
Submitted:
14 March 2024
Posted:
14 March 2024
You are already at the latest version
Abstract
Background: In recent years, whole blood parameters and derivatives have been used as prognostic criteria in the course of the disease in various diseases. The prognostic nutritional index (PNI), the systemic immune-inflammation index (SII), the neutrophil-lymphocyte ratio (NLR) have been adapted as an indicator of inflammation and have been widely studied to define the severity of inflammation in some diseases. The aim of this study was to evaluate the relationship between parameters such as NLR, SII, PNI, controlling nutritional status (CONUT) score, nutritional risk index (NRI) and with immunonutrition status and disease activity in patients with ischemic stroke of small vessel, large vessel and other etiologies. Methods: We retrospectively evaluated the records of 1454 consecutive ischemic stroke patients hospitalized in the emergency department of Gaziosmanpasa Education and Research Hospital from 2019 to 2023. Results: Of the 1350 SVO patients included in the study, 58.8% had small vessel, 29.3% had large vessel and 11.9% had other etiologies. There was a significant difference between the 3 etiology groups for PNI and CONUT. The median PNI was 47.03 (41.33-52.85) in the other etiology group, 35.29 (33.69-37.25) in the small vessel group, and 34.11 (30.23-36.87) in the large vessel group. The CONUT median was 5(5-6) in the small vessel group, 5(4-6) in the large vessel group and 4(4-4) in the other etiology group. In addition, CONUT and PNI were also found to be independent risk factors for death. A negative significant correlation was observed between PNI and NLR (r:-0.692), SII (r:-0.591), CONUT (r:-0.685). Significant correlations were observed between CONUT and NLR (r:0.402), SII (r:0.312). Conclusion: PNI and SII were significantly associated with disease activity. PNI, CONUT and NRI as a more accurate prognostic indicator of nutritional status in patients with ischemic stroke of small vessel, large vessel and other etiologies. NLR and SII may be important predictive markers in the course and prognosis of stroke.
Keywords:
Ischemic stroke
; prognostic nutritional index
; nutritional risk index
; controlling nutritional status
; systemic immune inflammation index
; neutrophil-lymphocyte ratio.
1. Introduction
A cerebrovascular accident (CVA), also known as a stroke, is a focal or generalised neurological deficit that develops suddenly, lasts for more than 24 hours, results in death and cannot be explained by any cause other than vascular cause [1,2]. The prevalence of patients with cerebrovascular disease is estimated to be more than 60 million. Approximately 16 million people worldwide are diagnosed with cerebrovascular disease each year [3,4]. In the population over the age of 60, cerebrovascular disease is the second leading cause of death in the world after cardiovascular diseases (CVD). It is the first cause of disability and loss of labour force [1,4,5,6]. Cerebrovascular diseases are one of the disease groups that cause negative effects on the national economy and health budget by causing both loss of labour force and death. In the United States of America and Europe, cerebrovascular disease is reported to be one of the disease groups that cause the highest health costs after CVD [7].
Stroke patients may lose their ability to eat and drink due to impaired consciousness, swallowing problems, posture disorder, decreased mobilisation, communication problems, fatigue, depression and visual perceptual disturbances. Approximately 90% of stroke patients are at risk of malnutrition [8]. Some studies have reported the existence of specific objective assessment indices reflecting the immune nutritional status of patients, such as the prognostic nutritional index (PNI) [9], the controlling nutritional status (CONUT) score [10] and the nutritional risk index (NRI). Calculated using serum albumin level and lymphocyte count [11,12], they represent useful screening tools for patient prognosis in various diseases [13,14,15,16].
In recent years, an index reflecting both neutrophil elevation reflecting the acute state of inflammation and lymphopenia following acute physiological stress has been used. This index, which is obtained by the neutrophil to lymphocyte ratio (NLR), has been used together with other inflammatory markers in studies and found to be a good indicator of inflammatory status [17]. It has been suggested that NLR may be used as a marker of inflammation in intensive care unit (ICU) [18]. It has been previously shown that an increase in neutrophil levels in acute coronary syndrome is associated with the extent of myocardial damage and short-term prognosis [19]. In studies, it has been found that early mortality is commonly associated with high NLR values in patients with ischaemic stroke [19,20,21]. In general PNI is an indicator of immunonutrition and NLR reflects inflammatory status, both have high accuracy, low cost and high reproducibility with wide application in blood research.
The aim of this study was to evaluate the relationship between parameters such as NLR, systemic immune-inflammation index (SII), CONUT, NRI and PNI with immunonutrition status and disease activity in patients with ischemic stroke of small vessel, large vessel and other etiologies
2. Material and Methods
2.1. Study Design and Population
The protocol for sample collection was approved by the University of Health Sciences, Gaziosmanpasa Education and Research Hospital, Clinical Research Ethics Committee (Date:30/03/2022/49). The study was performed to accordance to the 1975 Helsinki Declaration, updated in 2013. Informed consent was obtain from participant or their relative.
The 1454 stroke patients included in the study were categorised into 3 groups according to small vessel, large vessel and other etiologies. Patients were admitted to the emergency department of Gaziosnpasa Education and Research Hospital between 1 January 2019 and 1 June 2023. Chronic diseases of the patients were listed as hypertension (HT), diabetes mellitus (DM), atrial fibrillation, coronary artery disease (CAD), and hyperlipidemia.
Electronic records of patients hospitalized for ischemic stroke were scanned from the hospital’s electronic database system. Patients who developed stroke symptoms in the last 72 hours were selected. Patients’demographic and clinical characteristics were evaluated according to the National Institutes of Health Stroke Scale (NIHSS). NIHSS five and below were described as minor stroke and NIHSS six and above as severe stroke [22].
2.2. Inclusion Criteria
Patients were included if they had i) an acute ischemic stroke confirmed by cerebral computed tomography (CT) or magnetic resonance imaging and ii) peripheral blood sampling within 24 hours after stroke onset.
2.3. Exclusion Criteria
i) Patients with hematological disease, history of cancer, severe renal and hepatic insufficiency, and a history of infection starting within 72 hours from the onset of stroke symptoms were excluded from the assessment. ii) Patients with a brain stem, cerebellar, and acute hemorrhagic stroke wherein the effect of hematologic parameters on the prognosis could not be examined and which could seriously affect the prognosis were also excluded. iii) Patients receiving antibiotics, immunosuppressive therapy, and non-steroidal anti-inflammatory drugs were excluded from the study.
2.4. Laboratory Parameters
Blood samples were taken into standardized tubes without anticoagulant and containing dipotassium ethylenedinitro tetraacetic acid (EDTA) for CBC parameters. The result of CBC was recorded with automatic hematology analyzer (Sysmex XN-1000, Norderstedt, Germany). NLR, LMR, and PLR were calculated from neutrophil/ lymphocyte/ monocyte/ thrombocyte count. The SII was calculated as (platelet count × neutrophil count) /lymphocyte count [23].
Serum CRP levels were measured nephelometrically (Siemens-Dimention, Germany).
Routine biochemical parameters in blood were measured with an automated analyzer (COBAS 8000, ROCHE-2007, Tokyo, Japan).
Ferritin tests of the patients were conducted with the Roche Cobas e 801 device.
Prothrombin time (PT), activated partial prothrombin time (aPTT) and International-normalized-ratio (INR) were determined with a completely digital coagulation instrument of Ceveron- Alpha (Diapharma Group Inc., West Chester, Canada). D-dimer were analyzed from the whole blood on the AQT90 flex RadiometerVR (Bronshoj, Denmark).
2.5. Nutritional Indeces
Calculation of PNI, CONUT, and NRI scores:
PNI will be calculated according to the following formula: 10 x serum albumin value (g/dL) + 0.005 x peripheral lymphocyte count (/mm³). A higher PNI indicates a high risk of malnutrition [24].
CONUT score will be calculated according to the following formula: Serum albumin level, total lymphocyte count and total cholesterol level (range 0-12, higher = worse) [25]. In this scoring system, points are assigned for laboratory measurements according to different ranges: Serum albumin ≥ 3.5 g/dL: 0 points; 3.49-3.0: 2 points; 2.99-2.5: 4 points; and <2.5: 6 points; lymphocytes -1600/μL: 0 points; 1200-1599: 1 point; 800-1199: 2 points; and <800: 3 points; and total cholesterol > 180 mg/dL: 0 points; 140-179: 1 point; 100-139: 2 points; and <100: 3 points.
NRI will be calculated according to the following formula [26]: NRI = [(1.519 × serum albumin, g/dL) + (41.7 × weight (kg) / ideal body weight (IBW; kg)] [27]. Ideal body weight will be calculated using the Lorentz formula; height (cm) - 100 - [(height (cm) - 150)/4)] for men and height (cm) - 100 - [(height (cm) - 150)/2.5)] for women. Body mass index (BMI) was calculated and will be classified according to the World Health Organisation (WHO). A lower NRI indicates a higher risk of malnutrition [28].
2.6. Statistical Analysis
Statistical Package for the Social Sciences version 21.0 software package for Windows (IBM Corp., Armonk, NY, USA) and Jamovi 2.4.11 were used for data evaluation and analysis. Frequencies (n) and percentages (%) were used to present the descriptive characteristics of the data while numerical variables were represented through mean±standard deviation or median (25. persentile-75. persentile). A chi-square test was used to evaluate the distribution among categorical variables. Whether the data was normally distributed was analyzed through visuals (histograms) and descriptive techniques (coefficient of variation, skewness, and kurtosis) and analytical methods (Kolmogorov Smirnov Test). Kruskal-Wallis test were used for comparison of continuous variables between more than two groups; adjusted p values were used for post-hoc significance. Mann-Whitney U test was used for comparison of normal distributed variables between two groups. The logistic regression analysis was used to determine the risk factors for stroke-related mortality. Results were represented as Odds ratio (OR) and 95% confidence interval (95% CI). The Spearman correlation analyses were used for to evaluate relationship between tho numerical variables. A p-value <0.05 was considered for statistical significance.
3. Results
Of the 1350 SVO patients included in the study, 58.8% had small vessel, 29.3% had large vessel and 11.9% had other etiologies (Figure 1). Clinical and laboratory characteristics of the patients according to the etiology groups are shown in Table 1 and Table 2.
The proportion of males was 52% in the small vessel etiology group, 39.1% in the large vessel group and 88.8% in the other etiology group and there was a significant difference between them (p<0.001). The proportion of males was 52% in the small vessel etiology group, 39.1% in the large vessel group and 88.8% in the other etiology group and there was a significant difference between them (p<0.001). While the frequency of hypertension was similar among the 3 etiology groups (p:0.112), the frequency of diabetes and dyslipidaemia was higher in the small vessel group than in the large vessel group (p:0.027; p:0.021, respectively). The frequency of smoking and alcoholism was significantly higher in the other etiology group compared to the small vessel and large vessel groups (p:<0.001; <0.001, respectively). Survival rate was 68.1% in SVO patients, 80.2% in small vessel etiology, 80% in other etiologies, and 38.9% in large vessel etiologies. Survival was statistically significantly lower in the large vessel etiology group (p<0.001).
NIHSS, National Institutes of Health Stroke Scale; CONUT, controlled nutritional status Kruskal-Wallis test were used for the comparisons. Adjusted p values were used to identify which groups differed signifacantly. Lowercase letters are superscripted (a,b,c,d) to identify which variables are differed significantly.
NLR was significantly lower in the other etiology group compared to the small vessel and large vessel groups (1.27 (0.75-1.83); 4.46 (3.81-5.18); 4.63 (3.15-5.69); p<0.001). SII was significantly lower in the other etiology group compared to the small vessel and large vessel groups (243.34 (142.97-367.66); 871.04 (650.62-1102.69); 898.17 (565.27-1165.79); p<0.001). There was a significant difference between the 3 etiology groups for PNI (p<0.001). The median PNI was 47.03 (41.33-52.85) in the other etiology group, 35.29 (33.69-37.25) in the small vessel group, and 34.11 (30.23-36.87) in the large vessel group. The median NRI was 62.33 (56.23-67.06) in the large vessel group, 54.07 (48.53-61.57) in the small vessel group and 52.96 (46.26-63.54) in the other etiology group (p<0.001). There was a significant difference between the 3 etiology groups for CRP (p<0.001). CRP median was 108.83 (66.42-247.63) in the large vessel group, 46.5 (18.97-82.84) in the small vessel group and 69.2 (42.09-99.83) in the other etiology group. CONUT scores were also different between the 3 etiology groups (p<0.001). The CONUT median was 5[5,6] in the small vessel group, 5[4,5,6] in the large vessel group and 4[4,4] in the other etiology group.
Table 3 shows the results of univariate and multivariate logistic regression analysis for to evaluate risk factors for death. When the risk factors for deaths-related ischemic stroke were evaluated, large vessel etiology was 145.9 (95%CI: 65.1-327.0) times and small vessel etiology was 5.207 (95%CI: 2.67-10.15) times more risky than other etiologies. Diabetes (OR: 1.404; 95%CI: 1.048-1.880), dyslipidaemia (OR: 1.910; 95%CI: 1.286-2.837), age (OR: 1.014; 95%CI: 1.005-1.023), PNI (OR: 1.224; 95%CI: 1.180-1.269), CONUT (OR: 1.742; 95%CI: 1.513-2.007) were also found as risk factors. In addition, BMI (OR: 0.941; 95%CI: 0.911-0.971) and diastolic blood pressure (OR: 0.981; 95%CI: 0.965-0.997) were found to be protective factors.
Table 4 shows the association between NLR, SII, PNI, NRI and CONUT in the whole group and in the aetiology subgroups. A very weak negative correlation was observed between NRI and PNI only in the whole group (r:-0.095; p<0.001) and in the other etiology group (r:-0.188; p:0.017). In the whole group, a negative correlation was observed between PNI and NLR (r:-0.692;p<0.001, Figure 2), SII (r:-0.591;p<0.001, Figure 3), CONUT (r:-0.685;p<0.001, Figure 3); in addition, significant correlation was observed between these variables in 3 etiology subgroups. Significant correlations were observed between CONUT and NLR (r:0.402;p<0.001, Figure 4), SII (r:0.312; p<0.001, Figure 5), in the whole group; these correlations were also observed in the large vessel and small vessel groups.
4. Discussion
Cerebrovascular diseases, defined as stroke, is one of the diseases leading to serious mortality and morbidity. Between 16-25% of stroke patients are malnourished at admission, and the rate of malnutrition increases to 60% as the hospitalization period prolongs [29,30,31]. One of the key findings of the study, there was a significant difference between the 3 etiology groups for PNI and CONUT. In addition, CONUT and PNI were also found to be independent risk factors for death. A negative significant correlation was observed between PNI and NLR, SII, CONUT. Significant correlations were observed between CONUT and NLR, SII. Nutrition and inflammation play a role in the development of cerebrovascular diseases. Malnutrition in patients with cerebrovascular events is caused by underlying comorbidities, medications and inflammation. Thus, it could be used as a reliable nutritional and inflammation risk stratification tool in patients with cerebrovascular diseases.
Inflammation can be defined as tissue damage or the body's unique response in the presence of inflammatory stimuli. Prolonged inflammation can lead to insulin resistance, diabetes, heart disease, obesity and metabolic syndrome. In addition to factors such as smoking, alcohol, chronic infection, physical injuries and traumas, excitement, microorganisms, nutrition is among the factors that trigger chronic inflammation [32]. In current study, the frequency of smoking and alcoholism was significantly higher in the other etiology group compared to the small vessel and large vessel groups. It suggests a potential association between these lifestyle factors with small vessel and large vessel groups. These factors could contribute to or be associated with the development of strokes in this specific subgroup [33].
The survival rates are associated with different etiologies of strokes [33]. In current study, a breakdown of the survival rates for each etiological group: Small Vessel Etiology (SVO): 68.1%; small vessel etiology: 80.2%; other etiologies: 80%; large vessel etiologies: 38.9%. These rates suggest variations in survival outcomes depending on the underlying cause of the stroke. It's important to note that survival rates can be influenced by various factors, including the severity of the stroke, promptness of medical intervention, the effectiveness of treatments, and individual patient characteristics. A lower survival rate in the large vessel etiologies group may indicate that strokes with large vessel involvement tend to be more severe or have a higher risk of complications. Conversely, higher survival rates in other groups may suggest better prognoses associated with those specific etiologies [34].
Inflammatory response plays an important role in the pathophysiology of acute ischemic stroke [35]. Inflammation mediators are released in low amounts in normal brain tissue. In the ischemic brain, however, the expansion of the lesion induces the release of proinflammatory cytokines and immune cells [36]. In acute ischemic stroke patients, increased leukocyte and neutrophil counts in the early period correlated with increased infarct volume and stroke severity [37]. NLR is a newly defined marker that can be calculated simply by subtyping leukocytes and reflects the systemic inflammatory state [38]. In current study, NLR and SII was significantly lower in the other etiology group compared to the small vessel and large vessel groups. In the context of stroke, elevated NLR and SII has been linked to worse outcomes, including increased risk of stroke severity, larger infarct size, and higher mortality rates. Maestrini et al. [39] reported that circulating neutrophil counts and NLR were correlated with stroke severity and stroke outcome in patients with acute cerebral ischemia. Higher neutrophil counts and NLR were also independently associated with poorer outcomes and higher mortality rate at 3 month [39]. Researchers are still investigating the precise role of NLR in stroke pathophysiology and its potential as a prognostic marker and therapeutic target. However, its simplicity and availability through routine blood tests make it an attractive candidate for further study in stroke research and clinical practice. High SII values have been found to be associated with disease severity and poor prognosis in many diseases and malignancies [40,41,42,43,44]. In a study by Agard et al. [44], the researchers reported that NLR and SII are easily obtained biomarkers that can be used in early clinical decision making in cases of mild acute ischemic stroke with negative CT scan upon admission. Modulation of the inflammatory cell function plays a role in repairing brain damage after ischemia. Systemic inflammatory response may be involved in the prognosis of acute ischemic stroke [45,46]. Researchers are still investigating the precise role of NLR and SII in stroke pathophysiology and its potential as a prognostic marker and therapeutic target. However, its simplicity and availability through routine blood tests make it an attractive candidate for further study in stroke research and clinical practice.
Malnutrition is a serious public health problem that is associated with adverse outcomes in in ischemic stroke patients. Several objective nutritional tools were performed for evaluating malnutrition risk, including the NRI [26], CONUT [25], and PNI score [24]. The NRI is a tool used to assess the nutritional status of individuals, particularly in clinical settings. It's calculated using body weight and serum albumin level, both of which are indicators of nutritional status. The NRI provides a numerical score that categorizes patients into different risk groups based on their nutritional status. It's particularly useful in identifying individuals who are at risk of malnutrition or who have poor nutritional status, which can have significant implications for their overall health and outcomes in various medical conditions, including stroke [47,48,49]. In current study, there was a significant difference between the 3 etiology groups for PNI and the NRI score was highest in the large vessel group. In stroke patients, malnutrition and poor nutritional status can exacerbate complications, impair recovery, and increase the risk of mortality. Therefore, the NRI and PNI serve as a valuable tool for healthcare professionals to identify patients who may benefit from nutritional interventions and support [47,48,49]. Studies have shown that lower NRI scores are associated with worse outcomes in stroke patients, including increased mortality, longer hospital stays, and higher rates of complications. By assessing nutritional risk using the NRI, healthcare providers can implement appropriate interventions, such as dietary modifications, nutritional supplementation, and interdisciplinary care, to optimize outcomes and improve the quality of life for stroke patients. Overall, the PNI and NRI is a useful tool in the management of stroke patients, helping healthcare providers identify and address nutritional risk factors that may impact recovery and outcomes.
The CONUT score is another tool used to assess the nutritional status of individuals. It takes into account three parameters: serum albumin concentration, total lymphocyte count, and total cholesterol concentration. These parameters reflect different aspects of nutritional status and immune function. Each parameter is scored individually based on predetermined cutoff values, and then the scores are summed to obtain the CONUT score. The scoring system may vary slightly depending on the specific study or protocol being used, but generally, higher scores indicate poorer nutritional status. The CONUT score has been shown to be useful in assessing nutritional status and predicting outcomes in various medical conditions, including stroke. In stroke patients, malnutrition is common and can have significant implications for recovery and outcomes [47,48,49]. In current study, there was a significant difference between the 3 etiology groups for CONUT score was highest in the small vessel group. By using the CONUT score to assess nutritional status in stroke patients, healthcare providers can identify those who may benefit from nutritional interventions such as dietary modifications, oral nutritional supplements, or enteral feeding. Early identification and management of malnutrition can help improve outcomes and quality of life for stroke patients. Overall, the CONUT score serves as a valuable tool in the comprehensive care of stroke patients, helping healthcare providers address nutritional needs and optimize recovery.
When evaluating the risk factors for death related to ischemic stroke with a large vessel etiology, several factors as severity of occlusion, extent of ınfarction, reperfusion status, presence of comorbidities, age may play significant roles . In current study, diabetes, dyslipidaemia, age, PNI, CONUT were also found as risk factors. In addition, BMI and diastolic blood pressure were found to be protective factors. Understanding these risk factors can help healthcare providers identify patients at higher risk of death following ischemic stroke with a large vessel etiology and implement appropriate interventions to optimize outcomes and reduce mortality rates. Early recognition, aggressive management, and comprehensive post-stroke care are essential for improving survival in this high-risk population.
In current study, to explore the correlation between stroke etiology (large vessel and small vessel groups) and various nutritional and inflammatory markers (NLR, SII, PNI, NRI, and CONUT), statistical analysis such as Pearson correlation coefficient or Spearman's rank correlation coefficient can be employed. These measures quantify the strength and direction of the linear relationship between two variables. Here's how each marker may correlate with stroke etiology. Analyzing these correlations can provide insights into the relationship between stroke etiology and nutritional/inflammatory markers, helping to identify potential predictors of stroke severity and prognosis. It's essential to interpret these findings within the context of the study population, considering factors such as comorbidities, treatment modalities, and other confounding variables.
Our study suggested the role of PNI, CONUT and NRI as a more accurate prognostic indicator of nutritional status in patients with ischemic stroke of small vessel, large vessel and other etiologies. NLR and SII may be important predictive markers in the course and prognosis of stroke. For each marker, comparing mean values or distributions between the two stroke groups can provide insights into potential differences in nutritional and inflammatory status associated with different stroke etiologies. Additionally, correlation analysis can be performed to assess the strength and direction of the relationship between each marker and stroke etiology within each group separately. These analyses can help identify markers that may serve as predictors of stroke severity or prognosis and contribute to our understanding of the underlying mechanisms of large vessel and small vessel strokes. Nutritional therapy in ischemic patients should be a key component of stroke treatment. However, this data needs to be verified with further studies to be done in the literature.
Author Contributions
NFM, NU, MC, EA, NS and SBS conceptualized and designed this study. NFM performed data acquisition. NFM, SBS and HU performed the statistical analyses. NFM and HU drafted the manuscript. All authors fnalized the manuscript. NFM, NU and HU supervised the entire process. The authors read and approved the fnal manuscript.
Funding
No funding was received for conducting this study.
Data Availability Statement
The primary author must be contacted with a valid request in order to provide the data sets used in this study. The email address is huzun59@hotmail.com.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no competing interests.
References
- World Health Organization. Cardiovascular diseases (CVDs) fact sheets. 2021.
- O’Donnell, M.J.; Chin, S.L.; Rangarajan, S.; Xavier, D.; Liu, L.; Zhang, H.; Rao-Melacini, P.; Zhang, X.; Pais, P.; Agapay, S.; et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): A case-control study. Lancet 2016, 388, 761–775. [Google Scholar] [CrossRef]
- Heidenreich PA, Trogdon JG, Khavjou OA, Butler J, et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2011;123(8):933–44.
- Global regional. and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795–820.
- Veerbeek, J.M.; Kwakkel, G.; van Wegen, E.E.; Ket, J.C.; Heymans, M.W. Early Prediction of Outcome of Activities of Daily Living After Stroke. Stroke 2011, 42, 1482–1488. [Google Scholar] [CrossRef]
- Moretti Anfossi C, Ahumada Muñoz M, Tobar Fredes C, et al. Work Exposures and Development of Cardiovascular Diseases: A Systematic Review. Ann Work Expo Health. 2022;66(6):698-713.
- Tsao CW, Aday AW, Almarzooq ZI, et al. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association [published correction appears in Circulation. 2023 Feb 21;147(8):e622] [published correction appears in Circulation. 2023 Jul 25;148(4):e4]. Circulation. 2023;147(8):e93-e621.
- Nishioka, S.; Okamoto, T.; Takayama, M.; Urushihara, M.; Watanabe, M.; Kiriya, Y.; Shintani, K.; Nakagomi, H.; Kageyama, N. Malnutrition risk predicts recovery of full oral intake among older adult stroke patients undergoing enteral nutrition: Secondary analysis of a multicentre survey (the APPLE study). Clin. Nutr. 2016, 36, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Buzby, G.P.; Mullen, J.L.; Matthews, D.C.; Hobbs, C.L.; Rosato, E.F. Prognostic nutritional index in gastrointestinal surgery. Am. J. Surg. 1980, 139, 160–167. [Google Scholar] [CrossRef]
- Ignacio de Ulíbarri, J.; González-Madroño, A.; de Villar, N.G.P.; González, P.; González, B.; Mancha, A.; Rodríguez, F.; Fernández, G. CONUT: A tool for controlling nutritional status. First validation in a hospital population. Nutr. Hosp. 2005, 20, 38–45. [Google Scholar]
- Veterans Affairs Total Parenteral Nutrition Cooperative Study Group. Perioperative total parenteral nutrition in surgical patients. N Engl J Med. 1991;325:525-532.
- Naito, H.; Hosomi, N.; Nezu, T.; Kuzume, D.; Aoki, S.; Morimoto, Y.; Yoshida, T.; Shiga, Y.; Kinoshita, N.; Ueno, H.; et al. Prognostic role of the controlling nutritional status score in acute ischemic stroke among stroke subtypes. J. Neurol. Sci. 2020, 416, 116984. [Google Scholar] [CrossRef] [PubMed]
- López Espuela F, Roncero-Martín R, Zamorano JDP, et al. Controlling Nutritional Status (CONUT) Score as a Predictor of All-Cause Mortality at 3 Months in Stroke Patients. Biol Res Nurs. 2019;21(5):564-570.
- Lee, M.; Lim, J.-S.; Kim, Y.; Lee, J.H.; Kim, C.-H.; Lee, S.-H.; Jang, M.U.; Oh, M.S.; Lee, B.-C.; Yu, K.-H. Association between Geriatric Nutritional Risk Index and Post-Stroke Cognitive Outcomes. Nutrients 2021, 13, 1776. [Google Scholar] [CrossRef]
- Xiang, W.; Chen, X.; Ye, W.; Li, J.; Zhang, X.; Xie, D. Prognostic Nutritional Index for Predicting 3-Month Outcomes in Ischemic Stroke Patients Undergoing Thrombolysis. Front. Neurol. 2020, 11, 599. [Google Scholar] [CrossRef] [PubMed]
- Dai, C.; Yan, D.; Xu, M.; Huang, Q.; Ren, W. Geriatric Nutritional Risk Index is related to the risk of stroke-associated pneumonia. Brain Behav. 2022, 12, e2718. [Google Scholar] [CrossRef]
- Gibson, P.H.; Cuthbertson, B.H.; Croal, B.L.; Rae, D.; El-Shafei, H.; Gibson, G.; Jeffrey, R.R.; Buchan, K.G.; Hillis, G.S. Usefulness of Neutrophil/Lymphocyte Ratio As Predictor of New-Onset Atrial Fibrillation After Coronary Artery Bypass Grafting. Am. J. Cardiol. 2010, 105, 186–191. [Google Scholar] [CrossRef]
- Zahorec, R. Ratio of neutrophil to lymphocyte counts--rapid and simple parameter of systemic inflammation and stress in critically ill. Bratislavske Lekarske Listy 2001, 102, 5–14. [Google Scholar]
- Celikbilek, A.; Ismailogullari, S.; Zararsiz, G. Neutrophil to Lymphocyte Ratio Predicts Poor Prognosis in Ischemic Cerebrovascular Disease. J. Clin. Lab. Anal. 2014, 28, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Gökhan, S.; Ozhasenekler, A.; Durgun, H.M.; Akil, E.; Ustündag, M.; Orak, M. Neutrophil lymphocyte ratios in stroke subtypes and transient ischemic attack. . 2013, 17, 653–7. [Google Scholar]
- Tokgoz S, Keskin S, Kayrak M, Seyithanoglu A, Ogmegul A. Is neutrophil/lymphocyte ratio predict to short-term mortality in acute cerebral infarct independently from infarct volume? J Stroke Cerebrovasc. 2014;23(8), 2163-8.
- Kwon, H.-M.; Lee, Y.-S.; Bae, H.-J.; Kang, D.-W. Homocysteine as a Predictor of Early Neurological Deterioration in Acute Ischemic Stroke. Stroke 2014, 45, 871–873. [Google Scholar] [CrossRef]
- Hu B, Yang XR, Xu Y, Sun YF, Sun C, Guo W, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014; 20: 6212–22.
- Nishikawa, H.; Yoh, K.; Enomoto, H.; Ishii, N.; Iwata, Y.; Takata, R.; Nishimura, T.; Aizawa, N.; Sakai, Y.; Ikeda, N.; et al. The Relationship between Controlling Nutritional (CONUT) Score and Clinical Markers among Adults with Hepatitis C Virus Related Liver Cirrhosis. Nutrients 2018, 10, 1185. [Google Scholar] [CrossRef] [PubMed]
- Iseki, Y.; Shibutani, M.; Maeda, K.; Nagahara, H.; Ohtani, H.; Sugano, K.; Ikeya, T.; Muguruma, K.; Tanaka, H.; Toyokawa, T.; et al. Impact of the Preoperative Controlling Nutritional Status (CONUT) Score on the Survival after Curative Surgery for Colorectal Cancer. PLOS ONE 2015, 10, e0132488. [Google Scholar] [CrossRef]
- Bo, Y.; Wang, K.; Liu, Y.; You, J.; Cui, H.; Zhu, Y.; Lu, Q.; Yuan, L. The Geriatric Nutritional Risk Index Predicts Survival in Elderly Esophageal Squamous Cell Carcinoma Patients with Radiotherapy. PLOS ONE 2016, 11, e0155903–e0155903. [Google Scholar] [CrossRef] [PubMed]
- Al-Najjar, Y.; Clark, A.L. Predicting Outcome in Patients With Left Ventricular Systolic Chronic Heart Failure Using a Nutritional Risk Index. Am. J. Cardiol. 2012, 109, 1315–1320. [Google Scholar] [CrossRef] [PubMed]
- Onodera, T.; Goseki, N.; Kosaki, G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai zasshi 1984, 85, 1001–1005. [Google Scholar]
- Corrigan ML, Escuro AA, Celestin J, et al. Nutrition in the stroke patient. Nutr Clin Pract 2011; 26(3): 242-252.
- Sánchez-Moreno, C, Jiménez-Escrig A, Martín A. Stroke: Roles of B vitamins, homocysteine and antioxidants. Nutr Res Rev 2009; 22(1): 49-67.
- Mosselman MJ, Kruitwagen CL, Schuurmans MJ, et al, Malnutrition and risk of malnutrition in patients with stroke: Prevalence during hospital stay. J Neurosci Nurs 2013; 45(4): 194-204.
- Chen, L.; Deng, H.; Cui, H.; Fang, J.; Zuo, Z.; Deng, J.; Li, Y.; Wang, X.; Zhao, L. Inflammatory responses and inflammation-associated diseases in organs. Oncotarget 2018, 9, 7204–7218. [Google Scholar] [CrossRef]
- Velez, L.; Toffel, S.; Trejo-Lopez, J.; Kresak, J.L.; Beal, S.G. Educational Case: Etiologies, Mechanisms, and Treatment of Stroke. Acad. Pathol. 2020, 7, 2374289520901817. [Google Scholar] [CrossRef]
- Blank-Stein, N.; Mass, E. Macrophage and monocyte subsets in response to ischemic stroke. Eur. J. Immunol. 2023, 53, e2250233. [Google Scholar] [CrossRef]
- Chamorro A, Hallenbeck J. The harms and benefits of inflamatory and immune responses in vascular disease. Stroke. 2006;37:291-3.
- Worthmann, H.; Tryc, A.; Deb, M.; Goldbecker, A.; Ma, Y.; Tountopoulou, A.; Lichtinghagen, R.; Weissenborn, K. Linking infection and inflammation in acute ischemic stroke. Ann. New York Acad. Sci. 2010, 1207, 116–122. [Google Scholar] [CrossRef]
- Buck BH, Liebeskind DS, Saver JL, et al. Early neutrophilia is associated with volume of ischemic tissue in acute stroke. Stroke. 2008;39(2):355-360.
- Xue, J.; Huang, W.; Chen, X.; Li, Q.; Cai, Z.; Yu, T.; Shao, B. Neutrophil-to-Lymphocyte Ratio Is a Prognostic Marker in Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2017, 26, 650–657. [Google Scholar] [CrossRef]
- Maestrini I, Tagzirt M, Gautier S, et al. Analysis of the association of MPO and MMP-9 with stroke severity and outcome: Cohort study. Neurology. 2020;95(1):e97-e108.
- Mureșan, E.-M.; Golea, A.; Vesa. C.; Lenghel, M.; Csutak, C.; Perju-Dumbravă, L. Emergency department point-of-care biomarkers and day 90 functional outcome in spontaneous intracerebral hemorrhage: A single-center pilot study. Exp. Ther. Med. 2022, 23, 200. [Google Scholar] [CrossRef]
- Xie, M.; Yuan, K.; Zhu, X.; Chen, J.; Zhang, X.; Xie, Y.; Wu, M.; Wang, Z.; Liu, R.; Liu, X. Systemic Immune-Inflammation Index and Long-Term Mortality in Patients with Stroke-Associated Pneumonia. J. Inflamm. Res. 2023, 16, 1581–1593. [Google Scholar] [CrossRef]
- Huang, Y.-W.; Yin, X.-S.; Li, Z.-P. Association of the systemic immune-inflammation index (SII) and clinical outcomes in patients with stroke: A systematic review and meta-analysis. Front. Immunol. 2022, 13, 1090305. [Google Scholar] [CrossRef]
- Yang, R.; Chang, Q.; Meng, X.; Gao, N.; Wang, W. Prognostic value of Systemic immune-inflammation index in cancer: A meta-analysis. J. Cancer 2018, 9, 3295–3302. [Google Scholar] [CrossRef]
- Agard, T.A.; Hass, R.; Cavrak, M.E.; Foual, N.S.; Byrum, C.; Adcock, A.K.; Gehan, D.; Petrone, A.B. Neutrophil lymphocyte ratio (NLR) and systemic immune inflammatory index (SII) for the differential diagnosis of CT-negative mild acute ischemic stroke and transient ischemic attack. Int. J. Neurosci. 2023, 1–8. [Google Scholar] [CrossRef]
- Jiang, X.; Andjelkovic, A.V.; Zhu, L.; Yang, T.; Bennett, M.V.L.; Chen, J.; Keep, R.F.; Shi, Y. Blood-brain barrier dysfunction and recovery after ischemic stroke. Prog. Neurobiol. 2018, 163–164, 144–171. [Google Scholar] [CrossRef]
- Jayaraj, R.L.; Azimullah, S.; Beiram, R.; Jalal, F.Y.; Rosenberg, G.A. Neuroinflammation: Friend and foe for ischemic stroke. J. Neuroinflamm. 2019, 16, 142. [Google Scholar] [CrossRef] [PubMed]
- Yuan, K.; Zhu, S.; Wang, H.; Chen, J.; Zhang, X.; Xu, P.; Xie, Y.; Zhu, X.; Zhu, W.; Sun, W.; et al. Association between malnutrition and long-term mortality in older adults with ischemic stroke. Clin. Nutr. 2021, 40, 2535–2542. [Google Scholar] [CrossRef] [PubMed]
- Raposeiras Roubín S, Abu Assi E, Cespón Fernandez M, et al. Prevalence and Prognostic Significance of Malnutrition in Patients With Acute Coronary Syndrome. J Am Coll Cardiol. 2020;76(7):828-840.
- akmak EÖ, Öcal L, Erdoğan E, et al. Prognostic Value of 3 Nutritional Screening Tools to Predict 30-Day Outcome in Patients Undergoing Carotid Artery Stenting. Angiology. 2022;73(3):225-233.
- Pikula A, Howard BV, Seshadri S. Stroke and Diabetes. In: Cowie CC, Casagrande SS, Menke A, et al., eds. Diabetes in America. 3rd ed. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases (US); August 2018.
- Jensen, M.; Thomalla, G. Causes and Secondary Prevention of Acute Ischemic Stroke in Adults. 2019, 40, 022–030. [CrossRef]
- Bae, D.J.; Willey, J.Z.; Ibeh, C.; Yuzefpolskaya, M.; Colombo, P.C. Stroke and Mechanical Circulatory Support in Adults. Curr. Cardiol. Rep. 2023, 25, 1665–1675. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A flow chart of the selection of cases.
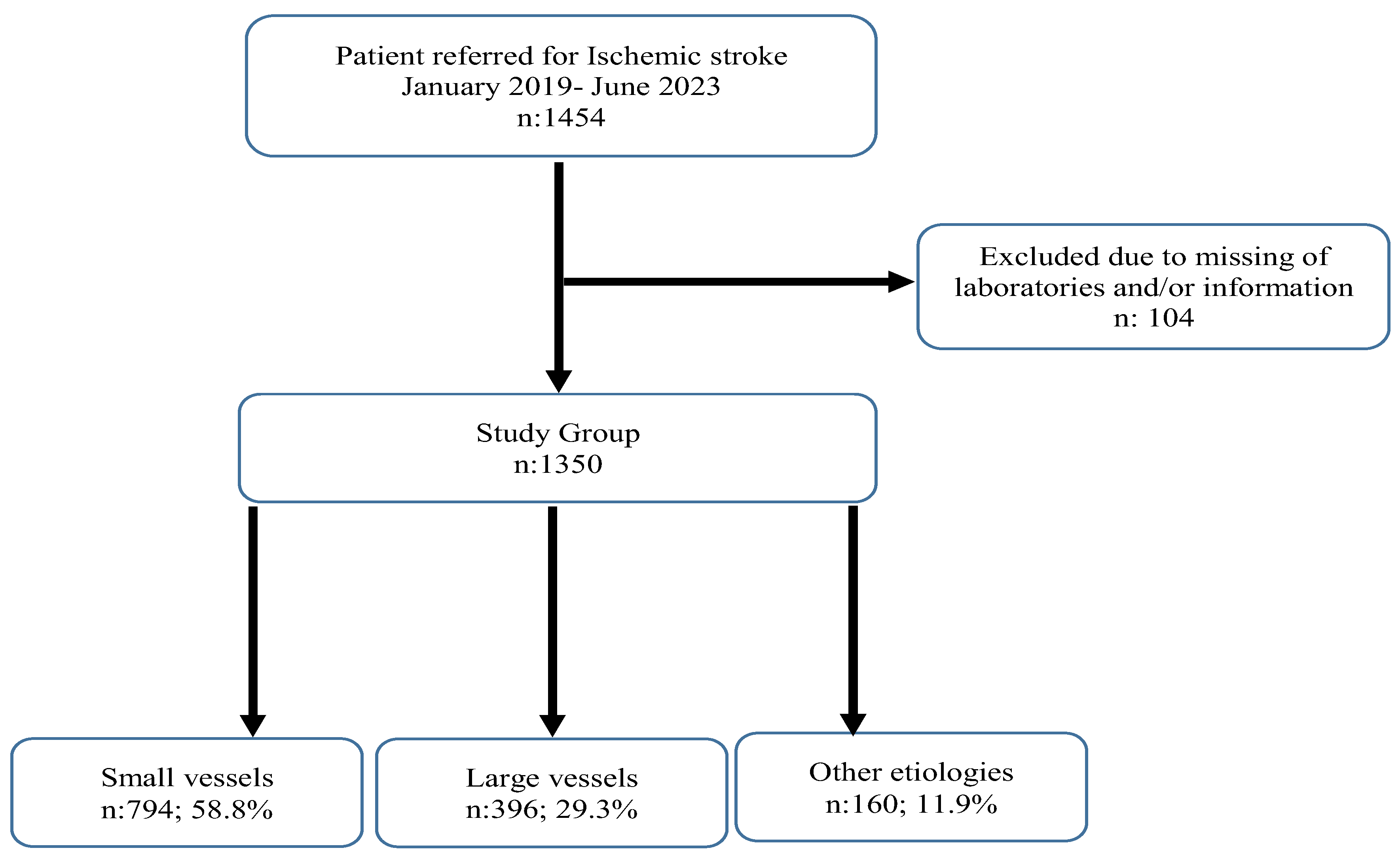
Figure 2.
The relationship between PNI and SII.
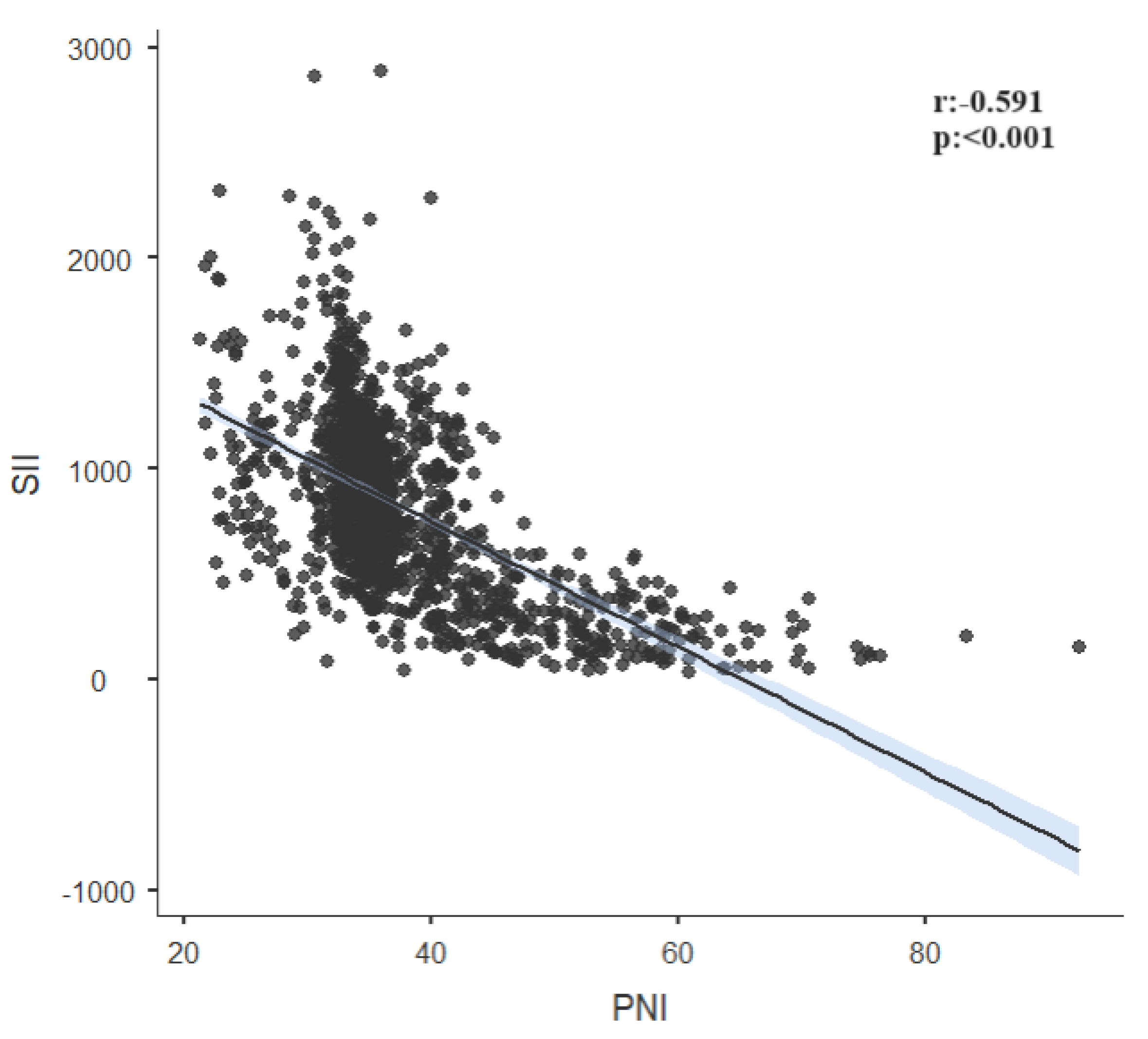
Figure 3.
The relationship between CONUT and PNI.
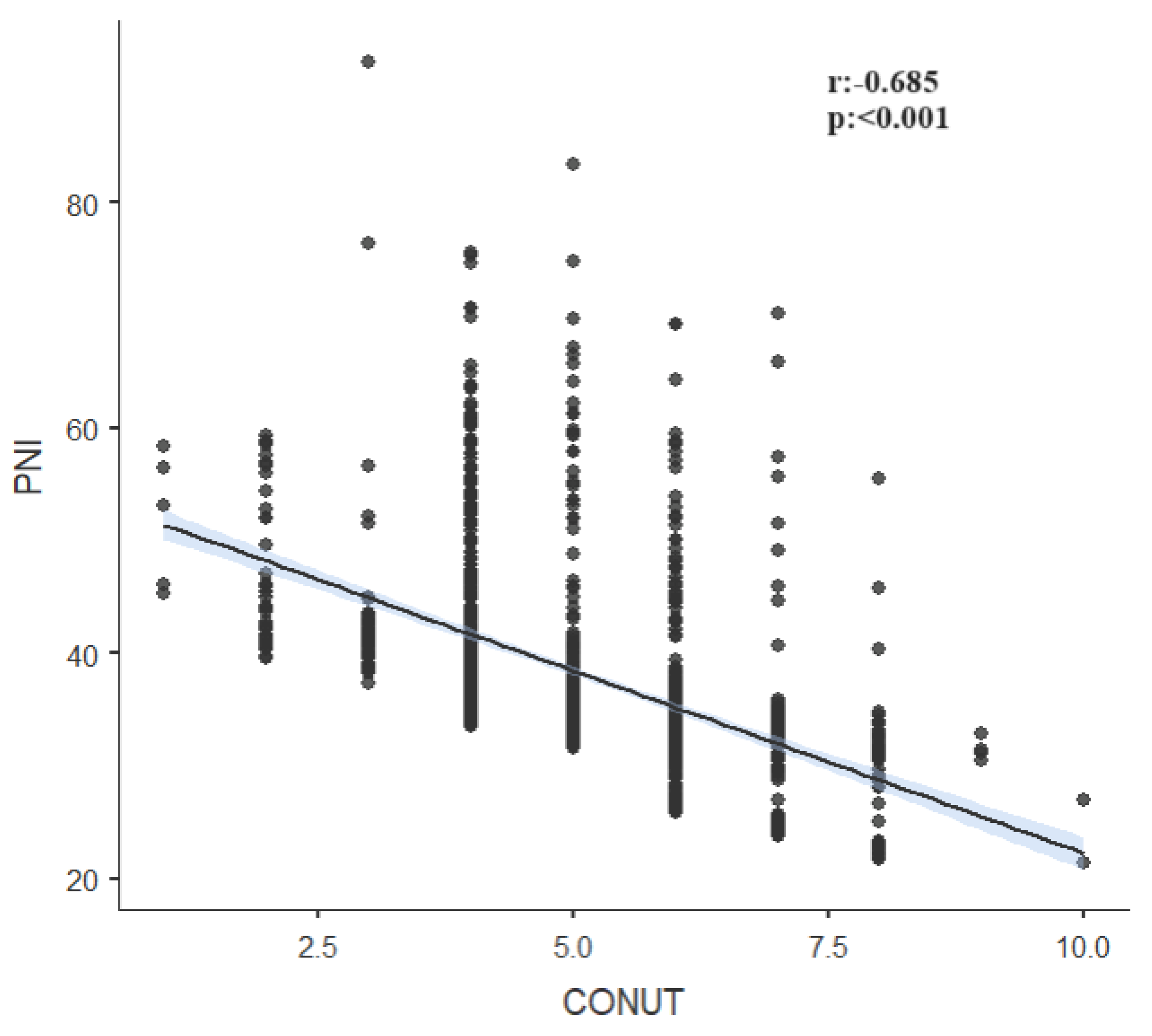
Figure 4.
The relationship between CONUT and NLR.
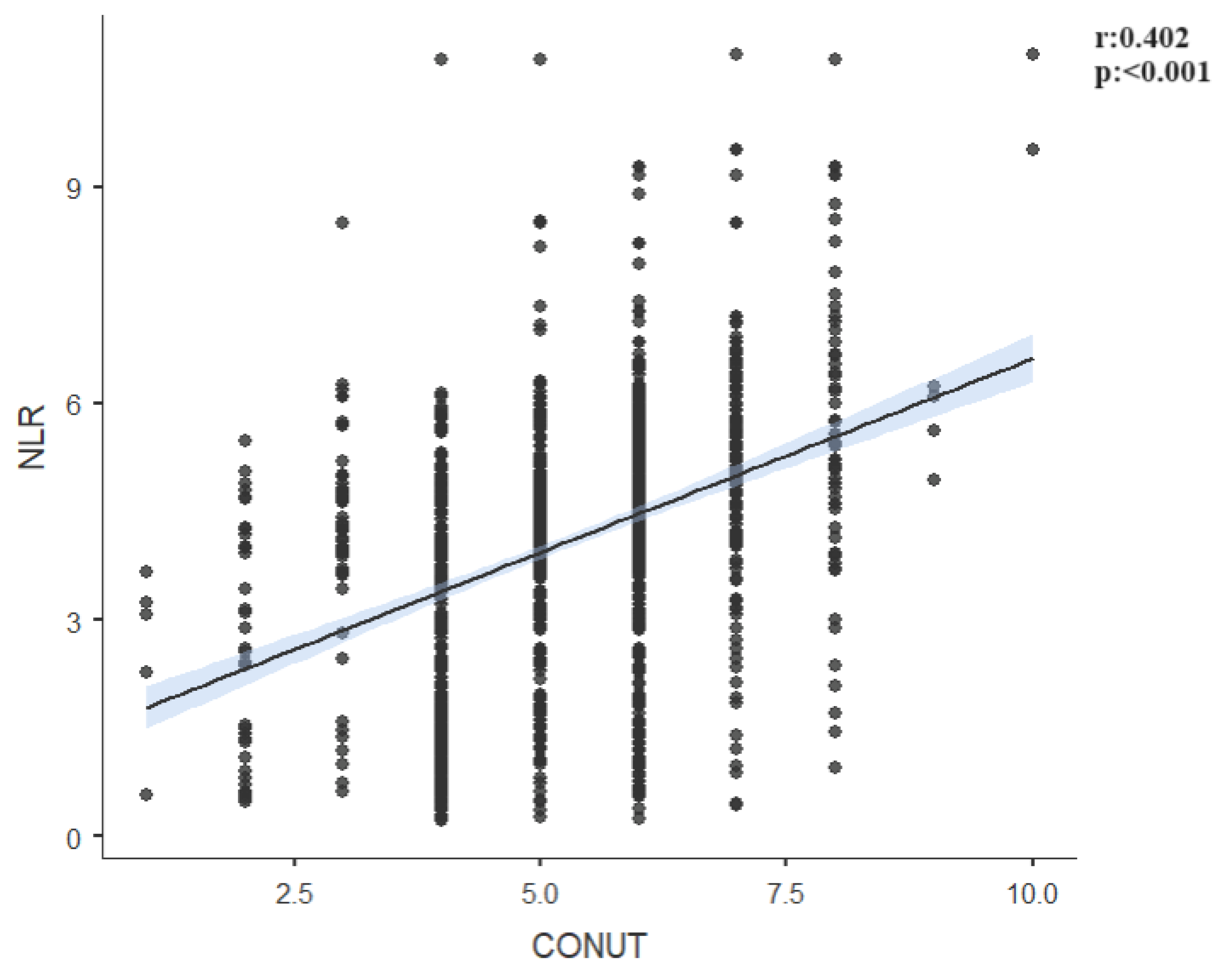
Figure 5.
The relationship between CONUT and SII.
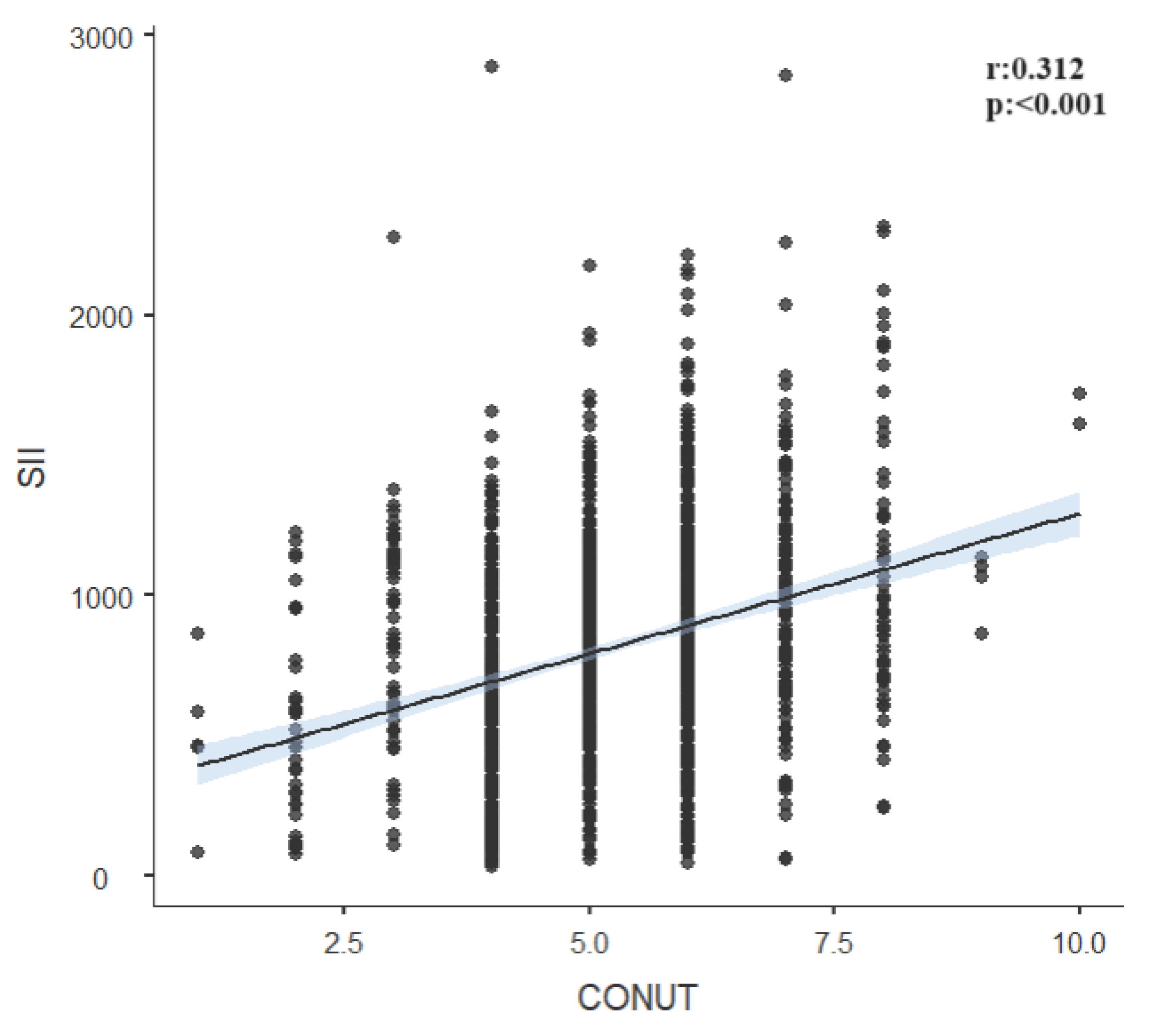

Table 1.
The distribution of gender and clinical characteristics according to etiology groups.
| All Groups | Small vessels(n:794; 58.8%) | Large vessels(n:396; 29.3%) | Other etiologies(n:160; 11.9%) | ||
|---|---|---|---|---|---|
| Gender | n(%) | n(%) | n(%) | n(%) | p value |
| Male | 710 (52.60%) | 413 (52.00%)a | 155 (39.10%)b | 142 (88.80%)c | <0.001 |
| Female | 640 (47.40%) | 381 (48.00%) | 241 (60.90%) | 18 (11.30%) | |
| Hypertension | 1046 (77.50%) | 630 (79.30%) | 293 (74.00%) | 123 (76.90%) | 0.112 |
| Diabetes | 649 (48.10%) | 399 (50.30%)a | 168 (42.40%)b | 82 (51.30%)a,b | 0.027 |
| Dyslipidemia | 1101 (81.60%) | 667 (84.00%) a | 309 (78.00%) b | 125 (78.10%) a,b | 0.021 |
| Smoking | 784 (58.10%) | 457 (57.60%) a | 201 (50.80%)a | 126 (78.80%)b | <0.001 |
| Alcoholism | 353 (26.10%) | 202 (25.40%) a | 82 (20.70%) a | 69 (43.10%) b | <0.001 |
| Survival | 919 (68.10%) | 637 (80.20%) a | 154 (38.90%)b | 128 (80.00%) a | <0.001 |
Chi-square test was applied.
Table 2.
The comparison of personal and laboratory characteristics of etiology groups.
| All Groups | Small vessels | Large vessels | Other etiologies | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean±Std | Median(25p-75p) | Mean±Std | Median(25p-75p) | Mean±Std | Median(25p-75p) | Mean±Std | Median(25p-75p) | p value | |
| Age (years) | 64.38±16.43 | 66(54-77) | 64.8±16.59 | 67(54-77) | 64.3±16.65 | 66(54-78) | 62.54±14.96 | 64(54.5-72.5) | 0,139 |
| Body Mass Index (kg/m2) | 28.3±5.26 | 27.78(24.28-32.27) | 27.23±4.97b | 26.57(23.41-30.74)b | 31.01±4.33a | 31.31(27.77-33.93)a | 26.94±6.24b | 25.87(22.46-31.74)b | <0.001 |
| Temperature (0C) | 36.99±0.46 | 37.1(36.7-37.5) | 37±0.46 | 37.1(36.7-37.5) | 36.99±0.44 | 36.9(36.7-37.5) | 36.94±0.45 | 36.9(36.6-37.3) | 0,337 |
| Systolik Blood Preasure (mmHg) | 157±20.2 | 153(143-163) | 155.22±19.28 a | 153(141-157) a | 159.61±20.88b | 154(144-164) b | 159.39±22.03a,b | 154(144-163) a,b | 0,005 |
| Diastolik Blood Preasure(mmHg) | 85.35±8.88 | 85(79-88) | 84.46±8.58 a | 84(79-88) a | 86.77±9.18 b | 85(80-89) b | 86.21±9.09 a,b | 85(79-88) a,b | 0,003 |
| NIHSS | 6.46±1.6 | 7(6-8) | 6.39±1.62 | 7(5-8) | 6.52±1.55 | 7(6-8) | 6.65±1.6 | 7(6-8) | 0,160 |
| Lymphocytes count | 2297.93±1539.62 | 1743.5(1459-2074) | 2041.91±1368.65 a | 1693.5(1459-1973) a | 2024.12±1327.16 a | 1667(1348.5-1998) a | 4246.06±1435.3 | 4200(2985-5370)b | <0.001 |
| Neutrophils count | 7260.04±1943.96 | 7786(6343-8212) | 7498.5±1369.85 a | 7832.5(7535-8194) a | 7536.37±2102.73 a | 7871(6330-8457) a | 5392.8±2781.42 b | 4670(3510-6900) b | <0.001 |
| Neutrophil lymphocyte ratio (NLR) | 4.06±1.81 | 4.23(2.96-5.16) | 4.35±1.4 a | 4.46(3.81-5.18) a | 4.54±1.93 a | 4.63(3.15-5.69) a | 1.44±0.95 b | 1.27(0.75-1.83) b | <0.001 |
| Systemic immune-inflammation index (SII) | 816.54±421.87 | 807.68(506.32-1092.19) | 872.76±346.11 a | 871.04(650.62-1102.69) a | 917.22±470.13 a | 898.17(565.27-1165.79) a | 288.36±204.25 b | 243.34(142.97-367.66) b | <0.001 |
| White blood cells count | 9.27±2.03 | 9(7.6-11) | 9.29±2.04 | 9(7.6-11) | 9.15±1.99 | 8.9(7.55-10.75) | 9.53±2.07 | 9.2(7.85-11.45) | 0,157 |
| Platelet count | 201.55±47.81 | 205.65(164.9-242.1) | 201.38±47.31 | 203.95(165.1-241.3) | 202.1±49.05 | 208.75(163.95-243.25) | 201.05±47.44 | 201.25(166.55-241.85) | 0,926 |
| Fasting glucose (mg/dL) | 134.35±56.77 | 120(102-145) | 134.07±56.61 | 120(102-145) | 134.57±56.08 | 120(100-145) | 135.18±59.52 | 120(102-145) | 0,971 |
| Albumin (g/dL) | 2.62±0.34 | 2.61(2.55-2.7) | 2.7±0.25 b | 2.62(2.59-2.72) b | 2.47±0.44 a | 2.6(2.29-2.69) a | 2.61±0.34 b | 2.61(2.54-2.71) b | <0.001 |
| Prognostic nutritional index (PNI) | 37.71±8.45 | 35.34(33.32-39.96) | 37.25±7.23 a | 35.29(33.69-37.25) a | 34.78±8.16 b | 34.11(30.23-36.87) b | 47.3±8.06 c | 47.03(41.33-52.85) c | <0.001 |
| Nutritional risk index (NRI) | 57.23±9.53 | 56.46(49.95-64.40) | 55.33±9.06 b | 54.07(48.53-61.57) b | 62.02±7.70 a | 62.33(56.23-67.06) a | 54.78±11.49 b | 52.96(46.26-63.54)b | <0.001 |
| Total cholesterol (mg/dL) | 232.72±145.96 | 159(146-267) | 149.02±11.41 a | 149(140-156) a | 346.79±174.67 b | 276(194-527) b | 365.78±138.26 a,b | 317.5(278-395) a,b | <0.001 |
| C-reactive protein (CRP) mg/L | 89.57±87.25 | 66.42(33.32-100.84) | 56.36±57.96 a | 46.5(18.97-82.84) a | 155.69±102.42 b | 108.83(66.42-247.63) b | 90.78±73.38 | 69.2(42.09-99.83) c | <0.001 |
| CONUT | 5.23±1.33 | 5(4-6) | 5.49±1.2 a | 5(5-6) a | 5.12±1.46 b | 5(4-6) b | 4.22±1.11 | 4(4-4) c | <0.001 |
Table 3.
The univariate and multivariate regression analysis results for to evaluate risk factors for death.
Table 3.
The univariate and multivariate regression analysis results for to evaluate risk factors for death.
| Univariate | Enter | Backward | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | p value | OR (95% CI) | p value | OR (95% CI) | p value | |
| Etiology (ref: Other etiology) | <0.001 | <0.001 | <0.001 | |||
| Small Vessels | 0.986(0.645-1.508) | 0.948 | 5.379(2.652-10.910) | <0.001 | 5.207(2.67-10.15) | <0.001 |
| Large vessels | 6.286(4.061-9.73) | <0.001 | 154.3(67.7-351.6) | <0.001 | 145.9(65.1-327.0) | <0.001 |
| Diabetes | 1.159(0.922-1.457) | 0.207 | 1.407(1.050-1.886) | 0.022 | 1.404(1.048-1.880) | 0.023 |
| Dyslipidemia | 1.643(1.196-2.258) | 0.002 | 2.067(1.308-3.268) | 0.002 | 1.910(1.286-2.837) | 0.001 |
| Age (years) | 1.008(1.001-1.015) | 0.024 | 1.014(1.005-1.023) | 0.003 | 1.014(1.005-1.023) | 0.003 |
| Body Mass Index (kg/m2) | 1.015(0.993-1.037) | 0.180 | 0.908(0.481-1.712) | 0.765 | 0.941(0.911-0.971) | <0.001 |
| Diastolik Blood Preasure (mmHg) | 0.989(0.976-1.002) | 0.088 | 0.982(0.965-0.998) | 0.030 | 0.981(0.965-0.997) | 0.023 |
| NIHSS | 1.059(0.985-1.138) | 0.121 | 0.949(0.857-1.051) | 0.317 | - | - |
| NLR | 0.846(0.793-0.903) | <0.001 | 0.984(0.820-1.179) | 0.858 | - | - |
| SII | 0.999(0.999-1.000) | <0.001 | 1.000(0.999-1.000) | 0.575 | - | - |
| PNI | 1.057(1.042-1.072) | <0.001 | 1.214(1.164-1.265) | <0.001 | 1.224(1.180-1.269) | <0.001 |
| NRI | 1.008(0.996-1.020) | 0.187 | 1.019(0.718-1.447) | 0.915 | - | - |
| CONUT | 0.950(0.872-1.035) | 0.244 | 1.743(1.483-2.049) | <0.001 | 1.742(1.513-2.007) | <0.001 |
Table 4.
The correlation analyses between inflamatuar markers and nutritional markers in all groups and etiology sub-groups.
Table 4.
The correlation analyses between inflamatuar markers and nutritional markers in all groups and etiology sub-groups.
| All Group | |||||
|---|---|---|---|---|---|
| Variables | SII | PNI | NRI | CONUT | |
| NLR | r | 0.826 | -0.692 | 0.034 | 0.402 |
| p | <0.001 | <0.001 | 0.208 | <0.001 | |
| SII | r | -0.591 | 0.039 | 0.312 | |
| p | <0.001 | 0.148 | <0.001 | ||
| PNI | r | -0.095 | -0.685 | ||
| p | <0.001 | <0.001 | |||
| NRI | r | -0.029 | |||
| p | 0.289 | ||||
| Small Vessels | |||||
| SII | PNI | NRI | CONUT | ||
| NLR | r | 0.694 | -0.653 | -0.036 | 0.335 |
| p | <0.001 | <0.001 | 0.311 | <0.001 | |
| SII | r | -0.455 | -0.015 | 0.164 | |
| p | <0.001 | 0.674 | <0.001 | ||
| PNI | r | 0.022 | -0.676 | ||
| p | 0.544 | <0.001 | |||
| NRI | r | -0.024 | |||
| p | 0.497 | ||||
| Large Vessels | |||||
| SII | PNI | NRI | CONUT | ||
| NLR | r | 0.837 | -0.577 | 0.004 | 0.389 |
| p | <0.001 | <0.001 | 0.937 | <0.001 | |
| SII | R | -0.504 | 0.023 | 0.321 | |
| p | <0.001 | 0.650 | <0.001 | ||
| PNI | r | -0.029 | -0.825 | ||
| p | 0.570 | <0.001 | |||
| NRI | r | -0.018 | |||
| p | 0.720 | ||||
| Other Etiologies | |||||
| SII | PNI | NRI | CONUT | ||
| NLR | R | 0.919 | -0.531 | 0.107 | 0.079 |
| p | <0.001 | <0.001 | 0.178 | 0.319 | |
| SII | r | -0.509 | 0.090 | 0.064 | |
| p | <0.001 | 0.258 | 0.424 | ||
| PNI | r | -0.188 | -0.434 | ||
| p | 0.017 | <0.001 | |||
| NRI | r | 0.035 | |||
| p | 0.659 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



