Submitted:
13 March 2024
Posted:
14 March 2024
You are already at the latest version
Abstract
Insulin resistance/hyperinsulinemia as an independent risk factor for the development and worsening of HFpEF.
Serafino Fazio MD¹, Valentina Mercurio MD, PhD2, Valeria Fazio MD3, Antonio Ruvolo MD⁴, Flora Affuso MD, PhD⁵.
Authors’ Affiliation:
¹ Department of Internal Medicine (retired Professor). Federico II University, Via Sergio Pansini 5. 80135 Naples, Italy.
2 Department of Translational Medical Sciences. Federico II University. Via Sergio Pasini 5. 80135 Naples, Italy.
³ UOC Medicina Interna, Azienda Ospedaliera di Caserta, 81100 Caserta, Italy,
⁴ UOC Cardiologia AORN dei colli PO CTO, Viale Colli Aminei 21, 80100 Naples, Italy.
⁵ Independent researcher, Viale Raffaello 74, 80129 Naples, Italy.
Abstract
Heart failure (HF) has become a subject of continuous interest since it has been declared new pandemic in 1997 because of the exponential increase in hospitalizations for HF in the latest years. HF is the final state to which all heart diseases of different etiologies lead if not adequately treated, therefore it is highly prevalent worldwide, with a progressive increase with age, reaching a prevalence of 10% in subjects over the age of 65 years. It should also be underlined that lately, while the prevalence of HF with left ventricular reduced ejection fraction (HFrEF) is slowly decreasing, the incidence of HF with left ventricular preserved ejection fraction (HFpEF) is progressively increasing.
In deed, among patients consecutively hospitalized for HF between 1987 and 2001 in a study from the Mayo Clinic Hospitals in Olmsted County, Minnesota, prevalence of HFpEF increased from 38% to 54%. HFpEF is typically characterized by concentric remodeling of the left ventricle (LV) with impaired diastolic function and increased filling pressures. Over the years, also the prevalence of insulin resistance/hyperinsulinemia in the general adult population has progressively increased, primarily due to lifestyle changes, particularly in developed and developing countries, with a range that globally ranges between 15.5% and 46.5%. Notably, insulin resistance (IR)/hyperinsulinemia (Hyperins) is present in up to 60% of patients with HF and is significantly higher in subjects with HfpEF.
In the scientific literature it has been well highlighted that the increased circulating levels of insulin are associated with conditions of insulin resistance are responsible for progressive cardiovascular alterations over the years. In the setting of HFpEF, insulin stimulates the concentric remodeling of the left ventricle with associated diastolic dysfunction, which, coincidentally. Unfortunately, IR/Hyperins, despite being a well-known cardiovascular risk factor, is still not screened in the general population and is not treated as promptly as it should be, and this could at least in part concur in the progressive increase in prevalence of HFpEF in the general adult population. The aim of this manuscript was to review scientific literature that support a pathophysiologic connection between IR/Hyperins and HFpEF to stimulate the scientific community towards the identification of hyperinsulinemia associated with insulin resistance as an independent cardiovascular risk factor in development and worsening of HF, believing that its adequate screening in the general population and appropriate treatment could reduce the prevalence of HFpEF and improve its progression.
Keywords:
insulin
; insulin signaling
; insulin resistance
; hyperinsulinemia
; cardiovascular system
; cardiovascular diseases
; cardiovascular risk factors
; diabetes
; HF
; HFpEF
Introduction
Despite the considerable progress made in the last decades in the prevention and treatment of cardiovascular diseases, they are still the main cause of mortality. In particular, in the European community there are approximately 2 million deaths from cardiovascular causes every year [1]. Heart failure (HF) is the culmination of cardiovascular diseases of different etiologies and its prevalence is progressively increasing, with over 64 million people estimated to be affected by it worldwide in 2017 [2,3]. Heart failure is classified based on symptoms and the ejection fraction of the left ventricle into: HF with reduced ejection fraction (left ventricular ejection fraction <50%, HFrEF) and HF with preserved ejection fraction (left ventricular ejection fraction ≥50%). In recent years prevalence of HFpEF has progressively increased, while the prevalence of HFrEF is slowly decreasing [4]. As well-known, HFpEF is characterized by concentric remodeling of the left ventricle, diastolic dysfunction with increased left ventricular filling pressures [4,5]. It is very likely that one of the main causes of this may be insulin resistance (IR) with associated increase in circulating insulin levels (Hyperinsulinemia) which is becoming increasingly prevalent in developed and developing countries, due to evident lifestyle changes [6,7,8]. We believe that insulin resistance (IR)/hyperinsulinemia (Hyperins) should be considered an independent risk factor for cardiovascular disease and, in particular, an important cause of the development and progressive worsening of HFpEF. The aim of this manuscript is the review of scientific literature that supports a pathophysiologic connection between IR/Hyperins and HFpEF to stimulate the scientific community towards the identification of hyperinsulinemia associated with insulin resistance as an independent cardiovascular risk factor in development and worsening of HF, believing that its adequate screening in the general population and appropriate treatment could reduce the prevalence of HFpEF and improve its progression.
For this reason we searched the most accredited scientific databases (Pubmed, Scopus, Science Direct, etc) for scientific literature on the topic using the following keywords: insulin, insulin signaling, insulin resistance, hyperinsulinemia, cardiovascular system, cardiovascular diseases, cardiovascular risk factors, diabetes, HF, HFpEF
Heart Failure
Heart failure (HF) can be generically defined as a clinical syndrome characterized by the reduced ability of the heart to pump and/or fill with blood, with increased filling pressures and secondary neurohormonal activation [4,5,8]. According to a recent consensus for a universal definition and classification of HF, According toa recent consensus for a universal definition and classification of HF, it was defined it was defined as a clinical syndrome characterized by symptoms and signs, caused by structural and/or functional anomalies of the heart, supported by elevated levels of natriuretic peptide and/or objective evidence of systemic or pulmonary congestion [4,9]. Based on left ventricular ejection fraction (EF), HF was classified s into three categories: 1. HF with reduced EF (HFrEF, with an EF≤40%); 2. HF with mildly reduced EF (HFmrEF, with an EF between 41 and 49%; 3. HF with preserved EF (HFpEF, with EF≥50%). Furthermore, based on the change in EF over time, for example following to the effects of the therapy, a new category was introduced, namely HF with improved EF, which was defined as HF with a starting EF ≤40% that improved ≥10 points and in any case went to an EF >40% [9]. In recent years, considering only the two main forms of HF, i.e. HFrEF and HFpEF, it was possible to notice a progressive reduction in the prevalence of the former with a progressive increase in the prevalence of the latter. In fact, in a study of patients consecutively hospitalized for HF between 1987 and 2001 at the Mayo Clinic Hospitals in Olmsted County, Minnesota, the patients with HFpEF increased from 38% to 54% [10]. Currently, HFpEF affects approximately 50% of patients with HF. HF is the main cause of hospitalization in patients aged over 65 years, and accounts for between 1 and 2% of all causes of hospitalization [11]. Improving treatment of HFpEF is becoming a priority, as it is expected to become the leading cause of HF in the coming years. HFpEF is characterized by an increase in filling pressures caused by the complex interaction of multiple components, of which the concentric remodeling of the left ventricle (LV) is a relevant component [11]. It is well known that the increase in heart stiffness resulting from aging is an important cause of diastolic dysfunction, therefore the general aging of the population concur to a further increase in the prevalence of HFpEF in the coming decades [12]. Furthermore, the current lack of specific therapies for this condition will make HFpEF one of the most relevant issues to be addressed. Over 50% of patients with HF also have IR with associated hyperins, and it is likely that this percentage is much higher in the setting of HFpEF [13]. In fact, it is known that diabetes is a very common comorbidity in patients with HFpEF, and that unfortunately its presence considerably worsens the course of HF, significantly increasing the number of hospitalizations and mortality [14,15], and this is more evident in patients with HFpEF [16,17].
Insulin Resistance/Hyperinsulinemia
Insulin resistance is a pathological condition whose prevalence is rapidly growing in recent decades, particularly in developed and developing countries, and, being little symptomatic or even asymptomatic, it is defined as a hidden pandemic that causes uncountable damages to the population, with relevant impact also in terms of health care systems spending [18]. It is characterized by a decreased sensitivity and metabolic response to insulin, so that at given insulin levels there are frankly reduced metabolic effects. For this reason, increased circulating insulin levels (hyprinsulinemia) are necessary to maintain blood glucose within the normal range. IR conditions are always characterized (as long as there is a sufficiently functioning pancreas) by Hyperins [7,18]. Therefore, IR/Hyperins, especially in terms of cariovascular effects, should be considered as a single entity. It is well known that IR is a key mechanism in the pathogenesis of type 2 diabetes, but also of systemic arterial hypertension, atherosclerosis, and, in particular, HFpEF, as well as other various atherosclerotic and non-atherosclerotic cardiovascular diseases [19,20,21] The increased circulating levels of insulin (Hyperins), associated with IR conditions, adversely affect the cardiovascular system over time. Insulin has many biological targets. Beyond skeletal muscle tissue, adipose tissue and the liver, also the cardiovascular system [22] is a relevant target of insulin actions, as insulin receptors are highly represented in myocardial cells and vascular smooth muscle cells as well as endothelial cells [23].
The gold standard for IR diagnosis is the euglycemic/hyper-insulinemic clamp, but this test is poorly applicable for screening purposes. In fact, many indices that are easier to acquire have been created, and among these the Homeostasis Model Assessment of IR index (HOMA-IR) and the triglyceride-glucose index (TyG) have demonstrated a good correlation with the euglycemic/hyper insulinemic clamp, and could be used for screening purpose. HOMA-IR is calculated by multiplying the fasting blood glucose value in mmol/L × the fasting insulinemia value in mU/L and dividing the result by 22.5 [(glycemia × insulinemia)/22.5]. The TyG index is obtained by calculating the natural logarithm of the product between the fasting triglyceride (Tg) value in mg/dl and the fasting blood sugar (FBG) value in mg/dl, then dividing the result by 2 [logn (serum Tg × FBG)/2]. A HOMA-IR index between 0.23 and 2.5 can be considered normal in the adult population, while the cut-off value for the TyG index is 4.5 [24,25].
IR/Hyperins and HFpEF
Chronic long-lasting hyperinsulinemia, that typically characterizes IR, can damage target organs, including the cardiovascular system [22]. Insulin signaling regulates heart growth, survival, substrate uptake and utilization, and mitochondrial metabolism. Therefore, an impaired insulin signaling may certainly contribute to the pathological ventricular remodeling of the heart, which can lead to the development and/or worsening of HF [23], in particular HFpEF. Insulin, binds both the insulin receptor (InsR) and that of insulin-like growth factor-1 (IGF-1 R), and this produces the activation of a signaling which in turn determines, through the phosphorylation of a tyrosine kinase, the activation of two main pathways, that of phosphoinositide-3 kinase (PI3K/Akt), and that of Shc-Ras-mitogen activated protein kinase (MAPK) [26]. The PI3K/Akt pathway predominantly mediates the metabolic actions of insulin, regulating glucose metabolism in muscle and in adipose and hepatic tissues; it also regulates nitric oxide (NO) formation by vascular endothelial and smooth muscle cells. The MAPKs are among the most ancient signal transduction pathways which coordinately regulate gene expression, mitosis, survival, apoptosis, differentiation, etc. and primarily mediate mitogenic and proliferative actions of insulin; furthermore, they stimulate endothelial cells to form increased amounts of the vasoconstrictor endothelin-1(ET-1) and increase the expression of adhesion molecules on the vascular endothelium [27,28]. In the normal subjects, these two pathways balance to maintain normal vascular homeostasis: the first pathway, stimulating NO production, causes vasodilatation and reduction in vascular resistance with increased blood flow to tissues, while the second one, stimulating ET-1 formation, causes vasoconstriction and activates the sympathetic system, leading to a hypertensive pattern and accelerating the development of cardiac hypertrophy and atherosclerosis.
Under conditions of IR, it is prevalently altered the PI3K-dependent pathway, while the MAPK-dependent pathway functioning is practically normal. For this reason, hyperins, resulting from IR in an attempt to maintain blood glucose within the normal range, increases the activity of MAPK pathway which, due to its mitogenic and proliferative actions, and to the stimulus to produce greater quantities of endothelin-1 (ET-1), in presence of reduced nitric oxide (NO) formation, causes chronic endothelial dysfunction with development and progressive worsening of atherosclerosis [29]. Hyperins determines arterial hypertension not only for the elevation of ET-1 and the increased sympathetic tone, but also because of anti-natriuretic effect of insulin [30]. In addition, the chronically increased circulating levels of insulin, for its mitogenic and proliferative effects on the cardiovascular system, produce proliferation of vascular smooth muscle cells and increased left ventricular mass (LVM) with concentric remodeling [31] (Figure 1). Such actions of hyperins may remain misrecognized for years, at least until overt type 2 diabetes appears or a cardiovascular event occurs. One study demonstrated that IR/Hyperins is highly prevalent among nondiabetic patients with HF. In these patients the IR indices progressively increase with the worsening of the NYHA classes of HF, and that patients with HF and IR have a significantly reduced capacity for physical exercise and a peak O2 reached but, unfortunately, the HF patients studied do not were distinguished in patients with HFrEF or HFpEF [14].
There is extensive scientific literature supporting the evidence that IR/Hyperins stimulate pathological remodeling of the left ventricle (LV). Indeed, diabetic cardiomyopathy is characterized by LV hypertrophy (LVH) [32] and LVH is a very strong predictor of adverse cardiovascular events, including the development of HFpEF, as it can determine an alteration to the normal filling of the LV with diastolic dysfunction and increased filling pressures [33].
IR/Hyperins was associated with LV concentric remodeling regardless of body mass index (BMI) levels. This may lead to hypothesize that treating IR/Hyperins could lead to a regression of LV concentric remodeling and slow the progression to HFpEF [34]. Diabetes in patients with HFpEF determines at least a double risk of hospitalizations and cardiovascular death, with a clear increase in the risk of mortality from any cause [16,17]. In fact, in the "Digoxin" study, diabetes was associated with a 68% increase in the risk of hospitalization and death due to HF [35], a result subsequently confirmed also in the "Preserve Study" [36]. In the "Relax" study it was verified that patients with HFpEF and diabetes had significantly higher levels of ET-1 and inflammation markers compared to patients with HFpEF but without diabetes [37]. As seen from this brief analysis of the literature, it is clear how the alterations caused over time at cardiovascular level by IR/Hyperins can determine and worsen, if not corrected, HFpEF as well as causing other adverse cardiovascular events. For this reason, we believe that it would be useful to screen the general population to promptly diagnose this pathology and treat it so as not to allow or, at least slow down, its negative evolution. Nowadays there are both drugs and natural substances that have been shown to reduce IR/Hyperins, as well as, obviously, the possibility of changing your lifestyle for the better. Among the various substances, we will focus on only a few that we believe, can produce, alone or in association, the best results: Sodium-Glucose Cotransporter-2 Inhibitors, metformin, and berberine.
Potential Treatments of IR/Hyperins
First of all, once identified, patients with IR/Hyperins should be informed of their condition, that, if not corrected, can over time produce important pathologies, especially affecting the cardiovascular system. They should be advised to improve their lifestyle, with a constant increase in physical activity and a reduction in caloric intake through balanced, low- carbohydrates diets [38,39]. However, in the daily clinical practice, often, even the most motivated patients are unable to maintain the lifestyle change made for a long time and, more often, they interrupt the path undertaken. For this reason, most patients with IR/Hyperins may benefit from therapeutic strategies with drugs or substances that act by improving insulin sensitivity and reducing circulating insulin levels.
A class of orally administered drugs, sodium-glucose cotransporter-2 inhibitors (SGLT2 Is), which include canaglifozin, dapaglifozin and empaglifozin, has recently been approved and marketed for the treatment of diabetes. These drugs demonstrated in randomized, double-blind and placebo-controlled trials to be associated with a significant reduction of the risk of hospitalization, death from cardiovascular events and death from any cause in patients with HF [40]. For this reason, they became part of the pillars in the pharmacological treatment of HF according to the latest European guidelines [5,40].
It should be underlined that the beneficial effect of these drugs in patients with HF was also confirmed, even more strongly, in patients with HFpEF. A recent meta-analysis carried out on 12,251 patients from the "DELIVER" and "EMPEROR-Preserved" studies demonstrated that treatment with SGLT2Is leadsto a significant reduction in both deaths from cardiovascular events and first hospitalizations for HF in patients with HFpEF [41]. It has been hypothesized that the mechanisms underlying the beneficial action of these drugs in these patients are multiple (regulation of blood volume, cardiorenal mechanisms, metabolic effects, improved cardiac remodeling, direct effects on contractility and sodium ion homeostasis, reduction of oxidative stress and inflammation, and so on) and still not completely clarified. However, beside such complex mechanisms, the administration of these drugs to subjects with IR/Hyperins, significantly prevalent among patients with HF, produces glycosuria and reduces the amount of circulating glucose. Consequently, the insulin levels necessary to maintain blood sugar within the normal range are drastically reduced, thus reducing the deleterious effects that Hyperins can cause in the cardiovascular system [42]. Indeed, various studies have demonstrated how SGLT2 Is therapy in patients with HFpEF determines a reduction in left ventricular mass (LVM) and concentric remodeling, producing an improvement in diastolic function and EF [43,44].
Metformin is an oral antidiabetic, commonly used since decades, belonging to the biguanide class. There is a vast scientific literature that supports the effectiveness of metformin in improving IR/Hyperins in both diabetic and non-diabetic subjects [45]. A recent review and meta-regression-analysis study clearly demonstrated that metformin treatment reduces mortality in patients with HF, especially in the subgroup of patients with HFpEF(p<0.003) [46]. Another meta-analysis study demonstrated that metformin reduces LVM and improves EF in both subjects with and without prior heart disease [47].
It is well known that the minute ventilation/carbon dioxide production slope (VE/VCO2 slope) is a strong predictor of prognosis among patients with HF, as the risk of mortality increases significantly if its value is >32.8 [48]. An interesting double-blind and placebo-controlled study demonstrated that metformin therapy for 4 months in non-diabetic but insulin-resistant HF patients resulted in a significant (p<0.001) improvement in IR indices associated with a significant (p<0.036) reduction of the VE/VCO2 slope [49].
Berberine is a plant alkaloid contained in numerous plants, including Coptis chinensis and Hydrastis canadensis, in use for over 2000 years in Chinese and Indian Ayurvedic medicine for its multiple beneficial effects on human health. Among its various positive effects, the one relating to the reduction of IR/Hyperins has been widely demonstrated in the literature [49,50,51]. A few years ago, a placebo-controlled study was published which aimed to verify, in patients with HF, the effects of berberine therapy on the heart. The evaluation was carried out at baseline, after 2 months, and after an average follow-up of 24 months. The results of this study demonstrated that berberine therapy in patients with HF resulted in a significant increase in EF and a reduction in the number and complexity of ventricular extrasystoles. Furthermore, at the 2-year follow-up, 7 patients had died in the berberine arm while 13 patients had died in the placebo arm (p<0.02) [52].
In another randomized, double-blind and placebo-controlled study, the 18-week treatment with a nutraceutical combination containing 500 mg of berberine in a group of patients with metabolic syndrome resulted in a significant (p<0.05) reduction in HOMA-IR and fasting insulin levels, and this was accompanied by a significant reduction in LVM, relative wall thickness and diastolic dysfunction [53]. These results were confirmed in a more recent multicenter randomized, double-blind and placebo-controlled study on a larger number of patients with metabolic syndrome and LVH, in which treatment with 500 mg of berberine per day for 6 months compared to placebo resulted in a significant (p<0.001) reduction of LVM [54]. The absorption of berberine at the intestinal level can be made more constant by the association of berberine with silymarin, which, in addition to enhancing the metabolic effects of berberine, improves its absorption by blocking intestinal P-glycoprotein [55].
Conclusions
The prevalence of HFpEF is progressively increasing along with IR/Hyperins syndrome, particularly in developed and developing countries. The scientific literature clearly demonstrates that the two conditions are closely related and are progressively increasing hospitalizations and healthcare costs, and the lack of intervention also means that, despite progress in the treatment of cardiovascular diseases and recognized risk factors, deaths from cardiovascular causes remain in the first place among the causes of death. Therefore, we believe, that it is necessary to consider IR/Hyperins as an independent cardiovascular risk factor and, in particular, for the development and worsening of HFpEF. t may Screening for IR/Hyperins in the general population should be advisable in order to promptly identify affected subjects and initiate a preventive treatment strategy.
References
- Istituto Superiore di Sanità. Le Statistiche Delle Malattie Cardiovascolari in Europa per il 2008; Istituto Superiore di Sanità-EpiCentro: Roma, Italy, 2008. [GoogleScholar].
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018; 392:1789–1858. Crossref PubMed WorldCat.
- Shahim B., Kapelios C.J., Savarese G., Lund L.H. Global Public Health Burden of Heart Failure: An Updated Review. Card Fail Rev. 2023; 9: e11. [CrossRef]
- Bozkurt B., Coats A.J.S., Tsutsui H., Abdelhamid C.M., Adamopoulos S., Albert N., Anker S.D., Atherton J., Bohm M., Butler J., Drazner M.H., Michael Felker G., Filippatos G., Fiuzat M., Fonarow G.C., Gomez-Mesa J.E., Heidenreich P., Imamura T., Jankowska E.A., Januzzi J., Khazanie P., Kinugawa K., Lam C.S.P., Matsue Y., Metra M., Ohtani T., Francesco Piepoli M., Ponikowski P., Rosano G.M.C., Sakata Y., Seferovic P., Starling RC., Teerlin J.R., Vardeny O., Yamamoto K., Yancy C., Zhang J., Zieroth S. Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association. Eur J Heart Fail 2021;23:352–380.Google Scholar Crossref PubMed WorldCat.
- McDonagh T.A., Metra M., Adamo M., Gardner R.S., Baumbach A., Böhm M., Burri H., Butler J., Čelutkienė J., Chioncel O., et al. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2023;44:3627–3639. [CrossRef]
- Riehle C., Abel E.D. Insulin Signaling and Heart Failure. Circ. Res. 2016;118:1151–1169. [CrossRef]
- Freeman A.M., Pennings N. StatPearls. StatPearls; Treasure Island, FL, USA: 2023. Insulin Resistance. [PubMed] [GoogleScholar].
- Fahed M., Jaoudeh M.G.A., Merhi S., Mosleh J.M.B., Ghadieh R., Al Hayek S., El Hayek Fares J.E. Evaluation of risk factor for insulin resistance: a cross sectional study among employees at a private university in Lebanon. BMC Endocr Disord. 2020;20:85. [CrossRef]
- Writing Committee; Maddox T.M., Januzzi J.L. Jr, Allen L.A., Breathett K., Butler J., Davis L.L., Fonarow G.C., Ibrahim N.E., Lindenfeld J., Masoudi F.A., Motiwala S.R., Oliveros E., Patterson J.H., Walsh M.N., Wasserman A., Yancy C.W., Youmans Q.R. 2021 Update to the 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment: Answers to 10 Pivotal Issues About Heart Failure With Reduced Ejection Fraction: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2021 Feb 16;77(6):772-810. [CrossRef]
- Pfeffer M.A., Shah A.M., Borlaug B.A.. Heart Failure With Preserved Ejection Fraction In Perspective. Circ Res. 2019 May 24;124(11):1598-1617. PMID: 31120821; PMCID: PMC6534165. [CrossRef]
- Ma C., Luo H., Fan L., Liu X., Gao C. Heart failure with preserved ejection fraction: an update on pathophysiology, diagnosis, treatment, and prognosis. Braz J Med Biol Res. 2020 Jun 5;53(7):e9646. Erratum in: Braz J Med Biol Res. 2021 Feb 26;54(4):e9646erratum. [CrossRef]
- Larson K.F., Malik A., Brozovich F.V. Aging and Heart Failure with Preserved Ejection Fraction. Compr Physiol. 2022 Aug 11;12(4):3813-3822. [CrossRef]
- Kristensen S.L., Jhund P.S., Lee M.M.Y., Køber L., Solomon S.D., Granger C.B., Yusuf S., Pfeffer M.A., Swedberg K., McMurray J.J.V.; CHARM Investigators and Committees. Prevalence of Prediabetes and Undiagnosed Diabetes in Patients with HFpEF and HFrEF and Associated Clinical Outcomes. Cardiovasc Drugs Ther. 2017 Dec;31(5-6):545-549. [CrossRef]
- Alzadjali M.A., Godfrey V., Khan F., Choy A., Doney A.S., Wong A.K., Petrie J.R., Struthers A.D., Lang C.C. Insulin Resistance Is Highly Prevalent and Is Associated with Reduced Exercise Tolerance in Nondiabetic Patients with Heart Failure. J. Am. Coll. Cardiol. 2009;53:747–753. [CrossRef]
- Chun S., Tu J.V., Wijeysundera H.C., Austin P.C., Wang X., Levy D., Lee D.S.. Lifetime analysis of hospitalizations and survival of patients newly admitted with heart failure. Circ Heart Fail. 2012 Jul 1;5(4):414-21. [CrossRef]
- Packer M. Differential Pathophysiological Mechanisms in Heart Failure with a Reduced or Preserved Ejection Fraction in Diabetes. JACC Heart Fail. 2021;9:535–549. [CrossRef]
- Hasegawa H., Komuro I. CHARM study-new strategy for the treatment of heart failure. Nihon Rinsho. Jpn. J. Clin. Med. 2004;62:995–1002. [PubMed] [GoogleScholar].
- Lebovitz H.E. Insulin resistance: definition and consequences. Exp Clin Endocrinol Diabetes. 2001;109 Suppl 2:S135-48. [CrossRef]
- Janssen J.A.M.J.L. Hyperinsulinemia and Its Pivotal Role in Aging, Obesity, Type 2 Diabetes, Cardiovascular Disease and Cancer. Int J Mol Sci. 2021 Jul 21;22(15):7797. [CrossRef]
- Jia G., DeMarco V.G., Sowers J.R. Insulin resistance and hyperinsulinaemia in diabetic cardiomyopathy. Nat Rev Endocrinol. 2016 Mar;12(3):144-53. Epub 2015 Dec 18. PMID: 26678809; PMCID: PMC4753054. [CrossRef]
- Reaven G.M. Insulin resistance/compensatory hyperinsulinemia, essential hypertension, and cardiovascular disease. J Clin Endocrinol Metab. 2003 Jun;88(6):2399-403. PMID: 12788834. [CrossRef]
- Ginsberg H.N. Insulin resistance and cardiovascular disease. J. Clin. Investig. 2000;106:453–458. [CrossRef]
- Abel E.D. Insulin signaling in the heart. Am. J. Physiol. Endocrinol. Metab. 2021;321:E130–E145. [CrossRef]
- Ziaee A., Esmailzadehha N., Oveisi S., Ghorbani A., Ghanei L. The threshold value of homeostasis model assessment for insulin resistance in Qazvin Metabolic Diseases Study (QMDS): Assessment of metabolic syndrome. J. Res. Health Sci. 2015;15:94–100. [PubMed] [GoogleScholar].
- Guerrero-Romero F., Simental-Mendía L.E., González-Ortiz M., Martínez-Abundis E., Ramos-Zavala M.G., Hernández-González S.O., Jacques-Camarena O., Rodríguez-Morán M. The Product of Triglycerides and Glucose, a Simple Measure of Insulin Sensitivity. Comparison with the Euglycemic-Hyperinsulinemic Clamp. J. Clin. Endocrinol. Metab. 2010;95:3347–3351. [CrossRef]
- Cai W., Sakaguchi M., Kleinridders A., Pino G.G.-D., Dreyfuss J.M., O’neill B.T., Ramirez A.K., Pan H., Winnay J.N., Boucher J., et al. Domain-dependent effects of insulin and IGF-1 receptors on signalling and gene expression. Nat. Commun. 2017;8:14892. [CrossRef]
- Chopra I., Li H.F., Wang H., Webster K.A. Phosphorylation of the insulin receptor by AMP-activated protein kinase (AMPK) promotes ligand-independent activation of the insulin signalling pathway in rodent muscle. Diabetologia. 2012;55:783–794. [CrossRef]
- Petersen M.C., Shulman G.I. Mechanisms of Insulin Action and Insulin Resistance. Physiol. Rev. 2018;98:2133–2223. [CrossRef]
- Mercurio V., Carlomagno G., Fazio V., Fazio S. Insulin resistance: Is it time for primary prevention? World J. Cardiol. 2012;4:1–7. [CrossRef]
- Bachmann K.N., Deger S.M., Alsouqi A., Huang S., Xu M., Ferguson J.F., Su Y.R., Niswender K.D., Ikizler T.A., Wang T.J. Acute effects of insulin on circulating natriuretic peptide levels in humans. PLoS ONE. 2018;13:e0196869. [CrossRef]
- Stout R.W. Insulin as a mitogenic factor: Role in the pathogenesis of cardiovascular disease. Am. J. Med. 1991;90:S62–S65. [CrossRef]
- Mohan M., Dihoum A., Mordi I.R., Choy A.-M., Rena G., Lang C.C. Left Ventricular Hypertrophy in Diabetic Cardiomyopathy: A Target for Intervention. Front. Cardiovasc. Med. 2021;8:746382. [CrossRef]
- Okwuosa T.M., Soliman E.Z., Lopez F., Williams K.A., Alonso A., Ferdinand K.C. Left ventricular hypertrophy and cardiovascular disease risk prediction and reclassification in blacks and whites: the Atherosclerosis Risk in Communities Study. Am Heart J. 2015 Jan;169(1):155-61.e5. Epub 2014 Oct 16. PMID: 25497261; PMCID: PMC4269255. [CrossRef]
- Shah R.V., Abbasi S.A., Heydari B., Rickers C., Jacobs D.R., Jr., Wang L., Kwong R.W., Bluemke D.A., Lima J.A.C., Jerosch-Herold M. Insulin resistance, subclinical left ventricular remodeling, and the obesity paradox: MESA (Multi-Ethnic Study of Atherosclerosis) J. Am. Coll. Cardiol. 2013;61:1698–1706. [CrossRef]
- Digitalis Investigation Group The effect of digoxin on mortality and morbidity in patients with heart failure. N. Engl. J. Med. 1997;336:525–533. [CrossRef]
- Massie B.M., Carson P.E., McMurray J.J., Komajda M., McKelvie R., Zile M.R., Andresen S., Donovan M., Iverson E., Staiger C., et al. Irbesartan in patients with heart failure and preserved ejection fraction. N. Engl. J. Med. 2008;359:2456–2467. [CrossRef]
- . Lindman B.R., Davila-Roman V.G., Mann D.L., McNulty S., Semigran M.J., Lewis G.D., de la Fuentes L., Vader J., Hernanderz A.H., Redfield M.M., et al. Cardiovascular phenotype in HFpEF patients with or without diabetes: A RELAX trial ancillary study. J. Am. Coll. Cardiol. 2014;64:541–549. [CrossRef]
- Szamosi A., Czinner A., Szamosi T., Sallai A., Hatunic M., Berla Z., Tomsits E., Almássy Z., Nolan J.J. Effect of diet and physical exercise treatment on insulin resistance syndrome of schoolchildren. J Am Coll Nutr. 2008 Feb;27(1):177-83. PMID: 18460496. [CrossRef]
- Ryan A.S. Insulin resistance with aging: effects of diet and exercise. Sports Med. 2000 Nov;30(5):327-46. [CrossRef]
- Butler J., Usman M.S., Khan M.S., Greene S.J., Friede T., Vaduganathan M., Filippatos G., Coats A.J.S., Anker S.D. Efficacy and safety of SGLT2 inhibitors in heart failure: Systematic review and meta-analysis. ESC Heart Fail. 2020;7:3298–3309. [CrossRef]
- Vaduganathan M., Docherty K.F., Claggett B.L., Jhund P.S., de Boer R.A., Hernandez A.F., Inzucchi S.E., Kosiborod M.N., Lam C.S.P., Martinez F., et al. SGLT2 inhibitors in patients with heart failure: A comprehensive meta-analysis of five randomised controlled trials. Lancet. 2022;400:757–767. [CrossRef]
- Hosokawa Y., Ogawa W. SGLT2 inhibitors for genetic and acquired insulin resistance: Considerations for clinical use. J. Diabetes Investig. 2020;11:1431–1433. [CrossRef]
- Salah H.M., Verma S., Santos-Gallego C.G., Bhatt A.S., Vaduganathan M., Khan M.S., Lopes R.D., Al’aref S.J., McGuire D.K., Fudim M. Sodium-Glucose Cotransporter 2 Inhibitors and Cardiac Remodeling. J. Cardiovasc. Transl. Res. 2022;15:944–956. [CrossRef]
- Dhingra N.K., Mistry N., Puar P., Verma R., Anker S., Mazer C.D., Verma S. SGLT2 inhibitors and cardiac remodelling: A systematic review and meta-analysis of randomized cardiac magnetic resonance imaging trials. ESC Heart Fail. 2021;8:4693–4700. [CrossRef]
- Herman R., Kravos N.A., Jensterle M., Janež A., Dolžan V. Metformin and Insulin Resistance: A Review of the Underlying Mechanisms behind Changes in GLUT4-Mediated Glucose Transport. Int J Mol Sci. 2022 Jan 23;23(3):1264. PMID: 35163187; PMCID: PMC8836112. [CrossRef]
- Halabi A., Sen J., Huynh Q., Marwick T.H. Metformin treatment in heart failure with preserved ejection fraction: A systematic review and meta-regression analysis. Cardiovasc. Diabetol. 2020;19:124. [CrossRef]
- Kamel A.M., Sabry N., Farid S. Effect of metformin on left ventricular mass and functional parameters in non-diabetic patients: A meta-analysis of randomized clinical trials. BMC Cardiovasc. Disord. 2022;22:405. [CrossRef]
- Shen Y., Zhang X., Ma W., Song H., Gong Z., Wang Q., Che L., Xu W., Jiang J., Xu J., et al. VE/VCO2 slope and its prognostic value in patients with chronic heart failure. Exp. Ther. Med. 2015;9:1407–1412. [CrossRef]
- Wong A.K., Symon R., AlZadjali M.A., Ang D.S., Ogston S., Choy A., Petrie J.R., Struthers A.D., Lang C.C. The effect of metformin on insulin resistance and exercise parameters in patients with heart failure. Eur. J. Heart Fail. 2012;14:1303–1310. [CrossRef]
- Cao C., Su M. Effects of berberine on glucose-lipid metabolism, inflammatory factors and insulin resistance in patients with metabolic syndrome. Exp Ther Med. 2019 Apr;17(4):3009-3014. Epub 2019 Feb 22. PMID: 30936971; PMCID: PMC6434235. [CrossRef]
- Imenshahidi M., Hosseinzadeh H. Berberine and barberry (Berberis vulgaris): A clinical review. Phytother Res. 2019 Mar;33(3):504-523. Epub 2019 Jan 13. PMID: 30637820. [CrossRef]
- Zeng X.-H., Li Y.-Y. Efficacy and safety of berberine for congestive heart failure secondary to ischemic or idiopathic dilated cardiomyopathy. Am. J. Cardiol. 2003;92:173–176. [CrossRef]
- Carlomagno G., Affuso F., Napoli R., Mercurio V., Fazio V., Micillo F., Pirozzi C., Ruvolo A., Saccá L., Fazio S. A nutraceutical combination improves insulin sensitivity in patients with metabolic syndrome. World J. Cardiol. 2012;4:77–83. [CrossRef]
- Mercurio V., Pucci G., Bosso G., Fazio V., Battista F., Iannuzzi A., Brambilla N., Vitalini C., D’Amato M., Giacovelli G., et al. A nutraceutical combination reduces left ventricular mass in subjects with metabolic syndrome and left ventricular hypertrophy: A multicenter, randomized, double-blind, placebo-controlled trial. Clin. Nutr. 2020;39:1379–1384. [CrossRef]
- Fogacci F., Grassi D., Rizzo M., Cicero A.F.G. Metabolic effect of berberine-silymarin association: A meta-analysis of randomized, double-blind, placebo-controlled clinical trials. Phytother Res. 2019 Apr;33(4):862-870. [CrossRef]
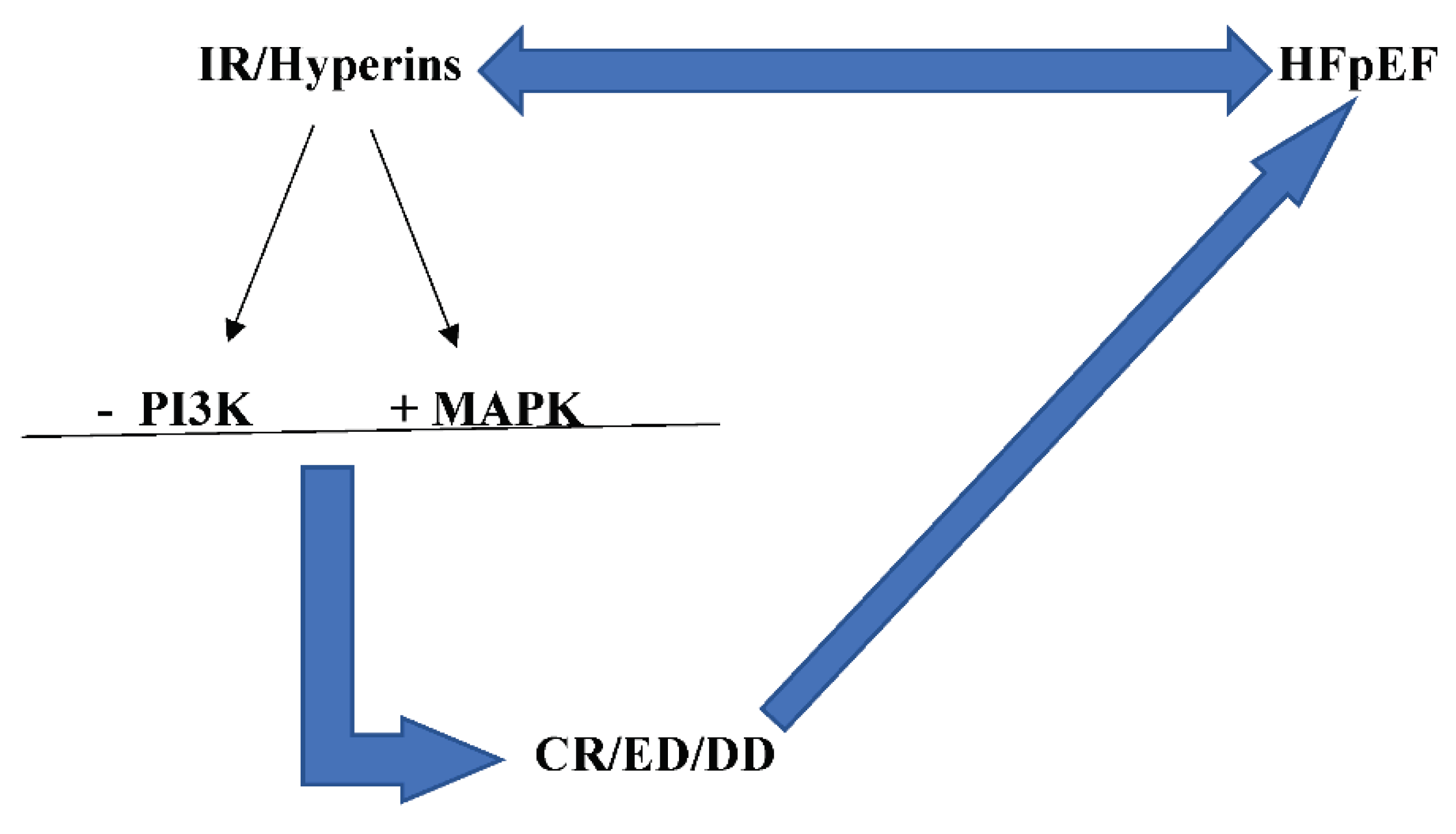
Figure 1.
IR/Hyperins and HFpEF are strictly related: Hyperins associated to IR, for the altered PI3K pathway and increased MAPK pathway activity, produces concentric remodeling and endothelial dysfunction, which, in turn, determine and/or worsen HFpEF.
Figure 1.
IR/Hyperins and HFpEF are strictly related: Hyperins associated to IR, for the altered PI3K pathway and increased MAPK pathway activity, produces concentric remodeling and endothelial dysfunction, which, in turn, determine and/or worsen HFpEF.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



