
Submitted:
13 March 2024
Posted:
14 March 2024
You are already at the latest version
Abstract
The recent setbacks in the withdrawal and approval delays of antibody treatments of neurodegenerative disorders (NDs) can be attributed to their poor entry across the blood-brain barrier (BBB). While several invasive and noninvasive approaches can be used to make the BBB more permeable, their inconsistency makes them a poor choice; however, if an antibody is chemically modified to attach a transferrin molecule that enhances its permeation across the BBB, this could be the most practical and useful modification that can transform the science of ND treatment. Antibodies can be conjugated with transferrin in vitro, but preferably through mRNA, as we propose to convert current treatments to bring faster treatment options. The mRNA technology yields products at a meager cost, which is a consideration for the affordability of these drugs globally. This paper provides complete details with templates to convert the current medicines and those under development into mRNA delivery systems to ensure clinical success, avoiding the current failures in their efficacy, more specifically the products that have demonstrated efficacy but are being removed from the market.
Keywords:
mRNA
; antibodies
; nanobodies
; neurological diseases
; protein aggregates
; protein misfolding
Introduction
Neurodegenerative diseases (NDs) are complex disorders with multifactorial pathology that result in progressive damage to neuronal cells and loss of neuronal connectivity, ultimately leading to impaired mobility and/or cognition. Protein aggregation due to misfolding and oligomerization gives rise to extracellular or intracellular inclusions, a common hallmark for many NDs. Further spreading of these amyloid aggregates in the nervous system–like prion-based infections, hence a prion-like mechanism–is often considered a significant element in the etiology of NDs (1). In the past few decades, many of the genetic and biochemical causes underlying NDs associated with protein aggregation were uncovered, leading to the distinction between rarer familial forms, where disease-causing mutations are genetically inherited, and the more common sporadic forms, where genetic and environmental risk factors drive the pathogenesis (2). In both cases, the affected proteins are found enriched in pathological aggregates, highlighting their importance in the manifestation of the disease. However, despite the accumulated knowledge and the many clinical trials in which attempts were made to alleviate protein aggregation, no therapeutic strategy has been broadly accepted to cure any of the NDs. This led many scientists to question whether protein aggregation is central to ND etiology or a manifestation of other underlying causes (3, 4). Nonetheless, collectively, the work of the past decades generated a more complex understanding of how each aggregation-prone protein engages with many key cellular pathways. This review aims to provide an overview of these intricate connections by combining core findings and more recent discoveries.
For each ND, different sets of genes are typically found mutated in the familial forms, and different brain regions and cell types are initially affected. For example, Huntington’s disease (HD) and spinocerebellar ataxia type 1 (SCA1) are linked to the expansion of the CAG repeat of the huntingtin (HTT) and ataxin 1 (ATXN1) genes, respectively, resulting in proteins with an unusually long polyglutamine (polyQ) tract that is very prone to aggregation and causes intracellular deposits in striatal neurons (5, 6). In Alzheimer’s disease (AD), two different types of deposits are observed. The aberrant cleavage products of the transmembrane protein amyloid-β (Aβ) precursor protein (APP) form extracellular plaque deposits in the temporal and parietal brain regions. In contrast, the protein tau (MAPT) accumulates intracellularly in neurofibrillary tangles (7). In Parkinsonś disease (PD), the primarily affected brain area is the substantia nigra (SN), where α-synuclein (α-syn; SNCA) aggregates are found to accumulate in dopaminergic neurons (8). In ALS, cellular aggregates of superoxide dismutase 1 (SOD1), RNA-binding protein FUS (FUsed in Sarcoma), and TAR-DNA–binding protein 43 (TDP-43) have been identified in motor neurons of the primary motor cortex, brainstem, and spinal cord (9). Therefore, it is essential to consider each of these proteins independently and in the context of the most affected cells. Note, while we will mainly use short protein names in this review, whenever a gene is linked to ND, the corresponding italicized gene name will also be indicated in brackets if it differs from the protein name.
Protein misfolding and aggregation of disease-associated proteins are facilitated by mutations and post-translation modifications (e.g., phosphorylation and protein cleavage) that avert the formation of the native protein structure. At the same time, in some other cases, misfolding can also seemingly occur sporadically without a clear explanation. Aggregation is first typically initiated by a seed or/and an oligomer, in which sequence-specific elements of the misfolded protein interact to adopt a non-native conformation, which can then convert other proteins into the toxic form. In many cases, the oligomerization of misfolded proteins leads to the formation of amyloid fibrils with a distinctive β-sheet structure that arises when soluble oligomers assemble into small protofibrils (10). When more proteins are converted into non-native forms, these protofibrils become longer fibrils that can then form more extensive cellular inclusions visible by light microscopy. Recently, it has been proposed that oligomerization may be favored by liquid–liquid phase separation of aggregation-prone proteins (11). Moreover, it is evident that there are different polymorphs for most amyloid fibrils in vitro and in vivo (polymorph is a term used to indicate the capacity of a polypeptide to generate fibrils with different structures) (12, 13).
The protein fibrils formed would be expected to be removed by the autoimmune responses. Still, the less efficient production of antibodies in the brain must be supported by systemic entry of the blood-brain barrier (BBB) (14, 15) leading to extensive research and development of these therapies.
An emerging therapeutic strategy in neurodegenerative diseases where antibodies are designed to target and clear abnormal protein aggregates. Two such monoclonal antibodies (mAbs), aducanumab and lecanemab, have received accelerated approval from the US FDA for the treatment of AD (16, 17); however, aducanumab is discontinued effective 2024, without reasons and with the claim that it is not due to issues with safety or efficacy (18). Another monoclonal antibody, donanemab, was in the advanced stages of development for patients with early AD (19) but the FDA has delayed its approval, likely due to a lack of proof of efficacy (20). Another drug, Relyvrio (BIIB054 (Cinpanemab), for ALS is being recalled due to lack of efficacy (21, 22). The data reporting on clinicaltrials.gov shows that around 250 interventional studies treat NDs involving antibodies (23). However, the status of the failure of antibodies to provide a treatment solution for NDs requires rethinking whether an antibody alone can be effective in NDs without adding functions to promote their entry across the BBB.
The options available to enhance the entry of antibodies into the brain include invasive techniques, including intra-cerebral injection, convection-enhanced delivery, and intra-cerebroventricular infusion (24). The BBB can be disrupted using bradykinin analogs, ultrasonography, and osmotic pressure (25). Adding microbubbles makes these techniques more effective (26,27). Pharmacological techniques involve encapsulating medications into liposomes or chemically modifying pharmaceuticals to lipophilic molecules (28). Opsonization and drug delivery by nanoparticles across the blood-brain barrier, in which the drug is adsorbed onto the particles passively (29). Intranasal delivery routes can bypass the BBB, offering a direct path to the CNS (30). While all these approaches can be effective, none allow a consistent and predictable response, which is one reason why these approaches have not been used in developing antibodies against NDs.
Transcytosis
One approach, a physiological procedure of transporter-mediated delivery, receptor-mediated transcytosis, and adsorptive-mediated transcytosi,s (31) offers a viable choice if the transcytosis mechanism is made part of the drug structure. The transferrin receptor (TfR1) (32) can effectively transport therapeutic levels of antibodies across the BBB (33) by attaching them to transferrin or transferrin-mimicking peptides, thereby facilitating their crossing of the BBB (34,35). Another target is the insulin receptor (IR), which, like the TfR, can mediate the transport of antibodies across the BBB, offering a pathway for therapeutic intervention (36). So, theoretically, a conjugate of insulin and an antibody should enhance the entry of antibodies across the BBB, though no such studies have been reported. (Figure 1).
The low-density lipoprotein receptor-related protein-1 (LRP1) also serves as a conduit for the delivery of certain therapeutics into the brain, capitalizing on its role in transporting various molecules, including lipoproteins and amyloid-beta precursors (37). LRP1, involved in transporting various endogenous ligands, including apolipoprotein E-containing lipoproteins, has been identified as an alternative pathway for BBB crossing. This receptor participates in the clearance of amyloid-beta from the brain and has been implicated in the transport of other therapeutic agents (38).
The decision to use transferrin or LRP1 as a delivery mechanism would thus be based on the specific requirements of the therapeutic agent, including its size, required dosage, and targeted area within the brain (39).
The other two proteins, GLUT1 and P-glycoprotein (P-gp), have not been well studied or found effective. (40).
We select transferrin as the choice conjugate for antibodies to enhance their penetration through the BBB. Connecting an antibody to a transferrin protein requires meticulous bioconjugation techniques. The process starts with the purification and accurate quantification of both proteins to ensure the success of subsequent reactions (41). The transferrin protein undergoes chemical activation to introduce functional groups capable of forming stable bonds with the antibody. This step typically employs crosslinking agents that introduce reactive groups such as N-hydroxysuccinimide (NHS) esters or maleimide onto the transferrin. The conditions under which transferrin is activated—temperature, pH, and reaction time—are carefully controlled to preserve protein integrity and function. The antibody is then introduced to the activated transferrin under conditions favoring the coupling reaction between the functional groups of both proteins. Optimal conditions are maintained to facilitate effective conjugation while preserving the biological functions of each molecule. Post-reaction, the conjugation mixture necessitates purification to isolate the desired antibody-transferrin conjugate from unreacted components and by-products. Techniques such as dialysis, gel filtration chromatography, or affinity chromatography are commonly employed for this purpose, each selected based on the specific properties of the conjugate and the reagents used. Finally, the success and efficiency of the conjugation process are established using analytical techniques like SDS-PAGE, Western blotting, or mass spectrometry to verify the formation of the conjugate and assess its molecular weight and purity. The biological activity of the conjugate, particularly its target specificity and cell-binding efficiency, is then tested in relevant bioassays to ensure that the functionalities of both the antibody and transferrin have been retained post-conjugation. This meticulous validation ensures the final product is suitable for its intended diagnostic or therapeutic applications.
While the linker is desirable to remain intact through the BBB transport and then break off, the latter part may not be necessary if there is enough flexibility to enable the antibody to bind with protofibrils without interference with the transcytosis agent.
However, creating a flexible link to remove constraints is desirable so that both molecules can interact independently. These linkers can include polyethylene glycol (PEG) spacers, which not only increase the flexibility of the conjugate but also enhance its solubility and reduce immunogenicity. The flexibility provided by such linkers can be crucial for allowing the proteins to move and interact with their targets effectively (42).
mRNA-Based Transcytosis
Presently, antibodies to treat NDs are produced by recombinant process. The bioconjugation process then follows their production and purification. However, suppose an antibody is produced by in vivo translation using mRNA. In that case, the conjugation can be made using glycine-serine-rich linkers often used in fusion proteins to provide flexibility and distance between functional domains (43). The (Gly-Gly-Gly-Ser)n linkers provide highly flexible links to minimize interference with the biological activity of the linked domains (44). The elastin-like polypeptides (ELPs) provide elasticity and flexibility (45). The helix-forming linkers adopt a helical structure to bridge protein domains to provide a balance between flexibility and stability (46).
The mRNA technology is preferred for its faster and lower cost development and does not face the complexity of the upstream and downstream processes and post-translational modification consideration. The mRNA sequence can be synthesized by in vitro transcription (IVT) in a cell-free environment: a linearized, plasmid DNA molecule is combined with ribonucleotides in the presence of bacteriophage RNA polymerase (of which T7 is the most widely used); the polymerases then recognize the promoter region in the DNA template and synthesize the RNA transcripts in the presence of ribonucleotides (47,48).
The mRNA template used to deliver antibodies is shown in Table 1, wherein the antibody heavy and light chains are linked using the GGGS link, and the transferrin is connected. The final sequence of the mRNA is presented for the antibodies currently in use or waiting to enter the market. The presented method of manufacturing and delivering these antibodies can change the availability of many treatments for NDs, and at a low cost, a consideration that must be addressed as these treatments become available, given the widespread of NDs, particularly in the developing countries, where affordability remains a significant factor blocking the entry of newer drug therapies.
The amino acid chain is structured as follows: Transferrin (PO2787)-GSGSGSGS-Heavy chain-GSGSGSGS-light chain. It is reverse-translated and then converted to RNA to provide an ORF. Table 1 shows three prime products facing withdrawal or delayed approval due to lower efficacy against NDs.
The mRNA design is presented in Table 2, wherein inserting the ORF will give the full sequence required to translate the antibody conjugated with transferrin.
Regulatory
The products listed above and others under development to treat NDs have cost billions of dollars; therefore, the decisions made by the developers to discontinue the development or withdraw the products due to lack of anticipated efficacy will be challenging to consider the structural modifications and adopting the mRNA technology financially challenging. However, presented correctly, the cost of the proposed changes can be reasonable, using a regulatory plan based on the FDA's new guideline (49) that encourages innovative approaches that apply to the regulatory plan. For example, a conjugate of an antibody with transferrin will be a new BLA but not necessarily require all studies mandated for a new biological drug since the primary molecule remains the same; it can be presented as an alternate delivery system. The mRNA expression will be a new BLA, but the studies that take years to establish safety and efficacy can be substantially reduced.
To establish the proof of efficacy, we recommend taking a pharmacokinetic analysis based on a radioactive drug (50) in animal species; the process involves making the current product radioactive and conjugating it with transferrin in vitro and then comparing the radio image with the same molecule but without conjugation. These studies can be conducted without regulatory involvement within a very short time (51) and with almost negligible cost. Once the proof of concept is established, the regulatory agencies should be approached with a development plan that includes efficacy testing. However, these studies could be minimized by using a GASK-based presentation based on comparable animal studies.
This is a new step in evolving regulatory science. Still, it is in the best interest of the regulatory agencies as well to promote the entry of more effective antibodies that can treat NDs.
Conclusions
Therapeutic antibodies represent one of the fastest-growing segments in the pharmaceutical industry (52) expanding the scope to various antibody types, including nanobodies and Ab fragments, with optimized affinity, stability, and solubility (53).
NDs frequently involve disordered proteins that the inefficient immune system of the brain is not capable of removing, leading to scores of untreatable disorders. Much of current research is focused on designing antibodies, and a few have been approved, yet their use remains limited due to their poor entry into the brain, even as nanobodies. The effectiveness of these antibodies can be substantially higher if they are conjugated with transferrin protein as a choice modification to enhance their entry into the brain. Currently, the dose of antibodies entering the brain is less than 1%; thus, any change brought by improved transit across the brain will dramatically change their efficacy. In our opinion, this modification should be a standard approach for all future treatments since this provides a more reproducible means of promoting the entry of antibodies into the brain compared to dozens of other invasive and noninvasive techniques (54).
Current antibodies to treat NDs are manufactured using recombinant engineering. This technology transformed the field of biological drugs (55) but now, half a century later, we are ready to explore its transition to mRNA, letting the ribosome bioreactors in the body do the job of mechanical bioreactors. Additionally, a significant advantage of mRNA technology is its ability to translate conjugated molecules, as proposed in this paper, and multiple target products, leading to remarkable future technologies (56).
The advantages of mRNA over recombinant process are (57) well established; besides the safety of RNA products as they do not enter the nucleus, the benefit of developing these products at a fraction of the cost of developing recombinant products and with speed that had never been possible in any new drug development, we encourage future developments of biological drugs to focus on mRNA technology that is continually evolving, yet fully established as a viable option to recombinant engineering. While the safety and efficacy testing should never be comprised over the cost of development, having comparable or even better profiling of these products to become accessible to the developing world that is currently deprived of these products (58). The affordability issue becomes more dire when it comes to the treatment of NDs (59) where the treatment costs range into scores of thousands of dollars per year, clearly taking them out of the reach of most patients. Since the development of mRNA is fast and costs much less than recombinant production (60), we have estimated that per dose cost of goods should not be higher than one dollar (57,60,61), not counting the amortization of the development cost; but that too is much lower than the billions of dollars spent on recombinant drugs.
Funding
None.
Conflicts of Interest
The authors are developers of mRNA therapies as executives of RNA Therapeutics, Inc. USA. The mRNA sequence reported is part of several pending US patents held by the authors
Roles
SKN: concept, structure, research; MM: Research, review, and writing.
References
- Goedert M. NEURODEGENERATION. Alzheimer's and Parkinson's diseases: The prion concept in relation to assembled Aβ, tau, and α-synuclein. Science. 2015;349(6248):1255555. [CrossRef]
- Bertram, L.; Tanzi, R.E. The genetic epidemiology of neurodegenerative disease. J. Clin. Investig. 2005, 115, 1449–1457. [CrossRef]
- Walsh DM, Selkoe DJ. A critical appraisal of the pathogenic protein spread hypothesis of neurodegeneration. Nat Rev Neurosci. 2016;17(4):251-60. [CrossRef]
- Makin, S. The amyloid hypothesis on trial. Nature 2018, 559, S4–S7. [CrossRef]
- Ross CA, Tabrizi SJ. Huntington's disease: from molecular pathogenesis to clinical treatment. Lancet Neurol. 2011;10(1):83-98. [CrossRef]
- Orr, H.T.; Zoghbi, H.Y. SCA1 molecular genetics: a history of a 13 year collaboration against glutamines. Hum. Mol. Genet. 2001, 10, 2307–2311. [CrossRef]
- Selkoe DJ, Hardy J. The amyloid hypothesis of Alzheimer's disease at 25 years. EMBO Mol Med. 2016;8(6):595-608. [CrossRef]
- Poewe W, Seppi K, Tanner CM, Halliday GM, Brundin P, Volkmann J, et al. Parkinson disease. Nat Rev Dis Primers. 2017;3:17013. [CrossRef]
- Foerster, B.R.; Welsh, R.C.; Feldman, E.L. 25 years of neuroimaging in amyotrophic lateral sclerosis. Nat. Rev. Neurol. 2013, 9, 513–524. [CrossRef]
- Iadanza, M.G.; Jackson, M.P.; Hewitt, E.W.; Ranson, N.A.; Radford, S.E. A new era for understanding amyloid structures and disease. Nat. Rev. Mol. Cell Biol. 2018, 19, 755–773. [CrossRef]
- Mathieu, C.; Pappu, R.V.; Taylor, J.P. Beyond aggregation: Pathological phase transitions in neurodegenerative disease. Science 2020, 370, 56–60. [CrossRef]
- Petkova AT, Leapman RD, Guo Z, Yau WM, Mattson MP, Tycko R. Self-propagating, molecular-level polymorphism in Alzheimer's beta-amyloid fibrils. Science. 2005;307(5707):262-5. [CrossRef]
- Fitzpatrick, A.W.P.; Falcon, B.; He, S.; Murzin, A.G.; Murshudov, G.; Garringer, H.J.; Crowther, R.A.; Ghetti, B.; Goedert, M.; Scheres, S.H.W. Cryo-EM structures of tau filaments from Alzheimer’s disease. Nature 2017, 547, 185–190. [CrossRef]
- Kwon, D. Rogue antibodies involved in almost one-fifth of COVID deaths. Nature 2021, 597, 162–162. [CrossRef]
- Zakariya, S.M.; Zehra, A.; Khan, R.H. Biophysical Insight into Protein Folding, Aggregate Formation and its Inhibition Strategies. Protein Pept. Lett. 2022, 29, 22–36. [CrossRef]
- Cummings, J.; Osse, A.M.L.; Cammann, D.; Powell, J.; Chen, J. Anti-Amyloid Monoclonal Antibodies for the Treatment of Alzheimer’s Disease. BioDrugs 2023, 38, 5–22. [CrossRef]
- Cummings J. Anti-Amyloid Monoclonal Antibodies are Transformative Treatments that Redefine Alzheimer's Disease Therapeutics. Drugs. 2023;83(7):569-76. [CrossRef]
- Association As. Aducanumab to Be Discontinued as an Alzheimer’s Treatment https://www.alz.org/alzheimers-dementia/treatments/aducanumab2024 [.
- Mintun, M.A.; Lo, A.C.; Evans, C.D.; Wessels, A.M.; Ardayfio, P.A.; Andersen, S.W.; Shcherbinin, S.; Sparks, J.; Sims, J.R.; Brys, M.; et al. Donanemab in Early Alzheimer’s Disease. New Engl. J. Med. 2021, 384, 1691–1704. [CrossRef]
- Post W. FDA delays Alzheimer’s drug for further review in surprise move https://www.washingtonpost.com/business/2024/03/08/eli-lilly-alzheimers-donanemab-fda/2024 [.
- Times N. A.L.S. Drug Relyvrio Fails Clinical Trial and May Be Withdrawn From the Market https://www.nytimes.com/2024/03/08/health/als-drug-relyvrio.html2024 [.
- Today PsN. Biogen Discontinues Development of Cinpanemab https://parkinsonsnewstoday.com/news/biogen-announcement-discontinue-cinpanemab-parkinsons/2024 [.
- Clinicaltrials.gov. Alzheimer’s Disease Antibody Response https://clinicaltrials.gov/search?cond=Neurological%20Disorder&aggFilters=studyType:int&term=Antibody%20Response&intr=antibody2024 [.
- Pardridge, W.M. Drug Targeting to the Brain. Pharm. Res. 2007, 24, 1733–1744. [CrossRef]
- Fortin, D.; Gendron, C.; Boudrias, M.; Garant, M. Enhanced chemotherapy delivery by intraarterial infusion and blood-brain barrier disruption in the treatment of cerebral metastasis. Cancer 2007, 109, 751–760. [CrossRef]
- Hynynen, K.; McDannold, N.; Vykhodtseva, N.; Jolesz, F.A. Noninvasive MR Imaging–guided Focal Opening of the Blood-Brain Barrier in Rabbits. Radiology 2001, 220, 640–646. [CrossRef]
- Burgess, A.; Hynynen, K. Noninvasive and Targeted Drug Delivery to the Brain Using Focused Ultrasound. ACS Chem. Neurosci. 2013, 4, 519–526. [CrossRef]
- Bradley, M.; Swindell, C.; Anthony, F.; Witman, P.; Devanesan, P.; Webb, N.; Baker, S.; Wolff, A.; Donehower, R. Tumor targeting by conjugation of DHA to paclitaxel. J. Control. Release 2001, 74, 233–236. [CrossRef]
- Moghimi, S.; Szebeni, J. Stealth liposomes and long circulating nanoparticles: critical issues in pharmacokinetics, opsonization and protein-binding properties. Prog. Lipid Res. 2003, 42, 463–478. [CrossRef]
- Dhuria, S.V.; Hanson, L.R.; Frey, W.H., 2nd. Intranasal delivery to the central nervous system: Mechanisms and experimental considerations. J. Pharm. Sci. 2010, 99, 1654–1673. [CrossRef]
- Jones, A.R.; Shusta, E.V. Blood–Brain Barrier Transport of Therapeutics via Receptor-Mediation. Pharm. Res. 2007, 24, 1759–1771. [CrossRef]
- Gao, Y.; Zhu, J.; Lu, H. Single domain antibody-based vectors in the delivery of biologics across the blood–brain barrier: a review. Drug Deliv. Transl. Res. 2020, 11, 1818–1828. [CrossRef]
- Bien-Ly, N.; Yu, Y.J.; Bumbaca, D.; Elstrott, J.; Boswell, C.A.; Zhang, Y.; Luk, W.; Lu, Y.; Dennis, M.S.; Weimer, R.M.; et al. Transferrin receptor (TfR) trafficking determines brain uptake of TfR antibody affinity variants. J. Exp. Med. 2014, 211, 233–244. [CrossRef]
- Pardridge, W.M. Drug Transport across the Blood–Brain Barrier. J. Cereb. Blood Flow Metab. 2012, 32, 1959–1972. [CrossRef]
- Zhang, Y.; Pardridge, W.M. Blood–brain barrier targeting of BDNF improves motor function in rats with middle cerebral artery occlusion. Brain Res. 2006, 1111, 227–229. [CrossRef]
- Boado RJ, Zhang Y, Zhang Y, Pardridge WM. Humanization of anti-human insulin receptor antibody for drug targeting across the human blood-brain barrier. Biotechnol Bioeng. 2007;96(2):381-91.
- Deane R, Bell RD, Sagare A, Zlokovic BV. Clearance of amyloid-beta peptide across the blood-brain barrier: implication for therapies in Alzheimer's disease. CNS Neurol Disord Drug Targets. 2009;8(1):16-30.
- Deane R, Wu Z, Sagare A, Davis J, Du Yan S, Hamm K, et al. LRP/amyloid beta-peptide interaction mediates differential brain efflux of Abeta isoforms. Neuron. 2004;43(3):333-44.
- Zlokovic, B.V. The Blood-Brain Barrier in Health and Chronic Neurodegenerative Disorders. Neuron 2008, 57, 178–201. [CrossRef]
- Pardridge WM. The blood-brain barrier: bottleneck in brain drug development. NeuroRx. 2005;2(1):3-14.
- Wilchek, M.; Bayer, E.A. The avidin-biotin complex in bioanalytical applications. Anal. Biochem. 1988, 171, 1–32. [CrossRef]
- Veronese, F.M.; Pasut, G. PEGylation, successful approach to drug delivery. Drug Discov. Today 2005, 10, 1451–1458. [CrossRef]
- Argos, P. An investigation of oligopeptides linking domains in protein tertiary structures and possible candidates for general gene fusion. J. Mol. Biol. 1990, 211, 943–958. [CrossRef]
- Carter, P.; Wells, J.A. Dissecting the catalytic triad of a serine protease. Nature 1988, 332, 564–568. [CrossRef]
- Urry, D.W. Physical Chemistry of Biological Free Energy Transduction As Demonstrated by Elastic Protein-Based Polymers. J. Phys. Chem. B 1997, 101, 11007–11028. [CrossRef]
- Arai, R.; Ueda, H.; Kitayama, A.; Kamiya, N.; Nagamune, T. Design of the linkers which effectively separate domains of a bifunctional fusion protein. Protein Eng. Des. Sel. 2001, 14, 529–532. [CrossRef]
- Huang, X.; Kong, N.; Zhang, X.; Cao, Y.; Langer, R.; Tao, W. The landscape of mRNA nanomedicine. Nat. Med. 2022, 28, 2273–2287. [CrossRef]
- Blakney, A.K.; Ip, S.; Geall, A.J. An Update on Self-Amplifying mRNA Vaccine Development. Vaccines 2021, 9, 97. [CrossRef]
- Niazi, S.K. The FDA’s New Guideline “Generally Accepted Scientific Knowledge” (GASK): An Opportunity to Expedite the Approval of Biosimilars. Pharmaceuticals 2023, 16, 1517. [CrossRef]
- Ban, W.; You, Y.; Yang, Z. Imaging Technologies for Cerebral Pharmacokinetic Studies: Progress and Perspectives. Biomedicines 2022, 10, 2447. [CrossRef]
- Marathe, P.H.; Shyu, W.C.; Humphreys, W.G. The Use of Radiolabeled Compounds for ADME Studies in Discovery and Exploratory Development. Curr. Pharm. Des. 2004, 10, 2991–3008. [CrossRef]
- Zuber C, Mitteregger G, Schuhmann N, Rey C, Knackmuss S, Rupprecht W, et al. Delivery of single-chain antibodies (scFvs) directed against the 37/67 kDa laminin receptor into mice via recombinant adeno-associated viral vectors for prion disease gene therapy. J Gen Virol. 2008;89(Pt 8):2055-61.
- Waraho-Zhmayev, D.; Meksiriporn, B.; Portnoff, A.D.; DeLisa, M.P. Optimizing recombinant antibodies for intracellular function using hitchhiker-mediated survival selection.. Protein Eng. Des. Sel. 2014, 27, 351–8. [CrossRef]
- Niazi, S.K. Non-Invasive Drug Delivery across the Blood–Brain Barrier: A Prospective Analysis. Pharmaceutics 2023, 15, 2599. [CrossRef]
- Berg, P.; Baltimore, D.; Boyer, H.W.; Cohen, S.N.; Davis, R.W.; Hogness, D.S.; Nathans, D.; Roblin, R.; Watson, J.D.; Weissman, S.; et al. Letter: Potential biohazards of recombinant DNA molecules.. 1974, 185, 303.
- Niazi, S.K. Anti-Idiotypic mRNA Vaccine to Treat Autoimmune Disorders. Vaccines 2023, 12, 9. [CrossRef]
- Niazi, S.K.; Magoola, M. mRNA and Synthesis-Based Therapeutic Proteins: A Non-Recombinant Affordable Option. Biologics 2023, 3, 355–379. [CrossRef]
- Klein, K.; Gencoglu, M.; Heisterberg, J.; Acha, V.; Stolk, P. The Global Landscape of Manufacturers of Follow-on Biologics: An Overview of Five Major Biosimilar Markets and 15 Countries. BioDrugs 2022, 37, 235–245. [CrossRef]
- Ross, E.L.; Weinberg, M.S.; Arnold, S.E. Cost-effectiveness of Aducanumab and Donanemab for Early Alzheimer Disease in the US. JAMA Neurol. 2022, 79, 478–487. [CrossRef]
- Niazi, S.K. RNA Therapeutics: A Healthcare Paradigm Shift. Biomedicines 2023, 11, 1275. [CrossRef]
- Niazi, S.K. Making COVID-19 mRNA vaccines accessible: challenges resolved. Expert Rev. Vaccines 2022, 21, 1163–1176. [CrossRef]
Figure 1.
Transferrin-fused antibodies transported across the BBB.
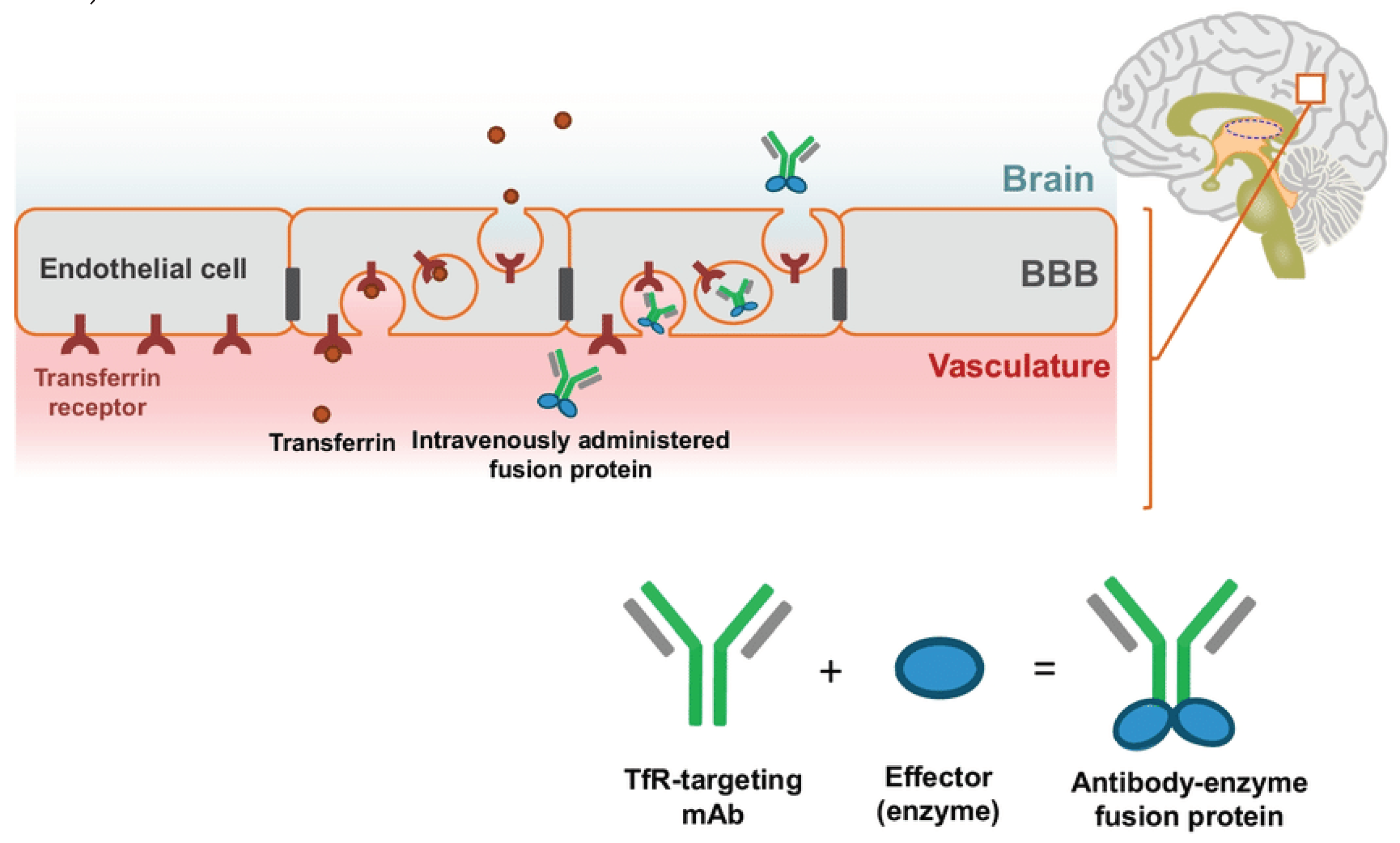

Table 1.
ORF examples of three antibodies (US Patents pending).
| Biogen withdrew Aducanumab (BLA 761178) |
| ΨACGCGGACCGCCACCCGCGCGACGACCACACGCGCCACGACCCGGACACGGACCGCCACGGCCΨAΨΨΨΨGGCACGCGACCACGCGCCACΨCGCΨΨGΨACΨΨCGCΨGGΨΨΨACGGΨCΨCGAAAGCGCΨAGΨAΨACΨΨΨΨCGCACΨAAGGCΨCGCΨACCGGGCΨCGCACCGCACGCACΨΨΨΨΨΨCGCΨCGAΨAGACCΨAACGΨAAGCGCGCΨAACGCCGCΨΨGCΨΨCGCCΨACGCCACΨGGGACCΨACGCCCGGACCACAΨACΨACGCAΨAGACCGCGGCΨΨGΨΨGGACΨΨΨGGCCACCACCGCCΨΨAAAAΨACCGΨCGΨΨΨCΨΨCΨAGGCGΨCΨGGAAAAΨAAΨACGCCACCGCCACCACΨΨΨΨΨΨCΨAΨCGCCGAAAGΨCΨACΨΨGGΨCGACGCGCCGΨΨΨΨΨΨΨCGACGGΨAΨGGCCGGACCCGGCGΨCGCGCCCGACCΨΨGΨAAGGCΨAACCGGACGACAΨAACGCΨAGACGGCCΨΨGGCGCGΨΨΨGGCGACCΨΨΨΨΨCGCCACCGCΨΨGAAAAAAΨCGCCGΨCGACGCGCGGCACGCGCCΨACCGΨGGCΨAAAAGGCGΨCGACACGGΨCGACACGGGCCCGACGCCGACGΨCGΨGGGACΨΨGGΨCAΨAAAACCGAΨAΨCGCCGCGCAAAΨΨΨACGGACΨΨΨCΨACCGCGCCCGCΨACACCGCAAACACΨΨΨGΨAΨCGΨGGΨAAAAACΨΨΨΨGGACCGCΨΨGΨΨΨCGCCΨAGCGCΨAGΨCAΨACΨΨGACGACACGGACCΨAΨΨGΨGGGCGΨΨΨGGCCACCΨACΨΨAΨAΨΨΨCΨAACGGΨAGACCGCGΨCCACGGCΨCGGΨAΨGGCACCACCGCGCGΨCGΨACCCGCCGΨΨΨCΨΨCΨAGACΨAAACCCΨΨGACGACΨΨGGΨCCGCGΨCCΨΨGΨAAAACCGΨΨΨCΨAΨΨΨΨCGΨΨΨCΨΨAAAGΨCGACAAAΨCGΨCGGGCGΨACCGΨΨΨCΨAGACGACAAAΨΨΨCΨAΨCGCGCGΨACCGAAAGACΨΨΨCACGGCGGCGCGΨACCΨACGCΨΨΨΨACAΨAGACCCGAΨACΨΨAΨACACΨGGCGCΨAAGCGΨΨGGACGCGCΨΨCCGΨGGACGGGCCΨΨCGCGGCΨGGCΨACΨΨACGΨΨΨGGCCACΨΨΨACCACGCGCGACΨCGGΨAGΨACΨΨGCGGACΨΨΨACGCΨACΨΨACCΨCGCACΨΨGΨCGCACCCGΨΨΨΨAACΨΨACGCACΨCGCGCCΨΨΨGGΨGGCΨΨCΨAACGΨAACGCΨΨΨΨAAΨACΨΨGCCGCΨΨCGCCΨACGCΨACΨCGGACCΨACCGCCGAAACACAΨAΨAACGCCCGΨΨΨACGCCGGACCACGGCCACGACCGCCΨΨΨΨGAΨAΨΨGΨΨΨΨCGCΨAΨΨGACGCΨΨCΨAΨGGGGCCΨΨCGCCCGAΨAAAACGCCACCGCCACCACΨΨΨΨΨΨΨCGCGCΨCGCΨAGACΨGGACCCΨAΨΨGGACΨΨΨCCGΨΨΨΨΨΨΨCGACGGΨAΨGGCGCCACCCGGCGΨGGCGCCCGACCΨΨGΨAAGGCΨACCCGGACGACAΨAΨΨGΨΨΨΨAAΨΨGGΨAACGGCGAAACΨACΨΨAAAAAAΨCGCΨΨCCGACGCGCGGCCCGΨCGΨΨΨΨΨΨCΨAΨCGΨCGGACACGΨΨΨGACACGΨACCCGΨCGCCGGACΨΨGGACACGCΨΨGGCΨΨGΨΨGΨΨΨCΨΨCCGAΨAAΨACCGAΨAΨGGCCGCGCAAAGCGACGGACCACCΨΨΨΨΨCCGCΨACACCGCAAACACΨΨΨGΨAGΨCΨGGCACGGCGΨCΨΨGΨGGCCGCCGΨΨΨΨΨGGGCCΨAGGCACCCGCΨΨΨΨΨGGACΨΨGCΨΨΨΨΨCΨAAΨACΨΨGACGACACGGACCΨACCGΨGGGCGΨΨΨGGCCACCΨΨCΨΨAΨACGCΨΨGACGGΨAGACCGCGCGCGCGGCΨΨGGΨACGCCACCACΨGGGCGΨΨΨCΨAΨΨΨCΨΨCGCACGCACGΨAΨΨΨΨAAGACGCGGΨCGΨCGΨCGΨAGACAAACCGΨCGΨΨGCACΨGGCΨAACGΨCGCCGΨΨGAAAACGGACAAAGCGΨCGCΨΨΨGGΨΨΨCΨAGACGACAAAGCGCΨACΨAΨGGCACACGGACCGCΨΨΨGACGΨACΨAGCGΨΨGΨGGAΨACΨΨΨΨΨAΨAGACCCGCΨΨCΨΨAΨACACΨΨΨCGCCACCCGΨΨGGACGCGΨΨΨACGΨCGΨGGΨCGΨCGGACGACCΨΨCGCACGΨGGAAAGCGGCGGGCCCGΨCGCCGΨCGCCGΨCGCCGΨCGCACGΨCGACCACCΨΨΨCGCCGCCGCCGCACCACGΨCGGCCCGGCGΨCGGACGCGGACΨCGACGCGCCGCΨCGCCGAAACGCAAAΨCGΨCGAΨACCGΨACGΨAACCCACGCGGΨCCGCGGCCCGΨΨΨCCGGACCΨΨACCCACCGCCACΨAAACCAAACΨACCGΨGGΨΨΨΨΨΨAΨAAΨAΨGGCΨAΨCGCACΨΨΨCCGGCGAAAΨGGΨAAΨCGGCGCΨAΨΨGΨCGΨΨΨΨΨGΨGGGACAΨAGACGΨCΨACΨΨGΨGGGACGCGCGCCΨΨCΨAΨGGCGCCACAΨAAΨAACGCGCGCGCΨAGCGCCGΨAACCGCGCGCGGCGCCGGGCAΨAAΨAΨACCΨACACACCCCGΨΨΨCCGΨGGΨGGCACΨGGCACΨCGΨCGCGCΨCGΨGGΨΨΨCCGGGCΨCGCACAAAGGCGACCGCGGCΨCGΨCGΨΨΨΨCGΨGGΨCGCCGCCGΨGGCGCCGCGACCCGACGGACCACΨΨΨCΨAAΨAAAAGGCCΨΨGGCCACΨGGCACΨCGACCΨΨGΨCGCCGCGCGACΨGGΨCGCCGCACGΨAΨGGAAAGGCCGCCACGACGΨCΨCGΨCGCCGGACAΨAΨCGGACΨCGΨCGCACCACΨGGCACGGCΨCGΨCGΨCGGACCCGΨGGGΨCΨGGAΨAΨAAACGΨΨGCACΨΨGGΨAΨΨΨGGCΨCGΨΨGΨGGΨΨΨCACCΨAΨΨΨGCGCACCΨΨGGCΨΨΨΨCGACGCΨAΨΨΨΨGGGΨAΨGGACGGGCGGCACGGGCCGCGGCCΨΨGACGACCCGCCGGGCΨCGCACAAAGACAAAGGCGGCΨΨΨGGCΨΨΨCΨAΨGGGACΨACΨAAΨCGGCGΨGGGGCCΨΨCACΨGGACGCACCACCACCΨACACΨCGGΨACΨΨCΨAGGCCΨΨCACΨΨΨAAAΨΨGACCAΨACACCΨACCGCACCΨΨCACGΨAΨΨGCGCΨΨΨΨGGΨΨΨGGCGCGCΨΨCΨΨGΨCAΨAΨΨGΨCGΨGGAΨAGCGCACCACΨCGCACGACΨGGCACGACGΨAGΨCCΨAACCGACΨΨGCCGΨΨΨCΨΨAΨAΨΨΨACGΨΨΨCACΨCGΨΨGΨΨΨCGCGACGGCCGCGGCΨAACΨΨΨΨΨΨGGΨAAΨCGΨΨΨCGCΨΨΨCCGGΨCGGCGCGCΨΨGGCGΨCCACAΨAΨGGGACGGCGGCΨCGGCGCΨΨCΨΨΨACΨGGΨΨΨΨΨGGΨCCACΨCGGACΨGGACGGACCACΨΨΨCCGAAAAΨAGGCΨCGCΨAΨAACGCCACCΨΨACCCΨΨΨCGΨΨGCCGGΨCGGCCΨΨΨΨGΨΨGAΨAΨΨΨΨGGΨGGGGCGGCCACGACCΨAΨCGCΨACCGΨCGAAAAAAGACAΨAΨCGΨΨΨGACΨGGCACCΨAΨΨΨΨCGGCGACCGΨCGΨCCCGΨΨGCACAAAΨCGACGΨCGCACΨACGΨACΨΨCGCGACGΨAΨΨGGΨAAΨAΨGGGΨCΨΨΨΨCGGACΨCGGACΨCGGGCCCGCCGΨCGCCGΨCGCCGΨCGCCGΨCGCΨAΨAAGΨCΨACΨGGGΨCΨCGGGCΨCGΨCGGACΨCGCGCΨCGCACCCGCΨAGCGCACΨGGΨAAΨGGACGGCGCGCΨCGGΨCΨCGΨAAΨCGΨCGAΨAGACΨΨGACCAΨAGΨCGΨCΨΨΨGGCCCGΨΨΨCGCGGCΨΨΨGACGACΨAAAΨACGCCGCΨCGΨCGGACGΨCΨCGCCGCACGGCΨCGGCGAAAΨCGCCGΨCGCCGΨCGCCGΨGGCΨAAAAΨGGGACΨGGΨAAΨCGΨCGGACGΨCGGCCΨΨCΨAAAACGCΨGGAΨAAΨAACGGΨCGΨCΨCGAΨAΨCGΨGGGGCGACΨGGAAACCGCCGCCGΨGGΨΨΨCACCΨΨΨAAΨΨΨGCGΨGGCACCGCCGCGGCΨCGCACAAAΨAAAAAGGCGGCΨCGCΨACΨΨGΨCGACΨΨΨΨCGCCGΨGGCGCΨCGCACCACACGGACGACΨΨGΨΨGAAAAΨAGGCGCGCΨΨCGCΨΨΨCACGΨCACCΨΨΨCACCΨAΨΨGCGCGACGΨCΨCGCCGΨΨGΨCGGΨCCΨΨΨCGCACΨGGCΨΨGΨCCΨAΨCGΨΨΨCΨAΨCGΨGGAΨAΨCGGACΨCGΨCGΨGGGACΨGGGACΨCGΨΨΨCGCCΨAAΨACΨΨΨΨΨGΨAΨΨΨCACAΨACGCACGCΨΨCACΨGGGΨAGΨCCCGGACΨCGΨCGGGCCACΨGGΨΨΨΨCGAAAΨΨGGCGCCGCΨΨACG |
| Lecanemab (BLA761269) |
| AΨGCGCCΨGGCGGΨGGGCGCGCΨGCΨGGΨGΨGCGCGGΨGCΨGGGCCΨGΨGCCΨGGCGGΨGCCGGAΨAAAACCGΨGCGCΨGGΨGCGCGGΨGAGCGAACAΨGAAGCGACCAAAΨGCCAGAGCΨΨΨCGCGAΨCAΨAΨGAAAAGCGΨGAΨΨCCGAGCGAΨGGCCCGAGCGΨGGCGΨGCGΨGAAAAAAGCGAGCΨAΨCΨGGAΨΨGCAΨΨCGCGCGAΨΨGCGGCGAACGAAGCGGAΨGCGGΨGACCCΨGGAΨGCGGGCCΨGGΨGΨAΨGAΨGCGΨAΨCΨGGCGCCGAACAACCΨGAAACCGGΨGGΨGGCGGAAΨΨΨΨAΨGGCAGCAAAGAAGAΨCCGCAGACCΨΨΨΨAΨΨAΨGCGGΨGGCGGΨGGΨGAAAAAAGAΨAGCGGCΨΨΨCAGAΨGAACCAGCΨGCGCGGCAAAAAAAGCΨGCCAΨACCGGCCΨGGGCCGCAGCGCGGGCΨGGAACAΨΨCCGAΨΨGGCCΨGCΨGΨAΨΨGCGAΨCΨGCCGGAACCGCGCAAACCGCΨGGAAAAAGCGGΨGGCGAACΨΨΨΨΨΨAGCGGCAGCΨGCGCGCCGΨGCGCGGAΨGGCACCGAΨΨΨΨCCGCAGCΨGΨGCCAGCΨGΨGCCCGGGCΨGCGGCΨGCAGCACCCΨGAACCAGΨAΨΨΨΨGGCΨAΨAGCGGCGCGΨΨΨAAAΨGCCΨGAAAGAΨGGCGCGGGCGAΨGΨGGCGΨΨΨGΨGAAACAΨAGCACCAΨΨΨΨΨGAAAACCΨGGCGAACAAAGCGGAΨCGCGAΨCAGΨAΨGAACΨGCΨGΨGCCΨGGAΨAACACCCGCAAACCGGΨGGAΨGAAΨAΨAAAGAΨΨGCCAΨCΨGGCGCAGGΨGCCGAGCCAΨACCGΨGGΨGGCGCGCAGCAΨGGGCGGCAAAGAAGAΨCΨGAΨΨΨGGGAACΨGCΨGAACCAGGCGCAGGAACAΨΨΨΨGGCAAAGAΨAAAAGCAAAGAAΨΨΨCAGCΨGΨΨΨAGCAGCCCGCAΨGGCAAAGAΨCΨGCΨGΨΨΨAAAGAΨAGCGCGCAΨGGCΨΨΨCΨGAAAGΨGCCGCCGCGCAΨGGAΨGCGAAAAΨGΨAΨCΨGGGCΨAΨGAAΨAΨGΨGACCGCGAΨΨCGCAACCΨGCGCGAAGGCACCΨGCCCGGAAGCGCCGACCGAΨGAAΨGCAAACCGGΨGAAAΨGGΨGCGCGCΨGAGCCAΨCAΨGAACGCCΨGAAAΨGCGAΨGAAΨGGAGCGΨGAACAGCGΨGGGCAAAAΨΨGAAΨGCGΨGAGCGCGGAAACCACCGAAGAΨΨGCAΨΨGCGAAAAΨΨAΨGAACGGCGAAGCGGAΨGCGAΨGAGCCΨGGAΨGGCGGCΨΨΨGΨGΨAΨAΨΨGCGGGCAAAΨGCGGCCΨGGΨGCCGGΨGCΨGGCGGAAAACΨAΨAACAAAAGCGAΨAACΨGCGAAGAΨACCCCGGAAGCGGGCΨAΨΨΨΨGCGGΨGGCGGΨGGΨGAAAAAAAGCGCGAGCGAΨCΨGACCΨGGGAΨAACCΨGAAAGGCAAAAAAAGCΨGCCAΨACCGCGGΨGGGCCGCACCGCGGGCΨGGAACAΨΨCCGAΨGGGCCΨGCΨGΨAΨAACAAAAΨΨAACCAΨΨGCCGCΨΨΨGAΨGAAΨΨΨΨΨΨAGCGAAGGCΨGCGCGCCGGGCAGCAAAAAAGAΨAGCAGCCΨGΨGCAAACΨGΨGCAΨGGGCAGCGGCCΨGAACCΨGΨGCGAACCGAACAACAAAGAAGGCΨAΨΨAΨGGCΨAΨACCGGCGCGΨΨΨCGCΨGCCΨGGΨGGAAAAAGGCGAΨGΨGGCGΨΨΨGΨGAAACAΨCAGACCGΨGCCGCAGAACACCGGCGGCAAAAACCCGGAΨCCGΨGGGCGAAAAACCΨGAACGAAAAAGAΨΨAΨGAACΨGCΨGΨGCCΨGGAΨGGCACCCGCAAACCGGΨGGAAGAAΨAΨGCGAACΨGCCAΨCΨGGCGCGCGCGCCGAACCAΨGCGGΨGGΨGACCCGCAAAGAΨAAAGAAGCGΨGCGΨGCAΨAAAAΨΨCΨGCGCCAGCAGCAGCAΨCΨGΨΨΨGGCAGCAACGΨGACCGAΨΨGCAGCGGCAACΨΨΨΨGCCΨGΨΨΨCGCAGCGAAACCAAAGAΨCΨGCΨGΨΨΨCGCGAΨGAΨACCGΨGΨGCCΨGGCGAAACΨGCAΨGAΨCGCAACACCΨAΨGAAAAAΨAΨCΨGGGCGAAGAAΨAΨGΨGAAAGCGGΨGGGCAACCΨGCGCAAAΨGCAGCACCAGCAGCCΨGCΨGGAAGCGΨGCACCΨΨΨCGCCGCCCGGGCAGCGGCAGCGGCAGCGGCAGCGAAGΨGCAGCΨGGΨGGAAAGCGGCGGCGGCCΨGGΨGCAGCCGGGCGGCAGCCΨGCGCCΨGAGCΨGCAGCGCGAGCGGCΨΨΨACCΨΨΨAGCAGCΨΨΨGGCAΨGCAΨΨGGGΨGCGCCAGGCGCCGGGCAAAGGCCΨGGAAΨGGGΨGGCGΨAΨAΨΨAGCAGCGGCAGCAGCACCAΨΨΨAΨΨAΨGGCGAΨACCGΨGAAAGGCCGCΨΨΨACCAΨΨAGCCGCGAΨAACGCGAAAAACAGCCΨGΨΨΨCΨGCAGAΨGAGCAGCCΨGCGCGCGGAAGAΨACCGCGGΨGΨAΨΨAΨΨGCGCGCGCGAAGGCGGCΨAΨΨAΨΨAΨGGCCGCAGCΨAΨΨAΨACCAΨGGAΨΨAΨΨGGGGCCAGGGCACCACCGΨGACCGΨGAGCAGCGCGAGCACCAAAGGCCCGAGCGΨGΨΨΨCCGCΨGGCGCCGAGCAGCAAAAGCACCAGCGGCGGCACCGCGGCGCΨGGGCΨGCCΨGGΨGAAAGAΨΨAΨΨΨΨCCGGAACCGGΨGACCGΨGAGCΨGGAACAGCGGCGCGCΨGACCAGCGGCGΨGCAΨACCΨΨΨCCGGCGGΨGCΨGCAGAGCAGCGGCCΨGΨAΨAGCCΨGAGCAGCGΨGGΨGACCGΨGCCGAGCAGCAGCCΨGGGCACCCAGACCΨAΨAΨΨΨGCAACGΨGAACCAΨAAACCGAGCAACACCAAAGΨGGAΨAAACGCGΨGGAACCGAAAAGCΨGCGAΨAAAACCCAΨACCΨGCCCGCCGΨGCCCGGCGCCGGAACΨGCΨGGGCGGCCCGAGCGΨGΨΨΨCΨGΨΨΨCCGCCGAAACCGAAAGAΨACCCΨGAΨGAΨΨAGCCGCACCCCGGAAGΨGACCΨGCGΨGGΨGGΨGGAΨGΨGAGCCAΨGAAGAΨCCGGAAGΨGAAAΨΨΨAACΨGGΨAΨGΨGGAΨGGCGΨGGAAGΨGCAΨAACGCGAAAACCAAACCGCGCGAAGAACAGΨAΨAACAGCACCΨAΨCGCGΨGGΨGAGCGΨGCΨGACCGΨGCΨGCAΨCAGGAΨΨGGCΨGAACGGCAAAGAAΨAΨAAAΨGCAAAGΨGAGCAACAAAGCGCΨGCCGGCGCCGAΨΨGAAAAAACCAΨΨAGCAAAGCGAAAGGCCAGCCGCGCGAACCGCAGGΨGΨAΨACCCΨGCCGCCGAGCCGCGAAGAAAΨGACCAAAAACCAGGΨGAGCCΨGACCΨGCCΨGGΨGAAAGGCΨΨΨΨAΨCCGAGCGAΨAΨΨGCGGΨGGAAΨGGGAAAGCAACGGCCAGCCGGAAAACAACΨAΨAAAACCACCCCGCCGGΨGCΨGGAΨAGCGAΨGGCAGCΨΨΨΨΨΨCΨGΨAΨAGCAAACΨGACCGΨGGAΨAAAAGCCGCΨGGCAGCAGGGCAACGΨGΨΨΨAGCΨGCAGCGΨGAΨGCAΨGAAGCGCΨGCAΨAACCAΨΨAΨACCCAGAAAAGCCΨGAGCCΨGAGCCCGGGCAAAGGCAGCGGCAGCGGCAGCGGCAGCGAΨGΨGGΨGAΨGACCCAGAGCCCGCΨGAGCCΨGCCGGΨGACCCCGGGCGCGCCGGCGAGCAΨΨAGCΨGCCGCAGCAGCCAGAGCAΨΨGΨGCAΨAGCAACGGCAACACCΨAΨCΨGGAAΨGGΨAΨCΨGCAGAAACCGGGCCAGAGCCCGAAACΨGCΨGAΨΨΨAΨAAAGΨGAGCAACCGCΨΨΨAGCGGCGΨGCCGGAΨCGCΨΨΨAGCGGCAGCGGCAGCGGCACCGAΨΨΨΨACCCΨGCGCAΨΨAGCCGCGΨGGAAGCGGAAGAΨGΨGGGCAΨΨΨAΨΨAΨΨGCΨΨΨCAGGGCAGCCAΨGΨGCCGCCGACCΨΨΨGGCCCGGGCACCAAACΨGGAAAΨΨAAACGCACCGΨGGCGGCGCCGAGCGΨGΨΨΨAΨΨΨΨΨCCGCCGAGCGAΨGAACAGCΨGAAAAGCGGCACCGCGAGCGΨGGΨGΨGCCΨGCΨGAACAACΨΨΨΨAΨCCGCGCGAAGCGAAAGΨGCAGΨGGAAAGΨGGAΨAACGCGCΨGCAGAGCGGCAACAGCCAGGAAAGCGΨGACCGAACAGGAΨAGCAAAGAΨAGCACCΨAΨAGCCΨGAGCAGCACCCΨGACCCΨGAGCAAAGCGGAΨΨAΨGAAAAACAΨAAAGΨGΨAΨGCGΨGCGAAGΨGACCCAΨCAGGGCCΨGAGCAGCCCGGΨGACCAAAAGCΨΨΨAACCGCGGCGAAΨGC |
| Cinpanemab (BLA pending); discontinued by Biogen |
| AΨGCGCCΨGGCGGΨGGGCGCGCΨGCΨGGΨGΨGCGCGGΨGCΨGGGCCΨGΨGCCΨGGCGGΨGCCGGAΨAAAACCGΨGCGCΨGGΨGCGCGGΨGAGCGAACAΨGAAGCGACCAAAΨGCCAGAGCΨΨΨCGCGAΨCAΨAΨGAAAAGCGΨGAΨΨCCGAGCGAΨGGCCCGAGCGΨGGCGΨGCGΨGAAAAAAGCGAGCΨAΨCΨGGAΨΨGCAΨΨCGCGCGAΨΨGCGGCGAACGAAGCGGAΨGCGGΨGACCCΨGGAΨGCGGGCCΨGGΨGΨAΨGAΨGCGΨAΨCΨGGCGCCGAACAACCΨGAAACCGGΨGGΨGGCGGAAΨΨΨΨAΨGGCAGCAAAGAAGAΨCCGCAGACCΨΨΨΨAΨΨAΨGCGGΨGGCGGΨGGΨGAAAAAAGAΨAGCGGCΨΨΨCAGAΨGAACCAGCΨGCGCGGCAAAAAAAGCΨGCCAΨACCGGCCΨGGGCCGCAGCGCGGGCΨGGAACAΨΨCCGAΨΨGGCCΨGCΨGΨAΨΨGCGAΨCΨGCCGGAACCGCGCAAACCGCΨGGAAAAAGCGGΨGGCGAACΨΨΨΨΨΨAGCGGCAGCΨGCGCGCCGΨGCGCGGAΨGGCACCGAΨΨΨΨCCGCAGCΨGΨGCCAGCΨGΨGCCCGGGCΨGCGGCΨGCAGCACCCΨGAACCAGΨAΨΨΨΨGGCΨAΨAGCGGCGCGΨΨΨAAAΨGCCΨGAAAGAΨGGCGCGGGCGAΨGΨGGCGΨΨΨGΨGAAACAΨAGCACCAΨΨΨΨΨGAAAACCΨGGCGAACAAAGCGGAΨCGCGAΨCAGΨAΨGAACΨGCΨGΨGCCΨGGAΨAACACCCGCAAACCGGΨGGAΨGAAΨAΨAAAGAΨΨGCCAΨCΨGGCGCAGGΨGCCGAGCCAΨACCGΨGGΨGGCGCGCAGCAΨGGGCGGCAAAGAAGAΨCΨGAΨΨΨGGGAACΨGCΨGAACCAGGCGCAGGAACAΨΨΨΨGGCAAAGAΨAAAAGCAAAGAAΨΨΨCAGCΨGΨΨΨAGCAGCCCGCAΨGGCAAAGAΨCΨGCΨGΨΨΨAAAGAΨAGCGCGCAΨGGCΨΨΨCΨGAAAGΨGCCGCCGCGCAΨGGAΨGCGAAAAΨGΨAΨCΨGGGCΨAΨGAAΨAΨGΨGACCGCGAΨΨCGCAACCΨGCGCGAAGGCACCΨGCCCGGAAGCGCCGACCGAΨGAAΨGCAAACCGGΨGAAAΨGGΨGCGCGCΨGAGCCAΨCAΨGAACGCCΨGAAAΨGCGAΨGAAΨGGAGCGΨGAACAGCGΨGGGCAAAAΨΨGAAΨGCGΨGAGCGCGGAAACCACCGAAGAΨΨGCAΨΨGCGAAAAΨΨAΨGAACGGCGAAGCGGAΨGCGAΨGAGCCΨGGAΨGGCGGCΨΨΨGΨGΨAΨAΨΨGCGGGCAAAΨGCGGCCΨGGΨGCCGGΨGCΨGGCGGAAAACΨAΨAACAAAAGCGAΨAACΨGCGAAGAΨACCCCGGAAGCGGGCΨAΨΨΨΨGCGGΨGGCGGΨGGΨGAAAAAAAGCGCGAGCGAΨCΨGACCΨGGGAΨAACCΨGAAAGGCAAAAAAAGCΨGCCAΨACCGCGGΨGGGCCGCACCGCGGGCΨGGAACAΨΨCCGAΨGGGCCΨGCΨGΨAΨAACAAAAΨΨAACCAΨΨGCCGCΨΨΨGAΨGAAΨΨΨΨΨΨAGCGAAGGCΨGCGCGCCGGGCAGCAAAAAAGAΨAGCAGCCΨGΨGCAAACΨGΨGCAΨGGGCAGCGGCCΨGAACCΨGΨGCGAACCGAACAACAAAGAAGGCΨAΨΨAΨGGCΨAΨACCGGCGCGΨΨΨCGCΨGCCΨGGΨGGAAAAAGGCGAΨGΨGGCGΨΨΨGΨGAAACAΨCAGACCGΨGCCGCAGAACACCGGCGGCAAAAACCCGGAΨCCGΨGGGCGAAAAACCΨGAACGAAAAAGAΨΨAΨGAACΨGCΨGΨGCCΨGGAΨGGCACCCGCAAACCGGΨGGAAGAAΨAΨGCGAACΨGCCAΨCΨGGCGCGCGCGCCGAACCAΨGCGGΨGGΨGACCCGCAAAGAΨAAAGAAGCGΨGCGΨGCAΨAAAAΨΨCΨGCGCCAGCAGCAGCAΨCΨGΨΨΨGGCAGCAACGΨGACCGAΨΨGCAGCGGCAACΨΨΨΨGCCΨGΨΨΨCGCAGCGAAACCAAAGAΨCΨGCΨGΨΨΨCGCGAΨGAΨACCGΨGΨGCCΨGGCGAAACΨGCAΨGAΨCGCAACACCΨAΨGAAAAAΨAΨCΨGGGCGAAGAAΨAΨGΨGAAAGCGGΨGGGCAACCΨGCGCAAAΨGCAGCACCAGCAGCCΨGCΨGGAAGCGΨGCACCΨΨΨCGCCGCCCGGGCAGCGGCAGCGGCAGCGGCAGCGAAGΨGCAGCΨGGΨGGAAAGCGGCGGCGGCCΨGGΨGGAACCGGGCGGCAGCCΨGCGCCΨGAGCΨGCGCGGΨGAGCGGCΨΨΨGAΨΨΨΨGAAAAAGCGΨGGAΨGAGCΨGGGΨGCGCCAGGCGCCGGGCCAGGGCCΨGCAGΨGGGΨGGCGCGCAΨΨAAAAGCACCGCGGAΨGGCGGCACCACCAGCΨAΨGCGGCGCCGGΨGGAAGGCCGCΨΨΨAΨΨAΨΨAGCCGCGAΨGAΨAGCCGCAACAΨGCΨGΨAΨCΨGCAGAΨGAACAGCCΨGAAAACCGAAGAΨACCGCGGΨGΨAΨΨAΨΨGCACCAGCGCGCAΨΨGGGGCCAGGGCACCCΨGGΨGACCGΨGAGCAGCGCGAGCACCAAAGGCCCGAGCGΨGΨΨΨCCGCΨGGCGCCGAGCAGCAAAAGCACCAGCGGCGGCACCGCGGCGCΨGGGCΨGCCΨGGΨGAAAGAΨΨAΨΨΨΨCCGGAACCGGΨGACCGΨGAGCΨGGAACAGCGGCGCGCΨGACCAGCGGCGΨGCAΨACCΨΨΨCCGGCGGΨGCΨGCAGAGCAGCGGCCΨGΨAΨAGCCΨGAGCAGCGΨGGΨGACCGΨGCCGAGCAGCAGCCΨGGGCACCCAGACCΨAΨAΨΨΨGCAACGΨGAACCAΨAAACCGAGCAACACCAAAGΨGGAΨAAACGCGΨGGAACCGAAAAGCΨGCGAΨAAAACCCAΨACCΨGCCCGCCGΨGCCCGGCGCCGGAACΨGCΨGGGCGGCCCGAGCGΨGΨΨΨCΨGΨΨΨCCGCCGAAACCGAAAGAΨACCCΨGAΨGAΨΨAGCCGCACCCCGGAAGΨGACCΨGCGΨGGΨGGΨGGAΨGΨGAGCCAΨGAAGAΨCCGGAAGΨGAAAΨΨΨAACΨGGΨAΨGΨGGAΨGGCGΨGGAAGΨGCAΨAACGCGAAAACCAAACCGCGCGAAGAACAGΨAΨAACAGCACCΨAΨCGCGΨGGΨGAGCGΨGCΨGACCGΨGCΨGCAΨCAGGAΨΨGGCΨGAACGGCAAAGAAΨAΨAAAΨGCAAAGΨGAGCAACAAAGCGCΨGCCGGCGCCGAΨΨGAAAAAACCAΨΨAGCAAAGCGAAAGGCCAGCCGCGCGAACCGCAGGΨGΨAΨACCCΨGCCGCCGAGCCGCGAAGAAAΨGACCAAAAACCAGGΨGAGCCΨGACCΨGCCΨGGΨGAAAGGCΨΨΨΨAΨCCGAGCGAΨAΨΨGCGGΨGGAAΨGGGAAAGCAACGGCCAGCCGGAAAACAACΨAΨAAAACCACCCCGCCGGΨGCΨGGAΨAGCGAΨGGCAGCΨΨΨΨΨΨCΨGΨAΨAGCAAACΨGACCGΨGGAΨAAAAGCCGCΨGGCAGCAGGGCAACGΨGΨΨΨAGCΨGCAGCGΨGAΨGCAΨGAAGCGCΨGCAΨAACCAΨΨAΨACCCAGAAAAGCCΨGAGCCΨGAGCCCGGGCGGCAGCGGCAGCGGCAGCGGCAGCAGCΨAΨGAACΨGACCCAGCCGCCGAGCGΨGAGCGΨGAGCCCGGGCCAGACCGCGCGCAΨΨACCΨGCAGCGGCGAAGCGCΨGCCGAΨGCAGΨΨΨGCGCAΨΨGGΨAΨCAGCAGCGCCCGGGCAAAGCGCCGGΨGAΨΨGΨGGΨGΨAΨAAAGAΨAGCGAACGCCCGAGCGGCGΨGCCGGAACGCΨΨΨAGCGGCAGCAGCAGCGGCACCACCGCGACCCΨGACCAΨΨACCGGCGΨGCAGGCGGAAGAΨGAAGCGGAΨΨAΨΨAΨΨGCCAGAGCCCGGAΨAGCACCAACACCΨAΨGAAGΨGΨΨΨGGCGGCGGCACCAAACΨGACCGΨGCΨGAGCCAGCCGAAAGCGGCGCCGAGCGΨGACCCΨGΨΨΨCCGCCGAGCAGCGAAGAACΨGCAGGCGAACAAAGCGACCCΨGGΨGΨGCCΨGAΨΨAGCGAΨΨΨΨΨAΨCCGGGCGCGGΨGACCGΨGGCGΨGGAAAGCGGAΨAGCAGCCCGGΨGAAAGCGGGCGΨGGAAACCACCACCCCGAGCAAACAGAGCAACAACAAAΨAΨGCGGCGAGCAGCΨAΨCΨGAGCCΨGACCCCGGAACAGΨGGAAAAGCCAΨCGCAGCΨAΨAGCΨGCCAGGΨGACCCAΨGAAGGCAGCACCGΨGGAAAAAACCGΨGGCGCCGACCGAAΨGCAGC |
Table 2.
mRNA template to produce antibody-transferrin conjugates.
| Element | Description |
| Cap (2) | A modified 5’-cap1 structure (m7G+m3'-5'-ppp-5'-Am): GA |
| 5’-UTR (52) | The 5´-untranslated region derived from human alpha-globin RNA with an optimized Kozak sequence. GAATAAACTAGTATTCTTCTGGTCCCCACAGACTCAGAGAGAACCCGCCACC |
| Signal peptide (48) | S glycoprotein signal peptide (extended leader sequence) guides translocation of the nascent polypeptide chain into the endoplasmic reticulum: ATGTTCGTGTTCCTGGTGCTGCTGCCTCTGGTGTCCAGCCAGTGTGTG |
| Coding region (n) | Codon-optimized sequence (ORF) |
| 3’-UTR (268) | The 3´ untranslated region comprises two sequence elements derived from the amino-terminal enhancer of split (AES) mRNA and the mitochondrial encoded 12S ribosomal RNA to confer RNA stability and high total protein expression: GCTAGCTGCCCCTTTCCCGTCCTGGGTACCCCGAGTCTCCCCCGACCTCGGGTCCCAGGTATGCTCCCACCTCCACCTGCCCCACTCACCACCTCTGCTAGTTCCAGACACCTCCCAAGCACGCAGCAATGCAGCTCAAAACGCTTAGCCTAGCCACACCCCCACGGGAAACAGCAGTGATTAACCTTTAGCAATAAACGAAAGTTTAACTAAGCTATACTAACCCCAGGGTTGGTCAATTTCGTGCCAGCCACACCCTGGAGCTAGC |
| poly(A) (110) | A 110-nucleotide poly(A)-tail consisting of a stretch of 30 adenosine residues, followed by a 10-nucleotide linker sequence and another 70 adenosine residues: AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAGCATATGACTAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



