
Submitted:
12 March 2024
Posted:
18 March 2024
You are already at the latest version
Abstract
The blood count is crucial for assessing bone marrow's cell production and differentiation during infections, gauging disease severity, and monitoring therapeutic responses. The profile of blood count in chronic form of paracoccidioidomycosis (PCM) has been insufficiently explored. To better understand the changes in hematological cells in different stages of the PCM chronic form, we evaluated the blood count, including immature blood cells in automated equipment, before and during the treatment follow-up of 62 chronic PCM patients. Predominantly male (96.8%) with an average age of 54.3 (SD 6.9) years, participants exhibited pre-treatment conditions such as anemia (45.2%), monocytosis (38.7%), and leukocytosis (17.7%) which became less frequent after clinical cure. Anemia was more prevalent in severe cases. Notably, hemoglobin and reticulocyte hemoglobin content increased, while leukocytes, monocytes, neutrophils, immature granulocytes, and platelets decreased. Chronic PCM induced manageable hematological abnormalities, mainly in the red blood series. Monocytosis, indicating monocytes' role in PCM's immune response, was frequent. Post-treatment, especially after achieving clinical cure, significant improvements were observed in various hematological indices, including immature granulocytes and reticulocyte hemoglobin content, underscoring the impact of infection on these parameters.
Keywords:
anemia
; blood cell count
; leukocyte count
; paracoccidioidomycosis
1. Introduction
Paracoccidioidomycosis (PCM) is a systemic mycosis endemic in Latin America whose etiological agents are fungi of the genus Paracoccidioides [1]. Brazil is considered the endemic center of this disease, where it ranks as the eighth leading cause of death resulting from chronic infectious disease [2].
The infection primarily affects the lungs, spreading through the lymphatic and hematogenous routes to any other organs. In most individuals who inhale the fungus, the progression of the infection is contained, and the course of disease will depend on the size of the inoculum, the pathogenicity and virulence of the fungus, the immune response, and possibly genetic factors [3]. Active PCM can be classified into acute/subacute and chronic forms. Acute/subacute form is known as the juvenile form because it affects children, adolescents, and young adults of both sexes aged under 30 years of age, in similar proportion (male: female ratio of 1.7:1.0). The chronic form affects individuals older than 30 years, usually males (male: female ratio of 22.0:1.0), with a prolonged duration of symptomatology [1]; it predominates in clinical practice, accounting for 75% to 90% of the cases [4,5,6].
The host-parasite interactions in PCM and the consequent inflammatory responses of the body can lead to changes in hematological cells, such as anemia, leukocytosis, and eosinophilia [7]. These findings are more commonly reported in the acute/subacute form of the disease. Few studies on blood cells in chronic PCM have been described, showing changes in the number of erythrocytes and the concentration of hemoglobin [8], as well as in the subpopulations of monocytes and lymphocytes, in untreated patients [9,10,11]. The complete blood count is a simple test performed routinely in most clinics and is important in the clinical management of infectious diseases. It is essential for elucidating whether the bone marrow is correctly performing its functions, with adequate cell production and differentiation, as well as gauging the severity of the condition and the response to treatment. The analysis of immature blood cells in automated equipment is replacing manual counting, becoming possible to assess the involvement of precursor cells in inflammatory and infectious activity, as well as the lack of iron in the body at an early stage.
To better understand the changes in hematological cells in different stages of the PCM chronic form, the present study evaluated the blood count before and during the treatment follow-up.
2. Patients and Methods
2.1. Ethical Aspects
This project was approved by the Committee of Ethics in Research with Human Beings of the Federal University of Mato Grosso do Sul (CEP - UFMS) (number CAAE 21534919.2.0000.0021). All participants signed informed consent forms.
2.2. Design, Place and Period of Study
This was a prospective, quantitative, epidemiological, observational study evaluating the hematological parameters of patients with chronic PCM before the beginning of treatment and during the healing process.
This study was conducted at the systemic mycoses outpatient clinic of the Infectious and Parasitic Diseases Unit of the Maria Aparecida Pedrossian University Hospital (UNIDIP-HUMAP) of the Federal University of Mato Grosso do Sul (HU-UFMS) in Campo Grande, Mato Grosso do Sul, Brazil, in patients diagnosed between 2013 and 2021.
2.3. Inclusion and Exclusion Criteria
Patients of both sexes with confirmed chronic PCM were included in the study. Exclusion criteria: Patients who did not undergo a blood count at the Service before starting treatment and those presenting comorbidities of infectious, inflammatory or neoplastic etiology.
2.4. Case Definition
Patients with suggestive clinical manifestations and one of the following findings were diagnosed with PCM: a) identification of typical Paracoccidioides spp. yeast forms in clinical samples by direct mycological examination, culture, or histopathological examination; b) detection of specific serum antibodies by the double agar gel immunodiffusion test.
2.5. Clinical and Demographic Data
For this study, clinical data were obtained from a prospectively collected database. Data related to sex, age, history of professional occupations, lifestyle habits, and clinical information such as disease severity and antifungal treatments were systematically collected at admission and during the follow-up. PCM severity was classified as mild, moderate, or severe, as described below [1].
Mild form: a decrease in body mass index (BMI) of less than 5% from the usual value and involvement of one or few organs or tissues without functional changes.
Severe form: three or more of the following criteria: a) loss of BMI of at least 10%; b) severe pulmonary involvement; c) involvement of other organs, such as the adrenal glands, central nervous system and bones; d) enlargement of lymph nodes in multiple chains in the superficial or deep tumoral form (> 2.0 cm in diameter, without suppuration) or in the suppurative form; e) high titers of anti-Paracoccidioides antibodies.
Moderate form: intermediate between the mild and severe forms.
Stages of the study. Laboratory data were obtained at four different stages in relationship to the treatment:
S0 – before treatment;
S1 – after treatment, with some clinical improvement;
S2 – after treatment, presenting clinical cure (disappearance of signs and symptoms of active disease);
S3 – after treatment, presenting serological cure (negative serology by the double agar gel immunodiffusion test, maintained for six months); or at least 12 months of clinical cure in patients with nonreactive serum.
The criteria for clinical and serological cure were those defined by Mendes et al. (2017) [1].
2.6. Laboratory Procedures
During the stages of the disease, the patients underwent the laboratory tests mentioned below.
Complete blood count, determined by the XN 3000-Series hematology analyzer (Sysmex Corporation, Kobe, Japan). Complete blood count parameters of cellular immaturity, evaluated only in patients included after 2017, when the software was available - immature granulocytes (IGs) - myelocytes, metamyelocytes, and promyelocytes, reticulocyte hemoglobin content (Ret-He), the fraction of immature reticulocytes (IRF), and the index of reticulated platelets (RIP). Manual leukocyte differential count performed when the equipment issued an alert.
The reference values adopted for the hematological parameters in this study were in accordance with Hoffbrand and Steensma, 2020., and Pekelharing et al., 2010 specifications [12,13] (Table S1).
Anemia, which was considered when the hemoglobin (Hb) level was <13.0 g/dL for male patients and < 12.0 for female patients.
2.7. Statistical Analysis
Statistical analysis was performed using Jamovi software (version 1.6) for Windows [14]. To determine whether the continuous variables had a normal distribution, the Shapiro‒Wilk test was used. Data that followed a normal distribution are presented as the mean ± standard deviation (SD). Data that did not follow a normal distribution are presented as the median and the first and third quartiles [Q1; Q3]. ANOVA and/or Friedman’s test were used to compare the continuous variables between the different stages (S0, S1, S2, and S3). Wilcoxon’s W test was applied to compare continuous variables in two stages (S0 versus S2). For the categorical variables, the Cochran Q test was used to compare the different stages, and the McNemar test was used for the association between two stages, S0 and S2. For the analysis of numerical variables in a single sample, the t test for one sample were used, respectively. Significance was set up at p < 0.05.
3. Results
A total of 88 patients was diagnosed with chronic PCM between May 2013 and February 2021, with an average of 7.8 new cases of chronic PCM per year. Of this total, 26 patients were excluded according to the criteria presented, and 62 patients participated in the study (Figure 1).
The 62 patients studied presented median age of 54 [49.0; 58.0] years old, and 60 (96.8%) of them were men, 55 (90.2%) farmers or former farmers, and 58 (93.5%) were smokers or former smokers; the moderate severity predominated (n = 37; 59.7%) (Table 1).
During the treatment follow-up, not all the patients showed compliance with the appointments. The median [first quartil; third quartil] time for patients to reach stage 1 was 2 months [1; 3], the stage 2 was 5 months [4.0; 8.5], and the stage 3 was 16 months [13; 25].
3.1. Red Blood Series
The analysis of the red blood series before treatment showed that 58.1% of the patients had at least one change. At this stage, anemia was observed in 28 (45.2%) patients, 21 (75%) of whom presenting the normocytic and normochromic type.
The follow-up of 55 patients showed that the frequency of anemia decreased at S2 (p = 0.008), while the evaluation of 29 patients revealed a tendency to reduce this prevalence along the stages S0-S3 (p = 0.063) (Table 2). The progress of erythrocytes, hemoglobin, hematocrit, MCV, MHC, and CMHC was very similar to that of anemia; except by the erythrocyte count that showed no difference along the stages S0-S3 (Figure 2 and Table S2).
3.2. White Blood Series
3.2.1. Frequency of Alterations
At admission, before the introduction of the treatment, 50 (80.6%) patients presented at least one alteration of the white blood series - leukocytosis: 11(17.7%), monocytosis: 24 (38.7%); lymphopenia: 19 (30.6%); eosinophilia: 15 (24.2%); neutrophilia: 8 (12.9%).
After treatment, the frequency of neutrophilia and monocytosis showed a decrease at the stage of clinical cure (S2), in the 55 cases evaluated (Table 3). However, the frequency of hematological alterations showed no differences in the stages S0 – S3, in the 29 patients under follow-up. A tendency to decrease was observed only with monocytosis (p=0.059) (Table 3).
3.2.2. White Blood Cell Counts
After treatment, a decrease of the leukocytes, neutrophils, and monocyte counts was observed at the stage of clinical cure (S2), in the 55 cases evaluated. (Figure 3 and Table S2). In addition, the neutrophil/lymphocyte ratio and the monocyte/lymphocyte ratio also decreased in the same period. However, no alteration of the cell counts was observed in the stages S0 – S3, in the 29 patients under follow-up. Nevertheless, the monocyte/lymphocyte ratio decreased in the period S0 – S3 (Figure 3 and Table S2).
3.3. Platelet Series
At admission, before treatment, thrombocytosis was present in 9.7% of the patients. During the follow-up, a decrease of the platelet count and platelet/lymphocyte ratio was observed both at the clinical cure, when 55 patients were evaluated, and at the serological cure, in the evaluation of 29 patients (Figure 4 and Table S2).
3.4. Cellular Immaturity
The cellular immaturity, evaluated in the granulocytes and in the red blood series, showed a decrease of the percentage of immature granulocytes (IGs), an increase of the reticulocyte hemoglobin content (Ret-He), and a tendency to the increase of the reticulocyte count (IPF) after reaching the clinical cure - at S3 (Table 4).
3.5. Influence of the Severity of the Paracoccidioidomycosis Patients on the Hematologic Alterations
Patients with the severe clinical form showed higher frequency of anemia than those with the mild and moderate forms, taken together (Table 5).
4. Discussion
Among the complementary laboratory tests, the complete blood count is one of the most requested in clinical practice and is essential in the diagnosis and control of infectious diseases. Abnormalities in blood cellularity before treatment result from the action of the fungus and/or the inflammatory response of the host, and it is expected that with treatment, they will return to normal. Understanding that blood counts aid in the clinical management of PCM, we present the analysis and interpretation of the blood counts of patients with the chronic form of the disease before treatment and during follow-up. This study evaluated the complete blood count and the parameter of cellular immaturity – the immature granulocytes (myelocytes, metamyelocytes and promyelocytes), the reticulocyte hemoglobin content – to assess functional iron deficiency and the reticulocytes production, and the index of reticulated platelets – to evaluate the thrombopoiesis.
The demographic, epidemiological, and clinical characteristics of the participants were similar to those observed in large series of PCM in its endemic area [4,5]: Males, farmers or former farmers, smokers, predominance of the mild/moderate PCM, and the mean age in the fifth decade.
Biological criteria are used to identify PCM cure. Thus, in this study, the different stages of PCM treatment were considered instead of a pre-established time. Improvement in symptoms was observed after approximately two months, reaching clinical cure at about five months after treatment. A similar time interval was also observed in another study [15].
Before treatment, erythrocyte, Hb, and hematocrit (Hct) values were below the reference values in most patients, which may be related to the activation of the immune system by the infectious process, with the release of cytokines such as tumor necrosis factor-α (TNF-α), interferon-γ (IFN-γ), interleukin 6 (IL-6) and interleukin 1 (IL-1). These cytokines inhibit erythropoietin, leading to inadequate production of bone marrow cells, activating phagocytic cells that remove circulating erythrocytes, decreasing their lifespan, and inducing the production of hepcidin and lactoferrin, which promote iron retention in the phagocytic mononuclear system [16]. Infectious and inflammatory processes with a longer course most often progress with the onset of anemia, known as anemia of inflammation (AI) [17]. PCM may also present with normal or low serum iron levels, normal or slightly increased ferritin, transferrin saturation >15% [18,19], low erythropoietin, and high C- reactive preotein (CRP) [20].
Several systemic infections caused by viruses, bacteria, protozoa, or fungi can lead to the emergence of AI [21]. Most tuberculosis patients showed hematological and inflammatory profiles consistent with AI, predominantly of the normochromic and normocytic type [22,23]. Our study showed similar results - anemia was observed in almost half of our patients at diagnosis, with a predominance of the normocytic normochromic type. After antifungal treatment, Hb and Hct increased, and anemia became rarer. Considering that anemia in PCM is, in general, an AI, the analysis of ferritin and transferrin saturation is recommended before starting iron supplementation since it can be harmful to the patient by favoring fungal growth, which depends on iron for its metabolism [24].
In automated equipment, the Ret-He parameter is an index that indicates the onset of iron deficiency in the body, assessing its incorporation into reticulocytes and contributing to the analyze of its status. Under conditions in which Hb synthesis is compromised, such as in AI, Ret-He may decrease [25]. In the present study, the mean values significantly increased with treatment.
Some leukocyte alterations were observed before treatment, especially monocytosis. Leukocytosis and neutrophilia were found only in a small percentage of patients The defense mechanism against infection is not simple and requires the involvement of many cells of the immune system, such as phagocytic cells—monocytes and neutrophils—which are the first line of defense of the body against infection by the fungus [26,27]. The role of neutrophils in PCM is still not entirely clear because while its phagocytic function is preserved, they fail to digest both P. brasiliensis yeast forms and conidia [28,29]. Although these cells are the first in the process of diapedesis to the site of infection, in PCM a persistence of neutrophils is observed in the tissue lesions caused by the fungus in the later stages of the disease. This fact has demonstrated the presence of neutrophils around the fungus in the chronic phase of PCM in infected mice [30] and in biopsied tissue [31]. Neutrophils also play a key role in the acquired immune response through the synthesis of pro-inflammatory cytokines, which help to mount a more efficient adaptive immune response [32].
IGs, one of the automated evaluation of the neutrophil precursor cells, were not above normal values before treatment but showed decrease upon clinical cure, suggesting involvement in the response to paracoccidioidal infection.
Although monocytosis was observed in less than a half of the patients before treatment, the blood monocytes count decreases after introduction of the antifungal compound. A previous study of patients with chronic PCM demonstrated that the blood monocytes count was higher than that of healthy individuals [10]. These findings demonstrate that these cells play a role in the response to the paracoccidioidal infection, confirming previous findings – monocytes and macrophages play a key role in phagocytosis, in both the innate and acquired immune response and are activated by cytokines, which can control the multiplication of the fungus [33]. In addition, the blood monocytes are attracted into the infected tissue by Paracoccidioides spp., where they undergo changes, but carrying out anti-paracoccidioidal activities and immune response [34].
The alterations of the lymphocytes count were few – a small percentage of lymphopenia and no lymphocytosis. However, an increase in the lymphocyte count was observed after specific antifungal treatment. These findings suggest that the functional compromise could be more relevant than the numerical ones. In addition, the few cases of lymphopenia in chronic PCM could be related to the reduction of the CD4+ subpopulation in the blood and high concentration of these cells in tissue granulomas [26,35].
The occurrence of eosinophilia in PCM patients is related to the high production of IL-5 interleukin due to the activation of the Th2 subpopulation [26], and has been reported mainly in the acute/subacute form [36,37]. As this study focused predominantly on cases of the mild or moderate chronic form, this finding was not awaited. In addition, intestinal parasitic diseases, which are known causes of eosinophilia - especially strongyloidiasis, have been frequently associated with PCM [6] but were not routinely investigated.
Thrombocytosis was observed only in less than 10% of the patients before treatment, but the decrease in platelet counts after treatment suggested an interference of PCM on this finding. Gorelik et al. (2017) [38] observed that the increased synthesis of the cytokines IL-3, IL-6, IL-11, and IFN-γ led to increased production of platelets in the bone marrow due to the stimulation of thrombopoietin. Platelets are also found at the site of tissue injury and play a role as immune cells in the parasite–host interaction, leading to platelet activation. This activation induces the release of several molecules, such as chemokines, cytokines [39] and proteins with antimicrobial action [40]. In addition, platelet activation leads to an increase in the adaptive immune response by activating phagocytic cells and their recruitment to the site of infection [39,41].
Due to the instability of leukocyte cells in infection/inflammation, the ratios between cells such as neutrophils/lymphocytes (NLR), monocytes/lymphocytes (MLR) and platelets/lymphocytes have been used as prognostic biomarkers in neoplasias [42] and in systemic inflammation [43]. Recently, in PCM caused by P. lutzii, the association of NLR with disease severity was reported, showing that it can be used as a biomarker of severity in PCM [44]. In the present study, the NLR, MLR and PLR ratios were evaluated, but no association was found between the cellular ratios and the severity of chronic PCM. However, there was a significant reduction in the healing process in MLR and PLR, reflecting the reduction of monocytes and platelets after treatment starting, respectively.
The main limitation of this study was the relatively small number of patients studied because of the low annual incidence of PCM [45]. Nevertheless, this is one of the few publications on hemogram that evaluated the data during the patients follow-up of the treatment.
5. Conclusion
Alterations of the blood count cells seems to be not so frequent nor so intense at admission of PCM patients with the chronic form, characterized by anemia and monocytosis. However, the follow-up of the patients under treatment shows other important alterations of the immature cells, including IGs and Ret-He, which could be explained by the immune response to the infection. The evaluation of this hematological dynamics, easy to perform and available in the clinical laboratories, helps the management of PCM patients.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, E.C.A.B., S.S.W. and A.M.M.P.; Methodology, E.C.A.B., S.S.W. and A.M.M.P.; Validation, A.M.M.P.; Formal Analysis, E.C.A.B., R.P.M. and A.M.M.P.; Investigation, E.C.A.B., A.O.F., I.V.S., V.L.T.F., A.A.R., B.C.A., S.E.R.S.; Resources, A.M.M.P.; Data Curation, E.C.A.B., and A.M.M.P.; Writing – Original Draft Preparation, E.C.A.B., R.P.M., S.S.W. and A.M.M.P.; Writing – Review, R.P.M.; Visualization, E.C.A.B., S.S.W. and A.M.M.P.; Supervision, Project Administration, and Funding Acquisition, A.M.M.P. All authors have read and agreed to the published version of the manuscript.
Funding
Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) – Código de Financiamento 001; Ministério da Ciência, Tecnologia e Inovação and Conselho Nacional de Desenvolvimento Científico e Tecnológico (grant numbers: 312910/2020–7 and 431,776/2016–4); Fundação de Apoio ao Desenvolvimento do Ensino, Ciência e Tecnologia do Estado de Mato Grosso do Sul (grant number: 71/000.478/2021); Universidade Federal do Mato Grosso do Sul.
Institutional Review Board Statement
This project was approved by the Committee of Ethics in Research with Human Beings of the Federal University of Mato Grosso do Sul (CEP - UFMS) (number CAAE 21534919.2.0000.0021).
Informed Consent Statement
All participants signed informed consent forms.
Data Availability Statement
Data are contained within the article and Supplementary Materials.
Acknowledgments
The authors thank the study participants and the team of health professionals from the Infectious and Parasitic Diseases Unit (UDIP) at Maria Aparecida Pedrossian University Hospital of the Federal University of Mato Grosso do Sul for their support in this Project.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mendes, R.P.; Cavalcante, R. de S.; Marques, S.A.; Marques, M.E.A.; Venturini, J.; Sylvestre, T.F.; Paniago, A.M.M.; Pereira, A.C.; da Silva, J. de F.; Fabro, A.T.; et al. Paracoccidioidomycosis: Current Perspectives from Brazil. TOMICROJ 2017, 11, 224–282. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, Z.F.; Silva, D. da; Lazéra, M.; Petri, V.; Oliveira, R.M. de; Sabroza, P.C.; Wanke, B. Paracoccidioidomycosis Mortality in Brazil (1980-1995). Cad. Saúde Pública 2002, 18, 1441–1454. [Google Scholar] [CrossRef]
- Londero, A.T. Paracoccidioidomicose: Patogenia, Formas Clínicas, Manifestações Pulmonares e Diagnóstico. 1986, 2, 41–57.
- Bellissimo-Rodrigues, F.; Bollela, V.R.; Da Fonseca, B.A.L.; Martinez, R. Endemic Paracoccidioidomycosis: Relationship between Clinical Presentation and Patients’ Demographic Features. Med Mycol 2013, 51, 313–318. [Google Scholar] [CrossRef] [PubMed]
- Matos, W.B. de; Santos, G.M.C. dos; Silva, V.E.B. da; Gonçalves, E. da G. do R.; Silva, A.R. da Paracoccidioidomycosis in the State of Maranhão, Brazil: Geographical and Clinical Aspects. Rev. Soc. Bras. Med. Trop. 2012, 45, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Paniago, A.M.M.; Aguiar, J.I.A.; Aguiar, E.S.; Cunha, R.V. da; Pereira, G.R. de O.L.; Londero, A.T.; Wanke, B. Paracoccidioidomicose: Estudo Clínico e Epidemiológico de 422 Casos Observados No Estado de Mato Grosso Do Sul. Rev. Soc. Bras. Med. Trop. 2003, 36, 455–459. [Google Scholar] [CrossRef]
- Pereira, R.M.; Bucaretchi, F.; Barison, E. de M.; Hessel, G.; Tresoldi, A.T. Paracoccidioidomycosis in Children: Clinical Presentation, Follow-up and Outcome. Rev. Inst. Med. trop. S. Paulo 2004, 46, 127–131. [Google Scholar] [CrossRef]
- de Oliveira Custódio, J.M.; Enokida, I.M.; Gonçalves, D.A.; Leone de Oliveira, S.M. do V.; Venturini, J.; Carvalho, L.R.; Mendes, R.P.; Paniago, A.M.M. Dynamics of Plasma Micronutrient Concentrations and Their Correlation with Serum Proteins and Thyroid Hormones in Patients with Paracoccidioidomycosis. PLoS ONE 2019, 14, e0226609. [Google Scholar] [CrossRef]
- Doedens, A.L.; Phan, A.T.; Stradner, M.H.; Fujimoto, J.K.; Nguyen, J.V.; Yang, E.; Johnson, R.S.; Goldrath, A.W. Hypoxia-Inducible Factors Enhance the Effector Responses of CD8+ T Cells to Persistent Antigen. Nat Immunol 2013, 14, 1173–1182. [Google Scholar] [CrossRef]
- Venturini, J.; Cavalcante, R.S.; de Assis Golim, M.; Marchetti, C.M.; de Azevedo, P.Z.; Amorim, B.C.; de Arruda, M.S.P.; Mendes, R.P. Phenotypic and Functional Evaluations of Peripheral Blood Monocytes from Chronic-Form Paracoccidioidomycosis Patients before and after Treatment. BMC Infect Dis 2014, 14, 552. [Google Scholar] [CrossRef]
- Xu, Y.; Chaudhury, A.; Zhang, M.; Savoldo, B.; Metelitsa, L.S.; Rodgers, J.; Yustein, J.T.; Neilson, J.R.; Dotti, G. Glycolysis Determines Dichotomous Regulation of T Cell Subsets in Hypoxia. Journal of Clinical Investigation 2016, 126, 2678–2688. [Google Scholar] [CrossRef]
- Hoffbrand, A.V.; Steensma, D.P. Hoffbrand’s Essential Haematology; Eighth edition.; John Wiley & Sons Ltd.: Hoboken, NJ, 2020; ISBN 978-1-119-49595-6. [Google Scholar]
- Pekelharing, J.M.; Hauss, O.; Jonge, R. de; Lokhof, J.; Sodikromo, J.; Spaans, M.; Brouwer, R.; Lathouder, S. de; Hinzmann, R. Haematology Reference Intervals for Established and Novel Parameters in Healthy Adults. Sysmex J Int. 2010, 20, 01–11. [Google Scholar]
- The jamovi project Jamovi; 2021.
- Cavalcante, R. de S.; Sylvestre, T.F.; Levorato, A.D.; de Carvalho, L.R.; Mendes, R.P. Comparison between Itraconazole and Cotrimoxazole in the Treatment of Paracoccidiodomycosis. PLoS Negl Trop Dis 2014, 8, e2793. [Google Scholar] [CrossRef]
- Weiss, G.; Ganz, T.; Goodnough, L.T. Anemia of Inflammation. Blood 2019, 133, 40–50. [Google Scholar] [CrossRef]
- Cartwright, G.E. The Anemia of Chronic Disorders. Semin Hematol 1966, 3, 351–375. [Google Scholar]
- Guralnik, J.M.; Eisenstaedt, R.S.; Ferrucci, L.; Klein, H.G.; Woodman, R.C. Prevalence of Anemia in Persons 65 Years and Older in the United States: Evidence for a High Rate of Unexplained Anemia. Blood 2004, 104, 2263–2268. [Google Scholar] [CrossRef] [PubMed]
- de Brito, E. da C.A.; Siqueira, I.V.; Venturini, J.; Félix, V.L.T.; dos Santos, A.O.G.M.; Mendes, R.P.; Weber, S.S.; Paniago, A.M.M. Iron Metabolism Disorders of Patients with Chronic Paracoccidioidomycosis. PLoS ONE 2023, 18, e0282218. [Google Scholar] [CrossRef]
- van Iperen, C.E.; Gaillard, C.A.J.M.; Kraaijenhagen, R.J.; Braam, B.G.; Marx, J.J.M.; van de Wiel, A. Response of Erythropoiesis and Iron Metabolism to Recombinant Human Erythropoietin in Intensive Care Unit Patients. Critical Care Medicine 2000, 28, 2773–2778. [Google Scholar] [CrossRef] [PubMed]
- Ganz, T.; Nemeth, E. Iron Sequestration and Anemia of Inflammation. Seminars in Hematology 2009, 46, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Kang, Y.A.; Yoon, Y.S.; Um, S.-W.; Lee, S.M.; Yoo, C.-G.; Kim, Y.W.; Han, S.K.; Shim, Y.-S.; Yim, J.-J. The Prevalence and Evolution of Anemia Associated with Tuberculosis. J Korean Med Sci 2006, 21, 1028. [Google Scholar] [CrossRef]
- Minchella, P.A.; Donkor, S.; Owolabi, O.; Sutherland, J.S.; McDermid, J.M. Complex Anemia in Tuberculosis: The Need to Consider Causes and Timing When Designing Interventions. Clinical Infectious Diseases 2015, 60, 764–772. [Google Scholar] [CrossRef]
- Bailão, E.F.L.C.; Parente, J.A.; Pigosso, L.L.; Castro, K.P. de; Fonseca, F.L.; Silva-Bailão, M.G.; Báo, S.N.; Bailão, A.M.; Rodrigues, M.L.; Hernandez, O.; et al. Hemoglobin Uptake by Paracoccidioides Spp. Is Receptor-Mediated. PLoS Negl Trop Dis 2014, 8, e2856. [Google Scholar] [CrossRef] [PubMed]
- Chinudomwong, P.; Binyasing, A.; Trongsakul, R.; Paisooksantivatana, K. Diagnostic Performance of Reticulocyte Hemoglobin Equivalent in Assessing the Iron Status. Clinical Laboratory Analysis 2020, 34, e23225. [Google Scholar] [CrossRef]
- Benard, G. An Overview of the Immunopathology of Human Paracoccidioidomycosis. Mycopathologia 2008, 165, 209–221. [Google Scholar] [CrossRef]
- Loures, F.V.; Pina, A.; Felonato, M.; Araújo, E.F.; Leite, K.R.M.; Calich, V.L.G. Toll-like Receptor 4 Signaling Leads to Severe Fungal Infection Associated with Enhanced Proinflammatory Immunity and Impaired Expansion of Regulatory T Cells. Infect Immun 2010, 78, 1078–1088. [Google Scholar] [CrossRef] [PubMed]
- Goihman-Yahr, M.; Rothenberg, A.; Bretaña, A.; Istúriz, G.; Rosquete, R.; Avila-Millán, E.; Viloria, N.; de Borges, N.S.; Carrasquero, M.; de Fernández, B.P.; et al. Digestion of Killed Paracoccidioides Brasiliensis by Neutrophils. Mycopathologia 1989, 106, 53–58. [Google Scholar] [CrossRef]
- Schaffner, A.; Davis, C.E.; Schaffner, T.; Markert, M.; Douglas, H.; Braude, A.I. In Vitro Susceptibility of Fungi to Killing by Neutrophil Granulocytes Discriminates between Primary Pathogenicity and Opportunism. J. Clin. Invest. 1986, 78, 511–524. [Google Scholar] [CrossRef]
- Xidieh, C.F.; Lenzi, H.L.; Calich, V.L.G.; Burger, E. Influence of the Genetic Background on the Pattern of Lesions Developed by Resistant and Susceptible Mice Infected with Paracoccidioides Brasiliensis. Medical Microbiology and Immunology 1999, 188, 41–49. [Google Scholar] [CrossRef]
- Franco, M.; Peracoli, M.T.; Soares, A.; Montenegro, R.; Mendes, R.P.; Meira, D.A. Host-Parasite Relationship in Paracoccidioidomycosis. Curr Top Med Mycol 1993, 5, 115–149. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, F.; Miyazaki, S. New Biodefense Strategies by Neutrophils. Arch Immunol Ther Exp (Warsz) 2005, 53, 226–233. [Google Scholar] [PubMed]
- Moscardi-Bacchi, M.; Brummer, E.; Stevens, D.A. Support of Paracoccidioides Brasiliensis Multiplication by Human Monocytes or Macrophages: Inhibition by Activated Phagocytes. Journal of Medical Microbiology 1994, 40, 159–164. [Google Scholar] [CrossRef]
- Calvi, S.A.; Soares, A.M.V.C.; Peraçoli, M.T.S.; Franco, M.; Ruiz, R.L.; Marcondes-Machado, J.; Fecchio, D.; Mattos, M.C.I.; Mendes, R.P. Study of Bronchoalveolar Lavage Fluid in Paracoccidioidomycosis: Cytopathology and Alveolar Macrophage Function in Response to Gamma Interferon; Comparison with Blood Monocytes. Microbes and Infection 2003, 5, 1373–1379. [Google Scholar] [CrossRef]
- Bava, A.J.; Mistchenko, A.S.; Palacios, M.F.; Estevez, M.E.; Tiraboschi, N.I.; Sen, L.; Negroni, R.; Diez, R.A. Lymphocyte Subpopulations and Cytokine Production in Paracoccidioidomycosis Patients. Microbiology and Immunology 1991, 35, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Braga, F.G.; Ruas, L.P.; Pereira, R.M.; Lima, X.T.; Antunes, E.; Mamoni, R.L.; Blotta, M.H.S.L. Functional and Phenotypic Evaluation of Eosinophils from Patients with the Acute Form of Paracoccidioidomycosis. PLoS Negl Trop Dis 2017, 11, e0005601. [Google Scholar] [CrossRef] [PubMed]
- Shikanai-Yasuda, M.A.; Higaki, Y.; Uip, D.E.; Mori, N.S.; Del Negro, G.; Melo, N.T.; Hutzler, R.U.; Amato Neto, V. Comprometimento Da Medula Óssea e Eosinofilia Na Paracoccidioidomicose. Rev. Inst. Med. trop. S. Paulo 1992, 34, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Gorelik, O.; Izhakian, S.; Barchel, D.; Almoznino-Sarafian, D.; Tzur, I.; Swarka, M.; Beberashvili, I.; Feldman, L.; Cohen, N.; Shteinshnaider, M. Prognostic Significance of Platelet Count Changes during Hospitalization for Community-Acquired Pneumonia. Platelets 2017, 28, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Semple, J.W.; Freedman, J. Platelets and Innate Immunity. Cell Mol Life Sci 2010, 67, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.; Kerrigan, S.W.; Watson, S.P. Platelets and the Innate Immune System: Mechanisms of Bacterial-Induced Platelet Activation. J Thromb Haemost 2011, 9, 1097–1107. [Google Scholar] [CrossRef] [PubMed]
- Pitchford, S.; Pan, D.; Welch, H.C.E. Platelets in Neutrophil Recruitment to Sites of Inflammation. Curr Opin Hematol 2017, 24, 23–31. [Google Scholar] [CrossRef]
- Morales, M.; Xue, X. Targeting Iron Metabolism in Cancer Therapy. Theranostics 2021, 11, 8412–8429. [Google Scholar] [CrossRef]
- Abakay, O.; Abakay, A.; Sen, H.S.; Tanrikulu, A.C. The Relationship Between Inflammatory Marker Levels and Pulmonary Tuberculosis Severity. Inflammation 2015, 38, 691–696. [Google Scholar] [CrossRef]
- Nery, A.F.; de Camargo, Z.P.; Rodrigues, A.M.; Portela, T.F.; Hoffmann-Santos, H.D.; Pinheiro, B.G.; Possa, A.P.; Cavalcante, L.R. da S.; Hagen, F.; Hahn, R.C. Puzzling Paracoccidioidomycosis: Factors Associated with the Severity of Paracoccidioides Lutzii Infections. Int J Infect Dis 2021, 107, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Coutinho, Z.F.; Wanke, B.; Travassos, C.; Oliveira, R.M.; Xavier, D.R.; Coimbra, C.E.A. Hospital Morbidity Due to Paracoccidioidomycosis in Brazil (1998-2006). Trop Med Int Health 2015, 20, 673–680. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of the selection of patients with the chronic form of paracoccidioidomycosis diagnosed in the Federal University of Mato Grosso do Sul, School of Medicine from 2013 to 2021. n: number of patients; S0 – before treatment; S1 - between the beginning of treatment and after clinical improvement; S2 - clinical cure; S3 - serological cure.
Figure 1.
Flowchart of the selection of patients with the chronic form of paracoccidioidomycosis diagnosed in the Federal University of Mato Grosso do Sul, School of Medicine from 2013 to 2021. n: number of patients; S0 – before treatment; S1 - between the beginning of treatment and after clinical improvement; S2 - clinical cure; S3 - serological cure.
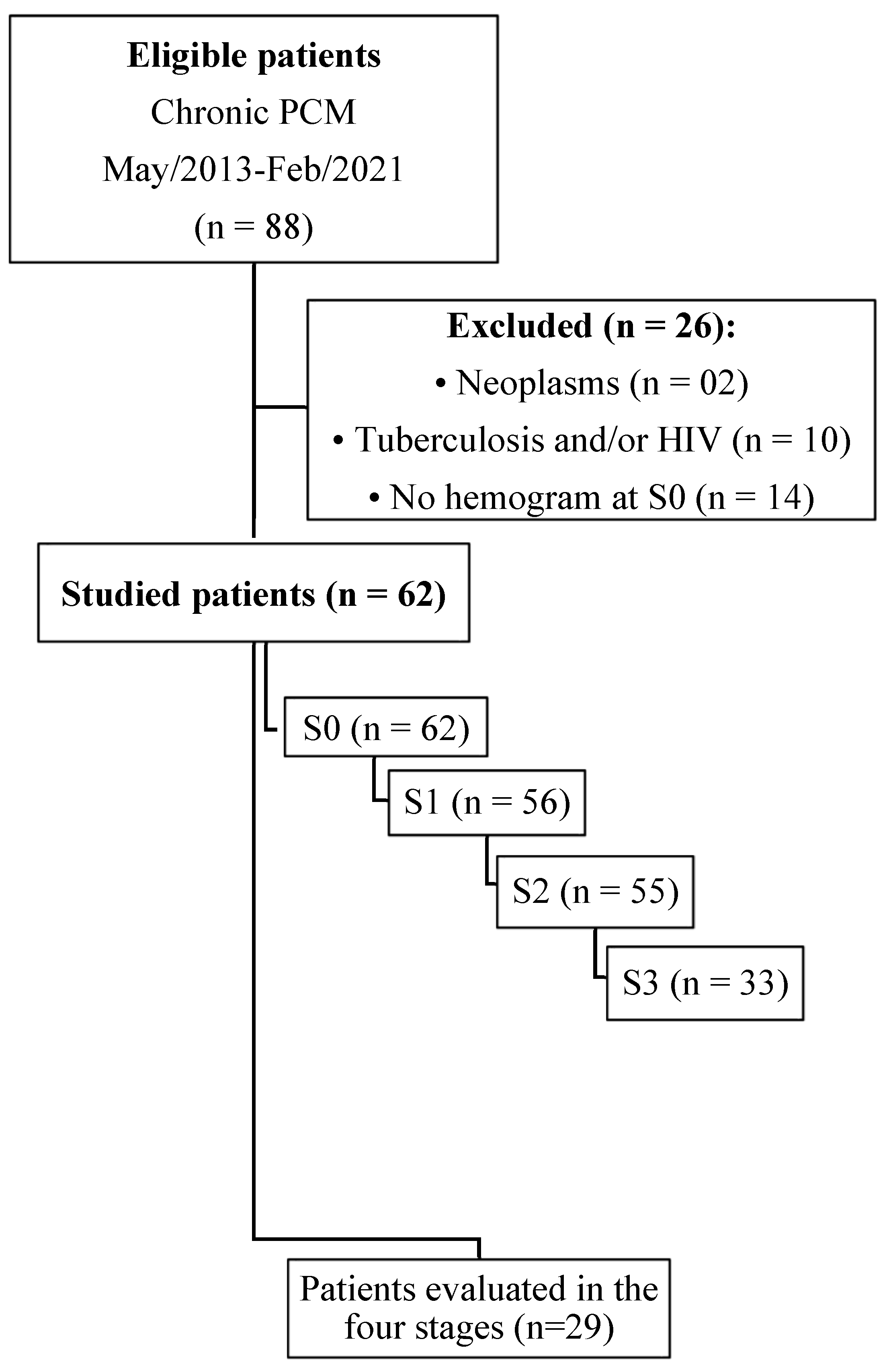
Figure 2.
Evaluation of the alterations observed in the blood red cells before treatment and its progress after introduction of the antifungal compounds. (A) Comparison of the erythrocyte values before treatment and at clinical cure; (B) Comparison of the erythrocyte values between the different stages; (C) Comparison of the hematocrit values before treatment and at clinical cure; (D) Comparison of the hematocrit values between the different stages; (E) Comparison of the hemoglobin values before treatment and at clinical cure; (F) Comparison of the hemoglobin values between the different stages. n: number of patients; S0 – before treatment; S1 - between the beginning of treatment and after clinical improvement; S2 – at clinical cure; S3 – at serological cure. Statistical analysis: Wilcoxon W test; Friedman test – post hoc (Durbin-Conover). Lower-case letters compare medians, different letters are statistically significant differences (p≤0.05), while medians followed by the same letter or not followed by any letter do not differ (p>0.05).
Figure 2.
Evaluation of the alterations observed in the blood red cells before treatment and its progress after introduction of the antifungal compounds. (A) Comparison of the erythrocyte values before treatment and at clinical cure; (B) Comparison of the erythrocyte values between the different stages; (C) Comparison of the hematocrit values before treatment and at clinical cure; (D) Comparison of the hematocrit values between the different stages; (E) Comparison of the hemoglobin values before treatment and at clinical cure; (F) Comparison of the hemoglobin values between the different stages. n: number of patients; S0 – before treatment; S1 - between the beginning of treatment and after clinical improvement; S2 – at clinical cure; S3 – at serological cure. Statistical analysis: Wilcoxon W test; Friedman test – post hoc (Durbin-Conover). Lower-case letters compare medians, different letters are statistically significant differences (p≤0.05), while medians followed by the same letter or not followed by any letter do not differ (p>0.05).
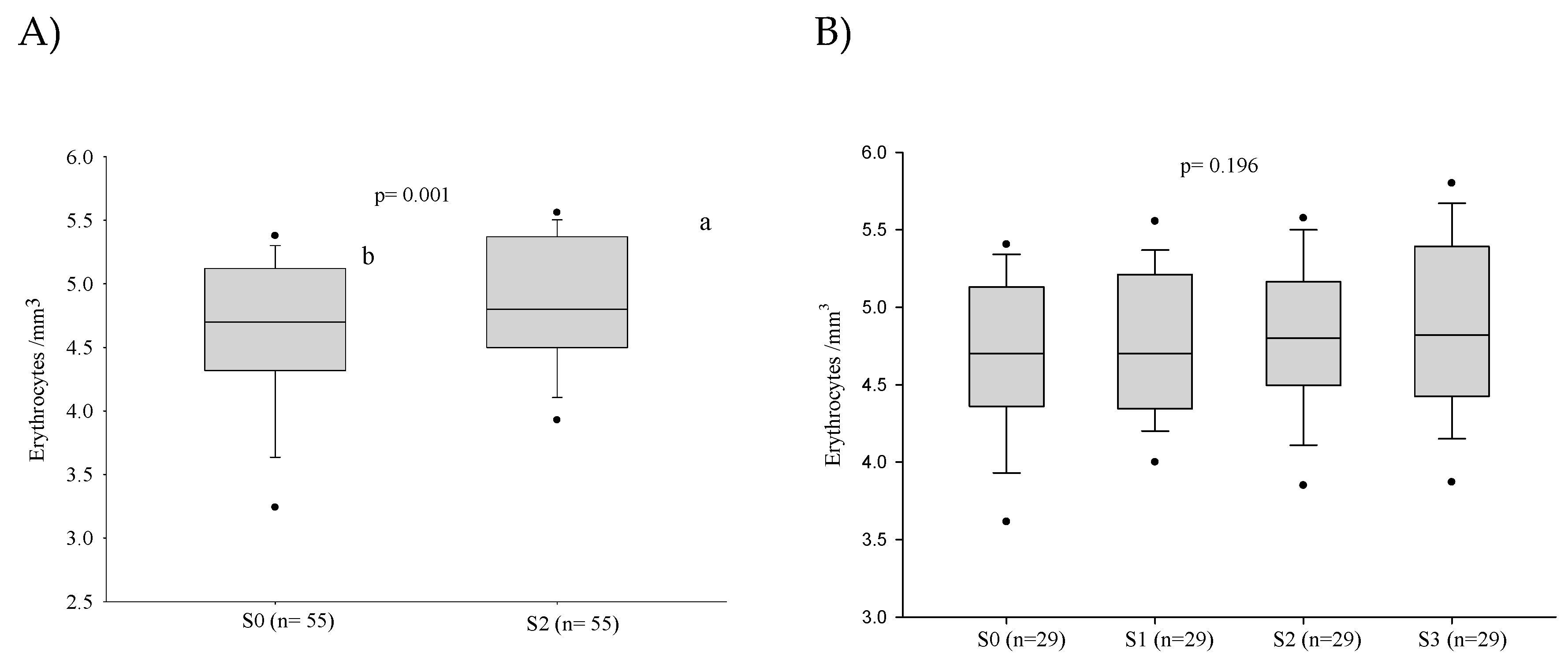
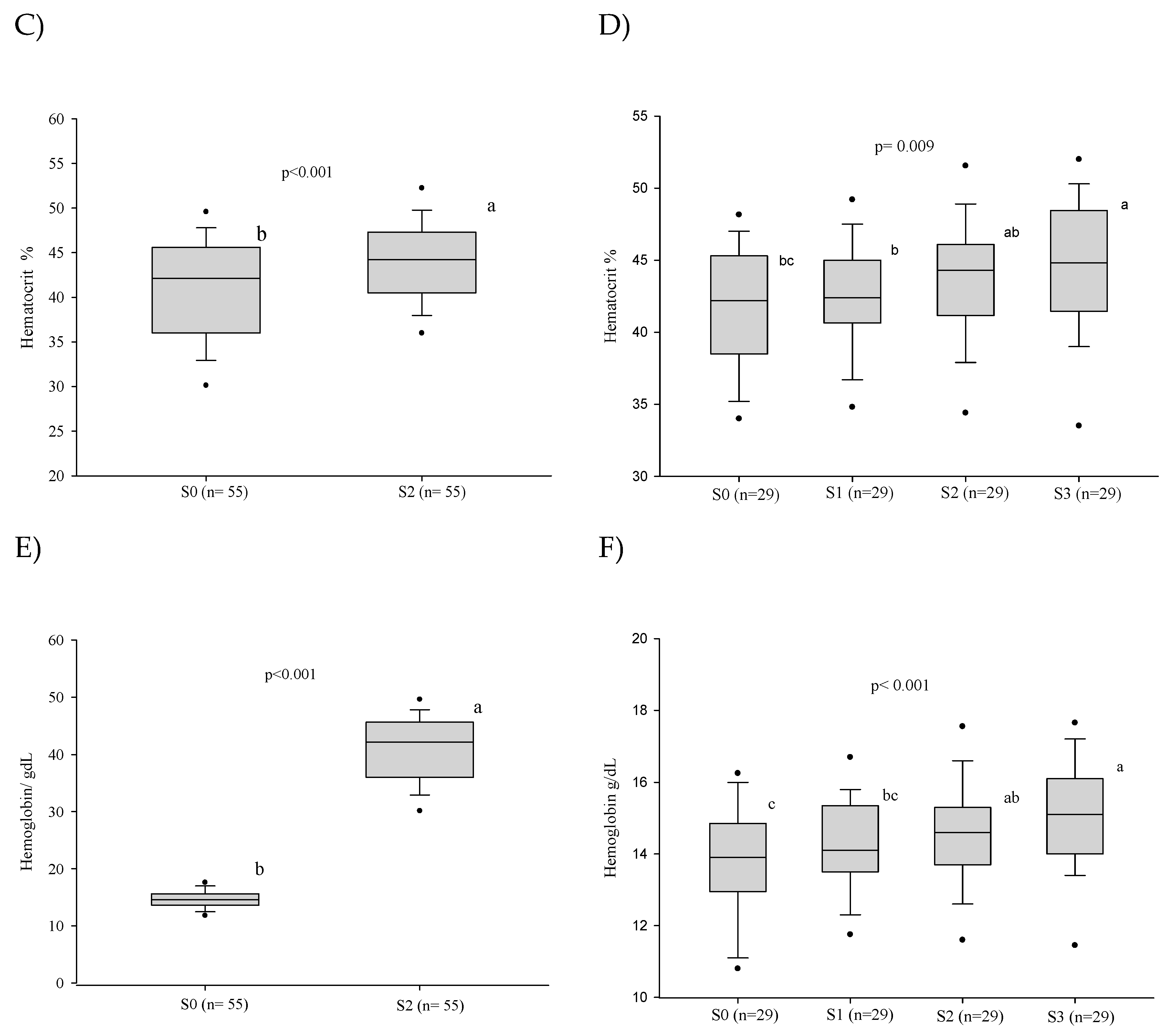
Figure 3.
Evaluation of the alterations observed in the white blood cells count (in number per cubic millimeter) before treatment and its progress after introduction of the antifungal compounds. (A) Comparison of the leukocytes values before treatment and at clinical cure; (B) Comparison of the leukocytes values between the different stages; (C) Comparison of the monocytes values before treatment and at clinical cure; (D) Comparison of the monocytes values between the different stages; (E) Comparison of the neutrophils values before treatment and at clinical cure; (F) Comparison of the neutrophils values between the different stages; (G) Comparison of the MLR values before treatment and at clinical cure; (H) Comparison of the MLR values between the different stages; (I) Comparison of the NLR values before treatment and at clinical cure; (J) Comparison of the NLR values between the different stages. n: number of patients; NLR: neutrophil/lymphocyte ratio; MLR: monocyte/lymphocyte ratio; S0 – before treatment; S1 - between the beginning of treatment and after clinical improvement; S2 - clinical cure; S3 - serological cure. Statistical analysis: Wilcoxon W test or paired Student’s t test; ANOVA – post hoc (Tukey), Friedman test – post hoc (Durbin-Conover). Lower-case letters compare medians; different letters indicate differences statistically significant (p≤0.05), while means followed by the same letter or not followed by any letter do not differ (p>0.05).
Figure 3.
Evaluation of the alterations observed in the white blood cells count (in number per cubic millimeter) before treatment and its progress after introduction of the antifungal compounds. (A) Comparison of the leukocytes values before treatment and at clinical cure; (B) Comparison of the leukocytes values between the different stages; (C) Comparison of the monocytes values before treatment and at clinical cure; (D) Comparison of the monocytes values between the different stages; (E) Comparison of the neutrophils values before treatment and at clinical cure; (F) Comparison of the neutrophils values between the different stages; (G) Comparison of the MLR values before treatment and at clinical cure; (H) Comparison of the MLR values between the different stages; (I) Comparison of the NLR values before treatment and at clinical cure; (J) Comparison of the NLR values between the different stages. n: number of patients; NLR: neutrophil/lymphocyte ratio; MLR: monocyte/lymphocyte ratio; S0 – before treatment; S1 - between the beginning of treatment and after clinical improvement; S2 - clinical cure; S3 - serological cure. Statistical analysis: Wilcoxon W test or paired Student’s t test; ANOVA – post hoc (Tukey), Friedman test – post hoc (Durbin-Conover). Lower-case letters compare medians; different letters indicate differences statistically significant (p≤0.05), while means followed by the same letter or not followed by any letter do not differ (p>0.05).
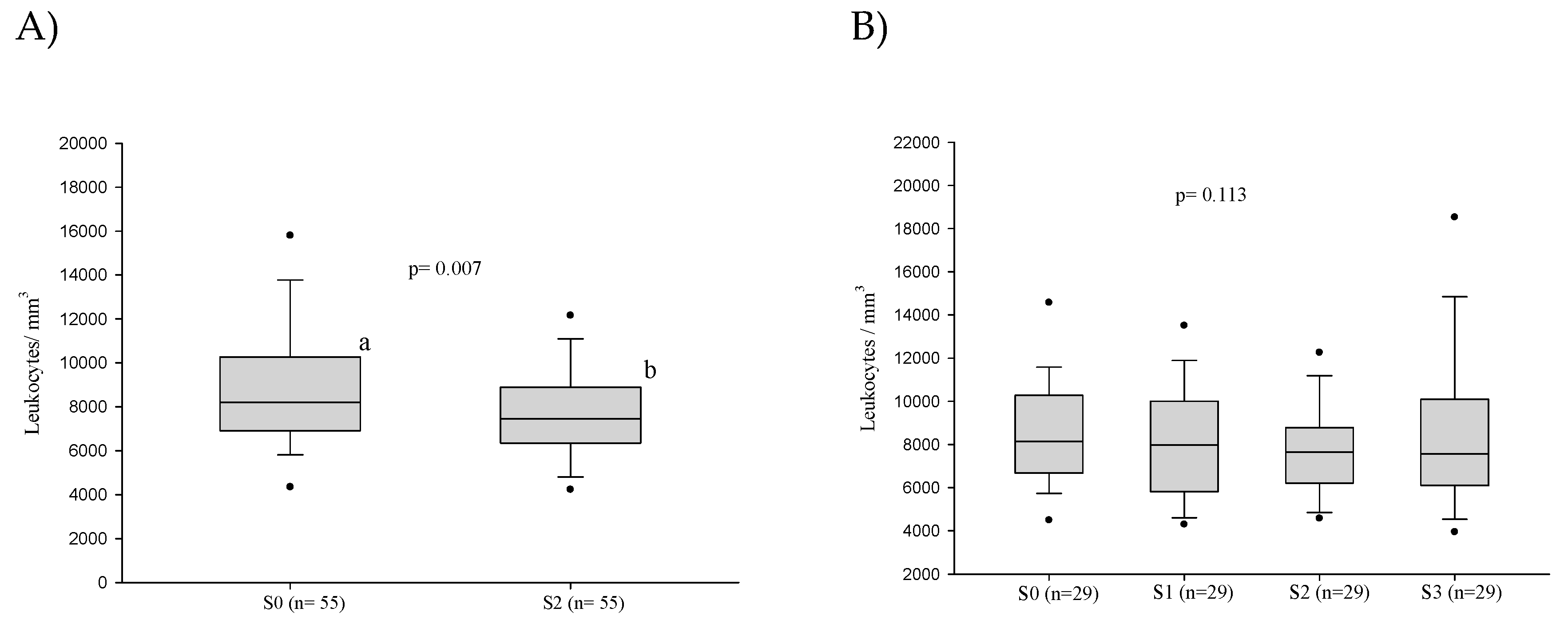
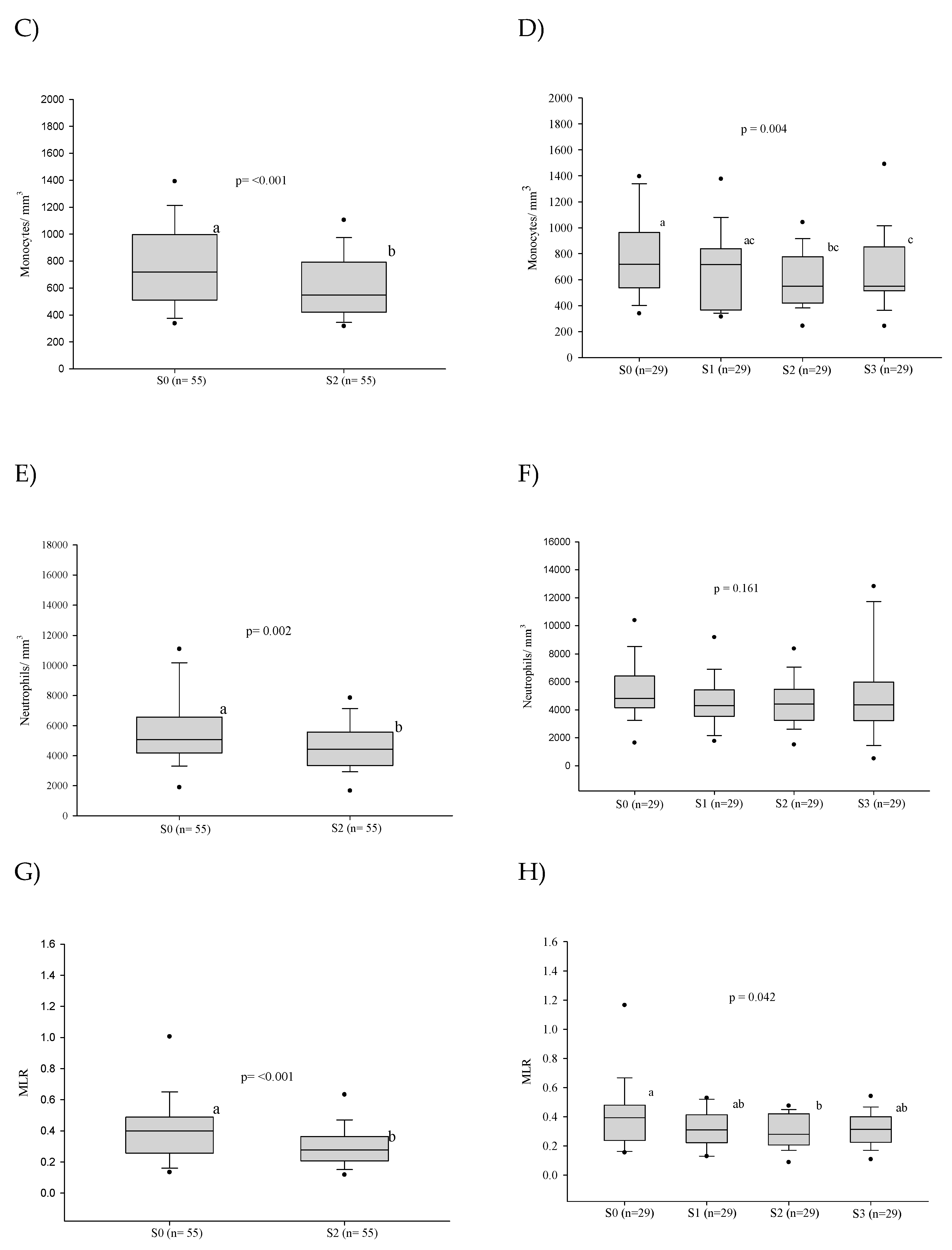
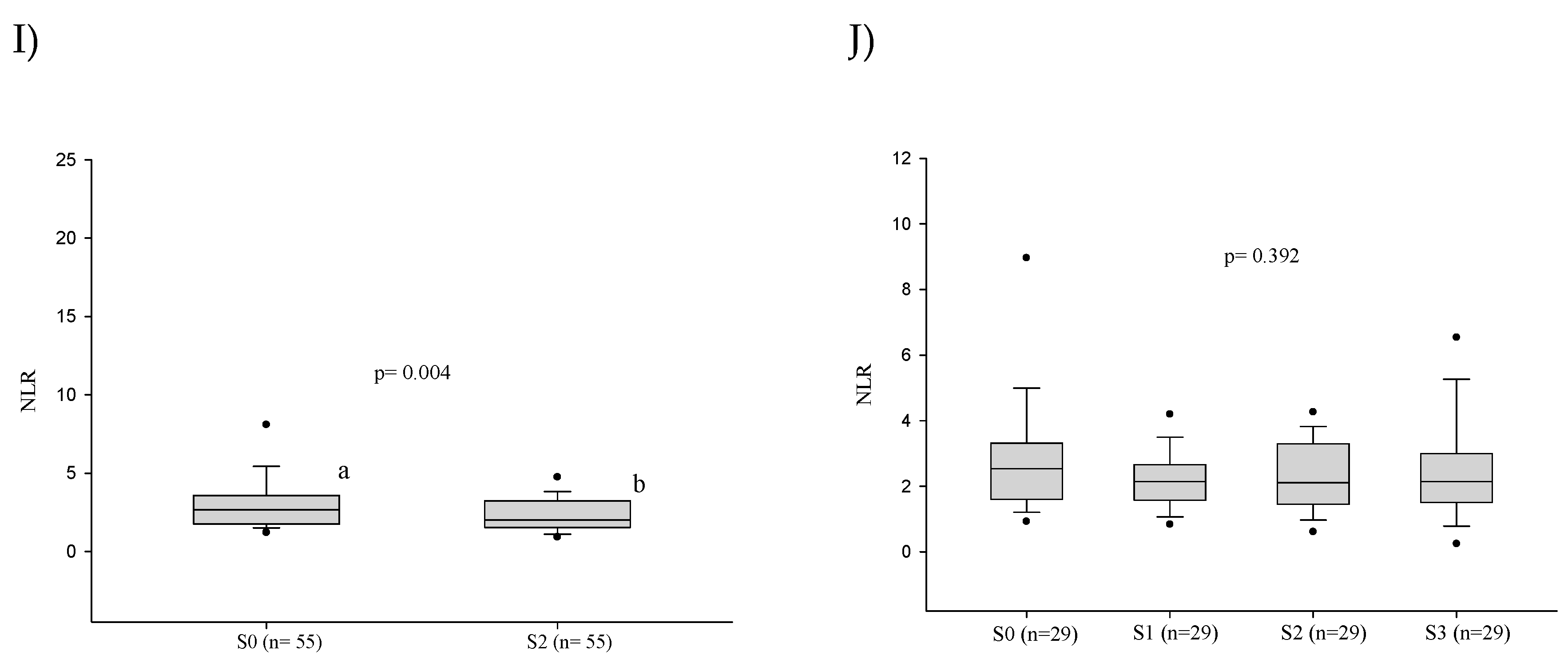
Figure 4.
Evaluation of the platelets count and the platelet/lymphocyte ratio before treatment and its progress after introduction of the antifungal compounds. (A) Comparison of the platelet values before treatment and at clinical cure; (B) Comparison of the platelet values between the different stages; (C) Comparison of the PLR values before treatment and at clinical cure; (D) Comparison of the PLR values between the different stages. n: number of patients; PLR: platelet/lymphocyte ratio; Platelet count: number x103/cubic millimeter; S0 – before treatment; S1 - between the beginning of treatment and after clinical improvement; S2 - clinical cure; S3 - serological cure. Statistical analysis: Wilcoxon W test or paired Student’s t test; ANOVA test – post hoc (Tukey), Friedman test – post hoc (Durbin-Conover). Lower-case letters compare medians; different letters indicate differences statistically significant (p≤0.05), while means followed by the same letter or not followed by any letter do not differ (p>0.05).
Figure 4.
Evaluation of the platelets count and the platelet/lymphocyte ratio before treatment and its progress after introduction of the antifungal compounds. (A) Comparison of the platelet values before treatment and at clinical cure; (B) Comparison of the platelet values between the different stages; (C) Comparison of the PLR values before treatment and at clinical cure; (D) Comparison of the PLR values between the different stages. n: number of patients; PLR: platelet/lymphocyte ratio; Platelet count: number x103/cubic millimeter; S0 – before treatment; S1 - between the beginning of treatment and after clinical improvement; S2 - clinical cure; S3 - serological cure. Statistical analysis: Wilcoxon W test or paired Student’s t test; ANOVA test – post hoc (Tukey), Friedman test – post hoc (Durbin-Conover). Lower-case letters compare medians; different letters indicate differences statistically significant (p≤0.05), while means followed by the same letter or not followed by any letter do not differ (p>0.05).
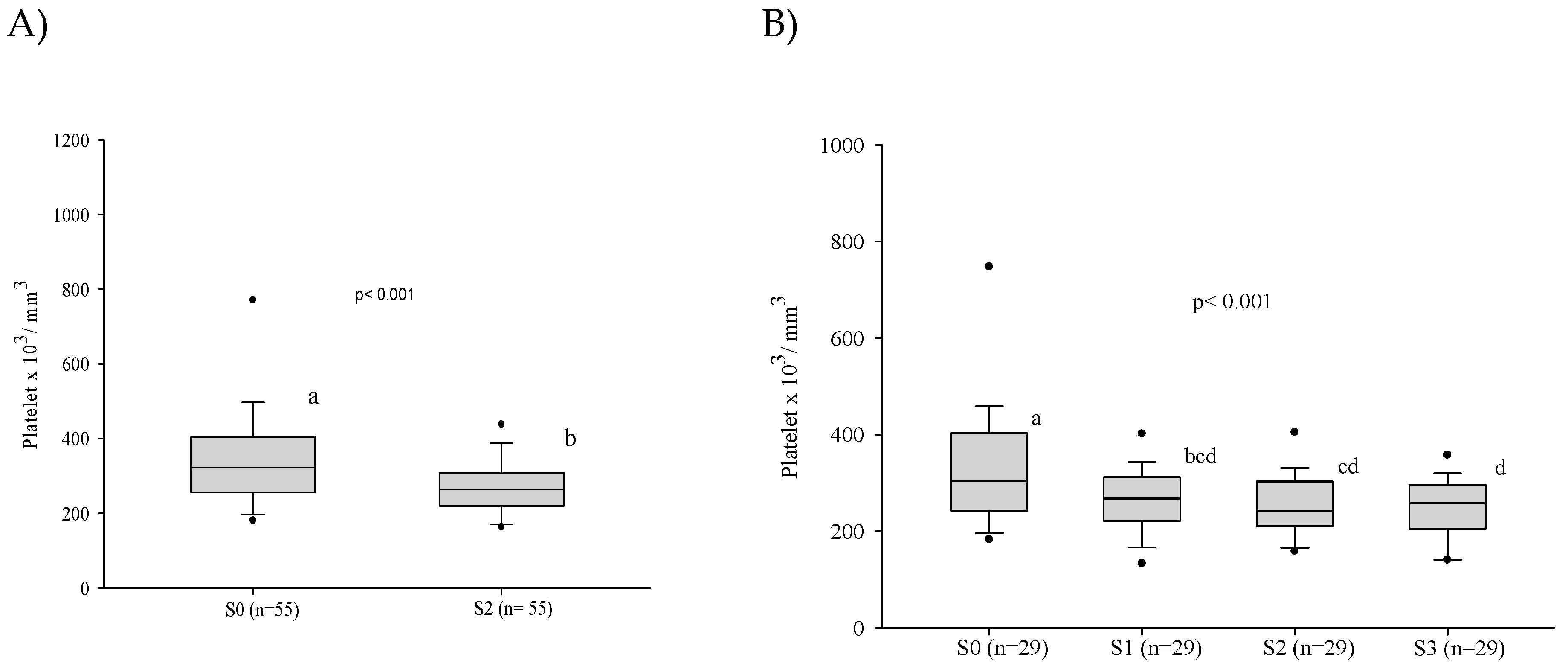
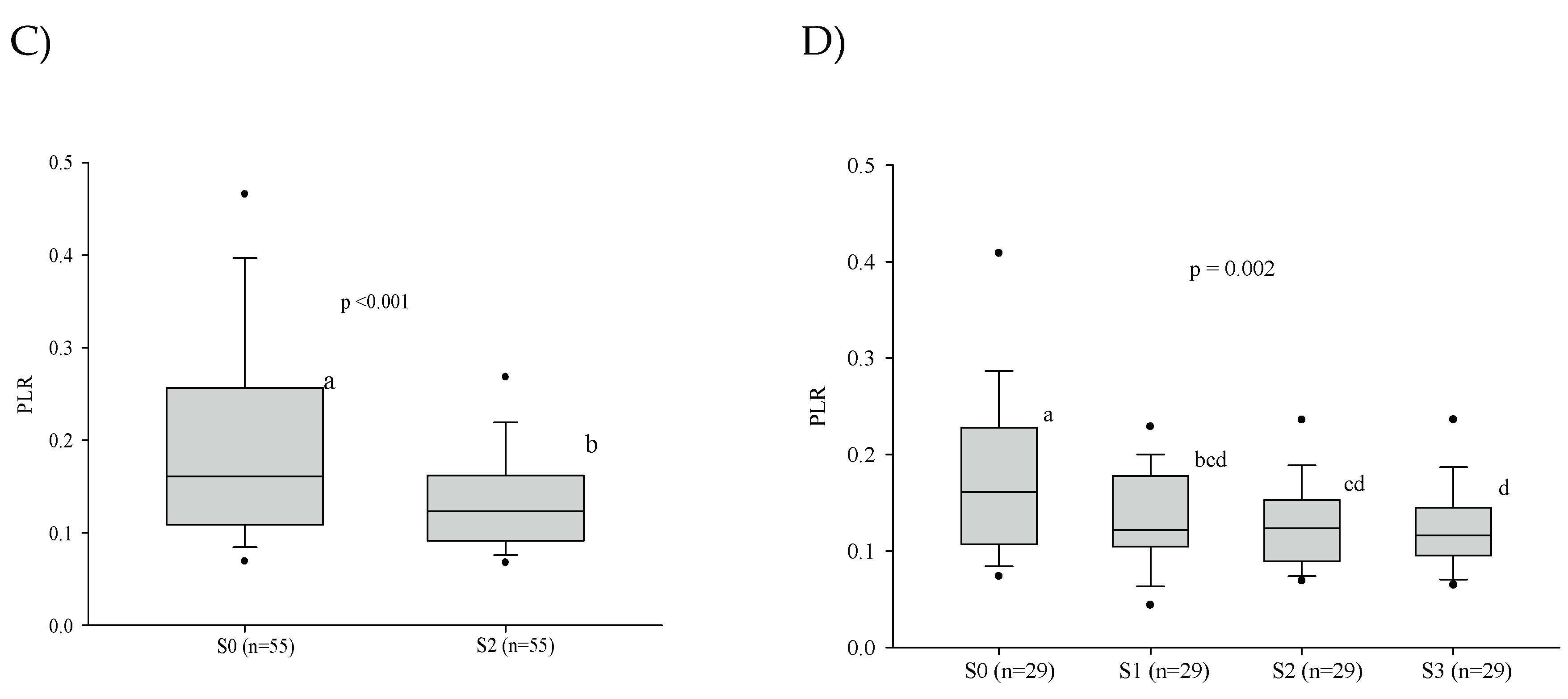

Table 1.
Sociodemographic and clinical findings of 62 patients with the chronic form of paracoccidioidomycosis treated at the Maria Aparecida Pedrossian University Hospital between 2013 and 2021.
Table 1.
Sociodemographic and clinical findings of 62 patients with the chronic form of paracoccidioidomycosis treated at the Maria Aparecida Pedrossian University Hospital between 2013 and 2021.
| Variables | n (%) | 95% CI | |
|---|---|---|---|
| Sex | |||
| Male | 60 (96.8) | 88.8 | 99.6 |
| Female | 02 (3.2) | 0.4 | 11.2 |
| Rural activity | |||
| Yes ǂ | 55 (88.7) | 78.1 | 95.3 |
| Never | 06 (9.7) | 3.6 | 19.8 |
| Ignored | 01 (1.6) | 0.0 | 8.6 |
| Use of Tobacco | |||
| Regularly | 51 (82.3) | 70.5 | 90.8 |
| Former smoker | 07 (11.3) | 4.6 | 21.9 |
| Never | 04 (6.5) | 1.8 | 15.7 |
| Degree of severity of PCM | |||
| Moderate | 37 (59.7) | 46.5 | 72.0 |
| Severe | 17 (27.4) | 16.8 | 40.2 |
| Mild | 08 (12.9) | 5.7 | 23.8 |
| Antifungal treatment | |||
| Itraconazole | 39 (62.9) | 49.7 | 74.8 |
| Cotrimoxazole | 23 (37.1) | 25.2 | 50.3 |
CI: confidence interval; n: number of patients; *mean (standard deviation -SD); Rural activity: Yes ǂ: individuals who performed rural work in the present or in the past.
Table 2.
Evaluation of the alterations observed in the blood red cells before treatment and its progress after introduction of the antifungal compounds.
Table 2.
Evaluation of the alterations observed in the blood red cells before treatment and its progress after introduction of the antifungal compounds.
| Variable | Patients | S0 | S1 | S2 | S3 | p value |
|---|---|---|---|---|---|---|
| (number) | n (%) | n (%) | n (%) | n (%) | ||
| Anemia | 62 | 28 (45.2) | ... | ... | ... | ... |
| 55* | 21 (39.3) | ... | 11(20.0) | ... | 0.008 | |
| 29** | 08 (27.6) | 06 (20.7) | 06 (20.7) | 03 (10.3) | 0.063 |
n: number of patients; ( ) – percentage; … not performed; S0 – before treatment; S1 - between the beginning of treatment and after clinical improvement; S2 - clinical cure; S3 - serological cure. Statistical analysis: McNemar test*; Cochran’s Q test**.
Table 3.
Evaluation of the prevalence of abnormalities observed in the white blood cells before treatment and its progress after introduction of the antifungal treatment.
Table 3.
Evaluation of the prevalence of abnormalities observed in the white blood cells before treatment and its progress after introduction of the antifungal treatment.
| Variable | Patients | S0 | S1 | S2 | S3 | p value |
|---|---|---|---|---|---|---|
| (number) | n (%) | n (%) | n (%) | n (%) | ||
| Leukopenia* | 55 | 02 (3.6) | ... | 02 (3.6) | ... | 0.564 |
| Leukopenia† | 29 | 01 (3.4) | - | - | 02 (6.9) | 0.317 |
| Leukocytosis* | 55 | 11 (20.0) | ... | 08 (14.5) | ... | 0.366 |
| Leukocytosis† | 29 | 06 (20.7) | 05 (17.2) | 06 (20.7) | 05 (17.2) | 0.940 |
| Neutropenia* | 55 | 01 (1.8) | ... | 03 (5.5) | ... | 0.157 |
| Neutropenia† | 29 | 01 (3.4) | 01 (3.4) | 02 (6.9) | 03 (10.3) | 0.194 |
| Neutrophilia* | 55 | 08 (14.5) | ... | 04 (7.3) | ... | 0.206 |
| Neutrophilia† | 29 | 03 (10.3) | 02 (6.9) | 02 (6.9) | 05 (17.2) | 0.429 |
| Eosinophilia* | 55 | 14 (25.4) | ... | 14 (25.4) | ... | 1.000 |
| Eosinophilia† | 29 | 09 (31.0) | 12 (41.4) | 10 (34.5) | 08 (27.6) | 0.274 |
| Monocytosis* | 55 | 22 (40.0) | ... | 09 (16.4) | ... | 0.003 |
| Monocytosis† | 29 | 11 (37.9) | 06 (20.7) | 04 (13.8) | 07 (24.1) | 0.059 |
| Lymphopenia* | 55 | 14 (25.5) | ... | 11 (20.0) | ... | 0.366 |
| Lymphopenia† | 29 | 06 (20.7) | 06 (20.7) | 06 (20.7) | 07 (24.1) | 0.954 |
| Lymphocytosis* | 55 | 03 (5.5) | ... | 03 (5.5) | ... | 1.000 |
| Lymphocytosis† | 29 | 03 (10.3) | 03 (10.3) | 02 (6.9) | 03 (10.3) | 0.801 |
n: number of patients; ( ) – percentage. S0 – before treatment; S1 - between the beginning of treatment and after clinical improvement; S2 - clinical cure; S3 - serological cure. Statistical analysis: McNemar test*; Cochran’s Q test†.
Table 4.
Comparison of the parameters of cellular immaturity in the complete blood count before treatment (S0) and at clinical cure (S2) in 12 patients with the chronic form of paracoccidioidomycosis.
Table 4.
Comparison of the parameters of cellular immaturity in the complete blood count before treatment (S0) and at clinical cure (S2) in 12 patients with the chronic form of paracoccidioidomycosis.
| Variables | S0 | S2 | p value |
|---|---|---|---|
| Mean±SD | Mean±SD | ||
| median [Q1; Q3] | median [Q1; Q3] | ||
| IGs† | 0.0 [0.0; 0.1] | 0.0 [0.0; 0.1] | 0.756 |
| IGs (%)† | 0.5 [0.3; 0.7] | 0.2 [0.0; 0.3] | 0.037 |
| Ret (%)* | 1.3±0.6 | 3.3±8.1 | 0.942 |
| IRF* | 6.8±2.8 | 7.0±4.0 | 0.441 |
| Ret-He* | 31.4±3.0 | 33.5±1.7 | 0.016 |
| IPF† | 31.6 [29.5; 33.9] | 33.7 [32.8; 34.3] | 0.056 |
SD: standard deviation; Q1: first quartile; Q3: third quartile; IG: immature granulocytes; Ret: reticulocytes; IRF: fraction of immature reticulocytes; Ret-He: reticulocyte hemoglobin content; IPF: reticulocyte count; Statistical test for paired-samples: Student’s t test* or Wilcoxon’s rank test†.
Table 5.
Comparison of the prevalence of altered hematological variables and C-reactive protein in 62 patients with the chronic form of paracoccidiodomycosis as to degree of severity.
Table 5.
Comparison of the prevalence of altered hematological variables and C-reactive protein in 62 patients with the chronic form of paracoccidiodomycosis as to degree of severity.
| Variables | Severe (n = 17) | Mild+Moderate (n = 45) | p value |
|---|---|---|---|
| n (%) | n (%) | ||
| Anemia | 12 (70.6) | 16 (35.6) | 0.013 |
| Leukopenia* | 0 (0.0) | 03 (6.7) | 0.555 |
| Leukocytosis | 02 (11.8) | 09 (20.0) | 0.712 |
| Neutropenia* | 0 (0.0) | 02 (4.4) | 1.000 |
| Neutrophilia* | 02 (11.8) | 06 (13.3) | 1.000 |
| Monocytosis | 07 (41.2) | 17 (37.8) | 0.806 |
| Eosinophilia | 02 (11.8) | 04 (8.9) | 0.662 |
| Lymphopenia | 02 (11.8) | 04 (8.9) | 0.662 |
| Lymphocytosis | 02 (11.8) | 09 (20.0) | 0.712 |
| Thrombocytosis* | 03 (17.6) | 03 (6.7) | 0.333 |
n = number of patients; ( ) - percentage; Statistical analysis: chi-square test or Fisher’s exact test*.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



