manufacturing facilities [19]. The Sohar Industrial Port, one of the largest in the Middle East, has witnessed rapid industrial development, resulting in the emission of several harmful substances like sulfur dioxide, nitrogen oxides, particulate matter, and volatile organic compounds [39,40]. These contaminants contribute to poor air quality in the surrounding area, posing potential risks to both the environment and human health [39,41].
Despite substantial industrial growth at Sohar Industrial Port, research on asthma severity in nearby residents is scarce. Existing studies mainly focus on asthma development, not severity. Moreover, the combined impact of air pollution from Sohar Industrial Port (SIP), Sohar Industrial Zone (SIZ), and Majan Industrial Zone (MIZ) has not been explored. Furthermore, the influence of wind direction on the port’s surroundings has not been studied. Therefore, this study aims to assess the relationship between air pollution and the severity of asthma symptoms among residents near the port to bridge the knowledge gap and understand the potential consequences of cumulative air pollution on asthma severity within major industrial complexes. The findings of this study shall enable policymakers, regulators, and public health authorities to develop targeted interventions to mitigate the detrimental effects of air pollution on respiratory health.
2. Methods
2.1. Study Population
The current study was carried out in the rapidly growing Sohar Industrial Port (SIP) area, a densely populated region in the Sultanate of Oman. Residents living in close proximity to the major industrial complex were considered the study population; it is estimated at about 108,274 people, according to the latest census. A sample of 410 asthma patients (46.1% males and 53.9% females, with the majority, ~73.2% under 50 years old) from 17 different areas surrounding the SIP was selected based on specific criteria that ensure representation and homogeneity. Medical data of the asthma patients was obtained from the national Al-Shifa electronic health recording system, authorized by the Omani Ministry of Health (MoH). Data collection occurred in three healthcare centers located in Nabr, Falaj Al Qabail, and Liwa, chosen for their proximity to the industrial complex and for the presence of a significant number of asthma patients in their records. Inclusion criteria ensured that participants had a confirmed diagnosis of asthma, excluding individuals with other respiratory diseases or comorbidities that could potentially confound the study results. Additionally, the study specifically included patients who had resided near the port for at least one year. The analysis did not include people with important missing data.
2.2. Asthma Severity Assessment
Qualified physicians conducted a thorough evaluation of the participants showing asthma symptoms to determine the severity classification and the assessment was in adherence to the standardized criteria established by the Global Initiative for Asthma (GINA) [42]. By considering the type and frequency of reported asthma symptoms, the physicians categorized the severity into three distinct levels: severe, moderate, and mild. This classification framework provided a comprehensive understanding of the range of asthma severity experienced by the studied participants, enabling a meaningful analysis of the impact of air pollution on their asthma symptoms.
2.3. Exposure Zones
Asthma patients were categorized into three exposure zones based on their closeness to the Sohar industrial port; High exposure zone: Within <6 kilometer radius of the port, residents endure high levels of air pollutants associated with asthma exacerbations [32,43]. They experience increased asthma symptoms, hospital admissions, and emergency department visits [43]. Middle exposure zone: Located between 6 and 12 kilometers from the port, this zone still poses significant health impacts, including increased asthma symptoms, decreased lung function, and a higher prevalence of asthma [44]. Low exposure zone: Areas beyond 12 kilometers from the port have comparatively lower levels of air pollution, but may still experience health effects during periods of elevated pollution from industrial activities or weather-related events [45].
2.4. Sample Size Determination
Sample size in this study (N. 410) was larger than estimated (N. 246) using standard sample size equation, based on the estimated asthmatic population in Sohar (~16000 patient) and the proportion of severe asthma among asthma patients (20%), desired confidence (95%), and the margin of errors (5%) levels.
2.5. Data Collection
Data for this study was collected from three state health centers located in the study provinces, utilizing the national Al-Shifa electronic health recording system. The system provided extensive data from 2014 to 2022, ensuring a broad temporal scope. Data security and patient privacy were of utmost importance, and the research team strictly adhered to relevant regulations, approvals, and data sharing agreements throughout the data collection process to ensure integrity and confidentiality.
Medical records were utilized to gather clinical data related to asthma severity, medical history and demographic information (gender, marital status, place of residence, number of years of residency, smoking status).
2.6. Statistical Analysis
Comparisons between groups were performed using chi-squared test in categorical outcomes and Mann–Whitney U-test between categorical and nonparametric numerical data. Risk ratios (RR) and the 95 % confidence interval (CI) were calculated for the different exposure zones and factors in the study. Descriptive statistics, data analysis and artificial neural network (ANN) fitting model were carried out with SPSS v22 (IBM Corp., Armonk, NY, USA), and the graphs were done using GraphPad Prism® 7 (GraphPad Software, San Diego, CA, USA) and the level of two-sided significance of P-value was < 0.05.
2.7. Ethical Considerations
Ethical approval and data sharing agreements were obtained from the appropriate authorities, including both Ministry of Health and the Ethics and biosafety committee at the college of medicine & Health Sciences at National university of Science and Technology. All data were de-identified and handled in compliance with data protection regulations to ensure patient confidentiality and privacy.
Given the retrospective nature of the study and the utilization of de-identified data from the Shefa system, where patient identities were rigorously safeguarded, the acquisition of individual consent was considered unnecessary.
3. Results
3.1. Distribution of Asthma Severity among Omani Patients
The distribution of asthma severity among 410 patients (46.1% males and 53.9% females) living in 17 different areas surrounding Sohar Industrial Port (SIP) was investigated in the current study. The majority of asthmatics were under 50 years old (73.2%), with severity significantly associated with the proximity to the port. Most cases were classified as moderate (53.2%), while severe (20.5%) and mild (26.3%) asthma rates were relatively similar among both male and female patients (Figure 1). Differences between moderate and other asthma severity levels were highly significant according to one sample Chi-square statistical test.
Asthma patients were sorted out into three zones representing different pollution exposure levels based on their geographic location and distance from SIP (Table 1). Data analysis revealed a notable clustering of asthma cases in the propinquity to SIP (51.2%), indicating a higher prevalence of the condition within these specific areas. Additionally, an increase in severe asthma rates as the distance to SIP decreased was observed, Low (13%), Middle (35.2%) and High (51.9%), suggesting a relationship between proximity to SIP and asthma severity. This pattern was consistent among both male and female patients, with no statistically significant differences found between the two genders.
A comprehensive analysis was performed to calculate the average of asthma severity among patients residing in the three exposure zones. The analysis considered the entire patient population as well as distinct groups based on gender (males and females) and the average of distances covered by these patients within each of the three exposure zones (Figure 2). Results showed a clear decrease in the average of asthma severity in the low-exposure zone compared to the other two zones, which had similar average of severities and margins of error. Although the average of asthma severity for male and female patients in the middle exposure zone was similar, males had a slightly lower average of severity in the high-exposure zone, while females had a lower average of severity in the low-exposure zone.
We further analyzed the relationship between asthma severity, gender, and distance from SIP by comparing the averages of distances between the patients residence and the port for severe asthma cases versus moderate and mild cases combined together (Figure 3). Confirming the strong association between severe asthma and proximity to SIP compared to combined asthma (6.25/7.88 km, P=0.071), this difference was more pronounced and significant for males (P=0.035) than for females (P=0.502). On the other hand, male patients with severe asthma were significantly closer to SIP than females (5.33/6.91 km, P=0.033), but no such difference was observed between males and females with combined moderate and mild asthma (~ 7.8 km, P=0.181).
3.2. Industrial Zones in Sohar and Severe Asthma
In addition to SIP (Latitude:24.4904, Longitude:56.615), other industrial areas in Sohar’s northern region, such as Sohar Industrial Zone (SIZ, 24.3813,56.6516) and Majan Industrial Area (MIA, 24.4322,56.5728), were also investigated in terms of their contribution to severe asthma risk. Patients were divided into high, middle, and low exposure zones around each industrial area, and a control area (CA, 24.5103,56.5157) located to the north-west of Sohar was selected for comparison (Table 2). A comparative analysis was conducted to assess the prevalence of severe asthma among patients with different forms of asthma, specifically in high and low exposure areas surrounding industrial zones. Our results demonstrated that severe asthma was most strongly associated with SIP, followed by MIA, when compared to SIZ or the control area. Furthermore, our findings showed statistically significant differences for both SIP and MIA. Significant statistical differences were observed between the compared groups for SIP and MIA, estabilshing the substantial impact of these industrial zones.
The study also investigated the relationship between exposure to SIP pollution and the development of severe asthma for patients in the northern, southern, and middle regions surrounding the port (Table 2). Patients in the intermediate category are precisely situated within a latitude range that coincides with SIP location, encompassing a width of 5 kilometers. Notably, patients located at longitude lines below 56.5 were intentionally excluded from the calculation. A comparison was made between the frequency of severe asthma cases and other forms of asthma for patients in the middle, northern, and southern regions. Interestingly, the central region exhibited the highest level of risk in contrast to the northern region, implying a greater degree of vulnerability. In a fascinating observation, the southern region displayed a comparable level of hazard to that of the port itself, as evidenced by the risk ratio between these two areas.
3.3. Industrial Areas and Prevalence of Severe Asthma
The geographical distribution of Omani asthma patients around SIP and other industrial areas, was mapped based on latitude and longitude coordinates of each geographical region (Figure 4). By comparing these coordinates with those of the industrial areas, a significant increase in severe asthma patients was found in the proximity to SIP and other industrial regions, particularly in Ghadfan (27%, 2.6 km from SIP), Falaj al-Qabil (28%, 6.4 km from SIP), and Majees (24%, 6 km from SIP). Furthermore, the risk ratio in these regions was considerably high, measuring 2.88, 2.97, and 2.55, respectively, compared to other areas. Additionally, the differences in severe asthma cases compared to the control condition (moderate and mild asthma in areas more than 12 km away from SIP) were statistically significant, as determined by Chi-square test (Table 3).
3.4. Age-Related Patterns in Asthma Severity
The prevalence of asthma across distinct age groups was examined and compared between total and high exposure areas (<6 km from SIP) for both males and females (Table 4). Our findings consistently reveal a prevalence of asthma in the young and middle-aged groups, each accounting for approximately 36.6% of cases. This pattern remains consistent in the high exposure zone, with a slight increase to approximately 39%. Notably, severe asthma represents the highest percentage within the middle-aged group, comprising around 27% of cases and approximately 50% of severe asthma instances.
Furthermore, the middle-aged group exhibits a two-fold higher risk for severe asthma compared to the youth one (<25), and this difference proves statistically significant. The risk ratio slightly decreases to 1.78 in the high exposure zone, yet the statistical significance remains intact. When comparing gender, males exhibit a higher risk ratio (2.8) for severe asthma within the middle-aged group. This difference persists regardless of the total condition or the area most exposed to pollution, with statistical significance observed in the total condition. Conversely, the elder group (>50) shows a relatively lower risk compared to the aforementioned age group, and the risk further decreases in the area with the highest pollution exposure (Table 4).
The severity of asthma across different age groups and genders was examined to gain insights into its patterns. A comparison of the average of asthma severity revealed distinct variations among these groups (Figure 5). Notably, asthma severity tended to increase in the middle-aged group (25-50 years) when compared to both young (<25 years) and elder (>50 years) groups, and these differences were statistically significant. Interestingly, within the area with a high pollution exposure (<6 km from SIP), levels of significance between these age groups seems to be decreased. However, a substantial difference was noticed in the average of asthma severity of males in the youth group, as compared to the middle-aged and elder ones. This difference was less prominent among females. Proximity to SIP did not appear to have a clear impact on the distribution of asthma severity across the different age groups, but seems to reduce the differences between these groups.
An analysis of the average of ages of patients according to their asthma severity levels revealed a direct relationship between the severity of asthma and the average of patients’ ages, and the difference between the patients with severe and mild asthma was statistically significant (P=0.02) (Figure 6). Interestingly, this relationship was distinctly apparent and statistically significant among males (severe/moderate P=0.033, severe/mild P<0.001, and moderate/mild P=0.002), whereas it was nearly absent among females. Moreover, significant differences in the average of ages across two asthma severity categories (moderate P=0.001 and mild P<0.001) were observed between males and females. Surprisingly, proximity to the port seemed to diminish the association between asthma severity and age and most of the significant differences seem to have been lost, except between severe and mild asthma in males which is reduced to P=0.018. In the case of females, this relationship even appeared to be reversed.
3.5. Asthma Severity and Smoking Status
In this study, we conducted an analysis on the association between smoking and asthma severity, with a particular focus on the impact of the primary pollution source, namely SIP. Notably, our findings revealed a remarkably low percentage (5.4%) of smokers among the patients included in the study. Moreover, we observed a higher prevalence of smokers (10.1%) among male patients compared to (1.4%) among female patients (Table 5). When examining the distribution of asthma severity levels among patients based on their smoking status, smokers exhibited a higher percentage (90.9%, 20 cases) of severe and moderate asthma compared to passive smokers (80.5%, 33 cases) and non-smokers (72%, 249 cases). However, these percentages slightly decreased: smokers (88.1%, 8 cases), passive smokers (81.8%, 18 cases), and non-smokers (71.5%, 128 cases) in the closest area to SIP with the highest pollution exposure (<6 km). Furthermore, when assessing the risk ratio associated with smoking, we found that smokers had higher chances at ~ 1.7 and 1.1 of developing severe asthma compared to mild asthma or combined asthma (mild and moderate) respectively, in comparison to non-smokers. These values decreased to 1.1 and 0.46 for patients residing in the highly exposed area.
A compelling pattern emerges when examining the average of asthma severity among different groups of patients, namely smokers, passive smokers, and non-smokers. A discernible and consistent gradient can be observed in the association between the average of asthma severity and smoking (Figure 7). However, it is noteworthy that this link becomes somewhat less distinct within the community of patients residing in close proximity to SIP. This finding implies that pollution stemming from the port may wield a more significant impact on the average of asthma severity than smoking itself.
3.6. Asthma Severity and Air Contaminants
During the process of collecting patients data, their opinions were solicited regarding the primary pollutants they believed to occur in their surroundings, potentially triggering their asthma symptoms (Table 6). The identified pollutants included dust, incense, perfume, and smoke. Among the surveyed asthmatic patients, 68.5% acknowledged the existence of pollution matter in their environment, which they considered a potential cause of their asthma symptoms. Interestingly, the percentage of severe asthmatics within this group (19.2%) was lower compared to those who were uncertain about the presence of a clear pollution factor in their surroundings (23.2%). Analyzing the four investigated pollutants, it was found that incense was the most frequently reported (33.4% of responses and 81.8% of respondents). However, incense had the lowest risk ratio (RR = 0.96) among the pollutants, indicating a lesser association with a severe asthma (20.1% of patients). When considering different types of asthma and comparing them with the exposed and unexposed populations, smoke emerged as the most significant risk factor for the development of severe asthma, with a risk ratio of 1.27. Dust followed closely with a risk ratio of 1.2, while perfume exhibited a risk ratio of 1.11. It is noteworthy that the risk ratios for smoke (1.41) and perfume (1.21) slightly increased in the area closest to the port (within a 6 km radius), whereas the one for dust decreased (1.02). Although the percentage of respondents who identified smoke as a contributing factor was the lowest (29.6%), it also collected the lowest affirmative responses (“yes”) regarding its presence as a pollutant (12.1%).
Subsequently, we conducted a thorough investigation of the disparities in “Yes” responses in contaminants survey between males and females, and the existence of a relationship with severe asthma as well as proximity to the port (Figure 8). The findings clearly indicated a statistically significant divergence of opinions regarding the negative impact of these pollutants on asthma development (P<0.001), except for dust and perfume where no significant differences were observed. Specifically, when comparing the percentage of male and female “Yes” voters, smoke emerged as the least significant pollution factor among those with a high statistical significance. It is noteworthy that there was an unanimous agreement, statistically significant, that incense was the most bothersome factor for male and female asthma patients. This perception remained consistent regardless of the severity of asthma or proximity to SIP. Additionally, an interesting observation was the increase, particularly among males, in affirming the presence of smoke contamination among the group of severe asthma patients and those living near SIP. Although not reaching full statistical significance, there was a notable difference of opinion on the effect of smoke between males and females in these three conditions, approaching significance (P=0.06 by the Chi-square test).
3.7. Predicting Asthma Risk by Artificial Neural Networks
A multilayer perceptron neural network was employed to construct a predictive model for a dependent variable, which represents the risk of developing asthma. The model was developed based on a set of predictor variables, namely age, smoking status, region, gender, and proximity to the three industrial zones. In this study, the dependent variable, referred to as “Asthma Risk (AR)”, was categorized into five levels ranging from 1 (Very Low Risk) to 5 (Very High Risk). To ensure homogenous comparisons, the covariates were rescaled using the standardized method as the default approach. To apply the neural network technique effectively, the dataset was partitioned into two distinct sets: a training set comprising 70% of the data (N = 286) and a testing set comprising the remaining 30% (N = 124). It is important to note that there were no missing values in either set. The training set was utilized to train the neural network and develop the model, while the testing set served as an independent dataset to monitor errors during training and prevent overfitting (Figure 9). For the construction of the AR network, a single hidden layer was employed, with the number of units in the layer architecture ranging from 1 to 50 [46].
The network stopping rule was implemented to terminate training when the maximum number of steps was reached without observing a decrease in error. The model achieved a 5.2% rate of incorrect predictions with a training time of 17 milliseconds and a cross entropy error of 52. Furthermore, the model’s performance was assessed again, yielding a percentage of incorrect predictions of 9.7% with a cross-entropy error of 45. The classification table displays the percentages of correct predictions, revealing an overall accuracy of 94.8% for the training dataset and 90.3% for the testing dataset. It is worth noting that the correct prediction percentages for risk levels were higher for average risk compared to very high or very low levels (Table 7).
We examined the sensitivity and specificity (represented as 1 − the false positive rate) of the model in predicting each level of AR model, using the combined training and testing samples. To assess the performance of the model, we employed the areas under the curve (ROC) analysis on combined training and testing samples. Remarkably, the ROC curve for all predicted AR levels surpassed a threshold of 0.98, indicating highly acceptable results.
Additionally, an assessment of the normalized importance of each predictor variable revealed the prominence of proximity to SIP as the most influential factor. Subsequently, several covariates such as proximity to MIA and SIZ areas, age, and regions followed in terms of importance (Figure 10). Conversely, smoking and gender had minimal impact on the constructed neural network model. Normalized importance serves as a quantifiable measure of the extent to which the predicted value of the dependent variable, AR, would be affected by the exclusion of a particular predictive indicator.
4. Discussion
The fast industrialization and expansion of Oman’s Sohar Industrial Port have led to a continuous growth in industries, resulting in an increased air pollution. Addressing this pressing issue necessitates the undertaking of a comprehensive study. The contemporary cross-sectional study aims to investigate the association between industrial air pollution from Sohar Industrial Port in Oman and respiratory health outcomes among individuals visiting health centers located in close vicinity to the port. Thus, our objective was to assess the prevalence and severity of asthma among a sample of 410 Omani asthma patients (46.1% males, 53.9% females). Most patients were under 50 years old (73.2%). Asthma severity distribution was as follows: moderate (53.2%), severe (20.5%), and mild (26.3%). Proximity to the port significantly influenced severity, with 51.2% residing within 6 km (high exposure zone). Severe asthma rates increased closer to the port, while the lowest severity was observed in the low exposure zone (>12 km). The middle (6-12 km) and high exposure zones had similar severity levels.
Results of this study show a close relationship between exposure to air pollution from Sohar Industrial Port and other industrial areas and the severity of asthma among patients living nearby. The percentage of severe asthma cases was higher among patients living closer to the port (<6 km), and decreased as the distance from the port increased. This indicates that proximity to the port is a critical risk factor for developing severe asthma. These findings align with previous studies. Al-Wahaibi and Zeka [47] also found that living closer to Sohar Industrial Zone increased the risk of asthma and other respiratory conditions. Other studies have linked industrial air pollution to worsen asthma symptoms due to irritants in the emissions [48,49]. Moreover, Mock et al. highlighted the significant impact of city industrial zoning on pediatric asthma outcomes in communities with limited access to air monitoring [50].
The current study’s findings are also in agreements with various international studies that found a strong association between living near ports or industrial sites and bad asthma outcomes [51,52]. For instance, a study by Guarnieri and Balmes [10] revealed that exposure to air pollutants, such as particulate matter and nitrogen dioxide, was associated with exacerbated asthma symptoms. Similarly, a study by Orellano et al. [53] found that exposure to traffic-related air pollution increased the risk of asthma exacerbation in children. This supports the notion that industrial pollution can play a vital role in exacerbating asthma and highlights the importance of considering the impact of proximity to industrial ports when examining asthma prevalence and severity.
Our study’s findings provide further support to the body of evidence that establishes a clear link between industrial exposure and heightened occurrences of severe asthma. Specifically, we observed that areas in close proximity to the Majan Industrial Area and Sohar Industrial Port, characterized by significant exposure, exhibited notably increased rates of severe asthma. The risk ratios associated with these high exposure zones were found to be 2.88 and 2.97 respectively. These results align with previous research conducted across diverse global regions, reinforcing the well-documented association between environmental pollution and respiratory diseases such as asthma.
Several research studies have shed light on the detrimental effects of air pollution on human health. Notably, a study conducted in China in 2016 revealed a strong correlation between air pollution resulting from industrial activities and the prevalence of asthma in children [54]. Similarly, a study conducted in the United States demonstrated that individuals residing in close proximity to industrial zones had elevated risks of developing respiratory diseases, including asthma [55].
Despite the lack of specific data from Oman, these international studies provide a comparative perspective. The current findings fill a significant gap in the literature by providing localized data from Oman. These results highlight the importance of addressing industrial pollution in Oman, particularly near high-exposure zones such as the Majan Industrial Area and Sohar Industrial Port, to mitigate the health risks associated with such exposure.
However, the southern region exhibits a comparatively lower risk ratio of 2.55, albeit still elevated, warranting a comprehensive inquiry. This divergence may be attributed to variations in industrial activities, wind patterns, or other environmental and demographic factors that could potentially modulate the dissemination and impacts of pollutants, necessitating thorough examination. These findings add to the growing body of evidence substantiating the link between industrial pollution and severe asthma. They underscore the need for effective environmental regulations and public health measures, especially in high-risk areas.
The finding of higher risks in the central region closest to the Sohar Industrial Port also aligns with the results of Raaschou-Nielsen et al. [56], who found the strongest associations between traffic-related air pollution exposure and childhood asthma hospital admissions within the first 500 m from major roads. The fact that the southern region further from the sources still experienced an increased risk ratio of 2.55 compared to the reference population suggests that the impact of industrial emissions may extend over a wider area, though risks do appear to reduce with distance from the source.
Notably, among male patients, the high-exposure zone showed a slightly lower average of severity compared to the middle-exposure zone. Conversely, female patients demonstrated a lower average of severity in the low-exposure zone. Severe asthma patients lived closer to the port (average 6.25 km) than moderate/mild patients (average 7.88 km). This was more significant for males (severe: 5.33 km, moderate/mild: 7.8 km). To provide further details, we compared our findings with results from studies conducted in the vicinity of Sohar Industrial Port, as well as in other countries. Our findings were compared with the results of previous studies carried out in the vicinity of Sohar Industrial Port, as well as in other countries [7,47,50,57,58,59,60,61].
Our results showed a clear decrease in the average of asthma severity in the low-exposure zone compared to the other two zones, which had similar averages of severity and margins of error. These findings are consistent with previous studies conducted near Sohar Industrial Port, where low-exposure areas exhibited lower asthma severity compared to high-exposure areas [47].
Furthermore, our examination of gender-specific differences revealed that, within the middle exposure zone, the average of asthma severity was similar for male and female patients. However, in the high exposure zone (within 6 km from the port), females exhibited slightly higher asthma severity compared to males. It is important to note that our study did not establish a general trend of men having more severe asthma than women. These gender-related findings align with previous international studies that have reported similar patterns of asthma severity based on gender and exposure levels which could be due to variations in occupational exposures, horizontal segregation in the workforce, and diverse behaviors within the workplace which can impact the level of exposure and subsequent health outcomes [62,63,64].
In addition, although the risk ratio for severe asthma was high for males across all three exposure zones, there was no universally established consensus that men had more severe asthma than women living away from industrial areas. Various lifestyle factors influence the severity of asthma. Men working in occupations with higher exposure to irritants or allergens may be more prone to asthma symptoms. Population-based studies in South Finland have shown a link between occupational exposures and prevalent asthma. Clinical evidence suggests that females experience increased asthma symptoms during puberty due to hormonal changes. Estrogen increases airway inflammation, while testosterone decreases it, as demonstrated in animal studies [65]. Occupational and lifestyle exposures contribute to the observed differences in asthma severity between men and women [66,67]. Additionally, individual sensitivity and the amount of irritants present can vary, leading to varying degrees of asthma symptoms [68].
In our study, severe asthma prevalence, compared to other levels of the disease, was the highest in patients aged 25-50 years (27.3%, 2.05 risk ratio). Furthermore, this middle age group had the highst percentage of sever asthma patients (48.8%) and the average of asthma severity (2.1) compared to other age groups. Studies have shown that around half of middle-aged asthma patients developed the condition in adulthood rather than during childhood [69] [70]. The annual incidence of asthma among adults is estimated to be 0.5%, similar to childhood incidence, but it remains uncertain whether adult-onset asthma is the same as childhood-onset asthma [71]. Interestingly, previous studies demonstrated that asthma in adults is progressing at a faster rate than in childhood. This could be due to the complexity of adult-onset asthma, which is characterized by a diverse range of symptoms and outcomes. Unlike childhood asthma, which often enters a period of remission, asthma in adulthood tends to be more severe and progressive [72,73].
Furthermore, our findings revealed that the elder group (>50 years) exhibited a lower level of severe asthma compared to the mentioned age range. Moreover, in areas with high pollution exposure, the risk decreased even further. A study on the natural history of asthma supported our findings, indicating that atopy is not a risk factor in the elderly age group [74]. Interestingly, older patients who develop asthma have a similar incidence rate to younger individuals (100 per 100,000) [75]. However, the severity of asthma tends to be more pronounced in the older age group due to poor lung function and fixed airway obstruction [76]. In contrast, a study by Al-wahaibi suggested that living near the exposure source increased the risk of asthma in individuals over 50, indicating greater vulnerability within this age group [47].
Our study revealed a high prevalence of incense use among both male and female asthma patients (33.4%), regardless of asthma severity or proximity to the source of indoor pollution (SIP). However, it is noteworthy that incense showed the lowest risk ratio (0.96 risk ratio). among the pollutants examined, indicating a weaker association with severe asthma [77]. These findings are consistent with previous research conducted on Omani children from two regions with varying asthma prevalence. The studies demonstrated that exposure to incense triggers asthma symptoms but does not have a significant association with the prevalence of current asthma [57]. In contrast, smoke emerged as the most significant risk factor for the development of severe asthma. In the present study, 5.4% of patients were smokers, mostly males (10.1% of all patients). Moreover, smokers had a higher risk to develop severe asthma (1.7 risk ratio) compared to non-smokers with mild asthma. Average of asthma severity was the highest in smokers, followed by passive smokers then non-smokers. This trend was less prominent near the port. This finding aligns with previous studies that have observed the detrimental effects of smoke originating from various sources, including environmental tobacco smoke, air pollution (such as wood smoke and particulate matter), industrial pollution, and vehicle emissions, on asthma symptoms and asthma risk [61]. The results of our study emphasize the importance of reducing exposure to smoke and implementing measures to mitigate its adverse effects on individuals with asthma [77].
A multilayer perceptron neural network was used to construct a predictive model for the risk of developing asthma. The model achieved an overall accuracy of 94.8% for the training dataset and 90.3% for the testing dataset. The areas under the ROC curve for all predicted risk levels exceeded a threshold of 0.98, indicating highly acceptable results. The analysis of predictor variables revealed that proximity to the SIP industrial zone exerted the greatest influence on asthma risk, followed by proximity to other industrial zones, age, and regions. However, smoking and gender had minimal impact on the neural network model. These findings are consistent with previous studies that demonstrated the effectiveness of various neural network models in accurately predicting asthma-related outcomes [78,79]. These studies consistently highlight the pivotal role of air pollution and meteorological variables as influential factors in asthma prediction. However, it is worth noting that the present study found that smoking and gender had minimal impact on the constructed neural network model, which is different from some previous research. For example, a study by Ho et al. [80] found that smoking status and gender were significant predictors of asthma risk. This discrepancy may be due to differences in the study population, especially the low percentage of smokers in Omani society, or the specific neural network architecture employed. In addition, our statistical analyzes did not show a direct relationship between asthma severity and gender, which makes our network’s prediction model more reasonable. Future research could explore the use of alternative neural network architectures or additional predictors to further improve the accuracy of these models.
5. Conclusion
The finding of this study provides several new insights into the relationship between industrial pollution exposure and asthma severity in Oman. Our study found higher rates of severe asthma north and south of SIP compared to the west, indicating localized differences in pollution exposure. This underscores the need for localized assessment of pollution emissions to understand the varying burden of asthma severity around SIP and other industrial zones. Moreover, Middle-aged men face a higher risk of severe asthma compared to other age groups, particularly when compared to women in the same age range. This highlights the need for targeted interventions to address pollution-related health effects in specific demographic groups. This finding is novel and not previously reported in Oman or the literature. Furthermore, smoking worsens asthma, but air pollution’s severe impact near pollution sources may overshadow the effects of smoking on asthma severity. The interaction between smoking and air pollution is complex, with their health burdens not simply adding up. Finally, our study emphasizes localized pollution controls for asthma near pollution sources. Regional controls may be ineffective due to high exposure “hotspots.” Recommendations include localized monitoring and mitigation in Oman. Therefore, our findings point to localized differences in impacts around pollution sources, an increased vulnerability in certain groups like middle-aged men, interactions between air pollution and smoking, and the need for localized pollution controls to maximize health benefits. By highlighting these localized aspects, this research helps build a more nuanced understanding of asthma and pollution in this region.
Author Contributors
Souad Al Okla initiated, designed and supervised the study. Abdul Qader Abbady conducted all statistical analysis. Both Al Okla and Abbady actively participated in the discussion of the results, interpretation of finding and writing the manuscript. Fatima Alzahra Alrasbi, Hawida Said Al Marhubi, Shima Salim Al Mataani and Yusra Mohammed Al Sawai involved in the data collection and conducting the literature review. Hasa Ibrahim Mohammed, Muna Ali Salim Al Mamari and Salwa Abdullah Abdulrahim Al Balushi provided access to patients, reviewing medical records, and contributed their expertise in collecting relevant data. All authors reviewed and approved the final version of the manuscript.
Role of funding source
Funding for this study is provided by the Research Council, Oman (BFP/RGP/EBR/18/160), The opinions, results and conclusions presented in this report are those of the authors and are independent from the funding sources.
Conflicts of interest
We declare that we have no conflicts of interest.
References
- E. Garcia, K.T. Berhane, T. Islam, R. McConnell, R. Urman, Z. Chen, F.D. Gilliland, Association of Changes in Air Quality With Incident Asthma in Children in California, 1993-2014., JAMA. 321 (2019) 1906–1915. [CrossRef]
- S.M. Simkovich, D. Goodman, C. Roa, M.E. Crocker, G.E. Gianella, B.J. Kirenga, R.A. Wise, W. Checkley, The health and social implications of household air pollution and respiratory diseases., NPJ Prim. Care Respir. Med. 29 (2019) 12. [CrossRef]
- C. Cheng, C. Han, Q. Fang, Y. Liu, X. Chi, X. Li, Associations between air pollutants and hospital admissions for chronic obstructive pulmonary disease in Jinan: potential benefits from air quality improvements., Environ. Sci. Pollut. Res. Int. 30 (2023) 46435–46445. [CrossRef]
- S.C. Anenberg, D.K. Henze, V. Tinney, P.L. Kinney, W. Raich, N. Fann, C.S. Malley, H. Roman, L. Lamsal, B. Duncan, R.V. Martin, A. van Donkelaar, M. Brauer, R. Doherty, J.E. Jonson, Y. Davila, K. Sudo, J.C.I. Kuylenstierna, Estimates of the Global Burden of Ambient PM2.5, Ozone, and NO2 on Asthma Incidence and Emergency Room Visits., Environ. Health Perspect. 126 (2018) 107004. [CrossRef]
- S. D’Antona, I. Castiglioni, D. Porro, C. Cava, Consequences of exposure to pollutants on respiratory health: From genetic correlations to causal relationships., PLoS ONE. 17 (2022) e0277235. [CrossRef]
- A.J. Cohen, M. Brauer, R. Burnett, H.R. Anderson, J. Frostad, K. Estep, K. Balakrishnan, B. Brunekreef, L. Dandona, R. Dandona, V. Feigin, G. Freedman, B. Hubbell, A. Jobling, H. Kan, L. Knibbs, Y. Liu, R. Martin, L. Morawska, C.A. Pope, M.H. Forouzanfar, Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015., Lancet. 389 (2017) 1907–1918. [CrossRef]
- G.D. Thurston, J.R. Balmes, E. Garcia, F.D. Gilliland, M.B. Rice, T. Schikowski, L.S. Van Winkle, I. Annesi-Maesano, E.G. Burchard, C. Carlsten, J.R. Harkema, H. Khreis, S.R. Kleeberger, U.P. Kodavanti, S.J. London, R. McConnell, D.B. Peden, K.E. Pinkerton, J. Reibman, C.W. White, Outdoor Air Pollution and New-Onset Airway Disease. An Official American Thoracic Society Workshop Report., Ann. Am. Thorac. Soc. 17 (2020) 387–398. [CrossRef]
- C.-K. Chang, Y.-K. Lin, C.-W. Lin, M.-W. Su, H.-W. Chu, C.-D. Wu, Y.-T. Zeng, B.-L. Chang, Effects of long-term exposure to major outdoor air pollutants for the risk of chronic inflammatory airway diseases in adults with potential interaction detection in Taiwan Biobank, Atmos. Environ. 288 (2022) 119296. [CrossRef]
- D. Kim, Z. Chen, L.-F. Zhou, S.-X. Huang, Air pollutants and early origins of respiratory diseases., Chronic Diseases and Translational Medicine. 4 (2018) 75–94. [CrossRef]
- M. Guarnieri, J.R. Balmes, Outdoor air pollution and asthma., Lancet. 383 (2014) 1581–1592. [CrossRef]
- T.F. Carr, E. Bleecker, Asthma heterogeneity and severity., World Allergy Organiz. J. 9 (2016) 41. [CrossRef]
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators, Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016., Lancet. 390 (2017) 1211–1259. https://doi.org/10.1016/S0140-6736(17)32154-2. [CrossRef]
- GBD 2015 Chronic Respiratory Disease Collaborators, Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015., Lancet Respir. Med. 5 (2017) 691–706. https://doi.org/10.1016/S2213-2600(17)30293-X. [CrossRef]
- Menzies-Gow, D.J. Jackson, M. Al-Ahmad, E.R. Bleecker, F. de B.G. Cosio Piqueras, S. Brunton, G.W. Canonica, C.K.N. Chan, J. Haughney, S. Holmes, J. Kocks, T. Winders, A renewed charter: key principles to improve patient care in severe asthma., Adv. Ther. 39 (2022) 5307–5326. [CrossRef]
- M. Netz, D.A. Fedele, R. Sweenie, D. Baker, M. Light, E.L. McQuaid, Asthma management responsibility, control, and quality of life among emerging adolescents., J. Pediatr. Psychol. 45 (2020) 40–49. [CrossRef]
- H.K. Reddel, E.D. Bateman, A. Becker, L.-P. Boulet, A.A. Cruz, J.M. Drazen, T. Haahtela, S.S. Hurd, H. Inoue, J.C. de Jongste, R.F. Lemanske, M.L. Levy, P.M. O’Byrne, P. Paggiaro, S.E. Pedersen, E. Pizzichini, M. Soto-Quiroz, S.J. Szefler, G.W.K. Wong, J.M. FitzGerald, A summary of the new GINA strategy: a roadmap to asthma control., Eur. Respir. J. 46 (2015) 622–639. [CrossRef]
- H. Tarraf, O. Aydin, D. Mungan, M. Albader, B. Mahboub, A. Doble, A. Lahlou, L. Tariq, F. Aziz, A. El Hasnaoui, Prevalence of asthma among the adult general population of five Middle Eastern countries: results of the SNAPSHOT program., BMC Pulm. Med. 18 (2018) 68. [CrossRef]
- N. Al-Busaidi, J.B. Soriano, Asthma Control in Oman: National Results within the Asthma Insights and Reality in the Gulf and the Near East (AIRGNE) Study., Sultan Qaboos Univ. Med. J. 11 (2011) 45–51.
- N. Al-Busaidi, Z. Habibulla, M. Bhatnagar, N. Al-Lawati, Y. Al-Mahrouqi, The burden of asthma in oman., Sultan Qaboos Univ. Med. J. 15 (2015) e184-90.
- N.H. Al-Busaidi, Z. Habibullah, J.B. Soriano, The asthma cost in oman., Sultan Qaboos Univ. Med. J. 13 (2013) 218–223.
- B.M.S. Al-Riyami, O.A.S. Al-Rawas, A.A. Al-Riyami, L.G. Jasim, A.J. Mohammed, A relatively high prevalence and severity of asthma, allergic rhinitis and atopic eczema in schoolchildren in the Sultanate of Oman., Respirology. 8 (2003) 69–76. [CrossRef]
- F. Kauffmann, F. Demenais, Gene-environment interactions in asthma and allergic diseases: challenges and perspectives., J. Allergy Clin. Immunol. 130 (2012) 1229–40; quiz 1241. [CrossRef]
- A.J. Burbank, A.K. Sood, M.J. Kesic, D.B. Peden, M.L. Hernandez, Environmental determinants of allergy and asthma in early life., J. Allergy Clin. Immunol. 140 (2017) 1–12. [CrossRef]
- R. Hall, I.P. Hall, I. Sayers, Genetic risk factors for the development of pulmonary disease identified by genome-wide association., Respirology. 24 (2019) 204–214. [CrossRef]
- F. Moheimani, A.C.-Y. Hsu, A.T. Reid, T. Williams, A. Kicic, S.M. Stick, P.M. Hansbro, P.A.B. Wark, D.A. Knight, The genetic and epigenetic landscapes of the epithelium in asthma., Respir. Res. 17 (2016) 119. [CrossRef]
- T. Zhang, P. Huang, C. Qiu, Progresses in epigenetic studies of asthma from the perspective of high-throughput analysis technologies: a narrative review., Ann. Transl. Med. 10 (2022) 493. [CrossRef]
- S. Salvi, S. Limaye, Effects of air pollution on allergy and asthma, in: P.K. Vedanthan, H.S. Nelson, S.N. Agashe, P.A. Mahesh, R. Katial (Eds.), Textbook of Allergy for the Clinician, CRC Press, Second edition. | Boca Raton : CRC Press, 2021., 2021: pp. 219–230. [CrossRef]
- T.A. Platts-Mills, S.P. Commins, Increasing prevalence of asthma and allergic rhinitis and the role of environmental factors, UpToDate. (2016).
- W. Lin, B. Brunekreef, U. Gehring, Meta-analysis of the effects of indoor nitrogen dioxide and gas cooking on asthma and wheeze in children., Int. J. Epidemiol. 42 (2013) 1724–1737. [CrossRef]
- R.J. Delfino, J. Wu, T. Tjoa, S.K. Gullesserian, B. Nickerson, D.L. Gillen, Asthma morbidity and ambient air pollution: effect modification by residential traffic-related air pollution., Epidemiology. 25 (2014) 48–57. [CrossRef]
- G. Bowatte, C. Lodge, A.J. Lowe, B. Erbas, J. Perret, M.J. Abramson, M. Matheson, S.C. Dharmage, The influence of childhood traffic-related air pollution exposure on asthma, allergy and sensitization: a systematic review and a meta-analysis of birth cohort studies., Allergy. 70 (2015) 245–256. [CrossRef]
- H. Khreis, C. Kelly, J. Tate, R. Parslow, K. Lucas, M. Nieuwenhuijsen, Exposure to traffic-related air pollution and risk of development of childhood asthma: A systematic review and meta-analysis, Environ. Int. 100 (2017) 1–31. [CrossRef]
- C.-R. Jung, W.-T. Chen, Y.-H. Tang, B.-F. Hwang, Fine particulate matter exposure during pregnancy and infancy and incident asthma., J. Allergy Clin. Immunol. 143 (2019) 2254-2262.e5. [CrossRef]
- E. Toskala, D.W. Kennedy, Asthma risk factors., Int. Forum Allergy Rhinol. 5 Suppl 1 (2015) S11-6. [CrossRef]
- M. Feng, Z. Yang, L. Pan, X. Lai, M. Xian, X. Huang, Y. Chen, P.C. Schröder, M. Roponen, B. Schaub, G.W.K. Wong, J. Li, Associations of early life exposures and environmental factors with asthma among children in rural and urban areas of guangdong, china., Chest. 149 (2016) 1030–1041. [CrossRef]
- M.E. Soto-Martínez, M.E. Soto-Quiros, A. Custovic, Childhood Asthma: Low and Middle-Income Countries Perspective., Acta Med. Acad. 49 (2020) 181–190. [CrossRef]
- GBD 2019 Universal Health Coverage Collaborators, Measuring universal health coverage based on an index of effective coverage of health services in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019., Lancet. 396 (2020) 1250–1284. [CrossRef]
- M.O. Zeitouni, M.S. Al-Moamary, M.L. Coussa, M. Riachy, B. Mahboub, F. AlHuraish, M.H. Zidan, M.M. Metwally, K. Aksu, E. Yavuz, I.S. Kalla, J. Chakaya, S. Abdelmadjid, H. Ghedira, Challenges and recommendations for the management of asthma in the Middle East and Africa., Ann. Thorac. Med. 17 (2022) 71–80. [CrossRef]
- Farahat, Air quality in the Gulf Cooperation Council (GCC) countries, in: Asian Atmospheric Pollution, Elsevier, 2022: pp. 201–226. [CrossRef]
- J. Yousif, N. Alattar,, M. Fekihal, Forecasting Models Based CO2 Emission for Sultanate of Oman, Int J Appl Eng Res. 12 (2012) 95–100.
- M.S. Baawain, A.S. Al-Serihi, Systematic Approach for the Prediction of Ground-Level Air Pollution (around an Industrial Port) Using an Artificial Neural Network, Aerosol Air Qual. Res. 14 (2014) 124–134. [CrossRef]
- GINA, Global Initiative for Asthma - GINA, GINA Main Report. (2022). https://ginasthma.org/gina-reports/ (accessed January 1, 2022).
- T. To, J. Zhu, P.J. Villeneuve, J. Simatovic, L. Feldman, C. Gao, D. Williams, H. Chen, S. Weichenthal, C. Wall, A.B. Miller, Chronic disease prevalence in women and air pollution--A 30-year longitudinal cohort study., Environ. Int. 80 (2015) 26–32. [CrossRef]
- S.B. Henderson, B. Beckerman, M. Jerrett, M. Brauer, Application of land use regression to estimate long-term concentrations of traffic-related nitrogen oxides and fine particulate matter., Environ. Sci. Technol. 41 (2007) 2422–2428. [CrossRef]
- Y. Zhang, H. Ni, L. Bai, Q. Cheng, H. Zhang, S. Wang, M. Xie, D. Zhao, H. Su, The short-term association between air pollution and childhood asthma hospital admissions in urban areas of Hefei City in China: A time-series study., Environ. Res. 169 (2019) 510–516. [CrossRef]
- G.E. Hinton, R.R. Salakhutdinov, Reducing the dimensionality of data with neural networks., Science. 313 (2006) 504–507. [CrossRef]
- Al-Wahaibi, A. Zeka, Health impacts from living near a major industrial park in Oman., BMC Public Health. 15 (2015) 524. [CrossRef]
- G.D. Nielsen, S.T. Larsen, P. Wolkoff, Recent trend in risk assessment of formaldehyde exposures from indoor air., Arch. Toxicol. 87 (2013) 73–98. [CrossRef]
- C.Y. Yang, J.F. Chiu, M.F. Cheng, M.C. Lin, Effects of indoor environmental factors on respiratory health of children in a subtropical climate., Environ. Res. 75 (1997) 49–55. [CrossRef]
- K. Mock, A.M. Palma, J. Wu, J. Billimek, K.D. Lu, Breathing room: industrial zoning and asthma incidence using school district health records in the city of santa ana, california., Int. J. Environ. Res. Public Health. 19 (2022). [CrossRef]
- J.S. Lwebuga-Mukasa, T.J. Oyana, P. Wydro, Risk factors for asthma prevalence and chronic respiratory illnesses among residents of different neighbourhoods in Buffalo, New York., J. Epidemiol. Community Health. 58 (2004) 951–957. [CrossRef]
- Y. Kim, J. Cho, F. Wen, S. Choi, The built environment and asthma: Los Angeles case study, J Public Health (Bangkok). 31 (2023) 57–64. [CrossRef]
- P. Orellano, N. Quaranta, J. Reynoso, B. Balbi, J. Vasquez, Effect of outdoor air pollution on asthma exacerbations in children and adults: Systematic review and multilevel meta-analysis., PLoS ONE. 12 (2017) e0174050. [CrossRef]
- Y. Jin, H. Andersson, S. Zhang, Air pollution control policies in china: A retrospective and prospects., Int. J. Environ. Res. Public Health. 13 (2016). [CrossRef]
- G. Cesaroni, F. Forastiere, M. Stafoggia, Z.J. Andersen, C. Badaloni, R. Beelen, B. Caracciolo, U. de Faire, R. Erbel, K.T. Eriksen, L. Fratiglioni, C. Galassi, R. Hampel, M. Heier, F. Hennig, A. Hilding, B. Hoffmann, D. Houthuijs, K.-H. Jöckel, M. Korek, A. Peters, Long term exposure to ambient air pollution and incidence of acute coronary events: prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project., BMJ. 348 (2014) f7412. [CrossRef]
- Raaschou-Nielsen, P. Vineis, B. Brunekreef, M. Nieuwenhuijsen, B. Hoffmann, F. Forastiere, A. Oudin, G. Hoek, K. Katsouyanni, P. Schwarze, R. Beelen, ESCAPE group, Air pollution and lung cancer in Europe - authors’ reply., Lancet Oncol. 14 (2013) e440. [CrossRef]
- Al-Rawas, A.A. Al-Maniri, B.M. Al-Riyami, Home exposure to Arabian incense (bakhour) and asthma symptoms in children: a community survey in two regions in Oman., BMC Pulm. Med. 9 (2009) 23. [CrossRef]
- H. Khreis, M. Cirach, N. Mueller, K. de Hoogh, G. Hoek, M.J. Nieuwenhuijsen, D. Rojas-Rueda, Outdoor air pollution and the burden of childhood asthma across Europe., Eur. Respir. J. 54 (2019). [CrossRef]
- Pierangeli, M.J. Nieuwenhuijsen, M. Cirach, D. Rojas-Rueda, Health equity and burden of childhood asthma - related to air pollution in Barcelona., Environ. Res. 186 (2020) 109067. [CrossRef]
- U. Gehring, A.H. Wijga, G.H. Koppelman, J.M. Vonk, H.A. Smit, B. Brunekreef, Air pollution and the development of asthma from birth until young adulthood., Eur. Respir. J. 56 (2020). [CrossRef]
- A.I. Tiotiu, P. Novakova, D. Nedeva, H.J. Chong-Neto, S. Novakova, P. Steiropoulos, K. Kowal, Impact of air pollution on asthma outcomes., Int. J. Environ. Res. Public Health. 17 (2020). [CrossRef]
- J.R. Balmes, M. Cisternas, P.J. Quinlan, L. Trupin, F.W. Lurmann, P.P. Katz, P.D. Blanc, Annual average ambient particulate matter exposure estimates, measured home particulate matter, and hair nicotine are associated with respiratory outcomes in adults with asthma., Environ. Res. 129 (2014) 1–10. [CrossRef]
- G. Moscato, C. Apfelbacher, K. Brockow, C. Eberle, J. Genuneit, C.G. Mortz, C. Quecchia, S. Quirce, A. Siracusa, S.M. Tarlo, V. van Kampen, J. Walusiak-Skorupa, M. Raulf, Gender and occupational allergy: Report from the task force of the EAACI Environmental and Occupational Allergy Interest Group., Allergy. 75 (2020) 2753–2763. [CrossRef]
- M. Kogevinas, J.-P. Zock, D. Jarvis, H. Kromhout, L. Lillienberg, E. Plana, K. Radon, K. Torén, A. Alliksoo, G. Benke, P.D. Blanc, A. Dahlman-Hoglund, A. D’Errico, M. Héry, S. Kennedy, N. Kunzli, B. Leynaert, M.C. Mirabelli, N. Muniozguren, D. Norbäck, J.M. Antó, Exposure to substances in the workplace and new-onset asthma: an international prospective population-based study (ECRHS-II)., Lancet. 370 (2007) 336–341. [CrossRef]
- H. Fuseini, D.C. Newcomb, Mechanisms driving gender differences in asthma., Curr. Allergy Asthma Rep. 17 (2017) 19. [CrossRef]
- G. Sit, N. Letellier, Y. Iwatsubo, M. Goldberg, B. Leynaert, R. Nadif, C. Ribet, N. Roche, Y. Roquelaure, R. Varraso, M. Zins, A. Descatha, N. Le Moual, O. Dumas, Occupational exposures to organic solvents and asthma symptoms in the CONSTANCES cohort., Int. J. Environ. Res. Public Health. 18 (2021). [CrossRef]
- P. Ilmarinen, L.E. Tuomisto, H. Kankaanranta, Phenotypes, Risk Factors, and Mechanisms of Adult-Onset Asthma., Mediators Inflamm. 2015 (2015) 514868. [CrossRef]
- R. Golden, Identifying an indoor air exposure limit for formaldehyde considering both irritation and cancer hazards., Crit. Rev. Toxicol. 41 (2011) 672–721. [CrossRef]
- D.J. Tan, E.H. Walters, J.L. Perret, J.A. Burgess, D.P. Johns, A.J. Lowe, C.J. Lodge, P. Hayati Rezvan, J.A. Simpson, S. Morrison, B.R. Thompson, P.S. Thomas, I. Feather, G.G. Giles, J.L. Hopper, M.J. Abramson, M.C. Matheson, S.C. Dharmage, Clinical and functional differences between early-onset and late-onset adult asthma: a population-based Tasmanian Longitudinal Health Study., Thorax. 71 (2016) 981–987. [CrossRef]
- G. Bowatte, B. Erbas, C.J. Lodge, L.D. Knibbs, L.C. Gurrin, G.B. Marks, P.S. Thomas, D.P. Johns, G.G. Giles, J. Hui, M. Dennekamp, J.L. Perret, M.J. Abramson, E.H. Walters, M.C. Matheson, S.C. Dharmage, Traffic-related air pollution exposure over a 5-year period is associated with increased risk of asthma and poor lung function in middle age., Eur. Respir. J. 50 (2017). [CrossRef]
- E. Rönmark, A. Lindberg, L. Watson, B. Lundbäck, Outcome and severity of adult onset asthma--report from the obstructive lung disease in northern Sweden studies (OLIN)., Respir. Med. 101 (2007) 2370–2377. [CrossRef]
- S. Bronnimann, B. Burrows, A prospective study of the natural history of asthma. Remission and relapse rates., Chest. 90 (1986) 480–484. [CrossRef]
- P. Maestrelli, Natural History of Adult-Onset Asthma, Am. J. Respir. Crit. Care Med. 169 (2004) 331–332. [CrossRef]
- G.A. Settipane, W.A. Greisner, R.J. Settipane, Natural history of asthma: a 23-year followup of college students., Ann. Allergy Asthma Immunol. 84 (2000) 499–503. [CrossRef]
- B.A. Bauer, C.E. Reed, J.W. Yunginger, P.C. Wollan, M.D. Silverstein, Incidence and outcomes of asthma in the elderly. A population-based study in Rochester, Minnesota., Chest. 111 (1997) 303–310. [CrossRef]
- C.E. Reed, The natural history of asthma in adults: the problem of irreversibility., J. Allergy Clin. Immunol. 103 (1999) 539–547. [CrossRef]
- M. Masoli, D. Fabian, S. Holt, R. Beasley, Global Initiative for Asthma (GINA) Program, The global burden of asthma: executive summary of the GINA Dissemination Committee report., Allergy. 59 (2004) 469–478. [CrossRef]
- Y. Feng, Y. Wang, C. Zeng, H. Mao, Artificial intelligence and machine learning in chronic airway diseases: focus on asthma and chronic obstructive pulmonary disease., Int. J. Med. Sci. 18 (2021) 2871–2889. [CrossRef]
- X. Li, S. Huang, A. Jiao, X. Yang, J. Yun, Y. Wang, X. Xue, Y. Chu, F. Liu, Y. Liu, M. Ren, X. Chen, N. Li, Y. Lu, Z. Mao, L. Tian, H. Xiang, Association between ambient fine particulate matter and preterm birth or term low birth weight: An updated systematic review and meta-analysis., Environ. Pollut. 227 (2017) 596–605. [CrossRef]
- W.-C. Ho, W.R. Hartley, L. Myers, M.-H. Lin, Y.-S. Lin, C.-H. Lien, R.-S. Lin, Air pollution, weather, and associated risk factors related to asthma prevalence and attack rate., Environ. Res. 104 (2007) 402–409. [CrossRef]
Figure 1.
Asthma severity percentages in the population and gender distribution. Percentages (%) of patients by asthma severity level (Severe, Moderate, and Mild) in all the population or clustered by gender.
Figure 1.
Asthma severity percentages in the population and gender distribution. Percentages (%) of patients by asthma severity level (Severe, Moderate, and Mild) in all the population or clustered by gender.
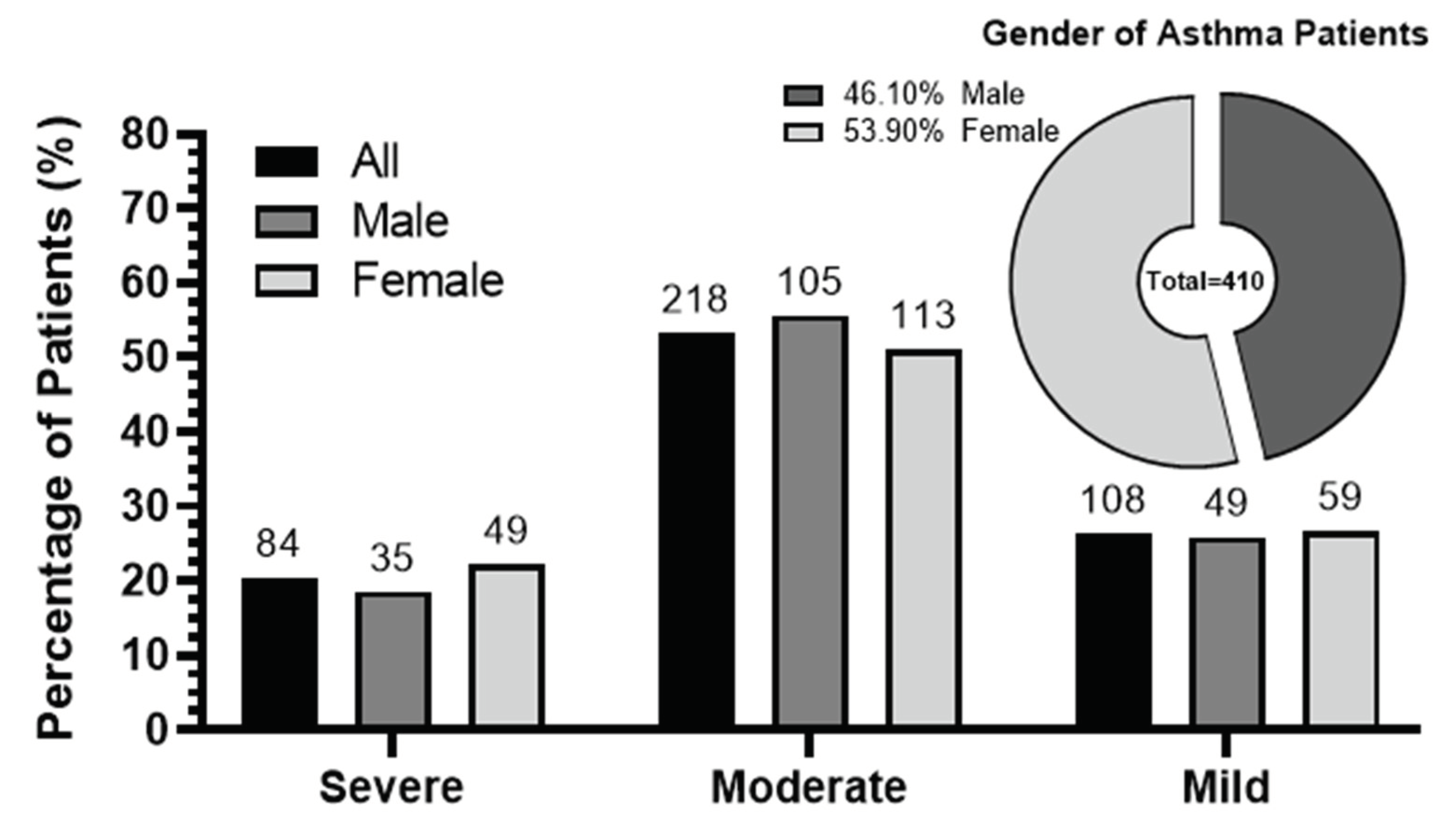
Figure 2.
The relationship between exposure zones and the average of asthma severity. The average of asthma severity of the studied population is depicted in relation to the exposure zones that were categorized as follow: High (<6 km), Middle (6-12 km), and Low (>12 km). To calculate the averages, asthma severity levels were represented by numerical values: Severe = 3, Moderate = 2, and Mild = 1. Error bars indicate the standard error of the means (SEM) and the number of patients is shown above each column. The average of distances (km) for the locations of these patients within each of the three exposure zones were shown.
Figure 2.
The relationship between exposure zones and the average of asthma severity. The average of asthma severity of the studied population is depicted in relation to the exposure zones that were categorized as follow: High (<6 km), Middle (6-12 km), and Low (>12 km). To calculate the averages, asthma severity levels were represented by numerical values: Severe = 3, Moderate = 2, and Mild = 1. Error bars indicate the standard error of the means (SEM) and the number of patients is shown above each column. The average of distances (km) for the locations of these patients within each of the three exposure zones were shown.
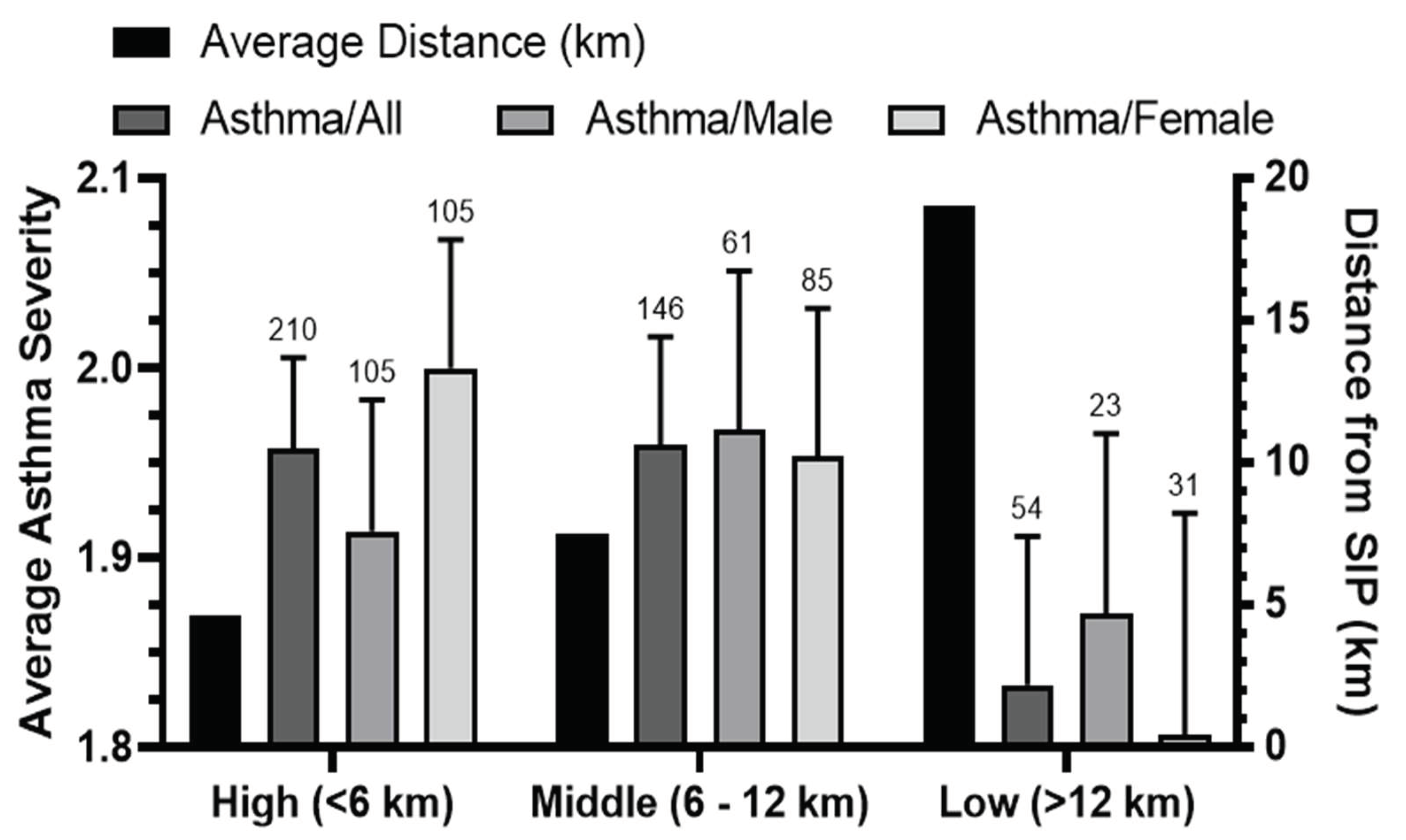
Figure 3.
The relationship between the severity of asthma and the average of distances of patients residences from SIP. Average of distances (km) was calculated for male, female, and all the population and categorized by different levels of asthma severity (Severe, Moderate/Mild) with SEM error bars. and the number of patients above each bar. The statistical differences were determined by Mann–Whitney U-test at P<0.05*.
Figure 3.
The relationship between the severity of asthma and the average of distances of patients residences from SIP. Average of distances (km) was calculated for male, female, and all the population and categorized by different levels of asthma severity (Severe, Moderate/Mild) with SEM error bars. and the number of patients above each bar. The statistical differences were determined by Mann–Whitney U-test at P<0.05*.
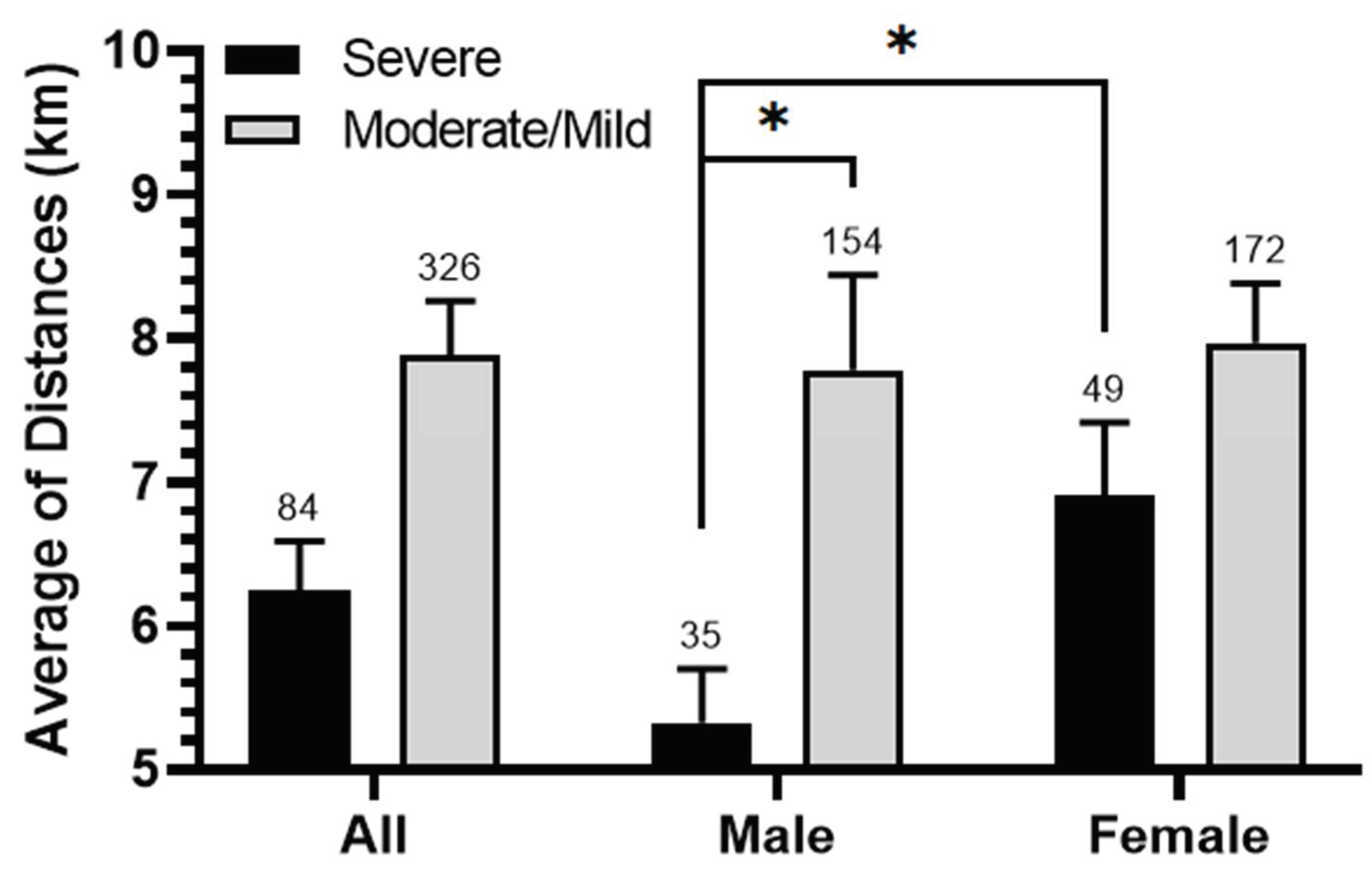
Figure 4.
Comprehensive map representing the dispersion of asthma patients around SIP. The map illustrates various regions where the patients reside. Each region is portrayed by a circle which size corresponds to either the total number of patients (A) or the percentage of severe asthma cases (B) within that particular region. Additionally, the map highlights the placement of Majan Industrial Area (MIA) and Sohar Industrial Zone (SIZ).
Figure 4.
Comprehensive map representing the dispersion of asthma patients around SIP. The map illustrates various regions where the patients reside. Each region is portrayed by a circle which size corresponds to either the total number of patients (A) or the percentage of severe asthma cases (B) within that particular region. Additionally, the map highlights the placement of Majan Industrial Area (MIA) and Sohar Industrial Zone (SIZ).
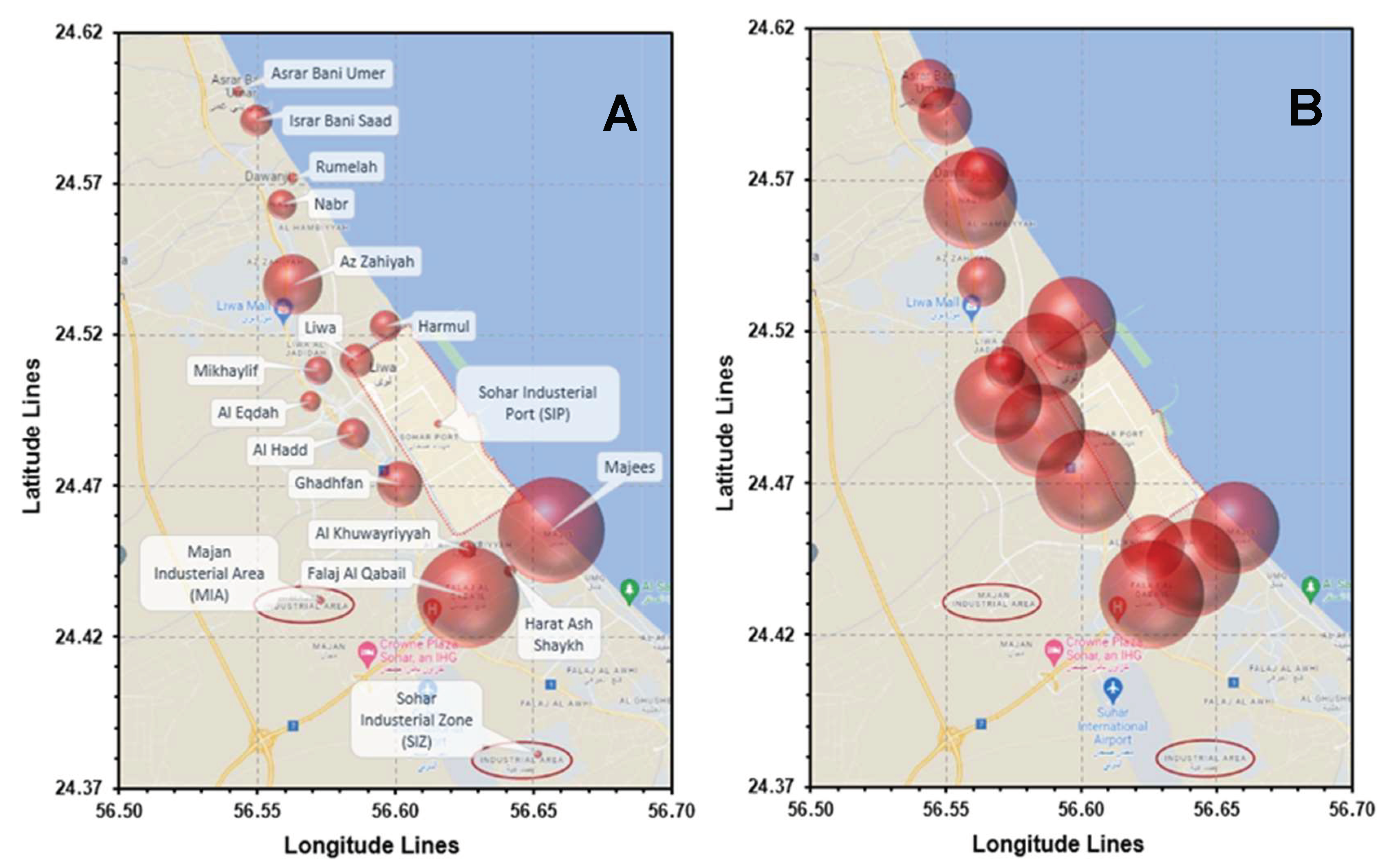
Figure 5.
The relationship between the age ranges and the average of asthma severity. Average of asthma severity (Severe = 3, Moderate = 2 and Mild = 1) was calculated in the studied population (All, Male and Female) in two location conditions (total and high exposure zone <6 Km from SIP) after clustering according to ages (<25, 25-50 and >50 years). Error bars represent the standard error of the means (SEM) and numbers of patients in each group are shown above the bars. The significance of the differences is determined by Mann–Whitney U-test at P<0.05* and P<0.005**.
Figure 5.
The relationship between the age ranges and the average of asthma severity. Average of asthma severity (Severe = 3, Moderate = 2 and Mild = 1) was calculated in the studied population (All, Male and Female) in two location conditions (total and high exposure zone <6 Km from SIP) after clustering according to ages (<25, 25-50 and >50 years). Error bars represent the standard error of the means (SEM) and numbers of patients in each group are shown above the bars. The significance of the differences is determined by Mann–Whitney U-test at P<0.05* and P<0.005**.
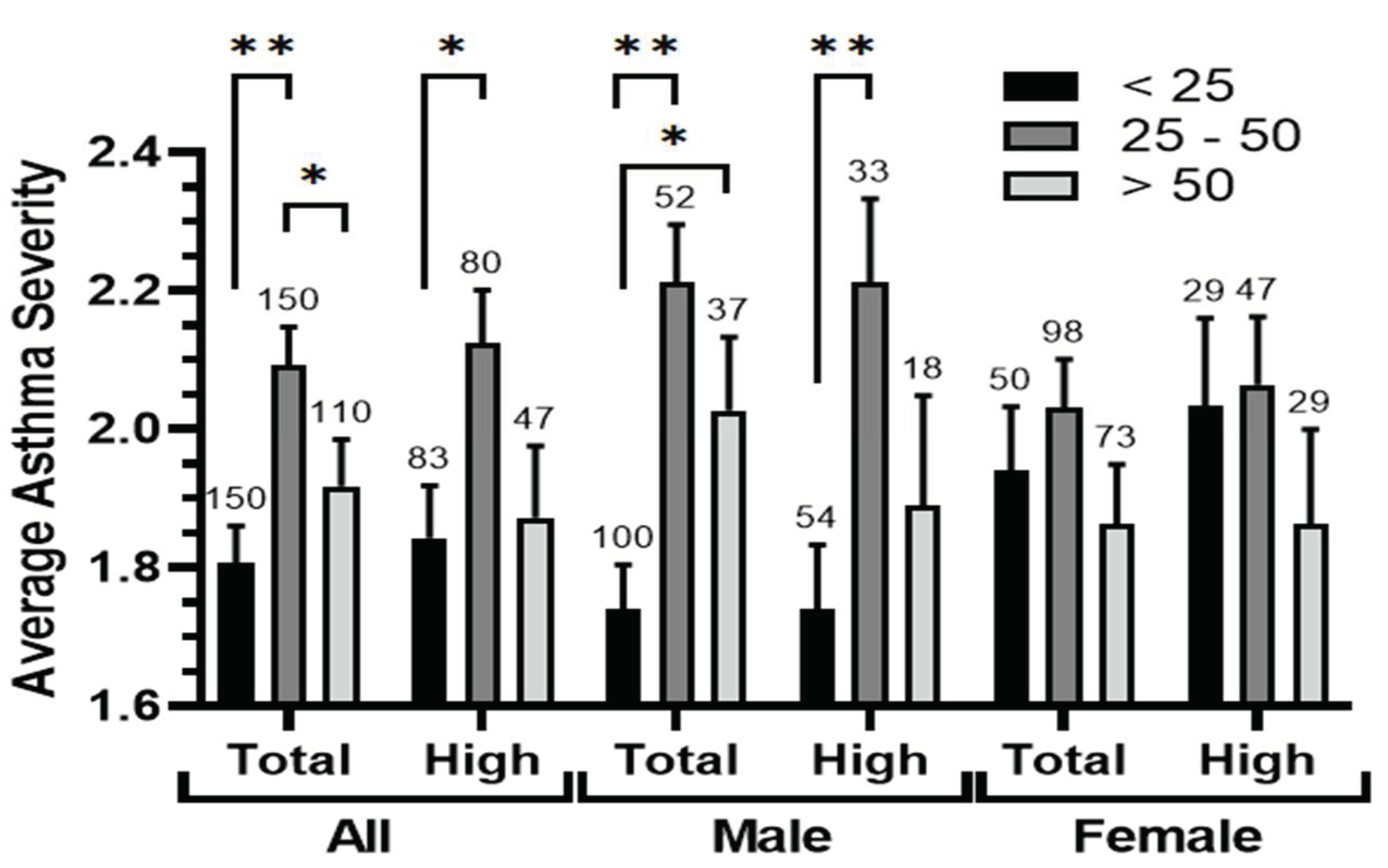
Figure 6.
The relationship between Asthma types and the average of patients ages. Average of patients ages in the studied population (All, Male and Female) in two locations (total and high exposure zone <6 km from SIP) clustered according to asthma level (severe, moderate and mild). Error bars represent the standard error of the means (SEM) and number of patients in each group are shown above the bars. The significance of the differences is determined by Mann–Whitney U-test at P<0.05* and P<0.005**.
Figure 6.
The relationship between Asthma types and the average of patients ages. Average of patients ages in the studied population (All, Male and Female) in two locations (total and high exposure zone <6 km from SIP) clustered according to asthma level (severe, moderate and mild). Error bars represent the standard error of the means (SEM) and number of patients in each group are shown above the bars. The significance of the differences is determined by Mann–Whitney U-test at P<0.05* and P<0.005**.
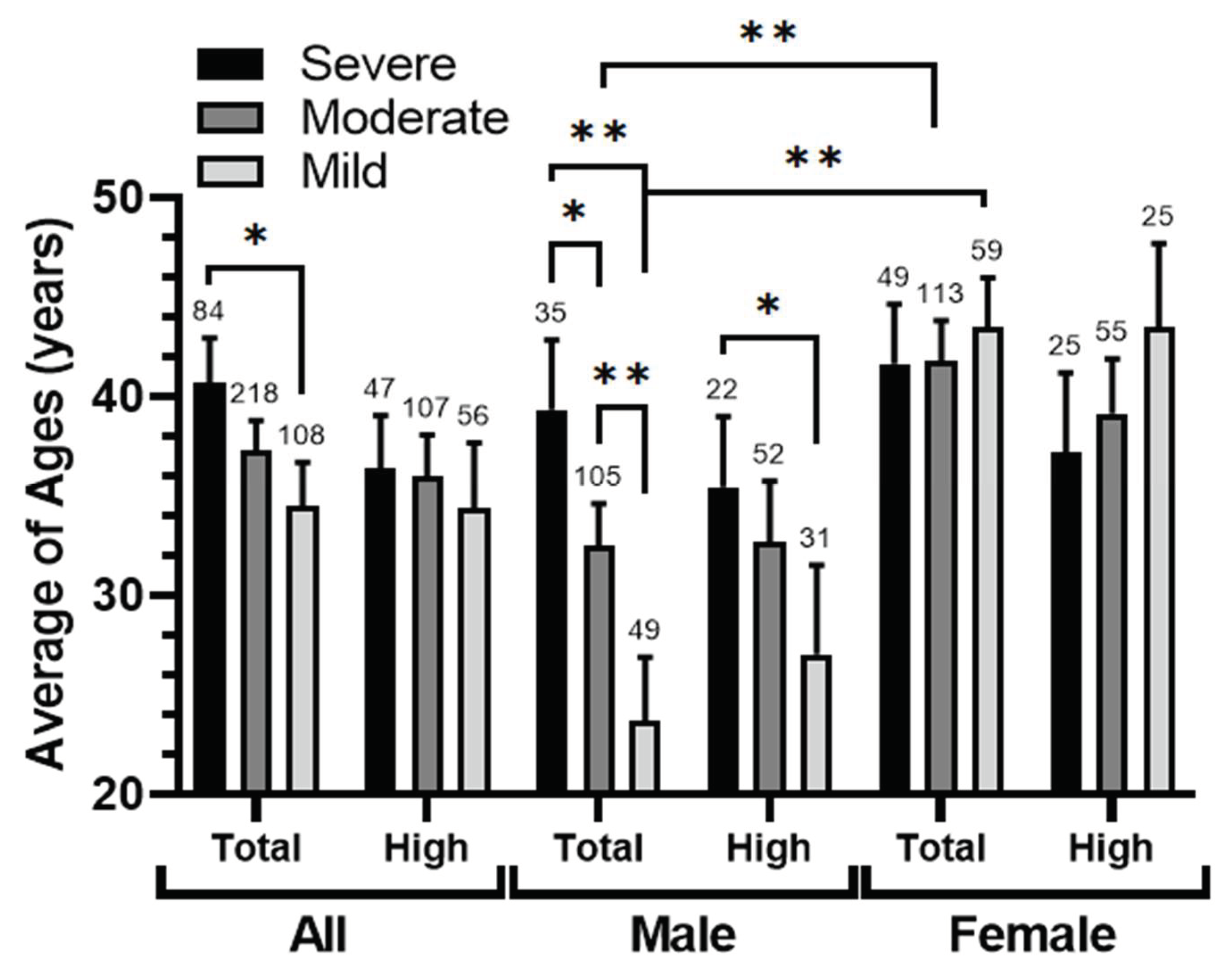
Figure 7.
The relationship between patients gender, smoking status, and the average of asthma severity. The average of asthma severity, categorized as severe (3), moderate (2), and mild (1), was calculated for male and female patients based on their smoking status: smokers, passive smokers, and non-smokers in the household. Error bars represent the standard error of the means (SEM), and the number of patients in each group is indicated above the respective bars.
Figure 7.
The relationship between patients gender, smoking status, and the average of asthma severity. The average of asthma severity, categorized as severe (3), moderate (2), and mild (1), was calculated for male and female patients based on their smoking status: smokers, passive smokers, and non-smokers in the household. Error bars represent the standard error of the means (SEM), and the number of patients in each group is indicated above the respective bars.
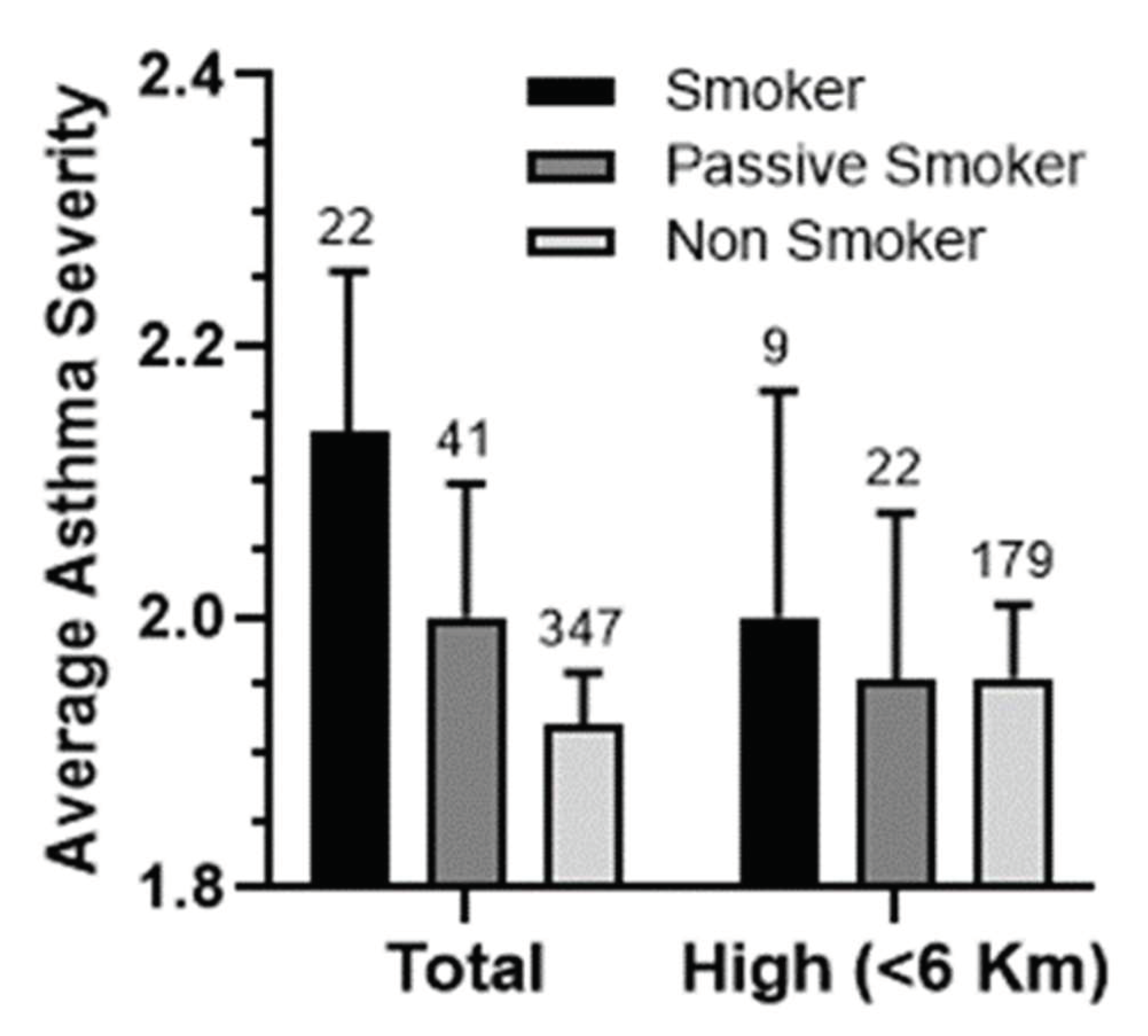
Figure 8.
Relationship Between Contaminant Exposure, Asthma, and Port Proximity. Comparison of the percentages of “Yes” responses from the survey conducted on exposure to contaminants, particularly dust, incense, perfume, and smoke. It explores the link between these percentages, gender (males and females), and their correlation with the severity of asthma and proximity to the port. The analysis is conducted for three groups: all patients (A), those with severe asthma (B), and those with severe asthma living within a 6-kilometer radius of the port (C).
Figure 8.
Relationship Between Contaminant Exposure, Asthma, and Port Proximity. Comparison of the percentages of “Yes” responses from the survey conducted on exposure to contaminants, particularly dust, incense, perfume, and smoke. It explores the link between these percentages, gender (males and females), and their correlation with the severity of asthma and proximity to the port. The analysis is conducted for three groups: all patients (A), those with severe asthma (B), and those with severe asthma living within a 6-kilometer radius of the port (C).
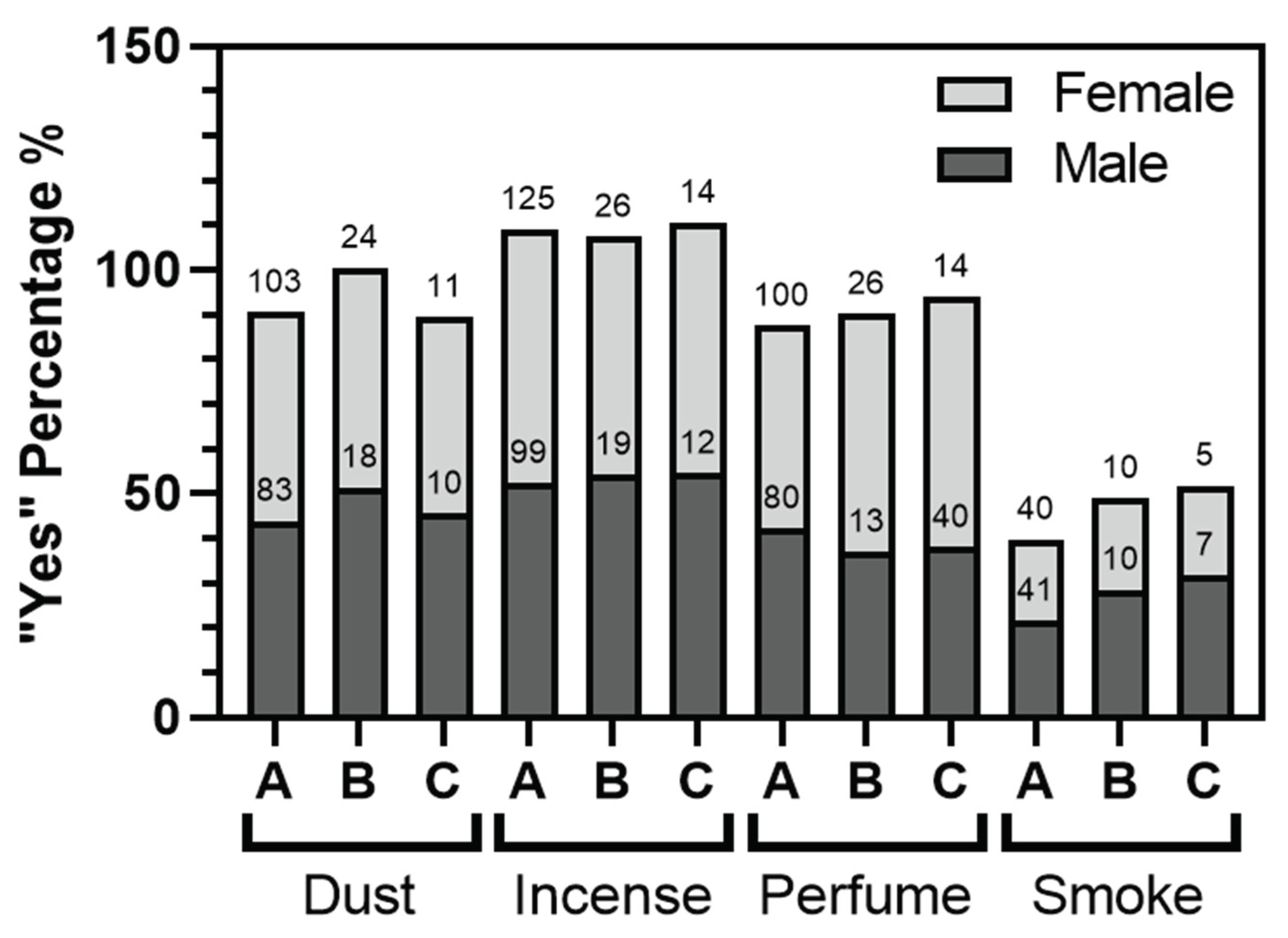
Figure 9.
Multilayer Perceptron – Architecture of Neural Network.
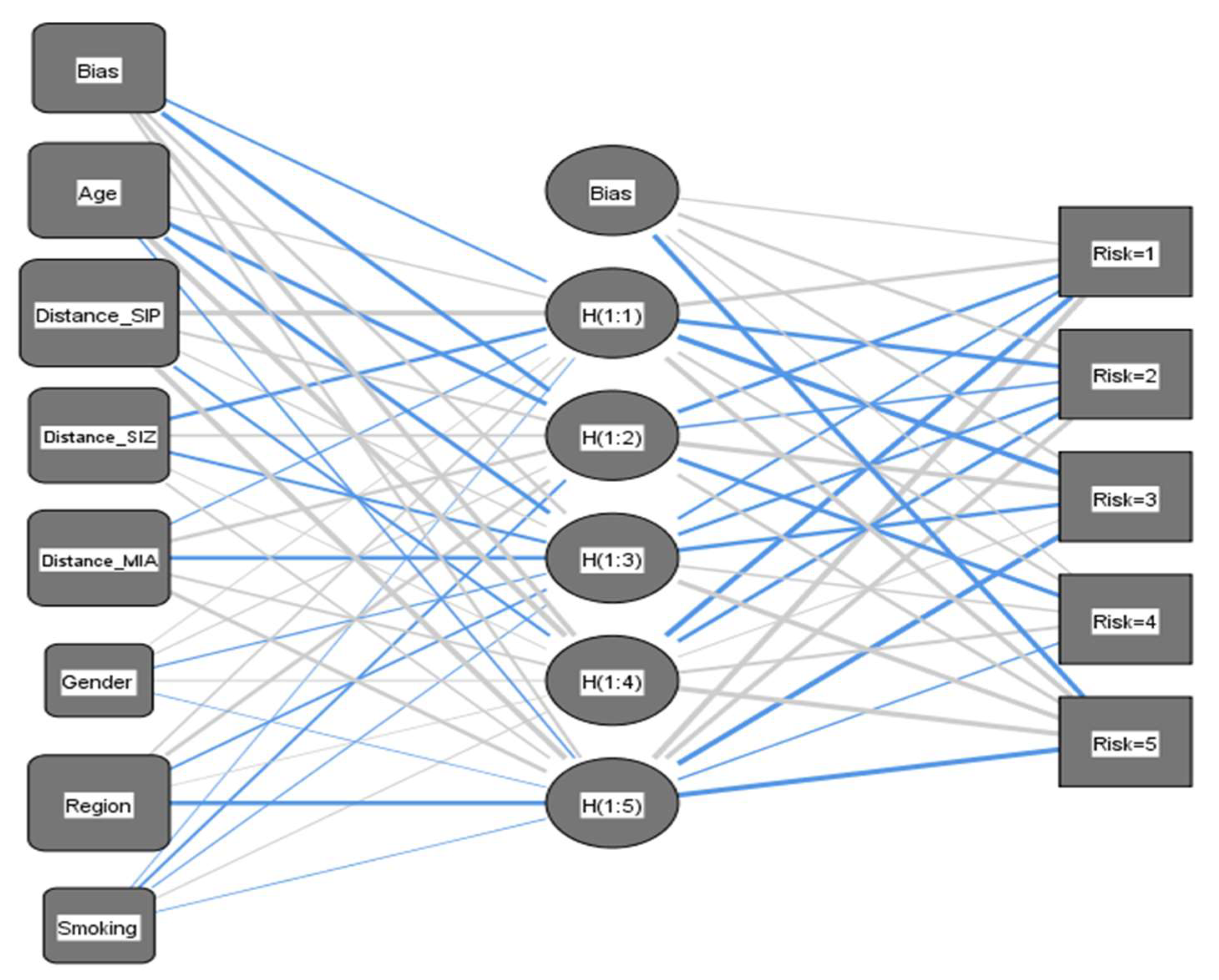
Figure 10.
Normalized Importance Analysis of Input Vectors. Normalized importance analysis of each predictor variable. The inset table provides a comprehensive overview of the importance and corresponding normalized importance values for different indicators.
Figure 10.
Normalized Importance Analysis of Input Vectors. Normalized importance analysis of each predictor variable. The inset table provides a comprehensive overview of the importance and corresponding normalized importance values for different indicators.
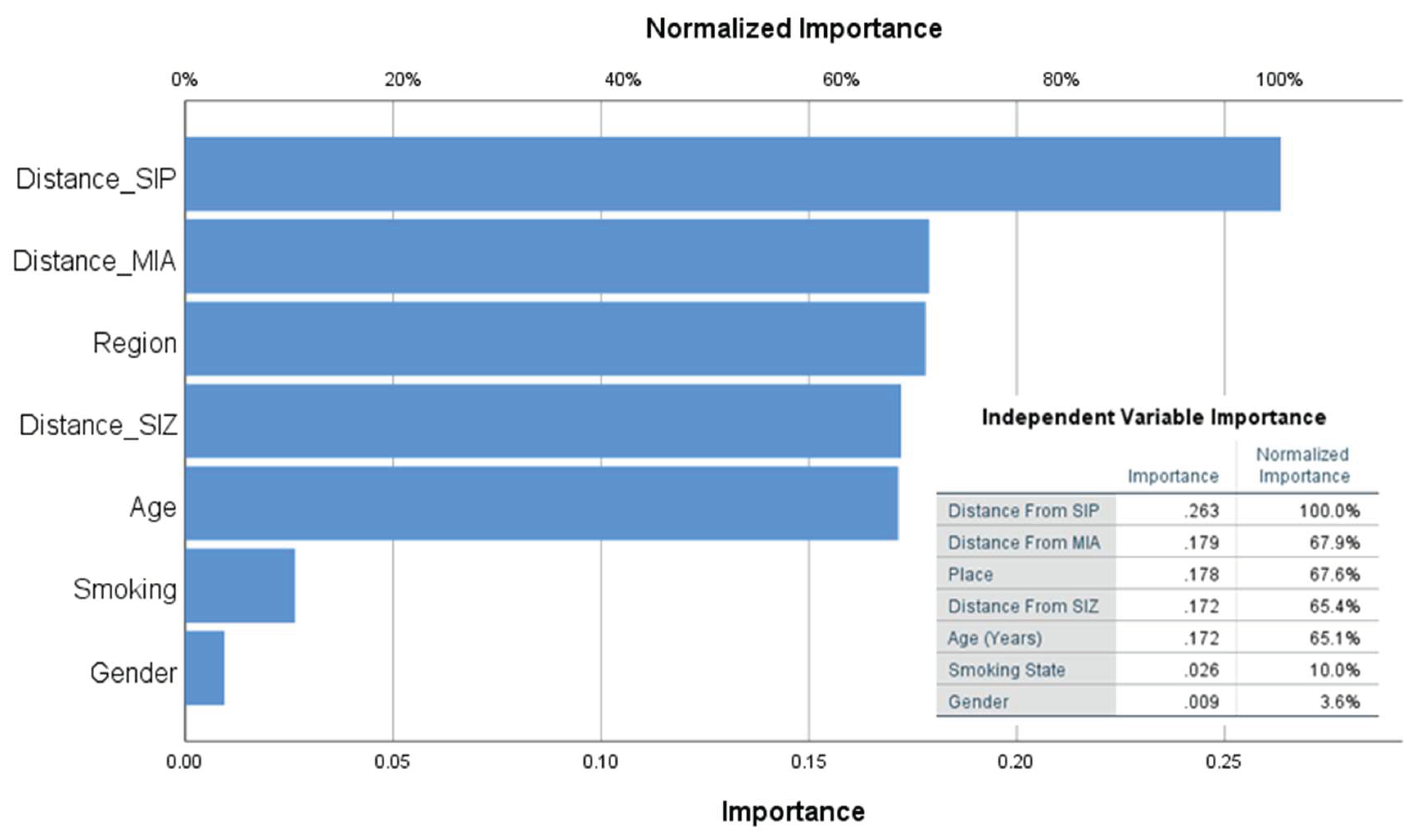

Table 1.
Descriptive statistics of the relationship between exposure zones and asthma severity. Characteristics of asthma severity levels (severe, moderate, and mild) in the studied population across exposure zones near SIP. Cases numbers and their percentages among asthma severity levels and among different exposure zones are shown.
Table 1.
Descriptive statistics of the relationship between exposure zones and asthma severity. Characteristics of asthma severity levels (severe, moderate, and mild) in the studied population across exposure zones near SIP. Cases numbers and their percentages among asthma severity levels and among different exposure zones are shown.
| Exposure Zone | Total | Severe | Moderate | Mild | |
|---|---|---|---|---|---|
| (Exposure Zones %) | Cases Number (Asthma severity % - Exposure zones %) |
||||
| All | High (<6 km) | 210 (51.2%) |
56 (26.7%-51.9%) |
107 (51%-49.1%) |
47 (22.4%-56%) |
| Middle (6 - 12 km) | 146 (35.6%) |
38 (26%-35.2%) |
76 (52.1%-34.9%) |
32 (21.9%-38.1%) |
|
| Low (>12 km) | 54 (13.2%) |
14 (25.9%-13%) |
35 (64.8%-16.1%) |
5 (9.3%-6%) |
|
| Male | High (<6 km) | 105 (55.6%) |
31 (29.5%-63.3%) |
52 (49.5%-49.5%) |
22 (21%-62.9%) |
| Middle (6 - 12 km) | 61 (32.3%) |
14 (23%-28.6%) |
35 (57.4%-33.3%) |
12 (19.7%-34.3%) |
|
| Low (>12 km) | 23 (12.2%) |
4 (17.4%-8.2%) |
18 (78.3%-17.1%) |
1 (4.3%-2.9%) |
|
| Female | High (<6 km) | 105 (47.5%) |
25 (23.8%-42.4%) |
55 (52.4%-48.7%) |
25 (23.8%-51%) |
| Middle (6 - 12 km) | 85 (38.5%) |
24 (28.2%-40.7%) |
41 (48.2%-36.3%) |
20 (23.5%-40.8%) |
|
| Low (>12 km) | 31 (14%) |
10 (32.3%-16.9%) |
17 (54.8%-15%) |
4 (12.9%-8.2%) |
|
Table 2.
The association between severe asthma cases and different industrial zones in the north of Sohar city. Asthma patients were categorized into three exposure zones based on their proximity to the pollution areas: Sohar Industrial Port (SIP), Sohar Industrial Zone (SIZ), and Majan Industrial Area (MIA). A control area (CA) was selected as a reference group. The table displays estimated risk ratios (RR) with confidence intervals (CI95%) and Chi-square test values (X2) for the high exposure zone, comparing the development of severe asthma symptoms to patients with moderate and mild asthma in the low exposure zone. The total number of cases and the number of cases compared between the different industrial zones are shown.
Table 2.
The association between severe asthma cases and different industrial zones in the north of Sohar city. Asthma patients were categorized into three exposure zones based on their proximity to the pollution areas: Sohar Industrial Port (SIP), Sohar Industrial Zone (SIZ), and Majan Industrial Area (MIA). A control area (CA) was selected as a reference group. The table displays estimated risk ratios (RR) with confidence intervals (CI95%) and Chi-square test values (X2) for the high exposure zone, comparing the development of severe asthma symptoms to patients with moderate and mild asthma in the low exposure zone. The total number of cases and the number of cases compared between the different industrial zones are shown.
| Valid Samples | High | Low | Severe Asthma (High/Low) | Moderate & Mild Asthma (High/Low) | RR (CI95%) | X2 | |
|---|---|---|---|---|---|---|---|
| SIP | 264 | <6 km | >12 km | 47/5 | 163/49 | 2.42 (1.01-5.78) | 0.031* |
| SIZ | 264 | <10 km | >20 km | 40/11 | 122/64 | 1.68 (0.92-3.09) | 0.081 |
| MIA | 176 | <6 km | >12 km | 27/11 | 72/66 | 1.91 (1.01-3.6) | 0.038* |
| CA | 323 | <8 km | >12 km | 25/41 | 118/139 | 0.77 (0.49-1.2) | 0.241 |
| SIP-North | 223 | Middle | North | 23/20 | 82/98 | 1.29 (0.75-2.21) | 0.349 |
| SIP-South | 269 | Middle | South | 23/40 | 82/124 | 0.9 (0.57-1.41) | 0.639 |
Table 3.
Risk ratios of different regions for developing severe asthma symptoms. The table preScheme 95. and Chi-square test values (X2) for various regions in relation to the development of severe asthma symptoms compared to patients with combined moderate and mild asthma in control regions (>12 Km) from SIP. The distances from SIP, SIZ, and MIA, as well as the number of cases (N) for each region.
Table 3.
Risk ratios of different regions for developing severe asthma symptoms. The table preScheme 95. and Chi-square test values (X2) for various regions in relation to the development of severe asthma symptoms compared to patients with combined moderate and mild asthma in control regions (>12 Km) from SIP. The distances from SIP, SIZ, and MIA, as well as the number of cases (N) for each region.
| Distance From SIP (km) | Distance From SIZ (km) | Distance From MIA (km) | Total N. | Severe Asthma N. | Moderate&Mild Asthma N. | Severe Asthma % | Latitude | Longitude | RR (CI95%) | χ2 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Ghadhfan | 2.6 | 11.3 | 5.3 | 30 | 8 | 22 | 27% | 24.471 | 56.602 | 2.88 (1.03-8.02) | 0.035* |
| Al Hadd | 3.4 | 13.8 | 6.2 | 21 | 5 | 16 | 24% | 24.487 | 56.585 | 2.57 (0.83-7.98) | 0.10 |
| Liwa | 4.0 | 16.0 | 8.8 | 22 | 5 | 17 | 23% | 24.512 | 56.586 | 2.45 (0.79-7.65) | 0.12 |
| Harmul | 4.1 | 16.7 | 10.3 | 21 | 5 | 16 | 24% | 24.523 | 56.596 | 2.57 (0.83-7.98) | 0.10 |
| Al Khuwayriyyah | 4.7 | 8.0 | 6.1 | 12 | 2 | 10 | 17% | 24.449 | 56.626 | 1.8 (0.4-8.2) | 0.45 |
| Al Eqdah | 5.1 | 15.7 | 7.2 | 13 | 3 | 10 | 23% | 24.498 | 56.569 | 2.49 (0.68-9.12) | 0.17 |
| Mikhaylif | 5.1 | 16.5 | 8.4 | 19 | 2 | 17 | 11% | 24.508 | 56.572 | 1.14 (0.24-5.38) | 0.87 |
| Majees | 6.0 | 8.2 | 9.6 | 72 | 17 | 55 | 24% | 24.455 | 56.657 | 2.55 (1-6.48) | 0.036* |
| Harat Ash Shaykh | 6.1 | 6.8 | 7.6 | 8 | 2 | 6 | 25% | 24.442 | 56.641 | 2.7 (0.63-11.65) | 0.19 |
| Falaj Al Qabail | 6.4 | 6.4 | 5.9 | 69 | 19 | 50 | 28% | 24.433 | 56.626 | 2.97 (1.19-7.45) | 0.011* |
| Az Zahiyah | 7.7 | 19.7 | 11.5 | 40 | 5 | 35 | 13% | 24.537 | 56.563 | 1.35 (0.42-4.35) | 0.61 |
| Nabr | 10.1 | 22.5 | 14.5 | 20 | 5 | 15 | 25% | 24.563 | 56.559 | 2.7 (0.87-8.35) | 0.08 |
| Rumelah | 10.7 | 23.1 | 15.4 | 7 | 1 | 6 | 14% | 24.572 | 56.563 | 1.54 (0.21-11.37) | 0.67 |
| Control | 19.0 | 26.0 | 18.8 | 54 | 5 | 49 | 9% | 24.505 | 56.499 | - | - |
Table 4.
Descriptive statistics of the relationship between patients ages and asthma severity. Distribution of asthma patients from the different types (severe, moderate and mild) on three Age ranges (<25, 25-50 and >50) in male and female patients in total compared to high exposure zone (<6 km from SIP). Estimated risk ratios (RR) with confidence intervals (CI95%) and Chi-square test values (X2) of the higher age ranges (25-50 and >50) to develop severe asthma symptoms compared to lower age range (<25) with combined asthma (moderate & mild).
Table 4.
Descriptive statistics of the relationship between patients ages and asthma severity. Distribution of asthma patients from the different types (severe, moderate and mild) on three Age ranges (<25, 25-50 and >50) in male and female patients in total compared to high exposure zone (<6 km from SIP). Estimated risk ratios (RR) with confidence intervals (CI95%) and Chi-square test values (X2) of the higher age ranges (25-50 and >50) to develop severe asthma symptoms compared to lower age range (<25) with combined asthma (moderate & mild).
| Exposure Zone | Age Range | Total | Severe | Moderate | Mild | All | Male | Female | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age ranges (%) |
Cases Number (Asthma severity % - Age range %) |
RR (CI95%) |
χ2 | RR (CI95%) |
χ2 | RR (CI95%) |
χ2 | ||||
| Total | < 25 | 150 (36.6%) |
20 (13.3%-23.8%) |
81 (54%-37.2%) |
49 (32.7%-45.4%) |
- | - | - | - | - | - |
| 25 - 50 | 150 (36.6%) |
41 (27.3%-48.8%) |
82 (54.7%-37.6%) |
27 (18%-25%) |
2.05 (1.26-3.33) |
0.003* | 2.8 (1.4-5.58) |
0.002* | 1.417 (0.72-2.80) |
0.304 | |
| > 50 | 110 (26.8%) |
23 (20.9%-27.4%) |
55 (50%-25.2%) |
32 (29.1%-29.6%) |
1.57 (0.91-2.71) |
0.104 | 1.97 (0.86-4.5) |
0.11 | 1.14 (0.54-2.4) |
0.727 | |
|
High <6 Km from SIP |
< 25 | 83 (39.5%) |
14 (16.9%-29.8%) |
42 (50.6%-39.3%) |
27 (32.5%-48.2%) |
- | - | - | - | - | - |
| 25 - 50 | 80 (38.1%) |
24 (30%-51.1%) |
42 (52.5%-39.3%) |
14 (17.5%-25%) |
1.78 (0.99-3.19) |
0.047* | 2.81 (1.23-6.4) |
0.1 | 1.058 (0.47-2.38) |
0.892 | |
| > 50 | 47 (22.4%) |
9 (19.1%-19.1%) |
23 (48.9%-21.5%) |
15 (31.9%-26.8%) |
1.14 (0.53-2.42) |
0.743 | 1.286 (0.37-4.46) |
0.694 | 0.857 (0.33-2.24) |
0.753 | |
Table 5.
The link between the patients smoking state and asthma severity. Descriptive statistics of the smoking status (Smoker, passive smoker and non-smoker) in male and female patients in total compared to the high exposure zone (<6 km from SIP) and the relationship with the asthma severity levels (severe, moderate and mild, *) are shown. Estimated risk ratios (RR) with confidence intervals (CI95%) and Chi-square test values (X2) of the different smoking states (Smokers and Passive smokers) to develop severe asthma symptoms compared to non smoker patients with mild or with combined asthma (moderate & mild, **) are also presented.
Table 5.
The link between the patients smoking state and asthma severity. Descriptive statistics of the smoking status (Smoker, passive smoker and non-smoker) in male and female patients in total compared to the high exposure zone (<6 km from SIP) and the relationship with the asthma severity levels (severe, moderate and mild, *) are shown. Estimated risk ratios (RR) with confidence intervals (CI95%) and Chi-square test values (X2) of the different smoking states (Smokers and Passive smokers) to develop severe asthma symptoms compared to non smoker patients with mild or with combined asthma (moderate & mild, **) are also presented.
| Exposure Zone | Smoking State | All | Male/Female | Severe* | Moderate* | Mild* | Severe/Mild | Severe/Comb** | ||
|---|---|---|---|---|---|---|---|---|---|---|
| (Smoking groups %) | Cases Number (Asthma severity % - Smoking groups %) |
RR (CI 95%) |
χ2 | RR (CI 95%) |
χ2 | |||||
| Total | Non Smoker | 347 (84.6%) |
155/192 (82.0%-86.9%) |
71 (20.5%-84.5%) |
178 (51.3%-81.6%) |
98 (28.2%-90.7%) |
- | - | - | - |
| Smoker | 22 (5.4%) |
19/3 (10.1%-1.4%) |
5 (22.7%-5.9%) |
15 (68.2%-6.9%) |
2 (9.1%-1.8%) |
1.7 (1.03-2.81) |
0.12 | 1.11 (0.5-2.47) |
0.80 | |
| Passive Smoker | 41 (10%) |
15/26 (7.9%-11.8%) |
8 (19.5%-9.5%) |
25 (61%-11.5%) |
8 (19.5%-7.4%) |
1.19 (0.71-2) |
0.54 | 0.95 (0.5-1.84) |
0.89 | |
|
High <6 Km from SIP |
Non Smoker | 179 (85.2%) |
89/90 (84.8%-85.7%) |
43 (24%-91.5%) |
85 (47.5%-79.4%) |
51 (28.5%-91.1%) |
- | - | - | - |
| Smoker | 9 (4.3%) |
8/1 (7.6%-1.0%) |
1 (11.1%-2.1%) |
7 (77.8%-6.5%) |
1 (11.1%-1.8%) |
1.09 (0.27-4.45) |
0.90 | 0.46 (0.07-2.99) |
0.37 | |
| Passive Smoker | 22 (10.5%) |
8/14 (7.6%-13.3%) |
3 (13.6%-6.4%) |
15 (68.2%-14%) |
4 (18.2%-7.1%) |
0.94 (0.39-2.27) |
0.88 | 0.57 (0.19-1.68) |
0.27 | |
Table 6.
Relationship between exposure to contaminants and asthma severity. Descriptive statistics regarding the levels of exposure to various contaminants and their corresponding asthma severity levels. The table provides estimated risk ratios (RR) with confidence intervals (CI95%) and Chi-square test values (X2) to evaluate the risk of patients developing severe asthma symptoms when exposed to different contaminants (dust, incense, perfume, and smoke) compared to non-exposed patients with a combined asthma (moderate and mild). The analysis is conducted for both the entire study area and a high exposure zone within a radius of less than 6 km from the port.
Table 6.
Relationship between exposure to contaminants and asthma severity. Descriptive statistics regarding the levels of exposure to various contaminants and their corresponding asthma severity levels. The table provides estimated risk ratios (RR) with confidence intervals (CI95%) and Chi-square test values (X2) to evaluate the risk of patients developing severe asthma symptoms when exposed to different contaminants (dust, incense, perfume, and smoke) compared to non-exposed patients with a combined asthma (moderate and mild). The analysis is conducted for both the entire study area and a high exposure zone within a radius of less than 6 km from the port.
| Contaminants | Respondent N | Respondent % | Responses % | Severe Asthma % | Severe Asthma Y/N | Comb Asthma Y/N | Total | High (<6 Km) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| RR (CI95%) |
χ2 | RR (CI95%) |
χ2 | |||||||
| Yes | 281 | 68.5% | - | 19.2% | 54 | 227 | 0.83 (0.56-1.23) |
0.347 | 0.76 (0.45-1.28) |
0.303 |
| Uncertain | 129 | 31.5% | - | 23.3% | 30 | 99 | - | - | - | - |
| Dust | 186 | 67.9% | 27.7% | 22.6% | 42/42 | 144/182 | 1.2 (0.82-1.76) |
0.339 | 1.02 (0.61-1.69) |
0.951 |
| Incense | 224 | 81.8% | 33.4% | 20.1% | 45/39 | 179/147 | 0.96 (0.65-1.4) |
0.826 | 1 (0.6-1.67) |
0.99 |
| Perfume | 180 | 65.7% | 26.8% | 21.7% | 39/45 | 141/185 | 1.11 (0.76-1.62) |
0.601 | 1.21 (0.73-2.01) |
0.457 |
| Smoke | 81 | 29.6% | 12.1% | 24.7% | 20/64 | 61/265 | 1.27 (0.82-1.97) |
0.295 | 1.41 (0.81-2.47) |
0.238 |
| Total Respondent | 274 | 100.0% | - | 19.3% | 53 | 221 | - | - | - | - |
| Total Responses | 671 | - | 100.0% | 21.8% | 146 | 525 | - | - | - | - |
Table 7.
Classification of percentage of prediction. The actual and expected number of samples based on the model, as well as the percentages of the correct predictions for each level of risk. The data is reported separately for the training and testing phases of constructing the neural network.
Table 7.
Classification of percentage of prediction. The actual and expected number of samples based on the model, as well as the percentages of the correct predictions for each level of risk. The data is reported separately for the training and testing phases of constructing the neural network.
|
|
Predicted | ||||||
|---|---|---|---|---|---|---|---|
| Very Low Risk | Low Risk | Average Risk | High Risk | Very High Risk | Percent Correct | ||
| Training | Very Low Risk | 47 | 1 | 0 | 0 | 0 | 97.9% |
| Low Risk | 1 | 59 | 4 | 0 | 0 | 92.2% | |
| Average Risk | 0 | 1 | 53 | 1 | 3 | 91.4% | |
| High Risk | 0 | 0 | 0 | 57 | 2 | 96.6% | |
| Very High Risk | 0 | 0 | 1 | 1 | 55 | 96.5% | |
| Overall Percent | 16.8% | 21.3% | 20.3% | 20.6% | 21.0% | 94.8% | |
| Testing | Very Low Risk | 29 | 0 | 0 | 0 | 0 | 100.0% |
| Low Risk | 1 | 24 | 1 | 1 | 1 | 88.9% | |
| Average Risk | 0 | 0 | 17 | 2 | 3 | 77.3% | |
| High Risk | 0 | 0 | 1 | 18 | 2 | 85.7% | |
| Very High Risk | 17.7 | 0 | 0 | 1 | 24 | 96.0% | |
| Overall Percent | 23.4% | 19.4% | 15.3% | 17.7% | 24.2% | 90.3% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



